
Submitted:
30 December 2023
Posted:
03 January 2024
You are already at the latest version
Abstract
Background. A strong association between Activities of Daily Living (ADL)/Instrumental Activities of Daily Living (IADL) disability, chronic disease, and depressive symptoms among different racial/ethnic groups of older adults has been well established. However, whether this relationship remains true among refugee populations such as Vietnamese in the United States has not yet been investigated.
Methods. Using linear regressions, we tested the relationships between ADL/IADL disability, common chronic diseases, and depressive symptoms among 208 Vietnamese-origin older adults from the two convenience samples in 2017 and 2018 (≥65 years) from the Vietnamese Aging and Care Survey (VACS) in the Houston, Texas area.
Results. Study participants (N=208) were 56.2% female of average 75.4 years old with low education and low socioeconomic status. Most self-rated their health as fair/poor (80%). Regression analyses showed significant associations between liver disease and total ADL/IADL difficulties with higher depressive symptoms.
Conclusions. Older Vietnamese with more ADL/IADL disability and liver disease reported higher depressive symptoms. Complications from chronic conditions and pain might limit activities and impact older Vietnamese psychologically. Healthcare professionals can connect older Vietnamese with culturally and linguistically relevant adult daycare centers to provide them with social and exercise opportunities.
Keywords:
chronic diseases
; depressive symptoms
; disability
; older adults
; Vietnamese
1. Introduction
A high prevalence of depressive symptoms among older adults (≥65 years) has been well-documented as it is a public health concern throughout the world [1]. Studies have found similar patterns among older adults across racial/ethnic groups that show having more chronic diseases is associated with increased levels of depressive symptoms [2,3,4]. Other studies have also found that older adults experience more depressive symptoms if they have some disability in addition to chronic diseases [5,6]. Arthritis, lung disease, stroke, and cancer have been associated with depressive symptoms among non-Hispanic Whites [7]. Black older adults with kidney disease were more likely to experience depressive symptoms in one study [8]. Diabetes, arthritis, and kidney disease have been associated with depressive symptoms among older Mexican Americans [9]. Among Chinese American older adults, depressive symptoms have been associated with hypertension, arthritis, high cholesterol, diabetes, and heart disease [10]. However, there is a paucity of information regarding the association of chronic diseases with depressive symptoms among refugee populations such as Vietnamese in the United States (U.S.).
Vietnamese Americans are one of the most recently arrived but rapidly growing Asian-origin populations, and currently the 4th largest Asian subgroup in the U.S.[11]. Their substantial immigration started about 48 years ago, after the fall of Saigon in 1975 and many have settled in California and Texas [12]. Currently, over 2.2 million Vietnamese-origin Americans live in the U.S., and their number is growing [13]. Studies of Vietnamese Americans are important due to their lifelong adversity such as a long civil war, traumatic escape from Vietnam, boat journeys, pirate attacks, and government camps [14]. After migration to the U.S., they often faced low socioeconomic status, low English language proficiency, and cultural and lifestyle barriers [13]. These adverse experiences certainly impact aspects of physical, mental, and cognitive health and have a multi-generational impact [15]. However, the health of Vietnamese-origin people in the U.S. has not received significant attention in the literature.
To address these knowledge gaps, we developed the Vietnamese Aging and Care Survey (VACS) and collected demographic and comprehensive health data on Vietnamese older adults and their family caregivers (N=199; VACS 1) in 2018 in Houston, Texas [16,17,18,19]. In 2021, 102 older adults and their family caregivers (N=204) participated in a follow-up study [20]. Houston has over 143,000 residents of Vietnamese origin, making it the 2nd largest Vietnamese-populated metropolitan area in the U.S.[21]. Limited studies in California have shown that Vietnamese older adults rate their health as poorer compared to their non-Hispanic White counterparts and also experience a higher prevalence of depressive symptoms [22,23]. A nationwide study [24] has found that Vietnamese-origin older adults have more Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) disability than White, Black, Hispanic, and other Asian-origin older adults. Our VACS data found similar patterns with respect to their self-rated health, physical disability, and higher depressive symptoms, as well as high levels of loneliness [17].
The purpose of this analysis is to examine the association of ADL and IADL disability and chronic diseases with depressive symptoms in Vietnamese-origin older adults. We hypothesize that several strong relationships between ADL/IADL functional disability and chronic health conditions, and depressive symptoms would be found among Vietnamese-origin older adults in Houston, Texas.
2. Methods
2.1. Data and Sample
We used the Hispanic Established Populations for Epidemiological Studies of the Elderly (H-EPESE)[25] as a model and developed a cross-sectional health survey of Vietnamese-origin older adults who live in the Houston area. The survey was administered in 2017 and collected data on physical, mental, and cognitive health, disability, social support, use of social services, filial expectation from children, and religiosity from 131 older participants. In 2021, we developed VACS 2 and included additional instruments focused on cognitive function (e.g., Montreal Cognitive Assessment)[26,27], as well as COVID-19 related questions.
Inclusion criteria for both VACS 1 and 2 were self-identification as Vietnamese, ages 65 years and older, spoke English or Vietnamese and lived in the greater Houston, Texas area at the time of the survey. We excluded those who lived in long-term care facilities or were hospitalized. The final sample size was 208 Vietnamese-origin older adults (VACS 1: 131 and VACS 2: 77 older adults).
Data collection took place in November 2017 and April-May 2018 for VACS 1, and January-August 2021 for VACS 2. We distributed the study flyers in Vietnamese and English through Vietnamese social service agencies, senior centers, community centers, Vietnamese churches, temples, and adult day centers, and snowball sampling was widely used. A written consent form was obtained from all the participants prior to the survey. The study was approved by the University of Houston’s Institutional Review Board (VACS 1: STUDY00000419 and VACS 2: STUDY00002733). For more details on sampling and data collection, please see our previous manuscripts [16,17,18,19,20].
2.2. Measures
Depressive symptoms were measured with the Vietnamese version of the 20-item Center for Epidemiologic Studies Depression Scale (CES-D) [28,29]. Scores range from 0 to 60 with higher scores indicating greater depressive symptoms, and a score of 16 or greater indicating risk of clinical depression [30].
Functional disability was measured by Katz’s ADL [31] and Lawton and Brody’s IADL scale [32]. ADLs included bathing, dressing, toileting, transferring from a bed to a chair, walking across a small room, continence, and feeding. The ADL scale was scored whether the participant needed assistance to perform each activity (1 = yes or 0 = no) with higher scores indicating more disability (range from 0 to 7). The IADL scale requires more complex skills such as using the telephone, shopping, preparing food, housekeeping, laundry, using transportation, medication management, and managing finances. Items were scored if the study participant was able to perform each activity (0 = yes or 1 = no) (range from 0 to 9); higher scores suggest greater IADL disability.
Global Health was captured with a self-rated overall health (good/excellent vs fair/poor). Chronic diseases examined included arthritis, cancer, diabetes, heart problems, hypertension, liver disease, lung disease, and stroke. Respondents were asked if a doctor had ever told them they had each disease.
Sociodemographic characteristics included age, gender (female, male), marital status (married/partnered, not married/partnered), years of residence in the U.S., years of education, annual household income (<$25,000, $25,000-$50,000, >$50,000), living arrangement (live alone, live with others), and language spoken at home (Vietnamese, Vietnamese and other language).
2.3. Analyses
Descriptive statistics were used to characterize the sample stratified by depressive symptom status and sample. Sociodemographic variables included in regression analyses were identified based on a confound approach [33]. Variables significantly related to both the independent (ADL and IADL disability) and dependent (depression symptoms) variables were included in subsequent analyses. Arthritis and liver disease were identified as health conditions associated with depression (not shown in the table). For linear regression analyses, a combined variable of functional disability was created by summing ADL and IADL disabilities (range 0-16) to account for the high correlation (r = 0.57, p <0.001) between these variables, as well as expand range and sensitivity of the measurement [34,35]. A nested general linear model comparison was planned: The first model regressed depression on sociodemographics (marital status, gender), 2nd model added diseases (arthritis, liver disease), and the final model with the combined ADL/IADL disability. No multicollinearity was found in any combination of variables. Statistical analyses were conducted in R [36].
3. Results
Sample characteristics stratified by depression status are presented in Table 1. Depression was categorized based on a CES-D cutoff score of 16 [30]. The participants (N=208) were 56.2% female, on average 75.4 years old (age range 65-97), and 63% were married/partnered. All of them (100%) were born in Vietnam and had lived in the U.S. for an average of 25 years. They had completed an average of 8.2 years of education in Vietnam, and 90.4% reported low socioeconomic status (≤ $25K). The vast majority (80%) lived with their family members or relatives and spoke Vietnamese only (88%). Most rated their health as fair or poor (80%) and 76% of them reported at least one chronic disease. Compared to those with CES-D scores within normal ranges, those with elevated CES-D scores (16+) were more likely to be not married or not partnered (28.2% vs 50%, p = 0.002) and were more likely to report one or more chronic diseases (71.0% vs 83.3%, p = 0.041). Sample characteristics stratified by sample (Table 2) demonstrated that, compared to participants from VACS 2, VACS 1 participants lived in the U.S. longer (21.04 vs 26.70, p = 0.005) and reported less IADL difficulties (5.26 vs 4.28, p = 0.041).
Linear regression results predicting depressive symptoms as measured with the CES-D scores are shown in Table 3. When adjusting for other predictors in the final model, individuals with liver disease reported 7.90 [95% CI = 2.35, 13.45] higher CES-D points than those without. Older adults who reported more disability in combined ADLs and IADLs reported more depressive symptoms by 0.40 [95% CI = 0.12, 0.69] points on the CES-D for every additional ADL or IADL impairment. Marginal effects of predictors associated with CES-D total scores in the final model are presented in Figure 1.
4. Discussion
Using a combination of VACS 1 and 2 data, we examined the associations between chronic health conditions (i.e., 8 common chronic diseases), as well as functional disability (i.e., ADLs and IADLs), and depressive symptoms among 208 Vietnamese-origin older adults who lived in the greater Houston, Texas area. We found that having arthritis was positively associated with depressive symptoms in bivariate analysis. Minh Hoa et al.’s study (2003) (N = 2,119) found that 14.5% of Vietnamese adults in urban cities in Vietnam suffered musculoskeletal pain, and osteoarthritis was the most common disease. Mwangi and colleagues’ 2015 study [37], examining common chronic diseases in 2,873 Vietnamese older adults in rural Vietnam also showed arthritis/osteoarthritis was the most common chronic disease (35%). Several other studies on older adults in Vietnam have shown similar patterns of high prevalence of osteoarthritis, chronic pain, and its association with depressive symptoms [38,39]. Based on these previous studies, our finding of an association between arthritis and depressive symptoms is well aligned with the literature. Having arthritis and suffering from chronic pain certainly would make older adults uncomfortable and distressed in their daily lives.
In addition, liver disease showed an even stronger association with depressive symptoms, which was robust to adjustment from sociodemographic factors. Similar to arthritis, liver disease, hepatitis B and C specifically, is a common chronic disease among Asian Americans, and older Vietnamese have historically been disproportionally affected by the disease in Vietnam [40]. Other studies have found a high prevalence of Hepatitis B among Vietnamese Americans [41], and a high incidence of liver cancer among Vietnamese-origin men and women [42]. Liver disease is also common among Vietnamese men due to high alcohol consumption as Vietnam is one of the highest alcohol-consuming countries in the world [43]. Symptoms of liver disease (e.g., chronic fatigue, abdominal pain) could certainly predispose Vietnamese older adults to feeling weak and distressed. Among the ADLs examined, bathing and eating were the strongest correlates of depressive symptoms, and among IADLs, managing finances has the strongest effect (not shown in the table).
Previous studies have established a strong relationship between physical functional disability and depressive symptoms in community-dwelling older adults [5,6]. However, whether the relationships were with ADL or IADL functions varied. For example, among Asian Americans, Japanese, Korean, and Taiwanese older adults reported more depressive symptoms when they had high IADL difficulties [44,45,46] while Koreans in another study reported more depressive symptoms when their ADL disability was high [47]. A study of older Chinese Americans showed associations with both ADL and IADL disability and depressive symptoms [10]. Having limited control over their basic functioning would restrict Vietnamese older adults’ daily activities. IADL functions, however, can be culturally and socioeconomically biased, especially among women who often rely on family members for assistance with instrumental activities.
Limitations of this study should be noted. First, we used a small convenience sample collected only within the greater Houston area, and our results may not be generalizable to older Vietnamese in other parts of the country. The number of some chronic conditions including liver disease was small. Future studies with larger and more representative samples might provide a better picture of the population’s physical and emotional function. While most Vietnamese-origin older adults live with other family members and enjoy high levels of social support, healthcare professionals can help them to better access culturally and linguistically relevant services to help ameliorate their physical and emotional problems [48,49].
Author Contributions
Conception & Design: CEM, JMG, KSM. Acquisition of data: CEM, KNN. Analysis & Interpretation of data: JMG, CEM, LDM, KSM. Drafting of manuscript: CEM, JMG. Critical review: CEM, OLM, KSM, JMG, LDM.
Funding
Miyawaki was partially funded by the National Institutes of Health (NIH)/National Institute on Aging (NIA) Texas Resource Center for Minority Aging Research (RCMAR) (P30AG059301). Meyer was partially funded by the NIH/NIA (R01AG067541, R24AG063718) and the Alzheimer’s Association (AARGD-19-619832).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the University of Houston (VACS 1: STUDY00000419, July 4, 2017, and VACS 2: STUDY00002733, December 18, 2020).
Informed Consent Statement
Written informed consent was obtained from all the participants prior to the survey.
Data Availability Statement
The data that support the findings of this study are available from the first author, CEM, upon reasonable request.
Acknowledgments
The authors appreciate the Executive Directors of VN TeamWork, Mr. Mike C. Nguyen and BPSOS-Houston, Ms. Jannette Diep, as well as a countless number of Vietnamese key personnel who facilitated years of sample recruitment. We thank all the Vietnamese older adults and their family caregivers who welcomed us to their homes and shared their health information despite their busy lives.
Conflicts of Interest Statement
All authors have no competing interests to declare.
References
- Hossain B, Yadav PK, Nagargoje VP, Vinod Joseph KJ. Association between physical limitations and depressive symptoms among Indian elderly: marital status as a moderator. BMC Psychiatry. 2021, 21, 573. [Google Scholar] [CrossRef]
- Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of co-morbid depression in adults with Type 2 diabetes: a systematic review and meta-analysis. Diabet Med. 2006, 23, 1165–1173. [Google Scholar] [CrossRef]
- Matcham F, Rayner L, Steer S, Hotopf M. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2013, 52, 2136–2148. [Google Scholar] [CrossRef]
- Palinkas LA, Wingard DL, Barrett-Connor E. The biocultural context of social networks and depression among the elderly. Soc. Sci. Med. 1990, 30, 441–447. [Google Scholar] [CrossRef]
- Berkman LF, Berkman CS, Kasl S, et al. Depressive symptoms in relation to physical health and functioning in the elderly. Am J Epidemiol. 1986, 124, 372–388. [Google Scholar] [CrossRef] [PubMed]
- Schmitz N, Wang J, Malla A, Lesage A. Joint effect of depression and chronic conditions on disability: results from a population-based study. Psychosom Med. 2007, 69, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Penninx BW, Beekman AT, Ormel J, et al. Psychological status among elderly people with chronic diseases: does type of disease play a part? J Psychosom Res. 1996, 40, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Bazargan M, Hamm-Baugh VP. The relationship between chronic illness and depression in a community of urban black elderly persons. J Gerontol B Psychol Sci Soc Sci. 1995, 50, S119–S127. [Google Scholar] [CrossRef]
- Black SA, Goodwin JS, Markides KS. The association between chronic diseases and depressive symptomatology in older Mexican Americans. J Gerontol A Biol Sci Med Sci. 1998, 53, M188–M194. [Google Scholar] [CrossRef]
- Kong D, Solomon P, Dong X. Depressive Symptoms and Onset of Functional Disability Over 2 Years: A Prospective Cohort Study. J Am Geriatr Soc. 2019, 67, S538–S544. [Google Scholar] [CrossRef]
- Budiman A, Ruiz NG. Asian Americans Are the Fastest-Growing Racial or Ethnic Group in the U.S. /: 2021. Retrieved from https, 2021; Retrieved from https://www.pewresearch.org/fact-tank/2021/04/09/asian-americans-are-the-fastest-growing-racial-or-ethnic-group-in-the-u-s/.
- Ruggles S, Flood S, Goeken R, Schouweiler M, Sobek M. IPUMS USA, /: IPUMS USA. 2022. Accessed January 23, 2023, https://usa.ipums.org/usa/.
- Alperin E, Batalova J. Vietnamese Immigrants in the United States, /: Institute (MPI); 2018. Retrieved from https, 2018; Retrieved from https://www.migrationpolicy.org/article/vietnamese-immigrants-united-states-5.
- Gold S., J. Mental health and illness in Vietnamese refugees. West J Emerg Med. 1992, 157, 290–294. [Google Scholar]
- Bloch A, Hirsch S. Inter-generational transnationalism: the impact of refugee backgrounds on second generation. Comp Migr Stud. 2018, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki CE, Chen NW, Meyer OL, Tran MT, Markides KS. Vietnamese adult-child and spousal caregivers of older adults in Houston, Texas: Results from the Vietnamese Aging and Care Survey (VACS). J Gerontol Soc Work. 2020, 63, 5–18. [Google Scholar] [CrossRef]
- Miyawaki CE, Liu M, Markides KS. Association between caregivers’ characteristics and older care recipients’ well-being among Vietnamese immigrant families in the United States. J Community Psychol. 2022, 50, 2214–2224. [Google Scholar] [CrossRef]
- Miyawaki CE, Liu M, Park VT, Tran MT, Markides KS. Social support as a moderator of physical disability and mental health in older Vietnamese immigrants in the U.S.: Results from the Vietnamese Aging and Care Survey (VACS). Geriatr Nur (Lond). 2022, 44, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki CE, Meyer OL, Chen NW, Markides KS. Health of Vietnamese older adults and caregiver’s psychological status in the United States: Result from the Vietnamese Aging and Care Survey. Clin Gerontol. 2020, 45, 1–9. [Google Scholar] [CrossRef]
- Miyawaki CE, Garcia JM, Nguyen KN, Park VT, Markides KS. Multiple chronic conditions and disability among Vietnamese older adults: Results from the Vietnamese Aging and Care Survey (VACS) [published online ahead of print, 2023 May 30]. J Racial Ethn Health Disparities, 2023. [CrossRef]
- Pew Research Center. Top 10 U.S. Metropolitan Areas by Vietnamese Population, 2019, Pew ResearchCenter: 2021. Accessed , 2022. https://www.pewresearch.org/social-trends/chart/top-10-u-s-metropolitanareas- by-vietnamese-population-2019/, 19 July 2021.
- Meyer OL, Nguyen KH, Dao TN, Vu P, Arean P, Hinton L. The sociocultural context of caregiving experiences for Vietnamese dementia family caregivers. Asian Am J Psychol. 2015, 6, 263–272. [Google Scholar] [CrossRef]
- Sorkin D, Tan AL, Hays RD, Mangione CM, Ngo-Metzger Q. Self-reported health status of Vietnamese and non-Hispanic white older adults in California. J Am Geriatr Soc. 2008, 56, 1543–1548. [Google Scholar] [CrossRef]
- Fuller-Thomson E, Brennenstuhl S, Hurd M. Comparison of disability rates among older adults in aggregated and separate Asian American/Pacific Islander subpopulations. Am J Public Health. 2011, 101, 7. [Google Scholar]
- Markides K, Chen NW, Angel R, Palmer R, Graham J. Hispanic Established Populations for the Epidemiologic Study of the Elderly (HEPESE) Wave 7, 2010-2011 [Arizona, California, Colorado, New Mexico, and Texas]. Published online 2016. [CrossRef]
- Do M, Ha Bui BK, K. Pham N, et al. Validation of MoCA test in Vietnamese language for cognitive impairment screening. J Glob Health Neurol Psychiatry, Published online May 20, 2022. [CrossRef]
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J Am Geriatr Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Radloff, LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Thai TT, Jones MK, Harris LM, Heard RC. Screening value of the Center for Epidemiologic Studies – Depression scale among people living with HIV/AIDS in Ho Chi Minh City, Vietnam: A validation study. BMC Psychiatry. 2016, 16, 145. [Google Scholar] [CrossRef]
- Nguyen HT, Le VA, Dunne M. Validity and reliability of the two scales measuring depression and anxiety used in community survey in Vietnamese adolescents. Vietnam J Public Health. 2007, 7, 25–31. [Google Scholar]
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA. 1963, 185, 914. [Google Scholar] [CrossRef]
- Lawton MP, Brody EM. Assessment of older people: Self-maintaining and instrumental activities of daily living. The Gerontologist. 1969, 9 Pt 1, 179–186. [Google Scholar] [CrossRef]
- Field-Fote, EE. Mediators and moderators, confounders and covariates: Exploring the variables that illuminate or obscure the "Active Ingredients" in neurorehabilitation. J Neurol Phys Ther. 2019, 43, 83–84. [Google Scholar] [CrossRef]
- Quiñones AR, Markwardt S, Botoseneanu A. Diabetes-multimorbidity combinations and disability among middle-aged and older adults. J Gen Intern Med. 2019, 34, 944–951. [Google Scholar] [CrossRef]
- Spector WD, Fleishman JA. Combining activities of daily living with instrumental activities of daily living to measure functional disability. J Gerontol B Psychol Sci Soc Sci. 1998, 53, S46–S57. [Google Scholar] [CrossRef]
- R Core Team. R: A language and environment for statistical computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Mwangi J, Kulane A, Van Hoi L. Chronic diseases among the elderly in a rural Vietnam: prevalence, associated socio-demographic factors and healthcare expenditures. Int J Equity Health. 2015, 14, 134. [Google Scholar] [CrossRef]
- Ho-Pham LT, Lai TQ, Mai LD, Doan MC, Pham HN, Nguyen TV. Prevalence of radiographic osteoarthritis of the knee and its relationship to self-reported pain. PLoS One. 2014, 9, e94563. [Google Scholar] [CrossRef]
- Nguyen AT, Nguyen THT, Nguyen TTH, et al. Chronic pain and associated factors related to depression among older patients in Hanoi, Vietnam. Int J Environ Res Public Health. 2021, 18, 9192. [Google Scholar] [CrossRef]
- Strong C, Hur K, Kim F, Pan J, Tran S, Juon HS. Sociodemographic characteristics, knowledge and prevalence of viral hepatitis infection among Vietnamese Americans at community screenings. J Immigr Minor Health. 2015, 17, 298–301. [Google Scholar] [CrossRef]
- Kowdley KV, Wang CC, Welch S, Roberts H, Brosgart CL. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology. 2012, 56, 422–433. [Google Scholar] [CrossRef]
- Pham C, Fong TL, Zhang J, Liu L. Striking racial/ethnic disparities in liver cancer incidence rates and temporal trends in California, 1988-2012. J Natl Cancer Inst. 2018, 110, 1259–1269. [Google Scholar] [CrossRef]
- Hanh HTM, Assanangkornchai S, Geater AF, Hanh VTM. Socioeconomic inequalities in alcohol use and some related consequences from a household perspective in Vietnam. Drug Alcohol Rev. 2019, 38, 274–283. [Google Scholar] [CrossRef]
- Ahn J, Kim BJ. The relationships between functional limitation, depression, suicidal ideation, and coping in older Korean immigrants. J Immigr Minor Health. 2015, 17, 1643–1653. [Google Scholar] [CrossRef]
- Chao, SF. Functional disability and depressive symptoms: Longitudinal effects of activity restriction, perceived stress, and social support. Aging Ment Health. 2014, 18, 767–776. [Google Scholar] [CrossRef]
- Kim BJ, Liu L, Nakaoka S, Jang S, Browne C. Depression among older Japanese Americans: The impact of functional (ADL & IADL) and cognitive status. Soc Work Health Care. 2018, 57, 109–125. [Google Scholar] [CrossRef]
- Kim BJ, Choi Y. The relationship between Activities of Daily Living (ADL), chronic diseases, and depression among older Korean immigrants. Educ Gerontol 2015, 41, 417–427. [CrossRef]
- Conn VS, Hafdahl AR, Mehr DR. Interventions to increase physical activity among healthy adults: Meta-analysis of outcomes. Am J Public Health. 2011, 101, 751–758. [Google Scholar] [CrossRef]
- Zagic D, Wuthrich VM, Rapee RM, Wolters N. Interventions to improve social connections: A systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. 2022, 57, 885–906. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Marginal Effect Plots of Significant Predictors in Model 3. Marginal effect plots estimated using ggeffects are presented. Plots show marginal effects after controlling for all other variables in the model.
Figure 1.
Marginal Effect Plots of Significant Predictors in Model 3. Marginal effect plots estimated using ggeffects are presented. Plots show marginal effects after controlling for all other variables in the model.
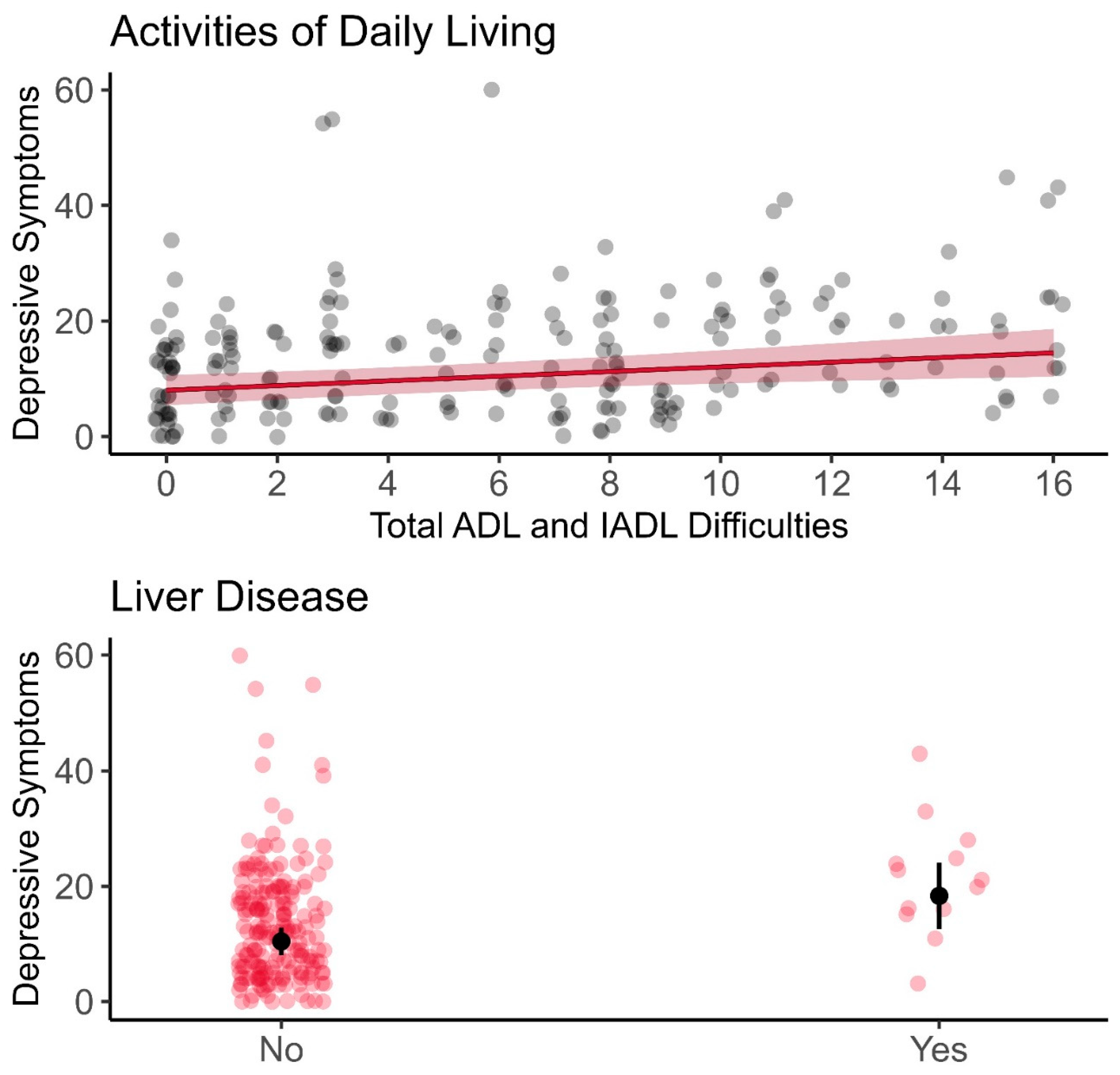

Table 1.
Characteristics of Vietnamese-Origin Older Adults (≥65 years) (N = 208).
| Full Sample | Depression | ||||
|---|---|---|---|---|---|
| CES-D <16 (n=124) | CES-D ≥16 (n=84) |
p | |||
| Sample | |||||
| VACS 1 | 131 (63.0) | 81 (65.3) | 50 (59.5) | 0.482 | |
| VACS 2 | 77 (37.0) | 43 (34.7) | 34 (40.3) | ||
| Years of Age | 75.42±7.17 (65-97) |
75.07±7.15 (65-97) |
75.94±7.22 (65-91) |
0.393 | |
| Gender | |||||
| Female | 117 (56.2) | 65 (52.4) | 52 (61.9) | 0.226 | |
| Male | 91 (43.8) | 59 (47.6) | 32 (38.1) | ||
| Marital Status | |||||
| Married/partnered | 131 (63.0) | 89 (71.8) | 42 (50.0) | 0.002 | |
| Not married | 77 (37.0) | 35 (28.2) | 42 (50.0) | ||
| Years in the U.S. | 24.56±13.92 (1-74) |
24.54 ±14.40 (1-74) |
24.60±13.27 (1-54) |
0.977 | |
| Years of Education | 8.22±5.49 (0-20) |
8.52±5.31 (0-19) |
7.77±5.74 (0-20) |
0.338 | |
| Household Income | |||||
| < $25,000 | 188 (90.4) | 111 (89.5) | 77 (91.7) | 0.762 | |
| $25,000-$50,000 | 13 (6.2) | 9 (7.3) | 4 (4.8) | ||
| > $50,000 | 7 (3.4) | 4 (3.2) | 3 (3.6) | ||
| Living Arrangement | |||||
| Live alone | 42 (20.2) | 23 (18.5) | 19 (22.6) | 0.588 | |
| Live with other(s) | 166 (79.8) | 101 (81.5) | 65 (77.4) | ||
| Language spoken at home | |||||
| Vietnamese only | 183 (88.0) | 109 (87.9) | 74 (88.1) | 1.000 | |
| Vietnamese & other | 25 (12.0) | 15 (12.1) | 10 (11.9) | ||
| Self-Rated Health | |||||
| Good/Excellent | 42 (20.2) | 31 (25.0) | 11 (13.1) | 0.055 | |
| Fair/poor | 166 (79.8) | 93 (75.0) | 73 (86.9) | ||
| Chronic Diseases | 158 (76.0) | 88 (71.0) | 70 (83.3) | 0.041 | |
| Arthritis | 104 (50.0) | 55 (44.4) | 49 (58.3) | 0.066 | |
| Cancer | 10 (4.8) | 6 (4.8) | 4 (4.8) | 1.000 | |
| Diabetes | 85 (40.9) | 52 (41.9) | 33 (39.3) | 0.812 | |
| Heart attack | 41 (19.7) | 21 (16.9) | 20 (23.8) | 0.296 | |
| Hypertension | 154 (74.0) | 90 (72.6) | 64 (76.2) | 0.673 | |
| Liver disease | 13 (6.2) | 3 (2.4) | 10 (11.9) | 0.013 | |
| Lung disease | 10 (6.2) | 5 (4.0) | 5 (6.0) | 0.760 | |
| Stroke | 23 (11.1) | 11 (8.9) | 12 (14.3) | 0.319 | |
| # of ADL disability | 1.37±2.19 | 1.08±2.00 | 1.80±2.39 | 0.020 | |
| # of IADL disability | 4.64±3.34 | 4.12±3.42 | 5.42±3.08 | 0.006 | |
| # of ADL and IADL disability | 6.01±4.93 | 5.60±4.97 | 6.71±4.81 | 0.116 | |
Note. M±SD (Range), N (%); M = mean; SD = standard deviation. ADL = Activities of Daily Living, Score ranges: 0-7; IADL = Instrumental Activities of Daily Living, Score ranges: 0-9. ADL/IADL score ranges: 0-16.
Table 2.
Characteristics of Vietnamese-Origin Older Adults by Sample (≥65 years) (N = 208).
| Full Sample | VACS 1 (n=131) |
VACS 2 (n=77) |
p | |
|---|---|---|---|---|
| Years of Age | 75.42±7.17 (65-97) |
75.50±6.38 (65-90) |
75.30±8.40 (65-97) |
0.848 |
| Gender | ||||
| Female | 117 (56.2) | 71 (54.2) | 46 (59.7) | 0.527 |
| Male | 91 (43.8) | 60 (45.8) | 31 (40.3) | |
| Marital Status | ||||
| Married/partnered | 131 (63.0) | 76 (58.0) | 55 (71.4) | 0.074 |
| Not married | 77 (37.0) | 55 (42.0) | 22 (28.6) | |
| Years in the U.S. | 24.56±13.92 (1-74) |
26.70±12.99 (1-68) |
21.04±14.76 (1-74) |
0.005 |
| Years of Education | 8.22±5.49 (0-20) |
7.96±5.63 (0-20) |
8.65±5.24 (0-18) |
0.385 |
| Household Income | ||||
| < $25,000 | 188 (90.4) | 123 (93.9) | 65 (84.4) | 0.060 |
| $25,000-$50,000 | 13 (6.2) | 6 (4.6) | 7 (9.1) | |
| > $50,000 | 7 (3.4) | 2 (1.5) | 5 (6.5) | |
| Living Arrangement | ||||
| Live alone | 42 (20.2) | 32 (24.4) | 10 (13.0) | 0.071 |
| Live with other(s) | 166 (79.8) | 99 (75.6) | 67 (87.0) | |
| Language spoken at home | ||||
| Vietnamese only | 183 (88.0) | 116 (88.5) | 67 (87.0) | 0.914 |
| Vietnamese & other | 25 (12.0) | 15 (11.5) | 10 (13.0) | |
| Self-Rated Health | ||||
| Good/Excellent | 42 (20.2) | 32 (24.4) | 10 (13.0) | 0.071 |
| Fair/poor | 166 (79.8) | 99 (75.6) | 67 (87.0) | |
| Chronic Diseases | 158 (76.0) | 96 (73.3) | 62 (80.5) | 0.410 |
| Arthritis | 104 (50.0) | 63 (48.1) | 41 (53.2) | 0.566 |
| Cancer | 10 (4.8) | 6 (4.6) | 4 (5.2) | 1.000 |
| Diabetes | 85 (40.9) | 53 (40.5) | 32 (41.6) | 0.992 |
| Heart attack | 41 (19.7) | 25 (19.1) | 16 (20.8) | 0.907 |
| Hypertension | 154 (74.0) | 98 (74.8) | 56 (72.7) | 0.867 |
| Liver disease | 13 (6.2) | 9 (6.9) | 4 (5.2) | 0.853 |
| Lung disease | 10 (6.2) | 4 (3.1) | 6 (7.8) | 0.227 |
| Stroke | 23 (11.1) | 11 (8.4) | 12 (15.6) | 0.172 |
| # of ADL disability | 1.37±2.19 | 1.32±2.17 | 1.45±2.24 | 0.672 |
| # of IADL disability | 4.64±3.34 | 4.28±3.34 | 5.26±3.27 | 0.041 |
| # of ADL and IADL disability | 6.01±4.93 | 5.60±4.97 | 6.71±4.81 | 0.116 |
Note. M±SD (Range), N (%); M = mean; SD = standard deviation. ADL = Activities of Daily Living, Score ranges: 0-7; IADL = Instrumental Activities of Daily Living, Score ranges: 0-9. ADL/IADL score ranges: 0-16.
Table 3.
Linear Regression Analysis Predicting Depressive Symptoms (N = 208).
| Predictors | Model 1: Demographics |
Model 2: Chronic Disease |
Model 3: Functional Disability |
|---|---|---|---|
| (Intercept) | 11.29 [9.11, 13.47]*** | 9.68 [7.30, 12.05]*** | 8.00 [5.38, 10.62]*** |
| Gender [Female] | 2.06 [-0.86, 4.97] | 1.90 [-1.02, 4.82] | 1.93 [-0.94, 4.81] |
| Marital Status [Not Married] | 4.05 [1.05, 7.04]** | 3.70 [0.77, 6.64]* | 2.77 [-0.19, 5.73]+ |
| Arthritis | 2.69 [-0.11, 5.48]+ | 1.80 [-1.03, 4.62] | |
| Liver Disease | 7.69 [2.05, 13.33]** | 7.90 [2.35, 13.45]** | |
| ADL & IADL Disability | 0.40 [0.12, 0.69]** | ||
| R2 | 0.057 | 0.110 | 0.143 |
| Adjusted R2 | 0.047 | 0.093 | 0.122 |
| AIC | 1557.7 | 1549.5 | 1543.7 |
| Residual df | 205 | 203 | 202 |
| Residual Sum of Squares | 20956.09 | 19764.33 | 19033.38 |
| Model Comparison F | - | 6.324 | 7.757 |
| Model Comparison p | - | 0.002 | 0.006 |
Note. Unstandardized regression coefficients are presented with 95% confidence intervals in brackets; p-value: + = <0.01, * = <0.05, ** = <0.01, *** = <0.001; IADL = Instrumental Activities of Daily Living; ADL = Activities of Daily Living.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



