
Submitted:
10 January 2024
Posted:
11 January 2024
You are already at the latest version
Abstract
Background and objectives: Musculoskeletal (MSK) pain significantly impacts physical activity and quality of life in the elderly, potentially influencing mortality. This study explored the relationship between MSK pain, physical activity, muscle mass, and mortality among older adults.
Material and Methods: We studied 1000 participants of the Korean Longitudinal Study on Health and Aging (KLoSHA), a prospective, population-based cohort study of people aged 65 years or older. Survival status was tracked over a 5-year period. Correlations between Low back pain (LBP), knee pain, regular exercise, appendicular skeletal muscle mass (ASM), and other variables were analyzed. Logistic regression analyzes were used to identify independent risk factors for mortality.
Results: Of the total participants, 829 (82.9%) survived after a 5-year period. Survivors tended to be younger, had a higher BMI, and were more active in regular exercise. In contrast, non-survivors exhibited a higher prevalence of both LBP and knee pain, along with increased instances of multiple MSK pain. Lower ASM correlated moderately with LBP and knee pain, whereas higher ASM was associated with regular exercise Lower ASM was moderately associated with LBP and knee pain, while higher ASM correlated with engagement in regular exercise. There was a moderate correlation between LBP and knee pain, both of which were associated with a lack of regular exercise. Age, sex, ASM, and regular exercise were significant predictors, even though MSK pain itself did not directly predict all-cause mortality.
Conclusions: This study demonstrated the independent association between ASM, regular exercise, and mortality. Although MSK pain did not directly correlate with all-cause mortality, the non-survivor group had higher levels of both single and multiple MSK pain. Recognizing the interplay of MSK pain, physical activity, and muscle mass for older adults, the research underscores the need for holistic strategies to enhance health outcomes in older individuals with MSK pain.
Keywords:
Low Back Pain
; Musculoskeletal pain
; Exercise
; Muscle
; Skeletal
; Mortality
1. Introduction
Musculoskeletal (MSK) pain exacts a considerable toll on individuals' physical activity levels and overall quality of life [1] With a global prevalence of around 30% [2], MSK pain is not only prevalent but also escalates significantly with advancing age [3]. The burden of MSK pain is poised to expand substantially in tandem with increasing global life expectancy [4]. Among these conditions, low back pain (LBP) and knee pains emerge as prominent afflictions, particularly affecting the elderly with more than 20% of this population worldwide suffering with LBP [5]. In the United States, 18.1% of older men and 23.5% of older women report knee pain [6].
In the context of MSK pain and mortality, the association between rheumatoid arthritis and increased mortality risk is well-established [7]. However, the prevalence of this condition is only about 2% [8] and the relationship might differ when examining the broader spectrum of MSK pain. Recent meta-analyses examining back pain and knee pain have shown that adults with knee pain exhibited a notable 35-37% increased risk of reduced time-to-mortality [9]. In the context of back pain, a sex-specific pattern emerged, with an association between back pain and mortality observed in women and among men experiencing severe back pain. Conversely, no such correlation was found in men or those with non-severe back pain, though the meta-analysis underscored significant heterogeneity among the included studies [10].
The connection between MSK pain and mortality may not be immediately apparent, as it doesn't directly impact vital organs or internal health. However, pain often leads to reduced physical activity [11], subsequently resulting in decreased muscle mass [12], the body’s largest endocrine organ, which is related to mortality [13]. Conversely, muscle affect pain perception [14] and also, physical activity can influence pain perception [15] through various factors such as mood. This interplay underscores the multidimensional relationship between MSK pain, physical activity, muscle mass, and their collective impact on mortality.
This study aimed to investigate the relationship between MSK pain, physical activity, muscle mass, and mortality among community-dwelling elderly Koreans aged over 65 years. The findings provide insights into the intricate interplay of these factors, offering implications for clinical practice and strategies for managing the aging population.
1. Materials and Methods
1.1. Study Subjects
This study leveraged data from KLoSHA, a population-based prospective cohort in Seongnam, South Korea, targeting community-dwelling individuals aged 65 or older, selected via multistage, stratified probability sampling [16]. The baseline assessment was conducted from September 2005 to September 2006, followed by a second wave five years later at Seoul National University Bundang Hospital (SNUBH). The baseline cohort comprised 1,000 participants, including 441 men and 559 women. This study was approved by the Institutional Review Boards of SNUBH (B-0508/023-003) and written informed consent was obtained from all participants.
1.1. Demographics and Anthropometric Measures
Demographic characteristics were collected through medical history assessments and questionnaires administered by nurses certified in epidemiological studies and geriatric patient assessment. Weight and height were measured following the anthropometric standardization reference manual [17] recorded in centimeters and kilograms and rounded to the nearest 0.1 unit. Body mass index (BMI) was calculated by dividing the total body weight (kg) by the height squared (m2). Waist circumference was measured horizontally at the narrowest part between the lowest rib and iliac crest. Appendicular skeletal muscle mass (ASM) was evaluated using a tetrapolar multi-frequency bioelectrical impedance analysis (Inbody 3; Biospace, Seoul, Korea), following a standardized procedure as previously reported [18]. This method has been validated against other body composition assessment techniques, including dual-energy X-ray absorptiometry, underwater weighing, and magnetic resonance imaging [19]. Metabolic syndrome was defined as the concurrent presence of at least three out of the following five criteria [20]: 1) waist circumference equal to or exceeding 90 cm in men or 85 cm in women [21], 2) triglyceride levels measuring 150 mg/dL or higher, 3) high-density lipoprotein cholesterol falling below 40 mg/dL in men or 50 mg/dL in women, 4) blood pressure equal to or greater than 130/85 mmHg, or the use of antihypertensive medication, and 5) fasting plasma glucose at or above 100 mg/dL, or the use of pharmaceutical treatment for diabetes mellitus. We ascertained the mortality status of participants (survivor or non-survivor) when inviting them for the second-wave evaluation of the cohort study.
1.1. Knee Pain, Low Back Pain, and Regular Exercise
The questionnaire used in this study included the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for the knee [22], the Oswestry Low Back Pain Disability Questionnaire (ODQ) [23], and the International Physical Activity Questionnaire [24]. In our study, participants were classified as experiencing knee pain if their responses on the WOMAC questionnaire showed a score of 3 or higher on a 5-point Likert scale, specifically for knee pain at rest or during walking. Likewise, participants who scored 3 or higher for pain intensity or back pain during walking on the 6-point Likert scale within the ODQ were coded as having LBP. Finally, regular exercisers were defined as individuals engaging in moderate or vigorous intensity physical activities for 30 minutes or more, on at least three occasions per week.
1.1. Statistical Analyses
Baseline characteristics were presented as mean ± standard deviation for continuous variables and as number of subjects (percentage) for categorical variables. Differences between the survivor and non-survivor groups were evaluated using independent t-tests for normally distributed continuous data and chi-squared tests for categorical data. The relationships among pain, regular exercise, and other variables were assessed using Cramer’s V or Phi correlation coefficients for nominal data, with significance determined by the chi-square test. Correlations were also examined individual pain types or the number of pain occurrences, regular exercise, and mortality. Simple logistic regression analyses were performed to identify potential predictors of death during the follow-up period. Variables with a p-value < 0.2 were subsequently included in multiple logistic regression models, employing a backward stepwise method to determine predictors of non-survival during the follow-up. All statistical analyses were conducted using IBM SPSS software (ver. 26.0; IBM Corp., Armonk, NY, USA). P-values < 0.05 were considered to indicate statistical significance.
1. Results
Of the 1,000 elderly individuals included in this study, 829 subjects (82.9%) survived after a 5-year follow-up. The mean age differed significantly between the survivor and non-survivor groups, being 74.8 ± 8.1 and 83.7 ± 7.8 years, respectively (p < 0.001). The survivor group exhibited a higher BMI (p < 0.001). Additionally, the prevalence of LBP (p < 0.001) and knee pain (p = 0.016) was greater among non-survivors, while the proportion of regular exercisers was higher among survivors (p < 0.001). Factors such as sex, metabolic syndrome presence, alcohol consumption, and smoking did not differ significantly between the groups (Table 1).
The correlation between pain, regular exercise, and other variables was nearly significant, excluding BMI. Age exhibited a moderate association with LBP. Females showed moderate associations with LBP, knee pain, and regular exercise. Low ASM correlated moderately with LBP and knee pain, whereas high ASM correlated with regular exercise. LBP and knee pain had a moderate association with each other and with a lack of regular exercise (Table 2). The non-survivor group showed significantly higher rates of MSK pain and multiple MSK pain. (Figure 1). Although correlations between pain occurrence and mortality were significant, the association was weak. (Table 2).
Univariate analysis indicated a significant association between age, BMI, LBP, knee pain, the presence of MSK pain, regular exercise, and non-survivor status. Multiple logistic regression analyses were conducted using individual pain types or the number of pain occurrences as variables. Both regression models yielded consistent results: age (OR = 1.095, 95% confidence interval [CI] 1.062-1.126, p < 0.001) was associated with increased mortality risk, while female sex (OR = 0.138, 95% CI 0.063-0.302, p < 0.001), ASM (OR = 0.822, 95% CI 0.732-0.923, p = 0.001), and regular exercise (OR = 0.465, 95% CI 0.287-0.754, p < 0.002) were negatively associated with mortality. LBP, knee pain, and the number of MSK pain occurrences were not predictive of mortality in the multivariate models (Table 3).
1. Discussion
In this study, the non-survivor group exhibited higher rates of LBP and knee pain, whereas survivors were more often regular exercisers. Furthermore, the non-survivor group demonstrated increased levels of both individual and multiple MSK pain. Lower ASM correlated moderately with LBP and knee pain, whereas higher ASM was associated with regular exercise. LBP and knee pain were moderately correlated and associated with a lack of regular exercise. Age, sex, ASM, and regular exercise were significant predictors, even though MSK pain itself did not directly predict all-cause mortality over a period of up to 6 years.
The all-cause mortality rate in the KLoSHA cohort was 17.1%. Since we did not include variables such as comorbid conditions, the specific association between mortality and various factors remains uncertain. However, while MSK pain did not emerge as an independent predictor, aging seemed to exert a more significant influence on mortality outcomes, likely due to age-related comorbidities. Nevertheless, addressing MSK pain remains crucial given its elevated prevalence among older adults, ranging from 40% to 60% [25]. This type of pain poses significant challenges in managing the elderly, impacting health outcomes related to falls, frailty, depression, and both cognitive and physical functional decline [26]. Additionally, multisite MSK pain affects a significant portion, ranging from 25% to 43%, of community-dwelling adults aged 65 years and older [27,28], contributing to increased disability in this age group [29]. This multisite pain is also associated with a more sedentary level of physical activity [30]. In our study, a higher proportion of older adults who did not survive reported experiencing both MSK pain and multisite MSK pain (22.9% vs. 12.3%) compared to survivors, suggesting a potentially higher risk of adverse health outcomes for this group.
LBP and knee pain are prevalent forms of MSK pain among older adults. Previous reviews suggest that such MSK pain might elevate mortality risks in the elderly [9,10,31]. However, the potential pathways explaining this association remain unclear. Research based on large population cohort datasets revealed that the interference of MSK pain with daily activities, rather than just its presence or severity, significantly influences mortality rates [32]. A systematic review indicated that older adults with MSK pain tend to be less physically active compared to those without such pain [11]. Elevated concerns about pain and the risk of falling may lead these individuals to restrict activities that could exacerbate their pain or precipitate falls [33]. Additionally, MSK pain correlates directly with increased mobility limitations [34]. Patients with chronic LBP frequently exhibit limited physical performance, especially in joint movement and overall body mobility, often adopting positions that emphasize abdominal strength [35]. Furthermore, increased LBP severity corresponds with diminished lower-extremity muscle performance and slower gait speeds [36]. Knee pain has been shown to significantly decrease maximum gait speed [37] and notably compromises balance, thereby affecting levels of physical activity [38]. Ultimately, physical inactivity due to MSK pain could amplify the risk of chronic ailments and mortality [32,39].
Regular physical activity has been shown to offer significant health benefits. The 2018 Physical Activity Guidelines for Americans [40] recommend that adults should participate in at least 150 minutes of moderate-intensity aerobic activity or 75 minutes of vigorous-intensity aerobic activity each week, or a combination of both. Adults adhering to these guidelines showed greatly reduced risk of all cause and cause specific mortality [41]. In this study, engaging in moderate or vigorous-intensity physical activities for at least 30 minutes, on a minimum of three occasions per week, demonstrated a beneficial effect in reducing mortality rates, underscoring the importance of regular exercise.
In our study, ASM emerged as an independent predictor of mortality and was associated with MSK pain. Skeletal muscles play a pivotal role in facilitating a wide spectrum of movements, ranging from powerful to delicate actions, underscoring their significance for physical performance [42]. As individuals advance in age, the inevitability of skeletal muscle atrophy becomes more pronounced, largely attributed to declining levels of testosterone, insulin-like growth factor-1 (IGF-1), and growth hormone. Contributing factors such as physical inactivity and malnutrition further exacerbate this muscle mass decline [43,44,45]. A recent review indicates that muscle mass in individuals aged 75 years or older declines at a rate of 0.64–0.70% per year in women and 0.80–0.98% per year in men, which is greater compared to younger age groups [46]. This age-related decline in muscle mass compromises physical performance [47], elevates the risk of physical disability in later life [48] and increases the overall mortality risk [49]. Additionally, levels of inflammatory cytokines are elevated in the elderly compared to younger individuals [50]. These cytokines not only initiate but also sustain pathological pain by directly activating nociceptive sensory neurons [51], Furthermore, they may hinder the differentiation of satellite cells, resulting in a gradual and progressive decline in muscle mass and quality [42]. As a consequence, older adults with reduced skeletal muscle mass may be more vulnerable to MSK pain.
When MSK pain in older adults remains inadequately managed, they often limit physical activity to mitigate discomfort or further pain. This avoidance or inability to engage in physical activities due to pain can lead to weight gain and exacerbate chronic conditions, thereby heightening mortality risks. Moreover, reduced physical activity contributes to disuse atrophy of skeletal muscles. Consequently, decreased muscle mass diminishes physical performance, leading to increased inactivity and elevated vulnerability to pain. This interplay between MSK pain, physical activity, and muscle mass imposes significant health burdens on older adults. The relationships observed among pain, ASM, and regular exercise in this study underscores the importance of holistic treatment approaches for MSK pain. Prolonged rest strategies to manage pain should be avoided to avert muscle atrophy and declining physical activity. Along with pain management, patients should be encouraged to engage in exercises tailored to their MSK pain level. Neglecting to offer these recommendations would continue to exacerbate the negative mortality implications associated with pain. Furthermore, incorporating rehabilitative measures like exercise and nutritional support to enhance ASM could potentially reduce mortality rates.
Our study has several noteworthy limitations. To begin, the sample size was relatively small, potentially limiting our ability to identify additional significant predictors of mortality. Another crucial consideration pertains to a key variable, physical activity, which relied on self-reported data and could introduce bias. Additionally, we did not differentiate the severity of pain or exercise intensity, missing an opportunity to establish a compelling dose-response relationship. Furthermore, our analysis was restricted to baseline values, offering limited insights into changes over the study period that could clarify the causal sequence between variables and mortality. We also did not include depression as a variable, despite its potential relevance to pain, physical activity, and mortality. Lastly, our examination was confined to all-cause mortality, without categorizing specific causes of death.
1. Conclusions
This study highlighted the independent association between ASM, regular exercise, and mortality. While MSK pain alone did not directly correlate with all-cause mortality, the non-survivor group showed elevated levels of both singular and multiple MSK pain. Recognizing the intricate relationship among MSK pain, physical activity, and muscle mass and their significance for older adults, this research emphasizes the necessity of comprehensive strategies. Such strategies should prioritize effective pain management and concurrently aim to maintain or enhance muscle mass and physical activity levels, thereby improving health outcomes in older individuals with MSK pain.
Author Contributions
Conceptualization, Lim SK, Chun SW.; Methodology, Lim JY, Lim SK, Chun SW.; Formal Analysis, Chun SW, Hwang S; Project administration, Lim JY, Lim SK, Chun SW.; Visualization: Lim SK, Chun SW, Hwang S.; Writing – original draft, Hwang S.; Writing – review and editing, Chun SW, Lee CH, Lim SK, Oh MK, Jang YJ, Kim C, Kim KW, Jang HC.; All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the grant of the Korean Health Technology R&D Project, Ministry of Health, Welfare and Family Affairs, Republic of Korea (Grant No. A092077). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
This study was approved by the Institutional Review Boards of SNUBH (B-0508/023-003).
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
This work was supported by the Soonchunhyang University Research Fund.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003, 81(9), 646-56.
- Cimmino MA, Ferrone C, Cutolo M. Epidemiology of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2011, 25(2), 173-83. [CrossRef]
- Fejer R, Ruhe A. What is the prevalence of musculoskeletal problems in the elderly population in developed countries? A systematic critical literature review. Chiropr Man Therap. 2012, 20, 1-52. [CrossRef]
- Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain—Where to from here? Am J Public Health. 2019, 109(1), 35–40. [CrossRef] [PubMed]
- Briggs AM, Cross MJ, Hoy DG, Sànchez-Riera L, Blyth FM, Woolf AD, March L. Musculoskeletal health conditions represent a global threat to healthy aging: A report for the 2015 World Health Organization world report on ageing and health. Gerontologist. 2016, 56 (suppl_2), S243-S55. [CrossRef]
- Andersen RE, Crespo CJ, Ling SM, Bathon JM, Bartlett SJ. Prevalence of significant knee pain among older Americans: Results from the Third National Health and Nutrition Examination Survey. J Am Geriatr Soc. 1999, 47(12), 1435-8. [CrossRef]
- Sokka T, Abelson B, Pincus T. Mortality in rheumatoid arthritis: 2008 update. Clin Exp Rheumatol. 2008, 26 (5 Suppl 51), S35-61.
- Rasch EK, Hirsch R, Paulose-Ram R, Hochberg MC. Prevalence of rheumatoid arthritis in persons 60 years of age and older in the United States: Effect of different methods of case classification. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 2003, 48(4), 917-26. [CrossRef]
- Leyland KM, Gates LS, Sanchez-Santos MT, Nevitt MC, Felson D, Jones G; et al. Knee osteoarthritis and time-to all-cause mortality in six community-based cohorts: An international meta-analysis of individual participant-level data. Aging Clin Exp Res. 2021, 33, 529-45. [CrossRef]
- Roseen EJ, Rajendran I, Stein P, Fredman L, Fink HA, LaValley MP, Saper RB. Association of back pain with mortality: A systematic review and meta-analysis of cohort studies. J Gen Intern Med. 2021, 36, 3148-58. [CrossRef]
- Stubbs B, Binnekade TT, Soundy A, Schofield P, Huijnen IP, Eggermont LH. Are older adults with chronic musculoskeletal pain less active than older adults without pain? A systematic review and meta-analysis. Pain Medicine. 2013, 14(9), 1316-31. [CrossRef]
- Baumgartner RN, Waters DL, Gallagher D, Morley JE, Garry PJ. Predictors of skeletal muscle mass in elderly men and women. Mech Ageing Dev. 1999, 107(2), 123-36. [CrossRef]
- Chuang S-Y, Chang H-Y, Lee M-S, Chen RC-Y, Pan W-H. Skeletal muscle mass and risk of death in an elderly population. Nutr Metab Cardiovasc Dis. 2014, 24(7), 784-91. [CrossRef]
- Pan F, Tian J, Scott D, Cicuttini F, Jones G. Muscle function, quality, and relative mass are associated with knee pain trajectory over 10.7 years. Pain. 2022, 163(3), 518-25. [CrossRef]
- Law LF, Sluka KA. How does physical activity modulate pain? Pain. 2017, 158(3), 369. [CrossRef] [PubMed]
- Park JH, Lim S, Lim J, Kim K, Han M, Yoon IY; et al. An overview of the Korean longitudinal study on health and aging. Psychiatry Investig. 2007, 4(2), 84.
- Tg, L. Anthropometric standardization reference manual. Human kinetics books. 1988:55-68.
- Lukaski HC, Johnson PE, Bolonchuk WW, Lykken GI. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am J Clin Nutr. 1985, 41(4), 810-7. [CrossRef]
- Mijnarends DM, Meijers JM, Halfens RJ, ter Borg S, Luiking YC, Verlaan S; et al. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J Am Med Dir Assoc. 2013, 14(3), 170-8. [CrossRef]
- Expert Panel on Detection E, Adults ToHBCi. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III. JAMA. 2001, 285(19), 2486-97. [CrossRef]
- Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ; et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. iabetes Res Clin Pract. 2007, 75(1), 72–80. [CrossRef]
- Bellamy, N. Validation study of WOMAC: A health status instrument for measuring clinically important patient-relevant outcomes following total hip or knee arthroplasty in osteoarthritis. J Orthop Rheumatol. 1988, 1, 95–108. [Google Scholar]
- Fairbank JC, Couper J, Davies JB, O'Brien JP. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980, 66(8), 271-3.
- Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE; et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003, 35(8), 1381-95. [CrossRef]
- Dahlhamer J, Lucas J, Zelaya C, Nahin R, Mackey S, DeBar L; et al. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018, 67(36), 1001-6. [CrossRef]
- Blyth FM, Noguchi N. Chronic musculoskeletal pain and its impact on older people. Best Pract Res Clin Rheumatol. 2017, 31(2), 160-8. [CrossRef]
- Eggermont LH, Bean JF, Guralnik JM, Leveille SG. Comparing pain severity versus pain location in the MOBILIZE Boston study: Chronic pain and lower extremity function. J Gerontol A Biol Sci Med Sci. 2009, 64(7), 763-70. [CrossRef]
- Croft P, Jordan K, Jinks C. "Pain elsewhere" and the impact of knee pain in older people. Arthritis Rheum. 2005, 52(8), 2350-4. [CrossRef]
- Rundell SD, Patel KV, Krook MA, Heagerty PJ, Suri P, Friedly JL; et al. Multi-site Pain Is Associated with Long-term Patient-Reported Outcomes in Older Adults with Persistent Back Pain. Pain Med. 2019, 20(10), 1898-906. [CrossRef]
- de Vitta A, Machado Maciel N, Bento TPF, Genebra C, Simeão S. Multisite musculoskeletal pain in the general population: A cross-sectional survey. Sao Paulo Med J. 2022, 140(1), 24–32. [CrossRef] [PubMed]
- Chen L, Ferreira ML, Nassar N, Preen DB, Hopper JL, Li S; et al. Association of chronic musculoskeletal pain with mortality among UK adults: A population-based cohort study with mediation analysis. EClinicalMedicine. 2021, 42. [CrossRef]
- Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ; et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur J Epidemiol. 2018, 33(9), 811-29. [CrossRef]
- Martin RR, Hadjistavropoulos T, McCreary DR. Fear of pain and fear of falling among younger and older adults with musculoskeletal pain conditions. Pain Res Manag. 2005, 10(4), 211-9. [CrossRef]
- Karttunen N, Lihavainen K, Sipilä S, Rantanen T, Sulkava R, Hartikainen S. Musculoskeletal pain and use of analgesics in relation to mobility limitation among community-dwelling persons aged 75 years and older. Eur J Pain. 2012, 16(1), 140-9. [CrossRef]
- Panhale VP, Gurav RS, Nahar SK. Association of Physical Performance and Fear-Avoidance Beliefs in Adults with Chronic Low Back Pain. Ann Med Health Sci Res. 2016, 6(6), 375-9. [CrossRef]
- Leveille SG, Guralnik JM, Hochberg M, Hirsch R, Ferrucci L, Langlois J; et al. Low back pain and disability in older women: Independent association with difficulty but not inability to perform daily activities. J Gerontol A Biol Sci Med Sci. 1999, 54(10), M487-93. [CrossRef]
- Kitayuguchi J, Kamada M, Hamano T, Nabika T, Shiwaku K, Kamioka H; et al. Association between knee pain and gait speed decline in rural J apanese community-dwelling older adults: 1-year prospective cohort study. Geriatr Gerontol Int. 2016, 16(1), 55–64. [CrossRef]
- Yanardag M, Şimşek TT, Yanardag F. Exploring the Relationship of Pain, Balance, Gait Function, and Quality of Life in Older Adults with Hip and Knee Pain. Pain Manag Nurs. 2021, 22(4), 503-8. [CrossRef]
- Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, Alter DA. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann Intern Med. 2015, 162(2), 123-32. [CrossRef]
- Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA; et al. The physical activity guidelines for Americans. JAMA. 2018, 320(19), 2020-8. [CrossRef]
- Zhao M, Veeranki SP, Magnussen CG, Xi B. Recommended physical activity and all cause and cause specific mortality in US adults: Prospective cohort study. BMJ. 2020, 370, m2031. [CrossRef]
- Tieland M, Trouwborst I, Clark BC. Skeletal muscle performance and ageing. J Cachexia Sarcopenia Muscle. 2018, 9(1), 3–19. [CrossRef]
- Nguyen CP, Hirsch MS, Moeny D, Kaul S, Mohamoud M, Joffe HV. Testosterone and "Age-Related Hypogonadism"--FDA Concerns. N Engl J Med. 2015, 373(8), 689-91. [CrossRef]
- Hermann M, Berger P. Hormonal changes in aging men: A therapeutic indication? Exp Gerontol. 2001, 36(7), 1075-82. [CrossRef]
- Curcio F, Ferro G, Basile C, Liguori I, Parrella P, Pirozzi F; et al. Biomarkers in sarcopenia: A multifactorial approach. Exp Gerontol. 2016, 85, 1–8. [CrossRef]
- Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front Physiol. 2012, 3, 260. [CrossRef]
- Wang DXM, Yao J, Zirek Y, Reijnierse EM, Maier AB. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J Cachexia Sarcopenia Muscle. 2020, 11(1), 3–25. [CrossRef] [PubMed]
- Berger MJ, Doherty TJ. Sarcopenia: Prevalence, mechanisms, and functional consequences. Interdiscip Top Gerontol. 2010, 37, 94–114. [CrossRef]
- Zhou HH, Liao Y, Peng Z, Liu F, Wang Q, Yang W. Association of muscle wasting with mortality risk among adults: A systematic review and meta-analysis of prospective studies. J Cachexia Sarcopenia Muscle. 2023, 14(4), 1596-612. [CrossRef]
- Stowe RP, Peek MK, Cutchin MP, Goodwin JS. Plasma cytokine levels in a population-based study: Relation to age and ethnicity. J Gerontol A Biol Sci Med Sci. 2010, 65(4), 429-33. [CrossRef]
- Zhang JM, An J. Cytokines, inflammation, and pain. Int Anesthesiol Clin. 2007, 45(2), 27–37. [CrossRef]
Figure 1.
The proportion of MSK Pain: (A) Individual pain and (B) Number of pain between Survivor and Non-Survivor Groups (n(%)). The non-survivor group showed significantly higher rates of MSK pain and multiple MSK pain.
Figure 1.
The proportion of MSK Pain: (A) Individual pain and (B) Number of pain between Survivor and Non-Survivor Groups (n(%)). The non-survivor group showed significantly higher rates of MSK pain and multiple MSK pain.
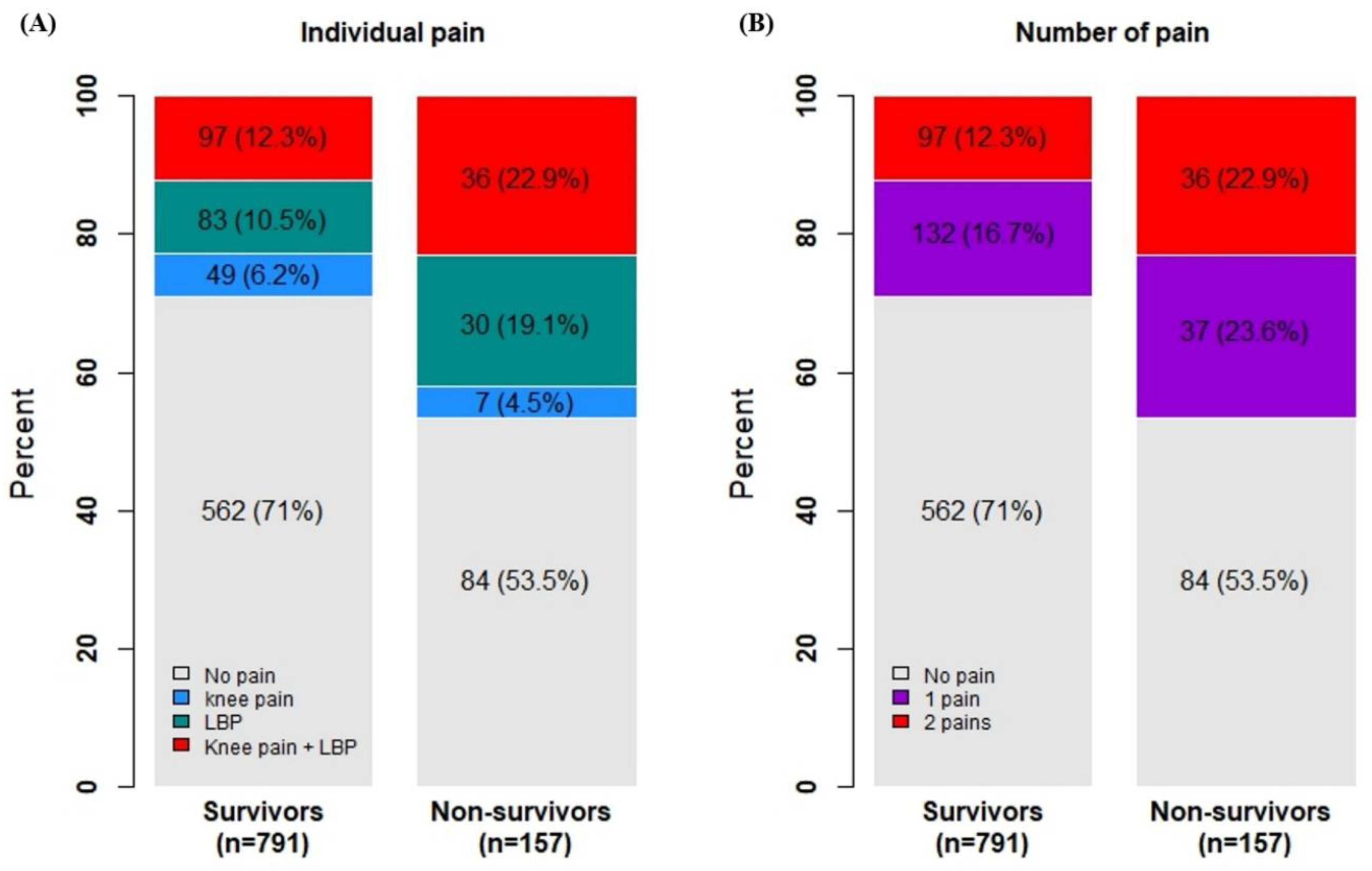

Table 1.
Characteristics of study participants.
| Total (n=1000) | Survivor (n = 829) |
Non-Survivor (n = 171) |
P-Value | ||
|---|---|---|---|---|---|
| Age (years) (n = 1000) | 76.3 ± 8.7 | 74.8 ± 8.1 | 83.7 ± 7.8 | < 0.001∗ | |
| Sex (n = 1000) | 0.061 | ||||
| Male | 441 (44.1) | 354 (42.7) | 87 (50.9) | ||
| Female | 559 (55.9) | 475 (57.3) | 84 (49.1) | ||
| BMI (m2/kg) (n = 871) | 24.0 ± 3.3 | 24.1 ± 3.3 | 22.9 ± 3.3 | < 0.001∗ | |
| ASM (kg) (n = 877) | 12.8 ± 3.3 | 12.9 ± 3.3 | 12.3 ± 3.5 | 0.098 | |
| Metabolic syndrome (n = 996) | 0.753 | ||||
| No | 631 (63.4) | 521 (63.1) | 110 (64.7) | ||
| Yes | 365 (36.6) | 305 (36.9) | 60 (36.3) | ||
| Low back pain (n = 950) | < 0.001∗ | ||||
| No | 703 (74.0) | 612 (77.3) | 91 (57.6) | ||
| Yes | 247 (26.0) | 180 (22.7) | 67 (42.4) | ||
| Knee pain (n = 949) | 0.016∗ | ||||
| No | 76.0 (80.1) | 645 (81.5) | 115 (72.8) | ||
| Yes | 189 (19.9) | 146 (18.5) | 43 (27.2) | ||
| Alcohol (n = 992) | 0.185 | ||||
| No | 761 (76.7) | 625 (75.8) | 136 (81.0) | ||
| Yes | 231 (23.3) | 199 (24.2) | 32 (19.0) | ||
| Smoking (n=1000) | 1.000 | ||||
| No | 711 (71.1) | 589 (71.0) | 122 (71.3) | ||
| Yes | 289 (28.9) | 240 (29.0) | 49 (28.7) | ||
| Regular exercise (n = 989) | < 0.001∗ | ||||
| No | 492 (49.7) | 377 (45.9) | 115 (68.5) | ||
| Yes | 497 (50.3) | 444 (54.1) | 53 (31.5) | ||
Values are presented as mean ± standard deviation or number (%). BMI, body mass index; ASM, appendicular skeletal muscle mass. ∗ Significant difference between groups, p < 0.05 by independent t-test and chi-square test.
Table 2.
Correlations among pain, regular exercise, and other variables, as well as between specific pain types or pain occurrences and mortality.
Table 2.
Correlations among pain, regular exercise, and other variables, as well as between specific pain types or pain occurrences and mortality.
| Variables | |||
|---|---|---|---|
| Variables | Low Back Pain | Knee Pain | Regular Exercise |
| Age | 0.220** | 0.160** | 0.152** |
| Sex | 0.255** | 0.279** | 0.291** |
| BMI | -0.008 | 0.086* | 0.035 |
| ASM | -0.245** | -0.236** | 0.311** |
| Metabolic syndrome | 0.091** | 0.148** | -0.069** |
| Low back pain | - | 0.506** | -0.245** |
| Knee pain | 0.506** | - | -0.264** |
| Alcohol | -0.127** | -0.176** | 0.129** |
| Smoking | -0.122** | -0.163** | 0.119** |
| Regular exercise | -0.245** | -0.264** | - |
| Individual pain† | MSK pain‡ | Regular exercise | |
| Mortality | 0.164** | 0.145** | -0.169** |
Values represent correlation coefficients (Cramer’s V, or Phi). BMI, body mass index; ASM, appendicular skeletal muscle mass; MSK, musculoskeletal. ** p< 0.01. † No pain, Low back pain, knee pain, Low back pain + knee pan. ‡ No pain, 1 pain (low back pain or knee pain), 2 pains (low back pain and knee pain).
Table 3.
Results of logistic regression analysis of factors associated with non-survivor at the follow-up.
Table 3.
Results of logistic regression analysis of factors associated with non-survivor at the follow-up.
| Characteristics | Univariate Model | Multivariate Model 1§ | Multivariate Model 2⁋ | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P | |
| Age | 1.133 (1.108-1.159) | < 0.001 | 1.095 (1.065-1.126) | < 0.001 | 1.095 (1.065-1.126) | < 0.001 |
| Sex (Female)* | 0.720 (0.517-1.001) | 0.051 | 0.138 (0.063-0.302) | < 0.001 | 0.138 (0.063-0.302) | < 0.001 |
| Metabolic syndrome | 0.932 (0.660-1.315) | 0.688 | ||||
| BMI | 0.897 (0.894-1.010) | 0.001 | 0.299 | 0.299 | ||
| ASM | 0.950 (0.383-0.751) | 0.098 | 0.822 (0.732-0.923) | 0.001 | 0.822 (0.732-0.923) | 0.001 |
| Low back pain | 2.503(1.752-3.576) | < 0.001 | 0.442 | |||
| Knee pain | 1.652 (1.114-2.499) | 0.012 | 0.956 | |||
| Alcohol | 0.739 (0.487-1.121) | 0.155 | 0.235 | 0.235 | ||
| Smoking | 0.986 (0.685-1.418) | 0.938 | ||||
| Regular exercise | 0.391 (0.275-0.557) | < 0.001 | 0.465 (0.287-0.754) | 0.002 | 0.465 (0.287-0.754) | 0.002 |
| MSK pain (1)† | 1.875 (1.219-2.885) | 0.004 | 0.979 | |||
| MSK pain (2)‡ | 2.483 (1.590-3.879) | < 0.001 | 0.661 | |||
BMI, body mass index; ASM, appendicular skeletal muscle mass; MSK, musculoskeletal; OR, odds ratio; CI: confidence interval.* reference: male. † Low back pain or knee pain. ‡ Low back pain and knee pain. § Including lower back pain and knee pain, respectively. ⁋ Including MSK pain categorized by number.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



