
Submitted:
19 January 2024
Posted:
19 January 2024
You are already at the latest version
Abstract
Inflammatory bowel diseases, comprising Crohn’s disease (CD) and ulcerative colitis (UC), are chronic, relapsing and remitting immune-mediated inflammatory diseases affecting the gastrointestinal tract. Ustekinumab (UST) is a monoclonal antibody blocking the p40 subunit of the anti-interleukin (IL) 12/23. Pivotal trials (CERTIFI and UNITI-IM for CD, UNIFI for UC) established the efficacy of UST for the induction and maintenance of remission in both CD and UC, with the most favorable results in naïve patients to biologics. In recent years, a wealth of ‘real-world’ data has emerged supporting positive clinical, endoscopic, and histological outcomes in patients treated with UST, as well as reassuring safety data. More recently, the results of the first head-to-head trials of UST and tumor necrosis factor (TNF) antagonists have been reported. Moreover, a number of studies exploring the role of UST in specific clinical settings, such as perianal CD, postoperative complications and recurrence, extraintestinal manifestations, chronic antibiotic-refractory pouchitis, and pregnancy, have been reported. This review explores results reported to date on UST, including those from pivotal trials, real-world data, and emerging studies regarding therapeutic drug monitoring and immunogenicity. The safety profile of UST was also reviewed.
Keywords:
crohn’s disease
; inflammatory bowel diseases
; mucosal healing
; safety
; remission
; ulcerative colitis
; ustekinumab
1. Introduction
Ulcerative colitis (UC) and Crohn’s disease (CD) are the two most common forms of inflammatory bowel disease (IBD). The IBDs are commonly observed in the Western world and are caused by a complex interaction between genetic and environmental factors [1]. Given that both diseases have a relapsing and remitting course, an aggressive therapeutic approach is frequently required to prevent complications [2].
After discovering the critical pathogenetic role of tumor necrosis factor-α (TNF-α) in IBD, monoclonal anti-TNF-α antibodies have been developed and successfully adopted in clinical practice. However, a number of patients do not respond or experience a secondary loss of response or intolerance to anti-TNF-α treatment. Thus, novel therapeutic agents targeting alternative pathogenetic pathways have been investigated and approved for IBD treatment [3,4,5,6].
Ustekinumab (UST) is a monoclonal antibody blocking the p40 subunit of the anti-interleukin (IL) 12/23 [7], showing significant efficacy and safety in treating psoriatic arthritis [8]. Since IBD and chronic arthritis share similar pathogenetic mechanisms, researchers tried to use UST in managing IBD.
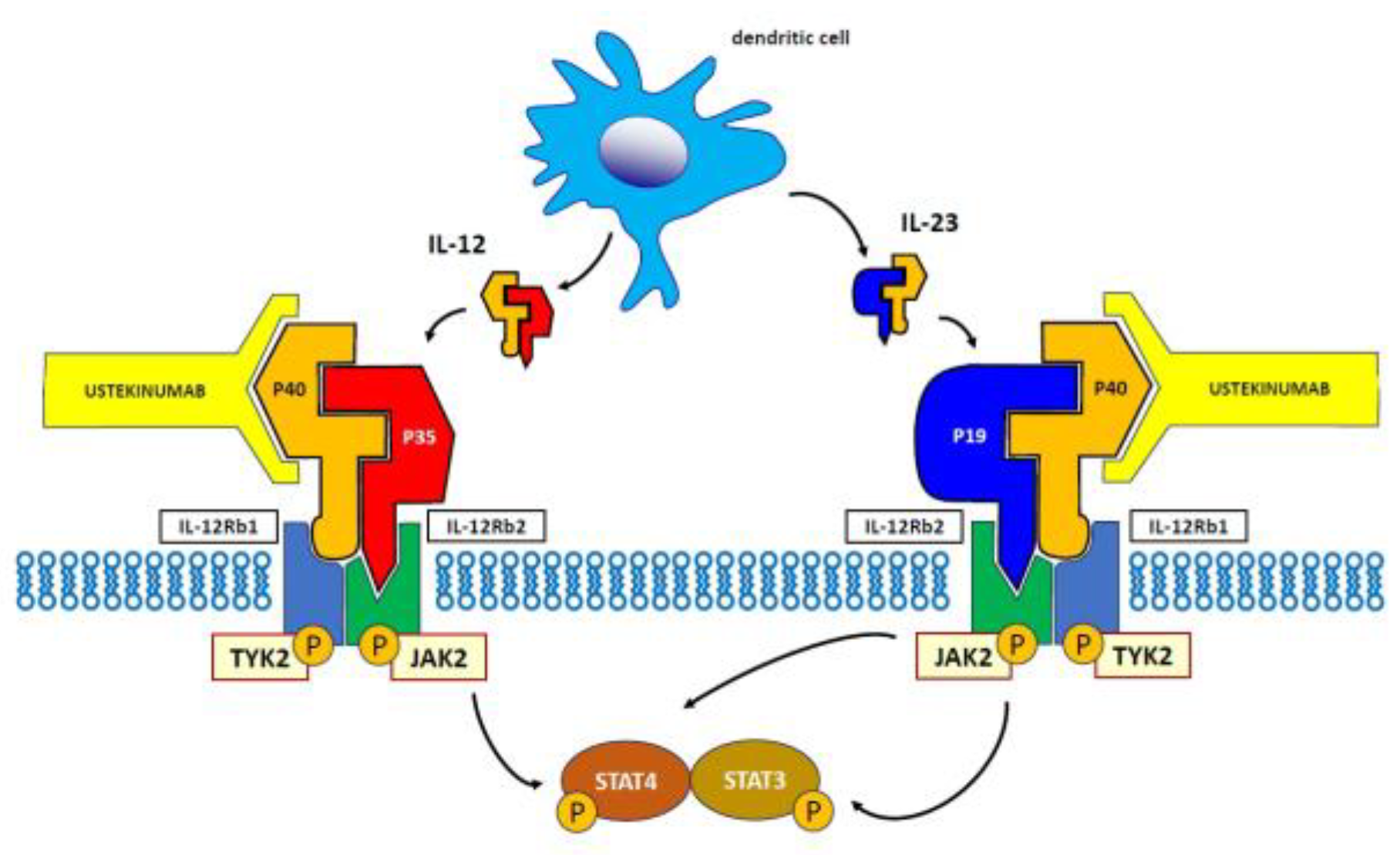
The IL-12 family is a cluster of cytokines, including IL-12, IL-23, IL-27 and IL-35. Although these molecules share structural features, they have different actions and properties. In particular, IL-23 and IL-12 are mainly pro-inflammatory cytokines produced in response to gut pathogens, which are essen-tial for the differentiation of CD4+ T naïve cells [9]. Their receptors transduce the signal via the JAK/STAT pathway—specifically, JAK2 and TYK2 are activated, then STAT4 is phosphorylated in response to IL12, while IL23 causes the phosphorylation of STAT3 and 4 [10]. IL-12 drives cell-mediated immunity by activating T-cell proliferation by Th1 cells [11,12]. This cytokine has a heterodimer structure composed of p40 and p35 protein subunits, and these, in turn, bind to a heterodimeric receptor complex consisting of IL-12 receptor (IL-12Rb1) and IL-12Rb2 chains expressed on the sur-face of T cells or natural killer (NK) cells [13]. IL-23 plays a major role in the expansion of committed Th17 cells [10,14]. This cytokine also is heterodimeric with p40 (common to both IL-12 and IL-23) and p19 protein subunits [15]. The specific intracellular signaling results in the expansion of committed Th17 cells [14]. As a consequence, the pharmacological blockade of the IL-12/23 axis interferes with the adaptive immune responses mediated by Th1 and Th17, which are highly relevant in the pathogenesis of CD [16], as well as UC [17].
More in detail, IL-12 induces the differentiation of a naïve cluster of CD4+ T cells into Th1 cells, producing interferon (IFN)-γ [9,13], whereas IL-23 specifically induces the differentiation of naïve CD4+ T cells into Th17 cells, with the activation of several proinflammatory cytokines, including IL-6, IL-17, and TNF-α [18]. Finally, IL-23 is capable of inducing a strong pro-inflammatory action through the activation of various target cells of the immune system, including CD8+ T cells, innate lymphoid cells, γ/δ T cells, and natural killers [19].
Genome-wide association studies (GWAS) have identified IL-12 and IL-23 as key cytokines in the pathogenesis of IBD [20], and therefore, therapies targeting the IL-12/IL-23 pathways have emerged and are in development.
Ustekinumab is a fully humanized IgG1k monoclonal antibody that binds to the p40 subunit of IL-12 and IL-23 and prevents their interaction with the IL-12 receptor, subsequently inhibiting IL-12 signaling and further activation of the Th1 cells subset. At the same time, it blocks the immune responses mediated by IL-23 and, in turn, the activation of the Th17 cells subset [7].
Pivotal trials (CERTIFI and UNITI-IM for CD, UNIFI for UC) established the efficacy of UST for the induction and maintenance of remission in both CD and UC, with the most favorable results in naϊve patients to biologics [21,22,23,24,25]. In recent years, a wealth of ‘real-world’ data has emerged supporting positive clinical, endoscopic, and histological outcomes in patients treated with UST confirming its safety [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59]. More recently, results of the first UST and an anti-TNF-α head-to-head trial have been reported [60]. Moreover, a number of studies exploring the role of UST in specific clinical settings, such as perianal CD [61,62,63], postoperative complications and recurrence [64,65,66], extraintestinal manifestations (EIMs) [67], chronic antibiotic-refractory pouchitis [68,69], and pregnancy appeared in the literature.
The aim of this review is to summarize the current literature regarding the mechanism of action of UST, data from registrational trials on safety and efficacy, including open-label extension (OLE), observational and emerging real-world (RW) evidence on its effectiveness in the treatment of IBD, and evolving paradigms with UST.
Figure 1.
Mechanism of action of ustekinumab.
2. Materials and Methods
A thorough literature search was conducted using PubMed to identify all relevant articles published until November 2023. Original articles and reviews were identified using the following search terms: “inflammatory bowel disease,” “Crohn’s disease,” and “Ulcerative colitis” matched with each of the following keywords: “Ustekinumab,” “Real life,” “Real world.” Additional articles were identified by reviewing the reference lists of selected pertinent articles. As a second step, we analyze and critically evaluate our sources, particularly RW studies with a significant number of patients.
3. Results
3.1. UST in CD
3.1.1. Evidence from Randomized Controlled Trials (RCTs)
The efficacy of UST in CD was initially investigated in two phase-2 RCTs. The first one was published in 2008, and it was a double-blind, cross-over trial on the clinical effects of UST in 104 patients with moderate-to-severe CD [70]. More specifically, patients were assigned (1:1:1:1) to subcutaneous (s.c.) placebo at weeks 0–3, then UST s.c. 90 mg at weeks 8–11; UST s.c. 90 mg at weeks 0–3, followed by placebo at weeks 8–11; intravenous (i.v.) placebo at week 0, then i.v. UST 4.5 mg/kg at week 8; or i.v. UST 4.5 mg/kg at week 0, followed by placebo at week 8. The primary endpoint of clinical response at week 8 (70-point decrement and at least 25% reduction from the baseline in the CD activity index [CDAI] score) was achieved in 49% and 40% (P = 0.34) of those who received UST and placebo, respectively. In a subgroup of patients who were previously treated with infliximab (IFX) (neither primary nor secondary nonresponders), clinical response at week 8 was significantly greater with UST compared with placebo (P<0.05). Higher baseline serum C-reactive protein (CRP) values predicted larger treatment effects with UST, especially in IFX-experienced patients, with a decrease in the CRP concentration paralleling clinic response observed with UST [71].
The second phase-2 RCT (CERTIFI) [21] assessed UST in 526 patients with moderate-severe CD resistant to anti-TNF treatment. Patients were assigned to receive i.v. UST at a dose of 1, 3, or 6 mg/kg, or placebo at week 0. The proportions of patients who reached the primary endpoint (clinical response at 6 weeks) were 36.6%, 34.1%, and 39.7% for 1, 3, and 6 mg of UST per kg, respectively, compared with 23.5% for placebo (P=0.005 for the comparison with the 6 mg/kg group). One hundred forty-five patients who responded to UST at 6 weeks were randomly assigned to s.c. UST 90 mg or placebo at weeks 8 and 16. The UST achieved significantly increased rates of clinical remission (41.7% vs. 27.4%, P=0.03) and a response (69.4% vs. 42.5%, P<0.001) at 22 weeks compared with placebo.
The promising results obtained in the two phase-2 trials paved the way for a phase-3 trials program, which was called UNITI. More in detail, two 8-week phase-3 induction trials (UNITI-1 and 2) and one 44-week phase-3 maintenance trial (IM-UNITI) were conducted [21,22,23]. The UNITI-1 trial included patients who were nonresponders or with unacceptable side effects to anti-TNF-α. In contrast, patients in the UNITI-2 trial were either naïve to biologics or anti-TNF-α experienced without failing. In the IM-UNITI, less than half (44%) of the patients had prior treatment with anti-TNF-α [21,22,23]. In these trials, UST was administered at 130 mg or approximately 6 mg per kg e.v., while at 90 mg s.c. every 8 or 12 weeks in maintaining remission.
The results of these pivotal studies were significant: the rates of response at week 6 among patients receiving UST e.v. were significantly higher than those enrolled in the placebo group (in the UNITI-1, 34.3%, 33.7%, and 21.5%, respectively, P≤0.003 vs. placebo; in the UNITI-2, 51.7%, 55.5%, and 28.7%, P<0.001 for both doses); the rate of remission at week 44 in the groups receiving UST every 8 weeks or every 12 weeks, 53.1% and 48.8%, respectively, were in remission at week 44, compared with 35.9% of those receiving placebo (P=0.005 and P=0.04, respectively).
Continued treatment with UST s.c. to maintain clinical response and remission through three years was investigated by another study (UNITI Long-Term Extension, UNITI-LTE). The IM-UNITI trial found that 38.0% of UST induction responders receiving the drug every 12 weeks and 43.0% receiving the drug every eight weeks were in remission at week 152 [22]. Finally, 34.4% of patients in the every-8-weeks group and 28.7% in the every-12-weeks group were in clinical remission at week 252 [23].
The SEAVUE is the first clinical trial to directly and prospectively compare two approved biologic treatments for CD, UST and adalimumab (ADA), in a randomized, double-blind, treat-through design [60].
In this study 386 patients who had failed conventional therapy and were biologic naïve were randomized to ADA or UST induction followed by maintenance therapy with a primary endpoint of clinical remission at week 52 (CDAI score <150). There was no significant difference in the proportion of patients in clinical remission between UST and ADA-treated patients (65% vs. 61%, P=0.42). ADA-treated patients had high rates of anti-drug antibodies compared to UST-treated patients (74% vs. 2%); however, the presence of anti-drug antibodies did not modify treatment response. Regarding endoscopic remission, at 52 week rates of endoscopic remission, defined as SES-CD ≤3, were largely equivalent (31% with adalimumab vs. 29% with UST) regardless of baseline SES-CD score.
3.2. ‘Real-world’ experience in CD
Real-world data provide greater insights into the effectiveness of therapy in a heterogeneous and more complex patient population representative of clinical practice. A growing body of evidence from RW data for UST provides credible evidence for its effectiveness and safety. After the UNITI pivotal trials' publication, several real-life studies from Europe, Asia, North and South Americas have been conducted, confirming its efficacy in daily practice.
3.2.1. UST for bio-experienced patients
In most real-life studies UST was used in the setting of anti-TNF-α failure or refractory to this treatment [72,73]. The RW studies in this specific setting reported that clinical remission at 24 weeks and (when available) at 52 weeks, ranged from 31% to 75%, and 25% to 60%, respectively [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. In addition, other parameters, ranging from mucosal healing (MH) to fecal calprotectin (FC) level, improved significantly under UST treatment [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. Interestingly, the results comparison of studies conducted on different continents, showed that UST works in the same way: between 24 and 52 weeks, the remission rate was about 25% in North America [32,34], 39% in South America [43], 25-60% in Europe [26,27,28,29,30,35,36,37,40,41,42,46,47,48], and 31-84% in Asia [31,38,39,45].
Two meta-analyses confirmed these results. In a systematic review and pooled analysis of real-world evidence only, Engel et al. found that the pooled remission rate at week 24 was 39% (range 18-65%) [74], and Macaluso et al. observed a pooled remission rate of 34% (range 18-65%) at week 24, and 40% at 52 weeks [75]. These results are superior to those obtained in pivotal trials, confirming a better response rate in RW studies.
In the absence of prospective, randomized clinical trials comparing available treatments, some RW studies often tried to overcome this limit using the propensity score, a statistical method able to reduce the selection bias, to compare head-to-head UST versus other biologics in this population setting. Ahmed et al. found that UST was not superior to ADA at week 56 (27% vs. 25%, P=0.820) [76]; Alric et al. found a higher response rate with UST than Vedolizumab (VDZ) at week 48 (54.4 vs. 38.8, <P=0.03) [77]. Lenti et al. found UST not superior to VDZ at week 14 (P=0.631) and week 52 (P=0.157) [78]. Singh et al. compared UST vs. anti-TNF-α and VDZ in a large population of CD patients. The UST was better than TNF-α antagonists and VDZ in term of response, however, differences in the hospitalization or surgery risk were not detected [79]. Onali et al found UST slight but not significant than better VDZ in obtaining clinical remission [80]. Finally, Kappelman et al. did not observe a difference in treatment persistence between UST and VDZ. Still, UST was associated with a lower rate of all-cause hospitalisation (adjusted hazard ratio [aHR] 0.73), nonsurgical CD hospitalisation (aHR 0.58), and hospitalization for infection (aHR 0.56) [81].
3.2.2. UST for bio-naïve patients
Real-world studies have also investigated UST in CD patients never exposed biologics. Overall, the remission rate was higher in this setting.
In a retrospective, multicenter, multinational consortium of UST-treated CD patients, the authors found a higher remission persistence at week 52 in bio-naïve vs. bio-experienced CD patients (55% vs. 40%, respectively). Significantly, prior anti-TNF-α (HR, 0.72) and VDZ exposure (HR, 0.65) were independently associated with lower likelihoods of achieving response to UST [82]. A Belgian study found a 12-month remission of about 74% [83], and a very recent Spanish study reported a remission at weeks 16 and 52 of 93% and 82%, respectively in CD patients [84]. These results were confirmed by a Canadian study reporting a clinical remission in 59% of bio-experienced and 79% of bio-naïve CD patients [85]. In contrast, in a Brazilian study, statistically significant differences were not observed in the remission rate recorded at one year between bio-experienced and bio-naïve CD patients treated with UST or VDZ (39.4 vs. 39.8: P=0.96), respectively [45].
Finally, UST with other biologics was also compared in a number of RW studies. In a retrospective study conducted in two tertiary centers, Rivière et al. compared UST with anti-TNF-α in bio-naïve CD patients with luminal disease. Authors found that anti-TNF-α as first-line biological therapy was better than UST at three months (P=0.02), whereas no difference was observed during a 40-month follow-up (P=0.29) [86]. These results were probably linked to the effect of IFX rather than ADA. Zhdanava et al. found that, at 12 months, bio-naïve UST-treated CD patients showed a significantly higher treatment persistence rate than ADA-treated CD patients [87]. On the other hand, a Belgian study was unable to detect differences in the clinical remission rate between ADA vs. UST bio-naïve CD patients at week 26 (adjusted odd ratio [aOR] 1.30; P=0.72) and at week 52 (aOR, 1.60; P=0.41) [88].
3.3. UST in UC
3.3.1. Evidence from Randomized Controlled Trials (RCTs)
More recently, UST has been approved by the European Medicines Agency (EMA) and the Food and Drugs Administration (FDA) to treat moderate to severe active UC patients with inadequate response, lost response to, or intolerance to either conventional therapy or biologic, or with medical contraindications to such therapies. UST efficacy and safety have been investigated in a double-blind, randomized phase-3 trial (UNIFI) among patients with moderate to severe active UC. This study consisted of a single protocol combining 8 weeks of induction therapy and 44 weeks of maintenance therapy, accounting for a total of 52 weeks of therapy [24]. Eligible patients were adults with moderate-to-severely active UC [defined as Full Mayo Score (FMS) ranging from 6 to 12, with a minimum endoscopic subscore of 2] and a history of inadequate benefit/intolerance to conventional or biological drugs or both. According to the endpoints, induction and maintenance were analyzed. In the ongoing long-term extension study, participants will continue with the same treatment regimen received at the end of the maintenance study [24].
At baseline, 961 patients were randomly assigned to either a single i.v. infusion of UST 130 mg, a dose based on weight that approximated to 6 mg/kg (260 mg, weight ≤55 kg; 390 mg, weight >55 kg and ≤85 kg; 520 mg, weight >85 kg), or placebo. Overall, nearly 48.0% of patients had previously failed biological therapies (13.4% both anti-TNF-α drugs and VDZ) and 51% of them were on concomitant steroids at enrollment.
Intravenous UST was more effective than placebo (15.6% vs. 5.3%) for inducing clinical remission in patients at week 8. Week 8 clinical responders were re-randomized into three different maintenance arms: 90 mg UST s.c. every 12 weeks (q12w), q8w, or placebo. Subcutaneous UST q12w or q8w was more effective than placebo (38.4% or 43.8% vs. 24%) for maintaining clinical remission in responders at induction at week 44. No significant differences were observed in patients with or without previous treatment failure with biologics [24].
After completing the maintenance phase, patients who received UST entered the long-term extension study until week 220, maintaining the same treatment regimens. At week 200, 55.2% were in symptomatic remission, with a greater proportion of biologic naïve patients (67.2%, 117/174) than those with a history of biologic failure (41.6%, 67/161). Finally, among patients in symptomatic remission at week 200, 96.4% were corticosteroid-free [89].
3.3.2.‘Real-world’ experience in UC
The first real-life experiences date back to a few years before the drug was approved for the treatment of UC. An Italian multicenter, retrospective study including seventy patients (64 CD and 6 UC) exposed to UST for concomitant active psoriasis, especially paradoxical forms, and psoriatic arthritis, UST s.c. showed a good effectiveness profile, irrespective of IBD activity, with a cumulative probability of maintaining UST treatment of 97.1% at 6 months and 77.1% at 12 months [33]. However, in that setting, patients received UST s.c. at the dosages and intervals approved for those conditions – specifically, they did not receive i.v. induction and the standard maintenance dosage was 45 mg q12w.
More recently, after the approval of UST for UC, some retrospective, observational studies, including unselected patients, have evaluated the effectiveness and safety of UST for UC in clinical practice [49,50,51,52,53,54,55,56,57,58,59,90]. Overall, although limited by the small simple sizes enrolled and the short follow-up time, these studies provided further credible evidence for effectiveness and safety of UST. A recent systematic review of thirteen real-life studies [86] noted that clinical remission and clinical response at induction were achieved in 24% to 61% of cases, and in 47% to 77% of cases, respectively. Moreover, clinical remission was achieved in 33% to 79% of cases at 52 weeks of follow-up, whereas steroid-free remission was reported in 6 studies and ranged from 14% to 67%. Finally, lack of effectiveness, refractory disease, and loss of response were the main reasons for UST discontinuation.
Regarding predictive factors that might predict clinical remission and response with UST, Hong et al. showed that a history of TNF-antagonist primary nonresponse and a baseline Mayo endoscopic score of 3, were negative predictors of clinical remission at three months [53]. Chaparro et al. showed that CRP serum concentration over the upper limit of the normal range was the only factor significantly associated with a lower probability of achieving remission [49].
Another recent systematic review with meta-analysis of RW included 19 studies, with 3786 patients, of which over 92% previously treated with any biologic, 61.1% with both anti-TNF and VDZ and 16.4% with any biologic and tofacitinib [91]. Among the UC patients, 45.4% were in clinical remission by weeks 8, 43.8% (38.4%-49.2%) by weeks 12-16, 44.6% by month 6, and 50.6% by month 12. Overall, 58.2% of patients displayed endoscopic improvement at month 12. Clinical response was achieved in 61.2%, 59.4%, 65.2%, and 76.8% at week 8, 12–16, month 6 and 12, respectively, and corticosteroid-free remission was achieved in 18.7%, 36.8%, 34.5% and 39% at week8, weeks 12–16, month 6 and 12, respectively. Overall, in 58.2% of patients endoscopic improvement at month 12 was observed. Interestingly, almost 30% of the patients needed dose escalation, which was effective in 40% of them. However, this meta-analysis suffers from several biases, ranging from high heterogeneity (>80%) in achieving remission at week 8 and one year to limited sample size in some included studies. Additionally, studies enrolling a higher proportion of patients with previous biological agents’ failure had a lower clinical remission rate. Parakkal et al. [55] and Honap et al. [54] reported remission rates of 23.9% and 20% at week 8 and 40.4% and 43.6% at week 26, respectively.
3.4. Safety
The safety profile of UST is very favorable. The pivotal trials UNITI-1 and -2 showed an adverse events (AEs) rate similar to placebo, both as overall rate (65.9% and 55.6% vs. 64.9% and 54.3%, respectively), and for serious AEs (7.2% and 2.9% vs. 6.1% and 5.8%, respectively). The IM-UNITI showed a similar safety profile of UST vs. placebo (81.7% vs. 83.5% for overall AEs, and 9.9% vs. 15.0% for severe AEs, respectively). Serious infection occurred in only 2.3% of the patients receiving UST and in the placebo group [21,22,23].
Regarding UC, overall, the UST safety in the UNIFI trial was consistent with the already known safety profile in all other approved indications, and rates of key safety events, including infections, were similar between UST and placebo. No deaths occurred among the primary population in the maintenance study. The rates of infection were similar across the treatment groups, and serious infections were infrequent: 1.7% in the q8w group; 3.5% in the q12w group; 2.3% with placebo. The number of AEs leading to discontinuation of the study agent was 20 in the placebo group; 5 and 9 in the q8w and q12w groups, respectively [24].
This favorable profile has also been confirmed in real life. In CD, overall, the mean rate of the AEs is about 11%, the large majority of them mild, and not requiring stopping treatment. Only one study reported an AEs rate of about 44%: a retrospective cohort study performed at a large single tertiary referral center in the US and analyzed the effect of UST in complex perianal disease [62]. The authors studied a challenging population: 61.3% reported prior perianal surgery, 36.2% taking concurrent immunomodulators at UST induction, and all patients were already treated with ≥2 anti-TNF [62]. Therefore, it was hypothesized that the population's characteristics could influence this high AEs rate.
In UC, a recent systematic review of RW data found that patients with AEs ranged from 2.6% to 32% [92]. In another recent systematic review with meta-analysis of RW the incidence rates (IRs) of colectomy, mild AEs, serious AEs and serious infections were 4.8, 7.9, 0.8 and 0.3 per 100 patient-years, respectively [91]. The most common non-infectious AE, except IBD exacerbation, was arthralgia (1.94%), followed by skin rash (1.55%).
3.5. UST in special situations
3.5.1. UST for perianal disease
UST has also been evaluated in specific clinical contexts, such as fistulizing perianal disease. UST seems to be less performing when used in managing fistulizing perianal CD. For example, a recent meta-analysis of controlled trials found UST effective in the induction of response but not in the induction of remission in those patients [93].
There are currently few RW studies in the literature on UST for perianal disease, reporting overall a modest effectiveness. The Groupe d'Étude Thérapeutique des Affections Inflammatoires du Tube Digestif assessed in detail the UST efficacy in perianal CD. Two hundred patients were included; 99% were previously exposed to at least one anti-TNF-α, and 28% were also exposed to VDZ. Successful treatment was obtained in 38% of patients, and successful seton removal was obtained in 33% of patients with their placement at the start of therapy [61]. In a retrospective cohort studied in a large single tertiary referral center, Godoy Brewer et al. found that, at 6 and 12 months, 48.1% and 55.6% of patients had an improved fistula response, but none achieved fistula remission [62]. Finally, according to the study of Yao et al., radiological healing of perianal fistulas was obtained in 44.8% of patients by using UST [63].
3.5.2. UST for postoperative recurrence
Despite the burden of postoperative recurrence after ileocolonic resection, no treatments have been approved to prevent recurrence in CD. Current ECCO guidelines recommend prophylactic immunosuppression with either thiopurines or anti-TNF-α agents to prevent postoperative recurrence in the presence of at least one of the clinical risk factors for recurrence [94].
Few RW studies are currently available in this specific setting of CD patients. A preliminary, retrospective study found that UST obtained MH, defined as Rutgeerts’score <2, in 73.3% of CD patients refractory to anti-TNF-α [65]. A recent prospective and comparative study showed a rate of endoscopic postoperative recurrence of 42% for UST and 40% for VDZ, in a cohort of patients exposed to anti-TNF therapy [64]. Finally, in a recent Italian study, Macaluso et al. confirmed the promising role of UST in preventing postoperative recurrence. The authors found 50% of endoscopic healing after a mean of 14.5±5.5 months following initiation of UST [66].
3.5.3. UST for extraintestinal manifestations.
The occurrence of extraintestinal manifestations (EIMs) during the course of IBD is challenging. Anti-TNF-α agents are well studied and validated in this field [95]. The use of other biologics, such as UST, as a therapeutic strategy remains unclear. Guillo et al. found recently that UST could be an effective option for the treatment of EIMs of CD, especially for dermatological and rheumatological manifestations [67]. An exciting study assessed the effect of UST on EIMs after the failure of anti-TNF-α agents. Twenty-four CD patients with EIM (17 with articular disease, nine with ankylosing spondylarthritis, three with rheumatoid arthritis, five with seronegative arthritis, four with erythema nodosum, one with uveitis; one with sclerosing cholangitis, and one with hidradenitis suppurativa) were treated with UST, with a significant improvement/remission of these EIMs [96].
More recently, a retrospective cohort study including IBD adult patients treated either with VDZ or UST and with EIMs before treatment initiation, showed clinical response of EIMs at week 52 in 36% (18/50) of patients treated with UST [97]. Moreover, safety profile and efficacy on EIMs also advocate in favor of UST as a reasonable candidate for the combination of targeted therapies, for patients with medical-refractory IBD without other medical options as well as for those with concomitant IBD and EIMs [98,99,100]. All these specific topics need further larger and longer studies.
3.5.4. UST for pouchitis
Restorative proctocolectomy with ileal pouch–anal anastomosis (IPAA) is routinely performed in patients with UC underging colectomy [101,102]. Idiopathic inflammation of the pouch —referred to as pouchitis— is the most common long-term complication of IPAA [103,104]; it develops in approximately half of patients within 5 years after surgery [105] and recurs in more than half of affected patients.
The conventional treatment for confirmed pouchitis is antibiotics such as ciprofloxacin and metronidazole [103]. Up to 15% of patients, however, develop chronic pouchitis and either become dependent on antibiotics for symptom relief or have continuous symptoms despite chronic antibiotic therapy [103,106,107,108]. Chronic antibiotic-refractory pouchitis represents an indication to biological therapy, mainly anti-TNF-α, whose short- and long-term (12 months) benefits are estimated to be around 50% [108]. Other treatments are usually recommended for refractory patients or for those with specific contraindications to anti-TNF-α drugs [109]. The real-life data for the use of UST in this setting are still scarce and limited by small sample sizes and large heterogeneity of therapy protocols/outcome definitions [9,10,11,12,13,14,15,16,17,18,19,20,21,35,45,47,48,55,61,62,63,68,69,70,71,72,73,74,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110]. In a retrospective, single-center study, 24 patients with chronic antibiotic-refractory pouchitis received UST (other pouch disorders were previously ruled out) at the dosage of 90 mg e.v. loading dose infusion followed by 90 mg subcutaneous injections q8w [68]. Of note, chronic antibiotic-refractory pouchitis had been previously treated unsuccessfully with other biologics in 12 patients (50.0%) and with immunomodulators in six (25.0%). After a median follow-up of 12.9 months (IQR = 7.9–16), 50.0% of patients achieved clinical response according to physician’s judgment and in terms of number of bowel movements per day. In 13 patients (54.2%) pouchoscopies were available post-UST treatment, in these patients, after a median time of 7.4 months (IQR = 4.6–10.6) since UST start, the median Pouchitis Disease Activity Index (PDAI) decreased from baseline 5 (IQR = 4–6) to 4 (IQR = 2–5) (P=0.016).
More recently, Dalal et al. reported on a cohort of 46 patients treated with UST with mixed pouch disorders, six chronic antibiotic-refractory pouchitis, 4 cuffitis, and 36 CD of the pouch [110]. Also in this study, all patients had prior anti-TNF exposure, and 24 of 46 (52.2%) with VDZ.
According to physician judgment, clinical response at 8-16 weeks was observed in 80.4% (37/46) of patients. Dose intensification to q6w or q4w was required in 23 patients (50.0%) after a median of 223 days, and a clinical response was obtained in 60.8% of them within the subsequent 8–16 weeks. Lower age at both UC diagnosis (HR = 0.94, 95% CI = 0.90–0.99) and UST start (HR = 0.96, 95% CI = 0.92–0.99) was associated with a shorter time to dose intensification.
In a recent systematic review to evaluate the efficacy of UST in chronic refractory pouchitis [69], clinical response and clinical remission were oberved in 63% and 10% of patients, respectively, after 4–12 weeks, whereas endoscopic response was reported in 60% of patients with chronic pouchitis after 24–32 weeks of treatment. Small sample sizes and large heterogeneity of therapy protocols/outcome definitions were significant limitations of the studies.
In conclusion, there is a limited and inconclusive body of evidence suggesting that UST may be a therapeutic option for patients with chronic pouchitis and CD of the pouch refractory to other therapies.
3.5.5. UST in pregnancy
The UST is an IgG1 and therefore crosses the placenta through the FcRn receptor as is the case with anti-TNF- α drugs. A favorable safety profile of UST for pregnant women has been initially observed among patients treated for psoriatic diseases [111]. Few data have been reported up to now for females affected by IBD, who conventionally receive higher doses compared with the dermatological and rheumatological indications. Although UST has not been extensively studied in pregnant women with IBD, existing data suggest it may be safe. Cases have been reported of mothers exposed to UST during preg-nancy and lactation without observable negative consequences for them or their children [112,113]. The effects of UST in pregnant women with IBD were also evaluated in 29 pregnancies in the PREGNANCY-GETAID study, without negative effects on maternal or neonatal outcomes. Overall, the 29 pregnancies resulted in 26 (90%) live births, two (7%) spontaneous abortions during the first trimester, and one (3%) elective termination. Mild maternal complications were reported in two patients. Rates of prematurity, spontaneous abortion, congenital malformations and maternal complications were comparable between the UST and anti-TNF-α groups [114]. These data were confirmed by the preliminary results from the DUMBO prospective registry [115]. Although UST appears to be safe during pregnancy, the experience is still limited, and its use should be individualized.
8. Conclusions
UST is a much-needed addition to the increasing armamentarium of IBD therapy, and its effectiveness in patients with other immune-mediated diseases, such as psoriasis and psoriatic arthritis, is particularly appealing. UST has shown efficacy both as a first-line both as a second-line agent for the induction and maintenance of remission in IBD. The safety profile is promising. Real-world data have supported its effectiveness and safety profile. Recent data on pregnancy, prevention of postoperative recurrence, fistulizing CD and pouchitis appear promising.
Author Contributions
Conceptualization, G.M. and A.T.; methodology, G.M.; software, G.M.P.; validation, G.M., A.T. and M.P.D.; formal analysis, G.M.; investigation, G.M., F.M.O.; resources, M.P.D.; data curation, G.M.; writing—original draft preparation, G.M.; writing—review and editing, G.M., A.T., F.M.O., P.U.S., G.M.P., M.P.D.; visualization, G.M.P.; supervision, M.P.D.; project administration, M.P.D.; funding acquisition, M.P.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data supporting the conclusions of this article are provided within the article and are available from the corresponding authors upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [PubMed]
- Ben-Horin, S. Loss of response to anti-tumor necrosis factors: what is the next step? Dig Dis 2014, 32, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Roda, G.; Jharap, B.; Neeraj, N.; Colombel, J.F. Loss of Response to Anti-TNFs: Definition, Epidemiology, and Management. Clin Transl Gastroenterol 2016, 7, e135. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Hanauer, S.B. Assessing response and loss of response to biological therapies in IBD. Am J Gastroenterol 2011, 106, 685–698. [Google Scholar] [CrossRef]
- Tursi, A.; Mocci, G.; Lorenzetti, R.; Allegretta, L.; Brandimarte, G.; Cassieri, C.; Colucci, R.; De Medici, A.; Faggiani, R.; Ferronato, A.; et al. Long-term real-life efficacy and safety of infliximab and adalimumab in the treatment of inflammatory bowel diseases outpatients. Eur J Gastroenterol Hepatol 2021, 33, 670–679. [Google Scholar] [CrossRef]
- Teng, M.W.; Bowman, E.P.; McElwee, J.J.; Smyth, M.J.; Casanova, J.L.; Cooper, A.M.; Cua, D.J. IL-12 and IL-23 cytokines: from discovery to targeted therapies for immune-mediated inflammatory diseases. Nat Med 2015, 21, 719–729. [Google Scholar] [CrossRef]
- Simons, N.; Degboe, Y.; Barnetche, T.; Cantagrel, A.; Ruyssen-Witrand, A.; Constantin, A. Biological DMARD efficacy in psoriatic arthritis: a systematic literature review and meta-analysis on articular, enthesitis, dactylitis, skin and functional outcomes. Clin Exp Rheumatol 2020, 38, 508–515. [Google Scholar]
- Moschen, A.R.; Tilg, H.; Raine, T. IL-12, IL-23 and IL-17 in IBD: immunobiology and therapeutic targeting. Nat Rev Gastroenterol Hepatol 2019, 16, 185–196. [Google Scholar] [CrossRef]
- Parham, C.; Chirica, M.; Timans, J.; Vaisberg, E.; Travis, M.; Cheung, J.; Pflanz, S.; Zhang, R.; Singh, K.P.; Vega, F.; et al. A receptor for the heterodimeric cytokine IL-23 is composed of IL-12Rbeta1 and a novel cytokine receptor subunit, IL-23R. J Immunol 2002, 168, 5699–5708. [Google Scholar] [CrossRef]
- Trinchieri, G. Interleukin-12 and the regulation of innate resistance and adaptive immunity. Nat Rev Immunol 2003, 3, 133–146. [Google Scholar] [CrossRef]
- Kobayashi, M.; Fitz, L.; Ryan, M.; Hewick, R.M.; Clark, S.C.; Chan, S.; Loudon, R.; Sherman, F.; Perussia, B.; Trinchieri, G. Identification and purification of natural killer cell stimulatory factor (NKSF), a cytokine with multiple biologic effects on human lymphocytes. J Exp Med 1989, 170, 827–845. [Google Scholar] [CrossRef] [PubMed]
- Presky, D.H.; Yang, H.; Minetti, L.J.; Chua, A.O.; Nabavi, N.; Wu, C.Y.; Gately, M.K.; Gubler, U. A functional interleukin 12 receptor complex is composed of two beta-type cytokine receptor subunits. Proc Natl Acad Sci U S A 1996, 93, 14002–14007. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, S.; Ghilardi, N.; Xie, M.H.; de Sauvage, F.J.; Gurney, A.L. Interleukin-23 promotes a distinct CD4 T cell activation state characterized by the production of interleukin-17. J Biol Chem 2003, 278, 1910–1914. [Google Scholar] [CrossRef]
- Benson, J.M.; Sachs, C.W.; Treacy, G.; Zhou, H.; Pendley, C.E.; Brodmerkel, C.M.; Shankar, G.; Mascelli, M.A. Therapeutic targeting of the IL-12/23 pathways: generation and characterization of ustekinumab. Nat Biotechnol 2011, 29, 615–624. [Google Scholar] [CrossRef]
- Xavier, R.J.; Podolsky, D.K. Unravelling the pathogenesis of inflammatory bowel disease. Nature 2007, 448, 427–434. [Google Scholar] [CrossRef]
- Gaffen, S.L.; Jain, R.; Garg, A.V.; Cua, D.J. The IL-23-IL-17 immune axis: from mechanisms to therapeutic testing. Nat Rev Immunol 2014, 14, 585–600. [Google Scholar] [CrossRef]
- Iwakura, Y.; Ishigame, H. The IL-23/IL-17 axis in inflammation. J Clin Invest 2006, 116, 1218–1222. [Google Scholar] [CrossRef] [PubMed]
- Neurath, M.F. IL-23 in inflammatory bowel diseases and colon cancer. Cytokine Growth Factor Rev 2019, 45, 1–8. [Google Scholar] [CrossRef]
- Jostins, L.; Ripke, S.; Weersma, R.K.; Duerr, R.H.; McGovern, D.P.; Hui, K.Y.; Lee, J.C.; Schumm, L.P.; Sharma, Y.; Anderson, C.A.; et al. Host-microbe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature 2012, 491, 119–124. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Gasink, C.; Gao, L.L.; Blank, M.A.; Johanns, J.; Guzzo, C.; Sands, B.E.; Hanauer, S.B.; Targan, S.; Rutgeerts, P.; et al. Ustekinumab induction and maintenance therapy in refractory Crohn's disease. N Engl J Med 2012, 367, 1519–1528. [Google Scholar] [CrossRef]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn's Disease. N Engl J Med 2016, 375, 1946–1960. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Sandborn, W.J.; Feagan, B.G.; Gasink, C.; Jacobstein, D.; Zou, B.; Johanns, J.; Adedokun, O.J.; Sands, B.E.; Rutgeerts, P.; et al. IM-UNITI: Three-year Efficacy, Safety, and Immunogenicity of Ustekinumab Treatment of Crohn's Disease. J Crohns Colitis 2020, 14, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Sandborn, W.J.; Panaccione, R.; O'Brien, C.D.; Zhang, H.; Johanns, J.; Adedokun, O.J.; Li, K.; Peyrin-Biroulet, L.; Van Assche, G.; et al. Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med 2019, 381, 1201–1214. [Google Scholar] [CrossRef] [PubMed]
- Abreu, M.T.; Rowbotham, D.S.; Danese, S.; Sandborn, W.J.; Miao, Y.; Zhang, H.; Tikhonov, I.; Panaccione, R.; Hisamatsu, T.; Scherl, E.J.; et al. Efficacy and Safety of Maintenance Ustekinumab for Ulcerative Colitis Through 3 Years: UNIFI Long-term Extension. J Crohns Colitis 2022, 16, 1222–1234. [Google Scholar] [CrossRef] [PubMed]
- Iborra, M.; Beltran, B.; Fernandez-Clotet, A.; Gutierrez, A.; Antolin, B.; Huguet, J.M.; De Francisco, R.; Merino, O.; Carpio, D.; Garcia-Lopez, S.; et al. Real-world short-term effectiveness of ustekinumab in 305 patients with Crohn's disease: results from the ENEIDA registry. Aliment Pharmacol Ther 2019, 50, 278–288. [Google Scholar] [CrossRef]
- Liefferinckx, C.; Verstockt, B.; Gils, A.; Noman, M.; Van Kemseke, C.; Macken, E.; De Vos, M.; Van Moerkercke, W.; Rahier, J.F.; Bossuyt, P.; et al. Long-term Clinical Effectiveness of Ustekinumab in Patients with Crohn's Disease Who Failed Biologic Therapies: A National Cohort Study. J Crohns Colitis 2019, 13, 1401–1409. [Google Scholar] [CrossRef]
- Biemans, V.B.C.; van der Meulen-de Jong, A.E.; van der Woude, C.J.; Lowenberg, M.; Dijkstra, G.; Oldenburg, B.; de Boer, N.K.H.; van der Marel, S.; Bodelier, A.G.L.; Jansen, J.M.; et al. Ustekinumab for Crohn's Disease: Results of the ICC Registry, a Nationwide Prospective Observational Cohort Study. J Crohns Colitis 2020, 14, 33–45. [Google Scholar] [CrossRef]
- Hoffmann, P.; Krisam, J.; Wehling, C.; Kloeters-Plachky, P.; Leopold, Y.; Belling, N.; Gauss, A. Ustekinumab: "Real-world" outcomes and potential predictors of nonresponse in treatment-refractory Crohn's disease. World J Gastroenterol 2019, 25, 4481–4492. [Google Scholar] [CrossRef]
- Eberl, A.; Hallinen, T.; Af Bjorkesten, C.G.; Heikkinen, M.; Hirsi, E.; Kellokumpu, M.; Koskinen, I.; Moilanen, V.; Nielsen, C.; Nuutinen, H.; et al. Ustekinumab for Crohn's disease: a nationwide real-life cohort study from Finland (FINUSTE). Scand J Gastroenterol 2019, 54, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Bar-Gil Shitrit, A.; Ben-Ya'acov, A.; Siterman, M.; Waterman, M.; Hirsh, A.; Schwartz, D.; Zittan, E.; Adler, Y.; Koslowsky, B.; Avni-Biron, I.; et al. Safety and effectiveness of ustekinumab for induction of remission in patients with Crohn's disease: A multicenter Israeli study. United European Gastroenterol J 2020, 8, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.; Evers Carlini, L.; Duley, C.; Garrett, A.; Annis, K.; Wagnon, J.; Dalal, R.; Scoville, E.; Beaulieu, D.; Schwartz, D.; et al. A Single Center Experience With Long-Term Ustekinumab Use and Reinduction in Patients With Refractory Crohn Disease. Crohns Colitis 360 2020, 2, otaa013. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, D.; Daperno, M.; Fiorino, G.; Savarino, E.; Mosso, E.; Biancone, L.; Testa, A.; Sarpi, L.; Cappello, M.; Bodini, G.; et al. Real-life effectiveness of ustekinumab in inflammatory bowel disease patients with concomitant psoriasis or psoriatic arthritis: An IG-IBD study. Dig Liver Dis 2019, 51, 972–977. [Google Scholar] [CrossRef]
- Ma, C.; Fedorak, R.N.; Kaplan, G.G.; Dieleman, L.A.; Devlin, S.M.; Stern, N.; Kroeker, K.I.; Seow, C.H.; Leung, Y.; Novak, K.L.; et al. Clinical, endoscopic and radiographic outcomes with ustekinumab in medically-refractory Crohn's disease: real world experience from a multicentre cohort. Aliment Pharmacol Ther 2017, 45, 1232–1243. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Fries, W.; Viola, A.; Costantino, G.; Muscianisi, M.; Cappello, M.; Guida, L.; Giuffrida, E.; Magnano, A.; Pluchino, D.; et al. Effectiveness of Ustekinumab on Crohn's Disease Associated Spondyloarthropathy: Real-World Data from the Sicilian Network for Inflammatory Bowel Diseases (SN-IBD). Expert Opin Biol Ther 2020, 20, 1381–1384. [Google Scholar] [CrossRef]
- Viola, A.; Muscianisi, M.; Macaluso, F.S.; Ventimiglia, M.; Cappello, M.; Privitera, A.C.; Magnano, A.; Pluchino, D.; Magri, G.; Ferracane, C.; et al. Ustekinumab in Crohn's disease: Real-world outcomes from the Sicilian network for inflammatory bowel diseases. JGH Open 2021, 5, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.; Gravina, A.G.; Cuomo, A.; Mucherino, C.; Sgambato, D.; Facchiano, A.; Granata, L.; Priadko, K.; Pellegrino, R.; de Filippo, F.R.; et al. Efficacy of ustekinumab in the treatment of patients with Crohn's disease with failure to previous conventional or biologic therapy: a prospective observational real-life study. J Physiol Pharmacol 2021, 72. [Google Scholar] [CrossRef]
- Yokoyama, S.; Asano, T.; Nagano, K.; Tsuchiya, H.; Takagishi, M.; Tsujioka, S.; Miura, N.; Matsumoto, T. Safety and effectiveness of ustekinumab in Crohn's disease: Interim results of post-marketing surveillance in Japan. J Gastroenterol Hepatol 2021, 36, 3069–3076. [Google Scholar] [CrossRef]
- Yao, J.Y.; Zhang, M.; Wang, W.; Peng, X.; Zhao, J.Z.; Liu, T.; Li, Z.W.; Sun, H.T.; Hu, P.; Zhi, M. Ustekinumab trough concentration affects clinical and endoscopic outcomes in patients with refractory Crohn's disease: a Chinese real-world study. BMC Gastroenterol 2021, 21, 380. [Google Scholar] [CrossRef]
- Tursi, A.; Mocci, G.; Cuomo, A.; Allegretta, L.; Aragona, G.; Colucci, R.; Della Valle, N.; Ferronato, A.; Forti, G.; Gaiani, F.; et al. Real-life efficacy and safety of Ustekinumab as second- or third-line therapy in Crohn's disease: results from a large Italian cohort study. Eur Rev Med Pharmacol Sci 2021, 25, 2099–2108. [Google Scholar] [CrossRef]
- Scribano, M.L.; Aratari, A.; Neri, B.; Bezzio, C.; Balestrieri, P.; Baccolini, V.; Falasco, G.; Camastra, C.; Pantanella, P.; Monterubbianesi, R.; et al. Effectiveness of ustekinumab in patients with refractory Crohn's disease: a multicentre real-life study in Italy. Therap Adv Gastroenterol 2022, 15, 17562848211072412. [Google Scholar] [CrossRef] [PubMed]
- Ylisaukko-Oja, T.; Puttonen, M.; Jokelainen, J.; Koivusalo, M.; Tamminen, K.; Torvinen, S.; Voutilainen, M. Dose-escalation of adalimumab, golimumab or ustekinumab in inflammatory bowel diseases: characterization and implications in real-life clinical practice. Scand J Gastroenterol 2022, 57, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Parra, R.S.; Chebli, J.M.F.; Queiroz, N.S.F.; Damiao, A.; de Azevedo, M.F.C.; Chebli, L.A.; Bertges, E.R.; Alves Junior, A.J.T.; Ambrogini Junior, O.; da Silva, B.; et al. Long-term effectiveness and safety of ustekinumab in bio-naive and bio-experienced anti-tumor necrosis factor patients with Crohn's disease: a real-world multicenter Brazilian study. BMC Gastroenterol 2022, 22, 199. [Google Scholar] [CrossRef]
- Forss, A.; Clements, M.; Myrelid, P.; Strid, H.; Soderman, C.; Wagner, A.; Andersson, D.; Hjelm, F.; group, P.S.s.; Olen, O.; et al. Ustekinumab Is Associated with Real-World Long-Term Effectiveness and Improved Health-Related Quality of Life in Crohn's Disease. Dig Dis Sci 2023, 68, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Esaki, M.; Ihara, Y.; Tominaga, N.; Takedomi, H.; Tsuruoka, N.; Akutagawa, T.; Yukimoto, T.; Kawasaki, K.; Umeno, J.; Torisu, T.; et al. Predictive factors of the clinical efficacy of ustekinumab in patients with refractory Crohn's disease: tertiary centers experience in Japan. Int J Colorectal Dis 2023, 38, 57. [Google Scholar] [CrossRef] [PubMed]
- Casas-Deza, D.; Lamuela-Calvo, L.J.; Gomollon, F.; Arbones-Mainar, J.M.; Caballol, B.; Gisbert, J.P.; Rivero, M.; Sanchez-Rodriguez, E.; Arias Garcia, L.; Gutierrez Casbas, A.; et al. Effectiveness and Safety of Ustekinumab in Elderly Patients with Crohn's Disease: Real World Evidence From the ENEIDA Registry. J Crohns Colitis 2023, 17, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo Gonzalez, L.; Valdes Delgado, T.; Vazquez Moron, J.M.; Castro Laria, L.; Leo Carnerero, E.; Maldonado Perez, M.B.; Sanchez Capilla, D.; Pallares Manrique, H.; Saez Diaz, A.; Arguelles Arias, F.; et al. Ustekinumab in Crohn's disease: real-world outcomes and predictors of response. Rev Esp Enferm Dig 2022, 114, 272–279. [Google Scholar] [CrossRef]
- Bacaksiz, F.; Ari, D.; Gokbulut, V.; Ozturk, O.; Kayacetin, E. One-year real life data of our patients with moderate-severe Crohn's disease who underwent ustekinumab therapy. Scott Med J 2021, 66, 152–157. [Google Scholar] [CrossRef]
- Chaparro, M.; Garre, A.; Iborra, M.; Sierra-Ausin, M.; Barreiro-de Acosta, M.; Fernandez-Clotet, A.; de Castro, L.; Bosca-Watts, M.; Casanova, M.J.; Lopez-Garcia, A.; et al. Effectiveness and Safety of Ustekinumab in Ulcerative Colitis: Real-world Evidence from the ENEIDA Registry. J Crohns Colitis 2021, 15, 1846–1851. [Google Scholar] [CrossRef]
- Fumery, M.; Filippi, J.; Abitbol, V.; Biron, A.; Laharie, D.; Serrero, M.; Altwegg, R.; Bouhnik, Y.; Peyrin-Biroulet, L.; Gilletta, C.; et al. Effectiveness and safety of ustekinumab maintenance therapy in 103 patients with ulcerative colitis: a GETAID cohort study. Aliment Pharmacol Ther 2021, 54, 944–951. [Google Scholar] [CrossRef]
- Amiot, A.; Filippi, J.; Abitbol, V.; Cadiot, G.; Laharie, D.; Serrero, M.; Altwegg, R.; Bouhnik, Y.; Peyrin-Biroulet, L.; Gilletta, C.; et al. Effectiveness and safety of ustekinumab induction therapy for 103 patients with ulcerative colitis: a GETAID multicentre real-world cohort study. Aliment Pharmacol Ther 2020, 51, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Chiappetta, M.F.; Viola, A.; Mastronardi, M.; Turchini, L.; Carparelli, S.; Orlando, A.; Biscaglia, G.; Miranda, A.; Guida, L.; Costantino, G.; et al. One-year effectiveness and safety of ustekinumab in ulcerative colitis: a multicenter real-world study from Italy. Expert Opin Biol Ther 2021, 21, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.J.; Krugliak Cleveland, N.; Akiyama, S.; Zullow, S.; Yi, Y.; Shaffer, S.R.; Malter, L.B.; Axelrad, J.E.; Chang, S.; Hudesman, D.P.; et al. Real-World Effectiveness and Safety of Ustekinumab for Ulcerative Colitis From 2 Tertiary IBD Centers in the United States. Crohns Colitis 360 2021, 3, otab002. [Google Scholar] [CrossRef] [PubMed]
- Honap, S.; Al-Hillawi, L.; Baillie, S.; Bancil, A.; Matini, L.; Lau, R.; Kok, K.B.; Patel, K.; Walsh, A.; Irving, P.M.; et al. Ustekinumab for the treatment of moderate to severe ulcerative colitis: a multicentre UK cohort study. Frontline Gastroenterol 2022, 13, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Parakkal, D.; Johnson, A.; Fenster, M.; Ramos, G.; Zulqarnain, M.; Ullman, T.; Huang, L.; Gutierrez, A.; Bruss, A.; Ungaro, R.; et al. Real-World Effectiveness And Safety Of Ustekinumab In Patients With Ulcerative Colitis: A Multi-Centre Study. Journal of Crohn's and Colitis 2021, 15, S349–S350. [Google Scholar] [CrossRef]
- Ecker, D.; Fuchssteiner, H.; Gregus, M.; Piringer, P.; Wewalka, F.; Schöfl, R.; Kienbauer, M. Ustekinumab for Ulcerative Colitis A Real-World Experience - Retrospective Data Analysis of the IBD Cohort Ordensklinikum Linz. United European Gastroenterology Journal 2021, 9, 490–490. [Google Scholar] [CrossRef]
- Alsoud, D.; De Hertogh, G.; Compernolle, G.; Tops, S.; Sabino, J.; Ferrante, M.; Thomas, D.; Vermeire, S.; Verstockt, B. Real-world Endoscopic and Histological Outcomes Are Correlated with Ustekinumab Exposure in Patients with Ulcerative Colitis. J Crohns Colitis 2022, 16, 1562–1570. [Google Scholar] [CrossRef]
- Thunberg, J.; Bjorkqvist, O.; Hedin, C.R.H.; Forss, A.; Soderman, C.; Bergemalm, D.; Group, S.S.; Olen, O.; Hjortswang, H.; Strid, H.; et al. Ustekinumab treatment in ulcerative colitis: Real-world data from the Swedish inflammatory bowel disease quality register. United European Gastroenterol J 2022, 10, 631–639. [Google Scholar] [CrossRef]
- Ochsenkuhn, T.; Tillack, C.; Szokodi, D.; Janelidze, S.; Schnitzler, F. Clinical outcomes with ustekinumab as rescue treatment in therapy-refractory or therapy-intolerant ulcerative colitis. United European Gastroenterol J 2020, 8, 91–98. [Google Scholar] [CrossRef]
- Sands, B.E.; Irving, P.M.; Hoops, T.; Izanec, J.L.; Gao, L.L.; Gasink, C.; Greenspan, A.; Allez, M.; Danese, S.; Hanauer, S.B.; et al. Ustekinumab versus adalimumab for induction and maintenance therapy in biologic-naive patients with moderately to severely active Crohn's disease: a multicentre, randomised, double-blind, parallel-group, phase 3b trial. Lancet 2022, 399, 2200–2211. [Google Scholar] [CrossRef]
- Chapuis-Biron, C.; Kirchgesner, J.; Pariente, B.; Bouhnik, Y.; Amiot, A.; Viennot, S.; Serrero, M.; Fumery, M.; Allez, M.; Siproudhis, L.; et al. Ustekinumab for Perianal Crohn's Disease: The BioLAP Multicenter Study From the GETAID. Am J Gastroenterol 2020, 115, 1812–1820. [Google Scholar] [CrossRef]
- Godoy Brewer, G.M.; Salem, G.; Afzal, M.A.; Limketkai, B.N.; Haq, Z.; Tajamal, M.; Melia, J.; Lazarev, M.; Selaru, F.M.; Parian, A.M. Ustekinumab is effective for perianal fistulising Crohn's disease: a real-world experience and systematic review with meta-analysis. BMJ Open Gastroenterol 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zhang, H.; Su, T.; Peng, X.; Zhao, J.; Liu, T.; Wang, W.; Hu, P.; Zhi, M.; Zhang, M. Ustekinumab Promotes Radiological Fistula Healing in Perianal Fistulizing Crohn's Disease: A Retrospective Real-World Analysis. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Mañosa, M.; Fernandez-Clotet, A.; Nos, P.; Martin-Arranz, M.D.; Manceñido, N.; Carbajo, A.; Hinojosa, E.; Hernandez-Camba, A.; Muñoz-Perez, R.; Bosca-Watts, M.; et al. Ustekinumab and vedolizumab for the prevention of postoperative recurrence of Crohn's disease: Results from the ENEIDA registry. Dig Liver Dis 2023, 55, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Mocci, G.; Picchio, M.; Elisei, W.; Maconi, G. Letter: ustekinumab for the treatment of post-surgical and refractory Crohn's disease. Aliment Pharmacol Ther 2021, 53, 859–860. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Grova, M.; Mocciaro, F.; Di Mitri, R.; Privitera, A.C.; Distefano, M.E.; Vitello, A.; Camilleri, S.; Ferracane, C.; Pluchino, D.; et al. Ustekinumab is a promising option for the treatment of postoperative recurrence of Crohn's disease. J Gastroenterol Hepatol 2023, 38, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Guillo, L.; D'Amico, F.; Danese, S.; Peyrin-Biroulet, L. Ustekinumab for Extra-intestinal Manifestations of Inflammatory Bowel Disease: A Systematic Literature Review. J Crohns Colitis 2021, 15, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Ollech, J.E.; Rubin, D.T.; Glick, L.; Weisshof, R.; El Jurdi, K.; Israel, A.; Krugliak Cleveland, N.; Hyman, N.; Sakuraba, A.; Pekow, J.; et al. Ustekinumab Is Effective for the Treatment of Chronic Antibiotic-Refractory Pouchitis. Dig Dis Sci 2019, 64, 3596–3601. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, C.; Soliman, Y.Y.; Massidda, M.; Vadala di Prampero, S.F.; Bulajic, M.; Sorrentino, D. Is Ustekinumab Effective in Refractory Crohn's Disease of the Pouch and Chronic Pouchitis? A Systematic Review. Dig Dis Sci 2022, 67, 1948–1955. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Fedorak, R.N.; Scherl, E.; Fleisher, M.R.; Katz, S.; Johanns, J.; Blank, M.; Rutgeerts, P.; Ustekinumab Crohn's Disease Study, G. A randomized trial of Ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with moderate-to-severe Crohn's disease. Gastroenterology 2008, 135, 1130–1141. [Google Scholar] [CrossRef]
- Toedter, G.P.; Blank, M.; Lang, Y.; Chen, D.; Sandborn, W.J.; de Villiers, W.J. Relationship of C-reactive protein with clinical response after therapy with ustekinumab in Crohn's disease. Am J Gastroenterol 2009, 104, 2768–2773. [Google Scholar] [CrossRef] [PubMed]
- Allez, M.; Karmiris, K.; Louis, E.; Van Assche, G.; Ben-Horin, S.; Klein, A.; Van der Woude, J.; Baert, F.; Eliakim, R.; Katsanos, K.; et al. Report of the ECCO pathogenesis workshop on anti-TNF therapy failures in inflammatory bowel diseases: definitions, frequency and pharmacological aspects. J Crohns Colitis 2010, 4, 355–366. [Google Scholar] [CrossRef]
- Chowers, Y.; Sturm, A.; Sans, M.; Papadakis, K.; Gazouli, M.; Harbord, M.; Jahnel, J.; Mantzaris, G.J.; Meier, J.; Mottet, C.; et al. Report of the ECCO workshop on anti-TNF therapy failures in inflammatory bowel diseases: biological roles and effects of TNF and TNF antagonists. J Crohns Colitis 2010, 4, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Engel, T.; Yung, D.E.; Ma, C.; Pariente, B.; P, W.I.; Eliakim, R.; Ungar, B.; Ben-Horin, S.; Kopylov, U. Effectiveness and safety of Ustekinumab for Crohn's disease; systematic review and pooled analysis of real-world evidence. Dig Liver Dis 2019, 51, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Maida, M.; Ventimiglia, M.; Cottone, M.; Orlando, A. Effectiveness and safety of Ustekinumab for the treatment of Crohn's disease in real-life experiences: a meta-analysis of observational studies. Expert Opin Biol Ther 2020, 20, 193–203. [Google Scholar] [CrossRef]
- Ahmed, Z.; Venkata, K.; Zhang, N.; Malik, T.A. Comparative Effectiveness of Ustekinumab Versus Adalimumab in Induction of Clinical Response and Remission in Crohn's Disease: Experience of a Real-World Cohort at a Tertiary Care Inflammatory Bowel Disease Referral Center. Gastroenterology Res 2019, 12, 245–251. [Google Scholar] [CrossRef]
- Alric, H.; Amiot, A.; Kirchgesner, J.; Treton, X.; Allez, M.; Bouhnik, Y.; Beaugerie, L.; Carbonnel, F.; Meyer, A. The effectiveness of either ustekinumab or vedolizumab in 239 patients with Crohn's disease refractory to anti-tumour necrosis factor. Aliment Pharmacol Ther 2020, 51, 948–957. [Google Scholar] [CrossRef]
- Lenti, M.V.; Levison, S.; Eliadou, E.; Willert, R.; Kemp, K.; Carter, A.; Stansfield, C.; Assadsangabi, A.; Singh, S.; Crooks, B.; et al. A real-world, long-term experience on effectiveness and safety of vedolizumab in adult patients with inflammatory bowel disease: The Cross Pennine study. Dig Liver Dis 2018, 50, 1299–1304.e2355. [Google Scholar] [CrossRef]
- Singh, S.; Kim, J.; Luo, J.; Paul, P.; Rudrapatna, V.; Park, S.; Zheng, K.; Syal, G.; Ha, C.; Fleshner, P.; et al. Comparative Safety and Effectiveness of Biologic Therapy for Crohn's Disease: A CA-IBD Cohort Study. Clin Gastroenterol Hepatol 2023, 21, 2359–2369. [Google Scholar] [CrossRef] [PubMed]
- Onali, S.; Pugliese, D.; Caprioli, F.A.; Orlando, A.; Biancone, L.; Nardone, O.M.; Imperatore, N.; Fiorino, G.; Cappello, M.; Viola, A.; et al. An Objective Comparison of Vedolizumab and Ustekinumab Effectiveness in Crohn's Disease Patients' Failure to TNF-Alpha Inhibitors. Am J Gastroenterol 2022, 117, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Kappelman, M.D.; Adimadhyam, S.; Hou, L.; Wolfe, A.E.; Smith, S.; Simon, A.L.; Moyneur, E.; Reynolds, J.S.; Toh, S.; Dobes, A.; et al. Real-World Evidence Comparing Vedolizumab and Ustekinumab in Antitumor Necrosis Factor-Experienced Patients With Crohn's Disease. Am J Gastroenterol 2023, 118, 674–684. [Google Scholar] [CrossRef]
- Johnson, A.M.; Barsky, M.; Ahmed, W.; Zullow, S.; Galati, J.; Jairath, V.; Narula, N.; Peerani, F.; Click, B.H.; Coburn, E.S.; et al. The Real-World Effectiveness and Safety of Ustekinumab in the Treatment of Crohn's Disease: Results From the SUCCESS Consortium. Am J Gastroenterol 2023, 118, 317–328. [Google Scholar] [CrossRef]
- Monin, L.; Dubois, S.; Reenaers, C.; Van Kemseke, C.; Latour, P.; Van Daele, D.; Vieujean, S.; Seidel, L.; Louis, E. Ustekinumab in bio-naive and bio-failure Crohn's disease patients: Results from a << real-life >> monocentric cohort. Dig Liver Dis 2021, 53, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Valdés Delgado, T.; Olmedo Martín, R.; Iborra, M.; Herrera de Guisé, C.; Fuentes-Valenzuela, E.; Melcarne, L.; Martín-Rodríguez, M.; Kolle Casso, L.; De Castro Parga, L.; Ponferrada Díaz, A.; et al. Effectiveness and safety of ustekinumab in bio-naive Crohn's disease patients: a multicentre observational retrospective study. Therap Adv Gastroenterol 2023, 16, 17562848231153560. [Google Scholar] [CrossRef]
- Sedano, R.; Guizzetti, L.; McDonald, C.; Beaton, M.; Chande, N.; Gregor, J.; Sey, M.; Wilson, A.; Jairath, V. Clinical, Endoscopic, and Radiological Effectiveness of Ustekinumab in Bio-naive Versus Bio-experienced Patients With Crohn's Disease: Real-world Experience From a Large Canadian Center. Inflamm Bowel Dis 2023, 29, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Rivière, P.; Kanters, C.; Pellet, G.; Ni, A.; Hupe, M.; Aboulhamid, N.; Poullenot, F.; Bitton, A.; Zerbib, F.; Lakatos, P.L.; et al. Comparative Effectiveness of Ustekinumab and Anti-TNF Agent as First-Line Biological Therapy in Luminal Crohn's Disease: A Retrospective Study From 2 Referral Centers. Inflamm Bowel Dis 2023, 29, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Zhdanava, M.; Ding, Z.; Manceur, A.M.; Muser, E.; Lefebvre, P.; Holiday, C.; Lafeuille, M.H.; Pilon, D. Treatment persistence among bio-naive patients with Crohn's disease initiated on ustekinumab or adalimumab. Curr Med Res Opin 2023, 39, 533–543. [Google Scholar] [CrossRef]
- Moens, A.; Alsoud, D.; Verstockt, B.; Sabino, J.; Ferrante, M.; Vermeire, S. Adalimumab versus ustekinumab as first-line biological in moderate-to-severe Crohn's disease: real-life cohort from a tertiary referral center. Eur J Gastroenterol Hepatol 2022, 34, 1015–1020. [Google Scholar] [CrossRef]
- Afif, W.; Arasaradnam, R.P.; Abreu, M.T.; Danese, S.; Sandborn, W.J.; Miao, Y.; Zhang, H.; Panaccione, R.; Hisamatsu, T.; Scherl, E.J.; et al. Efficacy and Safety of Ustekinumab for Ulcerative Colitis Through 4 Years: Final Results of the UNIFI Long-term Maintenance Study. Am J Gastroenterol 2023. [Google Scholar] [CrossRef]
- Iborra, M.; Ferreiro-Iglesias, R.; Maria Dolores, M.A.; Mesonero Gismero, F.; Minguez, A.; Porto-Silva, S.; Garcia-Ramirez, L.; Garcia de la Filia, I.; Aguas, M.; Nieto-Garcia, L.; et al. Real-world long-term effectiveness of ustekinumab in ulcerative colitis: results from a spanish open-label cohort. Scand J Gastroenterol 2023, 1–9. [Google Scholar] [CrossRef]
- Taxonera, C.; Olivares, D.; Lopez-Garcia, O.N.; Alba, C. Meta-analysis: Real-world effectiveness and safety of ustekinumab in patients with ulcerative colitis. Aliment Pharmacol Ther 2023, 57, 610–619. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Parody-Rua, E.; Chaparro, M. Efficacy, Effectiveness, and Safety of Ustekinumab for the Treatment of Ulcerative Colitis: A Systematic Review. Inflamm Bowel Dis 2023. [Google Scholar] [CrossRef]
- Shehab, M.; Alrashed, F.; Heron, V.; Restellini, S.; Bessissow, T. Comparative Efficacy of Biologic Therapies for Inducing Response and Remission in Fistulizing Crohn's Disease: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Inflamm Bowel Dis 2023, 29, 367–375. [Google Scholar] [CrossRef]
- Gionchetti, P.; Dignass, A.; Danese, S.; Magro Dias, F.J.; Rogler, G.; Lakatos, P.L.; Adamina, M.; Ardizzone, S.; Buskens, C.J.; Sebastian, S.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn's Disease 2016: Part 2: Surgical Management and Special Situations. J Crohns Colitis 2017, 11, 135–149.e27. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Van Assche, G.; Gomez-Ulloa, D.; Garcia-Alvarez, L.; Lara, N.; Black, C.M.; Kachroo, S. Systematic Review of Tumor Necrosis Factor Antagonists in Extraintestinal Manifestations in Inflammatory Bowel Disease. Clin Gastroenterol Hepatol 2017, 15, 25–36.e27. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Mocci, G.; Maconi, G. Effect of Ustekinumab on Extraintestinal Diseases in Refractory Crohn's Disease. J Crohns Colitis 2021, 15, 1399–1400. [Google Scholar] [CrossRef]
- Livne-Margolin, M.; Ling, D.; Attia-Konyo, S.; Abitbol, C.M.; Haj-Natour, O.; Ungar, B.; Ben-Horin, S.; Kopylov, U. Ustekinumab and vedolizumab for extraintestinal manifestations in inflammatory bowel disease - a retrospective study. Dig Liver Dis 2023, 55, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Privitera, G.; Pugliese, D.; Onali, S.; Petito, V.; Scaldaferri, F.; Gasbarrini, A.; Danese, S.; Armuzzi, A. Combination therapy in inflammatory bowel disease - from traditional immunosuppressors towards the new paradigm of dual targeted therapy. Autoimmun Rev 2021, 20, 102832. [Google Scholar] [CrossRef]
- McCormack, M.D.; Wahedna, N.A.; Aldulaimi, D.; Hawker, P. Emerging role of dual biologic therapy for the treatment of inflammatory bowel disease. World J Clin Cases 2023, 11, 2621–2630. [Google Scholar] [CrossRef] [PubMed]
- Berinstein, E.M.; Sheehan, J.L.; Jacob, J.; Steiner, C.A.; Stidham, R.W.; Shannon, C.; Bishu, S.; Levine, J.; Cohen-Mekelburg, S.A.; Waljee, A.K.; et al. Efficacy and Safety of Dual Targeted Therapy for Partially or Non-responsive Inflammatory Bowel Disease: A Systematic Review of the Literature. Dig Dis Sci 2023, 68, 2604–2623. [Google Scholar] [CrossRef]
- Targownik, L.E.; Singh, H.; Nugent, Z.; Bernstein, C.N. The epidemiology of colectomy in ulcerative colitis: results from a population-based cohort. Am J Gastroenterol 2012, 107, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- Solberg, I.C.; Lygren, I.; Jahnsen, J.; Aadland, E.; Hoie, O.; Cvancarova, M.; Bernklev, T.; Henriksen, M.; Sauar, J.; Vatn, M.H.; et al. Clinical course during the first 10 years of ulcerative colitis: results from a population-based inception cohort (IBSEN Study). Scand J Gastroenterol 2009, 44, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J Crohns Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Shen, B. Pouchitis: what every gastroenterologist needs to know. Clin Gastroenterol Hepatol 2013, 11, 1538–1549. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, M.; Declerck, S.; De Hertogh, G.; Van Assche, G.; Geboes, K.; Rutgeerts, P.; Penninckx, F.; Vermeire, S.; D'Hoore, A. Outcome after proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis. Inflamm Bowel Dis 2008, 14, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Dalal, R.L.; Shen, B.; Schwartz, D.A. Management of Pouchitis and Other Common Complications of the Pouch. Inflamm Bowel Dis 2018, 24, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Bar, F.; Kuhbacher, T.; Dietrich, N.A.; Krause, T.; Stallmach, A.; Teich, N.; Schreiber, S.; Walldorf, J.; Schmelz, R.; Buning, C.; et al. Vedolizumab in the treatment of chronic, antibiotic-dependent or refractory pouchitis. Aliment Pharmacol Ther 2018, 47, 581–587. [Google Scholar] [CrossRef]
- Huguet, M.; Pereira, B.; Goutte, M.; Goutorbe, F.; Dubois, A.; Bommelaer, G.; Buisson, A. Systematic Review With Meta-Analysis: Anti-TNF Therapy in Refractory Pouchitis and Crohn's Disease-Like Complications of the Pouch After Ileal Pouch-Anal Anastomosis Following Colectomy for Ulcerative Colitis. Inflamm Bowel Dis 2018, 24, 261–268. [Google Scholar] [CrossRef]
- Godoy-Brewer, G.; Salem, G.; Limketkai, B.; Selaru, F.M.; Grossen, A.; Policarpo, T.; Haq, Z.; Parian, A.M. Use of Biologics for the Treatment of Inflammatory Conditions of the Pouch: A Systematic Review. J Clin Gastroenterol 2024, 58, 183–194. [Google Scholar] [CrossRef]
- Dalal, R.S.; Gupta, S.; Goodrick, H.; Mitri, J.; Allegretti, J.R. Outcomes of Standard and Intensified Dosing of Ustekinumab for Chronic Pouch Disorders. Inflamm Bowel Dis 2022, 28, 146–149. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Chaparro, M. Safety of New Biologics (Vedolizumab and Ustekinumab) and Small Molecules (Tofacitinib) During Pregnancy: A Review. Drugs 2020, 80, 1085–1100. [Google Scholar] [CrossRef] [PubMed]
- Klenske, E.; Osaba, L.; Nagore, D.; Rath, T.; Neurath, M.F.; Atreya, R. Drug Levels in the Maternal Serum, Cord Blood and Breast Milk of a Ustekinumab-Treated Patient with Crohn's Disease. J Crohns Colitis 2019, 13, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Gorodensky, J.H.; Bernatsky, S.; Afif, W.; Filion, K.B.; Vinet, E. Ustekinumab Safety in Pregnancy: A Comprehensive Review. Arthritis Care Res (Hoboken) 2023, 75, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Wils, P.; Seksik, P.; Stefanescu, C.; Nancey, S.; Allez, M.; Pineton de Chambrun, G.; Altwegg, R.; Gilletta, C.; Vuitton, L.; Viennot, S.; et al. Safety of ustekinumab or vedolizumab in pregnant inflammatory bowel disease patients: a multicentre cohort study. Aliment Pharmacol Ther 2021, 53, 460–470. [Google Scholar] [CrossRef]
- Chaparro, M.; Gutiérrez, A.; Calviño-Suárez, C.; Huguet, J.M.; Calvo, M.; Aguas, M.; Camargo Camero, R.; de Jorge Turrión, M.A.; Hervías Cruz, D.; López Serrano, P.; et al. Safety of ustekinumab in pregnant patients with inflammatory bowel disease and in their offspring: results from the DUMBO registry of GETECCU. Journal of Crohn's and Colitis 2021, 16. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



