
Submitted:
09 January 2024
Posted:
10 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic has led to a substantial revolution in the incorporation of digital solutions in healthcare. This systematic review investigates the enduring physical and psychological consequences individuals experience up to two years post-recovery. Additionally, it focuses on examining the influence of mHealth interventions on these effects. Significantly, 41.7% of survivors experience lingering symptoms that have not been addressed, while 14.1% encounter difficulties in returning to work. The presence of anxiety, compromised respiratory functioning, and persistent symptoms highlight the immediate requirement for specific therapies. Telehealth, particularly telerehabilitation, presents itself as a possible way to address these difficulties. The study thoroughly examines 10 studies encompassing 749 COVID-19 patients, investigating the efficacy of telerehabilitation therapies in addressing various health markers. Telerehabilitation-based breathing exercises yield substantial enhancements in functional performance, dyspnea, and overall well-being. The results emphasize the potential of telerehabilitation to have a favorable effect on patient outcomes, however more research is needed to strengthen the existing evidence basis as one of the most important limitation is the limited number of trials and the evaluation of varied therapies. The analysis highlights the significance of digital solutions in post-COVID care and calls for ongoing research to improve comprehension and implementation of telehealth interventions in a swiftly changing healthcare environment.
Keywords:
telerehabilitation
; COVID-19
; digital healthcare
; post-COVID care
; health-related consequence
; rehabilitation
; COVID-19 sequelae
1. Introduction
COVID-19 as defined by the World Health Organization (WHO) is an infectious disease caused by the SARS-CoV-2 virus, significantly impacting the healthcare system, including rehabilitative care [1]. As the world navigates the multifaceted challenges posed by the COVID-19 pandemic, the repercussions extend beyond the acute phase, giving rise to a critical need for sustained healthcare strategies.
It has been indeed shown that while the majority of individuals affected by COVID-19 experience mild-to-moderate illness, around 10% to 15% develop severe symptoms, with 5% reaching a critical state [2]. The duration of recovery from COVID-19 varies depending on the severity of symptoms, averaging two to three weeks [3]. While pulmonary impairments represent the most common manifestation of COVID-19, there is a plethora of extrapulmonary manifestations [4]. There is a growing body of evidence supporting the notion of extra-respiratory dissemination of coronaviruses. Although the majority of individuals recover fully within 12 weeks post-infection, a significant proportion of patients with history of COVID-19 may encounter various long-term health consequences.
In addition, the pandemic has brought unprecedented challenges to global health and economies, catalyzing a transformative shift towards digital solutions across various industries [5]. Notably, education swiftly embraced remote learning strategies, and health care organizations rapidly adopted digital solutions and advanced technologies to overcome pandemic-induced challenges [6]. While digital tools initially addressed acute needs, the ongoing evolution of these solutions presents an opportunity to define and adopt new models of care. In fact, as a result, the long-anticipated digital transformation in healthcare was accelerated, a change that was previously slower to materialize despite constant introductions of new technologies. The list of emerging digital solutions is expanding rapidly, in health care, encompassing video visits, mobile apps, wearable devices, chatbots, artificial intelligence-powered diagnostics, voice-interface systems, and mobile sensors. This digital revolution has given rise to a new category of services, including the oversight of individuals in home quarantine and large-scale population surveillance.
The International Classification of Functioning (ICF) [7] is of utmost importance in the ever-changing digital healthcare environment and the urgent requirement for continuous healthcare initiatives in the aftermath of the COVID-19 pandemic. The ICF offers a complete structure for comprehending health and states associated to health [8]. It surpasses conventional medical models by integrating social and environmental aspects that impact an individual’s functioning. In light of the complex problems and enduring repercussions of COVID-19, the ICF plays a crucial role in evaluating the comprehensive effects of the virus on individuals’ physical, psychological, and social well-being. By taking into account not just the medical elements but also the wider dimensions of functioning, the ICF allows for a more detailed comprehension of the long-term consequences of COVID-19.
The imperative to combat COVID-19 and the anticipation of recurring waves have underscored the need to review and sustain the digital technologies implemented during the crisis period.
Rehabilitative care faced challenges during the pandemic due to obligated limited contacts between patients and clinicians, necessitating alternatives to face-to-face interactions. Telemedicine and remote consultation have proven effective in maintaining patient care during times when in-person interactions are restricted [9,10,11]. In fact, Telehealth, or telemedicine, emerged as a viable solution, with telerehabilitation specifically addressing therapeutic rehabilitation at a distance using telecommunication technologies [12]. This innovative approach involves active collaboration between healthcare providers and patients, enabling remote prescription and oversight of treatment while patients actively engage in rehabilitation within their daily living context.
Recent efforts sought to unravel this enigma through a comprehensive meta-analysis of survivors’ health-related consequences, shedding light on the landscape of sequelae two years post-SARS-CoV-2 infection [13]. In this meta-analysis, encompassing twelve studies with 1,289,044 participants from 11 countries, the investigation aimed to elucidate the health outcomes and sequelae experienced by COVID-19 survivors at the two-year mark. Alarmingly, 41.7% of survivors continued to grapple with at least one unresolved symptom, while 14.1% found themselves unable to resume work. The spectrum of persistent symptoms included fatigue (27.4%), sleep difficulties (25.1%), impaired diffusion capacity for carbon monoxide (24.6%), hair loss (10.2%), and dyspnea (10.1%). Furthermore, individuals with a history of severe infection exhibited a higher propensity for anxiety and experienced pronounced impairments in respiratory functions. Anxiety was notably prevalent (OR = 1.69), while impairments in forced vital capacity (OR = 9.70), total lung capacity (OR = 3.51), and residual volume (OR = 3.35) persisted after recovery. Factors contributing to a higher risk of long-term sequelae included older age, predominantly female gender, pre-existing medical comorbidities, severe infection status, corticosteroid therapy, and heightened inflammation during the acute phase. These findings underscore the substantial and lingering impact of COVID-19 on survivors, emphasizing the urgent need for intervention strategies. Two years after recovery, a significant proportion of survivors, comprising 41.7%, grapple with neurological, physical, and psychological sequelae. We created an ICF model summarizing the different complications induced by the COVID-19 in Figure 1.
The imperative to preclude persistent or emerging long-term sequelae is evident, prompting a call for targeted interventions to mitigate the risks associated with long COVID. In the evolving landscape of digital healthcare, addressing the extended consequences of COVID-19 becomes integral to ensuring comprehensive and sustained care for affected individuals.
Telemedicine services can be synchronous, involving real-time discussions between patients and healthcare providers, or asynchronous, utilizing a "store-and-forward" technique for the collection and forwarding of medical history and reports, the definition of the different types of services are presented in Figure 2.
Previous reviews demonstrated the feasibility and effectiveness of telerehabilitation during the pandemic, emphasizing its ability to provide ongoing care for patients with various conditions [14]. However, the need for further research, especially in the context of post-pandemic care, was acknowledged. Other reviews specifically investigated the efficacy of telerehabilitation for the management of COVID-19 patients [15,16]. Results revealed that breathing exercises administered via telerehabilitation exhibited a significant improvement in functional scores and breathing function. Despite the low certainty of evidence, adverse events were predominantly mild or moderate, occurring at comparable frequencies in both the telerehabilitation and control groups. The findings collectively suggest that telerehabilitation holds promise in enhancing functional capacity, mitigating dyspnea, improving performance, and addressing physical aspects of quality of life, all while maintaining a low incidence of adverse events [17].
This review aims to contribute additional evidence to reinforce the findings of previous research, extending the focus to the post-COVID era. This work explores perspectives in telerehabilitation research, suggesting its potential as an added value in conventional care beyond the immediate challenges posed by the pandemic.
2. Methods
2.1. Search Strategy
For the literature search, several databases have been consulted for studies published to the first of December 2023. PubMed, Embase and Scopus were searched. MESH terms and title/abstract-based search terms for mobile health (‘mHealth’ OR ‘mobile health’ OR ‘applications’), COVID-19 (‘covid*’ OR ‘SARS-CoV-2’) and rehabilitation (‘rehabilitation’ OR ‘revalidation’ OR ‘reeducation’) were used to retrieve studies. References from selected papers and from other relevant articles were screened for potential additional studies in accordance with the snowball principle. The search was limited to journal articles published in English.
The PRISMA flowchart for updated systematic reviews was followed for screening [18]. All results were uploaded on Rayyan to filter out duplicates and then screening was done independently by 2 reviewers based on title/abstract. Subsequently, the remaining studies were checked for inclusion based on the PICOS criteria (Table 1). In case of conflict, the two reviewers deliberated with each other.
2.2. Eligibility Criteria
The following PICOs criteria were defined to guide our search strategy [19].
2.3. Quality Assessment
The PEDro scale, recognized as a valid and reliable tool for evaluating randomized controlled trials (RCTs), was employed for the assessment of methodological quality [20,21]. The quality of RCTs was independently evaluated by two reviewers in a blinded fashion to mitigate potential methodological bias [22]. Final decisions regarding the quality of each RCT were reached through consensus. In instances of disagreement, a third author was consulted. Consequently, RCTs were categorized into three groups: low quality (0-3 / 10), moderate quality (4-6 / 10), and high quality (7-10 / 10) [22].
2.4. Data Extraction
The following information was extracted from the included studies: characteristics of the patients (age, gender, COVID status), intervention (type, number of sessions, length, frequency, duration), type of control, main outcomes, and conclusions (including feasibility and effectiveness).
2.5. Ethical Approval
This review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations [23]. For the present study, no ethics committee approval was necessary.
3. Results
A comprehensive search utilizing various combinations of search terms yielded a total of 1678 results. Following a curation process involving the examination of titles and abstracts, 225 articles were included. The primary reasons for exclusion were the articles being systematic reviews, feasibility studies, or not directly related to the intended topic.
The remaining articles underwent a thorough full-text review, during which two-hundred fifteen were found to not meet the inclusion criteria. Consequently, the scoping review now comprises a total of 10 articles that met the established criteria. The complete flow chart of study inclusion is presented in Figure 3.
3.1. Characteristics of the Included Studies and Patients
Table 2 provides a comprehensive overview of the 10 included studies, detailing their respective characteristics. In total 749 COVID-19 patients were included in this review: 384 in the intervention group and 362 in the control group.
The studies originated from diverse geographical locations, including China (n = 3), Spain (n = 3), the USA (n = 2), Brazil (n = 1), and Iran (n = 1). The majority of the studies concentrated on the target group of individuals experiencing persistent symptoms such as dyspnea after the acute phase (n = 8). The other included studies focused on hospitalized COVID-19 patients (n = 2). In total the ten studies comprised the results of 749 COVID-19 patients, 384 of them were included in the intervention group and the other 362 in the control group.
3.2. Qualitity Assessment
The PEDro Scale yielded an average score of 8, indicative of a commendable level of methodological quality. The global level of evidence for randomized controlled trials (RCTs) was deemed satisfactory. A summary of the quality assessement is presented in Figure 4.
3.3. Evaluation Variables
Among the included studies, the evaluated aspects were divided into the classification of the ICF model: body and structure, activities and participation.
All studies focus on the domain of body and structure. Only 30 % focuses on activities, and 10% focuses on participation. Only one individual study focuses on the three domains of the ICF – model (see Figure 5).
In the domain of ’body and structure, the recurrent measurements encompassed the six-minute walking test, strength assessment (e.g., hand grip), pulmonary function, dyspnea, anxiety, sleep quality, depression, cardiopulmonary fitness, symptom burden, balance, and fear. Within the activity domain, measurements included physical activity level, step count, functional evaluation, level of independence, quality of life, Sit-to-Stand test, and affective status. Lastly, in the participation domain, measurements such as community social support, social support, and sociodemographic information were collected. Some studies also incorporated non-specific measurements outside the ICF-model, such as assessing the feasibility, usability, and satisfaction of the mHealth tools being utilized.
3.4. Telerehabilitation Methods
The predominant telerehabilitation approaches employed in the selected studies encompassed primarily holistic telerehabilitation applications (n = 4). These applications offered a comprehensive suite of features, including exercises, pulmonary rehabilitation, communication, and information. Additionally, there were applications specifically designed for pulmonary exercise alone (n = 3), as well as remote monitoring apps (n = 2) and remote guidance apps (n = 1). It is to note that different terms were used in the literature, therefore we summarized the different eHealth disciplines in Figure 5 to ease the interpretation of the results and comparison with the literature.
3.5. Clinical Efficacy
The comprehensive analysis of various mHealth interventions for COVID-19 recovery unveiled a spectrum of outcomes. Among these studies was the examination of applications, revealing that significant usage of such mHealth apps correlated with enhanced physical and cognitive function, mental health and quality of life.
3.5.1. Physical Function and Exercise Capacity
Interventions focused on physical function and exercise capacity are crucial in recovering patients’ overall well-being. Churchill et al. (2023) and Rodriguez-Blanco et al., (2021) demonstrate the efficacy of structured physical therapy sessions, resulting in higher step counts and enhanced performance in functional tests [24,25]. These findings emphasize the need of starting rehabilitation early and customizing it to improve mobility and reduce the functional decrease commonly observed during COVID-19 recovery. Capin et al. (2022) have taken a complete strategy that highlights the potential advantages of telerehabilitation [26]. This approach provides a practical way to achieve long-term improvements in exercise capacity and functional results.
3.5.2. Mental Health and Quality of Life
It is crucial to prioritize the mental health components of post-COVID-19 recuperation, as individuals frequently experience psychological discomfort after being unwell. The research conducted by Wei et al. (2020) and Liu et al. (2021) provide insights into therapies targeted at mitigating depression, anxiety, and insomnia [27,28]. The self-help tactics utilized by Wei et al. and the cognitive-behavioral therapy (cCBT) implemented by Liu et al. provide useful insights into the efficacy of focused mental health therapies. From a clinical perspective, it is crucial to include these methods in the post-COVID-19 care process in order to promote a comprehensive strategy that takes into account both the physical and psychological recovery of patients. This will ensure a patient-centered healthcare approach that addresses all aspects of their well-being.
3.5.3. Sleep Quality and Fatigue
The clinical worry regarding the influence of COVID-19 on sleep quality and exhaustion persists beyond the acute period of the illness. Hajibashi et al. (2023) tackle these concerns by employing pulmonary telerehabilitation, which leads to notable enhancements in sleep quality and decreases in fatigue and anxiety [29]. For clinicians in charge of post-COVID-19 care, it is essential to acknowledge and tackle sleep disruptions and exhaustion due to their capacity to hinder recovery and contribute to lasting disability [28].
3.5.4. Cognitive Function
The significance of cognitive function in post-COVID-19 treatment is typically disregarded, although it is highlighted as a crucial factor in the studies conducted by Samper-Pardo et al. (2023) and Campos et al. (2023) [30,31]. These research studies emphasize the favorable correlation between the utilization of applications, remote monitoring, and enhanced cognitive results. For therapists, it is crucial to acknowledge the possible cognitive consequences of COVID-19. It is vital to incorporate cognitive evaluations and specific therapies into rehabilitation. Recognizing the relationship between physical and cognitive health is essential for developing comprehensive care methods that effectively address the complex issues patients encounter during the recovery phase. Healthcare professionals can enhance the overall quality of life and optimize the cognitive well-being of post-COVID-19 patients by implementing therapies that focus on cognition.

Table 2.
Characteristics of the included studies.
| Study, country | Population | Intervention | Control | Outcomes | Results | Quality |
|---|---|---|---|---|---|---|
|
Samper-Pardo et al. 2023 Spain [30] |
100 Primary Health Care long COVID patients (18+) |
n = 52 ReCOVery APP and standard therapy |
n = 48 Treatment as usual methods established by their general practitioner |
Quality of life (SF-36), Sociodemographic variables, self-reported persistent symptoms, use of ReCOVery APP, cognitive domains (MoCA), physical functioning, Affective status (HADS); Sleep quality (ISI), social support (MOS-SS); Community social support (PCSQ), Physical Activity (IPAQ-SF), personal factors | Approximately 25% of participants actively utilized the app. Results from a linear regression model indicate that increased usage time predicts enhanced physical function (b = 0.001; p = 0.005) and community social support (b = 0.004; p = 0.021). Additionally, heightened self-efficacy and health literacy are associated with improved cognitive function (b = 0.346; p = 0.001) and a reduction in symptoms (b = 0.226; p = 0.002). | 8 |
|
Churchill et al., 2023 USA [24] |
44 participants discharged home following hospitalisation with COVID-19 (with and without intensive care unit (ICU) stay) <40 |
n = 27 Physical therapy and education sessions |
n = 14 Weekly check-in calls |
Demographics, Physical function testing, a health diar via fitbit Steps |
Step counts increased in favour of the intervention group (P <.001) culminating in an average daily step count of 7658 (P<.001) at the end of week 3. During the remaining 9 weeks, weekly step counts increased by an average of 67 (P<.001) steps per week, resulting in a final estimate of 8258 (P<.001) |
8 |
|
Hajibashi et al., 2023 Iran [29] |
52 Discharged COVID-19 patients (18–65) |
n = 26 pulmonary telerehabilitation and progressive muscle relaxation for 6 weeks |
n = 26 pulmonary telerehabilitation fir 6 weeks |
Functional capacity and secondary (dyspnoea, anxiety, depression, fatigue, sleep quality, and quality of life | The experimental group showed significantly higher sleep quality (P = 0.001) and significantly lower fatigue (P = 0.041) and anxiety (P = 0.001) than the comparison group. No between-group differences were observed in terms of other outcomes (P > 0.05) | 10 |
|
Campos et al., 2023 Brazil [31] |
37 Adults with persistent symptoms of COVID-19 |
n = 15 Remote monitoring with health guidance |
n = 22 Face to face rehabilitation 8 weeks (2/week) |
Fatigue, dyspnea, and exercise capacity, Lung function, functional status, symptoms of anxiety and depression, attention, memory, handgrip strength, and knee extensor strength were secondary outcome measures | Both groups showed improved fatigue and exercise capacity. Exercise rehabilitation improved dyspnea, anxiety, attention, and short-term memory. | 8 |
|
Capin et al., 2022 USA [26] |
44 Participants discharged home following hospitalisation with COVID-19 (with and without intensive care unit (ICU) stay) |
n = 29 12 individual biobehaviourally informed, app-facilitated, multicomponent telerehabilitation sessions with a licenced physical therapist |
n = 15 Education on exercise and COVID-19 recovery trajectory, physical activity and vitals monitoring, and weekly check-ins with study staff. |
Primary outcome was feasibility, including safety and session adherence. Secondary outcomes included preliminary efficacy outcomes including tests of function and balance; patient-reported outcome measures; a cognitive assessment; and average daily step count. The 30 s chair stand test was the main secondary (efficacy) outcome | 8% (11/29) of the intervention group compared with 60% (9/15) of the control group experienced an AE (p=0.21), most of which were minor, over the course of the 12-week study. 27 of 29 participants (93%; 95% CI 77% to 99%) receiving the intervention attended ≥75% of sessions. Both groups demonstrated clinically meaningful improvement in secondary outcomes with no statistically significant differences between groups. | 8 |
|
Rodriguez-Blanco, 2021 Spain [25] |
36 COVID-19 patients with mild to moderate symptomatology in the acute stage |
n = 18 Muscle conditioning telerehabilitation |
n = 18 No physical activity |
Six-minute walking test, multidimensional dyspnoea-12, thirty seconds sit-to-stand test, and Borg Scale | Both groups were comparable at baseline. Statistically significant improvement between groups (p < 0.05) in favor of the experimental group was obtained. Ninety percent adherence was found in our program. | 6 |
|
Li et al., 2022 China [32] |
120 Formerly hospitalised COVID-19 survivors with remaining dyspnoea complaints |
n = 59 TERECO Unsupervised home-based 6-week exercise programme comprising breathing control and thoracic expansion, aerobic exercise and LMS exercise, delivered via smartphone, and remotely monitored with heart rate telemetry. |
n = 61 Short educational instructions |
6 min walking distance (6MWD), squat time in seconds; pulmonary function assessed by spirometry; HRQOL measured (SF-12) and mMRC-dyspnea. | Adjusted between-group difference in change in 6MWD was 65.45 m (p<0.001) at post-treatment and 68.62 m (p<0.001) at follow-up. Treatment effects for LMS were 20.12 s (p<0.001) post-treatment and 22.23 s (p<0.001) at follow-up. No group differences were found for lung function except post-treatment maximum voluntary ventilation. Increase in SF-12 physical component was greater in the TERECO group with treatment effects estimated as 3.79 (p=0.004) at post-treatment and 2.69 (p=0.045) at follow-up. | 7 |
|
Gonzalez-Gerez et al., 2021 Spain [33] |
38 COVID-19 patients with mild to moderate symptomatology in the acute stage (18 – 75 years old) |
n = 19 Pulmonary rehabilitation |
n = 19 No physical activity |
Six-Minute Walk Test, Multidimensional Dyspnoea-12, Thirty-Second Sit-To-Stand Test, and Borg Scale. | Significant differences were found for all of the outcome measures in favor of the experimental group (P< 0.05). | 9 |
| Wei et al., 2020 China [27] | 26 COVID-19 patients (40 – 50 years old) |
n = 13 Self-help intervention containing four main components: breath relaxation training, mindfulness (body scan), “refuge” skills, and butterfly hug method. |
n = 13 Supportive care |
Hamilton Depression Rating Scale, Hamilton Anxiety Rating Scale | Depression and anxiety were significantly decreased in patients of the intervention group at the end of the first and second weeks when compared with the patients of the control group |
9 |
|
Liu et al., 2021 China [28] |
252 COVID-19 patients (45 – 45 years old) |
n = 126 Computerized cognitive behavioral therapy (cCBT). The system can systematically intervene in patients’cognition, emotions, and behavior through an offline mobile terminal. |
n = 126 Conventional treatment (periodic psychological assessments, general psychological support, and consultations discussing overall well-being and disease activity) |
Hamilton Depression Rating Scale, Hamilton Anxiety Rating Scale, Self-Rating Depression Scale, Self-Rating Anxiety Scale, Athens Insomnia Scale | The cCBT group displayed a significantly decreased scores after the intervention compared to the conventional group (all P<.001). A mixed-effects repeated measures model revealed significant improvement in symptoms of depression, anxiety and insomnia during the postintervention and follow-up periods in the cCBT group | 8 |
4. Discussion
4.1. Main Findings
Our results indicated that mHealth can be used in both patients with acute COVID-19 (i.e., hospitalized patients) and in the chronic phase (i.e., telerehabilitation). Furthermore, the combination of conventional therapy and mHealth supported care emerged as notably more effective in improving sleep quality [28,29,30], alleviating anxiety [27,28,29,30,31], reducing dyspnea [27,28,31,32,33], and reducing fatigue/improving physical function [24,25,26,27,28,29,30,31,32,33]. The results of the different included studies provide robust support for telerehabilitation’s efficacy in addressing dyspnea, muscle strength, ambulation, and depression. While several studies accentuated the multifaceted potential of telerehabilitation in COVID-19 recovery, a contrasting viewpoint emerged, advocating for the indispensability of traditional rehabilitation interventions. Interestingly such type of technology can also been used to monitor the evolution of patients [34], as remote monitoring exhibited promise by fostering increased step counts, suggesting a plausible surrogate for physiological recovery [24]. The variety of approaches highlights the importance of a multidimensional strategy for comprehensive post-COVID-19 care.
These results are in line with the results of a previous review published in 2022 [16]. The findings of this study highlight several positive outcomes associated with telerehabilitation interventions across various health indicators. Breathing exercises delivered through telerehabilitation demonstrated significant improvements in the participation and function items of the ICF: 6-minute walk distance, 30-second sit-to-stand test performance, Multidimensional Dyspnoea-12 questionnaire scores, and perceived effort on the 0-to-10 Borg scale, albeit with low certainty of evidence. These results underscore the potential benefits of telerehabilitation in positively impacting functional performance, dyspnea, and overall well-being, despite the need for further research to strengthen the evidence base.
In this review we focused on COVID-19 patients, but such kind of app can be used with patients suffering from other (chronic) respiratory conditions such as COPD (chronic obstructive pulmonary disease) [35], asthma [36], lung cancer [37], and cystic fibrosis [38]. Moreover, such type of app can also be used with healthy subjects. For example, in a study evaluating and interventions involving Fear of COVID-19 Scale, HAMA, Pittsburgh Sleep Quality Index (PSQI), and EQ-5D-3L, significant improvements were observed in healthy individuals receiving the intervention. The intervention included an information session about COVID-19 at the study’s outset via a mobile phone video application, coupled with a breathing and relaxation exercise program conducted twice daily [39].
Another study found that breathing exercises are feasible even in health individuals. App users positioned their phones adjacent but not proximal to their mouths and the inclusion of onscreen text or video instructional materials did not significantly affect this distance. Participants expressed a clear preference for the app (100%, n=24), citing motivation for sustained inspirations. Notably, app features like gamification (75%, n=18) and breath counter (83.3%, n=20) were well-regarded, emphasizing user satisfaction and engagement [40].
4.2. Limitation of the Systematic Review
The findings of this systematic review must be interpreted in the context of certain limitations. Firstly, the restricted number of incorporated studies and the broad variety of treatments (such as procedures, applications, outcomes, etc.) introduce complexity to the process of comparing and extrapolating the results. While the possibility of expanding the scope of this review to include studies on alternative telerehabilitation systems or those integrating mHealth with additional devices or sensors was taken into account, doing so would have meant sacrificing the practical aspects that are inherent to mHealth, namely, its portability, affordability, and user-friendliness.
This review was limited to RCTs but interesting results can also be found in observational studies. For example, a study analyzing 58 patients discharged from the ICUs found that a mHealth program can improve health-related quality of life breathlessness, symptom burden, weekly mental health status, and COPD Assessment Test indicating a positive impact on symptom burden. Additionally, there were favorable changes in mental health status, as evidenced by a decrease in the Hospital Anxiety and Depression Scale [41].
4.3. Future and Related Works
In this paper we focus on the use of mHealth, while other new approaches and technology can be used to provide (tele)rehabilitation services to patients. We have seen in the methods that mHealth in part of telerehabilitation and more evidence and publication are available concerning telerehabilitation.
Combined with external sensors: 88 individuals experiencing persistent fatigue and dyspnea post-COVID-19 underwent an 8-week supervised home-based respiratory muscle training program. Divided into inspiratory and expiratory training groups, participants engaged in 40-minute daily sessions using a threshold pressure device supervised through a virtual platform. Quality of life improved significantly, but not exercise tolerance. Both inspiratory and expiratory training enhanced respiratory muscle function and lower limb strength without notable effects on lung function or psychological status [42].
Other examples are serious games and virtual reality (VR). In a systematic review, authors analyze the use of VR interventions for the rehabilitation of individuals afflicted with COVID-19. The study identified a predominant emphasis on cognitive rehabilitation, with two papers (66%) employing immersion VR, while one study (33%) utilized non-immersive VR for physical rehabilitation. Notably, virtual reality was delivered to patients in the form of a game in two papers (66%). The results of this research suggest that virtual reality games have the potential to positively impact functional and cognitive outcomes, elevate patient satisfaction levels, and empower individuals to take an active role in their healthcare management. Given the unique challenges faced by COVID-19 patients, the evolving landscape of healthcare delivery, and the critical role of rehabilitation during quarantine, the exploration of novel techniques is imperative to ensure continued treatment, facilitate a return to normalcy, and ultimately improve the overall quality of life for these individuals [43].
Here we focus on patients with COVID-19, however it is crucial to acknowledge the significant burden on the shoulders of healthcare professionals amid this pandemic, which undeniably affects their mental health. mHealth can be used to improve mental wellbeing of the clinicians. In a pilot randomized controlled crossover trial involving 34 clinicians, mHealth demonstrated above-average feasibility and acceptability Significant improvements were observed in anxiety, resilience, and patient-related burnout in the intervention group compared to the waitlisted group after one month, indicating the potential of mHealth in enhancing the well-being of healthcare professionals [44].
More generally speaking, telemedicine also exhibits promising outcomes. It has demonstrated notable improvements in alleviating psychological stress, addressing mental disorders, and significantly reducing overall stress levels among COVID-19 patients. Additionally, telemedicine was proven effective in providing benefits such as tailored monitoring of vital parameters for home-isolated patients, and facilitating clinicians in early identification of clinical deterioration [45].
Utilizing technology and social media-based interventions emerges as a promising approach for advancing health and well-being, particularly in circumstances such as a pandemic [46]. Nevertheless, there is a recognized necessity for the formulation of guidelines regulating social media usage to mitigate potential risks and counter the dissemination of misinformation.
It is to note that the COVID-19 pandemic accelerated the development and implementation of mHealth solutions in the field of rehabilitation. While concrete evidence regarding the management of (long)-COVID patients remains limited, numerous individual studies and review are now highlighting the added values of mHealth in addressing various pathologies or conditions. This includes but is not limited to stroke, patients undergoing chemotherapy [47], patients with fibromyalgia [48], after bariatric surgery [49], hip and knee osteoarthritis [50], and urinary incontinence [51]. A consistent positive aspect found in the studies evaluating mHealth is that these interventions are well-received by patients, leading to greater adherence [52,53] and patient satisfaction [54,55].
4.4. Implications for the Rehabilitation
The transformative impact of the COVID-19 pandemic on societal dynamics is evident. Notably, the evolving peaks of the crisis have disrupted the assured continuity of care [56]. In response, rehabilitation services have undergone essential modifications and adaptations in their modalities of service provision and delivery to meet the exigencies imposed by the pandemic [57]. As healthcare professionals, incorporating these strategies into post-COVID-19 treatment programs could be crucial in enhancing recovery progress and reducing long-term physical impairments.
Nevertheless, several challenges still slowdown the integration of mHealth applications into clinical rehabilitation practices [58], necessitating comprehensive resolution before widespread implementation. Foremost among these challenges is the imperative need for the acknowledgment and acceptance of mHealth applications as integral components of rehabilitation interventions. The COVID-19 pandemic, while disruptive to healthcare systems, has concurrently catalyzed the development, implementation, and recognition of mHealth within clinical contexts [59]. However, it is crucial to recognize that many of the measures implemented during the crisis may be transient, and sustained efforts toward mHealth integration are contingent upon post-crisis commitment.
A pivotal obstacle lies in the current categorization of mobile solutions, which are presently subsumed under the same classifications as pharmaceuticals. This categorization not only introduces validation challenges but also poses obstacles to reimbursement processes [60]. Consequently, a paradigm shift in intervention nomenclature is imperative. Additionally, a prevalent limitation stems from the predominant development of mHealth solutions within research projects, rendering them largely inaccessible to the general patient population. This discrepancy underscores the second major impediment — the absence of social security reimbursement.
While the intricacies of healthcare system organization and participation in revalidation processes vary across countries, it is noteworthy that financial considerations and a deficiency in knowledge and experience with new technologies are universal barriers to the widespread adoption of telemedicine and telehealth. Notably, patients, irrespective of their specific pathologies or medical disciplines, consistently cite financial concerns and a lack of familiarity with technology as primary impediments [58,61]. While many patients exhibit familiarity with smartphones, apps, and mobile technology, thus mitigating concerns for a majority, this may not hold true for certain demographics, such as older adults with dementia, who may encounter substantial barriers [62,63].
In overcoming these barriers, it is imperative to not only address patient education but also focus efforts on healthcare professionals. The latter must undergo comprehensive training in the nuances of mHealth technology, including its limitations, to effectively endorse and encourage patient utilization. A valuable framework that can provide guidance in this educational endeavor is the NASSS (Non-adoption, Abandonment, challenges to scale-up, spread and sustainability) framework [64]. This model examines implementation of technology across seven domains, ranging from characteristics of the disease and patient population to funding and legislation). As the trajectory toward mHealth integration unfolds, a strategic emphasis on educational initiatives, guided by the insights provided by the NASSS framework, becomes pivotal for both patients and healthcare professionals alike.
5. Conclusions
The evaluated research and interventions highlight the capacity of telehealth and digital apps to have a positive influence on a range of health outcomes. Telerehabilitation therapies have shown positive trends in increasing functional performance, lowering symptom load, and promoting overall well-being in persons with chronic respiratory diseases. Significantly, the implementation of breathing exercises via telehealth resulted in notable enhancements in various clinical aspects.
Furthermore, when considering mental health and concerns connected to COVID-19, the incorporation of mobile phone applications, informational sessions, and relaxation exercises shown significant enhancements in fear of COVID-19, levels of anxiety, and quality of sleep. The utilization of digital therapeutics shown a level of efficacy that is comparable to conventional therapy, eliciting a pronounced inclination from users towards its distinctive attributes and gamification components.
Although these findings show promise, it is crucial to recognize the necessity for additional research to enhance the evidence and address limits in study designs and uncertainties. With the ongoing advancement of technology, adopting telehealth solutions can provide significant opportunity to improve the accessibility of healthcare, engage patients more effectively, and ultimately boost overall health outcomes. In conclusion, the data that has been examined supports the further investigation and adoption of digital interventions in healthcare to enhance patient outcomes and provide comprehensive, patient-centered care.
Author Contributions
Conceptualization, K.D. and B.B.; methodology, K.D., J.M. and B.B.; formal analysis, K.D. and B.B.; data curation, K.D. and J.M.; writing—original draft preparation, B.B.; writing—review and editing, K.D., J.M. and B.B.; visualization, K.D. and B.B.; supervision, B.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed 2020, 91, 157–160. [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [CrossRef]
- Burn, E.; Tebé, C.; Fernandez-Bertolin, S.; Aragon, M.; Recalde, M.; Roel, E.; Prats-Uribe, A.; Prieto-Alhambra, D.; Duarte-Salles, T. The Natural History of Symptomatic COVID-19 during the First Wave in Catalonia. Nat Commun 2021, 12, 777. [CrossRef]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an Acute to Chronic Disease? Potential Long-Term Health Consequences. Critical Reviews in Clinical Laboratory Sciences 2021, 58, 297–310. [CrossRef]
- Alwan, N.A. Surveillance Is Underestimating the Burden of the COVID-19 Pandemic. The Lancet 2020, 0. [CrossRef]
- Luo, Y.; Li, Q.; Jeong, H.; Cheatham, L. The Association between Social Determinants of Health and Psychological Distress during the COVID-19 Pandemic: A Secondary Analysis among Four Racial/Ethnic Groups. BMC Public Health 2022, 22, 2193. [CrossRef]
- Eadie, T.L. The ICF: A Proposed Framework for Comprehensive Rehabilitation of Individuals Who Use Alaryngeal Speech. Am J Speech Lang Pathol 2003, 12, 189–197. [CrossRef]
- Angeli, J.M.; Schwab, S.M.; Huijs, L.; Sheehan, A.; Harpster, K. ICF-Inspired Goal-Setting in Developmental Rehabilitation: An Innovative Framework for Pediatric Therapists. Physiother Theory Pract 2019, 1–10. [CrossRef]
- Hartasanchez, S.A.; Heen, A.F.; Kunneman, M.; García-Bautista, A.; Hargraves, I.G.; Prokop, L.J.; May, C.R.; Montori, V.M. Remote Shared Decision Making through Telemedicine: A Systematic Review of the Literature. Patient Educ Couns 2022, 105, 356–365. [CrossRef]
- Ward, K.; Vagholkar, S.; Sakur, F.; Khatri, N.N.; Lau, A.Y.S. Visit Types in Primary Care With Telehealth Use During the COVID-19 Pandemic: Systematic Review. JMIR Med Inform 2022, 10, e40469. [CrossRef]
- Nanda, M.; Sharma, R. A Review of Patient Satisfaction and Experience with Telemedicine: A Virtual Solution During and Beyond COVID-19 Pandemic. Telemed J E Health 2021, 27, 1325–1331. [CrossRef]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil Assist Technol 2017, 4, e7. [CrossRef]
- Rahmati, M.; Udeh, R.; Yon, D.K.; Lee, S.W.; Dolja-Gore, X.; McEVoy, M.; Kenna, T.; Jacob, L.; López Sánchez, G.F.; Koyanagi, A.; et al. A Systematic Review and Meta-Analysis of Long-Term Sequelae of COVID-19 2-Year after SARS-CoV-2 Infection: A Call to Action for Neurological, Physical, and Psychological Sciences. J Med Virol 2023, 95, e28852. [CrossRef]
- Brigo, E.; Rintala, A.; Kossi, O.; Verwaest, F.; Vanhoof, O.; Feys, P.; Bonnechère, B. Using Telehealth to Guarantee the Continuity of Rehabilitation during the COVID-19 Pandemic: A Systematic Review. Int J Environ Res Public Health 2022, 19, 10325. [CrossRef]
- Huang, J.; Fan, Y.; Zhao, K.; Yang, C.; Zhao, Z.; Chen, Y.; Yang, J.; Wang, T.; Qu, Y. Do Patients with and Survivors of COVID-19 Benefit from Telerehabilitation? A Meta-Analysis of Randomized Controlled Trials. Front Public Health 2022, 10, 954754. [CrossRef]
- Vieira, A.G. da S.; Pinto, A.C.P.N.; Garcia, B.M.S.P.; Eid, R.A.C.; Mól, C.G.; Nawa, R.K. Telerehabilitation Improves Physical Function and Reduces Dyspnoea in People with COVID-19 and Post-COVID-19 Conditions: A Systematic Review. J Physiother 2022, 68, 90–98. [CrossRef]
- Seid, A.A.; Aychiluhm, S.B.; Mohammed, A.A. Effectiveness and Feasibility of Telerehabilitation in Patients with COVID-19: A Systematic Review and Meta-Analysis. BMJ Open 2022, 12, e063961. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int J Surg 2021, 88, 105906. [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv Res 2014, 14. [CrossRef]
- de Morton, N.A. The PEDro Scale Is a Valid Measure of the Methodological Quality of Clinical Trials: A Demographic Study. Aust J Physiother 2009, 55, 129–133. [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys Ther 2003, 83, 713–721. [CrossRef]
- Moseley, A.M.; Rahman, P.; Wells, G.A.; Zadro, J.R.; Sherrington, C.; Toupin-April, K.; Brosseau, L. Agreement between the Cochrane Risk of Bias Tool and Physiotherapy Evidence Database (PEDro) Scale: A Meta-Epidemiological Study of Randomized Controlled Trials of Physical Therapy Interventions. PLoS One 2019, 14, e0222770. [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLOS Medicine 2009, 6, e1000100. [CrossRef]
- Churchill, L.; Morrow, M.; Capin, J.J.; Jolley, S.E.; Hare, K.; MaWhinney, S.; Stevens-Lapsley, J.E.; Erlandson, K.M. Using Wearable Technology to Quantify Physical Activity Recovery: Secondary Report From the AFTER (App-Facilitated Tele-Rehabilitation) Program for COVID-19 Survivors Randomized Study. JMIR Rehabil Assist Technol 2023, 10, e43436. [CrossRef]
- Rodriguez-Blanco, C.; Gonzalez-Gerez, J.J.; Bernal-Utrera, C.; Anarte-Lazo, E.; Perez-Ale, M.; Saavedra-Hernandez, M. Short-Term Effects of a Conditioning Telerehabilitation Program in Confined Patients Affected by COVID-19 in the Acute Phase. A Pilot Randomized Controlled Trial. Medicina 2021, 57, 684. [CrossRef]
- Capin, J.J.; Jolley, S.E.; Morrow, M.; Connors, M.; Hare, K.; MaWhinney, S.; Nordon-Craft, A.; Rauzi, M.; Flynn, S.; Stevens-Lapsley, J.E.; et al. Safety, Feasibility and Initial Efficacy of an App-Facilitated Telerehabilitation (AFTER) Programme for COVID-19 Survivors: A Pilot Randomised Study. BMJ Open 2022, 12, e061285. [CrossRef]
- Wei, N.; Huang, B.; Lu, S.; Hu, J.; Zhou, X.; Hu, C.; Chen, J.; Huang, J.; Li, S.; Wang, Z.; et al. Efficacy of Internet-Based Integrated Intervention on Depression and Anxiety Symptoms in Patients with COVID-19. J Zhejiang Univ Sci B 2020, 21, 400–404. [CrossRef]
- Liu, Z.; Qiao, D.; Xu, Y.; Zhao, W.; Yang, Y.; Wen, D.; Li, X.; Nie, X.; Dong, Y.; Tang, S.; et al. The Efficacy of Computerized Cognitive Behavioral Therapy for Depressive and Anxiety Symptoms in Patients With COVID-19: Randomized Controlled Trial. Journal of Medical Internet Research 2021, 23, e26883. [CrossRef]
- Hajibashi, A.; Sarrafzadeh, J.; Amiri, A.; Salehi, R.; Vasaghi-Gharamaleki, B. Effect of Progressive Muscle Relaxation as an Add-on to Pulmonary Telerehabilitation in Discharged Patients with COVID-19: A Randomised Controlled Trial. Complement Ther Clin Pract 2023, 51, 101730. [CrossRef]
- Samper-Pardo, M.; León-Herrera, S.; Oliván-Blázquez, B.; Méndez-López, F.; Domínguez-García, M.; Sánchez-Recio, R. Effectiveness of a Telerehabilitation Intervention Using ReCOVery APP of Long COVID Patients: A Randomized, 3-Month Follow-up Clinical Trial. Sci Rep 2023, 13, 7943. [CrossRef]
- Campos, M.C.; Nery, T.; Speck, A.E.; Arpini, M.; Antunes, M.M.; De Bem Alves, A.C.; De Souza Santos, N.; Matos, M.P.P.; Schmidt, N.; Bicca, L.R.; et al. Rehabilitation Improves Persistent Symptoms of COVID-19: A Non-Randomized, Controlled, Open Study in Brazil. Am J Phys Med Rehabil 2023. [CrossRef]
- Li, J.; Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Zheng, C.; Fang, X.; Cheng, W.; et al. A Telerehabilitation Programme in Post-Discharge COVID-19 Patients (TERECO): A Randomised Controlled Trial. Thorax 2022, 77, 697–706. [CrossRef]
- Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; Anarte-Lazo, E.; Bernal-Utrera, C.; Perez-Ale, M.; Rodriguez-Blanco, C. Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study. IJERPH 2021, 18, 7511. [CrossRef]
- Bonnechère, B.; Timmermans, A.; Michiels, S. Current Technology Developments Can Improve the Quality of Research and Level of Evidence for Rehabilitation Interventions: A Narrative Review. Sensors (Basel) 2023, 23, 875. [CrossRef]
- Hartman, M.; Mináriková, J.; Batalik, L.; Pepera, G.; Su, J.J.; Formiga, M.F.; Cahalin, L.; Dosbaba, F. Effects of Home-Based Training with Internet Telehealth Guidance in COPD Patients Entering Pulmonary Rehabilitation: A Systematic Review. Int J Chron Obstruct Pulmon Dis 2023, 18, 2305–2319. [CrossRef]
- Sapouna, V.; Kitixis, P.; Petrou, E.; Michailidou, T.; Dalamarinis, P.; Kortianou, E. Mobile Health Applications Designed for Self-Management of Chronic Pulmonary Diseases in Children and Adolescents: A Systematic Mapping Review. J Bras Pneumol 2023, 49, e20230201. [CrossRef]
- Garavand, A.; Khodaveisi, T.; Aslani, N.; Hosseiniravandi, M.; Shams, R.; Behmanesh, A. Telemedicine in Cancer Care during COVID-19 Pandemic: A Systematic Mapping Study. Health Technol (Berl) 2023, 1–14. [CrossRef]
- Fainardi, V.; Capoferri, G.; Tornesello, M.; Pisi, G.; Esposito, S. Telemedicine and Its Application in Cystic Fibrosis. J Pers Med 2023, 13, 1041. [CrossRef]
- Kepenek-Varol, B.; Zeren, M.; Dinçer, R.; Erkaya, S. Breathing and Relaxation Exercises Help Improving Fear of COVID-19, Anxiety, and Sleep Quality: A Randomized Controlled Trial. J Integr Complement Med 2022, 28, 579–586. [CrossRef]
- Baxter, C.A.; Carroll, J.-A.; Keogh, B.; Vandelanotte, C. Virtual Respiratory Therapy Delivered through a Smartphone App: A Mixed-Methods Randomised Usability Study. BMJ Open Respir Res 2022, 9, e001221. [CrossRef]
- Kohlbrenner, D.; Kuhn, M.; Stüssi-Helbling, M.; Nordmann, Y.; Spielmanns, M.; Clarenbach, C.F. Longitudinal Smartphone-Based Post-Hospitalisation Symptom Monitoring in SARS-CoV-2 Associated Respiratory Failure: A Multi-Centre Observational Study. Frontiers in Rehabilitation Sciences 2021, 2. [CrossRef]
- Del Corral, T.; Fabero-Garrido, R.; Plaza-Manzano, G.; Fernández-de-Las-Peñas, C.; Navarro-Santana, M.; López-de-Uralde-Villanueva, I. Home-Based Respiratory Muscle Training on Quality of Life and Exercise Tolerance in Long-Term Post-COVID-19: Randomized Controlled Trial. Ann Phys Rehabil Med 2023, 66, 101709. [CrossRef]
- Ahmadi Marzaleh, M.; Peyravi, M.; Azhdari, N.; Bahaadinbeigy, K.; Sharifian, R.; Samad-Soltani, T.; Sarpourian, F. Virtual Reality Applications for Rehabilitation of COVID-19 Patients: A Systematic Review. Health Sci Rep 2022, 5, e853. [CrossRef]
- Kirykowicz, K.; Jaworski, B.; Owen, J.; Kirschbaum, C.; Seedat, S.; van den Heuvel, L.L. Feasibility, Acceptability and Preliminary Efficacy of a Mental Health Self-Management App in Clinicians Working during the COVID-19 Pandemic: A Pilot Randomised Controlled Trial. Psychiatry Res 2023, 329, 115493. [CrossRef]
- Monteleone, G.; Terzulli, G.; Cefaloni, F.; Bonini, M.; Richeldi, L. The Impact of Telemedicine during Severe Acute Respiratory Syndrome Coronavirus 2 Pandemic and Future Perspectives: A Systematic Review. Respiration 2023, 102, 879–890. [CrossRef]
- Dixit, S.; Nandakumar, G. Promoting Healthy Lifestyles Using Information Technology during the COVID-19 Pandemic. Rev Cardiovasc Med 2021, 22, 115–125. [CrossRef]
- Shi, N.; Wong, A.K.C.; Wong, F.K.Y.; Sha, L. Mobile Health Application-Based Interventions to Improve Self-Management of Chemotherapy-Related Symptoms Among People with Breast Cancer Who Are Undergoing Chemotherapy: A Systematic Review. Oncologist 2023, 28, e175–e182. [CrossRef]
- Kashikar-Zuck, S.; Barnett, K.A.; Williams, S.E.; Pfeiffer, M.; Thomas, S.; Beasley, K.; Chamberlin, L.A.; Mundo, K.; Ittenbach, R.F.; Peugh, J.; et al. FIT Teens RCT for Juvenile Fibromyalgia: Protocol Adaptations in Response to the COVID 19 Pandemic. Contemp Clin Trials Commun 2022, 30, 101039. [CrossRef]
- Ali, O.I.; Abdelraouf, O.R.; El-Gendy, A.M.; Abdelgalil, A.A.; Abdelaal, A.K.; Dahlawi, H.A.; Selim, A.O. Efficacy of Telehealth Core Exercises during COVID-19 after Bariatric Surgery: A Randomized Controlled Trial. Eur J Phys Rehabil Med 2022, 58, 845–852. [CrossRef]
- Yang, Y.; Li, S.; Cai, Y.; Zhang, Q.; Ge, P.; Shang, S.; Han, H. Effectiveness of Telehealth-Based Exercise Interventions on Pain, Physical Function and Quality of Life in Patients with Knee Osteoarthritis: A Meta-Analysis. J Clin Nurs 2023, 32, 2505–2520. [CrossRef]
- Santiago, M.; Cardoso-Teixeira, P.; Pereira, S.; Firmino-Machado, J.; Moreira, S. A Hybrid-Telerehabilitation Versus a Conventional Program for Urinary Incontinence: A Randomized Trial during COVID-19 Pandemic. Int Urogynecol J 2023, 34, 717–727. [CrossRef]
- Bennell, K.L.; Marshall, C.J.; Dobson, F.; Kasza, J.; Lonsdale, C.; Hinman, R.S. Does a Web-Based Exercise Programming System Improve Home Exercise Adherence for People With Musculoskeletal Conditions?: A Randomized Controlled Trial. Am J Phys Med Rehabil 2019, 98, 850–858. [CrossRef]
- Lambert, T.E.; Harvey, L.A.; Avdalis, C.; Chen, L.W.; Jeyalingam, S.; Pratt, C.A.; Tatum, H.J.; Bowden, J.L.; Lucas, B.R. An App with Remote Support Achieves Better Adherence to Home Exercise Programs than Paper Handouts in People with Musculoskeletal Conditions: A Randomised Trial. J Physiother 2017, 63, 161–167. [CrossRef]
- Lawford, B.J.; Delany, C.; Bennell, K.L.; Hinman, R.S. “I Was Really Sceptical...But It Worked Really Well”: A Qualitative Study of Patient Perceptions of Telephone-Delivered Exercise Therapy by Physiotherapists for People with Knee Osteoarthritis. Osteoarthritis Cartilage 2018, 26, 741–750. [CrossRef]
- Moffet, H.; Tousignant, M.; Nadeau, S.; Mérette, C.; Boissy, P.; Corriveau, H.; Marquis, F.; Cabana, F.; Belzile, É.L.; Ranger, P.; et al. Patient Satisfaction with In-Home Telerehabilitation After Total Knee Arthroplasty: Results from a Randomized Controlled Trial. Telemed J E Health 2017, 23, 80–87. [CrossRef]
- Wahezi, S.E.; Kohan, L.R.; Spektor, B.; Brancolini, S.; Emerick, T.; Fronterhouse, J.M.; Luedi, M.M.; Colon, M.A.; Kitei, P.M.; Anitescu, M.; et al. Telemedicine and Current Clinical Practice Trends in the COVID-19 Pandemic. Best Pract Res Clin Anaesthesiol 2021, 35, 307–319. [CrossRef]
- Van Hove, O.; Gillet, A.; Tack, J.; Reychler, G.; Guatteri, M.; Ballarin, A.; Thomas, J.; Espinoza, R.; Bonnier, F.; Norrenberg, M.; et al. Development of a Medium Care Unit Using an Inexperienced Respiratory Staff: Lessons Learned during the COVID-19 Pandemic. IJERPH 2022, 19, 7349. [CrossRef]
- Scott Kruse, C.; Karem, P.; Shifflett, K.; Vegi, L.; Ravi, K.; Brooks, M. Evaluating Barriers to Adopting Telemedicine Worldwide: A Systematic Review. J Telemed Telecare 2018, 24, 4–12. [CrossRef]
- Marra, C.; Gordon, W.J.; Stern, A.D. Use of Connected Digital Products in Clinical Research Following the COVID-19 Pandemic: A Comprehensive Analysis of Clinical Trials. BMJ Open 2021, 11, e047341. [CrossRef]
- Carl, J.R.; Jones, D.J.; Lindhiem, O.J.; Doss, B.D.; Weingardt, K.R.; Timmons, A.C.; Comer, J.S. Regulating Digital Therapeutics for Mental Health: Opportunities, Challenges, and the Essential Role of Psychologists. Br J Clin Psychol 2021. [CrossRef]
- Rangachari, P.; Mushiana, S.S.; Herbert, K. A Narrative Review of Factors Historically Influencing Telehealth Use across Six Medical Specialties in the United States. Int J Environ Res Public Health 2021, 18, 4995. [CrossRef]
- Almathami, H.K.Y.; Win, K.T.; Vlahu-Gjorgievska, E. Barriers and Facilitators That Influence Telemedicine-Based, Real-Time, Online Consultation at Patients’ Homes: Systematic Literature Review. J Med Internet Res 2020, 22, e16407. [CrossRef]
- Engelsma, T.; Jaspers, M.W.M.; Peute, L.W. Considerate mHealth Design for Older Adults with Alzheimer’s Disease and Related Dementias (ADRD): A Scoping Review on Usability Barriers and Design Suggestions. Int J Med Inform 2021, 152, 104494. [CrossRef]
- James, H.M.; Papoutsi, C.; Wherton, J.; Greenhalgh, T.; Shaw, S.E. Spread, Scale-up, and Sustainability of Video Consulting in Health Care: Systematic Review and Synthesis Guided by the NASSS Framework. J Med Internet Res 2021, 23, e23775. [CrossRef]
Figure 1.
ICF model for COVID-19 repercussion and sequelae.
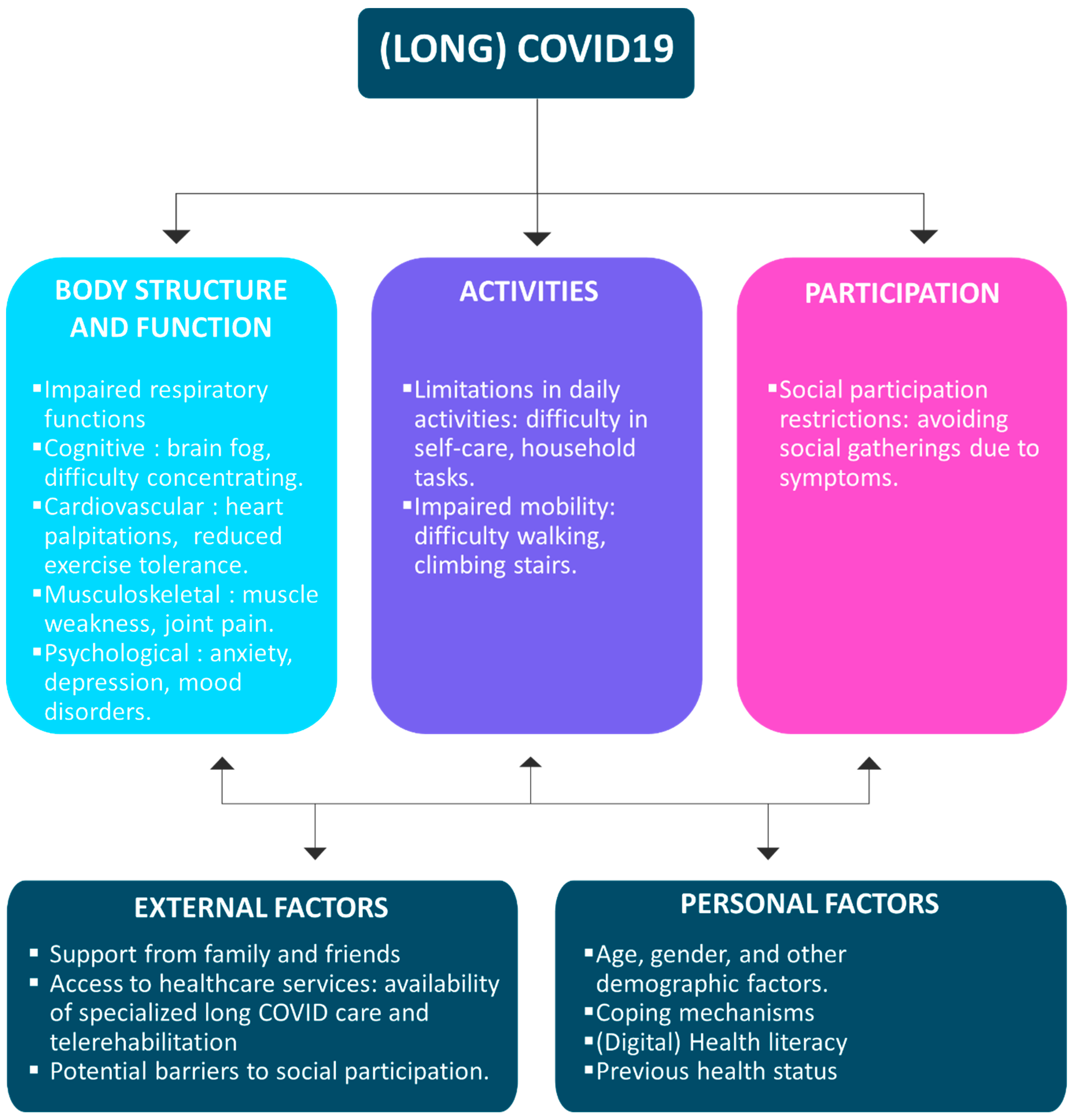
Figure 2.
Definitions and organizations of eHealth, telehealth and mHealth services.
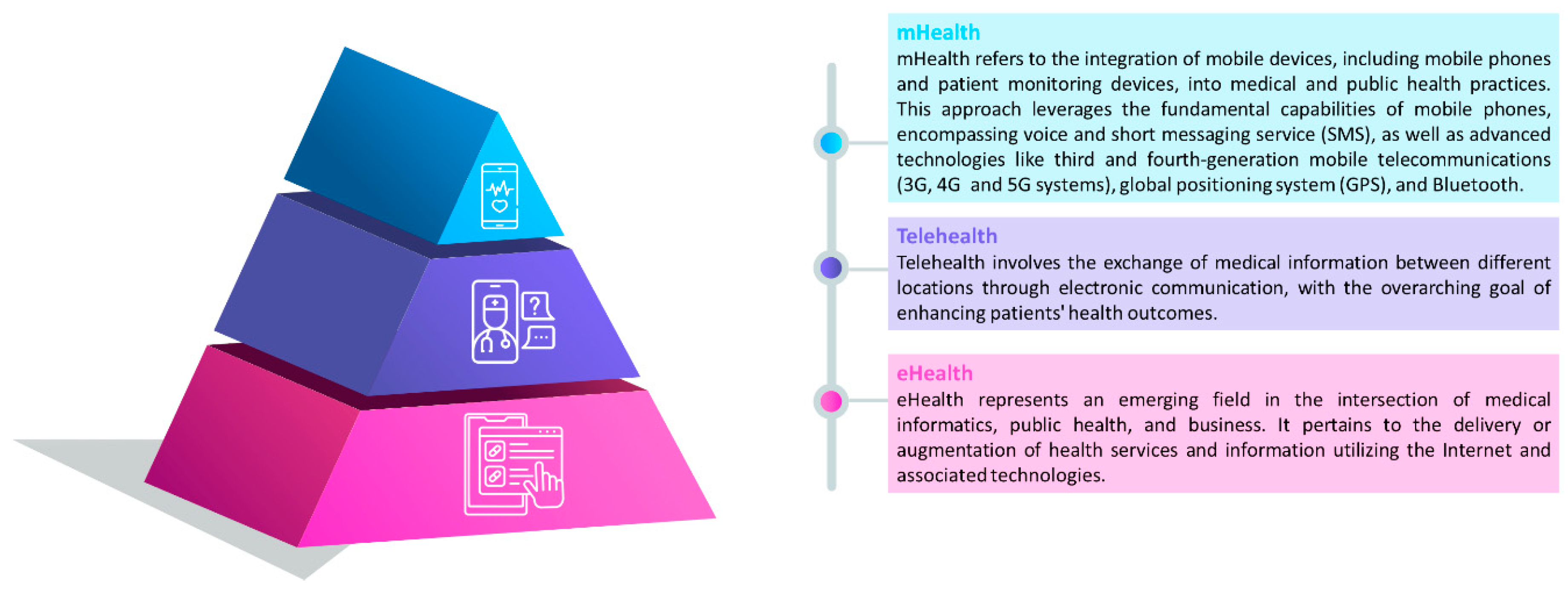
Figure 3.
Flow chart of study selection.
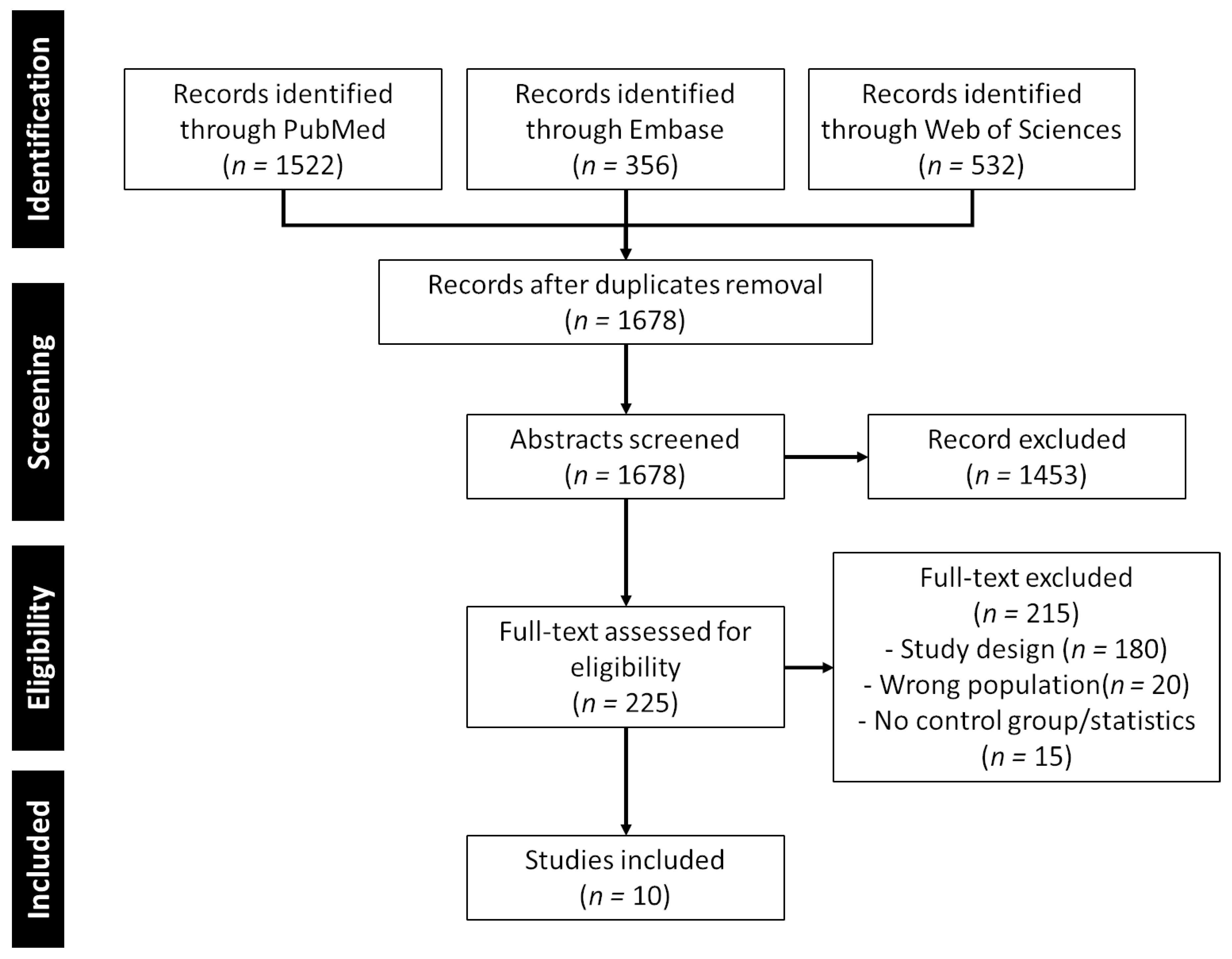
Figure 4.
Quality of the study, author’s judgement broken down for each item of the PEDro scale across all included studies.
Figure 4.
Quality of the study, author’s judgement broken down for each item of the PEDro scale across all included studies.
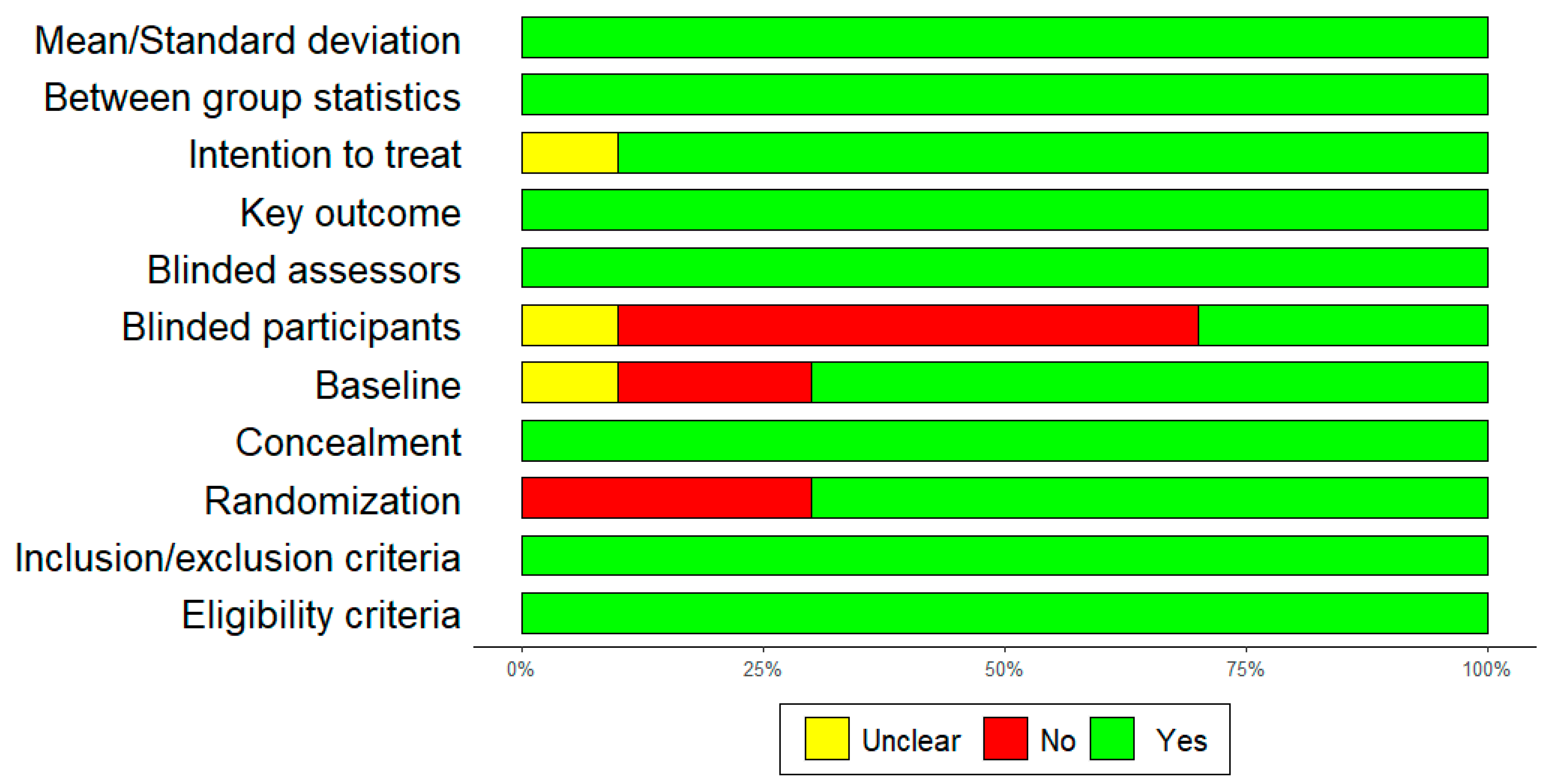
Figure 5.
Main outcomes of the included studies according to the ICF framework.

Table 1.
PICOs’ strategy.
| Population | Patients with confirmed COVID-19. |
| Intervention | Patient education (information about COVID-19, causes, risk factors, healthy diet, treatment modalities and exercises), or physical exercises or activities (strengthening exercises, gait training, cycling, walking, gardening, etc.) through mHealth. |
| Comparison | Any other intervention (i.e., physical exercises or activities, patient education without mHealth) or no intervention |
| Outcome | Any type of outcome measure related to the International Classification of Functioning, Disability and Health (ICF) [8] |
| Study Design | Randomized Controlled studies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



