
Submitted:
29 January 2024
Posted:
29 January 2024
You are already at the latest version
Abstract
Background
Few data exist on comparative long-term outcomes of severe aortic stenosis (AS) patients with different flow-gradient patterns undergoing transcatheter aortic valve implantation (TAVI). This study sought to evaluate the impact of pre-TAVI flow-gradient pattern on long-term clinical outcomes after TAVI and assess changes in left ventricular ejection fraction (LVEF) of different subtypes of AS patients following TAVI.
Methods
Consecutive patients with severe AS undergoing TAVI in our institution were screened and prospectively enrolled. Patients were divided in four subgroups according to pre-TAVI flow/gradient pattern: (i) low flow - low gradient (LF-LG): stroke volume indexed (SVi) ≤ 35ml/m2 and mean gradient (MG) < 40mmHg), (ii) normal flow - low gradient (NF-LG): SVi > 35ml/m2 and MG < 40mmHg, (iii) low flow - high gradient (LF-HG) : SVi
≤ 35ml/m2 and MG ≥ 40mmHg and (iv) normal flow - high gradient (NF-HG): SVi > 35 ml/m2 and MG ≥ 40mmHg. Transthoracic echocardiography was repeated at 1-year follow-up. Clinical follow-up was obtained at 12 months, and yearly thereafter until 5-year follow up was complete for all patients.
Results
A total of 272 patients with complete echocardiographic and clinical follow-up were included in our analysis. Their mean age was 80±7 years and the majority of patients (N=138, 50.2%) were women. 62 patients (22.8% of the study population) were distributed in LF-LG group, 98 patients (36%) were LF-HG patients, 95 patients (34.9%) were NF-HG, while 17 patients (6.3%) were NF-LG. There was a greater prevalence of comorbidities among LF-LG AS patients. One-year all-cause mortality differed significantly between the four subgroups of AS patients (log rank p: 0.022) and was more prevalent among LF-LG patients (25.8%) compared to LF-HG (11.3%), NF-HG (6.3%) and NF-LG patients (18.8%). At 5-year follow-up, global mortality remained persistently higher among LF-LG patients (64.5%) compared to LF-HG (47.9%), NF-HG (42.9%) and NF-LG patients (58.8%) (log rank p: 0.029). At multivariable Cox hazard regression analysis, baseline SVi (HR: 0.951, 95% C.I.; 0.918 – 0.984), the presence of at least moderate tricuspid regurgitation at baseline (HR: 3.091, 95% C.I: 1.645 - 5.809) and at least moderate paravalvular leak (PVL) post-TAVI (HR: 1.456 , 95% C.I.: 1.106 - 1.792 ) were significant independent predictors of late global mortality. LF-LG patients and LF-HG patients exhibited a significant increase in LVEF at 1-year follow-up. A lower LVEF (p<0.001) and a lower Svi (p<0.001) at baseline were associated with LVEF improvement at 1 year.
Conclusions
Patients with LF-LG AS have acceptable 1-year outcomes with significant improvement in LVEF at 1-year follow-up, but exhibit an exceedingly high 5-year mortality following TAVI. The presence of low transvalvular flow and at least moderate tricuspid regurgitation at baseline and significant paravalvular leak post-TAVI were associated with poorer long-term outcomes in the entire cohort of AS patients. The presence of a low LVEF or a low SVi predicts LVEF improvement at 1-year.
Keywords:
flow
; gradient
; aortic stenosis
; transcatheter aortic valve implantation
; mortality
; long term
; left ventricular ejection fraction
Clinical Perspective
- ▪ Low flow-low gradient (LF-LG) aortic stenosis (AS) patients consistently exhibit poorer clinical outcomes up to 5 years of follow-up after transcatheter aortic valve implantation (TAVI) compared to other subtypes of AS patients.
- ▪ Low flow AS patients derive the greatest benefit in terms of left ventricular ejection fraction (LVEF) improvement at 1 year following TAVI.
- ▪ Tricuspid regurgitation at baseline and post-TAVI paravalvular leak (PVL) have detrimental long-term prognostic value and could dictate a closer surveillance of TAVI patients.
1. Introduction
Based on the current European and American guidelines, severe aortic stenosis (AS) is defined as an effective aortic valve area (AVA) of <1 cm2 (or indexed for body surface area [BSA], AVA/BSA <0.6 cm2/m2) and a mean pressure gradient (MPG) and peak velocity (Vmax) of ≥ 40 mmHg and ≥ 4.0 m/s, respectively [1,2]. However, in clinical practice there is frequently an inconsistency in diagnostic criteria in patients in whom AS appears to be severe based on AVA but moderate or even mild based on transvalvular gradients [3,4,5,6,7]. This inconsistency is caused by a reduced left ventricular (LV) stroke volume, which leads to a reduction of transaortic flow and gradient. A low-flow, low-gradient (LF-LG) severe AS in relation to a decrease in left ventricular ejection fraction (LVEF) (i.e. LVEF<50%) (low EF, LF-LG AS) may be observed in approximately 5% to 10% of patients with severe AS [8,9]. Conservative management of these patients has been associated with a dismal prognosis, with survival rates <70% and <50% at 1-and 3-year follow-up, respectively [10]. In the last years, a second type of LF-LG AS patients has been recognised with low-flow conditions caused by a decreased stroke volume due to a small LV cavity size and a restrictive physiology [5]. This phenomenon has been described as “paradoxical” low-flow, low-gradient AS (PLF-LGAS), as it might be observed despite a preserved EF (LVEF ≥50%) in approximately 10%-25% of patients with severe AS [7,11,12,13,14]. In patients with LFLG-AS, surgical aortic valve replacement (SAVR) has been associated with a significant improvement of mid- to long-term survival, but operative mortality remains high (6% to 30%) [9,15,16,17].
Transcatheter aortic valve implantation (TAVI) has revolutionized the treatment of severe AS, since its introduction into clinical practice as an alternative option to surgical aortic valve replacement (SAVR) in intermediate and high to prohibitive risk patients [18,19,20,21,22]. In the last years, numerous technological refinements and the growing experience have expanded the indications for TAVI towards treatment of younger, lower risk patients [23,24]. The increased number of AS patients, who are appropriate candidates for TAVI has created a wide spectrum of AS patients with different phenotypes, in which TAVI long term safety and efficacy has not yet been well investigated. Recent observational studies have suggested that TAVI represents an alternative treatment strategy to SAVR for treating patients with LFLG-AS [25,26,27,28,29,30,31,32,33,34]. Yet, these data are limited by their retrospective nature and relatively short duration of follow-up. Hence, an ongoing debate exists concerning the therapeutic advantages of TAVI across the various AS phenotypes based on flow/gradient pattern. The aim of our study was to assess late clinical outcomes and their contributing factors as well as LVEF changes over time following TAVI in the entire spectrum of AS patients based on the baseline flow/gradient pattern.
2. Methods
2.1. Study Population
All patients with severe symptomatic AS referred for TAVI in our institution between January 1, 2015, and December 31, 2018 were screened for inclusion in our study. Patient enrollment and data collection started on January 2015 and 302 patients were prospectively enrolled until December 2018. Echocardiograms at baseline and one year after TAVI were acquired for longitudinal data analysis. Patients were followed up by clinical visits or phone contact at 12 months after TAVI and yearly thereafter until all patients completed the 5-year follow up. Only patients with available clinical and echocardiographic data were included in the study. Indication for TAVI was based on the assessment of the Heart Team of our institution, taking into account clinical, anatomical and echocardiographic characteristics according to the guidelines. All participants underwent comprehensive physical examination, coronary angiography and multi-slice computed tomography (MSCT) before TAVI. Informed consent was obtained from all subjects involved in the study. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of our institution (Hippokration General Hospital of Athens). A total of 30 patients were excluded due to missing clinical follow-up data or unavailable echocardiograms. Self-expandable transcatheter heart valves were implanted in all patients. Transfemoral access was the preferred access, whereas subclavian access was used only in patients with inappropriate iliofemoral anatomy.
2.2. Clinical Data
Baseline demographic characteristics (sex, gender, age, body mass index), comorbidities (diabetes mellitus, hypertension, coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD), peripheral arterial disease (PAD), chronic kidney disease (CKD), history of myocardial infarction (MI), previous cardiac interventions; percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery (CABG), Euroscore II (European system for cardiac operative risk evaluation) and NYHA (New York Heart Association) functional class were recorded. The presence of CAD was defined as a history of percutaneous coronary intervention or surgical treatment or the presence of angiographically significant stenosis (>50%) in at least one epicardial coronary artery. CKD was defined according to Kidney Disease Improving Global Outcomes (KDIGO) criteria.
2.3. Doppler Echocardiography
All patients underwent comprehensive echocardiographic examination pre-TAVI and at 1-year post-TAVI. Echocardiographic parameters included the following variables: mean transvalvular gradient, peak aortic jet velocity (Vmax), aortic jet velocity time integral (VTI), LV outflow tract (LVOT) diameter, LVOT VTI, AVA and stroke volume (SV). AVA was estimated using the continuity equation. SV was calculated using the cross-sectional area of the LVOT and VTI of the LVOT flow as follows: SVLVOT= (cross-sectional areaLVOT)*VTILVOT. VTILVOT was acquired by the pulsed wave Doppler technique. Stroke volume index (SVi) was measured using the following equation: SV/BSA (Body Surface Area). LVEF was measured by the biplane Simpson method.
Severe AS is defined as an effective aortic valve area (AVA) of <1 cm2 (or indexed for [BSA], AVA/BSA <0.6 cm2/m 2) a mean pressure gradient (MPG) of ≥40 mmHg and peak aortic velocity (Vmax) of >4.0 m/s. Low-flow (LF) was defined as a LV stroke volume index (SVi) ≤ 35mL/m2, normal flow (NF) as SVi > 35ml/m 2, low-gradient (LG) as a mean transvalvular gradient <40 mm Hg and high gradient (HG) as a mean gradient ≥ 40 mmηg2. Accordingly, based on transvalvular flow (F) and gradient (G) we have divided our patients in four distinct subgroups; low-flow, high-gradient (LF-HG), low-flow, low-gradient (LF-LG), normal-flow, high-gradient (NF-HG) and normal-flow, low-gradient (NF-LG). (Table 1).
2.4. Study Endpoints
The primary endpoints were: 1) early (1-year) and late (5-year) all-cause mortality and changes in LVEF from baseline to 1-year follow up. Secondary endpoints were 1-year and 5-year cardiovascular mortality, 1-year MACE (Major Adverse Cardiovascular Events) rates, periprocedural events (permanent pacemaker implantation, major vascular complications, major bleeding complications at 30 days following TAVI) and factors associated with increased late global mortality and LVEF improvement at 1 year. MACE is a composite outcome, which includes all-cause mortality, non-fatal MI and non-fatal stroke. The definition and the evaluation of clinical events was performed according to VARC-2 (Valve Academic Research Consortium-2) criteria. Bleeding events were considered as major, when they were categorized as grade 3-5, according to Bleeding Academy Research Consortium (BARC).
2.5. Statistical Analysis
Continuous data were expressed as mean ± SD or median (interquartile range) and were tested for the normality of distribution with the Shapiro-Wilk test. Categorical data were expressed as numbers and percentages. Patients were compared with the Student’s t-test or the Wilcoxon rank sum test for continuous variables and with the chi-square test or Fisher exact test for categorical variables, as appropriate. Kaplan-Meier curves and log-rank test of the time-to-event data were used to evaluate global and cardiovascular mortality. The association between baseline clinical, echocardiographic variables and periprocedural variables with global mortality was assessed with the use of Cox proportional hazard analyses. Variables with a p value <0.10 in univariable analysis were entered into the multivariable model. A paired samples t-test was used to analyze the changes in LVEF over time. The predictors of improvement in LVEF at 1-year follow-up were determined using a linear regression analysis. All p-values <0.05 were considered statistically significant. Statistical analysis was performed using the statistical package SPSS (version 26, SPSS Inc., Chicago, IL, USA).
3. Results
Between January 1, 2015, and December 31, 2018, a total of 302 patients undergoing TAVI in our center were screened and considered as eligible for inclusion in the study. Completed echocardiographic and clinical follow-up up to five years was available in 272 patients. Baseline demographic and clinical characteristics are presented comprehensively in Table 2. Mean age was 80±7 years and 51.8% were women. The median Euroscore II was 5.14 {interquartile range (IQR): 4.22-6.48}. LF-LG AS was present in 62 patients, while 95 patients presented with NF-HG AS, 98 patients had LF-HG AS and 17 patients presented with NF-LG AS. LF-LG AS patients had a higher prevalence of previous myocardial infarction (MI) (p=0.005) and showed a trend towards a greater prevalence of comorbidities such as peripheral artery disease and at least moderate mitral regurgitation. This was reflected by the significantly higher Euroscore II in the LF-LG group compared with the other groups of patients (p=0.004 for between group difference). History of CABG was more common among LG compared to HG patients.
Echocardiographic and MSCT- derived variables were compared between the different groups of AS patients. Baseline LVEF, mean gradient, AVA and SVi were significantly lower among LF-LG patients (all p<0.001). There was no significant difference in the pre-TAVI pulmonary artery systolic pressure between groups. The rate of severe aortic valve (AV) calcification assessed semi-quantitatively by MSCT was also comparable between groups (Table 3).
3.1. One-Year and Late Clinical Outcomes
The one-year clinical outcomes are shown in Table 4. One-year all-cause mortality was significantly higher in LF-LG patients compared to NF-HG patients (25.8% vs 6.3% respectively, p=0.011) but not compared to NF-LG (25.8% vs 18.8% respectively, p=0.729) or LF-HG patients (25.8% vs 11.5% respectively, p=0.084) (Table 4). Median follow up duration was 59 months (IQR: 31 to 81 months) and the late cumulative clinical outcomes are shown in Table 4. A total of 137 patients died at five-year follow up, leading to a global cumulative mortality of 50.36%. Death was from cardiovascular causes in 75 patients (27.57%). Five-year all-cause mortality was significantly higher in LF-LG patients compared to NF-HG patients (64.5% vs 42.5% respectively, p=0.038) but not compared to NF-LG patients (64.5% vs 58.8% respectively, p=1.00) and LF-HG patients (64.5% vs 47.9% respectively, p=0.152). This was confirmed by the multivariable Cox proportional hazard regression analysis, where the presence of LF-LG AS was independently associated with increased late all-cause mortality (HR: 1.757, p=0.018) with NF-HG AS being the reference standard.
One-year cardiovascular mortality differed significantly between the four subgroups of AS patients (p=0.018), which was driven primarily by the significantly higher cardiovascular mortality of LF-LG compared to LF-HG patients (19.3% vs 3.1% respectively, p=0.008). At 5-year follow-up, cardiovascular mortality was significantly higher in LF-LG patients (53.2%), compared to LF-HG (21.4%, p=0.001) and NF-HG patients (17.9%, p=0.001) but not compared to NF-LG patients (23.5%, p=0.075). The Kaplan-Meier curves for global and cardiovascular mortality at 1-year and 5-year follow-up are shown in Figure 1A, Figure 1B and Figure 2A, Figure 2B respectively.
Incidence of one-year MACCE (a composite endpoint of death, non-fatal MI, non-fatal stroke) was significantly higher in patients with LF-LG pattern, compared to NF-HG patients (25.8% vs 8.4% respectively, p=0.029), but was comparable to NF-LG and LF-HG patients (p=1.00 and p= 0.092 respectively). No statistically significant between groups differences were observed regarding the rates of periprocedural events (permanent pacemaker implantation, major vascular complications and life-threatening/major bleeding complications at 30 days following TAVI). (Table 5).
3.2. Predictors of Late Global Mortality
The factors associated with long term all-cause mortality in univariate analysis were included in the multivariate model (Table 6). In a multivariable Cox proportional hazards model, the independent predictors of late global mortality after TAVI in the entire cohort were transvalvular flow and the presence of at least moderate tricuspid regurgitation at the baseline echocardiographic evaluation (HR: 3.091, 95% CI: 1.645 -5.809, p<0.001) as well as the presence of moderate or greater post-TAVI PVL (paravalvular leak) (HR: 1.456 95% CI: 1.106 -1.792, p=0.042).
3.3. Impact of Pre-Tavi Flow on Late Outcomes
Patients who exhibited low flow pre-procedurally by means of the Doppler-based estimation of SVi had increased 5 year all-cause and cardiovascular mortality compared to patients with normal flow, which is depicted in the respective Kaplan-Meier survival curves (Figure 3A and Figure 3B respectively). This was confirmed in the multivariable Cox proportional hazard regression analysis, where SVi emerged as a significant independent predictor of late global mortality after TAVI (HR:0.951 per unit increase of SVi, p=0.004).(Table 6).
3.4. Changes in LVEF over Time
A total of 282 patients had an echocardiographic examination at 1 year follow up (93.3% of the initially screened population) and all of them had a baseline echocardiogram for comparison. Among the patients included in the study, 70 patients (25.7%) exhibited some degree of improvement in LVEF at follow-up (mean increase of 3.23%; 95% C.I.: 1.67% to 4.83%, p<0.001). Patients in the LF-LG and LF-HG subgroups had a statistically significant increase in LVEF over time (p=0.023 and p=0.003 respectively), while in NF-LG and NF-HG patients no impact was observed on their LVEF 1 year after TAVI (Figure 4).
In multivariable linear regression analysis, the factors independently associated with LVEF improvement at 1 year follow up was the presence of a lower LVEF at baseline (OR: 0.906, 95% CI: 0.873-0.940, p<0.001, per unit increase of baseline LVEF) and the presence of a lower SVi at baseline (OR:0.898, 95% CI: 0.864-0.931, p<0.001, per unit increase of SVi).
4. Discussion
The evolving clinical indications for TAVI have been recently illustrated by the results of several randomized trials, collectively showing TAVI to represent a valid alternative to SAVR for patients with intermediate to high operative risk [35]. Recent observational studies dedicated to LF-LG AS patients have outlined favorable early outcomes following TAVI [36] with lower 30-day mortality rates compared to those reported in prior TAVI studies evaluating LF-LG AS patients [37,38] as well as SAVR studies in LF-LG AS, despite including younger and lower risk patients [9,10,16,17,38,39,40,41,42,43]. However, despite the good early results post-TAVI in LF-LG AS patients and the constant optimization of the final hemodynamic result achieved with the latest THVs (transcatheter heart valves), the mid-term all-cause mortality remains high with approximately one third of LF-LG patients dying after a median follow-up of 2 years [44]. Our study wished to expand on that knowledge and investigate whether this rise in all-cause mortality in LF-LG AS patients persists up to 5 years of follow-up and holds statistical significance over the other subgroups of AS patients.
Our study confirms the relatively high one-year mortality among LF-LG AS patients reported in previous studies as approximately one fourth of LF-LG patients had died at 1 year following TAVI. The excess in global mortality among LF-LG patients can be seen throughout the follow-up period up to 5 years [33,38]. In particular, LF-LG patients exhibited greater 5-year all-cause as well as cardiovascular mortality rates compared to NF-HG AS patients, while there was a trend towards greater long-term all-cause mortality compared to LF-HG and NF-LG patients. The main factors associated with poorer long-term outcomes after TAVI was the presence of a low transvalvular flow and at least moderate tricuspid regurgitation at the baseline echocardiographic evaluation and the presence of at least moderate paravalvular leak following TAVI. In line with the staging classification of the extent of cardiac damage associated with AS proposed by Genereux et al., our findings add to the prognostic value of tricuspid regurgitation, the latter being a marker of advanced cardiac damage in AS patients [45]. Of note, we have shown that tricuspid regurgitation is a powerful predictor of long-term all-cause mortality after TAVI beyond 1 year.
Some studies suggested that TAVI may be associated with enhanced and more rapid recovery of LV function compared with SAVR especially among patients with depressed systolic function, and this could be of major importance in patients with LFLG-AS [32,34]. Indeed, in our study approximately 50% of LF-LG patients improved their LVEF at 1-year follow-up and there was a greater improvement in LVEF at 1-year among LF-LG and LF-HG patients compared to NF-LG and NF-HG patients. In fact, LVEF recovery at 1-year follow-up was predicted by a lower baseline LVEF and stroke volume index, which could probably leave more space for improvement over time.
5. Limitations
Our study has several limitations that should be addressed. Firstly, this was a single center study. Whereas most patients were included in this study prospectively, data were collected retrospectively in about one-half of the patients. The study had no onsite monitoring or event adjudication committee. This was partially compensated by remote electronic data monitoring to actively search and correct missing and/or inconsistent information, including a thorough evaluation of the causes of mortality. In addition, no centralized echocardiography core lab analysis was performed on the echocardiographic data. We acknowledge that the number of primary endpoint events was small to allow for genereralization of our findings. Finally, we could not systematically collect and provide DSE (dobutamine stress echocardiography) data on LF-LG patients with low LVEF and assess its prognostic relevance.
6. Conclusions
Patients with LF-LG AS have acceptable 1-year outcomes with significant improvement in LVEF at 1 year follow-up, but exhibit an exceedingly high 5-year mortality following TAVI. The presence of low transvalvular flow and at least moderate tricuspid regurgitation at baseline and significant paravalvular leak post- TAVI were associated with poorer long-term outcomes in the entire cohort of AS patients. The presence of a low LVEF or a low SVi predicts LVEF improvement at 1-year.
Author Contributions
Conceptualization, G.O., M.D.; Methodology, G.O., A.A.; Formal Analysis, G.O.; Investigation, C.S., M.K., A.A.; Data Curation, M.X., P.T., C.S., N.K.,M.K.; Writing – Original Draft Preparation, G.O., A.A.; Writing – Review & Editing, M.D.; Supervision, K.S., G.L., A.S.; Project Administration, C.T., K.T.; Funding Acquisition, K.T.”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Hippokration General Hospital of Athens.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data presented in the study are available to the editors upon request.
Abbreviations
AS: Aortic stenosis
AV: Aortic valve
AVA: Aortic valve area
CABG: Coronary artery bypass graft
CKD: Chronic kidney disease
COPD: Chronic obstructive pulmonary disease
CV: Cardiovascular
DSE: Dobutamine stress echocardiography
F: Flow
HG: High gradient
LF-LG: Low flow- low gradient
LVEF: Left ventricular ejection fraction
MACCE: Major adverse cardiovascular and cerebrovascular events
MG: Mean gradient
MI: Myocardial infarction
MR: Mitral regurgitation
MSCT: Multi-slice computed tomography
PAD: Peripheral artery disease
PASP: Pulmonary artery systolic pressure
PCI: Percutaneous coronary intervention
PVL: Paravalvular leak
SAVR: Surgical aortic valve replacement
SVi: Stroke volume indexed
TAVI: Transcatheter aortic valve implantation
TR: Tricuspid regurgitation
References
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, Jneid H, Krieger E V., Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143. [CrossRef]
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W, Neumann F-J, Myers P, Abdelhamid M, Achenbach S, Asteggiano R, Barili F, Borger MA, Carrel T, Collet J-P, Foldager D, Habib G, Hassager C, Irs A, Iung B, Jahangiri M, Katus HA, Koskinas KC, Massberg S, Mueller CE, Nielsen JC, Pibarot P, Rakisheva A, Roffi M, Rubboli A, Shlyakhto E, Siepe M, Sitges M, Sondergaard L, Sousa-Uva M, Tarantini G, Zamorano JL, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W, Benchabi Y, Chilingaryan A, Metzler B, Rustamova Y, Shumavets V, Lancellotti P, Smajic E, Trendafilova-Lazarova D, Samardzic J, Karakyriou M, Palecek T, Sanchez Dahl J, Meshaal MS, Palm K, Virtanen M, Bouleti C, Bakhutashvili Z, Achenbach S, Boutsikou M, Kertész AB, Danielsen R, Topilsky Y, Golino P, Tuleutayev R, Elezi S, Kerimkulov A, Rudzitis A, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561–632. [CrossRef]
- Clavel M-A, Dumesnil JG, Capoulade R, Mathieu P, Sénéchal M, Pibarot P. Outcome of Patients With Aortic Stenosis, Small Valve Area, and Low-Flow, Low-Gradient Despite Preserved Left Ventricular Ejection Fraction. J Am Coll Cardiol. 2012;60:1259–1267. [CrossRef]
- Lauten J, Rost C, Breithardt OA, Seligmann C, Klinghammer L, Daniel WG, Flachskampf FA. Invasive Hemodynamic Characteristics of Low Gradient Severe Aortic Stenosis Despite Preserved Ejection Fraction. J Am Coll Cardiol. 2013;61:1799–1808. [CrossRef]
- Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical Low-Flow, Low-Gradient Severe Aortic Stenosis Despite Preserved Ejection Fraction Is Associated With Higher Afterload and Reduced Survival. Circulation. 2007;115:2856–2864. [CrossRef]
- Dumesnil JG, Pibarot P. Low-flow, low-gradient severe aortic stenosis in patients with normal ejection fraction. Curr Opin Cardiol. 2013;28:524–530. [CrossRef]
- Pibarot P, Dumesnil JG. Low-Flow, Low-Gradient Aortic Stenosis With Normal and Depressed Left Ventricular Ejection Fraction. J Am Coll Cardiol. 2012;60:1845–1853. [CrossRef]
- Kulik A, Burwash IG, Kapila V, Mesana TG, Ruel M. Long-Term Outcomes After Valve Replacement for Low-Gradient Aortic Stenosis. Circulation. 2006;114. [CrossRef]
- Connolly HM, Oh JK, Schaff H V., Roger VL, Osborn SL, Hodge DO, Tajik AJ. Severe Aortic Stenosis With Low Transvalvular Gradient and Severe Left Ventricular Dysfunction. Circulation. 2000;101:1940–1946. [CrossRef]
- Monin J-L, Quéré J-P, Monchi M, Petit H, Baleynaud S, Chauvel C, Pop C, Ohlmann P, Lelguen C, Dehant P, Tribouilloy C, Guéret P. Low-Gradient Aortic Stenosis. Circulation. 2003;108:319–324. [CrossRef]
- Minners J, Allgeier M, Gohlke-Baerwolf C, Kienzle R-P, Neumann F-J, Jander N. Inconsistent grading of aortic valve stenosis by current guidelines: haemodynamic studies in patients with apparently normal left ventricular function. Heart. 2010;96:1463–1468. [CrossRef]
- Dumesnil JG, Pibarot P, Carabello B. Paradoxical low flow and/or low gradient severe aortic stenosis despite preserved left ventricular ejection fraction: implications for diagnosis and treatment. Eur Heart J. 2010;31:281–289. [CrossRef]
- Barasch E, Fan D, Chukwu EO, Han J, Passick M, Petillo F, Norales A, Reichek N. Severe isolated aortic stenosis with normal left ventricular systolic function and low transvalvular gradients: pathophysiologic and prognostic insights. J Heart Valve Dis. 2008;17:81–8.
- Adda J, Mielot C, Giorgi R, Cransac F, Zirphile X, Donal E, Sportouch-Dukhan C, Réant P, Laffitte S, Cade S, Le Dolley Y, Thuny F, Touboul N, Lavoute C, Avierinos J-F, Lancellotti P, Habib G. Low-Flow, Low-Gradient Severe Aortic Stenosis Despite Normal Ejection Fraction Is Associated With Severe Left Ventricular Dysfunction as Assessed by Speckle-Tracking Echocardiography. Circ Cardiovasc Imaging. 2012;5:27–35. [CrossRef]
- Pereira JJ, Lauer MS, Bashir M, Afridi I, Blackstone EH, Stewart WJ, McCarthy PM, Thomas JD, Asher CR. Survival after aortic valve replacement forsevere aortic stenosis with low transvalvular gradients and severe left ventricular dysfunction. J Am Coll Cardiol. 2002;39:1356–1363. [CrossRef]
- Levy F, Laurent M, Monin JL, Maillet JM, Pasquet A, Le Tourneau T, Petit-Eisenmann H, Gori M, Jobic Y, Bauer F, Chauvel C, Leguerrier A, Tribouilloy C. Aortic Valve Replacement for Low-Flow/Low-Gradient Aortic Stenosis. J Am Coll Cardiol. 2008;51:1466–1472. [CrossRef]
- Tribouilloy C, Lévy F, Rusinaru D, Guéret P, Petit-Eisenmann H, Baleynaud S, Jobic Y, Adams C, Lelong B, Pasquet A, Chauvel C, Metz D, Quéré J-P, Monin J-L. Outcome After Aortic Valve Replacement for Low-Flow/Low-Gradient Aortic Stenosis Without Contractile Reserve on Dobutamine Stress Echocardiography. J Am Coll Cardiol. 2009;53:1865–1873. [CrossRef]
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, Thourani VH, Tuzcu EM, Miller DC, Herrmann HC, Doshi D, Cohen DJ, Pichard AD, Kapadia S, Dewey T, Babaliaros V, Szeto WY, Williams MR, Kereiakes D, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Moses JW, Trento A, Brown DL, Fearon WF, Pibarot P, Hahn RT, Jaber WA, Anderson WN, Alu MC, Webb JG. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. New England Journal of Medicine. 2016;374:1609–1620. [CrossRef]
- Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Søndergaard L, Mumtaz M, Adams DH, Deeb GM, Maini B, Gada H, Chetcuti S, Gleason T, Heiser J, Lange R, Merhi W, Oh JK, Olsen PS, Piazza N, Williams M, Windecker S, Yakubov SJ, Grube E, Makkar R, Lee JS, Conte J, Vang E, Nguyen H, Chang Y, Mugglin AS, Serruys PWJC, Kappetein AP. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. New England Journal of Medicine. 2017;376:1321–1331. [CrossRef]
- Gleason TG, Reardon MJ, Popma JJ, Deeb GM, Yakubov SJ, Lee JS, Kleiman NS, Chetcuti S, Hermiller JB, Heiser J, Merhi W, Zorn GL, Tadros P, Robinson N, Petrossian G, Hughes GC, Harrison JK, Conte J V., Mumtaz M, Oh JK, Huang J, Adams DH. 5-Year Outcomes of Self-Expanding Transcatheter Versus Surgical Aortic Valve Replacement in High-Risk Patients. J Am Coll Cardiol. 2018;72:2687–2696. [CrossRef]
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S. Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery. New England Journal of Medicine. 2010;363:1597–1607. [CrossRef]
- Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. New England Journal of Medicine. 2011;364:2187–2198. [CrossRef]
- Pibarot P, Salaun E, Dahou A, Avenatti E, Guzzetti E, Annabi M-S, Toubal O, Bernier M, Beaudoin J, Ong G, Ternacle J, Krapf L, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Leipsic J, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Généreux P, Pershad A, Alu MC, Xu K, Rogers E, Webb JG, Smith CR, Mack MJ, Leon MB, Hahn RT. Echocardiographic Results of Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients. Circulation. 2020;141:1527–1537. [CrossRef]
- Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, Forrest JK, Tchétché D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. New England Journal of Medicine. 2019;380:1706–1715. [CrossRef]
- Saybolt MD, Fiorilli PN, Gertz ZM, Herrmann HC. Low-Flow Severe Aortic Stenosis. Circ Cardiovasc Interv. 2017;10. [CrossRef]
- Gotzmann M, Lindstaedt M, Bojara W, Ewers A, Mügge A. Clinical outcome of transcatheter aortic valve implantation in patients with low-flow, low gradient aortic stenosis. Catheterization and Cardiovascular Interventions. 2012;79:693–701. [CrossRef]
- Lauten A, Zahn R, Horack M, Sievert H, Linke A, Ferrari M, Harnath A, Grube E, Gerckens U, Kuck K-H, Sack S, Senges J, Figulla HR. Transcatheter Aortic Valve Implantation in Patients With Low-Flow, Low-Gradient Aortic Stenosis. JACC Cardiovasc Interv. 2012;5:552–559. [CrossRef]
- O’Sullivan CJ, Stortecky S, Heg D, Pilgrim T, Hosek N, Buellesfeld L, Khattab AA, Nietlispach F, Moschovitis A, Zanchin T, Meier B, Windecker S, Wenaweser P. Clinical outcomes of patients with low-flow, low-gradient, severe aortic stenosis and either preserved or reduced ejection fraction undergoing transcatheter aortic valve implantation. Eur Heart J. 2013;34:3437–3450. [CrossRef]
- Elhmidi Y, Piazza N, Krane M, Deutsch M, Mazzitelli D, Lange R, Bleiziffer S. Clinical presentation and outcomes after transcatheter aortic valve implantation in patients with low flow/low gradient severe aortic stenosis. Catheterization and Cardiovascular Interventions. 2014;84:283–290. [CrossRef]
- Kamperidis V, Joyce E, Debonnaire P, Katsanos S, van Rosendael PJ, van der Kley F, Sianos G, Bax JJ, Ajmone Marsan N, Delgado V. Left Ventricular Functional Recovery and Remodeling in Low-Flow Low-Gradient Severe Aortic Stenosis after Transcatheter Aortic Valve Implantation. Journal of the American Society of Echocardiography. 2014;27:817–825. [CrossRef]
- Herrmann HC, Pibarot P, Hueter I, Gertz ZM, Stewart WJ, Kapadia S, Tuzcu EM, Babaliaros V, Thourani V, Szeto WY, Bavaria JE, Kodali S, Hahn RT, Williams M, Miller DC, Douglas PS, Leon MB. Predictors of Mortality and Outcomes of Therapy in Low-Flow Severe Aortic Stenosis. Circulation. 2013;127:2316–2326. [CrossRef]
- Ben-Dor I, Maluenda G, Iyasu GD, Laynez-Carnicero A, Hauville C, Torguson R, Okubagzi P, Xue Z, Goldstein SA, Lindsay J, Satler LF, Pichard AD, Waksman R. Comparison of Outcome of Higher Versus Lower Transvalvular Gradients in Patients With Severe Aortic Stenosis and Low (<40%) Left Ventricular Ejection Fraction. Am J Cardiol. 2012;109:1031–1037. [CrossRef]
- Lauten A, Figulla HR, Möllmann H, Holzhey D, Kötting J, Beckmann A, Veit C, Cremer J, Kuck K-H, Lange R, Zahn R, Sack S, Schuler G, Walther T, Beyersdorf F, Böhm M, Heusch G, Meinertz T, Neumann T, Welz A, Mohr FW, Hamm CW. TAVI for low-flow, low-gradient severe aortic stenosis with preserved or reduced ejection fraction: a subgroup analysis from the German Aortic Valve Registry (GARY). EuroIntervention. 2014;10:850–859. [CrossRef]
- Clavel MA, Webb JG, Rodés-Cabau J, Masson JB, Dumont E, De Larochellière R, Doyle D, Bergeron S, Baumgartner H, Burwash IG, Dumesnil JG, Mundigler G, Moss R, Kempny A, Bagur R, Bergler-Klein J, Gurvitch R, Mathieu P, Pibarot P. Comparison Between Transcatheter and Surgical Prosthetic Valve Implantation in Patients With Severe Aortic Stenosis and Reduced Left Ventricular Ejection Fraction. Circulation. 2010;122:1928–1936. [CrossRef]
- Rodés-Cabau J. Transcatheter aortic valve implantation: current and future approaches. Nat Rev Cardiol. 2012;9:15–29. [CrossRef]
- Ribeiro HB, Lerakis S, Gilard M, Cavalcante JL, Makkar R, Herrmann HC, Windecker S, Enriquez-Sarano M, Cheema AN, Nombela-Franco L, Amat-Santos I, Muñoz-García AJ, Garcia del Blanco B, Zajarias A, Lisko JC, Hayek S, Babaliaros V, Le Ven F, Gleason TG, Chakravarty T, Szeto WY, Clavel M-A, de Agustin A, Serra V, Schindler JT, Dahou A, Puri R, Pelletier-Beaumont E, Côté M, Pibarot P, Rodés-Cabau J. Transcatheter Aortic Valve Replacement in Patients With Low-Flow, Low-Gradient Aortic Stenosis. J Am Coll Cardiol. 2018;71:1297–1308. [CrossRef]
- Herrmann HC, Pibarot P, Hueter I, Gertz ZM, Stewart WJ, Kapadia S, Tuzcu EM, Babaliaros V, Thourani V, Szeto WY, Bavaria JE, Kodali S, Hahn RT, Williams M, Miller DC, Douglas PS, Leon MB. Predictors of Mortality and Outcomes of Therapy in Low-Flow Severe Aortic Stenosis. Circulation. 2013;127:2316–2326. [CrossRef]
- Baron SJ, Arnold S V., Herrmann HC, Holmes DR, Szeto WY, Allen KB, Chhatriwalla AK, Vemulapali S, O’Brien S, Dai D, Cohen DJ. Impact of Ejection Fraction and Aortic Valve Gradient on Outcomes of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2016;67:2349–2358. [CrossRef]
- Connolly HM, Oh JK, Orszulak TA, Osborn SL, Roger VL, Hodge DO, Bailey KR, Seward JB, Tajik AJ. Aortic Valve Replacement for Aortic Stenosis With Severe Left Ventricular Dysfunction. Circulation. 1997;95:2395–2400. [CrossRef]
- Clavel M-A, Berthelot-Richer M, Le Ven F, Capoulade R, Dahou A, Dumesnil JG, Mathieu P, Pibarot P. Impact of Classic and Paradoxical Low Flow on Survival After Aortic Valve Replacement for Severe Aortic Stenosis. J Am Coll Cardiol. 2015;65:645– 653. [CrossRef]
- Quere J-P, Monin J-L, Levy F, Petit H, Baleynaud S, Chauvel C, Pop C, Ohlmann P, Lelguen C, Dehant P, Gueret P, Tribouilloy C. Influence of Preoperative Left Ventricular Contractile Reserve on Postoperative Ejection Fraction in Low-Gradient Aortic Stenosis. Circulation. 2006;113:1738–1744. [CrossRef]
- Monin J-L, Monchi M, Kirsch MEW, Petit-Eisenmann H, Baleynaud S, Chauvel C, Metz D, Adams C, Quere J-P, Gueret P, Tribouilloy C. Low-gradient aortic stenosis: impact of prosthesis-patient mismatch on survival. Eur Heart J. 2007;28:2620–2626. [CrossRef]
- Vaquette B. Valve replacement in patients with critical aortic stenosis and depressed left ventricular function: predictors of operative risk, left ventricular function recovery, and long term outcome. Heart. 2005;91:1324–1329. [CrossRef]
- Ribeiro JM, Teixeira R, Siserman A, Puga L, Lopes J, Sousa JP, Lourenço C, Belo A, Gonçalves L. Impact of previous coronary artery bypass grafting in patients presenting with an acute coronary syndrome: Current trends and clinical implications. Eur Heart J Acute Cardiovasc Care. 2020;9:731–740. [CrossRef]
- Généreux P, Pibarot P, Redfors B, Mack MJ, Makkar RR, Jaber WA, Svensson LG, Kapadia S, Tuzcu EM, Thourani VH, Babaliaros V, Herrmann HC, Szeto WY, Cohen DJ, Lindman BR, McAndrew T, Alu MC, Douglas PS, Hahn RT, Kodali SK, Smith CR, Miller DC, Webb JG, Leon MB. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur Heart J. 2017;38:3351–3358. [CrossRef]
Figure 1.
Kaplan-Meier survival curves at 1 year follow-up showing (A) global and (B) cardiovascular mortality across different AS subgroups based on pre-TAVI flow/gradient status. * LF-; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, CV; Cardiovascular.
Figure 1.
Kaplan-Meier survival curves at 1 year follow-up showing (A) global and (B) cardiovascular mortality across different AS subgroups based on pre-TAVI flow/gradient status. * LF-; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, CV; Cardiovascular.
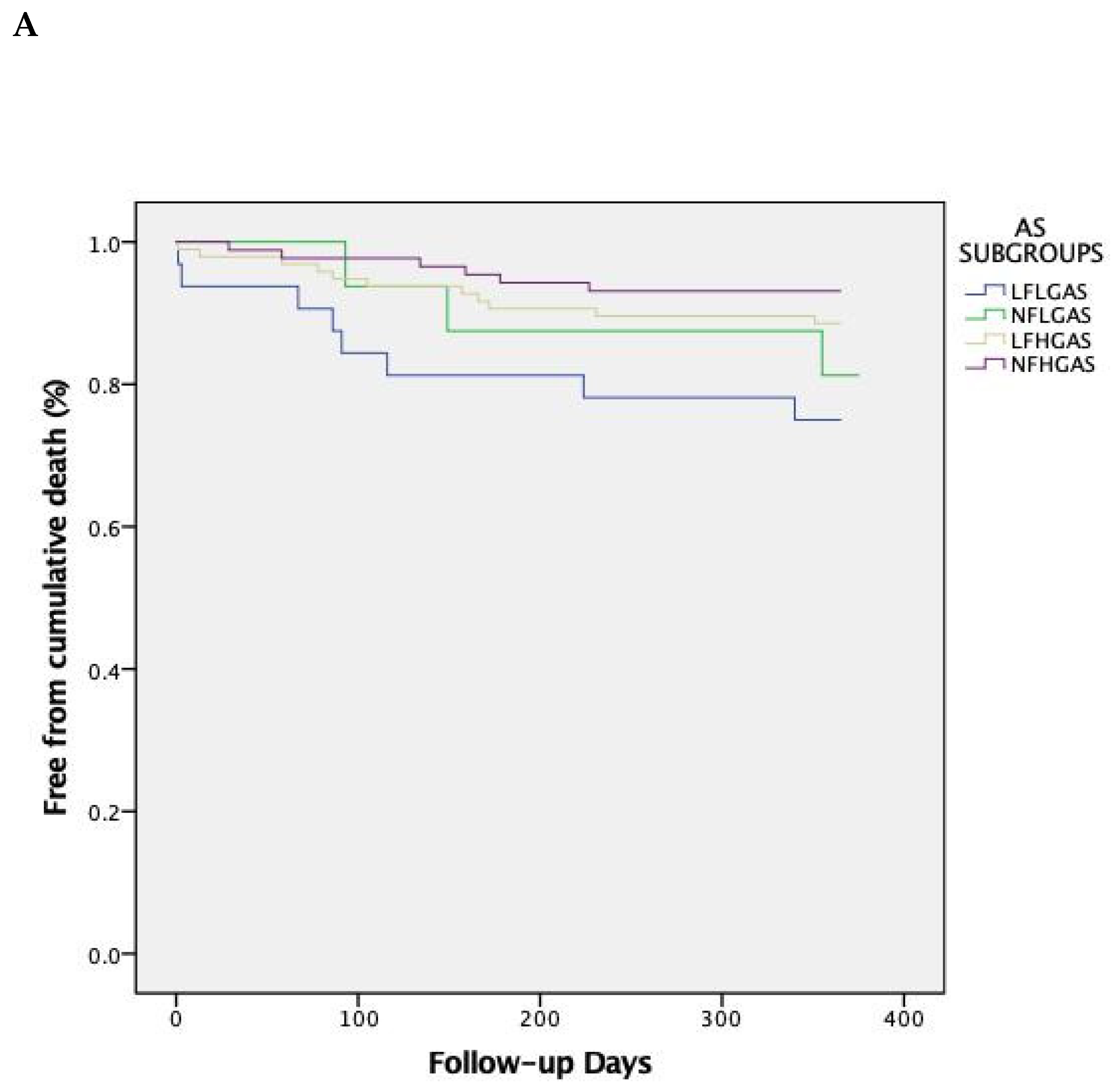
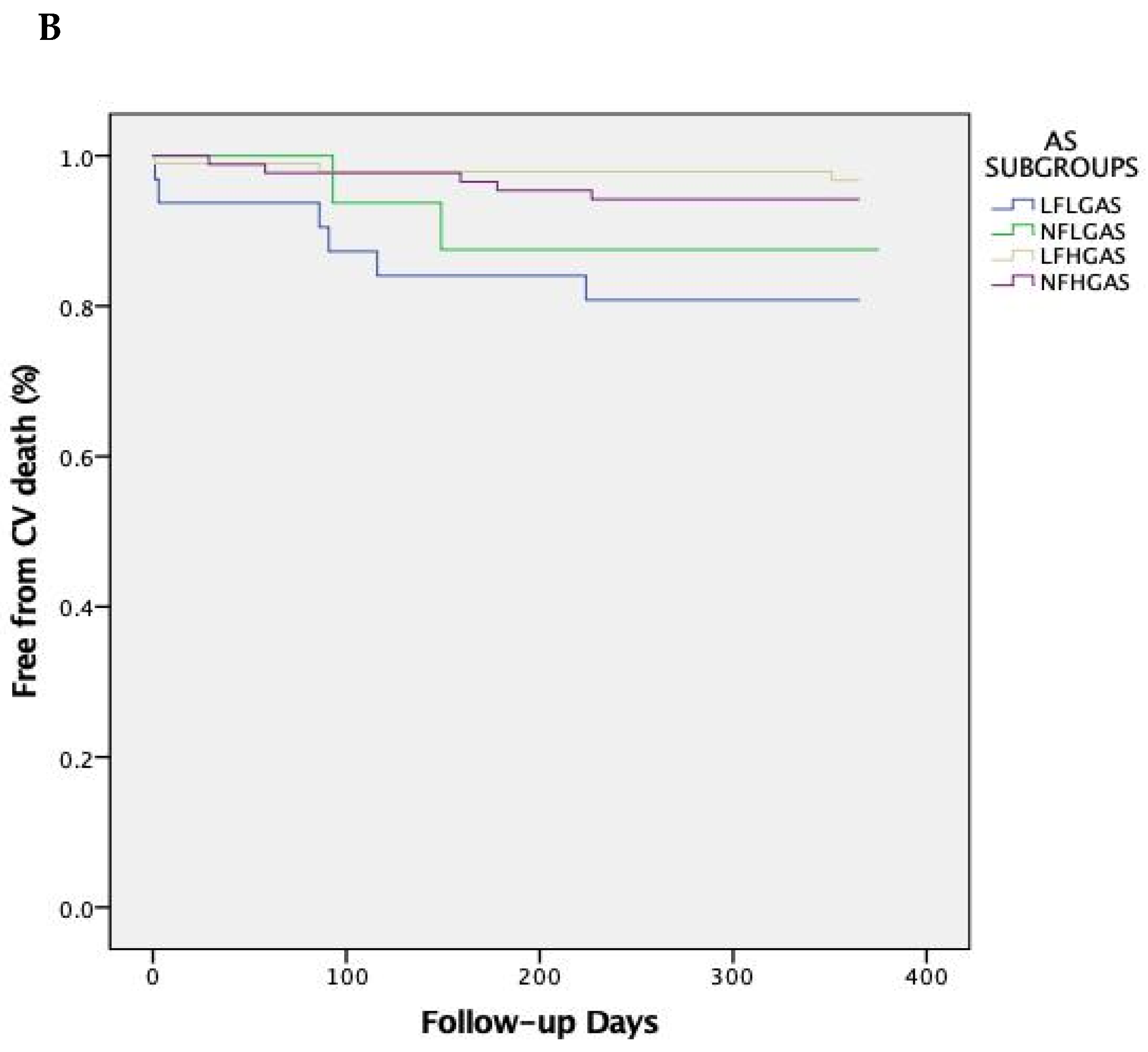
Figure 2.
Kaplan-Meier survival curves at 5-year follow-up showing (A) global and (B) cardiovascular mortality across different AS subgroups based on pre-TAVI flow/gradient status. * LF-; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, CV; Cardiovascular.
Figure 2.
Kaplan-Meier survival curves at 5-year follow-up showing (A) global and (B) cardiovascular mortality across different AS subgroups based on pre-TAVI flow/gradient status. * LF-; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, CV; Cardiovascular.
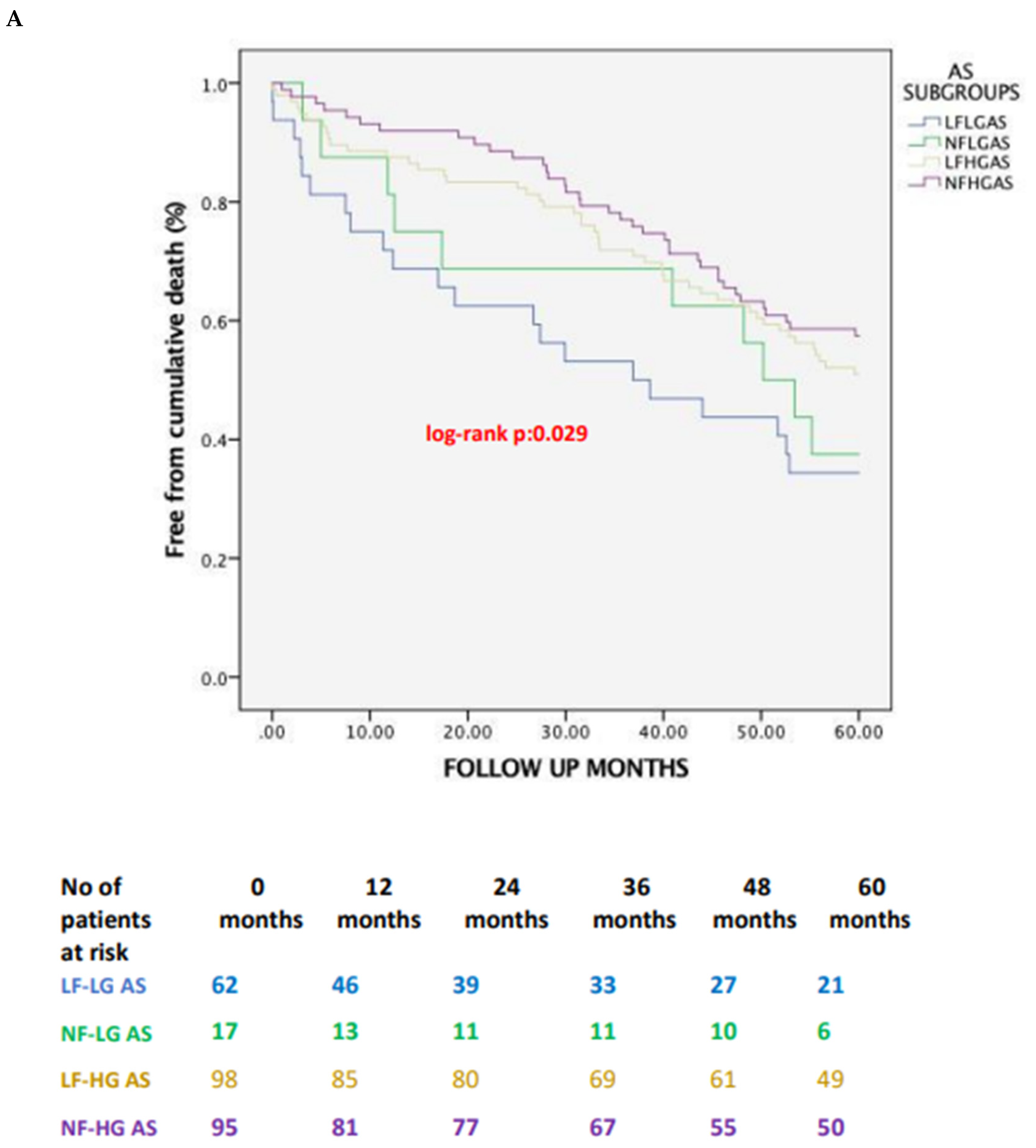
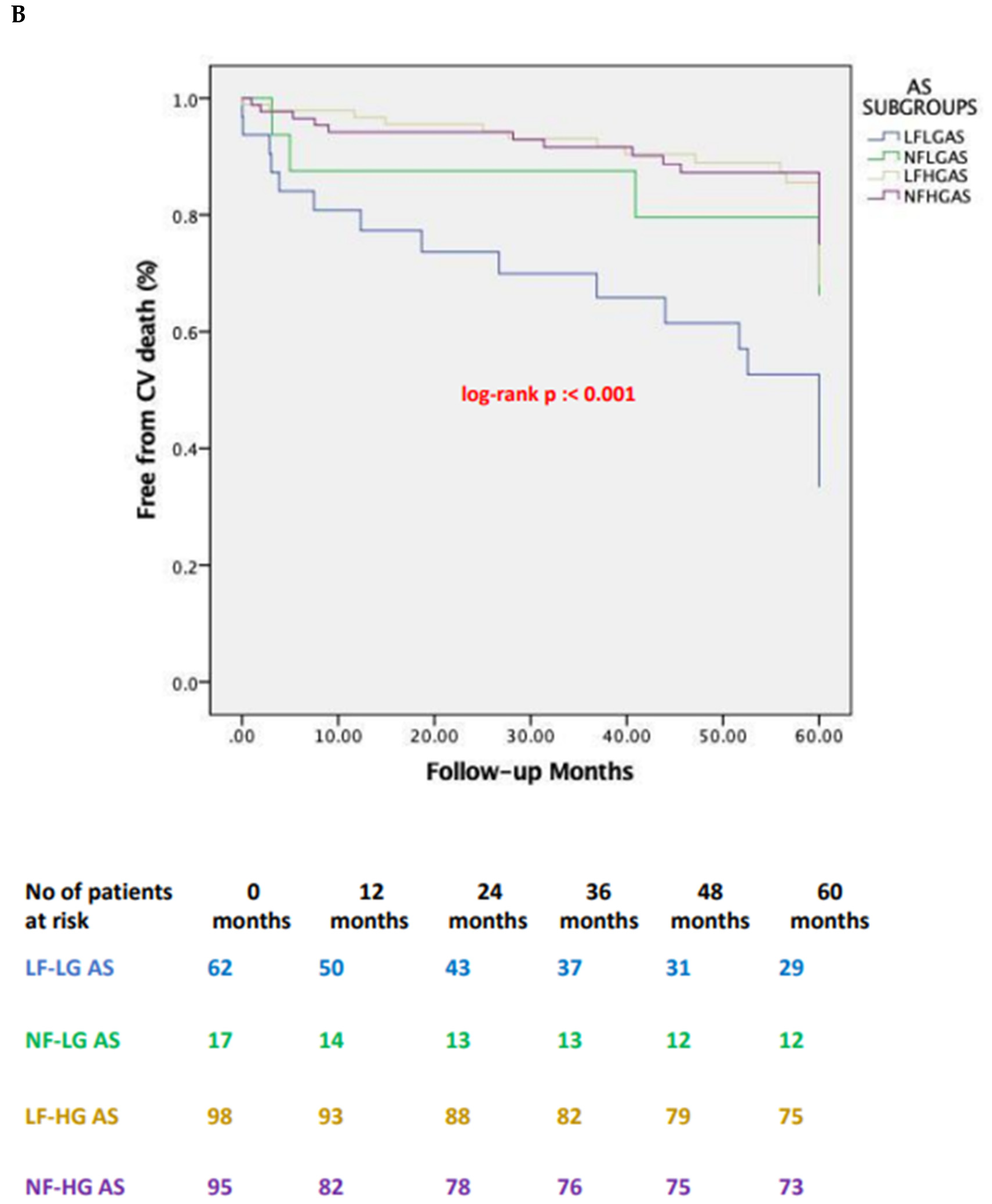
Figure 3.
Kaplan -Meier survival curves at 5- year follow-up showing (A) global and (B) cardiovascular mortality stratified based on pre-TAVI flow status. *CV; Cardiovascular.
Figure 3.
Kaplan -Meier survival curves at 5- year follow-up showing (A) global and (B) cardiovascular mortality stratified based on pre-TAVI flow status. *CV; Cardiovascular.
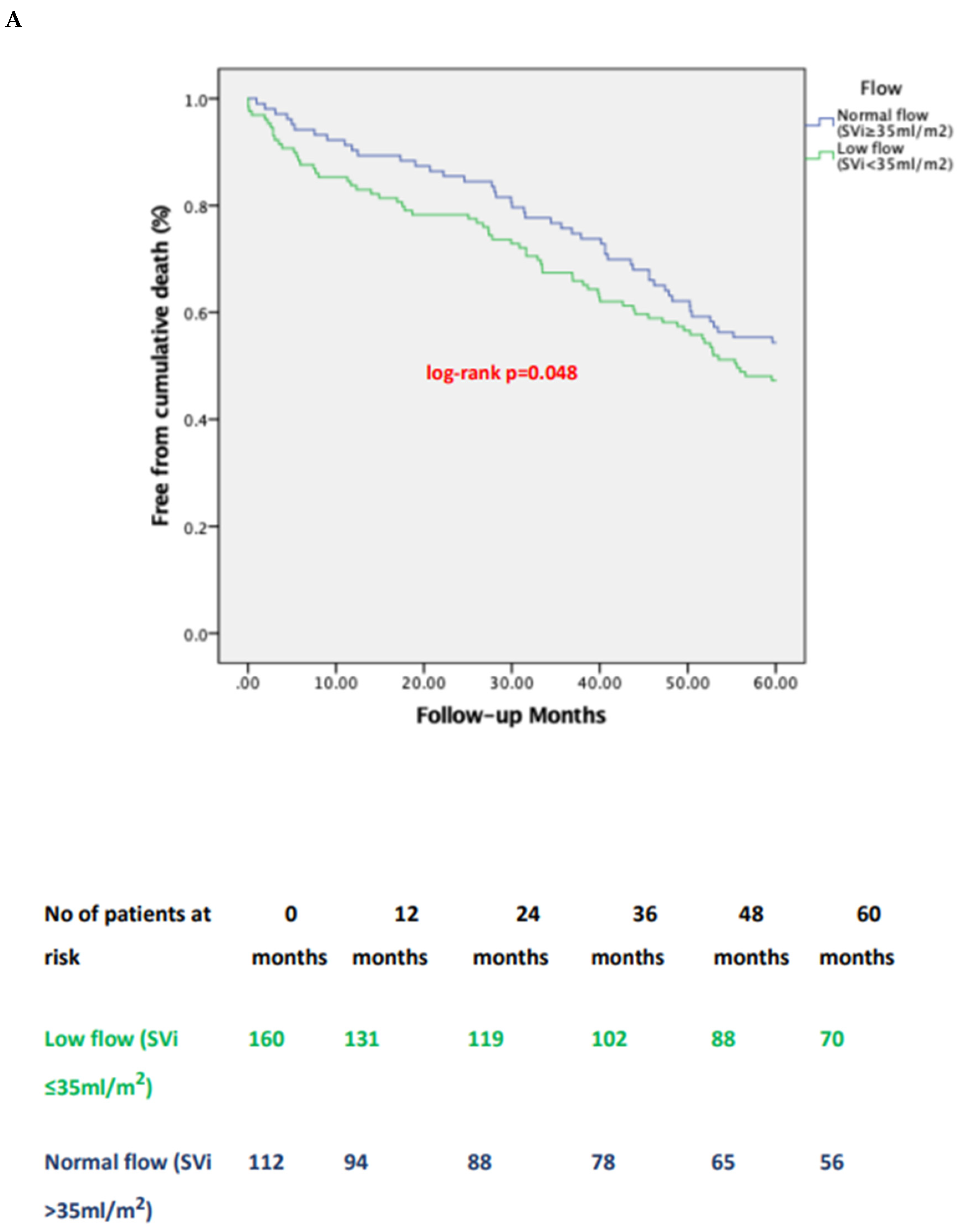
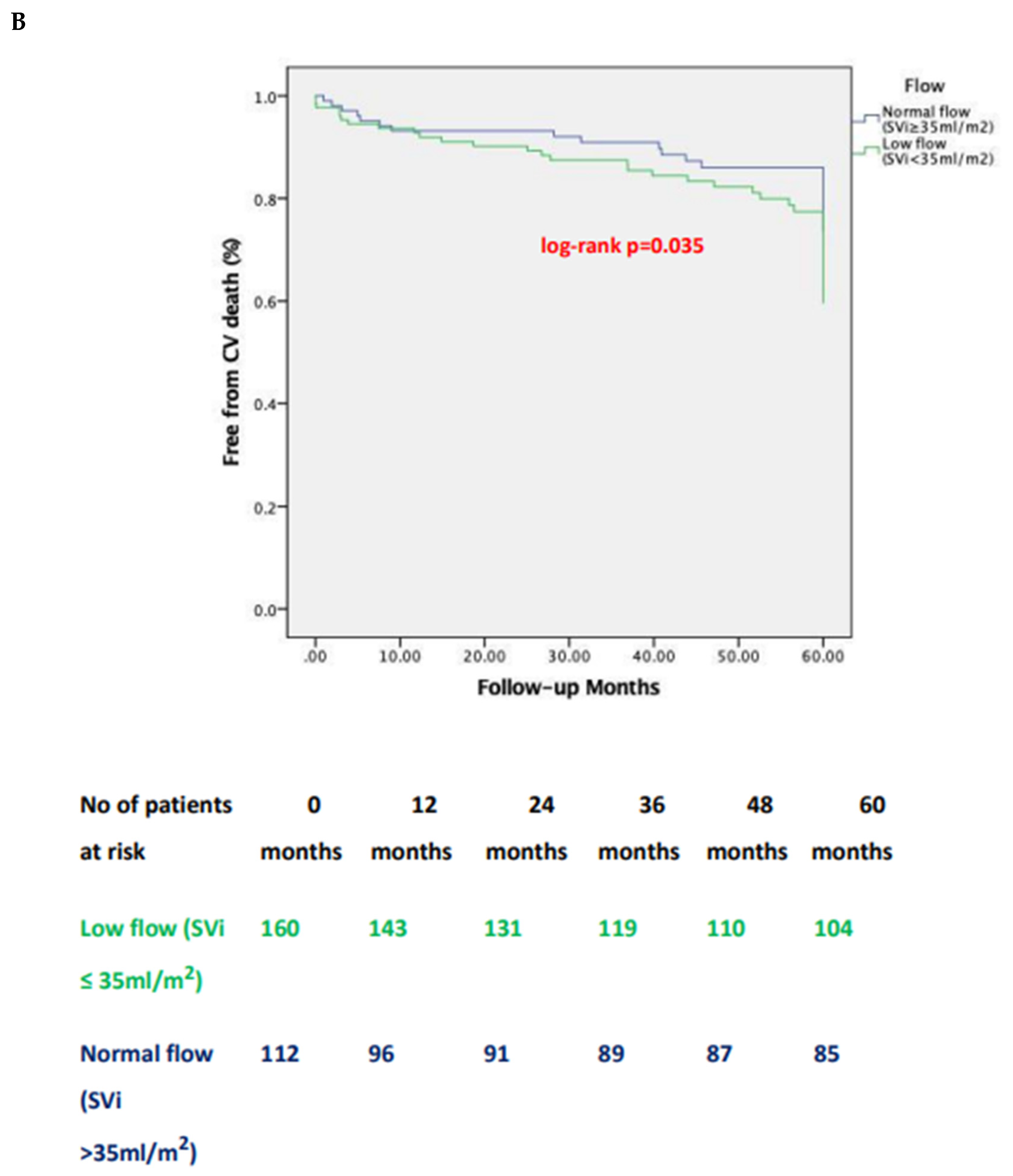
Figure 4.
Changes in LVEF over time across different AS subgroups according to pre-TAVI flow/gradient status. * LF-; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, LVEF; Left Ventricular Ejection Fraction.
Figure 4.
Changes in LVEF over time across different AS subgroups according to pre-TAVI flow/gradient status. * LF-; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, LVEF; Left Ventricular Ejection Fraction.
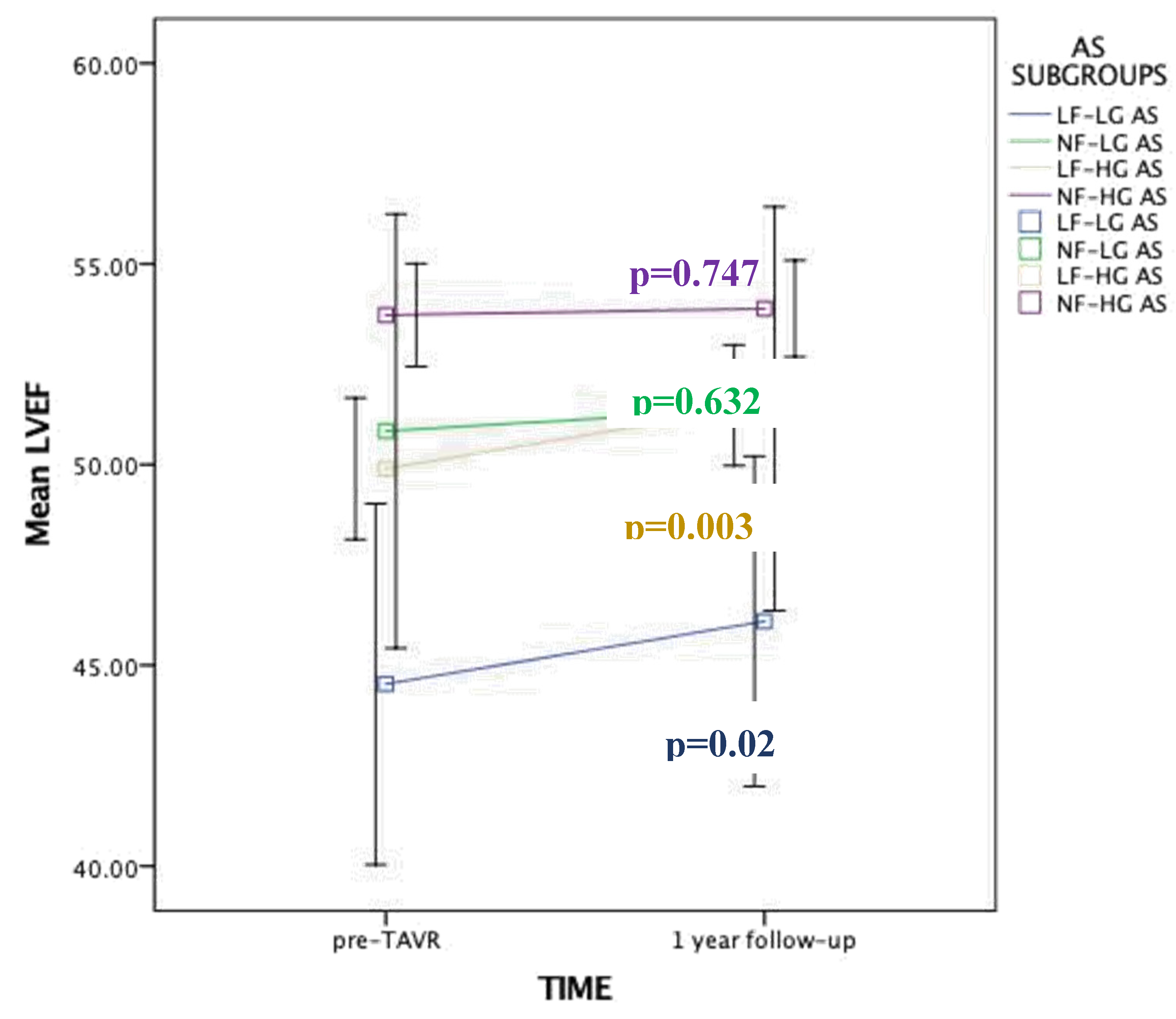

Table 1.
Subgroup definitions.
| Groups | Mean transvalvular gradient | Stroke Volume index |
|---|---|---|
| Low-flow, high-gradient | ≥40 mm Hg | ≤35mL/m2 |
| (LF-HG) | ||
| Low-flow, low-gradient | <40 mm Hg | ≤35mL/m2 |
| (LF-LG) | ||
| Normal-flow, high- | ≥40 mm Hg | >35mL/m2 |
| gradient (NF-HG) | ||
| Normal-flow, low-gradient | <40 mm Hg | >35mL/m2 |
| (NF-LG) |
Table 2.
Baseline demographic and clinical characteristics of the study population.
| All patients | NF-HG AS | LF-HG AS | NF-LG AS | LF-LG AS | P value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (N=272) | 95 | (34.9%) | 98 | (36%) | 17 | (6.3%) | 62 | (22.8%) | |||
| Age, yrs | 80 | ± 7 | 80 | ± 7 | 81 | ± 7 | 77 | ± 8 | 78 | ± 9 | 0.124 |
| BMI, kg/m2 | 26.06±3.17 | 25.32±2.75 | 26.83±3.48 | 26.54±3.64 | 25.67±2.56 | 0.008 | |||||
| Male, (%) | 134 (49.2%) | 34 | (35.8%) | 50 | (51%) | 9 (52.9%) | 41(65.6%) | 0.018 | |||
| Diabetes, (%) | 87 | (32%) | 32 | (33.7%) | 29 | (29.6%) | 7 (41.2%) | 19 | (31.3%) | 0.623 | |
| Hypertension, (%) | 206 (75.7%) | 67 | (70.5%) | 76 | (77.6%) | 11 | (64.7%) | 52 | (84.4%) | 0.475 | |
| CAD, (%) | 129 (47.4%) | 41 | (43.2%) | 44 | (44.9%) | 9 (52.9%) | 35 | (56,3%) | 0.268 | ||
| Previous MI, (%) | 55 | (20.2%) | 18 | (18.9%) | 15 | (15.3%) | 3 (17.6%) | 19 | (31.3%) | 0.005 | |
| Previous PCI, (%) | 36 | (13.2%) | 11 | (11.2%) | 11 | (10.8%) | 2 (14.3%) | 12 | (19.2%) | 0.689 | |
| Previous CABG, (%) | 63 | (23.2%) | 12 | (12.4%) | 24 | (25.3%) | 6 (35.7%) | 21(34.6%) | 0.025 | ||
| CKD, (%) | 114 (41.9%) | 36 | (37.9%) | 42 | (42.9%) | 5 (29.4%) | 31 | (50%) | 0.469 | ||
| PAD, (%) | 100 (36.7%) | 29 | (30.5%) | 30 | (30.6%) | 4 (23.5%) | 37 | (59.4%) | 0.063 | ||
| COPD, (%) | 71 | (26.1%) | 22 | (23.2%) | 25 | (25.5%) | 7 (41.2%) | 17 | (28.1%) | 0.694 | |
| EUROSCOREII | 5.14 {4.22- | 4.50 {3.42- | 5.15 {4.60- | 5.62 {4.95- | 8.34 {4.84- | 0.004 | |||||
| 6.48} | 6.0} | 6.48} | 6.88} | 13.58} | |||||||
| NYHA III/IV, (%) | 265 (97.4%) | 92 | (97.9%) | 96 | (98%) | 17 | (100)% | 60 | (96.9%) | 0.850 | |
BMI; Body Mass Index, CABG; Coronary Artery Bypass Graft surgery, CAD; Coronary Artery Disease, CKD; Chronic Kidney Disease COPD; Chronic Obstructive Pulmonary Disease, HG; High-Gradient, LF; Low-Flow, LG; Low-Gradient, MI; Myocardial Infarction; NF; Normal Flow, NYHA; New York Heart Association, PAD; Peripheral Arterial Disease, PCI; Percutaneous Coronary Interventions. Euroscore II is presented as median value {interquartile range}. Categorical variables are expressed as absolute numbers and percentages N(%), continuous variables as mean ± SD.
Table 3.
Baseline echocardiographic and MSCT variables of the study population.
| All patients | NFHGAS | LFHGAS | NFLGAS | LFLGAS | P | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (N=272) | (N=95) | (N=98) | (N=17) | (N=62) | value | ||||||
| LVEF,% | 51 | ± 9 | 54 | ± 6 | 50 | ± 9 | 50 | ± 11 | 44 | ± 12 | <0.001 |
| Mean gradient, | 50 | ± 15 | 57 | ± 14 | 53 | ± 11 | 34 | ± 6 | 32 | ± 9 | <0.001 |
| mmHg | |||||||||||
| AVA, cm2 | 0.61 ± 0.15 | 0.68 ± 0.14 | 0.52 ± 0.11 | 0.77 ± 0.11 | 0.59 ± 0.16 | <0.001 | |||||
| Moderate-severe | 86 | (31.6%) | 19 | (20.3%) | 34 | (35%) | 7 (38.5%) | 26 | (42.9%) | 0.069 | |
| MR pre TAVi | |||||||||||
| Moderate-severe TR | 64 (23.5%) | 19 | (20%) | 28 | (28.6%) | 5 (29.4%) | 12 | (19.3%) | 0.438 | ||
| pre TAVi | |||||||||||
| Stroke volume | 35 | ± 11 | 45 | ± 9 | 29 | ± 6 | 40 | ± 4 | 26 | ± 5 | <0.001 |
| indexed, ml/m2 | |||||||||||
| Pulmonary artery | 44.43±12.50 | 44.95±12.52 | 44.98±13.46 | 41.76±8.46 | 42.61±11.22 | 0.620 | |||||
| systolic pressure | |||||||||||
| (PASP) (mmHg) | |||||||||||
| Severe AV | 172 (63.2%) | 58 | (61.4%) | 62 | (63.2%) | 14 | (80%) | 38 | (61.1%) | 0.717 | |
| calcification based | |||||||||||
| on MSCT | |||||||||||
LVEF; Left Ventricular Ejection Fraction, AVA; Aortic Valve Area, MR; Mitral Regurgitation, TAVI; Transcatheter Aortic Valve Implantation, TR; Tricuspid Regurgitation, AV; Aortic Valve, MSCT; Multi-Slice Computed Tomography. Categorical variables are expressed as absolute numbers and percentages, continuous as Mean ± SD.
Table 4.
Primary endpoints: 1-year and 5-year all-cause mortality rates. Secondary endpoints: 1-year and 5-year CV mortality rates, 1-year MACCE rates. Values are N (%).
Table 4.
Primary endpoints: 1-year and 5-year all-cause mortality rates. Secondary endpoints: 1-year and 5-year CV mortality rates, 1-year MACCE rates. Values are N (%).
| LF-LG AS | NF-LG AS | LF-HG AS | NF-HG | p LF-LG AS | p LF-LG AS | p LF-LG AS | P* | ||
| (N=62) | (N=17) | (N=98) | AS | vs NF-LG | vs LF-HG | vs NF-HG | |||
| (N=95) | AS | AS | AS | ||||||
| 1-year | all- | 16 (25.8) | 3 (18.8) | 11 (11.5) | 6 (6.3) | 0.729 | 0.084 | 0.011 | 0.048 |
| cause | |||||||||
| mortality, | |||||||||
| N (%) | |||||||||
| 1-year | CV | 12 (19.3) | 2 (12.5) | 3 (3.1) | 5 (5.7) | 0.701 | 0.008 | 0.067 | 0.018 |
| mortality, | |||||||||
| N (%) | |||||||||
| Stroke | at 1 | 2 (3.2%) | 1 (5.9) | 2 (2) | 2 (2.1) | 1.000 | 1.000 | 0.802 | 0.868 |
| year, N (%) | |||||||||
| 1-year | 16 (25.8) | 3 (18.8) | 12 (12.2) | 8 (8.4) | 1.000 | 0.092 | 0.029 | 0.097 | |
| MACCE | |||||||||
| (death, | non- | ||||||||
| fatal | MI, | ||||||||
| non-fatal | |||||||||
| stroke), N(%) | |||||||||
| 5-year | all- | 40 (64.5) | 10 (58.8) | 47 (47.9) | 40 (42.5) | 1.000 | 0.152 | 0.038 | 0.047 |
| cause | |||||||||
| mortality, | |||||||||
| N (%) | |||||||||
| 5-year | CV | 33 (53.2) | 4 (23.5) | 21 (21.4) | 17 (17.9) | 0.075 | 0.001 | 0.001 | 0.002 |
| mortality, | |||||||||
| N (%) | |||||||||
LF; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient, CV; Cardiovascular, MACCE; Major Adverse Cardiovascular and Cerebrovascular Events. P*: p value for between group comparison.
Table 5.
30-Day secondary endpoint events.
| LF-LG | NF-LG | LF-HG | NF-HG | p LF-LG vs | p LF-LG vs | p LF-LG vs | P* | |
|---|---|---|---|---|---|---|---|---|
| (N=62) | (N=17) | (N=98) | (N=95) | NF-LG | LF-HG | NF-HG | ||
| 30-day PPI | 31 | 7 | 41(41.8) | 34 | 0.683 | 0.419 | 0.147 | 0.561 |
| N (%) | (50) | (41.2) | (35.8) | |||||
| 30-day Major | 2 (3.2) | 1 (5.9) | 8 (8.2) | 7 (7.4) | 0.660 | 0.294 | 0.353 | 0.755 |
| vascular | ||||||||
| complications N | ||||||||
| (%) | ||||||||
| 30-day Life | 9 | 2 | 12 | 15(15.8) | 0.659 | 0.622 | 0.965 | 0.863 |
| threatening/major | (14.5) | (11.7) | (12.2) | |||||
| bleeding | ||||||||
| complications N | ||||||||
| (%) | ||||||||
PPI; Permanent Pacemaker Implantation, LF; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient. Values are N (%). P*: p value for between group comparison.
Table 6.
Multivariable Cox proportional hazards regression analysis with late (5-year) all-cause mortality as the dependent variable.
Table 6.
Multivariable Cox proportional hazards regression analysis with late (5-year) all-cause mortality as the dependent variable.
| 95.0% CI for Exp(B) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | Wald | df | Sig. | Exp(B) | Lower | Upper | ||
| EUROSCORE II | |||||||||
| -.025 | .016 | 2.455 | 1 | .117 | .975 | .945 | 1.006 | ||
| CHRONIC KIDNEY | |||||||||
| DISEASE | .429 | .275 | 2.441 | 1 | .118 | 1.536 | .896 | 2.633 | |
| PRIOR MI | |||||||||
| .139 | .301 | .213 | 1 | .645 | 1.149 | .637 | 2.072 | ||
| Pre-TAVI MR ≥ | |||||||||
| moderate | .069 | .291 | .057 | 1 | .812 | 1.072 | .606 | 1.894 | |
| Pre-TAVI TR ≥ | 1.128 | .322 | 12.288 | 1 | .000 | 3.091 | 1.645 | 5.809 | |
| moderate | |||||||||
| Pre-TAVI PASP | |||||||||
| .005 | .012 | .194 | 1 | .660 | 1.005 | .983 | 1.028 | ||
| Pre-TAVI SVi | |||||||||
| -.051 | .018 | 8.316 | 1 | 0.004 | .951 | .918 | .984 | ||
| Post-TAVI PASP | .010 | .013 | .641 | 1 | .423 | 1.010 | .985 | 1.036 | |
| Post-TAVI PVL ≥ | 1.105 | 0.288 | 11.677 | 1 | 0.042 | 1.456 | 1.106 | 1.792 | |
| moderate | |||||||||
| FLOW-GRADIENT STATE*US* | 9.030 | 3 | .029 | ||||||
| LF-HG AS | -.374 | .505 | .548 | 1 | .459 | .688 | .256 | 1.852 | |
| NF-LG AS | .564 | .553 | 1.039 | 1 | .308 | 0.360 | .594 | 5.197 | |
| LF-LG AS | -1.022 | .433 | 5.572 | 1 | .018 | 1.757 | .154 | .841 | |
*NF-HG AS is set as reference. MI; Myocardial Infarction, MR; Mitral Regurgitation, TR; Tricuspid Regurgitation, PASP; Pulmonary Artery Systolic Pressure, Svi; Stroke Volume indexed, PVL; Paravalvular Leak, LF; Low Flow, LG; Low Gradient, NF; Normal Flow, HG; High Gradient.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



