
Submitted:
02 January 2024
Posted:
03 January 2024
You are already at the latest version
Abstract
Background and Aims: Late diagnosis of sepsis is associated with adverse consequences and high mortality rate.
The aim of this study was to evaluate the diagnostic value of hematologic research parameters, that reflect the cell morphology of blood cells, available on the BC 6800 plus automated analyzer (Mindray) for the early detection of sepsis.
Materials and Methods: A complete blood count (CBC) was performed by Mindray BC 6800 Plus Analyzer in 327 patients (223 with a confirmed diagnosis of sepsis following sepsis-3 criteria, 104 without sepsis), admitted at the Intensive Care Unit of the Novara’s Hospital (Italy) and in 56 patients with localized infection.
Results: In univariate logistic regression, age, Hb, RDW, MO#, NMR, NeuX, NeuY, NeuZ, LymX, MonX, MonY, MonZ were associated with sepsis (p<0.005). In multivariate analysis, only RDW, NeuX, NeuY, NeuZ, MonX and MonZ were found to be independent predictors of sepsis (p<0.005). Morphological research parameters are confirmed to be predictors of sepsis even when analyzing the group with localized infection.
Conclusions: In addition to already established biomarkers and basic CBC parameters, new morphological cell parameters can be a valuable aid in the early diagnosis of sepsis at no additional cost.
Keywords:
affordable health care
; early diagnosis
; leukocyte parameters
; morphological changes
; Red Cell Distribution Width (RDW)
; sepsis
1. Introduction
Sepsis is a life-threatening condition caused by a systemic and dysregulated host response to infection [1]. Sepsis is one of the leading causes of death in hospitalized patients and is also a major contributor to neonatal mortality and morbidity, especially in low- and middle-income countries [2,3]. According to the World Health Organization (WHO) and the Global Burden of Diseases report, sepsis is estimated to affect nearly 50 million people each year and cause 11 million deaths annually, accounting for 20% of all deaths worldwide [4]. Initiatives such as the World Sepsis Alliance and World Sepsis Day have raised awareness and promote sepsis prevention and early detection, which are critical to improve outcomes [5,6].
The diagnosis of sepsis is based on clinical and laboratory parameters that indicate the presence of infection and organ dysfunction. The most specific test for diagnosing sepsis include blood cultures, used to confirm the diagnosis of sepsis and identify the source of infection, but its sensitivity is quite low, and results typically take around 2 days to become available after sample collection [7]. Due to this time lag, alternative circulating biomarkers with higher sensitivity and faster turnaround for results are commonly used. Currently, the primary biological markers employed in sepsis diagnosis are procalcitonin (PCT) and C-reactive protein (CRP), that can reflect the severity of the infection and help guide treatment decisions [8,9]. However, CRP has a significant drawback as its specificity is limited; it can also be elevated in various other inflammation-related conditions [10]. On the other hand, PCT is considered one of the most specific markers for bacterial sepsis, and its concentration is closely associated with disease severity, mortality, and organ failure [10]. Nevertheless, PCT can produce false negative results in patients with invasive fungal infections, and it may be elevated in noninfectious conditions; furthermore, the cost of PCT testing is relatively high, making it less desirable for routine use [10]. Therefore, at present, serial PCT testing is primarily recommended for monitoring purposes and guiding appropriate antibiotic treatment rather than serving as an initial diagnostic tool [8].
Laboratory medicine holds a pivotal role in sepsis diagnosis, continuously exploring novel biomarkers to enhance diagnostic capabilities. Among these prospects, CD64, also referred to as Fc receptor 1, stands out as a rising biomarker. This high-affinity receptor on neutrophils binds to the Fc portion of the Immunoglobulin-G heavy chain. Neutrophil CD64 orchestrates functions within both innate and adaptive immune responses and its levels notably surge within 4-6 hours in response to infection-induced proinflammatory cytokines. The expression of CD64 emerges as a promising candidate biomarker for sepsis [11].
Moreover, several studies have shown that leukocyte morphological parameters play an important role in the diagnosis of sepsis [12]. One example is monocyte distribution width (MDW), a new laboratory parameter obtained from a complete blood count (CBC) that measures morphological and dimensional variability of monocytes in the blood [13,14]. MDW is a promising tool for the diagnosis and management of sepsis, and its use in clinical practice may improve outcomes in sepsis patients [15,16]. However, the MDW parameter is only calculated by Beckman Coulter’s (Miami, Florida, USA) new generation hematology analyzers, which is a potential limitation to its wide application [17].
Several other research-use-only (RUO) cell parameters may be obtained from CBC results, which are inexpensive and easily accessible. In particular, BC-6800 Plus (Mindray, China) offers high-resolution, three-dimensional SF cube technology that provides highly detailed information on blood cell morphology in terms of leukocyte volume, cytoplasmic and nuclear complexity, nucleic acid (DNA and RNA) content. This information is automatically converted into quantitative RUO parameters describing cell morphology: NeuX, NeuY, NeuZ, MonX, MonY, MonZ, LymX, LymY, LymZ.
The aim of the present study was to evaluate the diagnostic value of RUO blood cell parameters, provided by the BC 6800 Plus Analyzer, for the early identification of sepsis in the Intensive Care Unit (ICU).
2. Materials and methods
2.1. Study design
A retrospective observational study was conducted at the University Hospital (AOU) “Maggiore della Carità”, Novara, Italy. The study protocol was approved by the Ethics Committee of the University Hospital “Maggiore della Carità” (CE 127/2023), Novara, Italy and performed in accordance with the current revision of the Helsinki Declaration.
2.2. Study population
Laboratory data from day 1, corresponding to ICU admission, were analyzed. Data were extracted from the Laboratory Information System (LIS) into an Excel database using TD Synergy software (Siemens Healthcare) and LabExpert software (Mindray) and were anonymized.
We reviewed the electronic medical records of 223 patients admitted to the ICU between July 2021 and October 2022, who were subsequently diagnosed with sepsis. The criteria for sepsis diagnosis were based on the Third International Consensus Definitions of Sepsis and Septic Shock (Sepsis-3 Criteria) [1]. The consensus recommends a sepsis diagnosis with suspected infection and a Sequential Organ Failure Assessment (SOFA) score (used to determine level of organ dysfunction and mortality risk in ICU) of 2 or higher [18]. Only patients with suspected infection and a SOFA score ≥ 2 but negative for SARS-CoV-2 were selected.
A control group of 104 individuals consecutively admitted to the ICU for a traumatic and noninfectious event was also included in the study. Exclusion Criteria were missing quantitative RUO parameters; underlying hemato-oncological disease and positivity for SARS-CoV-2.
Demographic characteristics, such as age and sex, and SOFA score at ICU admission were collected for all patients. As components of SOFA score, Glasgow Coma Scale (GCS) [19], the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2), mean arterial pressure (MAP), blood creatinine, bilirubin levels and blood culture test results were recorded. Furthermore, blood lactates, ICU and hospital length of stay (LOS) and mortality were evaluated.
Then, a third group of 56 patients with urinary tract infection admitted to the Internal Medicine department was subsequently recruited in order to validate diagnostic model of sepsis obtained from the statistical analysis of the first two groups of patients. To do so, we reviewed all the clinical records of the patients admitted to the ward from 1st July 2021 to 1st July 2023 and we selected all those with a documented respiratory or urinary infection and a SOFA Score < 2. Exclusion Criteria were missing quantitative RUO parameters, underlying hemato-oncological disease and positivity for SARS-CoV-2.
2.3. Data Collection
CBC was performed on EDTA-K2 anticoagulant whole blood samples using the BC-6800 Plus Hematology Analyzer (Mindray, China), CRP was measured on lithium heparin anticoagulant blood samples using the ADVIA 1800 Clinical Chemistry System (Siemens Healthineers, Germany), and PCT was determined on lithium heparin anticoagulant blood samples using the ADVIA Centaur® XP Immunoassay System (Siemens Healthiness, Germany).
The quantitative RUO parameters NeuX, NeuY, NeuZ, MonX, MonY, MonZ, LymX, LymY, LymZ provided by the BC 6800 Plus Analyzer were assessed. These parameters are numerical data indicating the center of gravity position of the measured events. They are related to cell morphology (volume, granularity, and complexity of each cell) and are useful for evaluating and characterizing the cells in a blood sample [20,21]. The stability of the cellular RUO position parameters was first tested on a group of 80 consecutive samples taken completely at random from routine procedures. All samples were processed within two hours of blood collection. The experimental data (study design: 80 samples, stored at room temperature or at 4°C and measured a t0, t1=2hs, t2=8hs, t3=24hs) show that all evaluated quantitative RUO parameters are stable up to 2 hours after blood collection (deviations<4%). Storing the sample at 4°C did not provide any advantage. In addition, the repeatability of the cellular RUO parameters was tested by analyzing 50 samples with 3 different modules of the BC 6800 Plus Analyzer. The repeatability for all cellular parameters was < 4% (data not shown).
2.4. Statistical analysis
Statistical analyses were performed by SPSS statistical software v.17.0 (SPSS Inc., Chicago, IL, USA) and R Language v.4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). Normality distribution was assessed preliminarily by q-q plot and Shapiro–Wilk tests. Differences between groups for continuous variables or categorical were estimated by Mann–Whitney U test and Fisher’s exact test, respectively. Diagnostic accuracy for the prediction of sepsis was evaluated by a Receiver Operating Characteristic (ROC) curve analysis and reported as the Area Under the Curve (AUC) and 95% confidence interval. Differences between the AUCs were evaluated by the DeLong method. Differences in mortality were evaluated by Log Rank test.
The association between predictors and sepsis was examined using univariate and multivariate logistic regression. The association between predictors and time to mortality within ICU or hospital was evaluated by univariate and multivariate Cox regression.
3. Results
A total of 327 electronic records were reviewed, of which 223 patients with sepsis (60% males, 40% females), while 104 patients (68% males, 32% females) were not septic and were used as controls. Population characteristics are shown in Table 1. Overall patients had a median age of 70 (57 – 77) years, with an average SOFA score of 6 (4 – 8) and a Glasgow Coma Score (GCS) at ICU admission of 15 (9 – 15). Age, mean arterial pressure (MAP), and the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2) on admission differed significantly between patients with and without sepsis (71 (60 – 78) vs 64 (52 – 75) years, 79 (65 – 93) vs 90 (71 – 107) mmHg, and 175 (116 – 274) vs 303 (174 – 403) mmHg, respectively, p <0.05), whereas median SOFA score was not dissimilar between the two groups. Furthermore, levels of creatinine (114.95 (61.89-203.37) vs 61.89 (53.05-88.42) μmol/L, p<0.05) and lactate (1.6 (1.0 – 3.1) vs 1.4 (0.9 – 2.6) mmol/L) levels were higher in the sepsis group compared to controls, while no significant differences were found in bilirubin concentrations. Bacteremia was suspected in 81% of the patients. Blood cultures resulted positive in the 36% of the cases. Coagulase-negative Staphylococcus were found in 18 patients. Lastly, ICU and hospital length of stay differ between the two groups (respectively, p=0.05 and p=0.011), and mortality was significantly higher in sepsis patients than in controls (ICU mortality 34% vs 20%, Log Rank test p=0.002; hospital mortality 45% vs 21%, Log Rank test p=0.012).
Data are presented as number and percentage or median and IQR. SOFA: Sequential Organ Failure Assessment; PaO2/FiO2: ratio of arterial oxygen partial pressure to fractional inspired oxygen; PLT: platelets; GCS, Glasgow coma score; Lac: lactate; MAP: mean arterial pressure; ICU, intensive care unit; LOS, length of stay. Bold values denote statistical significance at the p<0.05 level.
Initially, only blood counts were analyzed to assess the ability of blood count parameters alone, both standard and RUO, for early diagnosis of sepsis. On admission, many hematological parameters differed significantly between patients with and without sepsis, as detailed in Table 2: hemoglobin (Hb), Red Cell Distribution Width (RDW), White Blood Cells count (WBC), lymphocyte count (LY#), monocyte count (MO#), neutrophil-to-monocyte ratio (NMR), lymphocyte-to-monocyte ratio (LMR), NeuX, NeuY, NeuZ, LymX, MonX, MonY, MonZ, CRP and PCT.
In univariate logistic regression analysis, age, Hb, RDW, MO#, NMR, NeuX, NeuY, NeuZ, LymX, MonX, MonY, MonZ were associated with sepsis (Table 3). However, in multivariate analysis, only RDW, NeuX, NeuY, NeuZ, MonX and MonZ were found to be independent predictors of sepsis. The multivariate model correctly classified up to 85% of cases (false negative FN 7%, false positive FP 7%). The AUC for sepsis of the multivariate model was 0.92 (95%CI 0.89-0.95) (Figure 1).
In addition, CRP and PCT were significantly elevated on admission in patients with sepsis compared with patients without sepsis (Table 2). The AUCs for sepsis of CRP and PCT were 0.83 (95%CI 0.79-0.88; p<0.001) and 0.78 (95%CI 0.73-0.84; p<0.001), respectively (Table 4). However, the AUC for sepsis of our multivariate model was significantly higher than the AUCs of both CRP and PCT (Bonferroni’s correction, both p<0.001). No difference was instead evident between CRP and PCT. Finally, CRP was added to the univariate and multivariate analysis: the new model correctly classified up to 88% of cases (FN 7%, FP 5%).
Predictors of mortality within ICU and within hospital were evaluated by univariate and multivariate Cox regression. As detailed in Table 5, at the univariate Cox regression analysis, age, RDW, NeuX, NeuY, LymY, LymZ, MonX were associated to mortality within ICU, whereas age, RDW, NLR, NeuX, NeuY, LymY, LymZ, MonX and MonY were associated to mortality within Hospital. At the multivariate Cox regression analysis, age, NeuY, LymY and MonX were independent predictors of shorter time to mortality within ICU, whereas age, NeuY, LymY and MonY were independent predictors of shorter time to mortality within Hospital (Table 5).
Finally, the third group of 56 patients with localized infection but not sepsis (SOFA Score<2), was compared to sepsis group, and it was comparable for sex distribution (M:F 27:29 vs. 134:89; p=0.13) but, as expected, significantly older (82 (76-90) vs. 71 (60-78) p<0.001).
Many hematological parameters of patients with respiratory or urinary tract infection differed significantly from those of patients with sepsis, as shown in Table 6. In univariate analysis, age, Hb, MO#, NLR, NMR, PLT, NeuX, NeuY, MonX, MonY and CRP were found to be associated with sepsis (Table 7). As detailed in Table 7, in multivariate analysis, without and with CRP, only age, Hb, NMR, PLT, NeuY and MonY were found to be independent predictors of sepsis. The multivariate model correctly classified up to 89% of cases (false negative FN 4%, false positive FP 7%). The AUC for sepsis of the multivariate model was 0.91 (95%CI 0.86-0.95) (Figure 2). In addition, CRP and PCT were significantly elevated on admission in patients with sepsis compared with patients without sepsis (Table 6). The AUCs for sepsis of CRP and PCT were 0.62 (95%CI 0.54-0.69; p=0.008) and 0.69 (95%CI 0.59-0.78; p<0.001), respectively (Figure 2). However, the AUC for sepsis of our multivariate model was significantly higher than the AUCs of both CRP and PCT (Bonferroni’s correction, both p<0.001). No difference was instead evident between CRP and PCT. Finally, CRP was added to the univariate and multivariate analysis: the new model correctly classified up to 89% of cases (FN 4%, FP 7%).
4. Discussion
In recent years, several studies have emphasized the central role of complete blood count (CBC) analysis and morphological parameters in the early diagnosis of sepsis. Buoro et al. emphasized that parameters such as the immature platelet fraction (IPF#) and the reticulocyte ratio (RET %) are risk predictors for the development of sepsis in critically ill patients and allow early patient management before clinically visible systemic infections occur [24]. Pelagalli et al. presented a study showing that leukocyte differential count and several parameters related to cell population data (CPD) determined with the Mindray BC-6800 Plus analyzer have predictive value for sepsis screening. This suggests that blood count and CPD can be used as plausible markers for early sepsis diagnosis in emergency situations, facilitating timely clinical intervention [25].
The present study focused on the analysis of several standard and RUO cellular morphological parameters derived from patient CBC results, accessible and cost-effective for all laboratories, not only for users of the BC 6800 plus. The multivariate analysis specifically identified NeuX, NeuY, NeuZ, MonX, MonZ and RDW as independent predictors of sepsis. Combining these parameters in a multivariate model showed strong predictive power and correctly classified up to 85% of cases. NeuX, NeuY, NeuZ, MonX, MonZ and RDW proved to be useful parameters for early diagnosis of sepsis and performed better than using PCT and/or CRP alone. The multivariate analysis model was improved with the addition of CRP and was able to correctly classify up to 88% of cases. PCT was not included in the statistical model because it is a costly test with a high rate of inappropriate queries and should be used primarily to guide antibiotic therapy. In addition, NeuY, MonX and LymY were found to be independent predictors of shorter time to mortality within ICU/hospital, which is also useful for clinicians in predicting the outcome of sepsis early. The RUO parameters could therefore also be useful in determining appropriate therapeutic strategies for septic patients.
The importance of neutrophil and monocyte morphological parameters in sepsis has already been underlined in previous studies [21,26,27]. Our study confirmed in a Caucasian population the data presented by Zhang et al. who showed that the parameters NeuX, NeuY, MonX and MonY determined by the BC 6800 Plus analyzer (Mindray) were significantly increased in the sepsis group compared with the bacterial infection group, indicating their potential usefulness in sepsis diagnosis and in differentiating bacterial infections. In addition, our study confirmed that the morphologic parameters, especially NEU-Y, have higher diagnostic predictive power for sepsis compared to CRP [21]. Under the action of various bacterial and viral stimuli, monocytes undergo morphological and structural changes, which reflect their activation state and allow them to perform multiple biological functions, modulating the immune response and the resolution and/or progression of the disease [28].
In sepsis, the monocytes change their size, undergo an amoeboid transformation and increase CD16 expression [16]. Monocyte activation is measured by the MonZ parameter for size and the MonX parameter for structural changes in the blood count. Accurate measurement of these morphologic changes in septic patients, in addition to routine CBC data, is undoubtedly an added value and clinically relevant, especially when monitoring other biomarkers is costly, such as in resource-limited settings or in neonatal care [29].
Similarly, neutrophil granulocytes also play a key role in the immune response, which is monitored by Neu-X, Neu-Y and Neu-Z. These cells primarily combat pathogens via phagocytosis, engulfing and eradicating microorganisms to clear infections [30]. In sepsis neutrophil function can impair, prompting dysregulation and an inflammatory cytokine storm. Overactive neutrophils release excess pro-inflammatory molecules that damage tissues and organs [31]. Neutrophils form NETs in sepsis that immobilize pathogens, but this can impede blood flow and increase inflammation [32]. Therefore, during sepsis neutrophils undergo a whole range of morphological and functional changes, which can be well described and accurately measured by neutrophil morphological parameters. In particular, the present work suggests that the inclusion of the research parameters NeuX, NeuY, NeuZ together with MonX, MonZ can improve the accuracy of sepsis diagnosis.
Finally, in our study, the morphological parameter of red blood cells, RDW, also proved to be an early independent predictor of sepsis risk in ICU patients. It has already been established that there is a correlation between the onset and development of sepsis and the level of RDW and that RDW is an important predictor of death in patients with sepsis [33].
In recent years, RDW has proven to be a valuable diagnostic index, not only for differentiating thalassemias and microcytic iron deficiency anemias, but also for assessing various non-hematologic diseases, including sepsis [34]. RDW is closely related to inflammatory markers such as CRP. It has been postulated that inflammation may impair the maturation process of red blood cells, leading to accelerated entry of immature erythrocytes into the circulation [35]. RDW is influenced by the lifespan of erythrocytes. Consequently, RDW could be an indicator of a chronic inflammatory response, in contrast to conventional markers like CRP that primarily reflect an ongoing, acute inflammatory reaction [34]. In addition, an increased RDW value in sepsis patients could indicate the presence of organ dysfunction and consequently a poorer prognosis [34].
Due to its retrospective nature, our study has a limitation that needs to be discussed. Patients with confirmed sepsis were compared with an ICU population affected by non-septic disease, whereas a more appropriate control group would have consisted of patients with suspected but unproven sepsis. Such categorization is often not possible when retrospectively recruiting patients by analyzing electronic records. Furthermore, according to clinical guidelines [36], ICU patients with a strong suspicion of sepsis are treated as septic regardless of confirmation of infection. To overcome this limitation, a third control group with localized infection but without sepsis was recruited. In the univariate logistic regression analysis, the cellular RUO position parameters NeuX, NeuY, MonX and MonY were associated with sepsis. The multivariate analysis specifically identified NeuY and MonY as independent predictors of sepsis, confirming the important role of RUO parameters in the early diagnosis of sepsis. The combination of these parameters in a multivariate model showed strong predictive power and correctly classified up to 89% of cases.
In conclusion, the integration of morphologic research parameters from automated blood cell analyzers together with traditional clinical signs, the SOFA score and established biomarkers could improve sepsis diagnosis and treatment, facilitate rapid intervention and potentially lead to better patient outcomes. RUO cell parameters can be accurately measured with any new generation hematology analyzer and provide additional information to conventionally reported blood count parameters. Importantly, this additional analysis does not incur additional costs compared to a normal blood count, making RUO testing cost-effective and accessible to all laboratories, including non-specialized spokes laboratories. Consequently, the RUO parameters could be used worldwide for the early diagnosis of sepsis at no additional cost.
Despite the limitations discussed, the data presented emphasize the diagnostic potential of the integrated use of RUO cell parameters, which accurately reflect the morphological and functional changes of leukocytes and erythrocytes during sepsis and beyond, in combination with the parameters already recorded in the complete blood count. The use of morphological RUO parameters is very promising for clinical practice and their future use could prove crucial for the development of diagnostic algorithms for different pathologies thanks to the combined use of Artificial Intelligence and Machine Learning. However, further validation of the available data in other cohorts, in larger studies and in a prospective study is needed. Future studies should focus on investigating the diagnostic utility and potential clinical applications of morphologic parameters to improve sepsis outcomes and patient care.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Molloy, E.J.; Bearer, C.F. Paediatric and neonatal sepsis and inflammation. Pediatr. Res. 2022, 91, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Markwart, R.; Saito, H.; Harder, T.; Tomczyk, S.; Cassini, A.; Fleischmann-Struzek, C.; Reichert, F.; Eckmanns, T.; Allegranzi, B. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1536–1551. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet. 2020, 395, 200–211. [Google Scholar] [CrossRef]
- Schlapbach, L.J.; Kissoon, N.; Alhawsawi, A.; Aljuaid, M.H.; Daniels, R.; Gorordo-Delsol, L.A.; Machado, F.; Malik, I.; Nsutebu, E.F.; Finfer, S.; et al. World Sepsis Day: a global agenda to target a leading cause of morbidity and mortality. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 319, L518–L522. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, K.; Daniels, R.; Kissoon, N.; Machado, F.R.; Schachter, R.D.; Finfer, S. Recognizing Sepsis as a Global Health Priority - A WHO Resolution. NEJM 2017, 377, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.P.; Stenstrom, R.; Paquette, K.; Stabler, S.N.; Akhter, M.; Davidson, A.C.; Gavric, M.; Lawandi, A.; Jinah, R.; Saeed, Z.; et al. Blood Culture Results Before and After Antimicrobial Administration in Patients With Severe Manifestations of Sepsis: A Diagnostic Study. Ann. Intern. Med. 2019, 171, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, P.; Coelho, L.; Dal-Pizzol, F.; Ferrer, R.; Huttner, A.; Conway Morris, A.; Nobre, V.; Ramirez, P.; Rouze, A.; Salluh, J.; et al. How to use biomarkers of infection or sepsis at the bedside: guide to clinicians. Intensive Care Med. 2023, 49, 142–153. [Google Scholar] [CrossRef]
- Pierrakos, C.; Velissaris, D.; Bisdorff, M.; Marshall, J.C.; Vincent, J.L. Biomarkers of sepsis: time for a reappraisal. Crit. Care 2020, 24, 287. [Google Scholar] [CrossRef]
- Hassan, J.; Khan, S.; Zahra, R.; Razaq, A.; Zain, A.; Razaq, L.; Razaq, M. Role of Procalcitonin and C-reactive Protein as Predictors of Sepsis and in Managing Sepsis in Postoperative Patients: A Systematic Review. Cureus 2022, 14, e31067. [Google Scholar] [CrossRef]
- Patnaik, R.; Azim, A.; Agarwal, V. Neutrophil CD64 a Diagnostic and Prognostic Marker of Sepsis in Adult Critically Ill Patients: A Brief Review. Indian J. Crit. Care Med. 2020, 24, 1242–1250. [Google Scholar]
- Urrechaga, E.; Bóveda, O.; Aguirre, U. Role of leucocytes cell population data in the early detection of sepsis. J. Clin. Pathol. 2018, 71, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Ciaccio, A.M.; Agnello, L.; Sasso, B.L.; Giglio, R.V.; Iacona, A.; Gambino, C.M.; Scazzone, C.; Tuttolomondo, A.; Ciaccio, M. Monocyte Distribution Width (MDW) as a biomarker of sepsis: An evidenced-based laboratory medicine approach. Clin. Chim. Acta 2023, 540, 117214. [Google Scholar] [CrossRef] [PubMed]
- Agnello, L.; Vidali, M.; Lo Sasso, B.; Giglio, R.V.; Gambino, C.M.; Scazzone, C.; Ciaccio, A.M.; Bivona, G.; Ciaccio, M. Monocyte distribution width (MDW) as a screening tool for early detecting sepsis: a systematic review and meta-analysis. CCLM 2022, 60, 786–792. [Google Scholar] [CrossRef]
- Crouser, E.D.; Parrillo, J.E.; Seymour, C.; Angus, D.C.; Bicking, K.; Tejidor, L.; Magari, R.; Careaga, D.; Williams, J.; Closser, D.R.; et al. Improved Early Detection of Sepsis in the ED With a Novel Monocyte Distribution Width Biomarker. Chest 2017, 152, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Crouser, E.D.; Parrillo, J.E.; Seymour, C.W.; Angus, D.C.; Bicking, K.; Esguerra, V.G.; Peck-Palmer, O.M.; Magari, R.T.; Julian, M.W.; Kleven, J.M.; et al. Monocyte Distribution Width: A Novel Indicator of Sepsis-2 and Sepsis-3 in High-Risk Emergency Department Patients. Crit. Care Med. 2019, 47, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Polilli, E.; Sozio, F.; Frattari, A.; Persichitti, L.; Sensi, M.; Posata, R.; Di Gregorio, M.; Sciacca, A.; Flacco, M.E.; Manzoli, L.; et al. Comparison of Monocyte Distribution Width (MDW) and Procalcitonin for early recognition of sepsis. PLoS ONE 2020, 15, e0227300. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Sun, P.; Li, N.; Zhang, S.; Liu, S.; Zhang, H.; Yue, B. Combination of NeuX and NeuZ can predict neutrophil dysplasia features of myelodysplastic neoplasms in peripheral blood. Int. J. Lab. Hematol. 2023, 45, 522–527. [Google Scholar] [CrossRef]
- Zhang, W.; Zhang, Z.; Pan, S.; Li, J.; Yang, Y.; Qi, H.; Xie, J.; Qu, J. The clinical value of hematological neutrophil and monocyte parameters in the diagnosis and identification of sepsis, Ann. Transl. Med. 2021, 9, 1680. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Wang, Y.; Xie, M.; Qiu, S.; Zhou, J. Elevated neutrophil - to - monocyte ratio as a prognostic marker for poor outcomes in neonatal sepsis. Heliyon 2022, 8, e11181. [Google Scholar] [CrossRef] [PubMed]
- Piotrowski, D.; Sączewska-Piotrowska, A.; Jaroszewicz, J.; Boroń-Kaczmarska, A. Lymphocyte-To-Monocyte Ratio as the Best Simple Predictor of Bacterial Infection in Patients with Liver Cirrhosis. IJERPH 2020, 17, 1727. [Google Scholar] [CrossRef] [PubMed]
- Buoro, S.; Manenti, B.; Seghezzi, M.; Dominoni, P.; Barbui, T.; Ghirardi, A.; Carobbio, A.; Marchesi, G.; Riva, I.; Nasi, A.; et al. Innovative haematological parameters for early diagnosis of sepsis in adult patients admitted in intensive care unit. J. Clin. Pathol. 2018, 71, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Pelagalli, M.; Giovannelli, A.; Calabrese, C.; Sarubbi, S.; Minieri, M.; Nuccetelli, M.; et al. Leucocyte differential count and morphometric parameters by Mindray BC-6800 Plus: a possible predictive tool for screening of sepsis. Biochimica Clinica 2023, 47, 141–150. [Google Scholar]
- Arora, P.; Gupta, P.K.; Lingaiah, R.; Mukhopadhyay, A.K. Volume, conductivity, and scatter parameters of leukocytes as early markers of sepsis and treatment response. J. Lab. Physicians 2019, 11, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Mammen, J.; Choudhuri, J.; Paul, J.; Sudarsan, T.I.; Josephine, T.; Mahasampath, G.; Jeyaseelan, V.; Nair, S.C.; Peter, J.V. Cytomorphometric Neutrophil and Monocyte Markers May Strengthen the Diagnosis of Sepsis. J. Intensive Care Med. 2018, 33, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Pamer, E.G. Monocyte recruitment during infection and inflammation. Nat. Rev. Immunol. 2011, 11, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, L.; Luo, J. Diagnostic and Prognostic Value of Monocyte Distribution Width in Sepsis. J. Inflamm. Res. 2022, 15, 4107–4117. [Google Scholar] [CrossRef]
- Jones, H.R.; Robb, C.T.; Perretti, M.; Rossi, A.G. The role of neutrophils in inflammation resolution. Semin. Immunol. 2016, 28, 137–145. [Google Scholar] [CrossRef]
- Zhu, C.L.; Wang, Y.; Liu, Q.; Li, H.R.; Yu, C.M.; Li, P.; Deng, X.M.; Wang, J.F. Dysregulation of neutrophil death in sepsis. Front. immunol. 2022, 13, 963955. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhang, H.; Qu, M.; Nan, K.; Cao, H.; Cata, J.P.; Chen, W.; Miao, C. Review: The Emerging Role of Neutrophil Extracellular Traps in Sepsis and Sepsis-Associated Thrombosis. Front. Cell. Infect. Microbiol. 2021, 11, 653228. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Zhang, L.; Tang, X.; Tang, Y. The Value of Neutrophil/Lymphocyte Ratio Combined with Red Blood Cell Distribution Width in Evaluating the Prognosis of Emergency Patients with Sepsis. Emerg. Med. Int. 2022, 1673572. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.D.; Lippi, G.; Montagnana, M. Diagnostic and prognostic value of red blood cell distribution width in sepsis: A narrative review. Clin. Biochem. 2020, 77, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Cervellin, G.; Meschi, T.; Lippi, G. The role of red blood cell distribution width in cardiovascular and thrombotic disorders. CCLM 2011, 50, 635–641. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
Figure 1.
ROC curve analysis for the comparison between multivariate model, CRP and PCT in sepsis prediction. CRP, C-reactive protein; PCT, procalcitonin.
Figure 1.
ROC curve analysis for the comparison between multivariate model, CRP and PCT in sepsis prediction. CRP, C-reactive protein; PCT, procalcitonin.
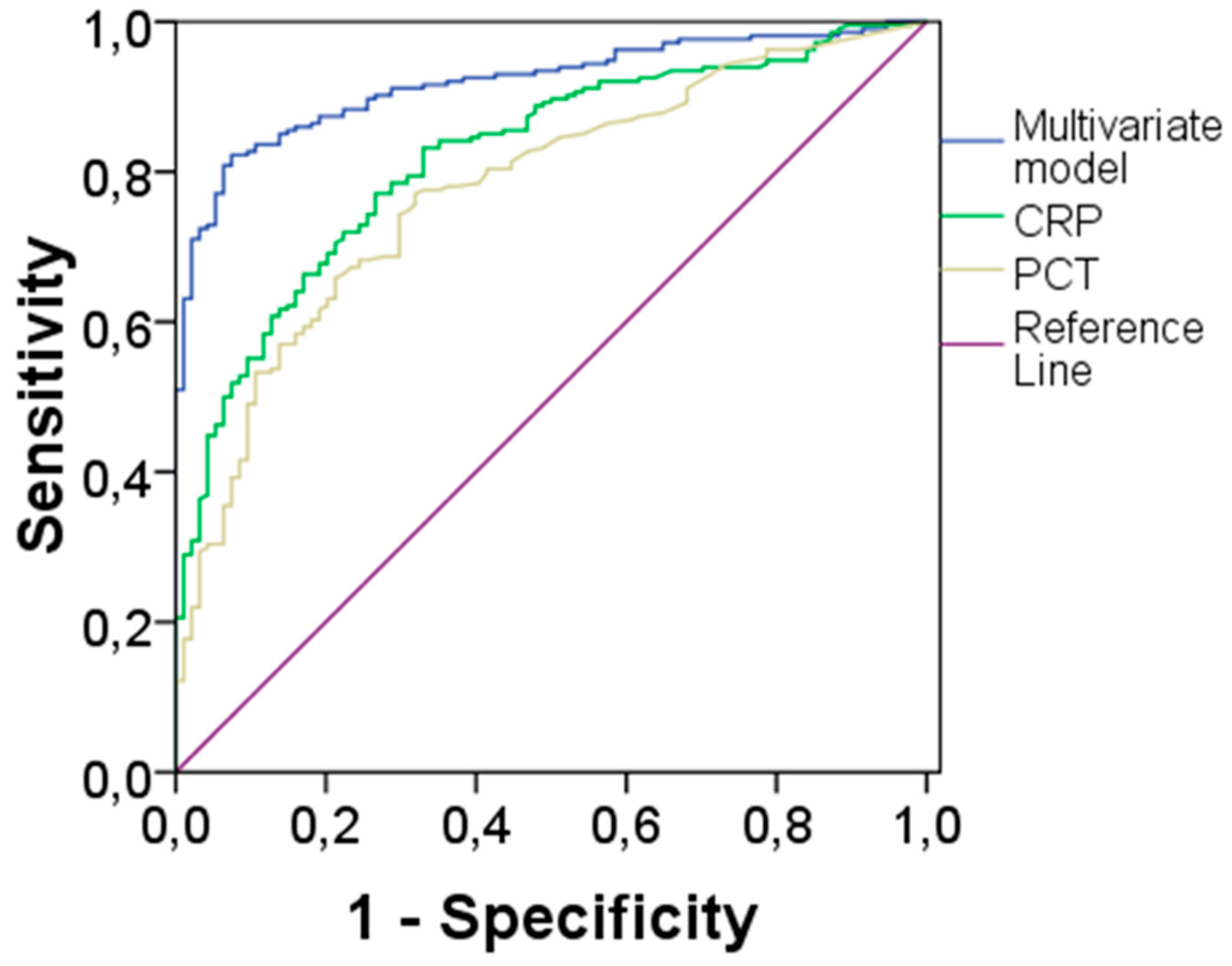
Figure 2.
ROC curve analysis for the comparison between multivariate model, CRP and PCT in sepsis prediction. CRP, C-reactive protein; PCT, procalcitonin.
Figure 2.
ROC curve analysis for the comparison between multivariate model, CRP and PCT in sepsis prediction. CRP, C-reactive protein; PCT, procalcitonin.
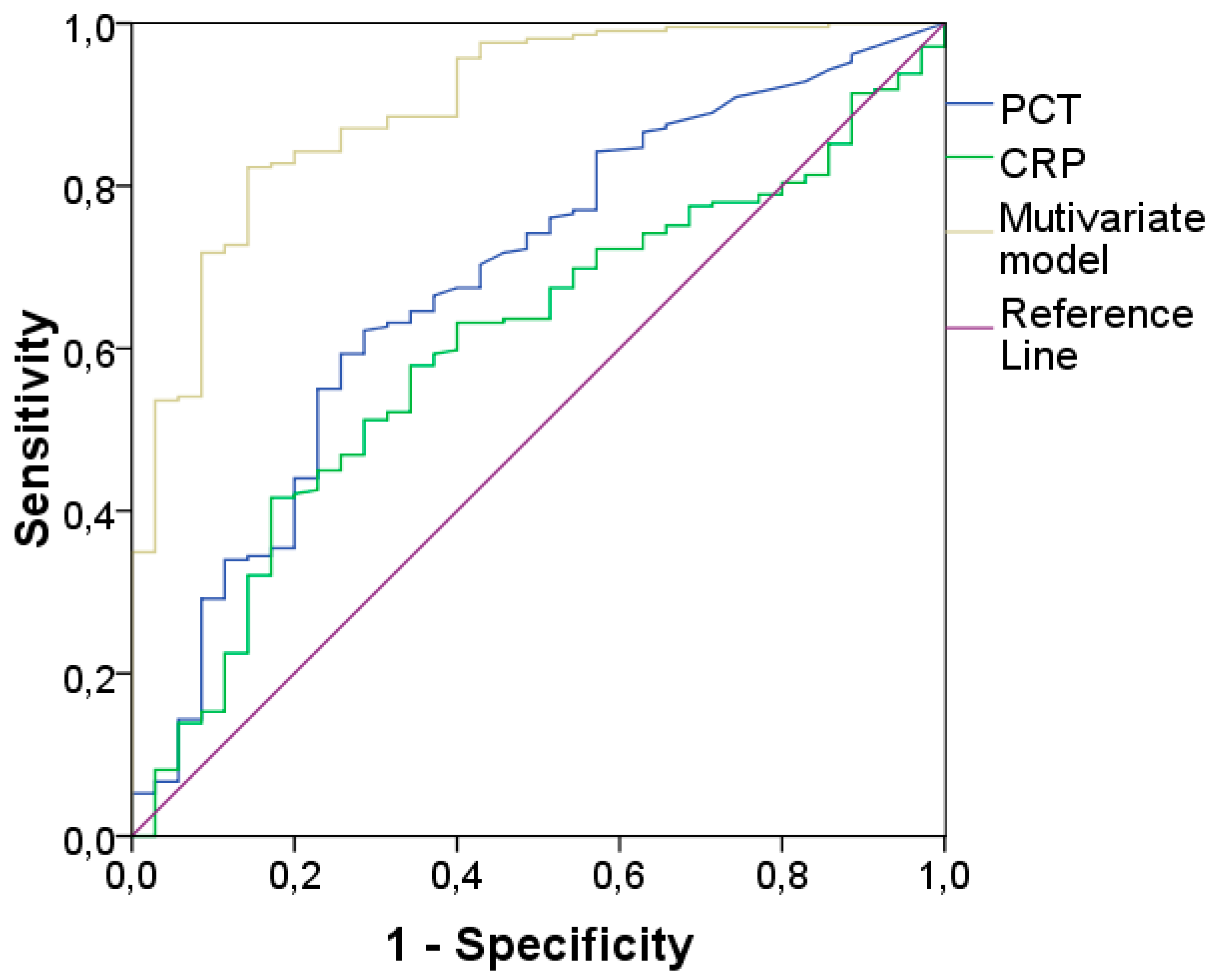

Table 1.
Patient demographic and clinical characteristics.
| Demographic and clinical characteristics | All patients n = 327 |
Sepsis patients n = 223 |
Non-sepsis patients n = 104 |
|---|---|---|---|
| Age, years | 70 (57 – 77) | 71 (60 – 78) | 64 (52 – 75) |
|
Male, n (%) Female, n (%) |
205 (63) 122 (37) |
134 (60) 89 (40) |
71 (68) 33 (32) |
| SOFA SCORE | 6 (4 – 8) | 6 (4 – 8) | 6 (4 – 7) |
| PaO2/FiO2, mmHg | 209 (130 – 332) | 175 (116 – 274) | 303 (174 – 403) |
| PLT, x109/L | 195 (131 – 259) | 190 (116 – 261) | 206 (163 – 255) |
| MAP, mmHg | 81 (67 – 97) | 79 (65 – 93) | 90 (71 – 107) |
| Bilirubin, μmol/L | 13.68 (10.26-23.94) | 15.39 (10.26-25.65) | 13.68 (8.55-20.52) |
| Creatinine, μmol/L | 87.54 (61.89-150.31) | 114.95 (61.89-203.37) | 61.89 (53.05-88.42) |
| GCS | 15 (9 – 15) | 15 (14 – 15) | 8 (5 – 14) |
| Lac, mmol/L | 1.6 (1 - 3) | 1.6 (1.0 – 3.1) | 1.4 (0.9 – 2.6) |
| ICU LOS, d | 3 (1 – 9) | 3 (1 – 7) | 5.5 (1.0 – 12) |
| Hospital LOS, d | 17 (8 – 32) | 19 (10 – 33) | 11 (6 – 28) |
| ICU mortality, n (%) | 98 (30) | 77 (34) | 21 (20) |
| Hospital mortality, n (%) | 122 (37) | 100 (45) | 22 (21) |
Table 2.
Hematologic and biochemical data of the study population divided in sepsis and without sepsis groups.
Table 2.
Hematologic and biochemical data of the study population divided in sepsis and without sepsis groups.
| PREDICTOR | Without Sepsis (n=104) | With Sepsis (n=223) | p-Value |
|---|---|---|---|
| Hb, g/L | 127 (107-142) | 108 (90-128) | <0.001 |
| RDW, % | 13.4 (12.7-14.3) | 14.8 (13.8-16.6) | <0.001 |
| WBC,x109/L | 12.7 (10.1-16.1) | 11.2 (6.8-15.8) | 0.022 |
| NE#,x109/L | 11.0 (8.1-14.1) | 9.6 (5.5-14.0) | 0.061 |
| LY#,x109/L | 0.8 (0.5-1.3) | 0.6 (0.4-1.1) | 0.002 |
| MO#,x109/L | 0.6 (0.4-0.9) | 0.4 (0.2-0.7) | <0.001 |
| NLR | 13.6 (6.6-22.5) | 13.4 (6.9-24.5) | 0.644 |
| NMR | 16.8 (12.2-24.3) | 21.5 (13.3-36.2) | <0.001 |
| LMR | 1.3 (0.8-2.1 | 1.5 (0.9-2.8) | 0.030 |
| PLT,x109/L | 206 (163-255) | 190 (116-261) | 0.099 |
| NeuX | 361 (345-389) | 408 (371-446) | <0.001 |
| NeuY | 479 (455-500) | 541 (495-607) | <0.001 |
| NeuZ | 1858 (1793-1910) | 1792 (1712-1874) | <0.001 |
| LymX | 94 (90-99) | 97 (91-104) | 0.002 |
| LymY | 765 (736-805) | 775 (728-833) | 0.203 |
| LymZ | 962 (944-978) | 954 (931-982) | 0.484 |
| MonX | 208 (202-218) | 224 (211-245) | <0.001 |
| MonY | 1046 (996-1080) | 1144 (1065-1225) | <0.001 |
| MonZ | 1312 (1292-1334) | 1348 (1303-1408) | <0.001 |
| CRP, mg/L | 20.6 (8.6-54.3) | 140.6 (64.8-207.2) | <0.001 |
| PCT, ng/mL | 0.17 (0.08-0.54) | 2.67 (0.36-19.60) | <0.001 |
Hb, hemoglobin; RDW, red distribution width; WBC, white blood cells; NE#, absolute number of neutrophils; LY#, absolute number of lymphocytes; MO#, absolute number of monocytes; NLR, neutrophils/lymphocytes ratio; NMR, neutrophils/monocytes ratio; LMR, lymphocytes/monocytes ratio; PLT, platelets; Neu, neutrophils; Lym, lymphocytes; Mon, monocytes; CRP, C-reactive protein; PCT, procalcitonin. Statistical significance was calculated according to nonparametric Mann-Whitney test and Fisher’s exact test. Bold values denote statistical significance at the p<0.05 level.
Table 3.
Univariate and multivariate logistic regression analysis for sepsis (without and with CRP).
Table 3.
Univariate and multivariate logistic regression analysis for sepsis (without and with CRP).
| PREDICTOR | UNIVARIATE LR | MULTIVARIATE LR without CRP | MULTIVARIATE LR with CRP |
|---|---|---|---|
| Age | <0.001 | 0.608 | 0.579 |
| Sex | 0.155 | ||
| Hb | <0.001 | 0.797 | 0.574 |
| RDW | <0.001 | 0.005 | 0.002 |
| WBC | 0.490 | ||
| NE# | 0.749 | ||
| LY# | 0.397 | ||
| MO# | <0.001 | 0.125 | 0.026 |
| NLR | 0.152 | ||
| NMR | 0.003 | 0.103 | 0.142 |
| LMR | 0.295 | ||
| PLT | 0.915 | ||
| NeuX | <0.001 | <0.001 | 0.001 |
| NeuY | <0.001 | <0.001 | 0.006 |
| NeuZ | <0.001 | <0.001 | <0.001 |
| LymX | 0.001 | 0.648 | 0.719 |
| LymY | 0.072 | ||
| LymZ | 0.426 | ||
| MonX | <0.001 | 0.040 | 0.229 |
| MonY | <0.001 | 0.638 | 0.584 |
| MonZ | <0.001 | 0.031 | 0.005 |
| CRP | <0.001 | <0.001 |
Hb, hemoglobin; RDW, red distribution width; WBC, white blood cells; NE#, absolute number of neutrophils; LY#, absolute number of lymphocytes; MO#, absolute number of monocytes; NLR, neutrophils/lymphocytes ratio; NMR, neutrophils/monocytes ratio; LMR, lymphocytes/monocytes ratio; PLT, platelets; Neu, neutrophils; Lym, lymphocytes; Mon, monocytes; CRP, C-reactive protein. Bold values denote statistical significance at the p<0.05 level.
Table 4.
AUC, 95% CI, CUT-OFF, Sensitivity, Specificity for each biomarker (CRP, PCT and Multivariate Model).
Table 4.
AUC, 95% CI, CUT-OFF, Sensitivity, Specificity for each biomarker (CRP, PCT and Multivariate Model).
| BIOMARKER | AUC | 95% CI | CUT-OFF* | Sensitivity | Specificity |
|---|---|---|---|---|---|
| CRP | 0.83 | 0.79-0.88 | 6.07 | 77% | 77% |
| PCT | 0.78 | 0.73-0.84 | 0.33 | 77% | 70% |
| Multivariate Model | 0.92 | 0.89-0.95 | 0.655# | 82% | 89% |
*calculated by Youden index; #cut-off for predicted probabilities of the multivariate model.
Table 5.
Univariate and multivariate Cox Regression (CR) analysis for mortality within ICU and Hospital.
Table 5.
Univariate and multivariate Cox Regression (CR) analysis for mortality within ICU and Hospital.
| PREDICTOR | UNIVARIATE CR within ICU | MULTIVARIATE CR within ICU | UNIVARIATE CR within Hospital | MULTIVARIATE CR within Hospital |
|---|---|---|---|---|
| Age | <0.001 | <0.001 | <0.001 | <0.001 |
| Sex | 0.370 | 0.740 | ||
| Hb | 0.087 | 0.216 | ||
| RDW | <0.001 | 0.068 | <0.001 | 0.138 |
| WBC | 0.778 | 0.143 | ||
| NE# | 0.695 | 0.190 | ||
| LY# | 0.498 | 0.531 | ||
| MO# | 0.265 | 0.106 | ||
| NLR | 0.164 | 0.027 | 0.158 | |
| NMR | 0.536 | 0.981 | ||
| LMR | 0.210 | 0.530 | ||
| PLT | 0.522 | 0.071 | ||
| NeuX | 0.005 | 0.331 | 0.005 | 0.748 |
| NeuY | <0.001 | <0.001 | <0.001 | 0.040 |
| NeuZ | 0.258 | 0.300 | ||
| LymX | 0.657 | 0.439 | ||
| LymY | <0.001 | <0.001 | <0.001 | <0.001 |
| LymZ | 0.026 | 0.320 | 0.013 | 0.065 |
| MonX | <0.001 | 0.041 | 0.002 | 0.373 |
| MonY | 0.055 | 0.024 | 0.021 | |
| MonZ | 0.146 | 0.216 | ||
| CRP | 0.292 | 0.407 |
Hb, hemoglobin; RDW, red distribution width; WBC, white blood cells; NE#, absolute number of neutrophils; LY#, absolute number of lymphocytes; MO#, absolute number of monocytes; NLR, neutrophils/lymphocytes ratio; NMR, neutrophils/monocytes ratio; LMR, lymphocytes/monocytes ratio; PLT, platelets; Neu, neutrophils; Lym, lymphocytes; Mon, monocytes. Bold values denote statistical significance at the p<0.05 level.
Table 6.
Hematologic and biochemical data of the study population divided in sepsis and urinary tract infection groups.
Table 6.
Hematologic and biochemical data of the study population divided in sepsis and urinary tract infection groups.
| PREDICTOR | Without sepsis (n=56) | With sepsis (n=223) | p-Value |
|---|---|---|---|
| Hb, g/L | 125 (115-137) | 108 (90-128) | <0.001 |
| RDW, % | 14.5 (13.3-15.6) | 14.8 (13.8-16.6) | 0.074 |
| WBC,x109/L | 12.5 (8.5-17.6) | 11.2 (6.8-15.8) | 0.096 |
| NE#,x109/L | 10.4 (7.1-15.3) | 9.6 (5.5-14.0) | 0.340 |
| LY#,x109/L | 1.2 (0.8-1.7) | 0.6 (0.4-1.1) | <0.001 |
| MO#,x109/L | 0.7 (0.5-0.9) | 0.4 (0.2-0.7) | <0.001 |
| NLR | 9.1 (4.8-16.6) | 13.4 (6.9-24.5) | 0.003 |
| NMR | 15.3 (10.7-20.9) | 21.5 (13.3-36.2) | <0.001 |
| LMR | 1.6 (1.0-2.5) | 1.5 (0.9-2.8) | 0.953 |
| PLT,x109/L | 264 (200-322) | 190 (116-261) | <0.001 |
| NeuX | 387 (350-421) | 408 (371-446) | 0.008 |
| NeuY | 467 (437-512) | 541 (495-607) | <0.001 |
| NeuZ | 1770 (1684-1861) | 1792 (1712-1874) | 0.084 |
| LymX | 95 (91-101) | 97 (91-104) | 0.180 |
| LymY | 771 (738-823) | 775 (728-833) | 0.857 |
| LymZ | 966 (950-988) | 954 (931-982) | 0.008 |
| MonX | 219 (206-229) | 224 (211-245) | 0.003 |
| MonY | 1096 (1045-1161) | 1144 (1065-1225) | 0.005 |
| MonZ | 1349 (1318-1400) | 1348 (1303-1408) | 0.585 |
| CRP, mg/L | 94.5 (44.6-154.2) | 140.6 (64.8-207.2) | 0.008 |
| PCT, ng/mL | 0.37 (0.10-1.74) | 2.67 (0.36-19.60) | <0.001 |
Hb, hemoglobin; RDW, red distribution width; WBC, white blood cells; NE#, absolute number of neutrophils; LY#, absolute number of lymphocytes; MO#, absolute number of monocytes; NLR, neutrophils/lymphocytes ratio; NMR, neutrophils/monocytes ratio; LMR, lymphocytes/monocytes ratio; PLT, platelets; Neu, neutrophils; Lym, lymphocytes; Mon, monocytes; CRP, C-reactive protein; PCT, procalcitonin. Statistical significance was calculated according to nonparametric Mann-Whitney test and Fisher’s exact test. Bold values denote statistical significance at the p<0.05 level.
Table 7.
Univariate and multivariate logistic regression analysis for sepsis (without and with CRP) in sepsis and urinary tract infection groups.
Table 7.
Univariate and multivariate logistic regression analysis for sepsis (without and with CRP) in sepsis and urinary tract infection groups.
| PREDICTOR | UNIVARIATE LR | MULTIVARIATE LR without CRP |
MULTIVARIATE LR with CRP |
|---|---|---|---|
| Age | <0.001 | <0.001 | <0.001 |
| Sex | 0.110 | ||
| Hb | <0.001 | 0.005 | 0.006 |
| RDW | 0.086 | ||
| WBC | 0.510 | ||
| NE# | 0.938 | ||
| LY# | 0.101 | ||
| MO# | <0.001 | 0.779 | 0.838 |
| NLR | 0.007 | 0.180 | 0.188 |
| NMR | <0.001 | 0.049 | 0.047 |
| LMR | 0.322 | ||
| PLT | <0.001 | 0.007* | 0.007 |
| NeuX | 0.005 | 0.495 | 0.473 |
| NeuY | <0.001 | <0.001 | <0.001 |
| NeuZ | 0.061 | ||
| LymX | 0.055 | ||
| LymY | 0.576 | ||
| LymZ | 0.117 | ||
| MonX | 0.002 | 0.916 | 0.846 |
| MonY | 0.007 | 0.013 | 0.013 |
| MonZ | 0.845 | ||
| CRP | 0.017 | 0.633 |
Hb, hemoglobin; RDW, red distribution width; WBC, white blood cells; NE#, absolute number of neutrophils; LY#, absolute number of lymphocytes; MO#, absolute number of monocytes; NLR, neutrophils/lymphocytes ratio; NMR, neutrophils/monocytes ratio; LMR, lymphocytes/monocytes ratio; PLT, platelets; Neu, neutrophils; Lym, lymphocytes; Mon, monocytes; CRP, C-reactive protein. Bold values denote statistical significance at the p<0.05 level.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



