
Submitted:
30 January 2024
Posted:
31 January 2024
You are already at the latest version
Abstract
Background: Takayasu’s arteritis is a rare type of vasculitis, with severe complications like stroke, ischemic heart disease, pulmonary hypertension, secondary hypertension, aneurysms. Diagnosis is conducted by clinical and angiographic criteria. Treatment is medical and surgical, but unfortunately, the outcome is reserved. Case presentation: A 34- year- old Caucasian women had an ischemic stroke (2009). She was diagnosed with Takayasu’s arteritis and she received treatment with methotrexate, prednisolone, antiplatelet agents, with a mild improvement of clinical state. After 5 years (2014) she associated ascending aorta aneurysm, pulmonary hypertension, mild aortic regurgitation. The surgical treatment solved both ascending aorta aneurysm and left carotid artery stenosis (ultrasound in 2009 and computed tomography angiogram in 2014). Morphopathology revealed typical appearance for Takayasu’s arteritis. Tumor necrosis factor inhibitors (TNF-inhibitors) were associated to methotrexate. At 48 years (2023) she developed coronary heart disease (angina, electrocardiogram); echocardiography revealed severe pulmonary hypertension; angiography described normal coronary arteries, abdominal aorta pseudoaneurysm and arterial-venous fistula, with origin in right coronary artery and drainage on medium pulmonary artery. The patient refused surgical/ interventional treatment; she received again TNF- inhibitors, methotrexate, antiplatelet agents, statins. Conclusions: This case report presents us a severe form of Takayasu’s arteritis. We consider that morphopathology had a great importance in revealing to clinicians the typical appearance and the stadialization of inflammatory arterial process: acute or chronic. The verdict of morphopathologist was chronic phase, with acute relapses, so we decided that immunosuppressive treatment was still necessary.
Keywords:
Takayasu’s arteritis
; angiography
; clinical criteria
; morphopatology
1. Introduction
Takayasu’s arteritis is a specific vasculitis, diagnosed and treated by teams, composed by rheumathologist, imaging specialist, cardiologist, interventional cardiologist, cardiac surgeon, pathologist. The disease affects large arteries, leading in advanced stages to stenosis, aneurysmal dilation, occlusion [1]. The first case was presented in 1908, by Mikito Takayasu, at The Annual Meeting of the Japan Ophtalmology Society; he noticed arteriovenous anastomosis around the papilla at a 21-year-old woman [2]. Mikito Takayasu didn’t precise any other medical involvement at his patient, but his name was kept for this disease. At the same congress, another two ophthalmologists presented patients with similar changes of retinal vessels, but they also noticed the absence of radial artery pulsation- Katsutomo Onishi and Tsurukichi Kagoshima [3]. In 1921, Minoru Nakajima proposed four criteria for the diagnosis - three of them were related to ophthalmology and one was addressed to radial artery pulseless [4]. Since then, clinicians published about this disease: Shimizu 1951 [5], Kojima 1961 [6], Hirose 1962 [7], Hidano 1981 [8], are only a part of them in the history of Takayasu’s arteritis. American College of Rheumatology (ACR) published 6 diagnosis criteria, for Takayasu’s arteritis (1990) , as the following: onset before 40 years; superior limbs claudication; diminished pulsation on brachial artery; at least 10 mmHg difference in systolic blood pressure, between right and left arm; bruit over abdominal aorta/subclavian arteries; narrowing or occlusion of aorta or main branches at angiography. At least 3 of 6 criteria were a certain diagnosis of this disease [9]. In 2022 , the same ACR, updated these criteria, as the following (after diagnosis of medium-vessel and/or large-vessel arteritis was made ; after other vasculitis were excluded; age ≤ 60 years): female sex (+1); limb claudication (+2); angina pectoris (+2); arterial bruit (+2); diminished pulsation of superior limb arteries (+2); diminished pulsation of carotid artery (+2); difference ≥ 20mmHg, between right and left arm(+1); number of arterial territories involved (+1to +3); paired artery affected (+1); abdominal aorta plus renal/mesenteric arteries affected (+3). A total score ≥ 5 means a certain diagnosis of the disease [10]. Nowadays, clinicians can use vascular imaging provided not only by classical angiography, but also by computed tomography, magnetic resonance imaging, positron emission tomography. Fluorodeoxyglucosepositron emission tomography (FDG-PET) measures vascular inflammation and calculates integrated disease activity index [11]. Morphopathology plays a major role if the patient receives surgical treatment; fragments from arteries can reveal the involvement of all layers: adventitia inflammation, destruction of media elastic tissue, neovascularization of intima and media [12]. Triggers for this autoimmune disorder can be tuberculosis, with different locations [13]. Differential diagnosis is made with arteritis from syphilis, systemic erythematous lupus, rheumatoid arthritis and Marfan syndrome [14]. Treatment is medical and/or interventional, surgical. Steroids and/or methotrexate are preferred as immunosuppressive therapy [15,16]. Tumor necrosis factor (TNF) inhibitors are modern medications [17]. Surgical therapy is addressed for aneurysms, aortic regurgitation, arterial stenosis (when interventional angioplasty and stenting aren’t appropriate; interventional methods can usually solve arterial stenosis). Prognosis is uncertain, with relapses and possible complications, like stroke, aortic dissection/rupture, myocardial infarction, severe pulmonary hypertension, side effects of immunosuppresive therapy-cancers, infections [18].
2. Case Presentation
A 48-year-old woman (2023), Caucasian, is referred to the cardiologist, due to increased, prolonged crises of angina pectoris, during the last 2 months. Her past medical history began in 2009, when she was 34-year-old, with an acute onset: sudden right hemiparesis, associated with fever, weight loss - 5 kg in 1 month, malaise and increased acute phase reactants levels. She was diagnosed and treated for pulmonary tuberculosis, one year before stroke. She was hospitalized on Neurology department and clinical exam revealed a blood pressure difference of 30 mmHg, between right and left arm (1 point according to ACR 2022 criteria for Takayasu arteritis), left carotid artery bruit (2 points), diminished pulsation of superior limb arteries (2 points), so a total score 7. The suspicion of Takayasu arteritis (an ACR score ≥ 5) was confirmed by rheumatologist. She received Prednisolone 50 mg/day (1mg/kg), Methotrexate 20 mg/day, Aspirin 100 mg/day; general symptoms vanished, neurological recovery was almost complete, after 3 months and acute phase reactants levels normalized, after 1 month. Doppler ultrasound of cervical arteries revealed a critical stenosis (75%) on left carotid artery, but the patient refused interventional/surgical therapy. The maintenance treatment, after discharge, consisted by Prednisolone 20 mg/day, Methotrexate 5 mg/day, Aspirin 100 mg/day, lifestyle changes (work, stress, nutrition). After 5 years, in 2014, when she was 39-year-old, she was hospitalized on Cardiology department, with malaise, sweating, dispneea on minor efforts, palpitations. Echocardiography precised moderate pulmonary hypertension. Computed tomography angiography confirmed critical stenosis of left carotid artery - 85% (already discovered, 5 years ago, by Doppler ultrasound) and the occurance of ascending aorta aneurysm; both problems were solved by cardiovascular surgery. Anatomical fragments from aorta and carotid artery had typical modifications for Takayasu’s arteritis -Figure 1 (EVG=Elastic Van Gieson discoloration) and Figure 2.
Tumor necrosis factor inhibitors, Infliximab 150mg, intravenously (initially, then after 2 weeks, after 6 weeks, then every 8 weeks) were associated to methotrexate, for 2 years. Her evolution was improved, until 2023, when she noticed severe and prolonged crisis of angina pectoris. Electrocardiogram revealed ST segment depression in DI, avL and V2-V6, with giant negative T waves - Figure 3.
Blood tests were recommended in emergency, due to clinical description of severe angina pectoris and profonde alterations of electrocardiogram, which could suggest a possible non-STEMI. Table 1 reflects normal values for biomarkers (ASAT and ALAT < 40 IU/L; CPK= 30-135 IU/L in females; Troponin T and I < 14ng/L); therefore, an acute myocardial infarction was excluded.
The cardiologist prescribed betablockers - Nebivolol 5 mg/day, antiplatelet agents - Aspirin 100 mg/day, statins - Atorvastatine 20 mg/day, angiotensine converting enzyme inhibitors - Perindopril 5 mg/day. Angina was diminished, as well as electrocardiographic alterations. Transthoracic echocardiography revealed signs of severe pulmonary hypertension: a pressure half time for pulmonary regurgitation, PHT= 124msec, Figure 4 (ranges ≤ 150 msec means severe pulmonary hypertension) and a systolic pulmonary artery pressure = 62 mmHg, Figure 5 (ranges ≥ 55 mmHg means severe pulmonary hypertension).
A coronarography was recommended and large coronary arteries were permeable, without significant lesions-Figure 6. Angina and electrocardiographic alterations were explained by microvascular lesions (female, hipercolesterolemia) and coronary steal mechanism, described in Takayasu’s arteritis.
Angiography revealed an abdominal aorta pseudoaneurysm - Figure 7 and an arterial-venous fistula, with origin on righ coronary artery and drainage on medium pulmonary artery-Figure 8.
Conservatory treatment was decided, with tumor necrosis factor inhibitors, Infliximab 150 mg every 8 weeks, intravenously, Methotrexate 20mg, weekly, antiplatelet agents, statins (the patient refused a new operation).
3. Discussions
Our case report had the first manifestation of arterial involvement a stroke, due to left carotid artery (major branch of aorta) stenosis. Tombeti and Mason ascertained that inflammation in Takayasu’s arteritis can be noticed in principal branches of the aorta [19]. General symptoms (fever, malaise, weight lose) associated to the stroke raised the clinical suspicion of vasculitis. Adventitia is the first site of injury [20] and inflammation of its vasa vasorum leads to fibrosis. Media is destroyed by infiltration with immune cells and granulomas; the last layer involved by thickening is intima [21]. The differential diagnosis between stable and active Takayasu’s arteritis can be done by Interferon-γ ranges; when the disease is active this cytokine is increased [22]. Disease’s activity is referring to arterial inflammation, expressed through worsening symptoms and signs. Morphopathology can sustain this difference - active or stable disease and is possible when surgery is applied. In our case, the morphopathological aspects, like thickened intima and adventitia, suggested a stable disease; the other aspect, inflammatory infiltration of media, with monocytes, was typical for active disease. This is a peculiar aspect of our case, an interesting mixture between acute and chronic patterns, despite specific treatments. Parakh and Yadev described three phases in Takayasu’s arteritis: systemic features, arterial inflammation and stenosis [23]. Our patient revealed an onset with general symptoms (2009); the third stage (left carotid artery stenosis was diagnosed by Doppler ultrasound also in 2009) was concomitant with the first stage (general symptoms), in a female with ACR criteria for Takayasu’s arteritis. The second stage of the disease (arterial inflammation) had also expressed in 2009, by monocytes infiltration in media and adventitia. The simultaneous presence of all three stages is another peculiar aspect of our patient. A trigger factor for Takayasu’s arteritis is tuberculosis; many patients, diagnosed with this vasculitis, had also tuberculosis in their past medical history and this situation was revealed in our case, too. Arnaud et al. presumed that mycobacterial antigens had cross reactions in Takayasu’ s arteritis, even they didn’t discover Mycobacterium tuberculosis granulomas, inside vasculitis lesions [24].
Doppler ultrasound is an important technique for diagnosis only in carotid stenosis, because aorta, major branches and abdominal arteries have a difficult/impossible approach by echography [25]. The radiologist confirmed by Doppler ultrasound, left carotid artery stenosis in our patient. Gold standard imaging technique in this disease is computed tomography angiography; it can reveal thickened intima and active disease - an outside ring intima, which suggests adventitia and media inflammation [26]. We utilised computed tomography angiography in 2014, for the diagnosis of ascending aorta aneurysm and classical angiography in 2023, for the approach of coronary arteries and abdominal aorta. In our case, severe pulmonary hypertension, was explained by direct involvement of pulmonary arteries in Takayasu’s arteritis and also by fistula, which provided a left to right shunt (from right coronary artery to medium pulmonary artery). Angina pectoris had coronary steal mechanism, described in Takayasu’ s arteritis, as coronary arteries were permeable on angiography. Biotherapy is a modern approach in Takayasu’s arteritis; Farfer et al revealed a clinical improvement in 61% patients and 3 of 96 patients had the regression of inflammatory alterations on magnetic resonance imaging [27]. Our patient received conventional immunosupresive therapy at the beginning, but since 2014, tumor necrosis factor inhibitors, Infliximab, were associated to classical therapy. Despite this modern approach of the disease, the evolution was unfavorable, with complications already mentioned. For future months, we hope to convince the patient, to accept surgical treatment for abdominal aorta aneurysm and arterial-venous fistula.
4. Conclusions
The diagnosis of Takayasu’s arteritis was on advanced stage, in our case, with a neu-rogical complication - ischemic stroke. We constituted an interdisciplinary team, with permanent communication between cardiologist, radiologist, interventional cardiologist, cardiac surgeon, rheumatologist, morphopathologist. The diagnosis criteria were fulfilled from the first clinical presentation and permitted as an adequate approach with imagistic methods, modern medical and surgical therapy. The prognosis was unfavorable, as the patient had multiple lesions of arteries from coronary, carotid and pulmonary territories, abdominal and ascending aorta.
Author Contributions
All the authors had equal contributions. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and informed consent was given by the patient prior to publication.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Data are available upon request due to privacy restrictions.
Acknowledgments
The authors want to precise the technical support provided by Andreea Beatrice Manea, Software Engineer at Handshake Company, San Francisco, California, United States of America.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wen, D.; Du, X.; Ma, C.S. Takayasu’s arteritis: diagnosis, treatment and prognosis. Int Rev Immunol 2012, 31, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Takayasu, M. A case with peculiar changes of the retinal central vessels. Acta Soc Ophtal Jpn 1908, 12, 554–555. [Google Scholar]
- Numaro, F. Introductory remarks for special issue of Takayasu’ s arteritis. Heart Vess 1992, Suppl. 7, 3–5. [Google Scholar] [CrossRef]
- Chikashi, T. History of Takayasu’s arteritis and Dr. M.Takayasu. IntJ Rheum Dis 2014, 17, 931–935. [Google Scholar] [CrossRef]
- Shimizu, K.; Sano, K. Pulseless disease. J Neuropat Exp Neurol 1951, 1, 37–47. [Google Scholar]
- Kojima,K.; Shimizu, S.; Awaja, S.; Watanabe, I.; Niimi, K.; Yoshida, N. A case of pulseless disease associated with obstruction of the branch of the central retinal artery. Rinsho Ganka 1961, Dec 15, 1246–1249.
- Hirose, K. Entity of Takayasu-Ohnishi’ s syndrome (so called pulseless disease). Rinsho Ganka 1962, Apr16, 441–445. [Google Scholar]
- Hidano, A.; Watanabe, K. Pyoderma gangrenosum and cardiovasculopathies, particularly Takayasu’s arteritis. Review of the Japanese literature. Ann Dermatol Venereol 1981, 108, 13–21. [Google Scholar] [PubMed]
- Arend, W.P.; Michel, B.A.; Bloch, D.A.; Hunder, G.G.; Calabrese, L.H.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, W.R. et al. The ACR 1990 criteria for the classification of Takayasu’s arteritis. Arthritis Rheum 1990, 33, 1129-1134. [CrossRef]
- Grayson, P.C.; Ponte, C.; Suppiah, R.; Robson, C.J.; Gribbons, K.B.; Judge, A.; Craven, A.; Kalid, S.; Hutchings, A.; Danda, D.; Lukmani, R.A.; Watts, R.A.; Merkel, P.A.; DCVAS Study Group. 2022 ACR/EULAR classification criteria for Takayasu’s arteritis. Ann Rheum Dis 2022, 81, 1654-1660. [CrossRef]
- Marvisi, C.; Bolek, E.C.; Alman, M.A.; Alessi, H.; Redmond, C.; Muratore, F.; Galli, E.; Ricordi, C.; Kaymaz-Tahra, S.; Ozguven, S.; Alibaz-Oner, F.; Direskeneli, H.; Salvarani, C.; Quinn, K.A.; Grayson, P.C. Development of the Takayasu’s arteritis integrated disease activity index. Arthritis Care Res, 2023, Dec 7. [CrossRef]
- Inder, S.J.; Bobryshev, Y.V.; Cherian, M.S.; Wang, A.Y.; Lord, R. S.; Masuda, K.; Yutani, C. Immunophenothypic analysis of the aortic wall in Takayasu’s arteritis: involvement of lymphocytes, dendritic cells and granulocytes in immunoinflammatory reaction. Cardiovasc Surg, 2000, 8, 141-148. [CrossRef]
- Zhang, Y.; Fan, P.; Luo, F.; Zhang, H.M.; Son, L.; Ma, W.J.; Wu, H.Y.; Cai, J.; Wang, L.P.; Zhou, X.L. Tuberculosis in Takayasu’s arteritis: a retrospective study in 1105 Chinese patients.J Geriatr Cardiol, 2019, 16, 648-655. [CrossRef]
- Moriwaki, R.; Noda, M.; Yajima, M.; Sharma, B.K.; Numano, F. Clinical manifestations of Takayasu’s arteritis in India and Japan-new classification of angiographic findings. Angiol 1997, 48, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Kerr, G.S..; Hollahan, C.W.; Giordano, J.; Leavitt, R.Y.; Fauci, A.S.; Rottem, M.; Hofmann, G.S. Takayasu’s arteritis. Ann Intern Med, 1994, 120, 919-929. [CrossRef]
- Johnston, S.L.; Lock, R.Y..; Gompels, M.M. Takayasu’s arteritis: a review. .J Clin Pathol 2002, 55, 481–486. [CrossRef]
- Schmidt, J.; Kermani, T.; Bacani, A.K.; Crowson, C.S.; Matteson, E.L.; Warrington, K.J. Tumor necrosis factor inhibitors in patients with Takayasu’s arteritis: experience from a referral center with long- term follow up. Arthritis Care Res, 2012, 64, 1079-1083. [CrossRef]
- Comarmond, C.; Biard, L.; Lambert, M.; Mekinian, A.; Ferfar, Y.; Kahn, J.E.; Benhamou, Y; Chiche, L.; Koskas, K.; Cluzel, P.; Hachulla, E.; Messas, E.; Resche-Rigon, M.; Cacoub, P.; Miraud, T.; Saadoun, D.; French Takayasu Network. Long-term outcomes and prognostic factors of complications Takayasu’s arteritis. Circ 2017, 136, 1114-1122. [CrossRef]
- Tombetti, E.; Mason, J.C. Takayasu arteritis: advanced understanding is leading to new horizons. Rheumatol Oxf Engl, 2019, 58, 206–219. [Google Scholar] [CrossRef]
- Arnaud, L.; Haroche, J.; Mathian, A.; Gorochov, G.; Amoura, Z. Pathogenesis of Takayasu’s arteritis: a 2011 update. Autoimmun Rev, 2011, 11, 61–67. [Google Scholar] [CrossRef]
- Yoshifuji, H. Pathophysiology of large vessel vasculitis and utility of interleukin-6 inhibition therapy. Mod Rheumatol, 2019, 29, 287–293. [Google Scholar] [CrossRef]
- Goel, R.; Kabeerdoss, J.; Ram, B.; Prakash, J.A.J.; Babji, S.; Nair, A.; Jeyaseelan, V.; Matthew, J.; Balaji, V.; Joseph, G.; Danda,D. Serum cytokine profile in Asian Indian patients with Takayasu arteritis and its association with disease activity. Open Rheumatol J, 2017, 11, 23–29. [CrossRef] [PubMed]
- Parakh, R.; Yadav, A. Takayasu’s arteritis: an Indian perspective. Eur J Vasc Endovasc Surg, 2007, 33, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, L.; Cambau, E.; Brocheriou, I.; Koskas, F.; Kieffer, E.; Piette, J.C.; Amoura, Z. Absence of mycobacterium tuberculosis in arterial lesions from patients with Takayasu’s arteritis. J Rheumatol, 2009, 36, 1682–1685. [Google Scholar] [CrossRef] [PubMed]
- Chaubal, N.; Dighe, M.; Shah, M. Sonographic and color doppler findings in Aortoarteritis (Takayasu Arteritis). J Ultrasound Med, 2004, 23, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, N.; Hayashi, K.; Sakamoto, I.; Ogawa, Y.; Matsumoto, T. Takayasu arteritis: protean radiologic manifestations and diagnosis. RadioGraphics 1997, 17, 579–594. [Google Scholar] [CrossRef] [PubMed]
- Ferfar, Y.; Mirault, T.; Desbois, A.C.; Comarmond, C.; Messas, E.; Savey, L.; Domot, F.; Cacoub, P.; Saadoun, D. Biotherapies in large vessel vasculitis. Autoimmun Rev, 2016, 15, 544–551. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Morphopathological exam - Thickened intima, with fibrosis; alteration of elastic structure of media; thickened adventitia (EVG, x10).
Figure 1.
Morphopathological exam - Thickened intima, with fibrosis; alteration of elastic structure of media; thickened adventitia (EVG, x10).
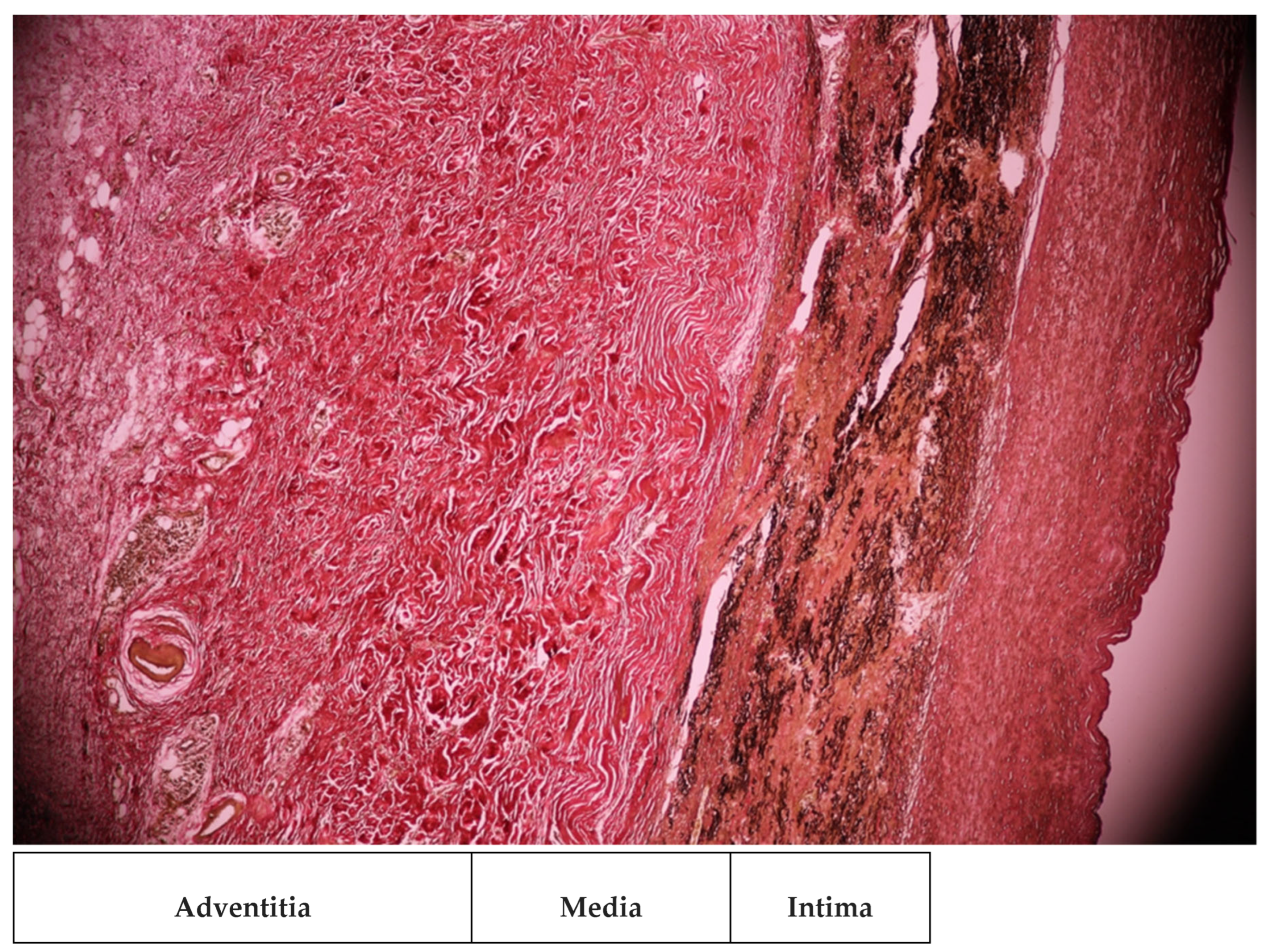
Figure 2.
Morphopatological exam - Inflammatory infiltration with monocytes in media and adventitia (EVG, X200).
Figure 2.
Morphopatological exam - Inflammatory infiltration with monocytes in media and adventitia (EVG, X200).
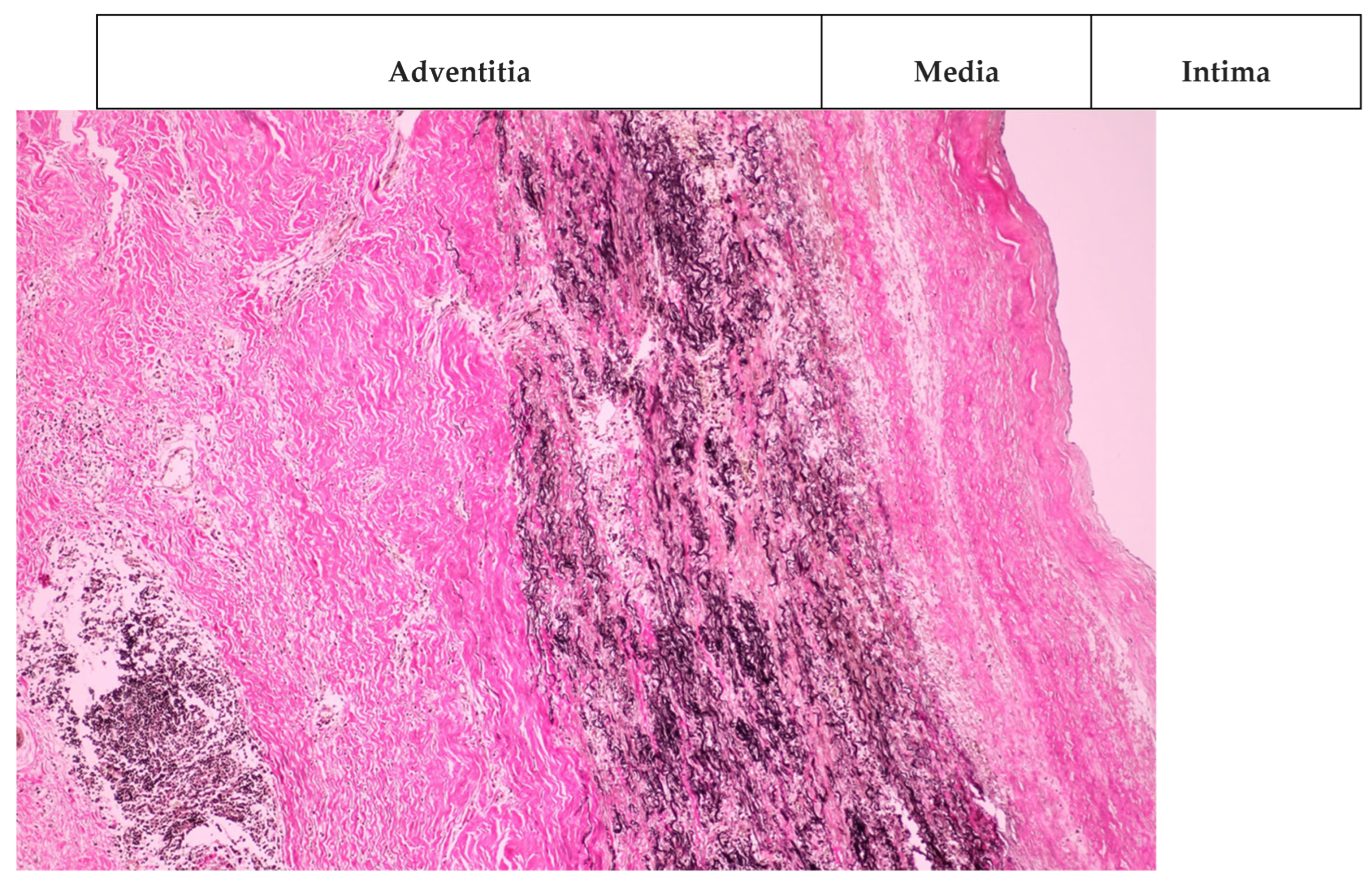
Figure 3.
Electrocardiogram.
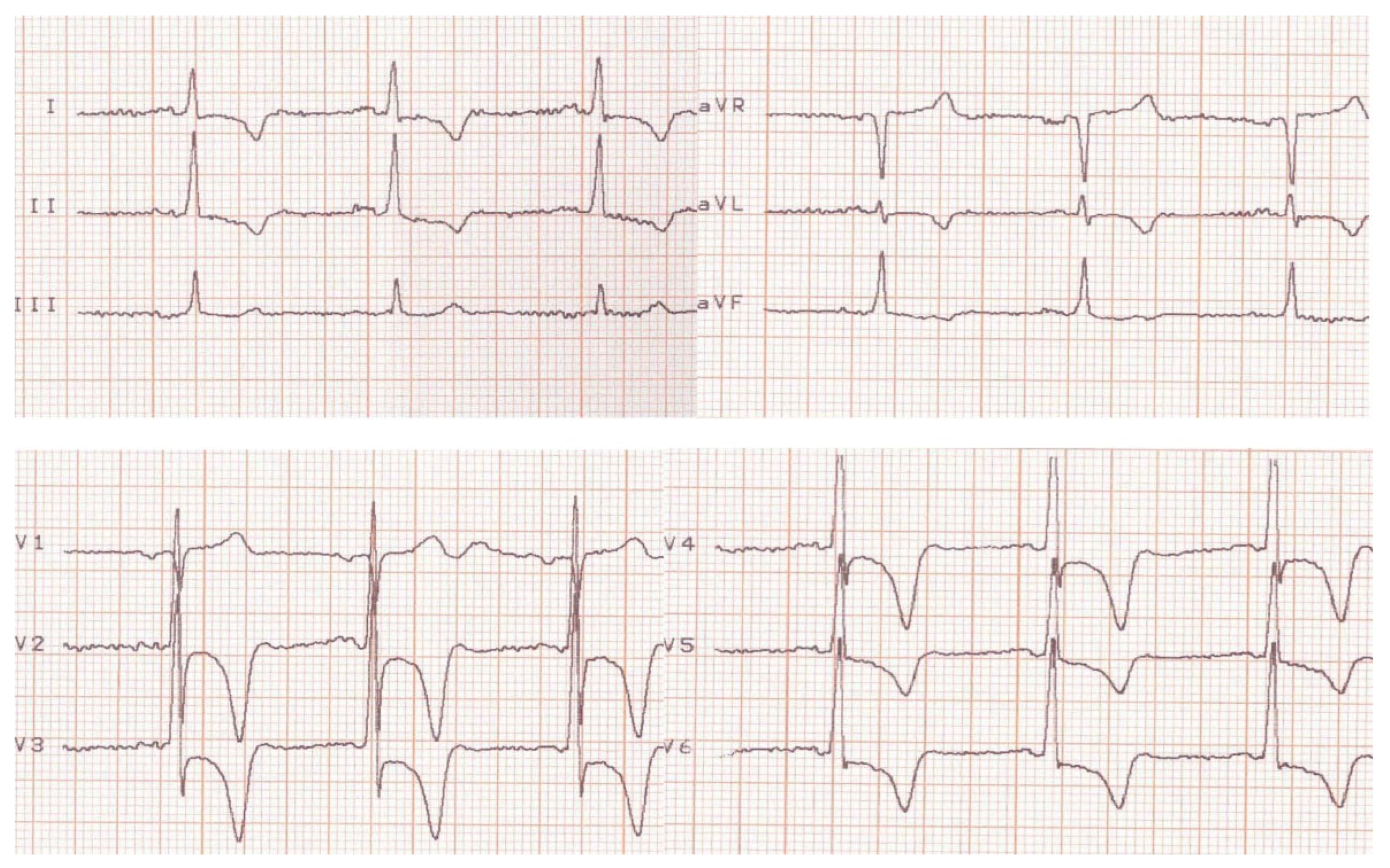
Figure 4.
Echocardiogram – PHT = 124msec for pulmonary regurgitation.
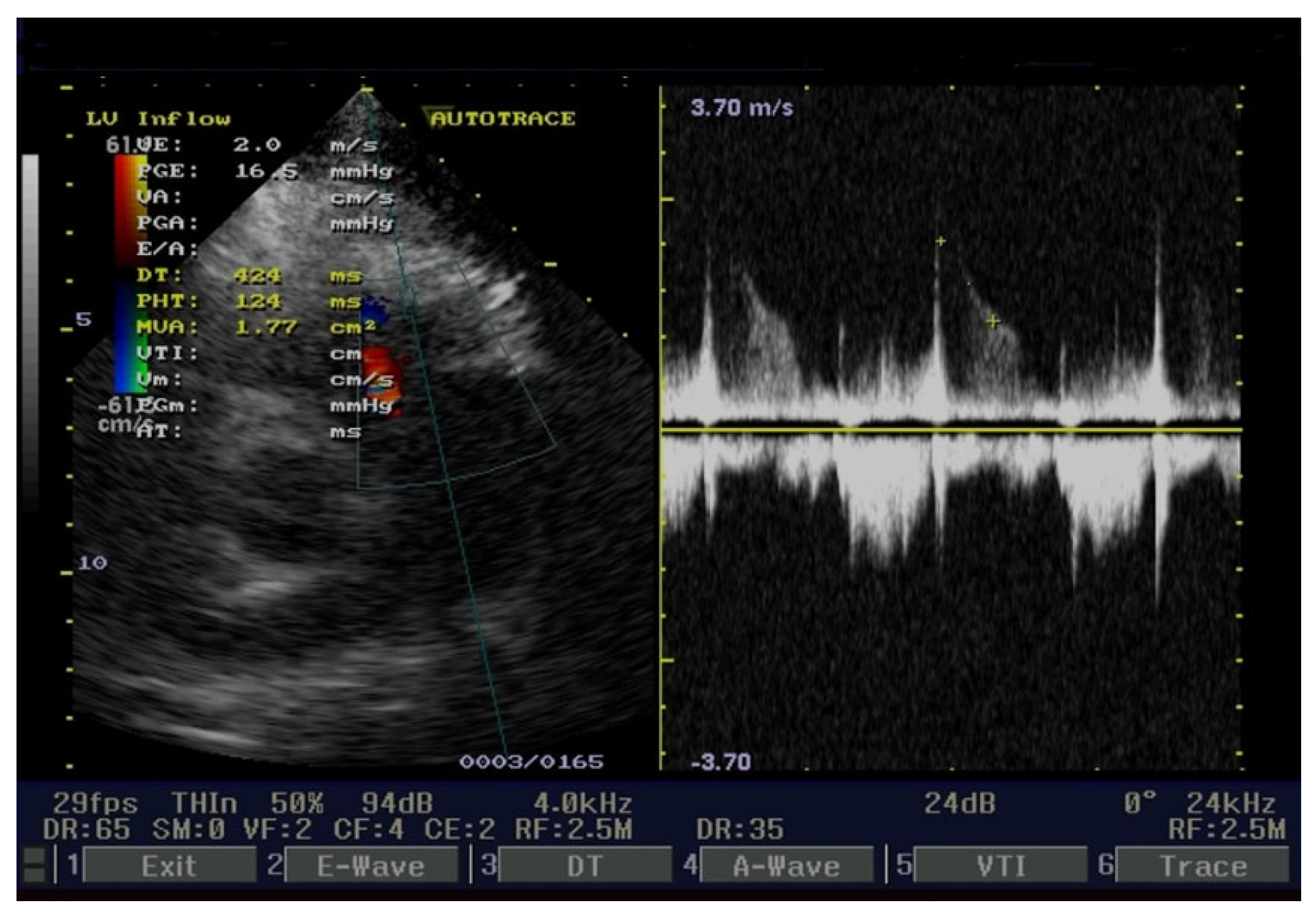
Figure 5.
Echocardiogram -systolic artery pulmonary pressure = 62 mmHg.
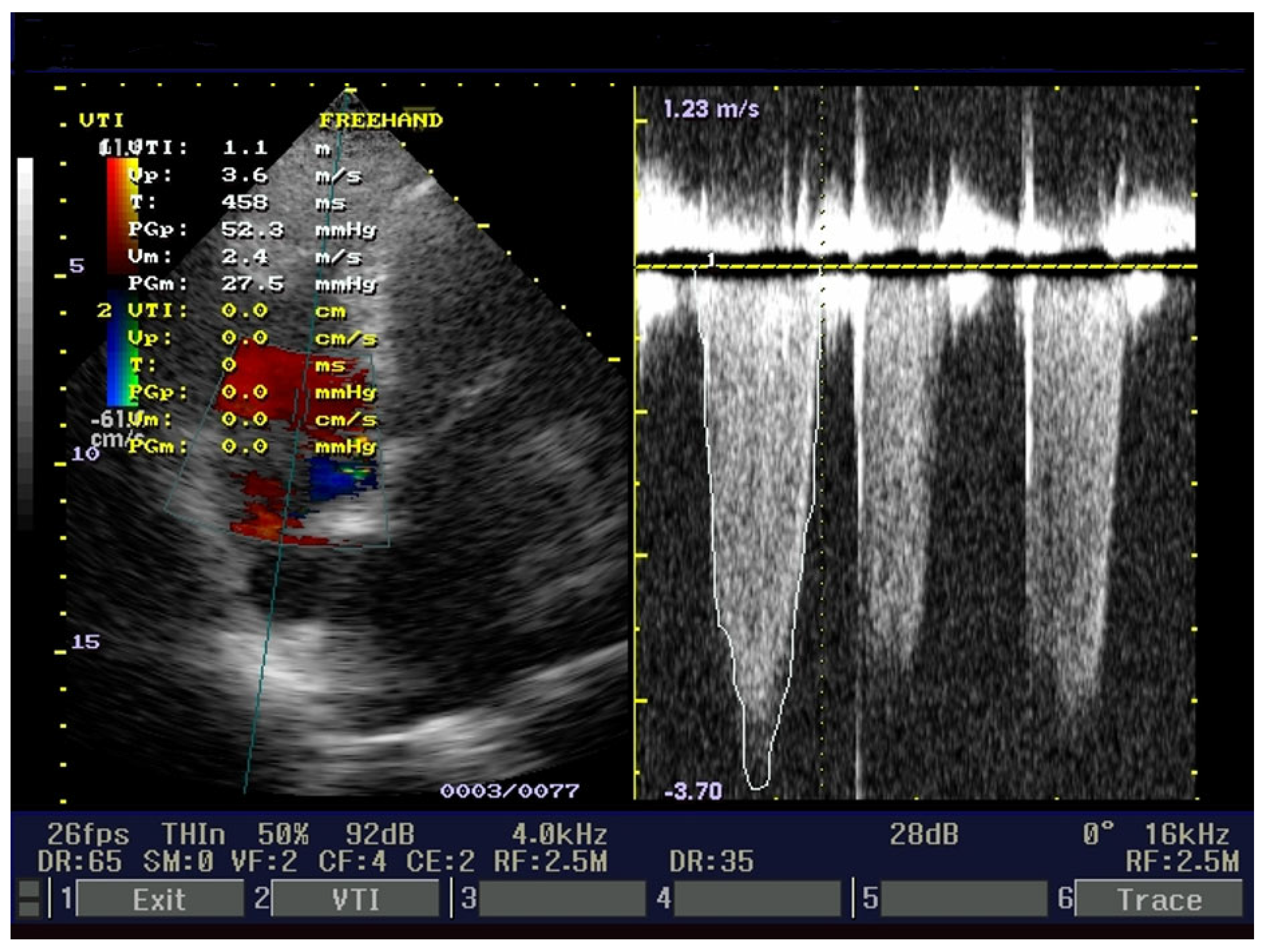
Figure 6.
Coronarography - permeable large arteries.
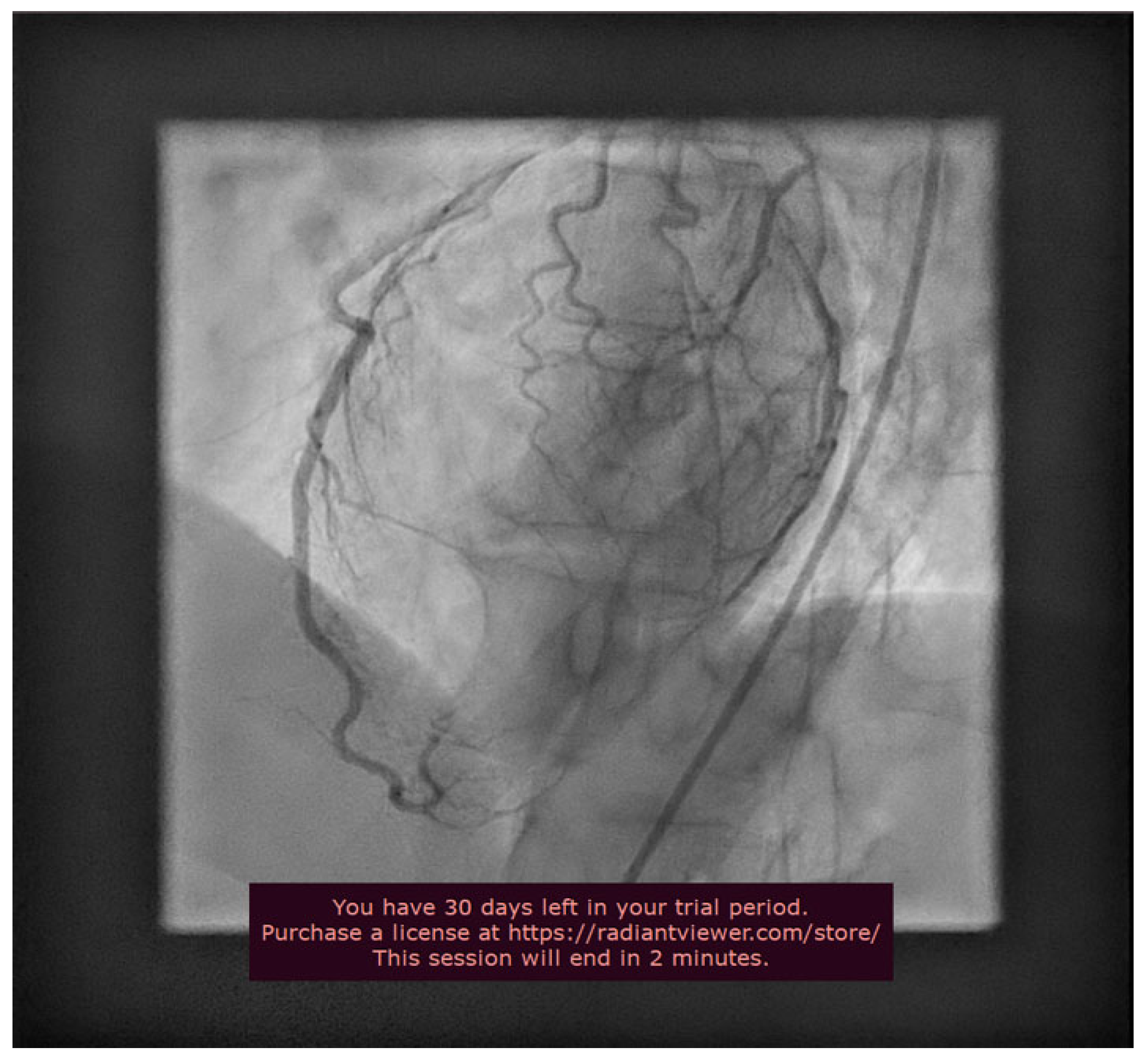
Figure 7.
Aortography - Abdominal aoarta pseudoaneurysm.
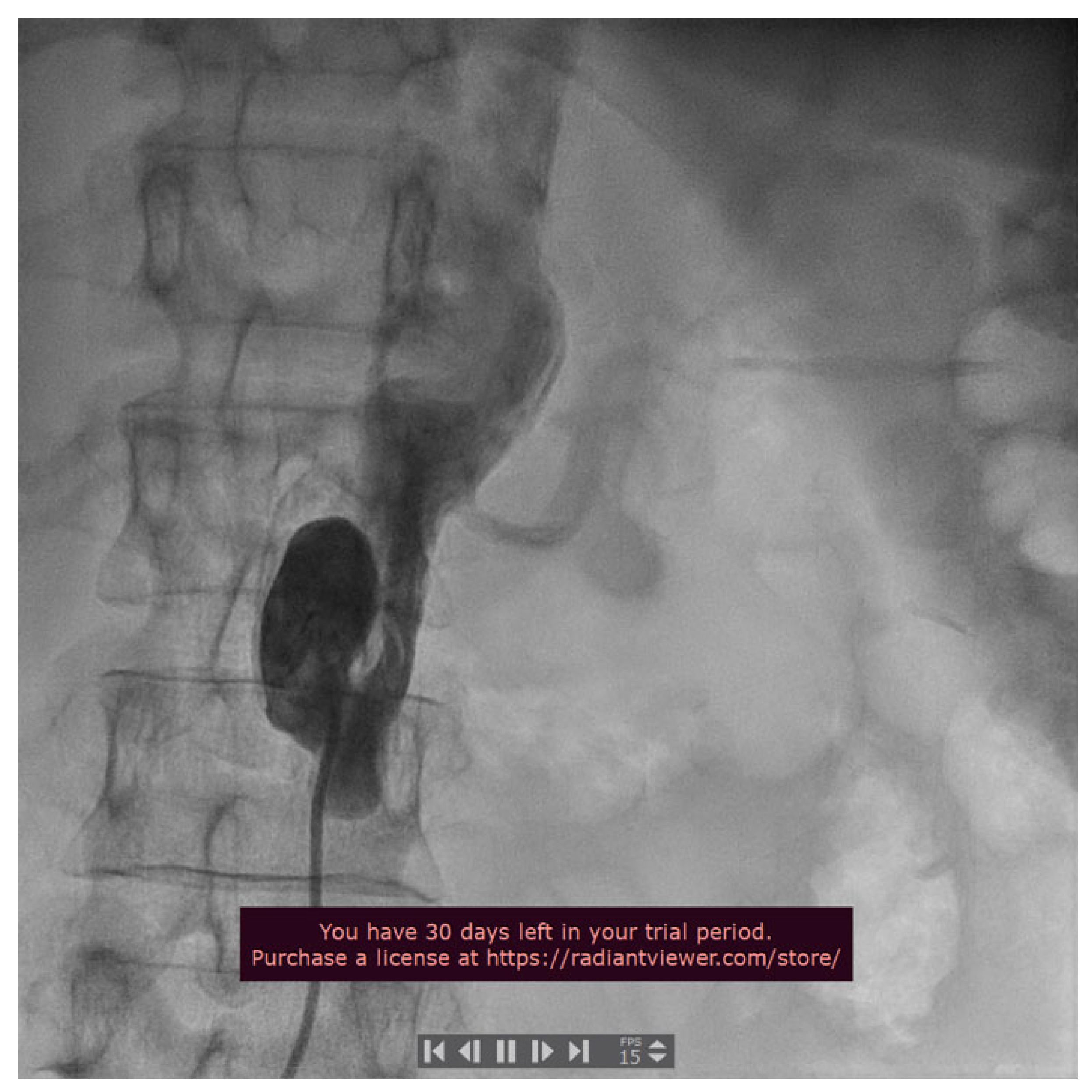
Figure 8.
Angiography -Arterial-venous fistula.
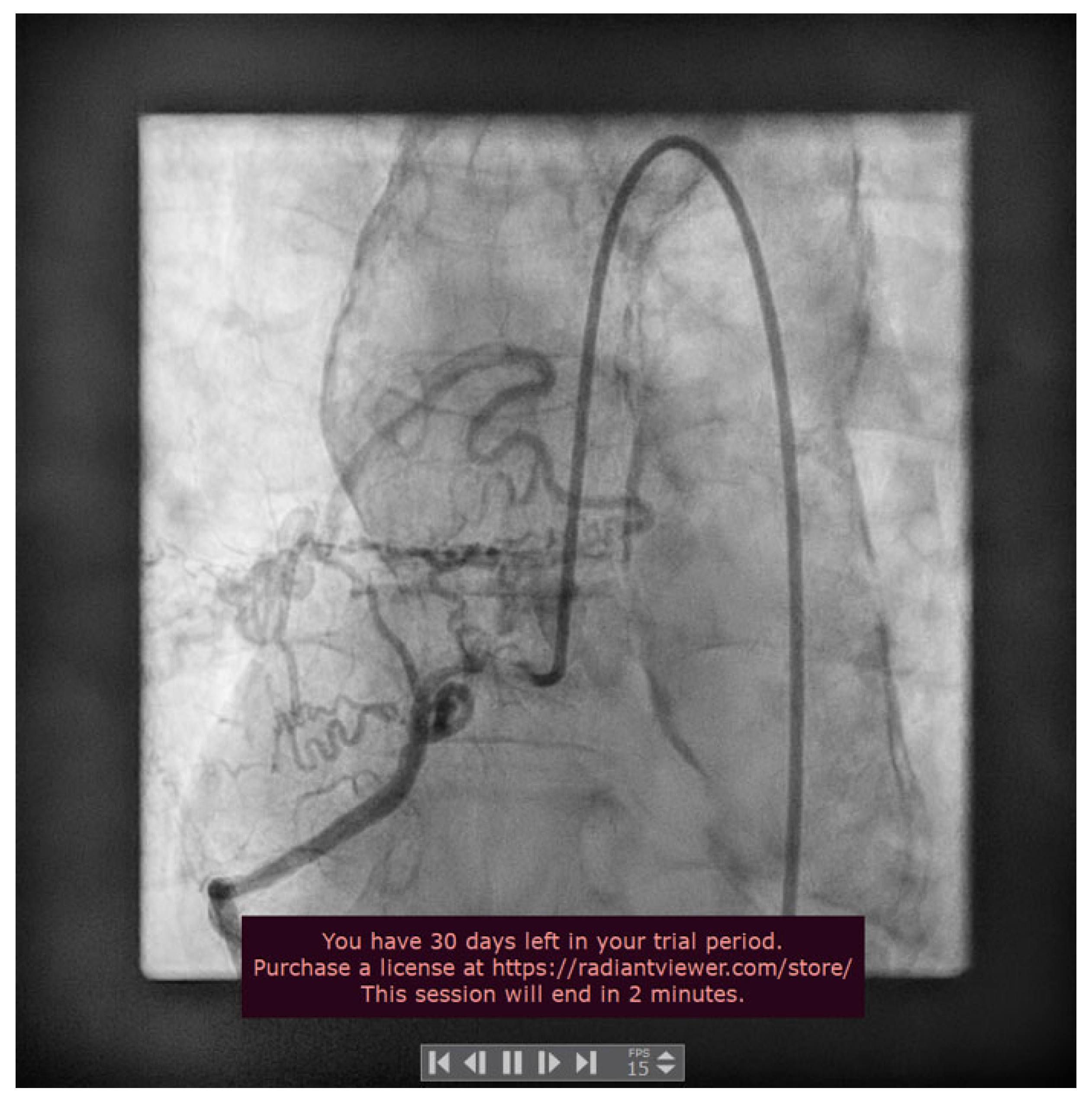

Table 1.
Laboratory findings.
| Laboratory finding | 1st day | 2nd day | 3rd day |
|---|---|---|---|
| AST (IU/L)1 | 32 | 27 | 31 |
| ALT (IU/L)2 | 25 | 22 | 29 |
| CPK ( IU/L)3 | 48 | 52 | 58 |
| CPK-MB (IU/L)4 | 2 | 1 | 2 |
| Troponin T(ng/L) | 3.1 | 4.3 | 1.5 |
| Troponin I (ng/L) | 2.6 | 3.7 | 1.4 |
1AST=aspartate aminotransferase; 2ALT= alanine aminotransferase; 3 CPK=creatine phosphokinase; 4 CPK-MB= creatine phosphokinase myocardial bound.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



