
Submitted:
05 January 2024
Posted:
08 January 2024
You are already at the latest version
Abstract
Upon declaration of poliovirus (PV) type 2 eradication in 2015, the World Health Organization (WHO) published PV containment requirements in the Global Action Plan III (GAPIII) for mitigating risks of a facility-associated release post-eradication. In 2018, the 71st World Health Assembly resolution urged Member States retaining PV to appoint a National Authority for Containment (NAC), reduce the number of PV facilities, and submit applications for containment certification. The United States (US) NAC was established in 2018 for containment oversight, and two paths to WHO GAPIII containment certification were developed. Facilities retaining PV were identified through national poliovirus containment surveys. US NAC conducted 27 site visits at 18 facilities (20 laboratories: A/BSL-2 (65%), A/BSL-3 (20%), and storage-only (15%)) to verify implementation of US NAC’s preliminary containment measures. NAC identified areas for improvement in seven categories: primary containment, decontamination, hand hygiene, security, emergency response, training, and immunization practices. Sixteen facility applications were endorsed to pursue poliovirus-essential facility (PEF) certification whereas four facilities opted to withdraw during the containment certification process. The US made noteworthy progress in PV containment to enhance biosafety and biosecurity practices at US PV facilities to safeguard the polio eradication effort.
Keywords:
polio
; GAPIII
; poliovirus containment
; NAC
; poliovirus-essential facility
; PEF
1. Introduction
Two of the three wild poliovirus (WPV) serotypes, type 2 and type 3, were declared eradicated in 2015 and 2019, respectively [1]. Wild poliovirus type 1 remains endemic in only two countries (Afghanistan and Pakistan) [1]. In the United States (US), the last wild poliovirus outbreak occurred in 1979 [2]. Wild polioviruses were eliminated in the US due to successful childhood immunization programs with the live attenuated oral poliovirus vaccine (OPV) that was later replaced with an inactivated injectable intramuscular formulation in 2000 [2,3]. Since the Global Polio Eradication Initiative (GPEI) was founded in 1988, the global incidence of wild poliovirus has declined from 350,000 cases a year in 176 countries to 22 cases in 2 countries in 2022, with an additional 8 cases in Mozambique linked to importation of virus circulating in Pakistan [1]. Globally, continued use of OPV contributed to outbreaks of neurovirulent circulating vaccine-derived poliovirus (cVDPV) in areas with low population immunity [1]. Since most cVDPV outbreaks were caused by OPV/Sabin strain type 2 (OPV2), World Health Organization (WHO) member states synchronized a global switch in April 2016 from trivalent OPV (tOPV, contains Sabin strain types 1, 2, 3) to bivalent OPV (bOPV, contains Sabin strain types 1 and 3) for routine and supplementary immunization programs. The global cessation of routine OPV2 use triggered stringent containment requirements for all poliovirus type 2 (PV2) materials to minimize the risk of reintroduction of PV2 from facilities back into communities [4,5,6,7,8].
The WHO Global Action Plan to minimize poliovirus facility-associated risk after type-specific eradication of wild polioviruses and sequential cessation of oral polio vaccine use, 3rd ed. (GAPIII) outlines facility containment requirements to mitigate the risks of a facility-associated release of poliovirus [9], and in 2022, WHO released the Global Action Plan for poliovirus containment, 4th ed. (GAPIV) [10] to address public comments received on GAPIII with full implementation anticipated by 2026. The World Health Assembly (WHA) resolution 71.16 in May 2018 urged countries retaining polioviruses to 1) reduce the number of facilities, 2) appoint a National Authority for Containment (NAC) for oversight of containment activities, and 3) have facilities selected to retain polioviruses to submit applications for participation in the containment certification program no later than December 2019 [11]. Countries are working to implement GAPIII/GAPIV containment guidelines including appointment of NACs and conducting national surveys to identify facilities retaining poliovirus infectious materials (e.g., seed stocks and virus isolates) and potentially infectious materials (PIM [12], e.g., stool or upper respiratory specimens not known to contain poliovirus that were collected in a time and place when poliovirus was circulating or OPV was used) [4]. Further, countries must identify and approve a limited number of facilities as designated poliovirus-essential facilities (PEFs) permitted to retain polioviruses in accordance with GAPIII/GAPIV [9,10]) and applicable national laws, regulations, or standards. These facilities must be certified against GAPIII/GAPIV requirements via an auditing process described in the WHO GAPIII Containment Certification Scheme [13]. The WHO and GPEI’s Global Commission for the Certification of Poliomyelitis Eradication (GCC) provides oversight and uses an independent committee, the GCC Containment Working Group (GCC-CWG), to make recommendations to the GCC for endorsement of PEF containment certificates. A GCC-endorsed and NAC-countersigned application provides assurance to the global community that the facility’s implementation of GAPIII/GAPIV is appropriate and consistent worldwide [13].
While US poliovirus survey activities began in 2002 with the first national survey [14], in January 2017, the Poliovirus Containment Activity was established within the U.S. Centers for Disease Control and Prevention (CDC) to perform the global poliovirus containment functions in the United States. In January 2018, the US Department of Health and Human Services Acting Assistant Secretary of Health approved the designation of the Poliovirus Containment Activity as the US NAC. The US NAC operates with eight full-time government employees responsible for the national poliovirus inventory (surveys) and oversight of GAPIII containment certification. The US NAC director also has oversight responsibilities as the US National Poliovirus Containment Coordinator, who oversees the national survey and inventory. We report the establishment of a national poliovirus containment program, describe a voluntary containment certification process for poliovirus-essential facilities, and share preliminary results of poliovirus laboratory containment implementation in the United States.
2. Materials and Methods
2.1. US Poliovirus Containment Program
A national program was established within the CDC Office of Readiness and Response to provide oversight of poliovirus containment in the United States. US NAC created a website, guidance, and a containment certification process for facilities retaining eradicated poliovirus materials. PV2 infectious materials (i.e., wild, vaccine-derived poliovirus (VDPV), OPV/Sabin viruses) and, since 2019, wild and vaccine-derived poliovirus type 3 materials (WPV3/VDPV3) are subject to WHO’s GAPIII containment requirements and should be held only in PEFs. Poliovirus-essential facility containment certification is overseen by the US NAC audit team. The audit team is composed of four auditors with expertise in microbiology and biosafety, and prior experience performing regulatory inspections of US select agent laboratories. Auditors also completed the WHO GAPIII auditor training course and maintain ISO45001:2018 and ISO19011:2018 certifications.
2.2. Facility Identification and Outreach
US facilities retaining PV materials were identified by three national surveys conducted by CDC between 2002 – 2022, which were used to determine the national inventory of PV materials [14,15,16]. US NAC used survey results to identify and contact facilities reporting PV materials and perform outreach with webinars and site visits to provide training on WHO GAPIII containment certification. Facilities not entering the WHO Containment Certification Scheme submitted documentation to the US NAC attesting to the destruction, inactivation, or transfer of PV materials. Facilities reporting materials that were not yet subject to containment (e.g., OPV/Sabin 1) could retain their inventory without registering as a PEF.
2.3. Certification Process
As the first step in the certification process, GCC requested that facilities complete a Certificate of Participation (CP) application, provide a description of preliminary containment conditions/risk mitigation strategies used to safeguard PV materials, and provide a time-bound action plan describing progress for implementation of GAPIII containment or a commitment to conclude work prior to the established global CP expiry date [13]. Once a facility’s CP application information was endorsed by US NAC, the application was submitted to WHO for additional processing and release to the GCC-CWG for review and GCC endorsement. Facilities that perform critical national or international activities with PV materials and plan to retain PV for an extended period were enrolled to be audited against GAPIII/GAPIV to become fully certified PEFs. Two paths for CP in the GAPIII/GAPIV PEF auditing scheme are available for a phased transition to WHO GAPIII/GAPIV containment in the United States (Figure 1).
2.4. Site Visits
Site visits were conducted for verification of facility CP application information and for periodic monitoring once the CP was awarded. Site visits consisted of laboratory tours, personnel interviews, completion of a facility questionnaire, and document review by US NAC auditors and CDC technical subject matter experts to assess preliminary containment conditions/risk mitigation strategies, laboratory features, and inventory of PV materials during 2018-2022. In lieu of an onsite visit, two virtual site visits were conducted in October and November 2020 with adapted assessment criteria due to the COVID-19 pandemic. Findings were communicated to the facility in writing following each site visit, and when applicable, the facility submitted information on corrective actions taken to resolve identified findings.
2.5. Information Collection and Analysis
CDC determined that the national survey, facility questionnaire, and CP application information collection activities conducted under the project are exempt from the requirements of the Paperwork Reduction Act (PRA) as they fall under the activities authorized under the National Childhood Vaccine Injury Act (NCVIA) at section 2102(a)(6)-(a)(7) of the Public Health Service Act (42 USC 300aa-2(a)(6)-(a)(7). This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy. §See e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. Descriptive statistical analyses (median, frequency) on PEF data sets were performed in Microsoft 365 Excel v2102; maps were created in Microsoft Power BI v2.95.804.0.
3. Results
3.1. Facility Identification and Outreach
A total of 30 potential PEFs (retaining WPV2/VDPV2, OPV2, and/or WPV3/VDPV3 infectious materials) located in 15 states were identified via national poliovirus containment surveys and correspondence to CDC between 2017-2022. Following US NAC initial outreach, facility leadership at ten facilities (10/30, 33%) opted to destroy, inactivate, or transfer PV infectious materials rather than seek certification as a PEF. As of 31 December 2022, a total of 10 PEFs in seven states remained active in the containment certification process (Figure 2). The annual number of potential PEFs in the United States fluctuated between 2017-2022, with the largest decrease (20 to 12, 40% reduction) occurring in 2018 following initial US NAC outreach (Figure 3).
3.2. Certificate of Participation Application
The US NAC developed a fillable CP application adapted from the WHO CP form [13]. The US NAC CP application collected facility information on essential work, virus type (wild, vaccine-derived, OPV, novel oral polio vaccine (nOPV)), viral propagation volume, number of essential personnel, laboratory locations, a time-bound action plan to either complete work under a CP or implement GAPIII/GAPIV, and final certification goal (i.e., plans for completion of PV work or to be audited against GAPIII/GAPIV standards for certification as a PEF). The US NAC CP application required approval and signatures from the facility principal investigator, institutional biosafety officer, and a senior institutional representative (e.g., Director, University President) to affirm full commitment by facility partners to engage in the containment certification process.
A total of 20 potential PEFs submitted CP applications to US NAC as of 31 December 2022, where two of the facilities operated PV laboratories at different physical addresses. Two of twenty CP applications were withdrawn at the facilities’ request prior to US NAC verification of risk mitigation strategies and excluded from this analysis. Eighteen potential PEFs were comprised of academic, commercial and government facility types. No PV vaccine manufacturers operate in the United States. Most US facilities (12/18, 67%) will complete critical work with PV prior to the CP global expiry date, while six facilities will seek additional GAPIII certification as PEFs.
3.3. Preliminary Containment Conditions – Risk Mitigation Strategies
An external US working group was established under a CDC federal advisory committee with subject matter expertise in biosafety, containment laboratories, public health, emergency response, and infectious diseases. Seven experts provided input to US NAC on best practices to safeguard polioviruses in domestic laboratories. In 2018, US NAC developed 35 laboratory risk mitigation strategies adapted from GAPIII elements and Biosafety in Microbiological and Biomedical Laboratories (BMBL) 5th edition guidance [17], and in 2020, the list of risk mitigation strategies was updated with 15 additional containment strategies (Table 1). These strategies were developed in consultation with the external working group and feedback from PEFs. Risk mitigation strategies were selected based on gaps identified during US NAC facility outreach, focused on enhanced biosafety practices considered most likely to mitigate risk of a potential PV occupational exposure or release, and in the 2020 revision, to address potential biosecurity and emergency management risks and expand containment to WPV3/VDPV3 infectious materials. US NAC provided training on risk mitigation strategies to facilities and requested progress on their implementation during the CP application process, at a minimum of two months later. The risk mitigation strategies were the recommended minimum safeguards for PV infectious materials in US laboratories effective until the global CP expiry date.
3.4. Certification Process
Results for facilities identified in the national survey and participation in containment certification are shown in Table 2. The first step in the PEF containment certification process has multiple steps including 1) US NAC endorsement, 2) WHO review, 3) GCC-CWG review and recommendation to GCC, 4) GCC endorsement, and 5) US NAC issuance of CP to PEF. Prior to endorsement, US NAC assessed PEFs based on critical national or international work activities, laboratory features, and implementation of preliminary containment conditions/risk mitigation strategies during site visits. US NAC also communicated with facilities to resolve incomplete CP application information, site visit findings, and requests for clarification resulting from reviews by the WHO and the GCC-CWG during the certification process.
Characteristics for eighteen PEFs (n=20 PV laboratory sites), laboratory design and 27 laboratory features are shown in Table 3. US PEFs that enrolled in the CP process used and/or stored PV in A/BSL-2 (65%), A/BSL-3 (20%), and storage (15%) areas. Some PV laboratories had enhanced features, including GAPIII facility requirements such as a ventilation system maintaining inward directional airflow (55%), double-door personnel airlock/anteroom (35%), personal walk-through exit shower (10%), and effluent decontamination system (5%) (Table 3).
3.5. Site Visits
During 2018-2022, US NAC conducted a total of 27 site visits at 20 PV laboratories in 18 PEFs to verify preliminary containment conditions/risk mitigation strategies. From June 2018 to June 2020, US NAC assessed 35 risk mitigation strategies and found US PEFs adopted preliminary containment conditions (median = 22.5, max = 30, min = 3) during 14 site visits. US NAC also found a similar trend (median = 29, max = 43, min = 15) when the number of risk mitigation strategies was increased to 50 (n=13 visits), with an increase from a minimum of 3 to 15 strategies observed during these visits. Results for risk mitigation strategies assessed, and PEF containment practices verified during site visits are shown in Table 1.
US NAC found PEFs separated the PV laboratory room from public areas with two doors (25/27, 93%), reduced quantities of polioviruses stored (20/27, 74%), segregated PV from all other materials (22/27, 81%), and dedicated reagents used for PV work (15/27, 56%). In the United States, a limited number of PEFs perform animal studies with PV serotypes subject to containment, and thus, animal containment criteria were not applicable to most facilities. US NAC observed animal-specific risk assessments and HEPA-filtered exhaust on containment caging systems at two PEFs performing animal work, but one of the two PEFs did not fully implement recommended animal PV containment practices (i.e., a dedicated caging system, animal recordkeeping through final disposition, and emergency response plans for an escaped animal) (Table 1).
Areas for improvement included use of certified primary containment devices for manipulation of PV materials, appropriate decontamination of solid and liquid biohazardous waste, hand hygiene practices, training, and proof of PV immunization records for essential personnel granted access to PV laboratories and materials (Figure 4). Some PV laboratory sites (8/20, 40%) fully implemented the recommended personal protective equipment (PPE) for laboratory staff. For PPE, a nose and mouth covering had the lowest implementation observed by US NAC during site visits (8/27, 30%) (Figure 4). Similarly, facility security controls and emergency response protocols needed modifications to address poliovirus containment (Figure 4). For example, US NAC observed PV laboratories did not restrict access only to essential personnel for PV laboratory and storage areas (9/27, 33%). Facilities implemented corrective actions to resolve US NAC findings prior to issuance of CPs. US NAC also conducted periodic monitoring after the CP was awarded for several PEFs (7/18, 39%) to ensure containment practices were maintained.
3.6. US NAC and GCC-Endorsement
National and global endorsement and associated processing times for facility CP applications are shown in Table 2. US NAC received completed CP application information (i.e., CP application, preliminary containment conditions- risk mitigation strategies, time-bound action plan, material inventory, resolution of site visit findings) for 17 of 18 PEFs. GCC-CWG requested clarification on eight applications and returned three CP applications as ‘unsatisfactory’ requiring PEF reapplication. A total of sixteen PEFs were endorsed by GCC in the United States as of June 2023. Extended processing times (median days = 233, min = 91, max = 678) were observed for US PEFs to achieve NAC and GCC endorsed CP applications (Table 2).
3.7. Withdrawal of PEFs
Following GCC-endorsement, six PEFs completed essential work with WPV2, WPV3, OPV/Sabin 2, and/or received a temporary waiver from WHO to exclude research activities with nOPV2 from the Containment Certification Scheme resulting in ten active PEFs as of 31 December 2022 (Figure 3). To withdraw from containment certification, PEFs submitted a written statement signed by the principal investigator or institutional representative requesting to withdraw from containment certification, documentation with two witness signatures of the transfer, inactivation, or destruction of WPV2/WPV3, OPV2 materials, and a description of validated decontamination methods used to decommission laboratory areas. US NAC reviewed the documentation and notified the WHO of the withdrawal. Overall, a substantial reduction (20/30, 67%) in the number of potential US PEFs has occurred since appointment of the US NAC.
4. Discussion
Poliovirus containment is a key goal of the poliovirus eradication strategy and a prerequisite for future certification of a poliovirus-free world [18]. As of November 2023, WHO reported a total of 22 countries with plans to retain PV materials in 69 PEFs, with 42 designated PEFs awarded GCC-endorsed CPs to become audited against GAPIII [4,19]. While some countries experienced delays in appointing a NAC [4,19], US NAC was established in January 2018 following a process initiated by CDC. The rapid implementation of containment activities in the US was likely due to existing partnerships between CDC and WHO, monthly coordination meetings between US NAC and WHO, the establishment of an external working group, and allocation of CDC resources and full-time staffing to US NAC. These activities supported engagement of PV laboratories in the certification process and safeguarded PV infectious materials with enhanced safety and security practices. Notably, all US PV laboratories reporting WPV2/VDPV2, OPV2, WPV3/VDPV3 infectious materials in the national survey participated in the containment certification process or opted to destroy, inactivate, or transfer these materials to comply with GAPIII/GAPIV. We report on progress made towards a successful transition to more stringent GAPIII/GAPIV containment in the United States.
Poliovirus does not currently meet the criteria for classification as a select agent in the United States, and as a result, the United States does not have a legal framework to require containment of polioviruses as of November 2023 [20]. Further, poliovirus has previously been classified as a risk group 2 agent with recommended biosafety level 2 (BSL-2) laboratories and containment practices as described in BMBL guidelines [17], whereas poliovirus containment is closely aligned to enhanced BSL-3 laboratories and practices [9,10]. These issues presented a challenge to the immediate implementation of GAPIII containment by facilities performing essential work with polioviruses. Most US PEFs planned to complete work under a CP and not seek additional certification. Thus, the United States developed a phased approach to manage a voluntary program of facilities retaining WPV2/VDPV2, OPV2 and WPV3/VDPV3 to work with and store these viruses safely and securely while progressing toward stringent containment measures outlined in GAPIII/GAPIV.
The total number of PEFs in the United States fluctuated between 2017-2022, with the largest decrease occurring in 2018. The PEFs reported GAPIII containment requirements as a deterrent for retention of PV materials. However, since 2019, a modest reduction in PEFs was balanced with newly identified facilities. Globally, the United States continues to have the largest number of facilities retaining polioviruses that entered WHO’s Containment Certification Scheme as of November 2023 [19]. Several US PEFs did not modify operations to comply with GAPIII containment, consistent with the 2018 WHA resolution [11], until contacted by US NAC. As a result, US NAC developed recommendations for preliminary containment conditions/risk mitigation strategies in consultation with an independent US working group and PEF partners that were realistic for facilities to achieve in a short time. The US NAC risk mitigation strategies were standardized for transparency and consistency in the certification process due to the large number of US PEFs. US NAC found that site visits and discussions with facility personnel were critical to raise awareness of containment requirements and to verify implementation of practices prior to endorsement of CP applications.
US NAC also observed gaps in PEF biocontainment practices during site visits, including some fundamental GAPIII principles. For example, many PEFs had not verified PV immunizations for essential personnel, ensured stringent adherence to hand hygiene practices, or required use of certified primary containment devices for all manipulations of PV infectious materials. These site visit findings, along with a reported 21 incidents of PV release at research laboratories and vaccine production facilities that have occurred globally since 2000, resulting in 16 poliovirus infections [21], suggest current containment practices in PV laboratories should be reviewed and strengthened . US NAC site visits were instrumental in observing PV biocontainment practices, and although gaps were identified, facilities resolved findings and improved poliovirus containment practices in designated US PEFs. These results show that a transition from decades of poliovirus research using BSL-2 laboratories and practices to higher biocontainment standards required time, engagement, and collaboration by all partners, particularly for enhanced laboratory containment of attenuated OPV2 vaccine viruses [6].
US NAC found that its PEF certification process resulted in consistent implementation of enhanced safety and security practices beyond BSL-2 standards for PV infectious materials. US NAC acknowledges that the risk mitigation strategies (preliminary containment conditions) reported here were not a substitute for WHO’s GAPIII/GAPIV containment requirements. In addition, the approach taken was risk-based and may not be applicable to all PEF-hosting countries globally. For example, poliovirus vaccines are not manufactured in the United States, a higher risk activity with multiple reported containment breaches [9,21,22,23]. The United States also complies with GAPIII/GAPIV requirements for national high population immunization coverage (93% inactivated poliovirus vaccine, third dose, as of 2022 [24,25]) as well as sanitation system safeguards to mitigate the transmission of disease such as those due to wild polioviruses.
US NAC continues to improve its guidance for PEFs and the risk mitigation strategies were updated with more descriptive information in 2020-2021, including containment of WPV3/VDPV3 and additional emergency response and security strategies aligned to the GAPIII/GAPIV standard. US NAC identified similar gaps in PEF readiness for these enhancements. As a result, PEF readiness for site visits and implementation of recommended enhanced containment conditions were factors that contributed to delays in the certification process. While our recommended preliminary containment conditions were adapted from GAPIII, PEF conformance to a more complex and systems based GAPIII/GAPIV standard suggests that additional time may be necessary for PEFs to achieve full conformance to GAPIII/GAPIV than currently outlined in the WHO Containment Certification Scheme [13]. No designated PEFs have been fully certified to GAPIII/GAPIV containment worldwide [4,19].
Poliovirus-essential facility CP applications required nearly 8 months (median days = 233, range 91-678) for endorsement by both US NAC and GCC from date of submission to US NAC. Currently, the WHO Containment Certification Scheme recommends NAC review of CP applications to determine if the PEF can potentially meet GAPIII criteria but does not specify site visit assessments for this first step [13]. US NAC incorporated site visits prior to its endorsement of PEFs, a significant contributing factor in longer processing times. While PEFs averaged less than three months to implement enhanced containment practices, one PEF required 418 days to implement recommended risk mitigation strategies due to limited availability of BSL-3 space during the COVID-19 pandemic. Despite a longer processing time, US NAC deemed these visits necessary before giving its endorsement of a designated PEF and instrumental in responding to WHO and/or GCC requests for clarification during their review processes. US NAC also found longer processing times were needed when GCC returned a few CP applications as unsatisfactory requiring reapplication. These CP applications required additional correspondence with WHO and GCC for resolution of reviewer feedback and resulted in an extended approval process. The CP processing times improved to less than six months for four US PEFs enrolled during 2020-2022 suggesting that, despite challenges and the COVID-19 pandemic, the US NAC processes are effective for the identification and certification of PEFs.
Overall, the United States successfully appointed a NAC, reduced the number of potential PEFs by 67%, and ensured all facilities retaining WPV2/VDPV2, OPV2 and WPV3/VDPV3 infectious materials in the national survey submitted CP applications. Notably, the United States is complying with the May 2018 World Health Assembly resolution 71.16 [11] without a national legal framework requiring containment of polioviruses. As of June 2023, one US PEF achieved an Interim Certificate of Containment against GAPIII to advance beyond the initial CP process ([26], unpublished data, manuscript in preparation). The United States is one of only three countries achieving this accomplishment. The results reported suggest that US NAC’s outreach and phased approach for implementation of stringent GAPIII/GAPIV containment measures, engagement of laboratory partners in preliminary containment recommendations and raising facility awareness of the risks posed by retaining eradicated polioviruses has led to the adoption of enhanced laboratory safeguards. US NAC will continue to monitor its national survey, PEFs, and report on the transition to GAPIII/GAPIV containment audits aligned with the anticipated global CP expiry date.
Limitations
The findings in this report are subject to at least three limitations. First, we were unable to account for possible underreporting of facilities retaining poliovirus materials in national surveys used for the identification of PEFs. Second, and related to the first limitation, the United States does not maintain a registry of laboratories, and thus, an unknown total number of laboratories limited the ability to perform an independent verification of laboratories retaining poliovirus materials. Third, the GAPIII and BMBL guidelines were sampled to develop risk mitigation strategies focused on biosafety practices, and thus, do not represent other mitigation measures that PEFs may use to reduce risks for retention of polioviruses.
5. Conclusions
The United States made noteworthy progress on the implementation of the WHO GAPIII/GAPIV Containment Certification Scheme. Globally, the United States was the second country to receive endorsement of a poliovirus- essential facility CP application by the GCC and has the highest number of PV facilities endorsed as designated poliovirus-essential facilities as of June 2023. US PEFs established a community of practice committed to implementation of containment certification, adopted enhanced biosafety and biosecurity containment practices for PV materials exceeding routine BSL-2 practices during the transition to WHO GAPIII/GAPIV containment, and US NAC engaged institutional leadership, biosafety professionals, and investigators in global poliovirus containment goals.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Author Contributions
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention (CDC). CO, BS, CS, AL, CM, SS, and KG performed containment site visits and reviewed the manuscript; CB led development of NAC website, performed outreach activities, and reviewed the manuscript; CO, CS, LHS led the experimental design, collection, and analysis of data; CO, CS prepared the figures and wrote the manuscript. LHS directed the poliovirus containment program.
Funding
US NAC received funding support from the Centers for Disease Control and Prevention, Global Health Center, Global Immunization Division.
Institutional Review Board Statement
CDC determined this activity (HSR#18110601) to be public health non-research, thus Institutional Review Board review was not required.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to privacy concerns for the poliovirus-essential facilities. Aggregated data is available from the corresponding author on reasonable request.
Acknowledgments
We thank the poliovirus-essential facilities for collaboration and participation in poliovirus containment, Daniel Sosin, Stephen Redd, Alison Mawle, Olen Kew (CDC) for leadership and US poliovirus containment program development, Mark Pallansch (CDC) for technical expertise and manuscript review, Cassandra Tansey (CDC) for technical expertise and development of animal containment guidance, the CDC/ORR Board of Scientific Counselors and Biological Agents Containment Working Group/Poliovirus Containment Working Group for review, technical expertise and support of US NAC policy recommendations.
Conflicts of Interest
The authors declare they have no conflict of interest. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the U.S. Centers for Disease Control and Prevention.
References
- Lee SE, Greene SA, Burns CC, et al. Progress Toward Poliomyelitis Eradication - Worldwide, January 2021-March 2023. MMWR Morb Mortal Wkly Rep. 2023;72(19):517-522. PMID: 37167156; PMCID: PMC10208367. [CrossRef]
- Strebel PM, Sutter RW, Cochi SL, et al. Epidemiology of poliomyelitis in the United States one decade after the last reported case of indigenous wild virus-associated disease. Clin Infect Dis 1992;14:568--79. [CrossRef]
- Advisory Committee on Immunization Practices (ACIP). Revised Recommendations for Routine Poliomyelitis Vaccination. MMWR Morb Mortal Wkly Rep. 1999;48(27). [CrossRef]
- Moffett DB, Llewellyn A, Singh H, et al. Progress Toward Poliovirus Containment Implementation — Worldwide, 2019–2020. MMWR Morb Mortal Wkly Rep. 2020;69:1330–1333. [CrossRef]
- Moffett DB, Llewellyn A, Singh H, et al. Progress Toward Poliovirus Containment Implementation - Worldwide, 2018-2019. MMWR Morb Mortal Wkly Rep. 2019;68(38):825-829. [CrossRef]
- Dowdle WR, Gary HE, Sanders R, van Loon AM. Can post-eradication laboratory containment of wild polioviruses be achieved? Bull World Health Organ. 2002;80(4):311-6.
- Bandyopadhyay AS, Singh H, Fournier-Caruana J et al. Facility-Associated Release of Polioviruses into Communities-Risks for the Post eradication Era. Emerg Infect Dis. 2019;25(7):1363-1369. [CrossRef]
- Duizer E, Ruijs WL, Putri Hintaran AD, et al. Wild poliovirus type 3 (WPV3)-shedding event following detection in environmental surveillance of poliovirus essential facilities, the Netherlands, November 2022 to January 2023. Euro Surveill. 2023; 28(5):2300049. PMID: 36729115; PMCID: PMC9896605. [CrossRef]
- World Health Organization. WHO global action plan to minimize poliovirus facility-associated risk after type-specific eradication of wild polioviruses and sequential cessation of oral polio vaccine use—GAPIII. 3rd ed. Geneva, Switzerland: World Health Organization; 2015.
- World Health Organization. WHO Global Action Plan for Poliovirus Containment, Fourth edition (unedited version). Geneva, Switzerland: World Health Organization; 2022.
- Seventy first World Health Assembly. WHA Resolution 71.16: Poliomyelitis – containment of polioviruses. 2018. https://polioeradication.org/wp-content/uploads/2019/05/A71_R16-en.pdf Accessed on December 6, 2023.
- World Health Organization. Guidance to minimize risks for facilities collecting, handling or storing materials potentially infectious for polioviruses (PIM Guidance). Geneva: World Health Organization; 2018.
- World Health Organization. Containment certification scheme to support the WHO global action plan for poliovirus containment (GAPIII-CCS). Geneva, Switzerland: World Health Organization; 2017.
- Centers for Disease Control and Prevention (CDC). National laboratory inventory for global poliovirus containment--United States, November 2003. MMWR Morb Mortal Wkly Rep. 2004;53(21):457-9.
- Centers for Disease Control and Prevention (CDC), United States National Authority for Containment. Past Poliovirus Surveys of U.S. Laboratories. https://www.cdc.gov/orr/polioviruscontainment/us-containment.htm. Accessed on December 6, 2023.
- Centers for Disease Control and Prevention (CDC). National Inventory for Poliovirus Containment: Minimizing Risk of Poliovirus Release from Laboratories in the United States. Federal Register. Notice 84(195):53731.
- US Department of Health and Human Services (HHS). CDC. Biosafety in microbiological and biomedical laboratories, 5th ed. Atlanta, GA: CDC; 2009. HHS Publication no. (CDC) 21-1112.
- Global Polio Eradication Initiative. Polio Endgame Strategy 2022-2026: Delivering on a promise. Geneva: World Health Organization; 2021.
- World Health Organization. Country progress towards poliovirus containment certification (website, data as of 20 November 2023). https://polioeradication.org/polio-today/preparing-for-a-polio-free-world/containment/. Accessed on December 6, 2023.
- U.S. Government Publishing Office. Electronic Code of Federal Regulations Title 42 Chapter 1 Subchapter F Part 73. https://www.ecfr.gov/current/title-42/chapter-I/subchapter-F/part-73 . Accessed on December 6, 2023.
- Irwin A. Polio is on the brink of eradication. Here's how to keep it from coming back. Nature. 2023; 623(7988):680-682. PMID: 37989772. [CrossRef]
- Jeannoël M, Antona D, Lazarus C, Lina B, Schuffenecker I. Risk Assessment and Virological Monitoring Following an Accidental Exposure to Concentrated Sabin Poliovirus Type 3 in France, November 2018. Vaccines (Basel). 2020;8(2):331. [CrossRef]
- Duizer E, Ruijs WL, van der Weijden CP, Timen A. Response to a wild poliovirus type 2 (WPV2)-shedding event following accidental exposure to WPV2, the Netherlands, April 2017. Euro Surveill. 2017;22:30542. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Polio vaccination coverage among children 19-35 months by State, HHS Region, and the United States, National Immunization Survey-Child (NIS-Child), 1995 through 2020. https://www.cdc.gov/vaccines/imz-managers/coverage/childvaxview/interactive-reports/index. Accessed on December 6, 2023.
- World Health Organization. Immunization Data portal, Polio 3rd dose coverage estimates. https://immunizationdata.who.int/pages/profiles/usa.htmlAccessed on December 6, 2023.
- Ottendorfer C et al. Implementation of GAPIII Laboratory Containment in Poliovirus-Essential Facilities – United States, 2017-2023. Manuscript in draft.
Figure 1.
Two certification paths for the phased transition to WHO GAPIII/GAPIV containment in the United States. (a) Certification path for PEF planning to conclude work prior to the global CP expiry date; (b) Certification path for PEF planning to continue work and implement GAPIII/GAPIV containment. CP - Certificate of Participation, ICC – Interim Certificate of Containment, CC – Certificate of Containment.
Figure 1.
Two certification paths for the phased transition to WHO GAPIII/GAPIV containment in the United States. (a) Certification path for PEF planning to conclude work prior to the global CP expiry date; (b) Certification path for PEF planning to continue work and implement GAPIII/GAPIV containment. CP - Certificate of Participation, ICC – Interim Certificate of Containment, CC – Certificate of Containment.
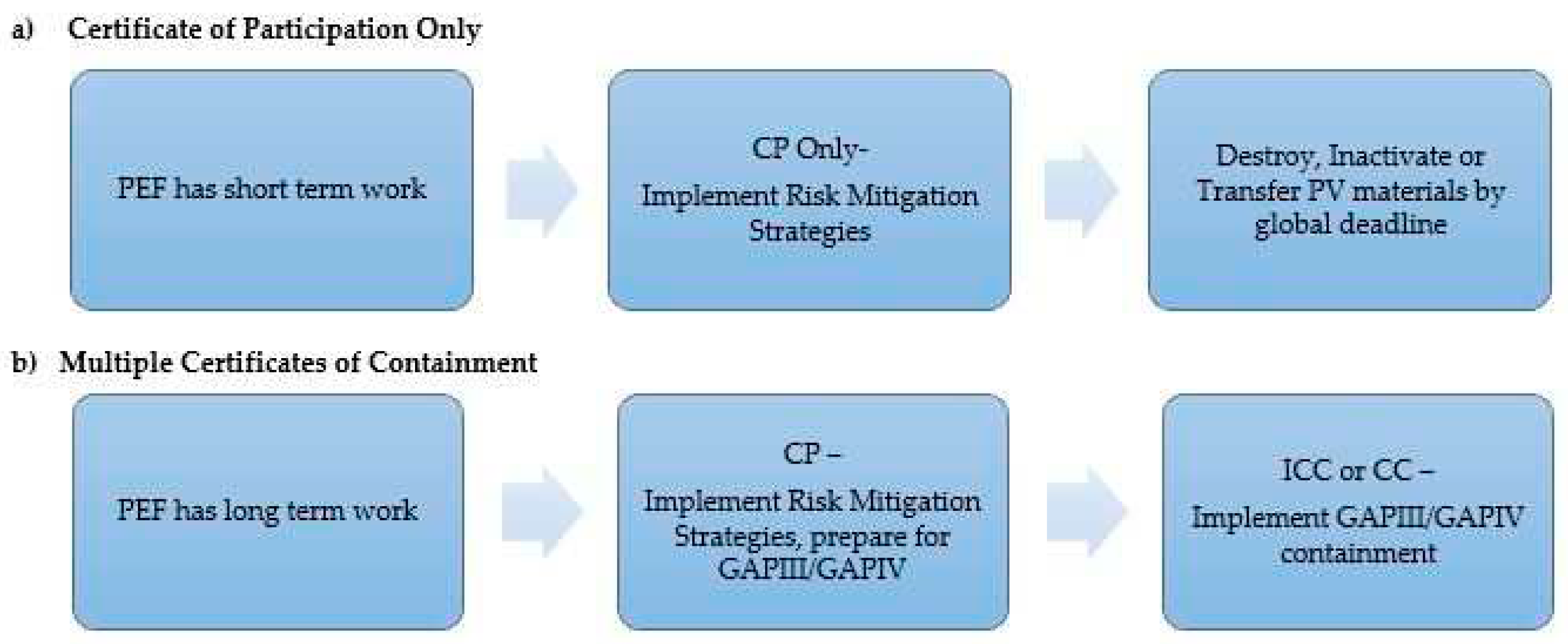
Figure 2.
U.S. states hosting Poliovirus-Essential Facilities between 2017-2022. (a) U.S. states hosting potential PEFs between 2017-2022 as reported by respondents to national poliovirus containment surveys or facility direct communication to CDC, (b) U.S. states hosting PEFs (WPV2/VDPV2, OPV2, and WPV3/VDPV3materials) endorsed by US NAC and GCC as of 31 December 2022.
Figure 2.
U.S. states hosting Poliovirus-Essential Facilities between 2017-2022. (a) U.S. states hosting potential PEFs between 2017-2022 as reported by respondents to national poliovirus containment surveys or facility direct communication to CDC, (b) U.S. states hosting PEFs (WPV2/VDPV2, OPV2, and WPV3/VDPV3materials) endorsed by US NAC and GCC as of 31 December 2022.
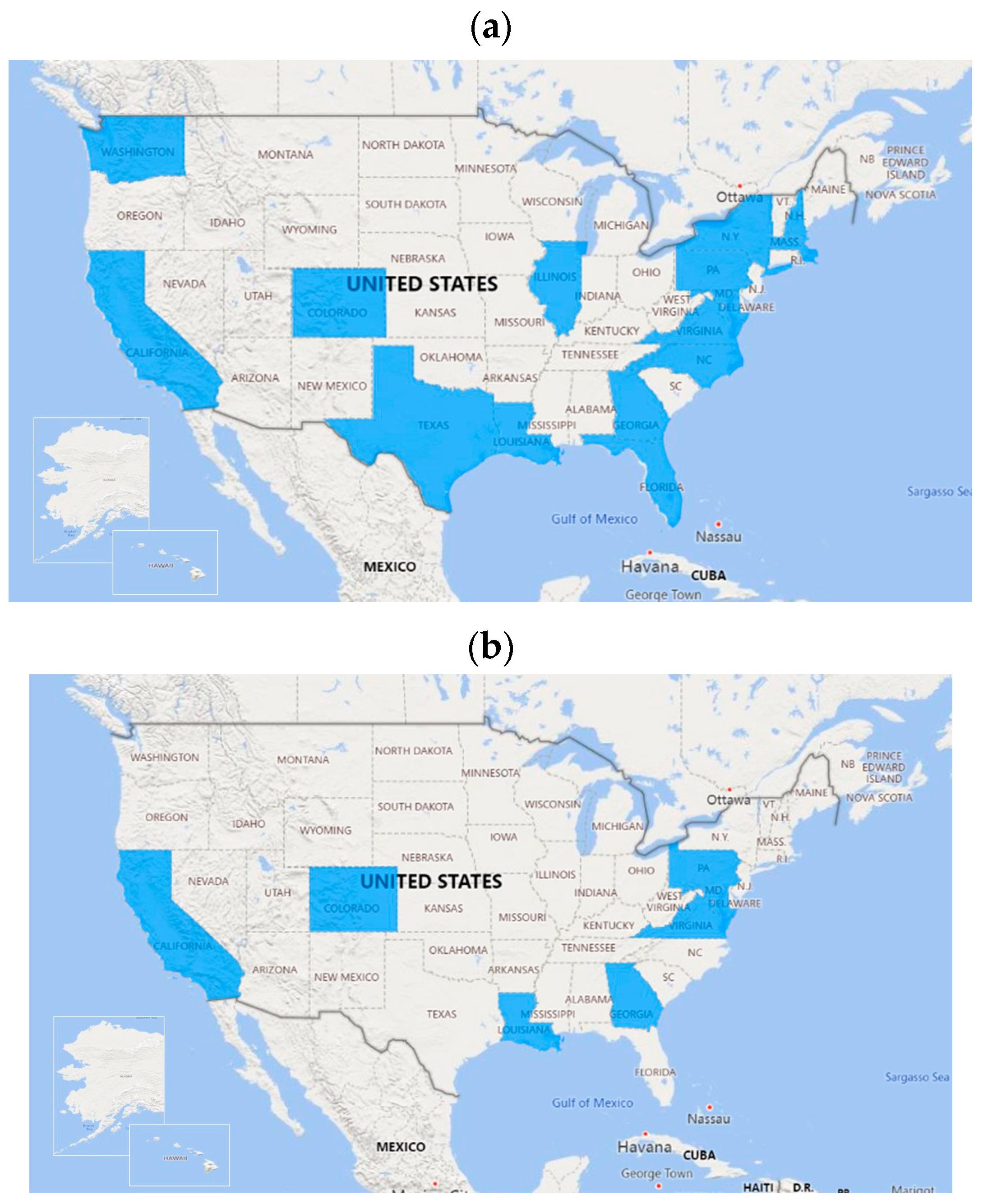
Figure 3.
Trends in poliovirus-essential facilities designated in the United States, 2017-2022. Number of active and withdrawn PEFs by year compared to cumulative count of potential PEFs (N=30) identified in national survey.
Figure 3.
Trends in poliovirus-essential facilities designated in the United States, 2017-2022. Number of active and withdrawn PEFs by year compared to cumulative count of potential PEFs (N=30) identified in national survey.
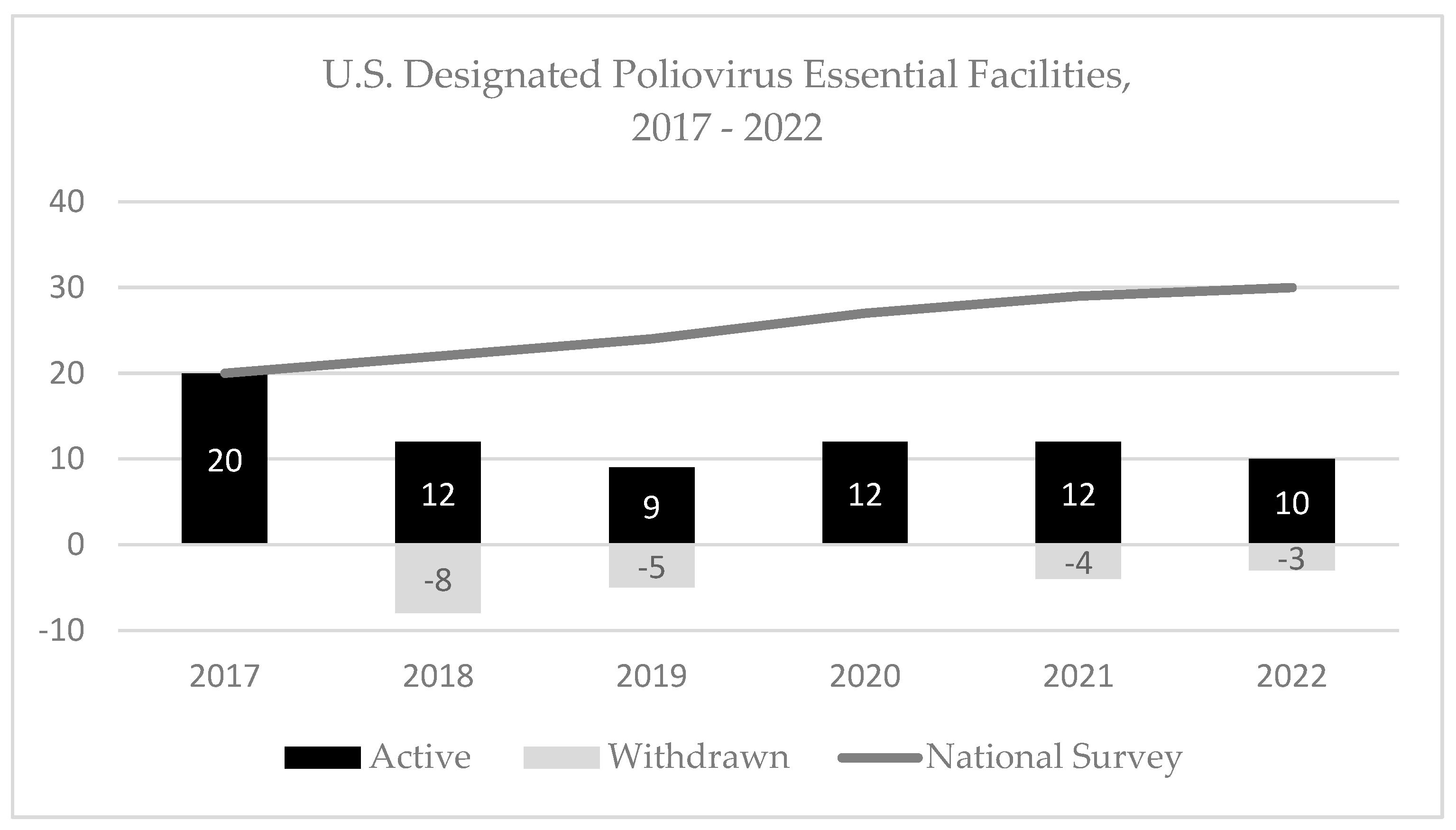
Figure 4.
Risk mitigation strategies implemented by U.S. PEFs at time of site visit (n=27), by category. (a) Biosafety category – seven key biosafety containment strategies. For storage only PEFs or PEFs that did not store PV, certain containment strategies were not applicable. (b) Biosafety category – five personal protective equipment (PPE) containment strategies, (c) Security category – three containment strategies. For freezers located in a PV-dedicated secured laboratory, a secured freezer is not applicable, and (d) Emergency response category – two containment strategies.
Figure 4.
Risk mitigation strategies implemented by U.S. PEFs at time of site visit (n=27), by category. (a) Biosafety category – seven key biosafety containment strategies. For storage only PEFs or PEFs that did not store PV, certain containment strategies were not applicable. (b) Biosafety category – five personal protective equipment (PPE) containment strategies, (c) Security category – three containment strategies. For freezers located in a PV-dedicated secured laboratory, a secured freezer is not applicable, and (d) Emergency response category – two containment strategies.
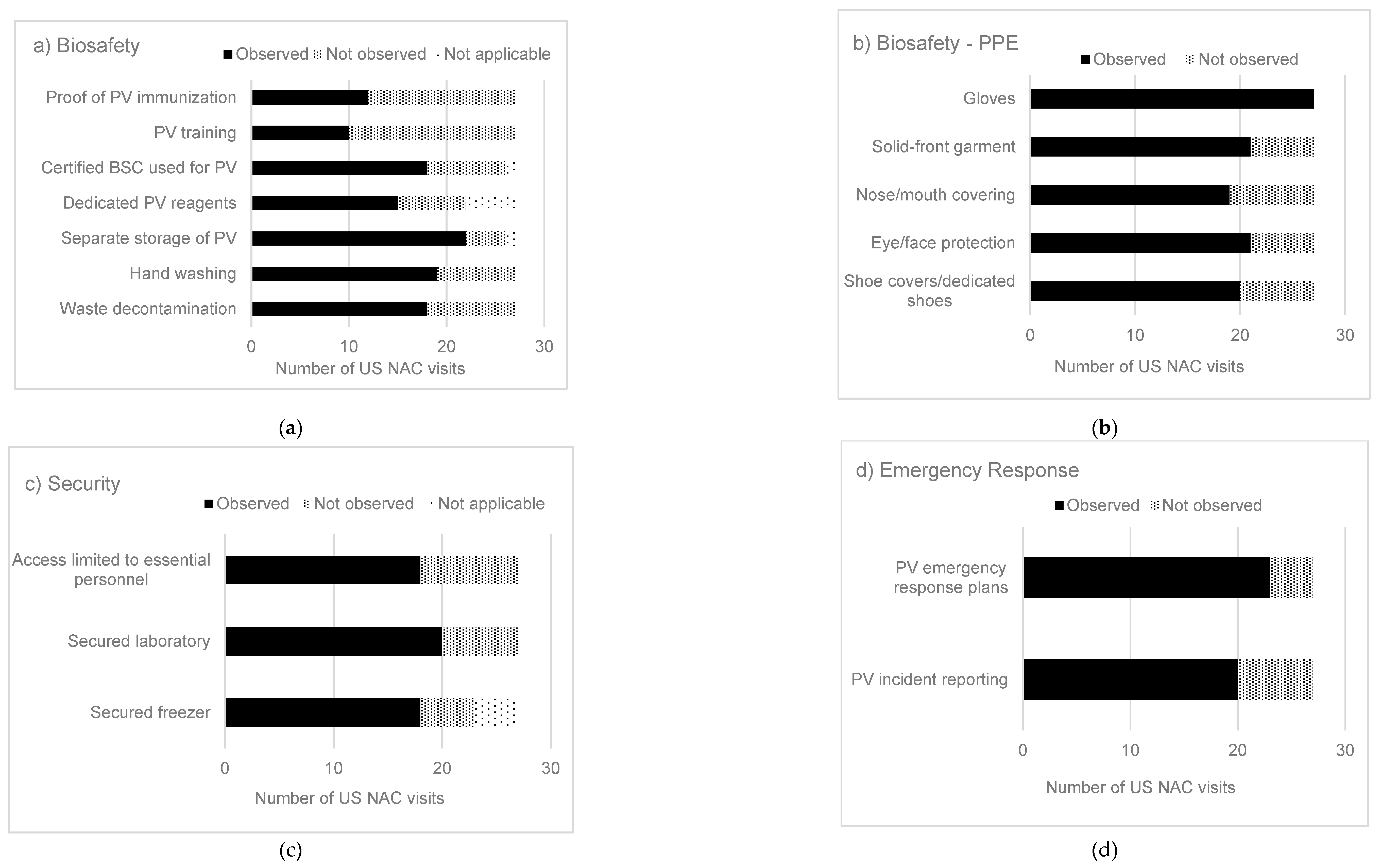

Table 1.
U.S. National Authority for Containment’s Risk Mitigation Strategies for Poliovirus Materials, 2018 - 2022.
Table 1.
U.S. National Authority for Containment’s Risk Mitigation Strategies for Poliovirus Materials, 2018 - 2022.
| No. | Hazard Controla | Category | Risk Mitigation Strategy for Poliovirus Materialsb | Containment Strategies Observed by US NAC |
|
|---|---|---|---|---|---|
| Frequency/No. visits | Percent (%) |
||||
| 1 | Elimination | Biosafety | Destroy unneeded poliovirus materials | 20/27 | 74 |
| 2 | Elimination | Biosafety | Inactivation, fixation or extraction of poliovirus materials | 8/27 | 30 |
| 3 | Engineering | Biosafety | Dedicated room (e.g., an isolation room within a larger laboratory) used for poliovirus | 8/27 | 30 |
| 4 | Engineering | Biosafety | Two doors are present between public areas and the laboratory room | 25/27 | 93 |
| 5 | Engineering | Biosafety | Certified BSC used for poliovirus work | 18/27 | 67 |
| 6 | Engineering | Biosafety | Centrifuge safety cups/sealed rotors that are loaded and unloaded in a BSC for poliovirus work | 11/27 | 41 |
| 7 | Engineering | Biosafety | Containment caging system with HEPA filtered exhaust used for housing PV-infected animals | 2/13 | 15 |
| 8 | Administrative | Biosafety | Risk assessments for poliovirus containment | 9/13 | 69 |
| 9 | Administrative | Biosafety | Risk assessments for animal work | 2/13 | 15 |
| 10 | Administrative | Biosafety | PV work reviewed/approved by institutional committees (i.e., institutional biosafety committee (IBC), institutional animal care and use committee (IACUC)) | 4/13 | 31 |
| 11 | Administrative | Biosafety | Dedicated BSC and incubator used for poliovirus | 10/27 | 37 |
| 12 | Administrative | Biosafety | Dedicated caging system used for PV-inoculated animals | 1/13 | 8 |
| 13 | Administrative | Biosafety | Shared laboratory uses PV spatial and temporal separation with appropriate decontamination procedures | 9/27 | 33 |
| 14 | Administrative | Biosafety | Personnel trained in poliovirus biosafety and security practices | 10/27 | 37 |
| 15 | Administrative | Biosafety | Personnel receive annual refresher training | 5/13 | 38 |
| 16 | Administrative | Biosafety | Personnel provide proof of poliovirus immunization | 12/27 | 44 |
| 17 | Administrative | Biosafety | Personnel enrolled in occupational health program | 12/27 | 44 |
| 18 | Administrative | Biosafety | Personnel competent in good microbiological techniques | 17/27 | 63 |
| 19 | Administrative | Biosafety | Personnel wash hands prior to exit of the laboratory | 19/27 | 70 |
| 20 | Administrative | Biosafety | Protective clothing and gloves removed prior to exit from the laboratory | 16/27 | 59 |
| 21 | Administrative | Biosafety | Reusable PPE is decontaminated prior to storage and reuse | 12/27 | 44 |
| 22 | Administrative | Biosafety | Disposable PPE is treated as biohazardous waste | 22/27 | 81 |
| 23 | Administrative | Biosafety | Durable leak proof transport container used when poliovirus is removed from primary containment | 17/27 | 63 |
| 24 | Administrative | Biosafety | Dedicated reagents used for poliovirus | 15/27 | 55 |
| 25 | Administrative | Biosafety | Segregate poliovirus from all other materials (e.g., in own clearly labeled freezer box) | 22/27 | 81 |
| 26 | Administrative | Biosafety | Perform work with one poliovirus serotype at a time to minimize potential cross-contamination (when possible) | 6/13 | 46 |
| 27 | Administrative | Biosafety | Decontamination of work surfaces | 18/27 | 67 |
| 28 | Administrative | Biosafety | All materials leaving the laboratory are decontaminated using an appropriate method (autoclave, incinerator) | 18/27 | 67 |
| 29 | Administrative | Biosafety | Periodic validation of autoclave decontamination procedures | 21/27 | 78 |
| 30 | Administrative | Biosafety | Containers with poliovirus are surface disinfected prior to removal from the BSC | 13/27 | 48 |
| 31 | Administrative | Biosafety | Procedures for decontamination of equipment are implemented | 14/27 | 52 |
| 32 | Administrative | Biosafety | Chemical treatment known to inactivate poliovirus implemented | 7/27 | 26 |
| 33 | Administrative | Security | Locked freezer where poliovirus is stored (when stored outside a dedicated, secured laboratory) | 18/27 | 67 |
| 34 | Administrative | Security | Locked laboratory | 20/27 | 74 |
| 35 | Administrative | Security | Limit access to personnel identified as essential by the facility | 18/27 | 67 |
| 36 | Administrative | Security | Poliovirus inventory records are current, accurate and complete | 7/13 | 54 |
| 37 | Administrative | Security | Poliovirus animal tracking and infected tissue inventory records | 1/13 | 8 |
| 38 | Administrative | Security | Security policies implemented for controlled access to poliovirus materials and areas | 9/13 | 69 |
| 39 | Administrative | Security | Individual entries into poliovirus areas are documented (e.g., electronic record, manual logbooks) | 8/13 | 61 |
| 40 | Administrative | Security | Visitor policy for entering poliovirus areas | 6/13 | 46 |
| 41 | Administrative | Emergency Response | Emergency response plans developed, including measures to protect personnel and the environment in the event of a releasec | 23/27 | 85 |
| 42 | Administrative | Emergency Response | Personnel report accidents or incidents with PV per institutional policy | 20/27 | 74 |
| 43 | Administrative | Emergency Response | Notify appropriate state and local agencies of possession of PV materials | 8/13 | 61 |
| 44 | Administrative | Emergency Response | Develop and coordinate emergency response plans with first responders | 7/13 | 54 |
| 45 | Administrative | Emergency Response | Develop response procedures for PV-infected escaped animals | 1/13 | 8 |
| 46 | PPEd | Biosafety | Protective laboratory clothing with a solid-front (e.g., disposable wrap-around gown, scrubs, coverall) | 21/27 | 78 |
| 47 | PPE | Biosafety | Gloves (double gloves are recommended) | 27/27 | 100 |
| 48 | PPE | Biosafety | Face or surgical mask or respirator | 19/27 | 70 |
| 49 | PPE | Biosafety | Eye and face protection for anticipated splashes or sprays (e.g., safety glasses, face shield) | 21/27 | 78 |
| 50 | PPE | Biosafety | Shoe covers or dedicated shoes | 20/27 | 74 |
aAdapted from Hierarchy of Controls = elimination, substitution, engineering controls, administrative controls, and personal protective equipment (PPE) in Hierarchy of Controls Workplace Safety & Health Topics Web site; CDC/The National Institute for Occupational Safety and Health (NIOSH), 2015. Available at: https://www.cdc.gov/niosh/topics/hierarchy/default.html. bU.S. NAC risk mitigation strategies (n=35) were implemented for poliovirus type 2 in 2018; additional risk mitigation strategies (n=15, numbers 7-10, 12, 15, 26, 36-40, 43-45) were implemented in late 2020 for WPV2/VDPV2, OPV2 and WPV3/VDPV3 materials. cIn October 2021, risk mitigation strategy for emergency response plans was updated to align response procedures for potential poliovirus exposures with WHO guidance. dPPE – personal protective equipment.
Table 2.
U.S. Poliovirus-Essential Facilities Participation in Containment Certification and Application Processing Times, 2018-2022.
Table 2.
U.S. Poliovirus-Essential Facilities Participation in Containment Certification and Application Processing Times, 2018-2022.
| CCSa Process | PEF Participation in Certification | Frequency (N=30) | Percent (%) | Time (days) | |
|---|---|---|---|---|---|
| Median | Range | ||||
| Option A | Facility submits CP application | 20 | 67 | - | - |
| USA requirement | i. Implement risk mitigation strategies | 18/20 | 90 | 83 | 3-418 |
| Step 1 | ii. NAC endorsement | 17/20 | 85 | 84 | 3-418 |
| Step 2 | iii. WHO review | 17/20 | 85 | 10 | 1-128 |
| Step 3 | iv. GCC-CWG review | 17/20 | 85 | 22 | 1-77 |
| Step 4 | v. GCC endorsementb | 16/20 | 80 | 12.5 | 1-463 |
| Step 5 | vi. CP issuedc | 15/20 | 75 | 233 | 91-678 |
| Step 6 | vii. Facility withdraws from certificationd | ||||
| - | • before US NAC endorsement | 3/20 | 15 | 39 | 38-373 |
| - | • before GCC endorsement | 1/20 | 5 | 608 | - |
| - | • ends work under valid CP | 6/20 | 30 | 841.5 | 151-1471 |
| Option B | No participation, destroy or transfer PV | 10 | 33 | - | - |
aCCS – Containment Certification Scheme [13]. bGCC returned 3 applications as ‘unsatisfactory’; 2 of 3 facilities reapplied and received GCC endorsement. cOne GCC-endorsed PEF plans to destroy WPV2, WPV3 and retain WPV1 only, US NAC issuance of certificate pending (data as of June 2023). dThree potential PEFs withdrew from containment certification scheme prior to US NAC endorsement (n=2 destroyed PV materials, n=1 opted not to receive PV materials). One PEF opted to transfer PV materials to another PEF instead of reapplication to achieve GCC endorsement. Six PEFs concluded work with containment PV strains under a valid CP and were withdrawn from containment certification as of 31 December 2022.
Table 3.
Characteristics, Laboratory Design, and Laboratory Features of U.S. Poliovirus-Essential Facilities (PEF).
Table 3.
Characteristics, Laboratory Design, and Laboratory Features of U.S. Poliovirus-Essential Facilities (PEF).
| PEF Characteristicsa | 27 Laboratory Featuresb | ||||
|---|---|---|---|---|---|
| N=18 PEFs | Frequency (N=18) |
Percent (%) |
PV Laboratory Sites (operated in 18 PEFs) | Frequency (n= 20) |
Percent (%) |
| Facility primary work objective | Containment boundary | ||||
| Biomedical research | 9 | 50 | Containment perimeter sealable for gaseous decontamination | 5 | 25 |
| Clinical diagnostic laboratory | 1 | 6 | Facility is equipped with a double-door personnel airlock/anteroom | 7 | 35 |
| Public health laboratory | 4 | 22 | Double doors are interlocked (physical or procedural) | 5 | 25 |
| Industrial/production laboratory | 2 | 11 | Backflow prevention on all services/ utilities passing across the boundary | 2 | 10 |
| Other | 2 | 11 | Sinks and Showers | ||
| Virus typec | Hands-free/automated hand washing sink | 8 | 40 | ||
| WPV2/VDPV2 | 9 | 50 | Personal exit shower | 4 | 20 |
| WPV3/VDPV3 | 6 | 33 | Personal walk-through exit shower | 2 | 10 |
| OPV/Sabin 2 | 12 | 67 | Emergency shower | 16 | 80 |
| nOPV2 | 6 | 33 | Ventilation System | ||
| Work type(s)d | Controlled air system maintains inward directional airflow | 11 | 55 | ||
| Research | 12 | 67 | Exhaust air is HEPA filtered | 7 | 35 |
| Vaccine production | 0 | 0 | Dedicated ventilation system to PV area (exhaust and supply) | 2 | 10 |
| Clinical trials | 3 | 17 | Backflow protection on supply air | 4 | 20 |
| Animal model | 4 | 22 | Ductwork sealable for gaseous decontamination | 4 | 20 |
| Diagnostics | 3 | 17 | Monitors/alarms to ensure directional airflow can be readily validated | 5 | 25 |
| QC testinge | 3 | 17 | Decontamination Systems | ||
| Storage only | 3 | 17 | Single door autoclave | 7 | 35 |
| Certification goalf | Pass-through autoclave | 5 | 25 | ||
| Certificate of Participation (CP) | 12 | 67 | Material airlock/decontamination chamber sealable for gaseous decontamination | 1 | 5 |
| Interim Certificate of Containment (ICC) | 1 | 5 | Dunk tank containing sufficient active compound to inactivate poliovirus | 1 | 5 |
| Certificate of Containment (CC) | 5 | 28 | Effluent decontamination system | 1 | 5 |
| Security | |||||
| Entry door(s) equipped with lock/lock cylinder rated as burglary resistant | 17 | 85 | |||
| Laboratory Design | Frequency (n = 20) |
Percent (%) | Lock(s) fail secure and allow egress only | 11 | 55 |
| Designg | Locked door with two-factor access control measure | 6 | 30 | ||
| A/BSL-3 | 4 | 20 | Video surveillance | 13 | 65 |
| A/BSL-2 | 13 | 65 | Two-person system for PV work | 7 | 35 |
| Storage only | 3 | 15 | Intrusion detection system | 8 | 40 |
| Facility perimeter is subject to constant monitoring | 13 | 65 | |||
| Facility is located on a secure site with perimeter control | 9 | 45 | |||
aPEFs (N=18, operated in 20 PV laboratory sites) with CP applications and preliminary containment conditions verified by US NAC. bPhysical laboratory features, when available, were reported with a list of preliminary containment conditions to GCC. These 27 laboratory features were not required by US NAC for endorsement of a CP. cWPV – wild poliovirus, VDPV – vaccine derived poliovirus, OPV – oral polio vaccine, nOPV- novel oral polio vaccine. 10 PEFs retain a combination of virus types. dWork type(s) –11 PEFs with one work type, 7 PEFs with more than one work type. eQC – quality control. fCertification goal -three facilities changed between CC and CP only goals, one facility changed from ICC to CP only goal compared to initial CP applications received. gA/BSL = animal/biosafety level. Data as of 31 Dec 2022.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



