
Submitted:
23 December 2023
Posted:
03 January 2024
You are already at the latest version
Abstract
Introduction: The objective of this study was: compare the continuous infusion of cefepime with the intermittent infusion in patients with sepsis caused by Gram negative bacilli (GNB). Methods: Randomized 1:1 multicenter double-blinded placebo-controlled study with allocation concealment. Multicenter study in Intensive Care Units of Colombia. Patients with sepsis, severe sepsis or septic shock and GNB suspected bacteraemia. Cefepime was administered for 7 to 14 days over 30 m intermittently every 8 h over 24 h plus continuous saline solution (0.9%) (G1) or 3 g administered continuously plus saline solution every 8 h (0.9%) (G2). Percentage of clinical response at 3, 7, 14 days, relapse at 28 days and mortality at discharge were measured. Results: The recruitment was stopped by suggestion of the Institutional Review Board (IRB), following an FDA alert about cefepime. Thirty-two patients were randomized, 25 received the intervention and GNB bacteremia was confirmed in 16 (9 G1 and 7 G 2). Favourable clinical response in days 3,7,14 was 88.8%, 88.8%, 77.8 % (G 1) and was similar for G 2 (85.7%). There were not relapses and deaths in G2 while in G1 one relapse and 2 deaths were observed. Conclusions: The results of this study support the use of cefepime for the treatment of Gram-negative infections in critically ill patients but we could not demonstrate differences between continuous or intermittent administration, because of the small sample size, given the early suspension of the study.
Keywords:
bacteraemia
; cefepime
; sepsis
; intravenous infusions
1. Introduction
Beta-lactams are the most widely used group of antimicrobials in the Intensive Care Unit (ICU), where there is great concern about infections caused by multidrug-resistant microorganisms [1,2]. Cefepime is a fourth-generation cephalosporin first approved in 1993 in Europe and 1996 in the USA for the treatment of pneumonia, urinary tract, skin and soft tissue infections, complicated intra-abdominal infections and febrile neutropenia; this antibiotic is broad spectrum and has activity for Gram-positive and mainly Gram-negative bacteria [3,4], so it is used as first line in patients with suspected or confirmed infections by resistant bacteria in ICU and hospitalization.
One of the most important pharmacokinetic/pharmacodynamic (PK/PD) properties of cefepime is its "time-dependent" bactericidal action, whereby its maximum action occurs when the concentration reaches a critical level, beyond which a higher rate of bacterial death is not obtained; This critical threshold is considered to occur between 1 and 4 times the minimum inhibitory concentration (MIC), so it is sought to ensure that the concentration remains above the MIC for most of the time, ideally more than 50% of the dosing interval [4,5].
One of the strategies proposed to optimize the administration of antimicrobials with time-dependent action, and to obtain greater efficacy and safety, particularly of beta-lactams such as cefepime, is to reduce the interval between doses and administer it with loading doses and then with continuous infusion [1]; this measure has even been shown to have an impact on the reduction of the appearance of resistance or selection of resistant subpopulations in animal models [6]. For the outcome of clinical failure, a systematic review showed that there is no difference between continuous versus intermittent infusion (OR 0.73, 95%CI 053-1.01), nor for mortality (OR 0.89, 95%CI 0.48-1.64, p=0.71), nor nephrotoxicity [7]. Similar results have been found for cefepime, with no clinical differences between continuous and intermittent administration of the drug [8]. Therefore, there is controversy about the clinical benefit of using continuous versus intermittent doses of cefepime in the ICU. The objective of this study was to compare the efficacy between continuous and intermittent infusions of cefepime by means of clinical and bacteriological cure of critical patients with sepsis and Gram-negative bacilli bacteremia.
2. Results
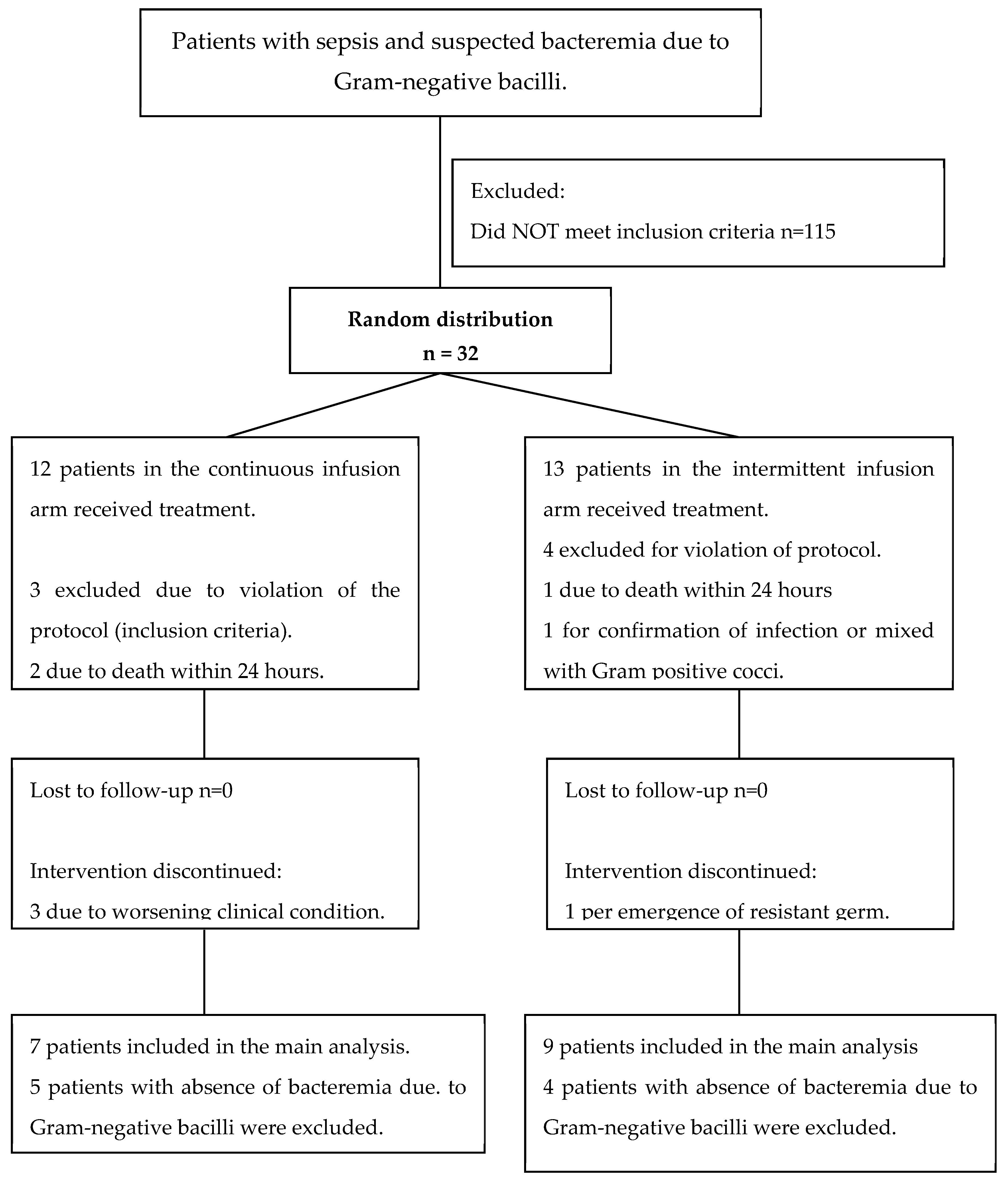
Patients: 226 patients were screened, in 7 institutions in Colombia between July 14, 2006 through October 31, 2007, of which, 32 were randomly distributed because they met inclusion criteria and had no exclusion criteria; of the randomized patients, it was necessary to exclude 7 for protocol violations (presence of exclusion criteria: chronic renal failure, use of immunosuppressants, mortality in less than 24 hours or the presence of a mixed infection or multidrug-resistant bacteria); finally, 12 patients were admitted for the continuous infusion group, of which Gram-negative bacilli bacteremia was documented in 7, and 13 patients for the intermittent infusion group, with documentation of Gram-negative bacilli bacteremia in 9. See Figure 1 for the distribution of the population studied.
The demographic and clinical characteristics of the 25 patients randomized in the two treatment groups are described in Table 1, these were similar especially in the average length of stay in the ICU prior to infection and clinical severity (APACHE and SOFA). The baseline characteristics of the population of the two treatment groups in which Gram-negative bacillus bacteremia was evidenced, in this case Enterobacteriaceae (mainly Escherichia coli and Pseudomonas aeruginosa), are shown in Table 2. During follow-up there was no loss of patients and it was even possible to continue observation of patients discontinued due to therapeutic failure.
Figure 1.
Flow chart of the distribution of the study population in the two arms of the study.
Primary Outcomes
Patients with sepsis in ICU:
Mortality: overall mortality was 16% in all patients; 2 patients died in each group.
Clinical response, microbiological response and relapse: these outcomes were evaluated in 24 ICU patients who had sepsis (12 patients in each group). Overall therapeutic failure was 24% in all patients, we identified a complete favorable clinical response at 14 days of 61.5% (8/12) in group 1 and 75% (9/12) in group 2, with no statistically significant differences. The different categories of clinical response at days 3 and 14 were similar for both treatment groups. We found a relapse at day 28 in one patient in the intermittent infusion group, and no relapse in the continuous infusion group. See Table 3.
Patients with Gram-negative bacilli bacteremia:
Mortality: The overall mortality of patients with Gram-negative bacilli bacteremia was 12%. We found that 2 patients in the intermittent infusion group died, while in the continuous infusion group there were no deaths.
Clinical response, microbiological response and relapse: in the 16 patients with documentation of Gram-negative bacilli bacteremia (9 in group 1 and 7 in group 2), we identified an overall therapeutic failure of 12.5%; there was a similar clinical response at days 3, 7 and 14 in both groups, with no differences in the considerations of complete favorable response, favorable or unfavorable improvement. We found a total favorable response at day 7 of 75% for both groups. Finally, one patient in the intermittent infusion group relapsed, while no relapse occurred in the continuous infusion group. See Table 4.
Secondary outcomes:
Patients with sepsis in ICU:
ICU length of stay for group 1 was shorter, 18.7+/- 10.5 days and in group 2 23+/-14.7 days, but this difference was not statistically significant. Total hospitalization time was similar for both groups, 10.6+/- 4.21 days for the intermittent infusion and 9.3+/-3.4 days for the continuous infusion and discontinuation of the drug was mainly due to improvement. See Table 3.
Patients with Gram-negative bacilli bacteremia:
ICU length of stay for group 1 was shorter, 16.8+/- 8.8 days and in group 2 22+/-13.31 days, but this difference was not statistically significant; for total hospitalization time, shorter duration was also found for the intermittent infusion group, 27.2 +/- 12.7 days, compared to the continuous infusion group, whose duration was 40.1 +/- 28.4 days, but these findings were not statistically significant. The duration of cefepime administration was similar for the groups, close to 10 days, and discontinuation of the drug was mainly due to improvement. See Table 4.

Table 3.
Clinical response, microbiological response, relapse and other outcomes in ICU patients with sepsis.
Table 3.
Clinical response, microbiological response, relapse and other outcomes in ICU patients with sepsis.
| Characteristics | Intermittent infusion n=12 |
Continuous infusion n=12 |
p+ Value |
|---|---|---|---|
| Mortality at discharge (n, %) | 2 (15.3) | 2 (16.6) | 0.47* |
|
Day 3 Presence of SIRS (n/total number evaluated, %) Clinical response* (n, %)
|
5/12 (41.6) 1 (7.69) 11 (84.62) 1 (7.69) |
6/12 (50.0) 0 (0) 10 (83.3) 2 (16.7) |
0.99 0.99 |
|
Day 7 Presence of SIRS (n/total number evaluated, %) Clinical response* (n, %)
|
5/12 (41.6) 5 (38.4) 5 (38.4) 3 (23.0) |
5/10 (50.0) 5 (41.6) 4 (33.3) 3 25.0) |
0.99 0.99 |
|
Day 14 Presence of SIRS (n/total number evaluated, %) Clinical response* (n, %) - Complete favorable - Favorable improvement - Unfavorable |
5/9 (55.5) 8 (61.5) 1 (7.7) 4 (30.7) |
5/9 (55.5) 9 (75.0) 0 3 (25.0) |
0.99 0.99 |
|
Day 28 Relapse (n/total number tested, %) |
1/10 (10) |
0/8 (0) |
0.99 |
| Length of stay in ICU (mean days, SD) |
18.7+/- 10.5 | 23+/-14.7 | 0.4+ |
| ICU length of stay after diagnosis of infection (mean days, SD) | 10.76+/- 9.5 | 17.9+/- 13.1 | 0.6+ |
| Time of hospitalization (mean days, SD) |
31.6+/- 15.9 | 35.8 +/- 24.8 | 0.9+ |
| Duration of cefepime administration (mean days +/-DS) | 10.6+/- 4.21 | 9.3+/-3.4 | 0.8+ |
| Cefepime discontinuation ratio (n, %) Improvement Worsening of clinical picture Appearance of multi-resistant germ |
10 (77) 2 (15.4) 1 (7.6) |
9 (75) 3 (25) 0 |
0.99* |
* All 25 patients were included in the evaluation of clinical response. + (Fisher's exact test).
Table 4.
Clinical response, microbiological response, relapse and other outcomes in patients with Gram-negative bacilli bacteremia.
Table 4.
Clinical response, microbiological response, relapse and other outcomes in patients with Gram-negative bacilli bacteremia.
| Characteristics | Intermittent infusion n = 9 |
Continuous infusion n = 7 |
p+ Value |
|---|---|---|---|
| Mortality at discharge (n, %) | 2 (22) | 0 | 0.30* |
|
Day 3 Presence of SIRS (n/total number evaluated, %) Clinical response* (n, %)
|
3/9 (33.3) 4 (44.4) 4 (44.4) 1 (11.1) |
4/7 (57.1) 4 (57.1) 2 (28.6) 1 (14.3) |
0.40 0.99 |
|
Day 7 Presence of SIRS (n/total number evaluated, %) Clinical response* (n, %)
Total favorable response (n, %) |
2/8 (25) 4 (44.4) 4 (44.4) 1 (11.1) 6/8 (75.0) 6/8 (75.0) |
4/7 (57.1) 4 (57.1) 2 (28.6) 1 (14.3) 4/4 (100) 3/4 (75.0) |
0.23 0.99 0.41 0.28 |
|
Day 14 Presence of SIRS (n/total number evaluated, %) Clinical response* (n, %)
|
2/5 (40) 6 (66.7) 1 (11.1) 2 (22.2) |
4/6 (66.7) 6 (85.7) 0 1 (14.3) |
0.39 0.99 |
|
Day 28 Relapse (n, %) |
1/7 (14.3) |
0/6 (0) |
0.99 |
| ICU length of stay (days, SD) | 16.8+/- 8.8 | 22+/-13.31 | 0.9+ |
| Length of ICU stay after diagnosis of infection (days, SD) | 8.22+/- 6.5 | 17+/- 7.8 | 0.6+ |
| Duration of cefepime administration (mean days +/-SD) | 10.6+/- 4.7 | 10.3+/-0.75 | 0.8+ |
| Cefepime discontinuation ratio (n, %) Improvement Worsening of clinical picture Appearance of multi-resistant germ |
8 (88.8) 0 1 (11.2) |
6 (85.7) 1 (14.3) 0 |
0.7* |
* All 16 patients (9 and 7, respectively) were included in the evaluation of clinical response. + (Fisher's exact test).
3. Discussion
Our multicenter study in ICU patients with Gram-negative bacilli bacteremia and sepsis, in whom continuous versus intermittent infusion administration of cefepime was compared, unfortunately had to be discontinued due to an FDA safety alert related to the drug [9]; because a meta-analysis reported an increased risk of all-cause mortality with the use of cefepime compared to other beta-lactams ([RR] 1.26 [95% CI 1.08-1.49]), with no differences for other outcomes such as clinical failure, microbiological failure, superinfections and adverse events, except for the comparison between cefepime and piperacillin+tazobactam with respect to clinical failure (RR 1. 09, CI 1.01-1.18; p=0.04) [10]. Another meta-analysis including 88 studies with 9467 patients in the cefepime administration group and 8288 patients in the beta-lactam comparator group found no difference in mortality risk (adjusted risk difference ARD per 1000 population of 5.38; 95 % [CI] - 1.53 to 12.28) [11]. Because of this finding and other similar results, cefepime is currently used.
Despite the discontinuation of our study, we found similar findings of overall mortality and clinical failure to those described in other studies with approximate clinical conditions with cefepime administration, e.g. Georges B, et.al. in an RCT with 50 patients, 9 of them with Gram-negative bacilli bacteremia, found that clinical outcome and bacteriological eradication did not differ significantly between the continuous and intermittent infusion groups, but there was continuous infusion of cefepime consistently maintained a serum concentration > 5 times the MIC of typical Gram-negative nosocomial pathogens, unlike the intermittent infusion group, which could lead to the conclusion that continuous infusion may have greater bactericidal activity without a clear impact on clinical outcomes [8,12]. Clinical and microbiological outcomes for continuous administration compared to intermittent administration of other beta-lactam-type antimicrobials in other studies have also shown no differences in clinical or microbiological impact between these administration strategies, for example in the case of ceftriaxone, cefotaxime and piperacillin+tazobactam [13,14,15].
Although it is true that this study could not demonstrate whether the form of administration of cefepime has an impact on the final clinical outcome, we can describe that in patients with severe sepsis or septic shock we found that mortality and overall therapeutic failure were 16% and 24%, so it is still valid to consider designing studies to address this question, especially in the context in which bacterial resistance continues to increase and there are few strategies currently available to contain them. The proposed studies should also evaluate other outcomes in addition to clinical effectiveness, such as cost minimization and reduction in the appearance of resistance, since studies in animal models have shown an impact on the reduction of resistance with the continuous administration of antibiotics [6].
Another factor to take into account in the evaluation of clinical and microbiological outcomes in ICU patients administered cefepime is the high variability of pharmacokinetic and pharmacodynamic parameters that can occur, because most patients have comorbidities such as acute kidney injury or chronic kidney disease and in general the critical condition of patients leads to a high variation for example of volume of distribution and clearance, this can trigger a higher risk of side effects and differences in treatment outcomes [4,16,17]. Some studies have shown that continuous or high-dose administration of cefepime in critically ill patients is associated with increased risk of adverse events such as neurotoxicity, precisely because of the high interindividual variability of different pharmacokinetic parameters [18], so more studies comparing these clinical outcomes of adverse events between drug administration strategies are also needed.
Our study had several limitations, including the low recruitment rate, the emergence of publications suggesting cautious use of the drug, and the intermittent availability of cefepime during the course of the investigation at the participating centers. The early closure of the study had a great impact on the number of patients included, with important difficulties for the interpretation and analysis of the results obtained. The low number of patients included at the time of the decision to discontinue led to the impossibility of fulfilling the main objective of the study, given the loss of internal validity. However, our study showed interesting results that contribute to the knowledge on the impact of antimicrobial stewardship strategies on clinical and microbiological outcomes.
4. Materials and Methods
Design: clinical, randomized, controlled, double-blind study. Patients who met the inclusion and exclusion criteria were randomized in a 1:1 ratio into the following groups: 1) Group 1 administration of cefepime in continuous intravenous infusion at a dose of 3 g/day in 150 mL of saline 0. 9% for a minimum of 3 days and a maximum of 14 days, with administration of 25-100 mL of 0.9% saline solution every 8 hours for 30 minutes, and 2) Group 2 of intermittent administration of cefepime (bolus of 1g to pass in 30 minutes) every 8 hours for a minimum of 3 days and a maximum of 14 days accompanied by 25-100 mL of 0.9% saline solution for 24 hours. In cases in which the isolated microorganism was resistant to cefepime or blood cultures did not show bacteremia due to Gram-negative bacilli, the patient was excluded from the study. See Figure 1. The protocol was registered in the clinical trials database of the National Institute of Health of the United States (http://www.clinicaltrials.gov) and was accepted with the identification number NCT0060609375.
Figure 2.
Study design.
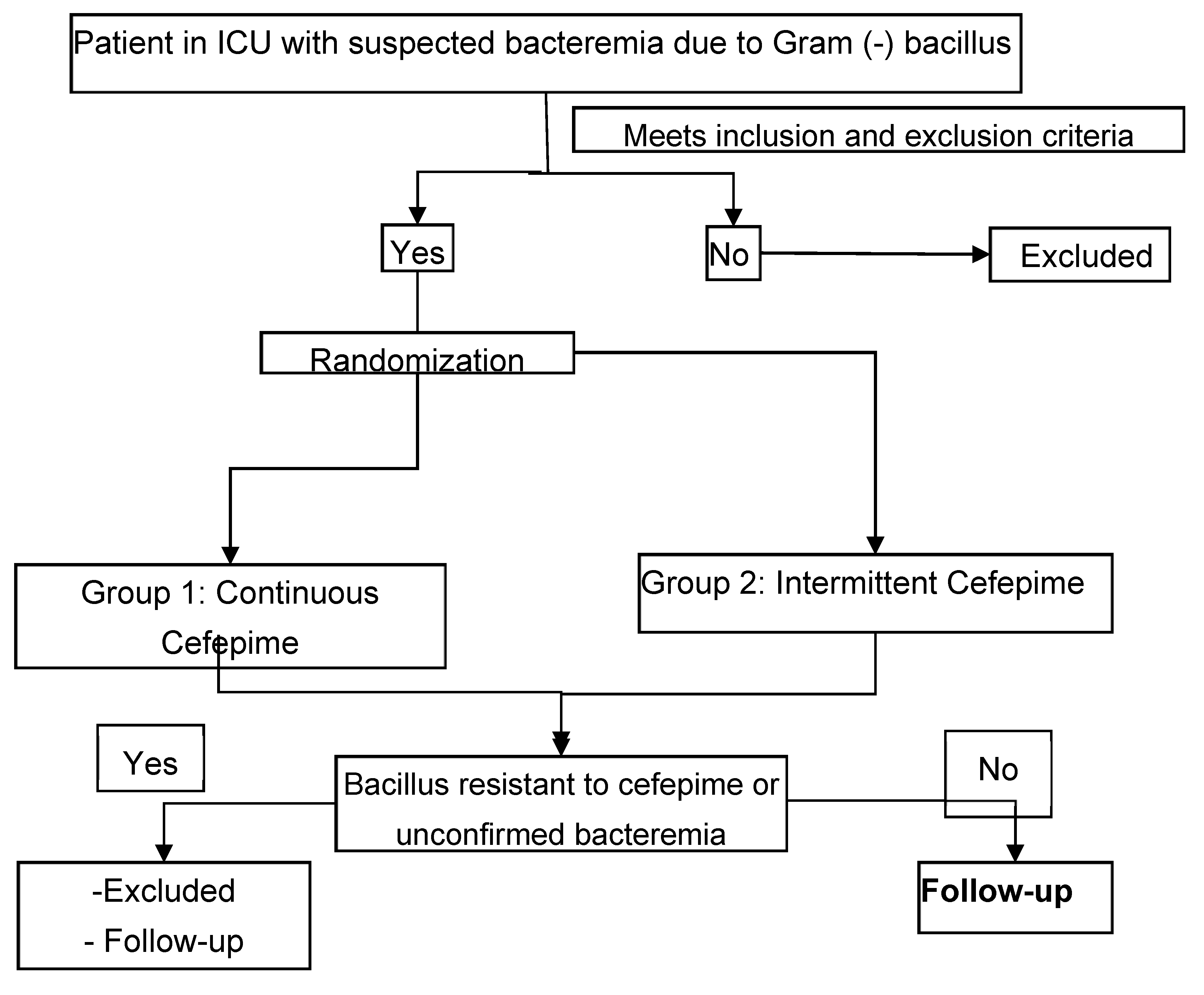
ICU: Intensive care unit
Population and sample: For screening all male or female patients with suspected skin, soft tissue, respiratory tract, urinary tract, intra-abdominal and intravascular sepsis attended in ICUs of mixed predominance (medical-surgical) of several institutions in Colombia, in which antibiotics in the form of continuous or intermittent infusion were prescribed in their usual practice, were included. The expected sample size calculation was 168 patients (84 in each arm) in one year. The calculation was made based on a cure rate of superiority [19].
Inclusion criteria: Patients over 18 years of age hospitalized in ICU with diagnosis of sepsis, severe sepsis or septic shock, with presence or suspicion of Gram-negative bacilli bacteremia, with possibility of follow-up, availability of venous access and patients in whom cefepime was considered the treatment of choice according to the criteria of the treating medical group.
Exclusion criteria: Patients with immunosuppression defined by the presence of neutropenia (neutrophil count less than 500 cells/mm3), HIV-AIDS infection with a CD4/mm3 count of less than 50 cells, chronic administration of immunosuppressive drugs (corticosteroids, azathioprine, cyclophosphamide, mycophenolate mofetil, etc.); chronic renal failure, pregnancy, patients considered by the treating doctor with a high probability of dying in the next 48 hours, for example with multiple organ failure with more than 5 organs compromised according to the criteria of Marshall et al. [20], patients with chronic infections such as osteomyelitis or users of osteosynthesis or prosthesis material, patients with endocarditis or with mixed infections that included microorganisms other than Gram-negative bacilli, use of cefepime during the last 30 days, infection by a Gram-negative bacillus resistant to cefepime, patients with concomitant administration of antibiotics with activity for Gram-negative bacilli, and finally patients allergic to cefepime.
Randomization and distribution concealment: Randomization was performed from tables of random numbers and allocation by blocks of 4 to maintain the same number of patients in each group; to hide the result of the allocation the sealed envelope system was used and to maintain the blindness only the nurse in charge of administering the medication, knew the group assigned for each patient. Once the patient was selected and met the inclusion and exclusion criteria, the research physician informed the head nurse, who by selecting a sealed envelope started the medication in the determined form of administration, In the Case Report Format (CRF) only a code appeared for later identification and in no case did the treating physician, the researcher of the institution or the principal investigator know the assigned group with respect to the form of administration of the medication before the analysis.
Procedures: Clinical and examination evaluations included demographic data, clinical history, complete physical examination, anamnesis of clinical symptoms, blood picture, blood chemistry, urinalysis and c-reactive protein at the beginning of the study, on day 3, 7, 14 and 28 of treatment; in addition, chest radiography was performed at each of these times, if the patient's clinical condition warranted it. Blood cultures were performed at the beginning of the study, at 7 and 14 days. Patients were followed up until day 28 of hospitalization or discharge.
Data collection: A data collection form was designed for this process, which was filled out by each of the investigators, reviewed and corrected by the study monitor and the principal researcher. A manual for filling out the CRF was created and a meeting was held with all the researchers and a nurse from each center. An initial visit was made to each participating center and additional training was provided to the medical, nursing and pharmacy teams.
Definition of the variables: SIRS (Systemic Inflammatory Response Syndrome), sepsis, severe sepsis and septic shock according to the criteria of Levy et al. [21]; for severe sepsis the criteria of Marshall et al. [20] were included. For the definitions of infection of each anatomical site the criteria of Calandra T and Cohen J. [22] were used. Gram-negative bacilli bacteremia was defined as the presence, in at least one blood culture of a microorganism subsequently identified as Gram-negative bacilli by manual and automated methods. Once the CRFs were completed, the information was reviewed and corrected, to be subsequently included in a database designed in the Access program (Microsoft® office 2003) (Annex 9) and then transferred for analysis in the Stata/SE 9.0 program (Texas, USA).
Outcomes: The primary outcomes were: 1) mortality at discharge 2) clinical response at 3, 7 and 14 days, which included favorable clinical response (resolution of all signs and symptoms of sepsis or SIRS), improvement (decrease in signs and symptoms of sepsis or SIRS, but no resolution of infectious disease), unfavorable (persistence of signs and symptoms of infection at the time of evaluation, in the absence of another microorganism or etiologic agent) and indeterminate clinical response (situation in which at the time of evaluation it was not possible to evaluate signs and symptoms); 3) microbiological response, divided into favorable (absence of isolation of the infecting microorganism in blood cultures taken on days 7 and 14), unfavorable microbiological response (persistence of the infecting germ), 4) total response (complete favorable response corresponding to favorable clinical and microbiological response), 5) relapse, defined as the renewed presence of signs and symptoms of infection with isolation of the same infecting microorganism. The secondary outcomes evaluated in the study were duration of cefepime administration, length of stay in ICU, length of stay in ICU after diagnosis of infection, and length of hospitalization.
Statistical analysis: This study was designed to demonstrate a superiority in clinical response in the continuous infusion group of 11%, according to the sample size calculation. An intention-to-treat analysis and analysis by patients who completed the study was intended. The main outcomes: clinical and microbiological response, total response, relapses, and mortality were analyzed using the chi-square test and Fisher's exact test for homogeneity of proportions including the calculation of confidence intervals. Comparison analysis at each time point was done on a cumulative basis of cases from previous time points, even though they were no longer available. For comparison of demographic and clinical variables at baseline, averages and standard deviations were used for numerical variables.
Ethical considerations: This study was conducted according to the regulations in force in Colombia (Resolution 8430 of 1993 in Article 11") and was approved by the research committee of each institution.
5. Conclusions
This study failed to demonstrate differences between continuous versus intermittent administration of cefepime in patients with Gram-negative bacilli bacteremia. The main reason was the early closure of the study due to doubts about the safety of the drug studied, which prevented us from obtaining the planned sample. We found that overall mortality and therapeutic failure was 16% and 24% in patients included in the study with a diagnosis of severe sepsis and septic shock, while in those with bacteremia it was 12% and 12.5%, respectively.
Author Contributions
Author contributions: All authors participated in the conceptualization, methodology, information collection, data analysis, discussion, writing and preparation of this research study.
Funding
This research received no direct funding.
Institutional Review Board Statement
The study was carried out in accordance with the Declaration of Helsinki and this study was conducted according to the regulations in force in Colombia (Resolution 8430 of 1993 in Article 11") and was approved by the research committee of each institution.
Informed Consent Statement
Patient consent was waived because this study had no intervention in medical behaviors or decisions made for the patient. It was carried out with the authorization of the institutional ethics committees, who agreed on this consideration.
Data Availability Statement
Additional data about the research are under the care of principal investigator Dr. Carlos Álvarez, including the researcher's manual, data collection form annexes, and complete statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guilhaumou R, Benaboud S, Bennis Y, Dahyot-Fizelier C, Dailly E, Gandia P, et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d'Anesthésie et Réanimation-SFAR). Crit Care. 2019;23(1):104. Epub 20190329. [CrossRef] [PubMed] [PubMed Central]
- Han Y, Zhang J, Zhang HZ, Zhang XY, Wang YM. Multidrug-resistant organisms in intensive care units and logistic analysis of risk factors. World J Clin Cases. 2022;10(6):1795-805. [CrossRef] [PubMed] [PubMed Central]
- Barradell LB, Bryson HM. Cefepime. A review of its antibacterial activity, pharmacokinetic properties and therapeutic use. Drugs. 1994;47(3):471-505. [CrossRef] [PubMed]
- Pais GM, Chang J, Barreto EF, Stitt G, Downes KJ, Alshaer MH, et al. Clinical Pharmacokinetics and Pharmacodynamics of Cefepime. Clin Pharmacokinet. 2022;61(7):929-53. Epub 20220629. [CrossRef] [PubMed] [PubMed Central]
- Burgess DS, Hastings RW, Hardin TC. Pharmacokinetics and pharmacodynamics of cefepime administered by intermittent and continuous infusion. Clin Ther. 2000;22(1):66-75. [CrossRef] [PubMed]
- DeRyke CA, Lee SY, Kuti JL, Nicolau DP. Optimising dosing strategies of antibacterials utilising pharmacodynamic principles: impact on the development of resistance. Drugs. 2006;66(1):1-14. [CrossRef] [PubMed]
- Kasiakou SK, Lawrence KR, Choulis N, Falagas ME. Continuous versus intermittent intravenous administration of antibacterials with time-dependent action: a systematic review of pharmacokinetic and pharmacodynamic parameters. Drugs. 2005;65(17):2499-511. [CrossRef] [PubMed]
- Georges B, Conil JM, Cougot P, Decun JF, Archambaud M, Seguin T, et al. Cefepime in critically ill patients: continuous infusion vs. an intermittent dosing regimen. Int J Clin Pharmacol Ther. 2005;43(8):360-9. [CrossRef] [PubMed]
- US Food and Drug Administration. Early Communication About an Ongoing Safety Review Cefepime (marketed as Maxipime). http://www.fda.gov/Cder/Drug/early_comm/cefepime.htm. Acceso 25 de febrero del 2008.
- Yahav D, Paul M, Fraser A, Sarid N, Leibovici L. Efficacy and safety of cefepime: a systematic review and meta-analysis. Lancet Infect Dis. 2007;7(5):338-48. [CrossRef] [PubMed]
- Kim PW, Wu YT, Cooper C, Rochester G, Valappil T, Wang Y, et al. Meta-analysis of a possible signal of increased mortality associated with cefepime use. Clin Infect Dis. 2010;51(4):381-9. [CrossRef] [PubMed]
- Georges, B. Georges, B., Saivin, S., Cougot, P. et al. Cefepime in critically ill patients: continuous infusion versus intermittent regimen. Crit Care 5 (Suppl 1), P093 (2001). [CrossRef]
- Roberts JA, Boots R, Rickard CM, Thomas P, Quinn J, Roberts DM, et al. Is continuous infusion ceftriaxone better than once-a-day dosing in intensive care? A randomized controlled pilot study. J Antimicrob Chemother. 2007;59(2):285-91. Epub 20061128. [CrossRef] [PubMed]
- van Zanten AR, Oudijk M, Nohlmans-Paulssen MK, van der Meer YG, Girbes AR, Polderman KH. Continuous vs. intermittent cefotaxime administration in patients with chronic obstructive pulmonary disease and respiratory tract infections: pharmacokinetics/pharmacodynamics, bacterial susceptibility and clinical efficacy. Br J Clin Pharmacol. 2007;63(1):100-9. Epub 20060721. [CrossRef] [PubMed] [PubMed Central]
- Lau WK, Mercer D, Itani KM, Nicolau DP, Kuti JL, Mansfield D, et al. Randomized, open-label, comparative study of piperacillin-tazobactam administered by continuous infusion versus intermittent infusion for treatment of hospitalized patients with complicated intra-abdominal infection. Antimicrob Agents Chemother. 2006;50(11):3556-61. Epub 20060828. [CrossRef] [PubMed] [PubMed Central]
- Chapuis TM, Giannoni E, Majcherczyk PA, Chioléro R, Schaller MD, Berger MM, et al. Prospective monitoring of cefepime in intensive care unit adult patients. Crit Care. 2010;14(2):R51. Epub 20100401. [CrossRef] [PubMed] [PubMed Central]
- Philpott CD, Droege CA, Droege ME, Healy DP, Courter JD, Ernst NE, et al. Pharmacokinetics and Pharmacodynamics of Extended-Infusion Cefepime in Critically Ill Patients Receiving Continuous Renal Replacement Therapy: A Prospective, Open-Label Study. Pharmacotherapy. 2019;39(11):1066-76. Epub 20191022. [CrossRef] [PubMed]
- Jean-Michel V, Homey C, Devos P, Delannoy PY, Boussekey N, Caulier T, et al. Continuous Infusion of High Doses of Cefepime in Intensive Care Unit: Assessment of Steady-State Plasma Level and Incidence on Neurotoxicity. Antibiotics (Basel). 2022;12(1). Epub 20221230. [CrossRef] [PubMed] [PubMed Central]
- Chow SC, Shao J, Wang H. Sample Size calculation in clinical research. Marcel Dekker Inc.New York 2004: 1-15; 27-32; 204-211.
- Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med. 1995;23(10):1638-52. [CrossRef] [PubMed]
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250-6. [CrossRef] [PubMed]
- Calandra T, Cohen J. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit Care Med. 2005;33(7):1538-48. [CrossRef] [PubMed]
Table 1.
Baseline characteristics of patients with sepsis in the ICU.
| Characteristics | Intermittent infusion n = 13 |
Continuous infusion n = 12 |
|---|---|---|
| Sex (n, %) Female |
9 (69.2) |
4 (33.3) |
| Age (mean years, SD) | 54.2 +/- 21.4 | 60.2 +/- 16.9 |
| Average ICU stay prior to infection (days, SD) | 8.+/-4.5 | 5.6+/-5.1 |
| APACHE II score at study entry (mean, SD) | 15.2 +/- 8.01 | 12.7 +/- 6.3 |
| SOFA score at study entry, (mean, SD) | 6+/- 3.3 | 8 +/- 3.5 |
| Classification (n, %) Sepsis Severe sepsis Septic shock Multiple organ failure |
9 (69.2) 3 (23.0) 1 (7.7) 0 |
6 (50.0) 2 (16.7) 2 (16.7) 2 (16.7) |
| Bacteremia (n, %) | 9 (69.2) | 7 (58.3) |
| Origin of infection (n, %) Pneumonia Urosepsis Catheter sepsis Peritonitis Skin and soft tissue Tracheobronchitis Surgical site infection Bloodstream infection |
1 (7.7) 5 (38.5) 2 (14.4) 1 (7.7) 1 (7.7) 1 (7.7) 1 (7.7) 1 (7.7) |
3 (25.0) 2 (16.6) 3 (25.0) 1 (8.3) 1 (8.3) 1 (8.3) 1 (8.3) 0 |
Table 2.
Baseline characteristics of patients with Gram-negative bacilli bacteremia.
| Characteristics | Intermittent infusion n = 9 |
Continuous infusion n = 7 |
|---|---|---|
| Sex (n, %) Female |
6 (67) |
3 (43) |
| Age (years, SD) | 55.3 +/- 20.5 | 63.4 +/- 15.4 |
| Mean ICU stay before infection (days, SD) | 8.6+/-5.6 | 5+/-5.9 |
| APACHE II score at study entry (mean, SD) | 16.55 +/- 9.3 | 13.28 +/- 5.40 |
| SOFA score at study entry, (mean, SD) | 5.33+/- 1.42 | 7.6 +/- 1.72 |
| Classification (n, %) Sepsis Severe sepsis Septic shock Multiple organ failure |
6 (66.7) 2 (22.2) 1 (11.1) 0 (0.0) |
3 (42.8) 2 (28.6) 1 (14.3) 1 (14.3) |
| Isolated germ (n, %) E. coli P. aeruginosa E. cloacae S. marcencens P. mirabilis K. oxytoca |
6 (66.7) 1 (11.1) 2 (22.2) |
2 (28.6) 2 (28.6) 0 1 (14.3) 1 (14.3) 1(14.3) |
| Origin of infection (n, %) Pneumonia Bloodstream Catheter sepsis Surgical site infection Urosepsis Skin and soft tissue |
1 (11.1) 2 (22.2) 1 (11.1) 4 (44.4) 1 (11.1) |
1 (12.5) 0 3 (37.5) 1 (12.5) 2 (25) 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



