
Submitted:
29 December 2023
Posted:
30 December 2023
You are already at the latest version
Abstract
Abstract: this study aimed to evaluate the benefits of applying 5 cmH2O of CPAP using a pediatric helmet during the recovery phase from general anesthesia in brachycephalic dogs. Brachycephalic dogs undergoing various surgical procedures were included in the study, and a total of 64 subjects were randomly assigned to receive either standard oxygen supplementation (NO-CPAP group) or oxygen supplementation combined with CPAP (CPAP group). The study evaluated arterial blood pH, blood gas partial pressures of O2 and CO2, arterial blood O2 saturation, and related parameters during recovery. The dogs were monitored, and helmet tolerance was assessed using predefined criteria. Of the initially assessed 69 dogs, 64 were enrolled, 32 in the CPAP group and 32 in the NO-CPAP group. Fifteen dogs in the NO-CPAP group were excluded based on predetermined criteria. The CPAP group showed significant improvements in PaO2, PaO2/FiO2, P(A-a)O2, F-Shunt, and respiratory rate compared to the NO-CPAP group (p < 0.001). The incidence of reintubation and helmet intolerance was higher in the NO-CPAP group (18% and 15.6%, respectively) than in the CPAP group (0%). This study highlights the potential benefits of incorporating CPAP, delivered through a pediatric helmet, in the perioperative management of brachycephalic dogs.
Keywords: Brachycephalic; dog; CPAP; oxygenation; anesthesia
Keywords:
Brachycephalic
; dog
; CPAP
; oxygenation
; anesthesia
1. Introduction
Brachycephalic airway obstructive syndrome (BOAS) is a condition that affects dogs with short noses and can result in severe respiratory difficulties [1]. Due to their peculiar anatomical characteristics, brachycephalic dogs are more prone to developing upper airway respiratory complications in the postoperative period. They may experience upper airway obstruction, resulting in an increased work of breathing and potential lower arterial partial pressure of oxygen and hypercapnia [2]. Consequently, ventilatory support may be required to protect the airway and control respiratory activity [3]. For these reasons, the recovery phase from general anesthesia emerges as a pivotal component in the perioperative management of brachycephalic dog breeds. Strategic planning of the recovery period is imperative, considering factors such as the placement of a temporary tracheostomy tube, administration of corticosteroids, and the utilization of sedation and nebulization [4,5].
Ideally, after extubation, brachycephalic dogs should be placed in sternal recumbency with their head elevated, neck extended, and the tongue drawn rostrally out of the mouth. This positioning is crucial for maintaining an open airway during the recovery phase [2]. Monitoring postoperative lung function involves using arterial blood gas measurements (especially PaO2), pulse oximetry (SpO2), and assessing the dog’s respiratory rate and effort [6,7,8]. Supplemental oxygen is often administered through flow-by oxygen, placement in an oxygen cage, or nasal oxygen lines [9,10,11]. In severe cases where dyspnea remains unresponsive to supplemental oxygen, dogs may need to be anesthetized and reintubated [7].
The application of pre-and postoperative continuous positive airway pressure (CPAP) therapy has been suggested in human patients with obstructive sleep apnea to enhance oxygenation, diminish airway swelling, reduce the work of breathing, and promote recovery [12].
CPAP therapy, a noninvasive ventilation mode, maintains positive airway pressure during spontaneous breathing without needing inspiratory support [13]. Its noninvasive nature eliminates the need for endotracheal intubation and allows delivery through diverse interfaces: including the Boussignac system connected to a veterinary conical face mask [14] and a helmet equipped with a CPAP valve [13].
Studies have demonstrated that, as in humans, CPAP improves ventilation in dogs and cats, elevates arterial oxygen concentration, decreases carbon dioxide levels and respiratory rate, expands upper airway diameters, reduces airway resistance and the work of breathing and enhances functional residual capacity [13,15,16]. Furthermore, the CPAP strategy may address pulmonary atelectasis by directly recruiting alveoli, thereby lowering physiological dead space [8].
Recent research indicates that in dogs recovering from general anesthesia with impaired pulmonary gas exchange after extubation (i.e., SpO2 < 95%), normoxemia is more efficiently and rapidly restored through the application of CPAP with the helmet, as opposed to oxygen therapy [8]. Despite the evident efficacy of CPAP in enhancing oxygenation in animals, its utilization with the helmet during the recovery period from general anesthesia in brachycephalic breeds has yet to be investigated.
The main objective of this study was to evaluate the benefits of administering CPAP using a pediatric helmet equipped with a positive end-expiratory pressure (PEEP) valve during the recovery phase from general anesthesia in brachycephalic dogs. The hypothesis proposed that applying 5 cmH2O of CPAP via the helmet for 30 minutes after extubation could improve ventilatory function, increasing blood oxygenation. To test this hypothesis, a comparative analysis was conducted between patients receiving 30 minutes of standard oxygen supplementation and those receiving oxygen supplementation combined with 5 cmH2O of CPAP during a similar timeframe. The study aimed to evaluate specific outcomes, including arterial blood pH (pH) and blood gas partial pressures of O2 and CO2 (PaO2, PaCO2; mmHg), arterial blood O2 saturation (SaO2), and surrogate calculations such as the PaO2 to FiO2 ratio (PaO2/FiO2) and the estimated percentage of intrapulmonary shunt (F-Shunt), during the recovery period in brachycephalic dogs instrumented with the helmet. A comparison was made between those in the continuous positive airway pressure group (CPAP group) and those without continuous positive airway pressure (NO-CPAP group). Additionally, helmet tolerance was evaluated using both strategies.
2. Materials and Methods
The study was approved by the Ethical Committee of the Clinical and Zootechnical Studies in Animals of the Department of Emergency and Organ Transplantation of the University of Bari, Italy (n. 04/2015 D.E.T.O.), and it was conducted in three centers: University of Bari (Bari, Italy), University of Pisa (Pisa, Italy) and Istituto Veterinario di Novara (Novara, Italy). This article is reported in accordance with the Consolidated Standard of Reporting Trials (CONSORT) Statement for the reporting of randomized controlled trials [17].
2.1. Animals
After the written owner consent, this prospective, randomized, multicenter clinical study, conducted from 2015 to 2016 included brachycephalic dogs with BOAS presented for surgical procedures related to or unrelated to the airways. Exclusion criteria were: duration of anesthesia shorter than 60 minutes, impossibility to collect the data required (e.g., blood gas), severe intolerance to the helmet and severe arterial blood desaturation (SpO2 < 85 %) which required reintubation. Allocation concealment was maintained using opaque envelopes, and random assignment was conducted utilizing a sequence generator available at http://www.random.org/.
All dogs were undergoing a physical and laboratory investigation, and patients affected by any other major diseases (except BAOS) were excluded from the study. Dogs of body mass less than 5 kg and pregnant females were excluded from the study. Solid food was withheld for 6 hours, and water for 2 hours.
2.2. Anesthetic management
Dogs were admitted to the clinic two hours before general anesthesia and housed individually in separate cages. Following acclimation, all dogs received methadone intramuscularly (IM) (0.3 mg kg–1; Semfortan, Dechra) as premedication (PREM). After aseptic preparation, a catheter was inserted into a cephalic vein and into a dorsal pedal artery, to administer fluids and drugs and to collect arterial blood samples for blood gas analysis (I-stat 1, CG8+ Cartridge, Abbott, UK), respectively. If the arterial catheter could not be placed or did not remain patent until the end of the trial, arterial blood was obtained through percutaneous puncture of an accessible artery. General anesthesia was induced with intravenous (IV) propofol (Proposure 10 mg mL–1; Merial) administered to effect after at least two minutes of preoxygenation via facemask. The trachea was intubated with an appropriately sized cuffed endotracheal tube and connected to a circular breathing system. Anesthesia was maintained with isoflurane [end-tidal isoflurane percentage (EtISO) between 1.1 – 1.4%; [18]] in a mixture of oxygen (FiO2 > 0.8). A constant rate IV infusion of fentanyl (5 – 15 µg kg–1 hour–1; Fentadon, Dechra) was given intraoperatively when necessary. All animals received lactated Ringer’s solution (B.Braun, Ringer Lattato, B.Braun, Italy) at 3 mL kg–1 hour–1.
During anesthesia, dogs were ventilated with a volume-controlled ventilation mode, using a VT of 12 mL kg–1 with an inspiratory to expiratory ratio of 1:2, 25% end-inspiratory pause, and 0 cmH2O PEEP. Respiratory frequency was titrated based on the end-tidal CO2 (EtCO2), following a predetermined stepwise protocol (Table 1).
Monitoring during general anesthesia included peripheral hemoglobin oxygen saturation (SpO2; %) assessed with a pulse oximetry probe on the tongue, heart rate (HR; beats/minute) obtained from lead II electrocardiography, non-invasive arterial blood pressure (systolic, diastolic, and mean arterial blood pressure; SAP, DAP, and MAP, respectively; mmHg) using an oscillometric method, core body temperature (T; ºC) monitored through an esophageal probe, respiratory rate (RR), EtCO2 and FiO2, using a multiparametric monitor.
Post-surgery, isoflurane administration was stopped, and dogs were gradually transitioned from mechanical ventilation to spontaneous breathing. Extubation occurred upon restoring the swallowing reflex, with all patients breathing room air between the conclusion of anesthesia and extubation. After extubation, a pediatric helmet (Dimar Air, DIMAR, Italy) was promptly placed on all patients, receiving oxygen at a flow rate ranging from 6 to 10 L/min through a Venturi Valve, resulting in a measured FiO2 inside the helmet of 0.3–0.4 (Oxygen–Air mixture). In this phase, according to randomization, patients were allocated to receive (YES/NOT) 5 cmH2O of CPAP.
2.3. Study protocol
Five minutes after disconnection from the anesthetic circuit, with the endotracheal tube still in place (T0) and breathing room air (i.e., FiO2 = 0.21), a first arterial blood gas analysis was performed in all patients. At the same times HR, RR and MAP were also recorded. Immediately after extubation, patients were allocated, according to randomization, into the CPAP and NO-CPAP groups. In the CPAP group, the PEEP valve of the helmet was adjusted to ensure 5 cmH2O of CPAP, with continuous monitoring of CPAP levels using a manometer equipped with the helmet. The PEEP valve was removed from the helmets of dogs in the NO-CPAP group. Helmet tolerance (HT) was assessed in all subjects using a predefined score (Staffieri et al., 2014; Table 2).
If dogs exhibited an HT score of 4, the helmet was removed, the dog was excluded from the trial, and oxygenation continued with a facemask if necessary. The incidence of helmet intolerance was recorded and analyzed. Heart rate, RR, MAP, CPAP, FiO2, and HT were recorded every 10 minutes during the trial. Peripheral SpO2 measurement, assessed with a pulse oximetry probe at an appropriate location, was consistently maintained in all cases during the study and in case SpO2 was lower than 85%, the patient was intubated and supported with ventilation based on the clinician’s assessment of the patient’s condition. In such cases, the trial was interrupted. The incidence of reintubation was recorded and analyzed. Thirty minutes after helmet application (T30), a second arterial blood gas analysis was performed for all patients and HR, RR, HT and MAP were also recorded. Cases where obtaining a second arterial blood sample was not feasible were excluded from subsequent analyses.
2.4. Gas blood assessment
Arterial blood gases were corrected for the patient’s body temperature at the time of sampling. The analyzer provided the SaO2 value. The PaO2/FiO2 was calculated as an index to describe pulmonary arterial blood oxygenation.
The alveolar-arterial oxygen gradient of O2 [P(A-a) O2] was calculated using the alveolar gas equation:
where PB is the barometric pressure, PH2O is the water vapor pressure, and R is the respiratory exchange ratio, assumed to be 0.8 [13]. The analyzer measured the PB during each analysis, and the PH2O was also corrected for the patient’s rectal temperature.
P(A-a)O2 = [(PB-PH2O) x FiO2 – PaCO2/R] – PaO2,
The estimated percentage of intrapulmonary shunt (F-Shunt) was calculated as follows [19]
where Cc′O2 is the pulmonary end-capillary oxygen content, CaO2 is the arterial oxygen content, and 3.5 mL dL–1 is an approximately fixed value of the arterial-to-mixed venous oxygen content difference. Cc′O2 and CaO2 were calculated as follows:
where Hb is the hemoglobin concentration (g dL–1), 1.31 is the oxygen-carrying capacity of hemoglobin (mL g–1), Sc′O2 is the pulmonary end-capillary oxygen saturation, 0.003 is the solubility coefficient of oxygen in dog plasma [20] and Pc′O2 is the pulmonary end-capillary partial pressure of oxygen. The Pc′O2 was assumed to be equal to PAO2. For PAO2 > 100 mmHg, Pc′O2 was assumed to be 100%; for PAO2 ≤ 100 mmHg, Pc′O2 was calculated from the actual PAO2 via the same method.
F-Shunt = ([Cc′O2 – CaO2] / [Cc′O2 – CaO2 + 3.5 mL dL–1]) × 100
Cc′O2 = Hb × 1.31 × Sc′O2 + 0.0031 × Pc′O2
CaO2 = Hb × 1.31 × SaO2 + 0.003 × PaO2
2.5. Statistical analysis
Sample size was calculated based on previous data [13] and an estimated clinically significant variation of PaO2/FiO2 of 20%. Power calculation was conducted for a two-tailed t-test with a power of 0.8 and an alpha error of 0.05 (Granmo, Version 7.12). The results of this analysis suggested that a minimum of 14 dogs per group would be sufficient to detect significant differences among groups.
All data were analyzed using MedCalc 12.7.0.0 software.
Normal distribution of the data was evaluated using the Shapiro-Wilk test. For all data, the mean and standard deviation were calculated. Data regarding age, bodyweight, anesthesia duration, blood gas assessment at PREM (PaO2, PaCO2 and pH), RR, HR and MAP were compared between groups with the one-way ANOVA test and the post-hoc analysis was performed with the Tukey test. The postoperative values at T0 and at T30 of HR, MAP, RR, HT, PaO2, PaO2/FiO2, P(A-a)O2, F-Shunt, SaO2, PaCO2 and helmet tolerance score were analyzed by 2 ways ANOVA with treatment, time and treatment by time interaction were included in the model as fixed effects. The Bonferroni test was used for post-hoc analysis. A P value <0.05 was considered statistically significant.
3. Results
A cohort of 69 brachycephalic dogs undergoing surgical procedures was initially assessed for eligibility. Subsequently, five cases were excluded due to non-compliance with inclusion criteria, specifically related to the duration of anesthesia. Consequently, 64 dogs were enrolled, with an equal distribution of 32 in each group. A total of fifteen dogs in the NO-CPAP group were excluded from the study based on the exclusion criteria; five were excluded due to an HT score of 4 (5/32, 15.6 %), six because an SpO2 < 85% and were reintubated (6/32, 18 %), and four because the second arterial blood sample was not feasible. Therefore, the study was completed by 32 animals in the CPAP group and 17 animals in the NO-CPAP group (Figure 1).
The baseline characteristics of the subjects by intervention group are presented in Table 3 and no statistical differences were observed.
Regarding the primary outcomes, a significant difference was observed between CPAP and NO-CPAP groups regarding the PaO2 (p < 0.001), PaO2/FiO2 (p < 0.001), P(A-a)O2 (p < 0.001), F-Shunt (p < 0.001) and RR (p = 0.03). There were no significant differences between the groups in PaCO2 (p = 0.13), pH (p = 0.09), HR and MAP, SaO2 and the HT (Table 4 and Figure 2, Figure 3, Figure 4 and Figure 5) between the dogs that completed the study. The incidence of reintubation (18% in the NO-CPAP group vs. 0% in the CPAP group) and HT (15.6% in the NO-CPAP group vs. 0% in the CPAP group) was higher in the NO-CPAP group compared to the CPAP group.
4. Discussion
This prospective, multicenter, randomized clinical study demonstrated that applying CPAP therapy using a pediatric helmet with 5 cm H2O for 30 minutes during the recovery phase from general anesthesia in brachycephalic dogs with BOAS enhanced blood oxygenation. Furthermore, compared to a non-CPAP approach, patients receiving 5 cm H2O CPAP exhibited reduced complications and a notable helmet tolerance, reflecting a more comfortable recovery.
The BOAS is notably prevalent among brachycephalic dogs, a group anatomically predisposed to postoperative hypoxia due to their airway morphology. Consequently, peri anesthetic mortality rates in brachycephalic breeds are considerably higher than in non-brachycephalic breeds. In particular, most deaths in brachycephalic breeds occur during the postoperative period, mainly due to respiratory complications [21]. Therefore, postoperative airway management in these breeds is paramount, aiming to mitigate the natural tendency for airway obstruction [2].
Helmet CPAP has demonstrated more tolerability in humans than other interfaces used in noninvasive ventilation strategies, offering effective sealing and airway stability. Studies have indicated that, when compared to conventional oxygen therapy, helmet CPAP reduces the intubation rate and lowers mortality [22].
The current study aligns with this pattern. Dogs receiving CPAP with the helmet exhibited a notable tolerance to the interface, contrasting with animals in the NO-CPAP group, which showed intolerance to the helmet and need for reintubation in 15.6 % and 18 % of the cases, respectively.
Given the specific conditions of this study, we can assume that CPAP administration was the discriminating factor that improved tolerance and reduced the need for reintubation. The only difference between the groups in this study was the CPAP therapy. Data from this study reveal that pre-extubation breathing of room air through the endotracheal tube led to consistently good and comparable oxygenation status between the two groups, suggesting a similar baseline oxygenation level at the end of anesthesia. More precisely, at baseline (T0) in both groups, the PaO2 measured approximately 90 mmHg, the PaO2/FiO2 ratio hovered around 300, and the F-Shunt was approximately 15%. Additionally, the RR and PaCO2 levels were similar between groups, suggesting comparable ventilation conditions at the initial measurement.
However, after extubation, airway obstruction activated, and oxygenation deteriorated in the NO-CPAP group, where a standard oxygen supplementation failed to maintain blood oxygenation. Data at T30 indicate a significant difference between the two noninvasive ventilatory support techniques used in this study. All in all, helmet CPAP increased PaO2 by 78% (91.8 vs. 164 mmHg) and PaO2/FiO2 by 56.7% (298 vs. 467). In contrast, animals in the NO-CPAP group showed worsened oxygenation at T30 compared to T0 despite the standard oxygen therapy. In the NO-CPAP group, there was a marginal and statistically non-significant increase of 14% in PaO2 (96 vs. 110 mmHg), accompanied by a 20% decrease in PaO2/FiO2 (310 vs. 246). Assuming an average FiO2 value of 0.35 and 21% at T30 and T0, respectively, it can be inferred that using CPAP, known to induce airway distension [16], facilitates improved tidal volume diffusion. These changes, in turn, enhance alveolar ventilation, improving the oxygenation [13].
This study also revealed that, despite similar PaCO2 levels in the CPAP and NO-CPAP groups at T30, there was a significant reduction in intrapulmonary shunts and a conserved respiratory rate in the CPAP group. Specifically, data on the intrapulmonary shunt, estimated using the F-Shunt formula, demonstrated that in subjects receiving CPAP, the percentage of shunt decreased by 50% at the end of treatment (16.6% vs. 7.4%) compared to the NO-CPAP group, where the F-Shunt remained unchanged (14.7% vs. 12.6%). This result suggests that the increased airway distension provided by the helmet CPAP reduced the work of breathing (decreased resistances), increased lung parenchyma distension, promoted alveolar recruitment, and, subsequently, reduced the intrapulmonary shunt [13,15]. This finding coincides with those reported in dogs with hypoxemic acute respiratory failure in which the helmet CPAP allows FiO2 to be increased approximately to 40% and significantly decreased the F-Shunt by 37% in most dogs [23].
Additional noteworthy data from the study include the reduction in P(A-a)O2 observed in the CPAP group at T30 compared to the NO-CPAP group. The significant increase in P(A-a)O2 in the NO-CPAP group suggests a degree of pulmonary atelectasis, providing insight into the differences between the groups. These findings align with those reported for dogs experiencing hypoxemic acute respiratory failure, where helmet CPAP increased PaO2 and PaO2/FiO2 ratio, accompanied by a significant decrease in P(A-a)O2 after CPAP therapy (pre-CPAP = 52.4 ± 17.07 mmHg vs. post-CPAP = 35.15 ± 22.98 mmHg). These changes suggest potential pulmonary recruitment of collapsed areas [23].
The PaCO2 values in dogs in the NO-CPAP group can be attributed to a dramatic 94% increase in RR (19 vs. 27 breaths/minute), suggesting a reduction in tidal volume at T30 in this population. Although not measured, the hypothetical reduction in tidal volume could be related to airway obstruction leading to postoperative dyspnea. In contrast, these findings were different in the CPAP group, where RR remained unchanged between T30 and T0, presumably due to ensuring airway patency [16,24,25].
In dogs with BOAS, airway protection through intubation resolves active airway obstruction. However, upon extubation, without support, the work of breathing increases, leading to respiratory fatigue, a gradual reduction in tidal volume, and the need to increase RR to maintain PaCO2 levels [2].
The helmet CPAP, as an alternative to non-invasive ventilatory support, appears promising for enhancing ventilation and blood oxygenation during anesthetic recovery in brachycephalic breeds. However, further studies are warranted to confirm this observation.
High-flow nasal cannula (HFNC) is an alternative technique for noninvasive respiratory support that has recently been introduced in veterinary medicine. It involves administering a very high (20-60 L/min), humidified, and heated gas flow into the animal’s nostrils (Krawec et al., 2022). This technique has been evaluated in a few cases for postoperative respiratory support in brachycephalic dogs [10]. The authors were able to prove that HFNC reduced dyspnea over time. However, this study did not have a control group and lacked any oxygenation assessment. For this reason, this study cannot be compared with our results, and future researchers could compare the two noninvasive respiratory support techniques in brachycephalic breeds.
This study has several limitations. Firstly, we did not stratify our population of dogs and results to consider the severity of BAOS; an aspect future studies may find valuable to explore. Additionally, the potential bias introduced by the unequal completion rates in the two groups could impact the results; however, the study’s minimum required number of cases for power calculation was maintained.
Moreover, our observation was confined to the initial 30 minutes of the postoperative period, and extending the observation period might have yielded additional insightful information. Future studies could address these limitations to enhance the comprehensiveness and robustness of the findings.
5. Conclusions
In conclusion, the study underscores the importance of strategic perioperative management in brachycephalic breeds, with a specific focus on the recovery phase. The application of CPAP, particularly via a pediatric helmet, demonstrates promising results in improving oxygenation during the recovery period. Further investigations and larger-scale studies are warranted to validate and generalize these findings, ultimately contributing to enhanced care for brachycephalic dogs undergoing surgical procedures.
Author Contributions
Conceptualization, F.S. and P.O..; methodology, A.B., V.R., and F.S.; software, C.V., P.O..; validation, C.V., P.O., M.S. C.P. A.C., L.L.. and F.S..; formal analysis, C.V., F.S., P.O., M.S., C.P..; investigation, A.B., V.R. A.C., L.L., F.S., .; resources, F.S., A.C..; data curation, F.S., C.V., M.S., C.P..; writing—original draft preparation, C.V., F.S., P.O.,.; writing—review and editing, M.S., C.P..; visualization, C.P., M.S..; supervision, P.O., F.S..; project administration, F.S., P.O..; funding acquisition, F.S., P.O:. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Ethical Committee of the Clinical and Zootechnical Studies in Animals of the Department of Emergency and Organ Transplantation of the University of Bari, Italy (n. 04/2015 D.E.T.O.), and it was conducted in three centers: University of Bari (Bari, Italy), University of Pisa (Pisa, Italy) and Istituto Veterinario di Novara (Novara, Italy). This article is reported in accordance with the Consolidated Standard of Reporting Trials (CONSORT) Statement for the reporting of randomized controlled trials.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available contacting the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Koch, D.A.; Arnold, S.; Hubler, M.; Montavon, P.M. Brachycephalic Syndrome in Dogs. Compend. Contin. Educ. Pract. Vet.-NORTH Am. Ed.- 2003, 25, 48–55. [Google Scholar]
- Downing, F.; Gibson, S. Anaesthesia of Brachycephalic Dogs. J. Small Anim. Pract. 2018, 59, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Hoareau, G.L.; Mellema, M.S.; Silverstein, D.C. Indication, Management, and Outcome of Brachycephalic Dogs Requiring Mechanical Ventilation. J. Vet. Emerg. Crit. Care San Antonio Tex 2001 2011, 21, 226–235. [Google Scholar] [CrossRef]
- Costa, R.S.; Abelson, A.L.; Lindsey, J.C.; Wetmore, L.A. Postoperative Regurgitation and Respiratory Complications in Brachycephalic Dogs Undergoing Airway Surgery before and after Implementation of a Standardized Perianesthetic Protocol. J. Am. Vet. Med. Assoc. 2020, 256, 899–905. [Google Scholar] [CrossRef]
- Fenner, J.; Henderson, C.; Demetriou, J. Nebulised Adrenaline in the Post-Operative Management of Brachycephalic Obstructive Airway Syndrome in Dogs: Short-Term Outcomes in 90 Cases (2014–2020). N. Z. Vet. J. 2023, 71, 329–336. [Google Scholar] [CrossRef]
- Alwood, A.J.; Brainard, B.M.; LaFond, E.; Drobatz, K.J.; King, L.G. Postoperative Pulmonary Complications in Dogs Undergoing Laparotomy: Frequency, Characterization and Disease-Related Risk Factors. J. Vet. Emerg. Crit. Care 2006, 16, 176–183. [Google Scholar] [CrossRef]
- Lindsay, B.; Cook, D.; Wetzel, J.-M.; Siess, S.; Moses, P. Brachycephalic Airway Syndrome: Management of Post-Operative Respiratory Complications in 248 Dogs. Aust. Vet. J. 2020, 98, 173–180. [Google Scholar] [CrossRef]
- Stabile, M.; Lacitignola, L.; Piemontese, M.R.; Di Bella, C.; Acquafredda, C.; Grasso, S.; Crovace, A.M.; Gomez de Segura, I.A.; Staffieri, F. Comparison of CPAP and Oxygen Therapy for Treatment of Postoperative Hypoxaemia in Dogs. J. Small Anim. Pract. 2021, 62, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Boyle, J. Oxygen Therapy. In Advanced Monitoring and Procedures for Small Animal Emergency and Critical Care; John Wiley & Sons, Ltd, 2012; pp. 261–273 ISBN 978-1-118-99724-6.
- Jagodich, T.A.; Bersenas, A.M.E.; Bateman, S.W.; Kerr, C.L. Preliminary Evaluation of the Use of High-Flow Nasal Cannula Oxygen Therapy during Recovery from General Anesthesia in Dogs with Obstructive Upper Airway Breathing. J. Vet. Emerg. Crit. Care 2020, 30, 487–492. [Google Scholar] [CrossRef]
- Senn, D.; Sigrist, N.; Forterre, F.; Howard, J.; Spreng, D. Retrospective Evaluation of Postoperative Nasotracheal Tubes for Oxygen Supplementation in Dogs Following Surgery for Brachycephalic Syndrome: 36 Cases (2003–2007). J. Vet. Emerg. Crit. Care 2011, 21, 261–267. [Google Scholar] [CrossRef]
- Martinez, G.; Faber, P. Obstructive Sleep Apnoea. Contin. Educ. Anaesth. Crit. Care Pain 2011, 11, 5–8. [Google Scholar] [CrossRef]
- Staffieri, F.; Crovace, A.; De Monte, V.; Centonze, P.; Gigante, G.; Grasso, S. Noninvasive Continuous Positive Airway Pressure Delivered Using a Pediatric Helmet in Dogs Recovering from General Anesthesia. J. Vet. Emerg. Crit. Care 2014, 24, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Briganti, A.; Melanie, P.; Portela, D.; Breghi, G.; Mama, K. Continuous Positive Airway Pressure Administered via Face Mask in Tranquilized Dogs. J. Vet. Emerg. Crit. Care 2010, 20, 503–508. [Google Scholar] [CrossRef]
- Di Bella, C.; Araos, J.; Lacitignola, L.; Grasso, S.; De Marzo, L.; Crovace, A.M.; Staffieri, F. Effects of Continuous Positive Airway Pressure Administered by a Helmet in Cats under General Anaesthesia. J. Feline Med. Surg. 2021, 23, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Rondelli, V.; Guarracino, A.; Iacobellis, P.; Grasso, S.; Stripoli, T.; Lacitignola, L.; Auriemma, E.; Romano, F.; Araos, J.D.; Staffieri, F. Evaluation of the Effects of Helmet Continuous Positive Airway Pressure on Laryngeal Size in Dogs Anesthetized with Propofol and Fentanyl Using Computed Tomography. J. Vet. Emerg. Crit. Care 2020, 30, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 Statement: Extension to Randomised Crossover Trials. BMJ 2019, 366, l4378. [Google Scholar] [CrossRef]
- Reed, R.; Doherty, T. Minimum Alveolar Concentration: Key Concepts and a Review of Its Pharmacological Reduction in Dogs. Part 1. Res. Vet. Sci. 2018, 117, 266–270. [Google Scholar] [CrossRef]
- Araos, J.D.; Larenza, M.P.; Boston, R.C.; De Monte, V.; De Marzo, C.; Grasso, S.; Haskins, S.C.; Crovace, A.; Staffieri, F. Use of the Oxygen Content-Based Index, Fshunt, as an Indicator of Pulmonary Venous Admixture at Various Inspired Oxygen Fractions in Anesthetized Sheep. Am. J. Vet. Res. 2012, 73, 2013–2020. [Google Scholar] [CrossRef]
- Haskins, S.; Pascoe, P.J.; Ilkiw, J.E.; Fudge, J.; Hopper, K.; Aldrich, J. Reference Cardiopulmonary Values in Normal Dogs. Comp. Med. 2005, 55. [Google Scholar]
- Oda, A.; Wang, W.H.; Hampton, A.K.; Robertson, J.B.; Posner, L.P. Perianesthetic Mortality in English Bulldogs: A Retrospective Analysis in 2010 - 2017. BMC Vet. Res. 2022, 18, 198. [Google Scholar] [CrossRef]
- Adi, O.; Fong, C.P.; Keong, Y.Y.; Apoo, F.N.; Roslan, N.L. Helmet CPAP in the Emergency Department: A Narrative Review. Am. J. Emerg. Med. 2023, 67, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Ceccherini, G.; Lippi, I.; Citi, S.; Perondi, F.; Pamapanini, M.; Guidi, G.; Briganti, A. Continuous Positive Airway Pressure (CPAP) Provision with a Pediatric Helmet for Treatment of Hypoxemic Acute Respiratory Failure in Dogs. J. Vet. Emerg. Crit. Care 2020, 30, 41–49. [Google Scholar] [CrossRef]
- Reissmann, H.K.; Ranieri, V.M.; Goldberg, P.; Gottfried, S.B. Continuous Positive Airway Pressure Facilitates Spontaneous Breathing in Weaning Chronic Obstructive Pulmonary Disease Patients by Improving Breathing Pattern and Gas Exchange. Intensive Care Med. 2000, 26, 1764–1772. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Pitoyo, C.W. Non-Invasive Ventilation in Acute Respiratory Failure. Acta Medica Indones. 2014, 46, 74–80. [Google Scholar]
Figure 1.
CONSORT flow diagram of the brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP.
Figure 1.
CONSORT flow diagram of the brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP.
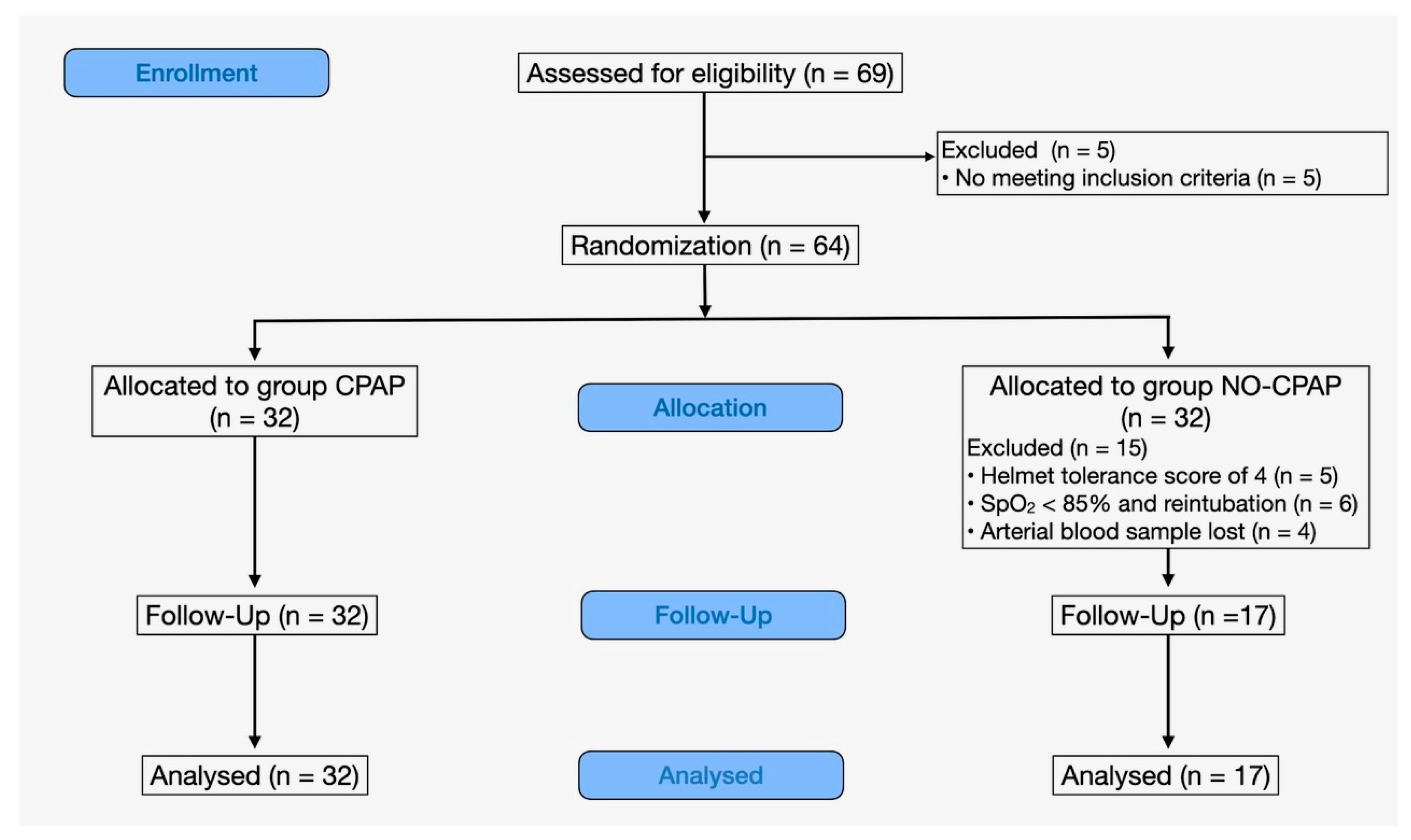
Figure 2.
Means ± standard deviations of the ratio of arterial partial oxygen tension to inspired oxygen fraction (PaO2/FiO2) in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FiO2= 0.21) and at T30 after 30 minutes of support (FiO2= 0.35-0.40).
Figure 2.
Means ± standard deviations of the ratio of arterial partial oxygen tension to inspired oxygen fraction (PaO2/FiO2) in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FiO2= 0.21) and at T30 after 30 minutes of support (FiO2= 0.35-0.40).
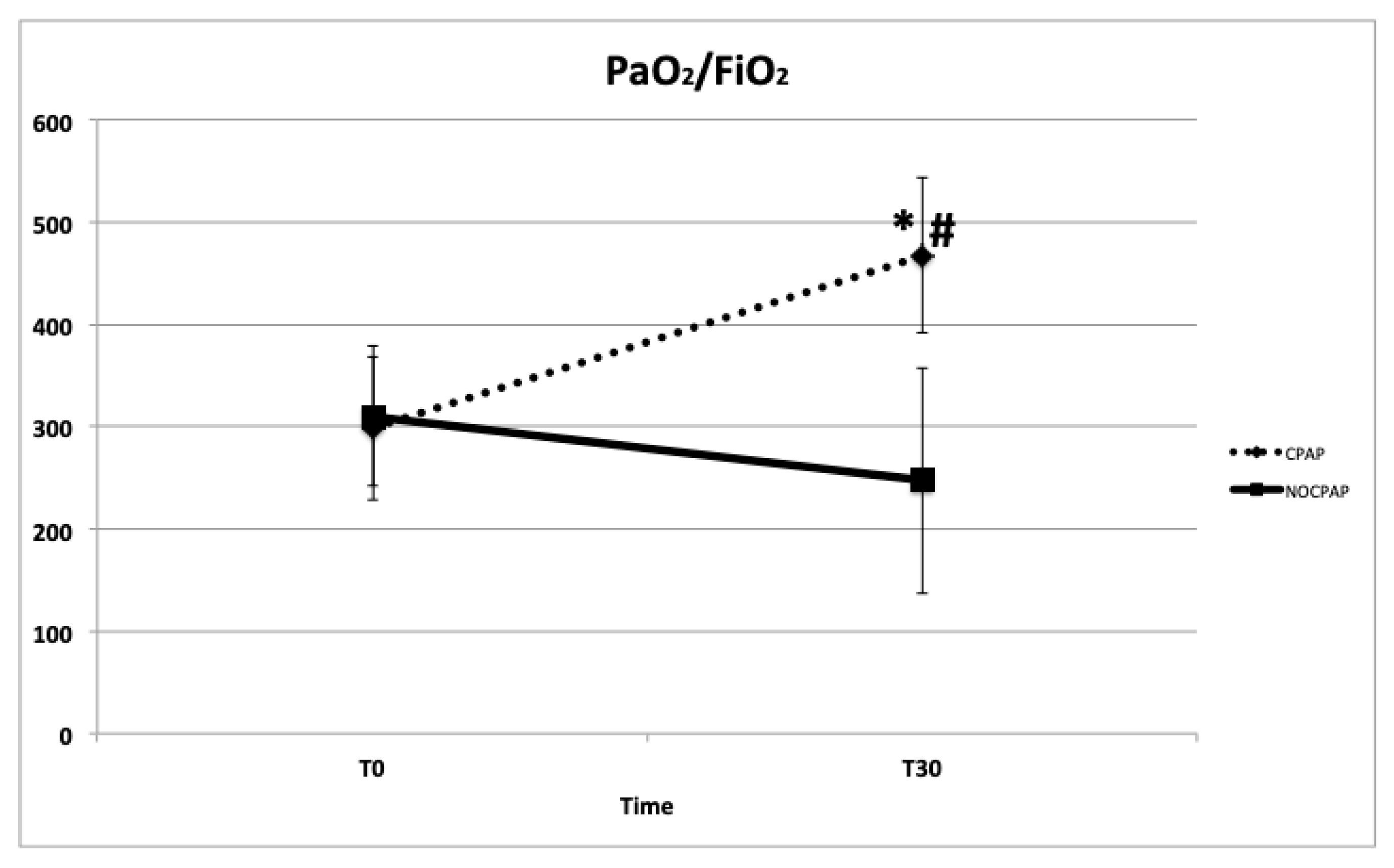
Figure 3.
Mean and standard deviation of alveolar-arterial difference of oxygen tension [P(A-a)O2] in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FiO2= 0.21) and at T30 after 30 minutes of support (FiO2: 0.35-0.40).
Figure 3.
Mean and standard deviation of alveolar-arterial difference of oxygen tension [P(A-a)O2] in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FiO2= 0.21) and at T30 after 30 minutes of support (FiO2: 0.35-0.40).
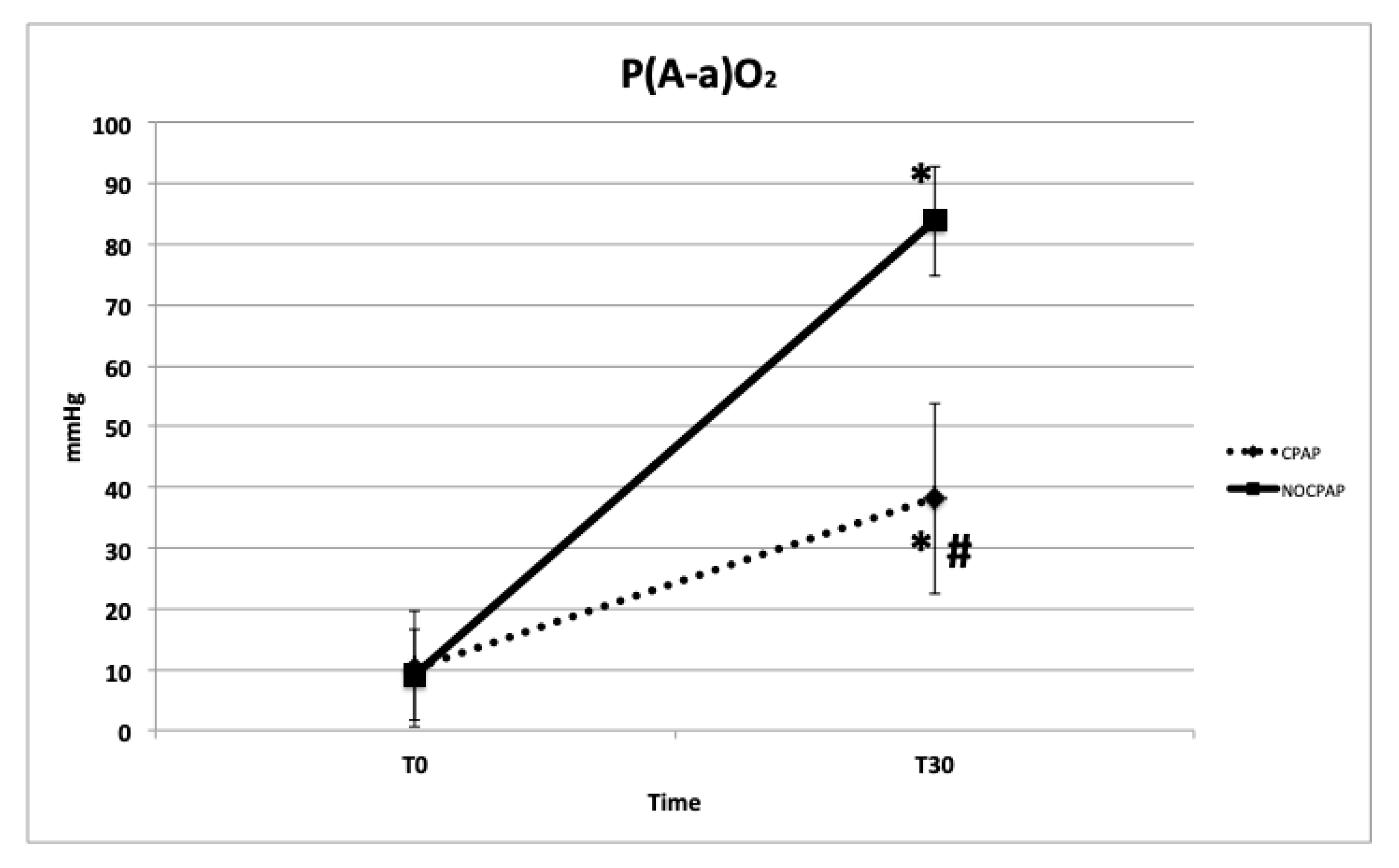
Figure 4.
Mean and standard deviation values of estimated intrapulmonary shunt fraction (F-Shunt) in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FiO2= 0.21) and at T30 after 30 minutes of support (FiO2= 0.35-0.40).
Figure 4.
Mean and standard deviation values of estimated intrapulmonary shunt fraction (F-Shunt) in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FiO2= 0.21) and at T30 after 30 minutes of support (FiO2= 0.35-0.40).
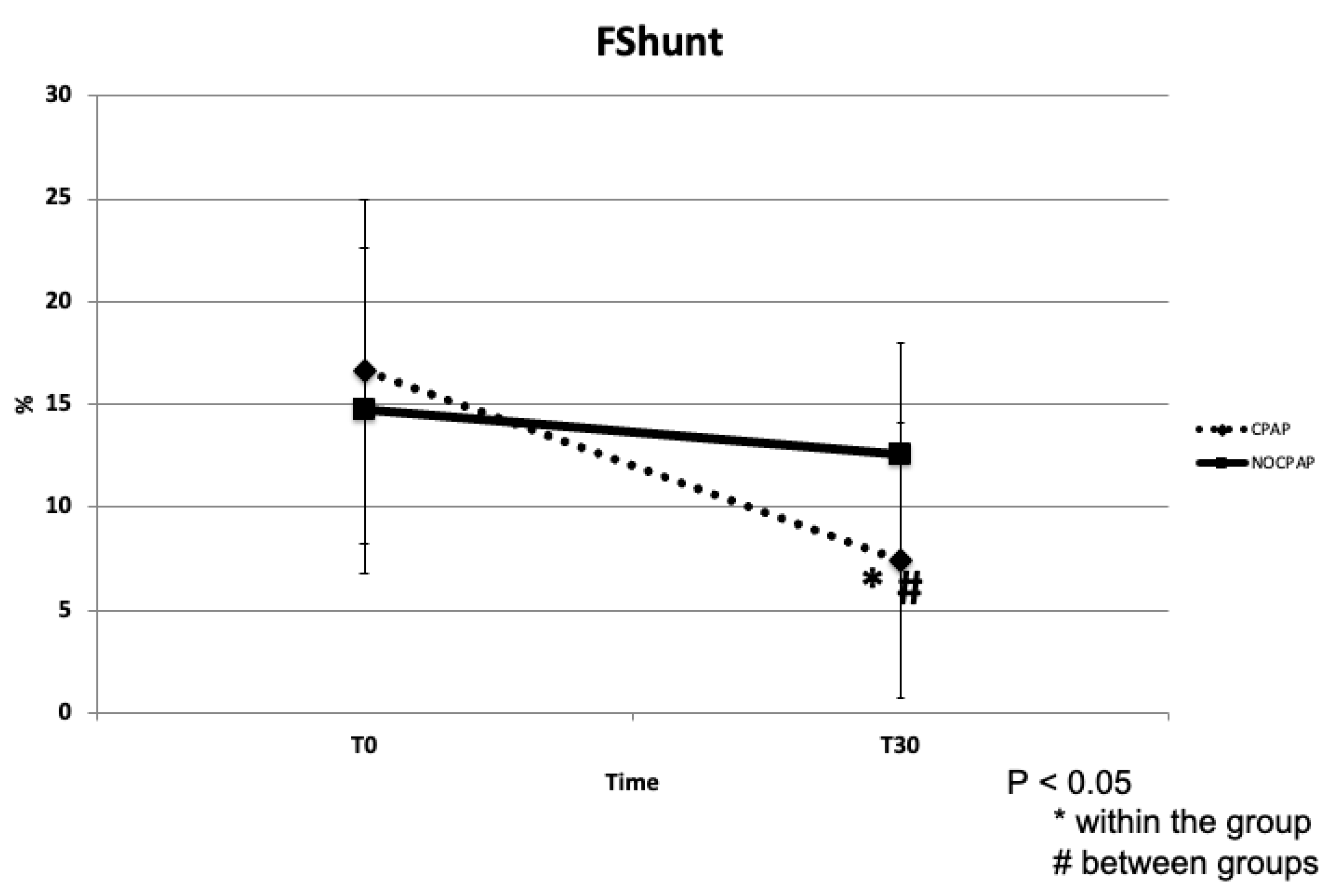
Figure 5.
Mean and standard deviation values of arterial partial pressure of carbon dioxide (PaCO2) in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FIO2= 0.21) and at T30 after 30 minutes of support (FIO2= 0.35–0.40).
Figure 5.
Mean and standard deviation values of arterial partial pressure of carbon dioxide (PaCO2) in brachycephalic dogs recovering from general anesthesia and receiving noninvasive oxygen support by means of a helmet with (CPAP group) or without (NO-CPAP group) 5 cmH2O of CPAP. Data are reported at T0, immediately prior to support (FIO2= 0.21) and at T30 after 30 minutes of support (FIO2= 0.35–0.40).
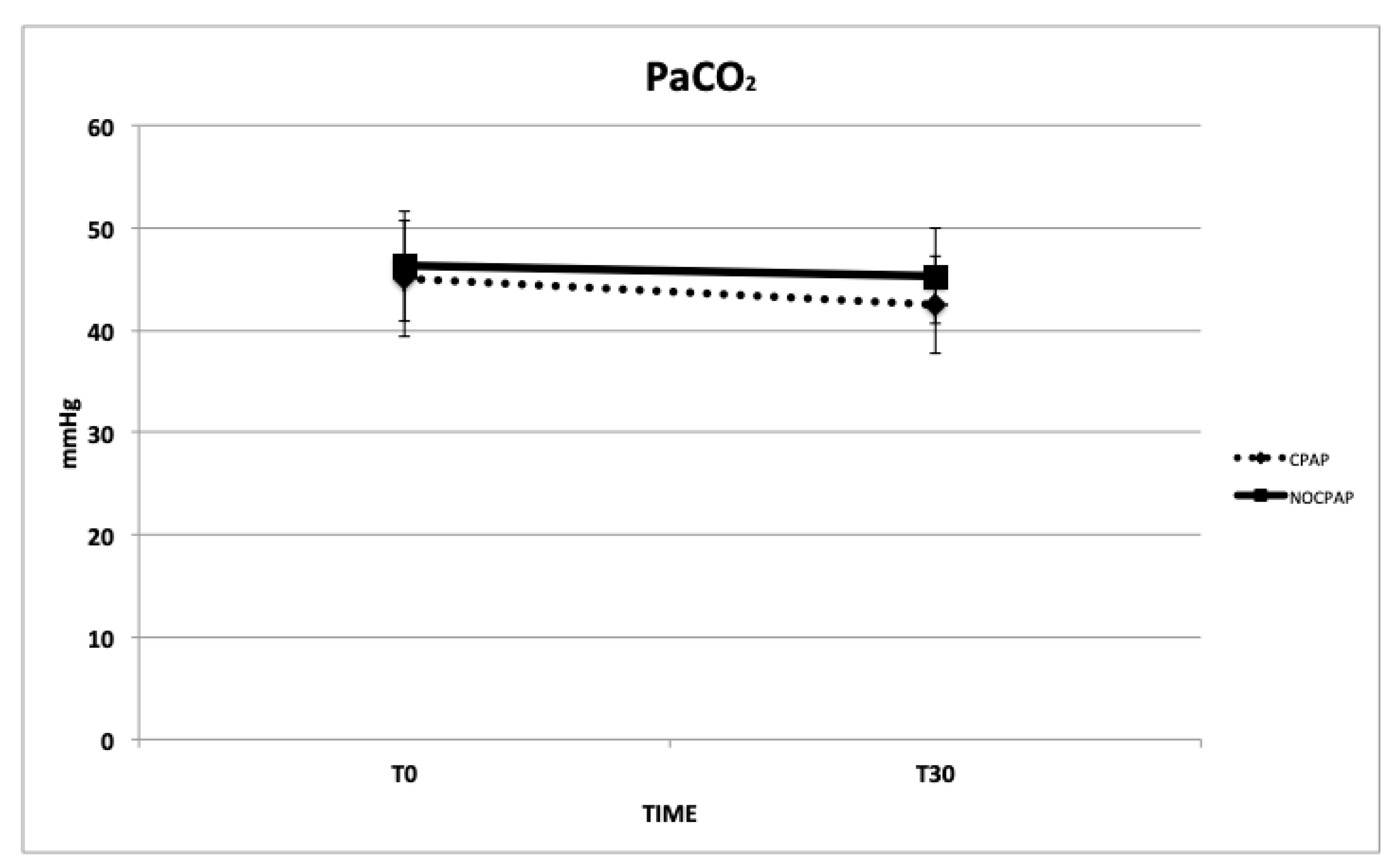

Table 1.
Predetermined stepwise protocol for adjusting respiratory rate (RR) to end-tidal CO2 (EtCO2) during volume-control mode ventilation in brachycephalic dogs undergoing surgical procedures exceeding 60 minutes.
Table 1.
Predetermined stepwise protocol for adjusting respiratory rate (RR) to end-tidal CO2 (EtCO2) during volume-control mode ventilation in brachycephalic dogs undergoing surgical procedures exceeding 60 minutes.
| RR (breaths/minute) | EtCO2 (mmHg) |
|---|---|
| < 20 | 40–45 |
| < 30 | 45–55 |
| < 40 | 55–65 |
Table 2.
Helmet tolerance score (Staffieri et al., 2014).
1. The patient is comfortable; no agitation; no attempts to remove the helmet. |
2. The patient tolerates the helmet, but looks stressed and afraid; no attempts to remove to helmet. |
3. The patient tries to remove the helmet and is agitated. It is still possible to keep the helmet on by gently restraining the patient. |
4. The patient does not tolerate the helmet, is restless, attempts to move and put the helmet, and needs extra sedation to tolerate the helmet |
Table 3.
Number of animals within each group that completed the study and respective data (mean ± standard deviation) of sex, age, bodyweight, duration of anesthesia, respiratory rate (RR), heart rate (HR), mean arterial pressure (MAP), arterial oxygen (PaO2) and carbon dioxide (PaCO2) tensions, and pH at premedication (PREM).
Table 3.
Number of animals within each group that completed the study and respective data (mean ± standard deviation) of sex, age, bodyweight, duration of anesthesia, respiratory rate (RR), heart rate (HR), mean arterial pressure (MAP), arterial oxygen (PaO2) and carbon dioxide (PaCO2) tensions, and pH at premedication (PREM).
| CPAP | NO-CPAP | P | |
|---|---|---|---|
| Dogs (n) | 32 | 17 | 0.34 |
| Sex (female/male; n) | 18/14 | 11/6 | 0.67 |
| Age (months) | 4.3 ± 3,0 | 4,9 ± 3,4 | 0.13 |
| Bodyweight (kg) | 15.8 ± 7.5 | 15.6 ± 5.4 | 0.21 |
| Duration of anesthesia (minutes) | 82 ± 13 | 88 ± 12 | 0.12 |
| RR (breaths/minute) at PREM | 27 ± 15 | 18 ± 5 | 0.11 |
| HR (beats/minutes) at PREM | 103 ± 18 | 107 ± 28 | 0.23 |
| MAP (mmHg) at PREM | 84 ± 5 | 84 ± 5 | 0.31 |
| PaO2 (mmHg) | 95 ± 6 | 93 ± 4 | 0.21 |
| PaCO2 (mmHg) | 34.1 ± 2.4 | 36.5 ± 3.6 | 0.09 |
| pH | 7.39 ± 0.02 | 7.34 ± 0.12 | 0.12 |
Table 4.
Mean ± standard deviation of respiratory rate (RR), heart rate (HR), mean arterial blood pressure (MAP), arterial oxygen (PaO2) and carbon dioxide (PaCO2) tensions, the PaO2 to inspired oxygen tension ratio (PaO2/FiO2), the estimated intrapulmonary shunt (F-Shunt), the arterial O2 saturation (SaO2) and the helmet tolerance score (HF) in the postoperative period pf dogs that completed the study divided in the two groups with (CPAP) and without (NO-CPAP) 5 cmH2O of CPAP. p < 0.05 *within groups, #between groups.
Table 4.
Mean ± standard deviation of respiratory rate (RR), heart rate (HR), mean arterial blood pressure (MAP), arterial oxygen (PaO2) and carbon dioxide (PaCO2) tensions, the PaO2 to inspired oxygen tension ratio (PaO2/FiO2), the estimated intrapulmonary shunt (F-Shunt), the arterial O2 saturation (SaO2) and the helmet tolerance score (HF) in the postoperative period pf dogs that completed the study divided in the two groups with (CPAP) and without (NO-CPAP) 5 cmH2O of CPAP. p < 0.05 *within groups, #between groups.
| Parameters | GROUP | T0 | T30 |
|---|---|---|---|
| RR (breaths/min) | CPAP NO-CPAP |
19.6 ± 9.1 19.1± 4.8 |
19.8 ± 10.5# 27.7 ± 12.6 |
| HR | CPAP NO-CPAP |
104 ± 24 99 ± 15 |
98 ± 18 93 ± 13 |
| MAP | CPAP NO-CPAP |
82 ± 7 81± 7 |
82 ± 10 84 ± 9 |
| PaO2 (mmHg) | CPAP NO-CPAP |
91.8 ± 20.4 96.1 ± 14.3 |
164.7 ± 27.5*# 110.4 ± 17.3 |
| PaO2/FiO2 | CPAP NO-CPAP |
298.1 ± 69.6 310.5 ± 68.3 |
467.1 ± 75.9*# 246.9 ± 109.8* |
| P(A-a)O2 mmHg | CPAP NO-CPAP |
10.2 ± 9.6 9.1 ± 7.5 |
38.1 ± 15.6*# 83.8 ± 9.1* |
| F-Shunt (%) | CPAP NO-CPAP |
16.6 ± 8.4 14.7 ± 7.9 |
7.4 ± 6.7*# 12.6 ± 5.4 |
| SaO2 | CPAP NO-CPAP |
95.4 ± 3.1 95.2 ± 2.1 |
98.8 ± 1.5 98.2 ± 1.5 |
| PaCO2 (mmHg) | CPAP NO-CPAP |
45.1 ± 5.7 46.3 ± 5.4 |
42.5 ± 4.8 45.3 ± 4.7 |
| HT | CPAP NO-CPAP |
2.4 ± 0.7 3.2 ± 0.5 |
1.8 ± 1.1 2.9 ± 0.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



