
Submitted:
01 February 2024
Posted:
02 February 2024
You are already at the latest version
Abstract
Background: Exercise is an accepted intervention to improve the quality of life (QoL) of breast cancer patients. Exercise programs have been developed and all have shown satisfactory results in improving QoL. There is a lack of research comparing different prescription modalities. The aim of this study is to evaluate the effectiveness of physical exercise (in-person, home-based, prescription) on QoL in breast cancer patients actively undergoing treatment; Methods Quasi-experimental study with randomized assignment to three groups (in-person: guided and supervised in-person exercise program; home-based exercise: guided and supervised exercise program with streaming monitoring; recommendation: exercise recommendation). Quality of life was measured using the QLQ-C30 questionnaire. Baseline and 24-week analysis. Results: The total sample analyzed was n=80. QoL improved significantly at 24 weeks in the face-to-face and home-based exercise groups, but not in the advice group. Exercise in all modalities improved fatigue, nausea, vomiting, appetite, and constipation. QoL at 24 weeks depended on active chemotherapy, tumor type, and assigned exercise group (r2 = 0.503; p < 0.001). Conclusions: QoL in breast cancer patients undergoing active treatment improves after a 24-week exercise program, especially in face-to-face and home-based exercise. Home-based exercise, streaming-based recommendation is a viable option for exercise recommendation.
Keywords:
Quality of life
; Breast Cancer
; Chemotherapy
; Exercise Program
1. Introduction
Breast cancer is the most common malignancy in women, accounting for 15% of all new cancer diagnoses worldwide. Its incidence is increasing due to increased life expectancy. Despite advances in early diagnosis and treatment, eradication involves therapies with numerous adverse effects during and after treatment. These include lymphedema, arthralgia, fatigue, osteoporosis, sleep disturbances, cardiotoxicity, peripheral neurotoxicity [1,2,3], and anxiety, fear, and depression [3].
As a result, these patients often experience poor quality of life and overall well-being [4]. This concern has led to the exploration of new strategies to improve the lives of these patients, including both pharmacologic and non-pharmacologic interventions such as the recommendation of physical exercise [5,6,7].
Exercise is an accepted intervention to improve the quality of life of cancer patients due to its benefits in cardiovascular and muscular health and fatigue reduction [1,2,3]. Its practice is safe and feasible at all stages of the oncological process [8], potentially reducing recurrence time, improving survival, and mitigating side effects of cancer treatments [9]. Given these benefits, current guidelines recommend that physical activity be incorporated into the routine of cancer patients [8,10].
However, cancer patients often do not meet the minimum exercise guidelines [11], which recommend 150 minutes per week of moderate-intensity aerobic exercise (heart rate 30-80%) or 75 minutes per week of vigorous exercise [12,13,14], combined with strength training 2-3 times per week [15]. Difficulty balancing daily routines, exercise, and medical appointments contributes to inadequate physical activity [16].
One of the main reasons for not exercising is the fear of causing harm or performing exercises that may be contraindicated in their health status [17]. Therefore, it is recommended that physical activity be performed in structured programs guided by oncology professionals [18], which provides women with a sense of security and increases adherence [19]. This aspect is crucial and challenging due to the scarcity of resources and trained personnel in the field of oncology.
Alternatives such as remote session monitoring have been shown to be a good alternative to traditional brochures [20] to reach a larger population. Participation in face-to-face group exercise programs has shown very satisfactory results in the quality of life of cancer patients [21]. Recently, new modalities such as home-based exercise or booklets have been incorporated [22].
Since there are no studies comparing the three modalities of exercise prescription - in-person group, home-based exercise, and pamphlet prescription - this study aims to determine the effectiveness of three modalities of exercise prescription (in-person, home-based exercise, pamphlet prescription) on the quality of life of breast cancer patients actively undergoing treatment.
2. Materials and Methods
Design: Quasi-experimental study with randomized assignment to three groups (in-person: 24-week guided and supervised in-person exercise program; home-based exercise: 24-week guided and supervised exercise program with streaming monitoring; recommendation: exercise recommendation guided by informational booklet, with baseline and 6-month analyses from the start of the study. The study period was October 2021 to July 2023.
Population and setting: Women diagnosed with breast cancer (stage I-IV) actively undergoing treatment (chemotherapy, radiotherapy, hormone therapy). Exercise prescription should not be contraindicated by the oncologist, and participants must agree to participate in the study. Group assignment was based on group capacity (35 people per group) according to the group sequence: face-to-face - home-based exercise - referral. The estimated sample size was based on a 95% confidence level, a 5% margin of error, and a population of 105, resulting in a sample size of 80 patients. Recruitment was carried out at the Medical Oncology Service of the Provincial Hospital Consortium of Castellón. The study was conducted according to the Declaration of Helsinki, approved by the Human Research Ethics Committee of the Castellón Provincial Hospital Consortium (Protocol dated January 29, 2020). Written informed consent was obtained from all participants prior to the study. The study, which currently lacks an identification code, has been registered on ClinicalTrials.gov. This code will be provided during the article review process.
Intervention: The intervention for each group consisted of a 24-week personal training program guided and supervised by a graduate in physical activity and sports, specialized in exercise and oncology. The sessions consisted of a 10-minute warm-up with joint mobility and balance exercises. This was followed by a 40-minute main exercise session to improve upper and lower body strength and cardiorespiratory fitness, focusing on all major muscle groups and using body weight, resistance bands and/or free weights, exercise mats, and materials available at home (plastic bottles, shopping bags, etc.). This portion included a combined circuit of 8-12 functional exercises (e.g., squats, front and side lunges, sit-ups, calf raises, glute bridges, core, biceps curls, shoulder presses, punches, jumping jacks, static walking/jogging). The circuit consisted of 2 sets of 10-12 repetitions for the functional strength exercises and 30 seconds for the aerobic exercises. Volume was progressively increased by modifying the number of repetitions and sets and the complexity of the exercises. A minimum rest period of 90 seconds was established between exercises. For home-based exercise, the synchronously supervised home-based group participated in a home-based exercise program streamed and supervised by their oncology team for 6 months. Participants were asked to complete a 60-minute combined resistance and aerobic exercise session two days per week for 6 months (24 weeks). The sessions were controlled, guided, and supervised by a cancer exercise specialist who encouraged and provided feedback to the participants while they could observe the performance, interact, or ask questions.
In the home-based exercise, Google Meet was used for the connection, using the teacher's and patient's cameras and microphones. The exercise program was guided and supervised via live streaming, with the same training plan as in the face-to-face group. Exercise prescription through weekly recommendations (informative booklet with types of exercises and descriptions of how to perform them) for the recommendation group. Attendance was monitored for the face-to-face and home-based exercise, with a minimum attendance of 70% of sessions.
Variables: Baseline (before group assignment) and 6-month analysis were performed on sociodemographic variables: age (years), marital status (married or in a relationship, separated or divorced, single, widowed), motherhood (yes or no), cohabitation (living alone or not), education level (primary, secondary, university), employment status (employed, unemployed, retired) and income (<1000 Euro, 1000 to 2000 Euro, >2000 Euro), clinical variables: tumor type (luminal A, luminal B (HER2+), luminal B (HER2), non-luminal, triple negative), treatment plan (adjuvant, neoadjuvant), laterality (right breast, left breast, bilateral), tumor stage (I, II, III, IV), chemotherapy (yes or no), radiotherapy (yes or no), hormone therapy (yes or no), and quality of life measured by the QLQ-C30 questionnaire (30 items): covering five cancer dimensions: physical functioning (items 1-5), daily activities (items 6 and 7), social (items 26 and 27), emotional (items 21-24), and cognitive (items 20 and 25). Three symptom scales: fatigue (items 10, 12 and 18), pain (items 9 and 19), nausea and vomiting (items 14-15). A global health scale (items 29-30) and individual items measuring disease and treatment symptoms: Shortness of breath (item 8), insomnia (item 11), loss of appetite (item 13), constipation (item 16), diarrhea (item 17), and financial impact (item 28). Likert-type response format, referring to a one-week period.
Statistical Analysis:
Statistical analysis was performed using IBM SPSS Statistics version 28 (IBM Corporation). The normal distribution of variables was verified by the Kolgomorov-Smirnov test (p < 0.05) . As the variables were not normally distributed, non-parametric statistical tests were applied. To describe the collected data, we used the mean and standard deviation for continuous variables, and frequency for categorical variables. The bivariate analyzes (pre-post) of repeated measures were performed using the Wilcoxon test.
Multiple regression analysis was performed using the forward stepwise method. Only normally distributed variables were used as dependent variables. The parsimony principle was applied to the models obtained [23]. Given the limited simple size and the non-normal distribution of the independent variables, the residual errors of the resulting models were checked to ensure their normal distribution and thus the reliability of our regression models [24]. To determine the predictive value of the model, the Cohen criterion was applied to one-way ANOVA models. This criterion indicates that R2 values below 0.10 do not represent a relevant explanatory value, while R2 values between 0.10 and 0.25 indicate a dependence of the explanation of the variance of the analyzed variable on the identified factors, and with R2 values above 0.25 we can affirm that the explanatory model is very clinically relevant. Statistical significance is assumed at p-value <0.05.
To calculate the reliability of the data obtained, we calculated Chronbach's alpha in the total result of the Global Health Scale and in the dimensions (physical functioning, daily activities, emotional, cognitive).
3. Results
3.1. Sociodemographic description of the sample
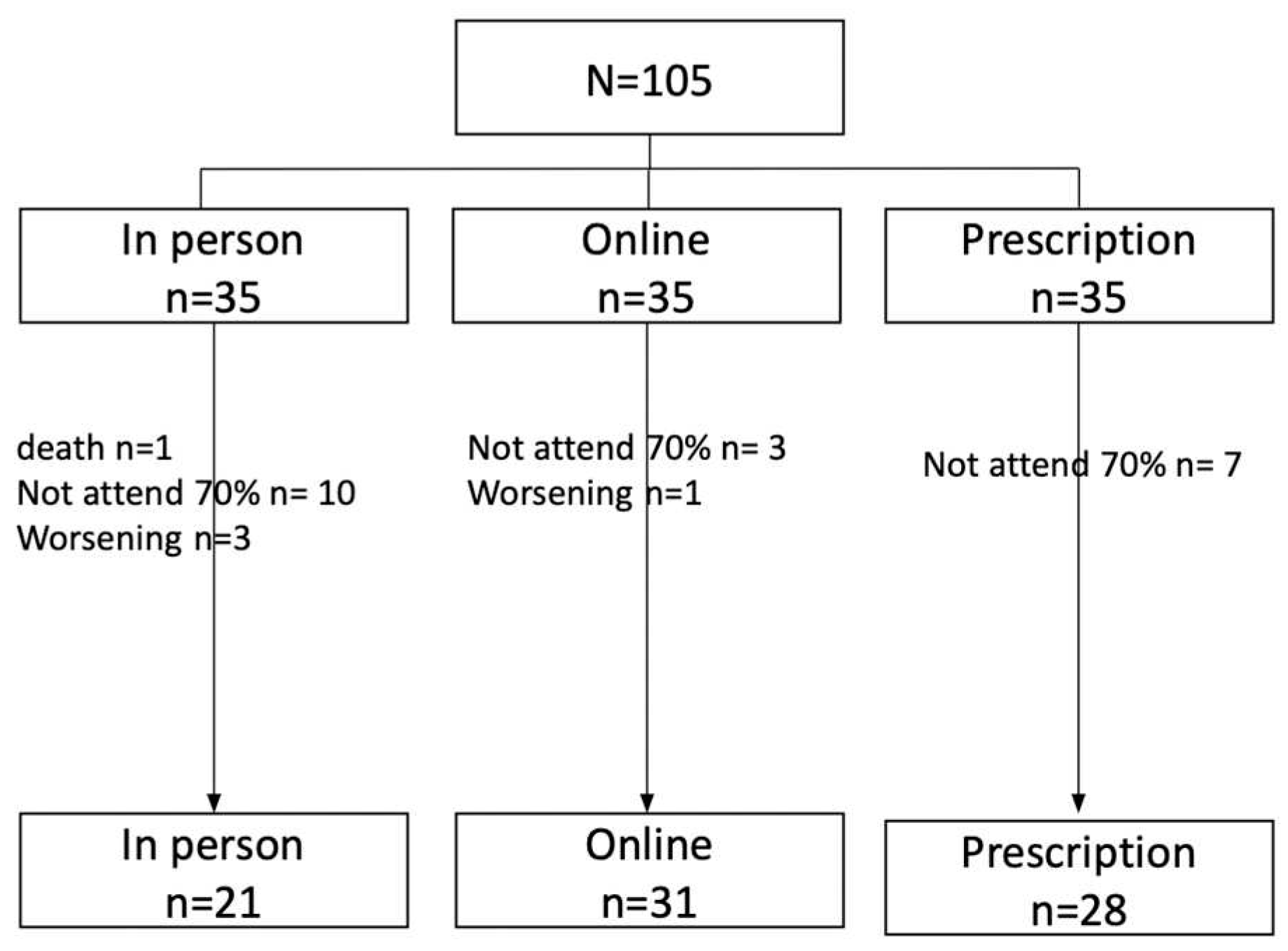
A total of N=105 patients meeting the inclusion criteria were recruited, with study completion in the face-to-face group (n=21; 26.3%), home-based exercise group (n=31; 38.8%), and recommendation group (n=28; 35%). The total sample analyzed was n=80. See flow chart for reasons for dropout by group.
Figure 1.
Flowchart of the process.
The mean age was 48.6 years, with married marital status (n=55; 68.8%), living with others (n=72; 90%), secondary education (n=35; 43.8%), employed (n=60; 75.5%), and income between 1000 and 2000 Euros (n=45; 56.3%), with no differences between groups according to allocation, see Table 1.
3.2. Description of the clinical status of the sample
The most common tumor according to pathological anatomy was ductal carcinoma (n=77; 96.6%), in the left breast (n=42; 53.8%), in stage II (n=43; 53.8%). The treatment plan was adjuvant in 55 cases (68.7%), 47 patients (60.2%) received chemotherapy during the study. The most commonly prescribed treatments were radiotherapy (n=68; 85%) and hormonal therapy (n=68; 85%). No differences were observed between groups according to allocation, see Table 2.
3.3. Quality of Life Results
As shown in Table 3, global quality of life improved significantly at 24 weeks in the face-to-face and home-based exercise groups, but not in the recommendation group.
By dimension, quality of life worsened significantly (p-value <0.05) in activities of daily living (baseline=43.40; 24 weeks=37.67), social dimension (baseline=50.30; 24 weeks=44.84), and emotional dimension (baseline=47.91; 24 weeks=43.84).
For symptoms, significant improvements (p-value <0.05) were observed for fatigue (baseline=51.31; 24 weeks=46.49), nausea and vomiting (baseline=33.10; 24 weeks=26.86), loss of appetite (baseline=35.94; 24 weeks=26.92), and constipation (baseline=45.63; 24 weeks=33.33). In the recommendation group, there was a significant improvement in constipation (baseline=40.48; 24 weeks=29.76), in the home exercise group, there were significant improvements in nausea and vomiting (baseline=37.68; 24 weeks=27.42), appetite loss (baseline=39.52; 24 weeks=26.92), and constipation (baseline=50.81; 24 weeks=36.54). The recommendation group did not show statistically significant differences in any of the symptoms.
3.4. Reliability of the QLQ-C30
Reliability, based on the calculation of global Cronbach's alpha and by dimension, ranged from 0.762 to 0.906. See Table 4.
3.5. Regression analysis results.
QOL at 24 weeks depended on active chemotherapy, tumor type, and assigned exercise group, accounting for 50.3% of the variance (r2 = 0.503; p < 0.001).
4. Discussion
The quality of life of breast cancer patients undergoing active treatment improves after a 24-week exercise program. These data support the importance of prescribing exercise during cancer treatment [1,2,3,8]. Physical activity is particularly effective in improving quality of life when delivered in person and virtually. These results are likely due to the development and supervision of these sessions by specialists in physical activity and cancer [18], which is consistent with the results of the Heiman study [1], which showed significant improvements in quality of life in patients who received guided and supervised exercise. Such supervision maximizes the benefits of exercise and helps women feel safe in their exercise routine [19].
In terms of dimensions, quality of life worsened significantly in the performance of activities of daily living, social dimension, and emotional dimension. No significant differences between the groups were observed in the analysis. Our results are not consistent with those of other researchers [21], who reported satisfactory results in improving QOL in all dimensions, both in home-based exercise prescription modalities [25] and in face-to-face sessions [5]. Our results may be more related to changes in family and social dynamics after diagnosis than to the benefits of exercise prescription. Most research has been conducted in breast cancer survivors who have completed their oncologic treatment and have experienced life changes after cancer [2,5,9,10,12,13,26].
Exercise in all modalities improved important aspects such as fatigue, nausea, vomiting, appetite, and constipation-symptoms that often lead to treatment discontinuation or delay. The face-to-face group, and especially home-based exercise, showed greater benefits in reducing nausea, vomiting, appetite loss, and constipation. These factors make home-based exercise, streaming-based programs a resource to consider in exercise recommendation. Therefore, it is an alternative to offer guided and supervised exercise programs to a larger population, as confirmed by other researchers [26,27].
The confidence level obtained from the QLQ-C30 scale is 0.898, data higher than those obtained in its original validation with a confidence level of 0.846 [28]. Although its validation was carried out in patients with breast cancer 6 and 12 months after the end of their treatments and based on the results of Aune's meta-analysis [7], they establish that this questionnaire is not adequate to reflect quality of life in the short term, since it presents a large variability of effect size when evaluated during treatment. Recommended questionnaires for assessing quality of life during treatment are the Functional Assessment of Therapy (FACT) questionnaire with its subscales of symptoms, physical well-being, and functional well-being, which have a Cronbach's alpha ranging from 0.55 to 0.76 [13]. Values lower than those reported in.
In conclusion, QoL is influenced by the type of treatment received during the trial, especially chemotherapy, which along with surgery [29] has the greatest impact on QoL-related symptoms, as well as tumor type. Luminal A breast cancer subtypes have a better prognosis after exercise [30]. Therefore, the explanatory model is associated with known quality of life variables in breast cancer patients.
5. Conclusions
The quality of life of breast cancer patients undergoing active treatment improves after a 24-week exercise program, especially in programs designed and supervised in-person and home-based exercise. Home-based exercise using the streaming-based modality is a good option for exercise prescription.
Author Contributions
Conceptualization: Suárez-Alcázar MP., García-Roca E and Folch Ayora A.; Methodology: Folch-Ayora A; Formal Analysis, Collado-Boira, E; Investigation: Recacha-Ponce P, Temprado-Albalat MD, Hernando-Domingo C, García-Roca E, Sala-Medina P; Baliño-Remiro P, Muriach-Sauri M, Flores-Buils R; Data Curation: Collado-Boira E; Writing – Original Draft Preparation: Suárez-Alcázar MP and Folch Ayora A; Writing – Review & Editing, Collado-Boira E; Project Administration: Suárez-Alcázar, MP.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the Declaration of Helsinki, approved by the Human Research Ethics Committee of the Castellón Provincial Hospital Consortium (Protocol dated January 29, 2020). The study, which currently lacks an identification code, has been registered on ClinicalTrials.gov. This code will be provided during the article review process.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
For ethical reasons related to the preservation of patient identity, the data presented in this study are available upon request to the corresponding author.
Acknowledgments
To all the women who have participated in the study, for their time, dedication, and motivation. To Chair of Physical Activity and Oncology (CAFO) and to all the team that has been part of this project.
Conflicts of Interest
The authors state that this research was carried out without commercial or financial relationships that could pose a conflict of interest. The results are shown truthfully and clearly, without any falsification or manipulation.
References
- Heiman J, Onerup A, Wessman C, Olofsson Bagge R. Recovery after breast cancer surgery following recommended pre and postoperative physical activity: (PhysSURG-B) randomized clinical trial. British Journal of Surgery [Internet]. 2021 Jan 27 [cited 2024 Jan 29];108(1):32–9. [CrossRef]
- Rastogi S, Tevaarwerk AJ, Sesto M, Van Remortel B, Date P, Gangnon R, et al. Effect of a technology-supported physical activity intervention on health-related quality of life, sleep, and processes of behavior change in cancer survivors: A randomized controlled trial. Psychooncology [Internet]. 2020 Nov 1 [cited 2023 Nov 22];29(11):1917–26. Available online: https://pubmed.ncbi.nlm.nih.gov/32808383/.
- Parkinson J, Bandera A, Crichton M, Shannon C, Woodward N, Hodgkinson A, et al. Poor Muscle Status, Dietary Protein Intake, Exercise Levels, Quality of Life and Physical Function in Women with Metastatic Breast Cancer at Chemotherapy Commencement and during Follow-Up. Curr Oncol [Internet]. 2023 Jan 1 [cited 2023 Nov 22];30(1):688–703. Available online: https://pubmed.ncbi.nlm.nih.gov/36661703/.
- Odikpo LC, Chiejina EN. Assessment of Practice and Outcome of Exercise on Quality of Life of Women with Breast Cancer in Delta State. Asian Pac J Cancer Prev [Internet]. 2021 Aug 1 [cited 2023 Nov 22];22(8):2377–83. Available online: https://pubmed.ncbi.nlm.nih.gov/34452549/.
- Aydin M, Kose E, Odabas I, Bingul BM, Demirci D, Aydin Z. The Effect of Exercise on Life Quality and Depression Levels of Breast Cancer Patients. Asian Pac J Cancer Prev [Internet]. 2021 [cited 2023 Nov 22];22(3):725–32. Available online: https://pubmed.ncbi.nlm.nih.gov/33773535/.
- García-Soidán JL, Pérez-Ribao I, Leirós-Rodríguez R, Soto-Rodríguez A. Long-Term Influence of the Practice of Physical Activity on the Self-Perceived Quality of Life of Women with Breast Cancer: A Randomized Controlled Trial. Int J Environ Res Public Health [Internet]. 2020 Jul 2 [cited 2023 Nov 22];17(14):1–12. Available online: https://pubmed.ncbi.nlm.nih.gov/32664375/.
- Aune D, Markozannes G, Abar L, Balducci K, Cariolou M, Nanu N, et al. Physical Activity and Health-Related Quality of Life in Women With Breast Cancer: A Meta-Analysis. JNCI Cancer Spectr [Internet]. 2022 Nov 1 [cited 2024 Jan 29];6(6). [CrossRef]
- Cormie P, Atkinson M, Bucci L, Cust A, Eakin E, Hayes S, et al. Clinical oncology society of australia position statement on exercise in cancer care. Medical Journal of Australia. 2018;209(4):184–7. [CrossRef]
- Lahart IM, Metsios GS, Nevill AM, Carmichael AR. Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database of Systematic Reviews. 2018 Jan 29;2018(1). [CrossRef]
- Campbell KL, Winters-Stone KM, Wiskemann J, May AM, Schwartz AL, Courneya KS, et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med Sci Sports Exerc [Internet]. 2019 Nov 1 [cited 2023 Nov 21];51(11):2375–90. Available online: https://pubmed.ncbi.nlm.nih.gov/31626055/.
- De Groef A, Geraerts I, Demeyer H, Van der Gucht E, Dams L, de Kinkelder C, et al. Physical activity levels after treatment for breast cancer: Two-year follow-up. Breast [Internet]. 2018 Aug 1 [cited 2023 Nov 21];40:23–8. Available online: https://pubmed.ncbi.nlm.nih.gov/29674221/.
- Sheppard VB, Dash C, Nomura S, Sutton AL, Franco RL, Lucas A, et al. Physical activity, health-related quality of life, and adjuvant endocrine therapy-related symptoms in women with hormone receptor-positive breast cancer. Cancer [Internet]. 2020 Sep 1 [cited 2023 Nov 22];126(17):4059–66. Available online: https://pubmed.ncbi.nlm.nih.gov/32614992/.
- Gavala-González J, Torres-Pérez A, Fernández-García JC. Impact of Rowing Training on Quality of Life and Physical Activity Levels in Female Breast Cancer Survivors. Int J Environ Res Public Health [Internet]. 2021 Jul 1 [cited 2023 Nov 22];18(13). Available online: https://pubmed.ncbi.nlm.nih.gov/34281126/.
- Sanft T, Harrigan M, Cartmel B, Ferrucci LM, Li FY, McGowan C, et al. Effect of healthy diet and exercise on chemotherapy completion rate in women with breast cancer: The Lifestyle, Exercise and Nutrition Early after Diagnosis (LEANer) study: Study protocol for a randomized clinical trial. Contemp Clin Trials [Internet]. 2021 Oct 1 [cited 2023 Nov 22];109. Available online: https://pubmed.ncbi.nlm.nih.gov/34274495/.
- Dieli-Conwright CM, Courneya KS, Demark-Wahnefried W, Sami N, Lee K, Sweeney FC, et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: a randomized controlled trial. Breast Cancer Res [Internet]. 2018 Oct 19 [cited 2024 Jan 29];20(1). Available online: https://pubmed.ncbi.nlm.nih.gov/30340503/.
- Inam F, Bergin RJ, Mizrahi D, Dunstan DW, Moore M, Maxwell-Davis N, et al. Diverse strategies are needed to support physical activity engagement in women who have had breast cancer. Support Care Cancer [Internet]. 2023 Dec 1 [cited 2023 Nov 21];31(12). Available online: https://pubmed.ncbi.nlm.nih.gov/37864656/.
- Murray J, Perry R, Pontifex E, Selva-Nayagam S, Bezak E, Bennett H. The impact of breast cancer on fears of exercise and exercise identity. Patient Educ Couns. 2022 Jul 1;105(7):2443–9. [CrossRef]
- Dennett AM, Peiris CL, Shields N, Morgan D, Taylor NF. Exercise therapy in oncology rehabilitation in Australia: A mixed-methods study. Asia Pac J Clin Oncol [Internet]. 2017 Oct 1 [cited 2023 Nov 21];13(5):e515–27. Available online: https://pubmed.ncbi.nlm.nih.gov/28004526/.
- Trinh L, Mutrie N, Campbell AM, Crawford JJ, Courneya KS. Effects of supervised exercise on motivational outcomes in breast cancer survivors at 5-year follow-up. Eur J Oncol Nurs [Internet]. 2014 Dec 1 [cited 2023 Nov 21];18(6):557–63. Available online: https://pubmed.ncbi.nlm.nih.gov/25181937/.
- Uhm KE, Yoo JS, Chung SH, Lee JD, Lee I, Kim J Il, et al. Effects of exercise intervention in breast cancer patients: is mobile health (mHealth) with pedometer more effective than conventional program using brochure? Breast Cancer Res Treat [Internet]. 2017 Feb 1 [cited 2023 Nov 21];161(3):443–52. Available online: https://pubmed.ncbi.nlm.nih.gov/27933450/.
- Rodríguez-Cañamero S, Cobo-Cuenca AI, Carmona-Torres JM, Pozuelo-Carrascosa DP, Santacruz-Salas E, Rabanales-Sotos JA, et al. Impact of physical exercise in advanced-stage cancer patients: Systematic review and meta-analysis. Cancer Med [Internet]. 2022 Oct 1 [cited 2023 Nov 21];11(19):3714–27. Available online: https://pubmed.ncbi.nlm.nih.gov/35411694/.
- Sotirova MB, McCaughan EM, Ramsey L, Flannagan C, Kerr DP, O’Connor SR, et al. Acceptability of online exercise-based interventions after breast cancer surgery: systematic review and narrative synthesis. J Cancer Surviv [Internet]. 2021 Apr 1 [cited 2023 Nov 21];15(2):281–310. Available online: https://pubmed.ncbi.nlm.nih.gov/32930924/.
- Stoica P, Söderström T. On the parsimony principle. Int J Control [Internet]. 1982 [cited 2024 Jan 29];36(3):409–18. Available online: https://www.tandfonline.com/doi/abs/10.1080/00207178208932904.
- Williams MN, Grajales CAG, Kurkiewicz D. Assumptions of Multiple Regression: Correcting Two Misconceptions. Practical Assessment, Research, and Evaluation [Internet]. 2019 Nov 25 [cited 2024 Jan 29];18(1):11. Available online: https://openpublishing.library.umass.edu/pare/article/id/1435/.
- Garcia-Roca ME, Rodriguez-Arrastia M, Ropero-Padilla C, Hernando Domingo C, Folch-Ayora A, Temprado-Albalat MD, et al. Breast Cancer Patients’ Experiences with Online Group-Based Physical Exercise in a COVID-19 Context: A Focus Group Study. J Pers Med [Internet]. 2022 Mar 1 [cited 2024 Jan 29];12(3):356. [CrossRef]
- Weiner LS, Nagel S, Su · H Irene, Hurst S, Levy SS, Arredondo EM, et al. A remotely delivered, peer-led intervention to improve physical activity and quality of life in younger breast cancer survivors. J Behav Med [Internet]. 2023 [cited 2023 Nov 30];46:578–93. [CrossRef]
- Cuthbert C, Twomey R, Bansal M, Rana B, Dhruva T, Livingston V, et al. The role of exercise for pain management in adults living with and beyond cancer: a systematic review and meta-analysis. Supportive Care in Cancer 2023 31:5 [Internet]. 2023 Apr 11 [cited 2024 Jan 29];31(5):1–25. Available online: https://link.springer.com/article/10.1007/s00520-023-07716-4.
- Zawisza K, Tobiasz-Adamczyk B, Nowak W, Kulig J, Jędrys J. Validity and reliability of the quality of life questionnaire (EORTC QLQ C30) and its breast cancer module (EORTC QLQ BR23). Ginekol Pol [Internet]. 2010 [cited 2024 Jan 30];81(4):262–7. Available online: https://journals.viamedica.pl/ginekologia_polska/article/view/46482.
- Kshirsagar A, Wani S. Health-related quality of life in patients with breast cancer surgery and undergoing chemotherapy in Ahmednagar district. J Cancer Res Ther [Internet]. 2021 Oct 1 [cited 2024 Jan 29];17(6):1335–8. Available online: https://europepmc.org/article/med/34916362.
- Ellingjord-Dale M, Vos L, Hjerkind KV, Hjartåker A, Russnes HG, Tretli S, et al. Alcohol, physical activity, smoking, and breast cancer subtypes in a large, nested case–control study from the Norwegian Breast Cancer Screening Program. Cancer Epidemiology Biomarkers and Prevention. 2017 Dec 1;26(12):1736–44. [CrossRef]

Table 1.
Sociodemographic description of the sample.
| In person n (%) |
Online n (%) |
Prescription n (%) |
Total n (%) |
|
|---|---|---|---|---|
| Age (mean±sd) | 46.1±8.7 | 49.0±8.9 | 50.1±7.9 | 48.6±8.6 |
| Marital Status | ||||
| Married or in a relationship | 14 (66.7) | 24 (77.4) | 17 (60.7) | 55 (68.8) |
| Separated or divorced | 2 (9.2) | 4 (12.9) | 5 (17.9) | 11 (13.8) |
| Single | 3 (14.3) | 2 (6.5) | 6 (21.4) | 11 (13.8) |
| Widowed | 2 (9.5) | 1 (3.2) | 0 (0.0) | 3 (3.8) |
| Motherhood (yes) | 15 (71.4) | 25 (80.6) | 22 (78.6) | 62 (78.5) |
| Cohabitation | ||||
| No live alone | 18 (85.7) | 30 (96.8) | 24 (85.7) | 72 (90) |
| Live alone | 3 (14.3) | 1 (3.2) | 4 (14.3) | 8 (10) |
| Education Level | ||||
| Primary | 3 (14.4) | 6 (19.4) | 5 (17.9) | 14 (17.6) |
| Secondary | 9 (42.8) | 12 (38.7) | 14 (50.0) | 35 (43.8) |
| University | 9 (42.8) | 13 (41.9) | 9 (32.1) | 31 (38.8) |
| Employment Status | ||||
| Employed | 18 (85.7) | 23 (74.2) | 19 (67.9) | 60 (75.5) |
| Unemployed | 2 (9.5) | 5 (16.1) | 8 (28.6) | 15 (18.8) |
| Retired | 1 (4.8) | 3 (9.7) | 1 (3.6) | 5 (6.3) |
| Income | ||||
| <1000 euros | 5 (23.8) | 13 (41.9) | 8 (28.6) | 26 (32.5) |
| 1000 - 2000 euros | 12 (57.1) | 15 (48.4) | 18 (64.3) | 45 (56.3) |
| >2000 euros | 4 (19.0) | 3 (9.7) | 2 (7.1) | 9 (11.3) |
Table 2.
Description of the clinical status of the sample.
| In person n (%) |
Online n (%) |
Prescription n (%) |
Total N (%) |
|
|---|---|---|---|---|
| Tumor Type | ||||
| Luminal A | 7 (33.3) | 12 (38.7) | 10 (35.7) | 29 (36.3) |
| Luminal B (her2 +) | 3 (14.3) | 4 (12.9) | 5 (17.8) | 12 (15.0) |
| Luminal B (her2 -) | 9 (42.8) | 11 (35.4) | 10 (35.7) | 30 (37.5) |
| Non luminal | 1 (4.8) | 2 (6.5) | 2 (7.2) | 5 (6.2) |
| Triple negative | 1 (4.8) | 2 (6.5) | 1 (3.6) | 4 (5.0) |
| Treatment plan | ||||
| Adjuvant | 15 (71.4) | 21 (67.7) | 19 (67.9) | 55 (68.7) |
| Neoadjuvant | 6 (28.6) | 10 (32.3) | 7 (25.0) | 23 (28.8) |
| Surgery only | - | - | 2 (7.1) | 2 (2.5) |
| Laterality | ||||
| Right breast | 10 (47.6) | 10 (32.3) | 10 (35.7) | 30 (37.5) |
| Left breast | 9 (42.9) | 17 (54.8) | 17 (60.79 | 43 (53.8) |
| Bilateral | 2 (9.5) | 4 (12.9) | 1 (3.6) | 7 (8.7) |
| Tumor stage | ||||
| I | 5 (23.8) | 9 (29.0) | 13 (46.4) | 27 (33.8) |
| II | 11 (52.4) | 20 (64.5) | 12 (42.9) | 43 (53.8) |
| III | 3 (14.3) | 1 (3.2) | 1 (3.6) | 5 (6.2) |
| IV | 2 (9.5) | 1 (3.2) | 2 (7.1) | 5 (6.2) |
| Treatment during the study | ||||
| Chemotherapy | 14 (66.7) | 16 (51.6) | 17 (60.7) | 47 (58.8) |
| Radiotherapy | 2 (9.5) | 4 (13.0) | 2 (7.1) | 8 (10.0) |
| Hormonotherapy | 5 (23.8) | 11 (35.5) | 9 (32.2) | 25 (31.2) |
| Prescribed treatment | ||||
| Chemotherapy | 18 (85.7) | 20 (64.5) | 18 (64.3) | 56 (70.9) |
| Radiotherapy | 16 (76.2) | 25 (80.6) | 27 (96.4) | 68 (85.0) |
| Hormonotherapy | 18 (85.7) | 25 (80.6) | 25 (89.3) | 68 (85.0) |
Table 3.
Quality of life results.
| Groups | Basal | 24 weeks | P Value/ d Cohen | |
|---|---|---|---|---|
| Global Health | ||||
| Total | 70.63 (±16.96) | 77.25(±14.29)* | <0.001/0.53 | |
| In person | 75.14 ( ±13.26) | 81.71(±13.67)* | 0.02/ 0.55 | |
| Online | 69.35( ±16.40) | 77.27(±13.83)* | 0.005 / 0.60 | |
| Prescription | 68.64 ( ±19.77) | 72.95(±14.72) | ||
| Dimensions | ||||
| Physical Functioning | Total | 34.01 ( ±10.44) | 34.20 ( ±11.93) | |
| In person | 30.24 ( ±6.01) | 30.48( ±4.71) | ||
| Online | 36.77 ( ±12.01) | 33.08 ( ±10.87) | ||
| Prescription | 39.09 ( ±10.59) | 33.75 ( ±16.08) | ||
| Daily Activities | Total | 43.40 ( ±19.92) | 37.67 ( ±16.28)* | |
| In person | 35.76 ( ±14.41) | 33.19 ( ±12.78) | <0.001/0.37 | |
| Online | 47.32 ( ±19.87) | 37.54 ( ±15.81) | 0.014/ 0.47 | |
| Prescription | 44.79 ( ±22.43) | 42.09 ( ±19.10) | ||
| Social | Total | 50.30 ( ±21.93) | 44.84 ( ±22.94)* | 0.018/0.35 |
| In person | 50.76 ( ±22.85) | 45.95 ( ±19.87) | ||
| Online | 53.74 ( ±22.41) | 47.69 ( ±23.98) | ||
| Prescription | 46.14 ( ±20.75) | 40.41 ( ±24.72) | ||
| Emotional | Total | 47.91 ( ±17.95) | 43.84 ( ±18.26)* | 0.014/0.26 |
| In person | 53.43 ( ±16.54) | 51.90 ( ±19.33) | ||
| Online | 49.29 ( ±21.97) | 39.73 ( ±15.41)* | 0.019/0.53 | |
| Prescription | 42.25 ( ±13.68) | 41.01 ( ±18.62) | ||
| cognitive | Total | 43.28 ( ±17.60) | 43.09 ( ±18.67) | |
| In person | 41.76 ( ±15.43) | 41.06 ( ±16.54) | ||
| Online | 44.13 ( ±15.82) | 42.04 ( ±17.33) | ||
| Prescription | 45.59 ( ±22.37) | 43.89 ( ±21.15) | ||
| Symptoms | ||||
| Fatigue | Total | 51.31 ( ±18.56) | 46.49 ( ±14.61)* | 0.007/0.31 |
| In person | 47.14 ( ±14.27) | 45.19 ( ±9.34) | ||
| Online | 54.74 ( ±20.22) | 45.54 ( ±14.07) | ||
| Prescription | 50.64 ( ±19.37) | 48.86 ( ±19.07) | ||
| Pain | Total | 46.69 ( ±19.20) | 46.75 ( ±16.72) | |
| In person | 41.24 ( ±13.86) | 43.67 ( ±14.62) | ||
| Online | 52.52 ( ±22.44) | 47.35 ( ±13.81) | ||
| Prescription | 44.32 (±17.56) | 49.01 ( ±31.42) | ||
| Nausea and Vomiting | Total | 33.10 (±12.74) | 26.86 (±6.27)* | <0.001/0.52 |
| In person | 30.43 (±9.39) | 26.24 (±3.91) | ||
| Online | 37.68 (±15.25) | 27.42 (±8.75)* | 0.009/0.71 | |
| Prescription | 30.04 (±10.58) | 26.77 (±4.56) | ||
| Shortness of breath | Total | 30.94 (±12.73) | 31.01 (±13.27) | |
| In person | 29.76 (±10.06) | 29.29 (±10.52) | ||
| Online | 33.06 (±16.31) | 28.85 (±9.19) | ||
| Prescription | 29.46 (±9.75) | 35.23 (±18.35) | ||
| insomnia | Total | 53.75 (±25.50) | 56.88 (±24.96) | |
| In person | 59.52 (±27.92) | 63.10 (±23.21) | ||
| Online | 54.84 (±26.94) | 53.85 (±24.18) | ||
| Prescription | 48.21 (±21.44) | 54.55 (±27.43) | ||
| Loss of appetite | Total | 35.94 (±18.16) | 28.99 (±11.03)* | 0.005/0.32 |
| In person | 33.33 (±12.07) | 29.76 (±10.06) | ||
| Online | 39.52 (±21.18) | 26.92 (±6.79)* | 0.013/0.55 | |
| Prescription | 33.93 (±18.27) | 30.68 (±15.29) | ||
| Constipation | Total | 45.63 (±26.91) | 33.33 (±16.42)* | <0.001/0.47 |
| In person | 40.48 (±24.33) | 29.76 (±12.79) * | 0.002/0.45 | |
| Online | 50.81 (±29.21) | 36.54 (±20.28)* | 0.002/0.56 | |
| Prescription | 43.75 (±26.02) | 32.95 (±14.19) | ||
| Diarrhea | Total | 31.25 (±15.15) | 28.62 (±9.85) | |
| In person | 30.95 (±13.47) | 28.57 (±8.96) | ||
| Online | 29.03 (±9.35) | 29.81 (±12.28) | ||
| Prescription | 33.93 (±20.65) | 27.27 (±7.35) | ||
| Financial impact | Total | 40.31 (±24.03) | 41.30 (±24.94) | |
| In person | 34.52 (±18.50) | 42.86 (±27.54) | ||
| Online | 46.77 (±27.94) | 44.23 (±25.79) | ||
| Prescription | 37.50 (±22.04) | 36.36 (±21.44) |
Table 4.
Reliability Scale.
| Alfa de Cronbach | |
|---|---|
| Global Health | 0.898 |
| Physical Functioning | 0.762 |
| Daily Activities | 0.829 |
| Social | 0.906 |
| Emotional | 0.886 |
| Cognitive | 0.877 |
Table 5.
Explanatory model of variance (regression).
| Model | R2 Adjusted | Standard Error |
F (p) |
|---|---|---|---|
|
Dependent Variable: Global Health Scale at 24 weeks into the program Covariates: Tumor type. Chemotherapy and Type of physical exercise program |
0.503 | 9.710 | 14.515(<0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



