
Submitted:
29 January 2024
Posted:
30 January 2024
You are already at the latest version
Abstract
Late type II endoleak (T2EL) arising from internal iliac artery (IIA) network may occur after endovascular aortic repair (EVAR) of aortoiliac aneurysm and may require embolization if sac enlargement is demonstrated. When direct antegrade access to ipsilateral IIA is not achievable due to previous vessel coverage and/or embolization, access to the nidus can be challenging. We report a case of T2EL originating from IIA network causing iliac sac enlargement in a patient previously treated by EVAR for artoiliac aneurysm with IIA embolization and coverage, in which embolization of the nidus was performed through a percutaneous sheathless access to ip-silateral superior gluteal artery (SGA). A literature review dealing with all cases of percutaneous direct SGA access for retrograde embolization of T2EL arising from IIA after previous EVAR is also reported. The research was conducted on Pubmed database using keywords “superior glu-teal artery access,” “transgluteal embolization” and “retrograde embolization for type II endo-leak”. Related articles and references were screened for suitable articles.
Keywords:
Endoleak
; Internal iliac artery
; Endovascular aortic repair
; Endovascular technique
; Superior gluteal artery
; Embolization.
1. Introduction
Endovascular aneurysm repair (EVAR) is the treatment of choice for infrarenal aortic aneurysms with fit anatomy. It showed significantly higher short-term survival rates compared with open surgery but long-term survival rates are equivalent and endovascular results are impaired by higher rates of aneurysm-related reinterventions. The principle of endovascular treatment of aneurysms is the exclusion of the diseased arterial segment from circulation to no longer expose the segment itself to arterial pressure. This principle is achieved through the placement of an endograft which requires, as a prerequisite for its correct functioning, the presence of a healthy artery at its proximal and distal edge and no collaterals through which the flow can be reversed. Any flow into the aneurysmatic sac outside the graft after EVAR represents an endoleak that is an important cause of recurrence of disease and reintervention. Endoleaks are classified as primary when they appear immediately after the endovascular repair or secondary when they appear during the follow-up after a prior imaging that showed no irregularities. Type I endoleak are classified as direct flow into the residual aneurismal sac trough the proximal or distal sealing zones due to poor adherence between the endograft and the arterial wall. Since their high risk of rupture they need prompt management. Type II endoleak are classified as retrograde flow from collaterals arising from the excluded arterial segment. Type III endoleak results from stent graft component maldeployment with inadequate overlap, distal stent graft migration or fabric tear. Just as Type I endoleaks, they expose the aneurysm to direct aortic pressure with subsequent risk of rupture and need well-timed management. Leakage through the stent graft material porosity is defined as Type IV endoleak. This type of endoleak was rarely seen with early stage stentgrafts and is rare with nowadays used devices. They do not require any re-intervention. Type V endoleak also named endotension is defined by sac expansion without any visible endoleak. Different possible mechanisms have been questioned with no definitive conclusions. Afterall, endotension may result in rupture and, as with Type II endoleak, treatment is suggested when the aneurismal sac increase >1 cm and consists of stent graft relining or explantation during open surgery with traditional aorto-iliac prosthetic bypass. The focus of this study is on secondary endoleak also named late type II endoleak. They can occur after EVAR with a prevalence at one year of follow-up of up to 16% [1]. Their clinical significance remains controversial, but surveillance is necessary and in some cases treatment is required to prevent rupture [2]. Their persistence, when associated with aneurismal sac expansion represents the most common cause of aneurysm-related reinterventions. Both open and endovascular surgery techniques have been described in this setting and the endovascular approach is nowadays the preferred one in patients with fit anatomy due to its shorter length of post-operative stay and lower morbidity compared with open surgery [3]. Many endovascular options exist aiming to embolize the aneurysmal sac and feeding vessels. But it may be difficult to reach the nidus of the endoleak by an anterograde route when a previous endovascular procedure had just been made. In particular, it may be difficult to reach the hypogastric artery with an anterograde route when coverage of the external iliac artery had been made for extensive iliac disease. The aim of the present study is to report the case of a T2EL of the common iliac artery (CIA) retrograde embolization with a percutaneous sheathless superior gluteal artery (SGA) access after a previous plug embolization of the internal iliac artery (IIA) with external iliac artery (EIA) extension and manual compression haemostasis. A comprehensive literature review of different strategies is also provided.
2. Case Presentation
In 2010 a 63 year-old man underwent elective EVAR for a 65 mm asymptomatic infrarenal aortic aneurysm discovered at computed tomography (CT) scan done as a completion of the aortic study due to the presence of an ascending aorta dilation. Other comorbidities included hypertension, hypercholesterolemia, mesangial glomerulonephritis and seronegative polyarthritis. After an initial loss to follow-up, in 2018 he presented with a 50 mm left common iliac artery aneurysm shown at an enhanced CT scan. Treatment consisted in iliac limb extension (Medtronic Endurant II, Minnesota, USA) into the external iliac artery and embolization of the main trunk of IIA with a 16 mm Amplatzer Vascular Plug (AGA Medical, Minnesota, USA). After 3 years, a CT scan demonstrated persistent enlargement of the left common iliac artery aneurysm reaching 7cm of diameter without clarifying its souce (Figure 1). An angiography through a left omeral access was planned. It showed a T2EL arising from the left IIA network. After discussing with the patient about treatment options, embolization through a percutaneous SGA access was planned. The procedure was conducted in an angiographic suite under general anaesthesia after systemic heparinization (5000 UI). At first, through a left omeral access, a 4Fr pigtail catheter (Cordis, Florida, USA) was positioned in the right CIA to angiographically identify the contralateral SGA. Then, the patient was placed in a prone position, so under duplex ultrasound (DUS) and angiographical guidance direct puncture of the left SGA was performed using an 18 Gauge 100 mm long needle. Over a 0.035-inch teflon-coated guidewire, a 4 Fr Ber catheter (Cordis Tempo, Florida, USA) was advanced in a sheathless fashion to the main trunk of the IIA. Then it was pushed beyond the plug in a transealing fashion using a hydrophilic stiff guide (Terumo Glidewire, New Jersey, USA), thus reaching the nidus of the leak. An intrasac angiography confirmed several small vessels from hypogastric network as source of the endoleak. A 2.7 Fr microcatheter (Rebar, Medtronic, Minnesota, USA) was placed in a coaxial fashion into the nidus and 3 4x60 cm Ruby-coil detachable coils (Penumbra, California, USA) were deployed to provide a scaffold. Then 6 ml of liquid embolic agent (Onyx 34, Medtronic, Minnesota, USA) were used to fill the flow channel as shown in Figure 2. Completion angiography demonstrated no further filling of the leak. Haemostasis of the puncture site was obtained by manual compression. In the postoperative period no ischemic or haemorrhagic complications were observed, and the patient was discharged on the second postoperative day. One year follow-up CT-scan demonstrated the stability of the left iliac aneurysm (Figure 3). Informed consent for publication was obtained by the participant.
3. Literature Search and Inclusion Criteria
The preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines were observed to conduct this review. A research on PubMed, Scopus, and the Cochrane Library for studies investigating the association between EVAR and the occurrence of type II endoleaks from hypogastric artery and secondary reinterventions was performed. The first search was conducted on June 1st, 2023. The following combination of keywords was used connected through Boolean operators to maximize sensitivity of the research: “embolization” AND ”internal iliac artery” AND ”superior gluteal artery” OR “endovascular aortic repair” AND “internal iliac artery” AND ”superior gluteal artery” OR “EVAR” AND “internal iliac artery” AND ”superior gluteal artery”. Related articles and references were screened for suitable articles. The last database search was finished on December 1st, 2023. Only articles in English language were evaluated. Only studies containing specific information about used materials for implantation were considered. Titles and abstracts were studied to identify articles compatible with our review. The abstracts which passed the initial screening underwent further full-text review. Articles providing other arterial access techniques were collected to report full range literature options and presented in discussion section.
3.1. Data Extraction of Included Studies
Data from the included studies were extracted by two authors independently (R.P. and A.E.). The following data were collected: arterial access site, technique of access site, feeding vessel embolization, aneurismal sac embolization, embolic agents, technical success and hemostasis technique. Technical success was defined by a second level imaging examination after the target intervention demonstrating no late contrast phase enhancement of residual aneurismal sac or sac dimension stability. Additional criteria of the included studies relevant to this review were also assessed. This included evaluating whether a detailed technical aspect of IIA embolization was well-described. The follow-up length and the imaging method for assessing technical success were also included.
3.3. Study Identification and Characteristics
A database with all studies in which a common/internal iliac artery aneurysm’ treatment was described utilizing a superior gluteal artery access was built. The database included 9 studies. All studies had full texts available, and they were evaluated for suitable articles. A total of 10 patients were included. The included studies were published between 2014 and 2023. The indication for treatment was iliac aneurismal sac dimension increase in all studies. No emergency treatments were included in the database.
3.4. Patients’ Characteristics and Technical Aspects
The average age of participants ranged between 56 and 86 years. 90% of patients were men. Mean aneurysm diameter varied between 47 mm to 75 mm. No studies reported the use of anticoagulants or antiplatelet agents. The principal method for IIA embolization was coils in all studies. The coils used were interlocking detachable coils (VortX; Boston Scientific, Natick, MA), Interlock (Boston Scientific, Marlborough, MA, USA), Nestor (Cook Medical, Bloomington, IN, USA), Target embolism coils (Stryker Neurovascular, Fremont, CA, USA), detachable Concerto coils (ev3 Endovascular, Inc, Plymouth, Minn), magnetic resonance compatible platinum coils (Penum- bra; Penumbra, Inc., Alameda, CA), spirali (Pyramed) coils, and Concerto detachable coils (Medtronic, Minneapolis, Minnesota). The adjunctive method for embolization varied widely. The embolic liquid agents were Lipiodol (Guerbet Group, Roissy, France), Histoacryl (Tissue Seal, Ann Arbor, MN, USA), Onyx (Medtronic Minneapolis, USA), and n-butil cyanoacrylate (Histoacryl, Melsungen, Germany). Human thrombin was utilized in only one case. Amplatzer II vascular plug were utilized in only one case (St. Jude Medical, Minnesota, MN, USA). The rate of technical success was 100% suggesting that the embolic method is not crucial. For hemostasis percutaneous site access site, coils embolization was utilized in two cases and closure device systems in two. Complications of access site occurred in only one case in which coils embolization of the vessel was utilized. Follow-up length ranged from 3 months to 1 year of the present case. A comparative analysis of access vessels, techniques and closure options utilized by different authors to treat CIA aneurysms caused by IIA retrograde flow is provided in Table 1.
4. Discussion
Late T2EL arising from IIA may occur after EVAR for aortoiliac aneurysm up to 16% through five years after the first procedure [1]. Nearly half of patients show aneurysmal sac growth and need intervention to avoid rupture. According to Werner Gibbins [6] secondary type II endoleaks are often the result of flow through patent iliolumbar or sacral artery collaterals that normally are little branches hardly visible during conventional angiography due to parallax effect. In support of this contention, a retrospective analysis over 53 procedures by Heye [7], conducted to evaluate whether T2EL is more frequent in case of antegrade residual flown versus total occlusion after coil embolization of IIA, demonstrated the same incidence of T2EL in both conditions and concluded that complete occlusion of the target vessel at the end of the procedure is not necessary to prevent type II endoleak after endograft placement for aortic or iliac aneurismatic disease but pointed out that in all cases in which an endoleak was detected, a patent iliolumbar artery at the origin of the hypogastric artery was present causing retrograde flow. That is the reason why several authors suggest identifying and occlude the iliolumbar artery when performing IIA embolization to avoid its retrograde flow with endoleak development during the follow-up [8,9]. Other factors influencing endoleak appearance are number and diameter of lumbar arteries and some authors suggest their embolization in selected cases[10]. Alternative causes may be the hypertrophy of vasa vasorum induced by the hypoxic environment in the arterial wall after covered stents deployment or inflammatory processes generated by the thrombus derived contents as explained by Patel and Fikani[11,12]. Despite their origin, T2EL from IIA true natural history is uncertain. They often resolve spontaneously but in half of cases endoleak may persist causing sac enlargement1,[13]. This occurrence may be a risk condition and reported iliac rupture cases during conservative management and poor results after emergency treatment suggest elective approach[14]. Specific guidelines are absent, but there is agreement about treatment if the sac has expanded >1 cm over the last year or if 5 mm expansion between two examinations was documented[15]. Past management consisted in open surgery with ligation of internal iliac artery, but nowadays lesser invasive procedures exist so current strategy reserves traditional surgery as a second option in suitable patients. Literature provides several treatment options suitable for different conditions and a narrative review of relevant articles about type II endoleak from IIA after EVAR was conducted to provide a summary of relevant treatment options. Aiming to reduce morbidity, laparoscopic aortic aneurysm repair has been proposed since 2001 [16]. Even they re-intervention were treated with the same technique and a laparoscopic endoleak treatment was described by Zou et al. [17] in a particular case of type II endoleak of both inferior mesenteric artery and internal iliac artery causing abdominal aneurysmal sac enlargement and pain. It allowed the concomitant treatment of the two endoleak at the same procedure in a relatively short time. But the technical difficulty and the poor reproducibility of the procedure limited the spread among vascular surgeons. In recent years the endovascular approach has advanced as the first choice. The endovascular goal is to interrupt the nidus flow by filling the nidus itself and embolize feeding vessels in order to relieve aneurysmal sac pressure. It is not always possible achieve the two targets and often procedures end when one of the two has been realized. Several studies dealing with T2EL treatment focused on the relative contribution of the two targets but failed to clarify whether sac embolization alone is better than feeding vessels occlusion [7]. This aspect can be explained by difficulty in revealing or reaching small collaterals vessels or anatomic variant. Afterall, this review did not evidence any difference regarding short-term result in terms of sac enlargement, freedom from recurrence of EL and reinterventions between the two techniques; furthermore, the only case of post procedural ischemic complication (buttock claudication) was observed after feeding vessel embolization (Table 1) and that is the reason why san embolization may be deemed sufficient. In our case endoleak source was unknown since the angiography demonstrated that the previous IIA plug had not dislocated and both common and external artery had been previously covered. So, our objective was the obliteration of the nidus itself. The endovascular route was challenging as coverage of EIA precluded direct IIA access. In these cases, different ways are feasible. Direct anterior percutaneous trans-iliopsoas sac puncture has been described [18]. It has the potential benefit of directly reaching the nidus of the endoleak but requires no vital structures like bowel loops between the aneurysmal sac and puncture site. Since patient motion can influence advancement of the needle, general anaesthesia is required but the major disadvantage is transferring the patient between the angio-suite and the CT scanner that increases operative time including the risk of dislocation of the needle. Cone beam CT can reduce operative time, but it is not available in all angio suites. A transosseous pelvic posterior CT guided approach is described as an alternative to the anterior one when a safe route which prevents lesions of vital structures is not present and it is chosen as the shortest, safest route into the aneurysm that avoids bowel’s loop19. Possible complications of this technique include osteomyelitis, retroperitoneal haemorrhage, and fracture of the bone being transgressed. Considering the invasiveness of this procedure, it can be performed when no anterior ways are eligible and an absolute contraindication about use of contrast iodine medium is present like increased creatinine levels or allergy has been shown by the patient. The transealing technique described by Coppi et al. [20] is a reliable option in which the nidus of the endoleak is reached through the virtual space between the arterial wall and represents a feasible and safe alternative in selected patients with T2El suppling aortic aneurismal sac. Unfortunately, it can only be applied safely when the graft lands on the common iliac artery. Otherwise, when the endograft lands on the external iliac artery this technique is ineligible owing to the smaller caliber of the vessel and risk of rupture or dissection. A different strategy can be used in chronic obstructive arterial disease in which multiple collateral pathways that dilate during time are observed and the transcatheter arterial approach via the deep femoral artery collateral pathways linking to the internal iliac artery circulation has been used [21] but it is technically demanding due to the complexity of the collateral pathway itself if present. In our case, direct puncture of the aneurysm was avoided since its anatomical features as well as the posterior approach for seronegative polyarthritis presented by the patient exposing for bone fracture. So, we decided for a superior gluteal approach. Embolization through retrograde, direct SGA access can solve all these issues as it allows a closer way to reach the target vessel without entering the peritoneal cavity or crossing the iliac bone eliminating associated risks. This approach has already been reported in recent years and during the literature review process we found 9 papers that utilized the same way for an overall amount of 10 patients4,6, [10,22,23,24,25,26,27]. Direct surgical exposure or CT guided puncture of the SGA could have been an alternative4, [28], but both fluoroscopic roadmapping and sonographic guidance provided a good visualisation of the target vessel allowing its puncture with a mini-invasive approach. Small or calcified target vessels can make difficult the endovascular access, but angiography excluded such a situation in our case. Anyway, multiple imaging supporting modalities are required and CT-guidance, DUS-guidance, and fluoroscopic-guidance alone or, most often, in combination are necessary. We too resorted to the combination of fluoroscopic and DUS-guidance. An innovative modality has been recently described by Chi et al who utilized a 18-gauge (7-cm) SMART Doppler ultrasound-guided needle vascular access device (Vascular Solutions, Minneapolis, Minn) to directly access the SGA24. At the end of the procedure, issues for access site hemostasis achievement raise since deep location of SGA and absence of bony structures to compress against. Embolization of the access site has been proposed [27] but the potential risk is represented by distal ischaemia. Alternatively, off-label use of arterial closure devices such as StarClose or Angio-Seal [24,26] can be utilized, but correct deployment of closure devices may be difficult when the target artery has a deep location and may require surgical exposure. Our strategy consisted of sheathless low-profile devices that made the arteriotomy very small. Furthermore, heparin neutralization at the end of the procedure made manual compression successful. One aspect that was never considered in any of the studies examined in this specific setting of endoleak arising from the internal iliac artery was the use of anticoagulants. However, there have been several studies comparing type II endoleak occurrence with abdominal aneurismal sac perfusion in patients treated with anticoagulation versus antiplatelet therapy alone. The first study postulating that anticoagulation can be an important factor influencing failure after endoluminal graft treatment was a case report by Torsello et al. [29] that reported a case of aneurysm rupture 16 months after a successful EVAR in a patient on coumadin due to atrial fibrillation. Even if no endoleak was detected at scheduled CT scan, aneurismal sac enlargement was noted before rupture and after emergency treatment the presence of thrombus in the proximal neck and the concomitant anticoagulant therapy were recognized as possible factors for endograft failure. But the biggest study evaluating long-term impact of anticoagulation on late endoleak occurrence after EVAR is that of Flohr et al. [30] that over a retrospective cohort of 29,783 patients found that late endoleaks were more common in patients treated with anticoagulation after EVAR.
5. Conclusion
This report confirms that embolization of T2EL arising from hypogastric network through percutaneous SGA access is a safe and effective, able to avoid complications related to other access such as direct aneurysm puncture. However, all studies on this specific setting report short-term results, and the longest follow-up is reported by our case with a 1-year CT-scan. Embolization technique and access site haemostasis remain an issue. Further studies need to be done to investigate the best haemostasis technique.
6. Future Directions
The pathogenesis of Type II endoleaks from internal iliac artery is still debated in literature. Some authors attribute particular value to the reflow from the ileo-lumbar artery while others emphasize the role of vasa vasorum hypertrophy induced by hypoxia and local inflammation secondary to the presence of covered stents. The diagnosis of endoleaks’ precise location in these cases can be difficult with CT scan alone, requiring, as in our case report, a diagnostic angiography to identify his exact origin. In fact, only after the angiography it was possible for us to plan a correct intra-operative strategy. If the diagnosis had been clarified before the therapeutic procedure, it would have been possible to better define the procedure. Therefore, our target as researchers is to identify these pathogenetic mechanisms to optimize surgical treatment. With this in mind, preoperative imaging needs to be as accurate as possible. Contrast enhanced ultrasound (CEUS) is a non-invasive method largely used for the diagnosis of vascular pathologies in several districts. In fact, recent studies demonstrated its beneficial contribution in carotid plaques’ characterization allowing a precise estimation of the grade of stenosis but also information about neovascularization of the lesion. This findings are necessary to determine signs of plaque ulcerations and to recognize vulnerable plaques, thus allowing risk stratification of patients which is based both on quantitative and qualitative plaque features [31]. Moreover, CEUS has already been applied in the follow-up of patients post EVAR with notable advantages. It allows to reduce patient and operator exposure to ionizing radiation and reduce the use of potentially nephrotoxic iodinated contrast medium. Furthermore, unlike CT, CEUS allows the visualization of the blood flow direction. For these reasons CEUS has been used at the end of the EVAR procedures for the final angiographic control to verify the patency of the implanted endoprosthesis modules and the absence of type I endoleaks amendable to immediate treatment [32]. However, CEUS is not yet a standardized method for the diagnosis of type II endoleaks from the iliac region. According to our opinion CEUS should be always performed in patients with residual aneurysmal sac growing, before surgery, to identify leaks’ origin.
Author Contributions
Conceptualization, A.E. and R.P.; methodology, R.P.; validation, D.M., A.N.G., G.I. and V.D.A.; original draft preparation, R.P.; review and editing, R.P. and A.E.; supervision, G.I.; V.D.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ruby C. Lo, Dominique B. Buck, Jeremy Herrmann, Allen D. Hamdan, Mark Wyers, Virendra I. Patel, Mark Fillinger, Marc L. Schermerhorn. Risk factors and consequences of persistent type II endoleaks. J Vasc Surg. 2016 April ; 63(4): 895–901. [CrossRef]
- Harada A, Morisaki K, Kurose S, Yoshino S, Yamashita S, Furuyama T, Mori M. Internal Iliac Artery Aneurysm Ruptures with No Visualized Endoleak 2 Years after Endovascular Repair. Ann Vasc Dis. 2022 Mar 25;15(1):45-48. [CrossRef]
- Xiang Y, Chen X, Zhao J, Huang B, Yuan D, Yang Y. Endovascular Treatment Versus Open Surgery for Isolated Iliac Artery Aneurysms: A Systematic Review and Meta-Analysis. Vasc Endovascular Surg. 2019 Jul;53(5):401-407. [CrossRef] [PubMed]
- Kim YJ, Rabei R, Connolly K, Pallav Kolli K, Lehrman E. Percutaneous approach options for embolization of endoleak after iliac artery aneurysm repair: stick the sac or stick the gluteal artery. Radiol Case Rep. 2021 Apr 10;16(6):1447-1450. [CrossRef]
- Kuzuya A, Fujimoto K, Iyomasa S, Matsuda M. Transluminal coil embolization of an inferior gluteal artery aneurysm by ultrasound-guided direct puncture of the target vessel. Eur J Vasc Endovasc Surg. 2005 Aug;30(2):130-2. [CrossRef]
- Werner-Gibbings K, Rogan C, Robinson D. Novel Treatment of an Enlarging Internal Iliac Artery Aneurysm in Association with a Type 2 Endoleak via Percutaneous Embolisation of the Superior Gluteal Artery through a Posterior Approach. Case Rep Vasc Med. 2013;2013:861624. [CrossRef]
- Heye S, Nevelsteen A, Maleux G. Internal iliac artery coil embolization in the prevention of potential type 2 endoleak after endovascular repair of abdominal aortoiliac and iliac artery aneurysms: effect of total occlusion versus residual flow. J Vasc Interv Radiol. 2005 Feb;16(2 Pt 1):235-9. [CrossRef]
- Yasui K, Kanazawa S, Mimura H, Dendo S, Hiraki Y, Irie H, Sano S. Recanalization 24 months after endovascular repair of a large internal iliac artery aneurysm with use of stent-graft. Acta Med Okayama. 2001 Oct;55(5):315-8. [CrossRef]
- Millon A, Paquet Y, Ben Ahmed S, Pinel G, Rosset E, Lermusiaux P. Midterm outcomes of embolisation of internal iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2013 Jan;45(1):22-7. [CrossRef]
- Couchet G, Pereira B, Carrieres C, Maumias T, Ribal JP, Ben Ahmed S, Rosset E. Predictive Factors for Type II Endoleaks after Treatment of Abdominal Aortic Aneurysm by Conventional Endovascular Aneurysm Repair. Ann Vasc Surg. 2015 Nov;29(8):1673-9. [CrossRef]
- Patel S, Chun JY, Morgan R. Enlarging aneurysm sac post EVAR - type V or occult type II Endoleak? CVIR Endovasc 2023 Feb 7;6(1):4. [CrossRef]
- Fikani A, Lermusiaux P, Della Schiava N, Millon A. Vasa vasorum associated with endoleak after endovascular repair of abdominal aortic aneurysm. Vasc Med 2021 Feb;26(1):89-90. [CrossRef]
- Martijn L. Dijkstra, Clark J. Zeebregts, Hence J. M. Verhagen, Joep A. W. Teijink, Adam H. Power, Dittmar Bockler, Patrick Peeters, Vicente Riambau, Jean-Pierre Becquemin, Michel M. P. J. Reijnen. Incidence, natural course, and outcome of type II endoleaks in infrarenal endovascular aneurysm repair based on the ENGAGE registry data. J Vasc Surg. 2020 Mar;71(3):780-789. [CrossRef]
- Regus, S. Ruptured Isolated Internal Iliac Aneurysm. Eur J Vasc Endovasc Surg 2023 Mar;65(3):345. [CrossRef]
- Wanhainen A, Verzini F, Van Herzeele I, Allaire E, Bown M, Cohnert T, Dick F, Van Herwaarden J, Karkos C, Koelemay M, Kölbel T, Loftus I, Mani K, Melissano G, Powell J, Szeberin Z. Editor’s Choice e European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur J Vasc Endovasc Surg (2019) 57, 8e93. [CrossRef]
- Dion YM, Gracia CR, Ben El Kadi H H. Totally laparoscopic abdominal aortic aneurysm repair. J Vasc Surg. 2001 Jan;33(1):181-5. [CrossRef]
- Zou J, Sun Y, Yang H, Ma H, Jiang J, Jiao Y, Zhang X. Laparoscopic ligation of inferior mesenteric artery and internal iliac artery for the treatment of symptomatic type II endoleak after endovascular aneurysm repair. Int Surg. 2014 Sep-Oct;99(5):681-3. [CrossRef]
- S. Heye, J. Vaninbroukx, K. Daenens, S. Houthoofd, G. Maleux. Embolization of an Internal Iliac Artery Aneurysm after Image-Guided Direct Puncture. Cardiovasc Intervent Radiol (2012) 35:807–814. [CrossRef]
- JJ. Gemmete, M Arabi, WB. Cwikiel. Percutaneous Transosseous Embolization of Internal Iliac Artery Aneurysm Type II Endoleak: Report of Two Cases. Cardiovasc Intervent Radiol (2011) 34:S122–S125. [CrossRef]
- G. Coppi, G. G. Coppi, G. Saitta, G. Coppi, S. Gennai, A. Lauricella, R. Silingardi. Transealing: A Novel and Simple Technique for Embolization of Type 2 Endoleaks Through Direct Sac Access From the Distal Stent-graft Landing Zone. Eur J Vasc Endovasc Surg. 2014 Apr;47(4):394-401. [CrossRef]
- Abderhalden S, Rancic Z, Lachat ML, Pfammatter T. Retrograde hypogastric artery embolization to treat iliac artery aneurysms growing after aortoiliac repair. J Vasc Interv Radiol. 2012 Jul;23(7):873-7. [CrossRef]
- Herskowitz MM, Walsh J, Jacobs DT. Direct sonographic-guided superior gluteal artery access for treatment of a previously treated expanding internal iliac artery aneurysm. J Vasc Surg. 2014 Jan;59(1):235-7. [CrossRef]
- Parlani G, Simonte G, Fiorucci B, De Rango P, Isernia G, Fischer MJ, Rebonato A. Bilateral Staged Computed Tomography-Guided Gluteal Artery Puncture for Internal Iliac Embolization in a Patient with Type II Endoleak. Ann Vasc Surg. 2016 Oct;36:293.e5-293.e10. [CrossRef]
- Menon PR, Agarwal S, Rees O. Direct puncture embolisation of the non-coil-embolised internal iliac artery post EVAR - a novel use of the Angio-Seal closure device. CVIR Endovasc. 2018;1(1):6. [CrossRef]
- Chi WK, Yan BP. Direct puncture of superior gluteal artery using a Doppler ultrasound-guided needle to access jailed internal iliac artery aneurysm. J Vasc Surg Cases Innov Tech. 2018 Dec 31;5(1):12-13. [CrossRef]
- Norris E, Bronzo B, Olorunsola O. Off Label Use of StarClose for Superior Gluteal Artery Puncture Closure Following Embolisation of an Internal Iliac Artery Type II Endoleak. EJVES Vasc Forum. 2021 Apr 1;51:1-4. [CrossRef]
- Fukumoto T, Ogawa Y, Chiba K, Nawata S, Morikawa S, Miyairi T, Mimura H, Nishimaki H. Coil Embolization of Recurrent Internal Iliac Artery Aneurysm via the Superior Gluteal Artery. Ann Vasc Dis. 2023 Jun 25;16(2):135-138. [CrossRef]
- Magishi K, Izumi Y, Tanaka K, Shimizu N, Uchida D. Surgical access of the gluteal artery to embolize a previously excluded, expanding internal iliac artery aneurysm. J Vasc Surg. 2007 Feb;45(2):387-90. [CrossRef]
- Torsello GB, Klenk E, Kasprzak B, Umscheid T. Rupture of abdominal aortic aneurysm previously treated by endovascular stentgraft. J Vasc Surg. 1998 Jul;28(1):184-7. [CrossRef]
- Flohr TR, Snow R, Aziz F. The fate of endoleaks after endovascular aneurysm repair and the impact of oral anticoagulation on their persistence. J Vasc Surg. 2021 Oct;74(4):1183-1192.e5. [CrossRef]
- Cantisani V, Di Leo N, David E, Clevert DA. Role of CEUS in Vascular Pathology. Ultraschall Med. 2021 Aug;42(4):348-366. English. [CrossRef]
- Illuminati G, Nardi P, Fresilli D, Sorrenti S, Lauro A, Pizzardi G, Ruggeri M, Ulisse S, Cantisani V, D'Andrea V. Fully Ultrasound-Assisted Endovascular Aneurysm Repair: Preliminary Report. Ann Vasc Surg. 2022 Aug;84:55-60. [CrossRef]
Figure 1.
Enhanced computed tomography scan showing the left common iliac artery aneurysm after coil embolization and external iliac extension in Figure 1A, and its enlargement with late contrast phase endoleak at 3 years follow-up in Figure 1B.
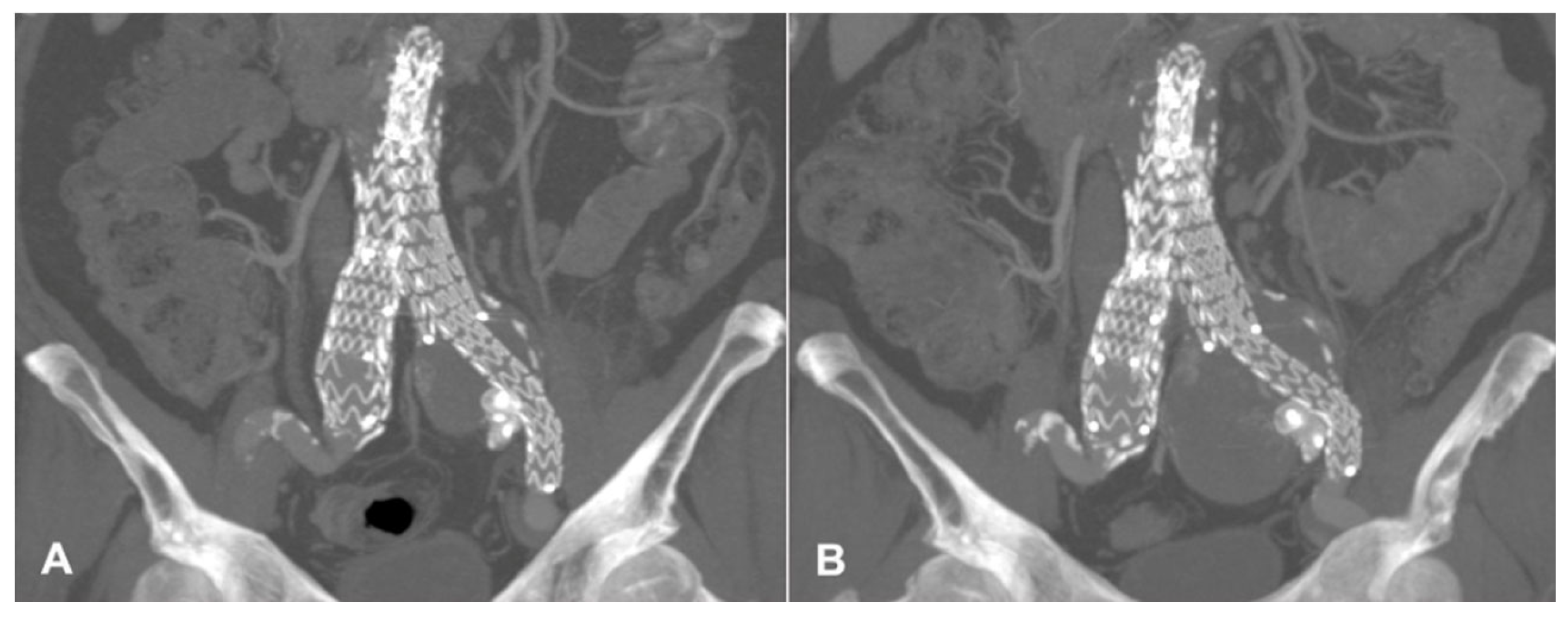
Figure 2.
Intraoperative angiography through the left hypogastric artery showing the common iliac artery aneurism nidus of the endoleak in figure 1A; Coil embolization with embolizing liquid agent in figure 1B and completion angiography with no further nidus visualization in figure 1C.
Figure 2.
Intraoperative angiography through the left hypogastric artery showing the common iliac artery aneurism nidus of the endoleak in figure 1A; Coil embolization with embolizing liquid agent in figure 1B and completion angiography with no further nidus visualization in figure 1C.
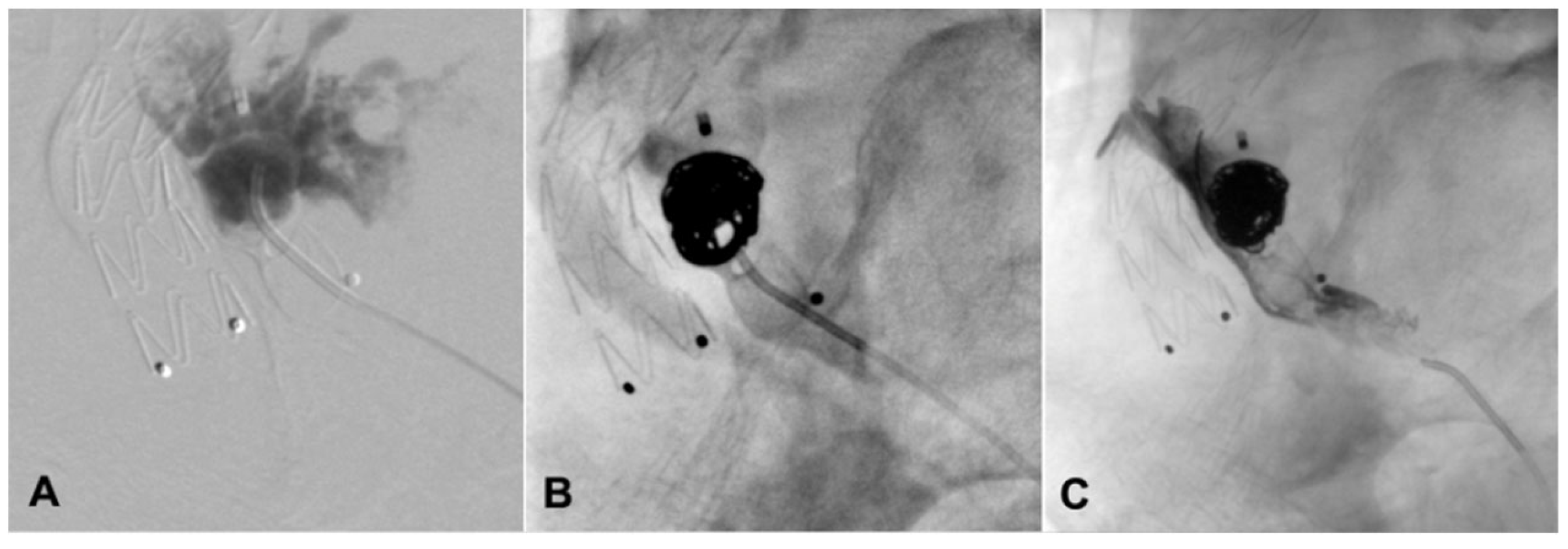
Figure 3.
1-year enhanced CT scan showing the left common iliac artery aneurysmatic sac stability and no endoleak during late contrast phase.
Figure 3.
1-year enhanced CT scan showing the left common iliac artery aneurysmatic sac stability and no endoleak during late contrast phase.
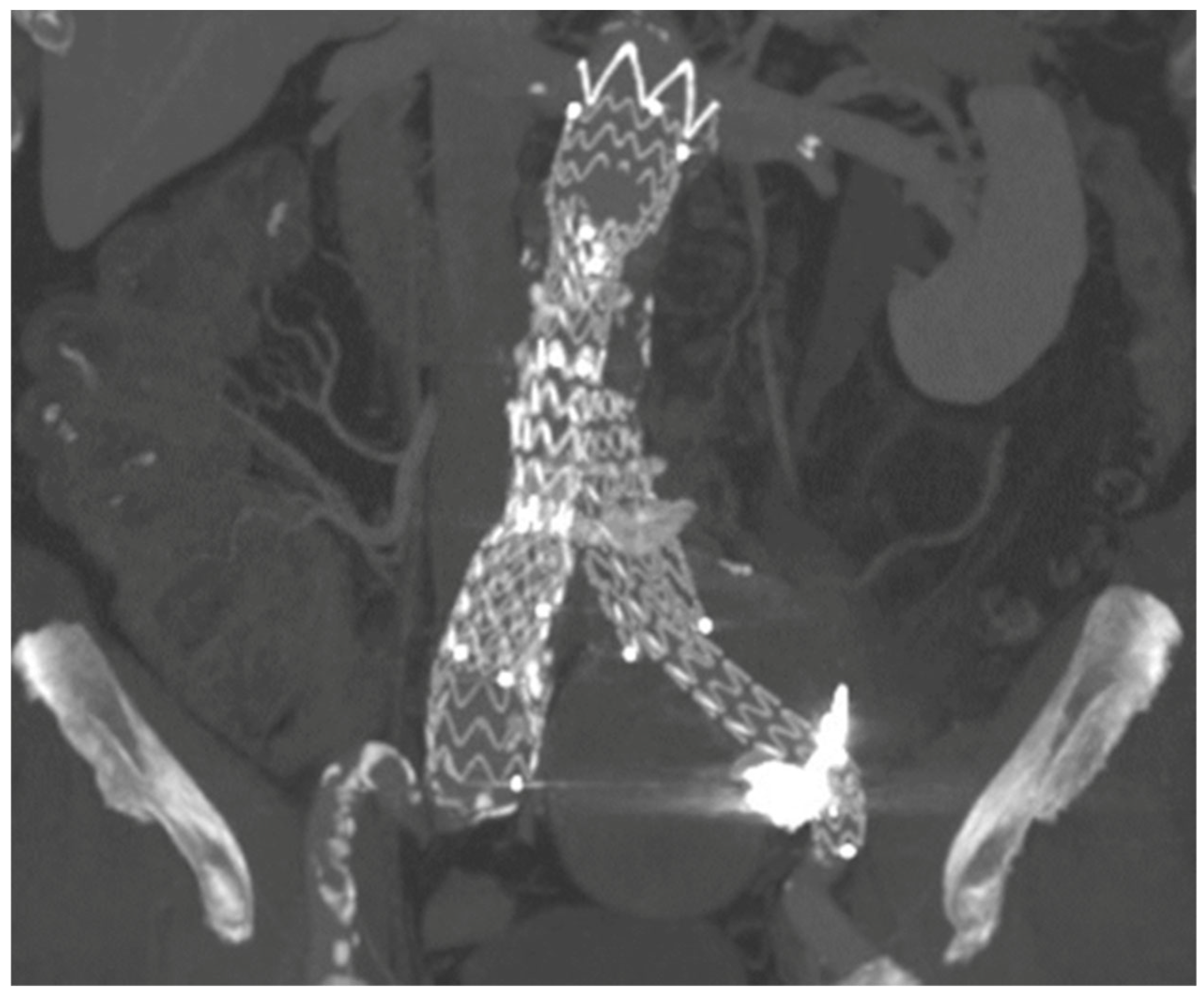

Table 1.
Technical details of reported cases of endovascular treatment of Type 2 endoleak.
| Author, Year | SGA Access | Embolization Technique | Haemostasis | Complication | Follow-Up |
|---|---|---|---|---|---|
| Patel, 2011 |
DUS guided, 4Fr sheath 18G needle |
Microcoils, embolization of the sac and feeding vessels | Manual compression | None | NA |
| Werner-Gibbings, 2013 | CT-guided, 17G needle, sheathless |
Embolization of feeding vessels with coils and sac embolization with liquid embolic agent | Manual compression | None | Not specified, stable sac |
| Herskowitz, 2014 |
Fluoroscopic + DUS guided, 21 G needle, 5Fr sheath |
Feeding vessels embolization with coils + sac embolization with coils and thrombin | Embolization of the SGA with coil + manual compression | None | 6-months CT scan, sac regression |
| Parlani, 2016 |
CT-guided, 21 G needle, sheathless |
Sac embolization with coils | Manual compression | None | 3-months CT-scan, stable sac |
| CT-guided, 21 G needle, sheathless |
Sac embolization with coils | Manual compression | None | 3-months CT-scan, stable sac | |
| Menon, 2018 |
DUS guided, Not specified |
Feeding vessels embolization with coils | Angio-Seal | None | 1-month CT-scan, stable sac |
| Chi, 2018 |
Fluoroscopic + DUS guided, 18 G needle, 5Fr sheath |
Sac embolization with coils and glue | Manual compression | None | CT-scan, stable sac |
| Kim, 2021 |
CT + DUS-guided, 21G needle, 3Fr sheath |
Feeding vessels embolization with coils + sac embolization with coils and liquid embolic agent | Manual compression | Thigh and buttock mild claudication | 1-month CT-scan, stable sac |
| Norris, 2021 |
Fluoroscopic guided, 22G needle, 6Fr sheath |
Sac embolization with coils, liquid embolic agent and plug | StarClose | None | 6-months CT-scan, stable sac |
| Fukumoto, 2023 |
Percutaneous, DUS guided, 18G needle, 17G happycath |
Feeding vessels + sac embolization with coils | Embolization of the SGA with coils | None | 6-months MRI, stable sac |
| Present case | Angiographic + DUS guided, 18G needle, sheathless |
Sac embolization with coils and liquid embolic agent | Manual compression | None | 12-months CT-scan, stable sac |
Legend: MRI, magnetic resonance imaging.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



