
Submitted:
01 February 2024
Posted:
02 February 2024
You are already at the latest version
Abstract
The aim of the study was to identify factors associated with non-adherence to tuberculosis (TB) preventive treatment among contacts with latent TB infection of new cases of pulmonary TB cases reported in Catalonia in 2019-2021. All contacts aged 18 years or older with a latent TB infection who received a TB preventive treatment were included in the study. The Chi square test and the odds ratios (OR) were used to assess the association between non-adherence to TB preventive treatment and the study variables, considering a p < 0.05 as statistically significant. Multiple logistic regression analysis was used to detect the in-dependent factors associated with TB preventive treatment non-adherence, considering a p < 0.05 as statistically significant. The percentage of non-adherence to TB preventive treatment found in this study was 23.7%. A multivariable logistic regression analysis determined that the following factors were significantly associated with TB preventive treatment non-adherence among adult contacts: “exposure at school or workplace” (aOR = 3.34), “exposure to an index case without laboratory confirmation of TB” (aOR = 2.07), “immigrant contact” (aOR = 1.81), “male gender” (aOR = 1.75) and “exposure duration <6 hours per week or sporadic exposure” (aOR = 1.60). By contrast, the factor “short-term TB preventive treatment regimen” (aOR = 0.38) was significantly associated with a lower treatment non-adherence. Adherence to TB preventive treatment should be improved among adult contacts of TB pulmonary cases with latent TB infection by recommending short-term treatment regimens and by developing health education activities, with a greater focus on contacts with factors associated with treatment non-adherence.
Keywords:
latent tuberculosis infection
; tuberculosis
; non-adherence to LTBI treatment
; factors of treatment non-adherence
; community health
1. Introduction
Tuberculosis (TB) is transmitted from patients with TB when they expel the bacillus Mycobacterium tuberculosis into the air and infect susceptible individuals. Individuals infected with TB bacteria can develop a TB disease or a latent TB infection, depending on whether they become sick or not, respectively. A TB disease occurs when the immune system cannot avoid the bacteria growth. A latent TB infection occurs when the immune system can avoid TB bacteria growth, but not to eliminate TB bacteria from the body. Latent TB infection is therefore characterized by the presence of immune responses to previously acquired Mycobacterium tuberculosis infection without clinical evidence of TB disease [1,2]. Most individuals with latent TB infection have no signs or symptoms of TB disease, although they have a 5% risk of developing TB disease in the first 2 years after infection and a 5−20% lifetime risk of developing TB [3]. In 2022, the global reported number of people with newly diagnosed TB was 7.5 million and 1.30 million deaths were caused by TB worldwide [2].
In 2015, all World Health Organization (WHO) and United Nations (UN) Member States committed to ending the TB epidemic, through their adoption of WHO’s End TB Strategy and the UN Sustainable Development Goals (SDGs) [4]. The United Nations second high-level meeting on the fight against tuberculosis, held on 22 September 2023, reaffirmed the UN commitment to end the tuberculosis epidemic by 2030 [5].
The global targets set in 2023 for the 2023−2027 period included to achieve 90% coverage of TB preventive treatment among contacts of pulmonary TB cases and other population groups at high risk of developing TB disease [2]. To achieve this objective, it was considered necessary to treat 20 million household contacts aged ≥5 years during the 2023−2027 period [2].
Screening and treating population groups at highest risk of progressing from TB infection to TB disease, such as contacts with latent TB infection of TB cases, is a critical preventive intervention to achieve the global targets of the End TB strategy [6,7,8]. For this reason, the WHO Guidelines on TB [6] and the WHO Guidelines on management of latent TB infection [7,8] proposed to implement the following activities at countries with TB incidence rates lower than 100 per 100,000 population:
- (1)
- Systematic testing and treatment of latent TB infection in adult contacts of pulmonary TB cases
- (2)
- Systematic testing and treatment of latent TB infection in immigrants from high TB burden countries.
- (3)
- Detection of latent TB infection based on interferon-gamma release assays (IGRA) or Mantoux tuberculin skin test (TST).
- (4)
- Detection of TB disease in individuals with TB symptoms or radiological abnormalities.
- (5)
- Administration of TB preventive treatments in individuals with latent TB infection.
- (6)
- Clinical monitoring of individuals receiving TB preventive treatment.
Based on the results of the sixth systematic review assessing their efficacy and safety [9], the WHO Guidelines on management of latent TB infection recommended the following TB preventive treatments: 3–4 months rifampicin, 3– 4 months isoniazid and rifampicin, 3 month regimen of weekly rifapentine and isoniazid, 6 month isoniazid, 9 month isoniazid [6,7,8].
Screening and treating adult contacts with latent TB infection of pulmonary TB cases must be a priority preventive intervention to prevent TB transmission and to achieve the global targets of the End TB strategy for several reasons. Firstly, treatment benefits outweigh treatment adverse effects [6,7,8,9]. Secondly, contacts of TB cases have an increased risk of progression from TB infection to TB disease compared to the general population [2,3,6,7,8]. Thirdly, TB preventive treatments can prevent progression from TB infection to TB disease in adult contacts [2,7,8]. Nevertheless, adherence to TB preventive treatment is necessary to achieve treatment effectiveness in preventing progression from TB infection to TB disease and consequently to prevent TB transmission in the community [6,7,8,10,11]. A study carried out in Spain, found a 11.1% (CI: 5.1–23.3) risk of TB at 5 years among contacts of pulmonary TB cases who did not complete the TB preventive treatment and 1.2% (95% CI: 0.5–3.0) among those who did [10].
In Catalonia, a region in the North-East of Spain with 8 million inhabitants, the incidence of TB was 12.5 cases per 100,000 inhabitants in 2021 [12]. TB incidence increased by 15.7% in 2021 compared with 2020 [12]. Detecting and treating adult contacts of pulmonary TB cases with latent TB infection is a priority public health intervention to prevent TB transmission and reduce TB morbidity and mortality in Catalonia, Spain [2,6,8,11]. The success of this strategy depends on achieving low percentages of TB preventive treatment non-adherence among adult contacts with latent TB infection [4,6,7,11].
The aim of the study was to assess non-adherence to TB preventive treatment and to identify factors associated with treatment non-adherence among adult contacts of pulmonary TB cases with latent TB infection in Catalonia in the 2019−2021 period.
2. Materials and Methods
2.1. Study Design
A population based cross sectional analytical study was performed. Adherence to TB preventive treatment was evaluated among contacts aged 18 years or older of new cases of pulmonary TB registered in Catalonia from 1 January 2019 to 30 June 2021.
All contacts aged 18 years or older (residing in Catalonia) with a latent TB infection who received a TB preventive treatment were included in the study. The latent TB infection was detected among contacts using the tuberculin test and/or the interferon gamma detection test (IGRA). Contacts with positive IGRA or tuberculin test (≥ 5 millimeters) results were considered infected [7,11]. Contacts with a positive test underwent a chest X-ray to detect radiographic anomalies compatible with pulmonary TB. Contacts presenting radiographic anomalies gave a sputum sample to determine the presence of acid-alcohol-resistant bacilli, make a culture and rule out TB [6,7]. Contacts presenting TB disease were excluded from the study.
2.2. Data Collection
A questionnaire was used to collect the following socio-demographic and health information: age, gender, place of birth, place of residence, exposure type, exposure duration, TB preventive treatment, adherence to TB preventive treatment, smoking habit, BCG vaccination, high-risk alcohol consumption, exposure to an index case without laboratory confirmed TB (smear, culture), exposure to an index case with pulmonary anomalies compatible with TB detected by computed tomography.
2.2. Data Analysis
Contacts were classified into two groups of TB preventive treatment adherence: 1) fully adherent if they had completed 80% or more of doses, and 2) non-adherent if they had completed less than 80% of doses [13,16,17]. TB preventive treatment regimens were classified into three categories: 1) short term regimen (rifampicin and isoniazid for three months, rifampicin for four months); 2) long term regimen (isoniazid for six and nine months); and 3) undefined regimen [6,7,8].
The exposure type was classified into four categories, based on the environment where the exposure was produced: cohabiting household, school, workplace, and recreational or ludic. The exposure duration was classified into four categories: daily exposure during 6 or more hours; daily exposure during less than 6 hours per day and ≥6 hours per week; daily exposure during less than 6 hours per week; and sporadic but intense contact (i.e. sharing car, sharing space in a poor ventilated places). High-risk alcohol consumption was defined as a daily consumption >40 grams in men and >24 grams in women or a medical record indicating alcohol abuse. Contacts were classified by their smoking habit into four categories: daily smoker, occasional smoker (at least 1 time per week), ex-smoker and never smoker.
Percentages and their 95% CI were determined for qualitative variables and means and standard deviations (SD) for quantitative variables. The Chi square test (Fisher’s exact test when necessary) and the Odds Ratios (OR) were used to assess the association between non-adherence to TB preventive treatment and study variables, considering a p < 0.05 as statistically significant. The crude ORs were adjusted using multiple logistic regression analysis, considering a p < 0.05 as statistically significant.
2.3. Bivariate Correlation among Study Variables
Bivariate correlation between TB preventive treatment non-adherence and factors significantly associated with this variable in the univariable analysis and among different significant factors were assessed using the Spearman’s rank correlation coefficient (ρ). A p<0.05 was considered as statistically significant. Binary dummy variables were developed for the following variables: TB preventive treatment regimen (short-term regimen vs. long-term/undefined regimen); exposure duration (<6 hours per week/sporadic exposure vs. ≥6 hours per week); high-risk alcohol consumption (yes vs. no); smoking habit (yes vs. no); exposure type (school/workplace exposure vs. cohabiting household/recreational exposure); contact age (≥30 years vs. <30 years); immigrant contact (yes vs. no); contact gender (male vs. female); exposure to an index case without laboratory TB confirmation (yes vs. no).
2.4. Multivariate Logistic Regression Analysis
Multivariable logistic regression analysis was used to detect factors associated independently with non-adherence to latent TB infection treatment. Two multivariable logistic regression models were developed: the full model and the reduced model. The full logistic regression model included all significant variables detected in the univariable analysis and age. The reduced model was developed using the forward variable selection method, using a probability-of-F-to-enter ≤ 0.05 and probability-of-F-to-remove ≥0.10. The reduced model was developed to obtain an optimal multivariable model with a lower number of variables than the full model. The statistical analysis was carried out using IBM-SPSS Version 18 (IBM-SPSS, Chicago, IL, USA).
3. Results
3.1. Population Studied
A total number of 984 contacts aged 18 years or more who received TB preventive treatment were included in the study (Figure 1).
1004 new cases of pulmonary TB and their 8107 contacts were registered by epidemiological services of Catalonia during the study period. 5504 (67.9%) contacts were aged 18 years or more and 1713 (31.1%) of them had a positive test (tuberculin, IGRA) for latent TB infection without TB disease (Figure 1). 984 (57.4%) contacts received a TB preventive treatment. 751 (76.3%) contacts were fully adherent to TB preventive treatment and 233 (23.7%) were non-adherent to TB preventive treatment (Figure 1).
3.1. Non-adherence to TB Preventive Treatement
This study found a percentage TB preventive treatment non-adherence among adult contacts of pulmonary TB cases of 23.7% (95% CI: 21.0−26.4%) (Table 1). A similar mean age was observed among fully adherent contacts (42 years; SD: 14.2) and non-adherent contacts (42.8 years, SD: 13).
Percentages of non-adherence to TB preventive treatment among adult contacts were significantly higher in the following situations: contacts exposed at school or workplace; contacts on short-term treatment regimen; contacts exposed to an index case without laboratory confirmation of TB; contacts with a high-risk alcohol consumption; contacts with an exposure duration lower than 6 hours per week or sporadic exposure; daily or occasional smokers; immigrant contacts; male contacts (Table 1).
Percentages of non-adherence to TB preventive treatment were 2 or more times greater in contacts with an exposure at school or workplace than in those exposed through cohabitation or a recreational activity; in contacts on long-term or undefined regimen than in those on short-term regimen; and in contacts exposed to an index case without TB laboratory confirmation than in those exposed to an index case with laboratory confirmation (Table 1). Percentages of non-adherence to TB preventive treatment less than 2 times greater in males than in females; in contacts with an exposure duration lower than 6 hours per week or sporadic exposure than in those with an exposure duration lower than 6 hours per week; in immigrant contacts than in autochthonous contacts; in daily or occasional smokers than in ex-smokers or never smokers; and in contacts with a high-risk alcohol consumption than in those without a high-risk alcohol consumption (Table 1).
Percentages of non-adherence to TB preventive treatment were higher in contacts aged 30 years or older and contacts vaccinated with the BCG vaccine compared to contacts aged 18-29 years and unvaccinated contacts, respectively, but the differences were not statistically significant (Table 1).
Percentages of treatment non-adherence in 2019, 2020 and 2021 were slightly different: 23.7% (95% CI: 19.7−27.7) in 2019, 17.6% (95% CI: 11.1−24.0) in 2020 and 24.7% (95% CI: 14.9−34.5) in 2021. Nevertheless, the differences were not statistically significant.
Contacts with multidrug-resistant TB (MDR-TB) or rifampicin resistant TB (RR-TB) have not been reported in this study. Adverse effects of latent TB infection treatment were not investigated in this study, but an adverse drug effect was reported for 19 (8.1%) contacts with non-adherence to TB preventive treatment.
Percentages of non-adherence to TB preventive treatment among contacts without data for the smoking habit (25.3%) and BCG vaccination (21.1%) were not different from the non-adherence percentage found in the study (23.7%).
3.2. Bivariate Correlation among Study Variables
Non-adherence to TB preventive treatment correlated significantly with the following variables (factors): treatment regimen (ρ = − 0.17, p < 0.001); contact gender (ρ = 0.06, p < 0.05); exposure duration (ρ = 0.11, p < 0.01); exposure type (ρ = 0.20, p < 0.001); high-risk alcohol consumption (ρ = 0.08, p < 0.05); smoking habit (ρ = 0.08, p < 0.05); immigrant contact (ρ = 0.07, p < 0.05); exposure to an index case without laboratory TB confirmation (ρ = 0.11, p < 0.01 (Supplementary Materials Table S1). The bivariate correlation between treatment non-adherence and treatment regimen was negative because short-term treatment regimens decreased treatment non-adherence.
The factor TB preventive treatment regimen correlated significantly with the following variables: exposure type (ρ = −0.07, p < 0.05); high-risk alcohol consumption (ρ = − 0.15, p < 0.001); smoking habit (ρ = −0.35, p < 0.001) and immigrant contact (ρ = 0.14, p < 0.001) (Supplementary Materials Table S1).
Other significant bivariate correlations were detected between the following variables: exposure type and exposure duration; exposure type and high-risk alcohol consumption; exposure type and smoking habit; exposure type and immigrant contact; exposure duration and high-risk alcohol consumption; exposure duration and immigrant contact; high-risk alcohol consumption and smoking habit; high-risk alcohol consumption and exposure to an index case without laboratory TB confirmation; smoking habit and immigrant contact; smoking habit and exposure to an index case without laboratory TB confirmation; immigrant contact and exposure to index case without laboratory TB confirmation (Supplementary Materials Table S1).
3.3. Multivariate Logistic Regression Analysis
The full multivariable logistic regression model, including the statistically significant variables detected in the univariable analysis, determined that only five factors were independently associated to TB preventive treatment non-adherence: treatment regimen, exposure type, index case without laboratory TB confirmation; immigration and contact gender (Table 2). Exposure at workplace or school (aOR = 3.19), exposure to an index case without laboratory confirmation of TB (aOR = 2.16), immigrant contact (aOR = 2.00) and male gender (aOR = 1.56) increased significantly treatment non-adherence, while short-term TB preventive treatment regimen (aOR = 0.44) reduced significantly treatment non-adherence (Table 2).
The reduced multivariable logistic regression model determined that six factors were independently associated to TB preventive treatment non-adherence: treatment regimen, exposure type, exposure to an index case without laboratory TB confirmation, immigration, contact gender and exposure duration (Table 2). The factors “exposure at school or workplace” (aOR = 3.34), “exposure to an index case without laboratory confirmation of TB” (aOR = 2.07), “immigrant contact” (aOR = 1.81), “male gender” (aOR = 1.75) and “low exposure duration” (aOR = 1.60) increased significantly TB preventive treatment non-adherence among adult contacts (Table 2). By contrast, the factor “short-term TB preventive treatment regimen” (aOR = 0.38) reduce significantly treatment non-adherence among adult contacts.
The forward selection method of SPSS program introduced the six factors in the model in the following order: exposure type, treatment regimen, immigration, contact gender, index case without laboratory TB confirmation, and exposure duration. The reduced logistic regression model included the factor exposure duration as an independent factor for treatment non-adherence after excluding the variables high-risk alcohol consumption and smoking habit from the model.
4. Discussion
Adherence to TB preventive treatment among adult contacts with latent TB infection is necessary for preventing progression from TB infection to TB disease [7,8,11,14]. The study found a percentage of non-adherence to TB preventive treatment of 23.7% among adult contacts of TB pulmonary cases in Catalonia, Spain. The multiple logistic regression analysis revealed that five factors increased (positive effect) and one factor decreased (negative effect) treatment non-adherence. The factors increasing TB preventive treatment included “exposure at school or workplace”, “short-term treatment regimen”, “exposure duration lower than 6 hours per week”, “exposure to an index TB case without laboratory confirmation of TB”, “immigrant contact” and “male gender”. By contrast, the factor “short-term treatment regimen” decreased treatment non-adherence. The six factors were associated with the treatment non-adherence independently of the effect on the treatment non-adherence of the other factors.
The factors “high-risk alcohol consumption” and “smoking habit” were associated with treatment non-adherence only in the univariable analysis. Consequently, their effects on the treatment non-adherence could be explained by their correlations with one of more of the factors included in the multivariable logistic regression models.
The factor exposure at school or workplace had the highest positive effect on treatment non-adherence, as it increased non-adherence by 234%. The factor index cases without laboratory confirmation of TB increased treatment non-adherence by 107%. The other three factors with a positive effect on treatment non-adherence (immigrant contact, male gender, low exposure duration) increased treatment non-adherence by 60−81%. By contrast, the factor short-term TB preventive treatment reduced the TB preventive treatment non-adherence by 62%.
The percentages of TB preventive treatment non-adherence among adult contacts of pulmonary TB cases found in Catalonia, Spain, in this study were similar or higher than that found in studies carried out in Spain [15,16,17,18]. In a study carried out in the province of Lleida in 2016, a non-adherence rate of 29.7 % was found in a cohort of 199 contacts (average of age of 45.1 years) [16]. In a study carried out in the city of Barcelona in 2019, a non-adherence percentage of 29.9% was found in a cohort of 184 infected contacts [17]. In a study carried out in the province of Alicante in 2011, a non-adherence percentage of 19.6% was found in a cohort of 338 contacts (average age of 34.1 years) [17]. In a study carried out in the city of Barcelona by the Vall d’Hebron Hospital in 2018−2020, a non-adherence percentage of 13.4% (95% CI: 9.1−17.7%) was found among 261 (24.1%) contacts [18]. Nevertheless, it is difficult to compare non-adherence rates observed in different studies due to their different methodologies and settings. The study carried out of in Alicante included contacts attended by Public Health Services and by the Preventive Medicine Service of Sant Joan Hospital, Alicante, and only tuberculin tests were used to detect latent TB infections [17]. In the study carried out by the Vall d’Hebron Hospital, contacts were treated by the hospital [18].
The percentages of TB preventive treatment non-adherence among adult contacts found in this study were similar, greater or lower than the percentages found in other studies carried out worldwide [19,20,21,22,23]. A systematic review and meta-analysis assessing barriers to TB preventive treatment adherence found percentages of non-adherence to TB preventive treatment ranging from 10% to 81% [19]. A prospective cohort study carried out in Norway in 2016 that included 726 individuals notified about TB preventive treatment by the Norwegian Surveillance System for Infectious Diseases found a non-adherence percentage of 9% [20]. A study carried out in Sweden in 2000−2007 found a non-adherence percentage of 24% [21]. A systematic review of studies assessing adherence to TB preventive treatment in the USA and Canada between 1997 and 2007 found non-adherence percentages ranging from 9% to 28% [22]. Nevertheless, it is difficult to compare the non-adherence percentages found in different studies due to differences in study design, study period, setting, population, treatment adherence definition and latent TB infection detection method.
Previous studies carried out in Spain found similar but not significant results for the factors associated to adherence to TB preventive treatment among contacts of TB cases. In the study carried out in Lleida in 2016, the percentage of adherence to TB preventive treatment was higher in women, autochthonous contacts, cohabitants of the index case and those exposed through cohabitation, although the differences were not statistically significant in the univariable and multivariable logistic regression analyses [16]. The crude ORs for adherence to TB preventive treatment were 1.7 (95% CI: 0.9−3.1) for women, 1.8 (95% CI: 1-0−3.4) for autochthonous contacts, 1.5 (95% CI: 0.8−2.9) for contacts cohabiting with an index case, and 1.4 (95% CI: 0.7−2.9) for household contacts [17]. The adjusted ORs were of 1.2 (95% CI: 0.6−2.4) for women, 1.5 (95% CI: 0.7−3.2) for autochthonous contacts, and 1.5 (95% CI: 0.9−3.7) for contacts cohabiting with an index case and 1.4 (95% CI: 0.7−2.9) for household contacts [16]. In the study carried out in Barcelona city, TB preventive treatment adherence among immigrants was a little higher compared to the Spanish-born populations (71.2% vs 67.8%) but adherence increased to 91.4% for the primary chemoprophylaxis cases [10]. In the study carried out in Alicante in 2011, the adherence to TB preventive treatment was lower in men and immigrant contacts, although the differences were not statistically significant in the univariable and multivariable logistic regression analyses [17]. The crude ORs were 0.6 (95% CI: 0.3−1.2) for men and 0.6 (0.3−1.3) for immigrant contacts. The adjusted ORs were of 0.4 (95% CI: 0.2−1.0) for men and 0.8 (0.3−2.1) for immigrant contacts [17].
Studies carried out worldwide found factors associated with TB preventive treatment adherence similar to those found in this study (treatment duration, immigrant contact), and factors different to those found in this study, such as absence of perception of risk, alcohol and drug use and unemployment [11,14,19,20,21,22,23,24,25]. Several studies found that short-term TB preventive treatment regimens were associated with a greater treatment adherence than long-term treatments [14,24,25,26,27]. Nevertheless, other studies did not find significant differences for treatment adherence using different regimens [20]. Currently, short-term TB preventive regimens are recommended based on their similar effectiveness compared with 6–9 months of isoniazid, favorable tolerability and higher treatment adherence [6,7,8,11,26,27].
Global targets and milestones for reductions in the burden of TB disease, in terms of TB incidence and number of TB deaths, have been proposed by the World Health Organization (WHO) and United Nations (UN) through the adoption of the WHO End TB Strategy (2016–2035) [4,5,28]. In regions such as Catalonia, which have already achieved less than 100 TB cases per million, the TB incidence objective of less than 1 TB case per million population should be achieved by 2050 [7,8]. The European Center for Disease Control and Prevention (ECDC) [11], the World Health Organization (WHO) Guidelines on TB [6] the WHO Guidelines on management of latent TB infection [7,8], the World Health Organization End of TB strategy [28] and the WHO’s Consolidated guidelines for programmatic management of latent TB infection [29] consider that contacts of pulmonary TB cases must be a priority population group for developing screening and TB preventive treatment activities. The global targets set in 2023 for the 2023−2027 period included to achieve 90% coverage of TB preventive treatment among contacts of pulmonary TB cases and other population groups at high risk of developing TB disease [2]. To achieve this objective is necessary to develop a programmatic approach [29] and to assess the health system, human, pharmaceutical and economic resources necessary. The programmatic approach includes the following activities: 1) identification of individuals at highest risk; 2) testing for TB infection; 3) excluding TB disease; 4) choosing the treatment option that is best suited to an individual; 5) managing treatment adverse events; 6) supporting medication adherence; and 7) monitoring programmatic performance [29].
The elements in TB prevention and control programs are based on all that is known about the clinical aspects, bacteriology, pathogenesis, epidemiology, prevention and treatment of the disease. The results obtained in this study showed that more human, pharmaceutical and economic resources are necessary in Catalonia, Spain, to increase adherence to treatment among contacts of pulmonary TB cases. The identification of factors associated with non-adherence to TB preventive treatment among contacts of pulmonary TB cases is important for guiding prevention activities to increase TB preventive treatment adherence in Catalonia, Spain. Based on the results obtained in this study, the following strategies can be used to increase treatment adherence: 1) to use short-term treatment regimens; and 2) to develop health education activities to improve treatment adherence among adult contacts with latent TB infection. A higher priority for health education activities should be given to the following groups: 1) contacts exposed at school or workplace; 2) contacts with an exposure duration lower than 6 hours per week; 3) contacts exposed to an index TB case without laboratory confirmation of TB; 4) immigrant contacts, and 5) male contacts.
In this study, an exposure to an index case without TB laboratory confirmation of TB. This finding suggests that contacts exposed to an index case without laboratory confirmation of TB could have a lower perception of TB risk compared to that for contacts exposed to an index case with laboratory confirmation of TB. For this reason, this group of contacts should have a higher priority for health education activities. All adult contacts included in this study had been exposed to confirmed cases of pulmonary TB. The TB disease was confirmed in index cases based on clinical data, laboratory tests, radiography and epidemiological data [2,6]. A positive result for acid-fast-bacilli (AFB) on a sputum smear (or other specimen) or/and a positive culture result confirmed TB disease among most index cases, although 9.4% of the contacts included in this study had been exposed to an index case without laboratory TB confirmation. In fact, a bacteriologic confirmation of pulmonary TB cannot be established in at least 15 to 20 % of patients with a clinical diagnosis of TB [30,31].
Other strategies proposed to increase treatment adherence among contacts of TB cases include the following ones: 1) to develop interventions to motivate patients and staff; 2) to develop social interventions; 3) to develop cultural interventions; and 4) to use advanced methods for assessing and monitoring TB preventive treatment adherence, such as direct observed therapy (DOT) [11,14,22,26].
This study presents several limitations. Firstly, non-adherence to TB preventive treatment was defined as less than 80% of doses. A definition for non-adherence based on dose-by-dose medication-taking could be more precise [32,33]. Nevertheless, the dose-by-dose data could not be obtained in this study, and fully adherence and non-adherence to TB preventive treatments was detected based on the 80% threshold in many studies [13,16,17,34], Secondly, the exposure duration was assessed using a qualitative approach based on four categories, which did not take into account the volume of air shared. However, this approach could make it possible a fast and simple evaluation. Thirdly, this study included all contacts of pulmonary TB cases reported by epidemiological services during the study period. Percentages of non-adherence to TB preventive treatment could be lower or lower than those observed in this study in different population groups if they were under or over reported by epidemiological services, respectively. Nevertheless, the development of a study for assessing whether fully adherence (completion) to TB preventive treatment was under or over reported was not possible due to economic and time limitations.
5. Conclusions
Non-adherence to TB preventive treatment among contacts of 18 years or more of cases of TB pulmonary found in this study was of 23.7%. The factors associated with non-adherence to TB preventive treatment detected in this study included the exposure at school or workplace, index cases without laboratory confirmation of TB, immigration, smoking habit, low exposure duration and male gender. Adherence to TB preventive treatment should be improved among adult contacts with latent TB infection of TB pulmonary cases by recommending short-term treatment regimens and by developing health education activities, with the higher priority focused on contacts with factors associated with treatment non-adherence.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Bivariate correlation among study variables. The correlation among study variables was assessed using the Spearman’s rank correlation coefficient (ρ). Binary dummy variables were developed for the following variables: TB preventive treatment regimen (short-term regimen vs. long-term/undefined regimen); exposure time (<6 hours per week/sporadic vs. ≥6 hours per week); exposure high-risk alcohol consumption (yes vs. no); smoking habit (yes vs. no); exposure type (workplace/school vs. cohabiting household/recreational); age (≥30 years vs. <30 years); immigration (yes vs. no); index case without laboratory TB confirmation (yes vs. no); gender (male vs. female).
Author Contributions
Conceptualization, P-R.,S.G.,D.T.,A.D.,I.P.,J.C.,J.P.M. and P.G; methodology, P.P-R. and P.G.; software, P.P-R. and I.P.; validation, P.P-R.,I.P and S.G.; formal analysis, P.P-R.,P.G.; investigation, P.P-R.,S.G.,D.T.,A.D.,I.P.,J.C.,J.P.M. and P.G.; resources, P.P-R.,S.G.,D.T.,A.D.,I.P.,J.C.,J.A.M. and P.G,; data curation, P.P-R., J.C. and I.P.; writing—original draft preparation, P.P-R.; writing—review and editing, P.P-R.,S.G.,D.T.,A.D.,I.P.,J.C.,J.P.M. and P.G; supervision, P.P-R.,S.G.,D.T.,A.D.,I.P.,J.C.,J.P.M. and P.G.; project administration, P.P-R.,S.G.,D.T.,A.D.,I.P.,J.C.,J.P.M. and P.G.; funding acquisition, P.P-R.,D.T.,I.P.,J.C. and P.G. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by a “Strategic Action in Health 2019−2021” research grant from the Instituto de Salud Carlos III, Ministry of Science and Innovation, Spain (Project PI18/01751).
Institutional Review Board Statement
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Arnau Vilanova University Hospital, Lleida, Spain (code: CEIC-2049).
Informed Consent Statement
Verbal informed consent was obtained from all individuals participant in the study.
Data Availability Statement
Data collected could be made available.
Acknowledgments
Authors would like to thank to all physicians and epidemiologists who have reported cases of pulmonary TB and registered their contacts.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shah, M.; Dorman, S.E. Latent Tuberculosis Infection. N. Engl. J. Med 2021, 385, 2271–2280. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global tuberculosis report 2023; World Health Organization: Geneva, 2023. [Google Scholar]
- Menzies, N.A.; Wolf, E.; Connors, D.; Bellerose, M.; Sbarra, A.N.; Cohen, T.; Hill, A.N.; Yaesoubi, R.; Galer, K.; White, P.J.; Abubakar, I.; Salomon, J.A. Progression from latent infection to active disease in dynamic tuberculosis transmission models: a systematic review of the validity of modelling assumptions. Lancet Infect. Dis. 2018; 18, e228–e38. [Google Scholar]
- World Health Organization (WHO). The End TB strategy. World Health Organization: Geneve, 2015; Available online: https://iris.who.int/bitstream/handle/10665/331326/WHO-HTM-TB-2015.19-eng.pdf?sequence=1 (accessed on 22 December 2023).
- United Nations (UN). Resolution adopted by the General Assembly on 5 October 2023. Political declaration of the high-level meeting on the fight against tuberculosis. Advancing science, finance and innovation, and their benefits, to urgently end the global tuberculosis epidemic, in particular by ensuring equitable access to prevention, testing, treatment and care. Available online: https://documents-dds-ny.un.org/doc/UNDOC/GEN/N23/306/91/PDF/N2330691.pdf?OpenElement (accessed on 12 January 2024).
- World Health Organization (WHO). Consolidated guidelines on tuberculosis. Module 1: prevention – tuberculosis preventive treatment; World Health Organization: Geneva, 2020. [Google Scholar]
- World Health Organization (WHO). Guidelines on the management of latent tuberculosis infection; WHO: Genera, 2015. [Google Scholar]
- Getahun, H.; Matteelli, A.; Abubakar, I.; Aziz, M.A.; Baddeley, A.; Barreira, D.; Den Boon, S.; Borroto Gutierrez, S.M.; Bruchfeld, J.; Burhan, E.; Cavalcante, S.; Cedillos, R.; Chaisson, R.; Chee, C.B.; Chesire, L.; Corbett, E.; Dara, M.; Denholm, J.; de Vries, G.; Falzon, D.; Ford, N.; Gale-Rowe, M.; Gilpin, C.; Girardi, E.; Go, U.Y.; Govindasamy, D.; Grant, A.; Grzemska, M.; Harris, R.; Horsburgh, C.R.; Ismayilov, A.; Jaramillo, E.; Kik, S.; Kranzer, K.; Lienhardt, C.; LoBue, P.; Lönnroth, K.; Marks, G.; Menzies, D.; Migliori, G.B.; Mosca, D.; Mukadi, Y.D.; Mwinga, A.; Nelson, L.; Nishikiori, N.; Oordt-Speets, A.; Rangaka, M.X.; Reis, A.; Rotz, L.; Sandgren, A.; Sañé Schepisi, M.; Schünemann, H.J.; Sharma, S.K.; Sotgiu, G.; Stagg, H.R.; Sterling, T.R.; Tayeb, T.; Uplekar, M.; van der Werf, M.J.; Vandevelde, W.; van Kessel, F.; van't Hoog, A.; Varma, J.K.; Vezhnina, N.; Voniatis, C.; Vonk Noordegraaf-Schouten, M.; Weil, D.; Weyer, K.; Wilkinson, R.J.; Yoshiyama, T.; Zellweger, J.P.; Raviglione, M. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur. Respir. J. 2015, 46, 1563–1576. [Google Scholar] [CrossRef] [PubMed]
- Stagg, H.R.; Zenner, D.; Harris, R.J.; Muñoz, I.; Lipman, M.C.; Abubakar, I. Treatment of latent tuberculosis infection: a network meta-analysis. Ann. Intern. Med. 2014, 161, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Martin-Sanchez, M.; Brugueras, S.; de Andre´s, A.; Simon, P.; Gorrindo, P.; Ros, M.; et al. Tuberculosis incidence among infected contacts detected through contact tracing of smear-positive patients. PLoS ONE 2019, 14, e0215322. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Programmatic management of latent tuberculosis infection in the European Union; ECDC: Stockholm, 2018. [Google Scholar]
- Departament de Salut. Memòria de la Secretaria de Salut Pública; Departament de Salut: Barcelona, 2023; Available online: https://salutpublica.gencat.cat/web/.content/minisite/aspcat/publicacio_formacio_recerca/publicacions/corporatives/memoria-sp-2021.pdf.
- Patel, A.R.; Campbell, J.R.; Sadatsafavi, M.; Marra, F.; Johnston, J.C.; Smillie, K.; Lester, R.T. Burden of non-adherence to latent tuberculosis infection drug therapy and the potential cost-effectiveness of adherence interventions in Canada: a simulation study. BMJ Open 2017, 7, e015108. [Google Scholar] [CrossRef] [PubMed]
- Stuurman, A.L.; Vonk Noordegraaf-Schouten, M.; van Kessel, F.; Oordt-Speets, A.M.; Sandgren, A.; van der Werf, M.J. Interventions for improving adherence to treatment for latent tuberculosis infection: a systematic review. BMC Infect. Dis. 2016, 16, 257. [Google Scholar] [CrossRef] [PubMed]
- Pina-Gutiérrez, J.M.; Ferrer-Traid, A.; Arias, C.; Sala-Farré, M.R.; López-Sanmartín, J.I. Cumplimiento y efectividad del tratamiento de la infección tuberculosa con isoniazida durante 9 meses en una cohorte de 755 pacientes. Med. Clin. (Barcelona) 2018, 103, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Ambrona de Marcos, V.; Bach Foradada, P.; Alsedà Graells, M.; Duque Jiménez, T.; Delgado Roche, E.; Aguilar Ariza, R.; Bravo Andrés, N.; Godoy, P. Cumplimiento del tratamiento de la infección tuberculosa latente en una cohorte de contactos de enfermos de tuberculosis. Rev. Esp. Salud Pública 2018, 92, e1–e11. [Google Scholar]
- Gallardo, C.R.; Gea Velázquez de Castro, M.T.; Requena Puche, J.; Miralles Bueno, J.J.; Rigo Medrano, M.V.; Aranaz Andrés, J.M. Factores asociados a la adherencia en el tratamiento de la infección tuberculosa. Aten. Primaria. 2014, 46, 6–14. [Google Scholar] [CrossRef]
- Puyana Ortiz, J.D.; Garcés Rodríguez, A.C.; Aznar, M.L.; Espinosa Pereiro, J.; Sánchez-Montalvá, A.; Martínez-Campreciós, J.; Saborit, N.; Rodrigo-Pendás, J.Á.; García Salgado, G.; Broto Cortes, C.; Delcor, N.S.; Oliveira, I.; Treviño Maruri, B.; Ciruelo, D.P.; Salvador, F.; Bosch-Nicolau, P.; Torrecilla-Martínez, I.; Zules-Oña, R.; Tórtola Fernández, M.T.; Molina, I. Adherence and Toxicity during the Treatment of Latent Tuberculous Infection in a Referral Center in Spain. Trop. Med. Infect. Dis. 2023, 8, 373. [Google Scholar] [CrossRef]
- Liu, Y.; Birch, S.; Newbold, K.B.; Essue, B.M. Barriers to treatment adherence for individuals with latent tuberculosis infection: A systematic search and narrative synthesis of the literature. Int. J. Health Plann. Manage. 2018, 33, e416–e433. [Google Scholar] [CrossRef] [PubMed]
- Schein, Y.L; Madebo, T.; Andersen, H.E.; Arnesen, T.M.; Dyrhol-Riise, A.M.; Tveiten, H.; White, R.A.; Winje, B.A. Treatment completion for latent tuberculosis infection in Norway: a prospective cohort study. BMC Infect. Dis. 2018, 18, 587. [Google Scholar] [CrossRef] [PubMed]
- Kan, B.; Kalin, M.; Bruchfeld, J. Completing treatment for latent tuberculosis: patient background matters. Int. J. Tuberc. Lung Dis. 2013, 17, 597–602. [Google Scholar] [CrossRef]
- Hirsch-Moverman, Y.; Daftary, A.; Franks, J.; Colson, P.W. Adherence to treatment for latent tuberculosis infection: systematic review of studies in the US and Canada. Int. J. Tuberc. Lung Dis. 2008, 12, 1235–1254. [Google Scholar] [PubMed]
- Rustage, K.; Lobe, J.; Hayward, S.E.; Kristensen, K.L.; Margineanu, I.; Stienstra, Y.; Goletti, D.; Zenner, D.; Noori, T.; Pareek, M.; Greenaway, C.; Friedland, J.S.; Nellums, L.B.; Hargreaves, S.; ESGITM and ESGMYC study groups. Initiation and completion of treatment for latent tuberculosis infection in migrants globally: a systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1701–1712. [Google Scholar] [CrossRef]
- Spyridis, N.P.; Spyridis, P.G.; Gelesme, A.; Sypsa, V.; Valianatou, M.; Metsou, F.; Gourgiotis, D.; Tsolia, M.N. The effectiveness of a 9-month regimen of isoniazid alone versus 3-and 4-month regimens of isoniazid plus rifampin for treatment of latent tuberculosis infection in children: results of an 11-year randomized study. Clin. Infect. Dis. 2007, 45, 715–722. [Google Scholar] [CrossRef]
- Sterling, T.R.; Njie, G.; Zenner, D.; Cohn, D.L.; Reves, R.; Ahmed, A.; Menzies, D.; Horsburgh, C.R.; Crane, C.M.; Burgos, M.; LoBue, P.; Winston, C.A.; Belknap, R. Guidelines for the Treatment of Latent Tuberculosis Infection: Recommendations from the National Tuberculosis Controllers Association and CDC, 2020. MMWR Recomm. Rep. 2020, 69, 1–11. [Google Scholar] [CrossRef]
- Chee, C.B.E.; Reves, R.; Zhang, Y.; Belknap, R. Latent tuberculosis infection: Opportunities and challenges. Respirology 2018, 10, 893–900. [Google Scholar] [CrossRef]
- Shah, R.; Khakhkhar, T.; Modi, B. Efficacy and Safety of Different Drug Regimens for Tuberculosis Preventive Treatment: A Systematic Review and Meta-Analysis. Cureus 2023, 15, e38182. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Implementing the end TB strategy: essentials; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organization (WHO). Latent TB Infection: Updated and consolidated guidelines for programmatic management. World Health Organization: Geneva, 2018; Available online: http://apps.who.int/iris/bitstream/handle/10665/260233/9789241550239-eng.pdf (accessed on 7 January 2023).
- Centers for Disease Control and Prevention CDC. Reported Tuberculosis in the United States:, 2016; US Department of Health and Human Services; CDC: Atlanta, GA, 2017. Available online: https://www.cdc.gov/tb/statistics/reports/2016/pdfs/2016_Surveillance_FullReport.pdf (accessed on 12 January 2024).
- Taylor, Z.; Marks, S.M.; Ríos Burrows, N.M.; Weis, S.E.; Stricof, R.L.; Miller, B. Causes and costs of hospitalization of tuberculosis patients in the United States. Int. J. Tuberc. Lung Dis. 2000, 4, 931−939. [Google Scholar]
- Vrijens, B.; De, G.S.; Hughes, D.A.; Przemys law, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; Matyjaszczyk, M.; Mshelia, C.; Clyne, W.; Aronson, J.K.; Urquhart, J.; ABC Project Team. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef] [PubMed]
- Stagg, H.R.; Flo Stagg, H.R.; Flook, M.; Martinecz, A.; Kielmann, K.; Abel Zur Wiesch, P.; Karat, A.S.; Lipman, M.C.I.; Sloan, D.J.; Walker, E.F.; Fielding, K.L. All nonadherence is equal but is some more equal than others? Tuberculosis in the digital era. ERJ Open Res. 2020, 6, 00315–2020. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Dion, M.J.; Rabinovitch, B.; Mannix, S.; Brassard, P.; Schwartzman, K. Treatment completion and costs of a randomized trial of rifampin for 4 months versus isoniazid for 9 months. Am. J. Respir. Crit. Care Med. 2004, 170, 445–449. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flux diagram of the study.
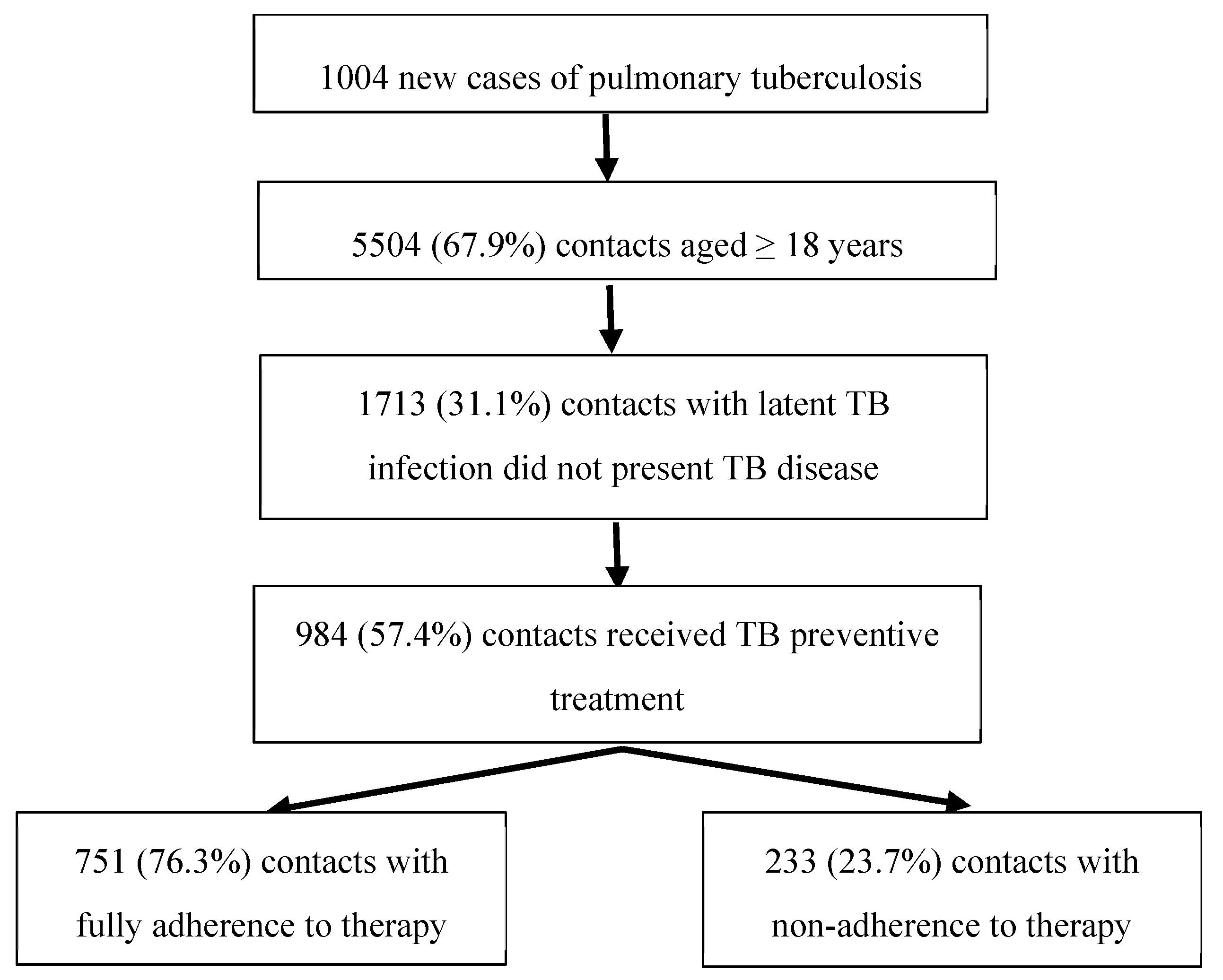

Table 1.
Factors associated with non-adherence to TB preventive treatment among contacts aged 18 years or more of pulmonary tuberculosis cases in Catalonia, Spain, in 2019−2021.
Table 1.
Factors associated with non-adherence to TB preventive treatment among contacts aged 18 years or more of pulmonary tuberculosis cases in Catalonia, Spain, in 2019−2021.
|
Variable |
Values |
Non-adherence to TB preventive treatment among contacts of pulmonary TB cases | |||
| No. | % (95% CI) | OR (95% CI) | n | ||
| Age (years) | 18 – 29 30 – 44 45 – 64 ≥64 |
47 75 99 12 |
20.9 (15.3−26.4) 23.4 (16.6−28.2) 25.7 (21.2−30.2) 22.2 (10.2−34.2) |
Reference 1.15 (0.77−1.75) 1.31 (0.88−1.94) 1.08 (0.53−2.21) |
225 320 385 54 |
| Total | 233 | 23.7 (21.0−26.4) | − | 984 | |
| Age (years) | 18 – 29 ≥ 30 years |
47 186 |
20.9 (15.3−26.4) 24.5 (21.4−27.6) |
Reference 1.23 (0.86−1.74) |
225 759 |
| Gender |
Male Female |
142 91 |
26.2 (22.4−30.0)+ 20.6 (16.7−24.5) |
1.37 (1.01−1.85) Reference |
542 442 |
| TB preventive treatment regimena |
Short-term Long-term Undefined |
51 68 114 |
14.6 (10.7−18.4) 26.3 (20.7−31.8)* 30.4 (25.1−32.3)* |
Reference 2.09 (1.39−3.13) 2.54 (1.76−3.68) |
350 259 375 |
| TB preventive treatment regimena | Short-term Long-term or undefined |
51 182 |
14.6 (10.7−18.4) 28.7 (25.1−32.3)* |
Reference 2.36 (1.67−3.32) |
350 634 |
| Exposure duration |
≥6 hours per day <6 h/day and ≥ 6 h/week <6 hours per week Sporadic exposure |
119 35 49 23 |
21.9 (14.8−21.0) 18.1 (30.3−41.6) 37.8 (25.0−26.1)** 28.0 (16.1−55.2) |
1.26 (0.83−1.92) Reference 2.30 (1.39−3.80) 1.76 (0.96−3.22) |
544 193 145 82 |
| Exposure duration |
≥ 6 hours per week <6 hours per week or Sporadic exposure |
154 72 |
20.9 (17.9−23.9)* 31.7 (25.4−38.0) |
Reference 1.76 (1.26−2.45) |
737 227 |
| Exposure type |
Cohabiting household Workplace Recreational School |
110 106 6 10 |
17.9 (14.8−21-0)* 35.9 (30.3−41.6) 14.3 (2.5−26.1) 35.7 (16.1−55.2) |
2.57 (1.88−3.53) 3.36 (1.37−8.25) Reference 1.01 (0.44−2.27) |
615 295 42 28 |
| Exposure type |
Cohabiting household or recreational Workplace or school |
116 116 |
17.7 (14.7−20.6)* 35.9 (30.5−41.3) |
Reference 2.61 (1.93−3.53) |
657 323 |
| Immigrant contact |
Yes No |
115 118 |
27.3 (22.9−31.7)+ 20.9 (17.5−24.4) |
1.42 (1.05−1.90) Reference |
421 563 |
| Smoking habit |
Daily smoker Occasional smoker Ex-smoker Never smoker |
51 49 3 67 |
28.5 (21.6−35.4) 24.9 (18.6−31.2) 14.5 (3.0−36.3) 19.8 (15.4−24.2)+ |
2.39 (0.67−8.47) 1.99 (0.56−7.03) Reference 1.48 (0.42−5.18) |
179 197 21 338 |
| Smoking habit |
Yes No |
100 70 |
26.6 (22.0−31.2)+ 19.5 (15.3−23.7) |
1.50 (1.06−2.11) Reference |
376 359 |
| BCG vaccination |
Yes No |
74 71 |
24.9 (19.8−30.0) 19.2 (15.0−23.3) |
1.37 (0.95−1.99) Reference |
297 370 |
| High-risk alcohol consumption | Yes No |
19 147 |
35.2 (21.5−48.8)+ 21.8 (18.6−25.0) |
1.94 (1.08−3.51) Reference |
54 674 |
| Exposure to an ndex case without laboratory confirmation of TB | Yes No |
34 192 |
38.2 (27.5−48.9)* 22.2 (19.6−25.3) |
2.16 (1.37−3.42) Reference |
89 854 |
| Exposure to an index case with pulmonary TB anomalies detected by computed tomography | Yes No |
49 124 |
25.8 (19.3−32.4) 24.7 (20.8−28.6) |
1.06 (0.72−1.55) Reference |
190 502 |
OR: odds ratio; CI: Confidence interval; TB: Tuberculosis; HIV: Human immunodeficiency virus; Reference: the reference group has an OR = 1; Significance level: * p < 0.001, ** p < 0.005, + p < 0.05; a. Short terms regimens included rifampicin and isoniazid for three months and rifampicin for four months. Long term regimens included isoniazid for six and nine months.
Table 2.
Multivariable logistic regression analysis assessing the variables explaining the non-adherence to TB preventive treatment among contacts aged ≥18 years of pulmonary TB cases in Catalonia, Spain, in 2019−2021.
Table 2.
Multivariable logistic regression analysis assessing the variables explaining the non-adherence to TB preventive treatment among contacts aged ≥18 years of pulmonary TB cases in Catalonia, Spain, in 2019−2021.
|
Variable Values compared |
Full regression model | Reduced regression model | |||
| aOR (95% CI) | p | aOR (95% CI) | p | ||
| Sex | men vs. women | 1.56 (0.94−2.57) | 0.012 | 1.75 (0.97−2.63) | 0.007 |
| Exposure duration |
<6 hours per week or sporadic vs. ≥6 hours per week | 1.54 (0.91−2.47) | 0.072 | 1.60 (0.93−2.55) | 0.049 |
| Exposure type |
workplace or school vs. cohabiting household or recreational |
3.19 (1.57−4.81) | <0.001 | 3.34 (1.61−5.00) | <0.001 |
| Smoking habit | yes vs. no | 1.41 (0.81−2.25) | 0.148 | − | − |
| High-risk alcohol consumption | yes vs. no | 0.93 (0.65−1.92) | 0.839 | − | − |
| Immigrant contact | yes vs. no | 2.00 (1.13−3.11) | 0.002 | 1.81 (1.01−2.72) | 0.004 |
| TB preventive treatment regimen | short-term vs. long-term or undefined | 0.44 (−0.34−0.71) | 0.001 | 0.38 (−0.49−0.61) | <0.001 |
| Exposure to an index case without laboratory TB confirmation | yes vs. no | 2.15 (1.38−3.98) | 0.014 | 2.07 (1.33−3.76) | <0.001 |
| Constant | 0.0.6 (−2.05−0.13) | <0.001 | 0.14 (−1.08−0.34) | <0.001 | |
aOR: adjusted Odds Ratio; CI: confidence Interval; TB: tuberculosis;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



