
Submitted:
09 January 2024
Posted:
10 January 2024
You are already at the latest version
Abstract
Keywords: Rhinoplasty - Augmentation rhinoplasty - Open rhinoplasty - Facial rejuvenation – Centrofacial lipofilling.
Keywords:
Rhinoplasty
; Augmentation rhinoplasty
; Open rhinoplasty
; Facial rejuvenation
; Centrofacial lipofilling
1. Introduction
Rhinoplasty represents one of the most popular plastic surgery procedures according to American Society of Plastic Surgeons [1]. This cosmetic procedure aims to restore harmony and symmetry in nasal shape and volumes trying to reach an ideal standard of beauty.
Historically, the standards of beauty had been always defined on Caucasian people, comparing these ideals to any patients, also defined as non-Caucasian [2,3,4], generating more often unsatisfaction in aesthetic result of the procedure in these patients.
Specifically, the concept of ethnic nose rhinoplasty rose and started defining a surgical procedure usually performed on non-Caucasian people [5]. It represents a great challenge for plastic surgeons. It aims to achieve results reshaping the nose according to patients’ face structure and not pursuing an ideal standard of beauty. In particular, in Afro-American patients the comprehension of facial structure, beauty norms and psychological background is fundamental while performing rhinoplasty. [6,7,8,9]
Lipofilling is gaining importance among plastic surgeons. It is a safe and effective procedure to obtain filler material and its use in facial cosmetic procedure is increasing. As stated before, rhinoplasty procedures have to be tailored on patients’ face and more often age-related volume loss of face and alteration of facial structures (malar hypoplasia, periapical hypoplasia and microgenia) can affect aesthetic outcome. Due to its central position on the face, rhinoplasty should be associated to treatment of other facial structure to optimize overall outcome [10,11]. Fat grafting can represent a safe alternative to facial implant or osteotomies, restoring or recreating volumes of the face with long lasting results [12,13,14,15,16]. Few studies described the use of lipofilling in combination with rhinoplasty. The aim of this study is to retrospectively analyze and describe our technique, the augmentation rhinoplasty and centrofacial lipofilling (ARCL) and evaluating the association of these two surgical techniques in achieving harmonic aesthetic results and patients’ satisfaction.
2. Materials and Methods
Study Design
We retrospectively reviewed patients who underwent ARCL at our clinic in Rio de Janeiro, Brazil, between January 2019 and December 2022.
The indication for rhinoplasty combined with centrofacial lipofilling was given by the aesthetic analysis of the senior author (CWR), or by specific request of the patient for a change in facial appearance or proportions. Rhinoplasty procedures included primary and secondary rhinoplasties for non-Caucasic patients. All patients were aged 18 years or older. All underwent autologous septal or costal cartilage dorsal augmentation rhinoplasty and concurrent centrofacial lipofilling. The minimum follow-up was one year.
Patients were excluded in case of history of nasal trauma, deformities of jaw or face, or congenital anomalies. Missing/incomplete data on demographics (age, sex, smoke habit, drug assumption, indication for surgery, and surgical procedure), as well as missing/incomplete follow-up were also considered exclusion criteria.
Detailed information regarding rhinoplasty and lipofilling procedures and possible complications was shared with all patients at the time of consultation. Informed written consent was obtained from all enrolled patients for analysis and publication of personal data. The article followed the principles of the Declaration of Helsinki.
By reviewing patient records, we analyzed demographics, indications for surgery, surgical procedures, postoperative pain (VAS), and complication rates. The volume of injected fat was quantified for each procedure. Fat grafting specific complications including infection, contour irregularities, cysts formation and fat emboli were also assessed. Photographic documentation was collected both before the surgeries, during the procedures and at the one-year follow-up. No further centrofacial fat grafting procedures were performed during the follow-up period for all patients.
Outcomes of interest consisted of rhinoplasty outcome, such as differences in nasal structures, global symmetry, nose shape and contour, and cartilage donor site morbidity. Furthermore, the results of centrofacial lipofilling were evaluated based on facial harmony, profile vision, femininity, attractiveness and youthfulness improvement analyzed using the modified 5-points Global Aesthetic Improvement Scale (S-GAIS)17. Each parameter presented a preoperative baseline score of 2 points, then it was evaluated based on the following scale: 1 = very much improved, 2 = much improved, 3 = improved, 4 = no change, 5 = worse. Moreover, the overall patient’s satisfaction was investigated according to the rhinoplasty outcomes evaluation (ROE) questionnaire.
The ROE consisted of 6 questions on a scale of 0 to 4, with the highest score related to increased patient satisfaction. The questionnaire was answered anonymously by each patient. The numerical value of each response was added, and the total was divided by 24 and multiplied by 100 to obtain a final result between 0 and 100, where 100 indicated absolute patient satisfaction and 0 indicated absolute disappointment.
Statistical analysis was performed with SPSS software (IBM Corp., Armonk, NY, USA) to test for any correlation between patient demographics and ARCL outcome. Statistical significance was defined as p < 0.05. The senior author designed and performed the described technique for all patients enrolled in the study.
Operative Technique
The operating strategy involves two surgeries performed in the same operating session. First the rhinoplasty, followed by centrofacial lipofilling. A careful preoperative analysis, including markings, is performed to determine the volume and placement area for the fat graft, with the patient in the standing position, before induction of anesthesia. All patients receive intraoperative antibiotic prophylaxis with amoxicillin and clavulanate. Midfacial fat grafting is always performed at the end of the procedure, after rhinoplasty. The main reason is that augmentation rhinoplasty significantly affects the overall facial harmony. As a result, a more precise facial analysis is only possible later, after rhinoplasty.
Rhinoplasty
The rhinoplasty is performed according to the open rhinoplasty technique by the senior author Carlos Weck Roxo. Technical details have been reported in a previous paper [9]. Briefly, the technique involves a dorsal augmentation open rhinoplasty, with costal cartilage grafts, performed under general anesthesia. The costal cartilage is commonly harvested from the sixth or the seventh rib, with a standard inframammary incision of 1,5 cm. Then, the harvested cartilage is cut and shaped into the required grafts. Moreover, some cartilages pieces are cut with a knife to create diced cartilages for dorsum augmentation. An inverted “V” incision of the columella allows for lower lateral cartilages exposure. Then, we proceed with SMASS debulking. Specifically, we separate the SMASS layer (below) and the Subdermic layer (on top), in an avascular plane, preserving vessels. The dissection continues over the upper lateral cartilages and bony dorsum up to the root of the nose.
After adequate dorsal exposure, the need for dorsal augmentation is assessed. Since most ethnic patients present with a low and wide nasal dorsum, with small nasal bones, low-high lateral osteotomies are usually performed, followed by subperiosteal diced cartilage dorsal augmentation until specifically needed. Then, the septoplasty is performed, and extended spreader grafts (ESG) and septal extension graft (SEG) are settled to stabilize and correct the septum and the tip. The lower lateral cartilages are reshaped, while inter-domal or trans-domal sutures allow for fine tip definition. Articulated alar rim grafts (AARGs) are settled to resolve external nasal valve collapse and help prevent nasal contracture and retraction. Finally, if necessary, onlay grafts can be performed for further adjustment of projection and tip definition. PDS 5.0 suture secures our grafts in place. Then, basal view inspection of the nose is performed to evaluate any alar base abnormalities. Eventually, alar base resection is realized to fix the excess flaring of the alar rims. External thermoplastic nasal splint are set and kept in place for one week.
Centrofacial Lipofilling
At the end of the rhinoplasty, we proceed with centrofacial lipofilling. The modified Klein solution (1:1,000,000) is infiltrated at the donor site, which is typically represented by the inner thigh using a 2.4 mm diameter cannula. At least 40 cc of fat are harvested and then decantated for 20 minutes to separate adipose tissue from oil and fluids. In addition, some fat is treated as Microfat for the finest definition. Microfat graft preparation is performed by transferring the harvested fat through the microfat transfer 20 times. Then, both fat and Microfat is passed to 1 ml syringes for subsequent injection.
Fat grafting address the tear through deformity, malar regions, nasolabial folds and the chin. The surgeon’s experience determines the volume of fat grafting in each area. To improve chin projection, a slight overcorrection is suggested in consideration of the higher absorption rate (almost 40%) that typically affects this area. The average volume that is necessary for chin augmentation is variable. A minimum chin augmentation requires 6cc, up to 10-12 cc for greater ones. By contrast, overcorrection is not necessary at the tear through deformity. For tear through deformity correction, 1cc of fat graft is typically injected at the deep layer, above the periosteum, plus another layer, intramuscular, of 1cc of Microfat. Microfat may also be used to treat hollow eye deformity. Similarly, nasolabial folds correction and malar region augmentation is normally accomplished by injecting 2cc of fat per area in each side. Figure 1.
Amoxicillin and clavulanic antibiotic are prescribed for 7 days. Oral Isotretinoin is started 1 week after surgery and continued for at least three months to prevent nasal inflammation and edema. Follow-up is regularly performed up to at least one year after surgery.list the authority that provided approval and the corresponding ethical approval code.
3. Results
Study Population
From January 2019 to December 2023, 307 patients underwent ARCL at our clinic in Rio de Janeiro. The senior author performed all surgeries. The average age was 43.2 years old (range 22-68), 82% were females, 18% were males. 21 (6.8%) were smokers, oral steroids were taken by 12 (3.9%).
A primary rhinoplasty was realized in 217 (70.7%), while secondary rhinoplasty in 90 (29.3%). Fat grafting was directed at the tear trough deformity 250 (81.44%), with an average fat volume of 1.1 cc (range 0.5 – 1.5 cc) on each side, malar region in 269 (87.6%), with an average fat volume 2.2 cc (range 1.75 – 2.5 cc) on each side, nasolabial folds in 190 (61.9%), average fat volume 4.2 cc (range 3–5 cc) on each side and the chin in 230 (75%) average fat volume 8.5 cc (range 5 – 12 cc). The minimum follow-up was 12 months for all patients (average follow-up 14, range 12-24 months).
Outcomes
Successful ARCL has been realized in all enrolled patients. Regarding the ethnic rhinoplasty specific complications, we did not observe any case of nasal contracture, cartilage grafts extrusion or collapse, and skin infection or necrosis. Minor infections were developed by 4 patients, successfully treated with oral antibiotics. For cartilage donor site morbidity, no wound dehiscence, infection or pneumothorax occurred. Secondary surgeries were not required in any cases.
Regarding centrofacial lipofilling, no infection, major contour irregularities, cysts formation and fat emboli occurred, only one case of fat show in lower eyelid. 5 patients complained of facial long edema, but all healed in three months without requiring specific treatments.
Post-operative pain according to VAS score was recorded on post-operative day 1 and day 7. The median value was 4 and 2 respectively.
At the one year follow-up, ARCL outcomes were evaluated by the surgeon and patient’s satisfaction was investigated according to the modified 5 points S-GAIS scale and the ROE questionnaire.
According to the modified S-GAIS scale, the average score for facial harmony was 1.3 (range 1-3), profile vision 1.2 (range 1-2), femininity 2.4 (range 1-4), attractiveness 2.2 (range 1-4), and youthfulness improvement 1.8 (range 1-2).
For the ROE questionary, satisfactory aesthetic results were reported by all patients, revealing a mean postoperative ROE score of 93,2.
Noses projection appears improved, including a defined tip. The nasal augmentation is preserved at the dorsum. No facial asymmetries are observed between the various structures. Fat grafting results are satisfactory, showing overall facial harmony improvement.
The relationship between complication rates and patients’ demographics, such as smoking status (smoker vs non-smoker), reason for surgery (primary vs secondary rhinoplasty), and surgical procedure (tear through deformity vs nasolabial folds vs malar region3.1. Subsection
4. Discussion
The art of rhinoplasty is constantly evolving. Although new surgical approaches, such as preservation rhinoplasty, have been developed in recent times, we believe that the open technique is the most appropriate in ethnic nose. [18,19,20,21] In fact, an open approach offers the best visualization, allowing accurate placement of the graft. An adequate aesthetic reconstruction could be more difficult and limited with classic intranasal techniques.8, [19,20]
Specifically, in augmentation rhinoplasty the use of a strong structural support by various extended spreader grafts (ESP) and septal extension graft (SEG) resulted in significantly better long-term results with maintenance of projection and reduced tip deformities. For this reason, we recommend reconstruction with this kind of graft. In addition, placement of a second partial SEG to delineate the tip makes the structure more stable and straight. [9]
Furthermor, it is crucial to achieve facial harmony that does not distort the physiognomy of non Caucasian patients. [21,22,23,24,25,26]
Centrofacial lipofilling holds pivotal significance in ethnic facial aesthetic surgery, precisely sculpting and enhancing features for diverse patients. This technique, blending artistry with medical precision, addresses age-related volume loss, ensuring natural outcomes. Particularly crucial in non-Caucasian populations, it harmonizes facial structures, emphasizing individualized beauty norms. By tailoring augmentation to patients’ unique facial characteristics, centrofacial lipofilling not only achieves aesthetically pleasing results but also contributes to patients’ cultural identity and satisfaction. [17] In the field of facial cosmetic procedures, this approach is a key tool for achieving personalized and culturally sensitive results for different patients. [27,28,29,30,31,32]
Moreover, according to our experience, lipofilling associated with rhinoplasty promotes anti-inflammatory effects, aiding in facial recovery and optimizing the overall outcome for enhanced patient well-being. [11,12,13,14]
Our study retrospectively analyzed patients who underwent open augmentation Rhinoplasty and Centrofacial Lipofilling (ARCL) in Rio de Janeiro between January 2019 and December 2022. The research focused on tailoring rhinoplasty to non-Caucasian patients, emphasizing ethnic considerations. Lipofilling, an increasingly utilized technique, was employed to address age-related volume loss and enhance overall aesthetic outcomes. The methodology involved a two-stage procedure, starting with rhinoplasty and concluding with centrofacial lipofilling.
The comprehensive evaluation encompassed aesthetic improvements, nasal projection, and facial harmony preservation. Noteworthy, fat grafting demonstrated satisfactory results, contributing to overall facial enhancement in the long term follow up. Specifically, postoperative assessments included the modified 5-point Global Aesthetic Improvement Scale (S-GAIS) and the Rhinoplasty Outcomes Evaluation (ROE) questionnaire. The average S-GAIS scores indicated positive outcomes for facial harmony (1.3), profile vision (1.2), femininity (2.4), attractiveness (2.2), and youthfulness improvement (1.8). The ROE questionnaire reported a mean score of 93.2, indicating high patient satisfaction.
Lastly, no significant complications were observed in ethnic rhinoplasty and lipofilling, with only minor infections promptly treated.
5. Conclusions
We propose our approach (ARCL), employed on a large number of ethnic noses, which can achieve long-term results and high patient satisfaction. This study has demonstrated that the association between augmentation rhinoplasty and centrofacial lipofilling is a safe procedure that contributes to improve functional and aesthetic outcomes. In conclusion, the ARCL technique, combining ethnic rhinoplasty and lipofilling, proved effective in achieving harmonious aesthetic outcomes for non-Caucasian patients. The study’s thorough methodology, including long-term follow-ups and objective assessments, strengthens its contributions to the field of plastic surgery. Future research may further explore variations in patient demographics and refine techniques for even more personalized and successful outcomes.
Author Contributions
M.P.: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. P.S.: Investigation, Writing – original draft. D.S: Validation, Writing – review & editing. R.C.: Conceptualization, Investigation. C.W. R.: Conceptualization, Investigation, Supervision. All authors read and approved the submitted version.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of “Policlinico Universitario Le Scotte, Siena, Italy.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper” if applicable.
Data Availability Statement
Data are available in the database of the instituto Carlos Roxo, Avenida Ayrton Senna n°1850, Rio de Janeiro, RJ 22775-003, Brazil.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- «ASPS Plastic Surgery Statistics 2022», s.d. Available online: https://www.plasticsurgery.org/documents/News/Statistics/2022/plastic-surgery-statistics-report-2022pdf.
- WE Matory Jr e WE Matory. «Definitions of beauty in the ethnic patient», Ethnic Considerations in Facial Aesthetic Surgery; Lippincott-Raven Publishers: Philadelphia, PA, USA, 1998; pp. 61–83. [Google Scholar]
- Steven, M. Hoefflin, Ethnic Rhinoplasty; Springer: New York, NY, USA, 1998. [Google Scholar] [CrossRef]
- Nelson Powell e Brian Humphreys, Proportions of the Aesthetic Face, American Academy of Facial Plastic and Reconstructive Surgery (Series); Thieme-Stratton New York: New York, NY, USA, 1984.
- Cobo, R. Ethnic Rhinoplasty. Facial Plast. Surg. 2019, 35, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Cerrati, E.W.; Thomas, J.R. The multicultural evolution of beauty in facial surgery. Braz. J. Otorhinolaryngol. 2017, 83, 373–374. [Google Scholar] [CrossRef] [PubMed]
- «Psychological Evaluation of Patients Seeking Rhinoplasty», consultato 26 dicembre 2023. Available online: http://www.eajm.org/en/psychological-evaluation-of-patients-seeking-rhinoplasty-132888.
- Bolletta, A.; Losco, L.; Pozzi, M.; Schettino, M.; Cigna, E. A Retrospective Study on Single-Stage Reconstruction of the Ear following Skin Cancer Excision in Elderly Patients. J. Clin. Med. 2022, 11, 838. [Google Scholar] [CrossRef]
- Pozzi, M.; Fàdel, C.; Bolletta, A.; Cuomo, R.; Roxo, C.W. Ethnic rhinoplasty: Preliminary results of our technique in the pursuit of the harmonious nose. J. Plast. Reconstr. Aesthetic Surg. 2023, 87, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Yaremchuk, M.J.; Vibhakar, D. Pyriform Aperture Augmentation as An Adjunct to Rhinoplasty. Clin. Plast. Surg. 2015, 43, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Sykes, J.M.; Suárez, G.A. Chin Advancement, Augmentation, and Reduction as Adjuncts to Rhinoplasty. Clin. Plast. Surg. 2016, 43, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Carvas, M.; Tonnard, P.; Verpaele, A. Rhinoplasty Combined With Centrofacial Lipofilling to Optimize Facial Proportions. Aesthetic Surg. J. Open Forum 2020, 2, ojz034. [Google Scholar] [CrossRef]
- Lindenblatt, N.; van Hulle, A.; Verpaele, A.M.; Tonnard, P.L. The Role of Microfat Grafting in Facial Contouring. Aesthetic Surg. J. 2015, 35, 763–771. [Google Scholar] [CrossRef]
- Krastev, T.K.; et al. Efficacy and Safety of Autologous Fat Transfer in Facial Reconstructive Surgery: A Systematic Review and Meta-Analysis. JAMA Facial Plast. Surg. 2018, 20, 351–60. [Google Scholar] [CrossRef]
- Cuomo, R.; Giardino, F.R.; Pozzi, M.; Nisi, G.; Sisti, A.; Han, J.; Nuzzo, A.; Muratori, A.; Cigna, E.; Losco, L.; et al. Management of skin damage of health workers’ face: the role of plastic surgery in the time of Pandemic. Acta Biomed. 2021, 12, e2021185. [Google Scholar] [CrossRef]
- Coleman, S.R. Structural Fat Grafting: More Than a Permanent Filler. Plast. Reconstr. Surg. 2006, 118, 108S–120S. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.J.; Cha, J.H.; Han, S.-E. Maximizing Thread Usage for Facial Rejuvenation: A Preliminary Patient Study. Aesthetic Plast. Surg. 2020, 45, 528–535. [Google Scholar] [CrossRef]
- Daniel, R.K.; Kosins, A.M. Current Trends in Preservation Rhinoplasty. Aesthetic Surg. J. Open Forum 2020, 2, ojaa003. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.; Shipchandler, T.Z. Update on the evidence for functional rhinoplasty techniques. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Romo, T., 3rd; Abraham, M.T. The ethnic nose. Facial Plast Surg. 2003, 19, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, M.; Marcaccini, G.; Giardino, F.R.; El Araby, M.M.; Nisi, G.; Grimaldi, L.; Cuomo, R. Flowchart in Post-Bariatric Surgery: A Research for the Appropriate Type and Timing of Plasties Reshaping the Body. Aesthetic Plast. Surg. 2023. [Google Scholar] [CrossRef]
- Patel, P.N.; Most, S.P. Concepts of Facial Aesthetics When Considering Ethnic Rhinoplasty. Otolaryngol. Clin. N. Am. 2020, 53, 195–208. [Google Scholar] [CrossRef]
- Pozzi, M.; Cuomo, R.; Giardino, F.R.; Nisi, G.; Grimaldi, L. A case of necrotizing fasciitis from a pedicure: when beauty centers become life-threatening. Acta Biomed. 2022, 93, e2022126. [Google Scholar] [CrossRef]
- Porter, J.P.; Olson, K.L. Anthropometric Facial Analysis of the African American Woman. Arch. Facial Plast. Surg. 2001, 3, 191–197. [Google Scholar] [CrossRef]
- Leong, S.C.; White, P.S. A comparison of aesthetic proportions between the healthy Caucasian nose and the aesthetic ideal. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 248–252. [Google Scholar] [CrossRef]
- Millard, D.R. Adjuncts in augmentation mentoplasty and cor- rective rhinoplasty. Plast Reconstr. Surg. 1965, 36, 48–61. [Google Scholar] [CrossRef]
- Giardino, F.R.; Cuomo, R.; Pozzi, M.; Marcaccini, G.; Bacchini, S.; El Araby, M.M.; Grimaldi, L.; Nisi, G. Erdheim–Chester Disease of the Breast: First Review and First Case of Isolated Severe Gynecomastia. Diagnostics 2023, 13, 1239. [Google Scholar] [CrossRef]
- Bueller, H. Ideal Facial Relationships and Goals. Facial Plast. Surg. 2018, 34, 458–465. [Google Scholar] [CrossRef]
- Hönn, M.; Göz, G. The Ideal of Facial Beauty: A Review. J. Orofac. Orthop. / Fortschritte der Kieferorthopädie 2007, 68, 6–16. [Google Scholar] [CrossRef]
- Susini, P.; Nisi, G.; Pierazzi, D.M.; Giardino, F.R.; Pozzi, M.; Grimaldi, L.; Cuomo, R. Advances on Capsular Contracture—Prevention and Management Strategies: A Narrative Review of the Literature. Plast. Reconstr. Surg. - Glob. Open 2023, 11, e5034. [Google Scholar] [CrossRef]
- Cortese, A.; D’Alessio, G.; Brongo, S.; Amato, M.; Sarno, M.R.; Claudio, P.P. New techniques in relation to new concepts of the aes- thetic of the face: technical considerations and aesthetic evaluation. J Craniofac Surg 2016, 27, e693–e695. [Google Scholar] [CrossRef]
- Betelli, R.; Arruda, G.; Almeida, W.; Grinfeld, A. How to Harmonize the Ethnic Nose. Facial Plast. Surg. 2016, 32, 620–624. [Google Scholar] [CrossRef]
Figure 1.
ARCL procedure. Liposuction at the level of the inner thigh and lipofilling at the end of rhinoplasty are shown.
Figure 1.
ARCL procedure. Liposuction at the level of the inner thigh and lipofilling at the end of rhinoplasty are shown.

Figure 2.
18 months follow-up; 28 y F. Primary rhinoplasty and centrofacial lipofilling.
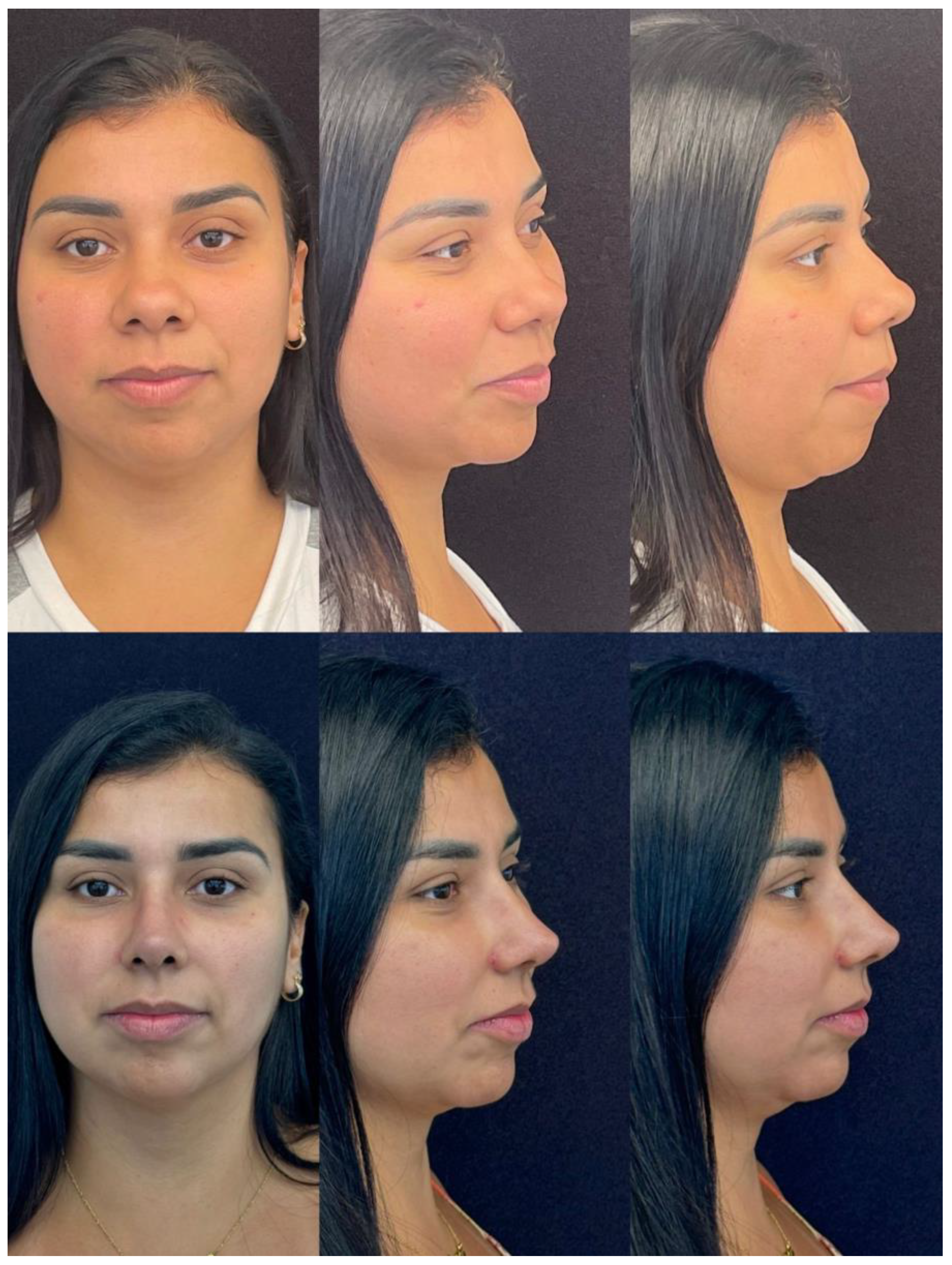
Figure 3.
12 months follow-up, 39 y F. Secondary rhinoplasty and centrofacial lipofilling.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



