Submitted:
29 December 2023
Posted:
29 December 2023
You are already at the latest version
Abstract
Tuberculosis (TB) is an infectious disease of global public health importance, caused by the Mycobacterium tuberculosis complex. Despite advances in diagnosis and treatment, this disease has worsened with the emergence of multidrug-resistant strains of tuberculosis We aim to present and review the history, progress, and future directions in the diagnosis of tuberculosis by evaluating the current methods of laboratory diagnosis of tuberculosis, with a special emphasis on microscopic examination, cultivation on solid and liquid medium, as well as an approach to molecular assays. The microscopic method, although widely used, has its limitations, and the use and evaluation of other techniques are essential for a complete and accurate diagnosis. Bacterial culture, both in solid and liquid mediums, are essential methods in the diagnosis of TB. Culture on solid medium provides specificity and accuracy, while culture on liquid medium brings rapidity and increased sensitivity. Molecular tests such as LPA and Xpert MTB/RIF have been found to offer significant benefits in the rapid and accurate diagnosis of TB, including drug-resistant forms. These tests allow the identification of resistance mutations and provide essential information for choosing the right treatment. We conclude that combined diagnostic methods, using several techniques and approaches, provide the best result in the laboratory diagnosis of TB. Improving the quality and accessibility of tests, as well as the implementation of advanced technologies, is essential to help improve the sensitivity, efficiency, and accuracy of TB diagnosis.
Keywords:
Tuberculosis
; Diagnosis
; Laboratory
1. Introduction
Tuberculosis (TB) is an infectious disease of global public health importance caused by the Mycobacterium tuberculosis complex. Alarmingly, the disease has worsened with the emergence of multidrug-resistant strains of tuberculosis (MDR-TB) [1]. Annually, it is estimated that approximately 450,000 new cases of MDR-TB occur according to a report from 2021 [2].
Early diagnosis and appropriate treatment of tuberculosis is an essential public health priority. In this context, microbiology laboratories play a vital role in rapid and accurate detection of tuberculosis and drug resistance.
According to the latest WHO report on tuberculosis, it reveals the dire consequences of the COVID-19 pandemic on access to diagnosis and treatment for the disease, jeopardizing global efforts to fight tuberculosis. The significant progress made before the pandemic has been interrupted or even reversed, accentuating the challenges in achieving the set goals.
One of the significant effects of the pandemic was the decline in the global number of people diagnosed with tuberculosis. In 2020, there was an 18% reduction compared to the previous year, followed by a partial recovery in 2021. Countries such as India, Indonesia and the Philippines recorded the steepest declines, meaning an increase in untreated cases, with potentially fatal impact and possibility of community spread of infection [2].
The estimated number of deaths caused by tuberculosis experienced a significant increase in the period 2019-2021, thus reversing the downward trend of the precedent years. In 2021, approximately 1.6 million deaths were recorded, of which 1.4 million were HIV-negative and 187,000 were HIV-positive. This worrying trend underscores the devastating impact of tuberculosis in the context of HIV infection [3].
There is an alarming increase in the global incidence rate of tuberculosis in the year 2021, reversing the downward trend maintained in previous decades. In parallel, there is a rise in cases of drug-resistant tuberculosis, which adds an additional layer of complexity to the management of the disease. Treatment of drug-resistant tuberculosis has also been affected by the pandemic. In 2020, the treatments experienced a temporary decrease, followed by a partial recovery in 2021. This evolution underlines the fragility of the medical system in the face of major external factors such as the COVID-19 pandemic [4,5].
To effectively treat tuberculosis, it is necessary to first make the correct diagnosis of the affected people. However, last year only 6.4 million out of a total of 10.6 million people with active TB were diagnosed and notified, which is a gap of about 40%. This gap indicates an urgent need to improve the process of TB diagnosis and access to appropriate health care [6,7].
- The role of the laboratory in the diagnosis and treatment of tuberculosis (TB) is crucial. In developed countries, the use of new technologies has facilitated rapid and accurate diagnosis, identification of the causative species, and determination of drug sensitivity [8]. In recent years, molecular tests based on nucleic acid amplification techniques have been developed. They provide a rapid, sensitive, and specific diagnosis of tuberculosis and allow the determination of drug sensitivity status. These molecular techniques are currently available or being implemented in developing countries. Nevertheless, traditional diagnostic methods such as microscopy and cultures cannot yet be completely replaced. Molecular tests can be applied in parallel with these methods for the diagnosis of TB or for drug susceptibility testing. However, the application of these molecular tests is often limited by the constraints of sputum sample storage and safe transport from remote health centers to central laboratories.
- Modern clinical microbiology laboratories have at their disposal a number of methods that provide an accurate and rapid laboratory diagnosis of tuberculosis. Molecular methods are now part of the diagnostic algorithm in many laboratories and have dramatically shortened the time to diagnosis [9].
- Improving the accessibility and use of current diagnostic methods, including direct microscopy, culture, and drug susceptibility testing, as well as the adoption of molecular TB diagnostic technologies, should be a priority in disease control efforts [10].
- Advances in molecular biology have led to the development of methods for the quick detection of M. tuberculosis and its drug resistance, thus providing important tools for the development of more efficient and sensitive diagnostic methods to contribute to tuberculosis control.
- In countries where TB laboratory services are integrated into general laboratory services or operate as a major private sector, the question arises whether improving the quality and accessibility of laboratory services can effectively contribute to TB control or will only expand their capacity.
- Recent evidence shows that the previous approach of providing separate and parallel TB laboratories was not effective enough to improve the health system. Currently, the quality of TB laboratories is increasing, and this can act as a catalyst or, conversely, as a limiting factor for other aspects of TB control [10].
Accurate and prompt diagnosis of TB is essential for the control and management of the disease, but there are numerous factors that affect the effectiveness of this process. These problems include the difficulty of correctly diagnosing latent and active forms of TB, the lack of precise protocols for different types of TB, and the difficulty of accessing diagnostic facilities in regions with limited resources [7,11].
It is essential to perform accurate drug susceptibility testing and to understand the genetic basis of M. tuberculosis drug resistance. Modern clinical microbiology laboratories have methods that provide accurate and rapid laboratory diagnosis of TB. However, the complications associated with MDR-TB and the increasing incidence of extremely drug-resistant (XDR) TB highlight the need for improved identification techniques for M. tuberculosis and drug susceptibility testing. In this regard, molecular biology has played an important role in the development of methods for the rapid detection of M. tuberculosis and its drug resistance. Research in the field of molecular diagnosis of tuberculosis is constantly advancing.
In addition, new treatment-resistant strains are emerging in areas where the disease was thought to have been eradicated. It is imperative to develop affordable, accurate and rapid diagnostic technologies adapted to the needs of developing countries [12].
The aim of this paper is to review and present the history, progress, and future directions in the molecular diagnosis of tuberculosis, including the general principles, diagnostic value, advantages, and disadvantages of molecular methods used for the detection and identification of Mycobacterium tuberculosis and associated disease. This review provides a comprehensive study on the use of microscopic examination, solid culture medium, liquid culture medium and molecular tests and highlight issues regarding TB diagnosis and suggest future directions for diagnostic research and development of TB.
2. Microscopic diagnosis of TB
2.1. Microscopic examination with Ziehl-Neelsen staining
Laboratory diagnosis of pulmonary tuberculosis is essential in combating the disease, having a significant role in patient management and isolation of contagious cases. In many developing countries with a high incidence of TB, advanced diagnostic methods and drug susceptibility testing are rarely available. These countries still rely on traditional methods of microscopic diagnosis and culture, but ineffective management and insufficient resources have hindered progress in (TB) control [13].
The standard method in laboratory diagnosis remains the microscopic examination of tuberculous bacilli in sputum smears, a technique that has been around for over 100 years. This provides valuable information for confirming the diagnosis and assessing the contagiousness of the patient [14,15].
Ziehl-Neelsen (ZN) staining microscopy is an essential method in the diagnosis of tuberculosis, especially where there is limited availability of facilities and equipment required for bacterial culture. This method is fast and offers the possibility to detect cases with a high bacterial load and a high risk of transmission [16,17].
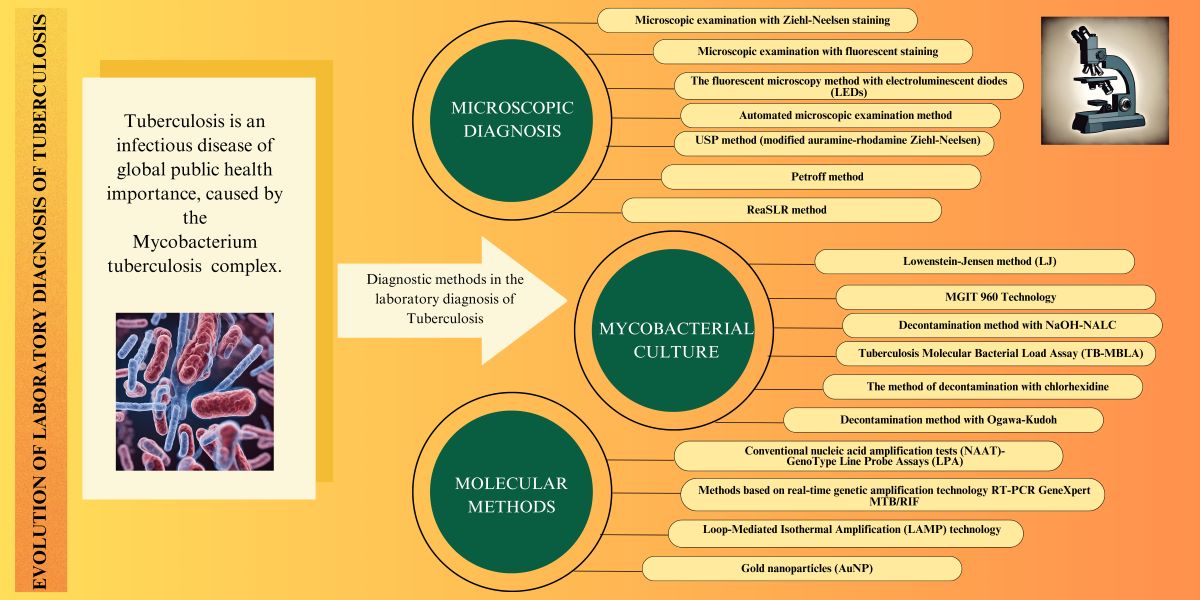
Figure 1.
Mycobacterium tuberculosis in sputum. Ziehl Neelsen staining at x1000 magnification; M. tuberculosis bacteria appear as thin and red bacilli. These bacteria are generally of variable length, but they are usually between 2-4 microns in length and 0.2-0.5 microns in width. In this staining method the bacteria appear on a pale blue background.
Figure 1.
Mycobacterium tuberculosis in sputum. Ziehl Neelsen staining at x1000 magnification; M. tuberculosis bacteria appear as thin and red bacilli. These bacteria are generally of variable length, but they are usually between 2-4 microns in length and 0.2-0.5 microns in width. In this staining method the bacteria appear on a pale blue background.
Sputum staining is a crucial technique for the diagnosis of pulmonary tuberculosis. Although analysis of sputum stained with acid-fast fuchsin (FA) is quick and simple, it can present problems and provide incorrect results in certain clinical situations. Ziehl-Neelsen staining, on the other hand, is a more accessible technique but has its limitations, with many factors that can influence the sensitivity and specificity of the results [18].
The sensitivity of the Ziehl-Neelsen staining test in sputum smear is influenced by the number of bacteria present and it has been evaluated in different studies with a variation between 22% and 80%, requiring between 104 and 105 bacilli in each ml of sputum for test to become positive [10,16,19].However, in cases of extrapulmonary tuberculosis, co-infected with HIV or in children, the number of bacteria may be lower than that required to obtain an optimal ZN staining [20,21].
On the other hand, research on study of a group of 544 adults with chronic cough, systematically chosen from two primary care clinics revealed significant aspects as follow[22]. The prevalence of HIV infection in the study cohort was 83%. Tuberculosis was the most common diagnosis, being confirmed or probable in 207 HIV-positive patients (46%) and in 27 HIV-negative patients (30%). Among them, 145 HIV-positive TB patients (70%) and 20 HIV-negative TB patients (74%) had smear-positive TB cases. Only 17 HIV-positive patients and 2 HIV-negative patients were found to have smear-negative but culture-positive TB cases. Another study showed a prevalence of 37.4% of TB/HIV co-infection [23]. But, it is important to note that the method is less effective in detecting tuberculosis in patients with HIV infection, due to the complexity of co-infection and the need for higher diagnostic sensitivity.
In some isolated regions of low-income countries, microscopic examination of sputum smears may be the only laboratory diagnostic method available, diagnosis of pulmonary TB being performed on clinical symptoms, chest radiography and the result of microscopic smear tests. The procedure involves appropriate staining of mycobacteria, with the widespread use of the Ziehl-Neelsen stain, which highlights acid-fast bacilli in shades of red-purple [24,25].
However, this method has some limitations. It requires specialized personnel, is time-consuming, and can result in a variable sensitivity of 60% to 70% compared to the culture method. In addition, there is a risk of errors in manual reporting of results. In countries with a high prevalence of pulmonary tuberculosis, laboratory professionals may be overworked and experience fatigue from the heavy workload. Also, the staining methods used require considerable resources [26].
Some of these factors include proper sample handling, thickness of smears, preparation and storage of reagents, quality of microscopes, and duration of staining [27]. In case of negative results, culture methods are used as a reference. In countries with a low incidence of tuberculosis, culture methods and other approaches are essential to identify and differentiate tuberculosis from other similar diseases caused by atypical mycobacteria [28].
In Papua New Guinea, the traditional method of sputum examination for tuberculosis involves the use of untreated sputum, a practice that presents some problems. The low sensitivity of the method and the potential risk of spreading tuberculosis bacteria in the laboratory are significant problems. In contrast, processing sputum with bleach, a more affordable and effective method, can improve the sensitivity of the test and reduce the risk of contamination in the laboratory. Thus, the use of bleach is proposed as a better, affordable, and effective alternative in sputum processing for TB diagnosis [29].
The relationship between the results of sputum smear microscopy and the time required to obtain positive results in liquid cultures was also investigated. It was found that the time required to obtain positive results is inversely proportional to the number of bacilli detected in the smears. There is also a tendency to accelerate the time to positive status, especially in the first two months of treatment. However, a significant proportion of patients continue to show acid-fast bacilli in sputum smears after two months of treatment[30].
2.2. Microscopic examination with fluorescent staining
In high-income countries, the commonly used method includes the use of concentrated smears with fluorescent staining, which can improve the sensitivity of the test, but involves higher costs [16,31].This technique involves the use of special fluorescent dyes that bind to bacteria and emit fluorescent light under illumination of a certain wavelength[32,33].The sensitivity of the FA method varies between 20% and 60%, and the concentrations of dyes, such as carbol-fuchsin and methylene blue, are essential for the detection of the M. tuberculosis. WHO recommends certain dye concentrations, but there are suggestions that the use of higher concentrations may improve results in clinical settings [34,35].
Auramine staining is a more sensitive and less time-consuming technique for the diagnosis of pulmonary tuberculosis compared to the conventional ZN method. This uses the mycolic acids in the cell wall of the bacteria to retain auramine O more efficiently than the carbol-fuchsin dye. Auramine O can detect M. tuberculosis in culture-negative specimens, which is useful in extrapulmonary tuberculosis [36].
2.3. The fluorescent microscopy method with electroluminescent diodes (LEDs)
Compared to the traditional Ziehl-Neelsen staining method. LED fluorescence microscopy (FM) is more affordable, more durable, and easier to use in the medical system. It also has the advantage that LEDs have a longer lifespan and do not emit ultraviolet (UV) light, reducing the need for darkrooms and energy consumption. This method increases the sensitivity and speed of sample examination, facilitating rapid detection of M. tuberculosis bacteria [37,38].
A study conducted in India showed how the Revised National Tuberculosis Control Program (RNTCP) adopted LED microscopy to replace the ZN method in Designated Microscopy Centers (DMC) in India. A significant change in the practice of microscopy centers was observed with the adoption of fluorescence microscopy with LEDs, thus replacing the traditional ZN method [37]. However, despite the progress made, this transition does not come without challenges.
One of these notable challenges concerns the instability of fluorescent dyes, which can affect the reliability and consistency of results obtained with this new method. Moreover, an important observation is that currently there are still no standardized international guidelines to direct and ensure quality in the efficient application of LED fluorescence microscopy [37,39].
A study carried out in Tanzania in 2017 investigated the frequency of non-tuberculous mycobacterial (NTM) infections among patients with a culture-negative diagnosis of pulmonary tuberculosis (TB) in countries with limited technology. From a sample of 94 patients, it was found that 26.60% had confirmed M. tuberculosis infections, while the rest were unconfirmed or false positive cases. In addition, cases of infections with nontuberculous mycobacteria and other bacteria were identified in culture-negative specimens. This emphasizes the importance of using advanced TB differential diagnosis techniques and rigorous clinical laboratory practices to avoid unnecessary administration of anti-TB drugs [40].
In Sudan, another study evaluated a new fluorescent technique compared to the ZN method for the detection of M. tuberculosis. The results showed that the fluorescent method is 16% more sensitive and three times faster than the ZN method [41].
Another study evaluated the effectiveness of different methods of diagnosing tuberculosis using sputum samples collected from patients suspected of having this disease. Of 362 samples analyzed, LED-FM identified 36 samples as positive, representing 9.9%, while (ZN) identified 42 (11.6%) and GeneXpert identified 50 (13.8%). Of the samples evaluated for the presence of mycobacteria, eight were identified as non-tuberculous mycobacteria (NTM). Of the remaining 332 samples, 45 (13.6%) were confirmed to have tuberculosis by culture, and 11 of these were co-infected with HIV (24.4%). The LED-FM and Gene Xpert methods showed good sensitivity and specificity in identifying tuberculosis cases [42].
2.4. Automated microscopic examination method
To assist pathologists in TB diagnosis and to avoid the conventional time-consuming manual screening process, Artificial Intelligence-Based Methods for identifying TB in ZN staining displaying a variety of specificity and sensibility. This method uses an automated microscope and specialized software to perform an operator-independent examination [43,44,45].
The automated method demonstrated a detection limit of bacilli/ml of sputum and a 100% positivity rate in the evaluation of sputum inoculated with Mycobacterium bovis, M. bacillus Calmette-Guerin (BCG) or Mycobacterium tuberculosis H37Rv.
In the evaluation of 93 sputum samples, the automated method achieved a sensitivity of 97.06% and a specificity of 86.44%. This method allows the storage and reading of up to 100 smear slides and allows the export of the results in the laboratory information system. Based on the preliminary results, it is proposed to implement this automated method in the routine workflow, where only smears detected positive by examination automated microscopic examination will be confirmed by standard microscopic examination [46].
2.5. USP method (modified auramine-rhodamine Ziehl-Neelsen)
This method uses a fluorescence microscope to make the bacteria visible and easy to identify. The tuberculosis diagnostic method uses the dyes: auramine and rhodamine, which bind to bacteria, including M. tuberculosis, becoming fluorescent under ultraviolet light. These bacteria are then visualized in a fluorescence microscope, highlighting them in the dark. However, the method may have limits in precision, and positive results require further confirmation by other, more precise methods, such as bacterial culture or molecular tests. A study from India published in 2014 analyzed the effectiveness of a new microscopy method called universal sample processing (USP), which has the potential to be used in laboratories with different infrastructure levels for the diagnosis of tuberculosis. Compared to the direct method and the NALC-NaOH smear microscopy method, the USP method demonstrated a marked improvement in sensitivity, identifying 18 additional positive samples, indicating the limitations of the direct smear method in detecting samples with a high bacilli load [47].There are studies showing the use of saliva in combination with AR fluorescent staining technique shows significant efficacy in diagnosis and screening of patients with pulmonary tuberculosis, obtaining a positivity of 76%, compared to 70% obtained by laboratory culture [48].
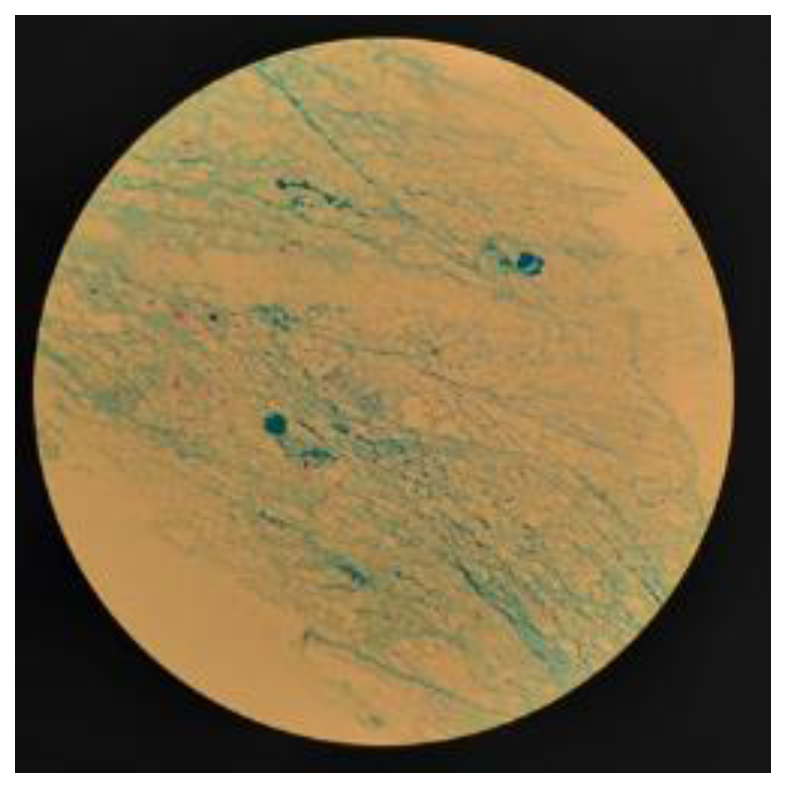
Figure 2.
Auramine-rhodamine fluorescent stain. Acid-fast bacteria usually appear fluorescent colors ranging from deep yellow to bright orange and red in this technique. Acid-fast bacilli may appear singly, in pairs, or in small groups, depending on the species detected and their density in the sample examined. The background in this staining technique is dark or black, which makes the fluorescent bacteria stand out clearly.
Figure 2.
Auramine-rhodamine fluorescent stain. Acid-fast bacteria usually appear fluorescent colors ranging from deep yellow to bright orange and red in this technique. Acid-fast bacilli may appear singly, in pairs, or in small groups, depending on the species detected and their density in the sample examined. The background in this staining technique is dark or black, which makes the fluorescent bacteria stand out clearly.
2.6. Petroff method
This is a technique used in microbiology laboratories to concentrate and process M. tuberculosis bacteria from sputum samples in order to increase the efficiency and sensitivity of subsequent tuberculosis tests. The process includes collection of sputum samples, preparation of a digestion solution to break down the samples, dilution and homogenization, centrifugation to sediment the bacteria, decantation and re-suspension of the bacteria in a concentrated solution. These concentrated bacteria are then used for various diagnostic tests, contributing to increased sensitivity and rapid and accurate diagnosis of tuberculosis. However, compared to the modified Petroff method, the USP method did not show a significant improvement in sensitivity [49].
In addition, no notable differences in diagnostic accuracy were found between the USP method and the modified Petroff method. Regarding culture methods, both USP and modified Petroff methods showed similar percentages of positivity, but the USP method had a higher culture contamination rate. Also, a disadvantage of the USP method is the high cost, due to the use of several expensive chemicals. In conclusion, the USP method, although providing better sensitivity than the direct method and the NALC-NaOH smear microscopy method, does not provide significant improvements over the modified Petroff method. Furthermore, the USP method is associated with higher rates of crop contamination and high costs [50].
2.7. ReaSLR method
This ReaSLR technique represents an innovative and affordable approach for processing sputum samples for the purpose of TB diagnosis. It is a simple and economical method that has had a significant impact on the sensitivity of smear microscopy in the detection of tuberculosis. The process involves fast liquefaction of the sputum sample with ReaSLR reagent, followed by filtration, concentration by centrifugation, and use of the resulting sediment for smear microscopy.
In a study carried out by the Department of Microbiology at the Sanjay Gandhi Institute of Medical Sciences in Lucknow, India, a total of 150 sputum samples were collected from patients with clinical suspicion of pulmonary TB, participants in either an inpatient clinic or at an outpatient clinic within the hospital between October 2012 and January 2013. In this context, the ReaSLR method, a simple and economical technique for diagnosing tuberculosis by processing sputum, was evaluated. The results showed that compared to the modified Petroff method, the ReaSLR method achieved a higher percentage of positive results (31.33% versus 12%). With a sensitivity of 90.47% and a specificity of 91.6%, the ReaSLR method outperformed the modified Petroff method, which recorded a sensitivity of 40.47% and a specificity of 99.07%. These findings indicate that the ReaSLR method shows potential as a more sensitive and promising option for the diagnosis of pulmonary tuberculosis and could be included in tuberculosis control programs. However, it is important to conduct further studies to evaluate the effectiveness of this method on a large scale [51].
3. Mycobacterial culture in TB diagnosis
3.1. Lowenstein-Jensen method (LJ)
Culture is the gold standard for the diagnosis of tuberculosis and a highly specific and sensitive detection method that can increase positivity by up to 30% in cases of negative sputum smear microscopy, providing definitive confirmation of the presence of M. tuberculosis and further allowing to perform drug susceptibility testing [52]. The Löwenstein-Jensen (LJ) culture technique involves taking a biological sample, such as sputum, which is then spread evenly over the surface of the solid medium. The medium is then kept under controlled temperature and humidity conditions, allowing the mycobacteria to grow and form characteristic colonies.
These colonies can then be examined under a microscope to identify the presence of specific tuberculosis bacteria. Colony development and morphology can provide essential information for accurate diagnosis. Despite its increased sensitivity compared to the examination of smears for acid-fast bacilli (80-85%), theLJ method is time-consuming, with results available after an incubation of 4-6 weeks [53]. False-positive MTB cultures are rarely questioned, but rates vary from 2% to 4%. Strict adherence to laboratory techniques and recognizing the possibility of false-positive MTB cultures, especially when they are not consistent with clinical data, are essential in preventing misdiagnosis of tuberculosis [54,55].
A study conducted in Indonesia for one year aimed to evaluate the performance of Thin-Layer Agar T (TLA) culture in the diagnosis of tuberculosis compared to the LJ culture method. The sensitivity of TLA was significantly higher than for LJwith a median time to detection significantly shorter, so TLA has been proposed as an equivalently sensitive but faster alternative, compared to the traditional method on LJ[56].
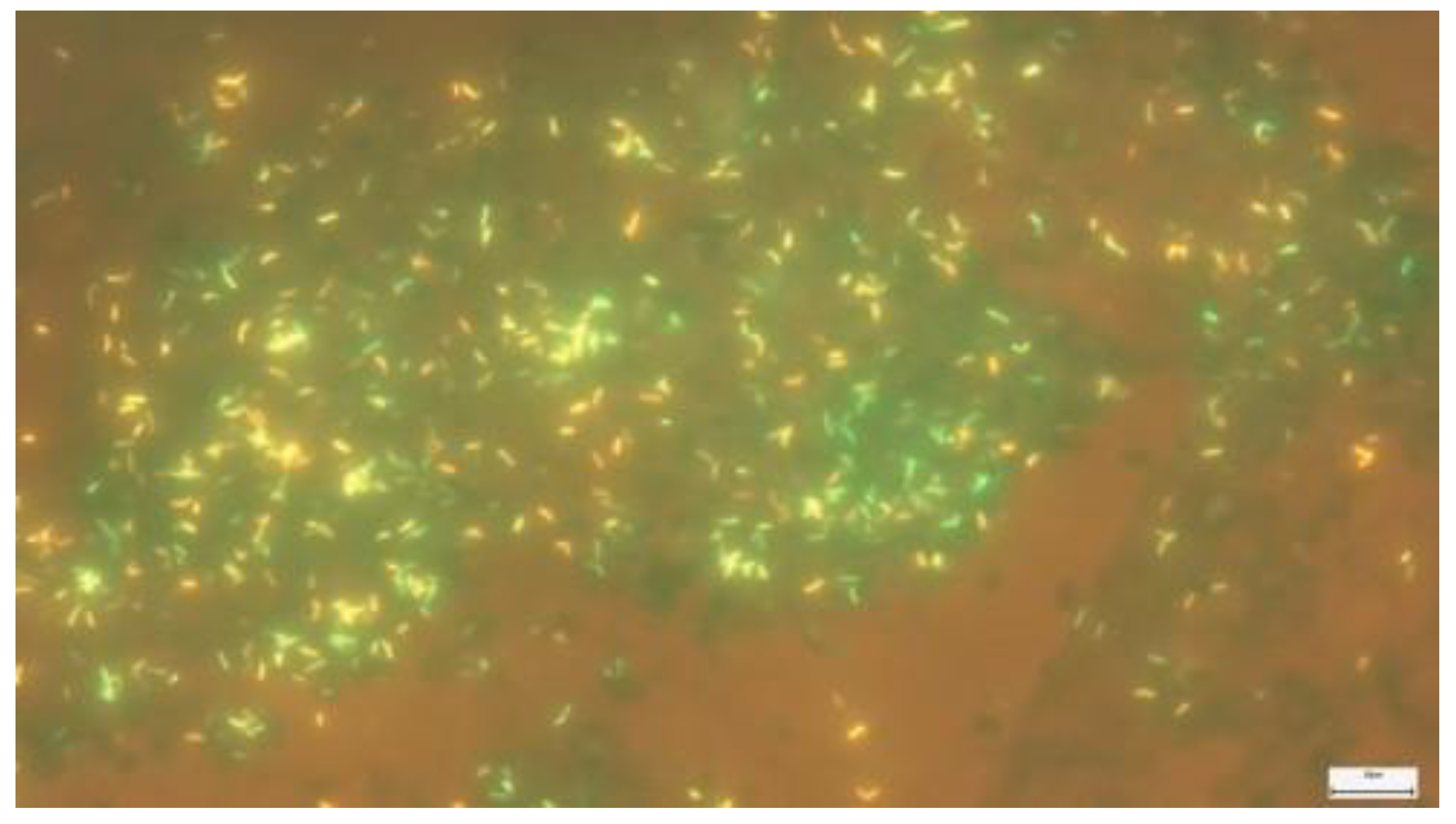
Figure 4.
Lowenstein-Jensen medium (LJ) characteristic colonies of M. tuberculosis.
3.2. MGIT 960 Technology
The MGIT 960 technique (Mycobacteria Growth Indicator Tube 960) is an advanced and automated method for the detection and cultivation of the bacterium M. tuberculosis. This innovative technique was developed to improve the efficiency and speed of the diagnostic process, allowing the growth of mycobacteria in special liquid media, in a controlled and monitored system. Biological samples are collected from patients with suspected tuberculosis and then treated to eliminate possible contaminants, ensuring a uniform suspension of bacteria. This bacterial suspension is placed in special culture tubes called "MGIT tubes", which contain an optimal liquid medium with nutrients and a fluorescent indicator. The MGIT tubes are inserted into an automatic device, BACTEC™ MGIT™ 320 instrument (Becton Dickinson) which continuously monitors the bacteria. As the bacteria multiply, they consume nutrients and produce gases, which leads to increased fluorescence and this is a detection in real time [57].
The BACTEC system Mycobacteria Growth Indicator Tube (MGIT) (Becton Dickinson, Taipei, Taiwan) is a sensitive, safe and automated liquid culture solution. However, the short time to a positive result is not reflected in rapid identification of mycobacteria in liquid cultures. Typically, the Mycobacterium complex tuberculosis (MTBC) and non-tuberculous mycobacteria (NTM) from positive MGIT cultures for growth and acid fast (AFB) (hereafter referred to as positive MGIT cultures) are identified by subculture on solid media. MTBC in liquid cultures can be identified in approximately 15 minutes through a variety of tape tests immunochromatographic [58].
Based on a thorough review of the scientific evidence and advice from experts in the field, this recommendation led to the adoption of liquid culture media as the reference standard in the diagnosis of tuberculosis. Although these provide faster results (approximately 10 days), liquid media are more susceptible to contamination and require special precautions to prevent cross-contamination [59]. National Reference Laboratory, from Colombia National Laboratory Network and National Institute of Health and Public Health Laboratories of Antioquia, carried out a comparative study between the method BACTEC™ MGIT™ 960 and the nitrate reductase (NRA) assay versus the ratio method on the Löwenstein-Jensen medium. The aim was to evaluate resistance to antituberculosis drugs. Of the 183 Mycobacterium isolates tuberculosis analyzed, MGIT 960 revealed a sensitivity and specificity of 90% for isoniazid (INH) and 100% and 99.4% for rifampicin (RMP), respectively. NRA showed a sensitivity and specificity of 86% and 94.7%, respectively, for INH, and 100% and 99% for PMR [60].
3.3. Decontamination method with NaOH-NALC
Sample decontamination is a crucial step in the preparation of biological samples before they are inoculated on Lowenstein-Jensen medium and liquid MGIT medium, distinct techniques used in the diagnosis of tuberculosis. Despite the fact that solid media are more resistant to contamination, the waiting time for obtaining results is higher. Also, liquid systems and drug susceptibility testing are more complex and sensitive but require rigorous control of contamination and isolation of nontuberculous mycobacteria [53].
Decontamination with the (NaOH-NALC) method is an essential step in the TB diagnosis process, but it is important to emphasize that the use of N-acetyl-L-cysteine (NALC) and sodium hydroxide (NaOH) can negatively influence recovery and viability bacteria in the samples.
This finding emphasizes the need for a careful approach to diagnostic and treatment methods [61,62].The conclusions obtained from the study indicate that the use of the (NALC-NaOH) method leads to a decrease in the efficiency in the recovery of M. tuberculosis bacteria from the samples. This finding is consistent with results obtained in previous studies, which observed a decrease in the recovery rate of approximately 20%. This emphasizes the need to adopt molecular diagnostic techniques for the precise identification of this bacterium [63].
Another article from Baltimore, Maryland presented a new sample processing method for more efficient detection of mycobacteria. This method used a substance called C18-carboxypropylbetaine (CB-18) and had increased sensitivity in both smear tests and cultures. Additional parameters of the CB-18 method were studied, showing that eliminating an incubation step further improved the results of the culture assays. The CB-18 method was compared with two other current processing methods (NALC-NaOH and Tween 80) for the recovery of mycobacterial isolates. The CB-18 method achieved the best results, with an average recovery of tuberculous isolates of 86% and non-tuberculous isolates of 73% [63].
Another study conducted reveals that long transport of samples to culture laboratories can lead to contamination and substantial loss of viability, thus impacting bacterial culture results. Cetylpyridinium chloride (CPC) transport medium using Difco buffer led to marked improvement in culture results [64,65].
As a result, transport of samples in CPC followed by decontamination with NALC-NaOH and neutralization with Difco buffer, gave the best culture results, both on liquid MGIT and on LJ mediums. These findings may lead to improved sample processing methods in tuberculosis diagnostic laboratories [65].
3.4. Tuberculosis Molecular Bacterial Load Assay (TB-MBLA)
It is a molecular bacterial burden assay to measure the loss of viability of M. tuberculosis following treatment with NALC-NaOH of M. tuberculosis H37Rv pure culture and clinical sputum samples from patients with pulmonary TB.
Following this study, the impact of NALC-NaOH use on MTB was investigated. By comparing this traditional method with a modern technique called MBLA, the researchers found that the use of NALC-NaOH leads to a significant decrease in the detectable bacterial load. This phenomenon was associated with a reduction in the number of colonies forming units (CFU) per milliliter and the number of viable cultures on solid media. Moreover, the use of NALC-NaOH has been observed to prolong the time required to obtain positive results in liquid cultures [66].
3.5. The method of decontamination with chlorhexidine
Another chlorhexidine method was shown to be less harmful to the viability of M. tuberculosis bacteria compared to the NALC-NaOH method. This allows better recovery of intact and viable bacteria from samples, which increases diagnostic sensitivity and accuracy.
A study conducted by the Institute Hospitalo-Universitaire from Marseille University in France focused on evaluating the effectiveness of chlorhexidine in the decontamination of sputum samples for MTB cultivation. By testing different concentrations of chlorhexidine (0.1%, 0.5% and 0.7%) on a sample of 191 clinical samples, the researchers identified that a concentration of 0.7% chlorhexidine recorded a contamination rate of 0%. These results suggest that chlorhexidine is an effective option for decontaminating sputum samples for MTB isolation, providing a reliable method of sample preparation for subsequent culture and detection [64].
3.6. Decontamination method with Ogawa-Kudoh
The Ogawa-Kudoh culture medium decontamination and inoculation method allows bacteria to be sampled, decontaminated, and cultivated in a controlled environment, facilitating the identification and confirmation of the presence of tuberculosis.
This culture medium contains agar, malt extract, glycerol and other nutrients that favor the growth of M. tuberculosis. It has a softer texture and is often used for the rapid cultivation and observation of bacterial colonies.
In a study conducted in Brazil, the two decontamination methods, respectively Ogawa-Kudoh and modified Petroff, were compared on a sample of 205 sputum samples taken from 166 patients. The results indicated that both methods demonstrated efficiency in the detection of mycobacteria, with no significant differences between them in terms of results or culture contamination rate. The conclusion of this study emphasized the excellent agreement between the two decontamination techniques [65].
4. Molecular methods
4.1. Conventional nucleic acid amplification tests (NAAT)
Several studies have demonstrated the utility of molecular biology tests for the diagnosis of tuberculosis. These nucleic acid amplification tests (NAATs) have demonstrated a sensitivity of 81%, offering higher performance especially in cases of patients with obvious symptoms of active tuberculosis [67].
New molecular technologies are now available for the rapid screening of TB drug resistance. The World Health Organization (WHO) has approved several molecular tests, such as the GenoType MTBDRplus line probe LPA test and GeneXpert MTB / RIF, to detect MDR-TB. In many countries, especially those with limited resources, these molecular tests are only available in reference laboratories [1].
4.1.2. GenoType Line Probe Assays (LPA)
Molecular tests such as LPA are considered ideal for rapid diagnosis and can be used directly on diagnostic samples. LPA uses nuclei acid amplification techniques such as PCR and reverse hybridization to rapidly detect drug resistance mutations.
Two affordable LPA tests are INNO-LiPA Rif TB and GenoType MTBDRplus. INNO-LiPA Rif TB was introduced by Innogenetics and has been approved by the WHO, with high sensitivity and specificity for the identification of M. tuberculosis bacteria and drug resistance mutations [68].
GenoType MTBDR, introduced by Hain Lifescience has a sensitivity and specificity of 99% and 100% for rifampicin resistance and 88.4% and 100% for isoniazid resistance. MTBDRplus, an improved version, has been validated by WHO and has shown outstanding analytical efficacy for the identification of multidrug-resistant tuberculosis (MDR-TB).
The GenoType MTBDRplus Test Version 2.0, approved by the WHO in 2012, allows instant identification of mutations and has a high recognition rate of rifampicin resistance. These molecular tests have made significant improvements in the diagnosis and identification of drug resistance in tuberculosis [16,69].
A retrospective analysis investigated the effectiveness of the sample amplification tests in the detection of M. tuberculosis complex and the diagnosis of multidrug-resistant tuberculosis (MDR-TB). The laboratory at the Microbiology Department of the Bhopal Memorial Hospital and Research Center in Madhya Pradesh, India, examined sputum samples from patients with suspected tuberculosis. Of the 1,294 acid-fast bacilli AFB-positive sputum samples tested with LPA, M. tuberculosis complex was detected in 94.04% of the samples, but not identified in 5.9% of them [70].
Also, 5.1% of sputum samples were found to be negative for M. tuberculosis complex by LPA and culture. In a small percentage of AFB-positive samples, M. tuberculosis complex could not be identified by LPA, even if confirmed by culture. These results highlight the limitations of the LPA test in detecting M. tuberculosis in certain sputum samples and highlight the importance of using multiple diagnostic methods for a complete and accurate assessment of MDR-TB [70].
Another study from Nigeria analyzed a total of 67 gastric samples and 31 sputum samples to assess the presence of M. tuberculosis in children. The M. tuberculosis detection method by sandblasting microscopy (SM) was found to provide positive results in 3.0% of gastric samples and in 16.1% of sputum samples. In contrast, the use of polymerase chain amplification (LPA) detected M. tuberculosis in 41.8% of gastric samples and in 58.1% of sputum samples [71].
Comparing these results with other similar studies, it was observed that the LPA method had a higher yield in detecting M. tuberculosis in sputum samples and the SM method provided poorer results overall. In addition, it was found that the use of LPA enabled the detection of M. tuberculosis in sputum samples that were initially negative for the SM test. These findings suggest that the use of the LPA method may improve the diagnosis of pulmonary tuberculosis in children, providing a higher sensitivity high in identifying M. tuberculosis in sputum samples [71].
Another study conducted in Central India looked at the 1528 sputum samples analyzed, 1294 were positive in the microscopic (smear) test and 234 were negative in this test. Of the 1294 LPA tests performed, 77 samples (5.9% of the total) did not show the specific band for the Mycobacterium tuberculosis complex. Of the samples with the TUB band present (1217 samples, different types of drug resistance were identified. A total of 67 (5.1%) sputum samples were negative for Mycobacterium tuberculosis complex by both LPA and culture [70].
The performance of the GenoType MTBDRplus assay is comparable to that of the GeneXpert MTB/RIF assay. A meta-analysis showed excellent sensitivity and specificity for the detection of resistance to isoniazid, rifampicin, and MDR-TB. However, the sensitivity of the test may vary, being higher in smear-positive cases and lower in smear-negative cases. Also, the test may have a high percentage of invalid results for direct smear-negative sputum samples [72].
4.2. Methods based on real-time genetic amplification technology RT-PCR GeneXpert MTB/RIF
The Xpert MTB/RIF assay is an automated, cartridge-based, easy-to-use system with a closed amplification system to prevent cross-specimen contamination. This test can be easily performed by laboratory technicians without the need for advanced biosafety equipment. In February 2015, the FDA approved the expanded use of the Xpert MTB/RIF test to reduce the isolation period of patients with suspected tuberculosis. According to the new guidelines, one or two negative Xpert MTB/RIF test results are sufficient to rule out pulmonary tuberculosis, in contrast to previous CDC recommendations that required isolation until three consecutive negative AFB smear results. from sputum, to rule out contagious tuberculosis [16]. The GeneXpert system is an innovative molecular diagnostic platform used for the rapid detection of M. tuberculosis. This system features an interface that allows users to enter data, interpret results, and monitor test progress. The MTB/RIF cartridge contains the necessary elements for the amplification and detection of the specific DNA of the bacterium M. tuberculosis and for the identification of mutations associated with rifampicin resistance. Through the cartridge, the MTB/RIF test can be performed quickly and without requiring any preparation laborious, which makes it suitable for use in field laboratories or in resource-limited areas, contributing to the diagnosis and management of the disease in an efficient manner.
The Xpert MTB/RIF test is a fully automated PCR test based on PCR in real time that de tects M. tuberculosis and mutations associated with resistance to rifampicin (RIF), the 81-bp basic region of the rpoB gene [73]. The analytical sensitivity of the Xpert MTB/RIF test is five genomic copies of purified DNA and 131 CFU·ml −1 of M. tuberculosis in sputum. It was not no cross-reactivity with non-tuberculous mycobacteria (NTM) detected [74].
Multinational evaluations have confirmed the feasibility, accuracy, and effectiveness of the Xpert MTB/RIF test in healthcare facilities in tuberculosis TB-endemic countries in Africa, Asia and Latin America. These results have led the World Health Organization to support the expanded use of this technology. Initially, WHO recommended the use of the Xpert MTB/RIF test for patients with suspected multidrug-resistant tuberculosis MDR-TB and those with HIV co-infection.
Recently, WHO recommended that programs move away from the use of smear microscopy and prioritize the initial use of the Xpert MTB/RIF test. The sensitivity and specificity of the Xpert MTB/RIF test for the diagnosis of pulmonary tuberculosis in adults are approximately 90% and 98%, respectively, using culture as the reference standard [75].
Several studies have investigated the possibility of using the Xpert MTB/RIF test instead of direct smear microscopy as the primary screening method for urgent clinical samples in a context characterized by a low prevalence of tuberculosis [73].
GeneXpert MTB/RIF, a test subject to numerous studies and validations in various clinical settings, has been shown by a meta-analysis in low- and middle-income countries to have a high aggregated sensitivity and specificity as an initial test replacing smear microscopy. With a sensitivity of 89% and a specificity of 99% it has proven effectiveness. However, the sensitivity of the test was higher in cases with positive results on microscopy than in those with negative results. Among people without HIV, the sensitivity was 86, while for those with HIV it was 79% [72].
In the context of extrapulmonary tuberculosis, a condition affecting organs and tissues outside the lungs, the performance of the GeneXpert MTB/RIF system was evaluated. The study included a considerable number of patients with various forms of extrapulmonary tuberculosis, such as nodular, peritoneal, bone-articular and genito-urinary tuberculosis. The GeneXpert MTB/RIF system was compared to the standard reference method, which involves culturing the bacterium and identifying it by traditional laboratory methods [76].
Extrapulmonary tuberculosis (EPTB) accounts for approximately one fifth of the total cases of tuberculosis in immunocompetent patients. The incidence of EPTB is significant increased in HIV-positive people, exceeding 50% of all tuberculosis cases associated with this condition. Despite the fact that molecular methods generally do not reached the expected level in the diagnosis of tuberculosis, the polymerase chain reaction technique (PCR) is proving to be a particularly useful tool in the diagnosis of EPTB and may, by also be used to identify drug-resistant strains [77,78].
In a study conducted at the Bacteriology Department of the Mohammed Military Hospital, Morocco, 714 patient samples were analyzed. The mean age was 47.21 ± 19.98 years, with the majority being male (66.4%). Of the total of 714 samples, 285 came from the lungs and 429 from other areas of the body. The positive detection rate by microscopy was 12.88%, by GeneXpert MTB/RIF it was 20.59%, and by culture it was 15.82%. For lung samples, positive detection rates were higher, 18.9% by microscopy, 23.85% by GeneXpert MTB/RIF, and 20.35% by culture. For extrapulmonary samples, the rates were lower, 9.71% by microscopy, 18.41% by GeneXpert MTB/RIF, and 12.82% by culture. GeneXpert MTB/RIF showed a sensitivity of approximately 78.2% and a specificity of 90.4% in both sample types, while for extrapulmonary samples these figures were 79.3% for sensitivity and 90, 3% for specificity [79].
A study was performed using two diagnostic methods: ZN smear and GeneXpert MTB/RIF test. The research focused on tuberculous meningitis (TBM), a severe form of tuberculosis. The GeneXpert MTB/RIF test was evaluated for the diagnosis of TBM in a large group of patients in Vietnam. Although the Ziehl-Neelsen smear remained the most sensitive technique, the GeneXpert MTB/RIF test made an important contribution to the early diagnosis of tuberculous meningitis [80,81,82].
Another study conducted in Korea analyzed the effectiveness of the Xpert MTB/RIF Test and a MTB nested PCR in the identification of Mycobacterium tuberculosis. Clinical lung samples and non-pulmonary were collected from 171 patients with suspected tuberculosis. The results showed that the sensitivity, specificity, value positive predictive value (PPV) and negative predictive value (NPP) of the Xpert Test MTB/RIF for the diagnosis of tuberculosis with Mycobacterium tuberculosis positive at culture were 86.1%, 97.8%, 91.2%, and 96.4%, respectively. In comparison, values of the nested PCR were 69.4%, 94.1%, 75.8%, and respectively 92.0%. In addition, the Xpert MTB/RIF test demonstrated a significantly longer response time short compared to nested PCR, with a median of 0 [0–4] days versus 4 [1–11] days, respectively (p under 0.001) [83].
Another study from Malaysia published in 2021 was carried out to reduce the underdiagnosis of pulmonary tuberculosis with negative ZN smear results, the clinical and radiological characteristics of patients with this form of tuberculosis were evaluated. The research included 235 patients from a clinic in Luyaun, between September 2016 and June 2017. Of the 50 cases of pulmonary tuberculosis with smear-positive results, 49 samples were confirmed positive by the Gene-Xpert MTB/RIF test and by cultivation (MTB). In contrast, of the 185 cases with pre-summative negative smear results, Gene-Xpert MTB/RIF test identified 21 positive cases. These results were confirmed by MTB cultivation. Compared with the traditional method of detecting acid-fast bacilli in sputum, the Gene-Xpert MTB/RIF test showed higher sensitivity and specificity with almost complete accuracy. This research highlights the importance of using the Gene-Xpert MTB/RIF test in the rapid and accurate diagnosis of pulmonary tuberculosis, thereby contributing to the reduction of underdiagnosis and the initiation of early treatment for this disease [84,85].
Also, research from the comparative study] analyzed the methods of rapid diagnosis of tuberculosis recurrence. Detection of recurrence can be challenging, given that M. tuberculosis specific DNA can be persistently present in sputum and bronchopulmonary samples, even when the disease is not active [86]. Further development of molecular tests included lowering the threshold of detection (via Xpert MTB/RIF Ultra technology) and additional gene analysis associated with resistance, resulting in significant improvement in diagnosis tuberculosis including in children [87,88].
In a study, the diagnostic accuracy of the detection of M. tuberculosis-specific DNA by either the Gene-Xpert MTB/RIF technique and the M. tuberculosis-specific ELISPOT method in bronchoalveolar lavage (BAL) samples was compared with the results of M. tuberculosis culture from sputum or bronchopulmonary samples in patients with suspected recurrence of pulmonary tuberculosis. Among the 44 patients with a history of tuberculosis and suspected recurrence of the disease, only 4 of them (9.1%) were confirmed to have recurrent tuberculosis by the culture method. As for the Gene-Xpert MTB/RIF method, it was able to detect M. tuberculosis DNA in bronchoalveolar lavage in 1 of 4 patients with recurrence (25%), as well as in 2 of 40 patients (5%) with previous tuberculosis without recurrence. In contrast, the BAL-ELISPOT technique, using a threshold of >4,000 target-specific early antigenic lymphocytes 6 or culture-filtered protein-specific interferon γ 10, provided positive results for all 4 patients with recurrence (100%) and for 2 of 40 patients (5%) with previous TB without recurrence [89].
In a study carried out at the Department of Bacteriology, Mohammed V Military Teaching Hospital / Faculty of Medicine and Pharmacy University Mohamed V, Rabat, a total of 714 samples were examined, 285 were taken from the lungs, and 429 from other areas of the body. The diagnostic methods used, microscopic examination (ZN), GeneXpert MTB/RIF and bacterial culture, had variable infection detection rates, depending on the type of samples (pulmonary or extrapulmonary). Positive detection rates for microscopy, ZN, GeneXpert MTB/RIF and culture were 12.88%, 20.59% and 15.82%, respectively. In detail, for lung samples, these rates were 18.9%, 23.85% and 20.35%, and for extrapulmonary samples, they were 9.71%, 18.41% and 12.82%. The GeneXpert MTB/RIF assay showed close sensitivity and specificity in pulmonary (78.2% and 90.4%) and extrapulmonary (79.3% and 90.3%) samples [79].
Despite the progress made, challenges are still encountered in efforts to develop more accurate methods for the diagnosis of tuberculosis. More than 50 diagnostic tests are currently in development, but rigorous evaluation of the entire diagnostic process faces difficulties, such as the absence of quality control reagents. It is crucial to make progress in the development of appropriate phenotypic testing methods and robust quality assurance systems [90].
The collection and transport of M. tuberculosis specimens continues to be a challenge in settings where tuberculosis is widespread and the necessary infrastructure to maintain specimen integrity is lacking. A study addressed this issue, and PrimeStore Molecular Transport Medium (MTM) was developed, which not only rapidly inactivates M. tuberculosis, but also preserves genomic DNA under high temperature conditions, thus facilitating subsequent molecular analysis, which provides information essential for a correct diagnosis and adequate treatment of tuberculosis patients [91].Molecular testing by Xpert MTB/RIF for tuberculosis could bring significant savings to health systems in high-income countries by decreasing the need for patient isolation and the total length of hospitalization [92].
One of the essential criteria for performance evaluation is participation laboratories to theExternal Quality Assessment (EQA) for the Xpert MTB/RIF test, which it is integrated into the quality assurance system necessary for clinical practice and laboratory. This system includes the pre-analytical, analytical and post-analytical processes, with the aim of guaranteeing the continuous quality of the tests [93].
4.3. Loop-Mediated Isothermal Amplification (LAMP) technology
Other molecular techniques include ligase chain amplification, for identifying drug resistance mutations, and LAMP, which is faster and less expensive than PCR [94,95].
LAMP is a fast and simplified NAAT platform developed by Eiken Chemical Co., Ltd(Tokyo, Japan). The technology uses four different primers specifically designed to recognize six distinct regions of the target gene, and the reaction process takes place at a constant (isothermal) temperature using the strand displacement reaction. A simplified amplification test technique was used in one study loop mediated isotherm (LAMP). The procedure was performed on a semisolid gel of polyacrylamide of dimensions 6 × 8, using a prototype deviceaccessible from the point of financial view. Each serving on the gel contains a small amount of only 670 nanoliters, thus reducing the need for large amounts of chemicals. DNA amplified is identified by means of the fluorescence of the LCGreen Plus+ dye, embedded in the gel along with other reagents [96].
Amplification and detection of gene products can be completed in one step by incubating the mixture of samples, primers, DNA polymerase with strand displacement activity and substrates at a constant temperature. Amplification efficiency is high, and DNA can be amplified 10^9-10^10 times in 15-60 min. Due to its high specificity, the presence of the amplified product can indicate the presence of the target gene. Currently, there is limited evidence regarding the accuracy of LAMP for TB detection.
A study conducted in Gambia, compared various methods of detecting tuberculosis using sputum samples, both in patients with symptoms suggestive of TB and in patients confirmed with this disease. The loop-mediated amplification assay for TB (TB-LAMP) was evaluated in comparison with other techniques such as smear microscopy with ZN, MGIT culture and GeneXpert MTB/RIF. The reference standard was culture. TB-LAMP showed an overall sensitivity of 99% and a specificity of 94%. In the latent class analysis, TB-LAMP had a sensitivity of 98.6% and a specificity of 99%, while GeneXpert had the highest sensitivity (99.1%) but the lowest specificity (96 %). Both TB-LAMP and GeneXpert showed high sensitivity and specificity in detecting TB, regardless of age or strain of infection. These findings underline the utility of both methods, GeneXpert and TB-LAMP, in the diagnosis of TB. However, although TB-LAMP requires less infrastructure, it cannot detect drug-resistant strains, making it more suitable for initial testing of new TB cases in medical clinics [97].
However, widespread implementation of these techniques in developing countries is still limited by lack of infrastructure, high costs, and lack of skilled personnel. In addition, the need for adequate transport and storage of samples is another important challenge.
Another study investigated the effectiveness of parallel tests for the diagnosis of pulmonary tuberculosis in patients whose smear results were negative. In this study, 258 patients were included, and different testing methods, including culture, GenXpert MTB/RIF, and SAT-TB, were compared. The results revealed that the use of parallel tests resulted in significantly higher sensitivity compared to individual testing. The parallel testing model demonstrated a significant improvement in diagnostic efficacy for smear-negative PTB. Thus, this method should be considered in clinical practice when PTB is suspected but smear results are negative [98].
The same LAMP is rapid assay to prove rifampicin and isoniazid resistance of TB Isolates [99].
4.4. Gold nanoparticles (AuNP)
Gold nanoparticles are among the most promising tools in the field of biosensing due to the numerous physicochemical properties derived from the nanoscale, which include enhanced spectroscopic signals and enzyme-mimicking properties [100].
Advances in nanotechnology open new perspectives for the development of rapid, sensitive, and cost-effective sensors for the detection of M. tuberculosis. The TB disease caused by M. bovis is clinically and pathologically indistinguishable from TB caused by MTB. In addition, both mycobacteria stain as acid fast bacilli, are 99.95% genome-wide similar, and have identical 16S rRNA sequences. Differentiating between them is crucial because M. bovis is intrinsically resistant to pyrazinamide, one of the commonly used first-line anti-TB drugs [101].
In one study, an innovative immunoassay was created and evaluated using ferromagnetic gold nanoparticles to detect and differentiate the main causative agents of human tuberculosis, namely MTB and M. bovis. By generating a single recombinant monoclonal antibody directed against a key MTBC-specific protein and combining it with a range of pre-existing antibodies targeting both cell surface and secreted antigens of MTB and M. bovis, the proposed assay was developed. NP bioconjugates, consisting of Au-Fe3O4 ferromagnetic gold nanoparticles, were obtained by direct binding of antibodies to these particles [101].
5. Conclusions
The previously described methods for the diagnosis of tuberculosis, such as molecular tests and the microscopic method, as well as bacterial culture, play an essential role in the effective detection and management of this serious disease. While many of these methods of diagnosis and treatment are promising, it is essential to continue research and develop more effective and cost-effective approaches to the management of tuberculosis. In particular, more studies are needed that focus on developing and testing new drugs and therapies, improving screening and diagnostic strategies, and improving approaches to TB control and prevention.
Nevertheless, the microscopic method remains a widely used diagnostic technique, especially in countries with limited resources. However, it is important to recognize the limitations of this method and consider the use and evaluation of other techniques to obtain a complete and accurate diagnosis.
Bacterial culture, both in solid and liquid media, are essential methods in the diagnosis of tuberculosis. Culture on solid media provides specificity and accuracy, while culture on liquid media brings speed and increased sensitivity. The use of these methods in combination can contribute to a complete and accurate diagnosis of tuberculosis.
Molecular diagnostic techniques have represented a major leap forward in the detection and management of tuberculosis. They enable the rapid identification of M. tuberculosis complex and drug resistance, thus providing critical information for choosing the appropriate treatment regimen. Molecular tests, such as LPA and GeneXpert MTB/RIF, offer significant benefits in the rapid and accurate diagnosis of tuberculosis, including drug-resistant forms. These tests allow the identification of resistance mutations and provide essential information for choosing the right treatment. Thus, molecular techniques are an essential tool for rapid and accurate diagnosis of tuberculosis and drug resistance. Although molecular tests are extremely useful, they also have important limitations. For example, these tests cannot distinguish between viable and non-viable M. tuberculosis complex, which means they are not suitable for monitoring treatment response. However, their widespread implementation in countries with limited resources requires a comprehensive approach that takes into account all specific challenges and needs.
In general, combined diagnostic methods, which use several techniques and approaches, give the best result in the diagnosis of tuberculosis. Improving the quality and accessibility of tests, as well as the implementation of advanced technologies, can help improve the sensitivity, efficiency, and accuracy of tuberculosis diagnosis.
It is essential that we continue research and development of new methods and technologies to improve the diagnosis and management of tuberculosis, given its significant impact on global health.
Author Contributions
Conceptualization, N.Z. and D.C.Z.; methodology, R.N. and A.C.; resources, R.H and C.Z.; data curation, N.Z. and D.C.Z.; writing—original draft preparation, N.Z. and C.Z.; writing—review and editing, D.C.Z., A.C. and R.H.; visualization, R.N.; supervision, D.C.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of Oradea.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rakotosamimanana, N.; Rabodoarivelo, M.S.; Palomino, J.C.; Martin, A.; Razanamparany, V.R. Exploring tuberculosis by molecular tests on DNA isolated from smear microscopy slides. Int. J. Infect. Dis. 2017, 56, 248–252. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization.Global Tuberculosis Report 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 10 August 2023).
- Heidary, M.; Shirani, M.; Moradi, M.; Goudarzi, M.; Pouriran, R.; Rezaeian, T.; Khoshnood, S. Tuberculosis challenges: Resistance, co-infection, diagnosis, and treatment. Eur J Microbiol Immunol (Bp). 2022, 12, 1–17. [Google Scholar] [CrossRef]
- Aghajani, J.; Farnia, P.; Farnia, P.; Ghanavi, J.; Saif, S.; Marjani, M.; Tabarsi, P.; Moniri, A.; Abtahian, Z.; Hoffner, S.; Velayati, A.A. Effect of COVID-19 Pandemic on Incidence of Mycobacterial Diseases among Suspected Tuberculosis Pulmonary Patients in Tehran, Iran. Int. J. Mycobacteriol 2022, 11, 415–422. [Google Scholar] [PubMed]
- Can Sarınoğlu, R.; Sili, U.; Eryuksel, E.; Olgun Yildizeli, S.; Cimsit, C.; Karahasan Yagci, A. Tuberculosis and COVID-19: An overlapping situation during pandemic. J. Infect. Dev. Ctries 2020, 14, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.; Nilsen, D.M.; Will, L.; Etkind, S.C.; Burgos, M.; Chorba, T. Essential Components of a Public Health Tuberculosis Prevention, Control, and Elimination Program: Recommendations of the Advisory Council for the Elimination of Tuberculosis and the National Tuberculosis Controllers Association. MMWR Recomm. Rep. 2020, 69, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Lalvani, A.; Pathan, A.A.; Durkan, H.; Wilkinson, K.A.; Whelan, A.; Deeks, J.J.; Reece, W.H.; Latif, M.; Pasvol, G.; Hill, A.V. Enhanced contact tracing and spatial tracking of Mycobacterium tuberculosis infection by enumeration of antigen-specific T cells. Lancet. 2001, 357, 2017–2021. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.; Ms, A.; Ryszewska, K.; Laszlo, A.; Blanc, L. Approach for the Strengthening of Laboratory Services for Tuberculosis Control. Published online 2006. Available online: https://www.who.int/publications/i/item/WHO-HTM-TB-2006.364 (accessed on 17 August 2023).
- Procop, G.W. Laboratory Diagnosis and Susceptibility Testing for Mycobacterium tuberculosis. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef]
- Azadi, D.; Motallebirad, T.; Ghaffari, K.; Shojaei, H. Mycobacteriosis and Tuberculosis: Laboratory Diagnosis. Open Microbiol. J. 2018, 12, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Asadi, L.; Croxen, M.; Heffernan, C.; Dhillon, M.; Paulsen, C.; Egedahl, M.L.; Tyrrell, G.; Doro-shenko, A.; Long, R. How much do smear-negative patients really contribute to tuberculosis transmissions? Re-examining an old question with new tools. EClinicalMedicine. 2022, 43, 101250. [Google Scholar] [CrossRef]
- Noncommercial culture and drug-susceptibility testing methods for screening patients at risk for multidrug-resistant tuberculosis Policy statement WHO Library Cataloguing-in-Publication Data Noncommercial culture and drug-susceptibility testing methods for screening patients at risk for multidrug-resistant tuberculosis: Policy statement. Published online 2011. Available online: www.who.int (accessed on 17 August 2023).
- Abebaw, Y.; Kebede, A.; Eshetu, K.; Tesfaye, E.; Tadesse, M.; Sinshaw, W.; Amare, M.; Gamtesa, D.F.; Zerihun, B.; Getu, M.; et al. Quality assurance practices in tuberculosis diagnostic health facilities in Ethiopia. PLoS ONE. 2022, 17, e0269601. [Google Scholar] [CrossRef]
- Evelina, L.; Olga, C.; Alina, M.; Adriana, N.; Stela, K.; Alexandru, C. Clinical and paraclinical similarities and differences between pulmonary tuberculosis and community-acquired pneumonia. Public. Health, Economics and Management in Medicine 2022, 93-S, 258–264. [Google Scholar]
- Shah, M.I.; Mishra, S.; Yadav, V.K.; Chauhan, A.; Sarkar, M.; Sharma, S.K.; Rout, C. Ziehl-Neelsen sputum smear microscopy image database: A resource to facilitate automated bacilli detection for tuberculosis diagnosis. J Med Imaging (Bellingham). 2017, 4, 027503. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, A.J.; Wengenack, N.L. Diagnosis of active tuberculosis disease: From microscopy to molecular techniques. J. Clin. Tuberc. Other Mycobact. Dis. 2016, 4, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Global laboratory initiative advancing TB diagnosis A publication of the Global Laboratory Initiative a Working Group of the Stop TB Partnership Mycobacteriology Laboratory Manual. Available online: https://stoptb.org/wg/gli/gat.asp, (accessed on 17 August 2023).
- Selvakumar, N.; Rahman, F.; Rajasekaran, S.; Narayanan, P.R.; Frieden, T.R. Inefficiency of 0.3% carbol fuchsin in ziehl-neelsen staining for detecting acid-fast bacilli. J. Clin. Microbiol. 2002, 40, 3041–3043. [Google Scholar] [CrossRef] [PubMed]
- Holani, A.G.; Ganvir, S.M.; Shah, N.N.; Bansode, S.C.; Shende, I.; Jawade, R.; Bijjargi, S.C. Demonstration of mycobacterium tuberculosis in sputum and saliva smears of tuberculosis patients using ziehl neelsen and flurochrome staining- a comparative study. J. Clin. Diagn. Res. 2014, 8, ZC42–ZC45. [Google Scholar]
- Khan, E.A.; Starke, J.R. Diagnosis of tuberculosis in children: Increased need for better methods. Emerg. Infect. Dis. 1995, 1, 115–123. [Google Scholar] [CrossRef]
- Stop TB Partnership. COMMUNITY SYSTEM STRENGTHENING AND TB. Available online: https://www.stoptb.org/supporting-global-fund/useful-resources-and-links, (accessed on 13 August 2023).
- Munyati, S.S.; Dhoba, T.; Makanza, E.D.; Mungofa, S.; Wellington, M.; Mutsvangwa, J.; Gwanzura, L.; Hakim, J.; Nyakabau, M.; Mason, P.R.; et al. Chronic cough in primary health care attendees, Harare, Zimbabwe: Diagnosis and impact of HIV infection. Clin. Infect. Dis. 2005, 40, 1818–1827. [Google Scholar] [CrossRef] [PubMed]
- Zeru, M.A. Prevalence and associated factors of HIV-TB co-infection among HIV patients: A retrospective Study. Afr. Health Sci. 2021, 21, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Romancenco, E. Microbiological diagnosis of tuberculosis. Guide. Chișinău; 2012. [Google Scholar]
- Shen, F.; Sergi, C. Sputum Analysis. [Updated 2023 Feb 20]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA; Available online: https://www.ncbi.nlm.nih.gov/books/NBK563195/ (accessed on 11 December 2023).
- European Centre for Disease Prevention and Control. European Union Standards for Tuberculosis Care. Available online: https://www.ecdc.europa.eu/en/publications-data/european-union-standards-tuberculosis-care-2017-update (accessed on 13 August 2023).
- Angra, P.; Becx-Bleumink, M.; Gilpin, C.; Joloba, M.; Jost, K.; Kam, K.M.; Kim, S.J.; Lumb, R.; Mitarai, S.; Ramsay, A.; et al. Ziehl-Neelsen staining: Strong red on weak blue, or weak red under strong blue? Int. J. Tuberc. Lung Dis. 2007, 11, 1160–1161. [Google Scholar]
- Tortoli, E.; Bartoloni, A.; Böttger, E.C.; Emler, S.; Garzelli, C.; Magliano, E.; Mantella, A.; Rastogi, N.; Rindi, L.; Scarparo, C.; Urbano, P. Burden of unidentifiable mycobacteria in a reference laboratory. J. Clin. Microbiol. 2001, 39, 4058–4065. [Google Scholar] [CrossRef]
- Makaen, J.; Maure, T. Bleach processed smear for Acid fast bacilli staining in Papua New Guinea. Lab. Med. 2014, 45, e140–e141. [Google Scholar] [CrossRef] [PubMed]
- Olaru, I.D.; Heyckendorf, J.; Grossmann, S.; Lange, C. Time to culture positivity and sputum smear microscopy during tuberculosis therapy. PLoS ONE. 2014, 9, e106075. [Google Scholar] [CrossRef] [PubMed]
- Desikan, P. Sputum smear microscopy in tuberculosis: Is it still relevant? Indian. J. Med. Res. 2013, 137, 442–444. [Google Scholar] [PubMed]
- Shapiro, H.M.; Hänscheid, T. Fuchsin fluorescence in Mycobacterium tuberculosis: The Ziehl-Neelsen stain in a new light. J. Microbiol. Methods. 2008, 74, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Bodal, V.K.; Bal, M.S.; Bhagat, S.; Kishan, J.; Deepika Brar, R.K. Fluorescent microscopy and Ziehl-Neelsen staining of bronchoalveolar lavage, bronchial washings, bronchoscopic brushing and post bronchoscopic sputum along with cytological examination in cases of suspected tuberculosis. Indian. J. Pathol. Microbiol. 2015, 58, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, K.; Lambert, M.L.; Walley, J. Clinical diagnosis of smear-negative pulmonary tuberculosis in low-income countries: The current evidence. Lancet Infect. Dis. 2003, 3, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, M.M.; Bakr, W.M.; Hussien, S.M.; Amine, A.E. Diagnosis of pulmonary tuberculosis using Ziehl-Neelsen stain or cold staining techniques? J. Egypt. Public. Health Assoc. 2016, 91, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Steingart, K.R.; Henry, M.; Ng, V.; Hopewell, P.C.; Ramsay, A.; Cunningham, J.; Urbanczik, R.; Perkins, M.; Aziz, M.A.; Pai, M. Fluorescence versus conventional sputum smear microscopy for tuberculosis: A systematic review. Lancet Infect. Dis. 2006, 6, 570–581. [Google Scholar] [CrossRef]
- Oommen, S.; Banaji, N. Laboratory diagnosis of tuberculosis: Advances in technology and drug susceptibility testing. Indian. J. Med. Microbiol. 2017, 35, 323–331. [Google Scholar] [CrossRef]
- Dzodanu, E.G.; Afrifa, J.; Acheampong, D.O.; Dadzie, I. Diagnostic Yield of Fluorescence and Ziehl-Neelsen Staining Techniques in the Diagnosis of Pulmonary Tuberculosis: A Comparative Study in a District Health Facility. Tuberc. Res. Treat. 2019, 2019, 4091937. [Google Scholar] [CrossRef]
- Fluorescent Light-Emitting Diode (LED) Microscopy for Diagnosis of Tuberculosis: Policy Statement. Geneva: World Health Organization. Available online:. 2011. (accessed on 12 August 2023).
- Mnyambwa, N.P.; Ngadaya, E.S.; Kimaro, G.; Kim, D.J.; Kazwala, R.; Petrucka, P.; Mfinanga, S.G. Assessment of sputum smear-positive but culture-negative results among newly diagnosed pulmonary tuberculosis patients in Tanzania. Int. J. Gen. Med. 2017, 10, 199–205. [Google Scholar] [CrossRef]
- Abbas, A.; Elrayah, E. ILED fluorescent microscope in laboratory diagnosis of tuberculosis. RMJ 2017, 42. [Google Scholar]
- Gelalcha, A.G.; Kebede, A.; Mamo, H. Light-emitting diode fluorescent microscopy and Xpert MTB/RIF® assay for diagnosis of pulmonary tuberculosis among patients attending Ambo hospital, west-central Ethiopia. BMC Infect. Dis. 2017, 17, 613. [Google Scholar] [CrossRef] [PubMed]
- Zurac, S.; Mogodici, C.; Poncu, T.; Trăscău, M.; Popp, C.; Nichita, L.; Cioplea, M.; Ceachi, B.; Sticlaru, L.; Cioroianu, A.; Busca, M.; Stefan, O.; Tudor, I.; Voicu, A.; Stanescu, D.; Mustatea, P.; Dumitru, C.; Bastian, A. A New Artificial Intelligence-Based Method for Identifying Mycobacterium Tuberculosis in Ziehl-Neelsen Stain on Tissue. Diagnostics (Basel). 2022, 12, 1484. [Google Scholar] [CrossRef] [PubMed]
- Del Carpio, C.; Dianderas, E.; Zimic, M.; Sheen, P.; Coronel, J.; Lavarello, R.; Kemper, G. An algorithm for detection of Tuberculosis bacilli in Ziehl-Neelsen sputum smear images. International Journal of Electrical and Computer Engineering. 2019, 9, 2968–2981. [Google Scholar] [CrossRef]
- Xiong, Y.; Ba, X.; Hou, A.; Zhang, K.; Chen, L.; Li, T. Automatic detection of mycobacterium tuberculosis using artificial intelligence. J. Thorac. Dis. 2018, 10, 1936–1940. [Google Scholar] [CrossRef]
- Zingue, D.; Weber, P.; Soltani, F.; Raoult, D.; Drancourt, M. Automatic microscopic detection of mycobacteria in sputum: A proof-of-concept. Nat. India Sci. Rep. 2018, 8, 11308. [Google Scholar] [CrossRef] [PubMed]
- Mittal, V.; Haider, F.; Singhal, S.; Jamal, S. Is universal sample processing methodology better than conventional techniques for detection of tuberculosis? Indian. J. Med. Microbiol. 2014, 32, 404–407. [Google Scholar] [CrossRef]
- Holani, A.G.; Ganvir, S.M.; Shah, N.N.; Bansode, S.C.; Shende, I.; Jawade, R.; Bijjargi, S.C. Demonstration of mycobacterium tuberculosis in sputum and saliva smears of tuberculosis patients using ziehl neelsen and flurochrome staining- a comparative study. J. Clin. Diagn. Res. 2014, 8, ZC42–ZC45. [Google Scholar]
- Chakravorty, S.; Dudeja, M.; Hanif, M.; Tyagi, J.S. Utility of universal sample processing methodology, combining smear microscopy, culture, and PCR, for diagnosis of pulmonary tuberculosis. J. Clin. Microbiol. 2005, 43, 2703–2708. [Google Scholar] [CrossRef]
- Cattamanchi, A.; Davis, J.L.; Worodria, W.; Yoo, S.; Matovu, J.; Kiidha, J.; Nankya, F.; Kyeyune, R.; Andama, A.; Joloba, M.; Osmond, D. Poor performance of universal sample processing method for diagnosis of pulmonary tuberculosis by smear microscopy and culture in Uganda. J. Clin. Microbiol. 2008, 46, 3325–3329. [Google Scholar] [CrossRef]
- Verma, S.; Dhole, T.N.; Kumar, M.; Kashyap, S. Novel approach for improving sensitivity of microscopic detection of acid-fast bacilli (AFB) by use of the ReaSLR method. J. Clin. Microbiol. 2013, 51, 3597–3601. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues da Costa, R.; Silva, M.R.; Augusto, C.J.; Gonçalves Leite, I.C. Fast, simple and cheap: Method modified from conventional cultivation for tuberculosis diagnosis allows seeding on Löwenstein-Jensen of any swab-embedded pulmonary samples decontaminated with sodium hydroxide. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.D.; Huf, G.; Vieira, M.A.; Costa, P.A.; Aguiar, F.; Marsico, A.G.; Fonseca, L.D.; Ricks, M.; Oliveira, M.M.; Detjen, A.; Fujiwara, P.I. Liquid vs Solid Culture Medium to Evaluate Proportion and Time to Change in Management of Suspects of Tuberculosis-A Pragmatic Randomized Trial in Secondary and Tertiary Health Care Units in Brazil. PLoS ONE. 2015, 10, e0127588. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.G.; Lindsey, P.H.; Harvey, C.F.; Bradley, K.K. Recognizing laboratory cross-contamination: Two false-positive cultures of Mycobacterium tuberculosis--Oklahoma, 2011. Chest. 2013, 144, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Mohammed Adam, M.A.; Ebraheem, R.S.M.; Bedri, S.A. Statistical Investigation of High Culture Contamination Rates in Mycobacteriology Laboratory. Front. Microbiol 2022, 13, 789725. [Google Scholar] [CrossRef]
- Battaglioli, T.; Rintiswati, N.; Martin, A.; Palupi, K.R.; Bernaerts, G.; Dwihardiani, B.; Ahmad, R.A.; Matthys, F.; Mahendradhata, Y.; Van Der Stuyft, P. Comparative performance of Thin Layer Agar and Löwenstein-Jensen culture for diagnosis of tuberculosis. Clin. Microbiol. Infect. 2013, 19, E502–E508. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Chapagain, M.; Gumbo, T. Effect of specimen processing, growth supplement, and different metabolic population on Mycobacterium tuberculosis laboratory diagnosis. PLoS ONE. 2020, 15, e0230927. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.; Munshi, S.K.; Banu Momi, M.S.; Rahman, F.; Noor, R. Evaluation of the effectiveness of BACTEC MGIT 960 for the detection of mycobacteria in Bangladesh. Int. J. Mycobacteriol. 2013, 2, 214–219. [Google Scholar] [CrossRef]
- Ryu, Y.J. Diagnosis of pulmonary tuberculosis: Recent advances and diagnostic algorithms. Tuberc Respir Dis (Seoul). 2015, 78, 64–71. [Google Scholar] [CrossRef]
- Zabaleta-Vanegas, A.P.; Llerena-Polo, C.; Orjuela-Gamboa, D.L.; Valbuena-Arias, Y.A.; García-González, L.M.; Mejía-Restrepo, G.; Bueno, J.; Garzón-Torres, M.C. Evaluation of BACTEC™ MGIT™ 960 and the nitrate reductase assay in the National Laboratory Network of Colombia. Int. J. Tuberc. Lung Dis. 2013, 17, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Yegian, D.; Budd, V. Toxic effect of sodium hydroxide on tubercle bacilli. Am. J. Clin. Pathol. 1952, 22, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Wallace, E.; Hendrickson, D.; Tolli, N.; Mehaffy, C.; Peña, M.; Nick, J.A.; Knabenbaur, P.; Watkins, J.; Simpson, A.; Amin, A.G.; et al. Culturing Mycobacteria. Methods Mol. Biol. 2021, 2314, 1–58. [Google Scholar] [PubMed]
- Thornton, C.G.; MacLellan, K.M.; Brink, T.L., Jr.; Passen, S. In vitro comparison of NALC-NaOH, tween 80, and C18-carboxypropylbetaine for processing of specimens for recovery of mycobacteria. J. Clin. Microbiol. 1998, 36, 3558–3566. [Google Scholar] [CrossRef] [PubMed]
- Asmar, S.; Drancourt, M. Chlorhexidine decontamination of sputum for culturing Mycobacterium tuberculosis. BMC Microbiol. 2015, 15, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.R.D.; Silva, S.F.D.; Fochat, R.C.; Macedo, R.L.; Pereira, T.V.; Silva, M.R.; Pinto, C.P.G.; Leite, I.C.G. Comparison between Ogawa-Kudoh and modified Petroff techniques for mycobacteria cultivation in the diagnosis of pulmonary tuberculosis. Einstein (Sao Paulo) 2018, 16, eAO4214. [Google Scholar] [CrossRef] [PubMed]
- Mtafya, B.; Sabiiti, W.; Sabi, I.; John, J.; Sichone, E.; Ntinginya, N.E.; Gillespie, S.H. Molecular Bacterial Load Assay Concurs with Culture on NaOH-Induced Loss of Mycobacterium tuberculosis Viability. J. Clin. Microbiol. 2019, 57, e01992-18. [Google Scholar] [CrossRef] [PubMed]
- Gressens, S.B.; Billard-Pomares, T.; Leboité, H.; Cruaud, P.; Bouchaud, O.; Carbonnelle, E.; Méchaï, F. Pulmonary tuberculosis: Evaluation of current diagnostic strategy. Infect. Dis. Now. 2021, 51, 273–278. [Google Scholar] [CrossRef]
- OMS. WHO consolidated guidelines on tuberculosis. Module 3: Diagnosis-rapid diagnostics for tuberculosis detection, 2021 update.World Health Organization. 2021, Module 3:1-164. Available online: https://www.who.int/publications/i/item/9789240029415 (accessed on 5 November 2023).
- Bhirud, P.; Joshi, A.; Hirani, N.; Chowdhary, A. Rapid laboratory diagnosis of pulmonary tuberculosis. Int. J. Mycobacteriol. 2017, 6, 296–301. [Google Scholar] [CrossRef]
- Desikan, P.; Panwalkar, N.; Mirza, S.B.; Chaturvedi, A.; Ansari, K.; Varathe, R.; Chourey, M.; Kumar, P.; Pandey, M. Line probe assay for detection of Mycobacterium tuberculosis complex: An experience from Central India. Indian. J. Med. Res. 2017, 145, 70–73. [Google Scholar] [CrossRef]
- Ebonyi, A.O.; Oguche, S.; Abok, I.I.; Isa, Y.O.; Ani, C.C.; Akhiwu, H.O.; Ihekaike, M.M.; Yiltok, E.S.; Ochoga, M.O.; Sagay, A.S. Improving the diagnosis of pulmonary tuberculosis using line probe assay and determining the factors associated with the disease in children in Jos, Nigeria. Germs. 2020, 10, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Dicks, K.V.; Stout, J.E. Molecular Diagnostics for Mycobacterium tuberculosis Infection. Annu. Rev. Med. 2019, 27, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Deggim, V.; Somoskovi, A.; Voit, A.; Böttger, E.C.; Bloemberg, G.V. Integrating the Xpert MTB/RIF assay into a diagnostic workflow for rapid detection of Mycobacterium tuberculosis in a low-prevalence area. J. Clin. Microbiol. 2013, 51, 2396–2399. [Google Scholar] [CrossRef] [PubMed]
- Weyer, K.; Mirzayev, F.; Migliori, G.B.; Van Gemert, W.; D'Ambrosio, L.; Zignol, M.; Floyd, K.; Centis, R.; Cirillo, D.M.; Tortoli, E.; Gilpin, C.; de Dieu Iragena, J.; Falzon, D.; Raviglione, M. Rapid molecular TB diagnosis: Evidence, policy making and global implementation of Xpert MTB/RIF. European Respiratory Journal , 2013, 42, 252–271. [Google Scholar] [CrossRef]
- Harries, A.D.; Kumar, A.M.V. Challenges and Progress with Diagnosing Pulmonary Tuberculosis in Low- and Middle-Income Countries. Diagnostics (Basel). 2018, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- Shinnick, T.M.; Starks, A.M.; Alexander, H.L.; Castro, K.G. Evaluation of the Cepheid Xpert MTB/RIF assay. Expert. Rev. Mol. Diagn. 2015, 15, 9–22. [Google Scholar] [CrossRef]
- Ajantha, G.S.; Shetty, P.C.; Kulkarni, R.D.; Biradar, U. PCR as a diagnostic tool for extra-pulmonary tuberculosis. J. Clin. Diagn. Res. 2013, 7, 1012–1015. [Google Scholar] [CrossRef] [PubMed]
- Rafael, L.L.; Raquel, M.S.; Rogelio, F.A.; Miroslava, F.P.; Alejandra-Isabel, J.G.; Paola, R.S. Discordant results between genotypic and phenotypic assays (Xpert MTB/RIF vs. BACTEC MGIT 960 system) for detection of RIF-resistant Mycobacterium tuberculosis isolates in a high burden region. Infect. Genet. Evol. 2021, 96, 105142. [Google Scholar] [CrossRef]
- Mechal, Y.; Benaissa, E.; El Mrimar, N.; Benlahlou, Y.; Bssaibis, F.; Zegmout, A.; Chadli, M.; Malik, Y.S.; Touil, N.; Abid, A.; Maleb, A.; Elouennass, M. Evaluation of GeneXpert MTB/RIF system performances in the diagnosis of extrapulmonary tuberculosis. BMC Infect Dis 2019, 19, 1069. [Google Scholar] [CrossRef]
- Daum, L.T.; Fourie, P.B.; Peters, R.P.; Rodriguez, J.D.; Worthy, S.A.; Khubbar, M.; Bhattacharyya, S.; Gradus, M.S.; Mboneni, T.; Marubini, E.E.; Helm, C.; Chambers, J.P.; Fischer, G.W. Xpert(®) MTB/RIF detection of Mycobacterium tuberculosis from sputum collected in molecular transport medium. Int. J. Tuberc. Lung Dis. 2016, 20, 1118–1124. [Google Scholar] [CrossRef]
- Ssebambulidde, K.; Gakuru, J.; Ellis, J.; Cresswell, F.V.; Bahr, N.C. Improving Technology to Diagnose Tuberculous Meningitis: Are We There Yet? Front. Neurol. 2022, 13, 892224. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, S.M.; Kussen, G.M.B.; Cogo, L.; Carvalho, J.H.; Nogueira, K. Diagnostic characteristics of Xpert MTB/RIF assay for the diagnosis of tuberculous meningitis and rifampicin resistance in Southern Brazil. Arq. Neuropsiquiatr. 2020, 78, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Woo, H.; Hyun, I.G.; Kim, C.; Choi, J.H.; Jang, S.H.; Park, S.M.; Kim, D.G.; Lee, M.G.; Jung, K.S.; Hyun, J.; Kim, H.S. A comparison between the efficiency of the Xpert MTB/RIF assay and nested PCR in identifying Mycobacterium tuberculosis during routine clinical practice. J. Thorac. Dis. 2014, 6, 625–631. [Google Scholar] [PubMed]
- Kabir, S.; Parash, M.T.H.; Emran, N.A.; Hossain, A.B.M.T.; Shimmi, S.C. Diagnostic challenges and Gene-Xpert utility in detecting Mycobacterium tuberculosis among suspected cases of Pulmonary tuberculosis. PLoS ONE. 2021, 16, e0251858. [Google Scholar] [CrossRef] [PubMed]
- Mekkaoui, L.; Hallin, M.; Mouchet, F.; Payen, M.C.; Maillart, E.; Clevenbergh, P.; Georgala, A.; Van den Wijngaert, S. Performance of Xpert MTB/RIF Ultra for diagnosis of pulmonary and extra-pulmonary tuberculosis, one year of use in a multi-centric hospital laboratory in Brussels, Belgium. PLoS ONE. 2021, 16, e0249734. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, D.R.; Biswas, J.R.; Lievesley, A.; Quinn, G.; Buckley, J.; John, L.; Davidson, R.N. False-positive Xpert(®) MTB/RIF more than seven years after cure. Int. J. Tuberc. Lung Dis. 2015, 19, 1264–1265. [Google Scholar] [CrossRef] [PubMed]
- Kay, A.W.; Ness, T.; Verkuijl, S.E.; Viney, K.; Brands, A.; Masini, T.; González Fernández, L.; Eisenhut, M.; Detjen, A.K.; Mandalakas, A.M.; Steingart, K.R.; Takwoingi, Y. Xpert MTB/RIF Ultra assay for tuberculosis disease and rifampicin resistance in children. Cochrane Database Syst. Rev. 2022, 9, CD013359. [Google Scholar] [PubMed]
- Ozkutuk, N.; Surucüoglu, S. Orta prevalanslı bölgede akciğer ve akciğer dışı tüberküloz tanısında Xpert MTB/RIF testinin değerlendirilmesi [Evaluation of the Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary tuberculosis in an intermediate-prevalence setting]. Mikrobiyol. Bul. 2014, 48, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Jafari, C.; Olaru, I.D.; Daduna, F.; Lange, C.; Kalsdorf, B. Rapid Diagnosis of Recurrent Paucibacillary Tuberculosis. Pathog. Immun. 2023, 7, 189–202. [Google Scholar] [CrossRef]
- Danchuk, S.N.; McIntosh, F.; Jamieson, F.B.; May, K.; Behr, M.A. Bacillus Calmette-Guérin strains with defined resistance mutations: A new tool for tuberculosis laboratory quality control. Clin. Microbiol. Infect. 2020, 26, e5–e384. [Google Scholar] [CrossRef]
- Daum, L.T.; Choi, Y.; Worthy, S.A.; Rodriguez, J.D.; Chambers, J.P.; Fischer, G.W. A molecular transport medium for collection, inactivation, transport, and detection of Mycobacterium tuberculosis. Int. J. Tuberc. Lung Dis. 2014, 18, 847–849. [Google Scholar] [CrossRef] [PubMed]
- Millman, A.J.; Dowdy, D.W.; Miller, C.R.; Brownell, R.; Metcalfe, J.Z.; Cattamanchi, A.; Davis, J.L. Rapid molecular testing for TB to guide respiratory isolation in the U.S.: A cost-benefit analysis. PLoS ONE. 2013, 8, e79669. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.; Albert, H.; Gilpin, C.; Alexander, H.; DeGruy, K.; Stevens, W. Multicenter feasibility study to assess external quality assessment panels for Xpert MTB/RIF assay in South Africa. J. Clin. Microbiol. 2014, 52, 2493–2499. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Kalantri, S.; Dheda, K. New tools and emerging technologies for the diagnosis of tuberculosis: Part II. Active tuberculosis and drug resistance. Expert. Rev. Mol. Diagn. 2006, 6, 423–432. [Google Scholar] [CrossRef]
- Jekloh, N.; Keawliam, P.; Mukem, D.; Rudeeaneksin, J.; Srisungngam, S.; Bunchoo, S.; Klayut, W.; Bhakdeenaun, P.; Phetsuksiri, B. Evaluation of an in-house loop-mediated isothermal amplification for Mycobacterium tuberculosis detection in a remote reference laboratory, Thailand. Rev. Inst. Med. Trop. Sao Paulo. 2022, 64, e57. [Google Scholar] [CrossRef]
- Manage, D.P.; Chui, L.; Pilarski, L.M. Sub-microliter scale in-gel loop-mediated isothermal amplification (LAMP) for detection of Mycobacterium tuberculosis. Microfluid. Nanofluid 2013, 14, 731–741. [Google Scholar] [CrossRef]
- Bojang, A.L.; Mendy, F.S.; Tientcheu, L.D.; Otu, J.; Antonio, M.; Kampmann, B.; Agbla, S.; Sutherland, J.S. Comparison of TB-LAMP, GeneXpert MTB/RIF and culture for diagnosis of pulmonary tuberculosis in The Gambia. J. Infect. 2016, 72, 332–337. [Google Scholar] [CrossRef]
- Fan, L.; Li, D.; Zhang, S.; Yao, L.; Hao, X.; Gu, J.; Li, H.; Niu, J.; Zhang, Z.; Zhu, C. Parallel Tests Using Culture, Xpert MTB/RIF, and SAT-TB in Sputum Plus Bronchial Alveolar Lavage Fluid Significantly Increase Diagnostic Performance of Smear-Negative Pulmonary Tuberculosis. Front. Microbiol. 2018, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.F.; Song, Y.M.; He, P.; Liu, D.X.; He, W.C.; Li, Y.M.; Zhao, Y.L. Evaluation of Multidrug Resistant Loop-mediated Isothermal Amplification Assay for Detecting the Drug Resistance of Mycobacterium tuberculosis. Biomed. Environ. Sci. 2021, 34, 616–622. [Google Scholar]
- Logan, N.; Lou-Franco, J.; Elliott, C.; Cao, C. Catalytic gold nanostars for SERS-based detection of mercury ions (Hg 2+ ) with inverse sensitivity. Environ. Sci. Nano. 2021, 8, 2718–2730. [Google Scholar] [CrossRef]
- Gilbride, B.; Schmidt Garcia Moreira, G.M.; Hust, M.; Cao, C.; Stewart, L. Catalytic ferromagnetic gold nanoparticle immunoassay for the detection and differentiation of Mycobacterium tuberculosis and Mycobacterium bovis. Anal. Chim. Acta. 2021, 1184, 339037. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



