Submitted:
02 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Functional health literacy is the ability to read, write, and speak about health. Functional health literacy events can nudge the development of children’s health identity when using valid and reliable reading materials that portray the “what, where, when, why, and with whom” to eat nutritious foods and be physically active. Children who lack social role models for healthy eating and physical activity may also lack development in language and motor skills. Therefore, literacy-rich environments are needed when developing cognitive-motor language skills with children. Children with obesogenic body frames can gain from the production of childcentric health narratives that draw upon the Habits of Mind and Habits of Health© Model to produce Electronic Texts for Health Literacy©. When health professionals plan and implement functional health literacy events so children can read, write, and speak about their own health, new behavioral patterns and routines emerge into performances of understanding. Constructivist pedagogical approaches can help children to create health narratives using multimodal language while practicing health literacy skills as a foundational impetus to health behaviors. Children who struggle with obesity can also gain social agency when writing with peer partners who serve as supportive collaborators when developing interactive health literacy.
Keywords:
obesogenic frames
; Habits of Mind and Habits of Health© Model
; functional health literacy
; interactive health literacy
; constructivist pedagogical approaches
; writing
1. Introduction
In a parable of the child who has a body frame size with an above average amount of adipose tissue, professionals and parents need to explore any emotional messages that are being signaled by the child within public and private view. Emotional communication for a child with an obesogenic frame can often be difficult because they may have an underdeveloped language (or vernacular) for health, a lack of encouragement by significant others, and insufficient balance between their identity and social agency. Moreover, in situations where the expressive language of the child is not supported by the arts, dance, or health literacy events, the body language of the child may be the only means of communication until the mind and body are taught to become integrated and whole through above-the-waist and below-the-waist rhythmical activities. Whereas past narratives have separated the corporeal body and the reasoning mind in human development for psychic analysis, the reintegration of a “Sound Mind and a Sound Body” (Locke, 1706) is an essential principle for the child when breathing at rest and when in motion. The rhythm of inhaling and exhaling oxygen from outside to inside of the body and mind forms a pattern for how much the child will be animated by their spirit breath to sit and stand, to move and rest, to skip and dance, to jump and run, and to hop and reach. When children practice health-related patterns and routines consistently using rhythm, continuity, and flow, the expressive language of the child will be a performance of understanding that increases in self-efficacy and social agency. However, language informs this performance of understanding by not only non-verbal communication but by verbal communication as well.
The interior environment of the human frame includes the core identity of the person, often constructed by the public feedback that the child receives. Whereas a child with underdeveloped speech and/or delayed language patterns may not know how to negotiate the hurt or disparaging looks or comments that result when living with an obesogenic body frame, the significant others who support that child’s emotional core with honor and respect will influence the child’s attitude or behavior, known as the frame of mind. The purpose of this paper is to advance a new genre of health literacy texts to explore a child’s frame of mind and behavioral intentions when participating in health literacy events that are child-centered, multimodal, and arts-based. This paper will highlight an integrated Habits of Mind and Habits of Health© model so that children are able to practice daily patterns and routines for health. By using words, pictures, numbers, rhythm, and environmental cues to construct Electronic Texts for Health Literacy©, children are also able to demonstrate health literacy when they construct narratives using health-related skills such as interpersonal communication, decision making, and goal setting, to name a few.
The National Health Education Standards (National Consensus for School Health Education, 2022) were written to guide the development of curricula, instruction, and assessment for preK-12 health education. Eight national standard statements promote student knowledge and skill development for health education. One of the eight standards focuses on health literacy, which reads “Students demonstrate health literacy by accessing valid and reliable health information, products, and services to enhance health”. The word “valid” refers to health information that is accurate, credible, and not misleading (National Consensus for School Health Education, 2022). The word “reliable” means consistent and trustworthy (National Consensus for School Health Education, 2022). Health literacy can include functional health literacy, which is a personal skill, and interactive health literacy, which is an interpersonal social skill. In the National Health Education Standards (2022), these two forms of health literacy are believed to be developmentally more age-appropriate across the preK-grade 12 school years than the highly cited original framework from Nutbeam (2000) or the findings by Schulenkorf, Sorensen, and Orkan (2022). Functional health literacy is “the ability to read, write, and speak about health” (Ubbes & Ausherman, 2018, p. 31) whereas interactive health literacy is the “interpersonal communication between people, including their interactive use of print and electronic materials to enhance health (Ubbes & Ausherman, 2018, p. 31).
In research with young children who were given the opportunity to speak for themselves, Derwig, Tiberg, & Hallstrom (2020) determined that children could take an active role in their health by interpreting illustrated health messages in a different way than adults. Child-centered constructivist approaches are encouraged (Ubbes & Whitesel, 2022) which includes age- and developmental-related needs for health literacy when distinguishing school children and adolescents from adults (Schulenkorf, Sorensen, & Orkan, 2022; Bröder, Okan, Bollweg, Bruland, Pinheiro, & Bauer, 2019) and when transitioning preschool children into preK-grade 12 schooling (Ubbes, 2023). According to the National Health Education Standards (National Consensus for School Health Education, 2022), some of the examples for performance expectations for grade 2 students would be “to use functional health literacy (e.g., reading, writing, and speaking) to access trustworthy health information to learn functional health knowledge”, and then by grade 5 “to use functional health literacy skills (e.g., reading, writing, and speaking) to access valid and reliable health information to learn about health behaviors”. Other grade 5 expectations would be to “access multimodal health messages (e.g., words, pictures, numbers, and/or gestures) in print or electronic materials to practice interactive health literacy). By grade 8, students would “access credible websites or health-related applications using technology to support health behaviors” and then in grade 12, students would “demonstrate functional health literacy (e.g., reading, writing, and speaking) to evaluate valid and reliable health information about a health behavior”.
For the purposes of this project, health literacy events are adopted from the work of Rumenapp and colleagues (2023, p. 11) who conceptualize them as “the ways in which students, teachers and other community members can use a focus on health literacy to accomplish particular health goals. It can also be used to allow researchers to advance work on understanding how classroom activities can utilize existing funds of knowledge in a responsive way as part of future health literacy curricula. In this way, schools can become sources of community empowerment in a society that sets up too many barriers to equitable health and education”. Therefore, in the current project, when children are encouraged to use functional health literacy to write health narratives about obesity prevention and other health behaviors, that literacy event is meeting health goals. The value of these health literacy events within health education, specifically, is to affect educational outcomes for student performance at school among children who are obese (Taras & Potts-Datema, 2005).
2. Materials and Methods
Children grow up learning health-related routines which can be foundational to life. Why not expose children to health-related messages via print and electronic books when they are also learning and practicing health behaviors? By reading to and reading with children, the language of health can be shared as an extension to the lifestyle practices of home and school. Both home and school environments should surround children with messages of health. Messages that are shared person to person are especially needed for children, but they cannot be the only health messages. Valid and reliable health information can be shared and vetted via print and electronic resources to augment what is exchanged during interpersonal conversations. A way to ensure that the information can be accessible for the greatest number of people is to use multimodal language approaches (Ubbes & Njoku, 2022) and multimedia approaches (e.g., print and electronic). In a systematic review of 12 empirical studies looking at health literacy in early childhood, Banfai-Csonka and colleagues (2022) found that picture-based messages or story-based messages with illustrations helped to support the development of health literacy when the studies focused on food, nutrition and oral health.
To ensure transactional communication occurs during interpersonal conversations, children should process the information being shared through receptive and expressive language. This includes repeating back what they heard and then determining whether they understood the information. Sometimes expressive language can also include the use of singing, drawing, acting, and dancing to communicate a performance of understanding (Perkins, 1988). This reflective and inquiry-based process can elicit ‘sources of knowledge’ being developed between children and their caregivers rather than ‘sources of information’ being the primary focus of the educational intervention. When interpersonal conversations involve the sharing of health knowledge, attitudes, and behavior and includes learning valid and reliable health information via technology, this can also be called interactive health literacy.
Language and literacy share a ‘symbiotic relationship’ (Nippold, 1988, p. 29). Word learning in any school subject is important. In health education, word learning is limited because very little time is dedicated to the subject matter in the academic curriculum. Lowe and colleagues (2022) suggested that “typically developing older children and adolescents independently absorb the meanings of new words through reading”, but children and adolescents with a language disorder will “need direct instruction in how to derive meaning from context”. Interactive health literacy may be an effective way to relate word meanings to personal health experiences through simulations or role plays with parents, peers, and health professionals. But since there is insufficient time for health education in the school curriculum, learning time should include be dedicated to cognitive-behavioral skill development and functional health knowledge. Interactive health literacy events would be especially helpful when children have a poor existing vocabulary knowledge about health and lack role models for practicing health-related skills and behaviors.
Health education is a social and behavioral science that communicates how individuals and groups of people can build cognitive-behavioral skills through continual practice. Cognitive-behavioral skills outlined by the Habits of Health and Habits of Mind Model© (Ubbes, 2008) support learners across the lifespan to recognize the relationship between their health habits and quality of life. Many of our Electronic Texts for Health© use one Habit of Health (behaviors) and one Habit of Mind (cognitive skills) to model how people can be healthy.
The collection of Electronic Texts for Health Literacy© that are the focus of this project have three language themes (Ubbes, 2024) woven through their design: 1) body language showing how human actions are described visually and named textually by its referent body part (or human senses) rather than assuming that an action of the body part “just happened” in the background; 2) written language showing how a personal health narrative is communicated in pictures and in words while using English (and sometimes, in at least one other language), and 3) oral language showing how health is talked about as an interactive literacy between a reader and one other person or groups of people – recognizing that meaning making and comprehension is socially constructed.
3. Results
The Health Literacy Database at Miami University served as the research tool for locating child-centric artistic materials on the topic of obesity and overweight that are known to be valid, reliable, authentic, and equitable for children, youth, and adults (Ubbes, 2024). A search for the number of Electronic Texts for Health Literacy© resulted in 98 health narratives on physical activity, 72 health narratives on nutrition, and 55 health narratives on relationships. Other health-related topics not included in this study were electronic texts for feelings, oral health, sleep, rest, quiet time, safety, hygiene, and stress management. From a total collection of 190 compositions, 52 percent focused on physical activity, 38 percent focused on nutrition, and 29 percent focused on relationships. A search for the term “obesity” produced only three Electronic Texts for Health Literacy©, which represented only 1 percent of the available health narratives. Therefore, selected narratives are depicted below in the result section to provide examples of valid and reliable information from which obesity can be prevented or reduced.
3.1. Conceptual Model and Theoretical Framework
The conceptual model for the project was the Habits of Health and Habits of Mind Model© shown in Figure 1 below. Students choose one Habit of Health (a health behavior) and one Habit of Mind (a cognitive skill) when writing an Electronic Text for Health Literacy©.
The theoretical framework used when writing the Electronic Texts for Health Literacy© was the Integrative Theory of Behavioral Prediction (Yzer, 2012), which has been described in detail elsewhere (Ubbes & Witter, 2021). Table 1 shows an example of a health literacy narrative which uses three components of the Integrative Theory of Behavioral Prediction, e.g., efficacy beliefs, health outcome beliefs, and normative beliefs. The transcript in the right column shows how the text of the health literacy narrative entitled “Making the Decision to Eat Fresh Food” is aligned to the three beliefs.
3.2. Figures, Tables and Schemes
Research results from the study are shown below with obesity prevention connections.
Figure 2.
Example of an Electronic Text for Health Literacy© Title Page.
Figure 3.
Example 2 of a Health Literacy Narrative for Obesity Prevention.

Figure 4.
Example of a Health Literacy Narrative for Goal Setting with the Spanish Translation for the Word ‘Hungry’.
Figure 4.
Example of a Health Literacy Narrative for Goal Setting with the Spanish Translation for the Word ‘Hungry’.

Figure 5.
Example of a Loss Frame Strategy for a Health Literacy Narrative for Goal Setting, including the Spanish Translation for the Word ‘Dinner’.
Figure 5.
Example of a Loss Frame Strategy for a Health Literacy Narrative for Goal Setting, including the Spanish Translation for the Word ‘Dinner’.

Figure 6.
Example of a Health Literacy Narrative on Building Healthy Relationships with Friends (Peers).
Figure 6.
Example of a Health Literacy Narrative on Building Healthy Relationships with Friends (Peers).
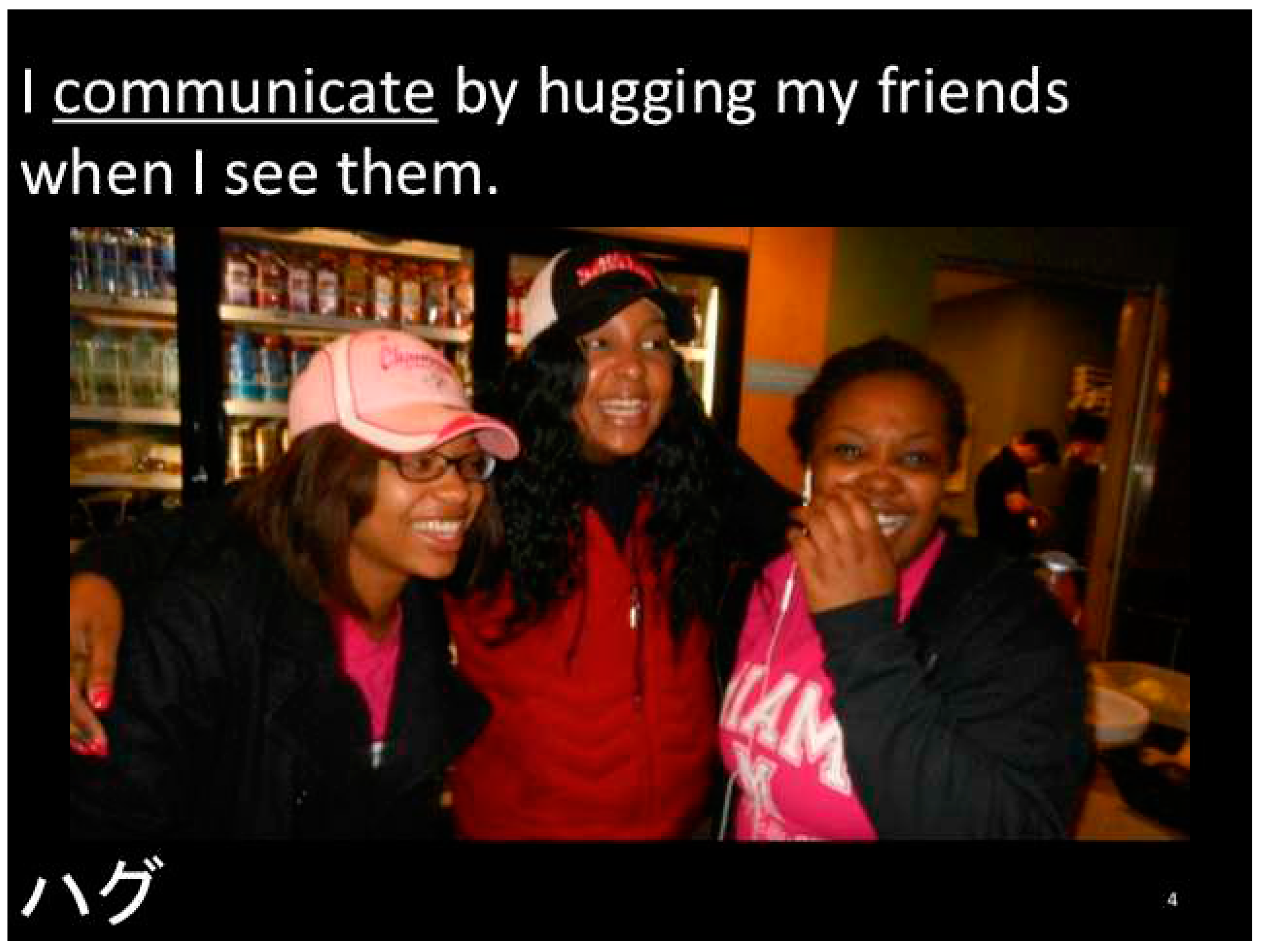
Figure 7.
Example of a Health Literacy Narrative for Building Healthy Relationships with a Parent by Staying Active During Middle School.
Figure 7.
Example of a Health Literacy Narrative for Building Healthy Relationships with a Parent by Staying Active During Middle School.

Figure 8.
Example of a Health Literacy Narrative for Healthy Eating with Social Norms from Peers.
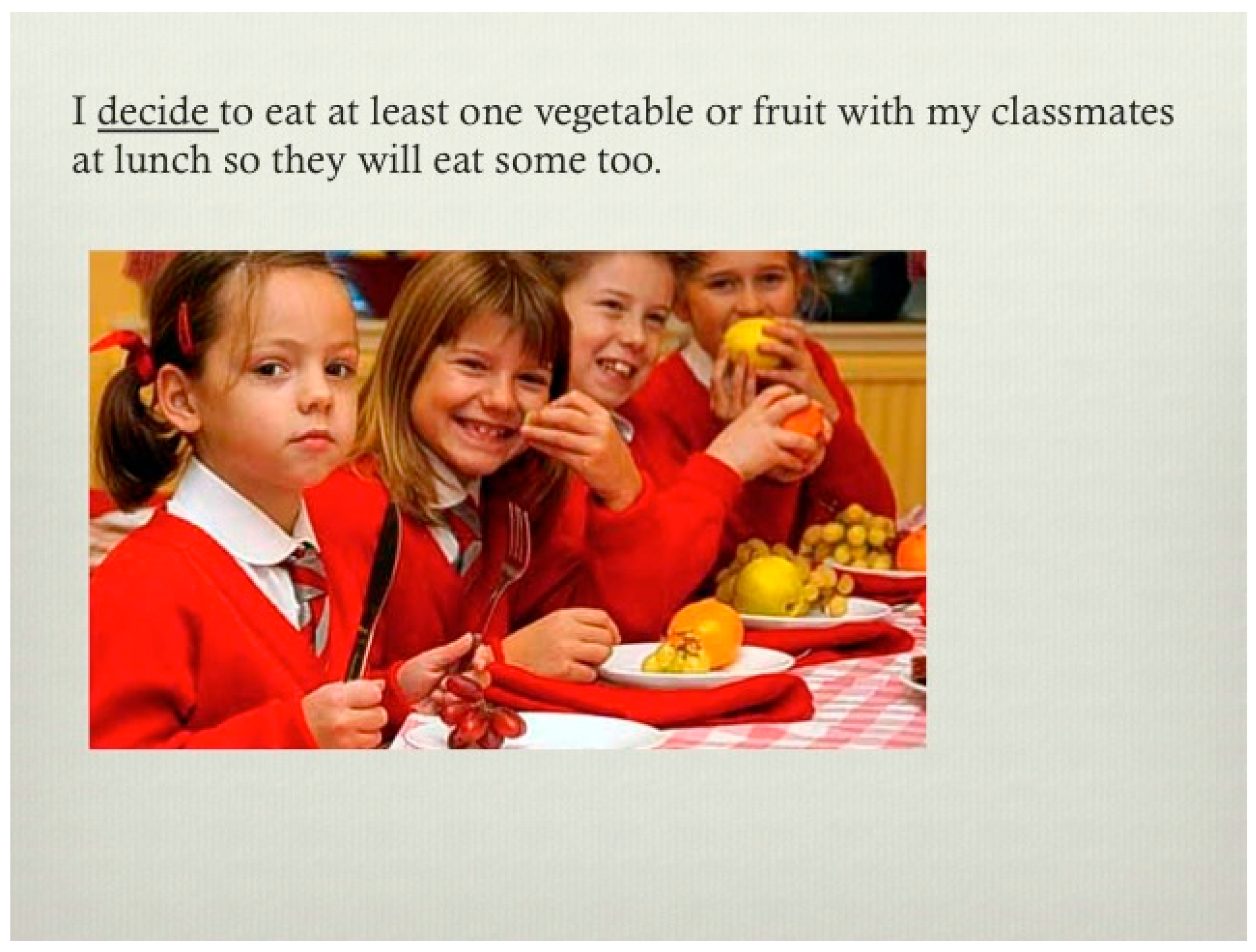
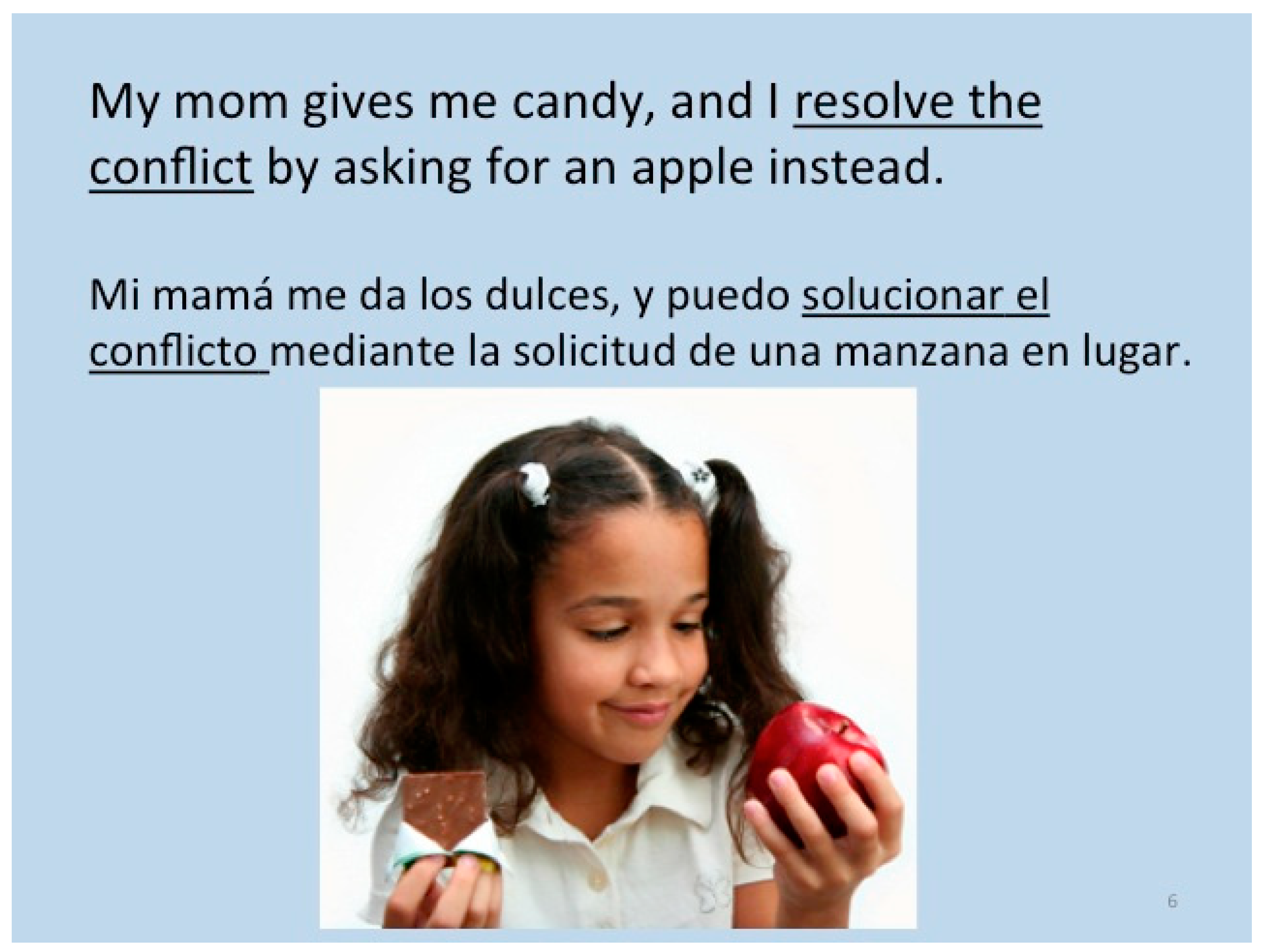
Figure 9.
Example of a Gain Frame Strategy for a Health Literacy Narrative on Healthy Eating and Physical Activity with Health Outcome Beliefs and Normative Beliefs within a Family Relationship.
Figure 9.
Example of a Gain Frame Strategy for a Health Literacy Narrative on Healthy Eating and Physical Activity with Health Outcome Beliefs and Normative Beliefs within a Family Relationship.
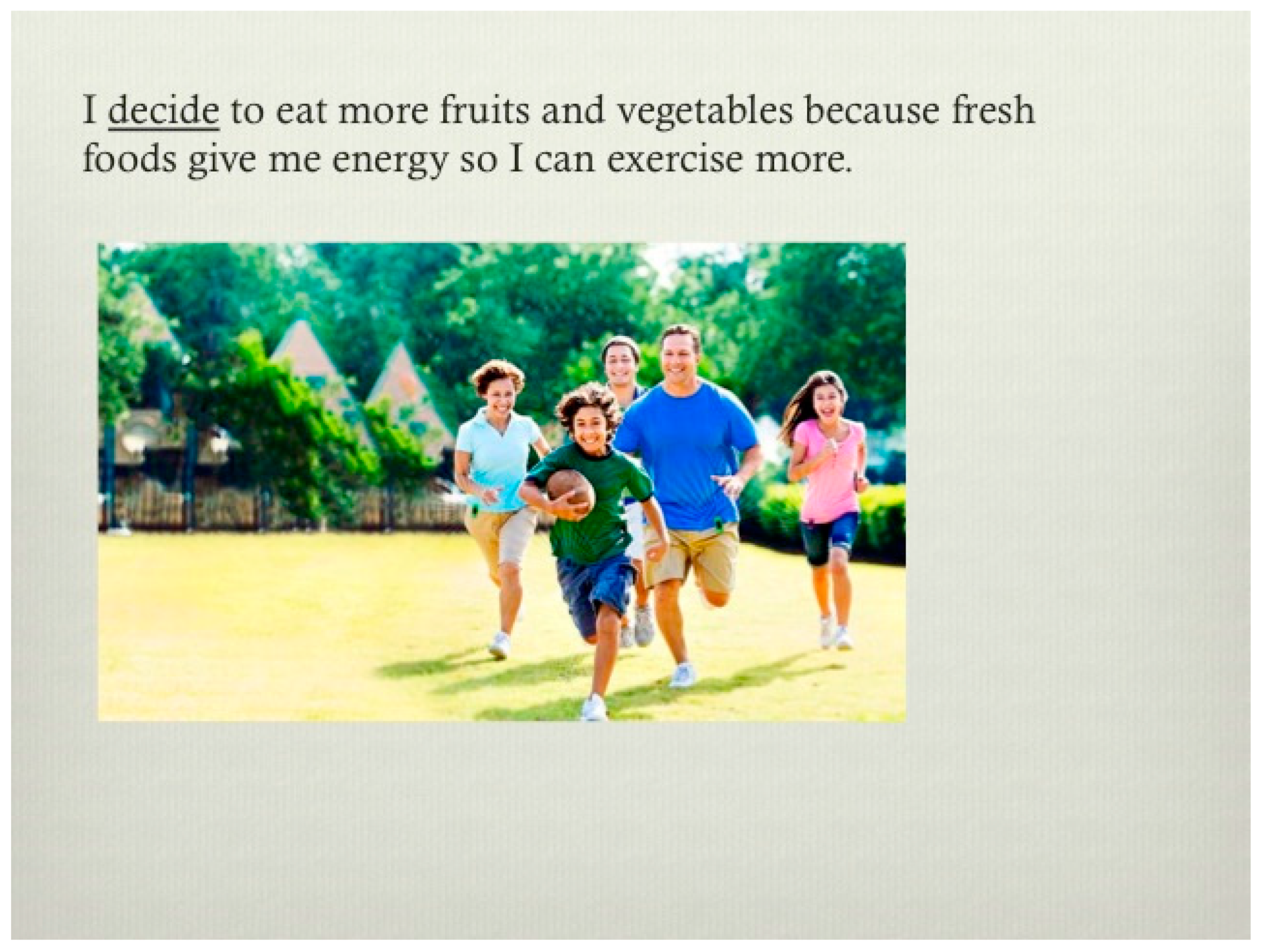
Figure 10.
Example of a Gain Frame Strategy for a Health Literacy Narrative on Nutrition, Including the Spanish translation of the sentence.
Figure 10.
Example of a Gain Frame Strategy for a Health Literacy Narrative on Nutrition, Including the Spanish translation of the sentence.
4. Discussion
Current data show that 21-24 percent of American children and adolescents are overweight, and another 16-18 percent are obese. Obesity is the most prevalent nutritional disorder among children and adolescents in the United States (Schwarz & Bhatia, 2023). The World Health Organization has indicated that overweight and obesity conditions kill people more than underweight conditions. In 2020, 39 million children under the age of five were overweight or obese. Globally, over 340 million children and adolescents aged 5 to 19 were overweight or obese in 2016 (WHO, 2021). The main health consequences of overweight and obesity are heart disease, stroke, osteoarthritis, and some cancers (including endometrial, breast, ovarian, prostate, liver, gallbladder, kidney, and colon)
In the current study, students chose to write about obesity or overweight using strategic ways that they could be working on health-related behaviors and life skills. Even though the “lived experiences” of the students as writers did not represent a wide selection of photos with obesogenic frame sizes, the Figure 5, Figure 6, Figure 9 and Figure 10 shown above indicated that students were aware of the gain frame and loss frame concepts regarding weight control through nutrition, physical activity, and social relationships when they wrote their health literacy narratives.
When working with the psychological aspects of obesity, educators and researchers need to support children and youth with underlying motivations for their obesity. Programs and educational materials should address the salient social norms (normative beliefs, health outcome beliefs, and self-efficacy beliefs) surrounding healthy and unhealthy decisions (Yzer, 2012) by doing semi-structured interviews to learn the needs and perspectives of children and youth. Creating new resources in tandem with young people also gives them a chance to co-write and compose narratives that are relatable and authentic for themselves. Schunk and DiBenedetto (2020) emphasize that self-efficacy is domain specific and that a general self-efficacy does not exist. Hence, research on cultural contexts is important since non-Western cultural tend to place greater emphasis on effort as a cause of success where Western cultures emphasize ability. By involving children in writing their own narratives of self-efficacy and choosing what cognitive skill they will employ when working toward a health behavior, the is a greater chance that their narrative constructions will draw from their cultural backgrounds.
One important educational goal for children and youth is to increase their awareness about the need for daily self-care. The Habits of Health and Habits of Mind© Model is a visual, textual, and gestural tool for supporting the development of healthy patterns and routines for everyday guidance and reflection. As children mature, the importance of setting boundaries to maintain or improve their health is also valuable. Boundaries can be described as frames of mind that are something you “set” or “make” based on a plan of action or story narrative. Prevention must be set and planned so with erratic schedules in children’s lives, including unhealthy social role models, crafting story narratives out of prevention approach fits quite nicely into health education curricula, including literacy courses where the focus can accommodate health literacy with dedicated teachers.
In its basic form, educators can use the health literacy framework provided in this paper to teach a deeper reading of an Electronic Text for Health Literacy© in order to first talk about it and interpret it on a social classroom level and then to search for deeper meaning on a personal level. As a pedagogical tool, teachers can ask students to write a health literacy text with a peer to gain multiple perspectives as they compose the narrative together in words, pictures, and numbers related to a health topic like obesity prevention. Teachers can also ask students to compose another health literacy text using a different cognitive skill so they can practice the health-related language or jargon for writing declarative sentences related to obesity prevention, such as healthy eating, physical activity, and building relationships with others. The motivation for this constructivist approach is that students have become too reliant on technology, and “have become disempowered, giving power to their digital devices, and not relying on the power within themselves. Students are no longer independent and free thinking; instead, they have become overly dependent on their smart phones, laptops and tablets, thereby disabling their capacity for self awareness, self-reflection and empathy toward others. Digital devices are numbing students’ sensibilities“ (Keator, 2018, p. 2). Because Keator suggests that students are “Fixated on their digital devices, (and) they no longer have the capacity to be self-aware, aware of the needs of others, engage a literary text or relate to their surrounding environment”, this project of functional health literacy and interactive health literacy brings students into a proactive use with their computers and digital devices to become healthier.
Future research should see how counselors, therapists, and social workers may also benefit from collaborating with children with an obesity or overweight condition to write something together while talking things out. The ability to craft artistically and even use personal photographs with parental approval may result in a health literacy narrative that helps children to become empowered by their written self-talk while practicing health-related skills, e.g., Habits of Mind. This form of child-centric narrative writing with health literacy as a frame of mind both visually and textually can be an educational way to develop literacy skills with health behaviors.
A recent area of concern in obesity prevention is oral health hygiene because the gut biome is responsible for balancing the lymphatics of the immune system for the health of the body and brain in disease prevention. According to the World Health Organization (2024), a key health-promoting message is that “Oral health is the state of the mouth, teeth and orofacial structures that enables individuals to perform essential functions such as eating, breathing and speaking, and encompasses psychosocial dimensions such as self-confidence, well-being and the ability to socialize and work without pain, discomfort and embarrassment. Oral health varies over the life course from early life to old age, is integral to general health and supports individuals in participating in society and achieving their potential”. When children do not brush and floss their teeth adequately and consistently, opportunistic diseases can occur – many with connections to overweight conditions and obesity.
5. Conclusions
This project is grounded in the hypothetical question “Whose Frame of Reference?” when working with children who have obesity or overweight conditions. The use of child-centric narratives is advanced using a constructivist pedagogical approach to explore children’s frame of mind and behavioral intentions with obesity and weight management. A new genre of health literacy texts provides a way to use visual-textual narratives to help children build their repertoire in functional health literacy and interactive health literacy while thinking about a Habit of Mind and a Habit of Health in tandem. Access to the academic website called the Health Literacy Database at Miami University (https://ulblwebp09.lib.miamioh.edu/healthliteracy/) will provide professionals and their students and clients with a writing template for developing reading, writing, and speaking skills for functional and interactive health literacy.
Supplementary Materials
I’m not sure if I have any of these. Please advise.
Funding
This research received no external funding.
Data Availability Statement
Links to publicly archived datasets are available at the Digital Literacy Partnership website @ https://dlp.lib.miamioh.edu Specific resources shared in this manuscript are available at the Health Literacy Database at Miami University @ https://dlp.lib.miamioh.edu/healthliteracy/ Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
Acknowledgements are made to Ken Irwin, Web Services Librarian, Miami University, King Library 302, 151 S. Campus Avenue, Oxford, OH 45056, for website upgrades to the Digital Literacy Partnership website during the writing of this manuscript. Administrative and technical support from Miami University Libraries is also acknowledged.
Conflicts of Interest
The author declares no conflicts of interest.
Appendix A
Depending upon space availability, I will be able to include a template for how to write sentences for an Electronic Text for Health Literacy.
References
- Bandura, A. (1997). Self-efficacy: The exercise of control. MacMillan.
- Bröder, J., Okan, O., Bollweg, T. M., Bruland, D., Pinheiro, P., & Bauer, U. (2019). Child and youth health literacy: a conceptual analysis and proposed target-group-centered definition. International Journal of Environmental Research and Public Health, 16(18), 3417. [CrossRef]
- Keator, M. (2018). Lectio Divina as contemplative pedagogy: Re-appropriating monastic practice for the humanities (Vol. 16). New York: Taylor & Francis. [CrossRef]
- Lowe, H., Henry, L., Wallinger, J., & Joffe, V. (2022). Teaching vocabulary to adolescents with language disorder: Perspectives from teachers and speech and language therapists. Child Language Teaching and Therapy, 1-20, . [CrossRef]
- Medline Plus. Calculating body frame size. National Library of Medicine. U.S. Department of Health and Human Services. National Institutes of Health. Available online: https://medlineplus.gov/ency/imagepages/17182.htm#top (Accessed on 1 February 2024).
- National Consensus for School Health Education. (2022). National Health Education Standards: Model Guidance for Curriculum and Instruction (3rd Edition) www.schoolhealtheducation.org.
- Nippold, M.A. (1988). Later Language Development. Boston: Little, Brown and Company.
- Nutbeam, D. (2000). Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International. 15: 259–267. [CrossRef]
- Rumenapp, J. C., Troiano, B., Adams, M., Moya, J., Lawrence, E., & Razfar, A. (2023). Developing health literacy events: A case study of teachers designing health curricula. Health Education Journal, 82(6), 651-663. [CrossRef]
- Schunk, D. H., & DiBenedetto, M. K. (2020). Motivation and social cognitive theory. Contemporary Educational Psychology, 60, 101832. [CrossRef]
- Taras, H., & Potts-Datema, W. (2005). Obesity and student performance at school. Journal of School Health, 75(8), 291-295. [CrossRef]
- Ubbes, V.A. and Miami University Libraries (2024). Digital Literacy Partnership website. Available online: https://ulblwebp09.lib.miamioh.edu (accessed on 1 February 2024).
- Ubbes, V.A. (2024). Emergent literacy is foundational to health literacy in children: Interdisciplinary relationships to boost child health. In Şenol, H. (Ed.). Recent Perspectives on Preschool Education and Care. IntechOpen. Available online: https://www.intechopen.com/chapters/88184 (Accessed on 1 February 2024). [CrossRef]
- Ubbes, V., & Whitesel, S. (2022). Use of an eBook for Oral Health Literacy© Curriculum to elicit functional health knowledge, decision making, and goal setting among school-aged children. International Electronic Journal of Elementary Education, 15(2), 145-159. [CrossRef]
- Ubbes, V. A., & Njoku, B. (2022). A curriculum, instruction, and assessment (CIA) framework for health literacy education (HLE) in medical and health professions schools. World Journal of Social Science Research, 9(1), 15-55. [CrossRef]
- Ubbes, V.A., & Witter, A.M. (2021). Parental influences on children’s oral health behaviors, reading behaviors, and reading attitudes associated with the sharing of a digital story from the eBook for Oral Health Literacy© Curriculum. Children and Teenagers. 4(3), 26-55. [CrossRef]
- Ubbes, V. A., & Ausherman, J. A. (2018). A historical interpretation of how 19th and 20th century books contributed an early language and vocabulary for health literacy. The Health Educator, 50(2), 26-40.
- Yzer, M. C. (2012). The integrated model of behavioral prediction as a tool for designing health messages. In H. Cho (Ed.), Designing Messages for Health Communication Campaigns: Theory and Practice (pp. 21-40). Thousand Oaks, CA: Sage.
- World Health Organization (2024). Oral health. Available online: https://www.who.int/health-topics/oral-health#tab=tab_1 (accessed on 1 February 2024).
Figure 1.
Habits of Health and Habits of Mind© Model.
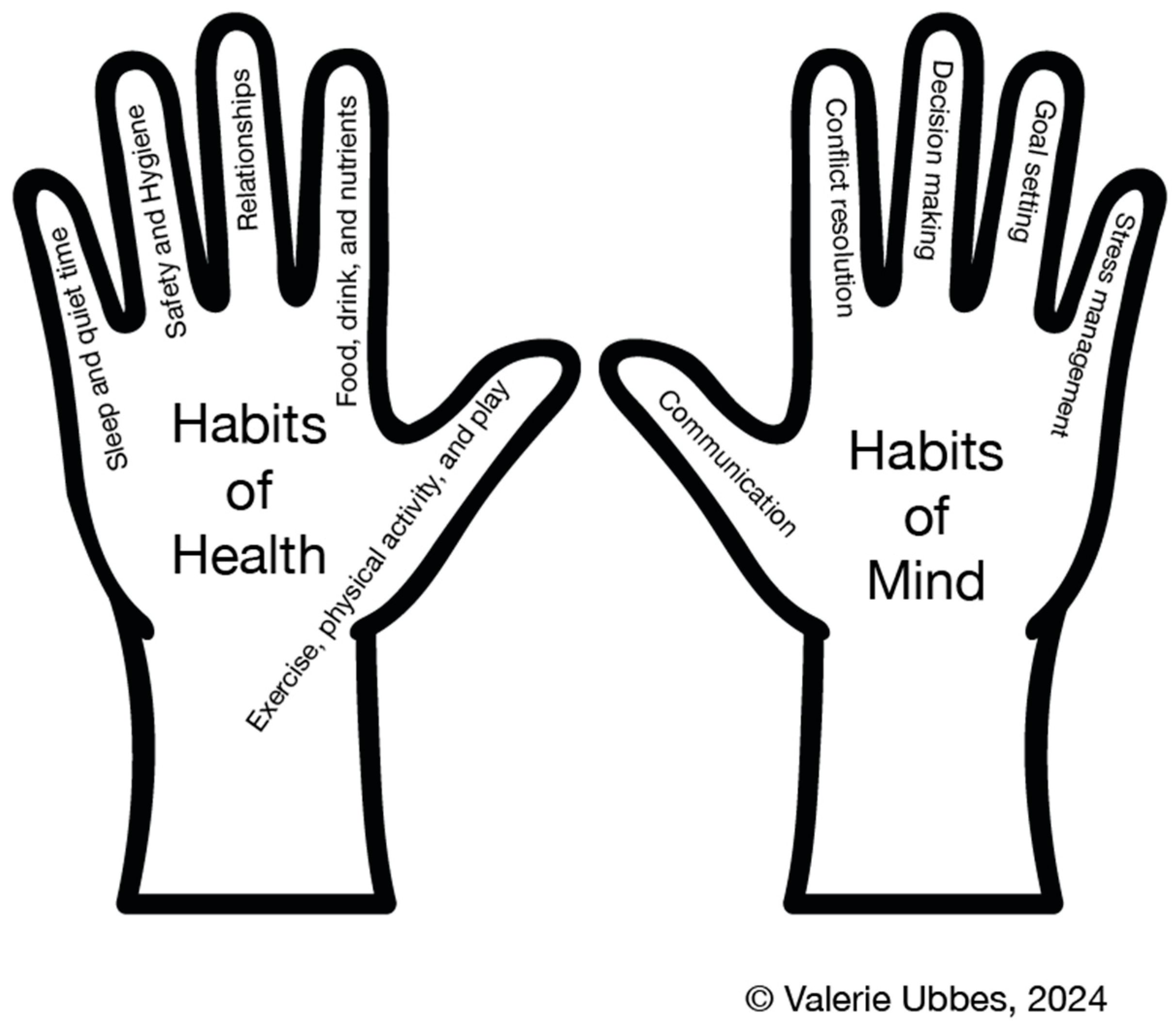

Table 1.
Example of a Health Literacy Narrative with Three Theoretical Components.
| Theoretical Components | Transcript of a Health Literacy Narrative |
|---|---|
| Skill: Decision Making |
Making the Decision to Eat Fresh Food By Melanie Dow https://ulblwebp09.lib.miamioh.edu/healthliteracy/items/show/298 |
| Efficacy Belief | I believe that I will make the decision to eat more fruits and vegetables at a young age because fresh food makes me live longer. |
| Health Outcome Belief | I decide to eat more fruits and vegetables because fresh foods give me energy so I can exercise more. |
| Health Outcome Belief | I decide to start buying my own fresh food so that I will prevent obesity. |
| Health Outcome Belief | I decide to start eating more fruits and vegetables because fresh foods can strengthen my immune system and prevent illnesses. |
| Normative Belief | I decide to encourage my family to start snacking on fresh food so that we will have a reduced risk for heart disease. |
| Normative Belief | I decide to eat at least one vegetable or fruit with my classmates at lunch so they will eat some too. |
| Health Outcome Belief | I decide to eat a fruit instead of a dessert after dinner in order to get my daily nutrient and vitamin intake. |
| Efficacy Belief | I believe that my decision to eat more fresh foods at meals will help me to live a healthier lifestyle. |
| Interactive Health Literacy | SummaryI’ve made the decision to eat fresh food. How about you? Have you made a decision too? |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



