
Submitted:
02 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Background: This study explores the impact of a gluten-free diet (GFD) on regional gastrointestinal (GI) transit times in individuals with celiac disease (CD) and non-celiac gluten sensitivity (NGCS). While a GFD is established for managing CD and wheat allergy, its effects on NGCS remain controversial due to inconclusive evidence. Methods: Utilizing a wireless motility and pH capsule (WMC) to assess regional and whole gut transit, newly diagnosed CD (n=12) and NGCS (n=12) patients underwent baseline evaluations, including measurements of gastric, small bowel, and colonic transit times. Results: At baseline conditions, individuals diagnosed with CD exhibited prolonged colonic and intestinal transit times when compared to those with NGCS (p<0.05). Following a 4-week GFD, CD patients experienced significant reductions in both intestinal and colonic transit times, along with enhanced small intestine contractility. NGCS individuals showed improvements in intestinal transit time and contractility with a GFD, although the colon exhibited no discernible effect. The GFD did not significantly impact intragastric, intestinal, or colonic pH. Conclusions: This study, employing WMC for the first time, provides novel insights into the positive effects of a GFD on intestinal and colonic transit, as well as contractility, in CD patients, and to a lesser extent, in those with NGCS.
Keywords:
celiac disease
; gluten
; diet
; non-celiac sensitivity
; wheat
1. Introduction
Celiac disease (CD) is an immune-mediated enteropathy that arises in genetically susceptible people after ingestion of dietary gluten per the Oslo definitions [1]. CD is a common disease recognized in multiple ethnicities and encountered across the globe, with a global estimated prevalence around 1% [2,3,4]. Conversely, non-gluten celiac sensitivity (NGCS) is a term encompassing the symptomatic and immunological manifestations precipitated by gluten- containing food ingestion in those where CD has been previously excluded [1]. In contrast to CD, people with NCGS lack elevations in celiac-specific antibodies and enteropathy [2,5,6]. Although an exact mechanism is yet to be elucidated, it is hypothesized that the innate but not adaptive immune response may play a part in NCGS [7,8]. Both CD and NGCS patients commonly experience gastrointestinal symptoms, ranging from abdominal discomfort to irregular bowel habits, necessitating a meticulous examination of the factors influencing, such as motility abnormalities. Dysmotility in the gastrointestinal (GI) tract has been described in patients with CD and may be linked to the generation of symptoms [9,10,11,12]. Some of the mechanisms associated with dysmotility in gluten-related disorders include impaired food absorption, low-grade inflammation in the small intestine, dysfunction of the autonomic nervous system, hormonal imbalances, and dysbiosis [13]. In fact, it has been described that a gluten-free diet (GFD) can reverse motor disturbances in patients with CD, but its effect on NGCS is unknown [11,13,14]. It is important to highlight that the few studies that have assessed motor alterations in the small intestine and colon in patients with CD have used tests such as small intestine manometry and oro-cecal transit [9,10,11,12,13,14].
Until the introduction of the wireless motility capsule (WMC) [SmartPill®, Given Imaging, Yoqneam, Israel], assessing the entire gut transit profile in a single test without radiation had proven challenging. The WMC represents a novel technique capable of measuring the whole gut transit time (WGTT) and regional transit times, including gastric emptying time (GET), small bowel transit time (SBTT), and colonic transit time (CTT) [16]. The capsule, measuring 26.8 mm in length and 11.7 mm in diameter, is equipped with three sensors for temperature (ranging between 25 and 49°C), pH (ranging between 0.05 and 9.0), and pressure (ranging between 0- and 350-mm Hg) [17]. As it traverses the gastrointestinal tract, the capsule continuously records various measurements, transmitting data wirelessly and in real-time to a receiver worn by the patient on their waist throughout the study. While numerous studies have explored the utility of WMC in identifying multiregional dysmotility in various conditions (such as diabetes [18], chronic constipation [19] and gastroparesis [20]), no current data is available regarding the GI tract transit profile among patients with celiac CD and other gluten-related disorders, such as NGCS.
While the implementation of a GFD has become a cornerstone in managing CD and NGCS, providing a therapeutic avenue to alleviate symptoms and prevent long-term complications, the specific influence of gluten withdrawal on WGTT warrants a more in-depth investigation. This study seeks to bridge this knowledge gap by employing the WMC, a non-invasive and patient-friendly technology, to monitor real-time transit dynamics in response to dietary modifications.
2. Materials and Methods
2.1. Patients
A prospective and observational study was conducted that consecutively recruited subjects that came to the gastroenterology department of our hospital for the evaluation of symptoms suggestive of CD or NCGS. Patients with a known CD or NCGS diagnosis that were already on a GFD were excluded. CD was diagnosed when, in the initial evaluation, patients tested positive for IgA tissue 2 transglutaminase antibodies (IgA-tTG2, Testline Clinical Diagnostics, Czech Republic) and/or IgG deaminated gliadin peptide antibodies (IgG-DGP, Testline Clinical Diagnostics), the presence of HLA-DQ2 and/or DQ8 haplotypes, and intestinal villous atrophy in duodenal biopsies according to the Marsh-Oberhüber classification [21]. The presence of NCGS was suspected when the subjects had negative serology tests and biopsies in the initial evaluation but complained of symptoms related to gluten ingestion. A gastroenterologist and a nutritionist evaluated those subjects, both of whom analyzed the gastrointestinal and/or extraintestinal symptoms (abdominal bloating, flatulence, bowel habit alterations, fatigue, headache, and muscle pain) and their relation to gluten intake utilizing the GSRS questionnaire [22]. The GSRS questionnaire has previously been used to evaluate the presence of digestive symptoms and extraintestinal manifestations in patients with NCGS, and its use is recommended in the Salerno consensus [5]. All the subjects were prescribed a GFD by a nutritionist and adherence to the diet was assessed through a food diary and weekly supervision for at least 6 weeks. NCGS diagnosis was made if the patients had a reduction > 30% in at least 3 of the symptoms evaluated in the GSRS for at least 50% of the time they were under observation (at least 3 of the 6 weekly evaluations). To confirm the NCGS diagnosis, all the subjects underwent a gluten challenge for 2 weeks (prescribed by the nutritionist, who recommended that the patient eat at least 8 g of gluten daily). Finally, NCGS was corroborated when the patients reported the reappearance of the previously evaluated symptoms. For the present analysis, the patients returned to a GFD after the gluten challenge phase of the study. Also, stool frequency was assessed using the Bristol stool form scale [23].
2.2. Baseline Evaluation
A baseline clinical evaluation and physical examination were performed on all the subjects. All the patients underwent the following assessments: body mass index (BMI) (kg/m2), and blood pressure (mm Hg), as well as the determination of glycemia (mg/dl), total cholesterol (mg/dl), HDL (mg/dl), and triglycerides (mg/dl).
Wireless Motility Capsule
All patients undergoing WMC testing at our institution follow a previously described standardized protocol [23]. Patients are instructed to refrain from using proton pump inhibitors 7 days prior to WMC ingestion, histamine-2-receptor antagonists 3 days prior and antacids 1 day prior to ingestion. They are also advised to stop using any prokinetic, antiemetic, anticholinergic, antidiarrheal agents, narcotic pain medications and non-steroidal anti-inflammatory drugs 3 days prior to testing. On the day of the procedure, after an overnight fast, the WMC is ingested directly after consumption of a standardized meal consisting of a nutrient bar: Smartbar® (Given Imaging, Yoqneam, Isreal) (266 kcal, 17% protein, 66% carbohydrate, 2% fat, and 3% fiber) and 50 cc of water. Patients then continue fasting for 6 hours after the ingestion of the capsule with small sips of water allowed. They are instructed to always wear a data receiver to their body (within five feet) for the duration of the study. The data receiver is a 6″ × 4″ × 1.5″ lightweight device that records data and contains a rechargeable battery. Patients are also asked to push the EVENT button and make an entry in a diary for certain events (e.g., food, bowel movements, sleep). They are asked not to consume alcohol, take any laxatives, antidiarrheal medications or start new medications (unless necessary) until the capsule is passed. After the end of the study, the receiver is returned, and data are downloaded for analysis. Data downloaded wase analyzed according to pH and temperature changes. GET is considered delayed if it is 5 hours or greater. It is defined as the duration the capsule takes from the time of ingestion until it reaches the duodenum (demarcated by an increase in pH by more than 3 units). SBTT, the time needed for capsule to travel from duodenum to cecum, is normal when it ranges between 2.5 and 6 hours and is determined by the sudden drop of pH by more than 1 unit and sustained for at least 30 minutes. CTT, the capsule transit duration from time of entry into cecum to exit from the body, is considered delayed if >59 hours and is determined by a sudden drop in temperature or loss of signal. WGTT is the sum of transit times through all three segments and is considered normal if <73 hours. Motility and contractility measures were calculated using 2 pieces of proprietary software (motiligi, version 3.0.20, and GIMS Data Viewer, version 3.0.0, Medtronic, Minneapolis, USA). MotiliGI—the contractility and motility measures provided by the software include mean peak amplitude of contractions, contractions per minute and the motility index (MI) in the small bowel [24]. Motility index is a composite parameter that incorporates both contraction frequency and amplitude and is calculated as ln (sum of amplitudes × number of contractions + 1) assessed on contractions >10 mm Hg, but <300 mm Hg [25]. It has previously been demonstrated as a useful summary measure, facilitating both a chronotropic and ionotropic assessments of GI motility, although its exact interpretation remains to be fully determined. Also, median pH along segments was calculated.
2.3. Intervention
All the subjects received recommendations for conducting a GFD prescribed by a nutritionist (described above) at the baseline. They were then given appointments every week for 4 weeks (one month). Adherence to the diet was evaluated through a questionnaire that took into consideration the foods consumed by the patient the week prior to the visit.
2.4. Final Evaluation
At the end of the 4 weeks, GSRS questionnaires and BSFS were applied. WMC was repeated to compare motility parameters before and after the intervention.
2.5. Statistical Analysis
Descriptive data are presented as the mean (SD) for normally distributed continuous variables, median (range) for non-normally distributed continuous variables, and number (%) for categorical variables. Chi-square test, Mann-Whitney U test, and the Wilcoxon signed rank test were used for the group comparisons, when indicated. All the differences were considered statistically significant with a p < 0.05. The analysis was performed utilizing the SPSS, version 21.0 (SPSS Inc, Chicago IL, USA) software. Informed consent was obtained from all the participants and the study was approved by the institutional ethics committee. It was funded by a grant from the CONACYT (FOSIS 2015-262023).
3. Results
3.1. Demographic and Clinical Data
We assessed 12 individuals with CD (mean age 39 ± 12 years, 11 females, mean BMI 21.2 ± 1.9 kg/m2) and 12 with NGCS (mean age 31 ± 5 years, 10 females, mean BMI 23.8 ± 2.1 kg/m2). The most common symptoms in patients with CD were bloating (12/12), abdominal pain (10/12), frequent bowel movements (8/12), nausea (6/12), borborygmi (5/12), diarrhea (4/12) and constipation (2/12). On the other hand, in patients with non-gluten celiac sensitivity, the most frequent symptoms were abdominal pain (12/12), bloating (8/12), headache (7/12), muscle pains (6/12), fogginess (4/12), and constipation (3/12).
Among the CD patients, 92% reported over 50% improvement in abdominal pain/distension at the onset of the GFD, while symptomatic improvement occurred in 67% of NGCS patients. In CD patients, there was a significant change in the Bristol Stool Form Scale (BSFS) at the conclusion of the GFD (median basal BSFS 5 versus median final BSFS 3, p=0.02). Conversely, NGCS patients showed no difference in the consistency of bowel movements based on the BSFS before and after GFD (baseline median 3 versus final median 3, p=0.99).
3.2. Motility Parameters
Table 1 displays variations in gastrointestinal transit times, both overall and regionally, between individuals with CD and those with non-celiac gluten sensitivity NGCS at the beginning and following four weeks of a GFD.Final del formulario
Under baseline conditions, individuals diagnosed with CD exhibited prolonged colonic and intestinal transit times when compared to those with NGCS (p<0.05, Table 1). Following a 4-week GFD diet in CD patients, there was a notable reduction in both intestinal and colonic transit times (Table 1, Figure 1). Additionally, GFD augmented small intestine contractility, as evidenced by increased numbers of contractions, greater amplitude, elevated pressure, and a heightened MI (Table 1). At the colonic level, GFD led to an increment in both the number of contractions and pressure (Table 1).
In individuals with NGCS, the GFD improved both intestinal transit time and contractility, but it had no discernible effect on the colon, as observed in Table 1. The gluten-free diet did not exhibit any statistically significant impact on intragastric, intestinal, or colonic pH.

Table 1.
Comparison of gastrointestinal motility parameters before and after 4 weeks of a gluten free diet (GFD) in celiac disease and non-gluten celiac sensitivity patients.
Table 1.
Comparison of gastrointestinal motility parameters before and after 4 weeks of a gluten free diet (GFD) in celiac disease and non-gluten celiac sensitivity patients.
| Motility parameters | Celiac disease (n=12) | Non gluten celiac sensitivity (n=12) | ||
| Before | After 4 weeks of GFD | Before | After 4 weeks of GFD | |
| Transit time (minutes) | ||||
|
156 ± 38 | 216 ± 48 | 183.6 ± 60 | 186 ± 54 |
| 252 ± 39 | 196±27 * | 264 ± 41 | 181±18 * | |
| 2150±1020 & | 1450±348 * | 1278 ± 452 | 1139 ± 365 | |
| 2394±960 & | 2104 ± 660 | 1672 ± 429 | 1577 ± 412 | |
| Small bowel motility parameters | ||||
|
109 ± 23 | 198±17 * | 116 ± 28 | 162±28 * |
|
2.4 ± 0.8 | 3.3±0.4 * | 2.8± 0.6 | 3.0 ± 0.7 |
|
1.68 ± 1.4 | 3.74±1.3 * | 3.63± 0.9 | 5.2±2.3 * |
|
136 ± 32 | 206±24 * | 160.5 ± 50 | 222±41 * |
| Colon motility parameters | ||||
|
98 ± 19 | 173±41 * | 107 ± 32 | 132 ± 47 |
|
3.1 ± 1.8 | 4.1 ± 1.9 | 4.2 ± 1.9 | 4.7 ±1.3 |
|
1.9 ± 0.7 | 3.1±0.8 * | 2.1 ± 0.8 | 2.7 ± 0.9 |
|
154 ± 61 | 208 ± 32 * | 197 ± 52 | 224 ± 68 |
| pH median | ||||
|
2.1 ± 0.5 | 1.9 ± 0.8 | 1.9 ± 0.3 | 1.8 ± 0.5 |
|
7.3 ± 0.6 | 6.9 ± 1.1 | 7.2 ± 0.8 | 7.1 ± 0.8 |
|
6.8 ± 0.8 | 6.7 ± 0.9 | 6.9 ±1.1 | 6.9 ± 0.7 |
a Motility index is a composite parameter that incorporates both contraction frequency and amplitude and is calculated as ln (sum of amplitudes × number of contractions + 1).& p<0.05 comparison between CD and NGCS. * p<0.05 comparison before and after gluten free diet. Continuous variables with normal-distribution, Welch Two Sample t-test; paired t- test. Continuous variable with non-normal-distribution, Wilcoxon rank sum test.
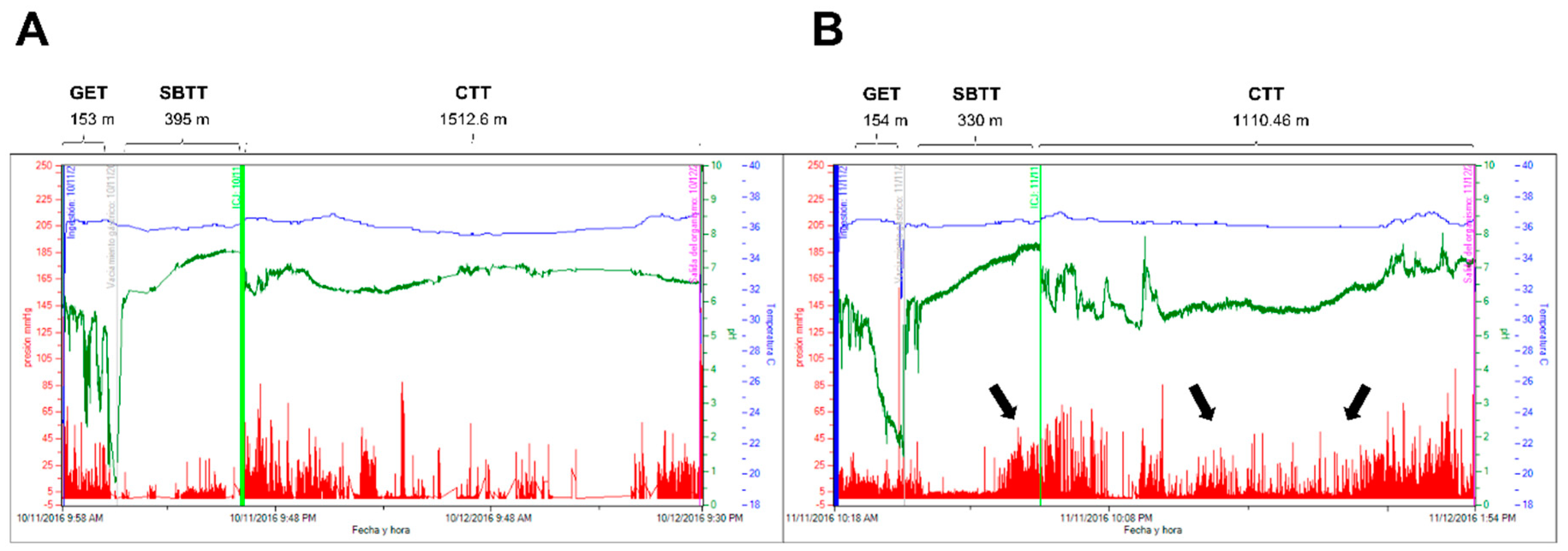
Figure 1.
Determination of landmarks and regional transit times on plot data obtained from a WMC recording in a celiac disease patient before (A) and after 4 weeks of a gluten free diet (B). Blue line: temperature; white line, pH: red line, pressure. The black arrows in panel B illustrate an evident increase in the motor activity of the small intestine (especially ileum) and colon after the gluten-free diet. GET: gastric emptying time; SBTT: small bowel transit time; CTT: colonic transit time.
Figure 1.
Determination of landmarks and regional transit times on plot data obtained from a WMC recording in a celiac disease patient before (A) and after 4 weeks of a gluten free diet (B). Blue line: temperature; white line, pH: red line, pressure. The black arrows in panel B illustrate an evident increase in the motor activity of the small intestine (especially ileum) and colon after the gluten-free diet. GET: gastric emptying time; SBTT: small bowel transit time; CTT: colonic transit time.
4. Discussion
In recent times, there has been heightened scrutiny of the management approaches for CD and NGCS particularly with a focus on dietary interventions. A pivotal area of investigation revolves around understanding the impact of a GFD on the gastrointestinal dynamics of individuals grappling with CD and NGCS. In this research we explored the intricate connection between gluten consumption and WGTT by utilizing the state-of-the-art WMC technology. The WMC provides an office-based, radiation free, standardized testing modality capable of simultaneously measuring gastric emptying time, small bowel transit time, and colon transit time. WMC has demonstrated comparable results with traditional radiolabeled and radiographic motility testing modalities [17]. WMC should be considered as an alternative for transit testing in suspected cases of gastroparesis, small bowel dysmotility, and colon transit testing, and considered the test of choice in suspected conditions of multiregional or generalized motility disorders [17,18,19,20].
Our findings are novel in several ways, as we employed precise definitions (Oslo criteria for celiac disease, Salerno criteria for non-gluten celiac sensitivity), innovative technology (WMC), and an ideal therapeutic intervention (gluten-free diet). Through this approach, we demonstrated that gluten induces colonic intestinal dysmotility, especially in patients with CD. Intestinal dysmotility occurs in a variety of disorders in which the gut has lost its ability to coordinate muscular activity because of endogenous or exogenous causes [9,13]. Such disorders may be primary or secondary and may manifest symptomatically in a variety of ways, including abdominal distention, recurrent obstruction, abdominal colicky pain, constipation, gastroesophageal reflux disease and recurrent vomiting. In a broad sense, any alteration in the transit of foods and secretions into the digestive tract may be considered an intestinal motility disorder.
Previous studies employing various methods such as mouth-to-cecum transit time, lactulose H2 breath test, antroduodenal manometry, ultrasound, colonic transit time with radiopaque markers, and 13C-occtanoid breath test have reported motor disturbances in the intestine and colon of patients with celiac disease [9,13]. However, these abnormalities have been not appropriately in NGCS.
In our study we found that compared to NGCS, CD exhibited prolonged colonic and intestinal transit times. These results are like those reported by Chiarioni [15] and Benini [14], where it is described that patients with celiac disease have a prolonged oro-cecal transit time when compared to a control group. On the other hand, in another study conducted by Bai and colleagues [26] using radiopaque markers, it was demonstrated that patients with CD have an accelerated colonic transit. The differences between studies may be explained using different methodologies and populations with more severe symptoms (e.g., patients with chronic diarrhea). In our patients with CD, the predominant symptoms were abdominal pain and distension, while only 4 out of 12 experienced diarrhea. Although, the classic presentation of CD is more common in young children, consisting primarily of gastrointestinal symptoms with malabsorption (chronic diarrhea, abdominal pain, distension, and failure to thrive or weight loss), some patients also present with constipation [27]. In adults, the presentation of CD is often more subtle and can be mistaken for irritable bowel syndrome, as in our cases [26,27,28].
Regarding the evidence of dysmotility in the small intestine, it has been reported that individuals with CD exhibit fasting motor abnormalities, including clustered contractions, giant jejunal contractions, and bursts of non-propagated contractions, observed in both adults and children with CD [9,10,11]. In a further study Bassotti et al. [12] validated that most of untreated celiac patients displayed distinct motor abnormalities in the upper gut during both fasting and fed periods. Although it is not precisely understood why gluten induces dysmotility, multiple mechanisms have been proposed, including: low-grad inflammation, diminished food absorption, dysfunction of the autonomic nervous system, hormonal imbalances, and dysbiosis [9,13].
What is clear, according to our results, is that a GFD has a positive effect on symptoms and reverses dysmotility in patients with CD, especially in the small intestine. Significantly, the frequency, amplitude, and pressure of the small intestine, measured by WMC, improved after the intestine was no longer exposed to gluten. Some previous studies have had examined the impact of a GFD on gastrointestinal motility. As in our study, there is evidence that dysmotility could be reversible with a GFD. For example, Cucciara et al [11] found that gut dysmotilities (reduction postprandial antral motility index and abnormal fasting and fed motor responses) disappeared in children with CD after GFD. In another study, through the use of the orocecal transit test with lactulose, it was demonstrated that after a GFD period, mouth-to-cecum transit time in patients was significantly reduced compared to prediet transit (134 +/- 8 vs 243 +/- 10 min, P = 0.0001) and did not show statistical difference when compared to that found in controls (P = 0.1) [15]. Benini et al. [29] showed that following mucosal recovery, the gastric emptying of a gluten-free meal improves, albeit it remains delayed in comparison to controls. Therefore, it is possible that the improvement in the motor function of the small intestine observed after a gluten-free diet is the result of inflammation resolution.
Non-celiac gluten sensitivity (NGCS) is a clinical entity characterized by the absence of CD and wheat allergy in patients that trigger reproducible symptomatic responses to gluten-containing foods consumption [31]. The absence of a clear definition, coupled with controversies in clinical trials, indicates a limited understanding of the etiopathogenesis and besides gluten other components such as fructans or protein alpha-amylase-trypsin inhibitors. In this population, our study demonstrates for first time that a GFD also has a positive effect on intestinal motility. There is only one previous study that shows that patients with NCGS, diagnosed by gluten-related symptoms and presence of IgG AGA, present with motility alterations that improve in most cases after a GFD [30]. Although an exact mechanism is yet to be elucidated, it is hypothesized that the innate but not adaptive immune response may play a part in NCGS [5,6,7,31]. Suggested factors encompass alterations in intestinal permeability, abnormal motility, and gut stimulation. In specific animal models, like mice expressing human leukocyte antigen (HLA)-DQ8 genes, gliadin has been proposed to induce hypercontractility of smooth muscle and dysfunction in cholinergic nerves, all without causing atrophy in the duodenal mucosa [32,33]. Studies involving mice indicate that wheat germ agglutinins provoke the release of IL-4 and IL-13, elevate inflammation, disrupt epithelial integrity, and enhance the synthesis of proinflammatory cytokines [34]. Therefore, just as it is described that inflammation and epithelial alterations are associated with intestinal motor dysfunctions in subjects with CD and that these are reversible, something similar may occur in patients with NGCS. Nevertheless, further investigations are required in this regard.
Although our study is innovative and the findings are thought-provoking, we must acknowledge some limitations. Firstly, it is a study with a small sample size, as conducting intervention studies with a GFD before and after is complex. Nevertheless, it is noteworthy that our patients exhibited good adherence to the treatment throughout the 4 weeks of the study. Another limitation is the absence of a healthy control group, as seen in other similar studies. However, we consider the most relevant statistical comparisons to be the intervention before and after, where each subject served as their own control. Lastly, the study assesses the effect of the GFD for only 4 weeks, and longer-term studies are needed, considering that histological recovery in patients with celiac disease can take 6 to 12 months.
5. Conclusions
In conclusion, this study demonstrates, for the first time using WMC, that a GFD improves intestinal and colonic transit, as well as contractility, in patients with CD. Similarly, albeit to a lesser extent, a gluten-free diet has a beneficial effect on the intestinal motility of patients with NGCS.
Author Contributions
Conceptualization, J.M.R.T; methodology, J.M.R.T and G.A.H.; software, G.A:H.; validation, J.M.R.T, O.C.Q and X.J.R.G; formal analysis, J.M.R.T and G.A.H.; investigation, O.C.Q, G.A.H, X.J.R.G and P.G.P; resources, J.M.R:T.; data curation, O.C.Q and G.A:H.; writing—original draft preparation, J.M.R.T and P-G.P.; writing—review and editing, J.M.R.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by CONACYT, Mexico, FOSIS 2015-262023.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Instituto de Investigaciones Médico Biológicas, Universidad Veracruzana, Veracruz, México. (Protocol code 2015/01/03) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions; a statement is still required.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ludvigsson J.F., Leffler D.A., Bai J.C., Biagi F., Fasano A., Green P.H., Hadjivassiliou M., Kaukinen K., Kelly C.P., Leonard J.N., Lundin K.E., Murray J.A., Sanders D.S., Walker M.M., Zingone F., Ciacci C. The Oslo definitions for coeliac disease and related terms. Gut 2013; 62(1):43-52. [CrossRef]
- Singh P., Arora A., Strand T.A., Leffler D.A., Catassi C., Green P.H., Kelly C.P., Ahuja V., Makharia G.K. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2018; 16:823-836. [CrossRef]
- Jansson-Knodell C.L., Rubio-Tapia A. Gluten-related disorders from bench to bedside. Clin Gastroenterol Hepatol. 2023: S1542-3565(23)00844-3. [CrossRef]
- Lindfors K., Ciacci C., Kurppa K., Lundin K.E.A., Makharia G.K., Mearin M.L., Murray J.A., Verdu E.F., Kaukinen K. Coeliac disease. Nat Rev Dis Primers. 2019 ;5(1):3. [CrossRef]
- Catassi C., Elli L., Bonaz B., Bouma G., Carroccio A., Castillejo G., Cellier C., Cristofori F., de Magistris L., Dolinsek J., Dieterich W., Francavilla R., Hadjivassiliou M., Holtmeier W., Körner U., Leffler D.A., Lundin K.E., Mazzarella G., Mulder C.J., Pellegrini N., Rostami K., Sanders D., Skodje G.I., Schuppan D., Ullrich R., Volta U., Williams M., Zevallos V.F., Zopf Y., Fasano A. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts' Criteria. Nutrients. 2015 18;7(6):4966-77. [CrossRef]
- Shiha M.G., Raju S.A., Penny H.A., Sanders D.S. Non-coeliac gluten sensitivity: from Salerno to Rome. Lancet Gastroenterol Hepatol. 2024;9(2):94-95. [CrossRef]
- Pinto-Sánchez M.I., Verdú E.F. Non-coeliac gluten sensitivity: are we closer to separating the wheat from the chaff? Gut 2016;65(12):1921-1922. [CrossRef]
- Junker Y., Zeissig S., Kim S.J, Barisani D., Wieser H., Leffler D.A., Zevallos V., Libermann T.A., Dillon S., Freitag T.L., Kelly C.P., Schuppan D. Wheat amylase trypsin inhibitors drive intestinal inflammation via activation of toll-like receptor 4. J Exp Med 2012; 209:2395–2408. [CrossRef]
- Usai-Satta P., Oppia F., Lai M., Cabras F. Motility Disorders in Celiac Disease and Non-Celiac Gluten Sensitivity: The Impact of a Gluten-Free Diet. Nutrients. 2018;10(11):1705. [CrossRef]
- Bassotti, G.; Castellucci, G.; Betti, C.; Fusaro, C.; Cavalletti, M.L.; Bertotto, A.; Spinozzi, F.; Morell, A.; Pello, M.A. Abnormal gastrointestinal motility in patients with celiac sprue. Dig. Dis. Sci. 1994, 39, 1947–1954. [Google Scholar] [CrossRef] [PubMed]
- Cucchiara, S.; Bassotti, G.; Castellucci, G.; Minella, R.; Betti, C.; Fusaro, C.; Morelli, A.; Bertotto, A.; Auricchio, S. Upper gastrointestinal motor abnormalities in children with active celiac disease. J. Pediatr. Gastroenterol. Nutr. 1995, 21, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Bassotti, G.; Villanacci, V.; Mazzocchi, A.; Mariano, M.; Incardona, P.; Clerici, C.; Morelli, A. Antroduodenojejunal motor activity in untreated and treated celiac disease patients. J. Gastroenterol. Hepatol. 2008, 23, e23–e28. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sanchez M.I., Bercik P., Verdu E.F. Motility alterations in celiac disease and non-celiac gluten sensitivity. Dig Dis. 2015;33(2):200-207. [CrossRef]
- Benini F., Mora A., Turini D., Bertolazzi S., Lanzarotto F., Ricci C., Villanacci V., Barbara G., Stanghellini V., Lanzini A. Slow gallbladder emptying reverts to normal but small intestinal transit of a physiological meal remains slow in celiac patients during gluten-free diet. Neurogastroenterol Motil. 2012;24(2):100-7, e79-80. [CrossRef]
- Chiarioni G., Bassotti G., Germani U., Battaglia E., Brentegani M.T., Morelli A., Vantini I. Gluten-free diet normalizes mouth-to-cecum transit of a caloric meal in adult patients with celiac disease. Dig Dis Sci. 1997 ;42(10):2100-5. [CrossRef]
- Saad R.J. The Wireless Motility Capsule: a One-Stop Shop for the Evaluation of GI Motility Disorders. Curr Gastroenterol Rep. 2016;18(3):14. [CrossRef]
- Arora Z., Parungao .JM., Lopez R., Heinlein C., Santisi J., Birgisson S. Clinical utility of wireless motility capsule in patients with suspected multiregional gastrointestinal dysmotility. Dig Dis Sci. 2015;60(5):1350-7. [CrossRef]
- Rouphael C., Arora Z., Thota P.N., Lopez R., Santisi J., Funk C., Cline M. Role of wireless motility capsule in the assessment and management of gastrointestinal dysmotility in patients with diabetes mellitus. Neurogastroenterol Motil. 2017 ;29(9). [CrossRef]
- Kuo B., Maneerattanaporn M., Lee A.A., Baker J.R., Wiener S.M., Chey W.D., Wilding G.E., Hasler W.L. Generalized transit delay on wireless motility capsule testing in patients with clinical suspicion of gastroparesis, small intestinal dysmotility, or slow transit constipation. Dig Dis Sci. 2011;56(10):2928-38. [CrossRef]
- Parkman H.P., Sharkey E., McCallum R.W., Hasler W.L., Koch K.L, Sarosiek I., Abell T.L., Kuo B., Shulman R.J., Grover M., Farrugia G., Schey R., Tonascia J., Hamilton F., Pasricha P.J; NIH/NIDDK Gastroparesis Consortium. Constipation in Patients With Symptoms of Gastroparesis: Analysis of Symptoms and Gastrointestinal Transit. Clin Gastroenterol Hepatol. 2022;20(3):546-558.e5. [CrossRef]
- Oberhuber G., Granditsch G., Vogelsang H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol, 1999;11: 1185-1194. [CrossRef]
- Kulich K. R, Madisch A., Pacini F, Piqué J.M., Regula J., Van Rensburg C.J., Ujszászy L., Carlsson J., Halling K., Wiklund I.K. Reliability and validity of the Gastrointestinal Symptom Rating Scale (GSRS) and Quality of Life in Reflux and Dyspepsia (QOLRAD) questionnaire in dyspepsia: a six-country study Health Qual Life Outcomes, 2008; 6:12. [CrossRef]
- Heaton K.W., Radvan J., Cripps H., Mountford R.A., Braddon F.E., Hughes A.O. Defecation frequency and timing, and stool form in the general population: a prospective study. Gut. 1992;33(6):818-24. [CrossRef]
- Rao S.S.C., Camilleri M., Hasler W.L., Maurer A.H., Parkman H.P., Saad R., Scott M.S., Simren M., Soffer E., Szarka L.Evaluation of gastrointestinal transit in clinical practice: position paper of the American and European Neurogastroenterology and Motility Societies. Neurogastroenterol Motil. 2011;23:8-23. Neurogastroenterol Motil. [CrossRef]
- Farmer A.D., Wegeberg A.L., Brock B., Hobson A.R., Mohammed S.D., Scott S.M., Bruckner-Holt C.E., Semler J.R., Hasler W.L., Hellström P.M., Drewes A.M., Brock C. Regional gastrointestinal contractility parameters using the wireless motility capsule: inter-observer reproducibility and influence of age, gender, and study country. Aliment Pharmacol Ther. 2018;47(3):391-400. [CrossRef]
- Bai, J.C.; Mauriño, E.; Martínez, C.; Vázquez, H.; Niveloni, S.; Soifer, G.; Flores, D.; Boerr, L.A. Abnormal colonic transit time in untreated celiac sprue. Acta Gastroenterol Latinoam. 1995, 25, 277–284. [Google Scholar] [PubMed]
- Kelly C.P., Bai J.C., Liu E., Leffler D.A. Advances in diagnosis and management of celiac disease. Gastroenterology. 2015;148(6):1175-86. [CrossRef]
- Sánchez-Vargas L.A., Thomas-Dupont P., Torres-Aguilera M., Azamar-Jacome A.A., Ramírez-Ceervanes K.L., Aedo-Garcés M.R., Meixueiro-Daza A., Roesch-Dietlen F., Grube-Pagola P., Vivanco-Cid H., Remes-Troche J.M. Prevalence of celiac disease and related antibodies in patients diagnosed with irritable bowel syndrome according to the Rome III criteria. A case-control study. Neurogastroenterol Motil. 2016;28(7):994-1000. [CrossRef]
- Benini, L.; Sembenini, C.; Salandini, L.; Dall’O, E.; Bonfante, F.; Vantini, I. Gastric emptying of realistic meals with and without gluten in patients with coeliac disease. Effect of jejunal mucosal recovery. Scand. J. Gastroenterol. 2001, 36, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sanchez M.I., Nardelli A., Borojevic R., De Palma G., Calo N.C., McCarville J., Caminero A., Basra D., Mordhorst A., Ignatova E., Hansen S., Uhde M., Norman G.L., Murray J.A., Smecuol E., Armstrong D., Bai J.C., Schuppan D., Collins S.M., Alaedini A., Moayyedi P., Verdu E.F., Bercik P. Gluten-Free Diet Reduces Symptoms, Particularly Diarrhea, in Patients With Irritable Bowel Syndrome and Antigliadin IgG. Clin Gastroenterol Hepatol. 2021;19(11):2343-2352.e8. [CrossRef]
- Barbaro M.R., Cremon C., Wrona D., Fuschi D., Marasco G., Stanghellini V., Barbara G. Non-Celiac Gluten Sensitivity in the Context of Functional Gastrointestinal Disorders. Nutrients 2020;12(12):3735. [CrossRef]
- Verdu E.F., Huang X., Natividad J., Lu J., Blennerhassett P.A., David C.S., McKay D.M., Murray J.A. Gliadin-dependent neuromuscular and epithelial secretory responses in gluten-sensitive HLA-DQ8 transgenic mice. Am J Physiol Gastrointest Liver Physiol. 2008;294(1):G217-225. [CrossRef]
- Verdu E.F., Armstrong D., Murray J.A. Between celiac disease and irritable bowel syndrome: the “no man’s land” of gluten sensitivity. Am J Gastroenterol. 2009;104(6):1587–94. [CrossRef]
- de Punder, K.; Pruimboom, L. The dietary intake of wheat and other cereal grains and their role in inflammation. Nutrients 2013, 5, 771–787. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



