
Submitted:
04 January 2024
Posted:
04 January 2024
You are already at the latest version
Abstract
Background and Objectives: This study aimed to evaluate the effects of subtalar joint axis-based balance exercises on the anterior talofibular ligament (ATFL) thickness, ankle strength, and ankle stability after an arthroscopic modified Broström operation (AMBO) for chronic ankle instability (CAI). Materials and Methods: The study included 47 patients diagnosed with CAI who underwent AMBO and were randomly divided into three groups: control (n=11), general balance exercise (n=17), and subtalar joint axis balance exercise (n=19), regardless of the affected area. Participants in the exercise rehabilitation group performed exercises for 60 min twice a week for 6 weeks, starting 6 weeks after AMBO. ATFL thickness, ankle strength, and ankle dynamic stability were measured using musculoskeletal ultrasonography, Biodex, and Y-balance test, respectively, before and after treatment. Results: Compared with the remaining groups, the subtalar joint axis balance exercise group had reduced ATFL thickness (p = 0.000), improved ankle strength for eversion (p = 0.000) and inversion (p = 0.000), and enhanced ankle stability (p = 0.000). Conclusions: The study results suggests that subtalar joint axis-based balance exercises may contribute to the early recovery of the ankle joint after AMBO.
Keywords:
Anterior talofibular ligament
; arthroscopic modified Broström operation
; chronic ankle instability
; subtalar joint axis balance exercises
1. Introduction
Ankle joint injuries are caused by walking on uneven ground, sudden changes in direction, sudden stops, and incorrect landings after jumping in daily life and sports activities [1]. Ankle injuries are among the most prevalent sports injuries, accounting for 10–30% of all sports injuries [2]. The most frequent injuries include lateral strain injuries, which occur through excessive suppression movements of plantar flexion, inversion, and rearfoot of the ankle, and external rotation movements of the leg [3]. Subtalar joint instability is a common complication of ankle sprains [4,5], and excessive inversion of the ankle and internal rotation of the talus result in lateral ankle sprains [5,6].
Among ankle injuries, inversion sprain accounts for over 85% of cases, whereas injuries of the anterior talofibular ligament (ATFL) comprise 70–80% [7]. According to the National Health Insurance Statistical Yearbook in the Republic of Korea in 2022, a total of 2,043,134 patients visited the hospital for an ankle sprain [8]. Approximately 10–50% of patients with ankle sprains demonstrate chronic ankle joint sprain symptoms, including chronic pain or repetitive reinjury [9,10]. Moreover, functional and mechanical instability for more than 6 months [11] and frequent ankle sprains cause physical deformation of the subtalar joint axis, ligaments, and the hindfoot [5]. However, secondary chronic ankle instability (CAI) with recurrent ankle sprains can persist in 10–30% of severe cases with ligament tears [12]. Patients with CAI have a high prevalence of cartilage degradation, anterior bone impingement, and soft tissue impingement [13]. The lack of interaction between the talus and calcaneus can lead to abnormal movement of the subtalar joint, causing a decline in foot and lower limb function and resulting in abnormal deformation of the foot structure. Ultimately, this condition increases the risk of ankle sprain or CAI [14].
Treatment for CAI may include nonsurgical or surgical approaches. Approximately 80% of patients improve after undergoing nonsurgical treatments through wearing orthosis on the ankle joint and performing strengthening exercises for the peroneal muscle; however, 20% require surgical treatment [15].
Recent advances in minimally invasive treatments have led to the development of several surgical options for managing CAI, offering faster recovery compared to traditional open surgery [16]. Less invasive operations are preferred over traditional open surgeries. Popular surgeries with minimally invasive techniques such as arthroscopic surgeries, include anterior cruciate ligament restoration and rotator cuff surgery [17]. The modified Broström operation (MBO) is widely used to treat lateral CAI [18,19]. The arthroscopic MBO (AMBO) is a surgical technique for preserving the fibular tendon and suturing the proximal portion of the inferior extensor retinaculum to the fibula, alleviating side effects of ankle joint stiffness [20] and preventing damage to the fibular tendon and sacral nerve owing to problems with tendon fixation [21]. Postoperatively, a rehabilitation exercise program is usually recommended for functional recovery of the ankle joint and return to daily life and sports, with a focus on the reduction of ankle joint pain, recovery of the normal range of motion (ROM), increase in muscular strength and endurance, power, neuromuscular recovery, and improvement of balance, cardiorespiratory endurance, and functional ability [22].
Mangwani et al. [23] reported that inversion and eversion muscle training is necessary for ankle stabilization by controlling muscle strength recovery and equilibrium of ankle joint plantar flexion and dorsiflexion. Balance exercises for ankle stabilization and static and dynamic balancing exercises were used to activate the inversion, eversion, supination, and pronation muscles. Static balance exercise refers to the ability to maintain the body in an upright position in space against the force of gravity on a fixed base surface, while dynamic balance exercise refers to the ability to maintain a posture without falling over while the body is moving [24]. Accordingly, supination and pronation motions at the subtalar joint are crucial for maintaining foot stability [25]. However, exercise programs using bottom up instability devices such as TOGU and BOSU balls are mainly used as ankle balance exercises [26]. To our knowledge, this study is the first to examine the effects of subtalar joint axis-based exercises on ATFL thickness, muscle strength, and dynamic stability in patients with CAI after undergoing an AMBO.
2. Materials and Methods
2.1. Participants
47 patients who underwent an AMBO for CAI were recruited from the Incheon Daechan Hospital (Republic of Korea). They were randomly divided into three groups regardless of their affected sides: the control (CON, n=11), general balance exercise (GBE, n=17), and subtalar joint axis balance exercise (SBE, n=19) groups. All patients were informed of the purpose and procedure of the study and signed a consent form before commencement. After the AMBO, the affected side was immobilized with plaster and an air splint for 4 weeks, and the patients performed ROM recovery exercises for 2 weeks. Thereafter, all patients performed balance exercises for 6 weeks. Finally, ATFL thickness ultrasonography, dynamic ankle stability, and isokinetic muscle function were assessed 12 weeks after achieving a sufficient ROM. All study procedures were approved by the Research Ethics Committee at Sun Moon University (approval number: SM-202211-050-2). The physical characteristics of the participants are shown in Table 1.
2.2. Rehabilitation program
Table 2 shows the rehabilitation program for the GBE group. The rehabilitation exercise program was modified from Brotzman and Wilke’s rehabilitation exercise program under the guidance of an exercise specialist [28]. Warm-up and cool-down were 10 min each, while the main exercise duration was 40 min, resulting in a total exercise time of 60 min, twice a week for 6 weeks. The rehabilitation exercise program comprised 4 phases. Phase 1 comprises ankle joint plantar flexion, dorsiflexion, eversion, and inversion exercises to prevent muscle atrophy caused by immobilization for 4 weeks postoperatively. Isometric exercises, isotonic exercises, partial weight bearing, and open kinetic chain exercises were performed within a range that allowed for gradual ROM improvement, with a focus on preventing pain.
In week 6 of phase 2, after achieving a normal ROM of the ankle joint, isotonic exercises, full weight bearing, and closed chain exercises were performed on both the contralateral and ipsilateral sides as strength training exercises. Each group performed proprioception and balance exercises, starting with a static balance exercise.
In week 8 of phase 3, balance and functional exercises were performed. The former included static and dynamic balance exercises. In the static balance exercise, resistance was applied through dumbbell and barbell weights that were “somewhat hard” according to the patient’s motor perception of muscle ability. For the functional exercise, exercises such as squat, lunge, side lunge were performed to strengthen the ankle and leg muscles.
In week 10 of phase 4, dumbbell and barbell weights were used for both static and dynamic balance, and functional exercises were performed. Jumping and running routines that may be employed in sports and daily life were used as functional exercises.
The exercises were performed on either the contralateral or ipsilateral side, and between sets, the ankle ROM, pain changes, and intensity adjustments were assessed. A 1 min rest period was provided between sets. Immediately after each exercise, an ice pack was applied to the affected area to prevent inflammation.
2.3. Physical therapy for the control group
The control group’s physical therapy program comprised 3 min of cryotherapy and 20 min of transcutaneous electrical nerve stimulation, totaling 23 min for 1–3 weeks. Heat therapy was conducted for 10 min twice a week for 12 weeks, starting 4–6 weeks post-surgery. Cryotherapy was performed using a cryo-injection device, the Cryo-T 2 model (Metrum Cryoflex Sp. z o. o., Sp. k. Poland), which delivered cryogenic carbon dioxide liquid gas at −78 °C to the affected area. Subsequently, a transcutaneous electrical nerve stimulation device (ESPURGE, ITO Co. Ltd., Tokyo, Japan) was used to produce a pulsation frequency ranging between 2 and 10 Hz, adjusted to an intensity that the patient felt comfortable [29].
2.4. GBE
The balance pad used for GBE (AIREX® Balance Pad, Switzerland) is commonly employed in clinical practice for balance training on unstable surfaces. The patients started performing balance exercises 6 weeks postoperatively; static and dynamic balance exercises were performed for 6 weeks thereafter (i.e., 12 weeks postoperatively). Static balance was maintained by flexing the hip while standing on one foot, and three sets of 10 repetitions lasting 5 s each were performed using dumbbells and a barbell for progressive loading. Dynamic balance exercises focused on lower extremity strength and involved single squat and single Y-squat exercises. They were also performed for 5 s, with 3 sets of 10 repetitions using dumbbells and a barbell for progressive loading. Balance exercises were conducted for a duration of 15 min.
2.5. SBE
Subtalar joint axis balance exercises were conducted using a specialized exercise tool called Pedalo (Grasleben, Germany). This tool is designed to rotate in the sagittal plane of the foot, creating an angle of about 16 degrees with a circular motion of 50 cm in diameter, aligning with the subtalar joint axis. Participants placed their feet on the rotating Pedalo and engaged in balance exercises that focused on the muscles responsible for supination and pronation of the foot (Figure 1). The exercises commenced 6 weeks postoperatively and continued until 12 weeks postoperatively. Both static and dynamic balance exercises were performed. For static balance training, participants were required to maintain their balance by flexing the hip joint while standing on a single leg. They completed three sets of 10 repetitions, with each repetition lasting for 5 s. To progressively increase difficulty and resistance, participants incorporated dumbbells and barbells into the exercise. Dynamic balance exercises were aimed at enhancing lower limb strength and involved movements such as single squat and single Y-squat exercises. Again, participants performed three sets of 10 repetitions for each of these dynamic exercises, with a focus on gradually adding more weight by using dumbbells and barbells. The entire balance exercise routine had a duration of 15 min, and the exercise was carefully designed to enhance balance, strengthen the lower limbs, and facilitate the recovery process postoperatively. The unique Pedalo exercise tool allowed for a specialized approach to subtalar joint axis balance exercises.
2.6. Ultrasonography
The same examiner assessed the ATFL thickness using musculoskeletal ultrasonography (MSUS). All images from ultrasonography examinations were stored on a picture archiving and communication system (PACS). An ultrasound image of the ATFL was obtained using a 5–13 MHz multifrequency linear transducer (Model Logiq 6 compact ultrasound machine; General Electric Company, Waukesha, WI). Because the ATFL is a superficial structure, the examiner set the transducer at a frequency of 12 MHz and image depth to 2.5 cm to capture the clearest, highest resolution image possible. The examination was conducted on the part connecting the anterior border and lateral side of the talar neck [29]. Ultrasonic gel (Aquasonic 100; Parker Laboratories, Inc, Fair-field, NJ, USA) was used to reduce friction with the skin, and the examination was performed within 10 min. Digitally obtained lateral ankle ultrasonography examination images were uploaded to PACS, and ATFL thickness was assessed.
2.7. Isokinetic muscle functions
Isokinetic muscle functions of the affected ankle were measured using the Biodex system 4 model (Biodex Medical Systems, Inc., N.Y., USA). To measure inversion and eversion strength, after three preliminary exercises for each item before measuring ankle function, the low speed was 60°/s five times. The rest time between each acceleration was 30 s, and the ankle joint movement range was performed within a pain free range [30]. Exercise duration was 15 min.
2.8. Dynamic stability
The dynamic stability was measured using a Y-Balance test (YBT) kit (Functional movement system, Danville, VA, USA). The proprioception and dynamic balancing ability of ankle joints was measured in three directions: anterior, posterior inner, and posterior outer [31]. The dynamic stability of the ankle joint was measured on both the affected and unaffected sides. After 3 practice sessions, the three aforementioned directions were measured from the center of the equipment in a single-leg stance 3 times for each lower extremity; the highest value was recorded.
If a participant i) lost their balance, ii) leaned on the upper section of the box to reach further, iii) hit the box and lost contact with it, iv) lost contact with the box during the pushing phase, or v) failed to return the reaching foot to the starting position, the attempt was dismissed.
The composite scores were computed by summing the reach distances of the anterior, posteromedial, and posterolateral directions, dividing the total by three times the participant’s leg length, and then multiplying by 100 to obtain a percentage. The distance between the anterior superior iliac spine and the most distal region of the medial malleolus was measured [32,33]. The rest period between tests was 20 s, and the total testing duration was 15 min.
2.9. Statistical analysis
For the data in this study, the mean and standard deviation were calculated using IBM SPSS 22.0 (SPSS Corp., Chicago, USA), and the subtalar joint axis balance exercise effect was analyzed using a two-way repeated measures analysis of variance (ANOVA). Post-hoc analysis was performed using the Tukey method, and the Bonferroni method was used to adjust the confidence interval. Statistical significance was set at α = 0.05.
3. Results
3.1. Change in ultrasonography results of ATFL thickness
Table 3 and Figure 2 show the ATFL thickness obtained via ultrasonography. The two-way repeated measures ANOVA revealed that, while no significant difference in ATFL thickness was observed between groups, a significant interaction was observed between group and time [F(2, 44) = 16.556, p = 0.000] and a significant change was observed in thickness over time [F(1, 44) = 109.649, p = 0.000]. Ultrasonography examination of ATFL thickness did not reveal any significance in between-group differences before and after treatment. 6 weeks after treatment, no significant differences were observed between the CON and GBE groups. However, SBE demonstrated decreased ATFL thickness compared with the CON (p = 0.008) and GBE (p = 0.033) groups, achieving the normal range. Significant differences in pre- and post-treatment values were observed in all three groups: CON (t = 3.112, p = 0.011), GBE (t = 8.239, p = 0.000), and SBE (t = 8.877, p = 0.000).
3.2. Changes in isokinetic muscle strength power
Table 4 presents the changes in isokinetic muscle strength power. For ankle EV isokinetic muscle strength power, the two-way repeated measures ANOVA indicated a significant interaction between group and time (F[2,44] = 9.508, p = 0.000) and a significant effect of time (F[1,44] = 43.685, p = 0.000), but no significant differences were found be-tween the groups. Ankle EV isokinetic muscle strength power did not reveal significant differences between groups before treatment. After 6 weeks of treatment, no significant difference between the CON and GBE groups was observed. However, the SBE group demonstrated a significant difference in the strength of the ankle EV muscle compared with the CON (p = 0.011) and GBE (p = 0.045) groups, confirming that subtalar joint axis balance exercise improves outcomes. The CON group did not demonstrate any significant differences in the pre- and post-treatment results 6 weeks postoperatively (t = −1.431, p = 0.183). Significant differences were found in the GBE (t = −3.579, p = 0.003) and SBE (t = −6.867, p = 0.000) groups.
Regarding ankle IV isokinetic muscle strength power, the two-way repeated measures ANOVA revealed a significant interaction between group and time (F[2,44] = 12.815, p = 0.000) and a significant effect of time (F[1, 44] = 62.930, p = 0.000), but no significant differences were observed between the groups. Ankle IV isokinetic muscle strength power did not show significant differences between groups before treatment. After 6 weeks of treatment, no significant differences between the CON and GBE group were observed. However, in SBE, a significant difference was observed in the strength of the ankle IV muscle compared with the CON (p = 0.012) and GBE (p = 0.048) groups, confirming that the strength of the SBE group improved. The CON group did not demonstrate any significant differences in pre- and post-treatment results 6 weeks postoperatively (t = −1.882, p = 0.089). Significant differences were found in the GBE (t = −3.895, p = 0.001) and SBE (t = −8.652, p = 0.000) groups.
3.3. Changes in dynamic stability
Table 5 presents the changes in dynamic stability. The two-way repeated measures ANOVA indicated a significant interaction between group and time (F[2,44] = 5.762, p = 0.006) and a significant effect of time (F[1,44] = 59.831, p = 0.000), but no significant differences were found between groups. Dynamic stability did not exhibit significant differences between groups before treatment. After 6 weeks of treatment, no significant differences were observed between the CON and GBE groups. However, the SBE group demonstrated a significant difference in balance ability compared with the CON (p = 0.000) and GBE (p = 0.000) groups. The SBE group also demonstrated significantly improved ankle stability. All three groups demonstrated significant differences in the pre- and 6-week post-treatment results: CON (t = −2.573, p = 0.028), GBE (t = −5.922, p = 0.000), and SBE (t = −6.146, p = 0.000).
4. Discussion
This study aimed to investigate the changes in ATFL thickness and ankle strength and stability by comparing general balance and subtalar joint axis balance exercise methods for 6 weeks after AMBO in patients with CAI. Through this study, we aimed to validate the clinical efficacy of SBE and suggest a novel exercise approach for patients with CAI after undergoing AMBO.
ATFL primarily serves as the main stabilizer of the ankle joint and is the most vulnerable ligament in common lateral ankle sprain injuries [34]. Three phases in the ligament healing process occur immediately after surgical repair: inflammatory (7 days), proliferative (2–3 weeks), and maturation or remodeling (4–26 weeks) [35,36]. MSUS imaging is a novel technique used in the field of sports medicine [37]. Therefore, in this study, we used MSUS to assess ATFL thickness. Previous studies have shown that the normal ATFL thickness is approximately 2 mm; however, partial tears increase it for more than 20%, and complete tears are not visible on imaging [38,39]. As both the extensor retinaculum and ATFL were sutured during the AMBO, the ATFL exhibited an increase in thickness to approximately 8 mm. ROM exercises begin after the proliferative phase, that is, during the ligament remodeling period, when Type III collagen is converted to the stronger Type I collagen, resulting in a decrease in the number of cells and density of blood vessels, as well as axial rearrangement of the collagen fibers [40].
In this study, after 6 weeks of exercise, ATFL thickness in the CON group decreased by 8.75%, while that of the GBE group decreased by 17.22%, but no significant difference was observed pre- and post-treatment. In contrast, in the SBE group, ATFL thickness decreased significantly by 33.93% (Pre: 8.99 ± 2.10 mm, Post: 5.94 ± 1.52 mm), approaching the normal range of thickness. Before exercise, there was no significant difference in ATFL thickness between groups. After 6 weeks of exercise, the SBE group exhibited the most substantial decrease in ATFL thickness among groups, with differences of 24.04% compared with the CON group and 18.18% compared with the GBE group.
In a previous study, patients with CAI showed morphological changes in the ATFL with the normal range as a reference, resulting in increased ATFL thickness and ankle instability [38]. In this study, ankle stability manifested as the change in ATFL thickness was reduced through postoperative exercise, with the SBE group demonstrating the greatest reduction.
Muscle function is crucial in CAI treatment [41]. CAI muscle strength training focuses on dorsiflexion strength to compensate for the lateral ankle instability caused by the initial ligament tear [42,43]. However, our study focused on the application of subtalar joint axis balance exercise. Clinically, subtalar joint movement is classified as inversion, eversion [44], and the ankle lateral muscles that act most in the motion of ankle inversion and eversion can be divided into the peroneal muscle and tibialis posterior muscle. The peroneal muscle is weaker than the tibialis posterior muscle [45]. It plays an important role in ankle inversion and prevents hyper inversion [45]. It also protects the ligament and joint upon ankle inversion, and its strength and functional recovery lead to improved control during ankle eversion and inversion [46,47].
Isokinetic muscle function is categorized into strength and endurance, which are effective in measuring a muscle’s maximal exercise capacity [48]. Peak torque is considered the gold standard for estimating skeletal strength [49].
In this study, after 6 weeks of exercise, the CON group’s EV muscle strength (60°/s) increased by 11.57%, while that of the GBE increased by 21.22%, but no significant pre- and post-treatment differences were observed. In contrast, the SBE group showed the greatest change in EV muscle strength (60°/s) at 48.61% (pre: 9.99 ± 5.59 N.M; post: 19.44 ± 4.22 N.M). Before exercise, there was no significant difference in EV muscle strength (60°/s) between groups. After 6 weeks of exercise, the SBE group demonstrated the most substantial increase in EV muscle strength (60°/s), with differences of 28.4% compared with the CON group and 19.55% compared with the GBE group.
Additionally, the IV muscle strength (60°/s) of the CON group increased by 24.54%, while that of the GBE group increased by 25.76%; however, no significant differences were observed. In contrast, the SBE group showed the greatest change in IV muscle strength (60°/s) at 56.39% (pre: 10.69 ± 7.89 N.M; post: 24.51 ± 9.29 N.M). Before exercise, there was no significant difference in EV muscle strength (60°/s) between groups. After 6 weeks of exercise, the SBE group demonstrated the most substantial increase in EV muscle strength (60°/s), with differences of 36.15% compared with the CON group and 24.77% compared with the GBE group.
Muscle weakness is associated with CAI, and strength training is an essential part of rehabilitation to prevent instability [50]. Decreased ankle strength contributes to balance loss, and enhanced ankle muscle strength has been shown to improve balance recovery [51,52].
Static and dynamic postural stability deficits have been reported to be the most important factors in the treatment of patients with CAI [53,54]. Weakness in the muscles and ligaments of the ankle can decrease static and dynamic balance abilities, resulting in instability of the center of gravity during various movements, including walking, changing direction, and landing [55]. Previous studies have shown reduced dynamic stability in the affected ankle of patients with CAI [54,56]. Additionally, CAI leads to subtalar joint instability, affecting overall pronation balance and supination forces operating across the subtalar joint axis by stabilizing the foot joints during weightbearing activities [57]. YBT is widely used to assess patients with CAI [58]. Many studies demonstrated the effects of various exercises on the symptoms of acute ankle sprains in CAI [59]. Typical rehabilitation exercises for ankle sprains comprise ROM exercises, isometric and isotonic strength training, and proprioceptive exercises [60]. Balance board exercises have been reported to improve ankle strength and balance [61], and coordination exercises such as the one step exercise have been reported to improve ankle strength and proprioception [62]. Generally, patients with CAI are often prescribed general balance exercises. However, the application of exercise for subtalar joint axis balance is yet to be well examined.
In this study, after 6 weeks of exercise, the dynamic stability of the CON group slightly increased by 5.51%, while that of the GBE group increased by 12.84%, but no significant pre- and post-treatment differences were observed. In contrast, the SBE group’s dynamic stability increased significantly by 17.57% (pre: 79.92 ± 11.35%; post: 96.95 ± 4.52%), indicating that this exercise was good for ankle stability. Before exercise, there was no significant difference in dynamic stability among groups. After 6 weeks of exercise, the SBE group demonstrated the most substantial increase in dynamic stability, with differences of 10.11% compared with the CON group and 7.92% compared with the GBE group.
These findings were similar to those of Anguish and Sandrey [63], who reported improvements in balance ability after a balance training program for patients with CAI. Therefore, as evidenced by this study, SBE decreased the change in ATFL thickness after AMBO, increasing ankle ROM and improving pain due to the increased strength of EV and IV, ultimately enhancing ankle stability.
Moreover, the uniqueness of the balance exercise in this study is that it was performed on a larger area of the sole of the foot during the GBE. However, in the balance exercise of the SBE, the circular Pedalo was used in the direction of the subtalar joint axis to reduce the area of the sole through which ground reaction force is transmitted, possibly resulting in improvements in the ankle ROM.
This study had several limitations. The number of patients participating in the 6 week study was limited, and when assessing only the treatment effect, a longer period of follow-up is needed to confirm long term effects and continuous improvement. Because some evaluation tools, such as ultrasonography, which was used to measure ATFL thickness, may have limits, the use of multiple evaluation tools is recommended. The height of the Pedalo used in the SBE is 5 cm, meaning that the height of the tool needs to be improved by lowering it while keeping stability in mind. Moreover, research into the development of exercise tools is also necessary. These limitations necessitate a more careful evaluation of the study results, and further studies addressing these limitations are warranted.
5. Conclusions
This study showed that subtalar joint axis balance exercise decreased ATFL thickness and, increased muscle strength and dynamic stability after AMBO. Based on the present results, subtalar joint axis balance exercise can be used to improve ankle stability and is necessary in research and clinical trials for various conditions. Future studies with extended term applications and exercise tools that are both suitable and secure for subtalar joint axis balance exercise are warranted.
Author Contributions
Conceptualization, J.M.P., M.S.S. and M.K.K.; methodology, J.M.P., H.D.N. and M.S.C.; validation, H.J.K. and H.D.N.; formal analysis, J.M.P. and M.S.S.; investigation, B.C.C., S.M.L. and S.H.H.; data curation, J.M.P. and M.S.S.; writing—original draft preparation, J.M.P. and M.S.S.; writing—review and editing, J.M.P., M.K.K. and S.H.H.; supervision, J.H.Y. and M.K.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
This study was approved by the Research Ethics Committee of Sun Moon University (SM-202211-050-2 and January 5, 2023).
Informed Consent Statement
Informed consent was obtained from subjects participating in the study.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Michell, T.B.; Ross, S.E.; Blackburn, J.T.; Hirth, C.J.; Guskiewicz, K.M. Functional balance training, with or without exercise sandals, for subjects with stable or unstable ankles. J. Athl Train. 2006, 41, 393–398. [Google Scholar]
- Feng, Y.; Ma, J.H.; Xiao, H.J.; Ao, R.G.; Zhang, F.G.; Li, W.C.; Wang, W.; Zeng, P.; Lu, T.; Revel, F.B.; et al. Randomized, double-blind, noninferiority study of diclofenac diethylamine 2.32% gel applied twice daily versus diclofenac diethylamine 1.16% gel applied four times daily in patients with acute ankle sprain. BMC. Musculoskeletal Disorders. 2022, 23, 1125–1135. [Google Scholar]
- Croy, T.; Saliba, S.; Saliba, E.; Anderson, M.W.; Hertel, J. Talofibular interval changes after acute ankle sprain: a stress ultrasonography study of ankle laxity. J. Sport Rehabil. 2013, 22, 257–263. [Google Scholar] [CrossRef]
- Renstrom, P.A.; Konradsen, L. Ankle ligament injuries. Br. J. Sports Med. 1997, 31, 11–20. [Google Scholar] [CrossRef]
- Kudo, S.; Aoyagi, T.; Kobayashi, T.; Koshino, Y.; Edama, M. Ultrasound imaging of subtalar joint instability for chronic ankle instability. Healthcare (Basel). 2023, 11, 2227–2237. [Google Scholar] [CrossRef]
- Fong, D.T.; Ha, S.C.; Mok, K.M.; Chan, C.W.; Chan, K.M. Kinematics analysis of ankle inversion ligamentous sprain injuries in sports: Five cases from televised tennis competitions. Am. J. Sports Med. 2012, 40, 2627–2632. [Google Scholar] [CrossRef]
- Michell, T.B.; Ross, S.E.; Blackburn, J.T.; Hirth, C.J.; Guskiewicz, K.M. Functional balance training, with or without exercise sandals, for subjects with stable or unstable ankles. J. Athl Train. 2006, 41, 393–398. [Google Scholar]
- Health insurance review & assessment service. HIRA bigdata open portal. The number of patients who visited the hospital for ankle sprains. Available online: https://opendata.hira.or.kr/op/opc/olap3thDsInfoTab3.do (accessed on 16 January 2023).
- Karlsson, J.; Lansinger, O. Lateral instability of the ankles joint. Clin Orthop. Relat Res. 1992, 276, 253–261. [Google Scholar] [CrossRef]
- Peter, J.W.; Trevvino, S.G.; Renstrom, P.A. Chronic lateral ankle instability. Foot Ankle. 1991, 12, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Wenning, M.; Gehring, D.; Mauch, M.; Schmal, H.; Ritzmann, R.; Paul, J. Functional deficits in chronic mechanical ankle instability. J. Orthop Surg. Res. 2020, 15, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Takao, M.; Matsui, K.; Stone, J.W.; Glazebrook, M.A.; Kennedy, J.G.; Guillo, S.; Calder, J.D.; Katlsson, J. Arthroscopic anterior talofibular ligament repair for lateral instability of the ankle. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1003–1006. [Google Scholar] [CrossRef]
- Odak, S.; Ahluwalia, R.; Shivarathre, D.G.; Mahmood, A.; Blucher, N.; Hennessy, M.; Platt, S. Arthroscopic evaluation of impingement and osteochondral lesions in chronic lateral ankle instability. Foot Ankle Int. 2015, 36, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.S.; Kirby, K.A.; Piazza, S.J. Determination of subtalar joint axis location by restriction of talocrural joint motion. Gait Posture. 2007, 25, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Baumhauer, J.F.; O’Brien, T. Surgical considerations in the treatment of ankle Instability. J. Athl Train. 2002, 37, 458–462. [Google Scholar] [PubMed]
- Vega, J.; Guelfi, M.; Malagelada, F.; 0Peña, F.; Dalmau-Pastor, M. Arthroscopic all-inside anterior talofibular ligament repair through a three-portal and no-ankle-distraction technique. JBJS. Essent Surg Tech. 2018, 8, e25–36. [Google Scholar] [CrossRef] [PubMed]
- Akinobu, N.; Shigeto, N.; Yoshiyuki, S.; Yukie, K.; Aki, F.; Ko, K.; Akihiro, S. Arthroscopic internal brace augmentation with arthroscopic modified Broström operation for chronic ankle instability. Arthrosc. Tech. 2021, 10, 995–1000. [Google Scholar]
- Kim, E.S.; Lee, K.T.; Park, J.S.; Lee, Y.K. Arthroscopic anterior talofibular ligament repair for chronic ankle instability with a suture anchor technique. Orthopedics. 2011, 34, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Moritz, M.; Ulf, K.H.; Ingmar, I. Arthroscopic modified Broström operation versus open reconstruction with local periosteal flap in chronic ankle instability. Arch. Orthop. Trauma Surg. 2022, 142, 3581–3588. [Google Scholar]
- Lee, K.T.; Kim, E.S.; Kim, Y.H.; Ryu, J.S.; Rhyu, I.J.; Lee, Y.K. All-inside arthroscopic modified Broström operation for chronic ankle instability: a biomechanical study. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1096–1100. [Google Scholar] [CrossRef]
- Gould, N.; Seligson, D.; Gassman, J. Early and late repair of lateral ligament of the ankle. Foot Ankle. 1980, 1, 84–89. [Google Scholar] [CrossRef]
- Braun, B.L. Effects of ankle sprain in a general clinic population 6 to 18 months after medical evaluation. Arch. Fam Med. 1999, 8, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Mangwani, J.; Hakmi, M.A.; Smith, T.W.D. Chronic lateral ankle instability: Review of anatomy, biomechanics, pathology, diagnosis and treatment. Foot. 2001, 11, 76–84. [Google Scholar] [CrossRef]
- O’Sullivan, S.B.; Schmitz, T.J.; Fulk, G.D. Physical rehabilitation: Assessment and treatment, 7rd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2019; pp. 147–149. [Google Scholar]
- Kirby, K.A. Lecithin in mania: A preliminary report. Am. J. Psychiatry. 2006, 96, 212–219. [Google Scholar]
- Nairn, B.C.; Sutherland, C.A.; Drake, J.D. Motion and muscle activity are affected by instability location during a squat exercise. J. Strength. Cond. Res. 2017, 31, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Brotzman, S.B.; Wilk, k. E. Clinical or thopaedic rehabilitation, 2nd ed.; Mosby: Philadelphia, PA, USA, 2003; pp. 391–392. [Google Scholar]
- Zhu, Y.; Feng, Y.; Peng, L. Effect of transcutaneous electrical nerve stimulation for pain control after total knee arthroplasty: A systematic review and meta-analysis. J. Rehabil Med. 2017, 49, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Kathy, L.; Geoff, G.; Todd, R.; Erik, A.W.; Joseph, G.; Thomas, W.K. Increased ligament thickness in previously sprained ankles as measured by musculoskeletal ultrasound. J. Athl Train. 2015, 50, 193–198. [Google Scholar]
- Park, J.H.; Rhyu, H.S.; Rhi, S.Y. The effects of instrument-assisted soft tissue mobilization rehabilitation exercise on range of motion, isokinetic strength, and balance in chronic ankle instability taekwondo players. J. Exerc Rehabil. 2020, 16, 516–521. [Google Scholar] [CrossRef]
- Plisky, P.J.; Grman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The reliability of an instrumented device for measuring components of the star excursion balance test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar]
- Linek, P.; Sikora, D.; Wolny, T.; Saulicz, E. Reliability and number of trials of Y balance test in adolescent athletes. Musculoskelet Sci. Pract. 2017, 31, 72–75. [Google Scholar] [CrossRef]
- Kim, J.G.; Lee, D.W.; Bae, K.C.; Choi, B.C.; Yang, S.J.; Cho, S.I.; Kim, D.H. Correlation of Y Balance with clinical scores and functional tests after anterior cruciate ligament reconstruction in young and middle-aged patients. Clin. Orthop. Surg. 2023, 15, 50–58. [Google Scholar] [CrossRef]
- Peng, L.; Yu, L.; Jia, J.; Gan, Y.; Ding, A.; Xiong, P.; Zhao, Y.; Yao, Y. The effect of thickness and elastic modulus of the anterior talofibular ligament on anterior ankle joint stiffness: A subject-specific finite element study. Front. Bioeng. Biotechnol. 2023, 11, 1175347. [Google Scholar] [CrossRef]
- Gulotta, L.V.; Rodeo, S.A. Growth factors for rotator cuff repair. Am. J, Sports Med. 2009, 28, 2126–2133. [Google Scholar] [CrossRef]
- Nikolaidou, O.; Migkou, S.; Karampalis, C. Rehabilitation after rotator cuff repair. Open. Orthop. J. 2017, 28, 154–162. [Google Scholar] [CrossRef]
- Liu, K.; Gustavsen, G.; Royer, T.; Wikstrom, E.A.; Glutting, J.; Kaminski, T.W. Increased ligament thickness in previously sprained ankles as measured by musculoskeletal ultrasound. J. Athl Train. 2015, 50, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.H.; Yang, Y.; Chen, S.Y.; Cai, Y.H. Ultrasound examination for the diagnosis of chronic anterior talofibular ligament injury. Acta. Radiol. 2012, 53, 1142–1145. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, T.H.; Lee, M.G.; Park, Y.G. Absence of ATFL remnant does not affect the clinical outcomes of the modified broström operation for chronic ankle instability. Knee surg. Sports Traumatol. Artrosc. 2020, 28, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Tuecking, L.R.; Erdle, B.; Bernstein, A.; Ogon, P.; Jaeger, M.; Südkamp, N.P.; Izadpanah, K.; Maier, D. Ligamentous healing potential of the acromioclavicular ligament following acute anatomical reconstruction. Arch. Orthop. Trauma Surg. 2022, 142, 2225–2234. [Google Scholar] [CrossRef] [PubMed]
- Hou, Z.C.; Miao, X.; Ao, Y.F.; Hu, Y.L.; Jiao, C.; Guo, Q.W.; Xie, X.; Zhao, F.; Pi, Y.B.; Li, N.; et al. Characteristics and predictors of muscle strength deficit in mechanical ankle instability. BMC. Musculoskeletal Disorders. 2020, 21, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Terada, M.; Pietrosimone, B.G.; Gribble, P.A. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. J. Athl Train. 2013, 48, 696–709. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.; Delahunt, E. Treatment of common deficits associated with chronic ankle instability. Sports Med. 2009, 39, 207–224. [Google Scholar] [CrossRef] [PubMed]
- Krähenbühl, N.; Horn-Lang, T.; Hintermann, B.; Knupp, M. The subtalar joint a complex mechanism. FORT. Open Rev. 2017, 2, 309–316. [Google Scholar] [CrossRef]
- Ferran, N.A.; Maffulli, N. Epidemiology of sprains of the lateral ankle ligament complex. Foot Ankle. Clin. 2006, 11, 659–662. [Google Scholar] [CrossRef]
- Jimenez-Reyes, P.; Samozino, P.; Morin, J.B. Optimized training for jumping performance using the force-velocity imbalance: Individual adaptation kinetics. PLoS. One 2019, 14, e0216681. [Google Scholar] [CrossRef]
- Triantafyllopoulos, I.K.; Economopoulos, D.G.; Panagopoulos, A.; Niekerk, L. Chronic lateral ankle instability in highly active patients: A treatment algorithm based on the arthroscopic assessment of the calcaneofibular Ligament. Cureus. 2021, 13, e14310. [Google Scholar] [CrossRef] [PubMed]
- Dekerle, J.; Barstow, T.J.; Regan, L.; Carter, H. The critical power concept in all-out isokinetic exercise. J. Sci. Med. Sport. 2014, 17, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P. Isokinetic evaluation of muscular performance: implications for muscle testing and rehabilitation. Int. J. Sports. Med. 1994, 15, S11–18. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.L.; Linens, S.W.; Motte, S.J.; Ross, S.E. Concentric evertor strength differences and functional ankle instability: a meta-analysis. J. Athl Train. 2009, 44, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.D.; Woollacott, M.H.; Jensen, J.L. Age-related changes in rate and magnitude of ankle torque development: Implications for balance control. J. Gerontol. A. Biol. Sci. Med. Sci. 1999, 54, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.A.; Woollacott, M.; Shivitz, N. Ankle force and rate of force production increase following high intensity strength training in frail older adults. Aging. Clin. Exp. Res. 2006, 18, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lu, J.; Cai, B.; Fan, S.; Jiang, X. Quantitative assessments of static and dynamic balance performance in patients with chronic ankle instability. Medicine (Baltimore) 2020, 99, e19775. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, S.H.; Choi, G.W.; H., W.; Jung, H.W.; Jang, W.Y. Individuals with recurrent ankle sprain demonstrate postural instability and neuromuscular control deficits in unaffected side. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 184–192. [Google Scholar] [CrossRef]
- Cain, M.S.; Garceau, S.W.; Linens, S.W. Effects of a 4-week biomechanical ankle platform system protocol on balance in high school athletes with chronic ankle instability. J. Sport Rehabil. 2017, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Park, S.H.; Kim, S.H.; Choi, G.W.; Kim, H.J. Relationship between isokinetic muscle strength and functional tests in chronic ankle instability. J. Foot. Ankle. Surg. 2019, 58, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Choisne, J.; Ringleb, S.I.; Samaan, M.A.; Bawab, S.Y.; Naik, D.; Anderson, C.D. Influence of kinematic analysis methods on detecting ankle and subtalar joint instability. J. Biomech. 2012, 45, 46–52. [Google Scholar] [CrossRef]
- Plisky, P.; Schwartkopf-Phifer, K.; Huebner, B.; Garner, M.B.; Bullock, G. Systematic review and meta-analysis of the Y-Balance test lower quarter: Reliability, discriminant validity, and predictive validity. Int. J. Sports Phys Ther. 2021, 16, 1190–1209. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Iqbal, Z.A.; Iqbal, A.; Ahmed, H.; Ramteke, S.U. Effect of chronic ankle sprain on pain, range of motion, proprioception, and balance among athletes. Int. J. Environ Res. Public Health 2020, 17, 5318. [Google Scholar] [CrossRef] [PubMed]
- Mattacola, C.G.; Dwyer, M.K. Rehabilitation of the ankle after acute sprain or chronic instability. J. Athl Train. 2002, 37, 413–429. [Google Scholar] [PubMed]
- Linens, S.W.; Ross, S.E.; Arnold, B.L. Wobble board rehabilitation for improving balance in ankles with chronic instability. Clin. J. Sport Med. 2016, 26, 76–82. [Google Scholar] [CrossRef]
- Bernier, J.N.; Perrin, D.H. Effect of coordination training on proprioception of the functionally unstable ankle. J. Orthop. Sports Phys Ther. 1998, 27, 264–75. [Google Scholar] [CrossRef]
- Anguish, B.; Sandrey, M.A. Two 4-week balance-training programs for chronic ankle instability. J. Athl Train. 2018, 53, 662–671. [Google Scholar] [CrossRef]
Figure 1.
SBE applies balance movements to the foot in the direction of the subtalar joint axis using a circular pedalo to activate ankle eversion muscles, inversion muscles, lisfranc joint, and chopart joint movements (Pedalo®, Grasleben, Germany). SBE: subtalar joint axis balance exercise.
Figure 1.
SBE applies balance movements to the foot in the direction of the subtalar joint axis using a circular pedalo to activate ankle eversion muscles, inversion muscles, lisfranc joint, and chopart joint movements (Pedalo®, Grasleben, Germany). SBE: subtalar joint axis balance exercise.
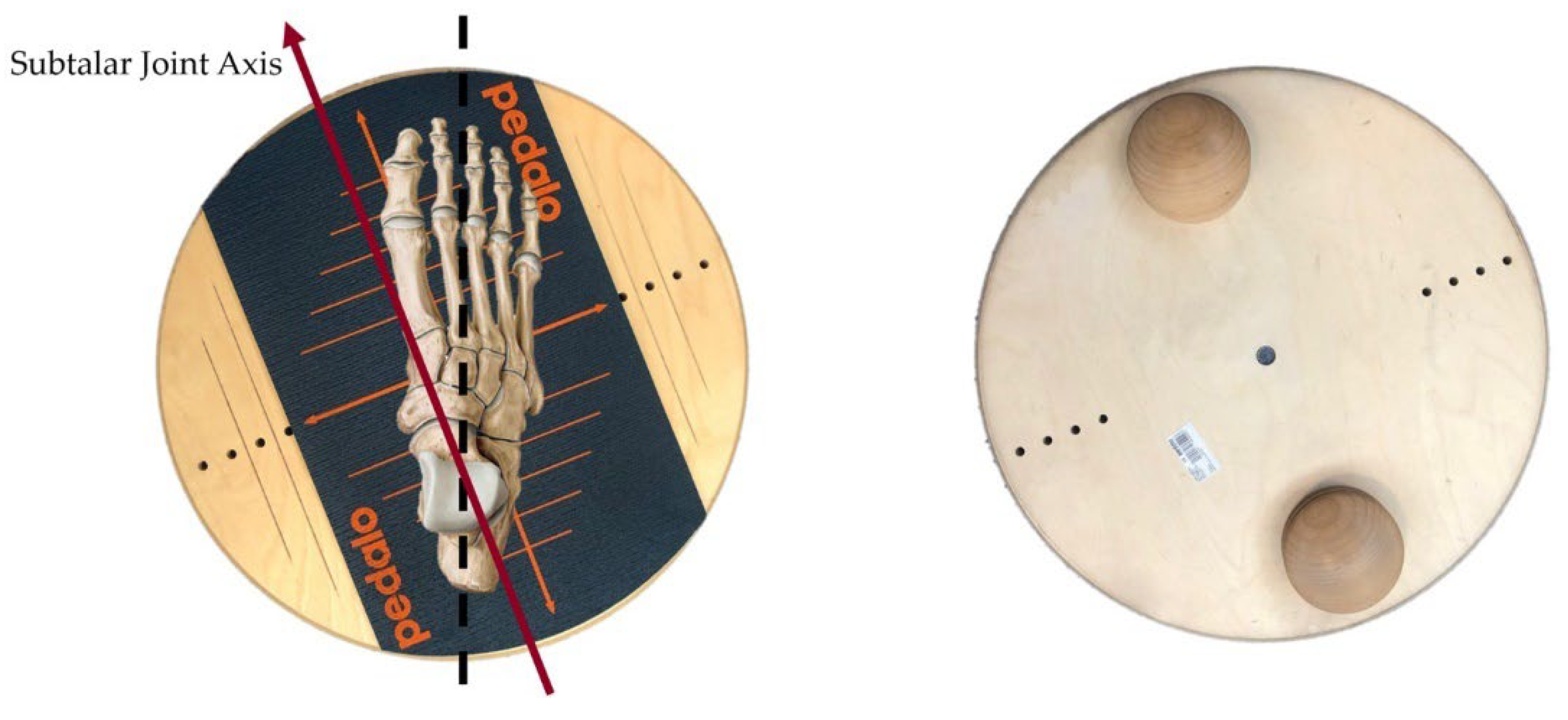
Figure 2.
Ultrasonography for the extensor retinaculum and anterior talofibular ligament. The double dashed arrow is a musculoskeletal ultrasound image of the extensor retinaculum and anterior talofibular ligament thickness measurement (scale bar = 5 mm). (A) ultrasound image after 6 weeks of AMBO, (B) ultrasound image after 12 weeks of AMBO and after balance exercise for 6 weeks. AMBO, arthroscopic modified Broström operation, FAB: fibula anterior border, TN: talus neck.
Figure 2.
Ultrasonography for the extensor retinaculum and anterior talofibular ligament. The double dashed arrow is a musculoskeletal ultrasound image of the extensor retinaculum and anterior talofibular ligament thickness measurement (scale bar = 5 mm). (A) ultrasound image after 6 weeks of AMBO, (B) ultrasound image after 12 weeks of AMBO and after balance exercise for 6 weeks. AMBO, arthroscopic modified Broström operation, FAB: fibula anterior border, TN: talus neck.
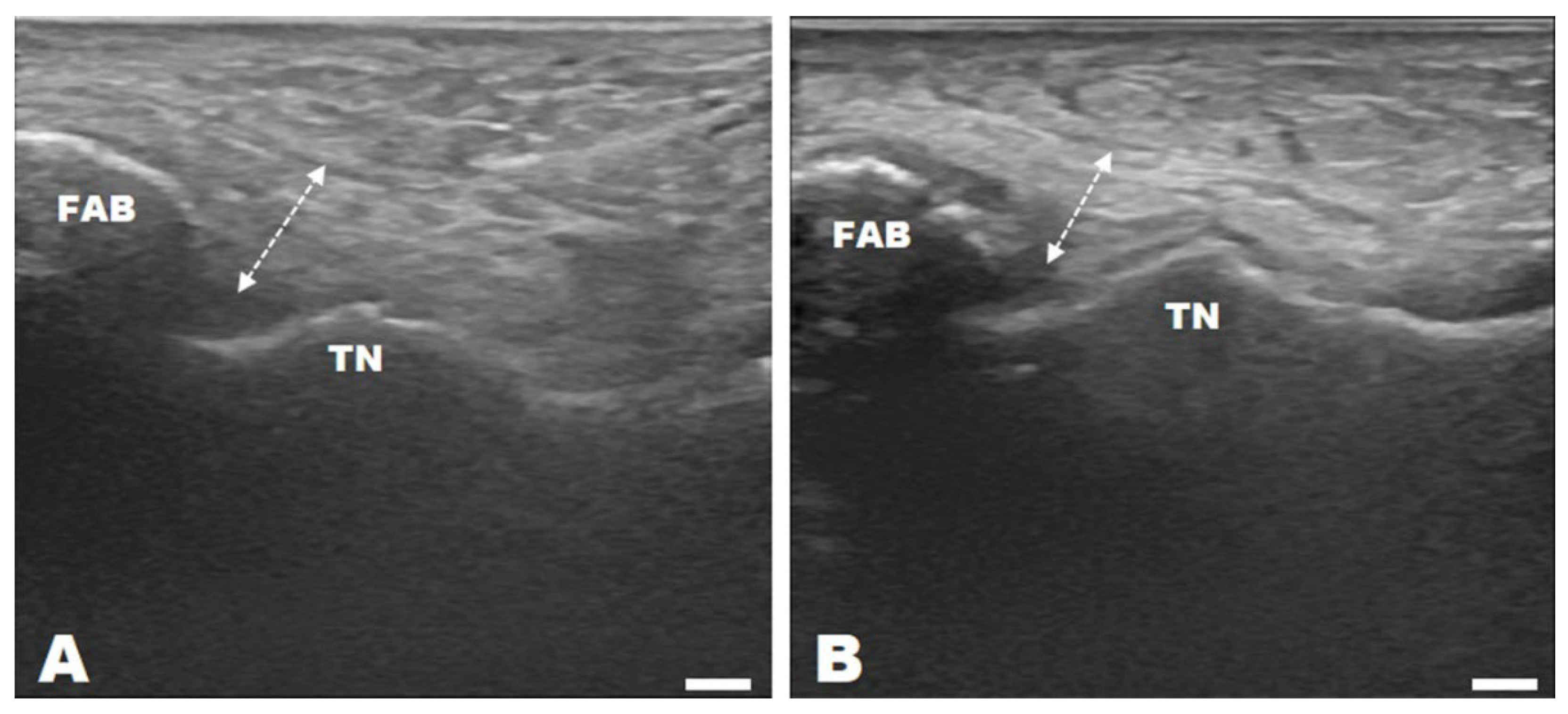

Table 1.
Baseline data of the study participants.
| Sex | Involved | Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | |||
|---|---|---|---|---|---|---|---|---|
| M | F | Rt | Lt | |||||
| CON (n=11) | 5 | 6 | 3 | 8 | 34 ± 14.76 | 169.55 ± 9.05 | 76.55 ± 21.76 | 26.34 ± 5.97 |
| GBE (n=17) | 8 | 9 | 5 | 12 | 28.53 ± 10.93 | 171 ± 10.20 | 67.82 ± 16.67 | 23.01 ± 4.44 |
| SBE (n=19) | 5 | 14 | 9 | 10 | 28.53 ± 9.75 | 165.16 ± 8.62 | 62.79 ± 12.78 | 22.83 ± 3 |
The data are presented as the mean ± standard deviation of the mean. BMI: body mass index, CON: control, GBE: general balance exercise, SBE: subtalar joint axis balance exercise.
Table 2.
Rehabilitation exercise program.
| Index | Exercise | Intensity | Side | |
|---|---|---|---|---|
| Warm up |
Flexibility | Begin gentle ROM exercises of the ankle (DF, PF, IV, EV) |
4–6 weeks (5 s x 10 reps) × 3 sets |
Involved |
| Intensive muscle exercise |
Isometric | Ankle towel isometric exercise (DF, PF, IV, EV) |
4–5 weeks (5 s x 10 reps) × 3 sets |
Involved |
| Isotonic | Towel pulling with toe Ankle tubing exercise (DF, PF, IV, EV) |
5–6 weeks (5 s x 10 reps) × 3 sets |
Involved | |
| Toe raise Calf raise |
5–6 weeks (5 s x 10 reps) × 3 sets |
Both | ||
| Functional | Squat Lunge Side lunge Single step up (box) |
6–12 weeks (5 s x 10 reps) × 3 sets |
Both | |
| Jump (jump: pain free jump in place) Hop (hop: one leg-jump hop) |
6–12 weeks 10 reps × 3 sets |
|||
| Running | 10–12 weeks 30 min | |||
| Static balance |
Single standing HF Single standing HF and SF (DB, BB) |
6–12 weeks (5 s x 10 reps) × 3 sets |
Both | |
| Dynamic balance | Single squat (DB, BB) Single Y-squat (DB, BB) |
8–12 weeks 10reps × 3 sets |
||
| Cool down |
Stretching | Foam roller | 10 min | Both |
ROM: range of motion, DF: dorsi flexion, PF: plantar flexion, IV: inversion, EV: eversion, HF: hip flexion, SF: shoulder flexion, DB: dumbbell, BB: barbell.
Table 3.
Changes in ATFL thickness obtained via ultrasonography. Units: mm.
| Pre | Post | Paired t-test | Two-way RM ANOVA | |||||
|---|---|---|---|---|---|---|---|---|
| t-value | p-value | F | p | |||||
| ATFL thickness via ultrasonography | CON (n=11) | 8.57 ± 1.99 a | 7.82 ± 2.11 a | 3.112 | 0.011* | G | 0.692 | 0.506 |
| GBE (n=17) | 8.77 ± 1.88 a | 7.26 ± 1.88 a | 8.239 | 0.000*** | T | 109.649 | 0.000*** | |
| SBE (n=19) | 8.99 ± 2.10 a | 5.94 ± 1.52 b | 8.877 | 0.000*** | G×T | 16.556 | 0.000*** | |
Data is presented as the mean ± standard deviation of the mean. Two-way RM ANOVA: two-way repeated measures analysis of variance. mm: millimeter, CON: control, GBE: general balance exercise, SBE: subtalar joint axis balance exercise, G: group, T: time, G×T: group × time. Values marked with different lowercase letters indicate a statistically significant difference between groups (p<0.05). Significant differences in pre- and post-test values (p<0.05). *p<0.05, **p<0.01, ***p<0.001.
Table 4.
Changes in isokinetic muscle strength power before and after rehabilitation exercises (60°/s). Units: N.M.
Table 4.
Changes in isokinetic muscle strength power before and after rehabilitation exercises (60°/s). Units: N.M.
| Pre | Post | Paired t-test | Two-way RM ANOVA | |||||
|---|---|---|---|---|---|---|---|---|
| t-value | p-value | F | p | |||||
| EV | CON (n=11) | 12.31 ± 4.76 a | 13.92 ± 5.11 a | –1.431 | 0.183 | G | 0.445 | 0.644 |
| GBE (n=17) | 11.54 ± 5.75 a | 15.64 ± 6.87 a | –3.579 | 0.003** | T | 43.685 | 0.000*** | |
| SBE (n=19) | 9.99 ± 5.59 a | 19.44 ± 4.22 b | –6.867 | 0.000*** | G×T | 9.508 | 0.000*** | |
| IV | CON (n=11) | 11.81 ± 6.27 a | 15.65 ± 7.26 a | –1.882 | 0.089 | G | 0.873 | 0.425 |
| GBE (n=17) | 13.69 ± 8.34 a | 18.44 ± 9.43 a | –3.895 | 0.001** | T | 62.930 | 0.000*** | |
| SBE (n=19) | 10.69 ± 7.89 a | 24.51 ± 9.29 b | –8.652 | 0.000*** | G×T | 12.815 | 0.000*** | |
Data is presented as the mean ± standard deviation of the mean. Two-way RM ANOVA: two-way repeated measures analysis of variance. N.M: newton meter, EV: eversion, IV: inversion, CON: control, GBE: general balance exercise, SBE: subtalar joint axis balance exercise, G: group, T: time, G×T: group × time. Values marked with different lowercase letters indicate a statistically significant difference between groups (p<0.05). Significant differences in pre- and post-test values (p<0.05). *p<0.05, **p<0.01, ***p<0.001.
Table 5.
Changes in dynamic stability. Units: %.
| Pre | Post | Paired t-test | Two-way RM ANOVA | |||||
|---|---|---|---|---|---|---|---|---|
| t-value | p-value | F | p | |||||
| Dynamic stability | CON (n=11) | 82.35 ± 6.9 a | 87.15 ± 7.43 a | –2.573 | 0.028* | G | 2.624 | 0.084 |
| GBE (n=17) | 77.79 ± 10.32 a | 89.25 ± 5.59 a | –5.922 | 0.000*** | T | 59.831 | 0.000*** | |
| SBE (n=19) | 79.92 ± 11.35 a | 96.95 ± 4.52 b | –6.146 | 0.000*** | G×T | 5.762 | 0.006** | |
Data is presented as the mean ± standard deviation of the mean. Two-way RM ANOVA: two-way repeated measures analysis of variance. %: percent, CON: control, GBE: general balance exercise, SBE: subtalar joint axis balance exercise, G: group, T: time, G×T: group × time. Values marked with different lowercase letters indicate a statistically significant difference between groups (p<0.05). Significant differences in pre- and post-test values (p<0.05). *p<0.05, **p<0.01, ***p<0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



