
Submitted:
15 January 2024
Posted:
16 January 2024
You are already at the latest version
Abstract
Emotional intelligence can contribute to quality of life and as a health predictor. The aim of this study is to analyze emotional intelligence, quality of life and the correlation factors associated in patients undergoing chronic hemodialysis. A quantitative, observational, cross-sectional design was performed, and one hundred and thirty-eight multi-centers hemodialysis patients were recruited. A battery of questionnaires, including Trait Meta-Mood Scale (TMMS-24), Kidney Disease Quality of Life-Short Form (KDQOL-SF), and an ad-hoc sociodemographic questionnaire, were answered. Sex differences existed when assessing the three dimensions of emotional intelligence: ranked by order, the highest scores in males were in clarity, repair, and attention. However, in females were in repair, clarity, and attention. Males had higher scores than females in emotional role (p=0.045). Younger participants had better scores in all physical functions (p=0.001) and vitality (p=0.038) than older. Moreover, those who had a higher level of education presented better physical function (p=0.027) and higher scores in emotional wellbeing (p=0.036). Finally, in females, emotional attention (p=0.046) and repair (p<0.001) were strongly associated with general health perception. The assessment of emotional intelligence considering sex differences in patients undergoing chronic hemodialysis can be an indicator of quality of life including the use in health interventions.
Keywords:
Chronic Kidney Disease
; Hemodialysis
; Emotional Intelligence
; Quality of life
; Sex differences
; Nursing
1. Introduction
1.1. Chronic kidney disease and its impact
Chronic Kidney Disease (CKD) is a serious illness that is not curable and has been recognized as a leading public health problem worldwide. Its estimated prevalence is between 11.7% and 15.1% in the world population [1,2]. In addition, the number of individuals suffering from it is growing globally and it is expected that the number of patients who will require renal replacement therapy will increase in the coming years [3,4,5,6]. Updated data show that the global all-age mortality rate from CKD increased 41.5% between 1990 and 2017 [7].
The most widely-used therapy around the world is hemodialysis (HD) [8] that entails an absolute life dependency on a blood filtering machine. The patient undergoing HD therapy usually suffers from stressful and threatening situations throughout his or her life, which often results in disability, and physical and psychological suffering [9]. Moreover, the adverse events in patients who suffer from advanced chronic kidney disease are multiple, such as pain [10], and can inform patient counselling and medical decision-making [11]. Mortality in renal replacement therapy has decreased due to technological advances. However, the morbidity risk for these chronic kidney patients continues to increase due to the existence of mental and physical negative impacts that affect their health-related quality of life (QL) [12].
1.2. Emotional intelligence
Research into the regulation and management of emotions and its potential implications for quality of life, has aroused great interest in all areas [13,14]. Emotional Intelligence (EI) is composed of three dimensions and can be defined as the ability to attend (emotional attention), understand (emotional clarity), and modify (mood repair) emotional states [15], as well as the ability to regulate emotions to promote emotional and intellectual growth [16]. However, a high level of emotional attention interferes negatively with the positive effect of mood repair and personal growth if it is not complemented by a clear understanding of emotions [17].
Many studies show the role of emotional intelligence as a predictor of positive emotional states as well as well-being [18,19], and it has an effect on the quality of life of elderly people with chronic disease [20]. When measured as a trait, emotional intelligence is more strongly associated with health than when measured as an ability and, therefore, it can be a possible health predictor [21].
Sex-related differences in emotion management is a reality given that sex differences in brain structure as well as psychological functioning do exist. Although females are better at recognizing emotions and expressing themselves more easily, males show greater responses to threatening cues and this may reflect different behavioural response tendencies between males and females [22]. In order to increase understanding of why males and females differ behaviourally, and why many psychiatric diagnoses show unequal sex ratios, brain studies have been developed and results show that sex and gender identity-related differences in humans effects from experience, rather than causing variability in gender identity [23]. In a study where adult brains were analyzed, it was found that most brains did not show a consistent sex-typical pattern in all regions [24]. Similarly, the same study found that brain connectivity was never consistently male-typical or female-typical in any of the brains. This interferes with the challenge of the interpretation of the outcomes.
Emotional intelligence and quality of life studies in patients undergoing chronic hemodialysis therapy are scarce. However, in 2016 a positive correlation between both variables was proven. Two years later, a positive effect of an educational program in emotional intelligence on quality of life was observed in HD patients [25,26].
Considering the risks and consequences of emotional disorders among hemodialysis patients, the literature has highlighted the role of emotional intelligence as an adequate tool to face stressful situations and achieve emotional well-being [27].
1.3. Quality of life in patients undergoing chronic hemodialysis therapy
Health-related quality of life is a concept that is closely influenced by an individual’s perception of their physical and psychological state, level of independence, social relations, and their relationship with the environment [28].
Complications stemming from hemodialysis therapy, and which may interfere in different areas of quality of life, are physical (loss of normal body function, sleep disorders, hemodialysis complications); psychological (pain, anxiety, depression, fatigue, self-image disturbance, decreased quality of life); and social (role change, perception of the disease, time in dialysis unit) [29,30,31].
Due to an increase in survival rates for patients with CKD, the outcome measures for dialysis therapy, such as quality of life, have become increasingly important not only as a quality assessment for health professionals, but also for patient survival [32,33]. Studies show how low quality of life leads to higher mortality and a greater number of hospitalizations [12]. Moreover, there are some differences in dialysis modality in relation to quality of life outcomes [34].
The quality of life of hemodialysis patients is affected by emotion-focused coping strategies and cognitive processing, which can both be affected by socio-environmental and situational factors related to emotional intelligence [27].
The aim of this study is to look into the factors that are related to emotional intelligence and quality of life of patients undergoing chronic hemodialysis therapy by sex. The authors hypothesize that emotional intelligence could be a modulating factor of quality of life in people undergoing chronic hemodialysis therapy according to sex differences, so the findings of this study are expected to draw more attention to the psychological distress of patients undergoing chronic HD therapy.
2. Materials and Methods
2.1. Aims
Firstly, we have analyzed emotional intelligence skills in relation to sex and age differences in patients undergoing chronic HD therapy. Secondly, we have studied quality of life of HD patients according to sex. Finally, we have described the correlation factors associated with emotional intelligence.
2.2. Methods
2.3. Study design
A descriptive, observational, cross-sectional, analytical, multicentre study was conducted [35] to determine the factors that affect quality of life in chronic HD patients as well as differences by age and sex.
2.4. Participants
The study was directed at all 297 patients included in the chronic HD program of a region of Catalonia (Spain) in a convenience sample of four HD centres which presented similar characteristics. The inclusion criteria required patients to be older than 18 years of age, attend one of the four different HD units, and voluntarily agree to participate. Patients who suffered from mental disorders or a clinical condition at the time of data collection and those with language barriers were excluded. After applying the above criteria, a total of 138 patients were eligible to answer the self-assessment questionnaires (46.5%).
2.5. Data Collection
Initially, permission to contact the patients was requested from the clinics or hospital direction as well as from the medical and nursing supervision members at the hemodialysis units. We informed not only the patients but also the professional members of the hemodialysis units about the purpose of the study, including confidentiality and voluntary participation. Data collection was undertaken during the time of HD therapy and paper format questionnaires were handed out to be answered in situ. Some patients requested to answer them at home due to physical difficulties, such as needle insertions or not carrying reading glasses at the time of HD therapy, and these questionnaires were returned on the next session.
2.6. Variables
The independent variables used to explain variations in quality of life were sociodemographic variables (sex, age, living situation and level of education). Emotional Intelligence was a modulating variable for quality of life. The dependent variables were those related to quality of life such as physical and mental dimensions.
2.7. Instruments
The participation ad-hoc questionnaire designed for sociodemographic data collection included the following variables: age and sex; level of studies (primary, secondary and university); living situation (alone, nursing homes, lives with family); employment status (employed, unemployed, retired, other situation); and monthly income (above or below €645, based on the Spanish minimum standard salary in 2016).
We assessed Emotional Intelligence with the Trait Meta-Mood Scale (TMMS-24) [15], Spanish translation and validation [36]. It is a self-report measure designed to assess individual’s beliefs about their own emotional abilities. This scale addresses three key aspects of perceived emotional intelligence: Attention conveys to what extent individuals tend to observe and think about their feelings and moods; Clarity evaluates the understanding of one’s emotional states, and Repair refers to the individual’s beliefs about their ability to regulate their feelings. Specifically, the TMMS-24 is a 24-item Likert-type scale on which participants are required to rate the extent to which they agree with each item on a 5-point scale with anchors of 1=strongly disagree and 5= strongly agree. The scale appeared to have adequate psychometric characteristics with high reliability (Cronbach Alpha: perception α=0.90; clarity, α=0.90, repair α=0.86) (test-retest reliability: perception=0.60, clarity=0.70, repair=0.83) [37]. The score on the different factors was obtained from the sum of the set of items on each scale. Items 1-8, 9-16, and 17-24 evaluated emotional attention, clarity, and repair correlatively. Based on these scores, participants were classified as: “need to improve”, “adequate” or “excellent” in emotional clarity/repair and “need to improve”, “adequate” and “too much” in emotional attention. This classification was made using different cut-off points for males and females as, according to the authors, there are sex differences in the handling of emotions.
Quality of life was measured with the Kidney Disease Quality of Life-Short Form questionnaire (KDQOL-SF) [38]. It consists of the generic 36-Item Short Form Health Survey (SF-36) [39] as well as 11 multi-item scales focusing on quality of life issues specific to patients with kidney disease. The generic survey consists of 8 scales that can provide two summative scores: physical and mental summative index. The internal consistency of the generic part is strong, alpha values range from .78 to .92 [40]. The questionnaire is completed with 44 specific items of kidney disease distributed on 11 scales. For the present research, one item was removed because it only referred to patients undergoing peritoneal dialysis. The specific part of the questionnaire had a high internal consistency with a Cronbach’s alpha α = .80 (with 2 exceptions α = .68 in cognitive function and α = 0.61 as social interaction). The average values of the objective scales oscillated between 25.6 (DT = 37.82) in work and 79.11 (DT = 19.75) in cognitive function in the percentage of possible total score (0 - 100). This instrument is the most used internationally because it assesses patients with kidney failure in a holistic way [41].
2.8. Statistical analysis
Statistical analysis was performed using Windows SPSS software, version 25.0 for IBM. Continuous variables were described as the mean and standard deviation or the median and interquartile range, according to their probability distribution. Continuous variables were compared with the Student’s t-test or with a one-way ANOVA and the categorical variables with the Chi-square test. A linear regression model was carried out to study the factors related to quality of life. The variables accepted for the lineal regression analyzes were the ones associated to emotional intelligence in the bivariant analysis. In all cases, a p-value < 0.05 was considered statistically significant.
2.9. Ethical considerations
This research study has complied with the fundamental ethical principles that govern the conduct of research. The anonymity of the participants was guaranteed at all times, and the informed consent form was signed by all participants prior to the start of data collection. The study was approved by the Ethics Committees of Clinical Research of the area of influence (acceptance number: 2014.016 date: 24/02/2014 act #3).
3. Results
3.1. Study sample characteristics
Participant demographics showed that there was a total of 138 participants of whom 89 were men and 48 were females (64.5%-35.5%). In relation to level of education, 76.8% of all participants had primary studies and only 5.1% university level. Nine out of ten participants lived with family and had an employment status of retirement, in greater proportion in males than in females (p=0.009). In terms of household income, we can underline that more than two thirds of males had a higher income than females (p=0.029)
In relation to the participants’ clinical characteristics, the mean hemodialysis time was 54.4 months (4.5 years) and a median of 36 [IQR 12-72] in males. In females, the mean hemodialysis time was 56.5 months (4.7 years) and a median of 42 [IQR 23-72] (p= 0.415). The hours of hemodialysis per session in males and females were 3.9 and 3.8, respectively (p=0.004). The number of hospitalizations over the last 3 months was 0.16 in males and 0.08 in females (p= 0.104).
3.2. Emotional Intelligence in chronic hemodialysis patients
Table 1 shows the descriptive values of the three dimensions of Emotional Intelligence, split by sex, because males and females had different reference values. The highest scores in males were in Clarity followed by Repair and finally in the Attention dimension. In females, the highest scores were firstly in Repair, followed by Clarity and finally in Attention.
Figure 1 and Figure 2 show the classification of emotional intelligence in males and females. As we can observe in Figure 1, the largest proportion of male participants scoring “Excellent” were in the Clarity dimension. Of those scoring “Adequate”, the largest percentage were in the Repair dimension. In females (Figure 2), however, the largest proportion of participants scoring “Excellent” were in the Repair dimension followed by Clarity, and a high proportion in Attention were in “Need to improve” (67.3).
When comparing emotional intelligence according to age groups in males, we observed that Attention, mean=24.1 (7.5), and Clarity, mean= (6.8), were higher in participants older than 64 years old. On the other hand, in terms of Repair, mean=28.3 (8.8), the highest scores corresponded to 46 to 65 year-old participants. However, there was no significant statistical differences between males according to age groups.
In females, the 25 to 45-year-old age group presented the highest scores in Attention, mean=29 (9.3), and Clarity, mean=31.3 (74). In the Repair dimension, the groups between 25 to 45 and 46 to 65 years of age had similar scores of 30.3 (7.8) and 30.6 (6.4), respectively, without significant statistical differences between females according to age groups.
3.3. Quality of life in chronic hemodialysis patients
With a general overview of the results obtained regarding the physical dimensions of quality of life, we can note that scores were low. The four physical dimensions of quality of life are shown in Table 2. There were significative differences in age groups where younger participants had a better score in all the physical functions than older participants (p=0.001). Moreover, those who had a higher level of education presented better physical function (p=0.027).
In relation to the mental dimensions of quality of life (Table 3), males presented higher scores than females in the emotional role (p=0.045). Younger participants had higher scores in vitality (p=0.038). Finally, participants who had university studies presented higher scores in emotional wellbeing (p=0.036).
In the linear regression model used to study the variables associated with the perception of general health, no sociodemographic variables were observed or related to the three dimensions of emotional intelligence in males. However, Attention (p=0.046) and Repair (p<0.01) were found to be strongly associated with perception of general health in female (Table 4 and Table 5).
4. Discussion
This study analysed emotional intelligence skills and quality of life in a sample of 138 patients undergoing chronic hemodialysis therapy. In relation to emotional intelligence, we could observe major differences in the dimensions of emotional attention and repair. More females than males (+33.3%) had low attention. However, 27.2% more males had adequate attention compared to females and finally 5.3% more males paid too much attention to emotions compared to females. Results showed that 9% more females had excellent emotional repair compared to males. These contradicting results could be explained by the characteristics and the different emotional stages that chronic hemodialysis therapy represents. This contradicts other results reporting higher emotional intelligence skills in females in a healthy population [42]. These differing patterns constitute an indication of a great sociodemographic diversity, as well as the progesterone phase of their menstrual cycle in young females could perform better on EI [43] and we did not control this potential confounder. Pardeler et al., 2018 exposed that cognitive abilities need to be considered when assessing emotional intelligence in healthy individuals as sex differences are present [44]. When analyzing EI as an ability-base approach rather than analyzing trait emotional intelligence, also appears that females have higher scores compared to males [45].
Across the majority of emotion-related outcomes, trait emotional intelligence tends to be a stronger predictor and, consequently, O’Connor et al (2019) suggest that new users of emotional intelligence should consider using a trait-based measure before assessing alternatives (14). When using self-report measures, such as TMMS-24, sex differences in results are shown. Thus, males perceive themselves as more emotionally intelligent than females, so these measures demonstrate levels of emotional attention that are too high [46].
We need to consider that negative emotions can have an impact and lead to higher emotional attention and clarity. Therefore, they enhance a state of anxiety, which is why it is relevant to achieve a balanced level of emotional intelligence in order not to suffer other disorders. Paying excessive attention to emotions can have detrimental effects, reducing the ability to regulate emotions [47]. Multiple aspects of intelligence need to be controlled when assessing emotional intelligence for the prediction of health outcomes [45].
When studying emotional intelligence by age, we can mention that our results were similar to the literature [48] as the ability to repair increased with age. These results could be related to life experience as well as better emotional control.
The existence of a positive correlation between emotional intelligence and quality of life in chronic hemodialysis patients was shown in 2016 using a different instrument from TTMS-24 (25). Other studies showed no sex difference in terms of quality of life and emotional intelligence, marital status, and educational levels [49].
As for emotional intelligence training, studies have shown great results in all dimensions. With a comparative study, there were significant correlations in the intervention group, obtaining statistically significant overall results: 42.00 + 10.22 before the intervention and 58.24 + 8.66 post intervention. Emotional Intelligence training has shown excellent results towards improving quality of life aspects, including reducing anxiety scores in HD patients [26,50]. Similar results exist in breast cancer patients where effective interventions such as physical activity and psychosocial interventions proved to have worthy outcomes [51].
Our results regarding quality of life by sex and age differ a little from others in the literature, as a study conducted in Jordan on participants undergoing hemodialysis therapy showed that males and younger participants ones had a higher mental quality of life than female participants in general [52]. The systematic review by Yapa [53], where quality of life and symptoms experienced by patients who have CKD and are not on dialysis were analyzed, concluded that quality of life decreased when symptoms increased. Thus, evidence on how and which symptoms change over time was inconclusive. One possibility could be due to gender-related biological factors as well as different lifestyles, socialization, and culture norms [23].
The study of quality of life in patients who suffer other chronic conditions is wide and results are similar. For example, Yalcin et al. (2008) demonstrated that higher emotional intelligence levels were related to a better quality of life and general well-being of people with diabetes [54]. Moreover, the way that females with breast cancer regulate their emotions influences their quality of life and enhances disease adaptation [55]. Emotional intelligence studies in patients who suffer from chronic obstructive pulmonary disease (COPD) showed an association with all domains of quality of life regardless of age [56]. This suggests that, since emotional intelligence is a trainable skill, there is an opportunity to convert this knowledge into management programs in order to improve the quality of life and well-being of such patients. In this sense, it has also been observed in the present study a strong association between general health and emotional intelligence of females. These sex differences could be explained by different responses in processing emotional signals [22] and the interrelation between cognitive abilities and the understanding of the emotions [42].
This research is not without limitations. Firstly, the use of self-report measures is prone to recall bias. Secondly the cross-sectional design has not allowed causal associations, or the direction of the associations to be studied. Thirdly, since most questionnaires were completed during HD therapy, the presence of medical staff and other patients may have influenced the objectivity of the responses and threatened data validity. Finally, we used the term sex, which often refers to biological phenotype. However, there are studies that indicate that the differences are related in the experience itself rather than in gender identity [23]. We believe that in future research on Emotional Intelligence, sex differences and gender identity should be considered separately.
This study has strengthened existing evidence that chronic HD therapy can have detrimental mental health effects in CKD patients. It has been proven that these negative health effects have an impact on patients’ wellbeing and quality of life and require effective measures in nursing practice to be developed and implemented.
A holistic view of CKD patients should be adopted by nephrology nurses in order to consider and care for different aspects of their suffering, including emotion management. Emotional intelligence is a promising protective factor for biological and psychological variables in populations who suffer a chronic condition [57]. Likewise, renal association guidelines currently recommend health-related quality of life to be monitored in patients undergoing renal replacement therapy [58].
We suggest that clinical practitioners treating chronic hemodialysis patients should assess levels of emotional attention, especially in females. If instability is detected, a complete psycho-emotional intervention should be conducted. Nurses have the capacity to establish a helping relationship and have at their disposal key resources to do so, for example, empowering hemodialysis patients to enhance their coping strategies [59].
Finally, quality of life is one of the main concerns of policymakers and public health planners in the community as well as an indicator of quality care. We aim to contribute to this knowledge with the present research.
5. Conclusions
Assessment of emotional intelligence in patients undergoing chronic hemodialysis therapy can be an indicator of clinical outcomes and improve health interventions as well as being a tool for evaluating the therapy carried out. Improving quality of life and subsequently enhancing emotional intelligence may prevent irreversible complications in patients undergoing chronic HD therapy.
Nurse managers need to guide nurses in applying emotional intelligence skills in daily practice with the aim of providing holistic patient care, obtaining positive outcomes of trait emotional intelligence and preventing psychological disorders.
Author Contributions
AMP led the conception, design, database search, data collection of the study. RSS did the statistical analysis and interpreted the data. DJC, MSS, MBB, SMJ contributed to the writing of the manuscript in collaboration with AMP. The authors read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the fundamental bioethical principals and the protocol was approved by the Ethics Committees of Clinical Research of the area of influence (acceptance number: 2014.016 date: 24/02/2014 act #3). The anonymity of the participants was guaranteed at all times, and the informed consent form was signed by all participants prior to the start of data collection.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that they have no conflict of interests.
List of Abbreviations
| HD | hemodialysis |
| TMMS-24 | Trait meta-mood scale |
| KDQOL-SF | Kidney disease quality of life-short form questionnaire |
| CDK | Chronic kidney disease |
| QL | Quality of life |
| EI | Emotional intelligence |
| SPSS | Statistical package for social sciences |
| IBM | International business machines corporation |
| IQR | Inter quartile rang |
| COPD | Chronic obstructive pulmonary disease |
References
- Lv, J.C.Z.L. Prevalence and Disease Burden of Chronic Kidney Disease. In Mechanisms and Therapies Advances in Experimental Medicine and Biology; Fibrosis, R., Liu, B.C., Eds.; Springer: Singapore, 2019; pp. 3–15. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global prevalence of chronic kidney disease–A systematic review and meta-analysis. PLoS One 2016, 11. [Google Scholar] [CrossRef]
- Eckardt, K.U.; Coresh, J.; Devuyst, O.; Johnson, R.J.; Köttgen, A.; Levey, A.S.; et al. Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 2013, 382, 158–169. [Google Scholar] [CrossRef]
- Thomas, B.; Wulf, S.; Bikbov, B.; Perico, N.; Cortinovis, M.; De Vaccaro, K.C.; et al. Maintenance dialysis throughout the world in years 1990 and 2010. J Am Soc Nephrol. 2015, 26, 2621–2633. [Google Scholar] [CrossRef]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; et al. Worldwide access to treatment for end-stage kidney disease: A systematic review. Lancet 2015, 385, 1975–1982. [Google Scholar] [CrossRef]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Lee, T.; Flythe, J.E.; Allon, M. Dialysis Care around the World: A Global Perspectives Series. Kidney360 2021, 2, 604–607. [Google Scholar] [CrossRef]
- Pabón-Varela, Y.; Paez-Hernandez, K.S.; Rodriguez-Daza, K.D.; Medina-Atencia, C.E.; López-Tavera, M.; Salcedo-Quintero, L.V. Calidad de vida del adulto con insuficiencia renal crónica, una mirada bibliográfica. Duazary 2015, 12, 157. Available online: https://revistas.unimagdalena.edu.co/index.php/duazary/article/view/1473/922 (accessed on 18 December 2020). [CrossRef]
- Fleishman, T.T.; Dreiher, J.; Shvartzman, P. Pain in Maintenance Hemodialysis Patients: A Multicenter Study. J Pain Symptom Manage 2018, 56, 178–184. [Google Scholar] [CrossRef]
- Grams, M.E.; Yang, W.; Rebholz, C.M.; Wang, X.; Porter, A.C.; Inker, L.A.; et al. Risks of Adverse Events in Advanced CKD: The Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis. 2017, 70, 337–346. [Google Scholar] [CrossRef]
- Perl, J.; Karaboyas, A.; Morgenstern, H.; Sen, A.; Rayner, H.C.; Vanholder, R.C.; et al. Association between changes in quality of life and mortality in hemodialysis patients: Results from the DOPPS. Nephrol Dial Transplant 2017, 32, 521–527. Available online: https://academic.oup.com/ndt/article/32/3/521/3060597 (accessed on 23 December 2020). [CrossRef]
- Fernández-Berrocal, P.; Extremera, N. Emotional intelligence: A theoretical and empirical review of its first 15 years of history. Psycothema 2006, 18, 7–12. [Google Scholar]
- O’Connor, P.J.; Hill, A.; Kaya, M.; Martin, B. The measurement of emotional intelligence: A critical review of the literature and recommendations for researchers and practitioners. Front Psychol. 2019, 10. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D.; Goldman, S.; Turvey, C.; Palfai, T. Emotional attention, clarity and repair: exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure, and Health; Pennebaker, J.W., Ed.; Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Mayer, J.; Salovey, P.; Caruso, D. Models of Emotional Intelligence; R. J. S. Cambridge University Press, 2000; pp. 396–420. [Google Scholar]
- Guil, R.; Ruiz-González, P.; Merchán-Clavellino, A.; Morales-Sánchez, L.; Zayas, A.; Gómez-Molinero, R. Breast Cancer and Resilience: The Controversial Role of Perceived Emotional Intelligence. Front Psychol. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Caruso, D.R.; Mayer, J.D.; Bryan, V.; Phillips, K.G.; Salovey, P. Measuring emotional and personal intelligence. In Positive Psychological Assessment: A Handbook of Models and Measures; Gallagher, M.W., Lopez, S.J., Eds.; American Psychological Association: Washington, DC, USA, 2019; pp. 233–245. [Google Scholar]
- Sarrionandia, A.; Mikolajczak, M. A meta-analysis of the possible behavioural and biological variables linking trait emotional intelligence to health. Heal Psychol Rev. 2020, 14, 220–244. [Google Scholar] [CrossRef]
- Moradi, F.; Tourani, S.; Ziapour, A.; Abbas, J.; hematti, M.; Moghadam, E.J.; et al. Emotional Intelligence and Quality of Life in Elderly Diabetic Patients. Int Q Community Health Educ. 2021, 42, 15–20. [Google Scholar] [CrossRef]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between Emotional Intelligence and health. Pers Individ Dif 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Kret, M.E.; De Gelder, B. A review on sex differences in processing emotional signals. Neuropsychologia 2012, 50, 1211–1221. [Google Scholar] [CrossRef]
- Hines, M. Neuroscience and sex/gender: Looking back and forward. J Neurosci. 2020, 40, 37–43. [Google Scholar] [CrossRef]
- Joel, D.; Berman, Z.; Tavor, I.; Wexler, N.; Gaber, O.; Stein, Y.; et al. Sex beyond the genitalia: The human brain mosaic. Proc Natl Acad Sci USA 2015, 112, 15468–15473. [Google Scholar] [CrossRef]
- Shahnavazi, Masoome, Zohreh Parsa Yekta FR and MSY. The Relationship between Emotional Intelligence and Quality of life among University Teachers. Int J Med Res Heal Sci. 2016, 5, 564–570. [Google Scholar]
- Shahnavazi, M.; Parsa-Yekta, Z.; Yekaninejad, M.S.; Amaniyan, S.; Griffiths, P.; Vaismoradi, M. The effect of the emotional intelligence education programme on quality of life in haemodialysis patients. Appl Nurs Res. 2018, 39, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Jesus, N.M.; Souza GF de Mendes-Rodrigues, C.; Almeida Neto OP de Rodrigues, D.D.M.; Cunha, C.M. Quality of life of individuals with chronic kidney disease on dialysis. J Bras Nefrol. 2019, 41, 364–374. [Google Scholar] [CrossRef]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- Jassal, S.V.; Karaboyas, A.; Comment, L.A.; Bieber, B.A.; Morgenstern, H.; Sen, A.; et al. Functional Dependence and Mortality in the International Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2016, 67, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Perales-Montilla, C.M.; Duschek, S.; Reyes-del Paso, G.A. Influencia de los factores emocionales sobre el informe de síntomas somáticos en pacientes en hemodiálisis crónica: relevancia de la ansiedad. Nefrologia 2013, 33, 816–825. [Google Scholar] [PubMed]
- Palmer, S.; Vecchio, M.; Craig, J.C.; Tonelli, M.; Johnson, D.W.; Nicolucci, A.; et al. Prevalence of depression in chronic kidney disease: Systematic review and meta-analysis of observational studies. Kidney Int 2013, 84, 179–191. [Google Scholar] [CrossRef]
- Cavanaugh, K.L. Patient Experience Assessment is a Requisite for Quality Evaluation: A Discussion of the In-Center Hemodialysis Consumer Assessment of Health Care Providers and Systems (ICH CAHPS) Survey. Semin Dial. 2016, 29, 135–143. [Google Scholar] [CrossRef]
- Kliger, A.S. Quality measures for dialysis: Time for a balanced scorecard. Clin J Am Soc Nephrol. 2016, 11, 363–368. [Google Scholar] [CrossRef]
- Chuasuwan, A.; Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Ingsathit, A.; et al. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual Life Outcomes 2020, 18, 1–11. [Google Scholar] [CrossRef]
- Watson, R. Quantitative research|Western Sydney University ResearchDirect. Nurs Stand 2015, 29, 44–48. Available online: https://researchdirect.westernsydney.edu.au/islandora/object/uws:34764 (accessed on 23 December 2020). [CrossRef] [PubMed]
- Fernández-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the Spanish modified version of the Traït Meta-Mood Scale. Psychol Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Angulo, R.; Albarracín, A.P. Validez y confiabilidad de la escala rasgo de metaconocimiento emocional (TMMS-24) en profesores universitarios. Rev Lebret 2018, 10, 61–72. [Google Scholar]
- Hays, R.D.; Kallich, J.D.; Mapes, D.L.; Coons, S.J.; WBC. Development of the kidney disease quality of life (KDQOL) instrument. Qual life Res. 1994, 3, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Prieto, L.A.J. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): un instrumento para la medida de los resultados clínicos [The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): an instrument for measuring clinical resu. Med Clin. 1995, 104, 771–776. [Google Scholar]
- Hays, R.D.; Kallich, J.D.; Mapes, D.L.; Coons, S.J.; Naseem, A.; Carter, W. Kidney Disease Quality of Life Short Forma (KDQOL-SFtm), version 1.3 ed; A Manual for Use and Scoring; 1997; pp. 1–43. Available online: https://www.rand.org/content/dam/rand/pubs/papers/2006/P7994.
- Pabón-Varela, Y.; Paez-Hernandez, K.S.; Rodriguez-Daza, C.K.D. Eustralia Medina-Atencia ML-T y LVS-Q. Adult’s life quality with chronic kidney disease, a bibliographic view. Rev Duazary. 2015, 12, 7. [Google Scholar]
- Joseph, D.L.; Newman, D.A. Emotional Intelligence: An Integrative Meta-Analysis and Cascading Model. J Appl Psychol. 2010, 95, 54–78. [Google Scholar] [CrossRef] [PubMed]
- Milivojevic, V.; Sinha, R.; Morgan, P.T.; Sofuoglu, M.; Helen, C. Fox. Effects of endogenous and exogenous progesterone on emotional intelligence in cocaine-dependent men and women who also abuse alcohol. Hum Psychopharmacol Clin Exp. 2014, 29, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Pardeller, S.; Frajo-apor, B.; Kemmler, G.; Hofer, A. Emotional Intelligence and cognitive abilities – associations and sex differences. Psychol Heal Med. 2018, 22, 1001–1010. [Google Scholar] [CrossRef]
- MacCann, C.; Joseph, D.L.; Newman, D.A.R.R. Emotional intelligence is a second-stratum factor of intelligence: Evidence from hierarchical and bifactor models. Emotion 2014, 14, 358–374. [Google Scholar] [CrossRef]
- Fischer, A.H.; Kret, M.E.; Broekens, J. Gender differences in emotion perception and self-reported emotional intelligence: A test of the emotion sensitivity hypothesis. PLoS One 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Guil, R.; Gómez-Molinero, R.; Merchán-Clavellino, A.; Gil-Olarte, P. Lights and Shadows of Trait Emotional Intelligence: Its Mediating Role in the Relationship Between Negative Affect and State Anxiety in University Students. Front Psychol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Mcguire, C.L. Preparing Future Healthcare Professionals: The Relationship Between Resilience Emotional Intelligence, and Age. Digit Commons @ ACU Electron Theses Diss 2021, 372. Available online: https://digitalcommons.acu.edu/etd.
- Abbasabad Arabi, H.; Bastani, F.; Navab, E.H.H. Investigating quality of life and its relationship with emotional intelligence (EQ) in elderly with diabetes. Iran J Psychiatry Clin Psychol. 2015, 21, 215–224. [Google Scholar]
- Yarahmadi, F.; Ghasemi, F.; Forooghi, S. The effects of emotional intelligence training on anxiety in hemodialysis patients. J Nurs Midwifery Sci. 2015, 2, 8. [Google Scholar]
- Mokhatri-Hesari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual Life Outcomes 2020, 18, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Muflih, S.; Alzoubi, K.H.; Al-Azzam, S.; Al-Husein, B. Depression symptoms and quality of life in patients receiving renal replacement therapy in Jordan: A cross-sectional study. Ann Med Surg 2021, 66, 102384. [Google Scholar] [CrossRef] [PubMed]
- Yapa, H.E.; Purtell, L.; Chambers, S.; Bonner, A. The Relationship Between Chronic Kidney Disease, Symptoms and Health-Related Quality of Life: A Systematic Review. J Ren Care. 2020, 46, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, B.M.; Karahan, T.F.; Ozcelik, M.; Igde, F.A. The effects of an emotional intelligence program on the quality of life and well-being of patients with type 2 diabetes mellitus. Diabetes Educ. 2008, 34, 1013–1024. [Google Scholar] [CrossRef]
- Baudry, A.S.; Lelorain, S.; Mahieuxe, M.; Christophe, V. Impact of emotional competence on supportive care needs, anxiety and depression symptoms of cancer patients: a multiple mediation model. Support Care Cancer 2018, 26, 223–230. [Google Scholar] [CrossRef]
- Benzo, R.P.; Kirsch, J.L.; Dulohery, M.M.; Abascal-Bolado, B. Emotional intelligence: A novel outcome associated with wellbeing and self-management in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2016, 13, 10–16. [Google Scholar] [CrossRef]
- Pérez-Fernández, A.; Fernández-Berrocal, P.; Gutiérrez-Cobo, M.J. The Relationship Between Emotional Intelligence and Diabetes Management: A Systematic Review. Front Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Ashby, D.; Borman, N.; Burton, J.; Corbett, R.; Davenport, A.; Farrington, K.; et al. Renal Association Clinical Practice Guideline on Haemodialysis. BMC Nephrol 2019, 20, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Coelho, J.; Sampaio, F.; Teixeira, S.; Parola, V.; Sequeira, C.; Lleixà Fortuño, M.; et al. A relação de ajuda como intervenção de enfermagem: Uma scoping review. Rev Port Enferm Saúde Ment 2020, 23, 63–72. [Google Scholar] [CrossRef]
Figure 1.
Level of emotional intelligence in male (%).
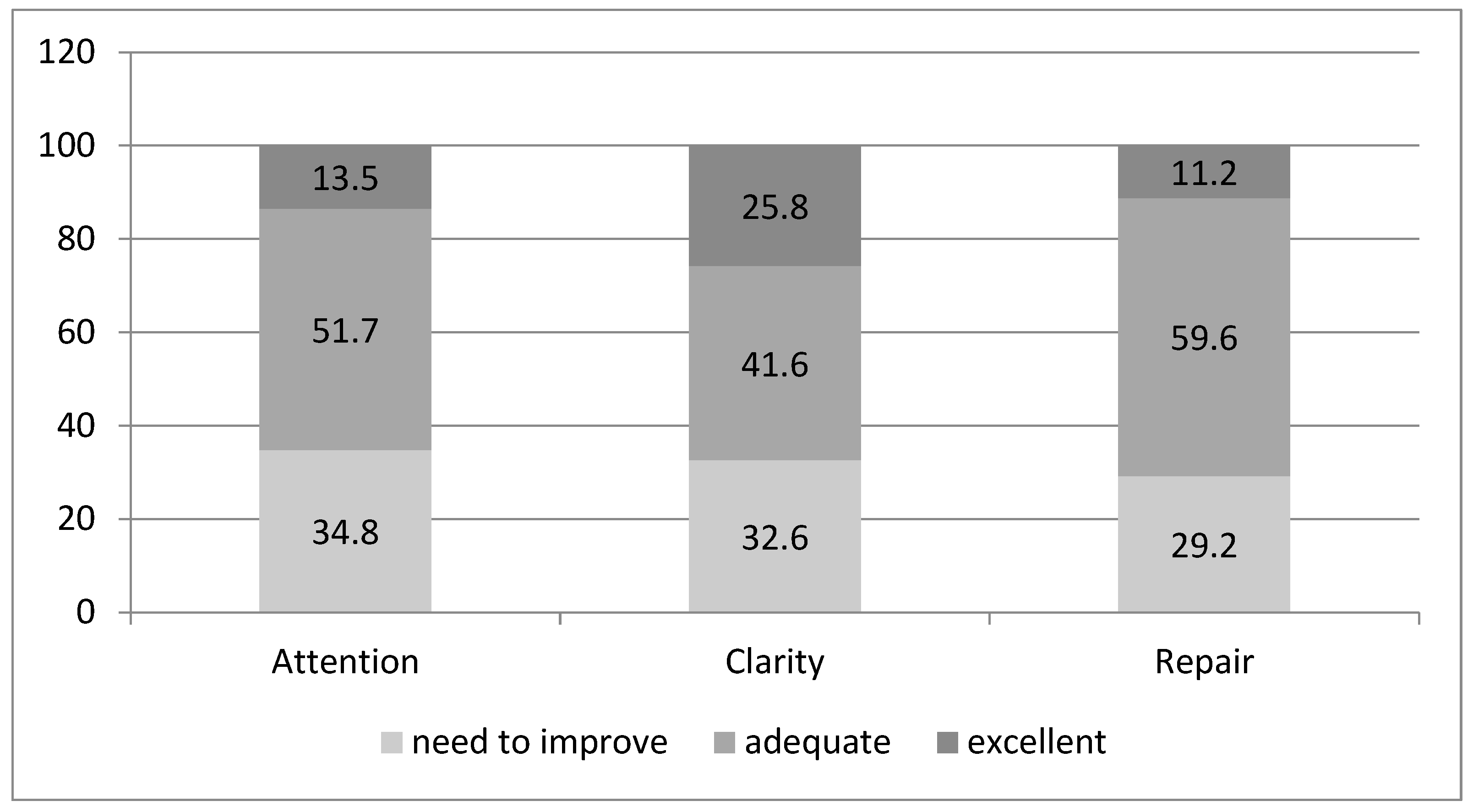
Figure 2.
Level of emotional intelligence in female (%).
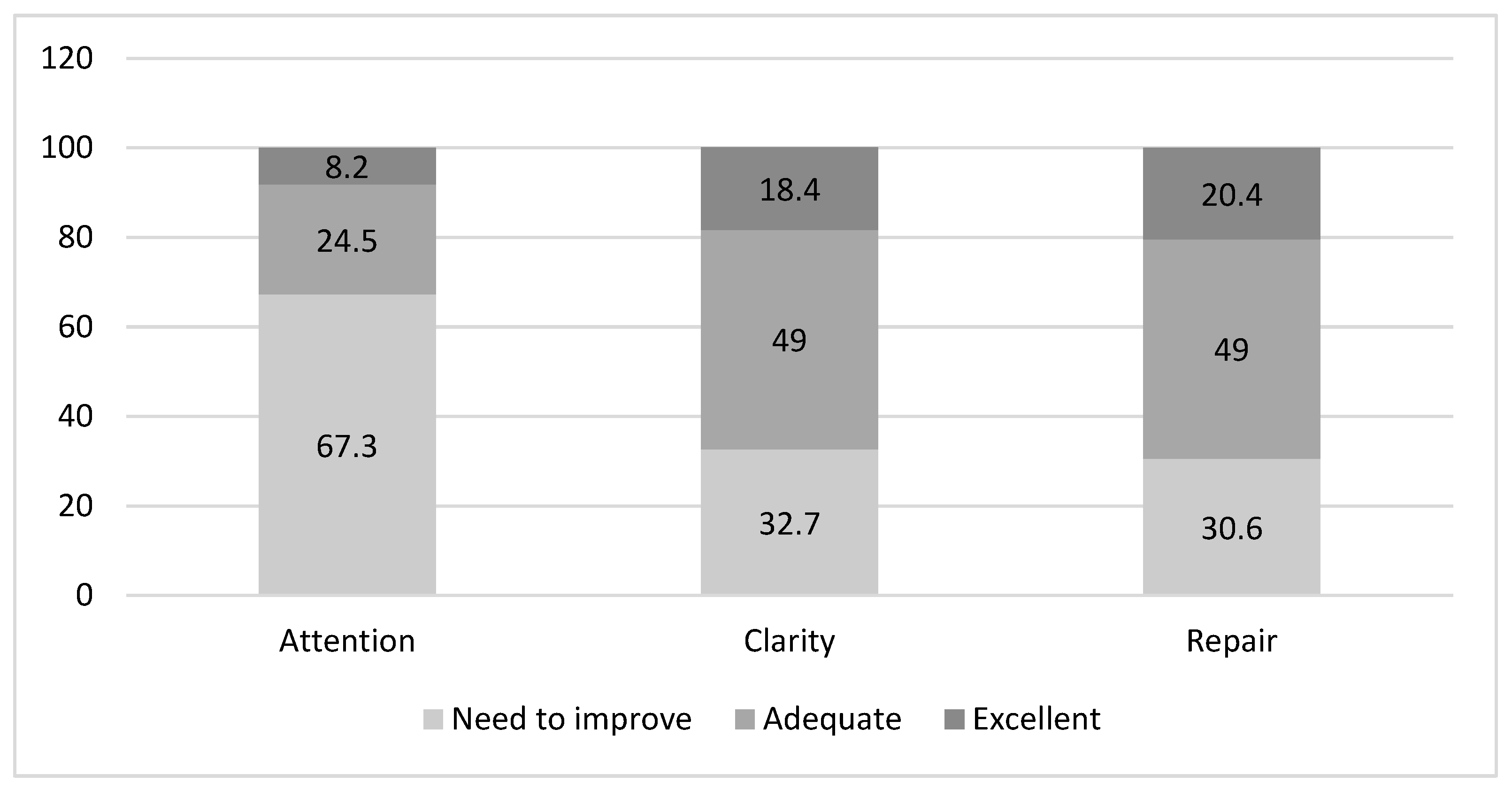

Table 1.
Description of emotional intelligence according to sex.
| Male | Female | |||
|---|---|---|---|---|
| Mean (standard deviation) | Median (interquartile) | Mean (standard deviation) | Median (interquartile) | |
| Attention | 23.8 (7.466) | 24.00 [17–30] | 22.29 (8.319) | 21.00 [16.50-29.50] |
| Clarity | 28.80 (7.478) | 27.00 [24–36] | 26.59 (8.178) | 25.00 [23.00-31.50] |
| Repair | 27.29 (7.271) | 29.00 [22–33] | 27.35 (8.268) | 28.00 [20.50-34.00] |
Table 2.
Relationship between physical dimensions of quality of life and sociodemographic variables.
Table 2.
Relationship between physical dimensions of quality of life and sociodemographic variables.
| Physical function | Physical role | Pain | General health | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | p | Mean | p | Mean | p | Mean | p | |
|
Sex Male Female |
52.13 (28.56) 46.00 (30.12) |
0.120 |
42.97 (40.41) 44.38 (38.94) |
0.422 |
57.27 (31.94) 53.62 (31.89) |
0.261 |
37.58 (20.74) 36.83 (20.45) |
0.419 |
|
Age 25-45 46-65 >65 |
75.52 (17.15) 57.16 (27.14) 40.79 (27.99) |
<0.001 |
56.57 (38.94) 41.89 (38.66) 41.15 (40.51) |
0.305 |
62.76 (27.87) 61.28 (31.70) 52.01 (32.52) |
0.207 |
39.73 (17.27) 42.02 (20.29) 34.63 (21.15) |
0.166 |
|
Living situation Alone With family Nursing homes |
57.22 (32.86) 48.38 (28.53) 77.50 (10.60) |
0.199 |
38.88 (39.50) 43.64 (40.19) 75.00 (0.00) |
0,478 |
55.13 (33.06) 55.46 (31.69) 93.75 (8.83) |
0.242 |
38.88 (16.58) 36.73 (21.09) 57.50 (17.67) |
0.348 |
|
Level of education Primary Secondary University |
46.32 (29.09) 61.80 (27.07) 62.85 (25.79) |
0.027 |
39.85 (39.30) 53.00 (39.07) 64.28 (45.31) |
0.122 |
53.58 (31.50) 60.80 (30.10) 75.00 (39.55) |
0.160 |
36.42 (20.39) 39.60 (22.68) 42.85 (15.77) |
0.604 |
*Results are shown with their mean and standard deviation.
Table 3.
Relationship between mental dimensions of quality of life and sociodemographic variables.
| Emotional wellbeing | Emotional Role | Social Function | Vitality | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | p | Mean | p | Mean | p | Mean | p | |
|
Sex Male Female |
64.51 (23.00) 61.38 (26.52) |
0.235 |
76.40 (37.42) 64.11 (45.33) |
0.045 |
66.03 (27.39) 61.22 (30.85) |
0.173 |
49.32 (24.27) 45.30 (27.22) |
0.187 |
|
Age 25-45 46-65 >65 |
68.42 (24.54) 65.18 (23.41) 61.43 (24.63) |
0.463 |
73.68 (39.40) 73.87 (38.59) 70.83 (42.27) |
0.916 |
71.44 (30.22) 65.20 (24.49) 62.28 (30.04) |
0.447 |
60.26 (22.20) 49.72 (23.83) 44.20 (25.93) |
0.038 |
|
Living situation Alone With family Nursing homes |
62.00 (23.61) 63.37 (24.58) 78.00 (2.82) |
0.679 |
79.62 (34.56) 70.97 (41.64) 66.66 (47.14) |
0.693 |
65.97 (26.36) 64.11 (29.14) 62.50 (35.35) |
0.964 |
44.44 (26.00) 48.13 (25.41) 65.00 (07.07) |
0.537 |
|
Level of education Primary Secondary University |
60.83 (24.17) 69.19 (24.11) 81.71 (15.45) |
0.036 |
69.26 (41.77) 81.33 (36.10) 80.95 (37.79) |
0.346 |
61.93 (28.23) 71.00 (29.69) 76.78 (28.34) |
0.182 |
46.41 (25.78) 49 .20 (23.34) 65.71 (20.70) |
0.143 |
*Results are shown with its mean and standard deviation.
Table 4.
Lineal regression model: variables associated to quality of life with general health. according to sex.
Table 4.
Lineal regression model: variables associated to quality of life with general health. according to sex.
| Coefficientsa.b | ||||||
|---|---|---|---|---|---|---|
| Non standarized coefficients | Standardized coefficients | t | Sig. | 95.0% CI for B | ||
| B | Std. Error | β | ||||
| Constant | 80.449 | 76.904 | 1.046 | .299 | -72.511 to 233.409 | |
| Age | .590 | .744 | .087 | .793 | .430 | -.890 to 2.070 |
| Level of education | 10.405 | 19.832 | .058 | .525 | .601 | -29.041 to 49.850 |
| Attention | -1.762 | 1.659 | -.128 | -1.062 | .291 | -5.062 to 1.538 |
| Clarity | -.253 | 2.057 | -.018 | -.123 | .903 | -4.345 to 3.839 |
| Repair | 3.805 | 2.200 | .270 | 1.730 | .087 | -.570 to 8.180 |
a, Sex = males; b, Dependent variable: general health; CI, confidence interval; R2 =0.06.
Table 5.
Lineal regression model: variables associated to quality of life with general health. according to sex.
Table 5.
Lineal regression model: variables associated to quality of life with general health. according to sex.
| Coefficientsa.b | ||||||
|---|---|---|---|---|---|---|
| Non standarized coefficients | Standardized coefficients | t | Sig. | 95.0% CI for B | ||
| B | Std. Error | β | ||||
| Constant | 242.504 | 96.294 | 2.518 | .016 | 48.309 to 436.699 | |
| Age | -1.666 | .866 | -.266 | -1.923 | .061 | -3.414 to .081 |
| Level of education | -6.354 | 27.897 | -.032 | -.228 | .821 | -62.614 to 49.905 |
| Attention | -3.730 | 1.816 | -.301 | -2.055 | .046 | -7.392 to -.069 |
| Clarity | -2.004 | 2.085 | -.159 | -.961 | .342 | -6.209 to 2.201 |
| Repair | 7.163 | 2.025 | .574 | 3.538 | <.001 | 3.080 to 11.247 |
a, Sex = females; b, Dependent variable= general health; CI, confidence interval; R2 =0.31.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



