Submitted:
13 January 2024
Posted:
15 January 2024
You are already at the latest version
Abstract
Among endocrine cancers, thyroid carcinoma is the most prevalent type of cancer. It's prevalence has been increased throughout the world during the last decades, which shows great regional variations. Considering the increasing prevalence and occurrence of thyroid cancer cases, in this study we: Among endocrine cancers, thyroid carcinoma is the most prevalent type of cancer. It's prevalence has been increased throughout the world during the last decades, which shows great regional variations. Considering the increasing prevalence and occurrence of thyroid cancer cases, in this study we decided to evaluate the clinical and pathological charactristics of this endocrine system cancer in the population of thyroid cancer patients reffered to imam Khomeini Hospital in Sari between March 2014 and March 2021. decided to evaluate the clinical and pathological charactristics of this endocrine system cancer in the population of thyroid cancer patients reffered to imam Khomeini Hospital in Sari between March 2014 and March 2021.
Keywords:
Thyroid carcinoma
; Prevalence
; Endocrine cancers
; Clinical characteristics
; Pathological charac-teristics
1. Introduction
Among endocrine cancers, thyroid carcinoma is the most prevalent type of cancer. It's prevalence has grown around the world in recent decades, with significant regional variations [1]. According to the International Agency for Research on Cancer (IARC) studies in 2020, thyroid cancer accounts for about 3% of all human malignancies. And there are approximately 586000 new cases worldwide each year [2]. In 2018, there were 567233 newly reported cases of thyroid cancer worldwide, with a significantly higher incidence in women compared to men (10.2 per 100000 versus 3.1 per 100000). The majority (over 95%) of thyroid cancers originate from thyroid follicular cells, which are categorized as differentiated, poorly differentiated and anaplastic. The main types of differentiated thyroid cancers are PTC (papillary thyroid carcinoma) and FTC (follicular thyroid carcinoma). In Africa, PTC and FTC are the most common histological types, with a notable proportion being FTC. In areas where there is a lack of iodine and a high number of people affected by goiter, follicular thyroid cancer (FTC) is frequently found. Over the 30 years, there has been a global increase in occurrence of papillary thyroid cancer (PTC) and tumors smaller than 20mm, while other types of thyroid cancer have either decreased or remained stable. The reasons for this trend are still the subject of debate [3]. The increased incidence of thyroid cancer is often attributed to increased detection due to better access to health care, rigorous health screening with increased use of thyroid imaging, and optimal management strategies [4]. Better diagnostic methods, such as the widespread use of thyroid ultrasound and an increase in thyroid biopsies, are the most significant factors that influences the rate of thyroid cancer diagnosis. Contrarily, the phenomena of over diagnosis likely predominates the actual changes in the epidemiology of thyroid cancer associated to longer life expectancy, variations in iodine consumption, and radiation exposure in the community under study [5]. The World Health Organization (WHO) classifies malignant tumors derived from thyroid follicular epithelium based on their histological characteristics. Five main types of thyroid cancer are identified: papillary thyroid cancer (PTC), follicular thyroid cancer (FTC), poorly differentiated thyroid cancer (PDTC), medullary thyroid cancer (MTC), and anaplastic thyroid cancer.(5) There is a wide range of clinical behavior in thyroid cancers, from tumors with typically low mortality to more aggressive malignancies like anaplastic thyroid cancer. In order to receive the optimal treatment, it is crucial to perform a thorough diagnostic examination before beginning the treatment [6]. Experts in the field of thyroid cancer have determined that the rise in the number of cases is mainly due to the detection of small T1 papillary tumors (less than 2 cm in size). These tumors are often over diagnosed and the cancers that are diagnosed are unlikely to cause harm to the patient [7]. This study aimed to evaluate the clinic pathological characteristics of thyroid cancer patients referred to Imam Khomeini Hospital of Sari between March 2014 and March 2021. We evaluated factors such as age group, gender, family history of thyroid cancer, history of hypothyroidism, distant metastasis in thyroid cancer, type of thyroid cancer pathology, tumor stage, capsule involvement, tumor size, and lymph node involvement.
2. Materials and Methods
The quantifiable population of this descriptive and retrospective study, which spans from early March 2014 to late March 2021, consists of all thyroid cancer patients referred to Imam Khomeini Hospital. The analysis of patient's medical records yields the knowledge about the necessary variables, which is then recorded in the table of variables. Following data collection, Chi – Square and Fisher's exact statistical tests are used in the SPSS 2020 program to examine the results. P value < 0.05 is considered to be a crucial level in all circumstances.
3. Results
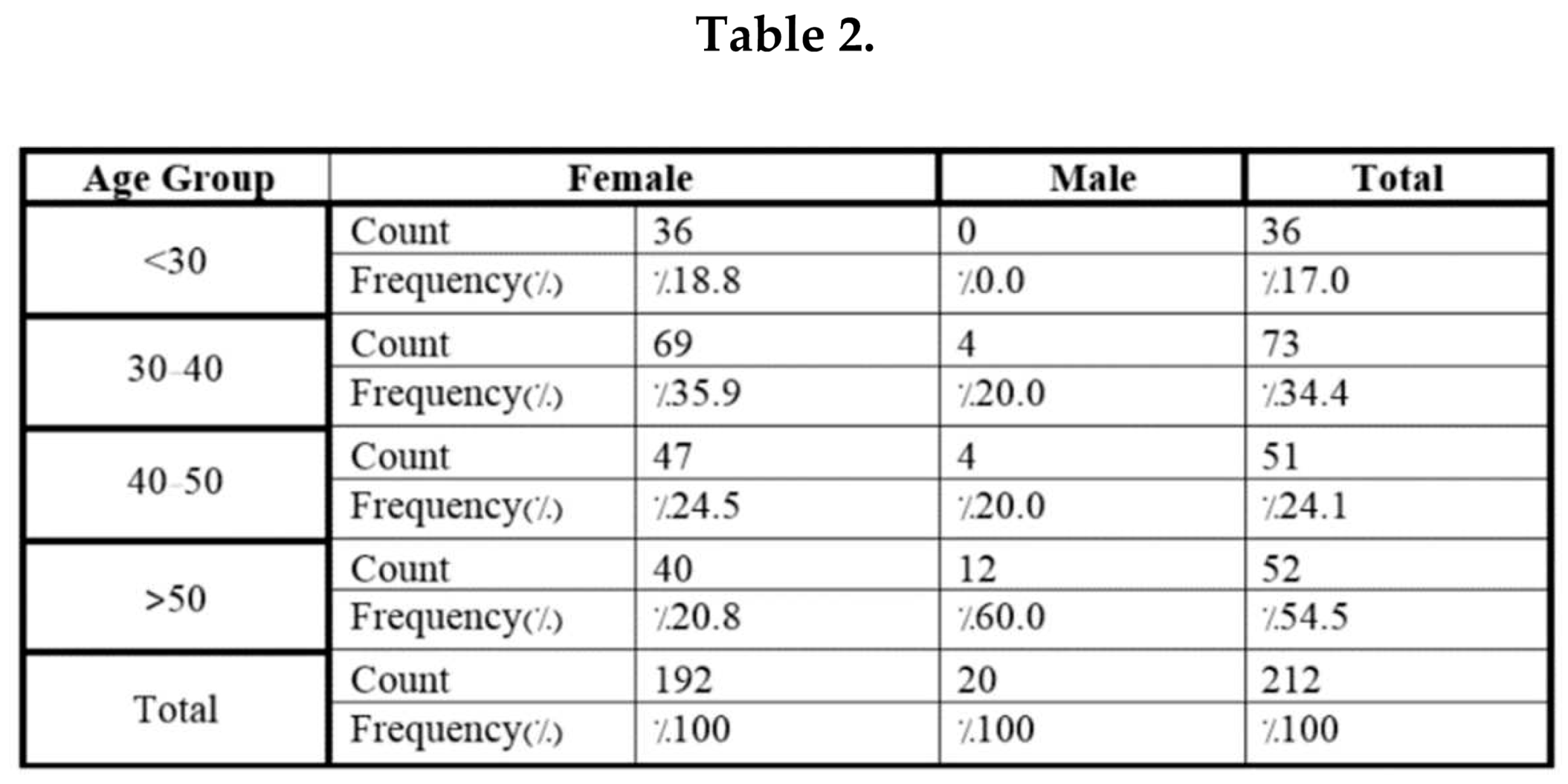
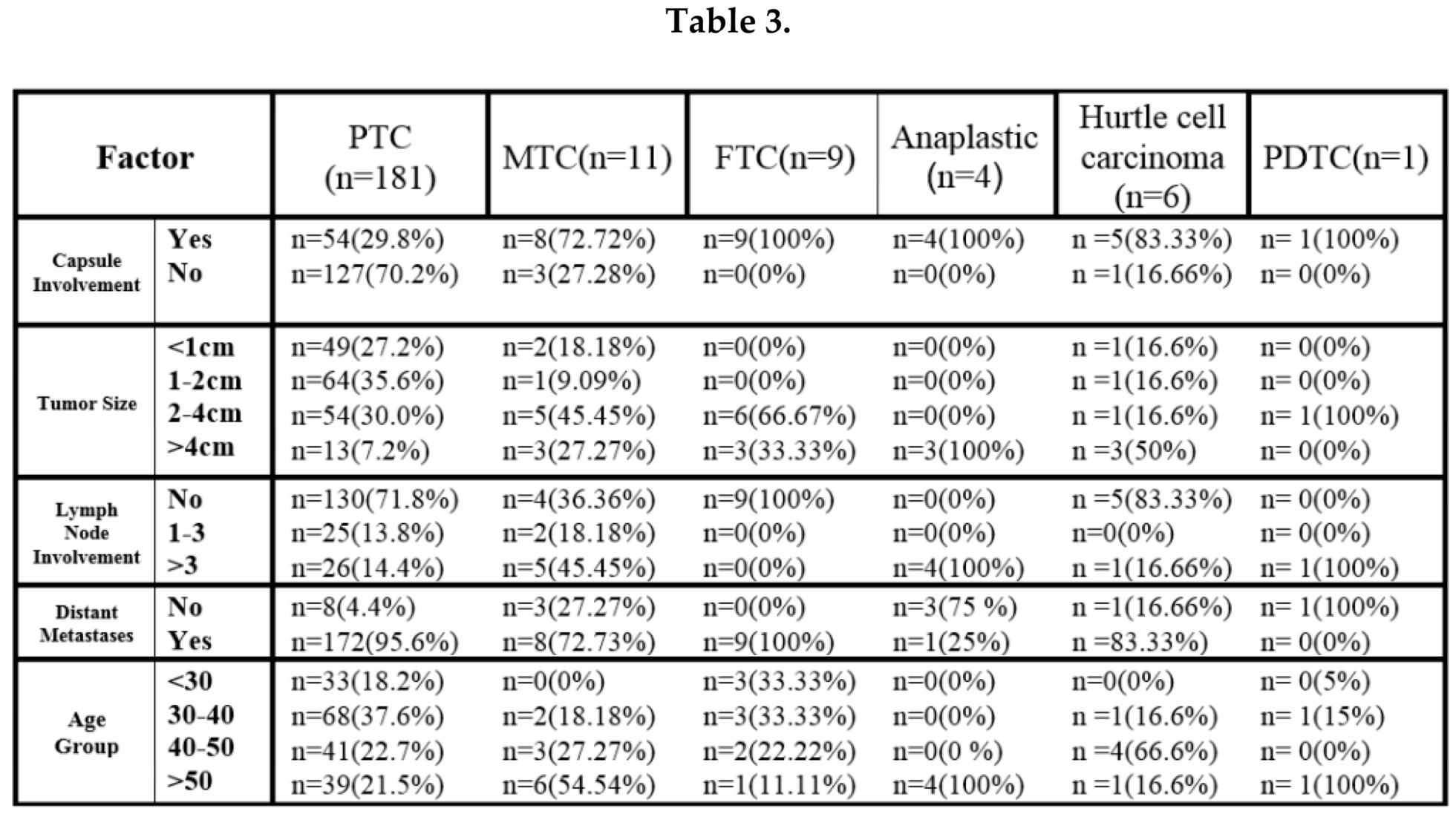
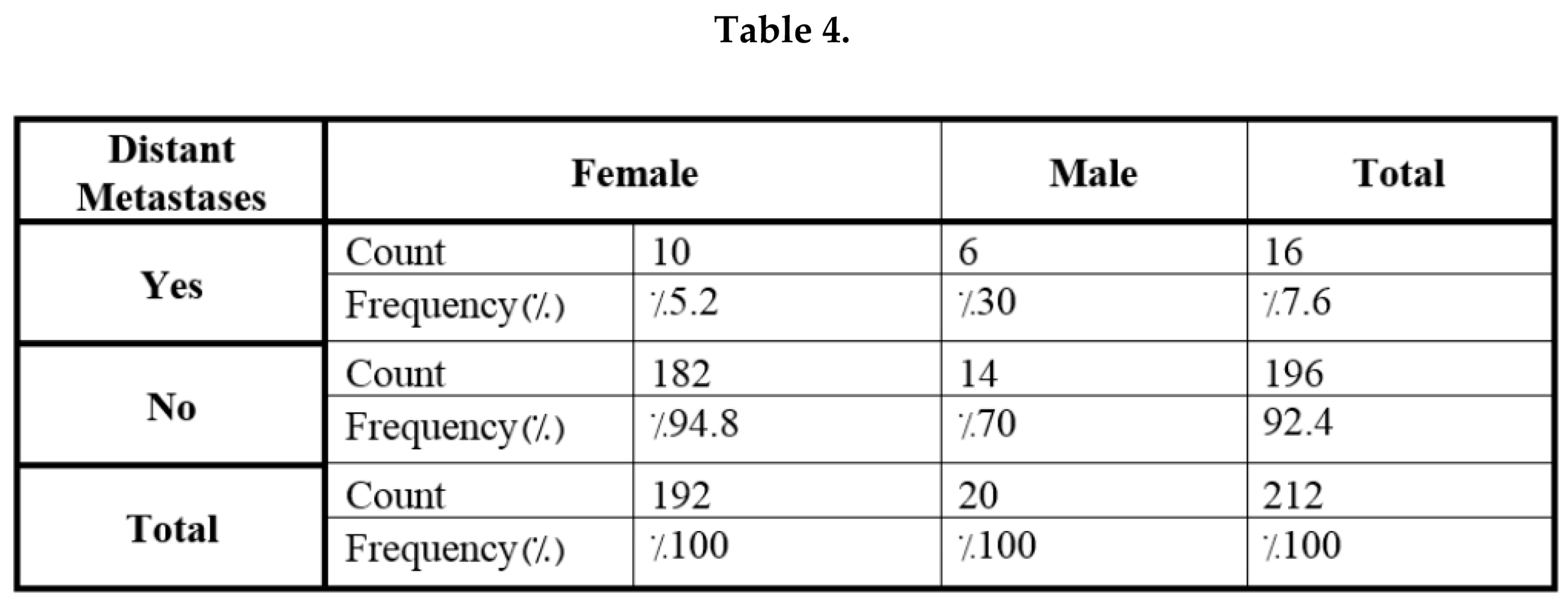
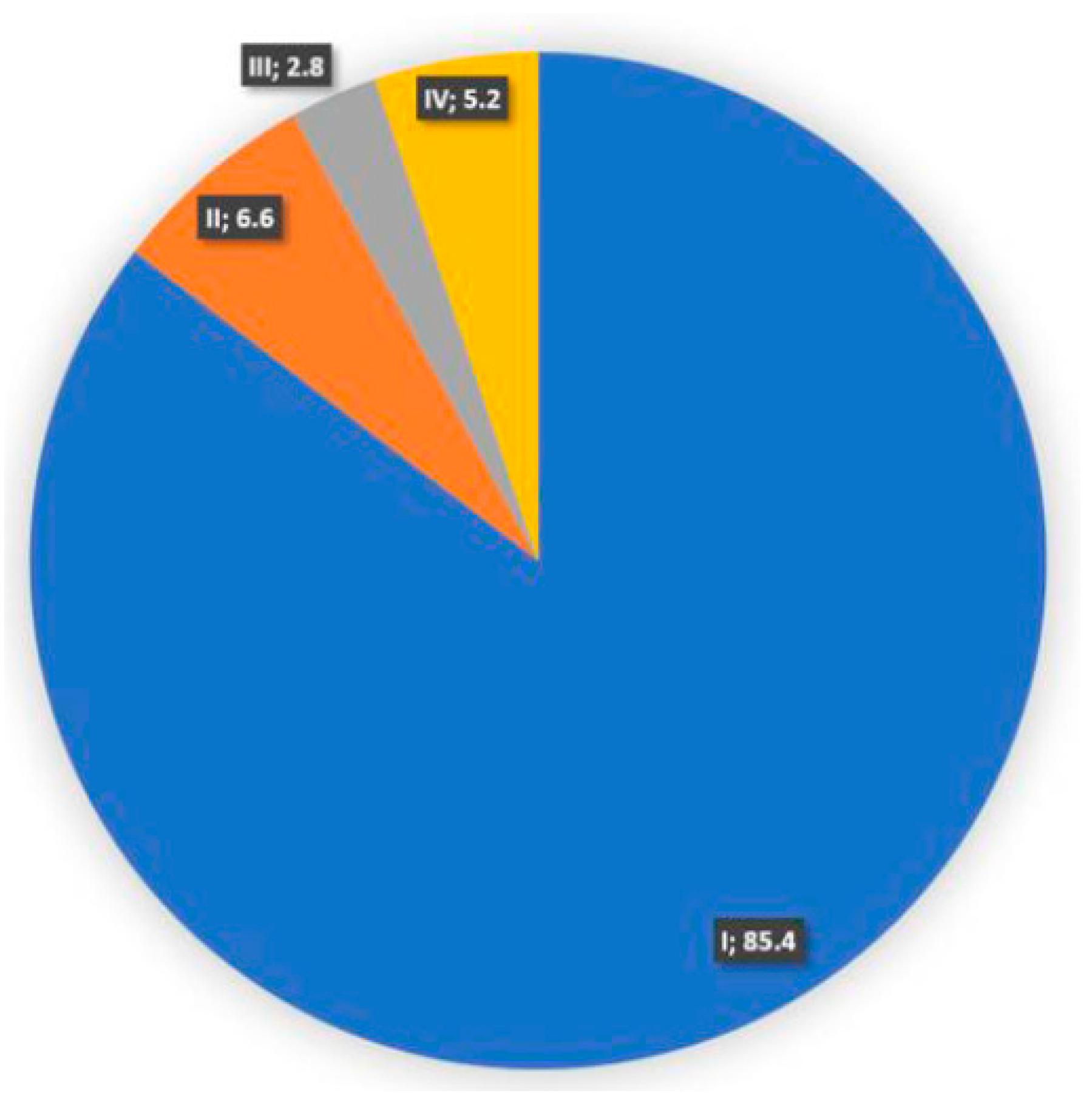
This study evaluated 214 patients with thyroid cancer, of which 212 had cancer derived from thyroid epithelium. The primary focus of this research was to analyze the clinicopathological characteristics of thyroid cancers originating from the thyroid epithelium. Two other patients, a 65-year-old female with B-cell lymphoma involving the thyroid and a 66-year-old man with metastatic laryngeal SCC cancer, both underwent total thyroidectomy to treat their respective thyroid tumors. Table 1 & Figure 1 reveal that the most prevalent histological variant of thyroid cancer in the studied population was PTC (181/212, 85.4%), followed by MTC (11/212, 5.2%), FTC (9/212, 4.2%), Hurtle cell carcinoma (6/212, 2.8%), Anaplastic thyroid carcinoma (4/212, 1.9%) and PDTC (1/212, 0.5%). Notably, the female to male prevalence ratio was 9.6 to 1 (192/212, 90.6% versus 20/212, 9.4%), indicating that the majority of patients with thyroid cancer in the studied population were female. An analysis of the average frequency of tumor size revealed that tumors measuring between 2 and 4 cm were the most common, accounting for 31.8% (67/212) of all cases (Figure 2). However, a closer look at Table 1 reveals that the total frequency of tumors smaller than 1 cm and those between 1 and 2 cm (118/212,55.9%) is actually the highest. In other words, most thyroid tumors are smaller than 2 cm, but the prevalence of tumors between 2 and 4 cm is on the rise. The most prevalent age range for thyroid cancer in studied population was 30 to 40 years (Table 1 & Figure 3). At the time of surgery, the majority of tumors were classified as stage I according to the AJCC classification system (Table 1 & Figure 4). To further investigate the involvement of lymph nodes in this population of thyroid cancer patients, we divided lymph node involvement into three categories: no lymph node involvement, 1 to 3 lymph node involvement and more than 3 lymph node involvement.147 patients (69.3%) did not have any lymph node involvement, 28 patients (13.2%) had involvement of one to three lymph nodes, and 37 patients (17.5%) had involvement of four or more lymph nodes. In general, 30.7% of patients in this study had lymph node involvement (Table 1). In this study, lymph node involvement refers to the total number of lymph nodes that have tumoral involvement in the pathological examination, not just the lymph nodes that are dissected during surgery. In the patients of the study population, the prevalence of capsule involvement, positive family history of thyroid cancer, distant metastasis, and history of hypothyroidism is respectively, 38.2%, 9.9%, 7.6%, and 33%. (Table 1). Our investigation revealed that most thyroid cancer patients were over 50 years old (12/20, 60%) in men and between 30 and 40 years old (69/192, 35.9%) in women (details of findings are presented in Table 2). The majority of papillary thyroid cancer cases (68/181, 37.6%) occurred in people between the ages of 30 and 40, while all anaplastic thyroid cancer patients were older than 50 (Table 3). In examining the frequency of distant metastasis in all types of thyroid cancers in the study population, out of 16 cases of distant metastasis, 8 cases were related to papillary thyroid cancers (8/181, 4.4% of all PTCs). The highest frequency of distant metastasis was in the population of anaplastic thyroid cancers (3/4, 75% of anaplastic thyroid cancers) (Table 3). The most distant metastasis was in the lung, and other organs in order of frequency are the posterior and lateral lymph nodes of the neck, brain, bone and skull. We also had one case of MTC metastatic to the lung and bone. In the evaluation of distant metastasis by gender in the patients of the study population, it has been shown that the frequency of distant metastasis in male patients with thyroid cancer (6/20, 30%) is higher than in female patients (10/192, 5.2%) (Table 4). It has been determined that, of the 181 papillary cancer cases in the study population, a total of 51 cases (28.2%) had lymph node involvement (whether involvement in 1 to 3 lymph nodes or more than 3 lymph nodes), according to an analysis of the frequency of lymph node involvement in each type of thyroid cancer in our study. In contrast to all FTC instances, all anaplastic carcinoma patients exhibited lymph node involvement (Table 3). The majority of papillary thyroid cancer tumors in the study to estimate the frequency of average size according to pathology had an average size between 1 and 2 cm (64/181, 35.6%). Anaplastic cancer tumors were all greater than 4 cm (Table 3). Out of 181 papillary cancer cases, 54 instances (29.8%) had capsule involvement, according to our study's analysis of capsule involvement in each kind of thyroid cancer. Capsule involvement was present in every instance of anaplastic carcinoma and FTC (Table 3).
4. Discussion
Given the increasing prevalence of thyroid cancer and the lack of research on the clinic pathological evaluation of patients with thyroid cancer at Mazandran University of Medical sciences, it is essential to conduct studies in this area. Such studies that analyze the clinic pathological characteristics of cancers can be a great aid to clinicians in accurately predicting the clinical behavior of the tumor. By understanding the clinic pathological characteristics of a tumor and the prognostic factors associated with it, healthcare professionals can improve the prognosis and response to treatment of cancer patients. This knowledge can help reduce mortality and morbidity, and enable clinicians to make informed decisions about the most effective treatment options based on the predicted outcome. Our study has revealed that thyroid cancer is more prevalent in women than in men, with a female – to – male ratio of 9.6 to 1. This finding has been corroborated by the most articles that have examined the clinic pathological aspects of this cancer, as evidenced by Zahi Abdul Sater's study [8]. Thus, it is clear that certain types of cancer are more common in certain genders. Also, in the study of Bo Youn Cho et al., 82.9% of thyroid cancer patients were female [9]. In the study by Uzma Bukheri et al., 82.4% of thyroid cancer patients were female [10]. This could be attributed to the fact that higher estrogen levels in women are considered a risk factor for thyroid cancer [11]. Additionally, increased detection of thyroid cancer in women, especially during the reproductive period and early life, could be due to annual gynecologic and obstetric examinations. While the gradual rise in thyroid cancer cases among men may be attributed to increased medical visits in later life [12]. Additionally, the higher prevalence of thyroid cancer in women compared to men could be due to the difference in the immune editing system and immune tolerance between the two genders [13]. Numerous studies have been conducted to explore the link between prior thyroid conditions, such as hypothyroidism, hyperthyroidism, multi nodular goiter, thyroid nodule, Hashimoto's and Grave's thyroiditis, and the risk of thyroid cancer. However, the epidemiological evidence regarding this association has been inconclusive [14]. It has been suggested that thyroid hormones and TSH can directly stimulate tumor growth through surface receptors, estrogen pathways, angiogenesis, and gene expression regulation [15]. The thyroid gland dysfunction is not only linked to other diseases, such as obesity [16], diabetes mellitus, and vascular diseases [17], but it can also increase the risk of cancer. Hypothyroidism is characterized by high levels of TSH, which is a known growth factor for thyroid nodules. The prolonged stimulation of TSH in hypothyroidism may contribute to the development or growth of thyroid carcinoma [18]. In a study conducted by Zoleika Moazezi et al., which explored the risk factors of thyroid cancer through a case – control study, the prevalence of hypothyroidism among thyroid cancer patients was found to be 30.4% [19]. Our own study corroborated this finding, with a frequency of 33% for hypothyroidism in the population of thyroid cancer patients. Papillary thyroid cancer is the most common histological variant of thyroid cancer, accounting for 80 – 85% of thyroid cancers. The 10- year survival rate of papillary cancer is more than 90% [20]. In our study, papillary thyroid cancer was the most common pathological variant of thyroid cancer with a frequency of 85.4%. In the study of Dr.Baqer L arijani et al., papillary thyroid cancer was the most frequent pathological variant of thyroid cancer with a frequency of 79.7% [21]. The frequency of the papillary variant of thyroid cancer was 92% according to Marco Capezzone et al [22], 69% according Umesh Jayarajah's study [23], and 78.8% according to Amani Saleh Hadi's study [24]. In our study, the most common histological variant of thyroid cancer after PTC was MTC, with a frequency of 5.2%. Marco Capezzone [22], Baqer Larijani [21], and most other studies conducted in connection with the clinic pathological evaluation of thyroid cancer have found that the most common pathological variant after PTC was FTC. Awra F.Flemban's research has revealed that the occurrence of MTC is on the rise [25]. In the United States alone, an estimated 1200 cases of MTC are diagnosed each year [26]. Despite this, the cause of the increasing prevalence of MTC in certain regions remains unclear [27]. Small local malignancies to large metastatic malignancies are all clinical manifestations of thyroid cancer [28]. Thyroid cancer patients who develop distant metastases, particularly differentiated thyroid carcinoma, have a worse chance of survival than thyroid cancer patients who do not [29]. Organs such the lung, bones, brain, and liver are the most typical locations for distant metastasis in thyroid tumors [30]. Only 10% of instances of anaplastic thyroid carcinoma are restricted to the thyroid, and about 50% of cases have distant metastases [31]. Age, high tumor size, vascular invasion, and lymph node involvement are among the characteristics that have been identified as risk factors for distant metastasis [32]. Our study found that 7.6% of thyroid cancer patients had distant metastases, which is lower than Fiaza A. Qari's study's 11% incidence [33]. The most frequent site of thyroid carcinoma distant metastasis in our analysis was the lung; this result is consistent with that of Abdul Aziz et al.'s study [34]. The population of anaplastic tumors in our study had the highest frequency of distant metastasis, followed by the population of medullary malignancies, and there were no occurrences of distant metastasis reported in FTC cases. The highest frequency of distant metastasis was associated with MTC in the study of Baqer Larijani et al., and in this study, the frequency of distant metastasis in the FTC thyroid cancer population was equivalent to 21.2% [21]. In our study frequency of distant metastasis in male thyroid cancer patients (30%) is more than in female thyroid cancer patients (5.2%). In other words, we can draw the conclusion that men are more likely than women to get severe thyroid malignancies. In contrast to the results of our investigation, the gender ratio in the study of Abdul Aziz et al. was equal [34] More research is necessary to support this finding. The majority of thyroid tumors that are newly discovered are smaller than 2 cm in size and are most often asymptomatic [35]. One of the clinico pathological charactristics that was also looked at in our investigation was tumor size. Our findings showed that tumors between 2 and 4 cm in size were the most prevalent, occurring 31.8% of the time (67/212) and that the prevalence of tumors of this size is rising, which is consistent with the results of Ramadani's study [36]. The incidence of tumors between 2 and 4 cm in size remained constant in the article presented by Kent et al [37]. Such a finding conflicts what we obtained from our research. One of the charactristics of cancer is the ability of tumor cells to invade nearby tissues [38]. When reviewing thyroidectomy materials, pathologists should be conversant with three forms of invasion: capsular invasion, vascular invasion for tumor categorization, and extra thyroidal invasion and extension for tumor staging. Currently, the cytological background and tumor tissue shape play a role in how capsular invasion and vascular invasion are used to categorize the kind of tumor [39]. The majority of thyroid neoplasms that have a follicular form and are encased in a fibrous capsule are actually thought to be slow-growing tumors [40]. 38.2% (81/212) of the thyroid tumors in our study had capsule involvement. This figure corresponds to 33.5% in Shaza Samargandy's study [41]. Lymph node involvement in our study refers to tumor infiltration in the cervical lymph nodes removed during thyroidectomy surgery. Lymph node involvement in thyroid malignancies was present in 30.7% (65/212) of the study population. In Izadi's study the prevalence of lymph node involvement in thyroid carcinoma was 21.3% [42]. This percentage in Samargandy's study was 24.9% [41].
5. Conclusion
The results of our research revealed that the most prevalent age group for thyroid cancer in the studied population was 30 to 40 years. Additionally, our study demonstrated that the incidence of thyroid cancer is higher in men over the age of 50, confirming that thyroid cancer is more common in older males. In our study, the majority of thyroid cancer patients in the study population, that is, approximately 90.6% were female. According to numerous articles and studies conducted worldwide, female gender itself is considered a risk factor for thyroid cancer. Our study results revealed the significance of family history of thyroid cancer in first – degree relatives and a history of thyroid disease in the patient (hypothyroidism, hyperthyroidism, thyroiditis, multi nodular goiter, etc.) in relation to thyroid cancer. This was further supported by our analysis and review of other relevant articles and researches. Consequently, it is advisable to have regular check – ups and to pay special attention to individuals with a family history of thyroid cancer and hypothyroidism for effective thyroid cancer screening. Our research has revealed that the most commonly observed histological type of thyroid cancer is Papillary Thyroid Carcinoma (PTC). This finding is in line with the results of other studies conducted around the world. Additionally, our study has also indicated that the prevalence of Medullary Thyroid Carcinoma (MTC) cases is on the rise, as reported in some articles. However, the exact cause of this increase is still unknown. Our research revealed that the majority of thyroid cancers were in stage I at the time of surgery, suggesting that the widespread use of diagnostic and imaging techniques like ultrasound and FNA have enabled early detection of the disease. Our research revealed that, on average, tumors in the population of thyroid cancer patients studied ranged from 2 to 4 cm in size, with the most frequent size being between 2 and 4 cm for all types of thyroid cancer. Notably, the most frequent size for papillary thyroid cancer was between 1 and 2 cm. The average size of tumors was most frequently found to be smaller than 1 cm and between 1 to 2 cm. This is largely attributed to the increasing prevalence of micro papillary carcinoma, a variant of PTC, as reported in numerous articles and studies. Our research has indicated that distant metastasis is less frequent in papillary types of thyroid cancer than in anaplastic and medullary types. Moreover, the lung is the most common site of distant metastasis in thyroid cancer. Additionally, our findings suggest that male patients are more likely to develop aggressive forms of thyroid cancer than female patients.
Acknowledgments
We would like to express our sincere gratitude to the dedicated members of Iman Khomeini Hospital of Sari for their invaluable support and contributions to the completion of this article. Their guidance and assistance have been instrumental in shaping the content and enhancing the quality of our work.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper. We affirm that we have disclosed any financial or personal connections that could be perceived as influencing the research presented in this article. This declaration includes, but is not limited to, employment, consultancies, honoraria, stock ownership, or any other financial interests.
References
- Bikas, A.; Burman, K.D. Epidemiology of thyroid cancer. The Thyroid and Its Diseases: A Comprehensive Guide for the Clinician 2019, 541–547.
- Xue, L.; Gong, Z.; Vlantis, A.C.; Chan, J.Y.; Meehan, K.; van Hasselt, C.A.; et al. Autophagy regulates anti-angiogenic property of lenvatinib in thyroid cancer. American journal of cancer research 2023, 13, 1457–1470. [Google Scholar] [PubMed]
- Boukheris, H.; Bettayeb, A.; Anderson, L.A.; Achour, Z.; Benbachir, F.Z.; Attar, S.; et al. Changes in the demographic and clinicopathological characteristics of thyroid cancer: a population-based investigation in Algeria, 1993-2013. Journal of cancer epidemiology 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Rendl, G.; Rodrigues, M.; Schweighofer-Zwink, G.; Hutter, J.; Hittmair, A.; Zellinger, B.; et al. Clinicopathological characteristics of thyroid cancer in the federal state of Salzburg. Wiener klinische Wochenschrift 2017, 129, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Chmielik, E.; Rusinek, D.; Oczko-Wojciechowska, M.; Jarzab, M.; Krajewska, J.; Czarniecka, A.; et al. Heterogeneity of Thyroid Cancer. Pathobiology: journal of immunopathology, molecular and cellular biology 2018, 85, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. The Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef] [PubMed]
- Loscalzo, J.; Fauci, A.S.; Kasper, D.L.; Hauser, S.; Longo, D.; Jameson, J.L. Harrison's Principles of Internal Medicine, (Vol. 1 & Vol. 2): McGraw Hill Professional; 2022.
- Abdul-Sater, Z.; Mukherji, D.; Adib, S.M.; Shamseddine, A.; Abu-Sitta, G.; Fadhil, I.; et al. Cancer registration in the Middle East, North Africa, and Turkey (MENAT) region: A tale of conflict, challenges, and opportunities. Frontiers in Oncology 2022, 12, 1050168. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.Y.; Choi, H.S.; Park, Y.J.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; et al. Changes in the clinicopathological characteristics and outcomes of thyroid cancer in Korea over the past four decades. Thyroid: official journal of the American Thyroid Association 2013, 23, 797–804. [Google Scholar] [CrossRef]
- Bukhari, U.; Sadiq, S.; Memon, J.; Baig, F. Thyroid carcinoma in Pakistan: a retrospective review of 998 cases from an academic referral center. Hematology/Oncology and Stem Cell Therapy 2009, 2, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA otolaryngology–head & neck surgery 2014, 140, 317–322. [Google Scholar]
- Du, L.; Wang, Y.; Sun, X.; Li, H.; Geng, X.; Ge, M.; et al. Thyroid cancer: trends in incidence, mortality and clinical-pathological patterns in Zhejiang Province, Southeast China. BMC cancer 2018, 18, 1–9. [Google Scholar] [CrossRef]
- Shobab, L.; Burman, K.D.; Wartofsky, L. Sex differences in differentiated thyroid cancer. Thyroid: official journal of the American Thyroid Association 2022, 32, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; de Vathaire, F.; Boutron-Ruault, M.-C.; Journy, N. Thyroid dysfunction and cancer incidence: a systematic review and meta-analysis. Endocrine-Related Cancer 2020, 27, 245–259. [Google Scholar]
- Moeller, L.C.; Führer, D. Thyroid hormone, thyroid hormone receptors, and cancer: a clinical perspective. Endocr Relat Cancer 2013, 20, R19–R29. [Google Scholar] [CrossRef] [PubMed]
- Laurberg, P.; Knudsen, N.; Andersen, S.; Carlé, A.; Pedersen, I.B.; Karmisholt, J. Thyroid function and obesity. European thyroid journal 2012, 1, 159–167. [Google Scholar] [CrossRef]
- Brandt, F.; Thvilum, M.; Almind, D.; Christensen, K.; Green, A.; Hegedüs, L.; et al. Morbidity before and after the diagnosis of hyperthyroidism: a nationwide register-based study. PloS one 2013, 8, e66711. [Google Scholar] [CrossRef]
- Jonklaas, J.; Nsouli-Maktabi, H.; Soldin, S.J. Endogenous thyrotropin and triiodothyronine concentrations in individuals with thyroid cancer. Thyroid: official journal of the American Thyroid Association 2008, 18, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Moazezi, Z.; Mahmoudi, M.; Yahyahpour, Y.; Alaleh, A. Risk factors of thyroid cancer in Babol, Northern Iran. Caspian Journal of Internal Medicine 2011, 2, 171. [Google Scholar] [PubMed]
- Dolidze, D.D.; Shabunin, A.V.; Mumladze, R.B.; Vardanyan, A.V.; Covantsev, S.D.; Shulutko, A.M.; et al. A narrative review of preventive central lymph node dissection in patients with papillary thyroid cancer-a necessity or an excess. Frontiers in Oncology 2022, 12, 906695. [Google Scholar] [CrossRef]
- Larijani, B.; Aghakhani, S.; Khajeh-Dini, H.; Baradar-Jalili, R. Clinico-pathological features of thyroid cancer as observed in five referral hospitals in Iran. Acta Oncologica 2003, 42, 334–337. [Google Scholar] [CrossRef]
- Capezzone, M.; Tosti Balducci, M.; Morabito, E.M.; Durante, C.; Piacentini, P.; Torregrossa, L. ; et al. High incidence of thyroid Cancer in southern Tuscany (Grosseto Province, Italy): potential role of environmental heavy metal pollution. Biomedicines 2023, 11, 298. [Google Scholar] [CrossRef]
- Jayarajah, U.; Fernando, A.; Prabashani, S.; Fernando, E.A.; Seneviratne, S.A. Incidence and histological patterns of thyroid cancer in Sri Lanka 2001-2010: an analysis of national cancer registry data. BMC cancer 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hadi, A.S.; Hamid, G.A. Diagnosis and Treatment of Patients with Thyroid Cancer in Yemen during the National war 2017-2021.
- Flemban, A.F.; Kabrah, S.; Alahmadi, H.; Alqurashi, R.K.; Turaes, A.S.; Almaghrabi, R.; et al. Patterns of Thyroid Cancer Mortality and Incidence in Saudi Arabia: A 30-Year Study. Diagnostics 2022, 12, 2716. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA: a cancer journal for clinicians 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Sosa, J.A. The changing incidence of thyroid cancer. Nature Reviews Endocrinology 2016, 12, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Machens, A.; Lorenz, K.; Weber, F.; Dralle, H. Risk patterns of distant metastases in follicular, papillary and medullary thyroid cancer. Hormone and Metabolic Research 2022, 54, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Sugitani, I.; Fujimoto, Y.; Yamamoto, N. Papillary thyroid carcinoma with distant metastases: survival predictors and the importance of local control. Surgery 2008, 143, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, D.; Levy, S.; Tsvetov, G.; Gorshtein, A.; Slutzky-Shraga, I.; Akirov, A.; et al. Long-term outcomes and prognostic factors in patients with differentiated thyroid cancer and distant metastases. Endocrine Practice 2017, 23, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-S.; Lee, J.S.; Yun, H.J.; Chang, H.; Kim, S.M.; Lee, Y.S.; et al. Prognosis of Anaplastic Thyroid Cancer with Distant Metastasis. Cancers 2022, 14, 5784. [Google Scholar] [CrossRef]
- Sugino, K.; Ito, K.; Nagahama, M.; Kitagawa, W.; Shibuya, H.; Ohkuwa, K.; et al. Prognosis and prognostic factors for distant metastases and tumor mortality in follicular thyroid carcinoma. Thyroid: official journal of the American Thyroid Association 2011, 21, 751–757. [Google Scholar] [CrossRef]
- Qari, F.A. Pattern of thyroid malignancy at a University Hospital in Western Saudi Arabia. Saudi med J 2004, 25, 866–870. [Google Scholar]
- Aziz, A.; Khan, S.A.; Suchal, Z.A.; Islam, N. Clinicopathological Characteristics and Treatment Outcome of Patients with Metastatic Differentiated Thyroid Cancer. Indian journal of endocrinology and metabolism 2022, 26, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Williams, V.L.; Hallanger Johnson, J.; Valderrabano, P. Thyroid cancer incidence trends in the United States: association with changes in professional guideline recommendations. Thyroid: official journal of the American Thyroid Association 2020, 30, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, M.; Saeidi, M.; Zarei, A.; Hasani, M. Investigating the demographic characteristics and pathological manifestations of thyroid Cancer during the last two decades (1997–2017) in patients referred to Baqiyatallah hospital, Tehran, Iran. Journal of Diabetes & Metabolic Disorders 2020, 19, 1165–1172. [Google Scholar]
- Kent, W.D.; Hall, S.F.; Isotalo, P.A.; Houlden, R.L.; George, R.L.; Groome, P.A. Increased incidence of differentiated thyroid carcinoma and detection of subclinical disease. Cmaj 2007, 177, 1357–1361. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: the next generation. cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Nikiforov, Y.E.; Seethala, R.R.; Tallini, G.; Baloch, Z.W.; Basolo, F.; Thompson, L.D.; et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment of indolent tumors. JAMA oncology 2016, 2, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M., Jacob, J., Eds. Invasion in thyroid cancer: controversies and best practices. Seminars in Diagnostic Pathology; 2020: Elsevier.
- Samargandy, S.; Qari, R.; Aljadani, A.; Assaqaf Sr, D.; Etaiwi, A.; Alghamdi, D.; et al. Clinicopathological characteristics of thyroid cancer in a Saudi academic hospital. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Izadi, B.; Jalilian, S.; Ramezani, M.; Sadeghi, M.; Khazaei, S. A study of clinicopathologic features of thyroid cancer in Western Iran: A 9-year experience. Clinical cancer Investigation journal 2019, 8. [Google Scholar]
Figure 1.
Frequency of Thyroid Cancer's Variants.
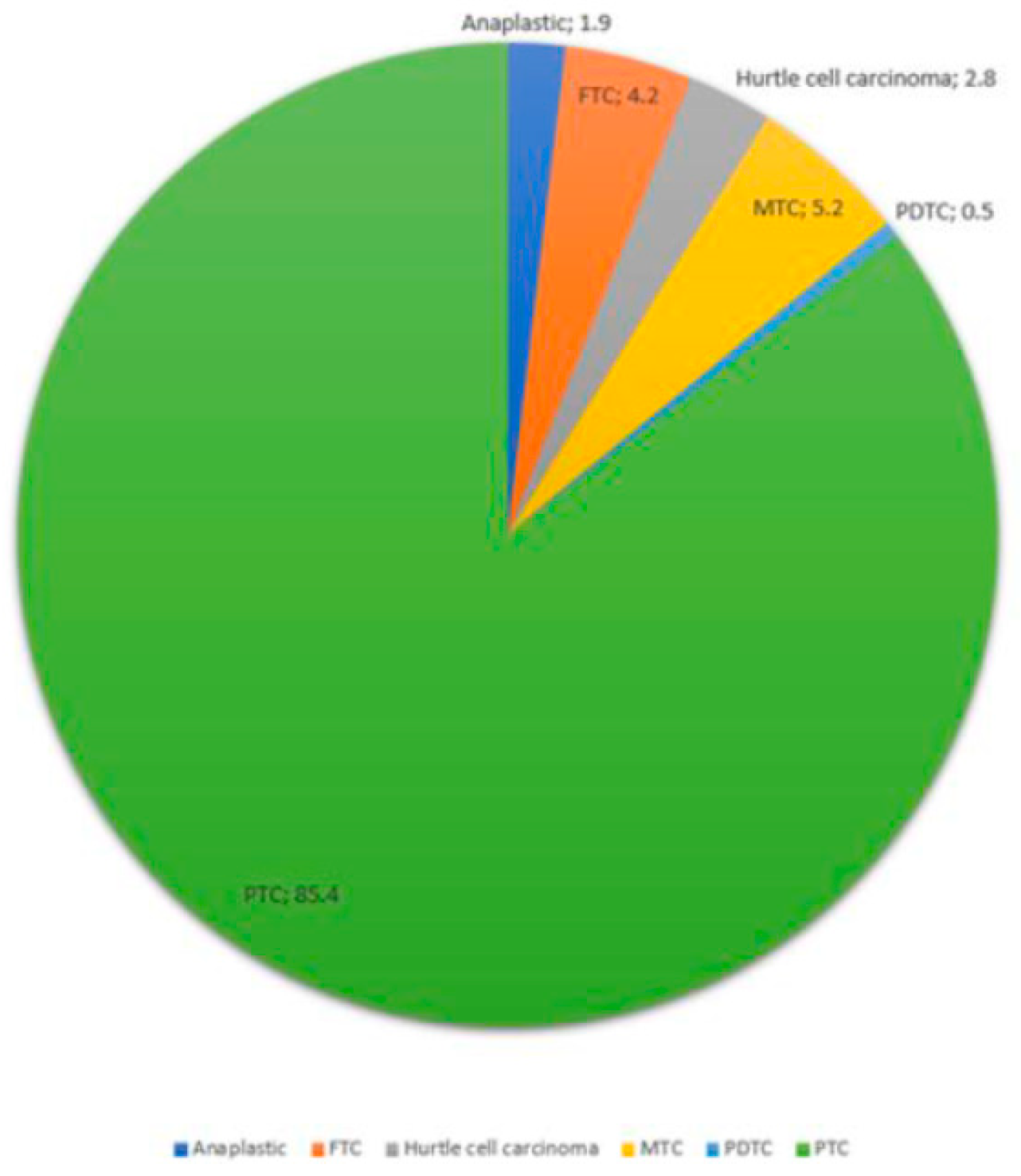
Figure 2.
Frequency of Tumor Size Range in Thyroid Cancer patients in studied population.
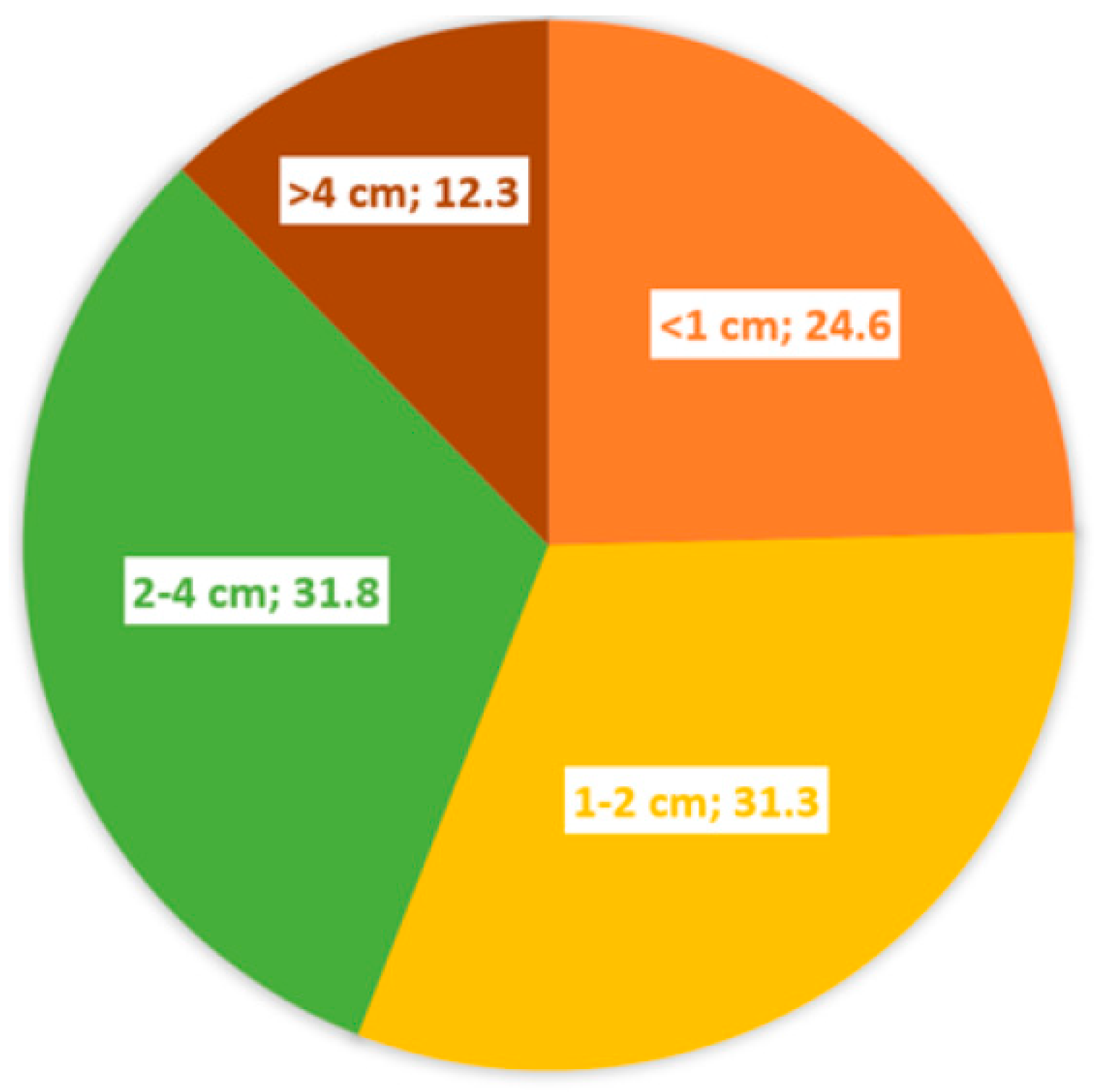
Figure 3.
Age groups frequency of Thyroid Cancer patients in studied population.
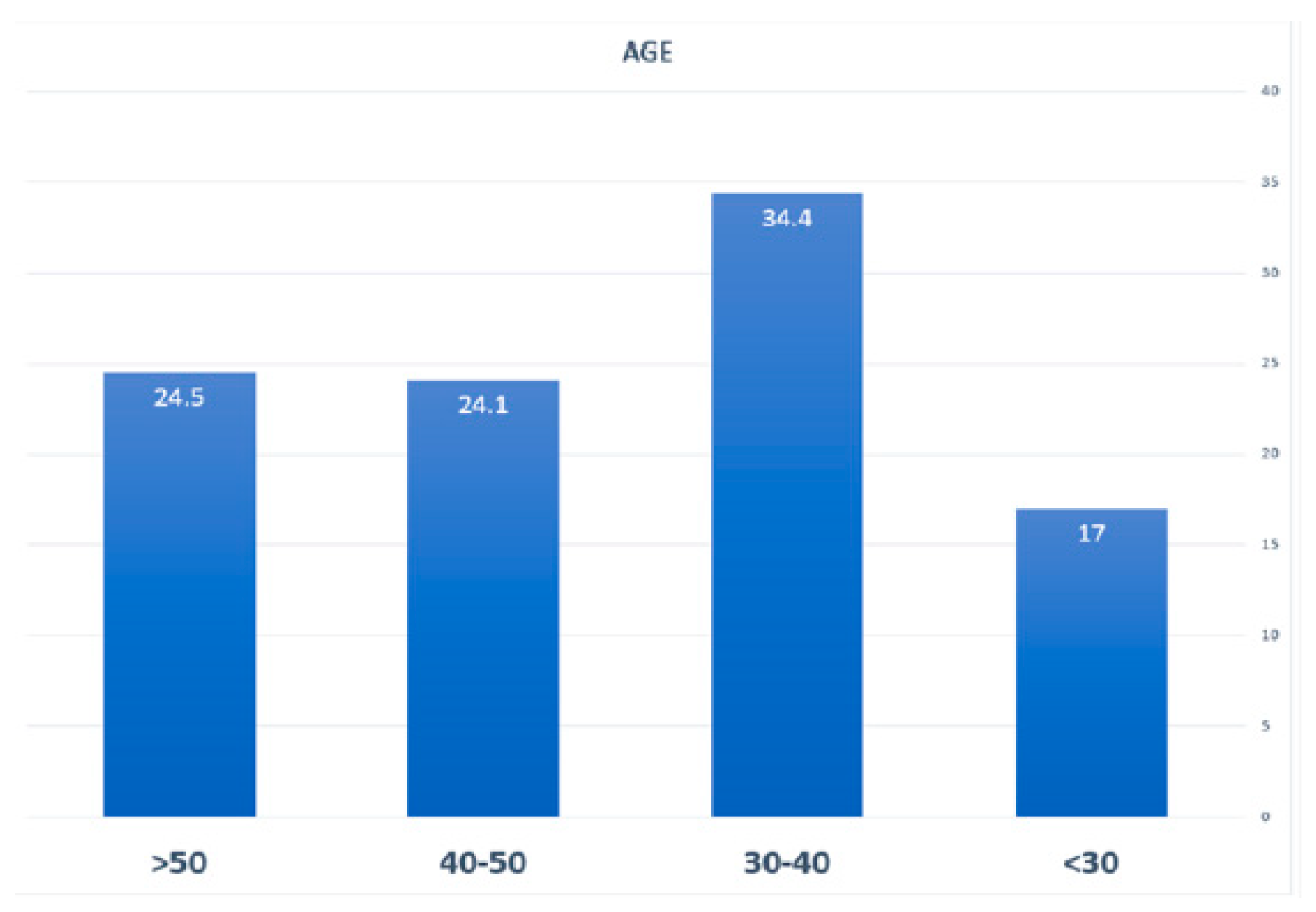
Figure 4.
Frequency of thyroid cancer stages in studied patients.

| Variables | total | Frequency (%) | |
|---|---|---|---|
| n =212 | |||
| Gender | male | 20 | %9.4 |
| female | 192 | %90.6 | |
| Pathology | PTC | 181 | %85.4 |
| FTC | 9 | %4.2 | |
| MTC | 11 | %5.2 | |
| Anaplastic | 4 | %1.9 | |
| Hurtle cell carcinoma | 6 | %2.8 | |
| PDTC | 1 | %0.5 | |
| Age Group | < 30 years | 36 | %17 |
| 30-40 | 73 | %34.4 | |
| 50-40 | 51 | %24.1 | |
| >50 | 52 | %24.5 | |
| Tumor size | <1cm | 52 | %24.6 |
| 1-2 cm | 66 | %31.3 | |
| 2-4 cm | 67 | %31.8 | |
| >4 cm | 27 | %12.3 | |
| Lymph node involvement | No | 147 | %69.3 |
| 1-3 Lymph node | 28 | %13.2 | |
| >3 Lymph node | 37 | %17.5 | |
| Lymph node involvement | Yes | 70 | %33 |
| No | 142 | %67 | |
| Distance metastases | No | 196 | %92.4 |
| Yes | 16 | %7.6 | |
| Capsule involvement | No | 131 | %61.8 |
| Yes | 81 | %38.2 | |
| Family history of thyroid cancer | No | 191 | %90.1 |
| Yes | 81 | %9.9 | |
| Stage | I | 181 | %85.4 |
| II | 14 | %6.6 | |
| III | 6 | %2.8 | |
| IV | 11 | %5.2 | |
| T | T1a | 58 | %27.4 |
| T1b | 58 | %27.4 | |
| T2 | 64 | %30.2 | |
| T3a | 16 | %7.5 | |
| T3b | 11 | %5.2 | |
| T4a | 2 | %0.9 | |
| T4b | 3 | %1.4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



