
Submitted:
09 January 2024
Posted:
09 January 2024
You are already at the latest version
Abstract
: Crohn’s disease (CD) is a multifactorial chronic disorder that involves a combination of factors as genetic, immune response and gut microbiota. Actually, the therapy comprises salicylates, immunosuppressive agents, corticosteroids, biologic drugs. International guidelines don’t recommend the use of antibiotics except for septic complications of CD patients. The increased evidence of the implication of gut bacteria in this chronic disease support the rationale for using antibiotics as primary treatment of active CD. In the last decades several pathogens have been reported to be involved in the development of CD, but only Escherichia coli (E.coli) species and Mycobacterium avium paratubercolosis (MAP), aroused the interest due to their strong association with CD pathogenesis. Several meta-analyses have been published concerning antibiotic treatment in CD patients but randomized trials of antibiotic treatments against E.coli and MAP did not show prolonged benefits, and only generated conflicting results so much so that several questions are still unresolved regarding trial design, antibiotic dosing, the formulation used, the treatment course and the outcome measures. In this article we attempted to provide an overview and update of the trials on antibiotic treatment in active CD patients taking into account the role of pathogens, the mechanism by which the different antibiotics act on harmful pathogens, and antibiotic resistance. Finally, we also tried to draw new lines for future studies to use antibiotics to treat active CD patients
Keywords:
Crohn’s disease
; Escherichia coli species
; Mycobacterium avium paratuberculosis
; antibiotic therapy.
1. Introduction
Current data suggest that Crohn’s Disease (CD) results from a dysregulation of the mucosal immune system in genetically predisposed individuals which leads to a strong and ongoing activation of the immunological response towards intestinal microflora [1].
What is the trigger of the onset of CD is still now an open question, despite of the countless progress that has been made in the definition of genetic and environmental risk factors and in understanding the pathways linked to the immune response that supports the inflammation characteristic of the pathology.
Several pathways are proposed to drive disease [2].
The overall effect of an inflammatory response in CD could be an additional risk factor responsible for development of the disease. In this regard specific molecular events which regulates the production of cytokines such as the loss of function mutations in the genes encoding interleukin (IL)-10, and its receptor (IL-10R) causes early onset in CD. Moreover, the regressive inheritance of rare and low frequency deleterious NOD2 variants contribute to 7-10% of CD cases [3].
The inflammatory response in CD is due by the balance between the key pro and anti-inflammatory cytokines: Tumor Necrosis Factor (TNF)α, IFN-γ, Interleukins (IL)- 1, IL-18, IL-33, IL-36, IL-38 with pro-inflammatory effect and IL-10, IL-4, IL-6. IL-11, IL-13, Trasforming Growth Factor (TGF)-β, as anti-inflammatory ones [3].
Cardinal symptoms of CD are several abdominal pain, diarrhea, bleeding, bowel obstruction and a variety of systemic symptoms affecting the mouth, eyes, joints, skin.
For decades aminosalicylates, immunosuppressive agents, corticosteroids have been the standard of care in active CD for the control of inflammation and to induce clinical remission.
To this days the biological drugs that target the cytokines, such as anti-TNFα, JAK inhibitors , monoclonal α4β7 integrin antibody, and anti IL 12\IL 23 are the armamentarium toobtain clinical and endoscopic remission.
When should therapy be initiated in CD, the route of administration, how to choose first and second biologic, the potential combination therapy with biologics, the safety of biologics, has been recently published in several articles [4,5,6].
However the introduction of anti –TNFα therapy has not yielded expected declines in hospitalization and intestinal resection in IBD [7].
In the last decades several pathogens (Table 1) have been regarded to have a role in the pathogenesis of CD [8,9], but only E.Coli species [10,11,12,13] and Mycobacterium avium paratubercolosis (MAP) [14,15], aroused the interest due to their strong association with CD pathogenesis.
In 1998 a new pathovar strain of E.Coli, defined as ‘Adherent Invasive E. Coli’ (AIEC), was isolated from ileal mucosa of CD patients, assuming that as a potential etiological agent of the disease [16]. AIEC was able to adhere to gut epithelial cells, to invade mucosa, to penetrate and replicate into macrophages and to release inflammatory cytokines [13,17,18,19].
It has been demonstrated that invasive E. coli strains isolated from CD patients, are able to survive and to replicate in large vacuoles within macrophages without inducing cell death.
To survive and replicate in the harsh environment encountered inside this compartment, AIEC strains elaborate several adaptation mechanisms that permit them to resist phagocytosis and to persist within macrophages, releasing large amounts of TNF-α [20].
Several independent studies, conducted by different methods, reported an increased presence , from 25% to 55% , of mucosal associated AIEC in CD patients [21,22,23]. AIEC was also recovered in 65% of chronic lesions and from about 100% of the biopsies from early lesions of CD patients [16].
In two recent reviews, AIEC was found in 23 and 29% of colonic mucosal biopsies from 69 and 304 CD patients, respectively [2,24].
All these studies supported the growing evidence that AIEC could be strongly involved in CD pathogenesis. Until now few studies have been performed related antibiotic treatment in active CD patients targeting AIEC.
In addition to the presence of AIEC, several studies [27,28,29] showed the presence of MAP in intestinal biopsies of active CD patients, and, for many years, it was also supposed that there may be an association between MAP and CD.
Mycobacteria, like AIEC, survive and persist within host macrophages, and effective anti-mycobacteria agents require intracellular penetration.
Recently Khan et al. [2] showed, by a RT-PCR method, a significantly increased prevalence of MAP (23.2%) in biopsy samples from CD patients, as compared to non IBD controls.
Mycobacterium tuberculosis and MAP show different antibiotic sensitivities [30].
Up to now several anti-MAP trials have been performed, some using single and others using up to four drugs [31].
Although some trials and several case reports described mucosal healing and eradication of MAP [32], randomized trials with anti-MAP antibiotic treatment did not show prolonged benefit for CD patients [33,34,35,36].
Townsend et al. showed that short-term antibiotic treatments, useful for induction and remission of active CD patients, were uncertain [37].
Long-term antibiotic treatments trials have been also performed, but several questions have been raised about all factors that could be limiting for the effectiveness of the antibiotic treatment: the trial design, the duration of treatment, dose, and combination of antibiotics.
Until now the choice of antibiotic treatment had always been arbitrary, and the primary endpoint was the clinical and endoscopic remission.
In this article we provide an overview and update of data from trials on antibiotic treatment in active CD patients, taking into account the role of pathogens in the progression of the disease and the mechanism of action of the different antibiotics on the harmful pathogens.
This review gives a brief outlook on the past, present and the future of antibiotic-based therapies for active CD patients.
Since we cannot exclude that the etiopathogenesis of CD may be due to AIEC in some cases and in some others to MAP, we suggest that antibiotic treatment for active CD patients needs to consider the target pathogens.
In fact, if the cause of the pathology is the presence of a specific bacterial species, its eradication should necessarily be a benefit for the regression of inflammation.
In the end we tried to draw up new lines for using antibiotics with personalized therapy in CD patients, taking into account the presence or the absence of a specific bacterial species.
2. Literature Search Strategy
A literature search was conducted using the National Institute of Health (NIH) website (http://www.clinicaltrials.gov) with antibiotic treatment as an intervention in human trials for CD patients targeting MAP and AIEC.
There was no restriction for language, research location, and research race.
We carried out the bibliographic search through the years 2002 to 2023.
The database was chosen because clinical trials around the world are registered on this website and the information are updated daily and all of these were reviewed and approved by the ethics committees or the appropriate agencies and obey the appropriate national/state health agency regulation.
We used advanced search without any language restriction. Invention box was entered “antibiotic Crohn”.
Studies having no relation to antibiotic treatment were excluded.
3. Antibiotic Treatment Targeting MAP in Active CD Patients
Several meta-analyses have been published concerning long-term antibiotic treatment targeting MAP in patients with active CD (Table 2).
Borgaonkar et al. [33] identified six randomized controlled trials (RCTs) using anti MAP therapy for 6 to 24 months. The two trials, both of which used corticosteroids in combination with antimicrobial therapy, yielded a pooled odds ratio (OR) of maintenance of remission in treatment versus controls of 3.37, which was statistically significant (95% CI: 1.38-8.24; p=0.013).
The subgroup analysis of other four trials, which did not use corticosteroids to induce remission, yielded a pooled odds ratio of maintenance of remission in treatment versus control of 0.69 (95% CI: 0.39-1.21), which was not statistically significant (p=0.25).
The pooled OR of maintenance of remission in treatment versus control for all these six studies was 1.10 (95% CI: 0.69-1.74) in favor of treatment, which was not statistically significant (p = 0.78).
These results suggest that antimicrobial therapy is effective in maintaining remission in patients with CD after a course of corticosteroids combined with anti-MAP therapy.
Feller et al [34], in a systematic review and meta-analysis of placebo, controlled trials, examined 13 treatment regimens in 865 patients. The average duration of the treatment was 6 months.
Outcomes were remission in patients with active disease and relapse in patients with inactive disease.
The trials using nitroimidazoles showed benefit with an OR of 3.54. Similarly, the OR for the 4 trials using clofazimine was 2.86.
In reverse, no benefit was evident for classic drugs against tuberculosis (OR=0.58). Results for clarithromycin were heterogeneous (p =0.005), and in three trials with rifaximin the OR was 2.07.
The conclusion of this study was that the long-term treatment with nitroimidazoles or clofazimine or ciprofloxacin appeared to be effective in active CD patients, while little evidence of a benefit was found for clarithromycin and for the classical tuberculosis drugs.
Khan et al [35], in a systematic review including 10 RCTs and 1160 patients, evaluated the antibiotic effect on remission and relapse of adult active CD patients.
Different kinds of antibiotics were tested such as macrolides, fluoroquinolones, 5-nitroimidazole and rifaximin, either alone or in combination, for 4 to 16 weeks.
There was a statistically significant effect of antibiotics to induce remission in active CD patients compared to placebo (OR=0.85; 95% CI: 0.73-0.99).
Selby et al [38], in a double blinded, placebo, controlled trial, studied 213 active CD patients randomized to a 2-year course of daily clarithromycin, rifabutin and clofazimine or placebo in addition to a 16 weeks therapy course of prednisolone.
Primary endpoint was at least one relapse between 12, 24 and 36 months.
Of 122 subjects entering the maintenance phase, 39% taking antibiotics experienced at least one relapse between week 16 and 52, compared to 56% taking placebo (OR: 2.04; p=0.054).
The differences for antibiotics versus placebo patients were not statistically significant.
The authors concluded that the study did not support a significative pathogenic role for MAP in most CD patients.
The Graham multicenter MAP US study [39] was the first global, randomized trial to assess the efficacy of an anti-MAP therapy (RHB-104) for 12 months in active CD patients.
The anti-MAP therapy, in addition to standard therapy, demonstrated a clinical meaningful and statistically significant treatment effect in the protocol, defining a primary endpoint of remission (CDAI < 150) at week 26, along with secondary endpoint of early remission at week 16, and durable remission through week 52.
The remission, with or without anti TNF therapy, was at 26 weeks, significantly higher than placebo (37% vs 23%, p=0.07).
At week 16 the remission was 42% vs 29% (p=0.015).
Agrawal et al. [40] in a small cohort of CD pediatric patients concluded that anti MAP therapy may be effective more than currently utilized therapies for the induction of clinical and endoscopic remission. Although only 47% of patients achieved a clinical remission at their first clinical follow-up, a total of 93% of patients achieved remission at the subsequent follow up appointments after an overage of 5 months of treatment (p<0.001).
Lastly several case series have also been published as concerning long term antibiotic treatment targeting MAP [41,42].
In the Agrawal case series, profound remission was found in CD patients requiring no further treatments for 3-23 years [41].
However, both, trials and case series, gave conflicting results and no definitive conclusions could be drawn about the favorable effect of anti-MAP therapy on the putative MAP infection in CD patients.
Moreover, prophylactic antitubercular therapy was found to accelerate disease progression in patients with CD receiving anti TNF-α therapy [43].
4. Antibiotic Treatment Targeting AIEC in Active CD Patients
Most infections due to intracellular bacteria respond poorly to antibiotic treatment [44].
The lack of antibacterial activity is also due to antibiotic inactivation by the low pH of the phagolysosomes in which antimicrobial bacteria live [45].
Like Coxiella burnetii, Tropheryma whipplei and other several bacteria, also AIEC replicates into the macrophage phagolysosomes.
Wiseman et al. [46] firstly described the effect of pH on the inhibitory activity of chloroquine against E. coli.
Recently, hydroxychloroquine (HCQ) demonstrated to enhance antibiotic efficacy and macrophage killing of AIEC due to its alkalizing effect on the pH of phagolysosomes [47].
In the Flanagan study [48], HCQ showed synergistic effects with doxycycline and ciprofloxacin that are effective antibiotics against intracellular AIEC.
Moreover, both HCQ and vitamin D caused dose dependent inhibition of intramacrophagic AIEC replication after 3 hours from infection [48].
Rodhes et al. [49], in a randomized trial for the treatment of active CD patients, evaluated a prolonged antibiotic treatment with ciprofloxacin, doxycycline and HCQ for 4 weeks, followed by 20 weeks of doxycycline and HCQ, comparing antibiotics with budesonide treatment.
The results, including crossover, showed the remission of 9 on 24 active CD patients treated with HCQ\antibiotics versus only 1 of 32 budesonide treated patients.
Overall results on the efficacy of antibiotic treatment in AIEC positive CD patients are still few and unimpressive.
Further clinical trials will be necessary to assess the efficacy of a combination of antibiotics targeting AIEC.
5. Short Term Antibiotic Treatment
Several RCTs utilizing short term antibiotic treatment for induction and remission of CD produced conflicting results.
Steinart et al [50] in a RCTs including 134 patients treated with metronidazole and ciprofloxacin in combination with budenoside, found no differences in remission rate compared with placebo (OR 1.02,CI 0.62-1.66) (Table 3).
Rahimi et al [51] in a meta-analysis of a broad spectrum antibiotics, found that patients receiving antibacterial theraphy for two weeks up to 24 weeks, were 2.257 times more likely to have clinical improvement than those receiving placebo (Table 3)
Six randomized placebo controlled trials were included in the meta-analysis. Pulling the results from these trials yelded an OR 2.157 (CI 1.678-3.036) from antimycrobial therapy compared with placebo.
The conclusion from this study was that the broad-spectrum antibiotics improved clinical outcomes in patients with CD
Prantera et al [52] in a clinical trial studied 402 CD patients after 12 weeks of rifaximine treatment. 62% of patients were in clinical remission (p<0.005) after the treatment (Table 3).
Wang et al [53] in a meta-analysis of broad spectrum antibiotic therapy, after a treatment of 2-16 weeks, observed a clinical improvement in 56%of patients from antibiotic group and 37.9% in placebo group (OR:1.35 for clinical improvment (Table 3).
Su et al [54] in a systematic review and meta-analysis examined 1407 CD patients. The antibiotics included ciprofloxacin, clarithromicin, metronidazole and rifaximin, for at least 4 weeks. A pooled analysis revealed that, compared with placebo, CD patients benefited to a certain extent (RR 1.32; p<0.00001). However subgroup analysis showed that there was no significant difference between ciprofloxacin and control (Table 3).
Townsend et al [37] analyzed 13 elegible RCTs comparing antibiotics to placebo or active comparator in adult CD patients. Ciprofloxacine, rifaximine, metronidazole, clarithromycine, cothrimoxazole, alone or in combination, provided only a modest benefit for the induction and maintenaince of remission (OD ratio 0.86 at 6-10 weeks, or 0.77 at 10-14 weeks) (Table 3).
Due to the relatively low number of high quality studies on antibiotics, and the high variability in antibiotics trialed, treatment course and outcomes measures, drawing firm conclusions remains difficult.
6. Other Therapeutic Strategies Targeting AIEC
Since antimicrobial resistance was observed to antibiotics considered effective against intracellular AIEC, other possible strategies targeting AIEC have also been proposed:
- -
- Anti-adhesive molecules
Monovalent mannosides are promising candidate for an alternative and complementary approach for CD patients colonized by AIEC [55].
Type-1 pyli are utilized by Gram- bacteria to adhere the host tissue and thus are a key virulence factor in CD.
The type-1 pylus mediated the recognition and attachment of AIEC strain to the host [56].
A mannoside recognizing Fim-H adhesion, blocking the adhesion of bacteria to cells , is found at the type-1 pilus.
Until now a large panel of mannoside derived Fim H antagonist have been tested for the ability to inhibit E.coli adhesion to host cells [57].
- -
- Fecal microbiota transplantation
Fecal microbiota transplantation (FMT) is an emerging approach for IBD treatment, restoring essential components of intestinal flora.
This procedure involves the transfer of processed feces from donors into the gastrointestinal tract of receiving patients. In a recent systematic review and meta-analysis a total of 596 pediatric and adult IBD patients were enrolled to receive FMT therapy [58]. The pooled estimated clinical remission for CD patients was 30 % (CI: 11-52%).
Recently, the efficacy of FMT has been demonstrated in CD patients, in independent studies [59,60,61,62].
In asystematic review and meta-analysis Cheng et al [63] evaluated the efficacy and safety of FMT treatment in CD patients. Twelve trials were analyzed: after FMT treatment 0.62% (CI: 0.48-0.51) of patients achieved clinical remission and 0.79% (CI: 0.71-0.89) clinical response. More adverse events were minor and self-resolved.
- -
- Probiotics, prebiotics, postbiotics
The administration of presumed anti-inflammatory probiotics have been tested in CD patients [64], and the efficacy and safety of probiotics for the induction and remission of CD patients has been reported.
In the Cochrane database of systematic reviews [65] after 6 months of treatment there were no significative differences between probiotic treatment and placebo for the induction of remission in CD (OR 1.06; CI: 0.65-1.71).
The colicin, as species-specific antibiotics, were also investigated.
Colicin enter AIEC containing vacuoles within macrophages and could be delivered either as a purified protein or through colic producing bacteria.
The use of E. coli Nissle 1917, as a Colicin producing prebiotic, allowed these bacteria to secrete the selected colicin which was toxic for AIEC strain [66].
The colicin could be potentially useful to target specific pathogens such as AIEC, in which maintenance of a healthy microbiome is desirable.
- -
- Phage therapy
Phage therapy is a biological treatment against bacterial infection.
The use of phage therapy targets only a limited number of bacterial strains.
An interesting study showed that LF82-P2, LF82-P6 and LF82-P8 phages were effective against AIEC in a mouse model [67].
Galtier et al [68] found that a single day of oral treatment with bacteriophages significantly decreased intestinal colonization by LF82 AIEC strain.
Phage therapy has been explored as promising tool for the eradication of AIEC in CD [69].
Moreover, phage therapy against AIEC, in CD patients, was found safe and effective [70].
- -
- Stem cells
Nowadays stem cells therapy is widely implied in treating CD.
Although mesenchymal and adipose-derived tissue stem cells provide to be safe in treating CD, there is still a lack of evidence on the efficacy of stem cells therapy for active CD.
Moreover, there are still debates on a optimal protocol to use such therapy in these patients. [71].
Recently, it has been reported the mechanism of healing of CD patients after mesenchimal stem cells therapy.
7. Discussion
The effectiveness of antibiotics coupled with their most favorable adverse effect profile and lower cost, compared with biologic drugs or immunomodulators, represent a more attractive therapeutic option for moderate or severe active CD treatment.
Generally, the use of traditional antibiotics has shown poor efficacy in active CD, so they are mostly indicated to treat septic complication in postoperative settings.
The rationale for using antibiotics as primary treatment for CD is based on the increased evidence implicating gut bacteria in the pathogenesis of the disease.
However, until when the target organism and its site of action (intracellular or extracellular) are unknown, the choice of antibiotics can only be arbitrary, and the use of a single antibiotic for a short-term treatment can result in an antibiotic resistance [44].
Overall, in the Annual Epidemiological Report for 2021 [72], in the European Union, E. coli was the most commonly bacteria species (39.4%) with antimicrobial resistance of all reported cases.
Antimicrobial agents such as penicillins, cephalosporins and aminoglycosides, which penetrate poorly into macrophages, are generally ineffective in diseases induced by pathogens allocated within macrophages (Figure 1).
On the contrary, azithromycin, ciprofloxacin, clarithromycin, rifampin, sulfamethoxazole, tetracycline and trimethoprim have been demonstrated to be effective against pathogens such as E.coli or MAP internalized by macrophages (Figure 1).
For these reasons, a combination therapy using antibiotics penetrating macrophages may provide a more effective treatment, when targeting AIEC [73].
It has been reported that acid condition of phagolysosomes, in which E. coli is located, inhibits the antibiotic activity. HCQ, as alkalinizing agent, demonstrated synergistic effects with doxycycline and ciprofloxacin, enhancing antibiotic efficacy against intramacrophagic AIEC [47,48].
Rodhes et al [49] found no significant differences in remission or response rates at 10, 24 or 52 weeks between the antibiotics/HCQ combination and a standard 12-week course of budesonide, when assessed with intention to treat-analysis.
In this study, to eradicate AIEC in CD patients, ciprofloxacin was used only for 4 weeks, and doxycycline was used alone for 20 weeks, an antibiotic treatment used for too short time to get a favorable response.
It is our opinion that the unfavorable results of Rhodes’s trial were due to antibiotic resistance.
Dogan et al [74] showed that AIEC resistance to one or more antimicrobials agents was present in 75% of AIEC colonized CD patients and in 60% of AIEC colonized normal ileum patients (p<0.05).
None of these strains was simultaneously resistant to ciprofloxacin, tetracycline, and trimethoprim.
In AIEC colonized CD patients resistance to ciprofloxacin, tetracycline, clarithromycin, rifampicin and trimethoprim\sulfamethoxazole was found in 25%, 50%, 37.5%, 37.5% and 50%, respectively [73].
It has also been supposed for years that there may be association between MAP and CD.
Several RCTs showed favorable but conflicting results in the clinical remission of CD patients after prolonged therapy with multiple anti MAP drugs [39,40,41].
Unfortunately, only in few trials a MAP detection was performed before treatment, often using inconsistent methods such as cultured techniques which have many limitations, including poor sensitivity.
Moreover, in all trials carried out, the primary endpoint to antibiotic treatment was always the clinical and endoscopic remission and the relapse, evaluated by CDAI and SES-CD.
6. Conclusions
In the light of the data in literature we can’t exclude that the etiopathogenesis of some CD patients may be due to AIEC in some cases and in some others to MAP and that the antibiotic treatment for active CD patients needs to consider the target pathogens.
In active CD patients, colonized by AIEC or MAP, a combination of antibiotics penetrating macrophages should be done for at least 6 months to avoid antimicrobial resistance.
The primary endpoint should be the eradication of the pathogens at the end of treatment.
Finally, the secondary endpoint could be the clinical and endoscopic remission by using CDAI and SES-CD.
7. Future Directions
For all patients with a new diagnosis of CD, by clinical and endoscopic findings, we recommend detecting AIEC and MAP in ileal\colonic mucosal biopsies by using RT-PCR methods.
In AIEC associated active CD patients, the antibiotic therapy could be made with a combination of multiples macrophage penetrating antibiotics.
To avoid the antibiotic resistance, HCQ could also be used in combination with ciprofloxacin, tetracycline, and trimethoprim for at least 6 months (Figure 2).
In case of MAP associated active CD patients, we suggest the anti-MAP therapy for a long-term treatment through 6 months with rifabutin, clarithromycin and clofazimine (Figure 2).
For all AIEC or MAP colonized CD patients, treated with anti-microbial therapy, the primary endpoints should be the eradication of AIEC or MAP, carried out at the end of treatment, by RT- PCR methods (Figure 2).
The secondary endpoints could be clinical and endoscopic remission, evaluated by CDAI\SES CD.
Finally, conventional therapy could be suggested only for not associated AIEC or MAP CD patients (Figure 2).
Author Contributions
Conceptualization and draft, Gaetano Iaquinto; writing—review and editing, Vera Rotondi Aufiero; review, editing and supervision, Carmine Sellitto, Giuseppe Mazzarella, Antonio De Luca, Salvatore Iaquinto, Angelica Lucariello and Raffaele Melina.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roda G, Chien Ng S, Kotze PG, et al. Crohn's disease [published correction appears in Nat Rev Dis Primers. 2020 Apr 6;6(1):26] [published correction appears in Nat Rev Dis Primers. 2020 May 20;6(1):42] [published correction appears in Nat Rev Dis Primers. 2020 Jun 19;6(1):51]. Nat Rev Dis Primers. 2020;6(1):22]. [CrossRef]
- Khan IA, Nayak B, Markandey M, et al. Differential prevalence of pathobionts and host gene polymorphisms in chronic inflammatory intestinal diseases: Crohn's disease and inte-stinal tuberculosis. PLoS One 2021, 16, e0256098. [CrossRef]
- Vebr M, Pomahačová R, Sýkora J, Schwarz J. A Narrative Review of Cytokine Networks: Pathophysiological and Therapeutic Implications for Inflammatory Bowel Disease Patho-genesis. Biomedicines. 2023, 11, 3229. [CrossRef]
- Queiroz NSF, Barros LL, Azevedo MFC, Oba J, Sobrado CW, Carlos AS, Milani LR, Sipahi AM, Damião AOMC. Management of inflammatory bowel disease patients in the COVID-19 pandemic era: a Brazilian tertiary referral center guidance. Clinics (Sao Paulo). 2020, 75, e1909. [Google Scholar] [CrossRef]
- Liefferinckx C, Cremer A, Franchimont D. Switching biologics used in inflammatory bowel diseases: how to deal with in practice? Current Opinion in Pharmacology 2020, 55, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Colombel JF, Panaccione R, Bossuyt P, et al. Effect of tight control management on Crohn's disease (CALM): a multicentre, randomised, controlled phase 3 trial [published cor-rection appears in Lancet. 2018, 390, 2768]. Lancet 2017, 390, 2779–2789. [Google Scholar] [CrossRef]
- Murthy SK, Begum J, Benchimol EI, et al. Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study. Gut 2020, 69, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Ahmed M, Metwaly A, Haller D. Modeling microbe-host interaction in the pathogene-sis of Crohn's disease. Int J Med Microbiol. 2021, 311, 151489. [Google Scholar] [CrossRef]
- Iaquinto G., Rotondi Aufiero V., Mazzarella G. et al. Pathogens in Crohn’s disease: the role of Adherent Invasive Escherichia Coli. [CrossRef]
- Mirsepasi-Lauridsen HC, Vallance BA, Krogfelt KA, Petersen AM. Escherichia coli Pathobionts Associated with Inflammatory Bowel Disease. Clin Microbiol Rev. 2019, 32, e00060-18. [Google Scholar] [CrossRef]
- Palmela C, Chevarin C, Xu Z, et al. Adherent-invasive Escherichia coli in inflammatory bowel disease. Gut. 2018, 67, 574–587. [Google Scholar] [CrossRef] [PubMed]
- Shaler CR, Elhenawy W, Coombes BK. The Unique Lifestyle of Crohn's Disease-Associated Adherent-Invasive Esch-erichia coli. J Mol Biol. 2019, 431, 2970–2981. [Google Scholar] [CrossRef] [PubMed]
- Zheng L, Duan SL, Dai YC, Wu SC. Role of adherent invasive Escherichia coli in pathogenesis of inflammatory bowel disease. World J Clin Cases. 2022, 10, 11671–11689. [Google Scholar] [CrossRef]
- Agrawal G, Aitken J, Hamblin H, Collins M, Borody TJ. Putting Crohn's on the MAP: Five Common Questions on the Contribution of Mycobacterium avium subspecies paratuberculosis to the Pathophysiology of Crohn's Disease. Dig Dis Sci. 2021, 66, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Aitken JM, Phan K, Bodman SE, et al. A Mycobacterium species for Crohn's disease? Pathology. 2021, 53, 818–823. [Google Scholar] [CrossRef]
- Darfeuille-Michaud A, Neut C, Barnich N, et al. Presence of adherent Escherichia coli strains in ileal mucosa of patients with Crohn's disease. Gastroenterology. 1998, 115, 1405–13. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella G, Perna A, Marano A, et al. Pathogenic Role of Associated Adherent-Invasive Escherichia coli in Crohn's Disease. J Cell Physiol. 2017, 232, 2860–2868. [Google Scholar] [CrossRef] [PubMed]
- Lee JG, Han DS, Jo SV, et al. Characteristics and pathogenic role of adherent-invasive Escherichia coli in inflammatory bowel disease: Potential impact on clinical outcomes. PLoS One 2019, 14, e0216165. [Google Scholar] [CrossRef]
- Mansour S, Asrar T, Elhenawy W. The multifaceted virulence of ad-herent-invasive Escherichia coli. Gut Microbes. 2023, 15, 2172669. [Google Scholar] [CrossRef]
- Glasser AL, Boudeau J, Barnich N, et al. Adherent invasive Escherichia coli strains from patients with Crohn’s disease survive and replicate within macrophages without inducing host cell death. Infect Immun 2001, 69, 5529–5537. [Google Scholar] [CrossRef]
- Campbell J., Borody, T. J., & Leis, S.. The many faces of Crohn’s disease: latest concepts in etiology. Open J Int Med 2012, 2, 107. [CrossRef]
- Darfeuille-Michaud A, Boudeau J, Bulois P, et al. High prevalence of adherent-invasive Escherichia coli associated with ileal mucosa in Crohn's disease. Gastroenterology 2004, 127, 412–421. [Google Scholar] [CrossRef]
- Vazeille E, Fumery M, et al. Faster and less invasive tools to identify patients with ileal colonization by adherent-invasive E. coli in Crohn's disease. United European Gastroenterol J. 2021, 9, 1007–1018. [Google Scholar] [CrossRef] [PubMed]
- Nadalian B, Yadegar A, Houri H, et al. Prevalence of the pathobiont adherent-invasive Escherichia coli and inflammatory bowel disease: a systematic review and meta-analysis. Journal of Gastroenterology and Hepatology. 2021, 36, 852–863. [Google Scholar] [CrossRef] [PubMed]
- Petersen, AM. Gastrointestinal dysbiosis and Escherichia coli pathobionts in inflammatory bowel diseases. APMIS. 2022, 130 (Suppl. 144), 1–38. [Google Scholar] [CrossRef] [PubMed]
- Rhodes JM, Subramanian S, Flanagan PK, et al. Randomized Trial of Ciprofloxacin Doxycycline and Hydroxychloroquine Versus Budesonide in Active Crohn's Disease. Dig Dis Sci. 2021, 66, 2700–2711. [Google Scholar] [CrossRef] [PubMed]
- Aitken JM, Phan K, Bodman SE, et al. A Mycobacterium species for Crohn's disease? Pathology 2021, 53, 818–823. [Google Scholar] [CrossRef]
- Naser SA, Sagramsingh SR, Naser AS, et al. Mycobacterium avium subspecies paratuberculosis causes Crohn’s disease in some inflammatory bowel disease patients. World J Gastroenterol 2014, 20, 7403–7415. [Google Scholar] [CrossRef] [PubMed]
- Autschbach F, Eisold S, Hinz U, et al. High prevalence of Mycobacterium avium subspecies paratuberculosis IS900 DNA in gut tissues from individuals with Crohn's disease. Gut 2005, 54, 944–949. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, RJ. Is Crohn's disease caused by a mycobacterium? Comparisons with le-prosy, tuberculosis, and Johne's disease. Lancet Infect Dis. 2003, 3, 507–514. [Google Scholar] [CrossRef]
- Mintz MJ, Lukin DJ. Mycobacterium avium subspecies paratuberculosis (MAP) and Crohn's disease: the debate continues. Transl Gastroenterol Hepatol. 2023, 8, 28. [Google Scholar] [CrossRef]
- Chamberlin W, Borody TJ, Campbell J. Primary treatment of Crohn's disease: combi-ned antibiotics taking center stage. Expert Rev Clin Immunol. 2011, 7, 751–760. [Google Scholar] [CrossRef]
- Borgaonkar MR, MacIntosh DG, Fardy JM. A meta-analysis of anti mycobacterial therapy for Crohn’s disease. Am J Gastroenterol. 2000, 95, 725–729. [Google Scholar] [CrossRef]
- Feller M, Huwiler K, Schoepfer A, et al. Long-term antibiotic treatment for Crohn's disease: systematic review and me-ta-analysis of placebo-controlled trials. Clin. Infect. Dis. 2010, 50, 473–480. [Google Scholar] [CrossRef]
- Khan J, Ullman TA, Ford AC, et al. Antibiotic therapy in inflammatory bowel disease: a systematic review and meta-analysis. Am J Gastroenterol. 2011, 106, 661–673. [Google Scholar] [CrossRef]
- Savarino E, Bertani L, Ceccarelli L, et al. Antimicrobial treatment with the fixed-dose antibiotic combination RHB-104 for Mycobacterium avium subspecies paratuberculosis in Crohn's disease: pharmacological and clinical implications. Expert Opin Biol Ther. 2019, 19, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Townsend CM, Parker CE, MacDonald JK, et al. Antibiotics for induction and maintenance of remission in Crohn's disease. Cochrane Database Syst Rev. 2019, 2, CD012730. [Google Scholar] [CrossRef]
- Selby W, Pavli P, Crotty B, et al. Antibiotics in Crohn's Disease Study Group. Two-year combination antibiotic therapy with clarithromycin, rifabutin, and clofazimine for Crohn's disease. Gastroenterology 2007, 132, 2313–2319. [Google Scholar] [CrossRef] [PubMed]
- Graham D, Naser S, Offman E, et al. RHB-104, a Fixed-Dose, Oral Antibiotic Combination Against Mycobacterium Avium Paratuberculosis (MAP) Infection, Is Effective in Moderately to Severely Active Crohn's Disease. The American Journal of Gastroenterology 2019, 114, S376–S377. [Google Scholar] [CrossRef]
- Agrawal G, Hamblin H, Clancy A, Borody T. Anti-Mycobacterial Antibiotic Therapy Induc-es Remission in Active Paediatric Crohn's Disease. Microorganisms. 2020, 8, 1112. [Google Scholar] [CrossRef] [PubMed]
- Agrawal G, Clancy A, Huynh R, et al. Profound remission in Crohn's disease requiring no further treatment for 3-23 years: a case series. Gut pathogens 2020, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Honap, S., Johnston, E.L., Agrawal, G., Al-Hakim, B., Hermon-Taylor, J., & Sanderson, J.D. An-ti-Mycobacterium paratuberculosis (MAP) therapy for Crohn’s disease: an overview and update. Frontline Gastroenterology 2020, 12, 397–403. [CrossRef]
- Liu F, Tang J, Ye L, Tan J, Qiu Y, Hu F, He J, Chen B, He Y, Zeng Z, Mao R, Cao Q, Gao X, Chen M. Prophylactic Antitubercular Therapy Is Associated With Accelerated Disease Pro-gression in Patients With Crohn's Disease Receiving Anti-TNF Therapy: A Retrospective Multicenter Study. Clin Transl Gastroenterol. 2022, 13, e00493. [Google Scholar] [CrossRef] [PubMed]
- Demarre G, Prudent V, Schenk H, et al. The Crohn's disease-associated Escherichia coli strain LF82 relies on SOS and stringent responses to survive, multiply and tolerate antibi-otics within macrophages. PLoS Pathog. 2019, 15, e1008123. [Google Scholar] [CrossRef]
- Munita JM, Arias CA. Mechanisms of Antibiotic Resistance. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef]
- Wiseman, D. The effect of pH on the inhibitory activity of chloroquine against Esche-richia coli. J Pharm. Pharmacol. 1972, 24, 162P. [Google Scholar]
- Flanagan PK, Campbell BJ, Rhodes JM. Hydroxychloroquine as a treatment for Crohn's disease: enhancing antibiotic efficacy and macrophage killing of E coli. Gut 2012, 61, A60–A61. [Google Scholar] [CrossRef]
- Flanagan PK, Chiewchengchol D, Wright HL, et al. Killing of Escherichia coli by Crohn's Disease Monocyte-derived Macrophages and Its Enhancement by Hydroxychloroquine and Vitamin D. Inflamm. Bowel Dis. 2015, 21, 1499–1510. [Google Scholar] [CrossRef] [PubMed]
- Rhodes JM, Subramanian S, Flanagan PK, et al. Randomized Trial of Ciprofloxacin Doxycy-cline and Hydroxychloroquine Versus Budesonide in Active Crohn's Disease. Dig Dis Sci. 2021, 66, 2700–2711. [Google Scholar] [CrossRef]
- Steinhart AH, Feagan BG, Wong CJ, et al. Combined budesonide and antibiotic therapy for active Crohn's disease: a randomized controlled trial. Gastroenterology. 2002, 123, 33–40. [Google Scholar] [CrossRef]
- Rahimi R, Nikfar S, Rezaie A, Abdollahi M. A meta-analysis of broad-spectrum anti-biotic therapy in patients with active Crohn's disease. Clin Ther. 2006, 28, 1983–1988. [Google Scholar] [CrossRef]
- Prantera C, Lochs H, Grimaldi M, et al. Rifaximin-extended intestinal release induces remission in patients with moderately active Crohn's disease. Gastroenterology. 2012, 142, 473–481.e4. [Google Scholar] [CrossRef]
- Wang SL, Wang ZR, Yang CQ. Meta-analysis of broad-spectrum antibiotic therapy in patients with active inflammatory bowel disease. Exp Ther Med. 2012, 4, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Su JW, Ma JJ, Zhang HJ. Use of antibiotics in patients with Crohn's disease: a syste-matic review and meta-analysis. J Dig Dis. 2015, 16, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Sivignon A, Bouckaert J, Bernard J , et al. The potential of FimH as a novel therapeutic target for the treatment of Crohn’s disease, Expert Opinion on Therapeutic Targets. Expert Opinion on Therapeutic Targets 2017, 21, 837–847. [CrossRef] [PubMed]
- Barnich N, Carvalho FA, Glasser AL, Darcha C, Jantscheff P, Allez M, Peeters H, Bommelaer G, Desreumaux P, Colombel JF, Darfeuille-Michaud A. CEACAM6 acts as a receptor for adherent-invasive E. coli, supporting ileal mucosa colonization in Crohn disease. J Clin Invest. 2007, 117. [CrossRef]
- Mydock-McGrane, L. K., Hannan, T. J., &Janetka, J. W. Rational design strate-gies for FimH antagonists: new drugs on the horizon for urinary tract infection and Crohn's disease. Expert opinion on drug discovery 2017, 12, 711–731. [CrossRef]
- Fang, H., Fu, L., & Wang, J. Protocol for Fecal Microbiota Transplantation in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. BioMed research international 2018, 2018, 8941340. [CrossRef]
- Gordon, H., & Harbord, M. A patient with severe Crohn's colitis responds to Faecal Microbiota Transplantation. Journal of Crohn's & colitis 2014, 8, 256–257. [CrossRef]
- Cui, B., Feng, Q., Wang, H., Wang, M., Peng, Z., Li, P., Huang, G., Liu, Z., Wu, P., Fan, Z., Ji, G., Wang, X., Wu, K., Fan, D., & Zhang, F. Fecal microbiota transplantation through mid-gut for refractory Crohn's disease: safety, feasibility, and efficacy trial results. Journal of gastroenterology and hepatology 2015, 30, 51–58. [CrossRef]
- Kao D, Hotte N, Gillevet P, Madsen K. Fecal micro-biota transplantation inducing remission in Crohn's colitis and the associ-ated changes in fecal microbial profile. J Clin Gastroenterol 2014, 48, 625–628. [Google Scholar] [CrossRef]
- Vermeire S, Joossens M, Verbeke K, et al. Pilot Study on the safety and efficacy of faecal microbiota transplanta-tion in re-fractory Crohn's disease. Paper presented at: Digestive Diseases Week 2012; 2012 May 19-22; San Diego, CA. Gastroenterology 2012, 142, S360. [Google Scholar] [CrossRef]
- Cheng, F., Huang, Z., Wei, W., & Li, Z. Fecal microbiota transplantation for Crohn's disease: a systematic review and me-ta-analysis. Techniques in coloproctology 2021, 25, 495–504. [CrossRef]
- Tsilingiri, K., & Rescigno, M. Postbiotics: what else? Beneficial microbes 2013, 4, 101–107. [CrossRef]
- Limketkai, B. N., Akobeng, A. K., Gordon, M., &Adepoju, A. A. Probiotics for in-duction of remission in Crohn's disease. The Cochrane database of systematic reviews 2020, 7, CD006634. [CrossRef]
- Kotłowski, R. Use of Escherichia coli Nissle 1917 producing recombinant colicins for treatment of IBD patients. Med Hypotheses. 2016, 93, 8–10. [Google Scholar] [CrossRef]
- Sivignon A, Chervy M, Chevarin C, Ragot E, Billard E, Denizot J, Barnich N. An adherent-invasive Escherichia coli-colonized mouse model to evaluate microbiota-targeting strategies in Crohn's disease. Dis Model Mech. 2022, 15, dmm049707. [Google Scholar] [CrossRef]
- Galtier, M., De Sordi, L., Sivignon, A., de Vallée, A., Maura, D., Neut, C., Rahmouni, O., Wannerberger, K., Darfeuille-Michaud, A., Desreumaux, P., Barnich, N., &Debarbieux, L. Bacteriophages Targeting Adherent Invasive Escherichia coli Strains as a Promising New Treatment for Crohn's Disease. Journal of Crohn's & coli-tis 2017, 11, 840–847. [CrossRef]
- Gutiérrez, B., & Domingo-Calap, P. Phage Therapy in Gastrointestinal Diseas-es. Microorganisms 2020, 8, 1420. [CrossRef]
- Bou-cher, D., &Barnich, N. Phage Therapy Against Adherent-invasive E. coli: Towards a Promising Treatment of Crohn's Disease Patients? Journal of Crohn's & colitis 2022, 16, 1509–1510. [CrossRef]
- Mohammadi TC, Jazi K, Bolouriyan A, Soleymanitabar A. Stem cells in treatment of crohn's disease: Recent advances and future directions. Transpl Immunol. 2023, 80, 101903. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe/European Centre for Disease Prevention and Control. An-timicrobial resistance surveillance in Europe 2022 – 2020 data. Copenhagen: WHO Region-al Office for Europe; 2022.
- Subramanian S, Roberts CL, Hart CA, et al. Replication of Colonic Crohn's Disease Mucosal Escherichia coli Isolates within Macrophages and Their Susceptibility to Antibiotics. Anti-microb. Agents Chemother. 2008, 52, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Dogan B, Scherl E, Bosworth B, et al. Multidrug resistance is common in Escherichia coli associated with ileal Crohn's disease. Inflamm. Bowel Dis. 2013, 19, 141–150. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mechanisms by which antibiotics act on harmful pathogens.
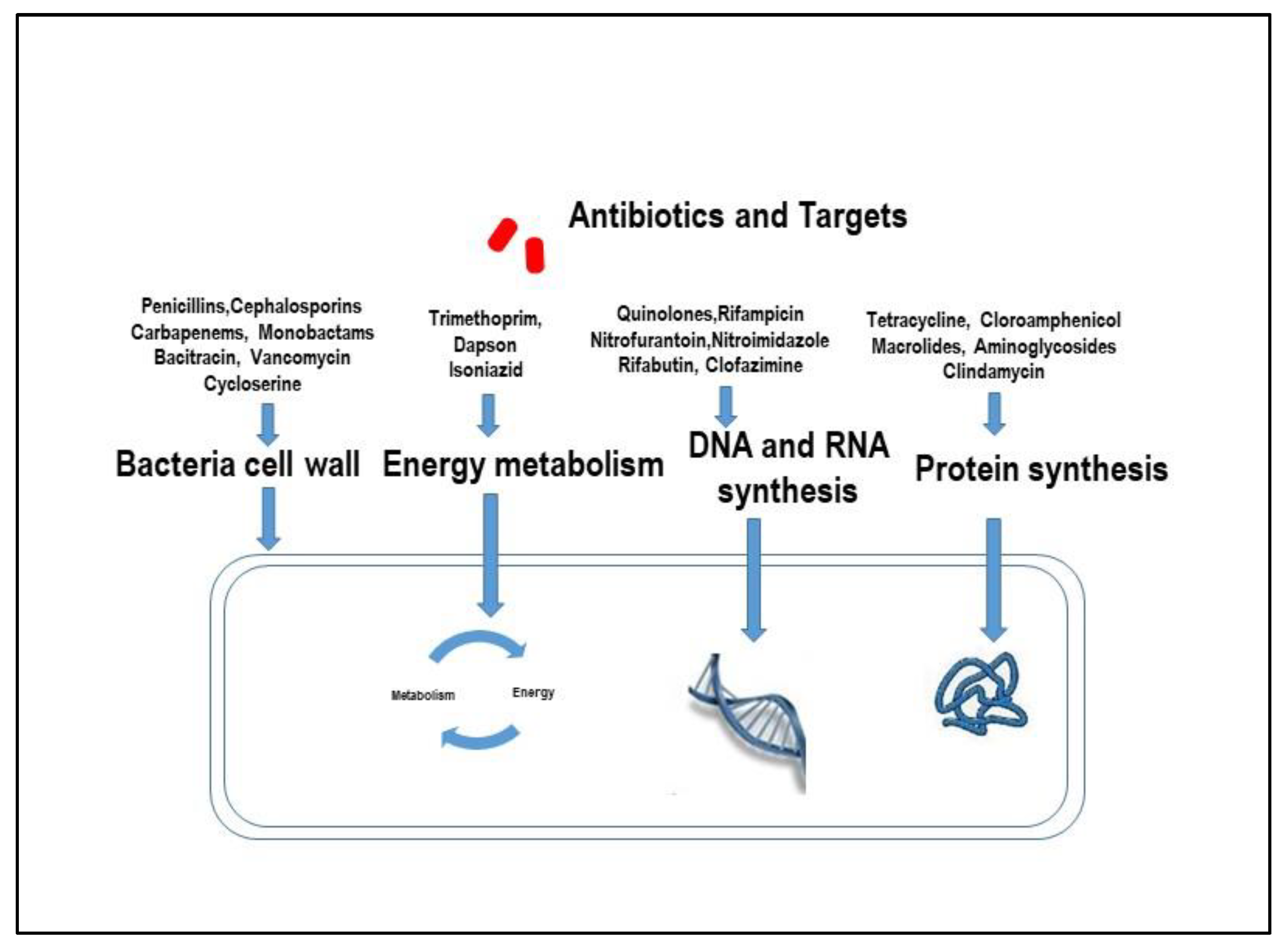
Figure 2.
Schematic workflow for antibiotic treatment of active CD patients (HCQ: Hydroxychloroquine; AIEC: Adherent Invasive E. coli; MAP: Mycobacterium Avium Paratubercolosis; CDAI; Crohn’s Disease Activity Index; SES-CD: Simple Endoscopic Score for Crohn’s Disease; RT-PCR: Real Time Polymerase Chain Reaction).
Figure 2.
Schematic workflow for antibiotic treatment of active CD patients (HCQ: Hydroxychloroquine; AIEC: Adherent Invasive E. coli; MAP: Mycobacterium Avium Paratubercolosis; CDAI; Crohn’s Disease Activity Index; SES-CD: Simple Endoscopic Score for Crohn’s Disease; RT-PCR: Real Time Polymerase Chain Reaction).
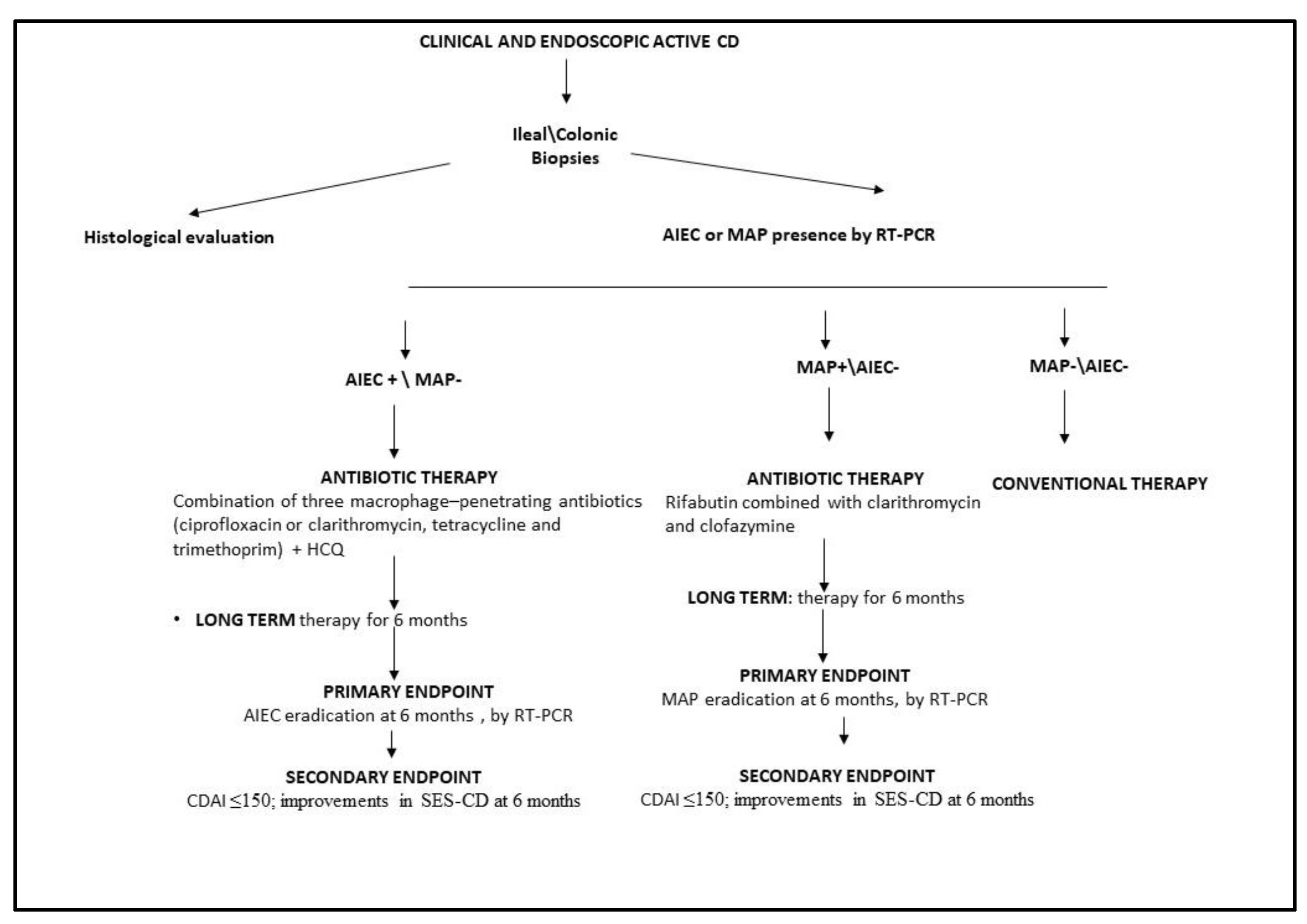

Table 1.
Pathogens potentially involved in CD.
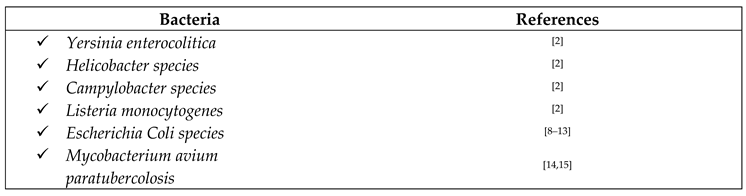 |
Table 2.
Long-term antibiotic treatment targeting MAP in active CD patients.
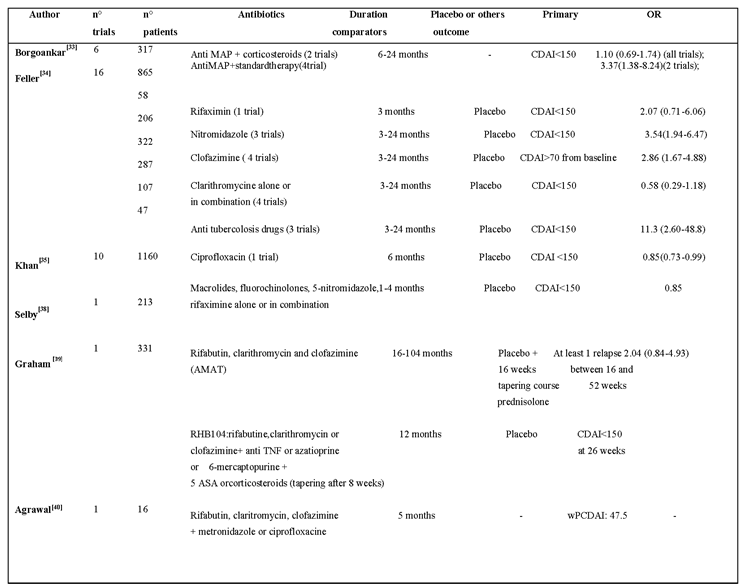 |
Table legend: OR: Odds Ratio; CDAI: Crohn's Disease Activity Index; wP CDAI: Weighted Pediatric Crohn's Disease Activity Index.
Table 3.
Short-term antibiotic treatment in active CD patients.
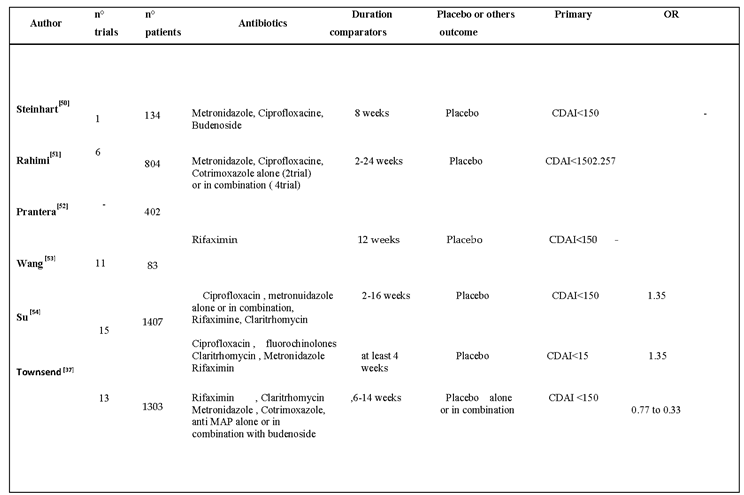 |
Table legend: OR: Odds Ratio; CDAI: Crohn's Disease Activity Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



