
Submitted:
02 January 2024
Posted:
03 January 2024
You are already at the latest version
Abstract
Especially in the last two decades, due to the developments in durable mechanical
circulatory support (MCS) technology and applications, left ventricular assist (LVAD) implantation has become used in more fragile end-stage heart failure patients with higher risk.
Despite advances in technology and patient care processes, right heart failure remains the leading cause of morbidity and mortality after durable LVAD implantation. It is difficult to make decisions about the type and duration of MCS during preoperative evaluation, and many clinical, hemodynamic, biochemical and echocardiographic criteria must be taken into account when evaluating the right ventricle.
Complex quantitative scoring systems, including measurements of different risk factors for postimplant right ventricular failure, and composite variables, including the anatomical and functional status of the right ventricle, have been used to decide between left or biventricular assist device implantation.
The successful use of artificial intelligence (AI) and machine learning (ML) in various applications in the medical field has paved the way for the idea of using it to better predict possible conditions such as right heart failure after LVAD implantation.
This review aims to evaluate the current situation of risk prediction models using AI and ML technology, which have become popular in recent years, and possible future developments in predicting right heart failure after the application of durable MCS systems.
Keywords:
left ventricular assist device
; right heart failure
; right ventricle failure
; artificial intelligence
; machine learning
1. Introduction
Despite all major pharmacological and clinical improvements for cardiovascular disease management, heart failure still remains a global public health concern, with dramatic increases annually. It is known that 64 million individuals in U.S.A. are affected from this heart disease and the hospitalization rate has tripled in the last 30 years [1]. Although heart transplantation remains the best therapeutic option for select patients, the number of available and eligible donors are severely lacking. Since ventricular assist device implantation for advanced end stage heart failure patients first begun, treatment strategies for heart failure changed dramatically. Currently, left ventricular assist device (LVAD) implantation is the most accepted alternative treatment option of heart transplantation for refractory advanced heart failure patients, where the aim can be as bridge to transplantation or as destination therapy. LVADs provide both safer implantation and better quality of life than biventricular assist devices (BVADs). As a result of the advancements in LVAD technology and experience 1-year survival after implantation has now increased to over 80% [2,3,4,5,6]. In spite of significant improvements in life expectancy, quality of life, decrease in hospital stay and reduced re-hospitalization rates after LVAD implantation, there are still well known and serious side effects that medical researchers are still working on in order to discover viable solutions that can yield better outcomes. One of the most challenging and prevalent side effects of LVAD implantations which is the topic of our review, is right heart failure (RHF) that may develop afterwards and may cause significant early and/or long-term detrimental effects.
RHF occurs between 10-40% in all cases after LVAD implantation [7,8,9,10,11,12,13,14,15,16,17,18,19]. Late RHF may occur in up to 10–20% of LVAD patients [20,21,22,23,24,25]. The main reasons for this wide prevalence range reported in different studies are differences in the diagnostic criteria of RHF, patient demographic characteristics, and institutional management strategies [26,27]. Even though well accepted signs and symptoms of RHF are known by all clinicians; there remains no universally classification and definition algorithms. Some studies based on clinical statue like high central venous pressure (CVP), requirement of inotropic support, increase in pulmonary arterial pressure, nitric oxide (NO) inhalation or requirement of mechanically support for right ventricle [28,29,30,31,32,33]. The time course of the RHF onset is another type of definition used in few studies They revealed as “acute”; During the first 24 hours of LVAD implantation, “early”; between first 48 hours -14 days and “late”; after the first 14 days [34].
Over time, some changes have been made to eliminate ambiguity and inconsistency in the definition of RHF [35,36,37,38]. Recently, the Mechanical Circulatory Support Academic Research Consortium has proposed a broader, more comprehensive definition of RHF after LVAD [39].
Due to the high morbidity and mortality of RHF after LVAD implantation, effective treatment methods are quite comprehensive and depend on centers experience and opportunities. Initial therapy after post-LVAD RHF starts with pharmaceutical treatment. (inotropic support, NO inhalation, forced diuresis). If RHF still remain after efficient medical treatment; mechanically device support is coming into consideration even with high mortality. The incidence of requiring an RVAD following LVAD implantation is approximately 10-20% [40,41,42,43,44,45,46].
Therefore, it is critical to decide whether the patient needs BVAD before or during surgery at the latest. However, despite the preparations and precautions taken by evaluating many clinical, hemodynamic, biochemical and echocardiographic criteria, it is not always possible to make the right choice between LVAD and BVAD. In order to make the right decision, it is important to thoroughly evaluate the right ventricular anatomy and functions before surgery.
Over the years, many risk prediction models have been proposed to accurately determine the risk of developing right ventricular failure, which predisposes to multiple organ failure, hemorrhagic and thrombotic complications after mechanical support system applications.
As a result of the increase in MCS experience and the number of cases, multifaceted analyzes of post-LVAD outcomes and complications have become a necessity. The fact that most studies are conducted in a single center and on relatively small patient groups reduces the reliability of the analyses of pre- and postoperative results. Variable characteristics of VADs and patient demographics also make meaningful interpretation difficult. Additionally, due to the complex and heterogeneous pathophysiology of RHF, it is not easy to classify or generate a risk score for post-LVAD RHF. However, risk scores created with the use of multivariate analyzes have provided significant benefits in determining the development of RHF. Thus, it would not be wrong to say that one of the most useful things to do to prevent RHF after LVAD is to use a validated risk scoring system.
On the other hand, with the increasing use of AI and ML applications in the medical field in recent years, the doors of a new development have been opened in this regard. The number of studies conducted on this subject is increasing year by year.
First proposed by Alan Turing in 1950, AI is the concept of creating a digital mind that can learn, and “think” like a human mind can. ML is a process that is encompassed by AI, where a software model is can learn to acquire new data and interpret it in a meaningful way towards the task at hand, therefore providing useful feedback and surpass classical algorithm-based computer programming. It is viable that an AI could fulfill any and all given assignments as long as the ML model is sophisticated enough [47,48,49].
There are two main approaches to ML with many more subtypes and variations below them. “Supervised ML” involves identifying and labeling data with known class information and training the ML model with this knowledge available. Therefore, ML model can then determine common properties within each class and thus “learn” to identify that class on its own. Supervised ML, however, requires manual data set preparation for labelling and needs expert knowledge about the task [50,51].
The second approach of “unsupervised ML” is done by making all the data available to the software model, withholding the information about classes and letting the ML model decide which cases belong together according to their data similarities. Unsupervised ML can be very beneficial for obtaining new information about complex systems with many variables as clustering decisions and feature associations will be made by the model on its own, sometimes yielding previously unexpected results. The large size of data that is needed for unsupervised ML model is usually more difficult to prepare and sometimes limits the process [50,51]. A flowchart visually explaining ML process is shown in Figure 1.
There are many industrial and commercial uses for AI that is already proving itself as a powerful tool when used correctly. Although healthcare is understandably a field that should be more careful when adopting new ideas, it seems inevitable that AI will play a huge role as an assistive tool in patient care as well. Regarding our subject matter, it can be easily imagined that AI will be able to help in a multitude of ways, such as discovering RHF mechanism hidden parameter relationships, early prediction of risk groups pre-implantation, identification of clinical parameters critical for early RHF detection post implantation and determining treatment plans for RHF patients post implantation in order to change prognosis. Achieving all of these tasks, through conventional means, seems to be a difficult undertaking when the sheer volume of data analysis that would be necessary is considered. Therefore, utilizing AI for this job appears to be a natural fit [52,53,54,55].
Purpose of this study is to review and highlight recent advances in uses of AI for evaluating RHF after LVAD implantation, as these types of research will lead to a better understanding of a common issue with LVAD implantations, which is of critical importance.
2. Method
Available literature has been scanned by using following phrases; “artificial intelligence and left ventricular assist device”, “machine learning and left ventricular assist device”, “right heart failure and machine learning”, “prediction of right heart failure after LVAD”, “deep learning and LVAD”. Pubmed, Web of Science, Google Scholar databases were used in order to search for published articles. For achieving a better understanding of the role of AI and ML techniques, we also reviewed studies relating to previous risk scoring systems and summarized them all with their pros and cons. All published articles were analyzed by authors of this review. We found 9 studies using conventional risk score systems and 9 studies using AI systems (Table 1) for prediction of RHF after LVAD implantation.
2.1. Conventionally risk prediction scores
In 2008, Matthews et al. used multivariate logistic regression in patients whom underwent mostly pulsatile LVAD implantation [56]. They defined right ventricular failure (rate 35%) as; the need for post-operative IV inotrope support for >14 days, inhaled nitric oxide for ≥48 hours, right-sided circulatory support or hospital discharge on an inotrope. The multivariate technique used in this study allowed the simultaneous evaluation of many risk factors that may suggest different results when evaluated separately. An elevated ALT, vasopressor requirement, high bilirubin and creatinine levels were predictors of RHF in multivariate analyses. Additionally, the Michigan right ventricular failure risk scoring (vasopressor requirement 4 points; AST ≥80 IU/l 2 points; bilirubin ≥2.0 mg/dl → 2.5 points, creatinine ≥2.3 mg/dl 3 points; renal replacement therapy 3 points) was formulated to better stratify RV failure risk in LVAD candidates. The Michigan right ventricular failure risk score (RVFRS) is the first model for pre-operative risk stratification of RV failure in LVAD candidates. RVFRS was ≤3.0 in 88% of patients who did not develop right ventricular failure (specificity = 88%). Right ventricular failure was developed in 80% of patients with RVFRS ≥5.5 (positive predictive value = 80%).
In the same year Fitzpatrick et al., reviewed patients whom underwent mainly pulsatile LVAD implantation [57]. According to the findings on echocardiography performed during preoperative examination, right ventricular dysfunction (rate 37%) is divided into three classes: mild, moderate and severe. This study identified that preoperative low cardiac index (CI) (≤ 2.2l/min/m2) and right ventricle stroke work index (RVSWI) (≤ 0.25mmHg/l/m2), severe pre-VAD RV dysfunction, high creatinine level (≥1.9mg/dl), previous cardiac surgery, and hypotension (≤96mmHg) independently associated with the need for biventricular support. For each of these variables, if a patient met the “high risk” criteria, he or she was given a score of 1 for that variable. By calculating these risk factors together, Penn RVAD risk score was created: 18. (CI)+ 18. (RVSWI) + 17. (creatinine)+16. (previous cardiac surgery) +16. (RV dysfunction) +13. (systolic blood pressure). After analysis of this risk scoring, it was revealed that successful LVAD support was predicted in patients with a score below 50, while the probability of BiVAD placement was high in patients with a score of 50 and above (83% and 80% sensitivity and specificity, respectively).
In one of the previous study, which used multivariate logistic regression analysis, have pointed 3 preoperative factors that seemed were significantly associated with RVF after LVAD implantation: (1) need of intra-aortic balloon counterpulsation before the operation, (2) increased in pulmonary vascular resistance, and (3) the device implantation as a destination therapy [58]. The authors defined RVF (rate 44%) as the need for inhaled NO for >48 hours, the need for IV inotropes for >14 days, and/or RVAD implantation. The risk score (Utah RV Risk Score) was calculated as the sum of the points assigned for the existence some perioperative variables. Intra-aortic balloon counterpulsation (IABP), 4 points; pulmonary vascular resistance (PVR), quartile 1 (≤1.7 Wood units), 1 point; quartile 2 (1.8 –2.7 Wood units), 2 points; quartile 3 (2.8 – 4.2 Wood units), 3 points; and quartile 4 (≥4.3 Wood units), 4 points; inotrope dependency, 2.5 points; DT patients were given 3.5 points; beta-blocker, 2 points. angiotensin-converting enzyme inhibitor and/or angiotensin II receptor blocker, -2.5 points; and obesity, 2 points. The developed RVF risk score effectively predicted the risk of RV failure. They also showed that the presence of perioperative RVF was strongly associated with postoperative mortality in patients undergoing LVAD implantation. Additionally, their results revealed a significant reduction in survival at days 30, 180, and 365 after LVAD implantation using the risk score model. The subgroup with a risk score of 12.5 had significantly lower 1-year survival compared to the subgroups with a lower risk score.
Kormos et al. evaluated the incidence, risk factors, and effect on outcomes of right ventricular failure in patients implanted with continuous-flow LVAD (HeartMate II) [59]. RVF (rate 20%) is defined as RVAD that lasts >14 days after implantation, requires IV inotropes, and/or requires initiation of inotropic support more than 14 days after implantation. Multivariate analysis showed that central venous pressure/pulmonary capillary wedge pressure ratio (CVP/PCWP) greater than 0.63, need for preoperative ventilator support, and BUN level greater than 39 mg/dL were independent predictors of right ventricular failure after HeartMate II implantation. Authors also concluded that, rates of RVF and RVAD need in patients with the HeartMate II are low relative to previous results with pulsatile LVADs and support the use of new generation continuous flow device in end-stage heart failure.
In another study, Atluri et al. defined severe right ventricular dysfunction based on echocardiographic parameters, taking into account right ventricular contractility, tricuspid regurgitation, and tricuspid annular motion [60]. In multivariate logistic regression analysis, CVP>15 mmHg, severe RV dysfunction, preoperative intubation, severe Tricuspid regurgitation and Tachycardia were determined to be major criteria predicting the need for biventricular support. Based on this analysis, they established the CRITT score as a predictor of RVF. In the “CRITT” score, each of the five variables is given a score of 0 or 1. Ninety-three percent of patients with a score of 1 or lower underwent successful isolated LVAD therapy. However, 80% of patients with a score of 4 or above required biventricular assistance. They concluded that patients with a score of 2 or 3 were in the gray zone and could undergo isolated LVAD under appropriate pharmacological or temporary RVAD support. The ability to quickly calculate the CRITT score at the bedside without the need for complex calculations is an advantage that increases its applicability.
Many of the first proposed RV risk scoring systems did not use detailed imaging parameters to aid risk stratification. Raina et al. combined echocardiographic variables such as right ventricular fractional area change (RV FAC), left atrial (LA) volume index, and estimated right atrial (RA) pressure into an echocardiographic scoring system to estimate RVF [10]. Three points were assigned for LA volume index <38 mL/m2, 2 points for RV FAC <31%, and 2 points for estimated RA pressure >8 mm Hg. Thus, a score scale that can range from 0 to 7 points emerged. Prolonged RVF after LVAD implantation (rate 29%) was defined as the need for inotropes for more than 14 days after LVAD implantation or the need for temporary RVAD placement. Initial BiVAD criteria (rate 23%) were stated as severe RV dysfunction on transthoracic echocardiography, severe pulmonary hypertension with PVR >5 WU or RAP >15 mmHg, and persistence of ventricular arrhythmias causing hemodynamic instability. When RVF and non-RVF groups were compared, the echocardiographic score was significantly higher in the RVF group. They concluded that, combining echocardiographic variables into a simple easily interpreted echocardiographic scoring system significantly improved prediction of RVF versus any one echocardiographic variable alone, and, importantly, the echocardiographic score remained predictive after inclusion of clinical variables in multivariate models, despite the small sample size in their study.
After a while, a study from Germany proposed the ARVADE score, which consists of echocardiographic parameters ([61]. In this study, RVF (rate 57%) was defined as the need for placement of a temporary RVAD or the use of inotropic agents for at least 14 days. Multivariable analysis identified INTERMACS level 1, the Em/SLAT ratio ≥18.5 (Em: pulsed Doppler transmitral E wave; SLAT: tissue Doppler lateral systolic velocity), and the basal RVEDD ≥50 mm (right ventricular end-diastolic diameter) as independent predictors. An ARVADE score was calculated as the sum of points attributed according to the values of three variables: 3.0 points for Em/SLAT ≥ 18.5, 2.0 points for basal RVEDD≥50mm and 1.5 points for INTERMACS level 1. An ARVADE score >3.0 was predictive of post-implantation RVF, with a sensitivity of 89% and a specificity of 74%. Authors concluded that, the ARVADE score, calculated as the sum of scores for one clinical and three echocardiographic measures reflecting LV global systolic and diastolic dysfunction and RV congestion, may estimate suitability for LVAD implantation.
In 2018, Loforte et al. introduced a simple and easily memorized risk stratification tool (ALMA score) to determine whether isolated LVAD (continuous flow device) implantation could be tolerated in 258 patients from two centers [62]. Patients in the BiVAD cohort included those who had sudden RVF after isolated LVAD implantation and required early application of a temporary or long-term RV assist device (RVAD). Severe RVF defined as receiving short- or long-term right-sided circulatory support despite maximal dosage of continuous inotropic support and NO ventilation. A five-point risk score was developed based on the clinical variables identified in the multivariate logistic regression analysis. Then, 1 or 0 point was assigned for each of the variables in the institutionally defined “ALMA” score: Destination therapy (DT) intention, pulmonary artery pulsatility index (PAPi) <2, right ventricular stroke work index (RVSWi) <300 mm Hg/ml/m2, RV/ LV ratio >0.75, and Model for End-Stage Liver Disease Excluding International Normalized Ratio (MELD-XI) score >17. The predicted rate of RVF was increased from 9% for a score of less than 2, to 57% for a score of 2–3, and to 100% for a score of 4–5. In the resulting ROC curves, a score of 3 points provided sensitivity and specificity higher than 80% for the entire cohort. Based on this model, the Authors recommended isolated LVAD implantation for patients with a score of 0 or 1 and BiVAD for patients with a score of 4 or 5. They placed patients with a score of 2 in the gray area and stated that LVAD implantation could be performed for these patients accompanied by appropriate pharmacological and/or temporary RVAD support or tricuspid valve repair.
Historically, older RVF risk scores were developed in the era of pulsatile flow LVADs. The lack of validation studies has made it difficult for these models to accurately predict RVF in the current continuous-flow LVAD population. To more accurately predict RVF, models that use retrospective, predominantly single-center, primarily continuous-flow LVAD data have been developed. However, a common shortcoming of both old and new risk scoring models is that they are subject to limited external validation and had modest predictive value.
In 2018 Soliman et al. developed and validated a simple score to predict early RHF after continuous-flow LVAD implantation in a large population from the EUROMACS Registry [63]. Definition of RVF (rate 21.7%) was receiving short- or long-term RVAD support, continuous inotropic support for ≥14 days, and NO ventilation for ≥48 hours. They examined 82 potential preoperative predictors and CPB time as a operative variable for the association with RHF. The EUROMACS-RHF risk score is composed of severe RV dysfunction, 2 points; ratio of RA/PCWP ≥0.54, 2 points; advanced INTERMACS class 1-3, 2 points; need for ≥3 intravenous inotropes, 2.5 points; and hemoglobin ≤10 g/dL, 1 point. Composite 5-point score predicted early RHF after LVAD implantation; Moreover, as the score increased, the risk of both RHF and mortality increased. ROC curve analysis of the EUROMACS-RHF risk score was compared with previous risk scores and with individual known markers of RHF. They claimed that, The EUROMACS-RHF risk score outperformed previously published scores and known individual echocardiographic and hemodynamic markers of RHF. Finally, they validated the risk model in the validation cohort. The c index was 0.70 in the derivation versus 0.67 in the validation cohort. The Hosmer-Lemeshow goodness-of- fit P value was 0.61 in the validation cohort, which reflects an appropriate fit for the data in this cohort.
Early studies examining risk factors associated with RVF and developing various risk scores were generally based on the weighted sum of 4-7 risk factors contributing modest sensitivity or specificity. In addition, accurate prediction of patients at risk of RVF after LVAD implantation depends on the multidimensional and variable interaction of many perioperative variables that cannot be adequately captured by traditional multivariate modeling techniques. As a result, generalized recommendations for patient selection obtained from relatively small single-center patient groups have limited usefulness in practice.
Prediction models that we have summarized so far were conventional statistical analysis methods. As AI began proving itself more within healthcare, heart failure subgroups specific research increased as well, where considerable LVAD and heart transplant subjects related AI literature began populating journals more and more. Although studies mentioned above evaluated risk factors regarding post LVAD RHF, due to the fact that this is a multifactorial problem makes it especially hard to effectively investigate this issue properly through conventional means. It is for this reason that AI and ML enables a more comprehensive avenue of research on this topic.
2.2. AI based studies/risk scores
The use of Bayesian statistical modeling was proposed by Loghmanpour et al. to overcome the limited predictive capacity of risk scores obtained from existing multivariate analyses [64]. This recommendation of the Authors is based on the hypothesis that it is essential to consider the relationships and conditional probabilities between independent variables to achieve satisfactory statistical accuracy. In this context, Bayesian Network (BN) algorithms can account for nonlinear interactions between variables by identifying groups of risk factors and their conditional interdependencies. The Bayesian models reported in this study are particularly suitable for combining large sets of risk factors because they are based on conditional probabilities of the likelihood of RVF for a given combination of interrelated variables. The authors suggested that these algorithms better reflect prioritization of dynamic clinical information when using data provided by the INTERMACS registry. To the authors' knowledge, this is the first report of a prognostic RVF model following continuous-flow LVAD using the INTERMACS database and adopting ML methods for statistical analysis. They extracted 34 preoperative variables from INTERMACS data base of 10909 patients from 2006 to 2014 in order to predict RVF after LVAD implantation. The definition for RVF was based on the INTERMACS definition prior to 2014. Overall 2024 patients were diagnosed with RVF (18.5%), 293 with acute (<48 hours after implant) RVF (2.7%), 1036 with early (48 hours to 14 days) RVF (9.5%), and n=695 with late onset (>14 days) RVF (6.4%). Systolic PAP, pre-albumin, LDH and RVEF parameters were found to have the most predictive value among all the preoperative variables. The authors acknowledge that a retrospective study with incomplete data is not ideal for a more detailed analysis where RVF severity could have been also considered. Patients already considered too risky for LVAD implantation for RVF possibility and thus never received LVAD were unavoidably omitted from data set, perhaps skewing results.They analyzed accuracy, area under the ROC curve (AUC), sensitivity and specificity, respectively. According to their findings, The AUC of the Bayesian model was 0.90 for acute RV failure, 0.84 for early RV failure, and 0.88 for late RV failure after LVAD implantation, significantly outperformed all previously published risk scores.
In a 2018 study, Samura et al. utilized a supervised ML model in order to predict right ventricular assist device (RVAD) requirement for patients that will undergo LVAD implantations [65]. They used 42 preoperative clinical and hemodynamic parameters of 115 patients that proceeded to be implanted with a continuous flow LVAD between years 2013 and 2017. As a result of their study, 5 parameters were highlighted as having most predictive value, left ventricular end-diastolic dimension, left ventricular end-systolic dimension, left ventricular ejection fraction, etiology of dilated phase of hypertrophic cardiomyopathy, and less-distensible right ventricle. 8 different ML algorithms were tested in order to obtain the best results and they declared that a derived Naïve Bayes model achieved a great accuracy of 95 % and area under curve (AUC) of 0.85. Researchers concluded that this method was useful and feasible in order to preoperatively predict which patients would likely need RVAD implantation.
Bellavia et al. used ML approach to find out the association between regional right ventricular and right atrial strain for prediction of right ventricular failure in both early and late postoperatively period [66]. Michigan risk score along with CVP and apical longitudinal systolic strain of the right ventricular free wall were found to be the most important predictors of acute RHF. For the chronic RHF, the most prominent predictors were right ventricular free wall systolic strain of the middle segment, right atrial strain and tricuspid annular plane systolic excursion.
Shad et al. used combining greyscale video data and optical flow streams from the video data with a three dimensional 152-layer deep learning ML algorithm. 1909 scans from 723 patients were evaluated in order to predict RHF development of LVAD patients [67]. The researchers used two clinical risk score systems; CRITT and PENN scores to identified potential risky patients for RHF after LVAD implantation. Subsequently they compared their deep learning and ML systems performance of against to risk scores. The study included 941 LVAD patient; separated in two; group one (n:182) presented RHF, group two (n:541) without RHF. While the researchers checked the area under curve (AUC) they found that AUC of CRITT and PENN scores are 0,616 and 0,605 respectively. The AUC of their AI systems is 0,729 which means the newly developed deep learning system is presented more accuracy to predict of RHF. Although they worked with small and limited data set the results were challenging and on account of that they believed that AI will find wider working place in cardiovascular disease especially for doing prediction studies. They further argue that, when RVAD implantation is planned beforehand and perhaps concurrently with LVAD implantation as opposed to emergent RVAD implantation after patient condition deteriorates. Therefore, being able to predict eventual RHF development for patients before LVAD implantation will improve patient survivability.
In 2021, Kilic et al. utilized extreme gradient boosting which is an ensemble ML algorithm in order to investigate preoperative data association with postoperative adverse events which translates to 90 days and 1-year survival rates [68]. This study involved 16120 patients from 170 centers where the data set was acquired from INTERMACS. It includes patient demographics, comorbidities, laboratory parameters, clinic visit measurements, interval events during hospitalization prior to LVAD insertion, and concomitant operative procedures. Post-LVAD data collected in INTERMACS includes adverse events and survival. Examples to these adverse events include thrombosis, RHF, infection and bleeding. Reportedly, end result of this study found that there was an improvement of 48.8% (p<0.001) in 90-day mortality prediction and 36.9% (p<0.001) improvement in 1-year mortality prediction with ML compared to usual logistic regression data analysis. ML models derived using the XGBoost algorithm were well calibrated and had improved discrimination over logistic regression. Based on these findings, they concluded that ML may have an important role in risk prediction in LVAD treatment, both independently and in addition to traditional modeling approaches such as logistic regression. Further study that focuses on specific adverse events prediction, such as RHF, may be conducted in order to better understand the underlying mechanisms of these clinical outcomes and which would translate to creating a better patient treatment plan accordingly.
Using the statistical computing tool called “R”, Kilic et al. evaluated data from ENDURANCE trials in 2020, which included 564 patients [69]. This study aimed to analyze the risk of major adverse events after LVAD implantation and how they transitioned to each other. These events were device malfunction, bleeding, infection, neurological / renal / respiratory dysfunction and RHF. They identified that most common adverse events were bleeding and infection. Interestingly, they found that RHF is one of the top three adverse events, bleeding and infection being the other two, that leads to further adverse events most often. The highest transition probabilities were found to be infection to infection (0.34), bleeding to bleeding (0.31), RHF to bleeding (0.31), RHF to infection (0.28), and bleeding to infection (0.26). Additionally, they found that RHF has the lowest median time to first adverse event with 3.5 days. Highlighting the importance of RHF for overall mortality rates post LVAD implantation, Patients with RHF are shown to have 50% mortality rates. RHF was also identified to be significantly linked with bleeding and infections, which it then follows that RHF prediction is vital to successful long term LVAD patient survivability.
2550 patient data from International Registry for Mechanically Assisted Circulatory Support (IMACS) database were utilized by Nayak et al. in 2022 in order to analyze 41 pre-implant variables of patients with acute post LVAD RHF [70]. An unsupervised ML model was used in their work, identifying 4 RHF phenotypes, where severe shock phenotype had worst clinical outcomes. Ischemic cardiomyopathy (ICM) with low grade shock and non ICM without shock were two other phenotypes identified. Best clinical outcomes were observed with ICM without shock phenotype. The notion of classifying patients into phenotypes may prove useful for future researches as applying separate ML based prediction or analysis models to significantly differing pathophysiologies for RHF could improve predictive capabilities of pre-implant evaluations overall.
The study that designed by Bahl et al. was one of the newest studies which focused on ML and RHF [71]. They preferred an “explainable” ML method called Boosted Decision Trees for analyze the preimplant patient factors in nonlinear interactions with RHF after LVAD implantation. The study includes the patients in INTERMACS registry who were implanted with their first durable LVAD between 2008 to 2017. A total of 186 potential risk factors were analyzed from 19,595 patients as unbiased and comprehensively as possible. This study was aimed at better quantifying and understanding how different clinical variables impact each other and the complex mechanism that leads to RHF after LVAD implantation. The study showed that in 19.1% of patients severe RHF was developed within the first 30 days. Thirty top predictors of RHF were identified. INTERMACS profile, Model for End-stage Liver Disease score, the number of inotropic infusions, hemoglobin, and race were the first five top factors. Additionally, many of these top factors showed nonlinear relationships with key risk inflection points such as INTERMACS profile 2-3, right atrial pressure of 15 mmHg, pulmonary artery pressure index of 3, and prealbumin of 23mg/dl. They claimed that, ML offers a number of algorithms that are far more flexible and are well equipped for high dimensional, nonlinear, and interacting relationships. They also believed that this study could open new era for researchers to formulate patient optimization strategies before LVAD implantation.
Using a Convolutional Neural Network (U-Net), Just et al. evaluated preoperative CT scan data of 137 patients in order to assess their body composition and then predict postoperative major complications after LVAD implantation [72]. Body composition evaluation included visceral and subcutaneous adipose tissue areas, psoas and total abdominal muscle areas and sarcopenia. The body composition parameters were correlated with postoperative major complication rates, such as postoperative infections, in hospital mortality and overall quality of life. They found that Adipose tissue distribution / concentration was a good predictor of postoperative infections, in-hospital mortality, impaired 6-minute walking distance and quality of life within 6 months postoperatively. While the study focuses on all cause related outcome prediction, RHF is one of the poor outcome classes that is present in the data set. Therefore, a focus study on the usefulness of AI in RHF prediction using a similar data set might be warranted. Method and performance summary of reviewed publications presented in Table 1.
3. Discussion
Although LVADs became a preferred surgical option for advanced heart failure; undesired postoperative complications still occur with considerable prevalence [73].
RHF is one of the life-threatening complications with an incidence estimated nearly 10%-40%. Many studies were designed to find out the pathophysiology of post-LVAD RHF [74,75,76,77,78,79,80,81,82] Increased RV preload and concomitant septal shift towards to left ventricle is the most well-known mechanisms [83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100]. Previously published prediction models were used to find out the link between post-LVAD RHF and possible risk factors as in linear interaction.
However, like RHF is, some clinical situations usually present with complex clinical aspects that may force the clinicians think versatile to improve the outcomes. ML is a new challenging method start to use in cardiovascular disease especially for decision making, prediction scores and prognostication. Compared with conventional statistical methods that work to find out the correlations between risk factors and outcomes with mathematical equations, ML aims to discover association between multiple variables and outcomes using linear and nonlinear interaction ways. The advantages of the technique have covered the most of gaps in the research field and give more opinion for future studies.
In this comprehensive review we analyzed and summarize published studies which already took place in literature and aimed report the prediction of RHF after LVAD implantation using ML.
As we summarized the details of the studies above, there some points that should be emphasis to clarify the aim of the ML approaches. For instance, the design of the studies is the most important checkpoint which increases the study’s value. The results of multicenter planned studies appear to be stronger for researchers. For this purpose, Kiliç et al. conducted a multicenter research which included more than 15000 patient’s data acquired from INTERMACS database. It is not easy for statistical methods to compare very large variable factors with each other in an unbiased way to find the most predictable ones. Another favorable feature of AI studies is determined with echocardiographic scans. Shad et al. reported that, data obtained with the help of AI performed better compared to manually obtained echocardiographic measurements and clinical risk scores (CRITT and Penn).AI based system directly analyses the spaciotemporal information from cardiac walls and valves instead of segmental evaluation of cardiac chambers. Consequently, the misleading results getting by manually calculation of cardiac functions were eliminated. While they used the biggest data set of echocardiography, they also noted some limitations. Because of the study was planned retrospectively, the acquisition of the echocardiography remains unstandardized. Additionally, the timing of the last echocardiographic scans was not in the same timeline for all patients. Although their focused that pre-training large video dataset was the key point of the study, they have been noted that prospective evaluation and time line standardization would bring out much better estimation [67].
Beside of the echocardiographic images used for making prediction in LVAD patients, Berlin Heart center researchers reported an interesting study designed as find out the relationship between body composition and postoperative LVAD complications used AI techniques. Total of 137 patient were included in study who had underwent for CT scan before surgery. Their AI based evaluation of body composition demonstrated that higher patients with higher visceral adipose and subcutaneously adipose tissue suffer worse postoperative outcomes. This study given an opinion to use CTt scan images for prediction analysis in LVAD patients [72].
As we analyzed in this review, ML models showed excellent discrimination in predicting RHF after LVAD implantation. The majority of AI studies achieved AUC rates above 0.6 when compared to contemporary clinical risk scores. ML-based AI prediction models allow clinicians to make more efficient assessments and gain more predictive insight into whether they will suffer from RHF. Depends all reviewed studies we can say that ML techniques have potential to improve clinical decision making and patient selection to improve better outcomes.
4. Limitations
Our review has some limitations. Our research included only medical databases as mentioned above. Therefore, we understand that there are many other databases and it is probable that paramedical publications in other scientific fields like biomedical engineering and bioinformatics may exist.
5. Conclusion
RHF is a severe problem can occur after LVAD implantation. To make a prediction for selected patients may help to decrease the incidence and reach better outcomes with these patients. Nowadays the classical statistical methods are started to giving hand to AI techniques which overcome to linear evaluation studies. As we can conclude from this review, AI techniques have begun to take place in paramedical fields as well as in the most specific subjects of medicine. It would be a correct approach for clinicians not to stay away from these developments. Although they have limitations at some points, we believe that ML procedures will also improve with advances in AI and computational science. In our opinion in very nearly future more studies will be design with using AI techniques.
Author Contributions
Conceptualization, O.B., C.O., T.Y.; methodology, O.B, T.Y and D.U.O.; validation; T.Y.; formal analysis D.U.O. and T.Y.; investigations; O.B., C.O., T.Y.; resources, C.O., T.Y.; data curation, C.O. and O.B.; writing—original draft preparation, O.B., C.O. T.Y.; writing—review and editing O.B., C.O., T.Y.; visualization, C.O.; supervision, D.U.O., T.Y.; project administration D.U.O., O.B., T.Y. All authors have read and agreed to the published version of the manuscript.
Funding
The research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data is provided within the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008 Aug 5;52(6):428-34. [CrossRef] [PubMed]
- Francica A, Loforte A, Attisani M, Maiani M, Iacovoni A, Nisi T, et.al. Five-Year Outcome After Continuous Flow LVAD With Full-Magnetic (HeartMate 3) Versus Hybrid Levitation System (HeartWare): A Propensity-Score Matched Study From an All-Comers Multicentre Registry. Transpl Int. 2023 Sep 4;36:11675. Erratum in: Transpl Int. 2023 Oct 09;36:12088. [CrossRef] [PubMed]
- Grewal J, Tripathi N, Bortner B, Gregoski MJ, Cook D, Britt A, et.al. A multicenter evaluation of the HeartMate 3 risk score. J Heart Lung Transplant. 2023 Dec 6:S1053-2498(23)02156-3. Epub ahead of print. [CrossRef] [PubMed]
- Mehra MR, Netuka I, Uriel N, Katz JN, Pagani FD, Jorde UP, et.al; ARIES-HM3 Investigators. Aspirin and Hemocompatibility Events With a Left Ventricular Assist Device in Advanced Heart Failure: The ARIES-HM3 Randomized Clinical Trial. JAMA. 2023 Dec 12;330(22):2171-2181. [CrossRef] [PubMed]
- Kirschner M, Topkara VK, Sun J, Kurlansky P, Kaku Y, Naka Y, et.al. Comparing 3-Year Survival and Readmissions between HeartMate 3 and Heart Transplant as Primary Treatment for Advanced Heart Failure. J Thorac Cardiovasc Surg. 2023 Dec 26:S0022-5223(23)01207-2. Epub ahead of print. [CrossRef] [PubMed]
- Jorde UP, Saeed O, Koehl D, Morris AA, Wood KL, Meyer DM, et.al. The Society of Thoracic Surgeons Intermacs 2023 Annual Report: Focus on Magnetically Levitated Devices. Ann Thorac Surg. 2024 Jan;117(1):33-44. Epub 2023 Nov 8. [CrossRef] [PubMed]
- Puwanant S, Hamilton KK, Klodell CT, Hill JA, Schofield RS, Cleeton TS, et.al. Tricuspid annular motion as a predictor of severe right ventricular failure after left ventricular assist device implantation. J Heart Lung Transplant. 2008 Oct;27(10):1102-7. [CrossRef] [PubMed]
- Potapov EV, Krabatsch T, Ventura HO, Hetzer R. Advances in mechanical circulatory support: year in review. J Heart Lung Transplant. 2011 May;30(5):487-93. [CrossRef] [PubMed]
- Rich, JD. Right ventricular failure in patients with left ventricular assist devices. Cardiol Clin. 2012 May;30(2):291-302. [CrossRef] [PubMed]
- Raina A, Seetha Rammohan HR, Gertz ZM, Rame JE, Woo YJ, Kirkpatrick JN. Postoperative right ventricular failure after left ventricular assist device placement is predicted by preoperative echocardiographic structural, hemodynamic, and functional parameters. J Card Fail. 2013 Jan;19(1):16-24. [CrossRef] [PubMed]
- Kalogeropoulos AP, Kelkar A, Weinberger JF, Morris AA, Georgiopoulou VV, Markham DW, et.al. Validation of clinical scores for right ventricular failure prediction after implantation of continuous-flow left ventricular assist devices. J Heart Lung Transplant. 2015 Dec;34(12):1595-603. Epub 2015 Jun 1. [CrossRef] [PubMed]
- Neyer J, Arsanjani R, Moriguchi J, Siegel R, Kobashigawa J. Echocardiographic parameters associated with right ventricular failure after left ventricular assist device: A review. J Heart Lung Transplant. 2016 Mar;35(3):283-293. Epub 2016 Jan 6. [CrossRef] [PubMed]
- Kang G, Ha R, Banerjee D. Pulmonary artery pulsatility index predicts right ventricular failure after left ventricular assist device implantation. J Heart Lung Transplant. 2016 Jan;35(1):67-73. Epub 2015 Jun 17. Erratum in: J Heart Lung Transplant. 2017 Nov;36(11):1272. [CrossRef] [PubMed]
- Loforte A, Grigioni F, Marinelli G. The risk of right ventricular failure with current continuous-flow left ventricular assist devices. Expert Rev Med Devices. 2017 Dec;14(12):969-983. Epub 2017 Nov 25. [CrossRef] [PubMed]
- Mehra MR, Uriel N, Naka Y, Cleveland JC Jr, Yuzefpolskaya M, Salerno CT, et.al.; MOMENTUM 3 Investigators. A Fully Magnetically Levitated Left Ventricular Assist Device - Final Report. N Engl J Med. 2019 Apr 25;380(17):1618-1627. Epub 2019 Mar 17. [CrossRef] [PubMed]
- Løgstrup BB, Nemec P, Schoenrath F, Gummert J, Pya Y, Potapov E, et.al. Heart failure etiology and risk of right heart failure in adult left ventricular assist device support: the European Registry for Patients with Mechanical Circulatory Support (EUROMACS). Scand Cardiovasc J. 2020 Oct;54(5):306-314. Epub 2020 Jun 18. [CrossRef] [PubMed]
- Frankfurter C, Molinero M, Vishram-Nielsen JKK, Foroutan F, Mak S, Rao V, et.al. Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation: A Systematic Review. Circ Heart Fail. 2020 Oct;13(10):e006994. Epub 2020 Sep 28. [CrossRef] [PubMed]
- Varshney AS, DeFilippis EM, Cowger JA, Netuka I, Pinney SP, Givertz MM. Trends and Outcomes of Left Ventricular Assist Device Therapy: JACC Focus Seminar. J Am Coll Cardiol. 2022 Mar 22;79(11):1092-1107. [CrossRef] [PubMed]
- Saeed D, Feldman D, Banayosy AE, Birks E, Blume E, Cowger J, et.al. The 2023 International Society for Heart and Lung Transplantation Guidelines for Mechanical Circulatory Support: A 10- Year Update. J Heart Lung Transplant. 2023 Jul;42(7):e1-e222. Epub 2023 May 25. [CrossRef] [PubMed]
- Takeda K, Takayama H, Colombo PC, Yuzefpolskaya M, Fukuhara S, Han J, et.al. Incidence and clinical significance of late right heart failure during continuous-flow left ventricular assist device support. J Heart Lung Transplant. 2015 Aug;34(8):1024-32. Epub 2015 Mar 26. [CrossRef] [PubMed]
- Kapelios CJ, Charitos C, Kaldara E, Malliaras K, Nana E, Pantsios C, et.al. Late-onset right ventricular dysfunction after mechanical support by a continuous-flow left ventricular assist device. J Heart Lung Transplant. 2015 Dec;34(12):1604-10. Epub 2015 Jun 11. [CrossRef] [PubMed]
- Rich JD, Gosev I, Patel CB, Joseph S, Katz JN, Eckman PM, et.al; Evolving Mechanical Support Research Group (EMERG) Investigators. The incidence, risk factors, and outcomes associated with late right-sided heart failure in patients supported with an axial-flow left ventricular assist device. J Heart Lung Transplant. 2017 Jan;36(1):50-58. Epub 2016 Aug 20. [CrossRef] [PubMed]
- Rame JE, Pagani FD, Kiernan MS, Oliveira GH, Birati EY, Atluri P, et.al. Evolution of Late Right Heart Failure With Left Ventricular Assist Devices and Association With Outcomes. J Am Coll Cardiol. 2021 Dec 7;78(23):2294-2308. [CrossRef] [PubMed]
- Alkhunaizi FA, Azih NI, Read JM, Goldberg RL, Gulati AA, Scheel PJ 3rd, et.al. Characteristics and Predictors of Late Right Heart Failure After Left Ventricular Assist Device Implantation. ASAIO J. 2023 Mar 1;69(3):315-323. Epub 2022 Oct 2. [CrossRef] [PubMed]
- Rajapreyar I, Soliman O, Brailovsky Y, Tedford RJ, Gibson G, Mohacsi P, et.al. Late Right Heart Failure After Left Ventricular Assist Device Implantation: Contemporary Insights and Future Perspectives. JACC Heart Fail. 2023 Aug;11(8 Pt 1):865-878. Epub 2023 May 31. Erratum in: JACC Heart Fail. 2023 Aug;11(8 Pt 1):1035. [CrossRef] [PubMed]
- Shah P, Yuzefpolskaya M, Hickey GW, Breathett K, Wever-Pinzon O, Ton VK, et.al. Twelfth Interagency Registry for Mechanically Assisted Circulatory Support Report: Readmissions After Left Ventricular Assist Device. Ann Thorac Surg. 2022 Mar;113(3):722-737. Epub 2022 Jan 7. [CrossRef] [PubMed]
- Hall SA, Copeland H, Alam A, Joseph SM. The "Right" Definition for Post-Left Ventricular Assist Device Right Heart Failure: The More We Learn, the Less We Know. Front Cardiovasc Med. 2022 Apr 26;9:893327. [CrossRef] [PubMed]
- Ochiai Y, McCarthy PM, Smedira NG, Banbury MK, Navia JL, Feng J, et.al. Predictors of severe right ventricular failure after implantable left ventricular assist device insertion: analysis of 245 patients. Circulation. 2002 Sep 24;106(12 Suppl 1):I198-202. [PubMed]
- Kavarana MN, Pessin-Minsley MS, Urtecho J, Catanese KA, Flannery M, Oz MC, et.al.. Right ventricular dysfunction and organ failure in left ventricular assist device recipients: a continuing problem. Ann Thorac Surg. 2002 Mar;73(3):745-50. [CrossRef] [PubMed]
- Dang NC, Topkara VK, Mercando M, Kay J, Kruger KH, Aboodi MS, et.al. Right heart failure after left ventricular assist device implantation in patients with chronic congestive heart failure. J Heart Lung Transplant. 2006 Jan;25(1):1-6. Epub 2005 Dec 9. [CrossRef] [PubMed]
- Craig, ML. Management of right ventricular failure in the era of ventricular assist device therapy. Curr Heart Fail Rep. 2011 Mar;8(1):65-71. [CrossRef] [PubMed]
- Kukucka M, Potapov E, Stepanenko A, Weller K, Mladenow A, Kuppe H, et.al. Acute impact of left ventricular unloading by left ventricular assist device on the right ventricle geometry and function: effect of nitric oxide inhalation. J Thorac Cardiovasc Surg. 2011 Apr;141(4):1009-14. [CrossRef] [PubMed]
- Grant AD, Smedira NG, Starling RC, Marwick TH. Independent and incremental role of quantitative right ventricular evaluation for the prediction of right ventricular failure after left ventricular assist device implantation. J Am Coll Cardiol. 2012 Aug 7;60(6):521-8. [CrossRef] [PubMed]
- Kanwar MK, Lohmueller LC, Kormos RL, Teuteberg JJ, Rogers JG, Lindenfeld J, et.al. A Bayesian Model to Predict Survival After Left Ventricular Assist Device Implantation. JACC Heart Fail. 2018 Sep;6(9):771-779. [CrossRef] [PubMed]
- Kirklin JK, Naftel DC, Kormos RL, Stevenson LW, Pagani FD, Miller MA, et.al. The Fourth INTERMACS Annual Report: 4,000 implants and counting. J Heart Lung Transplant. 2012 Feb;31(2):117-26. [CrossRef] [PubMed]
- Holman, WL. Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS): what have we learned and what will we learn? Circulation. 2012 Sep 11;126(11):1401-6. [CrossRef] [PubMed]
- Argiriou M, Kolokotron SM, Sakellaridis T, Argiriou O, Charitos C, Zarogoulidis P, et.al. Right heart failure post left ventricular assist device implantation. J Thorac Dis. 2014 Mar;6 Suppl 1(Suppl 1):S52-9. [CrossRef] [PubMed]
- Mehra MR, Park MH, Landzberg MJ, Lala A, Waxman AB; International Right Heart Failure Foundation Scientific Working Group. Right heart failure: toward a common language. J Heart Lung Transplant. 2014 Feb;33(2):123-6. [CrossRef] [PubMed]
- Kormos RL, Antonides CFJ, Goldstein DJ, Cowger JA, Starling RC, Kirklin JK, et.al. Updated definitions of adverse events for trials and registries of mechanical circulatory support: A consensus statement of the mechanical circulatory support academic research consortium. J Heart Lung Transplant. 2020 Aug;39(8):735-750. [CrossRef] [PubMed]
- Morgan JA, John R, Lee BJ, Oz MC, Naka Y. Is severe right ventricular failure in left ventricular assist device recipients a risk factor for unsuccessful bridging to transplant and post-transplant mortality. Ann Thorac Surg. 2004 Mar;77(3):859-63. [CrossRef] [PubMed]
- Takeda K, Naka Y, Yang JA, Uriel N, Colombo PC, Jorde UP, et.al. Outcome of unplanned right ventricular assist device support for severe right heart failure after implantable left ventricular assist device insertion. J Heart Lung Transplant. 2014 Feb;33(2):141-8. [CrossRef] [PubMed]
- Subramani S, Sharma A, Arora L, Hanada S, Krishnan S, Ramakrishna H. Perioperative Right Ventricular Dysfunction: Analysis of Outcomes. J Cardiothorac Vasc Anesth. 2022 Jan;36(1):309-320. [CrossRef] [PubMed]
- Ali HR, Kiernan MS, Choudhary G, Levine DJ, Sodha NR, Ehsan A, et.al. Right Ventricular Failure Post-Implantation of Left Ventricular Assist Device: Prevalence, Pathophysiology, and Predictors. ASAIO J. 2020 Jun;66(6):610-619. [CrossRef] [PubMed]
- Lo Coco V, De Piero ME, Massimi G, Chiarini G, Raffa GM, Kowalewski M, et.al. Right ventricular failure after left ventricular assist device implantation: a review of the literature. J Thorac Dis. 2021 Feb;13(2):1256-1269. [CrossRef] [PubMed]
- Bravo CA, Navarro AG, Dhaliwal KK, Khorsandi M, Keenan JE, Mudigonda P, et.al. Right heart failure after left ventricular assist device: From mechanisms to treatments. Front Cardiovasc Med. 2022 Oct 19;9:1023549. [CrossRef] [PubMed]
- Chamogeorgakis T, Toumpoulis I, Bonios MJ, Lanfear D, Williams C, Koliopoulou A, et.al. Treatment Strategies and Outcomes of Right Ventricular Failure Post Left Ventricular Assist Device Implantation: An INTERMACS Analysis. ASAIO J. 2023 Nov 27. [CrossRef] [PubMed]
- Harnad S. (2008) The Annotation Game: On Turing (1950) on Computing, Machinery, and Intelligence (PUBLISHED VERSION BOWDLERIZED). In, Epstein, Robert, Roberts, Gary and Beber, Grace (eds.) Parsing the Turing Test: Philosophical and Methodological Issues in the Quest for the Thinking Computer. Evolving Consciousness (01/01/08) Springer, pp. 23-66.
- Russell SJ, Norvig P. (2021). Artificial Intelligence: A Modern Approach (4th ed.). Hoboken: Pearson. ISBN 9780134610993.
- Mitchell TM (1997). Machine learning. McGraw-Hill. [CrossRef]
- Bishop CM (2006). Pattern Recognition and Machine Learning. Springer New York, NY. ISBN: 978-1-4939-3843-8.
- Mohri M, Rostamizadeh A, Talwalkar A. (2012). Foundations of Machine Learning. The MIT Press. ISBN 9780262018258.
- Nichols JA, Herbert Chan HW, Baker MAB. Machine learning: applications of artificial intelligence to imaging and diagnosis. Biophys Rev. 2019 Feb;11(1):111-118. [CrossRef] [PubMed]
- Quer G, Arnaout R, Henne M, Arnaout R. Machine Learning and the Future of Cardiovascular Care: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021 Jan 26;77(3):300-313. [CrossRef] [PubMed]
- Mortazavi BJ, Downing NS, Bucholz EM, Dharmarajan K, Manhapra A, Li SX, et.al. Analysis of Machine Learning Techniques for Heart Failure Readmissions. Circ Cardiovasc Qual Outcomes. 2016 Nov;9(6):629-640. [CrossRef] [PubMed]
- Folkert W Asselbergs, Alan G Fraser, Artificial intelligence in cardiology: the debate continues, European Heart Journal - Digital Health, Volume 2, Issue 4, December 2021, Pages 721–726. [CrossRef]
- Matthews JC, Koelling TM, Pagani FD, Aaronson KD. The right ventricular failure risk score a pre-operative tool for assessing the risk of right ventricular failure in left ventricular assist device candidates. J Am Coll Cardiol. 2008;51:2163–72.
- Fitzpatrick JR 3rd, Frederick JR, Hsu VM, Kozin ED, O'Hara ML, Howell E, et.al. Risk score derived from pre-operative data analysis predicts the need for biventricular mechanical circulatory support. J Heart Lung Transplant. 2008 Dec;27(12):1286-92. [CrossRef] [PubMed]
- Drakos SG, Janicki L, Horne BD, Kfoury AG, Reid BB, Clayson S, et.al. Risk factors predictive of right ventricular failure after left ventricular assist device implantation. Am J Cardiol. 2010 Apr 1;105(7):1030-5. [CrossRef] [PubMed]
- Kormos RL, Teuteberg JJ, Pagani FD, Russell SD, John R, Miller LW, et.al; HeartMate II Clinical Investigators. Right ventricular failure in patients with the HeartMate II continuous-flow left ventricular assist device: incidence, risk factors, and effect on outcomes. J Thorac Cardiovasc Surg. 2010 May;139(5):1316-24. [CrossRef] [PubMed]
- Atluri P, Goldstone AB, Fairman AS, MacArthur JW, Shudo Y, Cohen JE, et.al. Predicting right ventricular failure in the modern, continuous flow left ventricular assist device era. Ann Thorac Surg. 2013 Sep;96(3):857-63; discussion 863-4. [CrossRef] [PubMed]
- Aissaoui N, Salem JE, Paluszkiewicz L, Morshuis M, Guerot E, Gorria GM, Fagon JY et.al. Assessment of right ventricular dysfunction predictors before the implantation of a left ventricular assist device in end-stage heart failure patients using echocardiographic measures (ARVADE): Combination of left and right ventricular echocardiographic variables. Arch Cardiovasc Dis. 2015 May;108(5):300-9. [CrossRef] [PubMed]
- Loforte A, Montalto A, Musumeci F, Amarelli C, Mariani C, Polizzi V, et.al. Calculation of the ALMA Risk of Right Ventricular Failure After Left Ventricular Assist Device Implantation. ASAIO J. 2018 Nov/Dec;64(6):e140-e147.
- Soliman OII, Akin S, Muslem R, Boersma E, Manintveld OC, Krabatsch T, et.al.; EUROMACS Investigators. Derivation and Validation of a Novel Right-Sided Heart Failure Model After Implantation of Continuous Flow Left Ventricular Assist Devices: The EUROMACS (European Registry for Patients with Mechanical Circulatory Support) Right-Sided Heart Failure Risk Score. Circulation. 2018 Feb 27;137(9):891-906.
- Loghmanpour NA, Kormos RL, Kanwar MK, Teuteberg JJ, Murali S, Antaki JF. A Bayesian Model to Predict Right Ventricular Failure Following Left Ventricular Assist Device Therapy. JACC Heart Fail. 2016 Sep;4(9):711-21. [CrossRef] [PubMed]
- Samura T, Asanoi H, Toda K, Miyagawa S, Yoshikawa Y, Hata H, et.al. Prediction of Right Ventricular Failure After Left Ventricular Assist Device Implantation Using Machine Learning of Preoperative Hemodynamics. Circulation.2018;138,15318.
- Bellavia D, Iacovoni A, Agnese V, Falletta C, Coronnello C, Pasta S, et.al. Usefulness of regional right ventricular and right atrial strain for prediction of early and late right ventricular failure following a left ventricular assist device implant: A machine learning approach. Int J Artif Organs. 2020 May;43(5):297-314. [CrossRef] [PubMed]
- Shad R, Quach N, Fong R, Kasinpila P, Bowles C, Castro M, et.al. Predicting post-operative right ventricular failure using video-based deep learning. Nat Commun. 2021 Aug 31;12(1):5192. [CrossRef] [PubMed]
- Kilic A, Dochtermann D, Padman R, Miller JK, Dubrawski A. Using machine learning to improve risk prediction in durable left ventricular assist devices. PLoS One. 2021 Mar 10;16(3):e0247866. [CrossRef] [PubMed]
- Kilic A, Macickova J, Duan L, Movahedi F, Seese L, Zhang Y, at.al. Machine Learning Approaches to Analyzing Adverse Events Following Durable LVAD Implantation. Ann Thorac Surg. 2021 Sep;112(3):770-777. [CrossRef] [PubMed]
- Nayak A, Hu Y, Patel KJ, Ko Y, Okoh AK, Wang J, et.al. Machine Learning Algorithms Identify Distinct Phenotypes of Right Heart Failure After Left Ventricular Assist Device Implant. J Heart Lung Transplant. 2022:41(4), S39.
- Bahl A, Qureshi B, Zhang K, Bravo C, Mahr C, Li S. Explainable Machine Learning Analysis of Right Heart Failure After Left Ventricular Assist Device Implantation. ASAIO J. 2023 ;69(5):417-423. [CrossRef] [PubMed]
- Just IA, Schoenrath F, Roehrich L, Heil E, Stein J, Auer TA, et.al. Artificial intelligence-based analysis of body composition predicts outcome in patients receiving long-term mechanical circulatory support. J Cachexia Sarcopenia Muscle. 2023 Dec 26. [CrossRef] [PubMed]
- Gautam N, Ghanta SN, Clausen A, Saluja P, Sivakumar K, Dhar G, et.al. Contemporary Applications of Machine Learning for Device Therapy in Heart Failure. JACC Heart Fail. 2022 Sep;10(9):603-622. [CrossRef] [PubMed]
- Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008 Mar 18;117(11):1436-48. [CrossRef] [PubMed]
- Lampert BC, Teuteberg JJ. Right ventricular failure after left ventricular assist devices. J Heart Lung Transplant. 2015 Sep;34(9):1123-30. [CrossRef] [PubMed]
- Konstam MA, Kiernan MS, Bernstein D, Bozkurt B, Jacob M, Kapur NK, et.al; American Heart Association Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; and Council on Cardiovascular Surgery and Anesthesia. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement From the American Heart Association. Circulation. 2018 May 15;137(20):e578-e622. [CrossRef] [PubMed]
- El Hajj MC, Viray MC, Tedford RJ. Right Heart Failure: A Hemodynamic Review. Cardiol Clin. 2020 May;38(2):161-173. [CrossRef] [PubMed]
- Wang TS, Cevasco M, Birati EY, Mazurek JA. Predicting, Recognizing, and Treating Right Heart Failure in Patients Undergoing Durable LVAD Therapy. J Clin Med. 2022 ;11(11):2984. 25 May. [CrossRef] [PubMed]
- Cheng RK, Deng MC, Tseng CH, Shemin RJ, Kubak BM, MacLellan WR. Risk stratification in patients with advanced heart failure requiring biventricular assist device support as a bridge to cardiac transplantation. J Heart Lung Transplant. 2012 Aug;31(8):831-8. [CrossRef] [PubMed]
- Lo C, Murphy D, Summerhayes R, Quayle M, Burrell A, Bailey M, et.al. Right ventricular failure after implantation of continuous flow left ventricular assist device: analysis of predictors and outcomes. Clin Transplant. 2015 Sep;29(9):763-70. [CrossRef] [PubMed]
- Shiga T, Kinugawa K, Imamura T, Kato N, Endo M, Inaba T, et.al. Combination evaluation of preoperative risk indices predicts requirement of biventricular assist device. Circ J. 2012;76(12):2785-91. [CrossRef] [PubMed]
- Kurihara C, Critsinelis AC, Kawabori M, Sugiura T, Loor G, Civitello AB, et.al. Frequency and Consequences of Right-Sided Heart Failure After Continuous-Flow Left Ventricular Assist Device Implantation. Am J Cardiol. 2018 Feb 1;121(3):336-342. [CrossRef] [PubMed]
- Farrar DJ, Chow E, Wood JR, Hill JD. Anatomic interaction between the right and left ventricles during univentricular and biventricular circulatory support. ASAIO Trans. 1988 Jul-Sep;34(3):235-40. [PubMed]
- Moon MR, Bolger AF, DeAnda A, Komeda M, Daughters GT 2nd, Nikolic SD, et.al. Septal function during left ventricular unloading. Circulation. 1997 Mar 4;95(5):1320-7. [CrossRef] [PubMed]
- Feneley MP, Gavaghan TP, Baron DW, Branson JA, Roy PR, Morgan JJ. Contribution of left ventricular contraction to the generation of right ventricular systolic pressure in the human heart. Circulation. 1985 Mar;71(3):473-80. [CrossRef] [PubMed]
- Starling MR, Walsh RA, Dell'Italia LJ, Mancini GB, Lasher JC, Lancaster JL. The relationship of various measures of end-systole to left ventricular maximum time-varying elastance in man. Circulation. 1987 Jul;76(1):32-43. [CrossRef] [PubMed]
- Brown KA, Ditchey RV. Human right ventricular end-systolic pressure-volume relation defined by maximal elastance. Circulation. 1988 Jul;78(1):81-91. [CrossRef] [PubMed]
- Goldstein JA, Barzilai B, Rosamond TL, Eisenberg PR, Jaffe AS. Determinants of hemodynamic compromise with severe right ventricular infarction. Circulation. 1990 Aug;82(2):359-68. [CrossRef] [PubMed]
- Morgan JA, Paone G, Nemeh HW, Murthy R, Williams CT, Lanfear DE, et.al. Impact of continuous-flow left ventricular assist device support on right ventricular function. J Heart Lung Transplant. 2013 Apr;32(4):398-403. [CrossRef] [PubMed]
- Sunagawa K, Sagawa K, Maughan WL. Ventricular interaction with the loading system. Ann Biomed Eng. 1984;12(2):163-89. [CrossRef] [PubMed]
- Meineri M, Van Rensburg AE, Vegas A. Right ventricular failure after LVAD implantation: prevention and treatment. Best Pract Res Clin Anaesthesiol. 2012 Jun;26(2):217-29. [CrossRef] [PubMed]
- Pagani FD, Miller LW, Russell SD, Aaronson KD, John R, Boyle AJ, et.al; HeartMate II Investigators. Extended mechanical circulatory support with a continuous-flow rotary left ventricular assist device. J Am Coll Cardiol. 2009 Jul 21;54(4):312-21. [CrossRef] [PubMed]
- Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, et.al; HeartMate II Investigators. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. 2009 Dec 3;361(23):2241-51. Erratum in: N Engl J Med. 2018 Aug 16;379(7):697. [CrossRef] [PubMed]
- Van Meter CH Jr. Right heart failure: best treated by avoidance. Ann Thorac Surg. 2001 Mar;71(3 Suppl):S220-2. [CrossRef] [PubMed]
- Patlolla B, Beygui R, Haddad F. Right-ventricular failure following left ventricle assist device implantation. Curr Opin Cardiol. 2013 Mar;28(2):223-33. [CrossRef] [PubMed]
- Fitzpatrick JR 3rd, Frederick JR, Hiesinger W, Hsu VM, McCormick RC, Kozin ED, et.al. Early planned institution of biventricular mechanical circulatory support results in improved outcomes compared with delayed conversion of a left ventricular assist device to a biventricular assist device. J Thorac Cardiovasc Surg. 2009 Apr;137(4):971-7. [CrossRef] [PubMed]
- Tedford RJ, Hemnes AR, Russell SD, Wittstein IS, Mahmud M, Zaiman AL, et.al, Champion HC. PDE5A inhibitor treatment of persistent pulmonary hypertension after mechanical circulatory support. Circ Heart Fail. 2008 Nov;1(4):213-9. [CrossRef] [PubMed]
- Baumwol J, Macdonald PS, Keogh AM, Kotlyar E, Spratt P, Jansz P, et.al. Right heart failure and "failure to thrive" after left ventricular assist device: clinical predictors and outcomes. J Heart Lung Transplant. 2011 Aug;30(8):888-95. [CrossRef] [PubMed]
- Deswarte G, Kirsch M, Lesault PF, Trochu JN, Damy T. Right ventricular reserve and outcome after continuous-flow left ventricular assist device implantation. J Heart Lung Transplant. 2010 Oct;29(10):1196-8. [CrossRef] [PubMed]
- Lietz K, Long JW, Kfoury AG, Slaughter MS, Silver MA, Milano CA, et.al. Outcomes of left ventricular assist device implantation as destination therapy in the post-REMATCH era: implications for patient selection. Circulation. 2007 Jul 31;116(5):497-505. [CrossRef] [PubMed]
Figure 1.
A flowchart visually explaining machine learning process.
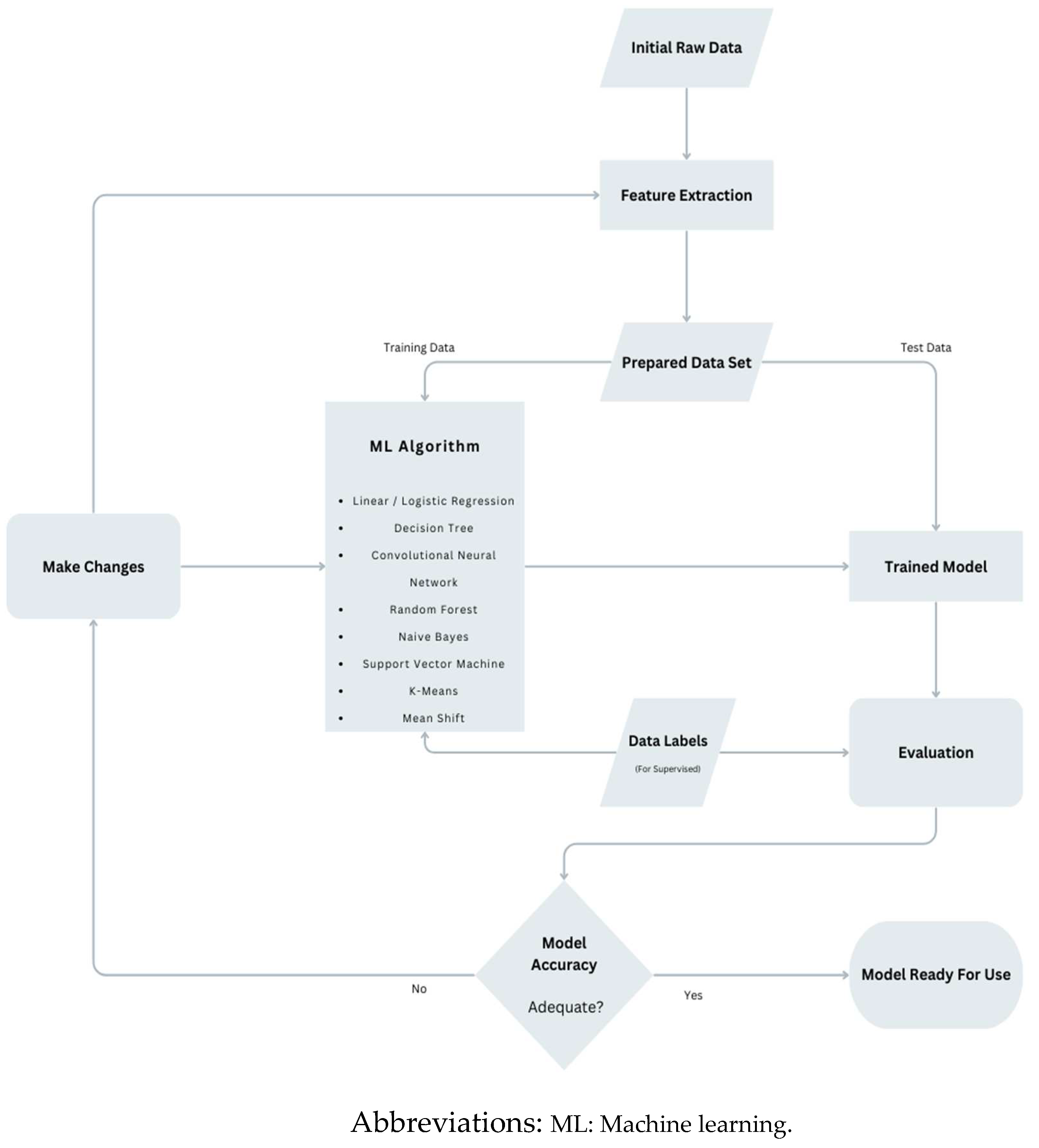

Table 1.
Method and performance summary of reviewed publications.
| Authors (et. al.) | Year | Title | Data Source | Findings |
| Loghmanpour [64] | 2016 | A Bayesian Model to Predict RVF following LVAD Therapy | INTERMACS data | Systolic PAP, pre-albumin, LDH and RV EF most predictive preoperative variables. AUC for acute, early, late RHF prediction between 0.83–0.90 sensitivity of 90% |
| Samura [65] | 2018 | Prediction of RVF after left LVAD implantation using ML of preoperative hemodynamics | Preoperative clinical and hemodynamic parameters | Prediction accuracy 95%, AUC 0.85 |
| Bellavia [66] | 2020 | Usefulness of regional RV and right atrial strain for prediction of early and late RVF following a LVAD implant: A ML approach | Biomarkers, Echocardiography, cath-lab measurements | Significant Predictors: Michigan risk score, CVP, systolic strain of RV free wall. ROC AUC 0.95 |
| Shad [67] | 2021 | Predicting post-operative RVF using video-based deep learning | Preoperative Echocardiography video | ML AUC 0.729, CRITT AUC 0.616, Penn AUC 0.605 |
| Kilic [68] | 2021 | Using ML to improve risk prediction in durable LVAD | INTERMACS data | 48.8% and 36.9% in 90-day and 1-year mortality prediction improvement with ML compared to usual logistic regression data analysis |
| Kilic [69] | 2021 | ML Approaches to Analyzing Adverse Events Following Durable LVAD Implantation | ENDURANCE trials | Bleeding, infection and RHF most common postoperative adverse events. RHF has strong transitive relationship with bleeding and infection |
| Nayak [70] | 2022 | ML Algorithms Identify Distinct Phenotypes of RHF After LVAD Implant | IMACS data | 4 post LVAD RHF phenotypes identified Clinical outcomes evaluated |
| Bahl [71] | 2023 | Explainable ML Analysis of RHF After LVAD Implantation | INTERMACS data | 5 best predictors identified Non-linear relationships identified |
| Just [72] | 2023 | AI-based analysis of body composition predicts outcome in patients receiving long-term MCS | Preoperative CT Scan | Adipose tissue as indicator for postoperative major complications. |
Abbreviations: RVF: Right ventricular failure; LVAD: Left ventricular assist device; INTERMACS: The Interagency Registry for Mechanically Assisted Circulatory Support; PAP: Pulmonary artery pressure; LDH: Lactate dehydrogenase; RV EF: Right ventricular ejection fraction; AUC: Area under the ROC Curve; RHF: Right heart failure; ML: Machine learning; CVP: Central venous pressure; ROC: Receiver operating characteristic; IMACS; International Registry for Mechanically Assisted Circulatory Support; MCS; Mechanical circulatory support; CT: Computed tomography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



