
Submitted:
23 January 2024
Posted:
24 January 2024
You are already at the latest version
Abstract
Background: The circadian system, a vital temporal regulator influencing physiological processes, has implications for cancer development and treatment response. Our study assesses circadian timing's impact on whole-brain radiotherapy outcomes in brain metastases for personalized cancer therapy insights.
Aim: Evaluate circadian influence on radiation treatment timing and its correlation with clinical outcomes. Identify patient populations benefiting from interventions synchronizing circadian rhythms, considering subgroup differences and potential disparities related to social determinants of health (SDoH).
Design: IRB-approved retrospective analysis of 237 patients undergoing whole-brain radiotherapy for brain metastases (2017–2021), receiving over 80% of treatments in the morning or afternoon. Survival analyses utilized Kaplan–Meier curves.
Setting/Participants: Single-institution study involving patients receiving whole-brain radiotherapy. Collected demographic, disease, and socioeconomic parameters from electronic medical records.
Results: Morning treatment (n=158) showed a trend towards improved overall survival vs. afternoon (n=79), median survival 158 vs. 79 days (p=0.20, HR=0.84, CI95% 0.84–0.91). Subgroup benefits for morning treatment in females (p=0.04) and trends in controlled primary disease (p=0.11) and breast cancer metastases (p=0.08). SDoH-based disparities observed, with Black and lower-income patients exhibiting diminished circadian influence.
Conclusions: Emphasizes chronobiological factors' relevance in brain metastases radiation therapy. Morning treatment correlates with improved survival, particularly in specific subgroups. Identifies potential circadian influence disparities based on SDoH, laying a foundation for personalized cancer therapy and interventions synchronizing circadian rhythms for enhanced treatment efficacy.
Keywords:
brain metastases
; cancer
; chronobiology
; circadian clocks
; radiation therapy
; whole-brain radiotherapy
; breast cancer
; lung cancer
; stress
1. Introduction
The circadian system is an endogenous temporal regulator that orchestrates a myriad of physiological processes in alignment with the Earth’s Day-night cycle. This chronobiological mechanism is not merely a passive observer but an active participant in the homeostatic balance, influencing behavioral patterns, metabolic processes, and cellular functions. Emerging evidence suggests that circadian rhythms may play a role in the development of cancer, the process of metastasis, and the response to cancer treatments [1–4].
The concept of chronoradiotherapy has emerged from the hypothesis that the efficacy and toxicity of radiation therapy may be modulated by the timing of its administration relative to the patient's circadian rhythms. While the body of research in this field is growing, it remains fragmented, particularly in the context of brain metastases and whole-brain radiotherapy. Studies have touched upon the potential benefits of time-of-day treatment delivery, yet the findings are heterogeneous and sometimes contradictory, underscoring a need for more focused research [5–11]. However, toxicity has been found to be decreased in patients treated with prostate cancer
The literature to date has provided valuable insights but often falls short of establishing a comprehensive understanding of the temporal dynamics in radiotherapy outcomes. Notably, the majority of these studies have been limited in scope, with few addressing the circadian phase's impact on whole-brain radiotherapy across a diverse array of primary cancers. Moreover, the existing research has tended to present isolated statistical outcomes without fully integrating them into the broader context of circadian biology's role in cancer treatment.
Disruptions in circadian rhythms have been associated with increased cancer risk and poor prognosis, suggesting a profound underlying connection between the body's internal clock and cancer pathophysiology. For instance, the suppression of melatonin due to circadian misalignment, has been linked to carcinogenesis, particularly in shift workers exposed to irregular light cycles [12–15]. Specifically, the World Health Organization (WHO) recently designated circadian disruption as a probable carcinogen, thus raising the need to understand how biological disruption of diurnal patterns promotes tumor development and leveraging this understanding to enhance treatment with coordinated time of treatment. At the genomic level, clock genes are known to be pivotal in the DNA damage response and have been implicated in cancer development, progression, and treatment response, yet the exact pathways and interactions remain to be elucidated [16–20].
Our study seeks to bridge this gap by systematically evaluating the impact of circadian timing on the outcomes of whole-brain radiotherapy in patients with brain metastases. We aim to provide an understanding of how treatment timing may correlate with clinical efficacy and toxicity, potentially offering a new paradigm in the personalization of cancer therapy.
2. Results
Data was collected for all consecutive patients with brain metastases between 2017 and 2021. We identified a total of 2040 patients in our database who began whole-brain radiotherapy between January 20, 2017 and June 2, 2021. Treatment times were documented in the EMR for 237 patients (median survival 91 days) who received at least 80% of their treatment in the same time window, making them eligible for analysis. Patients were split into two groups: 158 patients who received ≥80% of their total dose before 12:00pm (AM group), and 79 patients who received ≥80% of their total dose at or after 12:00pm (PM group).
The population of patients who received >80% of their treatment in the AM or PM are described in Table 1. Of these, 62% were female, and 50% were 65 years of age or older when diagnosed with brain metastases. The most common primary cancer site was lung (54%), followed by breast (18%). More than half of patients were overweight or obese defined by BMI. Most patients had a Karnofsky performance score of ≥70. In total, for the 237 patients who received ≥80% of their total dose within a single time window, 67% had radiation mostly in the morning and 33% had >80% of their radiation in the afternoon.
Survival curves comparing AM and PM groups for specified cohorts of patients are presented in Figure 1. For the entire cohort without subgrouping, there was a trend for improved survival for patients whose treatment delivered in the morning (AM group) compared with the afternoon (PM group) 158 vs. 79 overall (N=237, p=0.20, HR=0.84, CI95% 0.84–.91). To assess associations of chronobiology impact on disease status, cancer subtypes were evaluated as well as the disease status for those who had controlled metastatic cancer other than in the brain or those with more widespread disease. The breast cancer cohort revealed a trend to a survival advantage for morning radiation (n=43, p=0.081, HR=0.57, CI95% 0.922–3.38) with median survival in days (for AM vs. PM groups) being 124.5 vs. 50 for the breast cancer cohort with no notable differences for the lung cancer cohort (96 vs. 87, and for other known primaries (78 vs. 108).
To determine subsets of patients who would most benefit from modulating the timing of radiation delivery, or chronobiology modulation, patient characteristics, including gender, age, BMI, and KPS, were assessed to determine the impact of chronobiology on radiation outcomes. Subgroup analysis demonstrated a significant survival advantage associated with morning radiation for females (n=147, p=0.04, HR=0.69, CI95% 1.014–2.077), but not for males (n=90, p=0.55, HR=1.14, CI95% 0.57–1.35). Median survivals in days (for AM vs. PM groups) were 95.5 vs. 88 for females, 72.5 vs. 90.5 for males. We did note a trend toward longer survival after morning radiation in patients with BMI<25 that did not reach significance (n=91, p=0.053).
The impact of chronobiology was next assessed by assessing social structure by using race and average income as proxies for adverse social determinants of health (SDoH). For patients who experience adverse SDoH such as racism noted to be experienced by Black patients (p=0.41) and those with low average income, circadian influence on radiation outcomes was minimized. White patients (p=0.22) and those with high income levels seemed to be impacted more by morning treatments or timing of treatments (p=0.15).
3. Discussion
Chronotherapy has gained increasing attention for its potential in cancer care. Given the connections between chronobiology and cancer, the potential effects of chronoradiotherapy would be expected in the setting of robust circadian rhythms [1–4,6]. Our findings indicate a trend towards improved overall survival for patients receiving morning radiation, particularly evident in cohorts with controlled primary disease and those with breast cancer brain metastases. Notably, female patients also demonstrated a statistically significant survival advantage in the morning treatment group, regardless of subtyping for primary cancer. Additionally, the study identifies potential disparities in the influence of circadian rhythms based on SDoH, revealing differences in response to timing of treatment for patients with adverse social determinants, including race and income. These results underscore the relevance of considering circadian timing in radiation therapy planning and suggest avenues for further investigation and potential interventions to enhance treatment efficacy.
Radiation treatment delivered in the morning trended toward a significant improvement in survival which was more beneficial for patients having well controlled disease or those with a breast cancer primary tumor that metastasized to the brain. Previous studies have explored the timing of radiation therapy for brain metastases, including stereotactic radiosurgery and whole-brain radiotherapy [14,15,20]. Specifically, one study demonstrated that females with brain metastases treated in the same specific window of time, (either 08:00–11:00am, 11:00am–14:00pm, or 14:00h–17:00h p=0.14), patients had improved survival [23]. For this study, the authors sought to expand on previous findings by comparing two distinct cohorts: one receiving at least 80% of whole-brain treatments before noon and the other at least 80% in the afternoon. The intent was to capture the broader physiologic circadian differences between the timing of the groups treated. Taken together, prior studies and this current study demonstrate a convergence of results showing the contribution of circadian rhythm impact on outcomes for metastatic patients [24]. It was not surprising that there was a trend towards a significant impact of circadian influence on brain metastases originating from breast cancer due to the strong established relationship between the impact of chronobiology as noted by night shift workers and increased breast cancer risk which was first reported in 1969 [6,7,25]. Since that time, the molecular underpinnings of the impact of chronobiology on breast cancer progression has been investigated with clock proteins such as PER1 and PER2 having notable dysregulation in advanced cancers [26]. Our study also noted the influence of circadian regulation for patients with well controlled disease other than brain metastases which was not seen in patients with poorly controlled disease (Figure 1E-F). When disease burden is significant, circadian misalignment decreases the influence of clock proteins on tumor control [27]. Therefore, a future strategy would be to artificially augment the circadian response with novel therapeutics to improve radiation outcomes.
In evaluating the influence of chronobiology based on patient characteristics of brain metastases patients, a significant benefit was noted in female patients (Figure 2A-B), while those who were younger, did not have metabolic dysfunction (as determined by BMI), and had optimal performance status (KPS >70), had a trend toward a benefit to being treated in the morning with radiation. Our study noted a survival advantage among females with brain metastases who received whole-brain radiotherapy before 12:00h compared to those receiving treatment in the afternoon (Figure 2). The sex-dependent survival difference noted can be attributed to the interplay between circadian signaling and sex hormones [29]. Women have melatonin receptors on their ovaries which stimulates estrogen production which in part may explain the preferential circadian influence on our female population [30]. In fact, preclinical experiments are underway using novel melatonin-tamoxifen conjugate as an anti-cancer drug in breast cancer [31–34]. Additionally, circadian rhythms “are set to an earlier hour in women than in men,” which is congruent with the benefit noted in our study for women [35]. Furthermore, It has been noted that circadian misalignment is associated with metabolic dysfunction [28]. This is congruent with our findings that older patients, those with an elevated BMI, and lower functional status are less responsive to circadian influences (Figure 2C-H). Patients over 65 years old did not achieve a benefit from temporal treatment of radiation which aligns with the fact that the synchrony of circadian rhythms is known to decrease during the aging process [36]. The trend observed in the BMI<25 subgroup of improved response with morning treatment may be because of chronobiology health. In particular, it has been shown that obese patients have a misaligned circadian pattern, with some studies demonstrating this misalignment is more prevalent during the morning hours [37]. Therefore, gender and BMI should be considerations when designing future studies with interventions geared to targeting chronobiology.
Stressors that patients experience, such as adverse SDOH, including race and income status, disrupt the circadian patterns that are known to affect cancer [38]. The asynchrony of circadian impact on outcomes was noted in our patients who have low socioeconomic means or those who experience racism (Figure 3). Conversely, with less perceived stress in patients with increased income and the white patients not experiencing the stress of racism, who were more likely to have an intact circadian clock, had more of a benefit to morning timed radiation. Interestingly, circadian misalignment has been noted in racial/ethnic minorities a greater prevalence of night shift work, environmental factors (e.g., exposure to too much nighttime light, high noise pollution) and chronic conditions (e.g., diabetes, cardiovascular disease). [39]. In addition, black patients have a shorter free-running circadian period which is also known as tau and may contribute to the circadian misalignment [39]. Similarly, outside stressors are known to alter chronobiology. In fact, stress and stress hormones (cortisol, etc.) can cause circadian dysfunction by altering phase shifts [40]. This correlates with our finding that patients with less stress and less financial toxicity as noted by living in a zip code with average salaries higher than the median income for Pennsylvania, is linked to more of a response to timing of treatment.
There are limitations to our retrospective study including the fact that the study relied on treatment time as a proxy for patients’ biological' circadian phase, which can be misaligned with the actual biological circadian phase, especially in the setting context of cancer. Therefore, a larger prospective study should be considered in this space.
This study highlights the impact of chronobiology in radiation outcomes for patients with brain metastases. This is the first study to identify populations of patients most likely to derive benefit from interventional trials designed to synchronize circadian rhythms to improve radiation outcomes. More effective strategies should be sought to improve radiation outcomes for patients with brain metastases by improving chronobiology for patients who are older, obese, experience adverse SDoH and have increased tumor burden. Altering circadian patterns has the potential to increase the therapeutic efficacy of radiotherapy and this study is the first to discuss the ability with this to be a precision medicine approach by identifying populations most at risk of circadian dysregulation that will benefit from this approach. Understanding the importance of chronobiology on radiation outcomes, clinical trials could incorporate noninvasive methods of circadian resynchronization such as time restricted diet and/or sleep interventions to align patients’ circadian rhythms to improve outcomes.
4. Materials and Methods
We performed a single-institution (Thomas Jefferson University), IRB-approved (22E.432) retrospective analysis on the overall survival of patients with secondary brain neoplasms treated with whole-brain radiotherapy. Whole brain radiation was delivered in 10 fractions to a dose of 30Gy. Patients were eligible for our primary analysis if each of their treatment times was available in the electronic medical record (EMR) and at least 80% of their total radiation dose was received within a consistent time window, i.e., either before or after 12pm. For comparison, we performed a secondary analysis on patients who received 51–79% of their total radiation either before or after noon.
We utilized the EMR to collect patient characteristics as recorded at the time they were diagnosed with brain metastases. Collected characteristics were sex, race that was self reported, body mass index (BMI), residential zip code, primary disease site (lung, breast, non-lung or non-breast, or unknown/unspecified), age, presence of extracranial metastases, primary disease control, and Karnofsky performance scale (KPS) index. The latter four factors were used to assign patients to recursive partitioning analysis (RPA) classes I–III [21]. Median household incomes for each zip code were searched via https://www.incomebyzipcode.com/, and zip-based income brackets were recorded as a proxy for probable socioeconomic status [22].
Patient survivals were calculated in days from the date of their first treatment of whole-brain radiotherapy. Dates of death were confirmed via local obituaries if unavailable in the EMR. Kaplan–Meyer survival curves and median survivals were analyzed using Prism 9 GraphPad (Version 9.3.0), with Mantel–Cox log-rank tests at a significance threshold of p<0.05 and Mantel–Haenszel hazard ratio with 95% confidence intervals. Figures were generated in RStudio (Version 2023.09.1 Build 494).
Author Contributions
Conceptualization, N.G. N.; formal analysis, N.G.N. and S.E.B and L.C. and N.F. and K.Y.W. and A.A.S.; data curation, A.P.S. and J.L. and Y.B.S.; writing—original draft preparation, S.E.B. and L.C. and K.Y.W. and A.A.S.; writing—review and editing, S.E.B. and N.F.; supervision, N.L.S.; project administration, N.L.S.; funding acquisition, N.L.S. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: “This research was funded by NCI, grant number R01CA227479”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Thomas Jefferson University (IRB Control #16D.216, JeffTrial #8439).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest and the funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Takahashi JS, Hong HK, Ko CH, McDearmon EL. The genetics of mammalian circadian order and disorder: implications for physiology and disease. Nat Rev Genet. 2008;9:764-75. [CrossRef]
- Diamantopoulou Z, Castro-Giner F, Schwab FD, Foerster C, Saini M, Budinjas S, et al. The metastatic spread of breast cancer accelerates during sleep. Nature. 2022;607:156-62. [CrossRef]
- Wang C, Barnoud C, Cenerenti M, Sun M, Caffa I, Kizil B, et al. Dendritic cells direct circadian anti-tumour immune responses. Nature. 2023;614:136-43. [CrossRef]
- Kim DW, Byun JM, Lee JO, Kim JK, Koh Y. Chemotherapy delivery time affects treatment outcomes of female patients with diffuse large B cell lymphoma. JCI Insight. 2023;8. [CrossRef]
- Haus E. Chronobiology of the mammalian response to ionizing radiation. Potential applications in oncology. Chronobiol Int. 2002;19:77-100. [CrossRef]
- Bermúdez-Guzmán L, Blanco-Saborío A, Ramírez-Zamora J, Lovo E. The Time for Chronotherapy in Radiation Oncology. Front Oncol. 2021;11:687672. [CrossRef] [PubMed]
- Nelson N, Lombardo J, Matlack L, Smith A, Hines K, Shi W, et al. Chronoradiobiology of Breast Cancer: The Time Is Now to Link Circadian Rhythm and Radiation Biology. Int J Mol Sci. 2022;23. [CrossRef] [PubMed]
- Chan S, Rowbottom L, McDonald R, Zhang L, Bjarnason GA, Tsao M, et al. Could time of whole brain radiotherapy delivery impact overall survival in patients with multiple brain metastases? Ann Palliat Med. 2016;5:267-79. [CrossRef] [PubMed]
- Badiyan SN, Ferraro DJ, Yaddanapudi S, Drzymala RE, Lee AY, Silver SA, et al. Impact of time of day on outcomes after stereotactic radiosurgery for non-small cell lung cancer brain metastases. Cancer. 2013;119:3563-9. [CrossRef]
- Rahn DA, Ray DK, Schlesinger DJ, Steiner L, Sheehan JP, O'Quigley JM, et al. Gamma knife radiosurgery for brain metastasis of nonsmall cell lung cancer: is there a difference in outcome between morning and afternoon treatment? Cancer. 2011;117:414-20. [CrossRef]
- Kabolizadeh P, Wegner R, Bernard M, Heron D, Mintz A, Burton S. The effect of treatment time on outcome in non-small cell lung cancer brain metastases treated with stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2011;81:S301. [CrossRef]
- Straif K, Baan R, Grosse Y, Secretan B, El Ghissassi F, Bouvard V, et al. Carcinogenicity of shift-work, painting, and fire-fighting. Lancet Oncol. 2007;8:1065-6. [CrossRef] [PubMed]
- He C, Anand ST, Ebell MH, Vena JE, Robb SW. Circadian disrupting exposures and breast cancer risk: a meta-analysis. Int Arch Occup Environ Health. 2015;88:533-47. [CrossRef]
- Garcia-Saenz A, Sánchez de Miguel A, Espinosa A, Valentin A, Aragonés N, Llorca J, et al. Evaluating the Association between Artificial Light-at-Night Exposure and Breast and Prostate Cancer Risk in Spain (MCC-Spain Study). Environ Health Perspect. 2018;126:047011. [CrossRef]
- deHaro D, Kines KJ, Sokolowski M, Dauchy RT, Streva VA, Hill SM, et al. Regulation of L1 expression and retrotransposition by melatonin and its receptor: implications for cancer risk associated with light exposure at night. Nucleic Acids Res. 2014;42:7694-707. [CrossRef] [PubMed]
- Yao J, He C, Zhao W, Hu N, Long D. Circadian clock and cell cycle: Cancer and chronotherapy. Acta Histochem. 2021;123:151816. [CrossRef]
- Reszka E, Przybek M, Muurlink O, Pepłonska B. Circadian gene variants and breast cancer. Cancer Lett. 2017;390:137-45. [CrossRef]
- Siracusa LD, Bussard KM. The Clock Is Ticking: Countdown to Metastases. PLoS Genet. 2016;12:e1006299. [CrossRef]
- Johnson K, Chang-Claude J, Critchley AM, Kyriacou C, Lavers S, Rattay T, et al. Genetic Variants Predict Optimal Timing of Radiotherapy to Reduce Side-effects in Breast Cancer Patients. Clin Oncol (R Coll Radiol). 2019;31:9-16. [CrossRef]
- Zhang J, Lv H, Ji M, Wang Z, Wu W. Low circadian clock genes expression in cancers: A meta-analysis of its association with clinicopathological features and prognosis. PLoS One. 2020;15:e0233508. [CrossRef]
- Gaspar L, Scott C, Rotman M, Asbell S, Phillips T, Wasserman T, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. 1997;37:745-51. [CrossRef]
- Diez-Roux AV, Kiefe CI, Jacobs DR, Jr., Haan M, Jackson SA, Nieto FJ, et al. Area characteristics and individual-level socioeconomic position indicators in three population-based epidemiologic studies. Ann Epidemiol. 2001;11:395-405.
- Chan S, Zhang L, Rowbottom L, McDonald R, Bjarnason GA, Tsao M, et al. Effects of circadian rhythms and treatment times on the response of radiotherapy for painful bone metastases. Ann Palliat Med. 2017;6:14-25. [CrossRef]
- Steele TA, St Louis EK, Videnovic A, Auger RR. Circadian Rhythm Sleep-Wake Disorders: a Contemporary Review of Neurobiology, Treatment, and Dysregulation in Neurodegenerative Disease. Neurotherapeutics. 2021;18:53-74. [CrossRef]
- Hamilton T. Influence of environmental light and melatonin upon mammary tumour inductino. The British Jounral of Surgery. 1969; 56(10) 764-766. [CrossRef]
- Chen ST, Choo KB, Hou MF, Yeh KT, Kuo SJ, Chang JG. Deregualted expression of the PER1, PER2, and PER3 genes in breast cancers. Carcinogenesis. 2005; 26(7)1241-1246. [CrossRef]
- Innominato PF, Roche VP, Palesh OG, Ulusakarya A, Spiegel D, Levi FA. The circadian timing system in clinical oncology. Annals of medicine. 2014; 46(4), 191-207. [CrossRef] [PubMed]
- Maury E, Ramsey KM, Bass J. Circadian rhytms and metabolic syndrome: from experimental genetics to human disease. 2010; 106(3), 447-462. [PubMed]
- Kubatka P, Zubor P, Busselberg D, Kwon TK, Adamek M, Petrovic D, et al. Melatonin and breast cancer: Evidences from preclinical and human studies. Crit Rev Oncol Hematol. 2018;122:133-43. [CrossRef] [PubMed]
- Tamura H, Nakamura Y, Korkmaz A, Manchester LC, Tan DX, Sugino N, Reiter RJ. Melatonin and the ovary: physiological and pathophysiological impications. Fertility and sterlity. 2008; 92(1), 328-343. [CrossRef] [PubMed]
- Hasan M, Marzouk MA, Adhikari S, Wright TD, Miller BP, Matossian MD, et al. Pharmacological, Mechanistic, and Pharmacokinetic Assessment of Novel Melatonin-Tamoxifen Drug Conjugates as Breast Cancer Drugs. Mol Pharmacol. 2019;96:272-96. [CrossRef]
- Ball LJ, Palesh O, Kriegsfeld LJ. The Pathophysiologic Role of Disrupted Circadian and Neuroendocrine Rhythms in Breast Carcinogenesis. Endocr Rev. 2016;37:450-66. [CrossRef]
- Linder S, Hoogstraat M, Stelloo S, Eickhoff N, Schuurman K, de Barros H, et al. Drug-Induced Epigenomic Plasticity Reprograms Circadian Rhythm Regulation to Drive Prostate Cancer toward Androgen Independence. Cancer Discov. 2022;12:2074-97. [CrossRef]
- Zhu Y, Brown HN, Zhang Y, Stevens RG, Zheng T. Period3 structural variation: a circadian biomarker associated with breast cancer in young women. Cancer Epidemiol Biomarkers Prev. 2005;14:268-70. [CrossRef] [PubMed]
- Duffy JF, Cain SW, Chang AM, Phillips AJ, Munch MY, Gronfier C, Wyatt JK, Dijk DJ, Wright KP Jr, Czeisler CA. Sex difference in the near-24-hour insrinsic period of the human circadian timing system. Proceedings of the National Academy of Sciences of the United States of America. 2011; 108.
- Duffy JF, Zitting KM, Chinoy ED. Aging and Circadian rhythms. Sleep Medicine Clinics. 2015; 10(4) 423-434. [CrossRef]
- Simon SL, McWhirter L, Diniz Behn C, Bubar KM, KaarL, Pyle L, Rahat H, Garcia-Reyes Y, Carreau AM, Wright KP, Nadeau KJ, Cree-Green M. Morning circadian misalignment is associated with insulin resistance in girls with obesity and polycystic ovarian syndrome. The journal of clincial endocrinology and metabolism. 2019. 104(8), 3525-3534. [CrossRef]
- Dasari SS, Archer M, Mohamed NE, Tewari AK. Figueiro MG, Kypinaou N. Circadian Rhythm Disruption as a contributor to racial disparities in prostate cacner. Cancers. 2002; 14.
- Smith MR, Burgess HJ, Fogg LF, Eastman CI. Racial differences in the human endogenous circadian period. PloS. 2009; 4. [CrossRef]
- Rhythms. 2016;31:483-97.
- Ota SM, Kong X, Hut R, Suchecki D, Meerlo P. The impact of stress and stress hormones on endogenous clocks and circadian rhythms. Frontiers in neuroendicrinology. 2023;63. [CrossRef]
- Walker WH, Borniger JC. Molecular Mechanisms of Cancer-Induced Sleep Disruption. Int J Mol Sci. 2019;20. [CrossRef] [PubMed]
Figure 1.
Overall impact of treatment time on brain metastases patients by disease site and disease burden. Kaplan–Meyer survival curves were done to compare groups who received ≥80% of whole-brain radiotherapy in the AM vs. ≥80% PM for specified patient subsets: (a) all patients (p=0.20), (b) those with primary tumors arising from the breast (p=0.08) or (c) lung (p=0.36), or (d) other (p=0.99), (e) those who had their primary disease controlled (p=0.11), and (f) those who did not have their primary disease controlled (p=0.53). .
Figure 1.
Overall impact of treatment time on brain metastases patients by disease site and disease burden. Kaplan–Meyer survival curves were done to compare groups who received ≥80% of whole-brain radiotherapy in the AM vs. ≥80% PM for specified patient subsets: (a) all patients (p=0.20), (b) those with primary tumors arising from the breast (p=0.08) or (c) lung (p=0.36), or (d) other (p=0.99), (e) those who had their primary disease controlled (p=0.11), and (f) those who did not have their primary disease controlled (p=0.53). .
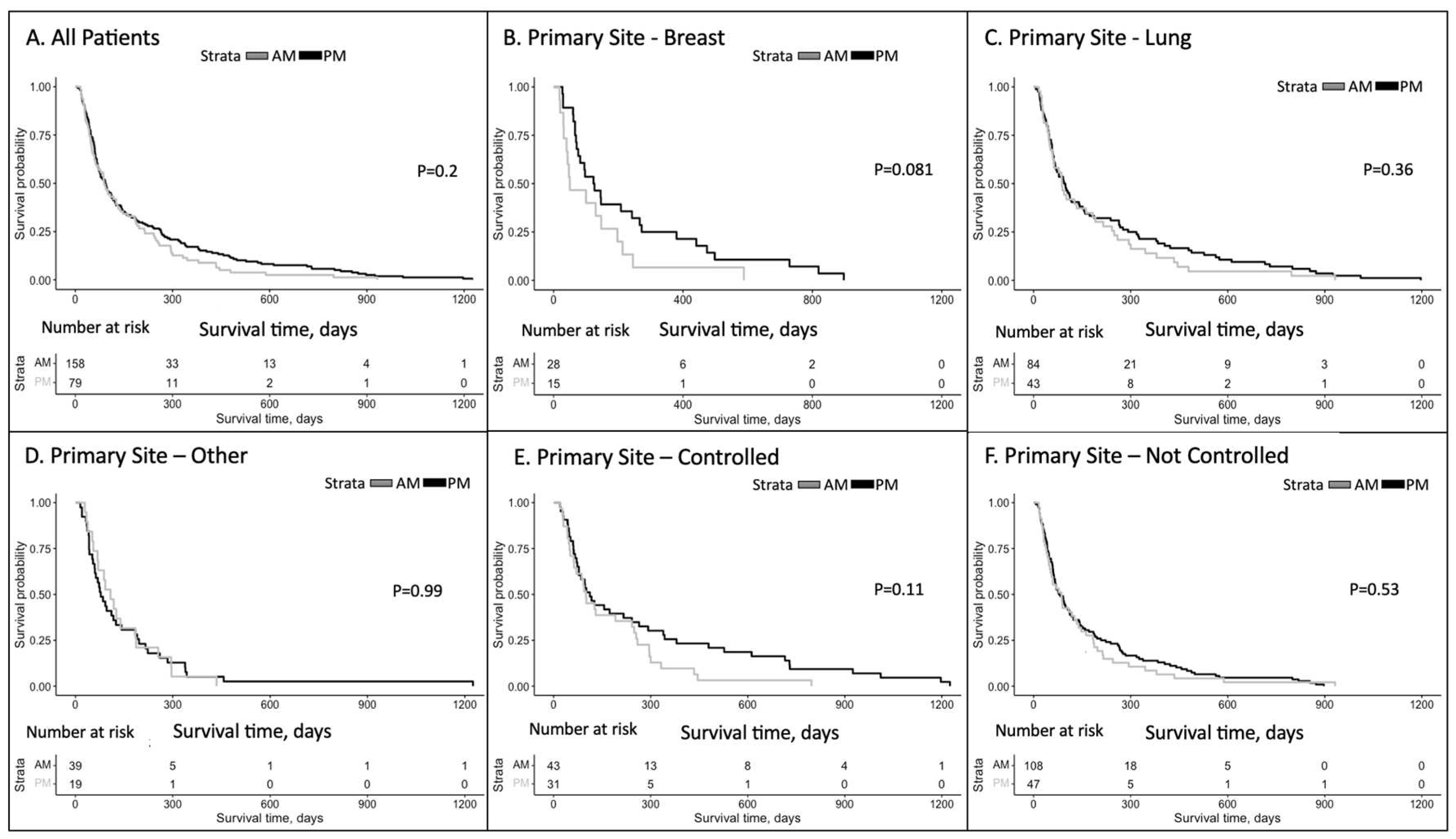
Figure 2.
Patient characteristics impacting the timing of radiation delivery for brain metastases patients. Kaplan–Meyer survival curves were done to compare groups who received ≥80% of whole-brain radiotherapy in the AM vs. ≥80% PM for specified patient subsets: (a) male patients (p=0.55), (b) female patients (p=0.04), (c) those who were younger than 65 years (p=0.15), (d) those who were 65 years or older (p=0.75), (e) those whose BMI was under 25 (p=0.053), (f) those whose BMI was over 25 (p=0.78), (g) those whose KPS was under 70 (p=0.36), and (h) those whose KPS was 70 or higher (p=0.14).
Figure 2.
Patient characteristics impacting the timing of radiation delivery for brain metastases patients. Kaplan–Meyer survival curves were done to compare groups who received ≥80% of whole-brain radiotherapy in the AM vs. ≥80% PM for specified patient subsets: (a) male patients (p=0.55), (b) female patients (p=0.04), (c) those who were younger than 65 years (p=0.15), (d) those who were 65 years or older (p=0.75), (e) those whose BMI was under 25 (p=0.053), (f) those whose BMI was over 25 (p=0.78), (g) those whose KPS was under 70 (p=0.36), and (h) those whose KPS was 70 or higher (p=0.14).
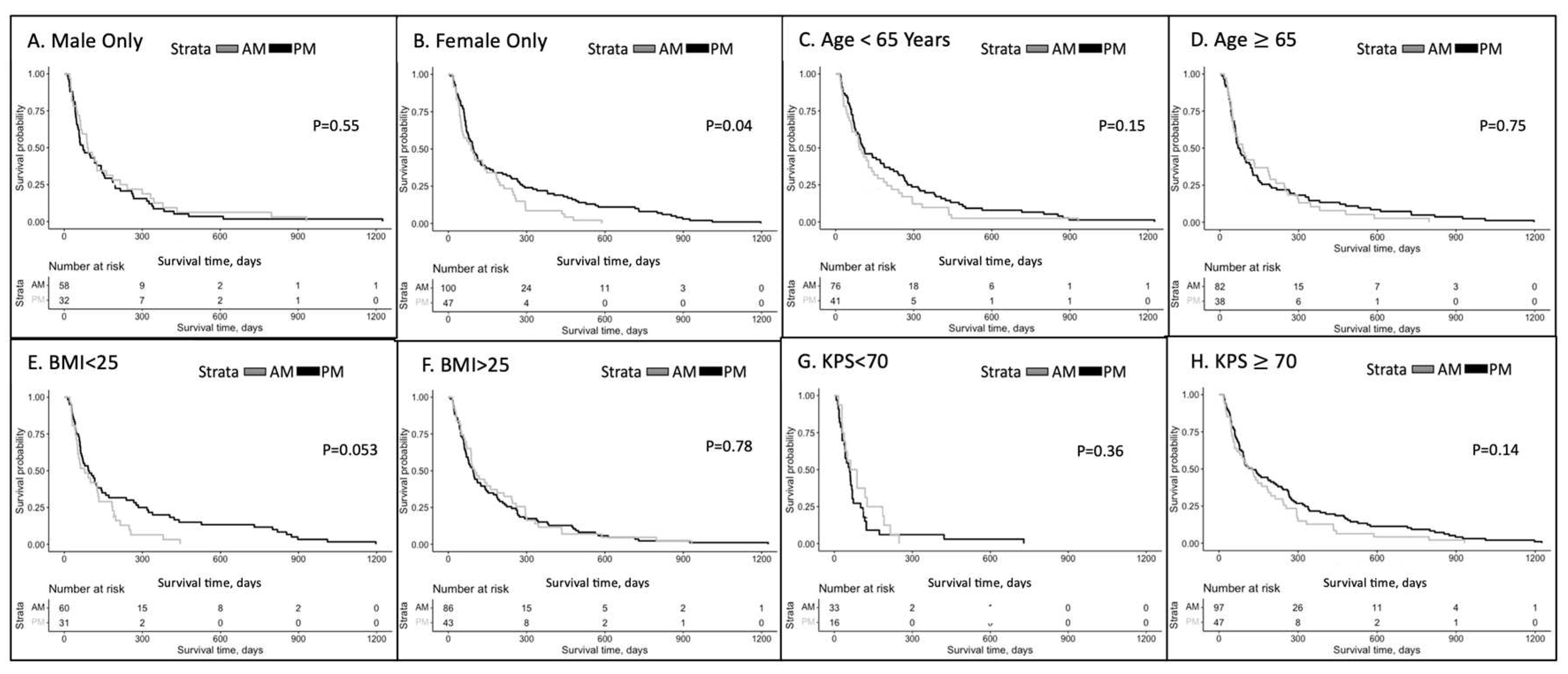
Figure 3.
Social determinants of health impacting the timing of radiation delivery for brain metastases patients. Kaplan–Meyer survival curves were done to compared groups who received ≥80% of whole-brain radiotherapy in the AM vs. ≥80% PM for specified patient subsets: (a) white patients (p=0.22), (b) Black patients (p=0.41), (c) those whose income level was below the medium income level of Philadelphia (p=0.79), and (d) those whose income level was above the medium income level of Philadelphia (p=0.15).
Figure 3.
Social determinants of health impacting the timing of radiation delivery for brain metastases patients. Kaplan–Meyer survival curves were done to compared groups who received ≥80% of whole-brain radiotherapy in the AM vs. ≥80% PM for specified patient subsets: (a) white patients (p=0.22), (b) Black patients (p=0.41), (c) those whose income level was below the medium income level of Philadelphia (p=0.79), and (d) those whose income level was above the medium income level of Philadelphia (p=0.15).
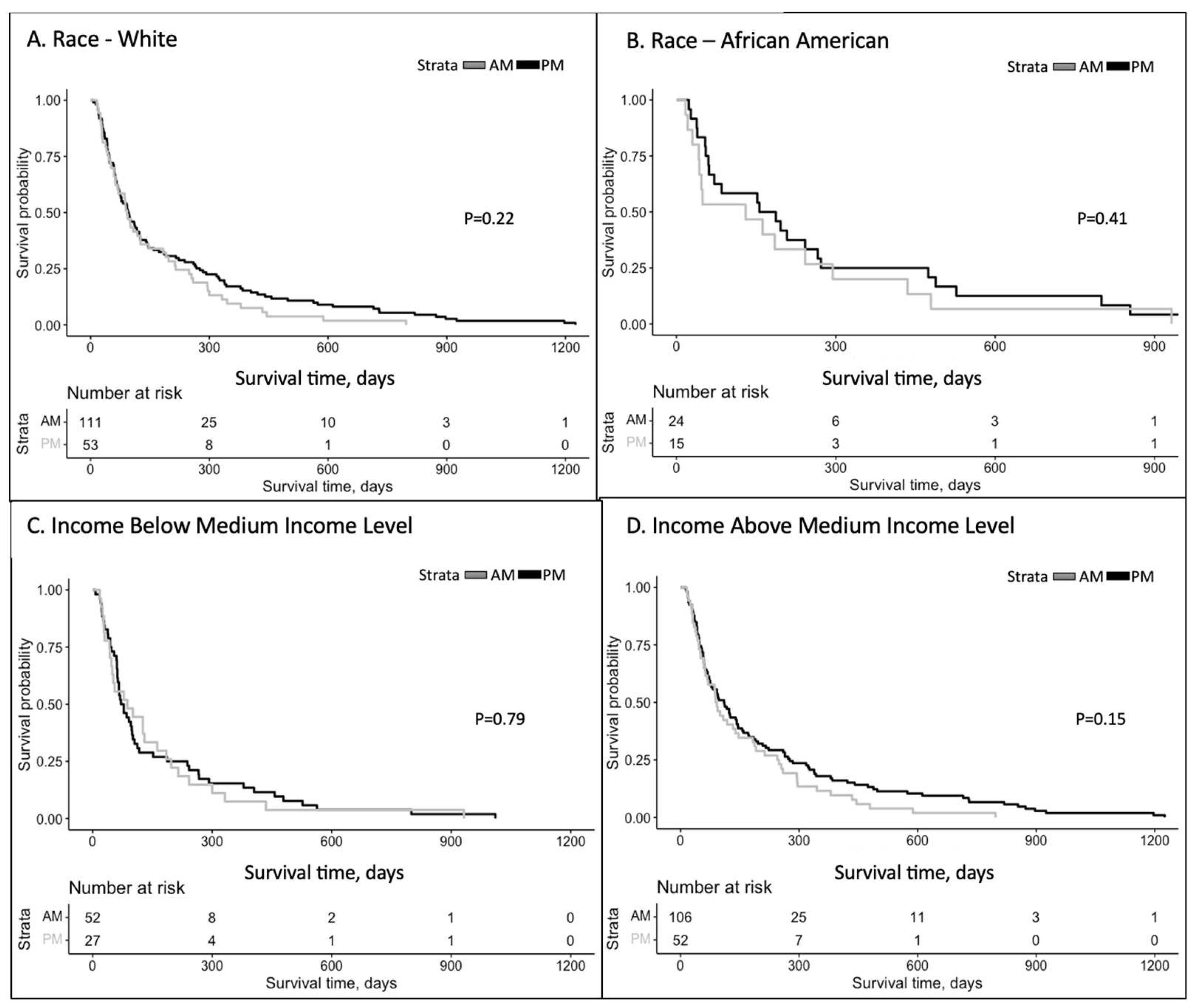

Table 1.
Patient demographics. Patients included in our retrospective analysis received whole-brain radiotherapy for brain metastasis, given that at least 80% of their total dose was received either before 12:00pm (≥80% AM) or after 12:00pm (≥80% PM).
Table 1.
Patient demographics. Patients included in our retrospective analysis received whole-brain radiotherapy for brain metastasis, given that at least 80% of their total dose was received either before 12:00pm (≥80% AM) or after 12:00pm (≥80% PM).
| Patients. | ≥80% AM Treatment % (n=158) | ≥80% PM Treatment % (n=79) | All patients |
| Deceased | 133 (84.18%) | 71 (89.87%) | 204 (86.08%) |
| Alive | 25 (15.82%) | 8 (10.13%) | 33 (13.92%) |
| Total | 158 | 79 | 237 |
| Sex | ≥80% AM | ≥80% PM | All ≥80% |
| Female | 100 (63.29%) | 47 (59.49%) | 147 (62.03%) |
| Male | 58 (36.71%) | 32 (40.51%) | 90 (37.97%) |
| Age at Dx | ≥80% AM | ≥80% PM | All ≥80% |
| <65 Years | 76 (48.10%) | 41 (51.90%) | 117 (49.37%) |
| ≥65 Years | 82 (51.90%) | 38 (48.10%) | 120 (50.63%) |
| Primary Site | ≥80% AM | ≥80% PM | All ≥80% |
| Breast | 28 (17.72%) | 15 (18.99%) | 43 (18.14%) |
| Lung | 84 (53.16%) | 43 (54.43%) | 127 (53.59%) |
| Other | 39 (24.68%) | 19 (24.05%) | 58 (24.47%) |
| Unknown | 7 (4.43%) | 2 (2.53%) | 9 (3.80%) |
| Primary Controlled | ≥80% AM | ≥80% PM | All ≥80% |
| Yes | 43 (27.22%) | 31 (39.24%) | 74 (31.22%) |
| No | 108 (68.35%) | 47 (59.49%) | 155 (65.40%) |
| N/A | 7 (4.43%) | 1 (1.27%) | 8 (3.38%) |
| KPS Index | ≥80% AM | ≥80% PM | All ≥80% |
| 70 | 97 (61.39%) | 47 (59.49%) | 144 (60.76%) |
| <70 | 33 (20.89%) | 16 (20.25%) | 49 (20.68%) |
| N/A | 28 (17.72%) | 16 (20.25%) | 44 (18.57%) |
| RPA Group | ≥80% AM | ≥80% PM | All ≥80% |
| Class 1 | 17 (10.76%) | 16 (20.25%) | 33 (13.92%) |
| Class 2 | 80 (50.63%) | 31 (39.24%) | 111 (46.84%) |
| Class 3 | 32 (20.25%) | 17 (21.52%) | 49 (20.68%) |
| N/A | 29 (18.35%) | 15 (18.99%) | 44 (18.57%) |
| Race/Ethnicity | ≥80% AM | ≥80% PM | All ≥80% |
| Asian | 4 (2.53%) | 1 (1.27%) | 5 (2.11%) |
| Black | 24 (15.19%) | 15 (18.99%) | 39 (16.46%) |
| Hispanic | 4 (2.53%) | 1 (1.27%) | 5 (2.11%) |
| White | 111 (70.25%) | 53 (67.09%) | 164 (69.25%) |
| N/A | 15 (9.49%) | 9 (11.39%) | 24 (10.13%) |
| BMI | ≥80% AM | ≥80% PM | All ≥80% |
| <25 | 60 (37.97%) | 31 (39.24%) | 91 (38.40%) |
| 25–30 | 48 (30.38%) | 21 (26.58%) | 69 (29.11%) |
| >30 | 38 (24.05%) | 22 (27.85%) | 60 (25.32%) |
| N/A | 12 (7.59%) | 5 (6.33%) | 17 (7.17%) |
| Patient Zip Code Median Income | ≥80% AM | ≥80% PM | All ≥80% |
| <$57,550K | 52 (32.91%) | 27 (34.18%) | 79 (33.33%) |
| >$57,500K | 106 (67.09%) | 52 (65.82%) | 158 (66.67%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



