
Submitted:
01 February 2024
Posted:
02 February 2024
You are already at the latest version
Abstract
Sickle cell disease (SCD) is a pathophysiological condition of chronic hemolysis, oxidative stress, and elevated inflammation. The transcription factor Nrf2 is a master regulator of oxidative stress. Here we reported that the FDA-approved, oral agent simvastatin, an inhibitor of hydroxymethyl-glutaryl coenzyme A reductase, significantly activates the expression of Nrf2 and antioxidant enzymes. Simvastatin also induces fetal hemoglobin expression in SCD patient erythroid progenitors and a transgenic mouse model. Simvastatin alleviates SCD symptoms by decreasing hemoglobin S sickling, oxidative stress, and inflammation stress in erythroblasts. Particularly, simvastatin increases cellular levels of cystine, the precursor for the biosynthesis of antioxidant reduced glutathione and decreases the iron content in SCD mouse spleen and liver tissues. Mechanistic studies suggest that simvastatin suppresses the expression of critical histone methyltransferase, Enhancer of zeste homolog 2 to reduce both global and gene-specific histone H3 lysine 27 trimethylation. These chromatin structural changes promote the assembly of transcription complexes to fetal γ-globin and antioxidant genes regulatory regions, in an antioxidative response element-dependent manner. In summary, our findings suggest that simvastatin activates fetal hemoglobin and antioxidant protein expression and modulates iron and cystine/reduced glutathione levels to improve the phenotype of SCD and represents a therapeutic strategy for further development.
Keywords:
sickle cell disease
; simvastatin
; Nrf2
; Enhancer of zeste homolog 2
; histone methylation
; fetal hemoglobin
; oxidative stress
1. Introduction
Sickle cell disease (SCD) is an inherited hematological disorder caused by an A to T mutation in the adult β-globin gene leading to the production of adult hemoglobin S (HbS) which polymerizes under hypoxia conditions [1,2]. The polymerization of HbS is the primary event in the pathogenesis of SCD leading to chronic hemolysis, and oxidative stress which contribute to stress erythropoiesis [3,4,5,6,7], systemic hypoxia [8,9,10,11], and abnormal metabolic programming [12,13,14,15,16]. Although progress has been made recently, SCD treatment options remain limited. Two critical strategies to treat SCD include γ-globin gene reactivation and reversal of oxidative stress [17]. For decades, hydroxyurea was the only FDA-approved treatment option for SCD [18], until the recent approval of Endari (oral L-glutamine) [19], crizanlizumab [20] and voxoletor [21]. Long-term experience with hydroxyurea has shown improvement in the clinical course, primarily through fetal hemoglobin (HbF) induction, but about 30% of SCD patients are not responsive. By contrast, Endari reverses oxidative stress by increasing the NADH and NAD redox potential and decreasing endothelial adhesion of sickle red blood cells [22]. However, there are multiple sources of pro-oxidant events that contribute to the clinical phenotype of chronic systemic oxidative stress in SCD such as increased generation of free radicals [23,24], elevated mitochondrial respiratory chain activity [25,26], and blood cell auto-oxidation [27]. Therefore additional therapeutic agents are under development for treatment of SCD [28], mainly targeting HbF induction, anti-red blood cell adhesion, pain-alleviation, antioxidative stress, or anti-inflammation. Unfortunately, the complex pathophysiology of SCD makes it unlikely that a single agent will prevent all SCD complications [29,30].
The transcription factor Nrf2 (Nuclear factor (erythroid-derived 2)-like 2) is the master regulator of the cellular oxidative stress response, which regulates a variety of antioxidant genes [31]. Nrf2 expression is predominantly regulated at the protein level through three distinct signaling pathways comprised of KEAP1 (Kelch-like ECH-associated protein 1), Hrd1, and β-TrCP (β-transducin repeat-containing protein), which promote Nrf2 proteasomal degradation by different mechanisms. KEAP1 is the main regulator for Nrf2 degradation through direct protein interactions. Under resting conditions, Nrf2 is sequestered in the cytoplasm by KEAP1 and directed for ubiquitination by the E3 ligase complex. Multiple small chemical compounds such as tert-Butylhydroquinone (tBHQ), diethylmaleate, and 2-cyano-3,12-dioxo-oleana-1,9(11)-dien-28-oic acid (CDDO-Im) modify KEAP1 and disrupt its interaction with Nrf2, leading to Nrf2 nuclear translocation and antioxidant gene activation [32]. In addition, Hrd1- and β-TrCP mediate Nrf2 degradation, and pharmacologic inhibition of their expression by all-trans retinoic acid [33], LS-102 [34], SB216763 [35] and 2,4-dihydropyrano[2,3-c]pyrazoles [36] promote Nrf2 protein stability and subsequent activation of the antioxidation response. Of these three pathways, the KEAP1-Nrf2 interaction has been most extensively investigated for its role in erythropoiesis, iron hemostasis and heme metabolism through the expression of AMBP, ABCB6, FECH, HRG1, FTL, FTH1 [37] and two critical regulators of globin gene expression BCL11A and KLF1 [37,38].
Notably, genetic evidence has shown that Nrf2 activation can specifically mitigate the severity of hemolytic anemia, and systemic and local inflammation in transgenic SCD mice via suppressing the proinflammatory response and reduction of reactive oxygen species (ROS) stress [39,40]. We demonstrated that Nrf2 ablation exacerbates the symptoms of SCD by decreasing expression of antioxidant factors and the globin genes [41,42]. Indeed, Nrf2 was found to mediate γ-globin gene transcription in human normal and sickle erythroid progenitors [43] through binding the proximal promoter antioxidant response element (ARE) and locus control region hypersensitive sites to facilitate chromatin looping structure during erythropoiesis [44]. We further investigated the important role of Nrf2 in mediating the ferroptosis stress response in SCD erythroblasts and transgenic animal models. Nrf2 ablation induced iron overload in SCD and metabolic reprogramming to induce histone hypermethylation in erythroblasts and suppressed antioxidant genes to increase lipid oxidation [42]. These findings indicated that the Nrf2 signaling pathway contributes to the regulation of the globin genes and the antioxidant stress response during erythropoiesis.
To explore HbF induction and enhanced antioxidant capacity for SCD treatment through the Nrf2 signaling pathway, our group and others have conducted investigations to discover agents that mediated Nrf2 activation. However, the clinical trial of the Nrf2 activator Bardoxolone methyl (CDDO-Me) in patients with chronic kidney disease showed the development of adverse cardiovascular events [45,46]. Hitherto, the efficacy-toxicity profile generated by different Nrf2 activating drugs has unique pharmacokinetic, pharmacodynamic, toxicokinetic, and toxicodynamic profiles. Therefore, repurposing FDA-approved drugs as novel SCD treatment options has been our focus. Previously dimethyl fumarate (DMF), the methyl ester of fumaric acid that disrupts the interaction between Keap1 and Nrf2 was FDA-approved for the treatment of multiple sclerosis. We later demonstrated the ability of DMF to mediated Nrf2 release and nuclear-translocation to activate γ-globin and anti-oxidative genes [32].
Other agents such as simvastatin and t-butylhydroquinone can induce γ-globin gene transcription through Nrf2 activation in tissue culture systems [38,47]. Moreover, simvastatin is an inhibitor for hydroxymethyl-glutaryl coenzyme A reductase, which activates the PI3K/Akt pathway to suppress GSK-3 activity and Nrf2 stabilization [48,49]. In addition to activating the Nrf2 signaling pathway, simvastatin mediates chromatin modifications via inhibition of histone deacetylase and DNA methyltransferase [50]. Simvastatin was also found to reduce chromatin accessibility at transcriptional enhanced associate domain elements to repress endothelial-to-mesenchymal transition to confer protection against endothelial dysfunction [51]. Moreover, simvastatin was demonstrated to inhibit HDAC1/2 and induce histone hyperacetylation to promote p21 expression and regulate tumor growth [52,53]. Notably, the efficacy of statins in the treatment of type 2 diabetes was attributed partially to DNA hypomethylation at the DHCR24, FAM50B, SC4MOL, AHRR, and ABCG1 gene loci [54,55]. The statins can also reverse subtelomeric methylation status in age-related diseases such as diabetes and inhibit Smad 6 and Smad 7 induction in autoimmune diseases [56,57]. However, whether simvastatin facilitates a disease modifying effect in SCD and the molecular mechanism involved has not been studied.
In this study, we aim to demonstrate the effect of simvastatin to mitigate HbS sickling and ROS stress levels in SCD erythroblasts in vitro and in SCD transgenic mice. Our mechanistic studies demonstrate the ability of simvastatin to upregulate Nrf2 signaling and silence enhancer of zeste homolog 2 (EZH2)-regulated histone methylation in mediating chromatin structure modifications to activate γ-globin and antioxidant gene transcription. Our findings support the development of the FDA-approved drug, simvastatin as a therapeutical option for treating SCD.
2. Materials and Methods
2.1. Chemicals and Reagents
Hydroxyurea (HU), dimethyl fumarate (DMF), dimethyl sulfoxide (DMSO), and H2O2 were obtained (Sigma-Aldrich, St. Louis, MO). Simvastatin (SIM) was purchased from Thermo Fisher Scientific (Hampton, NH).
2.2. Culture of Human SCD Patient Erythroblasts and H2O2 Exposure
Erythroid progenitors were generated from CD34+ stem cells isolated using microbeads selection of SCD patients peripheral blood mononuclear cells [44]. The anonymous collection of discarded blood samples from SCD patients undergoing chronic transfusion was classified as exempt by the Institutional Review Board at Augusta University and did not require informed consent. SCD patient CD34+ cells were cultured in a modified Fibach two-phase liquid culture system to generate erythroblasts at different stages of maturation [58]. Briefly, during phase 1, cells were grown in Iscove’s Modified Dulbecco medium with 15% fetal bovine serum, 15% human AB serum, 10 ng/mL interleukin-3, 50 ng/mL stem cell factor and 2 IU/mL erythropoietin (EPO; Sigma-Aldrich, St. Louis, MO). Phase 2 was initiated on day 7 with a similar medium without stem cell factor and interleukin 3. Chemical treatment of SCD erythroblasts was conducted on day 10 of culture and analyzed on day 12. Treatment with H2O2 at 40 µM for 8 h was completed where indicated, along with the different chemical treatments.
2.3. Animal Treatment
The preclinical Townes SCD mouse model (B6;129-Hbatm1(HBA)TowHbbtm2(HBG1,HBB*)Tow/Hbbtm3(HBG1,HBB)Tow/J) was characterized previously [59]. The experiments using the SCD mouse model were performed after approval by the Augusta University Institutional Animal Care and Use Committee. Two to three-month-old SCD mice (both sexes) were treated by intraperitoneal injections of HU (50 mg/kg), DMF (50 mg/kg), SIM (7.5 mg/kg), or water daily, 5 days a week for 4 weeks. Peripheral blood was drawn at week 0, 2 and 4. At the end of the treatment, mice were euthanized, spleen and liver were harvested, snap frozen, and stored for iron, NADPH, NADP+, GSSG, and GSH levels or fixed with 1% formaldehyde for tissue pathology analysis.
2.4. Complete Blood Count and Differential
Peripheral blood was collected in BD Vacutainer EDTA tubes by tail bleeding and automated complete blood count and differentials were completed on the Micros 60 CS/CT machine (HORIBA Medical/ABX Diagnostics, Irvine, CA) according to the manufacturer′s protocol.
2.5. Isolation of Mouse Spleen CD71+ Erythroblasts
Single-cell suspensions of SCD mouse spleen were prepared and CD71+ erythroblasts isolated after labeling with biotinylated CD71 antibody followed by streptavidin MicroBeads separation with MS Columns (Miltenyi Biotec, Auburn, CA) as we previously reported [42]. The single cells were processed for RNA, protein, and chromatin analysis.
2.6. Cell Proliferation and Viability
SCD erythroblasts at day 10 of culture were seeded at a density of 5 × 105 cells/ml in Phase 2 complete culture medium and treated with indicated concentrations of chemicals. On day 12 of the culture, cells were collected and evaluated for viability by trypan blue staining.
2.7. Flow Cytometry Analysis
Flow cytometry was performed to measure ROS using 2′-7′-dichlorodihydrofluorescein diacetate (DCFH-DA) (Invitrogen, Waltham, MA) staining. Cells were incubated with 10 μM DCFH-DA in complete culture medium for 30 min, washed twice with phosphate buffered saline, and ROS levels measured by flow cytometry analysis.
To measure the percentage of HbF expressing cells (%F-cells), erythroblasts were fixed with 1% formaldehyde, permeabilized with 0.4% Triton X100 and stained with FITC anti-HbF antibody (Supplemental Table S1); isotype control IgG was used to detect non-specific staining. To measure the percentage of %F-cells in mouse peripheral blood, samples were fixed with 0.1% glutaraldehyde and permeabilized before staining with isotype control or FITC-HbF antibodies similarly.
2.8. RBC Sickling Analysis
In vitro RBC sickling analysis was performed as previously published [43]. Briefly, Day 12 SCD erythroblasts with different chemical treatments were cultured under hypoxic conditions (1% O2, 5% CO2) for 14 h and fixed with 4% formaldehyde before moving to normal air. Using light microscopy, the number of sickle red blood cells was quantified by changes in cell morphology. Bright field images at 20× magnification were obtained on an EVOS Cell Imaging system (Thermo Fisher Scientifics, Hampton, NH). Areas were randomly selected where a single layer of erythrocytes were observed, and 500 cells/per treatment condition were counted in triplicate and the percentage of sickle cells calculated based on total red blood cells counted [60].
2.9. Quantitative RT-PCR
Total RNA was extracted from cells using Trizol (Invitrogen, Waltham, MA), reverse transcribed, and analyzed by quantitative PCR (qPCR) using gene-specific primers (Supplemental Table S2) with SYBR Green Supermix (Biorad). Relative levels of gene expression for both target and reference genes were calculated by the 2-ΔΔCt method based on Ct values. Data were presented as the mean ± standard deviation (SD) of fold-change in expression. All mRNA levels were normalized to endogenous β-actin expression.
2.10. Western Blot Analysis
The whole cell extracts from cultured SCD erythroblasts or isolated SCD mouse spleen CD71+ cells were prepared in RIPA buffer with protease inhibitors (Sigma-Aldrich, St. Louis, MO). For histone extract preparation, cells were homogenized in Triton extraction buffer (PBS containing 0.5% Triton X-100 and 2 mM phenylmethylsulfonyl fluoride) for nuclei isolation, and nuclear proteins were prepared by 0.2 N HCl acid extraction followed by neutralization with 1/10 volume of 2 M NaOH. Protein concentrations of the whole-cell and histone extracts were determined using the Bradford assay.
Whole-cell protein extract (30 μg) or histone extract (1 μg) were denatured, subjected to SDS-PAGE, and transferred to nitrocellulose membranes. After blocking with 5% nonfat dry milk in Tris-buffered saline and 0.1% Tween (TBS-T), the membranes were incubated with the indicated antibodies overnight at 4oC. β-actin and histone H3 were used as loading controls. After 1 h incubation with horseradish peroxidase-conjugated anti-Mouse or anti-Rabbit secondary antibodies (Santa Cruz Biotechnology, Dallas, TX), the membrane was washed and visualized by chemiluminescence in a FUJIFILM LAS-3000 system or GE Amersham ImageQuant 800 and quantified with ImageJ software.
2.11. GSH and GSSG Assay
The levels of reduced (GSH) and oxidized (GSSG) glutathione were measured using a GSH/GSSG-Glo™ Assay Kit (Promega, Madison, WI). Briefly, cultured SCD erythroblasts were washed with PBS once and three times of freeze-thaw out in ice-cold PBS containing 2 mM EDTA. The extracts were centrifuged, and the supernatant was collected and used immediately for the assay according to the manufacturer’s instructions. Luminescence was read by a Victor3 Multilabel Counter (Perkin Elmer, Waltham, MA) and GSH and GSSG levels normalized to cell numbers.
2.12. NQO1 Activity Assay
The cultured SCD erythroblasts were washed twice with PBS and assessed for NQO1 activity in whole cell extracts following reduction of menadione with cofactor NADH and WST1. The samples were assayed at 440 nm absorbance using a NQO1 Activity Assay Kit (Abcam, Waltham, MA), according to the manufacturer’s instructions. The NQO1 activity was normalized to protein content.
2.13. Measurement of Intracellular Cysteine Levels
Day 12 cultured erythroblasts were harvested, washed with PBS buffer once, and resuspended in distilled water. The intracellular amino acids were extracted by boiling for 10 min. The supernatant was collected after centrifugation and protein content was determined. The levels of cysteine in the supernatant were measured by a Cysteine Assay Kit (Sigma-Aldrich, St. Louis, MO) along with the cysteine standards. Cysteine levels after different treatments were compared after normalization to cell numbers.
2.14. Cystine Uptake Assay
The cystine uptake assay was conducted with BioTracker Cystine-FITC Live Cell Dye (Sigma, St. Louis, MO). Briefly, SCD Day 10 erythroblasts were cultured in a complete IMDM medium with cytokines and treated with DMSO or simvastatin for 48 h. Cystine-FITC was added to cultured SCD erythroblasts at 200 µM for 45 min allowing uptake then the cells were collected and washed followed by quantification of cellular levels of Cystine-FITC by flow cytometry analysis.
2.15. EZH2 Gene Knockdown Analysis
On day 2 of culture, SCD progenitors were transduced with lentiviral EZH2 shRNA particles and selected with puromycin until analysis. Two different shRNAs targeting sequences including ugacuucugugagcucauugc and guuuguuggcggaagcgugua (Supplemental Table S2) were constructed in pLKO.1 (Addgene, Watertown, MA, USA). A standard scramble sequence (shControl) targeting a nonspecific sequence ccuaagguuaagucgcccucg was used as a control. The shEZH2 knockdown efficacy was determined by Western blot analyses.
2.16. Chromatin Immunoprecipitation (ChIP)
ChIP assays were performed with indicated antibodies (Supplemental Table S1) using gene-specific primers (Supplemental Table S2) as previously reported with minor modifications [44,61]. Samples were immunoprecipitated with anti-NRF2, anti-TATA binding protein (TBP), anti-RNA polymerase II (Pol II), and H3K27Me3 antibodies (Supplemental Table S1). ChIP DNA was quantified by qPCR with gene locus specific primers to determine the pull-down signals. Rabbit normal IgG was used as a non-specific antibody control.
2.17. NADP+/NADPH Levels
Mouse spleen CD71+ cells (2x10^6) were washed with ice-cold PBS and homogenized in NADP or NADPH extraction buffer before being assayed with EnzyChrom™ NADP/NADPH Assay Kit (BioAssay Systems, Hayward, CA) according to the manufacturer’s instructions. The extracts were heated at 60oC for 5 min and then 20 μl of assay buffer and 100 μl of opposite extraction buffer was added to neutralize the extracts. The levels of NADP+/NADPH in the supernatant were determined by adding enzymes provided in the kit. Absorbance at 570 nm was measured according to the manufacturer’s instructions using a Synergy H1 hybrid plate reader (Biotek, Winooski, VT) to calculate NADP+/NADPH concentrations.
2.18. Histology, Immunohistochemistry, and Image Analysis
Mouse spleen and liver tissues were fixed in 10% neutral buffered formalin, dehydrated, and embedded in paraffin. Tissue sections (5 μm thickness) were subjected to hematoxylin and eosin (H&E) staining and subsequent Prussian blue staining (IHCworld, Ellicott City, MD) to visualize iron deposition.
2.19. Iron Content
Approximate 20 mg of mouse spleen and liver tissues were homogenized in 1 ml of distilled water and supernatants were collected by centrifugation at 4OC. The iron content in the supernatant was measured by an Iron assay kit (Bioassay Systems, Hayward, CA) and iron levels were normalized to protein content.
2.20. Statistical Analysis
Data from at least three independent biological replicates were reported as the mean ± SD. Statistical differences were determined by an unpaired Student’s t-test or by two-way ANOVA with the corresponding two-tailed significance (p value) determined. Statistical analysis was performed using GraphPad Prism 9 software (GraphPad Software Inc., San Diego, CA) and differences were considered significant at p < 0.05.
See Supplemental Materials for additional methods.
3. Results
3.1. Simvastatin Activates γ-Globin Gene Expression and Reverses Sickling of SCD Erythroblasts
Human sickle erythroid progenitors were cultured in a two-phase culture system (Figure 1A). On Day 10 of culture, cells were treated with DMSO (0.05%) control, HU, DMF, and simvastatin at different concentrations for 48 h. Untreated cells (UT) were also set aside for control. We first determined cell cytotoxicity and growth under the different conditions. HU (50 μM), DMF (100 μM), and SIM (5-10 μM) showed no cytotoxicity but suppressed cell growth, compared to UT or DMSO controls. Although SIM at lower concentrations did not affect cell growth or viability, SIM at 20 μM reduced both cell growth and viability in SCD erythroblasts (Supplemental Figure S1).
We next determined the effect of SIM on the production of fetal hemoglobin (HbF) and adult sickle hemoglobin (HbS) protein. Although at the lowest concentration of 2.5 μM SIM slightly induced HbF level, at higher concentrations of SIM (5-20 μM), HbF expression was significantly increased from 1.6- to 1.9-fold (Figure 1B); by contrast, HbS expression was not affected by SIM treatment. The percentage of HbF expressing cells (F-cell%) were measured in parallel by flow cytometry. In agreement with the Western blot data, F-cell% is increased significantly with higher concentrations of SIM (5-20 μM) to 26%-40%, an effect similar to HU and DMF treatments, compared to that of 22% F-cells with DMSO treatment (Figure 1C, D).
To further determine whether SIM could mediate an anti-sickling effect, SCD erythroblasts were incubated under hypoxia with different drug treatments. Similar to the effect of HU and DMF treatment, SIM produced anti-sickling effects, decreasing the number of sickled cells by 30-35%, compared to DMSO and UT controls (Figure 1E, F). Together, these findings suggest that SIM induces HbF expression to modify the phenotype of sickle erythroblasts.
3.2. Simvastatin Increases the Expression of NRF2 and Antioxidant Proteins
Previously, SIM was shown to upregulate NRF2 expression [38]. Recently, we demonstrated the important role of NRF2 in regulating the sensitivity of SCD erythroid cells to ferroptosis in vitro and mouse models of SCD. To extend these findings to sickle cells under oxidative stress, we first determined NRF2 levels in SCD erythroblasts treated with different concentrations of SIM. A significant dose-dependent increase in NRF2 expression, similar to that produced by the known classical Nrf2 inducer DMF, was observed (Figure 2A). In addition, the expression of classic downstream targets of Nrf2 such as antioxidant proteins NAD(P)H dehydrogenase [quinone] 1 (NQO1), catalase (CAT), glutamate-cysteine ligase modifier subunit and catalytic subunit (GCLM and GCLC), and SLC7A11 were significantly increased at both the mRNA and protein levels by SIM in a dose-dependent manner (Figure 2). Notably, GCLC and GCLM are critical for the biosynthesis of oxidated GSH while SLC7A11 mediated the transport of cystine for GSH generation. Together, these results support the ability of SIM to induce the Nrf2 signaling pathway to activate transcription of γ-globin and antioxidant genes.
3.3. Simvastatin Enhances SCD Erythroblasts Antioxidative Capacity
We next determined whether induction of Nrf2 signaling by SIM would affect the antioxidant capacity. SCD erythroblasts were treated with 40 μM of H2O2., which suppressed cell viability by about 20%; however, this suppression was rescued by simultaneous SIM treatment (Figure 3A). To investigate the effects of SIM on SCD erythroblast antioxidant capacity, we measured cellular reduced glutathione (GSH) and oxidative glutathione (GSSG) levels. Simvastatin significantly increased cellular GSH levels but did not affect GSSG, resulting in a higher ratio of GSH/GSSG (Figure 3B-D). Likewise, SIM increased NQO1 protein levels in a dose-dependent manner (Figure 3E).
Importantly, the availability of cysteine and its oxidative form cystine in the culture media contribute to the biosynthesis of GSH. A depletion of cystine in culture media led to significantly reduced levels of GSH and increased oxidative stress. Whether SIM affects cystine levels required for GSH synthesis is not known. To determine an effect of SIM on cystine levels, we treated erythroblasts with 5 µM SIM, and found significantly increased cystine levels by 40.4% (Figure 3F). To evaluate whether SIM affects cellular cystine uptake, we conducted a BioTracker Cystine-FITC assay by flow cytometry and found that SIM increased cystine uptake by 38.6% (Figure 3G). Together, these findings suggest that SIM can increase cystine uptake to promote an antioxidative effect.
3.4. Simvastatin Attenuates EZH2 expression and Histone H3K27Me3 to Modify Chromatin Structure in Gene Regulation
Previously, SIM was shown to downregulate histone lysine K27 trimethylation (H3K27Me3) through EZH2 and histone acetylation in a context-dependent manner [62,63]. To investigate whether SIM affects histone modifications in SCD erythroblasts, we determined global histone H3K27Me3 and histone H3 acetylation levels. Interestingly, though we did not detect an effect of SIM on histone acetylation, the level of the H3K27Me3 mark was significantly reduced (Figure 4A). Importantly, H3k27Me3 is regulated by the histone demethylases KDM6a/b and methyl transferases EZH1/2 [64], however, we did not detect changes in KDM6a/b or EZH1 mRNA levels after SIM treatment (Figure 4B). By contrast, a significant reduction of EZH2 expression was detected (Figure 4A), suggesting that EZH2 is the downstream factor facilitating the ability of SIM to mediate histone H3K27Me3 modifications.
3.5. EZH2 Regulates NRF2 Expression to Modify ARE Motif Chromatin Structure on Target Genes
Whether the global effects of SIM on H3K27Me3 levels will also affect NRF2 expression was subsequently determined. We knocked down EZH2 gene expression by shRNA which significantly decreased protein levels, along with reduced levels of H3K27Me3 (Figure 5A), confirming the methyl transferase activity of EZH2. By contrast, the level of NRF2, HbF, and antioxidant proteins NQO1, CAT, GCLM, and HMOX1 were significantly increased in shEZH2 cells (Figure 5A).
Since NRF2 regulates antioxidant genes through ARE motif binding, we evaluated whether SIM effected antioxidant gene expression through EZH2-mediated Nrf2 regulation. By ChIP assay, the chromatin structure in ARE motifs of individual genes was determined. We observed that SIM treatment significantly increased NRF2 binding to the ARE motifs of different target genes, along with increased association of TBP and Pol II but decreased H3K27Me3 (Figure 5B-E). Together, these findings suggest that one mechanism involved in EZH2 to control the expression of NRF2 expression and its downstream target genes is mediated through H3K27Me3 chromatin modifications.
3.6. In Vivo Treatment with Simvastatin Suppresses H3K27Me3 Modification in SCD Mice
The in vitro findings support SIM mediated γ-globin gene activation in SCD erythroblasts. To expand these results in vivo, we determined the ability of SIM to alter the SCD phenotype, using preclinical SCD mice treated with SIM (7.5 mg/kg) by daily intraperitoneal injects, 5 days a week for 4 weeks (a dose comparable to 5 μM SIM concentration used in vitro). We first determined the hematological parameters of SCD mice under treatment conditions for which we did not observe significant changes between SIM treatment and vehicle control, except for red blood counts (Supplemental Figure S2). However, F-cell% was remarkably increased in SCD mice treated with SIM, compared to vehicle controls (Figure 6A).
We next quantified histone and globin protein levels by Western blot of CD71+ erythroid cells isolated from spleen tissue. In vivo treatment with SIM decreased H3K27Me3 levels by 40.2% (Figure 6B), in agreement with in vitro findings. Moreover, SIM induced HbF protein and its coding gene HBG1 mRNA transcript levels but had no effects on the expression of HbS protein or its coding gene HBA mRNA transcript levels (Figure 6B, C), suggesting a gene specific effect of SIM.
To further investigate the in vivo chromatin structure effect by SIM, we conducted ChIP assays with SCD mouse spleen CD71+ cells. Of note, reduced H3K27Me3 levels were detected in the HBG1 promoter after SIM treatment, compared to vehicle treatment control mice. In contrast, we did not observe differences for H3K27Me3 levels in the HBA gene promoter after SIM treatment (Figure 6D). Moreover, the association of TBP and Pol II in the promoter of the HBG1 gene, but not that of the HBA gene, was evidently increased (Figure 6D). These data support the ability of SIM to regulate H3K27Me3 modifications and chromatin structure as part of the mechanism of HBG1 gene activation.
3.7. Simvastatin Protects against Organ Damage from SCD
The most common manifestation of SCD organ damage is splenomegaly along with liver and kidney damage, and increased iron deposition. Therefore, we examined these tissues to determine the effects of chronic SIM treatment on tissue phenotype. We observed significantly reduced spleen and liver sizes when normalized by body weight (Figure 7A, B). Spleen tissue staining by H&E for the vehicle and SIM treated SCD mice exhibited marked histological disorganization and notable reduction in white pulp and expanded red pulp (Figure 7C). Iron staining by Prussian blue showed SIM reduced iron content by 39.1% (p < 0.05) suggesting less hemolysis in the spleen, compared to vehicle controls (Figure 7D).
Likewise, there was structural liver damage and a substantial increase in iron for the vehicle treated SCD mice by H&E and Prussian blue staining respectively (Figure 7E). By contrast, chronic SIM treatment significantly improved liver structure with increased cell proliferation and reduced iron deposits by 22.9% (p < 0.05), compared to vehicle controls (Figure 7E-F).
3.8. Simvastatin Reduces ROS Levels and Inflammatory Stresses in Preclinical SCD Mice
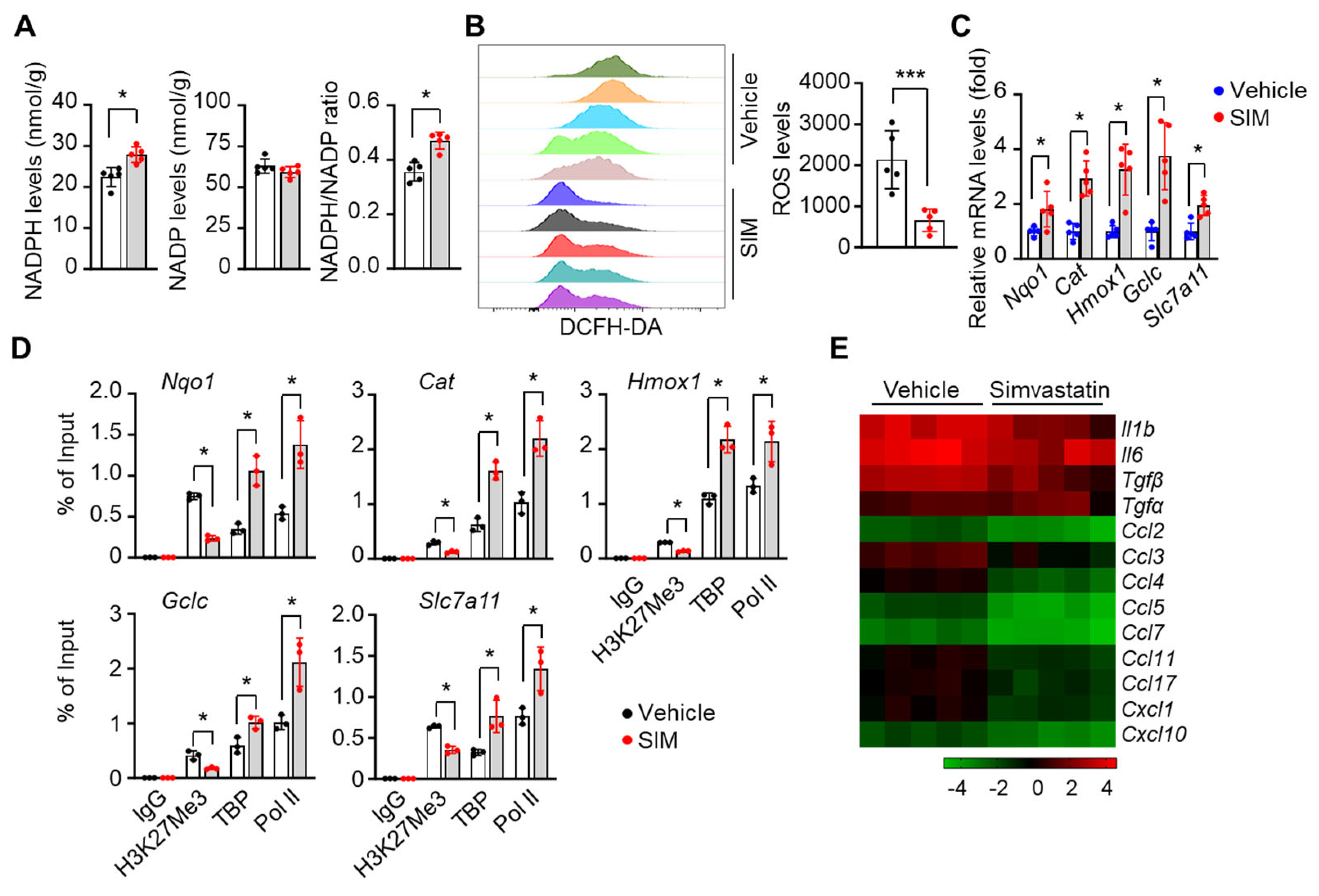
We next determined whether SIM affects ROS stress levels in spleen CD71+ erythroid cells. First, quantification of cellular NADPH, NADP content and their ratio showed that SIM increased NADPH levels by 24.3% and elevated the NADPH/NADP ratio by 32% (p<0.05) (Figure 8A). Furthermore, ROS levels determined by H2DCFDA flow cytometry showed that SIM reduced peripheral blood red cell ROS levels by >70% (p<0.01) (Figure 8B). Notably, the expression of Nrf2 targets Nqo1, Cat, Hmox1, Gclc, and Slc7a11 was manifestly increased after in vivo SIM treatment (Figure 8C). To further demonstrate that SIM upregulates antioxidant genes, we determined the chromatin structure in regulatory regions by ChIP assay. Consistent with the in vitro findings, SIM reduced the association of repressive H3K27Me3 marks in the promoters of Nqo1, Cat, Hmox1, Gclc, and Slc7a11 gene loci (Figure 8D).
It is well-established that chronic hemolysis in SCD leads to increased free heme levels and inflammation [1,2], whereas Nrf2 activator such as DMF has been shown to alleviate the inflammatory and oxidative stress [65]. Therefore, we determined the ability of SIM to suppress the expression of pro-inflammatory factors. Interestingly, a heatmap depiction shows the mRNA transcript levels of inflammatory factors were decreased by 47.5%-82.7% (p<0.05) except Tgfα which showed a 29.4% increase (p>0.05) (Figure 8E). Nevertheless, RNA transcription profiles support an in vivo anti-inflammatory effect of chronic SIM treatment.
4. Discussion
Sickle cell disease is produced by a single nucleotide mutation in the adult β-globin gene leading to HbS synthesis and polymerization under hypoxia conditions, resulting in intravascular hemolysis, cell adhesion, vascular occlusion, and ischemia–reperfusion injury from elevated oxidative stress. In addition to multiple approaches for γ-globin activation [17,28], other strategies to treat SCD include targeting the downstream long-term effects by reducing oxidative stress, cellular adhesion mediated by P-selectin interactions and increasing hemoglobin oxygen affinity to directly block HbS polymerization. These four strategies have the potential to inform drug combinations to best treat the clinical complications and severity of individual with SCD. In this study, we have chosen to explore the possibility of repurposing the novel FDA-approved agent SIM, which stabilized Nrf2 protein levels and γ-globin activation by creating open chromatin domains, and antioxidant and anti-inflammatory effects.
In the current study, we performed mechanistic studies which showed that SIM decreased global and gene loci specific H3K27me3 levels to affect heterochromatin for gene regulation in SCD erythroblasts (grown in culture) and SCD transgenic mice treatment in vivo. This effect of SIM facilitated an activation of the γ-globin and antioxidant genes at the mRNA and protein levels to reduce red blood cell sickling and ROS stress, demonstrating its dual effect in modifying phenotypic severity of SCD. Depending on the cellular environment, SIM can produce antioxidant effects by increasing the levels of reduced GSH such as in liver [66], generate an pro-oxidative stress in malignant conditions [67], or show no effect on oxidative stress regulation in healthy subjects [68]. Here we demonstrated that SIM promotes cellular uptake of cystine, the precursor for GSH biosynthesis, through Slc7a11 upregulation. In addition, both the catalytic (GCLC) and mediator (GCLM) subunits of the glutamate–cysteine ligase were upregulated by SIM to accelerate GSH biosynthesis and scavenging of ROS stress. Together, our findings and previous observations suggest a cellular environment-dependent effect of SIM in regulating oxidative stress.
Previously, SIM was shown to inhibit histone deacetylase activity specifically targeting HDAC1/2 at a comparable capability to well-studied HDAC inhibitors such as Trichostatin A and suberoylanilide hydroxamic acid [52,69,70]. Simvastatin also mediates induction of histone acetylation by activating the AMPK signaling pathway [63,71]. These HDAC inhibit functions of SIM affects the expression of genes whose products participate in cell proliferation. In addition, SIM modifies the expression of key epigenetic proteins such as DNMT1 and influences DNA methylation to regulate gene transcription [72,73]. Our results in SCD erythroblasts showed that SIM did not change histone acetylation levels, however, SIM reduced the suppressive histone code H3K27Me3, through EZH2 activation, but not through EZH1 or the histone demethylases KDM6a/b. Although we did not explore the mechanism of SIM-mediated reduction of EZH2, a previous study supports the ability of SIM to inhibit the function of METTL3 in downregulating EZH2 signals [74]. Those previous reports suggest cellular environment-specific mechanisms of SIM regulating histone modifications [75]. Of note, we previously showed that Nrf2 mediates metabolic reprogramming in erythroblasts to modify levels of the metabolite L-2-hydroxyglutarate, which is a competitor of α-ketoglutarate-dependent histone demethylases and thus regulating histone methylation [42]. Since we demonstrated that SIM enhances Nrf2 levels, our results raise the question whether SIM could affect metabolic profiling, histone methylation and gene expression through the Nrf2 signaling pathway in SCD erythroblasts. Future work will focus on answering this question.
From ChIP assay analysis using primers spanning the gene-specific ARE motifs, our results support Nrf2 activation and binding to target ARE motifs to activate downstream target γ-globin and antioxidant genes through EZH2 suppression by SIM to produce an open chromatin structure and increase binding of the general transcription factors, TBP and RNA Pol II. Previously, Nrf2 was shown to produce ARE-independent effects in regulating the expression of inflammatory factors, through binding to the proximity of the interleukin-6 and interleukin-1β genes to inhibit RNA Pol II recruitment and gene transcription in macrophages [76]. Though we are not able to exclude Nrf2 binding to regions devoid of ARE motifs to mediate γ-globin and antioxidant genes transcription, SIM reduced global and loci-specific H3K27Me3 levels, which led to chromatin structure changes at ARE motifs and other regions as supported by increased TBP and Pol II binding to promote gene transcription.
Related to the molecular function of EZH2, previous studies have shown the ability of EZH2 to act as a corepressor in cooperation with BCL11A, to achieve γ-globin gene silencing [77]. Indeed, EZH2 is broadly distribute at high levels across the HBB locus in non-erythroid cells compared to erythroid cells, suggesting its general suppressive effect on globin gene transcription [78]. Moreover, the EZH2 inhibitor Tazemetostat can significantly increase fetal hemoglobin expression in healthy and β-thalassemic human primary erythroid cells [79]. Therefore, those observations and our finding of SIM-mediated EZH2/H3K27Me3 suppression to activate γ-globin transcription could expand treatment options for SCD by inhibiting EZH2 expression.
In addition to activating HbF and antioxidant proteins, SIM suppressed pro-inflammatory signals in the SCD mouse model, which is in agreement with previous findings from human SCD clinical trials, where SIM administration reduced markers of inflammation and frequency of vaso-occlusive pain [80]. In a single center pilot study of adolescents and adults with SCD, SIM treatment for up to 3 months led to a dramatic reduction in the rate of SCD related pain and oral analgesic use; there was also improvement in soluble biomarkers of inflammation and an acceptable safety profile [81]. Inflammation and oxidative stress occur in chronic diseases and are closely correlated to each other, and mutually influenced. Therefore, the failure of antioxidant drug trials might result from failure to select appropriate agents that will target inflammation, and vice versa [82], whereas targeting both inflammation and oxidative stress simultaneously might generate synergistic effects. Importantly, oxidative and inflammatory stresses result from HbS polymerization and chronic hemolysis in SCD, therefore SIM has the potential to produce a three-fold effect including HbF induction, and inflammation and oxidative stress reduction to ameliorate the clinical severity of SCD.
A recent meta-analysis showed that statins can significantly decrease serum ferritin levels, which might be beneficial for the prevention and progression of atherosclerotic cardiovascular disease [83]. Indeed, iron overload causes inflammation and iron-dependent non-apoptotic cell death, i.e. ferroptosis. Individuals with SCD often suffer iron overload due to frequent blood transfusions, eventually requiring treatment with chelating agents to prevent liver and heart toxicity [84]. Our in vivo studies in SCD mice showed that SIM reduced the iron content in spleen and liver tissues. However, a link between chronic SIM use and iron deficiency was detected in humans [85]. Iron reduction by SIM is through the regulation of iron metabolism by HMOX1 expression [86]. We also observed an increase in HMOX1 expression in SCD mice treated chronically with SIM. Although at the SIM dose of 7.5 mg/kg/day, we did not observe adverse effects in SCD mice treated up to 4 weeks, a lower dose of SIM might be more beneficial and should be evaluated.
5. Conclusions
In conclusion, our study presents compelling evidence for the ability of SIM to activate γ-globin gene transcription and decrease red cell sickling, oxidative stress, and inflammation. Importantly, our study indicates that through regulating histone H3K27Me3 levels and modifying EZH2 expression, SIM affects histone methylation status to alter chromatin structure and Nrf2 binding to regulate gene expression. This chromatin modification promotes the assembly of transcription complexes on the fetal γ-globin and antioxidant genes. Moreover, our findings support the ability of SIM to modulate iron and cystine/GSH levels while decreasing pro-inflammatory signals. Lastly, in vivo experiments demonstrated that SIM treatment improved phenotypic characteristics in preclinical SCD mice, suggesting potential therapeutic benefit.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. List of antibodies. Table S2. List of DNA oligonucleotides. Figure S1. Effects of γ-globin inducers on cellular proliferation and viability of SCD erythroblasts. Figure S2. Peripheral blood hematological parameters of SCD mice treated with simvastatin. Figure S3. Uncropped Western blot images.
Author Contributions
Conceptualization, C.X., B.S.P. and X.Z.; Data curation, C.X., C.P. and M.T.; Formal analysis, C.X., C.P.; H.S., A.H. and B.S.P.; Funding acquisition, B.S.P. and X.Z.; Investigation, C.X., C.P. and M.T.; Methodology, C.X., C.P. and M.T.; Project administration, X.Z.; Resources, A.H.; Supervision, X.Z.; Writing – original draft, C.X. and C.P.; Writing – review & editing, B.S.P. and X.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Institutes of Health (NIH) National Institute of Diabetes and Digestive and Kidney Diseases R01DK119762 and R01DK139694 (X.Z.), Augusta University Intramural Pilots Project (IGPP00055) (X.Z. and B.P.), and National Heart, Lung, and Blood Institute R01HL149365 (B.P.).
Institutional Review Board Statement
All animal care and handling procedures in the present study were performed in accordance with the guidelines of the Institutional Animal Care and Use Committee at Augusta University (Approval numbers 2016-0830 and 2019-1010).
Data Availability Statement
All relevant data are within the manuscript and the Supplementary Materials. Any additional information required to re-analyze the data reported in this paper is available from B.P. and X.Z. upon request.
Acknowledgments
The authors thank the pediatric SCD patients and nurses for blood samples contributions and collections respectively.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rodgers, G.P.; Walker, E.C.; Podgor, M.J. Mortality in sickle cell disease. N Engl J Med 1994, 331, 1022–1023. [Google Scholar] [CrossRef]
- Rees, D.C.; Williams, T.N.; Gladwin, M.T. Sickle-cell disease. Lancet 2010, 376, 2018–2031. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.J.; Krishnamurti, L.; Kutok, J.L.; Biernacki, M.; Rogers, S.; Zhang, W.; Antin, J.H.; Ritz, J. Evidence for ineffective erythropoiesis in severe sickle cell disease. Blood 2005, 106, 3639–3645. [Google Scholar] [CrossRef] [PubMed]
- Chirico, E.N.; Pialoux, V. Role of oxidative stress in the pathogenesis of sickle cell disease. IUBMB Life 2012, 64, 72–80. [Google Scholar] [CrossRef]
- Silva, D.G.H.; Belini Junior, E.; de Almeida, E.A.; Bonini-Domingos, C.R. Oxidative stress in sickle cell disease: An overview of erythrocyte redox metabolism and current antioxidant therapeutic strategies. Free Radic Biol Med 2013, 65, 1101–1109. [Google Scholar] [CrossRef]
- Nur, E.; Biemond, B.J.; Otten, H.M.; Brandjes, D.P.; Schnog, J.J.; Group, C.S. Oxidative stress in sickle cell disease; pathophysiology and potential implications for disease management. Am J Hematol 2011, 86, 484–489. [Google Scholar] [CrossRef]
- Zhao, B.; Mei, Y.; Yang, J.; Ji, P. Erythropoietin-regulated oxidative stress negatively affects enucleation during terminal erythropoiesis. Exp Hematol 2016, 44, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Iampietro, M.; Giovannetti, T.; Tarazi, R. Hypoxia and inflammation in children with sickle cell disease: Implications for hippocampal functioning and episodic memory. Neuropsychol Rev 2014, 24, 252–265. [Google Scholar] [CrossRef]
- Kaul, D.K.; Hebbel, R.P. Hypoxia/reoxygenation causes inflammatory response in transgenic sickle mice but not in normal mice. J Clin Invest 2000, 106, 411–420. [Google Scholar] [CrossRef]
- Wu, H.; Bogdanov, M.; Zhang, Y.; Sun, K.; Zhao, S.; Song, A.; Luo, R.; Parchim, N.F.; Liu, H.; Huang, A.; et al. Hypoxia-mediated impaired erythrocyte Lands′ Cycle is pathogenic for sickle cell disease. Sci Rep 2016, 6, 29637. [Google Scholar] [CrossRef]
- Sun, K.; Xia, Y. New insights into sickle cell disease: A disease of hypoxia. Curr Opin Hematol 2013, 20, 215–221. [Google Scholar] [CrossRef]
- Ogunsile, F.J.; Bediako, S.M.; Nelson, J.; Cichowitz, C.; Yu, T.; Patrick Carroll, C.; Stewart, K.; Naik, R.; Haywood, C., Jr.; Lanzkron, S. Metabolic syndrome among adults living with sickle cell disease. Blood Cells Mol Dis 2019, 74, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Smiley, D.; Dagogo-Jack, S.; Umpierrez, G. Therapy insight: Metabolic and endocrine disorders in sickle cell disease. Nat Clin Pract Endocrinol Metab 2008, 4, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Darghouth, D.; Koehl, B.; Madalinski, G.; Heilier, J.F.; Bovee, P.; Xu, Y.; Olivier, M.F.; Bartolucci, P.; Benkerrou, M.; Pissard, S.; et al. Pathophysiology of sickle cell disease is mirrored by the red blood cell metabolome. Blood 2011, 117, e57–e66. [Google Scholar] [CrossRef] [PubMed]
- Raghavachari, N.; Xu, X.; Harris, A.; Villagra, J.; Logun, C.; Barb, J.; Solomon, M.A.; Suffredini, A.F.; Danner, R.L.; Kato, G.; et al. Amplified expression profiling of platelet transcriptome reveals changes in arginine metabolic pathways in patients with sickle cell disease. Circulation 2007, 115, 1551–1562. [Google Scholar] [CrossRef]
- Schnog, J.J.; Jager, E.H.; van der Dijs, F.P.; Duits, A.J.; Moshage, H.; Muskiet, F.D.; Muskiet, F.A. Evidence for a metabolic shift of arginine metabolism in sickle cell disease. Ann Hematol 2004, 83, 371–375. [Google Scholar] [CrossRef]
- Telen, M.J.; Malik, P.; Vercellotti, G.M. Therapeutic strategies for sickle cell disease: Towards a multi-agent approach. Nat Rev Drug Discov 2019, 18, 139–158. [Google Scholar] [CrossRef]
- Charache, S.; Terrin, M.L.; Moore, R.D.; Dover, G.J.; Barton, F.B.; Eckert, S.V.; McMahon, R.P.; Bonds, D.R. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. N Engl J Med 1995, 332, 1317–1322. [Google Scholar] [CrossRef]
- Niihara, Y.; Miller, S.T.; Kanter, J.; Lanzkron, S.; Smith, W.R.; Hsu, L.L.; Gordeuk, V.R.; Viswanathan, K.; Sarnaik, S.; Osunkwo, I.; et al. A Phase 3 Trial of l-Glutamine in Sickle Cell Disease. N Engl J Med 2018, 379, 226–235. [Google Scholar] [CrossRef]
- Ataga, K.I.; Kutlar, A.; Kanter, J.; Liles, D.; Cancado, R.; Friedrisch, J.; Guthrie, T.H.; Knight-Madden, J.; Alvarez, O.A.; Gordeuk, V.R.; et al. Crizanlizumab for the Prevention of Pain Crises in Sickle Cell Disease. N Engl J Med 2017, 376, 429–439. [Google Scholar] [CrossRef]
- Vichinsky, E.; Hoppe, C.C.; Ataga, K.I.; Ware, R.E.; Nduba, V.; El-Beshlawy, A.; Hassab, H.; Achebe, M.M.; Alkindi, S.; Brown, R.C.; et al. A Phase 3 Randomized Trial of Voxelotor in Sickle Cell Disease. N Engl J Med 2019, 381, 509–519. [Google Scholar] [CrossRef]
- Niihara, Y.; Zerez, C.R.; Akiyama, D.S.; Tanaka, K.R. Oral L-glutamine therapy for sickle cell anemia: I. Subjective clinical improvement and favorable change in red cell NAD redox potential. Am J Hematol 1998, 58, 117–121. [Google Scholar] [CrossRef]
- Klings, E.S.; Farber, H.W. Role of free radicals in the pathogenesis of acute chest syndrome in sickle cell disease. Respir Res 2001, 2, 280–285. [Google Scholar] [CrossRef]
- Queiroz, R.F.; Lima, E.S. Oxidative stress in sickle cell disease. Rev Bras Hematol Hemoter 2013, 35, 16–17. [Google Scholar] [CrossRef]
- Esperti, S.; Nader, E.; Stier, A.; Boisson, C.; Carin, R.; Marano, M.; Robert, M.; Martin, M.; Horand, F.; Cibiel, A.; et al. Increased retention of functional mitochondria in mature sickle red blood cells is associated with increased sickling tendency, hemolysis and oxidative stress. Haematologica 2023, 108, 3086–3094. [Google Scholar] [CrossRef]
- Jagadeeswaran, R.; Vazquez, B.A.; Thiruppathi, M.; Ganesh, B.B.; Ibanez, V.; Cui, S.; Engel, J.D.; Diamond, A.M.; Molokie, R.E.; DeSimone, J.; et al. Pharmacological inhibition of LSD1 and mTOR reduces mitochondrial retention and associated ROS levels in the red blood cells of sickle cell disease. Exp Hematol 2017, 50, 46–52. [Google Scholar] [CrossRef]
- Antwi-Boasiako, C.; Dankwah, G.B.; Aryee, R.; Hayfron-Benjamin, C.; Donkor, E.S.; Campbell, A.D. Oxidative Profile of Patients with Sickle Cell Disease. Med Sci (Basel) 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Telen, M.J. Beyond hydroxyurea: New and old drugs in the pipeline for sickle cell disease. Blood 2016, 127, 810–819. [Google Scholar] [CrossRef]
- Kapoor, S.; Little, J.A.; Pecker, L.H. Advances in the Treatment of Sickle Cell Disease. Mayo Clin Proc 2018, 93, 1810–1824. [Google Scholar] [CrossRef] [PubMed]
- Little, J.A.; McGowan, V.R.; Kato, G.J.; Partovi, K.S.; Feld, J.J.; Maric, I.; Martyr, S.; Taylor, J.G.t.; Machado, R.F.; Heller, T.; et al. Combination erythropoietin-hydroxyurea therapy in sickle cell disease: Experience from the National Institutes of Health and a literature review. Haematologica 2006, 91, 1076–1083. [Google Scholar] [PubMed]
- Itoh, K.; Chiba, T.; Takahashi, S.; Ishii, T.; Igarashi, K.; Katoh, Y.; Oyake, T.; Hayashi, N.; Satoh, K.; Hatayama, I.; et al. An Nrf2/small Maf heterodimer mediates the induction of phase II detoxifying enzyme genes through antioxidant response elements. Biochem Biophys Res Commun 1997, 236, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Takaya, K.; Suzuki, T.; Motohashi, H.; Onodera, K.; Satomi, S.; Kensler, T.W.; Yamamoto, M. Validation of the multiple sensor mechanism of the Keap1-Nrf2 system. Free Radic Biol Med 2012, 53, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Qian, W.; Chen, F.; Jin, Y.; Wang, F.; Lu, X.; Lee, S.R.; Su, D.; Chen, B. ATRA protects skin fibroblasts against UV-induced oxidative damage through inhibition of E3 ligase Hrd1. Mol Med Rep 2019, 20, 2294–2302. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Zhao, F.; Gao, B.; Tan, C.; Yagishita, N.; Nakajima, T.; Wong, P.K.; Chapman, E.; Fang, D.; Zhang, D.D. Hrd1 suppresses Nrf2-mediated cellular protection during liver cirrhosis. Genes Dev 2014, 28, 708–722. [Google Scholar] [CrossRef] [PubMed]
- Rada, P.; Rojo, A.I.; Chowdhry, S.; McMahon, M.; Hayes, J.D.; Cuadrado, A. SCF/beta-TrCP promotes glycogen synthase kinase 3-dependent degradation of the Nrf2 transcription factor in a Keap1-independent manner. Mol Cell Biol 2011, 31, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, I.; Michalska, P.; Tenti, G.; Cores, A.; Buendia, I.; Rojo, A.I.; Georgakopoulos, N.D.; Hernandez-Guijo, J.M.; Teresa Ramos, M.; Wells, G.; et al. Discovery of the first dual GSK3beta inhibitor/Nrf2 inducer. A new multitarget therapeutic strategy for Alzheimer′s disease. Sci Rep 2017, 7, 45701. [Google Scholar] [CrossRef]
- Chorley, B.N.; Campbell, M.R.; Wang, X.; Karaca, M.; Sambandan, D.; Bangura, F.; Xue, P.; Pi, J.; Kleeberger, S.R.; Bell, D.A. Identification of novel NRF2-regulated genes by ChIP-Seq: Influence on retinoid X receptor alpha. Nucleic Acids Res 2012, 40, 7416–7429. [Google Scholar] [CrossRef]
- Macari, E.R.; Schaeffer, E.K.; West, R.J.; Lowrey, C.H. Simvastatin and t-butylhydroquinone suppress KLF1 and BCL11A gene expression and additively increase fetal hemoglobin in primary human erythroid cells. Blood 2013, 121, 830–839. [Google Scholar] [CrossRef]
- Keleku-Lukwete, N.; Suzuki, M.; Otsuki, A.; Tsuchida, K.; Katayama, S.; Hayashi, M.; Naganuma, E.; Moriguchi, T.; Tanabe, O.; Engel, J.D.; et al. Amelioration of inflammation and tissue damage in sickle cell model mice by Nrf2 activation. Proc Natl Acad Sci U S A 2015, 112, 12169–12174. [Google Scholar] [CrossRef]
- Keleku-Lukwete, N.; Suzuki, M.; Panda, H.; Otsuki, A.; Katsuoka, F.; Saito, R.; Saigusa, D.; Uruno, A.; Yamamoto, M. Nrf2 activation in myeloid cells and endothelial cells differentially mitigates sickle cell disease pathology in mice. Blood Adv 2019, 3, 1285–1297. [Google Scholar] [CrossRef]
- Zhu, X.; Xi, C.; Thomas, B.; Pace, B.S. Loss of NRF2 function exacerbates the pathophysiology of sickle cell disease in a transgenic mouse model. Blood 2018, 131, 558–562. [Google Scholar] [CrossRef]
- Xi, C.; Pang, J.; Zhi, W.; Chang, C.S.; Siddaramappa, U.; Shi, H.; Horuzsko, A.; Pace, B.S.; Zhu, X. Nrf2 sensitizes ferroptosis through l-2-hydroxyglutarate-mediated chromatin modifications in sickle cell disease. Blood 2023, 142, 382–396. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, S.; Pace, B.; Gupta, D.; Sturtevant, S.; Li, B.; Makala, L.; Brittain, J.; Moore, N.; Vieira, B.F.; Thullen, T.; et al. Dimethyl fumarate increases fetal hemoglobin, provides heme detoxification, and corrects anemia in sickle cell disease. JCI Insight 2017, 2. [Google Scholar] [CrossRef]
- Zhu, X.; Li, B.; Pace, B.S. NRF2 mediates gamma-globin gene regulation and fetal hemoglobin induction in human erythroid progenitors. Haematologica 2017, 102, e285–e288. [Google Scholar] [CrossRef] [PubMed]
- Chin, M.P.; Wrolstad, D.; Bakris, G.L.; Chertow, G.M.; de Zeeuw, D.; Goldsberry, A.; Linde, P.G.; McCullough, P.A.; McMurray, J.J.; Wittes, J.; et al. Risk factors for heart failure in patients with type 2 diabetes mellitus and stage 4 chronic kidney disease treated with bardoxolone methyl. J Card Fail 2014, 20, 953–958. [Google Scholar] [CrossRef]
- Chin, M.P.; Reisman, S.A.; Bakris, G.L.; O′Grady, M.; Linde, P.G.; McCullough, P.A.; Packham, D.; Vaziri, N.D.; Ward, K.W.; Warnock, D.G.; et al. Mechanisms contributing to adverse cardiovascular events in patients with type 2 diabetes mellitus and stage 4 chronic kidney disease treated with bardoxolone methyl. Am J Nephrol 2014, 39, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Macari, E.R.; Lowrey, C.H. Induction of human fetal hemoglobin via the NRF2 antioxidant response signaling pathway. Blood 2011, 117, 5987–5997. [Google Scholar] [CrossRef]
- Salazar, M.; Rojo, A.I.; Velasco, D.; de Sagarra, R.M.; Cuadrado, A. Glycogen synthase kinase-3beta inhibits the xenobiotic and antioxidant cell response by direct phosphorylation and nuclear exclusion of the transcription factor Nrf2. J Biol Chem 2006, 281, 14841–14851. [Google Scholar] [CrossRef]
- Jain, A.K.; Jaiswal, A.K. GSK-3beta acts upstream of Fyn kinase in regulation of nuclear export and degradation of NF-E2 related factor 2. J Biol Chem 2007, 282, 16502–16510. [Google Scholar] [CrossRef]
- Mohammadzadeh, N.; Montecucco, F.; Carbone, F.; Xu, S.; Al-Rasadi, K.; Sahebkar, A. Statins: Epidrugs with effects on endothelial health? Eur J Clin Invest 2020, 50, e13388. [Google Scholar] [CrossRef]
- Liu, C.; Shen, M.; Tan, W.L.W.; Chen, I.Y.; Liu, Y.; Yu, X.; Yang, H.; Zhang, A.; Liu, Y.; Zhao, M.T.; et al. Statins improve endothelial function via suppression of epigenetic-driven EndMT. Nat Cardiovasc Res 2023, 2, 467–485. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Lin, J.H.; Chou, C.W.; Chang, Y.F.; Yeh, S.H.; Chen, C.C. Statins increase p21 through inhibition of histone deacetylase activity and release of promoter-associated HDAC1/2. Cancer Res 2008, 68, 2375–2383. [Google Scholar] [CrossRef] [PubMed]
- Tikoo, K.; Patel, G.; Kumar, S.; Karpe, P.A.; Sanghavi, M.; Malek, V.; Srinivasan, K. Tissue specific up regulation of ACE2 in rabbit model of atherosclerosis by atorvastatin: Role of epigenetic histone modifications. Biochem Pharmacol 2015, 93, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Rosales, C.; Portilla-Fernandez, E.; Nano, J.; Wilson, R.; Lehne, B.; Mishra, P.P.; Gao, X.; Ghanbari, M.; Rueda-Ochoa, O.L.; Juvinao-Quintero, D.; et al. Epigenetic Link Between Statin Therapy and Type 2 Diabetes. Diabetes Care 2020, 43, 875–884. [Google Scholar] [CrossRef]
- Feig, J.E.; Shang, Y.; Rotllan, N.; Vengrenyuk, Y.; Wu, C.; Shamir, R.; Torra, I.P.; Fernandez-Hernando, C.; Fisher, E.A.; Garabedian, M.J. Statins promote the regression of atherosclerosis via activation of the CCR7-dependent emigration pathway in macrophages. PLoS ONE 2011, 6, e28534. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Kim, K.K.; Shevach, E.M. Simvastatin induces Foxp3+ T regulatory cells by modulation of transforming growth factor-beta signal transduction. Immunology 2010, 130, 484–493. [Google Scholar] [CrossRef]
- Makino, N.; Maeda, T.; Abe, N. Short telomere subtelomeric hypomethylation is associated with telomere attrition in elderly diabetic patients (1). Can J Physiol Pharmacol 2019, 97, 335–339. [Google Scholar] [CrossRef]
- Zhu, X.; Wang, Y.; Pi, W.; Liu, H.; Wickrema, A.; Tuan, D. NF-Y recruits both transcription activator and repressor to modulate tissue- and developmental stage-specific expression of human gamma-globin gene. PLoS ONE 2012, 7, e47175. [Google Scholar] [CrossRef]
- Ryan, T.M.; Ciavatta, D.J.; Townes, T.M. Knockout-transgenic mouse model of sickle cell disease. Science 1997, 278, 873–876. [Google Scholar] [CrossRef]
- Zhang, Y.; Dai, Y.; Wen, J.; Zhang, W.; Grenz, A.; Sun, H.; Tao, L.; Lu, G.; Alexander, D.C.; Milburn, M.V.; et al. Detrimental effects of adenosine signaling in sickle cell disease. Nat Med 2011, 17, 79–86. [Google Scholar] [CrossRef]
- Zhu, X.; Ling, J.; Zhang, L.; Pi, W.; Wu, M.; Tuan, D. A facilitated tracking and transcription mechanism of long-range enhancer function. Nucleic Acids Res 2007, 35, 5532–5544. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, S.; Hayashi, H.; Kinoshita, K.; Abe, M.; Kuroki, H.; Tokunaga, R.; Tomiyasu, S.; Tanaka, H.; Sugita, H.; Arita, T.; et al. Statins inhibit tumor progression via an enhancer of zeste homolog 2-mediated epigenetic alteration in colorectal cancer. Int J Cancer 2014, 135, 2528–2536. [Google Scholar] [CrossRef] [PubMed]
- Okubo, K.; Miyai, K.; Kato, K.; Asano, T.; Sato, A. Simvastatin-romidepsin combination kills bladder cancer cells synergistically. Transl Oncol 2021, 14, 101154. [Google Scholar] [CrossRef] [PubMed]
- Greer, E.L.; Shi, Y. Histone methylation: A dynamic mark in health, disease and inheritance. Nat Rev Genet 2012, 13, 343–357. [Google Scholar] [CrossRef] [PubMed]
- Belcher, J.D.; Chen, C.; Nguyen, J.; Zhang, P.; Abdulla, F.; Nguyen, P.; Killeen, T.; Xu, P.; O′Sullivan, G.; Nath, K.A.; et al. Control of Oxidative Stress and Inflammation in Sickle Cell Disease with the Nrf2 Activator Dimethyl Fumarate. Antioxid Redox Signal 2017, 26, 748–762. [Google Scholar] [CrossRef]
- Liang, H.; Feng, Y.; Cui, R.; Qiu, M.; Zhang, J.; Liu, C. Simvastatin protects against acetaminophen-induced liver injury in mice. Biomed Pharmacother 2018, 98, 916–924. [Google Scholar] [CrossRef]
- McGregor, G.H.; Campbell, A.D.; Fey, S.K.; Tumanov, S.; Sumpton, D.; Blanco, G.R.; Mackay, G.; Nixon, C.; Vazquez, A.; Sansom, O.J.; et al. Targeting the Metabolic Response to Statin-Mediated Oxidative Stress Produces a Synergistic Antitumor Response. Cancer Res 2020, 80, 175–188. [Google Scholar] [CrossRef]
- Rasmussen, S.T.; Andersen, J.T.; Nielsen, T.K.; Cejvanovic, V.; Petersen, K.M.; Henriksen, T.; Weimann, A.; Lykkesfeldt, J.; Poulsen, H.E. Simvastatin and oxidative stress in humans: A randomized, double-blinded, placebo-controlled clinical trial. Redox Biol 2016, 9, 32–38. [Google Scholar] [CrossRef]
- Kumar, V.; Joshi, T.; Vatsa, N.; Singh, B.K.; Jana, N.R. Simvastatin Restores HDAC1/2 Activity and Improves Behavioral Deficits in Angelman Syndrome Model Mouse. Front Mol Neurosci 2019, 12, 289. [Google Scholar] [CrossRef]
- Mattioli, E.; Andrenacci, D.; Mai, A.; Valente, S.; Robijns, J.; De Vos, W.H.; Capanni, C.; Lattanzi, G. Statins and Histone Deacetylase Inhibitors Affect Lamin A/C - Histone Deacetylase 2 Interaction in Human Cells. Front Cell Dev Biol 2019, 7, 6. [Google Scholar] [CrossRef]
- Schmeck, B.; Beermann, W.; N′Guessan, P.D.; Hocke, A.C.; Opitz, B.; Eitel, J.; Dinh, Q.T.; Witzenrath, M.; Krull, M.; Suttorp, N.; et al. Simvastatin reduces Chlamydophila pneumoniae-mediated histone modifications and gene expression in cultured human endothelial cells. Circ Res 2008, 102, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Kodach, L.L.; Jacobs, R.J.; Voorneveld, P.W.; Wildenberg, M.E.; Verspaget, H.W.; van Wezel, T.; Morreau, H.; Hommes, D.W.; Peppelenbosch, M.P.; van den Brink, G.R.; et al. Statins augment the chemosensitivity of colorectal cancer cells inducing epigenetic reprogramming and reducing colorectal cancer cell ′stemness′ via the bone morphogenetic protein pathway. Gut 2011, 60, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- Alves, N.; Neuparth, T.; Barros, S.; Santos, M.M. The anti-lipidemic drug simvastatin modifies epigenetic biomarkers in the amphipod Gammarus locusta. Ecotoxicol Environ Saf 2021, 209, 111849. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.W.; Qi, J.W.; Hang, Y.; Wu, J.X.; Zhou, X.X.; Chen, J.Z.; Wang, J.; Wang, H.H. Simvastatin is beneficial to lung cancer progression by inducing METTL3-induced m6A modification on EZH2 mRNA. Eur Rev Med Pharmacol Sci 2020, 24, 4263–4270. [Google Scholar] [CrossRef] [PubMed]
- Bridgeman, S.; Northrop, W.; Ellison, G.; Sabapathy, T.; Melton, P.E.; Newsholme, P.; Mamotte, C.D.S. Statins Do Not Directly Inhibit the Activity of Major Epigenetic Modifying Enzymes. Cancers (Basel) 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, E.H.; Suzuki, T.; Funayama, R.; Nagashima, T.; Hayashi, M.; Sekine, H.; Tanaka, N.; Moriguchi, T.; Motohashi, H.; Nakayama, K.; et al. Nrf2 suppresses macrophage inflammatory response by blocking proinflammatory cytokine transcription. Nat Commun 2016, 7, 11624. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Bauer, D.E.; Kerenyi, M.A.; Vo, T.D.; Hou, S.; Hsu, Y.J.; Yao, H.; Trowbridge, J.J.; Mandel, G.; Orkin, S.H. Corepressor-dependent silencing of fetal hemoglobin expression by BCL11A. Proc Natl Acad Sci U S A 2013, 110, 6518–6523. [Google Scholar] [CrossRef]
- Kim, Y.W.; Kim, A. Characterization of histone H3K27 modifications in the beta-globin locus. Biochem Biophys Res Commun 2011, 405, 210–215. [Google Scholar] [CrossRef]
- Yu, L.; Myers, G.; Schneider, E.; Wang, Y.; Mathews, R.; Lim, K.C.; Siemieniak, D.; Tang, V.; Ginsburg, D.; Balbin-Cuesta, G.; et al. Identification of novel gamma-globin inducers among all potential erythroid druggable targets. Blood Adv 2022, 6, 3280–3285. [Google Scholar] [CrossRef]
- Hoppe, C.; Kuypers, F.; Larkin, S.; Hagar, W.; Vichinsky, E.; Styles, L. A pilot study of the short-term use of simvastatin in sickle cell disease: Effects on markers of vascular dysfunction. Br J Haematol 2011, 153, 655–663. [Google Scholar] [CrossRef]
- Hoppe, C.; Jacob, E.; Styles, L.; Kuypers, F.; Larkin, S.; Vichinsky, E. Simvastatin reduces vaso-occlusive pain in sickle cell anaemia: A pilot efficacy trial. Br J Haematol 2017, 177, 620–629. [Google Scholar] [CrossRef]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid Med Cell Longev 2016, 2016, 5698931. [Google Scholar] [CrossRef]
- Jamialahmadi, T.; Abbasifard, M.; Reiner, Z.; Rizzo, M.; Eid, A.H.; Sahebkar, A. The Effects of Statin Treatment on Serum Ferritin Levels: A Systematic Review and Meta-Analysis. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Coates, T.D.; Wood, J.C. How we manage iron overload in sickle cell patients. Br J Haematol 2017, 177, 703–716. [Google Scholar] [CrossRef]
- Ahn, J.; Lee, S.; Won, S. Possible link between statin and iron deficiency anemia: A South Korean nationwide population-based cohort study. Sci Adv 2023, 9, eadg6194. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.J.; Hong, E.M.; Kim, M.; Kim, J.H.; Jang, J.; Park, S.W.; Byun, H.W.; Koh, D.H.; Choi, M.H.; Kae, S.H.; et al. Simvastatin induces heme oxygenase-1 via NF-E2-related factor 2 (Nrf2) activation through ERK and PI3K/Akt pathway in colon cancer. Oncotarget 2016, 7, 46219–46229. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Simvastatin activates γ-globin expression to suppress sickling of SCD erythroblasts. (A) Two-phase culture of SCD patients’ peripheral blood CD34+ stem cells. (B) SCD erythroblasts at Day 10 of culture were treated with 0.1% DMSO, 50 µM hydroxyurea (HU), 100 µM dimethyl fumarate (DMF), 2.5-20 µM simvastatin (SIM), or untreated control (UT) for 48 h and protein expression of fetal hemoglobin (HbF) and adult sickle hemoglobin (HbS) was quantified. (C-D) SCD erythroblasts from the same culture were determined the percentage of HbF positive cells (F-cells %) by flow cytometry (C) and quantified (D). (E) Cell morphology was analyzed to measure the number of sickled erythroblasts under hypoxia for the different treatment conditions and the percentage of sickled cells quantified (F). Data represents the mean ± SD of three independent biological replicates. *, p < 0.05.
Figure 1.
Simvastatin activates γ-globin expression to suppress sickling of SCD erythroblasts. (A) Two-phase culture of SCD patients’ peripheral blood CD34+ stem cells. (B) SCD erythroblasts at Day 10 of culture were treated with 0.1% DMSO, 50 µM hydroxyurea (HU), 100 µM dimethyl fumarate (DMF), 2.5-20 µM simvastatin (SIM), or untreated control (UT) for 48 h and protein expression of fetal hemoglobin (HbF) and adult sickle hemoglobin (HbS) was quantified. (C-D) SCD erythroblasts from the same culture were determined the percentage of HbF positive cells (F-cells %) by flow cytometry (C) and quantified (D). (E) Cell morphology was analyzed to measure the number of sickled erythroblasts under hypoxia for the different treatment conditions and the percentage of sickled cells quantified (F). Data represents the mean ± SD of three independent biological replicates. *, p < 0.05.
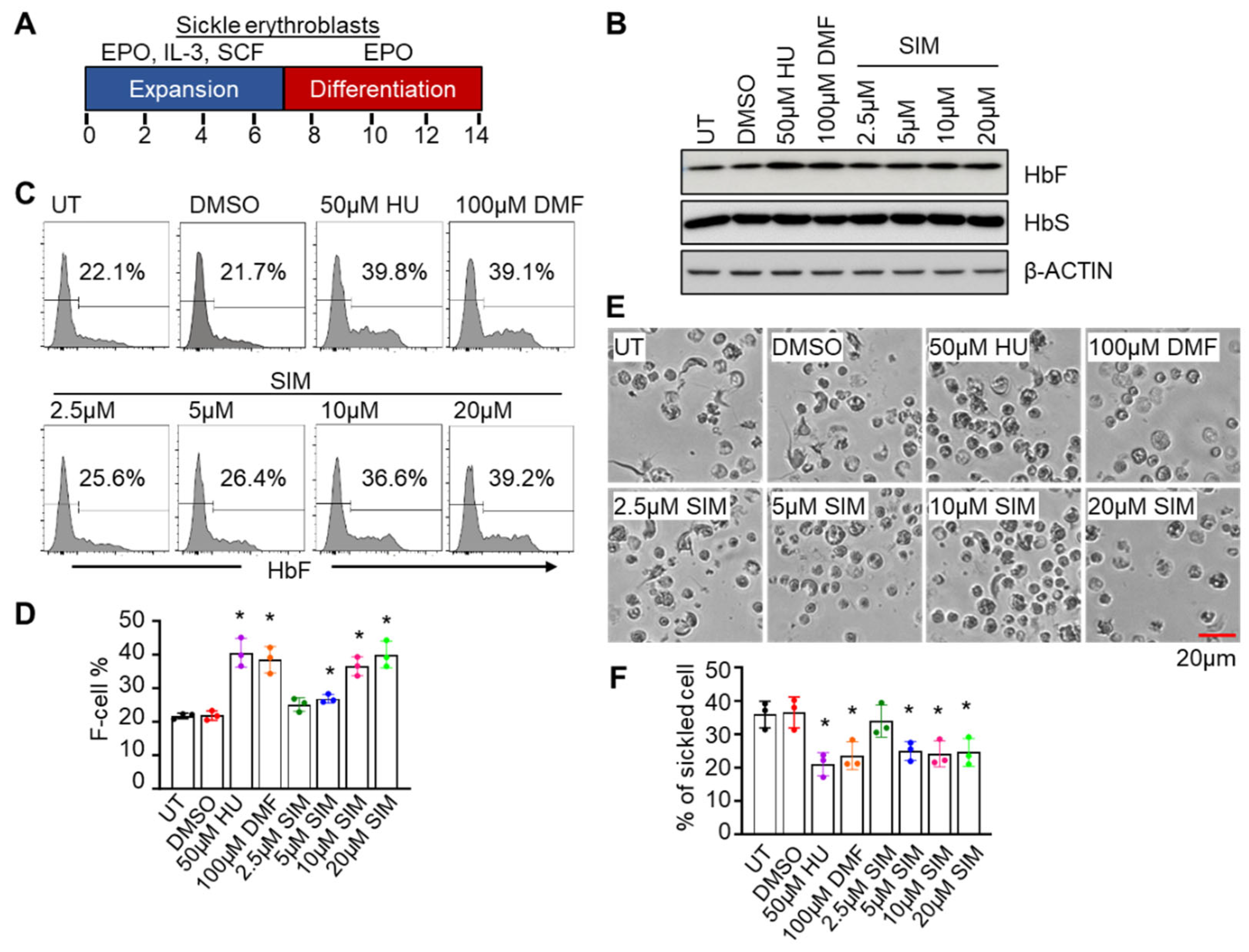
Figure 2.
Simvastatin increases the expression of NRF2 and antioxidant proteins. Day 12 SCD erythroblasts after 48 h treatment with 0.1% DMSO, 50 µM HU, 100 µM DMF, 2.5-20 µM simvastatin (SIM), or untreated control (UT) were detected for the expression of antioxidant factors at the protein (A) and mRNA levels (B). Data represents the mean ± SD of three biological replicates. *, p < 0.05.
Figure 2.
Simvastatin increases the expression of NRF2 and antioxidant proteins. Day 12 SCD erythroblasts after 48 h treatment with 0.1% DMSO, 50 µM HU, 100 µM DMF, 2.5-20 µM simvastatin (SIM), or untreated control (UT) were detected for the expression of antioxidant factors at the protein (A) and mRNA levels (B). Data represents the mean ± SD of three biological replicates. *, p < 0.05.
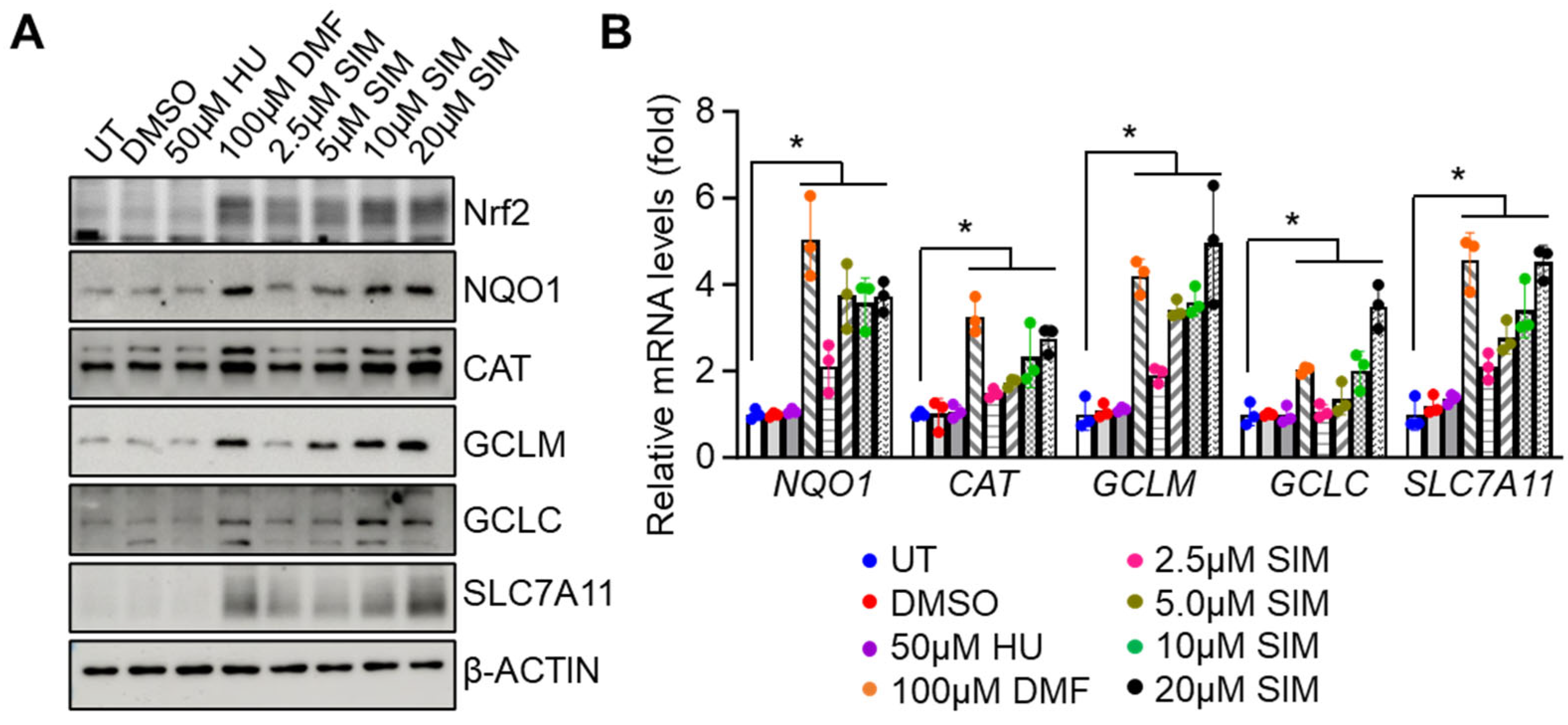
Figure 3.
Simvastatin increased the antioxidant capacity of SCD erythroblasts. Incubation with H2O2 (40µM) for 8 h was completed with Day 12 SCD erythroblasts after 48 h treatment of 2.5-20 µM simvastatin (SIM), then cellular viability (A) and the cellular content of reduced (GSH), oxidative (GSSG) glutathione and their ratio (B-D) were determined. The cellular NQO1 activity (E) and cystine contents (F) in the same cells cultured as described in panel A were measured with assay kits. (G) The cystine uptake efficacy of SCD erythroblasts was determined by a BioTracker Cystine-FITC Live Cell Dye followed by flow cytometry analysis. Data represents the mean ± SD of three biological replicates. *, p < 0.05.
Figure 3.
Simvastatin increased the antioxidant capacity of SCD erythroblasts. Incubation with H2O2 (40µM) for 8 h was completed with Day 12 SCD erythroblasts after 48 h treatment of 2.5-20 µM simvastatin (SIM), then cellular viability (A) and the cellular content of reduced (GSH), oxidative (GSSG) glutathione and their ratio (B-D) were determined. The cellular NQO1 activity (E) and cystine contents (F) in the same cells cultured as described in panel A were measured with assay kits. (G) The cystine uptake efficacy of SCD erythroblasts was determined by a BioTracker Cystine-FITC Live Cell Dye followed by flow cytometry analysis. Data represents the mean ± SD of three biological replicates. *, p < 0.05.
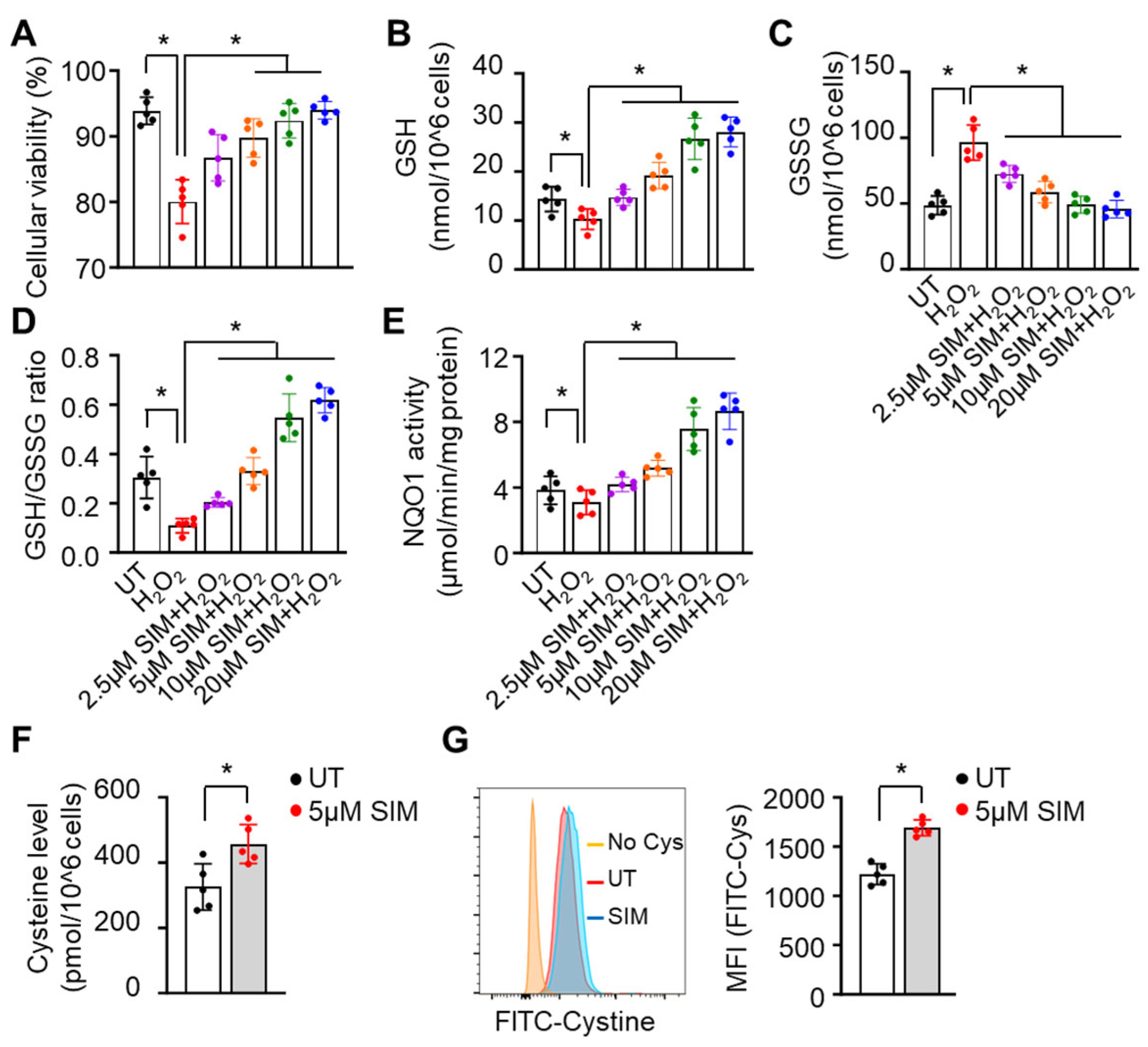
Figure 4.
Simvastatin attenuates EZH2 expression and histone H3K27Me3 levels to modify chromatin structure and gene expression. (A) Shown are the effects of SIM on histone H3 methylation (H3K27Me3), acetylation (AcH3), and EZH2 protein expression. Total histone H3 and β-ACTIN were loading controls. (B) Quantitative RT-PCR analysis of the relative mRNA levels of H3K27Me3 modifiers EZH1/2 and KDM6a/b in SCD erythroblasts treated with 2.5-20 µM simvastatin (SIM) or untreated control (UT). Data represents mean ± SD of three biological replicates. *, p < 0.05.
Figure 4.
Simvastatin attenuates EZH2 expression and histone H3K27Me3 levels to modify chromatin structure and gene expression. (A) Shown are the effects of SIM on histone H3 methylation (H3K27Me3), acetylation (AcH3), and EZH2 protein expression. Total histone H3 and β-ACTIN were loading controls. (B) Quantitative RT-PCR analysis of the relative mRNA levels of H3K27Me3 modifiers EZH1/2 and KDM6a/b in SCD erythroblasts treated with 2.5-20 µM simvastatin (SIM) or untreated control (UT). Data represents mean ± SD of three biological replicates. *, p < 0.05.
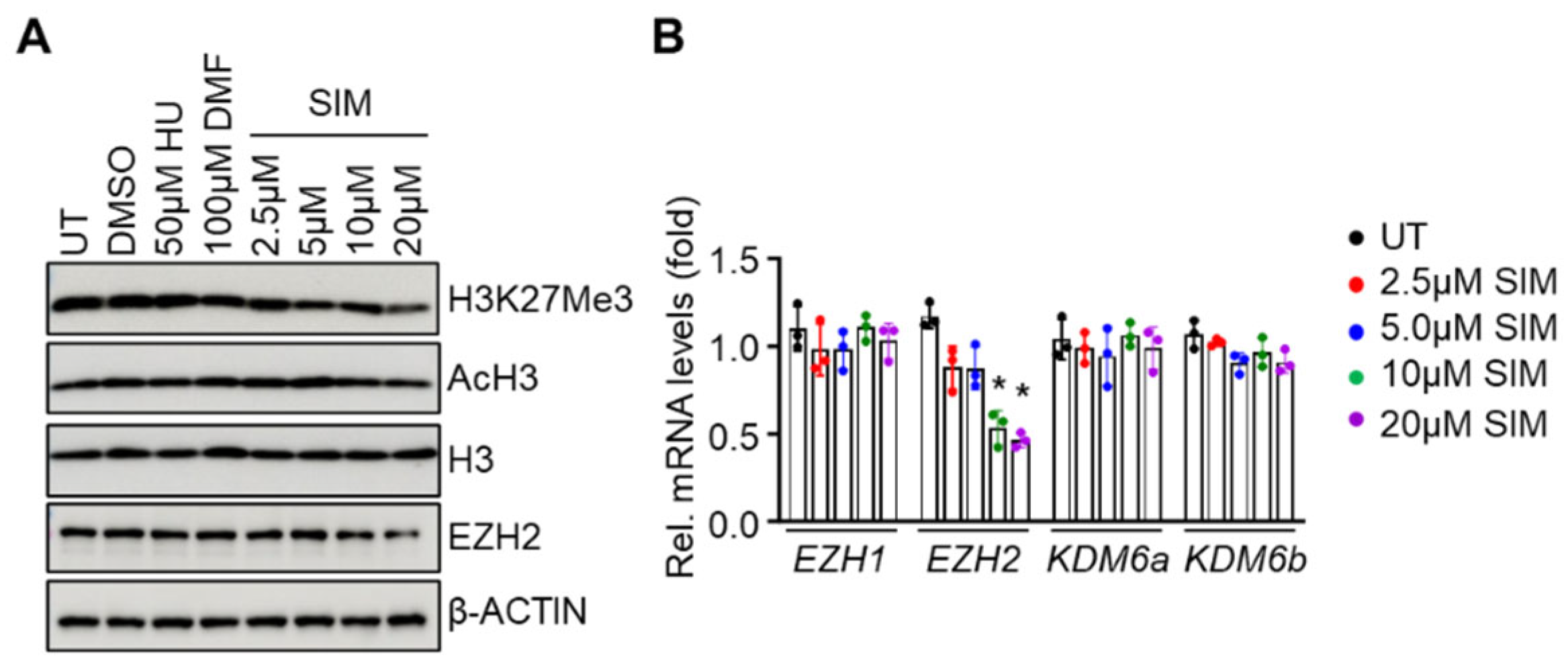
Figure 5.
EZH2 regulates NRF2 expression to alter ARE motif chromatin structure in target genes. (A) The effect of shEZH2 mediated gene silencing (two different constructs) on protein levels of NRF2, HbF, antioxidant factors, and H3K27Me3 were investigated. Histone H3 and β-ACTIN were loading controls. (B-E) ChIP assay determined the association of Nrf2, H3K27Me3, TATA box binding protein (TBP) and RNA polymerase II (Pol II) to the HBG1 (B), HMOX1 (C), NQO1 (D) and SLC7A11 (E) gene loci for simvastatin (SIM, 5µM) treated or untreated (UT) SCD erythroblasts. Primers spanning the ARE motifs of each gene were used. Data represents the mean ± SD of three biological replicates. *, p < 0.05.
Figure 5.
EZH2 regulates NRF2 expression to alter ARE motif chromatin structure in target genes. (A) The effect of shEZH2 mediated gene silencing (two different constructs) on protein levels of NRF2, HbF, antioxidant factors, and H3K27Me3 were investigated. Histone H3 and β-ACTIN were loading controls. (B-E) ChIP assay determined the association of Nrf2, H3K27Me3, TATA box binding protein (TBP) and RNA polymerase II (Pol II) to the HBG1 (B), HMOX1 (C), NQO1 (D) and SLC7A11 (E) gene loci for simvastatin (SIM, 5µM) treated or untreated (UT) SCD erythroblasts. Primers spanning the ARE motifs of each gene were used. Data represents the mean ± SD of three biological replicates. *, p < 0.05.
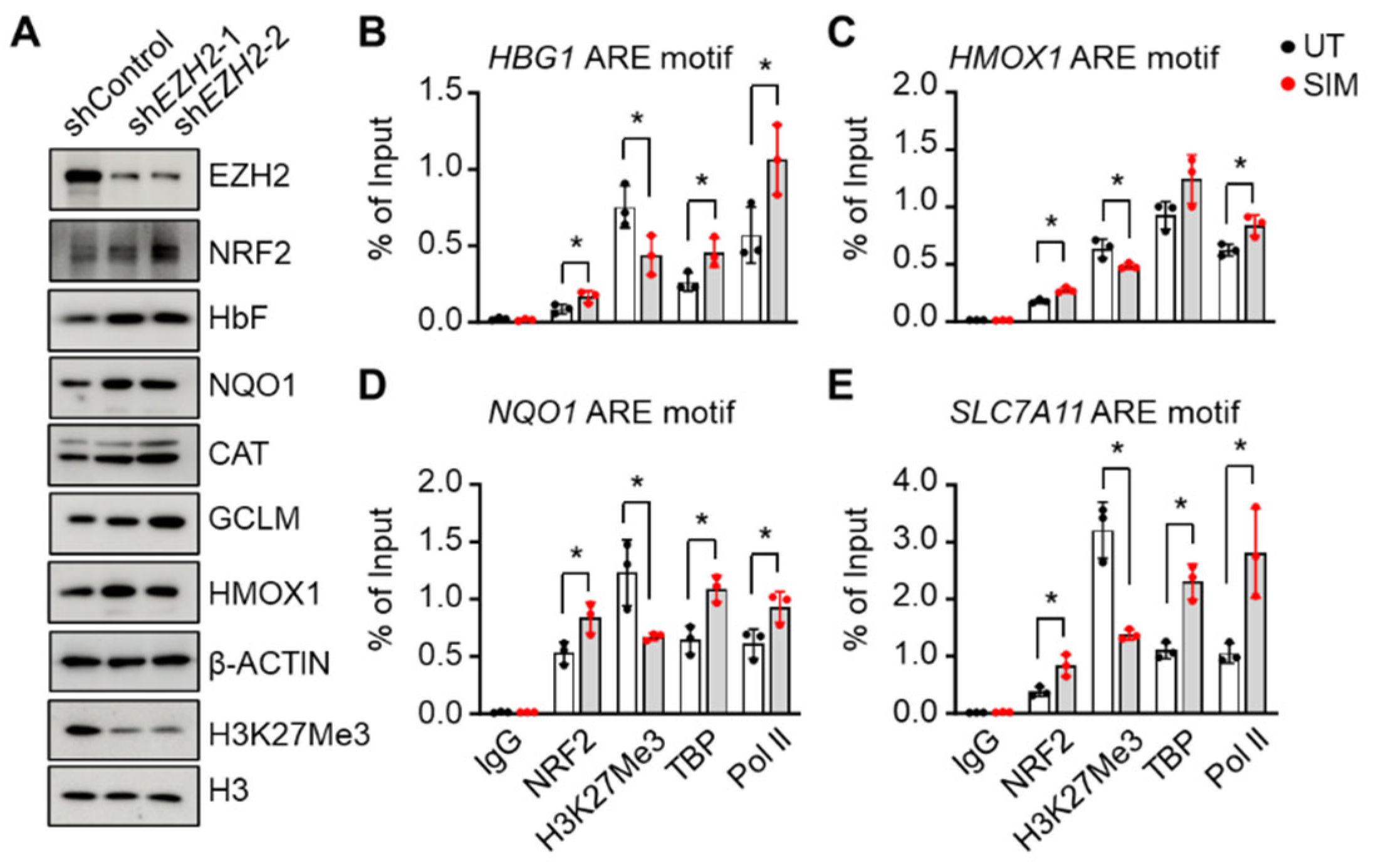
Figure 6.
Simvastatin suppresses H3K27Me3 modifications as a mechanism of fetal γ-globin activation in preclinical SCD mice. (A) Peripheral blood samples of SCD mice after 4 weeks of simvastatin treatment were determined the HbF expressing cells (F-cells) by flow cytometry. The F-cell % and mean fluorescence intensity (MFI) were quantified. (B-C) The spleen CD71+ cells from SIM-treated SCD mice were determined the expression of H3K27Me3, HbF, and HbS at the protein (B) and mRNA levels (C). (D) ChIP assay determined the association of H3K27Me3, TBP, and Pol II to the HBG1 and HBA gene loci in spleen CD71+ cells from SIM treated SCD mice. One-way ANOVA with Bonferroni’s multiple comparison tests was used for statistical analysis (n=5). *, p < 0.05.
Figure 6.
Simvastatin suppresses H3K27Me3 modifications as a mechanism of fetal γ-globin activation in preclinical SCD mice. (A) Peripheral blood samples of SCD mice after 4 weeks of simvastatin treatment were determined the HbF expressing cells (F-cells) by flow cytometry. The F-cell % and mean fluorescence intensity (MFI) were quantified. (B-C) The spleen CD71+ cells from SIM-treated SCD mice were determined the expression of H3K27Me3, HbF, and HbS at the protein (B) and mRNA levels (C). (D) ChIP assay determined the association of H3K27Me3, TBP, and Pol II to the HBG1 and HBA gene loci in spleen CD71+ cells from SIM treated SCD mice. One-way ANOVA with Bonferroni’s multiple comparison tests was used for statistical analysis (n=5). *, p < 0.05.
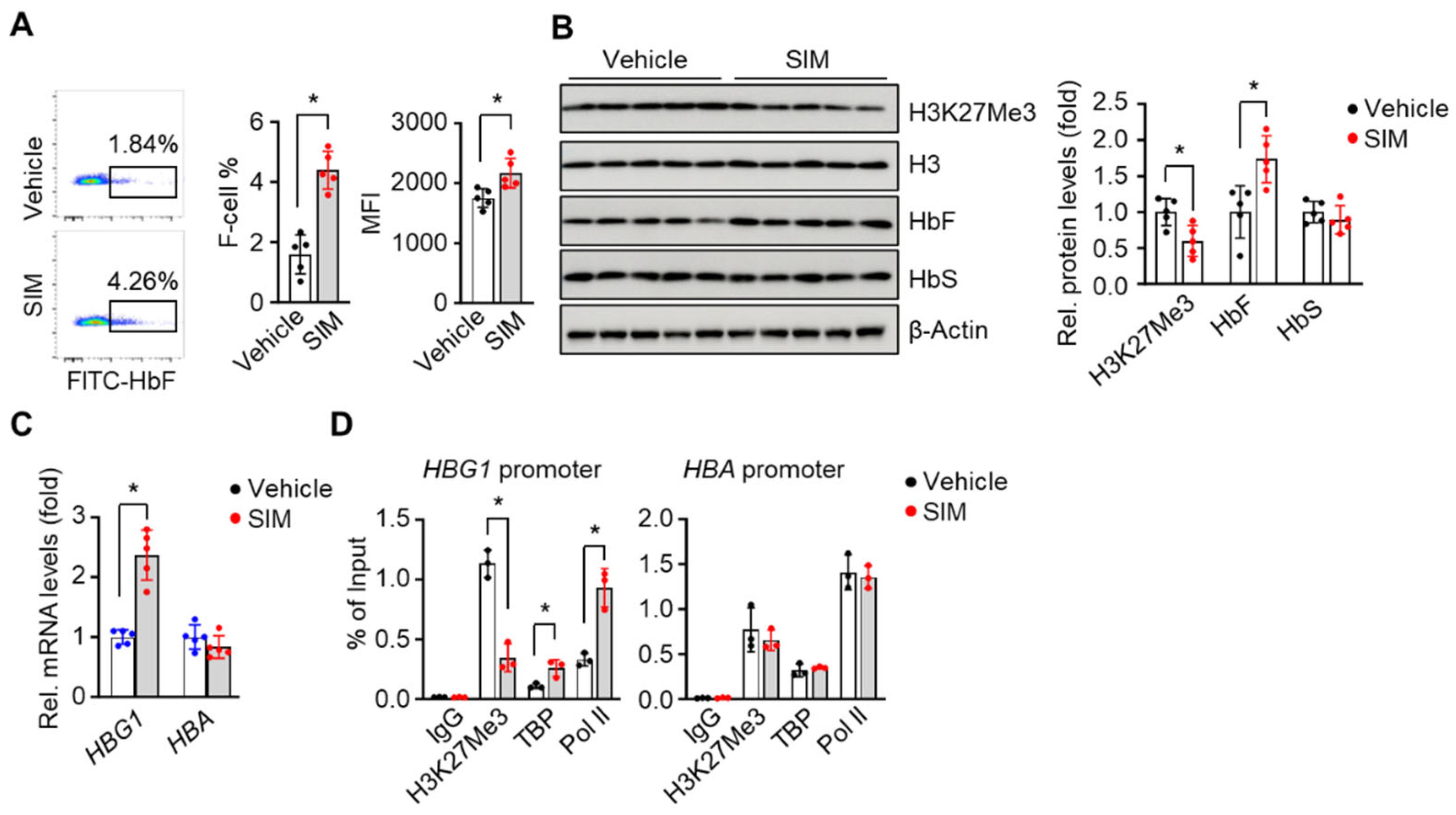
Figure 7.
Simvastatin reduces organ damage and iron content in preclinical SCD mice. (A-B) Representative images of the spleen (A) and liver (B) of SCD mice treated with or without simvastatin (SIM, 7.5 mg/kg daily) for 4 weeks. Quantification of spleen and liver weights are shown in the graph. (C) Representative H&E and Prussian blue staining of SIM-treated SCD mouse spleens. (D) The iron content in spleen tissue was quantified. (E) Representative H&E and Prussian blue staining of SIM-treated SCD mouse livers. (F) The iron content in liver tissues was quantified. Scale bar, 50 μm. One-way ANOVA with Bonferroni’s multiple comparison tests was used for statistical analysis (n=5). *, p < 0.05.
Figure 7.
Simvastatin reduces organ damage and iron content in preclinical SCD mice. (A-B) Representative images of the spleen (A) and liver (B) of SCD mice treated with or without simvastatin (SIM, 7.5 mg/kg daily) for 4 weeks. Quantification of spleen and liver weights are shown in the graph. (C) Representative H&E and Prussian blue staining of SIM-treated SCD mouse spleens. (D) The iron content in spleen tissue was quantified. (E) Representative H&E and Prussian blue staining of SIM-treated SCD mouse livers. (F) The iron content in liver tissues was quantified. Scale bar, 50 μm. One-way ANOVA with Bonferroni’s multiple comparison tests was used for statistical analysis (n=5). *, p < 0.05.
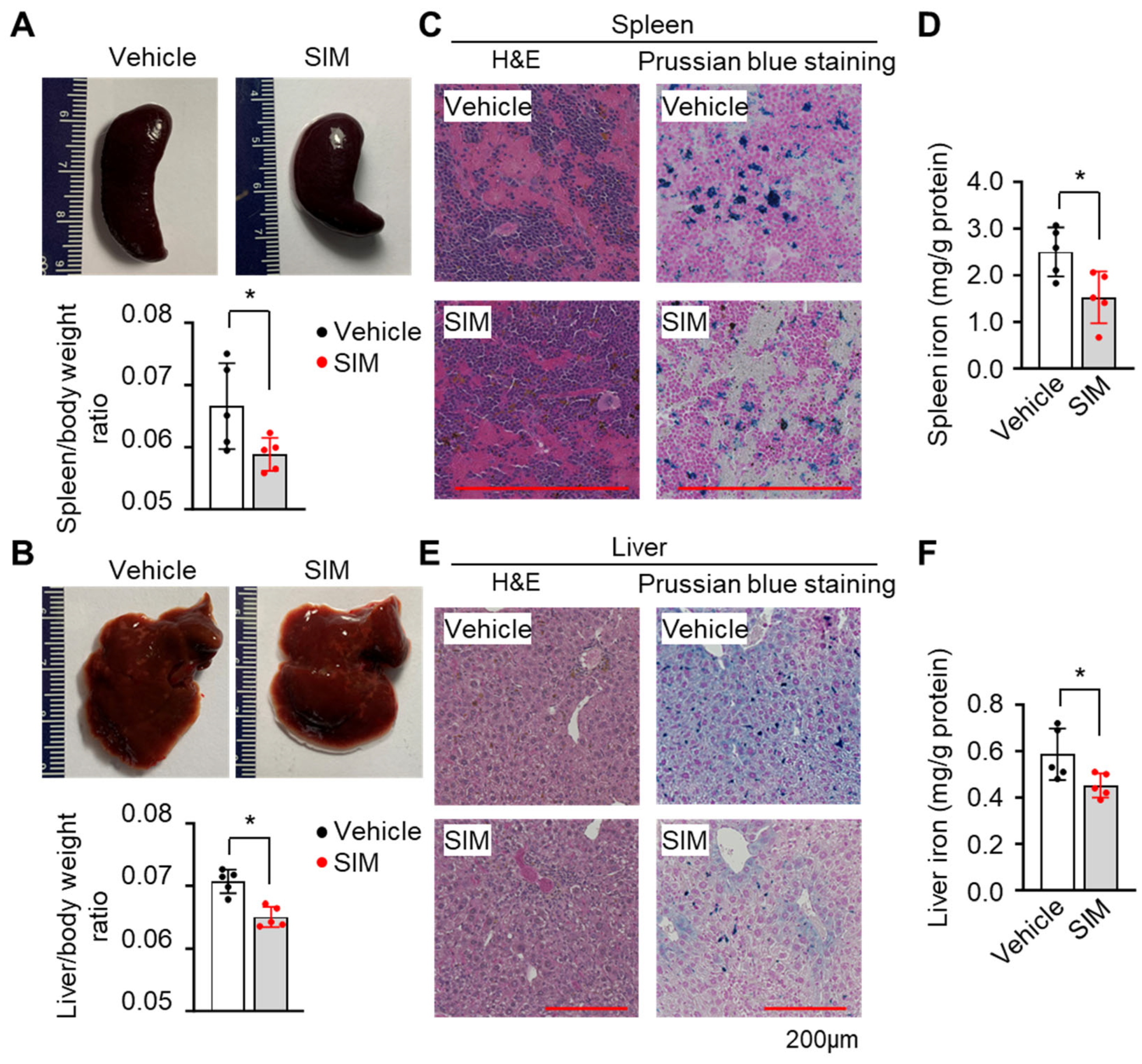
Figure 8.
Simvastatin mitigates reactive oxygen species (ROS) and inflammatory stress in preclinical SCD mice. Spleen CD71+ cells of SCD mice were determined the cellular NADPH andNADP+ levels and their ratio (A), ROS levels by 2′-7′-dichlorodihydrofluorescein diacetate (DCFH-DA) staining (B), and relative expression of antioxidant genes (C). (D) ChIP assay determined the association of H3K27Me3, TBP, and Pol II to the antioxidant gene loci (Nqo1, Cat, Hmox1, Gclc, and Slc7a11) in spleen CD71+ cells of SIM-treated SCD mice. (E) Heatmap representation of proinflammatory factor gene transcripts in spleen CD71+ cells of SCD mice between SIM and vehicle treatment control.. One-way ANOVA with Bonferroni’s multiple comparison tests was used for statistical analysis (n=5 mice). *, p < 0.05.
Figure 8.
Simvastatin mitigates reactive oxygen species (ROS) and inflammatory stress in preclinical SCD mice. Spleen CD71+ cells of SCD mice were determined the cellular NADPH andNADP+ levels and their ratio (A), ROS levels by 2′-7′-dichlorodihydrofluorescein diacetate (DCFH-DA) staining (B), and relative expression of antioxidant genes (C). (D) ChIP assay determined the association of H3K27Me3, TBP, and Pol II to the antioxidant gene loci (Nqo1, Cat, Hmox1, Gclc, and Slc7a11) in spleen CD71+ cells of SIM-treated SCD mice. (E) Heatmap representation of proinflammatory factor gene transcripts in spleen CD71+ cells of SCD mice between SIM and vehicle treatment control.. One-way ANOVA with Bonferroni’s multiple comparison tests was used for statistical analysis (n=5 mice). *, p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



