
Submitted:
30 January 2024
Posted:
31 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The aim of this retrospective study was to identify myocardial injury after COVID-19 inflamation and to explore whether myocardial damage could be a possible cause of the persistent symptoms following COVID-19 infection in previously healthy individuals.
The study included 139 patients who were enrolled between January-June 2021, mean age 46.7±15.2 years, 68 were men, 71 were women without known cardiac or pulmonary diseases. All patients underwent clinical work up, lab. analyses, cardiac ultrasound, and CMR on 1.5 T scanner using a recommended protocol for morphological and functional assessment before and after contrast media application with multi-parametric sequences.
In 39% of patients late gadolinium enhancement (LGE) was found as a sign of myocarditis. Fibrinogen was statistically significantly higher in patients with LGE than in those without LGE, (4.3±0.23 vs 3.2±0.14g/L, p<0.05; respectively), as well as D-dimer (1.8±0.3 vs 0.8±0.1 mg/L FEU). Also troponin was statistically significantly higher in patients with myocardial LGE (13.1±0.4ng/L) compared to those with normal myocardium (4.9±0.3ng/L, p<0.001). We demonstrated chest pain, fatigue and elevated troponin to be independent predictors for LGE. Septal LGE was shown to be predictor for arrhythmias.
The use of CMR is a potential risk stratification tool in evaluating outcomes following COVID-19 myocarditis.
Keywords:
myocarditis
; COVID-19 infection
; Cardiac magnetic resonance
; Late Gadolinium Enhancement and prognosis
1. Introduction
Myocarditis is an inflammatory process affecting the myocardium that may be caused by infective and toxic agents, immune-mediated factors. Myocarditis is the third most common cause of sudden cardiac death and has been associated with 5–12% of sudden cardiac deaths in young athletes [1]. Diagnosis by clinical assessment is not always reliable because myocarditis has a wide spectrum of clinical manifestations. Endomyocardial biopsy is the gold standard for the diagnosis of myocarditis, but it carries its own risks as an invasive procedure [2]. Recent research suggests that COVID -19 infection leads to endothelial damage of multiple organs, including the kidneys, heart, brain, and blood vessels, followed by systemic inflammation [3]. Besides affecting the respiratory system, COVID -19 infection has adverse effects on the cardiovascular system and has been associated with myocardial injury causing ischemia, inflammation, or myocarditis [4]. The development of myocarditis associated with COVID -19 infection leads to considerable morbidity and mortality along with a degree of myocardial injury that can be assessed using cardiac magnetic resonance imaging (CMR). Cardiac injury as a result of COVID -19 infection has been associated with worse prognosis [3].
CMR imaging allows comprehensive assessment of myocardial function and tissue characterization in patients with cardiovascular disease. Information provided by overall CMR analysis, including left ventricular ejection fraction, can be a useful tool to assess prognosis in cardiac disease in addition to conventional risk factors [5]. Therefore, CMR parameters of myocardial tissue damage and cardiac function are increasingly recognized in order to improve treatment and therapy in this population.
CMR as a non-invasive imaging modality has been introduced and its use has been established for detecting myocarditis. CMR allows non-invasive diagnosis of the disease but does not allow the underlying cause to be distinguished [6]. It has a high positive predictive value, making a diagnosis in up to 79% of pathologically proven myocarditis cases [7].
Nowadays CMR findings of myocarditis in patients post COVID -19 infection have become a subject of interest. The majority of patients who have cardiovascular complications related to COVID -19 infection have myocarditis as the primary cause of cardiac dysfunction [8]. COVID -19 infection is associated with myocardial injury in a significant number of patients. Myocardial injury in hospitalized patients with COVID -19 is accompanied by a worse prognosis [9]. Myocardial damage in a form of edema, LGE phenomenon/fibrosis and pericardial inflammation after COVID -19 infection was seen using CMR.
CMR imaging has benefit in assessing myocarditis using Lake Louise criteria (LLC) established in 2009. year that include the presence of edema, hyperemia, and necrosis/or fibrosis [10]. The original LLC were modified in 2018. year since several limitations were progressively discovered. As per the 2018. LLC, the diagnosis of CMR-based myocarditis should include at least one T1-based criterion (increased myocardial T1 relaxation times, extracellular volume, or Late Gadolinium Enhancement – LGE plus at least one T2-based criterion (increased myocardial T2 relaxation times, visible regional high T2 signal intensity representing edema on T2 STIR, or increased T2 signal intensity ratio) [11,12] (Figure 1).
Purpose
The purpose of our study was to identify myocardial injury in patients after COVID -19 infection and to explore the relationship between clinical and laboratory parameters and the degree of myocardial damage. Also, we intended to explore whether myocardial injury and inflammation could be a possible cause of the persistent symptoms following COVID -19 infection in previously healthy individuals.
2. Materials and Methods
Our study is a retrospective, single center analysis conducted in University Clinical Centre of Serbia and was performed in concordance with the Helsinki Declaration and International Conference on Harmonization of Good Clinical Practice. Written informed consent of patients was obtained after providing them all information regarding the study and the potential risks of participation.
2.1. Study Participants
The study included 139 patients who were enrolled between January and June 2021. The mean age of participants was 46.7±15.2 years, and 68 were men (49%) and 71 were women (51%) without known cardiac or pulmonary diseases. Patients were assessed based on reports of persistent fatigue, exertional dyspnea, chest pain and arrhythmias after COVID -19 convalescence. All patients underwent clinical work up, lab. analyses, cardiac ultrasound, and CMR.
Patients with Chronic Covid Syndrome (CCS) had a negative polymerase chain reaction test result and had experienced resolution of acute COVID -19 symptoms for at least 2 weeks before CMR was performed.
2.2. CMR Protocol
CMR was done using a standard protocol for morphological and functional assessment, LGE, as well as T1 and T2 mapping using Modified Look-Locker inversion recovery (MOLLI) sequence, before and after contrast media application. Before CMR scanning, the weight and height of the patients were measured and they were informed about the procedure. Examinations were performed using a 1.5T scanner (Avanto fit, Siemens Magnetom, Erlangen, Germany). During the evaluation, patients were placed lying down in the supine position, head first, with ECG pads placed on the chest.
Electrocardiogram-gated steady-state free-precession (SSFP) cine images were acquired in short-axis, two-chamber, three-chamber and four-chamber views for functional analysis. All images were obtained using retrospective gating during a gentle expiratory breath-hold. Short axis cine images were acquired as a stack from the mitral valve plane through the apex covering the entire ventricles, slice thickness was 8 mm, field of view 360x306 mm. T2-weighted with fat suppression sequences in short-axis and 4 chamber views were performed for visualization of myocardial edema.
T1 mapping was performed with modified MOLLI sequence, with a 3(3)3(3)5 sampling pattern, acquired pre- and 15 min following bolus contrast administration in 3 short-axis images (basal, mid-ventricular, and apical levels) and in a 4-chamber view with variable inversion preparation time, during the same cardiac phase at late diastole using the same imaging parameters. Acquisition parameters included echo time/repetition time = 1.13/279.84 ms, field of view = 360x306 mm, flip angle = 35°, matrix size = 256 x 168, GRAPPA = 2, 36 reference lines, cardiac delay time TD =504 ms, interpolation = 0.7x0.7, inversion-time increment 180 ms and phase partial Fourier 7/8. For myocardial T2 mapping, a six-echo gradient spin-echo sequence was applied.
LGE images were acquired after 8-10 minutes of contrast application using phase sensitive inversion recovery sequence (PSIR). Before patients were scanned, a time to inversion (TI) scout was done in order to select optimal inversion time for delayed enhancement. PSIR was done in SAX view covering the whole ventricle with slice thickness of 6 mm, and also in 2, 3 and 4-chamber views. LGE images were obtained at the different planes for the presence or the absence of enhancement in each segment. For contrast enhancement, a bolus of 0.2 mmol of Gadobutrol (Gadovist, Bayer Inc, Canada) per kilogram of body weight was administered.
2.3. Image Analysis
Image analysis was performed using dedicated software Syngo via by Siemens and reviewed by two experienced radiologists, one with experience in cardiac MRI over 20 years and the other with experience of 3 years. Using Argus (Siemens Healthcare, Erlangen, Germany), LV short-axis epicardial and endocardial borders were manually contoured at end-diastole and end-systole for determining EDV, ESV, SV, EF, and myocardial mass in short axis images. Parameters were recorded in absolute numbers and indexed by body surface area. Images were acquired in traditional multi-breath-hold cine CMR sequences.
The presence of focal areas of regional high signal intensities in a non-ischemic distribution pattern on T2 weighted sequence with fat suppression and on LGE images was visually assessed by two radiologists. Quantitative markers of myocardial edema were calculated by T2 mapping values. Reference cut off values for T1 and T2 mapping were measured by ROI. The cut-offs for the diagnosis of myocardial inflammation were greater than or equal to 1060 msec for myocardial T1 relaxation times and greater than or equal to 55 msec for myocardial T2 relaxation times.
2.4. Statistical Analysis
SPSS Statistics version 27 (IBM) was used for all statistical analyses. Participant characteristics are given as means ± standard error or as absolute frequencies with percentages. Data were checked for normal distribution by using Shapiro-Wilk test. Continuous variables were compared using the Student t test or Mann-Whitney U test, and categorical variables were compared using the Chi2 test. For comparison of continuous interindividual variables, the Student t test or Mann-Whitney test were used depending on that data distribution. For intra-individual comparisons, the Wilcoxon rank test was used.
For an exploratory analysis of potential predictors for cardiac fibrosis laboratory parameters, clinical symptoms and native T1 maps were first tested in a single variable analysis and then, if significantly different, in multivariate analysis. Hazard ratios with
95% CIs were calculated with Cox models. All tests were two-sided, and p<0.05 was considered indicative of statistically significant difference.
3. Results
3.1. Patient Characteristics
A total of 139 participants were included in this retrospective study and statistical evaluation. There were no significant differences between men and women regarding age (p=0.56).
The median time between initial COVID-19 diagnosis and CMR was 135 days (range 15- 378 days) (minimum 15 days, max 378 days). Participants undergoing CMR exam following recovery of COVID -19 infection reported dyspnea (58 pts, 41.7%) fatigue (82 pts, 59 %), chest pain (48 pts, 34.5%) and arrhythmias (54 pts, 39%) (Table 1).
3.2. CMR Findings
In this population, 85 pts (61.2%) had a normal myocardium on CMR, while in 54 patients (38.8%), LGE was found as a sign of myocarditis sequelae. Findings of myocarditis were more often seen in male than in female patients (61% vs 39%) with a statistical significance regarding sex (p=0.032, p<0.05), while there were no significant differences based on age (p=0.566). Statistically significant higher values of T1 mapping were seen in the LGE group (1103.9±17.2 ms) than in patients with normal myocardium (1063.5±9.7 ms) (t=-2.2, p=0.033)
3.3. Laboratory Parameters
Fibrinogen levels were statistically significantly higher in patients with LGE than in those without LGE (4.3±0.23; 3.2±0.14 g/L; respectively, p<0.001, t=-4). Also, D dimer levels were higher in patients with LGE (1.8±0.3 mg/L FEU) compared to those with no myocardial LGE (0.8±0.1mg/L FEU) This was statistically significant (p=0.005, Z=-3.9). Troponin was another laboratory parameter that was statistically significantly higher in patients with myocardial LGE (13.1±0.4 ng/L) compared to those with normal myocardium (4.9±0.3 ng/L) with p<0.001, Z=-9.5. Higher values of creatine kinase (CK) were found in the LGE group 143.9±12.4 u/L compared to the non-LGE group that had a mean value of CK of 112.8±6.9 u/L. There were statistically significant differences between those values (p<0.05) p=0.042, Z=-1.6.
3.4. Clinical Symptoms
Patients with fatigue as a symptom of COVID-19 infection had a 22-fold risk for LGE (Chi2 41.2, p<0.001), and 50 (61%) of them had myocardial injury or LGE, while 32 (39%) had normal myocardium.
Regarding dyspnea, there were no significant differences between groups with LGE and without LGE (Chi2 1.5, p=0.213). In patients with dyspnea, LGE was seen in 19 pts (32.8%) while 39 pts (67.2%) had normal CMR findings.
Chest pain was demonstrated to be a predictor for LGE (Chi2 9.3, p<0.01, p=0.002). In patients who had symptoms of chest pain, 27 had LGE (56.3%) while 21 pts had no LGE (43.7%).
We demonstrated in multivariate analysis that from all those parameters that were statistically significant in univariate analysis, only chest pain, fatigue and troponin elevation were independent predictors for LGE (Chi2 112.6, p<0.001, B=-10.6) adjusted for age and sex (Table 2).
3.5. LGE Localization
Regarding patients with LGE and myocardial damage (n=54), a 6-fold increased risk for arrhythmias was noted in comparison with those without myocardial fibrosis. Related to localization of LGE in patients with arrhythmias, only one patient had fibrosis in the lateral wall of left ventricle (4%), while fibrosis was seen in the septal wall in 8 pts (32%). Septal LGE was shown to be predictor for arrhythmias (Chi2 7.9, p=0.005).
Troponin elevation was also shown to be a predictor for palpitations. In patients with arrhythmias, mean troponin levels were 10.4±0.8 ng/L while in patients with no arrhythmias mean troponin levels were 7.4±0.5 ng/L and there was a statistically significant difference (p<0.001, Z=-3.3). T1 mapping was not demonstrated to be a predictor for palpitations since there were not statistically significant differences seen between groups with and without palpitations (p>0.05, p=0.122, t=-1.4; mean values 1100.8±21.4 ms, 1071±9.6 ms; respectively).
In multivariate analysis including troponin, LGE and native T1 maps, LGE was shown to be the only independent predictor for arrhythmias and palpitation. (Chi2 17.2, p<0.001)
4. Discussion
CMR is a noninvasive gold standard method for evaluating cardiac function, structure and tissue characterization. COVID -19 has now been determined to be a multisystem disease, affecting many parts of a human body. Fatigue and dyspnea have been described to be some of the most common post COVID -19 symptoms [13,14]. The long-term risks of CCS are still unknown, and the pathophysiology and outcome of CCS is poorly understood. We hypothesized that CCS may be caused by ongoing myocardial injury and inflammation and proceeded to investigate by CMR.
In our population of symptomatic patients following COVID -19 infection, the percentage of positive images for cardiac damage was lower than what was previously reported by Puntmann et al. [15] (78%), and Huang et al. [16] (58%), but rather similar to Wang et al. [17] (30%). We found evidence to support our hypothesis that CCS in young, previously healthy patients who have had COVID - 19 is caused by structural myocardial damage.
In the study by Puntmann [15], 33% of patients had a severe course of disease requiring hospitalization. In our study most participants with CCS had a mild initial course of COVID -19, but nonetheless myocardial damage was present in almost 39% of patients. Latent myocardial injury and inflammation could be one of explanations and possible reason for prolonged fatigue in these previously healthy patients. It should be noted that in the study by Kravchenko [18], individuals with CCS did not show signs of active myocardial injury or inflammation as determined by cardiac MRI. In the Kravchenko study [18], no connection was found between CCS symptoms and myocardial inflammation induced by COVID-19, despite other reported studies.
Our study determined that chest pain is an independent predictor for LGE and myocardial damage. In the literature, there are still no data regarding chest pain and segmental myocardial fibrosis in the LV in patients with myocardial infarction [19] as well as myocardial inflammation. Our study also did not find a connection between chest pain and localization of fibrosis.
We demonstrated in our research that besides clinical symptoms, there are laboratory parameters which could be predictors for myocardial fibrosis. It is well known that cardiac troponins are sensitive and specific markers of myocardial injury. In a study of hospitalized patients with COVID -19, cardiac injury was defined by elevated troponin levels (men > 26 ng/mL, women > 11 ng/mL) and was found in 30% of patients [20]. Elevated troponin levels in this population were associated with a higher in-hospital mortality rate when compared to patients who had normal troponin levels (40.9% vs 11.1%) [20].
Troponin levels in our population were noted to be an independent predictor for LGE. Also increased values of troponin were shown to be predictors for arrhythmias. Multiple previous studies reported and identified the prognostic significance of troponin elevations in cardiac patients, with higher levels being associated with an increased risk of acute coronary syndromes and heart failure [21,22,23]. Besides predicting poor outcomes in those conditions, this myocardial biomarker has an important prognostic significance in myocarditis.
Patients in our study with cardiac injury presented with more severe acute disease symptoms especially with a lower blood oxygen saturation level and higher inflammatory biomarkers including troponin and fibrinogen. Elevated troponin (above 10 ng/L in women and 15 ng/L in men) was detected in 40% and elevated fibrinogen levels (above 4g/l) were found in 17% of the study population. Those values were significantly higher in patients with proved myocardial damage. In Wuhan, elevated hs-Troponin was present in 7.2–12% of patients, and around 80% of those with myocardial damage needed intensive care [3]. Cardiac injury in patients has been associated with a lower short term survival rate compared to patients without myocardial damage, increasing the risk of short-term mortality by nearly two-fold [24].
As for the localization of LGE after COVID -19 infection most of our patients had infero-postero-lateral subepicardial damage, about 15%, that is quite often and typical in this type of myocarditis (Figure 2). We showed that when compared to other localization of LGE, most patients with septal LGE developed arrhythmias after COVID -19 infection (Table 3). Similar findings were presented in an Italian study, ITAMY, in which this septal localization of LGE had the worst outcome in the follow up of patients [25,26] (Figure 3).
It is known that CMR has prognostic value based on LGE presence, localization and pattern [26,27,28]. Grän et al. investigated retrospectively 744 patients with suspected myocarditis and reported that MACE (major adverse cardiovascular events) occurred in 15% and LGE was present on CMR in 44% of patients [28]. In terms of the LGE localization and myocardial pattern of LGE, mid-wall and patchy involvement demonstrated a more than 2-fold increased hazard to MACE [28]. Septal LGE location showed strong association with MACE, whereas lateral location did not show significant association with MACE [28] (Figure 4). In another study that investigated the difference between immune checkpoint inhibitor induced myocarditis (ICI-M) and virally-induced myocarditis, septal LGE was found to be a predictor of MACE in patients with drug induced myocarditis [29] (Figure 5).
LV ejection fraction obtained by CMR has been strongly correlated with clinical outcome after myocardial infarction [21,22]. In clinical practice, LV ejection fraction is still the most substantial predictor of adverse outcome and represents the basis for further treatment decisions. A recent study of patients with LVEF <40% and LGE presence found a significantly higher risk for a cardiovascular event in this group compared to those with better ejection fraction [30]. Therefore, it is useful to evaluate both CMR parameters, LVEF and LGE, in assessing cardiovascular risk. However, Sanguineti et al. studied 203 patients with myocarditis based on CMR criteria and found that LVEF was a predictor for MACE in adjusted analysis, whereas LGE-based variables were not [31]. In our population ejection fraction was preserved and has not been predictor for described complaints of patients.
CMR is a potentially helpful diagnostic tool in patients with COVID -19 presenting with myocardial injury and evidence of cardiac dysfunction [30,32]. Late gadolinium enhancement on CMR has been shown to be a promising method for improved long-term risk stratification and to evaluate further outcomes [33]. In this context, CMR should be considered to be an important step forward for personalized medicine and treatment. CMR has become a routine clinical and diagnostic method; however, the current prognostic evidence of this approach is still limited.
This study is the first and largest one in Serbia dealing with prognostic clinical and laboratory parameters in COVID -19 patients and the degree of myocardial damage.
5. Conclusion
Early detection of acute or chronic sequelae of infection is of utmost importance for determining the optimal therapeutic approach in patients with myocarditis. The use of CMR is a potential risk stratification tool in evaluating outcomes following COVID -19 myocarditis.
Limitation of study
It is important to note several limitations of our study. In each of the patients that were evaluated, this was the first CMR, so we cannot be sure that the reported CMR findings were not also present before SARS-CoV-2 infection. To minimize the role of pre-existing conditions, we included only patients without a history of treatment for cardiac and pulmonary disease. Also, no histopathologic analysis was performed regarding the presence of active myocarditis. However, the quantitative multiparametric MRI techniques that were applied have been reported to provide highly sensitive detection of subclinical myocardial edema and inflammation in post COVID -19 patients.
Author Contributions
Conceptualization ONA, GK and AR; methodology ONA and RM, software RM and AR, validation NDJ and MT; formal analysis NDJ and MT; investigation ONA and GK; resources GK and AR; data curation NDJ and MT; writing – original draft preparation ONA, NDJ and MT; writing – review and editing GK, AR and RM; visualization ONA and RM; Supervision RM, project administration ONA and RM; funding acquisition RM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical Committee of University Clinical Centre of Serbia for our study was not necessary since the patients underwent a routine procedure and diagnostic CMR imaging which is according to the rules of our Hospital and a part of patient's hospitalization and treatment in our country. Patients all signed form and consent for cardiac magnetic resonance and scanning with contrast application. .
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors would like to express their gratitude to Srdjan S. Nedeljkovic, MD, Anaesthesia at Harvard Medical School, Brigham and Women’s Hospital, for critically reading the draft versions of this article and for improving the English language.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vidal-Perez, R.; Abou Jokh Casas, C.; Agra-Bermejo, R.M.; Alvarez-Alvarez, B.; Grapsa, J.; Fontes-Carvalho, R.; Rigueiro Veloso, P.; Garcia Acuña, J.M.; Gonzalez-Juanatey, J.R. Myocardial infarction with non-obstructive coronary arteries: A comprehensive review and future research directions. World J Cardiol 2019, 11, 305–315. [Google Scholar] [CrossRef]
- Seferović, P.M.; Tsutsui, H.; Mcnamara, D.M.; Ristić, A.D.; Basso, C.; Bozkurt, B.; Cooper, L.T.; Filippatos, G.; Ide, T.; Inomata, T.; Klingel, K.; Linhart, A.; Lyon, A.R.; Mehra, M.R.; Polovina, M.; Milinković, I.; Nakamura, K.; Anker, S.D.; Veljić, I.; Ohtani, T.; Okumura, T.; Thum, T.; Tschöpe, C.; Rosano, G.; Coats, A.J.S.; Starling, R.C. Heart Failure Association, Heart Failure Society of America, and Japanese Heart Failure Society Position Statement on Endomyocardial Biopsy. J Card Fail. 2021, 27, 727–743. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; Huang, H.; Yang, B.; Huang, C. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 1–18. [Google Scholar] [CrossRef]
- Klem, I.; Shah, D.J.; White, R.D.; Pennell, D.J.; van Rossum, A.C.; Regenfus, M.; Sechtem, U.; Schvartzman, P.R.; Hunold, P.; Croisille, P.; Parker, M.; Judd, R.M.; Kim, R.J. Prognostic value of routine cardiac magnetic resonance assessment of left ventricular ejection fraction and myocardial damage: An international, multicenter study. Circ. Cardiovasc. Imaging 2011, 4, 610–619. [Google Scholar] [CrossRef]
- Broncano, J.; Bhalla, S.; Caro, P.; Hidalgo, A.; Vargas, D.; Williamson, E.; Gutiérrez, F.; Luna, A. Cardiac MRI in Patients with Acute Chest Pain. RadioGraphics 2021, 41, 8–31. [Google Scholar] [CrossRef]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; Atar, D.; Kaski, J.C.; Sechtem, U.; Tornvall, P. WG on Cardiovascular Pharmacotherapy. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 2017, 38, 143–153. [Google Scholar] [CrossRef]
- Haussner, W.; DeRosa, A.P.; Haussner, D.; Tran, J.; Torres-Lavoro, J.; Kamler, J.; Shah, K. COVID-19 associated myocarditis: a systematic review. Am J Emerg Med 2022, 51, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Castiello, T.; Georgiopoulos, G.; Finocchiaro, G.; Claudia, M.; Gianatti, A.; Delialis, D.; Aimo, A.; Prasad, S. COVID-19 and myocarditis: a systematic review and overview of current challenges. Heart Fail Rev. 2022, 27, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Duan, X.; Feng, G.; Sirajuddin, A.; Yin, G.; Zhuang, B.; He, J.; Xu, J.; Yang, W.; Wu, W.; Sun, X.; Zhao, S.; Wang, H.; Teng, Z.; Lu, M. Multiparametric Cardiovascular Magnetic Resonance in Acute Myocarditis: Comparison of 2009 and 2018 Lake Louise Criteria With Endomyocardial Biopsy Confirmation. Front Cardiovasc Med. 2021, 8, 739892. [Google Scholar] [CrossRef] [PubMed]
- Luetkens, J.A.; Faron, A.; Isaak, A.; Dabir, D.; Kuetting, D.; Feisst, A.; Schmeel, F.C.; Sprinkart, A.M.; Thomas, D. Comparison of original and 2018 Lake Louise criteria for diagnosis of acute myocarditis: results of a validation cohort. Radio Cardiothorac Imaging 2019, 1, e190010. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; Friedrich, M.G. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; Cheng, Z.; Yu, T.; Xia, J.; Wei, Y.; Wu, W.; Xie, X.; Yin, W.; Li, H.; Liu, M.; Xiao, Y.; Gao, H.; Guo, L.; Xie, J.; Wang, G.; Jiang, R.; Gao, Z.; Jin, Q.; Wang, J.; Cao, B. Clinical features of patients infected with 2019. novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Kravchenko, D.; Isaak, A.; Zimmer, S.; Mesropyan, N.; Reinert, M.; Faron, A.; Pieper, C.; Heine, A.; Velten, M.; Nattermann, J.; Kuetting, D.; Duerr, G.; Attenberger, U.; Luetkens, J. Cardiac MRI in Patients with Prolonged Cardiorespiratory Symptoms after Mild to Moderate COVID-19. Radiology 2021, 301, E419–E425. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; Vehreschild, M.; Nagel, E. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020, 5, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac involvement in patients recovered from COVID-2019 identified using magnetic resonance imaging. JACC Cardiovasc Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef]
- Wang, H.; Li, R.; Zhou, Z.; Jiang, H.; Yan, Z.; Tao, X.; Li, H.; Xu, L. Cardiac involvement in COVID-19 patients: mid-term follow up by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2021, 23, 14. [Google Scholar] [CrossRef]
- Kravchenko, D.; Isaak, A.; Zimmer, S.; Mesropyan, N.; Reinert, M.; Faron, A.; Pieper, C.C.; Heine, A.; Velten, M.; Nattermann, J.; Kuetting, D.; Duerr, G.D.; Attenberger, U.I.; Luetkens, J.A. Cardiac MRI in Patients with Prolonged Cardiorespiratory Symptoms after Mild to Moderate COVID-19. Radiology 2021, 301, E419–E425. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Habtemicael, Y.G.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Lanzillo, C.; Scatteia, A.; Di Roma, M.; Pontone, G.; Marra, M.P.; Barison, A.; Di Bella, G. Prognostic Value of Repeating Cardiac Magnetic Resonance in Patients With Acute Myocarditis. J Am Coll Cardiol. 2019, 74, 2439–2448. [Google Scholar] [CrossRef]
- Hijazi, Z.; Oldgren, J.; Andersson, U.; Connolly, S.J.; Ezekowitz, M.D.; Hohnloser, S.H. Cardiac biomarkers are associated with an increased risk of stroke and death in patients with atrial fibrillation: a Randomized Evaluation of Long-term Anticoagulation Therapy (RE-LY) substudy. Circulation. 2012, 125, 1605–1616. [Google Scholar] [CrossRef]
- Bulluck, H.; Dharmakumar, R.; Arai, A.E.; Berry, C.; Hausenloy, D.J. Cardiovascular Magnetic Resonance in Acute ST-Segment-Elevation Myocardial Infarction: Recent Advances, Controversies, and Future Directions. Circulation 2018, 137, 1949–1964. [Google Scholar] [CrossRef]
- Eitel, I.; de Waha, S.; Wohrle, J.; Fuernau, G.; Lurz, P.; Pauschinger, M.; Desch, S.; Schuler, G.; Thiele, H. Comprehensive prognosis assessment by CMR imaging after ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2014, 64, 1217–1226. [Google Scholar] [CrossRef]
- Reindl, M.; Reinstadler, S.J.; Tiller, C.; Kofler, M.; Theurl, M.; Klier, N.; Fleischmann, K.; Mayr, A.; Henninger, B.; Klug, G.; Metzler, B. ACEF score adapted to ST-elevation myocardial infarction patients: The ACEF-STEMI score. Int. J. Cardiol. 2018, 264, 18–24. [Google Scholar] [CrossRef]
- Sangita, S.; Eric, N.; Karl, H.; Scott, M.G.; Geltman, E.M. Use of Biomarkers to Predict Readmission for Congestive Heart Failure. Am. J. Cardiol. 2017, 119, 445–451. [Google Scholar] [CrossRef]
- Costabel, J.P.; Burgos, L.M.; Trivi, M. The Significance Of Troponin Elevation In Atrial Fibrillation. J Atr Fibrillation. 2017, 9, 1530. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; Di Roma, M.; Pontone, G.; Perazzolo, M.M.; Barison, A.; Di Bella, G. Cardiac MR with late gadolinium enhancement in acute myocarditis with preserved systolic function: ITAMY study. J Am Coll Cardiol 2017, 70, 1977–1987. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Wang, J.; Li, W.; Xu, Y.; Wan, K.; Zeng, R.; Chen, Y. The prognostic value of late gadolinium enhancement in myocarditis and clinically suspected myocarditis: systematic review and meta-analysis. Eur Radiol 2020, 30, 2616–2626. [Google Scholar] [CrossRef] [PubMed]
- Gräni, C.; Eichhorn, C.; Bière, L.; Murthy, V.L.; Agarwal, V.; Kaneko, K.; Cuddy, S.; Aghayev, A.; Steigner, M.; Blankstein, R.; Jerosch-Herold, M.; Kwong, R.Y. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017, 70, 1964–1976. [Google Scholar] [CrossRef] [PubMed]
- Cadour, F.; Cautela, J.; Rapacchi, S.; Varoquaux, A.; Habert, P.; Arnaud, F.; Jacquier, A.; Meilhac, A.; Paganelli, F.; Lalevée, N.; Scemama, U.; Thuny, F. Cardiac MRI Features and Prognostic Value in Immune Checkpoint Inhibitor-induced Myocarditis. Radiology. 2022, 303, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Friedrich, M.G.; Leiner, T.; Elias, M.D.; Ferreira, V.M.; Fenski, M.; Flamm, S.D.; Fogel, M.; Garg, R.; Halushka, M.K.; Hays, A.G.; Kawel-Boehm, N.; Kramer, C.M.; Nagel, E.; Ntusi, N.A.B.; Ostenfeld, E.; Pennell, D.J.; Raisi-Estabragh, Z.; Reeder, S.B.; Rochitte, C.E.; Starekova, J.; Suchá, D.; Tao, Q.; Schulz-Menger, J.; Bluemke, D.A.S.E.; Friedrich, M.G.; Leiner, T. Cardiovascular Magnetic Resonance for Patients With COVID-19. JACC Cardiovasc Imaging. 2022, 15, 685–699. [Google Scholar] [CrossRef] [PubMed]
- Sanguineti, F.; Garot, P.; Mana, M.; O'h-Ici, D.; Hovasse, T.; Unterseeh, T.; Louvard, Y.; Troussier, X.; Morice, M.C.; Garot, J. Cardio-vascular magnetic resonance predictors of clinical outcome in patients with suspected acute myocarditis. J Cardiovasc Magn Reson 2015, 17, 78. [Google Scholar] [CrossRef] [PubMed]
- Leite, W.F.; Dos Santos Povoa, R.M.; Caixeta, A.M.; Amodeo, C.; Szarf, G.; Bombig, M.T.N.; Izar, M.C.O.; Gioia, L.N.; Ribeiro, W.N.; Fonseca, F.A.H. Chest Pain in Acute Myocardial Infarction and Its Association With the Culprit Artery and Fibrotic Segment Identified by Cardiac Magnetic Resonance. Cardiol Res. 2023, 14, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Saleh, S.K.; Oraii, A.; Soleimani, A.; Hadadi, A.; Shajari, Z.; Montazeri, M.; Moradi, H.; Talebpour, M.; Naseri, A.S.; Balali, P.; Akhbari, M.; Ashraf, H. The association between cardiac injury and outcomes in hospitalized patients with COVID-19. Internal and Emergency Medicine 2020, 15, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
CMR of acute myocarditis demonstrated edema on (a) T2w fat suppression sequence – T2wFS, (b) T1 mapping, (c) T2 mapping and (d) Phase sensitive inversion recovery sequence (PSIR) – diffuse non ischemic mesomyocardial LGE.
Figure 1.
CMR of acute myocarditis demonstrated edema on (a) T2w fat suppression sequence – T2wFS, (b) T1 mapping, (c) T2 mapping and (d) Phase sensitive inversion recovery sequence (PSIR) – diffuse non ischemic mesomyocardial LGE.
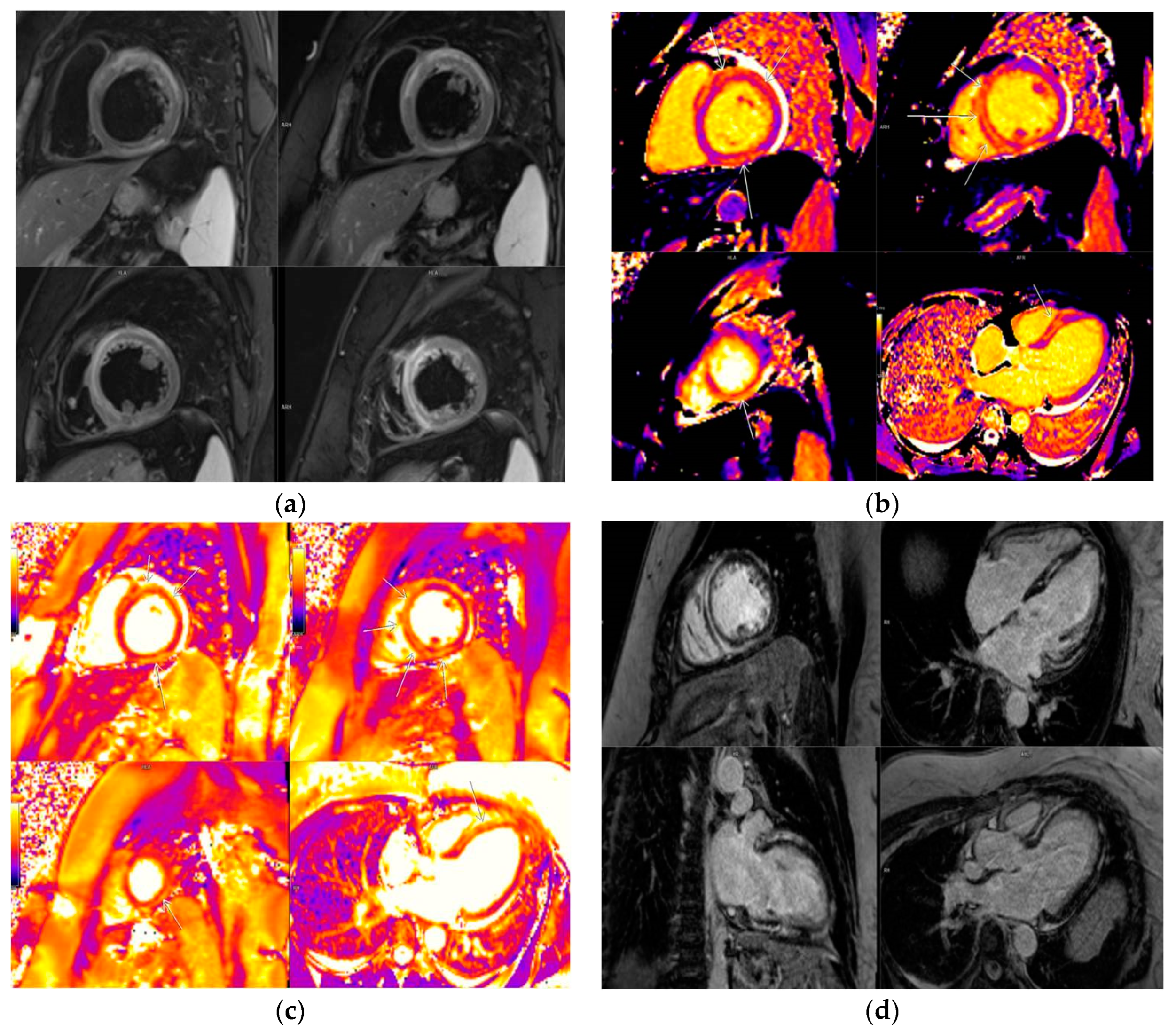
Figure 2.
CMR short axis view (SAX) - LGE in lateral wall basal and mid ventricle SAX with affection of pericardium.
Figure 2.
CMR short axis view (SAX) - LGE in lateral wall basal and mid ventricle SAX with affection of pericardium.
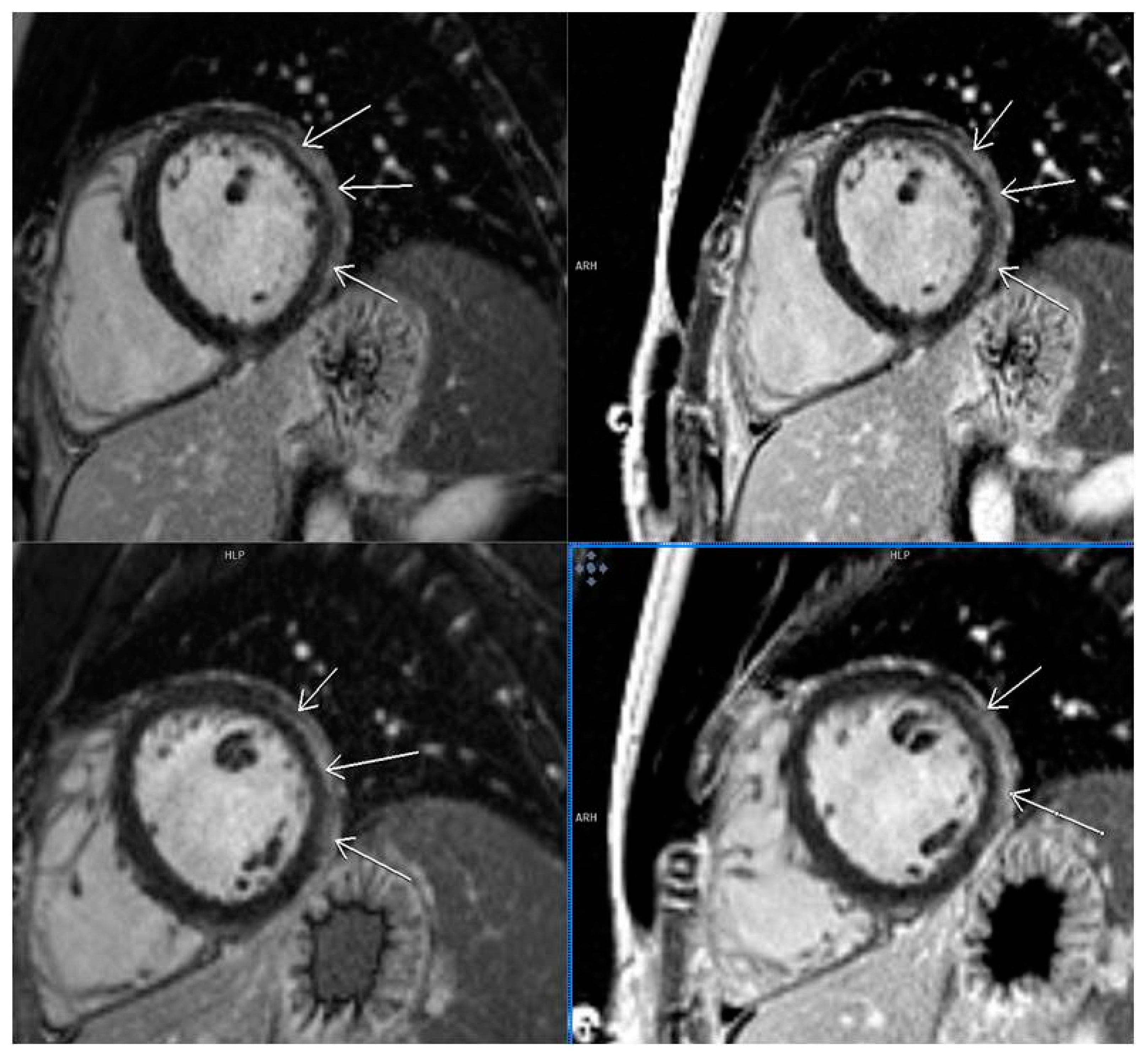
Figure 3.
CMR SAX - septal LGE on PSIR sequence.

Figure 4.
Phase sensitive inversion recovery sequence (PSIR) demonstrated subepicardial late gadolinium enhancement in lateral wall of left ventricle 4 chamber view (a) and mid SAX (b).
Figure 4.
Phase sensitive inversion recovery sequence (PSIR) demonstrated subepicardial late gadolinium enhancement in lateral wall of left ventricle 4 chamber view (a) and mid SAX (b).
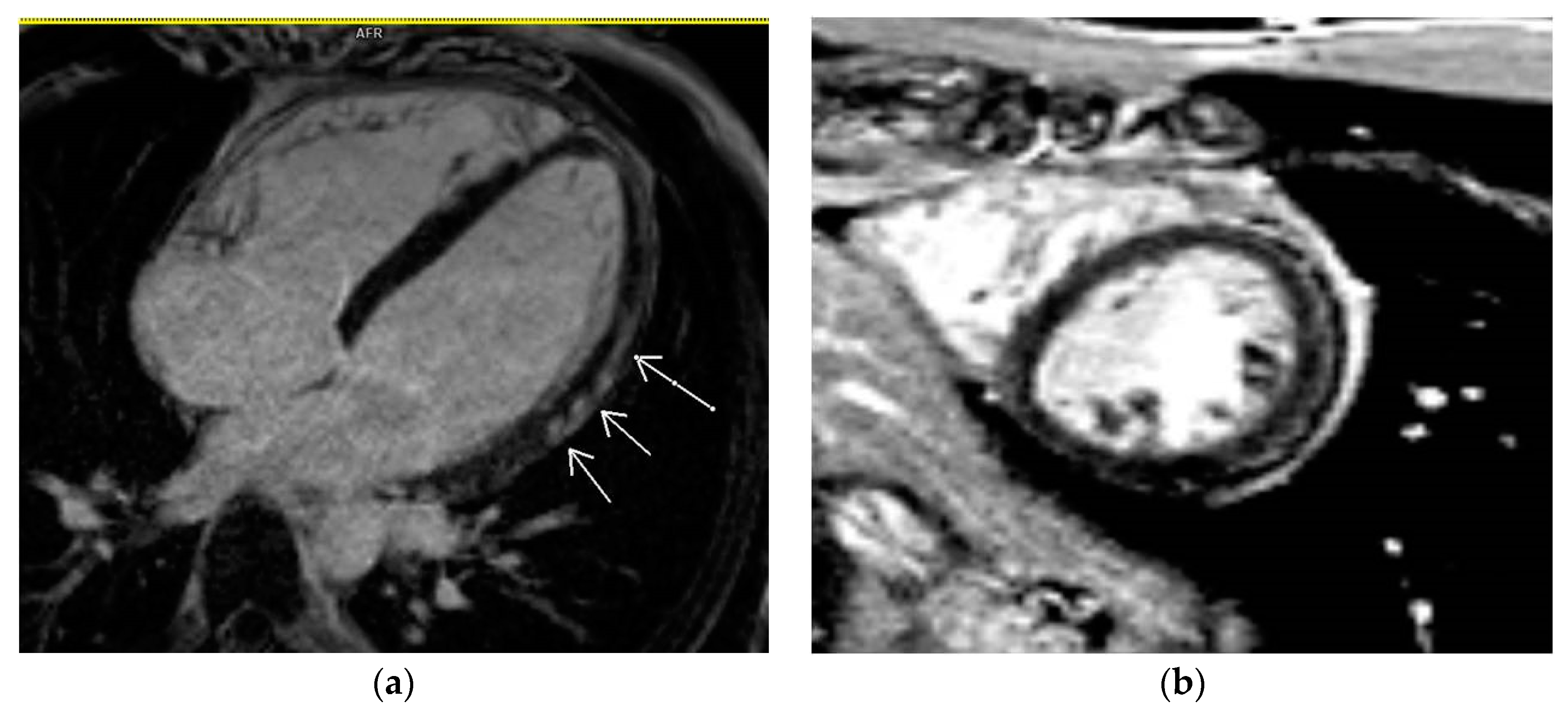
Figure 5.
Phase sensitive inversion recovery sequence (PSIR) demonstrated mesomyocardial late gadolinium enhancement in septum and inferior wall of left ventricle (insertion of septum and right ventricle).
Figure 5.
Phase sensitive inversion recovery sequence (PSIR) demonstrated mesomyocardial late gadolinium enhancement in septum and inferior wall of left ventricle (insertion of septum and right ventricle).
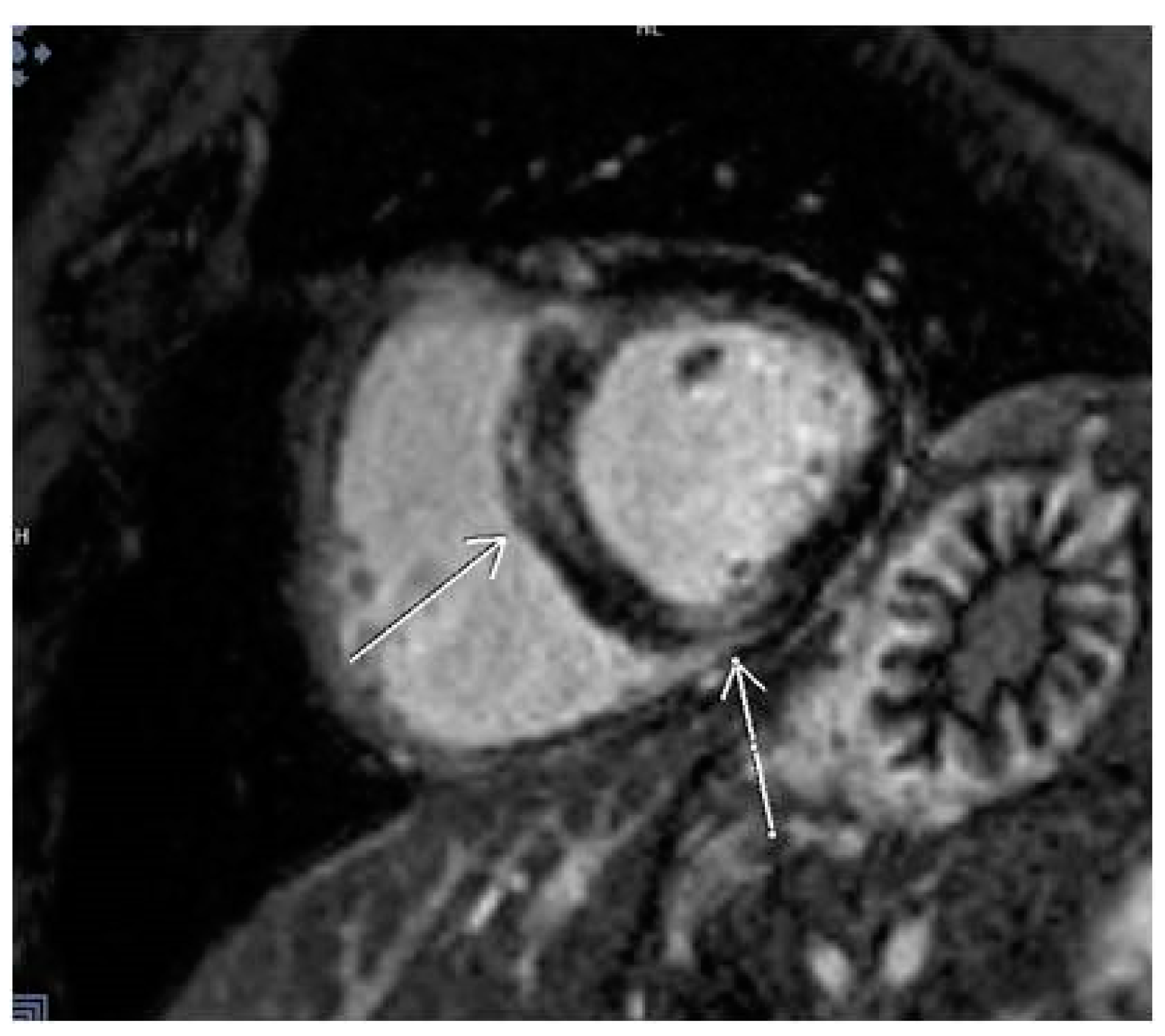

Table 1.
Demographic characteristics and clinical parameters of study population.
| Demographic characteristics | Result |
|---|---|
| Age | 46.76 ± 15.251 |
| Sex (male/female) | 68/71 (48.9%/51.1%) |
| Days from virus detection to CMR | 134.67±80.740 |
| Symptoms of COVID-19 | |
| Chest pain | 22 (15.8%) |
| Fatigue | 66 (47.5%) |
| Arrhythmias | 19 (13.7%) |
| Dyspnea | 40 (28.8%) |
| Lost of taste and smell | 24 (17.3%) |
| Digestive symptoms | 31 (22.3%) |
| Headache | 36 (25.9%) |
| Pneumonia | 66 (46.5%) |
| Co-morbidities | |
| Dyslipidemia | 6 (4.3%) |
| Hypertension | 24 (17.3%) |
| Diabetes mellitus type II | 10 (7.2%) |
| Smoking | 10 (7.2%) |
| Former smokers | 6 (4.3%) |
| Symptoms after COVID-19 | |
| Chest pain | 48 (34.5%) |
| Fatigue | 82 (58.9%) |
| Arrhythmias | 54 (38.8%) |
| Dyspnoea | 58 (41.7%) |
| ECG changes after COVID-19 | |
| Ischaemic changes | 18 (12.9%) |
| Arrhythmias | 14 (10.1%) |
| Right heart overload | 14 (10.1%) |
| CMR parameters | |
| LVEF | 62.37% ± 4.88 % |
| Patients with LGE | 54 (38.8%) |
| Patients without LGE | 85 (61.2%) |
| Localization of LGE | |
| Lateral | 11 (7.9%) |
| Septal | 9 (6.5%) |
| Multiple segments (more than 3) | 13 (9.4%) |
| Other localizations | 21 (15.1%) |
| Abbreviations: CMR: cardiac magnetic resonance, LVEF: left ventricular ejection fraction, LGE: late gadolinium enhancement. | |
Table 2.
Predictors for late gadolinium enhancement.
| Laboratory parameters | LGE negative patients (mean; SD) | LGE positive patients (mean; SD) | p values | Test values | Independent predictors for LGE |
|---|---|---|---|---|---|
| Troponin values | 4.9±0.3 ng/L | 13.1±0.4 ng/L | p<0.001 | Z=-9.5 | Yes |
| D-dimer levels | 0.8±0.1 mg/L FEU | 1.8±0.3 mg/L FEU | p=0.005 | Z -3,9 | No |
| Fibrinogen levels | 3.2±0.1 g/L | 4.3±0.23 g/L | p<0.001 | t=-4 | No |
| CK values | 143.9±12.4 u/L | 112.8±6.9 u/L | p=0.042 | Z=-1.6 | No |
| Clinical symptoms | |||||
| Chest pain | 43.7% | 56.3% | p=0.002 | Chi2 9.3 | Yes |
| Fatique | 39% | 61% | p<0.001 | Chi241.2 | Yes |
| Dyspnea | 67.2% | 32.8% | p=0.213 | Chi2 1.5 | No |
| CMR findings | |||||
| T1 mapping values | 1063.5±9.7 ms | 1103.9±17.2 ms | p=0.033 | t=-2.2 | Yes |
| Abbreviations: SD: standard deviation, LGE: late gadolinium enhancement, CMR: cardiac magnetic resonance, CK: creatine kinase. | |||||
Table 3.
Predictors for arrhythmias.
| Laboratory parameters | Patients with arrhythmias | Patients without arrhythmias | P values | Test values | Arrhythmias predictor |
|---|---|---|---|---|---|
| Troponin values | 10.4±0.8 ng/L | 7.4±0.5 ng/L | p<0.001 | Z=-3.3 | Yes |
| CMR findings | |||||
| Septal fibrosis | 32% | 3.4% | p=0.005 | Chi2 7.9 | Yes |
| T1 mapping | 1100.8±21.4ms | 1071.6±9.5ms | p=0.362 | Z=-0.912 | No |
| Abbreviations: CMR: cardiac magnetic resonance | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



