
Submitted:
31 January 2024
Posted:
31 January 2024
You are already at the latest version
Abstract
We conducted this systematic review with the objective to understand the efficacy and safety of proton pump inhibitors [PPIs] in the pediatric population. We have used PubMed to identify randomized controlled trials [RCTs] published between 1st June 2010 and 30th June 2023, in patients from birth to 18 years old, with gastroesophageal reflux disease [GERD], who received treatment with any PPI. The literature yielded 76 articles and 13 met inclusion criteria. For infants, PPIs were equal to placebo in reducing GERD symptoms in 4 articles. In 1, the number of GER episodes and esophageal acid exposure were lower in infants who received PPIs and left lateral position, but there was no significant improvement in symptoms. In another publication, the combination of PPIs and feeding modifications [FM] was not more effective than PPIs alone. For children and adolescents, PPIs were effective in improving symptoms and achieving mucosal and histological healing, which was subsequently maintained.
To conclude, PPIs are not effective to reduce symptoms related to GERD in infants, but are effective in older children, along with histological remission. Generally, PPIs are well tolerated, but it is important to not forget the possible adverse events [AE], especially if they are used for a long time.
Keywords:
gastroesophageal reflux disease
; efficacy
; safety
; proton-pump inhibitors
; pediatric patients
; systematic review
1. Introduction
Gastroesophageal reflux [GER] in the pediatric population is very common, usually it affects approximately 50% of infants under three months old[1], and tends to resolve spontaneously at 12-24 months[2]. It consists of a physiological process with the involuntary passage of gastric contents into the esophagus[3] and some of these reflux episodes result in regurgitation into the oral cavity. Most episodes are asymptomatic and do not cause complications. However, on fewer occasions, the intensity or frequency of regurgitations can cause troublesome symptoms, damage the esophagus and/or affect the general condition of the child, constituting gastroesophageal reflux disease [GERD][2,3].
The prevalence of GERD is difficult to establish because of its heterogeneity symptoms and it varies depending on the country and on the diagnostic criteria used [3,4,5]. As expected, as with GER, its incidence tends to decrease with time[3] in children without other pathology. The first month of life it could arises 25.5% and decreases to 1.1-1.6% at the age of 12 months[3,5]. In childhood and adolescence between 0.9% to 18.8% report symptoms like heartburn, epigastric pain or regurgitation[5,6]. Higher rates of GERD are seen in children with a history of prematurity[7,8], corrected esophageal atresia, developmental and neuromuscular disorders[9], cow’s milk protein allergy[3,10,11,12] or pulmonary disease, like Cystic Fibrosis [CF][13].
Clinical manifestations of GERD vary greatly depending on age and in infants are usually non-specific. It is important to differentiate healthy infants with daily regurgitation or vomiting without repercussion, frequently called ‘happy spitters’[14] from infants with GERD. In this patients, symptoms can include irritability, disturbed sleep, feeding refusal, vomits, failure to thrive, hematemesis or unexplained anemia, apnea and other respiratory symptoms, such as cough, wheezing, laryngitis or pneumonia[3,6,15]. In older children and adolescents, symptoms similar to adulthood like chronic heartburn, frequent regurgitation and chest pain after meals are typical[14].
Most times, diagnosis can be reached through a complete medical history and physical examination[16] when there are no warning signs. Sometimes diagnostic tests, such as ultrasound, barium study, pH-monitoring, occasionally combined with intraluminal impedance monitoring [pH-MII] or endoscopy with histological study, are necessary to reach the diagnosis[3,5,11] specially if there are atypical symptoms, warning signs, suspected complications or treatment failure[3,6].
The management for GERD depends on the age, clinical manifestations and complications, and it is based on a combination of conservative measures and pharmacological therapy, leaving surgical treatment for complex cases or when previous treatment fails[14].
Different guidelines for diagnosis and treatment have been published over last decade[11,17,18,19], with variable methodological approach[20], but most have in common a conservative initial management. The natural history of the disease tends to resolve spontaneously within the first year of life, so in infants, good information and parental support are essential. Other measures like overfeeding must be prevented, as it increases abdominal distension, making it more appropriate to offer smaller and more frequent feeds[14]. Breastfeeding should be encouraged for its protective effect against reflux[21]. In those infants that regurgitation could be caused by cow’s milk protein allergy, it is indicated an elimination diet of at least 2-4 weeks[11,21]. In children and adolescents lifestyle modifications are recommended, like avoiding exposure to tobacco smoke or alcohol in adolescents, prevent overweight and excess of caffeine and chocolate[14,22] as well as postural changes during sleep[14].
When aforementioned interventions are not sufficient, pharmacological treatment would be indicated. Although different drugs with acid suppressive effect or prokinetics are indicated, the most well-known and used drugs are proton pump inhibitors [PPIs], like omeprazole, lansoprazole, esomeprazole, rabeprazole and pantoprazole. They block irreversibly the gastric H,K-ATPase, inhibiting gastric acid secretion[23], so the main indication is treatment peptic acid related disease. Esomeprazole is approved by FDA for treatment of infants 1 to 11 months old with erosive esophagitis [EE] caused by acid-mediated GERD[1]. Although GERD guidelines indicate PPIs only for the treatment of EE[11,15], they are often prescribed empirically for childhood reflux and other manifestations that sometimes are in relation to GERD without confirming it[24]. This has led to an increase in the prescription of these drugs in pediatric age in recent years also in children[25,26,27].
PPIs are considered safe drugs, being the most reported adverse events [AEs] mild and in relation to gastrointestinal manifestations, such as nausea or diarrhea or skin reactions[14,24]. However, its chronic use has been linked to risk of gastrointestinal[28] and lower respiratory tract infections[29]. In addition, there are data that suggest a possible increased risk of fractures by changing osteoclast activity[30,31] or the development of allergic disease as a consequence of chronic hypochlorhydria[24,32], especially when used in the first months of life or for a long time.
A previous systematic review on the efficacy and safety of PPIs in the treatment of GERD in children was published[16]. Since then, new treatment guidelines have emerged[20] and the use of PPIs has expanded. Therefore, our objective was to conduct a systematic review to understand the efficacy and safety of PPI for GERD in pediatric patients.
2. Materials and Methods
This review was conducted in concordance with the guidelines outlined in the Preferred Reporting Items for a Systematic Review and Meta-Analysis [PRISMA][33]. To structure the review process, the population, intervention, comparison and outcome [PICO] model was followed[34,35][Table 1]. Additionally, before starting the systematic review, the study was registered with the International Prospective Register of Systematic Reviews [PROSPERO] with ID CRD42023473192.
2.1. Search strategy
A systematic literature review was conducted to identify relevant publications on the efficacy of PPIs as a treatment for GERD in children. For this purpose, the main database MEDLINE [Pubmed] was searched. The search strategy used in the MEDLINE database was restricted to randomized controlled trials [RCTs] published between June 2010 and June 2023, because the last systematic review includes articles until May 2010[16].
The search was performed by two researchers independently in PubMed database using the MESH terms filters: Randomized Controlled Trial, Child: birth-18 years, from 2010/6/1 - 2023/6/30. No language restriction was applied.
The search formula used in the MEDLINE database was: ["Omeprazole"[Mesh]] OR "Esomeprazole"[Majr:NoExp] OR "Lansoprazole"[Mesh] OR "Pantoprazole"[Mesh] OR ¨Dexlansoprazole¨ OR ¨Rabeprazol¨ OR "Proton Pump Inhibitors"[Mesh]] AND ["Gastroesophageal Reflux"[Mesh] OR "Gastroesophageal Reflux"[Majr:NoExp] OR "Esophagitis, Peptic"[Majr:NoExp]] AND ["Infant"[Mesh] OR "Child"[Mesh] OR "Adolescent"[Mesh]].
2.2. Inclusion and exclusion criteria
Inclusion criteria were:
- The study was a RCT.
- The target population was any pediatric patient [0 to 18 years of age] with GERD not secondary to another gastrointestinal pathology and receiving treatment with omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole or dexlansoprazole.
- One of the aims of the study was to evaluate the efficacy, AE and/of safety of PPI therapy.
- The intervention consisted of PPIs and was compared with another PPI, placebo, no treatment or alternative treatment.
- The outcome measure was effectiveness and/or safety of the different PPI for the treatment of GERD in the pediatric population.
Studies with pathologies that can worsen GER or can confuse clinical manifestations such as asthma, neurological disorders, CF, eosinophilic esophagitis o gastroesophageal interventions, were excluded.
2.3. Selection of studies and data extraction
Two authors [S.F.G. and A.M.A.] independently selected the articles included in the review by searching databases. They independently screened all titles and abstracts of identified RCTs for eligibility. If disagreement between 2 reviewers existed, consensus was formed or a third reviewer [A.S.B.] acted as referee. Duplicate references were eliminated. All studies deemed potentially relevant, and those for which abstracts did not offer adequate information for inclusion or exclusion, were retrieved in their entirety as full articles.
The total number of the sample and each group was analyzed for each study; the variables, characteristics of each treatment, duration of the intervention, follow-up time and the results of each trial were recorded.
Structured data extraction was performed from the original reports by 2 reviewers [S.MG. and A.M.A.] independently. The following data were extracted from the selected articles: study details [author, year of study, country, study design, sample size, duration of follow-up]; participant details [age, sex, method of GERD assessment, type of intervention [non-pharmacological treatment: head and body position after meals or diet without cow’s milk proteins, or pharmacological treatments], type of intervention, PPI studied, control group [another PPI, placebo or another treatment], treatment doses and treatment duration, primary and secondary objectives, outcomes measures, treatment monitorization [pH-monitoring, pH-MII, endoscopy, histological study], results, number and type of AEs.
3. Results
3.1. Study selection
The Pubmed database search yielded 76 records. They were selected by title and reviewed by abstract, and 55 articles were selected for full-text review. Finally, 13 articles[36,37,38,39,40,41,42,43,44,45,46,47,48] that match selection criteria were selected. The results of the search are summarized in the flow chart according to PRISMA statement 2020 in Figure 1 [Figure 1]. The reasons for the exclusion of articles that were read in full-text but not included in the review are summarized in Suplemmentary Table S1.
All the articles were published in 2010 or after that. 53.8% of the articles [7/13] have been published by authors from the United States [US], 23.1% authors from Poland [3/13], 1 from Iran, 1 from Australia and 1 from Netherlands, but most of the articles 84.6% [11/13] are multicenter studies that include European countries, the US and Canada.
Data from 1166 participants [54.5% males] with age between 0 and 18 years old were included. The sample size median was 64 [range between 49-268]. The age ranges in the studies vary widely. Most of them include patients under 1 year of age[36,37,38,46,47,48]. The remaining 7 articles include patients older than one year: 3 between 1 and 11 years[39,43,44], 1 include patients between 1-3 years[40], 1 between 1-5 years[45], 1 between 7 months and 18 years[42] and 1 between 12-17 years old[41].
The studies were categorised according to the age groups of the participants [infants, children and adolescents] due to the distinct manifestations of GERD symptoms in these populations and the potential variations in efficacy.
The diagnosis of GERD for inclusion in the studies was made in 5 studies by clinical criteria, in 2 studies by pH-MII, and the rest by clinical criteria confirmed by endoscopic findings[39,40,41,43,44,45].
Esomeprazole was the most studied PPI in 5 of the 13 articles[37,38,39,40,47], while rabeprazole was examined in 3 articles[43,44,48], omeprazole in 2[36,42], pantoprazole in 2[45,46] and dexlansoprazole in 1[41]. Five studies [38.46%] compared PPIs with placebo[37,41,46,47,48], other 5 [38.46%] are dose efficacy studies[39,40,43,44,45], 15.38% compared the use of PPIs with postural and dietary measures[36,38] and one study compared omeprazole with quince syrup[42].
3.2. Effectiveness of PPI
3.2.1. Infant population
We have identified 6 articles from children aged between 28 weeks postmenstrual age and 12 months with GERD[36,37,38,46,47,48]. They are summarized in Table 2. Two of these articles[36,37] have been carried out on neonates, 1 on patients from birth to 6 months of life[38] and the rest of them on patients between 1 month and 12 months.
In total, 101 neonates have been included[36,37], 45.7% were male, with a postmenstrual age [PMA] between 28-60 weeks. The diagnosis was made by the clinical manifestations in one of the studies[37] and by clinical symptoms and pH-impedance test in another one[36].
In relation with effectiveness, Davidson et al[37], compared esomeprazole with placebo and concluded that there were no significant differences in the number of GERD-related clinical manifestations between infants receiving esomeprazole and those who have received placebo. Jadcherla et al[36] have studied the impact of feeding strategies with acid suppression on esophageal reflexes. They compared neonates that have received omeprazole with patients that have received omeprazole and feeding modifications [FM] [restrictive feeding strategies with enteral nutrition till 140 ml/kg/day and body positional modifications]. They concluded that PPI treatment with FM did not significantly improve esophageal reflexes or signs and symptoms.
We retrieved 4 studies done in infants over 1 month of life[38,46,47,48]. The studies include 523 infants [60.5% males] with a mean age of 4 months [range between 2 weeks of life and 24 months of life]. To meet the inclusion criteria in the studies, the diagnosis of GERD was made in all of them through clinical manifestations [using different questionnaires: Modified GERD Symptom Questionnaire in Infants [GSQ-I], i-GERQ and i-GERQ reviewed [i-GERQ-R]]. Three of these RCTs compared PPIs by using placebo[46,47,48] and another one take into account body position and other antireflux therapies [Mylanta®] as controls[38].
Loots et al[38] published that the number of GER episodes and esophageal acid exposure are significatively lower in infants who received PPIs [esomeprazole] and left lateral position [LLP]. These results are not correlated with a significant improvement in symptoms other than vomiting. When PPIs are compared independently with antacids, PPIs produced a reduction in reflux index but not significatively. The same occurs when LLP is compared with head cot elevation [HE], where LLP produced a considerable reduction in total GER episodes [21 vs 10, p 0.056].
Unlike, Winter et al. 2010[46] found that during the initial 4-week treatment period with pantoprazole, all patients experienced a significant improvement in symptoms, analysed through weekly GERD symptom score [WGSS] [p<0.001], in comparison with baseline. However, during the double-blind phase of the study, no significant differences were found in terms of symptom worsening or improvement between the placebo group and the treatment group. Two years later, the same author published a study[47] where, in the open-label [OL] phase, esomeprazole was administered to all patients, resulting in a pronounced improvement in clinical scale scores and symptom scores. In the double-blind [DB] phase, symptoms worsened in patients who received placebo and those who received esomeprazole, with no significant differences between the two groups [48.8% vs. 38.5%, p = 0.28].
The same occurs in the study on rabeprazole published by Hussain et al[48] in which a significant improvement of symptoms is observed at the end of the OL phase, where all patients receive the same dose of rabeprazole [10 mg/day]. However, in the DB phase, no significant differences are found among the three groups [patients receiving rabeprazole 5 mg/day, rabeprazole 10 mg/day, or placebo].
3.2.2. Children population
Regarding children aged between 1-18 years old with GERD six articles have been identified[39,40,41,43,44,45]. Three of these articles[39,43,44] have been carried out on children aged between 1-11 years old, one on patients from 12-36 months of life[40], another one on patients between 1-5 years old[45] and the last of them[41] has done in adolescents [aged 12-17 years old]. The studies include 453 infants [55.1% males] with a mean age of 5.6 years [range between 1 year and 17 years of life] and GERD was diagnosed through endoscopic study in all children over one year old. Table 3 summarizes the studies in children.
In all articles included in this group, different doses of PPIs are compared with the aim of achieving histological remission in four of them[39,40,43,44] and improving symptoms[45]. In contrast to them, Gremse et al[41] after an OL phase where all included patients receive PPI treatment, compare PPI treatment [dexlansoprazole] with placebo, aiming to study efficacy in relation to histological remission and assess safety.
The published articles demonstrate that PPI treatment is effective in achieving histological healing in patients with EE in a high percentage of cases, reaching 100% histological remission in the study published by Tolia et al[40] and in the study by Baker et al[45]. No significantly higher rates of histological healing have been found when using higher doses of PPIs[39,40,43,44].
In the majority of the articles within this section, clinical improvement aligns with histological improvement. Tolia et al[40] noted a significant enhancement in symptoms across various treatment doses compared to the baseline. Similar findings were observed in the study by Baker et al[45], where symptoms improved in all treatment groups, although the improvement was not statistically significant in the group receiving a medium dose [0.6 mg/kg/day of pantoprazole].
An OL phase was done in the study by Gremse et al[41] all participants receive PPI treatment for 8 weeks, 88% achieve histological healing and entered in the maintenance phase. Subsequently, patients were randomized into two groups [PPI treatment or placebo]. For patients with Los Angeles grade A EE, similar healing rates were observed between dexlansoprazole [82%] and placebo [87%]. In cases of grade B, the differences with treatment were more pronounced [82% healing with dexlansoprazole and 13% in the placebo group]. Only one patient had baseline grade C EE, received placebo, and histological healing was not sustained.
3.2.3. Others
One article[42] involves patients aged 0 to 18 years with symptomatic GERD. In this study published by Zohalinezhad in 2015, patients were randomized into two treatment groups based on whether they received quince syrup or PPIs [omeprazole]. The diagnosis of GERD was made using clinical scales. In patients younger than one year, the GSQ-I was employed, in patients aged 1 to 4 years, the GSQ for young children [GSQ-YC], and in patients aged 5 to 18 years, the GERD assessment of symptoms in Pediatric questionnaire [GASP-Q].
The study included 79 patients [mean age 67.66 months], 37 patients under 59 months of life and 42 older. The most common symptom was refusal to eat/refusal to feed in young children, and burping or belching in older children. In little ones, symptoms significantly improved during and after treatment, but there were no significant differences between the control and treatment groups. The same occurred in older children. In both groups, weight significantly improved compared to the baseline situation, with no significant differences found between the two groups at week 4.
3.3. Safety and adverse events
In terms of safety all studies but two found AEs[36,42]. Among neonates, only Davidson et al[37] found AE, that were comparable between both groups [23.1% esomeprazole group, 34.6% placebo group]. The predominant AE was desaturation, occurring in 2 patients in the esomeprazole group and 1 in the placebo group.
In infants over 1 month of age, all authors reported AEs[38,46,47,48]. The majority of the reported AEs were not related to treatment with PPIs [no significant difference compared to the placebo group], and were generally mild-to-moderate. The most frequent AEs were associated with gastrointestinal symptoms [diarrhea, constipation, vomiting...], upper respiratory tract infections, and fever/pyrexia. Two of these authors documented serious AEs, including gastroenteritis [one patient with a rotavirus infection], failure to thrive, reduced oral intake, and weight loss[38,46].
Two articles found AEs, possibly or likely, related with treatment administration[47,48]. Winter et al[47] identified 4 patients with treatment-related AEs [abdominal pain, tachypnea, regurgitation and alanine aminotransferase elevation] and two of them persisted in the DB phase, [tachypnea -esomeprazole group-, alanine aminotransferase elevation -placebo group-]. Hussain et al[48], observed an increase in serum gastrin levels in rabeprazole-group patients.
In children, AEs were described in all articles included[39,40,41,43,44,45] with no significant differences between PPIs and placebo or with different dose of PPI.
Most of them are mild-to-moderate. The most common on-treatment AEs continued to be those related with gastrointestinal symptoms and also upper respiratory tract infections, rhinitis and nasopharyngitis. In this group, headache is also described as a frequent mild-to-moderate.
The AEs related to treatment that have been described were diarrhea and sleep disturbance in one study in patients treated with pantoprazole[45]; two other AEs in the dexlansoprazole treatment group were considered to be treatment related: abdominal pain in one patient and decrease appetite in another one[41].
Three authors reported serious treatment emergent adverse events [TEAEs] and included a case of convulsion [dexlansoprazole], recurrence of GERD [dexlansoprazole], H1N1 influenza [placebo][41]. Haddad et al[43] reported as severe TEAEs: abdominal pain, nausea, vomiting, bronchopneumonia, gastroenteritis, cough and choking and also describe lymphadenitis, bronchopneumonia and partial seizures with secondary generalisation[44].
Elevated serum gastrin levels were reported in Hussain et al[48] [rabeprazole] and in Gremse et al[41]. Mean serum gastrin levels for subjects that have been treated with dexlansoprazole in placebo group decreased to near-baseline later[41].
No study disclosed alterations in vital signs. There were no reported deaths in any of the studies during their course.
4. Discussion
In our review, we assessed the effectiveness and safety of different PPIs for the treatment of GERD in various age groups. Despite the increasing use of PPIs in the pediatric population, our systematic review has not found significant results in symptom improvement in the RCTs done in infants. These results are consistent with those published in the 2010 systematic review by van der Pol[16] where they observed that the use of PPIs was equally effective in reducing GERD symptoms as other drugs [ranitidine, antacids]. Additionally, different doses of the same PPI did not significantly modify the symptomatology[16]. In children, PPIs are effective in achieving histological healing and improving symptoms. However, the studies included in the review only compare different doses of PPIs, with no significant differences found between the various dosage groups. Only one study published in older children[41] compares the use of PPIs with a placebo, in which they are effective in achieving mucosal healing in patients with EE.
The evidence regarding the use of PPIs in the pediatric population for GERD is of very uncertain quality due to various factors, including the diversity of the population, variability in outcome measures, and the limited availability of RCTs comparing the response to PPI treatment with a placebo.
Most of the articles included in our review, especially in infants, use diagnostic clinical scales for GERD as inclusion criteria in the study. Clinical scales, such as GSQ-I or I-GERQ-R[49,50], have been used as tools to assess and quantify reflux symptoms in infants and young children. These scales typically include questions about the frequency and severity of symptoms, such as regurgitation, vomiting, irritability, and sleep problems. In our review, Winter et al 2010[46] included patients with a GSQ-I mean symptom frequency > 16 at screening, Loots et al[38] and Hussain et al[48] employed the I-GERQ-R and Zohalinedhad et al[42] used age-specific questionnaires to distinguish GERD symptoms in infants and children: GSQ-I was used in infants, GSQ-YC for children aged between 1 and 4 years old and GASP-Q for children with and age range 5-18 years old.
The evidence regarding the use of specific clinical scales for the diagnosis of GERD in children may vary and evolve over time. Currently, there is no clinical tool that serves as the gold standard for the diagnosis of GERD[3,11]. The decision to utilise these scales may depend on the preference and clinical practice of healthcare professionals, as well as the guidelines and recommendations in place.
ESPGHAN guidelines published in 2018[11] stated that infants under 12 months without warning signs, could be diagnosed with GERD through a detailed clinical history that pays attention to both personal and family history, along with a physical examination. Additional tests and anti-reflux therapies are only necessary in infants with some warning signs, such as refusal of intake, weight loss, or alterations in growth[11]. In these patients, reaching a diagnosis can be challenging because many symptoms present in GERD [crying, irritability, refusal to eat, vomiting] may also be present in other diseases. It is important to distinguish between "happy spitters" [infants with GER without disease] and infants with symptoms and complications related to GER, to avoid unnecessary changes in diet, medications, or additional tests.
In children older than 12 months, where GER is not usually physiological, additional tests are often necessary to exclude other diseases. In our review, the studies that include these patients[39,40,41,43,44,45], use clinical and but also all studies us endoscopic criteria to reach the diagnosis of GERD and assess the response to treatment.
The objective of endoscopy is to detect EE, microscopic esophagitis and other diseases with clinical manifestations similar to GERD [i.e. eosinophilic esophagitits][11]. There is no sufficient evidence to do the endoscopic study to achieve the diagnosis of GERD[11], but it could be interesting when suspecting complications related to GERD, before escalating the treatment[1,11] and in clinical trials to know mucosal healing with PPI, like presented here.
In the included studies, some of them[40,41] assess the diagnosis and severity of EE using the Los Angeles [LA] classification system[51]. The majority of included patients have mild [LA grade A] and moderate [LA grade B] EE, likely indicating a less advanced progression of GERD in pediatric population. Even though the LA classification system is not officially validated for the pediatric population, it serves as a tool for staging EE and assessing treatment response.
The incidence of EE in the population included in the systematic review is highly variable. Baker et al[45] report an incidence of 6.7%, while the rest of the patients are grouped into the histological esophagitis category. Patients included in the studies by Haddad[43,44] and Tolia[39,40] show an incidence of EE ranging between 39-49%. This prevalence is higher than reported in other studies, possibly because, in some studies like this published by Tolia et al[40], the included patients are those who did not initially respond to other measures. Gilger et al [52] reported a global incidence of 12.4%, ranging from 5.5% in infants to 19.6% in children aged 17 years.
The method for assessing the effectiveness of PPIs treatment in the studies included in the review was also predominantly through clinical scales. Most of the studies have been published before 2017 and assess treatment response through a questionnaire based on clinical manifestations. Only some studies done in children older than 12 months[39,40,41,43] investigated histological remission after treatment with PPIs. The majority of them[39,40,43], compare different doses of the same PPI to assess improvement in endoscopic studies. Only Gremse et al[41], compared dexlansoprazole with placebo in a cohort of patients between 12-17 years old. In this study[41], it was observed that 88% of patients achieved mucosal healing of EE in the OL phase, and this was maintained in the maintenance phase in 82% of patients who received dexlansoprazole and in 58% of patients who received placebo in the overall sample, with no significant differences between the two groups [P=0.114]. The remission rates in the different groups varied depending on the degree of EE. Thus, in patients with higher-grade EE, histological remission remained at a lower percentage in the placebo group [13% in grade B and 0% - with only one patient included - in grade C].
In the latest guidelines published by ESPGHAN[11], they do not specify the optimal method for evaluating the treatment response if symptoms persist after 4-8 weeks of initiating treatment and alarm symptoms have been ruled out. Indeed, it would be prudent to undergo an endoscopic investigation in cases requiring an escalation in therapy or in situations where there is a lack of response to PPI treatment. In the studies included in our review, the treatment time period in most groups is 8-12 weeks, with a treatment range depending on the study of between 2 and 24 weeks. Four studies were conducted in two phases[41,46,47,48], where symptoms improved significantly during the OL phase, and this improvement was sustained in a significant percentage of patients during the DB phase across various treatment groups [PPIs, different PPI doses, and placebo]. No significant differences were found between the different groups.
In infants, further studies that first assessed non-PPIs measures based on NASPGHAN-ESPGHAN guidelines[11] are needed. It is necessary to know the effectiveness of the non-pharmacological treatment with changes in body position during and after meals, and FM [avoiding overfeeding and specially cow's milk elimination diet during 2-4 weeks][3,11]. These measures are only evaluated in the study published by Jadcherla et al[36]. This trial compares a group receiving only PPI treatment with another receiving PPIs along with FM [volume restriction < 140 ml/kg/day, slow feeding for > 30 minutes in the right lateral position, and supine postprandial position]. The group with PPI and FM did not improve esophageal reflexes, respiratory changes, or symptoms, but distal esophageal contraction lower esophageal sphincter [LES] and LES tone decreased, and LES relaxation reflex occurrence is less frequent[36].
In infants who are breastfed, it is also important to maintain breastfeeding[5,11], as it has been observed that it could have a protective effect against GERD for various reasons, including differences in gastric emptying and a protective effect against cow's milk protein allergy. However, there are no robust studies supporting these recommendations.
Different factors may also play a role in how well the treatment works, especially in neonates and infants. In 2016, Kaguelidou[53] conducted a study to find the smallest amount of omeprazole that effectively treats pathological acid reflux in newborns, using a reflux index measured with pH-metry. The study found that the minimum effective dose depends on both the gestational age at birth and the postnatal age. It tends to be higher in older neonates and those born very prematurely, compared to younger neonates born closer to full term. In infants under 1 year of age, the results of DB RCTs in which PPIs are compared with placebo have not found significant benefits between both groups, although one study[38] did see a significant benefit treatment with esomeprazole improved exposure to acidic content compared to antacids [P=0.043]. In these studies, symptoms compared to the baseline state improved significantly during the OL phase, but this improvement was maintained during the DB phase without finding significant differences between the treatment and placebo groups.
During this age period, the doubt remains that the clinical changes in relation to improvement of GERD symptoms are related to the maturation process during the first months of life, in which the gastroesophageal sphincter matures with a reduction in episodes of LES relaxation, solid food are introduced and infants stay incorporated for longer, which improves GER[3,46].
As individuals with GERD grow older, their susceptibility to developing EE or other complications associated with the prolonged exposure of the esophagus to stomach acid rises. Despite symptoms in older children and adolescents being more specific, like heartburn, epigastric pain or cough, it is important to conduct complementary tests, including endoscopic examinations, to achieve a diagnosis and excluded potential complications. In contrast to infants, primary treatment for GERD in children involves the use of PPIs, along with dietary adjustments, with the goal of alleviating symptoms and achieving mucosal and histological healing. In our review, most articles examine varying doses of PPIs, except for one[41]. However, all of them have shown that PPI treatment is effective in achieving mucosal healing, and this improvement is accompanied by a relief in symptoms.
PPIs have also proven effective in maintaining histological healing over time. In the study by Gremse et al[41], 82% of patients maintained histological healing after 16 weeks of treatment with dexlansoprazole. In contrast, studies conducted in adults showed that only 66% of patients maintained remission[41]. This difference may be attributed to the fact that adults often present more severe degrees of EE[41]. We found similar results in the article published by Haddad et al[44], where 76.1% of patients maintained histological remission. The percentage of maintenance was lower in patients with moderate to severe disease.
Regarding AE, PPI appear to be safe in the pediatric age group. The most common harmful symtoms vary depending on the age group. In the neonatal period, episodes of desaturation are most frequent. From one month of age onward, infants more commonly experience upper respiratory tract infections and gastrointestinal disturbances [abdominal pain, nausea, vomiting, diarrhea], which have remained the most frequent AEs in older children.
Most studies in the field of AE with PPI focus on the long-term use of this drugs in the adult population[54,55]. Overall, systematics reviews shown that PPIs are safe and well-tolerated drugs when used over a short period of time[56]. It is known that prolonged use of PPIs is associated with more risk of both respiratory and gastrointestinal infections, probably as a consequence of an increase in gastric pH that favours bacterial colonization of both the respiratory and digestive tracts. This is because acid secretion serves as an important immunological barrier in the gastrointestinal tract[57,58].
In our review, the most frequently reported AEs are gastrointestinal disorders [vomiting, abdominal pain, and diarrhea] and upper respiratory infections, although they have not been directly related to the treatment. One of the most serious AE was a Rotavirus infection in an infant under 1 year of age that required hospital admission[38]. In infants under 1 year of age, where the most frequent AEs were infections, especially of the upper respiratory tract, doubt arises as to whether these AEs are related to treatment with PPIs, as no significant differences were found between the groups that received treatment with PPIs and the patients who received placebo[37,46,47,48], especially in an age period in which respiratory infections of viral origin are very common.
The AEs do not seem to be related to the drug dosage administered. Hussain et al[48] reported that children who received a lower drug dosage [6.7% in the group receiving 5 mg of rabeprazole] experienced more AEs than those who received a higher drug dosage [2.3% in the group receiving 10 mg of rabeprazole].
Other AEs associated with the prolonged use of PPIs are related to malabsorption of minerals or nutrients, such as magnesium and vitamin B12[57]. Absorption of vitamin B12 takes place after it separates from the protein to which it is bound [intrinsic factor], thanks to hydrochloric acid[57]. Surprisingly, in infants, no studies in our systematic review or published to out knowledge evaluate these circumstances[57].
It has been described in several studies that prolonged use of PPIs increases the production of gastrin[59,60,61]. PPIs block gastric acid secretion by inhibiting the proton pump in the parietal cells of the stomach. When gastric acidity is reduced, a compensatory response is activated in the body to try to restore the acid-base balance. Consequently, G cells in the gastric antrum are activated, releasing gastrin in an attempt to increase acid production. In our review, two authors have reported an increase in the serum gastrin levels in patients who had received treatment with rabeprazole[48] or dexlansoprazole[41]. Hussain et al[48] described that 5% of children included in the combined rabeprazole treated groups had elevated serum gastrin levels after the DB phase. Gremse et al[41] reported that the highest average elevation of gastrin occurred within the first 4 weeks of treatment during the OL phase. Subsequently, the levels remained stable until the end of the OL phase and during the maintenance phase in the treatment group. In the placebo group, gastrin levels had decreased to near-baseline after 8 weeks during the maintenance phase. However, the study does not specify the incidence of elevated gastrin levels. In adults, prolonged hypergastrinemia has been associated with hyperplasia of enteroendocrine cells and the development of gastric carcinoid tumour[62,63]. In children, hypergastrinemia secondary to the use of PPIs does not seem to be a concern, as it has been observed that gastrin levels return to normal once the treatment is discontinued. Additionally, secondary hyperacidity due to hypergastrinemia is not a clinically relevant issue when PPIs are used for a short period [<12 weeks][46,57].
Extended use of PPIs could also potentially lead to bone fractures, as a result of a decrease in calcium absorption, which is dependent on gastric acid, and the inhibition of the osteoclasts function[57]. The studies done in adults are controversial. In our review, no episodes of bone fracture are described. In the literature, Wang et al[64] in 2020 conducted a study involving over 100,000 patients under the age of 14. They observed that those who had been treated with PPIs had a significantly higher risk of minor fractures such as those in the upper and lower limbs, but they did not find association with spinal or head fractures. The risk of fractures was significantly higher in the group that received omeprazole, but no differences were found in patients that received other PPIs. The risk increased with a longer duration of treatment, but no correlation was found in relation to the daily dose[31,64]. Prior to this study, in 2015, Freedberg et al[65] conducted research in a very extensive patient cohort. In their study, they observed a dose-response effect with increased total exposure to PPIs in young adults [18-29 years old], but not in children [<18 years]. In 2019, Malchodi et al[30], published a study on 851,631 children under 14 years of age who received treatment with antacids [PPIs or H2 antagonists] during their first year of life. After adjusting for covariates, they found that patients who received PPIs alone [a 23% higher risk] or in combination with H2 antagonists [a 31% higher risk] had a higher risk of bone fractures. This association was not found in patients who received only H2 antagonists. Additionally, they found that a longer duration of antacid treatment and an earlier initiation increased the risk of bone fractures[30,31].
During the preparation of our work, a systematic review was published in Cochrane[1] in which they review the pharmacological treatment of GER in children. This review differs from our work in different reasons. First of all, it includes studies in patients with GER, not just GERD. Afterthat, it excludes studies that analyze dietary measures and other non-pharmacological treatments. Then, patients included are under 16 years of age, while in our study we include patients up to 18 years of age [as are those studied in the article published by Zohalinezhad et al. in 2015[42] and Gremse et al[41] and finally, the articles included are those published until September 2022. We did the review until June 2023, however, no article in our review that meets the inclusion criteria has been published after the year 2020.
The limitations identified in the studies for conducting a proper systematic review are as follows. First, in daily clinical practice, it is challenging to distinguish between GER and GERD, and these terms are often incorrectly used interchangeably. Second, symptoms are highly variable, nonspecific, and change with age, posing a diagnostic challenge, especially in infants who often present with crying and irritability—symptoms that can be present in various pathologies. Third, due to these obstacles, establishing the true prevalence of GERD is difficult. Fourth, there is currently no clinical tool that serves as the gold standard for diagnosing GERD in the pediatric population. Fifth, the majority of studies conducted in children do not incorporate a placebo control group and instead investigate the response to various doses of the same PPI, hence, it was not possible to study spontaneous healing in these patients.
However, our study summarizes the current evidence and is an initial step for future works in a pathology as common in children as GERD. Future lines of research would be studies that compare the effectiveness of PPIs with other non-pharmacological measures, such as postural measures, thickening of intake or, especially, cow´s milk protein exclusion diet as recommended in the ESPGHAN guidelines[11].
5. Conclusions
So far, there is no strong evidence that treatment with PPIs improves symptoms in infants with GERD. Its use is indicated when the symptoms persist despite non-pharmacological measures and a therapeutic trial with a diet free of cow's milk protein. In children and adolescents, the use of PPIs was effective in achieving histological remission in patients with EE, accompanied by an improvement in symptoms.
Despite this, PPIs have been found to be safe and well tolerated drugs in all age groups when used for a short period of time. It is crucial to prescribe these drugs judiciously, keeping in mind the described side effects, especially when employed over extended periods. More studies in the pediatric population are necessary to investigate the effectiveness and safety of PPIs.
Supplementary Materials
Table S1, Full-text articles assessed for eligibility read in full text but not included in the review.
Author Contributions
Dr Sara María Fernández González (S.F.G) conceptualized and designed the study, coordinated and supervised data collection, collected data, carried out the initial analyses, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr Ana Moreno Álvarez (A.M.A) conceptualized and designed the study, coordinated and supervised data collection, collected data, carried out the initial analyses, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr Alfonso Solar Boga (A.S.B) critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tighe MP, Andrews E, Liddicoat I, Afzal NA, Hayen A, Beattie RM. Pharmacological treatment of gastro-oesophageal reflux in children. Cochrane database Syst Rev. 2023, 8, CD008550. [Google Scholar]
- Armas Ramos H, Ortigosa del Castillo L. Reflujo gastroesofágico y esofagitis en niños. Soc Española Gastroenterol Hepatol y Nutr Pediátrica (eds) Trat en Gastroenterol Hepatol y Nutr pediátrica 2a ed [Internet]. 2008, 163–177. Available from: www.cedro.
- Sintusek P, Mutalib M, Thapar N. Gastroesophageal reflux disease in children: What’s new right now? World J Gastrointest Endosc. 2023, 15, 84–102.
- Eiamkulbutr S, Dumrisilp T, Sanpavat A, Sintusek P. Prevalence of gastroesophageal reflux disease in children with extraesophageal manifestations using combined-video, multichannel intraluminal impedance-pH study. World J Clin Pediatr. 2023, 12, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Singendonk M, Goudswaard E, Langendam M, van Wijk M, van Etten-Jamaludin F, Benninga M, et al. Prevalence of Gastroesophageal Reflux Disease Symptoms in Infants and Children. J Pediatr Gastroenterol Nutr [Internet]. 2019, 68, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Baird DC, Harker DJ KA. Diagnosis and Treatment of Gastroesophageal Reflux in Infants and Children. Am Fam Physician. 2015, 92, 705–714. [Google Scholar]
- Eichenwald EC, Yogman M, Lavin CA, Lemmon KM, Mattson G, Rafferty JR, et al. Diagnosis and management of gastroesophageal reflux in preterm infants. Pediatrics. 2018, 142, 1–9. [Google Scholar]
- Dong Seok L, Ji Won K, Kook Lae L, Byeong Gwan K. Prevalence and predictors of gastroesophageal reflux disease in pregnant women and its effects on quality of life and pregnancy outcomes. J Gynecol Res Obstet. 2021, 7, 008–011. [Google Scholar]
- Lauriti G, Lisi G, Lelli Chiesa P, Zani A, Pierro A. Gastroesophageal reflux in children with neurological impairment: a systematic review and meta-analysis. Pediatr Surg Int [Internet]. 2018, 34, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- O’Shea C, Khan R. There is an association between gastro-oesophageal reflux and cow’s milk protein intolerance. Ir J Med Sci. 2022, 191, 1717–1724. [Google Scholar] [CrossRef]
- Rosen R, Vandenplas Y, Singendonk M et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, a. J Pediatr Gastroenterol Nutr. 2018, 66, 516–554. [Google Scholar] [CrossRef]
- Meyer R, Vandenplas Y, Lozinsky AC, Vieira MC, Canani RB, Dupont C, et al. Diagnosis and management of food allergy-associated gastroesophageal reflux disease in young children—EAACI position paper. Pediatr Allergy Immunol. 2022, 33, 1–16. [Google Scholar]
- Dziekiewicz M, Mielus M, Lisowska A, Walkowiak J, Sands D, Radzikowski A, et al. Effect of omeprazole on symptoms of gastroesophageal reflux disease in children with cystic fibrosis. A randomized, double-blind, placebo-controlled trial. Eur Rev Med Pharmacol Sci. 2021, 25, 999–1005. [Google Scholar]
- Poddar, U. Gastroesophageal reflux disease (GERD) in children. Paediatr Int Child Health [Internet]. 2019, 39, 7–12. [Google Scholar] [CrossRef] [PubMed]
- 15. Davies I, Burman-Roy S, Murphy MS. Gastro-oesophageal reflux disease in children: NICE guidance. BMJ [Internet]. Available from. [CrossRef]
- Van Der Pol RJ, Smits MJ, Van Wijk MP, Omari TI, Tabbers MM, Benning MA. Efficacy of proton-pump inhibitors in children with gastroesophageal reflux disease: A systematic review. Pediatrics. 2011, 127, 925–935. [Google Scholar] [CrossRef] [PubMed]
- NICE. Gastro-oesophageal reflux disease and dyspepsia in adults: investigation and management (CG184). 2019, (October 2019):1–27. Available from: www.nice.org.uk/guidance/cg184%0Ahttps://www.nice.org.uk/guidance/cg184/chapter/1-Recommendations#helicobacter-pylori-testing-and-eradication.
- Mohan N, Matthai J, Bolia R, Agarwal J, Shrivastava R, Borkar VV. Diagnosis and Management of Gastroesophageal Reflux Disease in Children: Recommendations of Pediatric Gastroenterology Chapter of Indian Academy of Pediatrics, Indian Society of Pediatric Gastroenterology, Hepatology and Nutrition (ISPGHAN). Indian Pediatr. 2021, 58, 1163–1170.
- Lopez RN, Lemberg DA. Gastro-oesophageal reflux disease in infancy: a review based on international guidelines. Med J Aust. 2020, 212, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Harris J, Chorath K, Balar E, Xu K, Naik A, Moreira A, et al. Clinical Practice Guidelines on Pediatric Gastroesophageal Reflux Disease: A Systematic Quality Appraisal of International Guidelines. Pediatr Gastroenterol Hepatol Nutr. 2022, 25, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Chen PL, Soto-Ramírez N, Zhang H, Karmaus W. Association between Infant Feeding Modes and Gastroesophageal Reflux: A Repeated Measurement Analysis of the Infant Feeding Practices Study II. J Hum Lact. 2017, 33, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Djeddi D, Stephan-Blanchard E, Léké A, Ammari M, Delanaud S, Lemaire-Hurtel A-S, et al. Effects of Smoking Exposure in Infants on Gastroesophageal Reflux as a Function of the Sleep–, Wakefulness State. J Pediatr [Internet]. 2018, 201, 147–153. [Google Scholar] [CrossRef]
- Shin JM, Sachs G. Pharmacology of proton pump inhibitors. Curr Gastroenterol Rep. 2008, 10, 528–534. [Google Scholar] [CrossRef]
- Dipasquale V, Cicala G, Spina E, Romano C. A Narrative Review on Efficacy and Safety of Proton Pump Inhibitors in Children. Front Pharmacol. 2022, 13, 1–7. [Google Scholar]
- Yang S, Trinh NTH, Chalumeau M, Kaguelidou F, Ruemmele FM, Milic D, et al. Pediatric Prescriptions of Proton Pump Inhibitors in France (2009-2019): A Time-Series Analysis of Trends and Practice Guidelines Impact. J Pediatr [Internet]. 2022, 245, 158–164. [Google Scholar] [CrossRef]
- Aznar-Lou I, Reilev M, Lødrup AB, Rubio-Valera M, Haastrup PF, Pottegård A. Use of proton pump inhibitors among Danish children: A 16-year register-based nationwide study. Basic Clin Pharmacol Toxicol. 2019, 124, 704–710. [Google Scholar] [CrossRef]
- Levy EI, Salvatore S, Vandenplas Y, de Winter JP. Prescription of acid inhibitors in infants: an addiction hard to break. Eur J Pediatr. 2020, 179, 1957–1961. [Google Scholar] [CrossRef]
- Park YH, Seong JM, Cho S, Han HW, Kim JY, An SH, et al. Effects of proton pump inhibitor use on risk of Clostridium difficile infection: a hospital cohort study. J Gastroenterol. 2019, 54, 1052–1060. [Google Scholar] [CrossRef]
- 29. van der Sande LJTM, Jöbsis Q, Bannier MAGE, van de Garde EMW, Coremans JJM, de Vries F, et al. The risk of community-acquired pneumonia in children using gastric acid suppressants. Eur Respir J. 2021, 58.
- Malchodi L, Wagner K, Susi A, Gorman G, Hisle-Gorman E. Early Acid Suppression Therapy Exposure and Fracture in Young Children. Pediatrics. 2019, 144. [Google Scholar]
- Tavares M, Amil-Dias J. Proton-Pump Inhibitors: Do Children Break a Leg by Using Them? J Pediatr Gastroenterol Nutr. 2021, 73, 665–669. [Google Scholar] [CrossRef]
- Mitre E, Susi A, Kropp LE, Schwartz DJ, Gorman GH, Nylund CM. Association Between Use of Acid-Suppressive Medications and Antibiotics During Infancy and Allergic Diseases in Early Childhood. JAMA Pediatr. 2018, 172, e180315. [Google Scholar] [CrossRef] [PubMed]
- Yepes-Nuñez JJ, Urrútia G, Romero-García M, Alonso-Fernández S. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol. 2021, 74, 790–799.
- Brockmeier AJ, Ju M, Przybyła P, Ananiadou S. Improving reference prioritisation with PICO recognition. BMC Med Inform Decis Mak [Internet]. 2019, 19, 256. [Google Scholar] [CrossRef] [PubMed]
- Hosseini M-S, Jahanshahlou F, Akbarzadeh M-A, Zarei M, Vaez-Gharamaleki Y. Formulating Research Questions for Evidence-Based Studies. J Med Surgery, Public Heal [Internet]. 2023, 2, 100046. [CrossRef]
- Jadcherla SR, Hasenstab KA, Gulati IK, Helmick R, Ipek H, Yildiz V, et al. Impact of Feeding Strategies With Acid Suppression on Esophageal Reflexes in Human Neonates With Gastroesophageal Reflux Disease: A Single-Blinded Randomized Clinical Trial. Clin Transl Gastroenterol. 2020, 11, e00249. [Google Scholar] [CrossRef] [PubMed]
- Davidson G, Wenzl TG, Thomson M, Omari T, Barker P, Lundborg P, et al. Efficacy and safety of once-daily esomeprazole for the treatment of gastroesophageal reflux disease in neonatal patients. J Pediatr [Internet]. 2013, 163, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Loots C, Kritas S, Van Wijk M, McCall L, Peeters L, Lewindon P, et al. Body positioning and medical therapy for infantile gastroesophageal reflux symptoms. J Pediatr Gastroenterol Nutr. 2014, 59, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Tolia V, Youssef NN, Gilger MA, Traxler B, Illueca M. Esomeprazole for the treatment of erosive esophagitis in children: An international, multicenter, randomized, parallel-group, double-blind (for dose) study. J Pediatr Gastroenterol Nutr. 2015, 60, S24–30. [Google Scholar]
- Tolia V, Gilger MA, Barker PN, Illueca M. Healing of erosive esophagitis and improvement of symptoms of gastroesophageal reflux disease after esomeprazole treatment in children 12 to 36 months old. J Pediatr Gastroenterol Nutr. 2015, 60, S31–S36. [Google Scholar]
- Gremse D, Gold BD, Pilmer B, Hunt B, Korczowski B, Perez MC. Dual Delayed-Release Dexlansoprazole for Healing and Maintenance of Healed Erosive Esophagitis: A Safety Study in Adolescents. Dig Dis Sci [Internet]. 2019, 64, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Zohalinezhad ME, Imanieh MH, Samani SM, Mohagheghzadeh A, Dehghani SM, Haghighat M, et al. Effects of Quince syrup on clinical symptoms of children with symptomatic gastroesophageal reflux disease: A double-blind randomized controlled clinical trial. Complement Ther Clin Pract [Internet]. 2015, 21, 268–276. [Google Scholar] [CrossRef]
- Haddad I, Kierkus J, Tron E, Ulmer A, Hu P, Sloan S, et al. Efficacy and safety of rabeprazole in children (1-11 years) with gastroesophageal reflux disease. J Pediatr Gastroenterol Nutr. 2013, 57, 798–807. [Google Scholar] [CrossRef]
- Haddad I, Kierkus J, Tron E, Ulmer A, Hu P, Silber S, et al. Maintenance of efficacy and safety of rabeprazole in children with endoscopically proven GERD. J Pediatr Gastroenterol Nutr. 2014, 58, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Baker R, Tsou VM, Tung J, Sestini Baker S, Huihua Li, Wenjin Wang, et al. Clinical Results From a Randomized, Double-Blind, Dose-Ranging Study of Pantoprazole in Children Aged 1 Through 5 Years With Symptomatic Histologic or Erosive Esophagitis. Clin Pediatr (Phila) [Internet]. 2010, 49, 852–865. [Google Scholar] [CrossRef] [PubMed]
- Winter H, Kum-Nji P, Mahomedy SH, Kierkus J, Hinz M, Li H, et al. Efficacy and safety of pantoprazole delayed-release granules for oral suspension in a placebo-controlled treatment-withdrawal study in infants 1-11 months old with symptomatic GERD. J Pediatr Gastroenterol Nutr. 2010, 50, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Winter H, Gunasekaran T, Tolia V, Gottrand F, Barker PN, Illueca M. Esomeprazole for the treatment of GERD in infants ages 1-11 months. J Pediatr Gastroenterol Nutr. 2012, 55, 14–20. [Google Scholar] [CrossRef]
- Hussain S, Kierkus J, Hu P, Hoffman D, Lekich R, Sloan S, et al. Safety and efficacy of delayed release rabeprazole in 1-to 11-month-old infants with symptomatic GERD. J Pediatr Gastroenterol Nutr. 2014, 58, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Pliego R, Asbun-Bojalil J, Anguiano-Robledo L. Revisión sistemática cualitativa del uso de cuestionarios para el diagnóstico de ERGE en pediatría. Acta Pediátrica México. 2016, 37, 102. [Google Scholar] [CrossRef]
- Castro Salas U, Camacho Eugenio J, Becerra Riaño K, Zárate Vergara AC, Tirado Pérez IS. La identificación del reflujo gastroesofágico fisiológico evita estudios innecesarios. Biociencias. 2020, 15, 119–128. [Google Scholar] [CrossRef]
- Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999, 45, 172–180. [Google Scholar] [CrossRef]
- Gilger MA, Tolia V, Vandenplas Y, Youssef NN, Traxler B, Illueca M. Safety and tolerability of esomeprazole in children with gastroesophageal reflux disease. J Pediatr Gastroenterol Nutr. 2015, 60, S16–23. [Google Scholar]
- Kaguelidou F, Alberti C, Biran V, Bourdon O, Farnoux C, Zohar S, et al. Dose-finding study of omeprazole on gastric pH in neonates with gastro-esophageal acid reflux using a bayesian sequential approach. PLoS One. 2016, 11, 1–12. [Google Scholar]
- 54. Fossmark R, Martinsen TC, Waldum HL. Adverse Effects of Proton Pump Inhibitors-Evidence and Plausibility. Int J Mol Sci. 2019, 20.
- Maideen NMP. Adverse Effects Associated with Long-Term Use of Proton Pump Inhibitors. Chonnam Med J. 2023, 59, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Shanika LGT, Reynolds A, Pattison S, Braund R. Proton pump inhibitor use: systematic review of global trends and practices. Eur J Clin Pharmacol. 2023, 79, 1159–1172. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne P, Ito S. Toxicity of long-term use of proton pump inhibitors in children. Arch Dis Child. 2018; 103, 78–82.
- Yibirin M, De Oliveira D, Valera R, Plitt AE, Lutgen S. Adverse Effects Associated with Proton Pump Inhibitor Use. Cureus. 2021, 13, e12759. [Google Scholar]
- Lundell L, Vieth M, Gibson F, Nagy P, Kahrilas PJ. Systematic review: The effects of long-term proton pump inhibitor use on serum gastrin levels and gastric histology. Aliment Pharmacol Ther. 2015, 42, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Tatsuguchi A, Hoshino S, Kawami N, Gudis K, Nomura T, Shimizu A, et al. Influence of hypergastrinemia secondary to long-term proton pump inhibitor treatment on ECL cell tumorigenesis in human gastric mucosa. Pathol Res Pract [Internet]. 2020, 216, 153113. [Google Scholar] [CrossRef] [PubMed]
- Helgadóttir H, Lund SH, Gizurarson S, Metz DC, Björnsson ES. Predictors of Gastrin Elevation Following Proton Pump Inhibitor Therapy. J Clin Gastroenterol. 2020, 54, 227–234. [Google Scholar] [CrossRef]
- Shiotani A, Katsumata R, Gouda K, Fukushima S, Nakato R, Murao T, et al. Hypergastrinemia in Long-Term Use of Proton Pump Inhibitors. Digestion. 2018, 97, 154–162. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, DM. Proton Pump Inhibitor Use, Hypergastrinemia, and Gastric Carcinoids-What Is the Relationship? Int J Mol Sci. 2020, 21. [Google Scholar] [CrossRef]
- Wang Y-H, Wintzell V, Ludvigsson JF, Svanström H, Pasternak B. Association Between Proton Pump Inhibitor Use and Risk of Fracture in Children. JAMA Pediatr. 2020, 174, 543–551. [Google Scholar] [CrossRef]
- Freedberg DE, Haynes K, Denburg MR, Zemel BS, Leonard MB, Abrams JA, et al. Use of proton pump inhibitors is associated with fractures in young adults: a population-based study. Osteoporos Int a J Establ as result Coop between Eur Found Osteoporos Natl Osteoporos Found USA. 2015, 26, 2501–2507. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the search strategy and results. Based on PRISMA statement[33].
Figure 1.
Flowchart of the search strategy and results. Based on PRISMA statement[33].
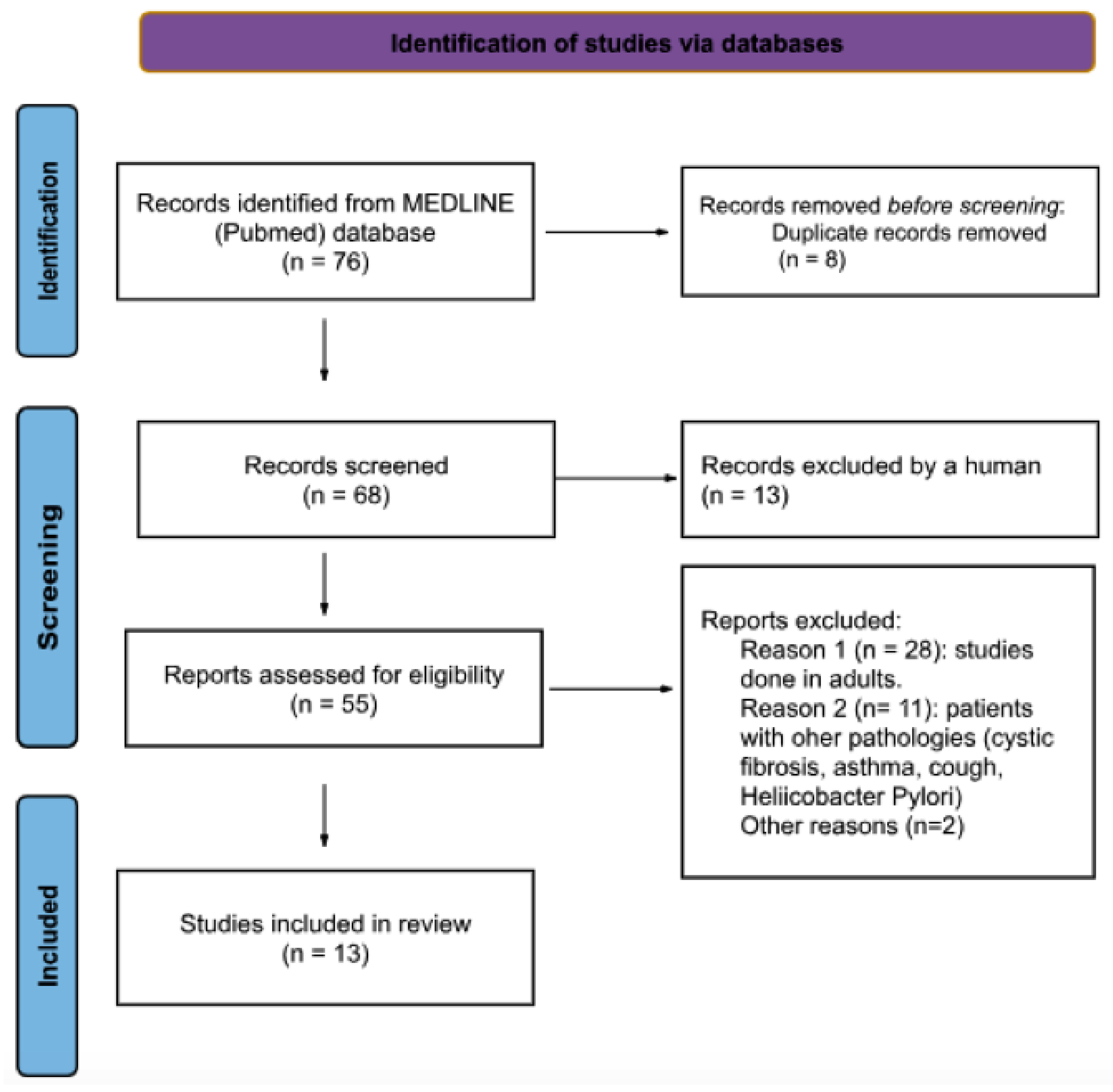

Table 1.
PICO criteria[34] for the inclusion of studies on the efficacy and AEs of PPIs for treatment of GERD.
Table 1.
PICO criteria[34] for the inclusion of studies on the efficacy and AEs of PPIs for treatment of GERD.
| Inclusion Criteria | ||
|---|---|---|
| Population | Patients from birth to 18 years old with GERD not secondary to another gastrointestinal pathology | |
| Intervention | The administration of PPI for treatment of GERD | |
| Comparison | Another PPIs, another dose of PPIs, placebo, no treatment, alternative therapy for GERD [antacid or H2 blocker] | |
| Outcomes | Effectivenes of PPis:
|
|
| Study design | Restricted to RCTs | |
1 GERD: gastroesophageal reflux disease; PPIs: proton pump inhibitors; RCTs: randomized controlled trials.
Table 2.
Characteristics of studies carried out in neonates and infants.
| Study | Objective, Participants, Diagnosis | Intervention (N, age) |
Control (N, age) |
Results | Adverse events |
|---|---|---|---|---|---|
| NEONATES | |||||
| Davidson et al. 2013 (ref) | Difference between esomeprazole and placebo. Neonates (PMA 28-44 w); clinical findings reproducible (8-h videocardiorespiratory monitoring) | Esomeprazole 0.5 mg/kg/day (n=25, 48.1 +/- 29.8 days) |
Placebo (n=26, 46.5 +/- 31.2 days) |
No statistically significant difference in the total number of GERD-related signs and symptoms from baseline observed by video and cardiorespiratory monitoring (esomeprazole:14.7%, placebo:14.1%, P=0.92) |
Esomeprazole: 23.1%, placebo: 34.6%. Most commonly reported: gastrointestinal disorders (9.6%), desaturation (2 esomeprazole, 1 placebo) |
| Study | Objective, Participants, Diagnosis |
Intervention (N, age) |
Control (N, age) |
Results | Adverse events |
| Jadcherla et al. 2020 (ref.) | Esophageal provocation–induced aerodigestive reflexes. Neonates GA < 42 w and PMA 34-60 w. Clinical symptoms of GERD and pH-impedance ARI ≥ 3% | Omeprazole 0.75 mg/kg/dose + FM bundle (n=25, PMA 41.2 +/- 3.1 w) |
Omeprazole 0.75 mg/kg/dose (n=24, PMA 41.4 +/- 2.2 w) |
Treatment groups did not differ in the frequency-occurrence of peristaltic reflex (OR = 0.8, 95% CI 0.4–1.6, P > 0.99). Follow-up in both groups: distal esophageal contraction and LES tone decreased, LES relaxation reflex less frequent (all P < 0.05) |
No found any AE in the study |
| INFANTS | |||||
| Winter et al. 2010 (ref) | Efficacy of pantoprazole; infants (1 and 11 m). Modified total GSQ-I >16 and a clinical diagnosis of suspected, symptomatic, or endoscopically proven GERD |
Pantoprazole 5 mg/day for infants 2.5 kg to <7 kg 10 mg/day for infants >7 kg to 15 kg (n=52, 5.15 +/- 2.81 m) |
Placebo (n=54, 5.04 +/- 2.81 m) |
OL phase: significant reduction in WGSSs from baseline (P < 0.001) with pantoprazole. DB phase: the decrease continued for both treatments groups, no significant differences of withdrawal rates due to lack of effectiveness |
AEs recorded: 29 pantoprazole group, 19 placebo group (no significant differences, all mild or moderate). Most common AEs in both groups: upper respiratory tract infections (13%) |
| Winter et al. 2012 (ref) | Efficacy and safety of esomeprazole; infants (1 to 11 m); GERD diagnosed by symptoms, confirmed by endoscopy or an investigator's determination of GERD | Esomeprazole 2.5 mg/day (3-5 kg) 5 mg/day (>5–7.5 kg) 10 mg/day (>7.5–12 kg) (n=39, 4.9 +/- 2.6 m) |
Placebo (n=41, 4.9 +/- 3.2 m) |
OL phase: 82.7% symptom improvement. DB phase: no significant differences between the treatment group and the placebo group regarding symptom worsening (38.8% vs. 48.5%, HR 0.69; 95% CI 0.35%-1.35%; P = 0.28) |
OL phase: 48% patients AEs. DB phase: 59% esomeprazole, 66% placebo. Most common: upper respiratory tract infection (15.4% and 9.8%, respectively). No serious AEs considered treatment related |
| Hussain et al. 2014 (ref) | Efficacy and safety of rabeprazole, infants (1 to 11 m), GERD resistant to conservative therapy and/or previous acid suppressive medications, I-GERQ >16 | Rabeprazole (n=178, 4.7 +/- 2.54) Rabeprazole 5 mg (n=90, 4.6 +/- 2.57) Rabeprazole 10 mg (n=88, 4.7 +/- 2.52 m) |
Placebo (n=90, 4.7 +/- 2.65 m) |
No differences in primary efficacy variables. Frequency of regurgitation (-0.79 vs -1.20 times/day; P=0.16) Mean increase weight- z scores (0.11 [0.329] vs 0.14 [0.295]; P= 0.440) I-GERQ score (-3.6 [-25%] vs -3.9 points [-27%]; P= 0.960) |
Similar rates of AEs (47%) both in the placebo and combined rabeprazole groups. Most common AEs: pyrexia (2% placebo, 7% rabeprazole), upper respiratory tract infection (6% vs 5%), GERD (8% vs 4%), and vomiting (6% vs 3%) |
| Loots et al. 2014 (ref) | Efficacy of LLP in GERD. Infants (birth-6 m). ph-impedance, monitoring, 8h video study, gastric emptying breath test, I-GERQ q |
Group 1 LLP + ES 1 mg/kg/day (n=12, 12 +/- 3w) Group 2 HE + ES 1 mg/kg/day (n=14, 12 +/- 3w) |
Group 3 LLP + AA (n=13, 14 +/-2 w) Group 4 HE + AA (n=12, 17 +/- 2 w) |
Vomiting was reduced in AA + LLP (P=0.042). LLP compared with HE produced greater reduction in total GER (P=0.056). Acid exposure was reduced on PPI compared with AA (P=0.043) |
No AEs correlated with treatment 5 patients AEs (urinary tract infection, constipation, diarrhea, vomiting). |
1 Abbreviations: AA: antacid; AEs: adverse events; ARI: acid reflux index; DB: double-blind; FM: feeding modifications; ES: esomeprazole, GA: gestational age; GERD: gastroesophageal reflux disease; GSQ-I GERD Symptom Questionnaire in Infants; HE: head of cot elevation; HR: hazard ratio; I-GERQ: infant gastroesophageal reflux questionnaire; LES: lower esophageal sphincter; LLP: left lateral position; M: months, Nº: number; OP: open-label; PMA: postmenstrual age; SD: standard deviation; W: weeks; WGSSs: weekly GERD symptom scores.
Table 3.
Characteristics of studies carried out in children.
| Study | Objective, Participants, Diagnosis | Intervention (N, age) |
Control (N, age) |
Results | Adverse events |
|---|---|---|---|---|---|
|
Tolia et al. 2010 (ref) |
Endoscopic healing of EE. Children 1-11 y. Endoscopically confirmed GERD |
Esomeprazole (8 w) <20 kg: 5 mg (n=26, mean 2.1 y, EE=12). ≥20 kg: 10 mg (n=31, mean 8.5 y, EE=16) |
Esomeprazole <20 kg: 10 mg (n=23, mean 2.5 y, EE=12). ≥20 kg: 20 mg (n=29, mean 8.3 y, EE=13) |
109 patients randomized: 49% EE. EE healed in 89%: <20kg/5mg 100%, <20kg/10mg 82%, ≥20 kg/10 mg 90%, ≥20 kg/20 mg 85% |
10/108 patients with AE related with esomeprazole (9.3%). 13 AE reported. Most common: diarrhea (n=3), headache (n=2), somnolence (n=2) |
|
Tolia et al 2010 (ref) |
EE healing and symptom improvement. Children 12-36 m with GERD. Diagnosis by clinic (PGA) and endoscopy |
Esomeprazole (8 w) 5 mg (n= 18, mean 21.8 m). 10 (56%) EE (28% LA grade A, 28% LA grade B). Baseline PGA: 45% mild, 50% moderate, 5% severe |
Esomeprazole (8 w) 10 mg (n=13, mean 22.5 months). 5 (39%) EE (23% LA grade A, 8% LA grade B, 8% LA grade C) Baseline PGA: 20% mild, 80% moderate |
31 patients: EE: 15 (48.4%), control: 100% healed. Final PGA: 5 mg: 45% none, 50% mild, 5% moderate. 10 mg: 20% none, 65% mild, 15% moderate |
Most common AE: vomiting, pyrexia and diarrhea |
|
Baker et al 2010 (ref) |
GERD symptom improvement. Children 1-5 years: GSQ-YC >3 and endoscopic HE (Hetzel Dent grade ≤2) or EE (Hetzel Dent grade > 2). |
Pantoprazole (8 w) 0.3mg/kg (LD): n= 18, 2.7 years (+/-1.6) |
Pantoprazole (8 w): 0.6 mg/kg (MD): n= 21, 1.9 y (+/-1.2) 1.2 mg/kg (HD): n= 21, 2.8 y (+/-1.3) |
60 patients (56 HE, 4 EE). Improvement in WGSS (HE population, 8w): LD: P < 0.001, MD: P = 0.063, HD: P < 0.001 Endoscopic healing: 100% of EE population |
Most common AE: upper respiratory infection, fever, diarrhea, rhinitis, vomiting, headache |
|
Haddad et al 2013 (ref) |
Endoscopic healing at 12 w. Children 1-11 years endoscopically/histologically GERD (Hetzel-Dent ≥1 and Histological Features of Reflux Esophagitis scale >0) and at least one symptom of GERD | Rabeprazole (12 w) <15 kg (LW): 5 mg (n=21, 2.4 +/-1.2 years, H-D score 1.7+/-0.97) ≥ 15 kg (HW): 10 mg (n=44, 7.6 +/-2.9 years, H-D score 1.5+/-0.70) |
Rabeprazole (12 w) < 15 kg (LW): 10 mg (n=19, 1.9 +/-1.1 years, H-D score 1.4 +/-0.60) ≥ 15 kg (HW): 20 mg (n= 43, 7.0 +/- 0.7 years, H-D score 1.4+/-0.62) |
108 patients: 87 endoscopic healing. LW/5mg: 82%, LW/10mg:94% HW/10 mg:76%, HW/20 mg:78% Change of GERD symptoms Severity scores: LW/5mg: -13.6, LW/5mg:-9 HW/10 mg:-10.6, HW/20 mg:-8.3 |
76% of children at least 1 AE, 5% serious AE. Cough (14%), vomiting (14%), abdominal pain (12%), diarrhea (11%) |
|
Haddad et al 2014 (ref) |
Endoscopic healing at 24 w. Children 1-11 years with endoscopic healing at 12 w in previous study (Hetzel-Dent 0 and Histological Features of Reflux Esophagitis scale = 0) |
Rabeprazole (12 w) <15 kg (LW): 5 mg (n=9, 2.4+/-1.24 years) ≥ 15 kg (HW): 10 mg (n=24, 7.7 +/-2.74 years) |
Rabeprazole (12 w) <15 kg (LW): 10 mg (n=8, 1.5+/-0.53 years) ≥ 15 kg (HW): 20 mg (n=23, 7.2 +/- 2.66 years) |
52 patients, 47 (90%) endoscopic healing. LW/5mg: 100%, LW/10mg:100% HW/10 mg: 89%, HW/20 mg: 85% Change of GERD symptoms Severity scores: LW/5mg: -3.8, LW/5mg:-3.6 HW/10 mg: -2.6, HW/20 mg:-3.0 |
63% at least 1 AE (5% severe). Upper respiratory tract infection (63%), vomiting (11%), abdominal pain (8%), diarrhea (6%). 5% related to medication |
|
Grense et al 2018 (ref.) |
Treatment emergent adverse events and healing of EE. Adolescents 12-17 years with symptoms and endoscopically confirmed EE and healing with dexlansoprazole 60 mg /day (8w) |
Dexlansoprazole 30 mg 16 w treatment period (n= 22, 14.6 +/- 1.41 years, LA grade A 61.5%, grade B 34.6%, grade C 3.8%) |
Placebo 16 w treatment period (n= 24, 14.8 +/- 1.75 years, LA grade A 56.0 %, grade B 44 %, grade C 0 %) |
62 patients 16 w treatment period Healing: Dexlansoprazole 82 % : grade A 82%, grade B 82%. Placebo 58%: grade A 87 %, grade B 13 % |
72.0% (D), 61.5% (placebo). More common headache (24.0% D, 15.4% placebo). ≥ 5% D: abdominal pain, nasopharingitis, sinusitis, upper respiratory tract infection |
1 Abbreviations: AEs: adverse events; GERD: gastroesophageal reflux disease, EE: erosive esophagitis; PGA: Physician Global Assessment; w: weeks of treatment, LA: Los Angeles classification for erosive esophagitis, HE: histologic esophagitis, WGSS: weekly GERD symptom score, GSQ-YC: GERD Symptom Questionnaire for Young Children, LW: low weight cohort, HW: high weight cohort, D: dexlansoprazole, Y: years.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



