
Submitted:
29 January 2024
Posted:
30 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background and Objectives: The COVID-19 pandemic influenced the management of patients with immune mediated rheumatic and musculoskeletal diseases (imRMDs) in various ways. The goal of our systematic review was to determine the influence of the first period of the COVID-19 pandemic on the management of imRMDs.
Materials and Methods: Systematic literature search of PubMed, Cochrane and Embase databases, including studies with adult patients on the influence of the COVID-19 pandemic on management of imRMDs. There were no restrictions regarding to study-design except for systematic reviews and case reports that were excluded as well as articles on the disease outcomes in case of SARS-CoV-2 infection. Two reviewers screened the studies for inclusion, and, in case of disagreement, consensus was reached after discussion.
Results: A total of 5969 potentially relevant studies were found, and, after title, abstract and full-text screening, 35 studies were included with data from 182’746 patients and 2018 rheumatologists. Non-availability of drugs, e.g., hydroxychloroquine and tocilizuab, was frequent (16–69% of patients). Further, medication non-adherence was reported among patients with different RMDs and between different drugs in 4–46% of patients. Changes to preexisting medication were reported in up to 33% of patients (e.g. reducing dose of steroids or cessation of biological disease-modifying antirheumatic drugs). Physical in-office consultations and laboratory testing decreased and as a consequence newly implemented remote consultations increased greatly with an increase of up to 80%.
Conclusion: The COVID-19 pandemic influenced the management of imRMDs, especially at the beginning. Influences were wide-ranging, affecting availability of pharmacies, adherence to medication or medication changes, doctor visits and laboratory testing. New systems of care were set up, including virtual clinics and video consultations. These new forms of health care delivery should be spread and implemented worldwide to routine clinical practice to be ready for future pandemics.
Keywords:
Covid-19
; pandemic
; influence
; rheumatic diseases
; treatment
1. Introduction
In 2019 the novel coronavirus SARS-CoV-2 was identified in China and spread rapidly over countries, causing a worldwide pandemic (1–5). Initially regarded as primarily affecting the lungs, corona virus disease 19 (COVID-19) is now known to be a multisystemic infectious disease that affects different organ systems (6). The course of COVID-19 ranges from mild, to severe and critical cases (depending on risk factors) often requiring intensive care (7).
Patients with immune-mediated rheumatic and musculoskeletal diseases (imRMD) are at higher risk of infections especially due to the use of immunosuppressive medication. The pandemic has therefore raised concerns amongst rheumatologists, especially regarding immunocompromised patients. Data from 2021 show that the risk for infection with SARS-CoV-2 is not increased (8) or is only slightly (9) elevated in patients with imRMDs compared to the general population, but, if infected, the risks for hospitalization or for a severe disease course are increased (7). Most conventional synthetic (csDMARD), biological (bDMARD) and targeted synthetic disease modifying antirheumatic drugs (tsDMARDs) do not seem to increase the risk of infection with SARS-CoV-2 or the risk of poor outcomes of COVID-19, exceptions being glucocorticoids > 10 mg/day, rituximab, mycophenolate mofetil (MMF) and, potentially, Janus kinase inhibitors (JAKi) (9).
The disease course of patients with imRMDs and SARS-CoV-2 infection has been studied widely, but systematic reviews describing the influence of the pandemic on the treatment of imRMDs are lacking.
The aim of this systematic review is to describe the influence of the COVID-19 pandemic on the management of imRMDs on adherence and changes in medications, on the access to rheumatological care and medications and on the use of other health care delivery forms.
2. Materials and Methods
This review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (10) . A comprehensive search was carried out in PubMed, Cochrane and Embase databases regarding publications from 01.12.2019 to 31.10. 2021. We used specific MeSH headings and additional keywords to identify studies (see search strategy in Appendix 1).
We selected articles in English or German including adult patients with imRMDs that evaluated the influence of the COVID-19 pandemic on the general management of imRMDs (Influence on adherence or changes in medications), on the access to rheumatological care and medications, and on the use of other health care delivery forms.
There were no restrictions regarding to study-design except for systematic reviews and case reports that were excluded as well as articles on the disease outcomes in case of SARS-CoV-2 infection. Studies found were screened independently by two reviewers (MS, SBa) for inclusion. In the first phase the studies were screened for title and abstract, followed by full-text screening and data extraction. In case of disagreement, consensus was reached after discussion between the two raters. Quality rating was performed according to the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence (11). Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) (12) was used as the literature management program and Zotero (Corporation for Digital Scholarship, Fairfax, USA) as reference management software (13). Because no randomized controlled trials were published and data were very heterogenous no meta-analysis was performed. Out of the included studies two clusters of “influences of COVID-19 pandemic” were formed and analyzed further regarding: (i) medical management of imRMDs; (ii) health care in general regarding imRMDs.
3. Results
Study Selection
The search strategy identified 5969 potentially relevant studies. Based on title and abstract and after removal of duplicates, 155 studies were assessed in full-text screening. A final total of 35 studies with data from 182’746 patients and from 2018 rheumatologists were included in the systematic review. Figure 1 shows the study flow.
Study characteristics and levels of evidence
The majority of included studies were surveys or questionnaires (14–47), which are evidence grade IV according to the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence (11). One was a cohort study, graded level III (48). Seventeen studies were from Europe (15,16,18,19,21,22,24,28–31,37,39,41,42,46,47), three from Africa (14,17,34) , ten from North America (23,25–27,33,35,36,38,45,48,49) and five from Asia (20,32,40,43,44). Details of the included studies are shown in Table 1.
- Outcomes
- 1) Influence on the medical management of imRMDs
Non-availability of rheumatic medication was a prevalent issue, important examples being hydroxychloroquine (HCQ) and tocilizumab. Shortages or difficulties in the availability of HCQ was an issue in 16–69% of patients (14,15,17,20,23,30,47), with the highest level reported from India (20). Shortages of tocilizumab was reported in 14% of patients (45,47).
Non-adherence to prescribed drugs was another issue. Non-adherence was defined in the different studies very heterogeneously as changing of medication, adaptation of dose or interval without professional health advice or as stopping of medication or irregular intake of medication without professional health advice. The overall non-adherence rate among all included studies was 4–46% of patients (16,26,29–32,43). High rates of non-adherence were reported by four studies (20,21,24,33), with the highest level (46% of patients) reported from India (20). The second highest level of non-adherence (almost 40% of patients) was reported from North America (33). A Swiss study (16) comparing medication adherence of patients with different imRMDs before and during the pandemic found only slight adherence reductions. A significant increase in non-adherence was only seen in patients with axial spondyloarthritis (axSpA) (13% medication non-adherence in pre-COVID-19 period versus 20% during the first wave, P = 0.003). The lowest level of medication non-adherence was reported from Denmark (21). In this study, compliance with medication was compared between the start of the first lockdown to three months later, when society was gradually reopened. Low levels of non-adherence were reported (4-6% at the start of the lockdown versus 2-4% three months later).
The drugs mostly changed or stopped were bDMARDs and JAKi (28,32). Low-dose prednisolone and csDMARDs were the least likely medications to be stopped. Longer disease duration of the underlying rheumatic disease and higher disease activity were significantly associated with medication discontinuation (19). Disease flares were described in high proportions of the patients (63-74 %), who had stopped their DMARDS (15,18).
Regarding different rheumatologic diseases, a study from India (43) found that 43% of patients with inflammatory arthritis, 31% with systemic lupus erythematodes (SLE), and 13% with inflammatory myositis and scleroderma (P < 0.05) stopped their treatment. Further detailed information regarding non-adherence to, or non-availability of medication is shown in Table 2.
Many studies reported reasons for changes in medication-taking. The following factors were significantly associated with change in at least one medication due to patients’ fear of COVID-19 (21): male sex (odds ratio (OR) 1.51, 95% confidence interval (95% CI) 1.21–1.89), age >80 years compared to <39 years (OR 0.11, 95% CI 0.006–0.52), lower education (OR 0.56, 95% CI 0.45–0.69), being employed (OR 1.52, 95% CI 1.16–1.99), and use of bDMARDs (OR 1.86, 95% CI 1.02–3.81). Further, there was a direct correlation of incidence of SARS-CoV-2 infections in the general population and medication non-adherence: the higher the incidence of COVID-19, the lower the medication adherence (24).
Lastly, there was also an influence of the pandemic on the treating physician regarding medication. Rheumatologists reduced the dose of steroids in 23–36% of patients (14,47) and, in 17% of patients, steroids were stopped completely (14). In contrast, csDMARDs were stopped only rarely (in 2 % of patients) (14), whereas bDMARDs were stopped more frequently (in 33% of patients) (15). In a few cases drug application intervals of bDMARDs were extended (28). Moreover rheumatologists were hesitant to start a bDMARD in 75% (47) or a tsDMARD in 14% (14) of cases.
- 2) Influence on healthcare in general
Singh et al. (45) reported an increase in alternative types of visits to the rheumatologist related to COVID-19 compared to the pre-COVID-19 era, such as telephone visits (plus 53%), video-based Veterans Affairs Video Connect (VVC) visits (plus 44%) and clinical video tele-health (CVT) visits with a facilitator (plus 29%). Bos et al. (46) reported telephone visits to be the most commonly used form of remote consultation, with 80% of rheumatologists using exclusively telephone consultations. In-person visits were conducted only in special circumstances, such as for joint aspiration (46).
From the patients’ perspective high levels of unwillingness to health care visits were reported (21–86%) (14,15,27,30,36). The highest levels with 86% of patients unwilling to attend the hospital were reported from Turkey (30). Inability to communicate with or to see the rheumatologist was also frequently reported by 7% (21) to 39% (20) of patients (17,20,21,25,30).
George et al. (27) and Banerjee et al. (36) reported avoidance of laboratory testing in 42% and 47% of patients, respectively. Patients with imRMDs were significantly less likely to avoid in-person visits (OR 0.79 (95% CI 0.70–0.89)) or laboratory tests compared to patients with non-autoimmune RMDs (35% versus 39%, OR 0.84 (95% CI 0.73–0.96) (26,48). Other factors associated with avoidance of in-person visits and laboratory testing were older age, low socioeconomic status, living in urban areas or in countries with higher COVID-19 activity and regarding medication receiving a bDMARD or JAKi (48).
4. Discussion
This systematic review showed that COVID-19 influenced health care behavior in patients, as well as in rheumatologists and other doctors. In many cases patients or doctors discontinued established medication. Further, the pandemic resulted in a collapse of supply chains, causing non-availability of medication, especially in the case of HCQ and tocilizumab. Healthcare appointments took place less frequently than usual and telehealth emerged as a solution, with remote consultations with physicians or with newly established telerehabilitation services.
Medication non-adherence was a common problem among patients. A possible explanation could be the low availability of remote consultations at the beginning of the pandemic, resulting in feelings of insecurity with patients stopping their medication as a self-management strategy. The classes of medication that were discontinued most frequently were bDMARDs and JAKi (26,30), possibly because these immunosuppressive medications are considered the most dangerous regarding infections.
Between different imRMDs, relevant differences in non-adherence to medication have been reported. Low numbers of non-adherence were reported in patients with vasculitis (37,38). Patients with vasculitis are usually aware of the disease course with serious relapses in the absence of maintenance therapy, which results in adherence to treatment (38). Another factor increasing medical compliance is that parenteral treatments are often only possible in the hospital setting and are therefore not postponed by patients.
The sudden discontinuation of anti-rheumatic therapy is a relevant issue, because it can lead to disease flares. A large proportion of patients with different imRMDs reported a flare after modifying their treatment (15,18). This supports the recommendation of not stopping treatment during the pandemic in situations other than suspected or confirmed SARS-CoV2-infection, because resulting disease flares and higher requirements for glucocorticoids could increase the risk of SARS-CoV-2 infection (36).
The pandemic, and mostly the fear of infection with SARS-CoV2, had a severe influence on the medication behavior of rheumatologists. A large proportion of rheumatologists reduced the dose or frequency of steroids (14,47,51), many changed DMARDs (14,22) or stopped them (14,15) and there was hesitancy to start new DMARDs (47,51).
N. Rebić et al. conducted a systematic review about the adherence to medication in patients with imRMDs (51) . They described non-adherence rates of 6.5- 34.2% and discontinuation rates of 2- 31.4% which are similar rates compared to the overall non-adherence rate of 4- 46% in our systematic review. They found slightly higher numbers of physicians who reduced the dose of steroids (23- 56 % v.s. 23- 36% in our review) and they also reported of a reluctance to start bDMARDS or tsDMARDS.
Different non-compliance rates to medical visits were reported between the different studies (22,30). Patients with autoimmune RMDs were significantly less likely to avoid in-person visits and laboratory tests compared to patients with non-autoimmune rheumatic diseases (26,48). These results may be explained with the fact that patients with imRMDs needed close monitoring because of their disease as well as their immunosuppressive treatment and that the fear of an infection with SARS-CoV2 was a more dominant factor determining behavior. Interestingly a study from North America (48) reported a normalization of the rates of follow-up visits a few months after the start of the pandemic, suggesting a rapid adaptation of patients and doctors to the pandemic circumstances.
The COVID-19 pandemic posed many challenges, but it also opened new opportunities for the development of health care systems. Because of the environmental risk factors for acquiring a SARS-CoV2-infection before vaccines existed, practical steps to reduce the infection risk were introduced, including social distancing, hand hygiene and use of face masks (9). As a consequence of social distancing patient consultations were performed remotely whenever possible, leading to an increase in telehealth care. Prior to 2019 telehealth care was very rare or non-existent, but its use grew rapidly during the COVID-19 pandemic. Nevertheless, there were huge differences between different countries in the implementation of telehealth. Data from the USA and Australia showed an increase in telehealth, whereas data from India reported that only a small proportion of patients were aware that telehealth existed, and even fewer used it. It is likely that many patients with imRMDs, especially those from non-urban parts of emerging countries, had no access to telehealth care during the COVID-19 pandemic. A major goal of telehealth was to try to avoid disruption of health care and to prevent patients from stopping their medication. In addition, telephone and video-based consultations were preferred in “stable patients” with known disease course and without the need for changing immunosuppressive medication (45).
Strengths and Limitations
This study has several strengths. Although most studies were of low evidence grade (III or IV), data from 182’746 patients and 2018 interviewed rheumatologists were included. Together with the fact that studies from four different continents and different countries were included, these large numbers paint a global picture of the influence of the pandemic on imRMDs. The influence covers a broad spectrum of issues occurring during the COVID-19 pandemic, including compliance with medication, shortage of certain medications and problems with delivery of health care. In addition, new aspects are described, such as telemedicine and telerehabilitation services, which were set up as substitutes for former in-person routine care.
The study also has limitations. First, regarding the heterogeneity of the reported outcomes and the study designs, it was not possible to carry out a meta-analysis and to evaluate the results statistically using odds ratios. Unclear and inhomogeneous reporting and extensive variation in research methods between studies creates barriers for comparison and generalization to specific patient populations. Furthermore, definitions of non-adherence with medication varied between studies, making it challenging to synthesize findings meaningfully. Most of the included studies were surveys, which leads to some typical limitations regarding the study design. Surveys may lead to inclusion biases, as patients who are more interested or worried about COVID-19 are generally more willing to participate. Responses are self-reported and cannot be verified. Survivorship bias is also probable, as very sick or deceased patients cannot participate. Further, patients with a relatively higher socioeconomic status have a greater online presence and affinity to online surveys and are therefore probably overrepresented. As many of the results were published only as case reports and congress abstracts those results were not included in the present study. Important information may therefore have been missed. Finally, this review shows only results regarding the influence on the treatment of imRMDs of the first wave of the COVID-19 pandemic lasting February 2020 to August 2020.
5. Conclusions
The COVID-19 pandemic influenced the management of patients with imRMDs, especially during first wave when no vaccine was available. The influence of the pandemic was diverse regarding adherence to medication, shortage of some medications, adherence to doctor visits or laboratory testing, and regarding governmental interventions. To preserve adherence to health care the COVID-19 pandemic was a starting point for new health care systems. Virtual clinics and remote and telehealth consultations were implemented. These new forms of health care delivery should be spread and implemented worldwide to routine clinical practice to be ready for future pandemics.
List of Abbreviations
axSpA: axial spondyloarthritis
csDMARDs, bDMARDs, tsDMARDs: conventional synthetic, biological and targeted synthetic disease modifying antirheumatic drugs csDMARDs, bDMARDs, tsDMARDs)
CVT: clinical video tele-health
HCQ: hydroxychloroquine
imRMDs: immune mediated Rheumatic and musculoskeletal diseases
JAKi: Janus kinase inhibitors
MMF: mycophenolate mofetil
NSAIDs: non-steroidal anti-inflammatory drugs
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PsoA : psoriasis arthritis RA: rheumatoid arthritis
SLE: systemic lupus erythematodes
VVC: video-based Veterans Affairs Video Connect
Author Contributions
Conceptualization, methodology, formal analysis and investigation MS and SBa; data curation MS; writing – original draft preparation MS, writing – review and editing MS and SBa; supervision SBa. All authors have read and agreed to the final version of the manuscript.
Funding
This research was funded by Kliniken Valens.
Data Availability Statement
For original data reported in this systematic review we refer to the original publications.
Conflicts of Interest
the authors declare that they have no competing interests.
References
- Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, Lee VJ. Presymptomatic Transmission of SARS-CoV-2 — Singapore, January 23–March 16, 2020. Morb Mortal Wkly Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, u. a. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020, 382, 727–733. [CrossRef] [PubMed]
- Aleem A, Samad ABA, Slenker AK. Emerging Variants of SARS-CoV-2 And Novel Therapeutics Against Coronavirus (COVID-19) [Internet]. StatPearls [Internet]. StatPearls Publishing; 2022 [zitiert 23. Oktober 2022]. Verfügbar unter: https://www.ncbi.nlm.nih.gov/books/NBK570580/.
- World Health Organisation. Tracking SARS-CoV-2 variants [Internet]. [zitiert 23. Oktober 2022]. Verfügbar unter: https://www.who.int/activities/tracking-SARS-CoV-2-variants.
- Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, u. a. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N Engl J Med. 2020, 382, 970–971. [CrossRef] [PubMed]
- Gupta A, Madhavan MV, Sehgal K, Nair N, Mahajan S, Sehrawat TS, u. a. Extrapulmonary manifestations of COVID-19. Nat Med. 2020, 26, 1017–1032. [CrossRef]
- Gandhi RT, Lynch JB, del Rio C. Mild or Moderate Covid-19. N Engl J Med. 2020, 383, 1757–1766. [CrossRef] [PubMed]
- Landewé RBM, Kroon FPB, Alunno A, Najm A, Bijlsma JW, Burmester GRR, u. a. EULAR recommendations for the management and vaccination of people with rheumatic and musculoskeletal diseases in the context of SARS-CoV-2: The 21 update. Ann Rheum Dis. 23. Februar 2022;annrheumdis-2021-222006. 20 November.
- Grainger R, Kim AHJ, Conway R, Yazdany J, Robinson PC. COVID-19 in people with rheumatic diseases: Risks, outcomes, treatment considerations. Nat Rev Rheumatol. 2022, 18, 191–204. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, u. a. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [CrossRef]
- Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009) — Centre for Evidence-Based Medicine (CEBM), University of Oxford [Internet]. [zitiert 2. Juni 2022]. Verfügbar unter: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.
- Covidence [Internet]. [zitiert 24. Dezember 2023]. Covidence - Better systematic review management. Verfügbar unter: https://www.covidence.org/.
- Zotero | Your personal research assistant [Internet]. [zitiert 31. Dezember 2022]. Verfügbar unter: https://www.zotero.org/.
- Akintayo RO, Akpabio AA, Kalla AA, Dey D, Migowa AN, Olaosebikan H, u. a. The impact of COVID-19 on rheumatology practice across Africa. Rheumatology 2021, 60, 392–398. [CrossRef]
- Batıbay S, Koçak Ulucaköy R, Özdemir B, Günendi Z, Göğüş FN. Clinical outcomes of Covid-19 in patients with rheumatic diseases and the effects of the pandemic on rheumatology outpatient care: A single-centre experience from Turkey. Int J Clin Pract. 2021, 75, e14442. [CrossRef]
- Ciurea A, Papagiannoulis E, Bürki K, von Loga I, Micheroli R, Möller B, u. a. Impact of the COVID-19 pandemic on the disease course of patients with inflammatory rheumatic diseases: Results from the Swiss Clinical Quality Management cohort. Ann Rheum Dis. 2021, 80, 238–241. [CrossRef]
- Ziadé N, el Kibbi L, Hmamouchi I, Abdulateef N, Halabi H, Hamdi W, u. a. Impact of the COVID-19 pandemic on patients with chronic rheumatic diseases: A study in 15 Arab countries. Int J Rheum Dis. 2020, 23, 1550–1557. [CrossRef] [PubMed]
- Costantino F, Bahier L, Tarancón LC, Leboime A, Vidal F, Bessalah L, u. a. COVID-19 in French patients with chronic inflammatory rheumatic diseases: Clinical features, risk factors and treatment adherence. Joint Bone Spine. 2021, 88, 105095. [CrossRef]
- Coskun BN, Yagiz B, Pehlivan Y, Dalkilic E. Attitudes of patients with a rheumatic disease on drug use in the COVID-19 pandemic. Adv Rheumatol. 2021, 61, 55. [CrossRef]
- Ganapati A, Padiyar S, Nair A, Gowri M, Kachroo U, Nair A, u. a. Impact of COVID-19 Pandemic and Resultant Lockdown in India on Patients with Chronic Rheumatic Diseases: An Online Survey. Indian J Rheumatol. 2021, 16, 30.
- Glintborg B, Jensen DV, Engel S, Terslev L, Pfeiffer Jensen M, Hendricks O, u. a. Self-protection strategies and health behaviour in patients with inflammatory rheumatic diseases during the COVID-19 pandemic: Results and predictors in more than 12 000 patients with inflammatory rheumatic diseases followed in the Danish DANBIO registry. RMD Open. 2021, 7, e001505. [CrossRef]
- Glintborg B, Jensen DV, Terslev L, Pfeiffer Jensen M, Hendricks O, Østergaard M, u. a. Impact of the COVID-19 pandemic on treat-to-target strategies and physical consultations in >7000 patients with inflammatory arthritis. Rheumatology. 2021, 60, SI3–12. [CrossRef]
- Mancuso CA, Duculan R, Jannat-Khah D, Barbhaiya M, Bass AR, Mandl LA, u. a. Modifications in Systemic Rheumatic Disease Medications: Patients’ Perspectives During the Height of the COVID-19 Pandemic in New York City. Arthritis Care Res. 2021, 73, 909–917. [CrossRef]
- Hasseli R, Müller-Ladner U, Keil F, Broll M, Dormann A, Fräbel C, u. a. The influence of the SARS-CoV-2 lockdown on patients with inflammatory rheumatic diseases on their adherence to immunomodulatory medication: A cross sectional study over 3 months in Germany. Rheumatology 2021, 60, SI51–8. [CrossRef]
- Hausmann JS, Kennedy K, Simard JF, Liew JW, Sparks JA, Moni TT, u. a. Immediate effect of the COVID-19 pandemic on patient health, health-care use, and behaviours: Results from an international survey of people with rheumatic diseases. Lancet Rheumatol. 2021, 3, e707–14. [CrossRef] [PubMed]
- George MD, Baker JF, Banerjee S, Busch H, Curtis D, Danila MI, u. a. Social Distancing, Health Care Disruptions, Telemedicine Use, and Treatment Interruption During the COVID-19 Pandemic in Patients With or Without Autoimmune Rheumatic Disease. ACR Open Rheumatol. 2021, 3, 381–389. [CrossRef] [PubMed]
- George MD, Venkatachalam S, Banerjee S, Baker JF, Merkel PA, Gavigan K, u. a. Concerns, Healthcare Use, and Treatment Interruptions in Patients With Common Autoimmune Rheumatic Diseases During the COVID-19 Pandemic. J Rheumatol. 2021, 48, 603–607. [CrossRef]
- Kalyoncu U, Pehli̇Van Y, Akar S, Kaşi̇Foğlu T, Ki̇Myon G, Karadağ Ö, u. a. Preferences of inflammatory arthritis patients for biological disease-modifying antirheumatic drugs in the first 100 days of the COVID-19 pandemic. Turk J Med Sci. 9. [CrossRef]
- Murray K, Quinn S, Turk M, O’Rourke A, Molloy E, O’Neill L, u. a. COVID-19 and rheumatic musculoskeletal disease patients: Infection rates, attitudes and medication adherence in an Irish population. Rheumatology 2021, 60, 902–906. [CrossRef] [PubMed]
- Seyahi E, Poyraz BC, Sut N, Akdogan S, Hamuryudan V. The psychological state and changes in the routine of the patients with rheumatic diseases during the coronavirus disease (COVID-19) outbreak in Turkey: A web-based cross-sectional survey. Rheumatol Int. 2020, 40, 1229–1238. [CrossRef]
- Sloan M, Gordon C, Harwood R, Lever E, Wincup C, Bosley M, u. a. The impact of the COVID-19 pandemic on the medical care and health-care behaviour of patients with lupus and other systemic autoimmune diseases: A mixed methods longitudinal study. Rheumatol Adv Pract. 2021, 5, rkaa072. [CrossRef]
- Hassen LM, Almaghlouth IA, Hassen IM, Daghestani MH, Almohisen AA, Alqurtas EM, u. a. Impact of COVID-19 outbreak on rheumatic patients’ perceptions and behaviors: A cross-sectional study. Int J Rheum Dis. 2020, 23, 1541–1549. [CrossRef] [PubMed]
- Guaracha-Basáñez GA, Contreras-Yáñez I, Hernández-Molina G, González-Marín A, Pacheco-Santiago LD, Valverde-Hernández SS, u. a. Clinical and bioethical implications of health care interruption during the COVID-19 pandemic: A cross-sectional study in outpatients with rheumatic diseases. Navarini L, Herausgeber. PLoS ONE. 2021, 16, e0253718. [Google Scholar] [CrossRef]
- Abualfadl E, Ismail F, Shereef RRE, Hassan E, Tharwat S, Mohamed EF, u. a. Impact of COVID-19 pandemic on rheumatoid arthritis from a Multi-Centre patient-reported questionnaire survey: Influence of gender, rural–urban gap and north–south gradient. Rheumatol Int. 2021, 41, 345–353. [CrossRef] [PubMed]
- Michaud K, Pedro S, Wipfler K, Agarwal E, Katz P. Changes in Disease-Modifying Antirheumatic Drug Treatment for Patients With Rheumatoid Arthritis in the US During the COVID-19 Pandemic: A Three-Month Observational Study. Arthritis Care Res. 2021, 73, 1322–1331. [CrossRef] [PubMed]
- Banerjee S, George M, Young K, Venkatachalam S, Gordon J, Burroughs C, u. a. Effects of the COVID-19 Pandemic on Patients Living With Vasculitis. ACR Open Rheumatol. 2021, 3, 17–24. [CrossRef]
- İNce B, Bektaş M, Koca N, Ağargün BF, Zarali S, Güzey DY, u. a. A single center survey study of systemic vasculitis and COVID-19 during the first months of pandemic. Turk J Med Sci. 7.
- Kant S, Morris A, Ravi S, Floyd L, Gapud E, Antichos B, u. a. The impact of COVID-19 pandemic on patients with ANCA associated vasculitis. J Nephrol. 2021, 34, 185–190. [CrossRef]
- Cornet A, Andersen J, Tani C, Mosca M. Hydroxychloroquine availability during COVID-19 crisis and its effect on patient anxiety. Lupus Sci Med. 2021, 8, e000496. [CrossRef]
- Rathi M, Singh P, Bi HP, Shivanna A, Kavadichanda C, Tripathy SR, u. a. Impact of the COVID-19 pandemic on patients with systemic lupus erythematosus: Observations from an Indian inception cohort. Lupus 2021, 30, 158–164. [CrossRef]
- Gupta L, Kharbanda R, Agarwal V, Misra DP, Agarwal V. Patient Perspectives on the Effect of the SARS-CoV-2 Pandemic on Patients With Systemic Sclerosis: An International Patient Survey. JCR J Clin Rheumatol. 2021, 27, 31–33. [CrossRef]
- Gupta L, Lilleker JB, Agarwal V, Chinoy H, Aggarwal R. COVID-19 and myositis – unique challenges for patients. Rheumatology 2021, 60, 907–910.
- Kavadichanda C, Shah S, Daber A, Bairwa D, Mathew A, Dunga S, u. a. Tele-rheumatology for overcoming socioeconomic barriers to healthcare in resource constrained settings: Lessons from COVID-19 pandemic. Rheumatology 2021, 60, 3369–3379. [CrossRef]
- Kavadichanda C, Shobha V, Ghosh P, Wakhlu A, Bairwa D, Mohanan M, u. a. Clinical and psychosocioeconomic impact of COVID-19 pandemic on patients of the Indian Progressive Systemic Sclerosis Registry (IPSSR). Rheumatol Adv Pract. 2021, 5, rkab027. [CrossRef]
- Singh JA, Richards JS, Chang E, Joseph A, Ng B. Management of Rheumatic Diseases During the COVID-19 Pandemic: A National Veterans Affairs Survey of Rheumatologists. Arthritis Care Res. Juli 2021, 73, 998–1003. [CrossRef]
- Bos WH, van Tubergen A, Vonkeman HE. Telemedicine for patients with rheumatic and musculoskeletal diseases during the COVID-19 pandemic; a positive experience in the Netherlands. Rheumatol Int. März 2021, 41, 565–573. [CrossRef]
- Dejaco C, Alunno A, Bijlsma JW, Boonen A, Combe B, Finckh A, u. a. Influence of COVID-19 pandemic on decisions for the management of people with inflammatory rheumatic and musculoskeletal diseases: A survey among EULAR countries. Ann Rheum Dis. 2021, 80, 518–526. [CrossRef]
- George MD, Danila MI, Watrous D, Reddy S, Alper J, Xie F, u. a. Disruptions in Rheumatology Care and the Rise of Telehealth in Response to the COVID-19 Pandemic in a Community Practice–Based Network. Arthritis Care Res. 2021, 73, 1153–1161. [CrossRef]
- Licciardone JC. Demographic Characteristics Associated With Utilization of Noninvasive Treatments for Chronic Low Back Pain and Related Clinical Outcomes During the COVID-19 Pandemic in the United States. J Am Board Fam Med. 2021, 34, S77–S84. [CrossRef] [PubMed]
- Rebić N, Park J, Garg R, Ellis U, Kelly A, Davidson E, u. a. A rapid review of medication taking (‘adherence’) among patients with rheumatic diseases during the COVID-19 pandemic. Arthritis Care Res. 2021, acr.24744. [CrossRef]
Figure 1.
Study flow diagram according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 [15].
Figure 1.
Study flow diagram according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 [15].
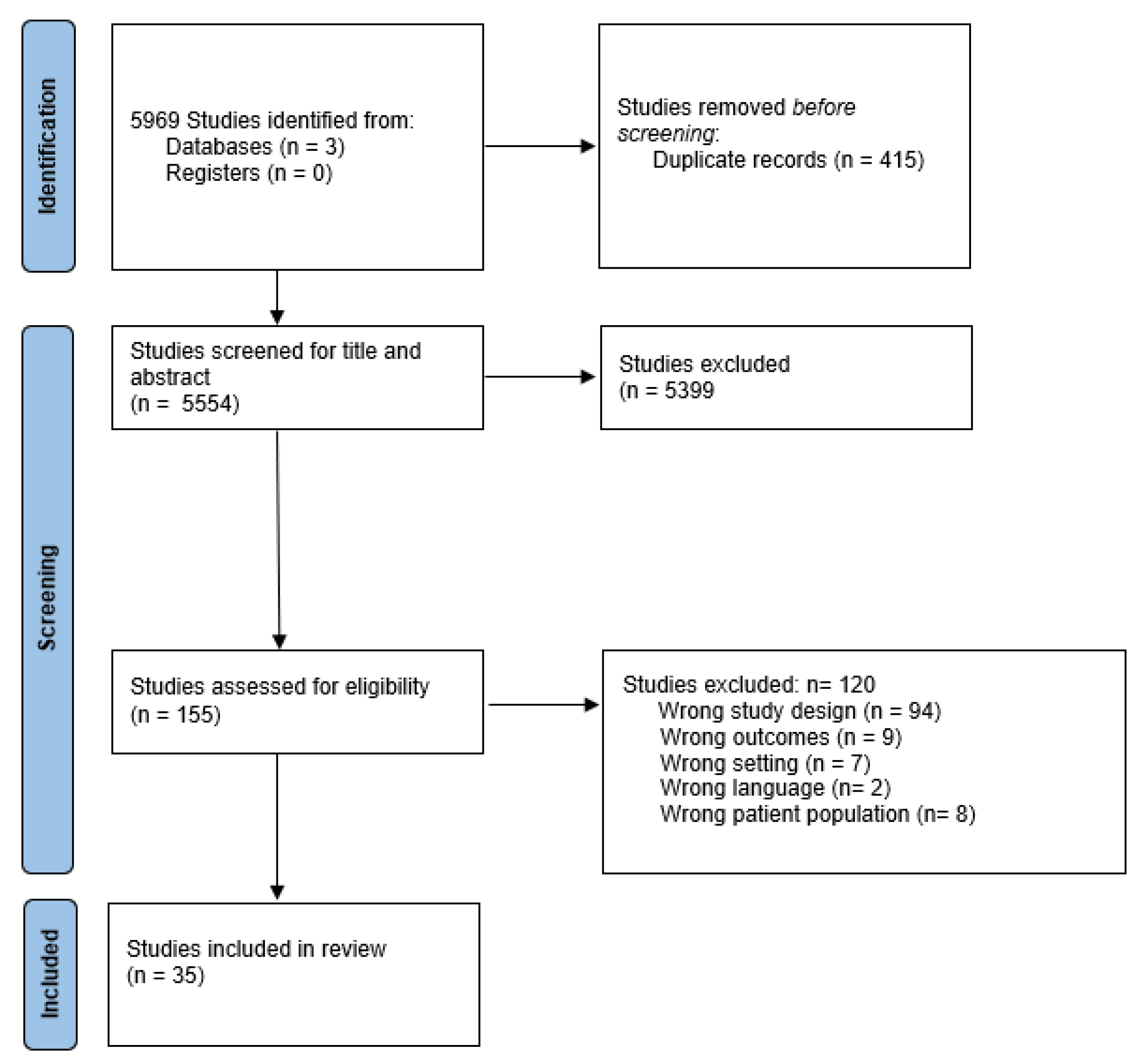

Table 1.
Characteristics of included studies.
| Study, Year, Country/World region | Study design | Reference number | Level of evidence | Research question | Population | Specific influence on the treatment/main outcome measures |
| Abualfadl et al. 2020 Egypt | Survey | 34 | IV | To determine the influence of the COVID-19 pandemic on patients with RA | 1037 patients with RA aged 18 years and older | The following percentage of patients had difficulties obtaining their anti-rheumatic medication: hydroxychloroquine/ chloroquine (42%), methotrexate (6%), biologics (2%), leflunomide (1%)) |
| Akintayo et al. 2021 Africa | Survey | 14 | IV | To identify changes in rheumatology service during the COVID-19 pandemic in Africa | 554 questionnaires completed by rheumatologist | 66% described shortage of hydroxychloroquine; 36% reduced corticoids; 16% stopped corticoids; 14% avoided start of biologics |
| Banerjee et al. 2020 USA | Survey | 36 | IV | To identify effects of COVID-19-pandemic on patients with vasculitis and especially their health related behaviour | 662 patients with vasculitis | 11% of all patients stopped their immunosuppressive therapy. 8% of patients temporarily discontinued rituximab. 13% reported avoiding receiving an infusion with rituximab. 6% of patients on < 10mg prednisone equivalent/ day and 11% > 10mg prednisone equivalent/ day stopped their medication. 66% of all patients avoided doctor’s visits. 47% of all patients avoided laboratory tests. 46% of all patients had a telehealth visit. |
| Batibay et al. 2021 Turkey | Survey | 15 | IV | To determine how the COVID-19 pandemic affected routine care in rheumatology and if there were any changes in rheumatologic medication use | 320 patients with different immune-mediated rheumatic diseases | 16% had problems in getting hydroxychloroquine; 12% changed medication without advice; 33% interrupted bDMARDs with advice from their physician; 9% stopped bDMARDs on their own |
| Bos et al.2020 Netherlands | Survey | 46 | IV | To determine the influence of COVID-19 pandemic on the delivery of care using telemedicine for patients with rheumatic musculoskeletal disease from the perspective of rheumatologists in the Netherlands | 75 members of the Dutch rheumatologist society were interviewed during 8–22 of May 2020 | 99% of the rheumatologists used telephone and 9% used video-consultations. More than 80% of the outpatient consultations were performed exclusively via telephone. |
| Ciurea et al. 2021 Switzerland | Survey | 16 | IV | Adherence to anti-rheumatic drugs before and during the first COVID-19 wave | 666 Patients with immune-mediated rheumatic diseases (RA, AxSpa and PsoA) compared pre-COVID and during COVID-19 wave. | 20% of AxSpA patients were not adherent to anti-rheumatic drugs during the first COVID wave (versus 13% pre-COVID); regarding the other diseases only a slight non-significant increase in nonadherence was observed |
| Cornet et al.2021 Europe | Survey | 39 | IV | Availability of hydroxychloroquine during the first wave of COVID-19 pandemic | 2075 patients with Lupus during the first wave of the COVID-19 pandemic registered in the Lupus Europe’s patient advisory network | 48% could get hydroxychloroquine from the first place they asked, 11% could get the drug by going to more than one pharmacy. 9% could not get any hydroxychloroquine during the first wave of the pandemic. During the second wave only 0.8% of patients could not get any hydroxychloroquine. |
| Coskun et al. 2021 Turkey | Survey | 19 | IV | To assess whether patients maintain their treatment for rheumatic conditions during the pandemic period (and determine the factors responsible for discontinuation) | 278 patients with immune-mediated rheumatic diseases (ankylosing spondylitis (AS) and RA) from Turkey | Overall 22% of patients reduced or stopped treatment. 27% of the patients stopped bDMARDS. 5% stopped low-dose glucocorticoids, 4% stopped methotrexate. |
| Costantino et al. 2021 France | Survey | 18 | IV | Consequences of the pandemic on rheumatic disease management | 655 Patients with immune mediated rheumatic diseases (AxSpA, RA, PsoA) | More than one-third of patients (34.2%) suspended or decreased the dosage of one drug. NSAIDs were the most commonly decreased medication (33.7% of patients), followed by bDMARDS (13.4%) and cDMARDS (10.1%). |
| Dejaco et al. 2020 Austria | Survey | 47 | IV | To asses how the COVID-19 pandemic has affected decisions of rheumatologists | 1286 rheumatologists have been questioned in 58 countries | 82% of rheumatologists indicated cancellation or postponement of face-to-face visits of new patients. 91% indicated cancellations/ postponements in follow-up patients (with 96% offering remote consultation). 74% of rheumatologists indicated bDMARDS/tsDMARDS were less likely to be started during pandemic. 49% reported shortage of HCQ and consequently it had to be stopped in 10% of patients. 14% reported shortage of tocilizumab. 15% recommended decreasing and 2% stopping NSAID in asymptomatic patients. 23% recommended to decrease and 0.1% to stop glucocorticoids in asymptomatic patients |
| Ganapati et al 2021 India | Survey | 20 | IV | To assess the impact of COVID-19 on patients with chronic rheumatic diseases |
1533 completed responses of patients with chronic rheumatic diseases (inflammatory and non inflammatory) across India | 47% of patients were fully compliant to medication. 35% were partly compliant and 11% discontinued their medication. 90% of patients experienced difficulty in procuring medication. 69% of patients on hydroxychloroquine had difficulty getting it. |
| George et al. 2021 North America | Survey | 27 | IV | To learn about patient’s concerns, healthcare disruption and use of telehealth as well as interruption in DMARDs. | 1,517 participants with common immune-mediated rheumatic diseases (RA, PsoA, SpA, or SLE) representing all 50 states of the USA | 15% of the patients without COVID-19 stopped their DMARDs, mostly on their own. |
| George et al. 2021 USA | Survey | 26 | IV | To better understand the concerns and behaviors of patients with autoimmune rheumatic disease compared with patients without autoimmune rheumatic diseases | 2319 patients with a non-autoimmune rheumatic disease and 6885 patients with an autoimmune rheumatic disease from America | 10% of patients with autoimmune rheumatic disease stopped immunomodulatory medication. Patients on biologics or JAK-inhibitors were more likely to stop their medication than the other patients in the population (OR 1.53 (1.22-1.90). Patients with autoimmune disease were significantly less likely to avoid in-person visits (predicted probability 45.2% versus 51.0%, OR 0.79) and avoid laboratory tests compared to patients with non-autoimmune rheumatic diseases (34.9% versus 38.8%, OR 0.84). Patients who had a telemedicine visit were at greater risk of stopping a medication than those with an office visit (OR 1.54) |
| George et al. 2021 USA | Cohort study | 48 | III | Examination of trends in in-person versus telehealth visits versus cancelled visits during COVID-19 pandemic | 126,550 patients extracted from the analytic cohort from the Columbus electronic health record data warehouse of the American Arthritis and Rheumatology Associates network during the year 2020 |
Overall follow-up visit volume decreased by 25% in the COVID-19 transition period but rebounded within a few months to pre-COVID-19 levels. Telehealth visits pre-COVID-19 were nearly non-existent and increased to 41% and 28% of all follow-up clinician visits in the COVID-19 transition period and after the first wave of the pandemic. 90% of telehealth visits were videobased, 7% by phone and 2% digital. Up to maximum of 60% of visits were cancelled during the COVID-19 transition period. The odds of starting a new biologic or JAKi therapy for an RA patient in the COVID-19 transition period in 2020 was substantially lower (adjusted odds ratio=0.55) compared to the corresponding 6-week period in 2019. |
| Glintborg et al. 2021 Denmark | Survey | 21 | IV | To explore self-protection and health behavior including adherence to disease-modifying anti-rheumatic treatment (DMARD) during the COVID-19 pandemic | 12 789 patients with immune-mediated rheumatic diseases (RA, PsoA, AxSpA, connective tissue disorders) | With the beginning of the pandemic restrictions 4% of patients changed the dosage of csDMARDS, whereas 3 months later only 2% of patients did. With the beginning of the pandemic restrictions 6% of patients changed the dosage of bDMARDS, whereas 3 months later only 4% of patients did. |
| Glintborg et al. 2021 Denmark | Survey | 22 | IV | To investigate if the pandemic affected the treat-to-target strategy as evaluated by disease activity and to evaluate access to physical consultations during the COVID-19 pandemic | 7836 patients with immune-mediated rheumatic diseases (RA, PsoA or AxSpA) from Denmark | Glucocorticoid-injections decreased relatively by 16% in patients with rheumatoid arthritis and by 10% in patients with psoriasis arthritis. DMARDS had been altered in dose in 13% of patients compared to before the pandemic. |
| Guaracha -Basanez et al 2021 Mexico | Survey | 33 | IV | To determine the influence of the pandemic on health care interruption on the clinical status of the underlying rheumatic disease | 670 patients with rheumatic diseases (mainly SLE and RA) in Mexico City | 60% of patients were found to be compliant with the prescribed treatment. 51% experienced health care interruptions. |
| Gupta et al. 2020 England | Survey | 42 | IV | To determine the influence of the COVID19-pandemic on the health care of patients with myositis | 608 patients with myositis from all over the world (mostly USA and England) | 26% of patients faced hurdles in procuring medicines. 25% of the included patients were due for infusions, 22% of which had to delay treatment and 7% were still searching for an alternative. Of the patients who faced difficulty in getting their medication 10% were forced to stop treatment due to the situation. Scheduled physiotherapy sessions were disrupted in 35%. 26% experienced difficulty in contacting their specialist, and 5% were unable to do so. |
| Gupta et al. 2021 England | Survey | 41 | IV | To determine the influence of the COVID-19 pandemic on the health-care of systemic scleroderma patients | 291 patients with scleroderma from all over the world | 15.1% of the patients on steroids required an increase in dose in the current situation. 38.1% of respondents faced hurdles in procuring medicines. Of the 14.4% that were on infusions, 45% had to delay it. Physiotherapy sessions were disrupted in 25%. 7% could not contact their specialist, another 24% experienced difficulty contacting their specialist. |
| Hasseli et al. 2021 Germany | Survey | 24 | IV | The goal was to determine the influence of the SARS-CoV-2 lockdown onpatients with immune-mediated rheumatic diseases on their adherence to immunomodulatory medication | 4252 patients with immune-mediated rheumatic disease from Germany | Before the national lockdown 4% of the patients discontinued their medication. During and after the national lockdown reported discontinuations decreased to 2%. |
| Hassen et al 2020 Saudi Arabia | Survey | 32 | IV | To understand the influence of the COVID-19 pandemic on health care behaviour of patients with immune-mediated rheumatic diseases | 637 patients with immune-mediated rheumatic disease from Saudi Arabia | Worsening disease activity perception was significantly associated with poor medication adherence. 86% were adherent and 14% were not adherent to their anti-rheumatic medication. 30% altered their prescribed medication(s) either by decreasing, increasing, or interrupting the dosage. 48% had trouble obtaining their medication during COVID-19 outbreak. |
| Hausmann et al 2021 USA (survey was worldwide) | Survey | 25 | IV | To determine the influence of the COVID-19 pandemic on health care behaviour of patients with immune-mediated rheumatic diseases | 9300 patients with inflammatory rheumatic diseases originating from 90 countries, mostly USA and Europe | 82% continued their anti-rheumatic medications as prescribed. The remaining 18% of participants treated with anti-rheumatic medications discontinued at least 1 of their medications. |
| Ince et al. 2021 Turkey | Survey | 37 | IV | To determine the influence of COVID-19 pandemic on disease activity and medical treatment of patients with vasculitis | 103 patients with vasculitis living in Turkey. | 32% of patients missed at least 1 outpatient appointment. Attendance rate for appointments was higher among patients who used parenteral treatment in comparison to oral treatment. 5% of patients were non-compliant to their medication. |
| Kalyoncu et al. 2021 Turkey | Survey | 28 | IV | The goal was to determine the treatment adherence of patients with immune-mediated arthritis receiving b/s DMARDs | 1394 patients with immune-mediated rheumatic diseases receiving either biologic- or synthetic DMARDS in Turkey | 18% of all patients discontinued their bDMARDs, 32% of them on recommendation of the physician, 45% on their own demand. 14% of the RA patients and 21% of the SpA patients discontinued their bDMARDs. Among patients with RA etanercept was the least frequently discontinued bDMARD (5.4% of the patients), whereas tocilizumab was the most frequently discontinued (20.5% of the patients). In the SpA patient group, those who discontinued their bDMARDs were younger than those who did not (median age, 40 years versus median age, 44 years. 57% of the communications between doctor and patient were by phone. 77% of the patients, who were communicating with their physician, were recommended to continue bDMARD therapy. |
| Kant et al. 2021 USA | Survey | 38 | IV | To determine the influence of the COVID-19 pandemic on the treatment and disease course of patients with ANCA-associated vasculitis | 206 patients with ANCA-associated vasculitis from 2 centres (Baltimore (USA) and Lancashire (UK) | 7% reduced medication dosage. 10% postponed maintenance rituximab infusion. 0% had regular in-person visit with physician. 69% had video visits with physician. 13% rescheduled clinic visits. 16% decreased blood collection frequency. |
| Kavadichanda et al. 2020 India | Survey | 43 | IV | To evaluate the feasibility of having teleconsultation among the socioeconomically marginalized sections of the society in India and the influence on medical treatment. | 373 patients from India with rheumatologic musculoskeletal diseases | 69% of patients continued the drugs based on previous prescriptions, 31% stopped them abruptly. 43% of patients with immune-mediated arthritis stopped their treatment abruptly compared to 31% of patients with SLE (31%) and 13% of patients with Inflammatory myositis or scleroderma. 90% found tele-rheumatology consultation easy to follow. 76% considered that tele-rheumatology was better than in-person consultation in circumstances of the pandemic. 16% felt that tele-rheumatology was not as good as in-person consultation. |
| Kavadichanda et al. 2021 India | Survey | 44 | IV | To evaluate the influence of COVID-19 Pandemic on access to healthcare of systemic sclerosis patients in India | 336 patients with systemic sclerosis from India | Scheduled outpatient visit was missed by 92% of the patients. 22% skipped drugs. 53% missed laboratory testing. 24% faced problems with availability of medicines. |
| Mancuso et al 2021 USA | Survey | 23 | IV | To obtain detailed information about patients’ experiences with their medications during the COVID-19 Pandemic | 112 Patients with immune-mediated rheumatic diseases in New York City | 11–14% of respondents reported self-imposed or physician-directed changes to medications. 61% of the patients treated with HCQ had difficulties obtaining it. |
| Michaud et al. 2020 USA | Survey | 35 | IV | To assess the influence of COVID-19 pandemic on medical treatment of patients with RA in the USA | 734 patients with RA in the USA | 30% of patients reported medication changes. Changers more commonly used glucocorticoids (33% versus 18%) and less commonly used non-hydroxychloroquine-conventional DMARDs (49% versus 62%) pre-COVID. While JAK inhibitor use was associated with change (OR 1.9), only pre-COVID glucocorticoids remained a strong predictor (OR 3.0). bDMARDs (irrespective of mechanism of action) and JAK-inhibitor users reported stopping or delaying the intake of that DMARD more often than users of csDMARDs or hydroxychloroquine (16–18% versus 4–8%). Overall 4–7% could not obtain their medication. 10% of hydroxychloroquine users could not obtain it. Percentage of respondents who cancelled or postponed appointments was between 28% and 35%. 42% and 47% respectively of patients on non-TNF bDMARD or JAK-inhibitors reported switching to telehealth appointments. 34–36% of patients on hydroxychloroquine and other csDMARDs reported switching to telehealth. 31% of patients in the TNF bDMARD group reported switching to telehealth. |
| Murray et al. 2021 Ireland | Survey | 29 | IV | The goal of the survey was to assess COVID-19 status, rheumatic musculoskeletal disease diagnoses and adherence to rheumatologic medication | 1381 patients with immune-mediated musculoskeletal diseases from Ireland | Adherence to anti-rheumatic medications was 84% and 57% were using health authorities guidelines for information on medication use. Adherence rates were higher amongst those who followed guidelines (89.3% versus 79.9%) and lower in those with COVID-19 symptoms (64.0% versus 85.1%). |
| Rathi et al. 2021 India | Survey | 40 | IV | To assess the influence of COVID-19-pandemic on the treatment of SLE | 1040 patients with SLE | 36% of patients reported problems in getting their prescribed medicines due to lockdown. Of these 40% of patients needed to change their medication schedule due to this non-availability. 1% of patients had missed their scheduled cyclophosphamide dose due to either non-availability of drug or facility to provide intravenous infusion. 22% of patients faced difficulty in the availability of hydroxychloroquine. 54% of patients missed their scheduled follow-up visits during the lockdown period. 37% of patients were unable to get their investigations done due to closure of laboratories and hospitals. |
| Seyahi et al. 2020 Turkey | Survey | 30 | IV | The goal was to learn about the healthcare behaviour of rheumatic disease patients during COVID-19 pandemic | 771 patients with rheumatic disease and as a control group 535 hospital workers, and 917 teachers/academic staff. | Overall 22% of the patients discontinued their medications. In patients with SpA 54% discontinued their medication. Biological DMARDS were the most frequent drugs whose doses were skipped or stopped: anti-IL-1 agents: in 40%, anti-TNF agents in 35%, interferon in 33%, tocilizumab in 29%, rituximab in 7% of the patients. Prednisolone (low dose), azathioprine, methotrexate, leflunomide, colchicine, and sulfasalazine were least likely (≤ 10% for each drug) to be skipped or stopped. 11% of the patients on hydroxychloroquine had to skip or stop the drug due to shortage or failure of prescription renewal. 86% of patients with rheumatic diseases were unwilling to go to the hospital. Only 14% of patients visited the outpatient clinic "as it was before", 43% "did not want to come", 28% "were advised to postpone their visits". |
| Singh et al. 2020 USA | Survey | 45 | IV | To assess the experience, views and opinions of rheumatology providers during the COVID-19 pandemic. | 103 rheumatologists answering a survey | 32% of responders reported a medication shortage. Shortage of hydroxychloroquine was reported in 45%, of IL-6 inhibitors in 15%, non-TNF biologics in 1%; Janus-inhibitors in 1%. An increase in 50% or more in the following types of visits related to COVID-19 were reported: (1) telephone visits, 53%; (2) video-based VA video connect (VVC) visits, 44%; and (3) clinical video tele-health (CVT) visits with a facilitator, 29%. |
| Sloan et al. 2021 UK | Survey | 31 | IV | To assess the influence of the COVID-19-pandemic on medical care and health care behaviour of patients with SLE and other autoimmune rheumatic diseases | 111 patients with autoimmune rheumatic diseases | 10% of patients reduced or stopped their medication and 10% increased the dose of their medication without advice of their doctor. 70% reported that their appointments, tests and treatments had been cancelled more/much more frequently since the pandemic. Between 35% and 45% felt that care from GPs, rheumatologists and other specialists had been worse/much worse during the pandemic. |
| Ziadé et al. 2020 Arab countries (Levant, Gulf, North Africa) | Survey | 17 | IV | Influence of the COVID-19 pandemic on access to rheumatology care for patients with chronic rheumatologic diseases | 2190 Patients with chronic rheumatic diseases from different Arab Countries | 70% reported no negative effect on medication adherence; 18% described shortage of hydroxychloroquine, thereof 15% had to stop medication due to shortage; 8% stopped medication because of fear of infections |
ARD = autoimmune rheumatic disease; AxSpA = axial spondyloarthritis; bDMARDS = biological disease modifying anti-rheumatic drugs; CQ = chloroquine; csDMARDS = conventional synthetic disease modifying anti-rheumatic drugs; GP = general practitioner; HCQ = hydroxychloroquine; NSAID = non-steroidal anti-inflammatory drug; OR = odds ratio; PsoA = psoriasis arthritis; RA = rheumatoid arthritis; SLE = systemic lupus erythematosus; SpA = spondyloarthritis; tsDMARDS = targeted synthetic disease modifying anti-rheumatic drugs.
Table 2.
Rates of non-adherence and of difficulties obtaining medication regarding different immune-mediated RMDs.
Table 2.
Rates of non-adherence and of difficulties obtaining medication regarding different immune-mediated RMDs.
| Disease | Non-adherence to or discontinuation of medication (% of patients)* |
Difficulties obtaining medication (% of patients)* |
| Inflammatory arthritis | ||
| Rheumatoid arthritis | 14% (bDMARDS) (27) 19% (29) 22% (DMARDS) (15) 23% (17) 25% (18) |
42% (hydroxychloroquine) (33) 10% (hydroxychloroquine) (34) 4-7% (34) |
| Vasculitis | ||
| Vasculitis in general | 5% (36) 11% (35) 20% (29) |
No information |
| Spondyloarthritis | ||
| Spondyloarthritis in general | 19% (18) 20% (DMARDS) (15) 21% (bDMARDS) (27) 38% (17) 54% (29) |
No information |
| Psoriasis arthritis | 19% (DMARDS) (15) 31% (17) |
No information |
| Myositis | ||
| Myositis in general | No information | 26% (41) (myositis) |
| Connective tissue diseases | ||
| overall | 14% (29) | No information |
| SLE | No information | 52% (hydroxychloroquine) (38) 29% (hydroxychloroquine) (39) 36% (39) |
| Systemic sclerosis | 22% (43) | 38% (40) 24% (43) |
| Periodic fever syndromes | ||
| Familial Mediterranean fever | 15% (29) | No information |
*If the number relates to a specific drug it is mentioned in brackets. Otherwise the number relates to non-adherence, discontinuation or difficulties obtaining medication in general (numbers in brackets=literature reference numbers).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



