
Submitted:
21 January 2024
Posted:
22 January 2024
You are already at the latest version
Abstract
High insertion torques increase the primary stability of dental implants, which might be beneficial for immediate loading protocols, but may lead to local ischemia and necrosis of the bone-implant interface. This study compared the outcomes of implants placed with low (<45Ncm), conventional(45-70Ncm), and high (≥75Ncm) insertion torques in All-on-4 concept cases with up to 2-year follow-up. Patients included in this study presented edentulous or partially dentate arches with an indication for full-arch rehabilitation. Implants were installed following the All on four protocol and were divided into 3 groups: Low, Conventional, and High torque, and were followed periodically for 2 years with ISQ measurements. The results showed no significant differences in success rates between the three groups. This suggests that high insertion torques may maintain higher primary stability values for immediately loaded implants during the healing period. Further studies are necessary to confirm these findings.
Keywords:
Dental implants
; primary stability
; insertion torques
; tilted implants
1. Introduction
Treatment protocols using osseointegrated implants have been widely used as an alternative treatment for oral rehabilitation of partially or totally edentulous patients with high success rates [1]. The original protocol for a well-succeeded installation of an osseointegrated implant includes the utilization of a biocompatible implant, atraumatic surgical techniques, and a healing period free of mechanical loading for at least three months. Mechanical factors could influence the bone-implant interface, leading to fibrous encapsulation instead of direct bone healing on this interface [2].
However, over the last years, functional loading of implants immediately after their placement has been used with high success rates in both arches [3]. This procedure reduces the number of surgical interventions, thus reducing the treatment time between surgical and prosthetic phases. Immediate loading was defined as the placement of an interim implant-supported structure up to 48 hours after implant insertion [4]. This procedure is often used in full-arch implant-supported rehabilitation with great long-term results [5].
The concept of micromovement threshold has been suggested, describing two types of movements on the bone-implant interface: macro movements and micromovement. While micromovements should not harm the direct bone-implant contact, macro movements could prevent this direct contact, resulting in fibrous interposition. For dental implants, this critical micromovement threshold has been demonstrated to be situated between 50 - 150µm, or a fibrous interface may be formed around the implant, resulting in implant failure [6]. The success of the implants, thus, is not related to immediate or delayed loading but instead to the micromovement threshold, which should not exceed 50 - 100µm at the interface [6].
High primary stability of the implant and the maintenance of that stability within the tolerable threshold are primary concerns during the healing period of immediately loaded implants. Considering that there are no direct measuring methods of micromovements in the bone-implant interface, indirect methods that evaluate the insertion torque values (ITV) and the implant stability quotient (ISQ) are the most common clinical methods to assess the primary stability of the implant for a predictable immediate loading protocol [7]. The value of the final insertion torque is the most used clinical parameter to assess primary stability: the peak of the insertion torque is directly related to the degree of micromovement: higher insertion torques provide more bone compression on the interface and thus, higher primary stability [8].
Nevertheless, the parameter of the minimum torque value for a safe, immediate loading protocol still needs to be well established. However, some authors report that torque values over 32Ncm indicate sufficient primary stability for that purpose [9,10].
There still needs to be more clinical data to ensure that high insertion torques provide a clinical advantage. The idea that excessive bone compression due to high insertion torques could lead to local ischemia and necrosis of the bone-implant interface has been reported in previous studies [1,11,12]. Sub-instrumentation, or undersized drilling, is a concept based on an osteotomy preparation that is smaller in diameter than the size of the implant, is also used to increase primary stability of implants. But this technique for bone instrumentation of an implant site could also present a clinical limitation: at some point, the insertion torque would be too high, and the biological damage would result in peri-implant bone necrosis [13]. According to this hypothesis, excessive torque values above 50Ncm could result in high-stress transmission to the adjacent bone, resulting in osseointegration failure [9].
The growing interest in immediate loading protocols and consequentially, the need for high primary stability levels through high insertion torques have increased the need to confirm that the compression necrosis hypothesis reported in the articles mentioned above could be scientifically demonstrated. Some studies have pointedly questioned compression necrosis hypothesis [14,15]. Although this hypothesis has been widely accepted in the literature, no study has been published confirming it [16]. An animal study [14] investigated the effect of high insertion torque (110Ncm mean – 150Ncm peak) on the osseointegration of unloaded implants. No implants failed during the study, and the authors concluded that these high insertions torque did not induce bone necrosis or implant failure; it was suggested that improving the primary stability of the implants could be relevant for immediate loading protocols.
Another human study [15] analyzed the clinical results of implants installed with high insertion torques over 70Ncm (110,6 mean – 176 peaks), and evaluated marginal bone levels around the implants. None of the implants failed during the follow-up period. The authors concluded that high insertion torques (up to 176Ncm) did not prevent osseointegration or affected marginal bone levels around the implants. Three other human studies that stated that high torque would be the ones higher than 50Ncm showed results comparable between implants placed with high or low torques in terms of implant survival [17,18,19], but two of them concluded that higher torque evidenced higher bone loss around these implants [17,18].
The literature on the effects of high insertion torques on the osseointegration of implants in vivo is still scarce, there are still many doubts about the possible injuries that these high torques could cause to local bone. This preliminary 2-year clinical prospective controlled case series study aimed to assess the effects of high insertion torque on the osseointegration of dental implants with All-on-four treatment protocols.
2. Materials and Methods
Pre-Surgical Evaluation
The study was conducted according to the declaration of Helsinki and approved by the Guarulhos University’s Ethics Committee in Clinical Research (IRB: 61544116.7.0000.5506), and involved patients presented for full arch rehabilitation treatment in the Guarulhos University (UnG, Guarulhos, SP, Brazil) from January 2017 to October 2017. All patients in this study showed completely or partially edentulous arches with remaining teeth indicated for extraction (maxilla and/or mandible). The indications for extraction in partially dentate included: longitudinal fractures, periodontal disease, endodontic failure, perforated roots, or prosthetic convenience. The inclusion criteria were: the need for full-arch rehabilitation with a completely fixed implant-supported prosthesis; adequate bone volume for implant installation. The patient’s ability and willingness to follow the study protocol; a good state of general health.
Bone volume was assessed using radiographic and tomographic measurements. The degree of bone resorption for inclusion in this study should be Division A or B, as suggested by Misch (1990) [20]. The volume of the maxillary and mandibular bone for inclusion in this study should be Division A, B, or Bw, as suggested by Misch and Judy (1987) [21]. The premaxillary and inter-foraminal bone height should be enough to allow the placement of two tilted distal implants with a minimum length of 13mm, and two axial anterior implants with a minimum length of 10mm, according to the All-on-4 protocol [22,23]. Patients that did not present these bone dimensions were excluded. The exclusion criteria were: inadequate bone volume, general and local health conditions that prevented the use of local anesthesia and/or intraoral surgery. General conditions that could lead to osseointegration problems, such as patients in the use of bisphosphonates for osteoporosis treatment; parafunctional habits, such as bruxism. Smoking was not used as an exclusion criterion.
All possible treatment options were offered to the patients. Patients enrolled in the study chose and authorized the procedure by signing a consent form according to the Helsinki Declaration (1975, revised in 2000). Diagnosis and treatment planning included: study models articulated in a semi-adjustable articulator, clinical photographs, panoramic radiographs (Figure 1), and cone bean computerized tomography to identify the anatomical structures and visualize the presence of pathology. After the project of the oral rehabilitation was ready, a multifunctional guide to determine the best implant placement positions was fabricated.
Surgical Protocol
Patients were medicated with 2 grams of amoxicillin intraorally 2 hours before the surgical procedure. None of the enrolled patients were allergic to penicillin. Immediately before surgery, patients rinsed with 2% chlorhexidine for 1 minute. All surgeries were performed by two very experienced surgeons (AC an TM). Local anesthesia was performed in all surgical procedures, with Articaine Chlorohydrate with adrenaline 1:100,000 (Figure 2). A supra-crestal incision was made up to the first molar region and two vertical releasing incisions in the first molar region. A mucoperiosteal flap was deflected, allowing the anatomical structures to be visualized (Figure 3). The drilling sequence for implant installation was performed according to the instructions of the implant manufacturer (Dérig, São Paulo, Brazil), following the All-on-4 protocol (Figure 4) [22,23]. During the bone instrumentation, sub-instrumentation was performed when the surgeon sensed by his experience that the implant sites would have poor bone density, to obtain the highest torque value possible in every site. This was decided by the surgeons upon their large experience on all on four treatments, in order to promote lateral compression of the bone, and thus, increase primary stability [13]. The implants used in this study were tapered, with a rough surface, internal tri-channel connection implants (TRI Bioneck RP ∅ 4.3mm, Dérig, São Paulo, Brazil) (Figure 5). The initial insertion of the implants was performed with the handpiece adjusted to an initial insertion torque of 45 Ncm. When the handpiece “stalled,” the implant was manually inserted with a custom-made torque wrench, which allowed measuring torques up to 200Ncm (Figure 6) until it was completely seated (Figure 7 and Figure 8). Maximum insertion torque values (ITV) and implant stability quotient (ISQ - Ostell, W&H, Gothenburg, Sweden) were recorded for each implant (Figure 9). Implants with ITV equal or higher than 75Ncm were included in the study for follow-up and measurements, while implants with ITV less than 75Ncm where not marked as interest in this study. Despite that, when all 4 implants reached torques equal to or greater than 45Ncm, immediate loading was performed. Straight multiunit abutments were tightened to the anterior implants with a 32 Ncm torque, and 17o or 30o angled multiunit abutments were drawn to the distal tilted implants with a 20Ncm torque. The surgical wounds were sutured with 4-0 silk thread after placing the abutments (Figure 10). If one or more implants in the arch did not reach an installation torque of 45Ncm, cover screws were installed over the implants, and primary wound closure was performed with a 4-0 silk thread. Patients were asked to rinse with 2% chlorhexidine 3 times daily after surgery. Amoxicillin 875 mg was prescribed two times a day for seven days. Ibuprofen 600mg was also prescribed twice daily for 5 days for pain control.
Prosthetic Protocol
All prostheses were planned and fabricated post-surgically. The implant-supported screw-retained prostheses were delivered in two different ways, varying according to the loading protocol, determined by the primary stability obtained during implant installation: immediate or delayed.
Immediate loading was performed in cases in which all four implants presented high primary stability, with installation torques over 45Ncm. Impressions of the implants and residual ridge were taken right after surgery using the multifunctional guide as an open-tray transfer, splinted with a low-shrinkage modeling resin (Pattern Resin, GC America Inc., USA). Only the putty soft addition silicon material (Futura AD, Nova DFL, Rio de Janeiro, Brazil) was used; no light body material was used to avoid penetration of the light material in the surgical wound, which could cause local irritation and further complications. On the next day the nickel-chromium metal bar, which had been made according to the position of the teeth in the multifunctional guide was tried and sent for mounting the teeth for patient’s approval. On the same day the esthetic appearance and maxillomandibular relations were proved. After dentist and patient approval, the prostheses were sent for full laboratory processing with acrylic. Installation and final occlusal adjustments of the full arch rehabilitation occurred 48 hours after surgery (Figure 11 and Figure 12).
Delayed loading was performed, in cases in which one or more implants did not reach 45Ncm. Throughout the 6 months of healing, patients wore conventional removable prostheses relined with a soft silicon liner (Ufi Gel, VOCO GmbH, Cuxhaven, Germany) to avoid contact of the acrylic with the submerged implants. Fixed prostheses were constructed after second-stage surgery, six months after the implant installation.
Follow-Up
Patients were followed up for two years after implant installation, according to the following appointment schedule: 7 days, 60 days, six months, 12 months, 18 months, and 24 months. The success criteria utilized in this study were as suggested by Misch (2008)- no mobility, no pain during function, less than 2mm of radiographic bone loss after initial surgery, and no history of exudates [24]. Implant clinical conditions were assessed in all follow-up appointments; patients were examined using periodontal probing, CT scans, radiographs (Figure 13), intra-and extra-oral photographs, and assessment of implant stability quotient (ISQ). All patients were instructed to use interdental brushes, dental floss, and an oral hygiene system based on high-pressure water spray twice a day for biofilm control. Professional control occurred at every follow-up appointment. Panoramic radiographs and CT scans were taken before and after surgery and at every follow-up appointment. The inspection in the follow-up appointments included assessment of oral hygiene, soft tissue health (peri-implant pockets, pain, and exudation), radiographic and tomographic aspects of the bone/implant interface, implant stability quotient (ISQ) measurements, screw loosening, and other possible complications.
3. Results
A total of 11 patients filled out the inclusion criteria for this study, 9 women and 2 men, with a mean age of 56. A total of 19 All-on-four treatments and 76 implants were placed, 10 in the maxilla (40 implants) and 9 in the mandible (36 implants). In 6 cases, the immediate load was performed in the maxilla, but with only 14 implants achieving 75 Ncm or more between these 6 patients, and in all 9 mandibles treatments it was possible to perform immediate load, with 29 implants achieving 75 Ncm or more between all 9 patients. A total of 43 implants were then selected to be analyzed in this study. No implants in this study were lost, neither on immediate nor delayed load treatment, i.e., independent of the insertion torque value, all implants survived till the last appointment. Initial Torque Values from the implants analyzed in this study (n=43) varied from 75Ncm to even more than 120Ncm; 14 in the maxilla and 29 in the mandible. 3 implants reached 150Ncm, 4 implants reached 180Ncm, and 2 implants achieved 200Ncm, all in the mandible. Although bone loss around the implant's neck was not a parameter measured in this study, radiographically, we could see there was no significant bone loss in none of the implants. Sub-instrumentation was performed in all maxilla instrumentation and in 6 of the 9 mandible cases and may have helped reach these higher insertion torque values.
Smoking habits seemed to have no influence on the survival of the implants. Three patients were light smokers (≤ 10 cigarettes a day), and 8 were non-smokers.
Table 1 shows the comparison of the ISQ measurement in the maxilla from the time of placement of the implants (initial) and the seven days, 7 to 60 days, means, from primary to secondary stability (osseointegration), and from the time of placement till the last follow-up, 24 months in 6 maxilla cases, and 12 months in 4 patients. Table 2 shows the comparison of the ISQ measurements in the mandible from the time of placement of the implants (initial) and the 7 days, 7 to 60 days, it means, from primary to secondary stability (osseointegration), and from the time of placement till the last follow-up, 24 months in 4 mandible cases, and 12 months in 4 cases. The Student`T test was used to determine if there is an association between the initial torque value (ITV) and the implant stability quotient (ISQ) at the initial and during the healing period (p<0,05). In maxilla treatment, only the recovery period (7-60 days) showed significance, and in mandible treatment, we always see a statistical difference.
4. Discussion
The primary stability of dental implants is defined as the capacity of the implant to resist axial, lateral, and rotational loads [8]. It is of utmost importance, especially for immediate loading protocols. In this study, we found 100% success in All-on-four protocols with immediate load and initial high torque regarding the region of the implant placed. The success of immediate loading has been well demonstrated in the literature; however, the stiffness of the assembly bone/implant/crown must be ensured to promote a predictable result [14,25,26]. Some factors influence the primary stability of an implant during installation. The first one is bone density; the mechanical properties of the bone are determined by its local composition. Implants installed in dense cortical bone present higher primary stability than implants placed in cancellous bone. The second factor is the role of the compressive stresses in the bone-implant interface: using a final bur of smaller diameter than the implant, a procedure known as sub-instrumentation of the implant site, results in significant compression of the local bone, resulting in radial stresses that can be beneficial to increase the primary stability of the implant [13]. Sub-instrumentation of the implant site provides an increase of the force moment necessary to install the implant in position. This force moment is referred to as the insertion torque. Increasing the insertion torque makes it possible to increase implant primary stability [1,14,15,27]. Some of the implants placed in the maxilla could even reach values higher than 100Ncm when sub-instrumentation was performed, showing the importance of the technique in low-density bone. The third factor is the geometry of the implant; tapered implants present higher primary stability levels compared to cylindrical implants [28]. Surface roughness also appears to influence implant stability; rough surface implants seem to present higher primary stability than smooth surface implants [29]. From a clinical standpoint, sub-instrumentation of implant sites seems to provide better primary stability levels to implants, regardless of the local bone density [11].
In the present study, all implants were installed with the highest insertion torque possible, considering the aforementioned influence factors. In order to enhance the chances of obtaining a high insertion torque, conical implants with rough surfaces were used (TRI Bioneck RP ∅ 4.3mm, Dérig, São Paulo, Brazil), both for the maxilla and mandible. In sites with high-density bone, the preparation of the implant site followed the manufacturer’s recommendations. In sites with poor bone density, sub-instrumentation of the site was performed, in order to promote lateral compression of the bone, increasing primary stability.
The idea that excessive bone compression could result in local ischemia and bone necrosis has been widely reported; this necrosis could result in periapical lesions on the implants, which could demand treatment with diverse degrees of invasiveness, including the removal of the implant [1,11]. Compression necrosis is still a hypothesis [16]: if the bone is compressed over its physiological tolerance, it could result in local ischemia with subsequent necrosis or sequestrum formation, which could further lead to implant failure. Besides, excessive torque could transmit high stresses to the marginal bone around the implant, a dense cortical bone with minimum blood supply, more susceptible to necrosis after installation [9,11,12,13,17,18].
An animal study [30] made a histological analysis of the effects of high insertion torques on the adjacent bone, with torque values of 80, 120, and 150Ncm. None of these high torque levels resulted in the failure of the implants. The 150Ncm group showed high compression of the adjacent bone, whereas the 80Ncm group presented a significantly smaller compression; the compressed bone areas in all groups evolved to bone regeneration, with no signs of ischemia or necrosis. The authors concluded that different torque levels resulted in different initial healing patterns, but there was no significant difference in the final histological patterns. They also concluded that high insertion torques promote greater bone remodeling around the implants, but did not prevent osseointegration from occurring.
To the present date, there were no clinical prospective studies that managed to demonstrate the occurrence of compression necrosis due to high insertion torque. Two papers reported implant failure supposedly due to high insertion torque, but both papers were reported of single clinical cases [31,32]. Our study showed results on high torques for implants placed by the All on four concept, which may have higher stability than single implants. Other studies reported higher bone resorption around implants with high insertion torque [17,18,33,34,35,36]. On the other hand, several studies, among them animal models [14,30,37,38,39,40,41,42] and human studies [15,43,44,45,46,47,48,49,50,51] analyzed the outcomes of high insertion torques, most of them equal or greater than 70Ncm, with the same parameters used in the present study; all these studies reported no significant differences between conventional and high insertion torques regarding success rates and/or marginal bone levels. Also, systematic reviews with meta-analyses [52,53,54,55,56] have also been published about high insertion torques; they observed no significant difference in marginal bone resorption and implant failure rate between implants inserted with high, regular or low insertion torque values.
A systematic review with meta-analysis on immediately loaded implants following the All-on-4 protocol for full-arch rehabilitation [57] reported that 74% of the implant failures occurred during the first 12 months, which consists of the healing period. These findings suggest that the critical period for the success of immediately loaded implants for full-arch rehabilitation is the healing period, in which the secondary stability is not yet enough, secure the osseointegration of the implant. Thus, reaching and maintaining high primary stability values during the healing period, as suggested by the present study, could be a valuable approach for immediately loaded implants, in order to increase security in the critical phase in which most of the failures occur.
In the present study, a significant number of implants reached considerably high insertion torques (32 implants with ITV's over 100Ncm). With such high insertion torque values, high stresses were transmitted to the adjacent bone, and high compression was made both to cancellous and cortical bone, due to the conical geometry of the implants. No signs of ischemia or necrosis resulting from this compression could be clinically and/or radiographically confirmed in any of the implants analyzed. Although we found higher ISQ values at the implant placement in the mandible than in the maxilla, at the last control appointment, both arches demonstrated similar results, regardless of the torque group. No implants failed during the 2-year follow-up of this study, and there was no significant difference in the marginal bone levels around the implants. The results of the present study indicated that high insertion torque did not induce ischemia or necrosis of the adjacent bone, as seen on other studies [17,18,33,34,35,36]. Instead, it promoted radial compression of the marginal bone, increasing the primary stability of the implant, which could be particularly significant when considering immediate loading protocols. High insertion torques could reach and maintain higher primary stability for immediately loaded implants during the healing period, which could mean more security to these implants during the critical healing period before secondary stability is reached. The ISQ measurements showed a small deep in these implants placed with ITV ≥ 75Ncm in the maxilla, with a recovery to the similar values found at the time of implant placement. But in the mandible, where we could see the higher values, the deep between primary and secondary stability was more evident, similar to another clinical study on the mandible [18]. These findings corroborate with another human study that evidenced that initial high torque >50Ncm don’t resulted in higher secondary stability, with 12-month follow-up [58]. But even with this, the ISQ measures showed the recovery to values considered optimal to maintain osseointegration without problems, as it was seen during the control appointments, with no bone loss higher than expected, no mobility, and no pain during masticatory function or pressure test during the period of the follow-up. This result seems to endorse the hypothesis that ITV higher than 80Ncm may not be harmful to peri-implant bone or affect clinically the stability of the implants.
This study presented some limitations such as the small sample size that reached de minimum of 75Ncm to enter in the analysis and comprehensive short-term follow-up (< 5 years). Another limitation to be pointed is that we didn’t have a 30 days ISQ measurement, that could include an important data on the osseointegration process. In addition, this study showed an interesting clinical point of view on the behavior of dental implants placed under higher torques. Earlier studies [9,10,14,16] showed that the insertion torque ranging between 25 and 32Ncm was sufficient to achieve primary stability, however, these studies evaluated implant systems that presented a dental implant mounted that supported torque forces not higher than 32Ncm. Finally, we must point out that osseointegration occurs even in implants placed with low torque insertion (<20Ncm) and the idea that low or higher insertion torques influence the bone-to-implant contact and peri-implant bone-tissue behavior depends on several other clinical variables such as bone architecture, macro- and microgeometry of the implants, and distribution of the occlusal load.
5. Conclusions
The results of this 2-year prospective case series study showed 100% success rate in implants placed with high insertion torques by the All on Four Concept. These results suggest that high insertion torques could be used to reach and maintain higher primary stability values for immediately loaded implants during the healing period. However, further longitudinal studies (> 5 years) are necessary to confirm these results.
Author Contributions
“Conceptualization, A.C.; T.M. and J.A.S.; methodology, A.C.; T.M.; J.A.S.; software, T.M.; R.B.; I.R.; validation, A.C., J.A.S. and T.M.; formal analysis, R.B.;I.R.;M.C.F.; investigation, A.C.;T.M; resources, A.C.; data curation, M.C.F.; D.R.F; writing—original draft preparation, A.C.; writing—review and editing, M.C.F.; J.A.S; visualization, J.A.S.; supervision, J.A.S.; project administration, A.C.; funding acquisition, A.C. All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding”.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki, and approved by the University of Guarulhos Ethics Committee in Clinical Research protocol code IRB: 61544116.7.0000.5506”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.” “Written informed consent has been obtained from the patient(s) to publish this paper”.
Data Availability Statement
“The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request”.
Conflicts of Interest
“The authors declare no conflicts of interest”.
References
- Meridith, N. Assessment of implant stability as a prognostic determinant. Int J Prosthodont 1998, 11, 491–501. [Google Scholar]
- Szmukler-Monkler, S.; Salama, H.; Reingewirtz, Y.; Dubruille, J.H. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. J Biomed Mater Res 1998, 43, 192–203. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Testori, T.; Kekovic, V.; Goker, F.; Tumedei, M.; Wang, H.L. A Systematic Review of Survival Rates of Osseointegrated Implants in Fully and Partially Edentulous Patients Following Immediate Loading. Journal of Clinical Medicine 2019, 8, 2142. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, G.S.Y.; de Magalhães, K.M.F.; Rocha, E.P.; Dos Santos, P.H.; Assunção, W.G. Oral health-related quality of life and satisfaction in edentulous patients rehabilitated with implant-supported full dentures all-on-four concept: a systematic review. Clinical Oral Investigation 2022, 26, 83–94. [Google Scholar] [CrossRef]
- Agliardi, E.L.; Pozzi, A.; Romeo, D.; Del Fabbro, M. Clinical outcomes of full-arch immediate fixed prostheses supported by two axial and two tilted implants: A retrospective cohort study with 12-15 years of follow-up. Clin Oral Implants Res 2023, 34, 351–366. [Google Scholar] [CrossRef] [PubMed]
- Wazen, R.; Currey, J.; Guo, H.; Brunski, J.; Helms, J.; Nanci, A. Micromotion-induced strain fields influence early stages of repair at bone–implant interfaces. Acta Biomater 2013, 9, 6663–6674. [Google Scholar] [CrossRef]
- Lee, J.; Pyo, S.W.; Cho, H.J.; An, J.S.; Lee, J.H.; Koo, K.T.; Lee, Y.M. Comparison of implant stability measurements between a resonance frequency analysis device and a modified damping capacity analysis device: An in vitro study. J Periodontal Implant Sci 2020, 50, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A Narrative Review of the Histological and Histomorphometrical Evaluation of the Peri-Implant Bone in Loaded and Unloaded Dental Implants. A 30-Year Experience (1988–2018). Int J Environ Res Public Health 2020, 17, 2088. [Google Scholar] [CrossRef] [PubMed]
- Sotto-Maior, B.S.; Rocha, E.P.; Almeida, E.O.; Freitas-Júnior, A.C.; Anchieta, R.B.; Del Bel Cury, A.A. Influence of high insertion torque on implant placement – an anisotropic bone stress analysis. Braz Dent J 2010, 21, 508–514. [Google Scholar] [CrossRef]
- Dos Santos, M.V.; Elias, C.N.; Lima, J.H.C. The effects of superficial roughness and design on the primary stability of dental implants. Clin Implant Dent Relat Res 2011, 13, 215–223. [Google Scholar] [CrossRef]
- Gonzáles-Martín, O.; Lee, E.A.; Veltri, M. CBCT fractal dimension changes at the Apex of immediate implants placed using undersized drilling. Clin Oral Impl Res 2012, 23, 954–957. [Google Scholar] [CrossRef] [PubMed]
- Isoda, K.; Ayukawa, Y.; Tsukiyama, Y.; Sogo, M.; Matsushita, Y.; Koyano, K. Relationship between the Bone Density Estimated by Cone-Beam Computed Tomography and the Primary Stability of Dental Implants: Relationship between Bone Density and Implant Stability. Clin Oral Implant Res 2012, 23, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Jimbo, R.; Tovar, N.; Anchieta, R.B.; Machado, L.S.; Marin, C.; Teixeira, H.S.; Coelho, P.G. The combined effects of undersized drilling and implant macrogeometry on bone healing around dental implants: an experimental study. Int J Oral Maxillofac Surg 2014, 43, 1269–75. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Todisco, M.; Consolo, U.; Travaglini, D. High versus low implant insertion torque: a histologic, histomorphometric, and biomechanical study in the sheep mandible. Int J Oral Maxillofac Implants 2011, 26, 837–849. [Google Scholar]
- Khayat, P.G.; Arnal, H.M.; Tourbah, B.I.; Sennerby, L. Clinical outcome of dental implants placed with high insertion torques (up to 176Ncm). Clin Implant Dent Relat Res 2013, 15, 227–233. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J. Implant insertion torque: its role in achieving primary stability of restorable dental implants. Compend Contin Educ Dent 2017, 38, 88–95. [Google Scholar] [PubMed]
- Aldahlawi, S.; Demeter, A.; Irinakis, T. The effect of implant placement torque on crestal bone remodeling after 1 year of loading. Clinical, Cosmetic and Investigational Dentistry 2018, 10, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Dahdal, S.; Alkhori, I.; Shihabi, S. Evaluation of the effectiveness of high insertion torques on implant stability quotient(ISQ) and marginal bone loss of implants in posterior mandible. Int J Dentistry Oral Sci 2021, 8, 4887–4891. [Google Scholar]
- Elbeialy, R.R.; El-Beialy, W.R. Outcome of dental implants placed with high insertion torque. Egyptian Dental Journal 2017, 63, 299–306. [Google Scholar] [CrossRef]
- Misch, C. Classifications and treatment options of the completely edentulous arch in implant dentistry. Dent Today 1990, 9, 26, 28–30. [Google Scholar]
- Misch, C.E.; Judy, K.W. Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol 1987, 4, 7–13. [Google Scholar]
- Malo, P.; Rangert, B.; Nobre, M. “All-on-Four” immediate-function concept with Branemark system implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res 2003, 5, 2–9. [Google Scholar] [CrossRef]
- Malo, P.; Rangert, B.; Nobre, M. All-on-4 immediate-function concept with Brånemark system implants for completely edentulous maxillae: a 1-year retrospective clinical study. Clin Implant Dent Relat Res 2005, 5, S88–S94. [Google Scholar] [CrossRef]
- Misch, C.E.; Perel, M.L.; Wang, H.L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; Schwartz-Arad, D.; Choukroun, J.; Gutierrez-Perez, J.L.; Marenzi, G.; Valavanis, D.K. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Daprile, G.; Piatelli, A. Determination of primary stability: a comparison of the surgeon’s perception and objective measurements. Int J Oral Maxillofac Implants 2010, 25, 558–561. [Google Scholar] [PubMed]
- Degidi, M.; Daprile, G.; Piatelli, A.; Iezzi, G. Development of a new implant primary stability parameter: insertion torque revisited. Clin Implant Dent Relat Res 2013, 15, 637–644. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, D.; Sennerby, L.; Meredith, N. Measurements comparing the initial stability of five designs of dental implants: a human cadaver study. Clin Impl Dent Relat Res 2000, 2, 85–92. [Google Scholar] [CrossRef]
- Bartold, P.M.; Kuliwaba, J.S.; Lee, V.; Shah, S.; Marino, V.; Fazzalari, N.L. Influence of surface roughness and shape on microdamage of the osseous surface adjacent to titanium dental implants. Clin Oral Impl Res 2011, 22, 613–618. [Google Scholar] [CrossRef]
- Javed, F.; Almas, K.; Crespi, R.; Romanos, G.E. Implant surface morphology and primary stability: is there a connection? Implant Dent 2011, 20, 40–46. [Google Scholar] [CrossRef]
- Campos, F.E.; Gomes, J.B.; Marin, C.; Teixeira, H.S.; Suzuki, M.; Witek, L.; Zanetta-Barbosa, D.; Coelho, P.G. Effect of drilling dimension on implant placement torque and early osseointegration stages: an experimental study in dogs. J Oral Maxillofac Surg 2012, 70, e43–50. [Google Scholar] [CrossRef]
- Piatelli, A.; Scarano, A.; Balleri, P.; Favero, G.A. Clinical and histological evaluation of an active “implant periapical lesion”. A case report. Int J Oral Maxillofac Implants 1998, 13, 713–716. [Google Scholar]
- Bashutski, J.D.; D'Silva, N.J.; Wang, H.L. Implant compression necrosis: current understanding and case report. J Periodontol 2009, 80, 700–704. [Google Scholar] [CrossRef]
- Duyck, J.; Corpas, L.; Vermeiren, S.; Ogawa, T.; Quirynen, M.; Vandamme, K.; Jacobs, R.; Naert, I. Histological, histomorphometrical, and radiological evaluation of an experimental implant design with a high insertion torque. Clin Oral Impl Res 2010, 21, 877–884. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Cochran, D.; Obrecht, M.; Pippenger, B.E.; Dard, M. Effect of Osteotomy preparation on osseointegration of immediately loaded, tapered dental implants. Adv Dent Res 2016, 28, 34–41. [Google Scholar] [CrossRef]
- Barone, A.; Alfonsi, F.; Derchi, G.; Tonelli, P.; Toti, P.; Marchionni, S.; Covani, U. The effect of insertion torque on the clinical outcome of single implants: a randomized clinical trial. Clin Implant Dent Relat Res 2016, 18, 588–600. [Google Scholar] [CrossRef]
- Marconcini, S.; Giammarinaro, E.; Toti, P.; Alfonsi, F.; Covani, U.; Barone, A. Longitudinal analysis on the effect of insertion torque on delayed single implants: A 3-year randomized clinical study. Clin Implant Dent Relat Res 201, ;20, 322-332.
- Warreth, A.; Polyois, J.; Lee, C.T.; Claffey, N. Generation of microdamage around endosseous implants. Clin Oral Impl Res 2009, 20, 1300–1306. [Google Scholar] [CrossRef]
- Consolo, U.; Travaglini, D.; Todisco, M.; Trisi, P.; Galli, S. Histologic and biomechanical evaluation of the effects of implant insertion torque on peri-implant bone healing. J Craniofac Surg 2013, 24, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Rea, M.; Botticelli, D.; Ricci, S.; Soldini, C.; Gonzáles, G.G.; Lang, N.P. Influence of immediate loading on healing of implants installed with different insertion torques – an experimental study in dogs. Clin Oral Impl Res 2015, 26, 90–95. [Google Scholar] [CrossRef]
- Duyck, J.; Roesems, R.; Cardoso, M.V.; Ogawa, T.; De Villa Camargos, G.; Vandamme, K. Effect of insertion torque on titanium implant osseointegration: an animal experimental study. Clin Oral Implants Res 2015, 26, 191–196. [Google Scholar] [CrossRef]
- Eom, T.G.; Kim, H.W.; Jeon, G.R.; Yun, M.J.; Huh, J.B.; Jeong, CM. Effects of different Implant dsteotomy dreparation sizes on implant stability and bone response in the minipig mandible. Int J Oral Maxillofac Implants 2016, 31, 997–1006. [Google Scholar] [CrossRef]
- Muktadar, A.K.; Gangaiah, M.; Chrcanovic, B.R.; Chowdhary, R. Evaluation of the effect of self-cutting and nonself-cutting thread designed implant with different thread depth on variable insertion torques: An histomorphometric analysis in rabbits. Clin Implant Dent Relat Res 2018, 20, 507–514. [Google Scholar] [CrossRef]
- Simunek, A.; Strnad, J.; Kopecka, D.; Brazda, T.; Pilathadka, S.; Chauhan, R.; Slezak, R.; Capek, L. Changes ins stability after healing of immediately loaded dental implants. Int J Oral Maxillofac Implants 2010, 25, 1085–1092. [Google Scholar]
- Gonzáles-Martin, O.; Lee, E.A.; Veltri, M. CBTC fractal dimension changes at the apex of immediate implants placed using undersized drilling. Clin Oral Impl Res 2012, 23, 954–957. [Google Scholar] [CrossRef]
- Makary, C.; Rebaudi, A.; Mokbel, N.; Naaman, N. Peak insertion torque correlated to histologically and clinically evaluated bone density. Implant Dent 2011, 20, 182–191. [Google Scholar] [CrossRef]
- Canizzaro, G.; Leone, M.; Ferri, V.; Viola, P.; Federico, G.; Esposito, M. Immediate loading of single implants inserted flapless with medium or high insertion torque: a 6-month follow-up of a split-mouth randomized controlled trial. Eur J Oral Implantol 2012, 5, 333–342. [Google Scholar]
- Grandi, T.; Garuti, G.; Samarani, R.; Guazzi, P.; Forabosco, A. Immediate loading of single post-extractive implants in the anterior maxilla: 12-month results from a multicenter clinical study. J Oral Implantol 2012, 38, 477–484. [Google Scholar] [CrossRef]
- Grandi, T.; Guazzi, P.; Samarani, R.; Grandi, G. Clinical outcome and bone healing of implants placed with high insertion torque: 12-month results from a multicenter controlled cohort study. Int J Oral Maxillofac Surg 2013, 42, 516–520. [Google Scholar] [CrossRef]
- Bidgoli, M.; Soheilifar, S.; Faradmal, J.; Soheilifar, S. High insertion torque and peri-implant bone loss: Is there a relationship? J Long Term Eff Med Implants 2015, 25, 209–213. [Google Scholar] [CrossRef]
- De Santis, D.; Cucchi, A.; Rigoni, G.; Longhi, C.; Nocini, P.F. Relationship between primary stability and crestal bone loss of implants placed with high insertion torque: A 3-Year prospective study. Int J Oral Maxillofac Implants 2016, 31, 1126–1134. [Google Scholar] [CrossRef]
- Makary, C.; Menhall, A.; Zammarie, C.; Lombardi, T.; Lee, S.Y.; Stacchi, C.; Park, K.B. Primary stability optimization by using fixtures with different thread depth according to bone density: a clinical prospective study on early loaded implants. Materials (Basel) 2019, 12, 2398. [Google Scholar] [CrossRef]
- Berardini, M.; Trisi, P.; Sinajari, B.; Rutjes, A.W.S.; Caputi, S. The effects of high insertion torque versus low insertion torque on marginal bone resorption and implant failure rates: a systematic review with meta-analyses. Implant Dent 2016, 25, 532–540. [Google Scholar] [CrossRef]
- Li, H.; Liang, Y.; Zheng, Q. Meta-analysis of correlations between marginal bone resorption and high insertion torque of dental implants. Int J Oral Maxillofac Implants 2015, 30, 767–72. [Google Scholar] [CrossRef]
- Lemos, C.A.A.; Verri, F.R.; de Oliveira Neto, O.B.; Cruz, R.S.; Luna Gomes, J.M.; da Silva Casado, B.G.; Pellizzer, E.P. Clinical effect of the high insertion torque on dental implants: A systematic review and meta-analysis. J Prosthet Dent 2021, 126, 490–496. [Google Scholar] [CrossRef]
- Atieh, MA.; Baqain, Z.H.; Tawse-Smith, A.; Ma, S.; Almoselli, M.; Lin, L.; Alsabeeha, N.H.M. The influence of insertion torque values on the failure and complication rates of dental implants: A systematic review and meta-analysis. Clin Implant Dent Relat Res. 2021, 23, 341–360. [Google Scholar] [CrossRef]
- Roca-Millan, E.; González-Navarro, B.; Domínguez-Mínger, J.; Marí-Roig, A.; Jané-Salas, E.; López-López, J. Implant insertion torque and marginal bone loss: A systematic review and meta-analysis. Int J Oral Implantol (Berl). 2020, 13, 345–353. [Google Scholar] [PubMed]
- Patzelt, S.B.M.; Bahat, O.; Reynolds, M.A.; Strub, J.R.S. The all-on-four treatment concept: a systematic review. Clin Implant Dent Relat Res 2014, 16, 836–855. [Google Scholar] [CrossRef]
- Cassetta, M.; Brandetti, G.; Altieri, F. Are the Insertion Torque Value and Implant Stability Quotient Correlated, and If So, Can Insertion Torque Values Predict Secondary Implant Stability? A Prospective Parallel Cohort Study. Int J Oral Maxillofac Implants 2022, 37, 135–142. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Baseline Panoramic radiograph.
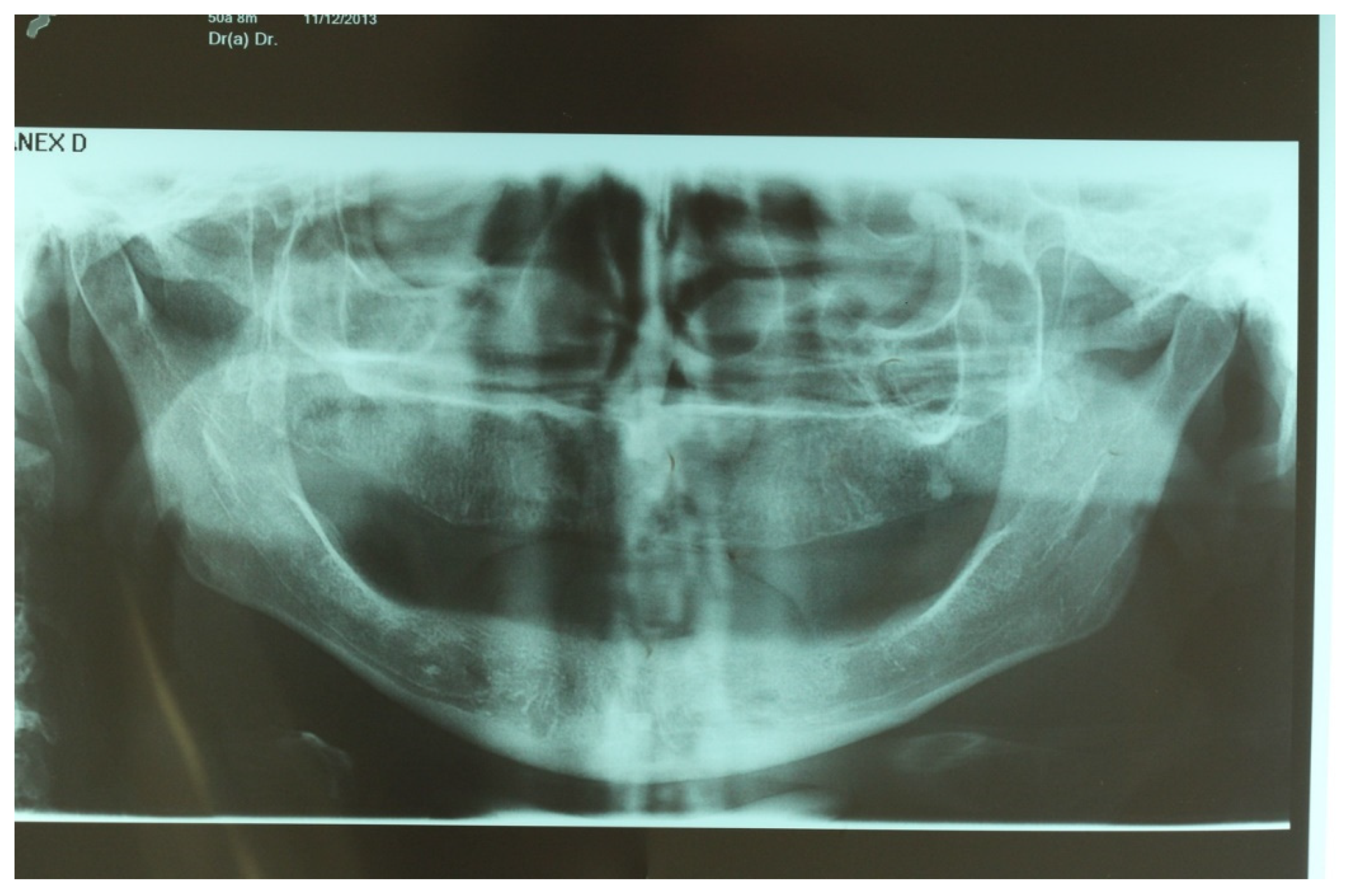
Figure 2.
Initial view from de lower arch after anesthesia.

Figure 3.
View of the mandible after the mucoperiosteal flap.
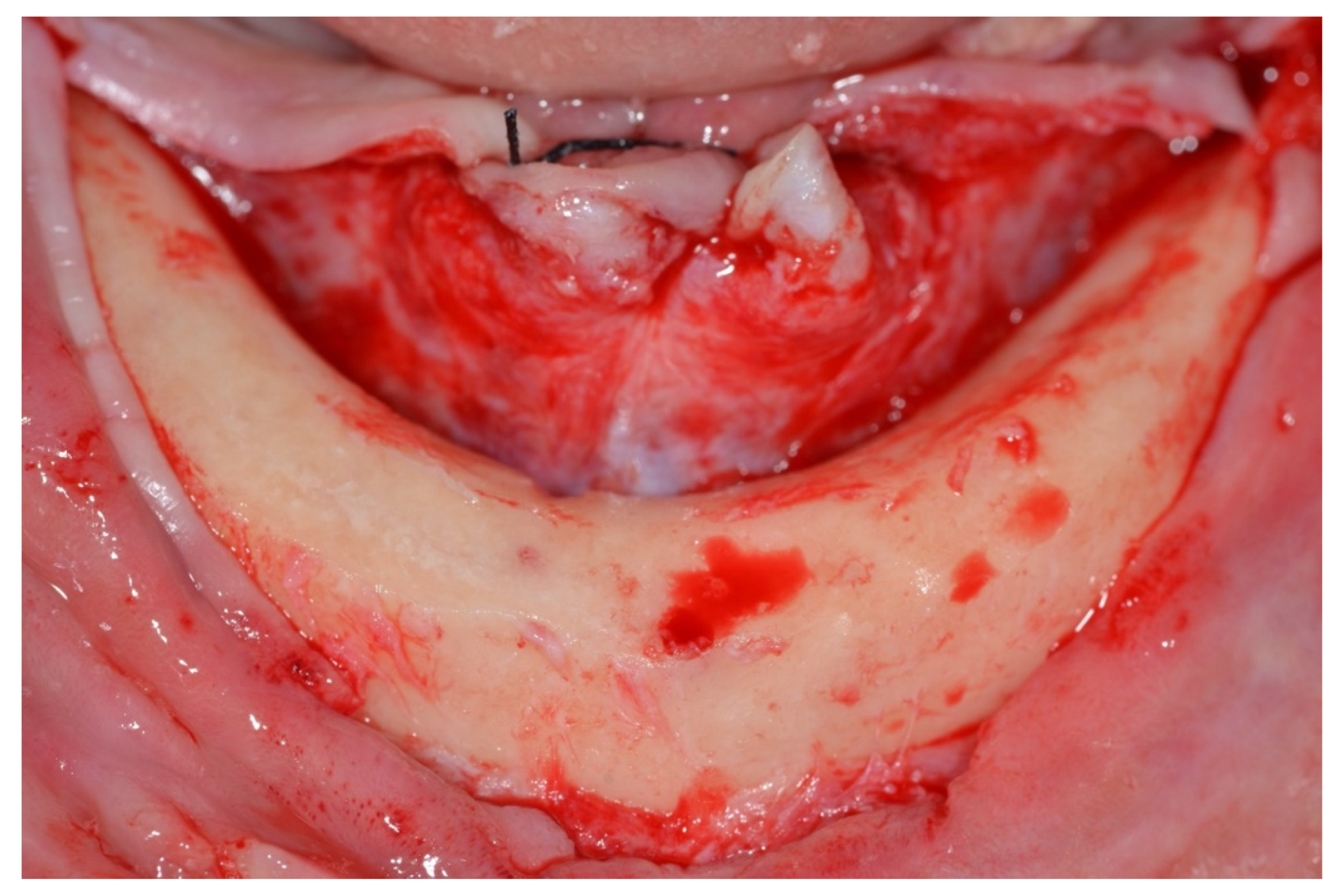
Figure 4.
View of the mandible with parallel pins to check implants positions for All on Four concept.
Figure 4.
View of the mandible with parallel pins to check implants positions for All on Four concept.
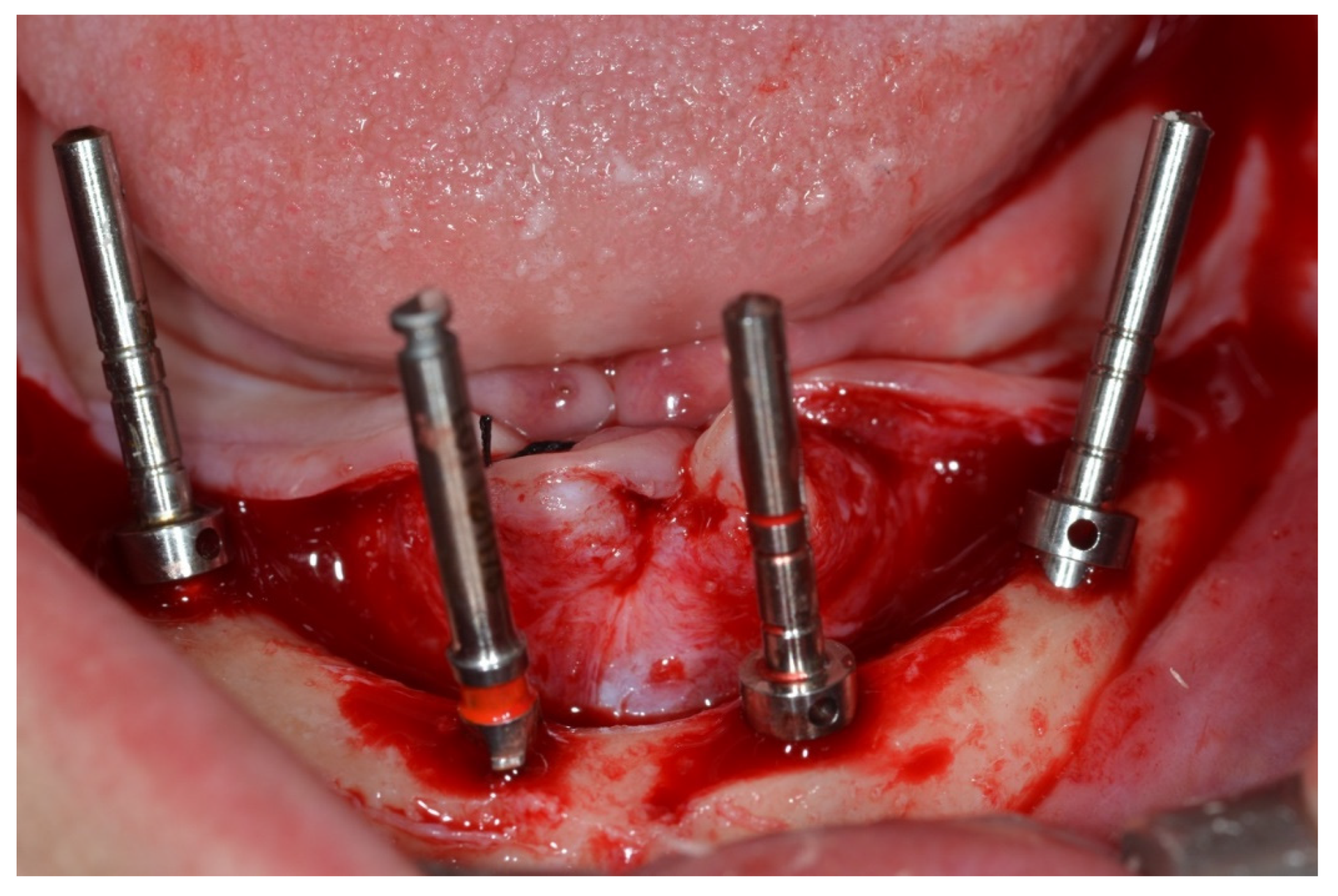
Figure 5.
Implant TRI Bioneck RP (Dérig, São Paulo, Brazil).

Figure 6.
Detail of the custom-made torque wrench allowing measurements up to 200Ncm.
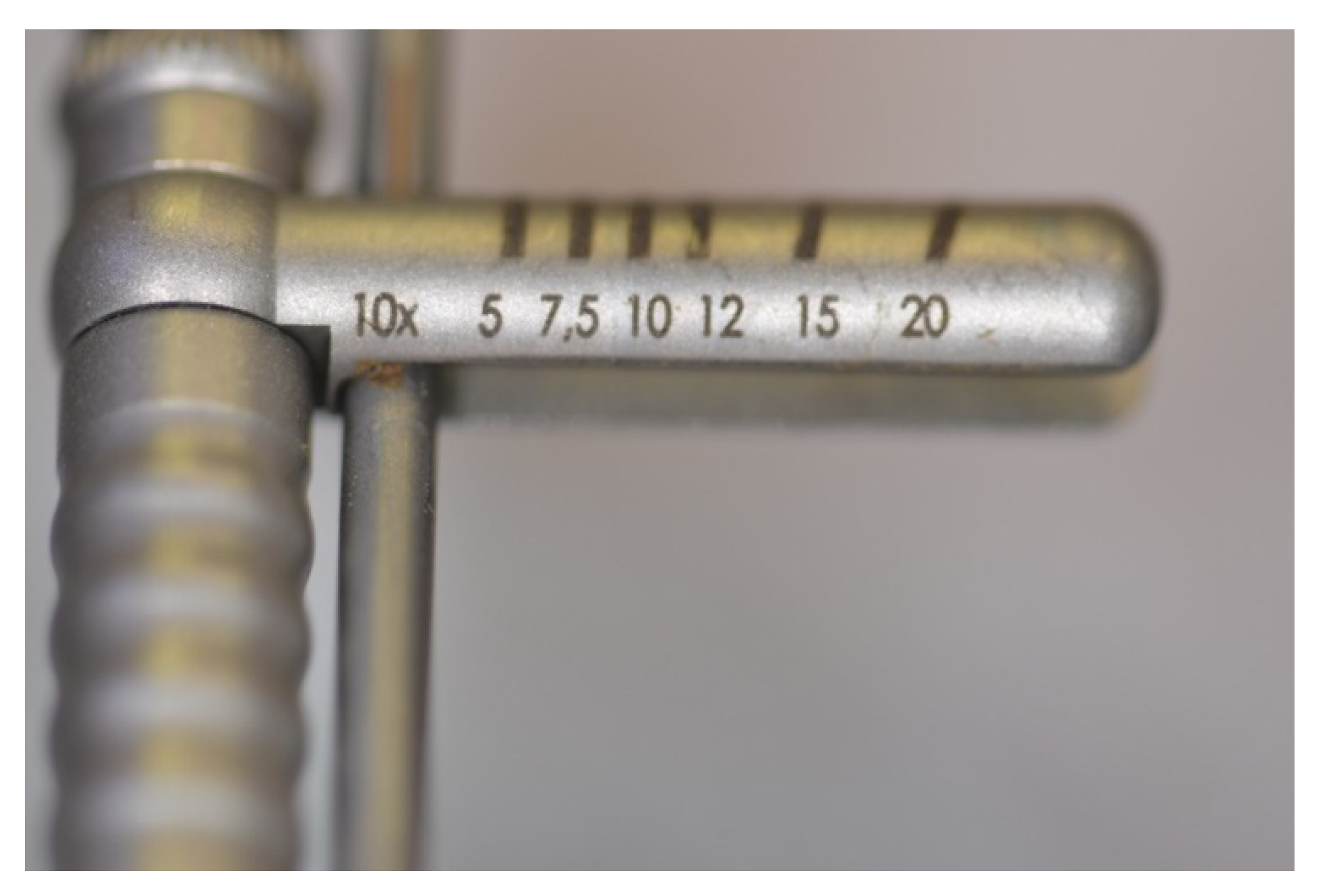
Figure 7.
Implants being placed on the All on Four Concept.
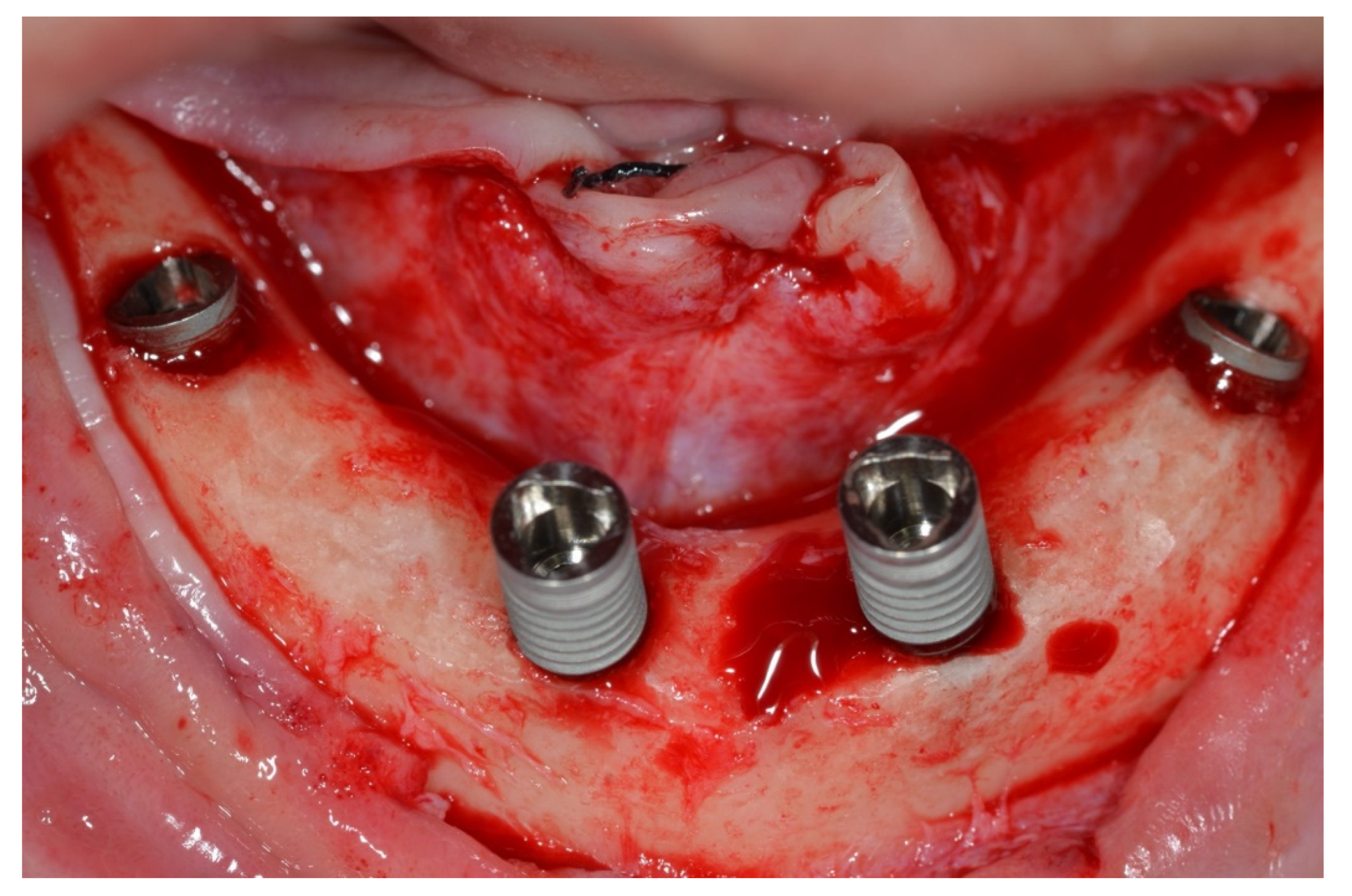
Figure 8.
Implant reaching 150Ncm on the wrench.
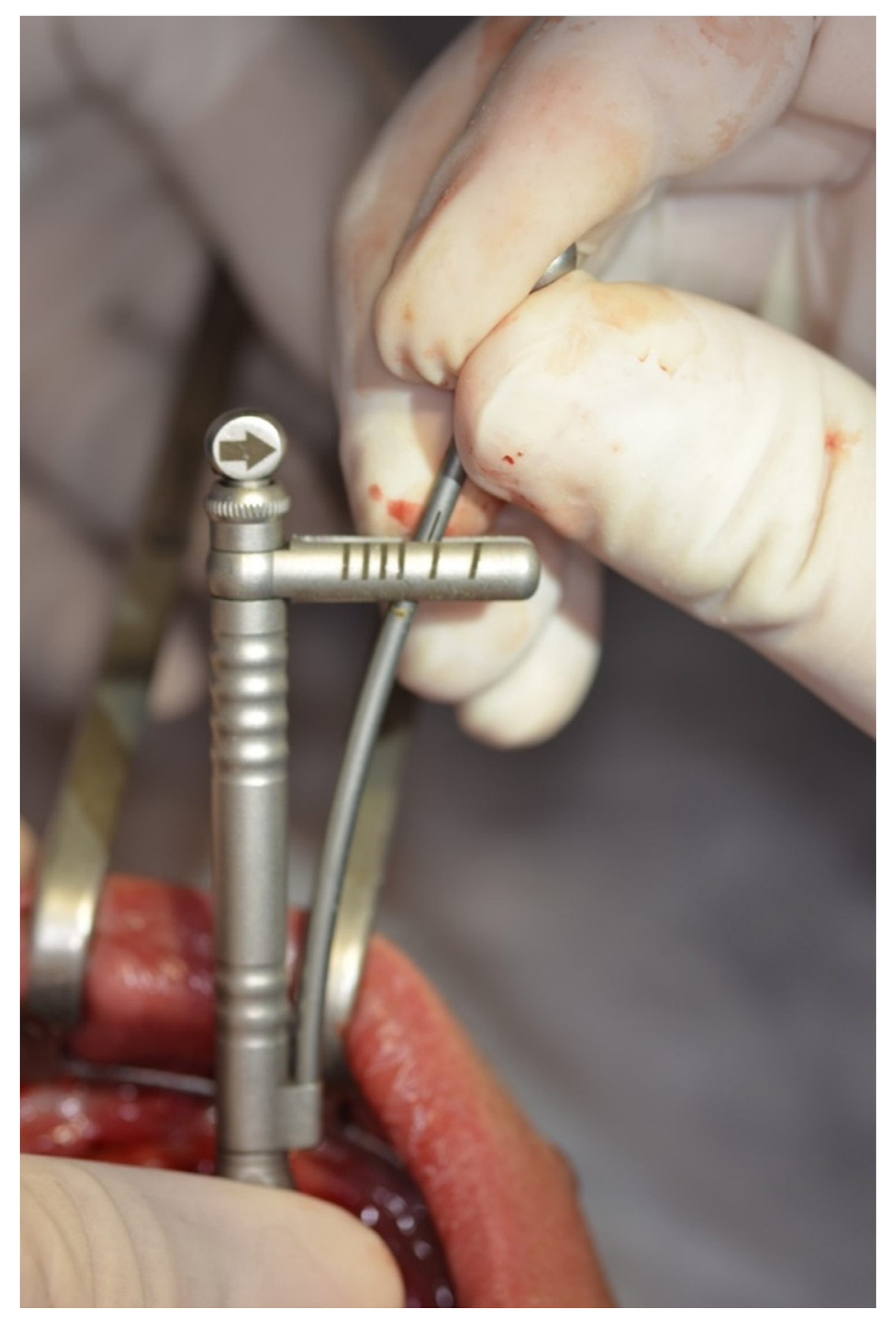
Figure 9.
Implant Stability Quotient recording after implant placement.
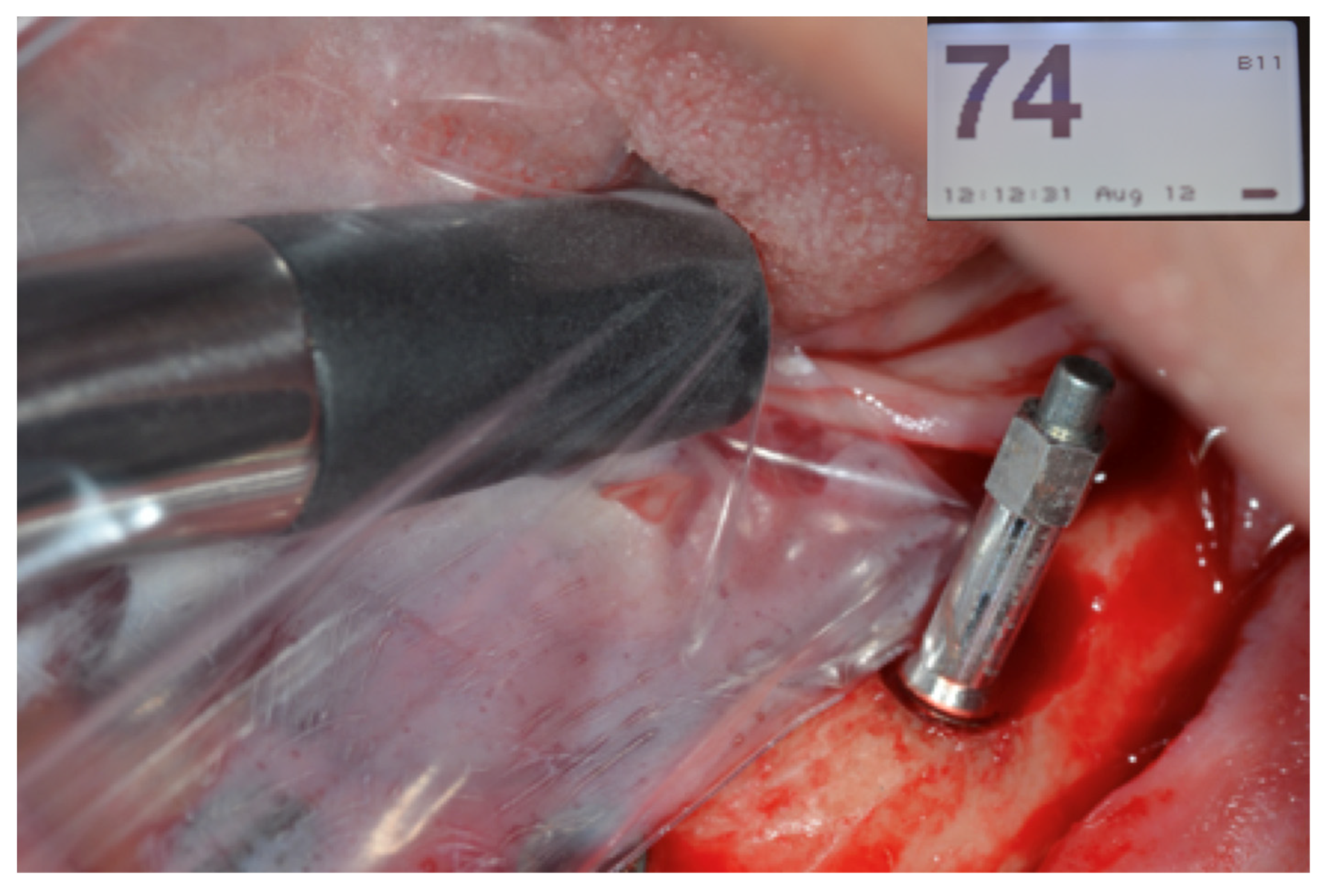
Figure 10.
Oclusal view of the mandible after multi-unit covers were installed and suture with 4.0 silk thread.
Figure 10.
Oclusal view of the mandible after multi-unit covers were installed and suture with 4.0 silk thread.
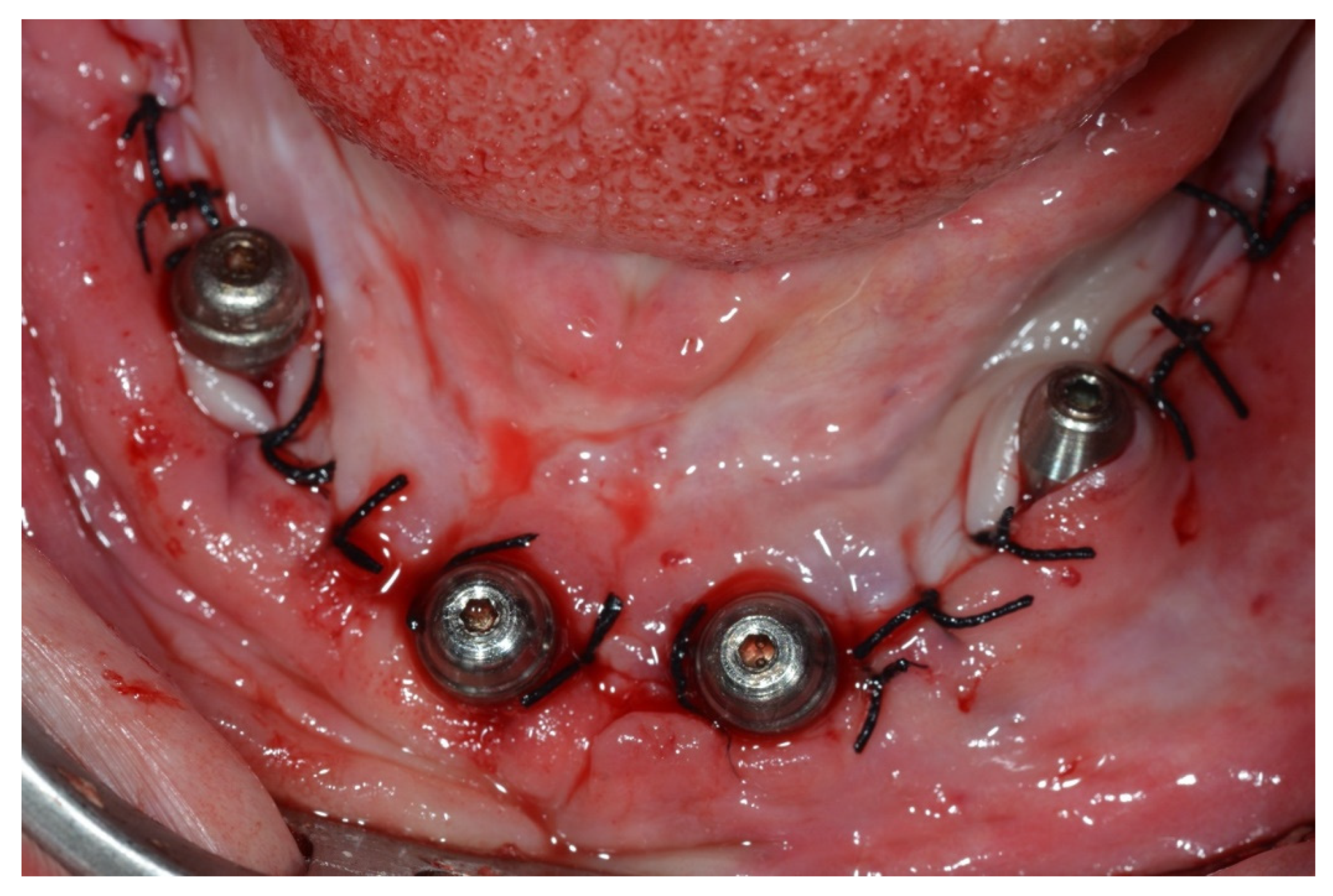
Figure 11.
Oclusal view of the mandible full-arch screwed rehabilitation 48 hours after surgery.

Figure 12.
Buccal view of both arches’ rehabilitations under the all on four concept, 48 hours after surgery.
Figure 12.
Buccal view of both arches’ rehabilitations under the all on four concept, 48 hours after surgery.

Figure 13.
2 years follow-up control panoramic radiograph.

Table 1.
Analysis of ISQ means according to torques above 70. ITV- initial torque value; ISQ-implant stability quotient; SD-standard deviation. p≤ 0,05 =statistical difference.
Table 1.
Analysis of ISQ means according to torques above 70. ITV- initial torque value; ISQ-implant stability quotient; SD-standard deviation. p≤ 0,05 =statistical difference.
| Initial | 7 days | P value | 7 days | 60 days | P value | Initial | 24 months | P value | |
| ITV (Ncm) |
Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | |||
| >70 | 63.5 (10.3) |
62.4 (9.7) |
0.3230 | 62.4 (9.7) |
62.6 (4.2) |
0.4633 | 63.5 (10.3) |
64.7 (6.1) |
0.3245 |
Table 2.
Analysis of ISQ means according to torques above 75. ITV- initial torque value; ISQ-implant stability quotient; SD-standard deviation. p≤ 0,05 = statistical difference.
Table 2.
Analysis of ISQ means according to torques above 75. ITV- initial torque value; ISQ-implant stability quotient; SD-standard deviation. p≤ 0,05 = statistical difference.
| Initial | 7 days | P value | 7 days | 60 days | P value | Initial | 24 months | P value | |
| ITV (Ncm) |
Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | Mean ISQ(SD) | |||
| ≥ 75 | 76.1 (9.3) |
59.7 (9.3) |
<0.001 | 59.7 (9.3) |
62.0 (8.4) |
0.0102 | 76.1 (9.3) |
65.3 (5.1) |
<0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



