
Submitted:
03 January 2024
Posted:
04 January 2024
You are already at the latest version
Abstract
Sleep is of vital necessity for health, it has a restorative and protective function for children and adolescents with chronic conditions and their families. The purpose was to identify the scientific production on sleep patterns in children and adolescents with chronic conditions and their families. This integrative review was developed in March and June 2022, of the MEDLINE, Web of Science, CINAHL and PSYCInfo. The articles included were original papers published be-tween January 2007 and mid-2022. Excluded were review studies that did not evaluate sleep and whose participants did not have chronic conditions or were not children, adolescents and/or their families. The searches returned 814 abstracts. After exclusions, 47 studies were selected to be read in full; of these, 29 were selected and were grouped empirically into four categories: major alterations in sleep patterns of children and adolescents with chronic conditions; the relationship between sleep disorders and symptoms in children and adolescents with chronic conditions; impaired sleep patterns of families of children and adolescents with chronic conditions; sleep alterations and their relationship with other problems in families of children and adolescents with chronic conditions. All studies showed sleep pattern impairment in children and adolescents with chronic conditions and their families.
Keywords:
child
; adolescent
; family
; chronic disease
; sleep-wake disorders
1. Introduction
Chronic conditions are increasingly common in populations worldwide, including among children and young people [1]. The resulting altered routines, use of technologies and medicines, adverse effects, coping with numerous symptoms and lengthy hospital stays all make sleep disturbances a common problem impairing the quality of life of children, adolescents and their families [2].
Sleep meets a basic human need in maintaining wellbeing. Especially in children and adolescents, recurrent sleep interruptions can interfere with growth, development, learning and health [2,3], while in adults, they can lead to psychological disorders, cognitive deficit, metabolic alterations, obesity, hypertension and diabetes [4,5].
In children with chronic conditions, the major sleep disorders are impaired sleep quality and hygiene and difficulty falling asleep. In hospital, children also tend to sleep less, because of diagnosis- and care-related factors [6].
Major sleep alterations in adults include: insomnia, breathing-related sleep disorders, central disorders of hypersomnolence, parasomnias, Circadian rhythm sleep disorders and sleep-related movements disorders [7].
The consequences of experiencing sleep disorders also include intensified symptoms such as pain, fatigue, behavioural problems, anxiety, depression, aggression and withdrawal [8].
Children’s illness and hospitalisation also alter their families routines, leading to burnout and physical, mental and social problems. Providing 24-hour care also leads to modifications in families’ sleep patterns, placing them at risk of health problems and threatening their ability to provide care [9].
In that light, this article aimed to identify the scientific production in the literature on sleep patterns in children and adolescents with chronic health conditions and their families.
2. Materials and Methods
An integrative review [10] in the following stages: identifying the topic and selecting the review question; establishing inclusion and exclusion criteria; specifying the information to be extracted and categorising the studies; evaluating the studies included; interpreting the findings; and synthesising the knowledge [11].
The review question was: “What are sleep patterns like in children and adolescents with chronic conditions and their families?”, which was formulated using the PICo [12], with “P” corresponding to the population/problem (children, adolescents and their families); “I”, to the phenomenon of interest (sleep pattern); and “C”, to the context (chronic condition).
Data were collected between March and July 2022. The data bases searched were MEDLINE® (via PubMed®), Web of Science, Cumulative Index of Nursing and Allied Health (CINAHL) and PSYCInfo. The standard search strategy, using controlled descriptors and alternative terms identified in Medical Subject Headings (MESH), was: (Child OR Children OR Adolescent OR Adolescents OR Teen OR Teenager OR Youth) AND (“Chronic Disease” OR “Chronic Diseases” OR “Disease, Chronic” OR “Chronic Illness” OR “Illness, Chronic” OR “Chronic condition” OR “Chronic Conditions") AND (Sleep OR “Sleep patterns” OR “Sleep Habits” OR “Sleep Wake Disorders” OR “Sleep Wake Disorder” OR “Wake Disorders, Sleep” OR “Sleep Disorders” OR “Sleep Disorder”) AND (Caregivers OR Caregiver OR Parents OR Family OR “Family Caregiver” OR Families OR “Family Members”). Also, the terms “Child, Preschool”, Infant and Adolescence, found in the CINAHL Headings, were added for the search of the CINAHL base, and the terms “Child Health” and “Adolescent Health”, found in the APA Thesaurus, were added for the search of the PSYCInfo base. Other articles were included by active searching.
Original research studies published between January 2007 and June 2022 were included, considering the most recent publication of the American Academy of Sleep guide to using actigraphy, which stipulated in 2007 that “actigraphy is indicated to delineate sleep patterns and document responses to treatment in normal infants and children and in special pediatric populations” [13]. The criteria excluded review studies, editorials and abstracts that did not evaluate sleep, whose participants had no chronic condition or which were not conducted with children, adolescents or their families.
Two of the authors, working independently, made a detailed reading of the titles and abstracts to as to assure that the text addressed the guiding question and met the inclusion and exclusion criteria. In cases of doubt, it was opted to include the publication and make the selection decision after reading the article in full.
Descriptive data analysis was carried out using a chart, created by the research group for data extraction and synthesis, containing the following information: article citation, country of origin, authors’ field, objectives, subjects, study method and sleep assessment instruments used, level of evidence and main findings. That chart made it possible to compare and organise the data, which were analysed and grouped into categories [14]. Level of evidence was identified on the basis of the study design, following [15]).
3. Results
The data base searches returned 814 references: 305 in MEDLINE® via PubMed®, 115 in CINAHL, 259 in Web of Science and 135 in PSYCInfo. After exclusion of 767 articles, 47 studies were selected to be read in full, of which 27 were retained in the results of this review. A further two articles were added by active search (Figure 1).
Studies were found in all years except 2021 and 2022. Prevalence was highest in 2019, when four studies were published [16,17,18,19].
As regards the countries where studies were conducted, the United States (USA) predominated, with 11 studies [20,21,22,23,24,25,26,27,28,29,30,31]. Of particular note were two multicentre studies, one in Brazil and the USA [32] and the other, in Brazil, Portugal and the USA [17].
Authors’ professional backgrounds were primarily in Medicine, in 14 studies [18,19,22,24,26,28,31,33,34,35,36,37,38,39], followed by Nursing, in six studies [17,25,29,32,40,41]. Interdisciplinary publications were also found, involving Nursing, Social Service and Medicine [16], Psychology and Medicine [23], Physiotherapy and Medicine [42] and Nursing and Medicine [30].
Study designs included: 15 qualitative or descriptive studies [16,17,18,21,22,23,25,29,30,32,33,34,36,37,39,40,43], 13 case-control or cross-sectional studies [19,26,27,28,31,35,38,41,42,44,45] and one non-randomised controlled study [20,24].
The most common chronic condition was cancer, addressed in five studies [17,18,23,30,32], followed, in three studies each, by Duchenne muscular dystrophy [35,44,45], chronic kidney disease [19,24,28], asthma [25,26,38] and cystic fibrosis [22,37,42].
The instruments most commonly used to assess sleep (Table 1) were the Pittsburgh sleep quality index (15 studies) [16,19,23,27,34,35,37,38,39,40,41,42,43,44,45], the sleep diary (5) [20,21,25,29,30,43] and actigraphy (5) [17,26,29,32,41].
Lastly, the studies selected were grouped empirically into four categories.
3.1. Category 1: major alterations in the sleep patterns of children and adolescents with chronic conditions
Eleven of the articles selected were included in this category.
One study of children (11 to 13 years old) with chronic diseases, such as asthma, epilepsy and diabetes, showed that they had more trouble falling and staying asleep than healthy children [33].
The second study found that the sleep quality of children and adolescents (eight to 18 years old) with Duchenne muscular dystrophy (DMD) was significantly worse than healthy controls, particularly as regards latency and duration [35].
One study of 301 children (from one to 16 years old) with mild and moderate chronic kidney disease (CKD) showed that 25% of them had moderate to severe sleep problems and that 29% reported having trouble sleeping or lack of energy. Also, daytime sleepiness was a common complaint, especially from those with low glomerular function rate [28].
Another study showed that children (five to 18 years old) with CKD returned higher scores for insomnia, daytime sleepiness and nocturnal waking [19]. Also, sleep disorders can be correlated with impaired health-related quality of life [24].
Children with allergic diseases (three to 18 years old) also experienced various different sleep dysfunctions, the most common being problems falling/staying asleep and disorders of the transition from sleep to wakefulness [36].
No significant differences in sleep disorders were found in children with asthma (seven to 16 years old) as compared with healthy children [38]. However, when the asthma was not properly controlled, children from seven to nine years old showed less sleep efficiency and hygiene [26].
Another article identified disagreement between the reports of children with asthma (nine to 11 years old) and their parents; that is, if the parent said the child’s sleep quality was “excellent”, only a small percentage of the children agreed [25].
In a population of 91 children and adolescents (one to 18 years old) with cystic fibrosis (CF), the most common sleep problems were long sleep latency, daytime sleepiness, mouth breathing [22].
In children and adolescents (10 to 19 years old) with cancer in chemotherapy treatment, sleep quality and hygiene were significantly worse. They also reported difficulty falling and staying asleep and in going back to sleep [30].
All the studies identified in this review showed impaired sleep patterns in children and adolescents with chronic conditions. The major alterations found were: difficulty falling and staying asleep, worse sleep latency and duration, low energy, daytime sleepiness, insomnia, disorders of the transition from sleep to wakefulness and worse sleep efficiency and hygiene.
3.2. Category 2: the relationship between sleep disorders and other symptoms in children and adolescents with chronic conditions
This category comprised five studies.
These individuals experienced numerous signs and symptoms that can be intensified by poor sleep quality. Children from eight to 16 years old with polyarticular arthritis, for example, reported that, when sleep was impaired, on the following day their pain indices were higher [21].
Seven-day actigraphy in 17 adolescents (mean age 14 years) with chronic musculoskeletal pain showed that six slept between seven and eight hours, seven slept less than seven hours and mean sleep efficiency was below 90% [29].
One comparative study using an actigraphic device in children and adolescents (eight to 18 years old) with cancer showed that, independently of the appearance of pain symptoms, these individuals did not sleep long enough [17].
Even after hospital discharge, alterations are still found in the sleep patterns of these children and adolescents with cancer (mean age 12 years). One study using actigraph data after discharge from hospital found sleep duration of approximately six hours and that, the shorter this time, the greater the likelihood of problems of tiredness. Sleep interruptions of around one hour were found in the children and two hours in the adolescents [32].
Another chronic condition causing sleep problems in children (six to 12 years old) was Attention-Deficit Hyperactivity Disorder (ADHD). Sleep problems were significantly greater in children with symptoms of mood dysregulation and hyperactivity-impulsivity [31].
The studies in this category demonstrated a relationship between sleep disorders and other symptoms, in which individuals may experience intensified pain symptoms, elevated fatigue levels and mood dysregulation problems
3.3. Category 3: impaired sleep patterns of families of children and adolescents with chronic conditions
Six of the articles selected were included in this category.
Overall, families of children with chronic conditions reported worse sleep quality, more symptoms of insomnia and chronic sleep deprivation than families of healthy children [27].
A study of parents of children (mean age 8.7 years) with respiratory disease and atopic dermatitis [27].
In families of children with CF, poor sleep quality was found in most of the 23 mothers of children under 18 years old admitted to hospital [42].
One study using actigraph data showed that families of technology-dependent children reported a mean 40 minutes less sleep per night than families of healthy children and three times more sleep deprivation [41].
A study of mothers of adolescents (mean age 18 years) with DMD found that they did not sleep as well as mothers of healthy children, particularly as regards sleep quality and latency. Specifically in the group of mother carers, worse sleep quality was found in those whose children had only recently begun using non-invasive ventilation [45].
Families in a study of children (three to 12 years old) with acute lymphoblastic leukaemia also reported a mean of less than six hours sleep per night, poor sleep efficiency, long sleep onset latencies and sleepiness that impaired daytime functioning [23].
Another study also identified worse sleep hygiene in a group of 150 mothers of children (mean age 10 years) with epilepsy [16].
All the studies identified in this category showed impairment to families’ sleep patterns, the major disturbances being: worse sleep latency, hygiene and quality, insomnia, high rates of interrupted sleep, shorter sleep duration and worse daytime functioning.
3.4. Category 4: sleep alterations and their relationship to other problems in families of children and adolescents with chronic conditions
Seven articles made up this category.
It has also been found that, as sleep quality parameters deteriorate, so anxiety and depression increase, as seen in a study of mothers of children (mean age 8.1 years) with asthma and CF [37].
Of 66 families of children (mean age 10 years) with autism, 53% showed sleep disorders, including difficulty falling and staying asleep or early waking, which were related to worse moods[43].
The mothers were also found to have high cortisol levels, which correlated with impaired sexu [44].
In another study, families of children under 19 years old with cancer reported sleep problems and anguish, showing that they were more likely to report parenting problems, chronic disease, insufficient social support and daytime sleepiness [18].
The mothers in a study of children and adolescents (one to 17 years old) with type 1 diabetes mellitus described heavier burdens of nocturnal care and sleep disorders, as well as fatigue, low energy, stress and irritability [34].
Mothers of children (four months to three years of age) with bronchopulmonary dysplasia reported sleeping a mean 5.8 hours per night and taking a mean 37.8 minutes to initiate sleep, indicating disturbed sleep, which was [40].
A study of 308 families of children (zero to 12 years old) with epilepsy identified poor sleep quality. Caregiver anxiety, sleep quality and the number of co-caregivers were predictors of caregiver depression [39].
The studies in this category found sleep disorders in families to be associated with symptoms including: anxiety, depression, worse mood, sexual dysfunction, anguish, fatigue and stress.
4. Discussion
The review data highlight both the fact that children and adolescents with chronic conditions and their families display sleep disorders and their relationships with other symptoms or problems.
In childhood specifically, sleep is extremely important for development. In the early years of life, children spend more time sleeping than awake, making for rapid physical and cerebral development [63].
Sleep performs a restorative, energy-conservation and protective function. Sleep deprivation can lead to significant alterations in the lives of the individuals concerned and their families, as regards physical, occupational, cognitive and social performance, in addition to impairing the quality of care provided to children and adolescents with chronic conditions [64].
The findings of this review show that insufficient sleep predisposes to physical and mental health problems, including diminished concentration, irritability, anxiety and depression, daytime sleepiness, anguish, fatigue and stress [65].
The Sociedade Portuguesa do Sono (2017) has recommended, by age group, that children from zero to three months sleep 14 to 17 hours a day; from four to 11 months, 12 to 15 hours; one to two years, 11 to 14 hours; three to five years, 10 to 13 hours; six to 13 years, nine to 11 hours; 14 to 17 years, eight to 10 hours; and, from 18 years on, seven to nine hours [66].
Just as the amount of sleep is important, so too is its quality. Healthy sleep should be of adequate duration, good quality, regular and undisturbed [66].
Sleep is affected by intrinsic factors, such as sex, age and puberty, as well as extrinsic factors, including the environment, noise, school hours, technology use, bedtime and even specific activities such as clinical care in hospital [65,67].
Alterations in children’s health conditions may cause effects on their sleep quality [65]. In hospital, the major causes of sleep disturbances in children and their families are noise, excessive illumination and administration of medicines [63].
In sick children and adolescents, broken sleep can have quite significant effects on recovery, it can also impair immune response and pain tolerance [68].
Sleep restoration strategies include sleeping and waking at regular times; keeping the sleeping environment quiet, dark and at a comfortable temperature; disconnecting electronic appliances one hour before sleeping; avoiding stimulating food or drink before sleeping; and avoiding strenuous activities two hours before sleeping [66].
In hospital, strategies that can be used include dimming illumination and reducing noise at night, grouping health care procedures and maintaining a homely environment, including having family members present [65].
Specifically as regards the children’s families, some of the strategies that can be used involve reducing overload by sharing care; maintaining a support network that includes primary care services, school and church; and engaging with continued education provided by health professionals, who can inform families of treatment options, update their understanding and formulate a dynamic care plan, all in ways that fit with the families’ routines [69].
5. Conclusions
The evidence revealed that the sleep patterns of children and adolescents with chronic conditions and their families are impaired, which can trigger or intensify physical and psychological symptoms. In the children’s families, impaired sleep was related to anxiety, depression, stress and sexual dysfunction. It is necessary to implement specific strategies to normalise sleep patterns in this population, so as to foster improved quality of life for the children and their families.
The results of this review demonstrate that multidisciplinary care, including nursing practices, in addition to a holistic view of the subject and his family, are extremely important to meet the real needs of children and adolescents with chronic conditions. These individuals need specialized health care, with the aim of minimizing the effects of the condition itself, treatment and hospitalization on the sleep pattern and, consequently, on the quality of life. Nursing needs to plan and act effectively to reduce sleep disorders, based on the assessment of the sleep pattern of children with chronic conditions using valid and reliable instruments. For this, the professional needs to be aware of the structure and duration of sleep for each age group and, from there, be able to assess the causes of disturbances, acting to eliminate or minimize them. In addition, given the fragility and particularity of assistance to this population, attention also needs to be directed towards the family. The nurse is capable of guaranteeing care for children and adolescents and health education for the whole family, ensuring safe care and maintaining the quality of life in homes as well.
Author Contributions
Conceptualization, W.S.X., M.P.A. and M.D.R.N.; methodology, W.S.X., M.P.A. and M.D.R.N.; formal analysis, W.S.X., M.P.A. and M.D.R.N.; investigation, W.S.X, M.P.A. and M.D.R.N; data curation, W.S.X. and M.P.A.; writing—original draft preparation, W.S.X, M.P.A and M.D.R.N.; writing—review and editing, W.S.X, M.P.A, M.D.R.N., F.M.S.R, L.F.S, B.B.M.A, P.S.B and L.C.N; supervision, W.S.X, M.P.A, M.D.R.N., F.M.S.R, L.F.S, B.B.M.A, P.S.B and L.C.N; project administration, W.S.X, M.P.A, M.D.R.N., F.M.S.R, L.F.S, B.B.M.A, P.S.B and L.C.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Associação Americana de Pediatria. Enfermedades crónicas. HealthyChildren.org. 2017. Available online: https://www.healthychildren.org/Spanish/health-issues/conditions/chronic/Paginas/default.aspx (accessed on 27 December 2023).
- Andrade, R.S. de; Santos, R. dos S.F.V. dos; Santos, A.E.V. dos; Andrade, N.L. de; Macedo, I.F. de; Nunes, M.D.R. Instrumentos para avaliação do padrão de sono em crianças com doenças crônicas: revisão integrativa. Revista Enfermagem UERJ 2018, 26, 31924. [CrossRef]
- Lee, S.; Narendran, G.; Tomfohr-Madsen, L.; Schulte, F. A systematic review of sleep in hospitalized pediatric cancer patients. Psychooncology 2017, 26, 1059–1069. [Google Scholar] [CrossRef] [PubMed]
- Murillo, R.; Lambiase, M.J.; Rockette-Wagner, B.J.; Kriska, A.M.; Haibach, J.P.; Thurston, R.C. Racial/Ethnic differences in the associations between physical activity and sleep duration: a population-based study. J Phys Act Health 2017, 14, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Amorim, J.R.; Silva, I.A.; Shimizu, I.S. Avaliação da qualidade de sono em pacientes com câncer de mama em quimioterapia. Revista Brasileira de Mastologia 2017, 27, 3–7. [Google Scholar] [CrossRef]
- Setoyama, A.; Ikeda, M.; Kamibeppu, K. Objective Assessment of Sleep Status and Its Correlates in Hospitalized Children with Cancer: Exploratory Study. Pediatr Int 2016, 58, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International Classification of Sleep Disorders-Third Edition. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Daniel, L.; Kazak, A.E.; Li, Y.; Hobbie, W.; Ginsberg, J.; Butler, E.; Schwartz, L. Relationship between sleep problems and psychological outcomes in adolescent and young adult cancer survivors and controls. Support Care Cancer 2016, 24, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, N.; Pahlavanzadeh, S.; Marofi, M. Effect of a supportive training program on anxiety in children with chronic kidney problems and their mothers’ caregiver burden. Iran J Nurs Midwifery Res 2019, 24, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The Integrative Review: Updated Methodology. Journal of advanced nursing 2005, 52. [Google Scholar] [CrossRef]
- Mendes, K.D.S.; Silveira, R.C. de C.P.; Galvão, C.M. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto contexto - enferm 2008, 17, 758–764. [CrossRef]
- The Joanna Briggs Institute (Org.). Reviewers’ Manual-Methodology for JBI Mixed Methods Systematic Reviews. 2014. Available online: http://joannabriggs.org/assets/docs/sumari/ReviewersManual_Mixed-Methods-Review-Methods-2014-ch1.pdf (accessed on 27 December 2023).
- Morgenthaler, T.; Alessi, C.; Friedman, L.; Owens, J.; Kapur, V.; Boehlecke, B.; Brown, T.; Chesson, A., Jr.; Coleman, J.; Lee-Chiong, T.; et al. Practice Parameters for the Use of Actigraphy in the Assessment of Sleep and Sleep Disorders: An Update for 2007. Sleep 2007, 30, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Cooper, H.M. Scientific Guidelines for Conducting Integrative Research Reviews Author ( s ). Review of Educational Research 1982, 52, 291–302. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Fineout-Overholt, E. Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice; Edição: 4.; Wolters Kluwer Health, 2018.
- Edelstein, O.E.; Shorer, T.; Shorer, Z.; Bachner, Y.G. Correlates of quality of life in mothers of children with diagnosed epilepsy. Epilepsy Behav 2019, 93, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.D.R.; Nascimento, L.C.; Fernandes, A.M.; Batalha, L.; De Campos, C.; Gonçalves, A.; Leite, A.C.A.B.; de Andrade Alvarenga, W.; de Lima, R.A.G.; Jacob, E. Pain, sleep patterns and health-related quality of life in paediatric patients with cancer. Eur J Cancer Care (Engl) 2019, 28, e13029. [Google Scholar] [CrossRef] [PubMed]
- Rensen, N.; Steur, L.M.H.; Schepers, S.A.; Merks, J.H.M.; Moll, A.C.; Grootenhuis, M.A.; Kaspers, G.J.L.; van Litsenburg, R.R.L. Concurrence of Sleep Problems and Distress: Prevalence and Determinants in Parents of Children with Cancer. European Journal of Psychotraumatology 2019, 10, 1639312. [Google Scholar] [CrossRef]
- Stabouli, S.; Gidaris, D.; Printza, N.; Dotis, J.; Papadimitriou, E.; Chrysaidou, K.; Papachristou, F.; Zafeiriou, D. Sleep Disorders and Executive Function in Children and Adolescents with Chronic Kidney Disease. Sleep Medicine 2019, 55, 33–39. [Google Scholar] [CrossRef]
- Allen, K.D.; Kuhn, B.R.; DeHaai, K.A.; Wallace, D.P. Evaluation of a behavioral treatment package to reduce sleep problems in children with Angelman Syndrome. Research in Developmental Disabilities 2013, 34, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Bromberg, M.H.; Gil, K.M.; Schanberg, L.E. Daily Sleep Quality and Mood as Predictors of Pain in Children with Juvenile Polyarticular Arthritis. Health Psychology 2011, 31, 202–209. [Google Scholar] [CrossRef]
- Byars, K.C.; Chini, B.; Hente, E.; Amin, R.; Boat, T. Sleep disturbance and sleep insufficiency in primary caregivers and their children with cystic fibrosis. Journal of Cystic Fibrosis 2020, 19, 777–782. [Google Scholar] [CrossRef]
- Daniel, L.C.; Walsh, C.M.; Meltzer, L.J.; Barakat, L.P.; Kloss, J.D. The Relationship between Child and Caregiver Sleep in Acute Lymphoblastic Leukemia Maintenance. Support Care Cancer 2018, 26, 1123–1132. [Google Scholar] [CrossRef]
- Davis, I.D.; Greenbaum, L.A.; Gipson, D.; Wu, L.L.; Sinha, R.; Matsuda-Abedini, M.; Emancipator, J.L.; Lane, J.C.; Hodgkins, K.; Nailescu, C.; et al. Prevalence of Sleep Disturbances in Children and Adolescents with Chronic Kidney Disease. Pediatr Nephrol 2012, 27, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Kieckhefer, G.M.; Lentz, M.J.; Tsai, S.-Y.; Ward, T.M. Parent-Child Agreement in Report of Nighttime Respiratory Symptoms and Sleep Disruptions and Quality. Journal of Pediatric Health Care 2009, 23, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.R.; Boergers, J.; Kopel, S.J.; McQuaid, E.L.; Seifer, R.; LeBourgeois, M.; Klein, R.B.; Esteban, C.A.; Fritz, G.K.; Koinis-Mitchell, D. Sleep Hygiene and Sleep Outcomes in a Sample of Urban Children With and Without Asthma. Journal of Pediatric Psychology 2017, 42, 825–836. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Booster, G.D. Sleep Disturbance in Caregivers of Children With Respiratory and Atopic Disease. Journal of Pediatric Psychology 2016, 41, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Roumelioti, M.-E.; Wentz, A.; Schneider, M.F.; Gerson, A.C.; Hooper, S.; Benfield, M.; Warady, B.A.; Furth, S.L.; Unruh, M.L. Sleep and Fatigue Symptoms in Children and Adolescents With CKD: A Cross-Sectional Analysis From the Chronic Kidney Disease in Children (CKiD) Study. Am J Kidney Dis 2010, 55, 269. [Google Scholar] [CrossRef]
- Tsai, S.-Y.; Labyak, S.E.; Richardson, L.P.; Lentz, M.J.; Brandt, P.A.; Ward, T.M.; Landis, C.A. Brief Report: Actigraphic Sleep and Daytime Naps in Adolescent Girls with Chronic Musculoskeletal Pain. Journal of Pediatric Psychology 2008, 33, 307–311. [Google Scholar] [CrossRef]
- Walker, A.J.; Johnson, K.P.; Miaskowski, C.; Lee, K.A.; Gedaly-Duff, V. Sleep Quality and Sleep Hygiene Behaviors of Adolescents during Chemotherapy. J Clin Sleep Med 2010, 6, 439–444, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2952746/. [Google Scholar] [CrossRef]
- Waxmonsky, J.G.; Mayes, S.D.; Calhoun, S.L.; Fernandez-Mendoza, J.; Waschbusch, D.A.; Bendixsen, B.H.; Bixler, E.O. The Association between Disruptive Mood Dysregulation Disorder Symptoms and Sleep Problems in Children with and without ADHD. Sleep Med 2017, 37, 180–186. [Google Scholar] [CrossRef]
- Nunes, M.D.R.; Jacob, E.; Adlard, K.; Secola, R.; Nascimento, L. Fatigue and Sleep Experiences at Home in Children and Adolescents With Cancer. Oncol Nurs Forum 2015, 42, 498–506. [Google Scholar] [CrossRef]
- Hysing, M.; Sivertsen, B.; Stormark, K.M.; Elgen, I.; Lundervold, A.J. Sleep in Children with Chronic Illness, and the Relation to Emotional and Behavioral Problems—A Population-Based Study. Journal of Pediatric Psychology 2009, 34, 665–670. [Google Scholar] [CrossRef]
- Macaulay, G.C.; Boucher, S.E.; Yogarajah, A.; Galland, B.C.; Wheeler, B.J. Sleep and Night-Time Caregiving in Parents of Children and Adolescents with Type 1 Diabetes Mellitus – A Qualitative Study. Behavioral Sleep Medicine 2020, 18, 622–636. [Google Scholar] [CrossRef]
- Ozyurt, G.; Bayram, E.; Karaoglu, P.; Kurul, S.H.; Yis, U. Quality of Life and Sleep in Children Diagnosed with Duchenne Muscular Dystrophy and Their Mothers’ Level of Anxiety: A Case-Control Study. Dusunen Adam The Journal of Psychiatry and Neurological Sciences 2015, 28. [Google Scholar] [CrossRef]
- Ridolo, E.; Caffarelli, C.; Olivieri, E.; Montagni, M.; Incorvaia, C.; Baiardini, I.; Canonica, G.W. Quality of Sleep in Allergic Children and Their Parents. Allergologia et Immunopathologia 2015, 43, 180–184. [Google Scholar] [CrossRef]
- Yilmaz, O.; Sogut, A.; Gulle, S.; Can, D.; Ertan, P.; Yuksel, H. Sleep Quality and Depression-Anxiety in Mothers of Children with Two Chronic Respiratory Diseases: Asthma and Cystic Fibrosis. J Cyst Fibros 2008, 7, 495–500. [Google Scholar] [CrossRef]
- Yuksel, H.; Sogut, A.; Yilmaz, O.; Demet, M.; Ergin, D.; Kirmaz, C. Evaluation of Sleep Quality and Anxiety-Depression Parameters in Asthmatic Children and Their Mothers. Respir Med 2007, 101, 2550–2554. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; et al. Survey of Insomnia and Related Social Psychological Factors Among Medical Staff Involved in the 2019 Novel Coronavirus Disease Outbreak. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Feeley, C.A.; Turner-Henson, A.; Christian, B.J.; Avis, K.T.; Heaton, K.; Lozano, D.; Su, X. Sleep Quality, Stress, Caregiver Burden, and Quality Of Life in Maternal Caregivers of Young Children With Bronchopulmonary Dysplasia. Journal of Pediatric Nursing 2014, 29, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Keilty, K.; Cohen, E.; Spalding, K.; Pullenayegum, E.; Stremler, R. Sleep Disturbance in Family Caregivers of Children Who Depend on Medical Technology. Arch Dis Child 2018, 103, 137–142. [Google Scholar] [CrossRef]
- Vardar-Yagli, N.; Saglam, M.; Inal-Ince, D.; Calik-Kutukcu, E.; Arikan, H.; Savci, S.; Ozcelik, U.; Kiper, N. Hospitalization of Children with Cystic Fibrosis Adversely Affects Mothers’ Physical Activity, Sleep Quality, and Psychological Status. J Child Fam Stud 2017, 26, 800–809. [Google Scholar] [CrossRef]
- da Estrela, C.; Barker, E.T.; Lantagne, S.; Gouin, J.-P. Chronic Parenting Stress and Mood Reactivity: The Role of Sleep Quality. Stress and Health 2018, 34, 296–305. [Google Scholar] [CrossRef]
- Nozoe, K.T.; Hachul, H.; Hirotsu, C.; Polesel, D.N.; Moreira, G.A.; Tufik, S.; Andersen, M.L. The Relationship Between Sexual Function and Quality of Sleep in Caregiving Mothers of Sons with Duchenne Muscular Dystrophy. Sexual Medicine 2014, 2, 133–140. [Google Scholar] [CrossRef]
- Nozoe, K.T.; Polesel, D.N.; Moreira, G.A.; Pires, G.N.; Akamine, R.T.; Tufik, S.; Andersen, M.L. Sleep Quality of Mother-Caregivers of Duchenne Muscular Dystrophy Patients. Sleep Breath 2016, 20, 129–134. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Research 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Bertolazi, A.N.; Fagondes, S.C.; Hoff, L.S.; Dartora, E.G.; da Silva Miozzo, I.C.; de Barba, M.E.F.; Menna Barreto, S.S. Validation of the Brazilian Portuguese Version of the Pittsburgh Sleep Quality Index. Sleep Medicine 2011, 12, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, J.S. Aktivitaet Und Ruhe Bei Den Menschen. Z Angew Psychol 1922, 20, 192–222, https://publikationen.ub.uni-frankfurt.de/frontdoor/index/index/year/2009/docId/11635. [Google Scholar]
- Sadeh, A.; Acebo, C. The Role of Actigraphy in Sleep Medicine. Sleep Med Rev 2002, 6, 113–124. [Google Scholar] [CrossRef]
- Telles, S.C.L.; Corrêa, É.A.; Caversan, B.L.; Mattos, J. de M.; Alves, R.S.C. O Significado Clínico da Actigrafia. Revista Neurociências 2011, 19, 153–161. [CrossRef]
- Chronic Kidney Disease in Children Study. About the CKiD Cohort Study 2003. Available online: https://statepi.jhsph.edu/ckid/welcome/about/ (accessed on 27 December 2023).
- Owens, J.A.; Spirito, A.; McGUINN, M.; Nobile, C. Sleep Habits and Sleep Disturbance in Elementary School-Aged Children. Journal of Developmental & Behavioral Pediatrics 2000, 21, 27–36, https://journals.lww.com/jrnldbp/Abstract/2000/02000/Sleep_Habits_and_Sleep_Disturbance_in_Elementary.5.aspx. [Google Scholar] [CrossRef]
- Silva, F.G.; Silva, C.R.; Braga, L.B.; Serrão Neto, A. Questionário de Hábitos de Sono das Crianças em Português - validação e comparação transcultural. J. Pediatr. (Rio J.) 2014, 90, 78–84. [Google Scholar] [CrossRef]
- LeBourgeois, M.K.; Giannotti, F.; Cortesi, F.; Wolfson, A.R.; Harsh, J. The Relationship Between Reported Sleep Quality and Sleep Hygiene in Italian and American Adolescents. Pediatrics 2005, 115, 257–265. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Bertolazi, A.N.; Fagondes, S.C.; Pedro, L.S.H.; Barreto, S.S.M.; Johns, M.W. Validação da escala de sonolência de Epworth em português para uso no Brasil. J Bras Pneumol 2009, 35, 877–883, https://www.jornaldepneumologia.com.br/details/636/pt-BR/validacao-da-escala-de-sonolencia-de-epworth-em-portugues-para-uso-no-brasil. [Google Scholar] [CrossRef]
- Chervin, R.D.; Hedger, K.; Dillon, J.E.; Pituch, K.J. Pediatric Sleep Questionnaire (PSQ): Validity and Reliability of Scales for Sleep-Disordered Breathing, Snoring, Sleepiness, and Behavioral Problems. Sleep Medicine 2000, 1, 21–32. [Google Scholar] [CrossRef]
- Bruni, O.; Ottaviano, S.; Guidetti, V.; Romoli, M.; Innocenzi, M.; Cortesi, F.; Giannotti, F. The Sleep Disturbance Scale for Children (SDSC). Construction and Validation of an Instrument to Evaluate Sleep Disturbances in Childhood and Adolescence. J Sleep Res 1996, 5, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Harsh, J.; Easley, A.; LeBourgeois, M.K. A Measure of Children’s Sleep Hygiene. Sleep, 2002; 25, A316–A317, https://aquila.usm.edu/fac_pubs/3620. [Google Scholar]
- Hale, L.; Berger, L.M.; LeBourgeois, M.K.; Brooks-Gunn, J. Social and Demographic Predictors of Preschoolers’ Bedtime Routines. J Dev Behav Pediatr 2009, 30, 394–402. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Insomnia: Psychological assessment and management; Guilford Press: New York, NY, US, 1993; pp. xvii, 238; ISBN 978-0-89862-210-2.
- Castro, L. de S. Adaptação e Validação Do Índice de Gravidade de Insânia (IGI): Caracterização Populacional, Valores Normativos e Aspectos Associados. Universidade Federal de São Paulo (UNIFESP) 2011, 103.
- Vecchi, C.R. Causes and Effects of Lack of Sleep in Hospitalized Children. Arch Argent Pediat 2020, 118. [Google Scholar] [CrossRef] [PubMed]
- Neves, G.S.M.L.; Giorelli, A.S.; Florido, P.; Gomes, M. da M. Transtornos do sono: visão geral. Rev. bras. neurol 2013, 49, 57–71, http://files.bvs.br/upload/S/0101-8469/2013/v49n2/a3749.pdf.
- Anggerainy, S.W.; Wanda, D.; Nurhaeni, N. Music Therapy and Story Telling: Nursing Interventions to Improve Sleep in Hospitalized Children. Comprehensive Child and Adolescent Nursing 2019, 42, 82–89. [Google Scholar] [CrossRef]
- Sociedade Portuguesa do Sono Recomendações SPS e SPP: prática da sesta da criança nas creches e infantários, públicos ou privados. Available online: https://www.spp.pt/UserFiles/file/Noticias_2017/VERSAO%20PROFISSIONAIS%20DE%20SAUDE_RECOMENDACOES%20SPS-SPP%20SESTA%20NA%20CRIANCA.pdf (accessed on 27 December 2023).
- Nunes, M.L.; Bruni, O. Insomnia in childhood and adolescence: clinical aspects, diagnosis, and therapeutic approach. Jornal de Pediatria (Versão em Português) 2015, 91, S26–S35. [Google Scholar] [CrossRef]
- Stickland, A.; Clayton, E.; Sankey, R.; Hill, C.M. A Qualitative Study of Sleep Quality in Children and Their Resident Parents When in Hospital. Arch Dis Child 2016, 101, 546–551. [Google Scholar] [CrossRef]
- Vaz, J.C.; Milbrath, V.M.; Gabatzm, R.I.B.; Krug, F.R.; Hirschmann, B.; Oliveira, M.M. de Cuidado à família da criança com doença crônica. Rev. enferm. UFPE on line 2018, 1397–1408. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram, following Prisma (2020).
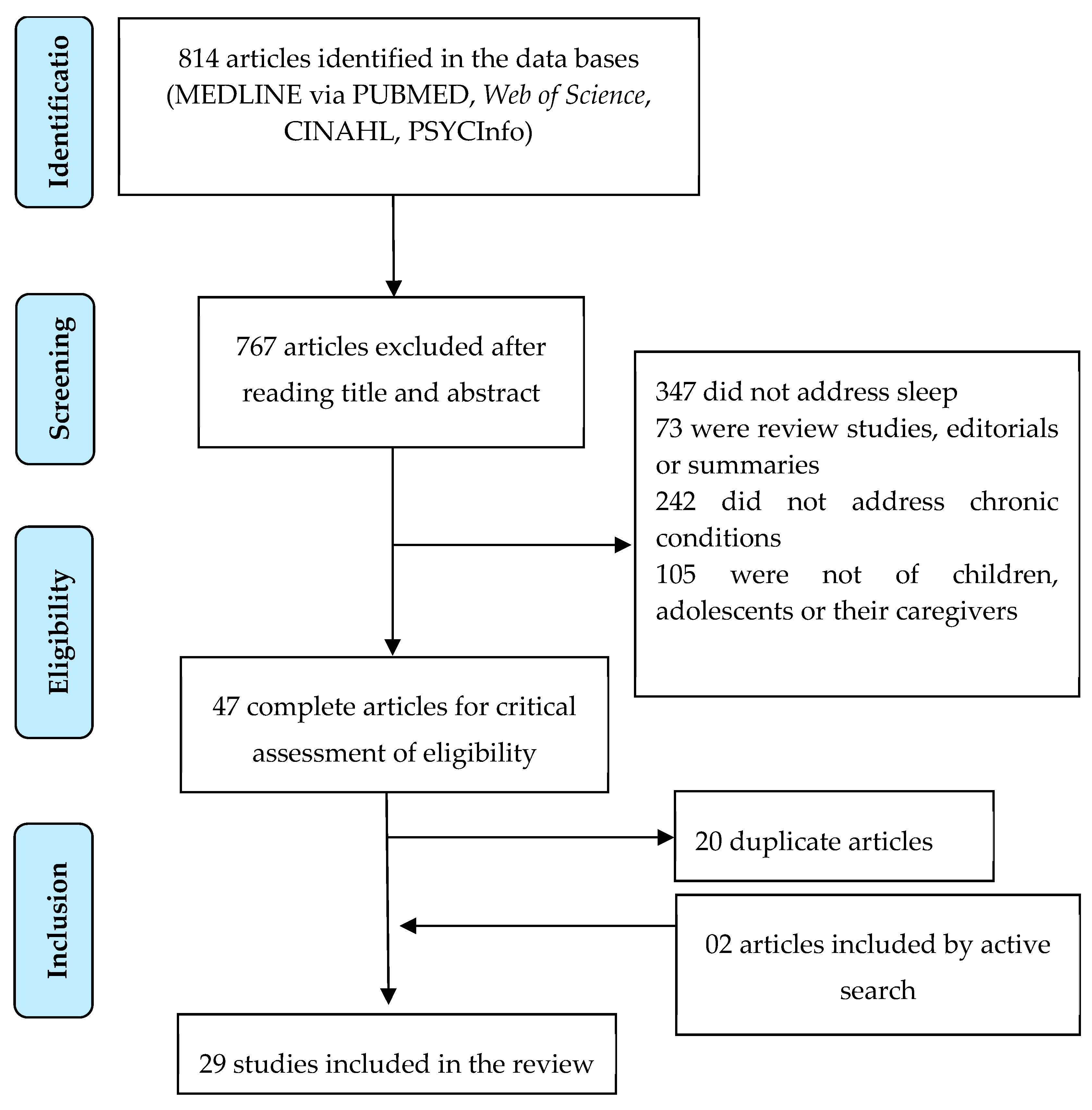

Table 1.
Characteristics of the sleep assessment instruments. Rio de Janeiro, 2023.
| INSTRUMENT | YEAR/COUNTRY OF ORIGIN | APPLICATION |
|---|---|---|
| Pittsburgh Sleep Quality Index (PSQI) | 1989/USA [46] | The instrument, comprising 19 questions relating to sleep quality and disturbance in the prior month, evaluates subjective quality, sleep latency, sleep duration, sleep efficiency, sleep disorders, use of medication and daytime dysfunction. The questions are graded into scores from zero (no difficulty) to three (severe difficulty) and the sum total ranges from zero to 21, where the greater the value, the worse the sleep quality [46,47] |
| Wrist Actigraphy | 1922/Germany [48]. | The wrist actigraph is a device in the form of a wristwatch with the ability to store data over a specified time period. The system’s scoring programme can calculate sleep efficiency and duration. The device is based on an acceleration sensor, which converts external factors, which produce motion and influence Circadian rhythm, into measurements. The numerical representation is aggregated into a constant time interval, generally called a period (for example, one minute) [49,50]. |
| CKiD Symptoms List | 2003/USA and Canada [51] | Chronic Kidney Disease in Children (CKiD) is a, prospective, observational study of children and adolescents with mild and moderate renal insufficiency. It produced a list of symptoms to be filled out for the prior month, indicating the number of days when the participant felt each of them, as well as describing the severity with which each symptom was experienced [51]. In the study selected for this review, participants responded with regard to the symptoms: “weakness”, “early waking”, “falling asleep during the day” and “diminished alertness” [28]. |
| Abbreviated Children’s Sleep Habits Questionnaire (CSHQ) | 2000/ USA [52] | This screening instrument answered by parents comprises 33 common items of child behaviour, grouped into three domains: Dyssomnias, Parassomnias and Respiratory Sleep Disturbances. The “long version” (48 items) includes other questions. Responses are scored on a three-point Likert scale (rarely = 0-1 night per week; sometimes = 2-4 nights per week; generally = 5-7 nights per week). Scores of 41 or more indicate possible sleep disorders [52,53]. |
| Adolescent Sleep-Wake Scale (ASWS) | 2005/Italy and USA [54] | This was developed as a children’s sleep-wake scale and is applied to adolescents from 12 to 18 years old. It comprises 28 items, divided into five dimensions of behaviour – going to bed, falling asleep, maintaining sleep, reinitiating sleep and returning to wakefulness – and using a six-point scale (“always”, “often, if not always”, “often”, “sometimes”, “now and then” and “never"). The higher the score, the better the sleep quality [54]. |
| Adolescent Sleep Hygiene Scale | 2005/Italy and USA [54]. | This is an adaptation of the Children’s Sleep Hygiene Scale, applicable to adolescents from 12 to 18 years old. It contains 28 items that assess issues that facilitate and hinder sleep, which are divided into nine domains: physiological, cognitive, emotional, sound environment, daytime sleep, substances, sleep routine, sleep stability and room/bed sharing. On a six-point scale (“always”, “often, if not always”, “quite often”, “sometimes”, “now and then” and "never"), the higher the score, the better the sleep hygiene behaviour [54]. |
| Epworth Sleepiness Scale | 1991/Australia [55] | This self-applied questionnaire assesses the likelihood of falling asleep (never, slight chance, moderate chance and high chance) in eight activities of daily living: sitting and reading; watching TV; sitting, inactive, in a public place; as a passenger in a car for an hour or more without stopping for a break; lying down to rest when circumstances permit; sitting and talking to someone; sitting quietly after a meal without alcohol; and in a car, while stopped for a few minutes in traffic or at a light. Total scores range from 0 to 24. A score of more than 10 suggests a diagnosis of excessive daytime sleepiness [55,56]. |
| Paediatric Sleep Questionnaire | 2000/USA [57] | Comprises around 20 items, which can be answered in about 5 minutes. The questionnaire, which evaluates symptoms of sleep disorders in children, includes scales for obstructive respiratory sleep-related disorders (mouth breathing, night sweats, nocturia, enuresis, nasal congestion, sleep bruxism, retarded growth, obesity), snoring, daytime sleepiness, insomnia and restless leg syndrome. Scores above 0.33 are considered to suggest a diagnosis of sleep-related disorder [57] |
| Sleep Disturbance Scale for Children | 1996/Italy [58] | Consists of a 26-item sleep evaluation instrument applicable to children from 3 to 18 years old. It assesses disorders of initiating and maintaining sleep, sleep breathing, arousal, sleep-wake transition, excessive daytime sleepiness and sleep hyperhidrosis. It uses a Likert-type scale scoring from 26 to 130. A score of 39 was established as the cut-off point suggestive of sleep disorders [58] |
| Children’s Sleep Hygiene Scale (CSHS) | 2002/USA [59] | This examines children’s sleep hygiene as reported by parents. It consists of 22 items that assess physiological, cognitive, emotional, environmental, sleep routine and sleep stability issues associated with sleep hygiene. Responses are on a six-point Likert scale range from Never to Always, with higher scores indicating better sleep hygiene [59] |
| General Sleep Inventory | 2009/USA [60] (Hale et al., 2009) | This scale uses parent-report data to assess whether the child: has a regular bedtime and, if so, at what time, and whether the family has enforced that bedtime in the prior five nights; whether the family has one or more sleep routines and, if so, whether the family has involved itself in those routines in the prior five nights. It also evaluates indicators of sleep routines: interaction with parents, non-interaction with parents, watching television or video, eating a snack and hygiene-related behaviour. It uses a six-point Likert scale from Never to Always [60]. The study selected for this review also evaluated whether the children shared a room, shared a bed, slept in their own bed, or in another room and how often they were disturbed by domestic and/or neighbourhood noise, as well as how many people lived in the domicile [26]. |
| Insomnia Severity Index (ISI) | 1993/USA [61] | This instrument evaluates patients’ perception of their insomnia. There are three versions: patient (self-report), third-party (spouse, for example) and doctor. It consists of seven items that assess: severity of difficulty initiating and maintaining sleep, early morning waking, satisfaction with the sleep pattern, interference in daytime functioning, perception of impairment attributed to sleep problem and degree of distress or concern caused by the sleep problem. Responses are on a scale of 0 to 4 points and the total ranges from 0 to 28. The higher the score, the more suggestive of severe insomnia [61,62]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



