
Submitted:
03 February 2024
Posted:
05 February 2024
You are already at the latest version
Abstract
Cardiotoxicity remains one of the leading causes of morbidity and mortality in childhood cancer survivors. This study aimed to evaluate cardiotoxic side effects of chemotherapeutic regimens in a pediatric population, as revealed by assessment of baseline end-of-treatment and in follow-up after 1 year. A prospective study was conducted on 39 children, enrolled over a period of 5 years (2017-2022), diagnosed with leukemia and receiving chemotherapy regimens. A multimodal echocardiographic evaluation was done (two-dimensional echocardiography and M-mode, tissue doppler imaging (TDI) and 2D-speckle tracking (2DST) before the initiation of the cytostatic treatment, at the end of the treatment and 1 year after the treatment. Ultrasound-derived parameter values were compared between evaluations and correlated with cumulative doses of chemotherapeutic agents used. There were no significant differences in mean values for any of the imagistic parameters analyzed. However, a significant correlation was found between E’value percentage variation and cumulative dose of both anthracyclines and antimetabolics administered (p=0.03). Moreover, a significant linear regression correlation was found between alkylating agent dose and global longitudinal strain (GLS)(p<0.01). Non-invasive cardiovascular imaging parameter values did not differ significantly from baseline in our study, but some of them seem to be dependent upon cumulative dose of cytostatic agents used. Further studies on larger populations and involving a longer follow-up period might provide more insight into cardiotoxicity of chemotherapy regimens.
Keywords:
echocardiography
; speckle-tracking
; cardiotoxicity
; chemotherapy
; children
1. Introduction
The Pediatric oncological diseases represent rare conditions, with an incidence of 400 new cases per year reported at national level, according to data curated between 2010 and 2017 by the Romanian pediatric oncological registry [1]. Still, cancers represent one of the leading cause of death at pediatric ages, in spite of significant advances in their specific treatment protocols in the past 50 years which yielded better survival rates [2,3]. However, chemotherapy regimens can lead to side effects which range from acute toxicity to prolonged, long-lasting, irreversible effects which impact quality of life [4,5,6]. The existence of the clinical field of cardio-oncology has shown the need for the research of the diseases and cytostatic treatments it being known that the survivors of cancer have a hight risk of developing cardiomyopathies secondary to cardiotoxicity.
Cardiotoxicity represents one of the most worrying complications related to cytostatic treatment, which can significantly increase morbidity and mortality in pediatric oncological diseases [7]. There are two types of cardiac toxicity described, depending on their reversibility [8]. Type I cardiotoxicity has been classically attributed to anthracycline use, as this class of drugs presents a high affinity for the inner mitochondrial membrane, inducing oxidative stress and consequently apoptosis [9].
Considering that many oncological patients can present cardiovascular risk factors and/or pre-existing asymptomatic cardiovascular diseases, baseline evaluation of cardiac function and its structure is recommended to be performed before initiation of treatment, as well as regularly during chemotherapy [7,9,10]. Early cardiac dysfunction usually translates into arrythmias and other ECG anomalies, as well as pericarditis or myocarditis [11]. Left ventricular (LV) dysfunction, regarded through a decrease in its ejection fraction (EF) can usually be depicted in the late evolution of cardiomyopathy, but its premature recognition can yield a better prevention of systolic heart failure through appropriate medication [11,12]. Therefore, a clear image of the cardiac structure and its systolic function should be obtained in each patient prior to treatment onset, which is easily achievable through transthoracic echocardiography (TTE) [13]. Invasive methods such as endomyocardial biopsy are considered the most accurate in assessing the extent of myocardial involvement, but are often considered as an ultimate option, due to the risks associated to the procedure [14]. Non-invasive methods are preferred, such as serum markers, which include the B-type natriuretic peptide (BNP), N-terminal pro-BNP (NT-proBNP) and troponin [13,15]. Long-term follow-up should involve periodic echocardiography monitoring and troponin I assessment, according to an expert consensus of the American Society of Echocardiography and the European Association of Cardiovascular Imaging [16].
Children undergoing chemotherapy regimens present a particularly high risk of developing heart failure on the long term, due to the wide use of anthracycline in childhood cancers, in more than half of different specific therapeutic regimens [17]. Toxic effect is dose-dependent, but constant exposure to low doses poses a significant long-time burden on the LV systolic function as well [18]. For precocious diagnosis of subclinical LV dysfunction, the addition of speckle-tracking to conventional echocardiography has been proposed in adults, which includes assessment of global longitudinal strain (GLS) [16]. This approach has also been considered in children, a meta-analysis revealing that speckle-tracking echocardiography can successfully identify early signs of myocardial injury in these age groups as well. However, a relation between myocardial deformation parameters and risk of heart failure has yet to be established in children, with more evidence being required on this matter [19].
The current study aimed to assess cardiotoxic effects of chemotherapeutic regimens in a pediatric population, as revealed by assessment of baseline and end-of-treatment speckle-tracking echocardiographic indices.
2. Materials and Methods
2.1. Study Population
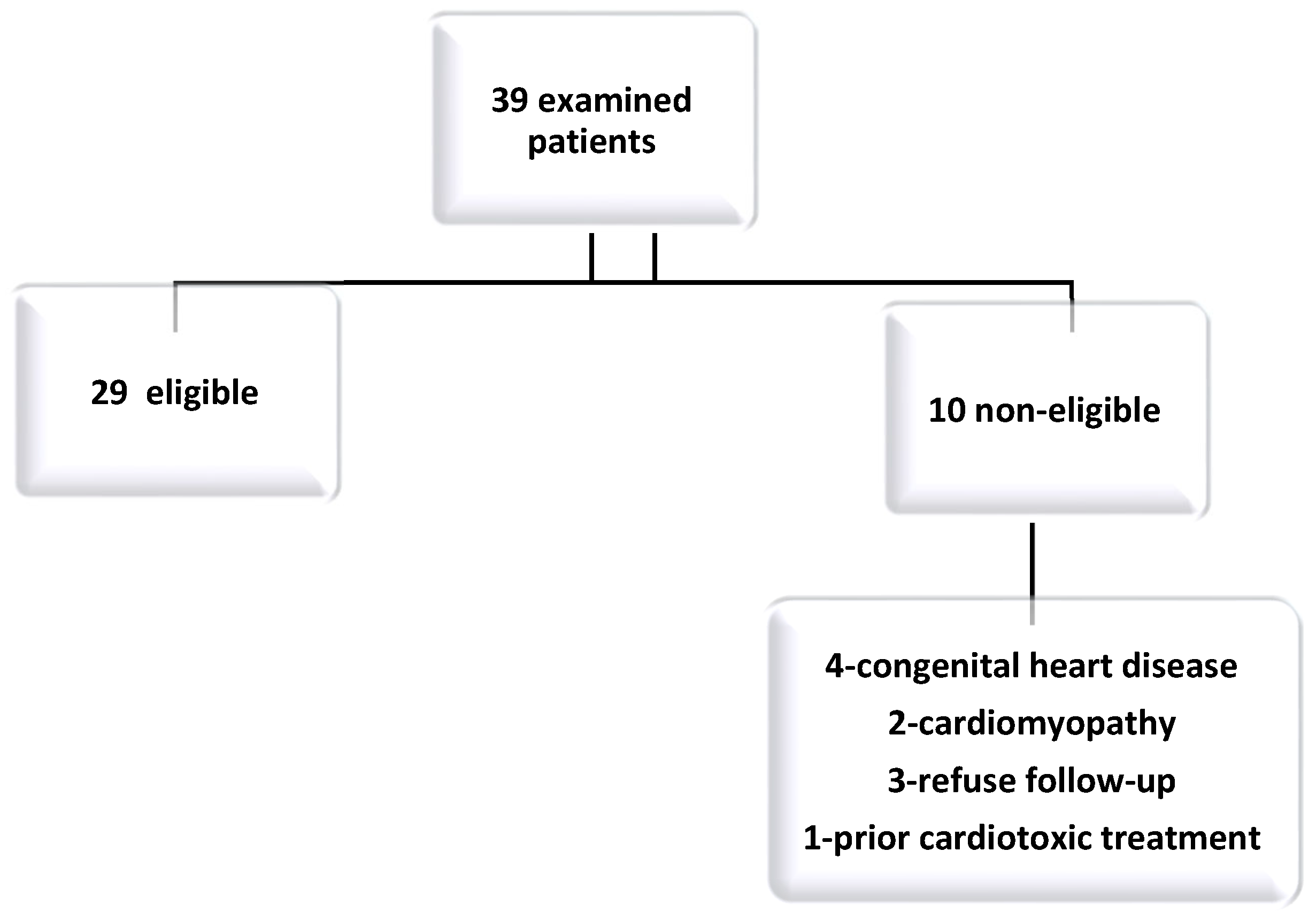
Study design—single center (Cardiovascular Emergency and Transplant Institute of Tg-Mures), longitudinal, prospective cohort study, that included 39 children, diagnosed with leukemia for a period of 5 years, from January 2017 until December 2022. All echocardiographies were performed with Philips Epiq 7 machine. The inclusion criteria were: patients with a diagnosis of acute leukemia who required chemotherapeutic regimens according to the latest therapeutic standardized protocols and presented a structurally and functionally normal heart upon the baseline echocardiography evaluation. The exclusion criteria were: patients with congenital heart disease, cardiomyopathy and patients who refused a control check-up. Furthermore, patients receiving chronic treatment with potential cardiotoxic adverse effects prior to cytostatic treatment initiation were also excluded from the study.
Figure 1.
Study flow chart.
2.2. Analysis of Sistolic and Diastolic Cardiac Function
Echocardiography exam was performed with a Philips Epiq 7 machine and 5-7Mhz phased-array matrix ultrasound probes. The examinations M mode, two-dimensional, tissue doppler imaging (TDI) and 2D speckle tracking (2DST) were performed prior to treatment initiation and at a mean follow-up of 209.5 days (±191 days) or at the end of the treatment and one year after treatment. Measurements were carried out in accordance with the recommendations of the American Society of Echocardiography [20]. Heart rate, electrocardiogram and blood pressure were recorded at the time of echocardiography.In compliance with the current guidelines for systolic function analysis, the EF was calculated using the Teicholz formula (in the absence of asynchrony signs) and the modified Simpson method (2D apical four chambers) [20]. Values of EF of less than 50% were considered indicative of a systolic dysfunction [21]. Transmitral flow patterns during early and late diastole were analized using pulsed Doppler. Velocities „E” and „a” were measured and their ratio was calculated considering a value greater than 2 as a sign of restrictive diastolic dysfunction or lesser than 1 as a delayed relaxation disastolic disfunction. Moreover, the evaluation of systolic and diastolic functions was performed using pulsed-wave tissue Doppler, lateral to the mitral annulus (apical 4 chambers view, during 5 cardiac cycles). Thus, systolic (Sa), early diastole (Ea) and late diastole (Aa) waves were considered as parameters of cardiac function and the value of „E/Ea” ratio above 10 was a marker of elevated LV pressure. Apical 2 chamber (A2C) and 4 chamber (A4C) views were acquired for 2D speckel tracking and for global longitudinal strain (GLS) assessment (Figure 2). A GLS value below 15% was considered abnormal.The recorded images were analyzed offline using a Philips Qlab 10 software. The data collected were used in the study to assess the evolution of cardiac function related to cumulative doses of cytostatics (by age and gender).
2.3. Ethics
The study was carried out in accordance with the principles stated in the Declaration of Helsinki. A signed, written informed consent was provided by at least one legal tutor of each patient prior to their inclusion in the study. Children whose caregivers refused to sign the informed consent form were not included in the study. The study was approved by the Ethics Committee of the George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu Mureș (Institutional Review Board number 33/01.03.2019). A signed informed consent was mandatory for which a thorough information session was carried for every parent or legal tutor of enrolled pediatric patients.
2.4. Statistical Analysis
Statistical analysis was performed using GraphPad Prism, version 9.0.2. Data were considered nominal or quantitative variables (ratios and range) and characterized by proportions or means, standard deviations (SD), medians and intervals. Data distribution normality testing was performed with the help of Kolmogorov-Smirnov test. ROUT test was applied for outlier identification. Mean comparison was conducted using the t test, whereas the Chi-square test was used to assess contingency tables. In order to assess procentual variation of each parameter evaluated during echocardiography and speckle-tracking echocardiography, the following formula was applied: [(first value-second value)*100/first value]. Correlations between cummulative doses of chemotherapeutics and ultrasound/speckle-tracking parameter variation were evaluated with the help of the linear regression equation. Every parameter was calculated in accordance with a 95% confidence intervals (95% CI), and a corresponding statistical significance level of 0.05.
2.5. Chemotherapy Protocol and Monitoring
All patients were treated according to the 2009 ALL IC-BFM protocol, which includes intensive treatment (with 3 stages: induction, consolidation and reinduction) and maintenance treatment. The induction phase involves the administration of prednisone, anthracycline (epirubicin), vincristine, asparaginase, cyclophosphamide, 6-mercaptopurine, cytarabine and methotrexate. The consolidation phase includes 6-mercaptopurine and methotrexate and the reinduction phase dexamethasone, anthracycline (epirubicin), vincristine, asparaginase, cyclophosphamide, thioguanine, cytarabine and methotrexate. Intensive treatment is followed by maintenance treatment with 6-mercaptopurine and methotrexate per os. Each patient had a complete baseline assessment prior to initiation of chemotherapy, echocardiography and blood tests (complete blood count, peripheral smear, C-reactive protein, complete biochemistry, coagulogram). Blood tests were monitored weekly during treatment, or more frequently in some patients depending on the evolution of post-chemotherapy laboratory parameters. All children included in this study were evaluated echocardiographically prior to the initiation of chemotherapy, subsequently a second evaluation was performed at the end of intensive treatment. It should be noted that the exact time interval between assessments varied from patient to patient, as some patients had some treatment delays during the chemotherapy protocol.
The 2009 ALL-IC BFM protocol consists of induction treatment with Epirubicin 30 mg/m2 on days 8, 15, 22 and 29; vincristine 1.5 mg/m2 on days 8, 15, 22 and 29; asparaginase 5000 U/m2 on days 12, 15, 18, 21, 24, 27, 30 and 33 and intrathecal methotrexate on days 1, 12 and 33. In the second part of induction, cyclophosphamide 1000 mg/m2 is administered on days 36 and 64 and cytarabine 75 mg/m2 4 cycles of 4 consecutive days and 6-mercaptopurine 60 mg/m2 28 days (days 36-63) and intrathecal methotrexate on days 45 and 59. Then consolidation treatment consisted of four cycles of high-dose methotrexate 3-5 g/m2 every 2 weeks and 6-mercaptopurine 25 mg/m2 56 days. Reinduction treatment included Epirubicin 30 mg/m2 on days 8, 15, 22 and 29; vincristine 1.5 mg/m2 on days 8, 15, 22 and 29; asparaginase 10000 U/m2 on days 8, 11, 15, 18 and in the second part cyclophosphamide 1000 mg/m2 on day 36, cytarabine 75 mg/m2, 2 cycles of 4 consecutive days, thioguanine 60 mg/m2 (14 days, days 36-63) and intrathecal methotrexate on days 38 and 45.
Maintenance treatment included oral administration of 6-mercaptopurine (6-MP) tablets and methotrexate.
3. Results
The population included in the study presented a mean age of 8.63 ± 5.69 standard deviations (SD). Male patients accounted for the largest group in our study population, representing 62%. Most of the patients enrolled in the study (66.66%) came from the rural environment. The baseline characteristics are showed in Table 1.
The echocardiographic assessment after the first cycle of chemotherapy showed an impairment of the ejection fraction (EF) in 32% of cases, with a mean decrease of Teciholtz EF of 14% compared to the baseline assessment. At the end of the study, of the total number of patients whose systolic function was stable after the first chemotherapy cycle, 46% of them had an average 24% impairment of EF compared to the second echocardiographic evaluation. The comparative analysis of the evolution of systolic function according to the sex of the patients shows a balanced distribution between the sexes, thus 45% of the female patients, respectively 47% of the male patients registered an impairment of FE at the end of the study, with an overall 62% of patients being males and 38% females within the group that had an alteration of sistolic function. It should be noted that the older age at inclusion in the study is more frequently associated with a regression of EF, without reaching the threshold of statistical significance. In order to identify the prognostic power of the echocardiographic EF-T for an early impairment of systolic function after administration of chemotherapy, ROC and AUC analyse has been performed, highlighting a threshold of 68% for EF. Accordingly, patients having a baseline EF value superior to the threshold, a decrease was observed, on average by 16% compared to the initial assessment (14% -41%). The use of this cutoff allowed early identification (pre-chemotherapy echocardiography) of patients at risk of systolic damage secondary to chemotherapy run (baseline compared to first follow-up, first follow-up towards the end of the study).Each 2D ultrasound and speckle-tracking parameter was compared between the initial evaluation and the second evaluation, conducted after completion of chemotherapy/before maintenance treatment. There were no significant differences between the two parameters for most of the analyzed parameters (p>0.05). However, a slight decrease in LV EF (assessed in accordance with the modified Simpson method) was noted upon the second evaluation (62.21 ± 4.19 versus 59.27 ± 7.14, p=0.03). These results have been depicted in Table 2.
We further sought to identify possible correlations between cumulative doses of the three main chemotherapeutic classes administered to patients included in the study and the echocardiography and/or speckle-tracking parameter variation. A few important associations were identified. A significant correlation between E’ percentage variation and anthracycline cumulative dose, as well as antimetabolite agents was identified (p=0.03 in both cases). A trend in percentage decrease of E’ value variation can be visualized in both Figure 3 and Figure 4 in association with increase in cumulative dose of the aforementioned therapeutic agents.
In case of alkylating agents, a significant correlation between cumulative dose increase of alkylating agents administered and GLS variation (p<0.01, respectively). As visualized in Figure 5, the tendency of negative variation (the second value surpasses the baseline value) is the highest in relation to the cumulative dose increase. Therefore, an increase in GLS is dependent on the ascending trend of cumulative dose of alkylating agents administered.
4. Discussion
Cardiac activity that generates efficient cardiac output at a low pressure filling level depends on ventricular systolic and diastolic function [16,22]. According to consensus statements from American Society of Echocardiography (ASE) and the European Association of cardiovascular Imaging (EACVI) cardiac dysfunction is defined as a decrease in the LVEF of more than 10% to a value [16]. The EF parameter is considered an echocardiographic standard for measuring myocardial dysfunction, implying some disadvantages related to the lack of detection of segmental dysfunctions with preserved contractility, the difficulty of assessing the LV apex and the inherent variability of the measurements [23,24,25]. Microstructural changes due to the type and dose of cytostatics will lead to necrosis or cell apoptosis and eventually to irreversible myocyte remodeling processes. We tried to identify some prognostic factors for the evolution of systolic function estimated as EF, testing a large number of correlations between various parameters and the evolution of EF. In our study LVEF at the end of the first cytostatic treatment was identified an impairment in 32% of cases, with a mean decrease of Teciholtz EF of 14% compared to the baseline assessment. It is known that EF can be influenced in these patients not only by the cytostatic treatment but also by adjacent conditions (severe infections or hyperhydration). Also LVEF (assessed in accordance with the modified Simpson method) was noted upon the second evaluation (62.21 ± 4.19 versus 59.27 ± 7.14, p=0.03-tabel 1). LVEF remains an indicator of dysfunction at asymptomatic left ventricular sistolic dysfunction in child cancer survivors but the measurement was performed with volumetric methods 3D. [26] Our values of LVEF were in agreement with those in the study conducted by Ardelean A. et al. where they showed mean values of LVEF of of 62.1 ± 5.5% for the patients receiving Doxorubicin treatment and 64.7 ± 5.9% for those treated with Epirubicin. [27]
The role of sex in the development of anthracycline cardiotoxicity in the pediatric population is yet to be studied.[28] There are some studies for oncologic pediatric population that have reported that female are at risk for developing cardiac atrophy, as measured by a decrease in left ventricular mass, and subsequent HF.[29,30] In their study Rosas Diaz et al. assessed the role of sex on incident heart failure in a large cohort of adult patients treated with anthracyclines and thei concluded that female sex was not associated with higher risk for heart failure in adult patients treated with anthracyclines [31]. In our study, the comparative analysis of the evolution of systolic function according to the sex of the patients shows a balanced distribution between the sexes, thus 45% of the female patients, respectively 47% of the male patients registered an impairment of FE at the end of the study.
Speckle-tracking echocardiography has been therefore proposed for assessment of subclinical myocardial dysfunction in children, mainly through evaluation of GLS and cumulative anthracyclines dose is an risk factor for early-onset or late-onset cardiotoxicity [32], but this parameter can be dependent on both pre-load and after-load [33,34]. There are however studies in the literature who support the use of myocardial work indices for assessment of early changes of cardiac dysfunction, which might even predict changes in GLS [35]. According to Suter and Ewer there are two types of cardiac toxicity: type I cardiotoxicity is an irreversible process, characterized by cellular loss, whereas type II involves a reversible, temporary dysfunction, caused by mitochondrial and protein alteration [8]. Studies in the literature have shown that exposure to toxic aggression induced by chemotherapeutic agents increases myocardial vulnerability, and the risk of developing irreversible lesions that can lead to cardiomyopathy is high [25,36,37]. In children as in adults, anthracyclines represent the drug class most commonly linked to cardiac damage [38,39]. Cumulative doses ranged in the our group of children analyzed was 120 mg/m², the low compared to average doses described in a review that can reach up to 375 mg/m² and we obtained a significant correlation between E’ percentage variation and anthracycline cumulative dose (Figure 2) [32]. As risk factors other than increased cumulative doses of anthracyclines include female sex (male patients accounted for the largest group in our study population, their prevalence being 62%), younger age at diagnosis (in our study a mean age was 8.6 years (±5.08years) and trisomy 21.
The toxic cardiac effects seem to be more augmented after long periods of therapy completion [40]. A study conducted at a mean period of 5 years after termination of chemotherapy proved that cancer survivors can exhibit changes in left ventricular strain, in spite of normal left ventricular function parameters, as identified during conventional echocardiography [41]. However, subclinical changes in cardiac function in children seem to vary greatly among various studies, but do not correlate with altered cardiovascular endurance tests [39,42]. Still, diastolic dysfunction seems to be common after anthracycline-based regimens and to precede systolic dysfunction [43]. In children with tachycardia, the pseudorestrictive appearance (E / A> 2) may occur due to fast relaxation with consequent shortening of filling time. Regarding the TDI, the relaxation of the LV is not influenced by the loading conditions or the geometry of the analyzed structure. The “E/Ea” ratio reflects the degree of compliance of the LV, corroborated with other parameters
Septal E/E’ ratio has been commonly regarded as an early, predictive marker of diastolic impairment, with an increase dependent upon the cumulative anthracycline dose used in 10-year survivors of childhood malignancies [44]. E/A ratio was also related to diastolic dysfunction in a pediatric study designed during a 5-year follow-up in children who had undergone chemotherapy [45]. Our results show that no significant associations in terms of E/E’ or E/A ratios were found (Figure 5 and Figure 6).
Similar findings were obtained by conducting the same analysis on antimetabolites, which are also known as potential cardiotoxic drugs, but there are no clear guidelines regarding supervision in patients who benefit from this particular medication [46].
Alkylating agents can also cause dose-dependent cardiotoxicity, through mostly unknown mechanisms, but assumingly through a significant inhibition of DNA transcription and, consequently, dampening of protein production [47,48]. The relatively lower doses administered in children might explain the lower incidence of cardiac side effects in children as opposed to adults [49]. These drugs also negatively impact systolic function, mainly the left ventricular EF, as well as diastolic heart failure, as regarded in adults patients treated with cisplatin [50]. This therapeutic class represented another point of interest in our study, and we detected significant changes in systolic markers, GLS in relation to cumulative dose administered (Figure 4).
We did not identify however significant mean changes in in baseline GLS and after its finalization, as opposed to other studies which have reported significant increase in baseline GLS percentage [51]. Several cut-off percentual changes have been proposed as markers of significant left ventricle impairment, but studies are still ongoing [52]. Through the current study, we tried to identify ultrasound traits of myocardial dysfunction in children undergoing various types of cytostatic therapeutic protocols, by assessing parameters suggestive of both systolic and diastolic function. The addition of speckle-tracking to conventional echocardiography represented a strength of the current study, as myocardial deformation parameters have been regarded as potential indicators of early cardiac injury [19]. The cardiotoxicity of anthracyclines is studied and proven by numerous studies. Understanding its mechanisms and early identification of cardiac dysfunction (subclinical) is beneficial for improving cardioprotective treatment. Cardioprotection methods based on the early echocardiographic determination of systolic dysfunction are being studied [53,54]. Therefore, a multidisciplinary approach involving pediatric cardiologists and oncologists, in a novel pediatric cardio-oncology field could positively impact the morbidity and mortality prognosis of pediatric patients with oncological pathology [55].
4.1. Limitations of Our Study
Despite the potential merits of this study, several limitations must be acknowledged. This study has involved a small study population. That could be explained due to unicentric study, conducted for a short follow-up period and the inclusion of only pediatric patients with acute leukemia. We did not choose to include a variety of cancer types and chemotherapy protocols because we wanted to avoid a heterogeneity of the cohort and selection bias. Another limitation is that our study does not include a correlation with cardiac biomarkers. Our aim was to emphasized the importance of the early determination of myocardial injury through noninvasive multimodal echocardiographic evaluation. These limitations might explain the abundance of insignificant results obtained.
An evaluation at a longer timespan and an expansion of the study on a larger population might pave the way towards a better understanding of long-term cardiac consequences of chemotherapeutic agents.
5. Conclusions
Speckle-tracking echocardiography has been regarded as a imagistic tool which aids precocious recognition of cardiac dysfunction in subjects who had benefitted from cytostatic treatment, with most studies focusing on long-term side effects of anthracyclines. In our study, we failed to identify significant differences from baseline values in mean ultrasound and speckle-tracking-derived parameters, assessed after treatment completion. A clearer picture of the cardiotoxic effects could be provided by expanding the research on larger populations and performing recurrent imagistic follow-ups on the long-term.
Author Contributions
Conceptualization, AF and MC; methodology, AF and MC; validation AF; formal analysis MS.; investigation, AF, ACP, SGR, LG and DT.; writing—original draft preparation AF, MS; writing—review and editing, AF, MS.; visualization, AF; supervision, AF and MC.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki,).and approved by the the Ethics Committee of the George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu Mureș (Institutional Review Board number 33/01.03.2019
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The raw data presented in this study can be obtained upon reasonable request addressed to Amalia Făgărășan amalia_fagarasan@yahoo.com.
Acknowledgments
Adrienne Horvath, Iarca Ionut, Andrea Fodor for administrative and technical support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Coza DD, Bucurenci DM. ANALIZA CAZUISTICII REGISTRULUI NATIONAL AL CANCERELOR LA COPIL IN ROMANIA 2010-2017 n.d.:19.
- Cancer in Children and Adolescents—NCI 2021. https://www.cancer.gov/types/childhood-cancers/child-adolescent-cancers-fact-sheet (accessed July 9, 2022).
- Saletta F, Seng MS, Lau LMS. Advances in paediatric cancer treatment. Transl Pediatr 2014;3:156–82. [CrossRef]
- Ruggiero A, Rizzo D, Catalano M, Coccia P, Triarico S, Attiná G. Acute chemotherapy-induced nausea and vomiting in children with cancer: Still waiting for a common consensus on treatment. J Int Med Res 2018;46:2149–56. [CrossRef]
- Ehrhardt MJ, Skinner R, Castellino SM. Renal and Hepatic Health After Childhood Cancer. Pediatr Clin North Am 2020;67:1203–17. [CrossRef]
- Ruggiero A, Skinner R, Khaled Zekri WZ. Editorial: Adverse and Toxic Effects of Childhood Cancer Treatments. Front Oncol 2021;11:795664. [CrossRef]
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J 2016;37:2768–801. [CrossRef]
- Suter TM, Ewer MS. Cancer drugs and the heart: importance and management. Eur Heart J 2013;34:1102–11. [CrossRef]
- Murabito A, Hirsch E, Ghigo A. Mechanisms of Anthracycline-Induced Cardiotoxicity: Is Mitochondrial Dysfunction the Answer? Front Cardiovasc Med 2020;7:35. [CrossRef]
- Manrique CR, Park M, Tiwari N, Plana JC, Garcia MJ. Diagnostic Strategies for Early Recognition of Cancer Therapeutics–Related Cardiac Dysfunction. Clin Med Insights Cardiol 2017;11:1179546817697983. [CrossRef]
- Oechsle K, Bokemeyer C. Kardiotoxizitäten bei Chemo- und Radiotherapie. Onkol 2009;15:157–62. [CrossRef]
- Ammon M, Arenja N, Leibundgut G, Buechel RR, Kuster GM, Kaufmann BA, et al. Cardiovascular management of cancer patients with chemotherapy-associated left ventricular systolic dysfunction in real-world clinical practice. J Card Fail 2013;19:629–34. [CrossRef]
- Germanakis I, Anagnostatou N, Kalmanti M. Troponins and natriuretic peptides in the monitoring of anthracycline cardiotoxicity. Pediatr Blood Cancer 2008;51:327–33. [CrossRef]
- Schlitt A, Jordan K, Vordermark D, Schwamborn J, Langer T, Thomssen C. Cardiotoxicity and Oncological Treatments. Dtsch Ärztebl Int 2014;111:161–8. [CrossRef]
- Cardinale D, Sandri MT, Martinoni A, Tricca A, Civelli M, Lamantia G, et al. Left ventricular dysfunction predicted by early troponin I release after high-dose chemotherapy. J Am Coll Cardiol 2000;36:517–22. [CrossRef]
- Plana JC, Galderisi M, Barac A, Ewer MS, Ky B, Scherrer-Crosbie M, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr 2014;27:911–39. [CrossRef]
- Lipshultz SE, Adams MJ. Cardiotoxicity after childhood cancer: beginning with the end in mind. J Clin Oncol Off J Am Soc Clin Oncol 2010;28:1276–81. [CrossRef]
- Mulrooney DA, Yeazel MW, Kawashima T, Mertens AC, Mitby P, Stovall M, et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ 2009;339:b4606. [CrossRef]
- Li VW-Y, So EK-F, Wong WH-S, Cheung Y-F. Myocardial Deformation Imaging by Speckle-Tracking Echocardiography for Assessment of Cardiotoxicity in Children during and after Chemotherapy: A Systematic Review and Meta-Analysis. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr 2022;35:629–56. [CrossRef]
- Lopez L, Colan SD, Frommelt PC, Ensing GJ, Kendall K, Younoszai AK, et al. Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr 2010;23:465–95; quiz 576–7. [CrossRef]
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016;18:891–975. [CrossRef]
- Thavendiranathan P, Grant AD, Negishi T, Plana JC, Popović ZB, Marwick TH. Reproducibility of echocardiographic techniques for sequential assessment of left ventricular ejection fraction and volumes: application to patients undergoing cancer chemotherapy. J Am Coll Cardiol 2013;61:77–84. [CrossRef]
- Otterstad JE, Froeland G, St John Sutton M, Holme I. Accuracy and reproducibility of biplane two-dimensional echocardiographic measurements of left ventricular dimensions and function. Eur Heart J 1997;18:507–13. [CrossRef]
- Yoldaş T, Yeşil Ş, Karademir S, Şahin G, Arman Örün U, Doğan V, et al. Evaluation of long-term cardiac side effects of anthracycline chemotherapy by conventional and non-conventional echocardiographic methods in childhood cancer survivors. Cardiol Young 2019;29:904–9. [CrossRef]
- López-Fernández T, Martín García A, Santaballa Beltrán A, Montero Luis Á, García Sanz R, Mazón Ramos P, et al. Cardio-Onco-Hematology in Clinical Practice. Position Paper and Recommendations. Rev Espanola Cardiol Engl Ed 2017;70:474–86. [CrossRef]
- Merkx R, Leerink JM, De Baat EC, Feijen EAM, Kok WEM, Mavinkurve-Groothuis AMC, et al. Asymptomatic systolic dysfunction on contemporary echocardiography in anthracycline-treated long-term childhood cancer survivors: a systematic review. J Cancer Surviv 2022;16:338–52. [CrossRef]
- Ardelean AM, Olariu IC, Isac R, Jurac R, Stolojanu C, Murariu M, et al. Correlation of Speckle-Tracking Echocardiography with Traditional Biomarkers in Predicting Cardiotoxicity among Pediatric Hemato-Oncology Patients: A Comprehensive Evaluation of Anthracycline Dosages and Treatment Protocols. Children 2023;10:1479. [CrossRef]
- Sex-Specific Cardiovascular Risks of Cancer and Its Therapies | Circulation Research n.d. https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.319901 (accessed January 13, 2024).
- Female Sex and Higher Drug Dose as Risk Factors for Late Cardiotoxic Effects of Doxorubicin Therapy for Childhood Cancer | NEJM n.d. https://www.nejm.org/doi/full/10.1056/NEJM199506293322602 (accessed January 13, 2024).
- Congestive Heart Failure After Treatment for Wilms’ Tumor: A Report From the National Wilms’ Tumor Study Group | Journal of Clinical Oncology n.d. https://ascopubs.org/doi/10.1200/JCO.2001.19.7.1926 (accessed January 13, 2024).
- Diaz ANR, Hurtado GP, Manzano AAA, Keyes MJ, Turissini C, Choudhary A, et al. Sex Differences in the Development of Anthracycline-Associated Heart Failure. J Card Fail 2023;0. [CrossRef]
- Kouwenberg TW, Van Dalen EC, Feijen EAM, Netea SA, Bolier M, Slieker MG, et al. Acute and early-onset cardiotoxicity in children and adolescents with cancer: a systematic review. BMC Cancer 2023;23:866. [CrossRef]
- Gherbesi E, Bergamaschi L, Cusmano I, Tien TT, Paolisso P, Foà A, et al. The usefulness of speckle tracking echocardiography in identifying subclinical myocardial dysfunction in young adults recovered from mild COVID-19. Echocardiogr Mt Kisco N 2022. [CrossRef]
- Cui C, Zheng Q, Li Y, Huang D, Hu Y, Wang Y, et al. Reference Values of Noninvasive Myocardial Work Indices Measured by Echocardiography in Healthy Children. Front Pediatr 2022;10:792526. [CrossRef]
- Zhan J, Van den Eynde J, Cordrey K, Long R, Danford DA, Hays AG, et al. Deterioration in myocardial work indices precedes changes in global longitudinal strain following anthracycline chemotherapy. Int J Cardiol 2022;363:171–8. [CrossRef]
- Adams MJ, Lipshultz SE. Pathophysiology of anthracycline- and radiation-associated cardiomyopathies: implications for screening and prevention. Pediatr Blood Cancer 2005;44:600–6. [CrossRef]
- Armenian SH, Hudson MM, Mulder RL, Chen MH, Constine LS, Dwyer M, et al. Recommendations for cardiomyopathy surveillance for survivors of childhood cancer: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol 2015;16:e123-136. [CrossRef]
- Bansal N, Blanco JG, Sharma UC, Pokharel S, Shisler S, Lipshultz SE. Cardiovascular diseases in survivors of childhood cancer. Cancer Metastasis Rev 2020;39:55–68. [CrossRef]
- Fulbright JM. Review of Cardiotoxicity in Pediatric Cancer Patients: During and after Therapy. Cardiol Res Pract 2011;2011:942090. [CrossRef]
- van der Pal HJ, van Dalen EC, Hauptmann M, Kok WE, Caron HN, van den Bos C, et al. Cardiac function in 5-year survivors of childhood cancer: a long-term follow-up study. Arch Intern Med 2010;170:1247–55. [CrossRef]
- Amedro P, Vincenti M, Abassi H, Lanot N, De La Villeon G, Guillaumont S, et al. Use of speckle tracking echocardiography to detect late anthracycline-induced cardiotoxicity in childhood cancer: A prospective controlled cross-sectional study. Int J Cardiol 2022;354:75–83. [CrossRef]
- De Caro E, Smeraldi A, Trocchio G, Calevo M, Hanau G, Pongiglione G. Subclinical cardiac dysfunction and exercise performance in childhood cancer survivors. Pediatr Blood Cancer 2011;56:122–6. [CrossRef]
- Serrano JM, González I, Del Castillo S, Muñiz J, Morales LJ, Moreno F, et al. Diastolic Dysfunction Following Anthracycline-Based Chemotherapy in Breast Cancer Patients: Incidence and Predictors. The Oncologist 2015;20:864–72. [CrossRef]
- Wolf CM, Reiner B, Kühn A, Hager A, Müller J, Meierhofer C, et al. Subclinical Cardiac Dysfunction in Childhood Cancer Survivors on 10-Years Follow-Up Correlates With Cumulative Anthracycline Dose and Is Best Detected by Cardiopulmonary Exercise Testing, Circulating Serum Biomarker, Speckle Tracking Echocardiography, and Tissue Doppler Imaging. Front Pediatr 2020;8:123. [CrossRef]
- Velensek V, Mazic U, Krzisnik C, Demšar D, Jazbec J, Jereb B. Cardiac damage after treatment of childhood cancer: A long-term follow-up. BMC Cancer 2008;8:141. [CrossRef]
- Stone JR, Kanneganti R, Abbasi M, Akhtari M. Monitoring for Chemotherapy-Related Cardiotoxicity in the Form of Left Ventricular Systolic Dysfunction: A Review of Current Recommendations. JCO Oncol Pract 2021;17:228–36. [CrossRef]
- Perez IE, Taveras Alam S, Hernandez GA, Sancassani R. Cancer Therapy-Related Cardiac Dysfunction: An Overview for the Clinician. Clin Med Insights Cardiol 2019;13:1179546819866445. [CrossRef]
- Gershwin ME, Goetzl EJ, Steinberg AD. Cyclophosphamide: use in practice. Ann Intern Med 1974;80:531–40. [CrossRef]
- Simbre VC, Duffy SA, Dadlani GH, Miller TL, Lipshultz SE. Cardiotoxicity of cancer chemotherapy: implications for children. Paediatr Drugs 2005;7:187–202. [CrossRef]
- Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation 2013;128:1927–95. [CrossRef]
- Alam S, Chandra S, Saran M, Chaudhary G, Sharma A, Bhandhari M, et al. To study the usefulness and comparison of myocardial strain imaging by 2D and 3D echocardiography for early detection of cardiotoxicity in patients undergoing cardiotoxic chemotherapy. Indian Heart J 2019;71:468–75. [CrossRef]
- Onishi T, Fukuda Y, Miyazaki S, Yamada H, Tanaka H, Sakamoto J, et al. Practical guidance for echocardiography for cancer therapeutics-related cardiac dysfunction. J Echocardiogr 2021;19:1–20. [CrossRef]
- Guimarães LC, Fidale TM, Pereira TCR, Lopes PR, Ferreira-Junior MD, Deconte SR, et al. Cardioprotective Effects of Leucine Supplementation against Doxorubicin-Induced Cardiotoxicit. Cardiovasc Toxicol 2024. [CrossRef]
- Armenian SH, Hudson MM, Lindenfeld L, Chen S, Chow EJ, Colan S, et al. Effect of carvedilol versus placebo on cardiac function in anthracycline-exposed survivors of childhood cancer (PREVENT-HF): a randomised, controlled, phase 2b trial. Lancet Oncol 2024:S1470-2045(23)00637-X. [CrossRef]
- Rose-Felker K, Effinger K, Kelleman MS, Sachdeva R, Meacham LR, Border WL. Improving paediatric cardiologists’ awareness about the needs of childhood cancer survivors: results of a single-centre directed educational initiative. Cardiol Young 2019;29:808–12. [CrossRef]
Figure 2.
Echocardiographic global longitudinal strain assessment. HR: heart rate, Avg: average EDV: end-diastolic volume, ESV: end-systolic volume, EF: ejection fraction, SD: standard deviation, AP3: apical-3-chambers view, AP4: apical-4-chambers view, AP2: apical-2-chambers view, L: longitudinal.
Figure 2.
Echocardiographic global longitudinal strain assessment. HR: heart rate, Avg: average EDV: end-diastolic volume, ESV: end-systolic volume, EF: ejection fraction, SD: standard deviation, AP3: apical-3-chambers view, AP4: apical-4-chambers view, AP2: apical-2-chambers view, L: longitudinal.
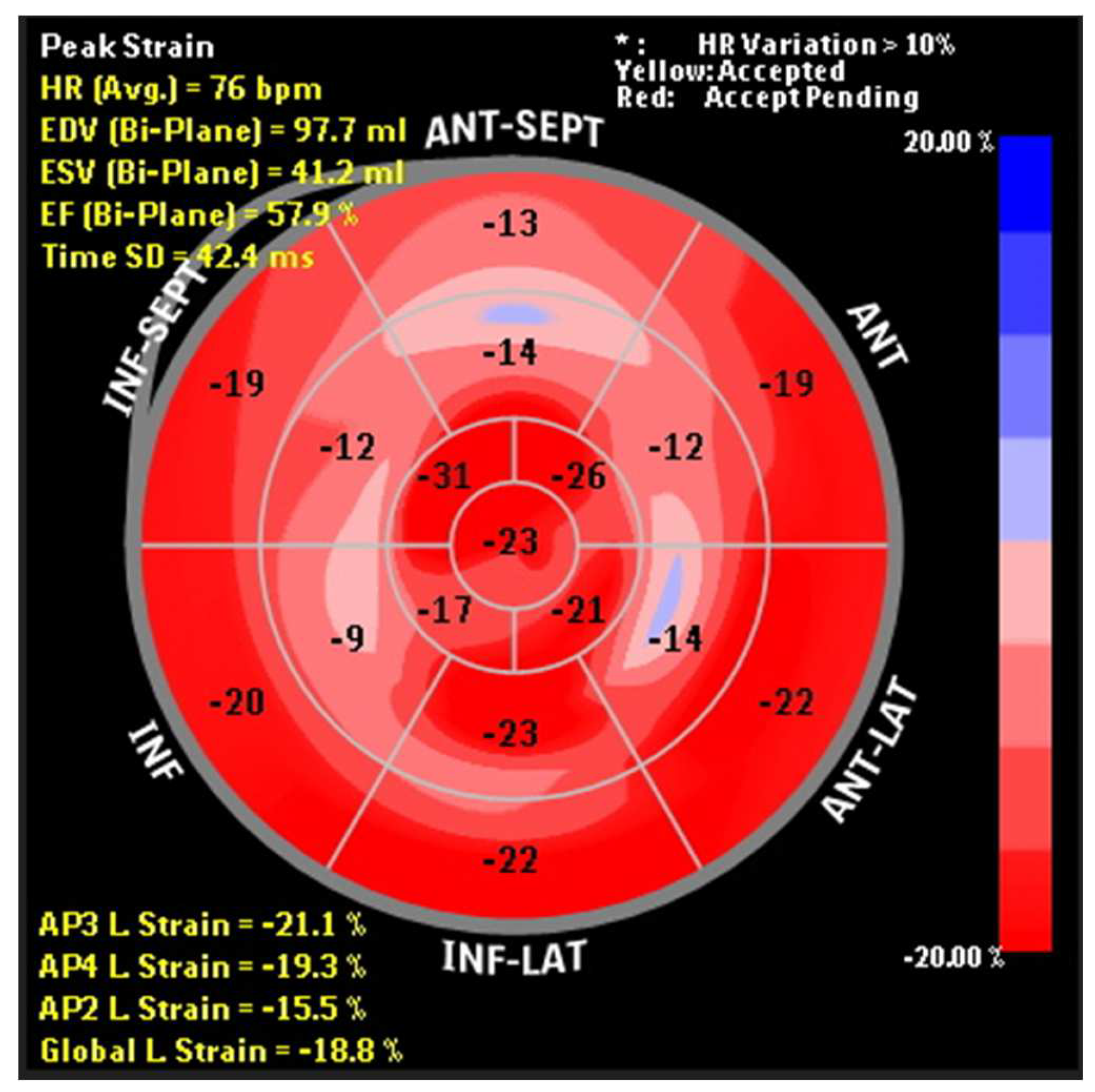
Figure 3.
Linear regression correlation between anthracycline cumulative dose administered and E’ value percentage variation.
Figure 3.
Linear regression correlation between anthracycline cumulative dose administered and E’ value percentage variation.
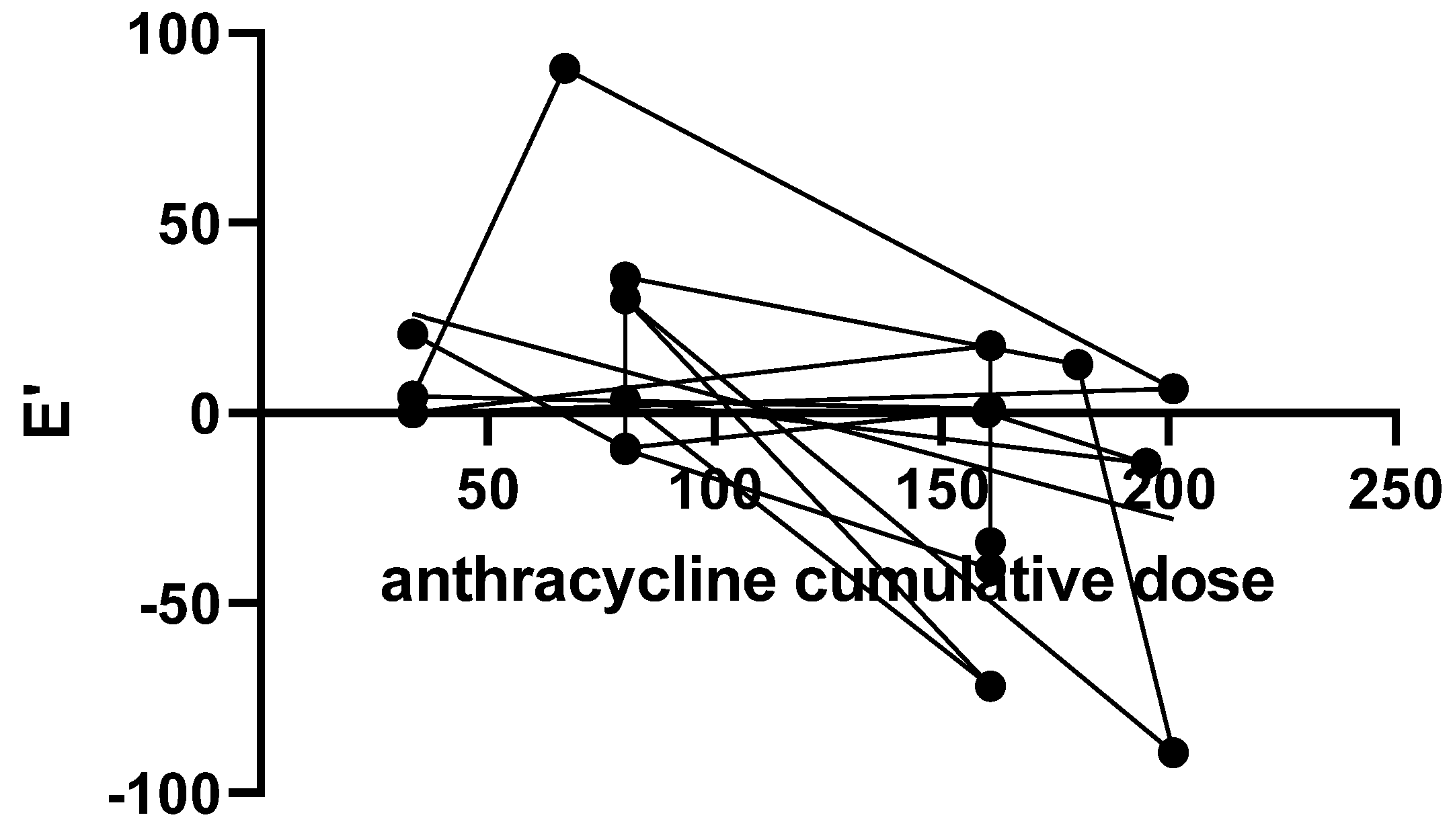
Figure 4.
Linear regression correlation between antimetabolite cumulative dose administered and E’ value percentage variation.
Figure 4.
Linear regression correlation between antimetabolite cumulative dose administered and E’ value percentage variation.
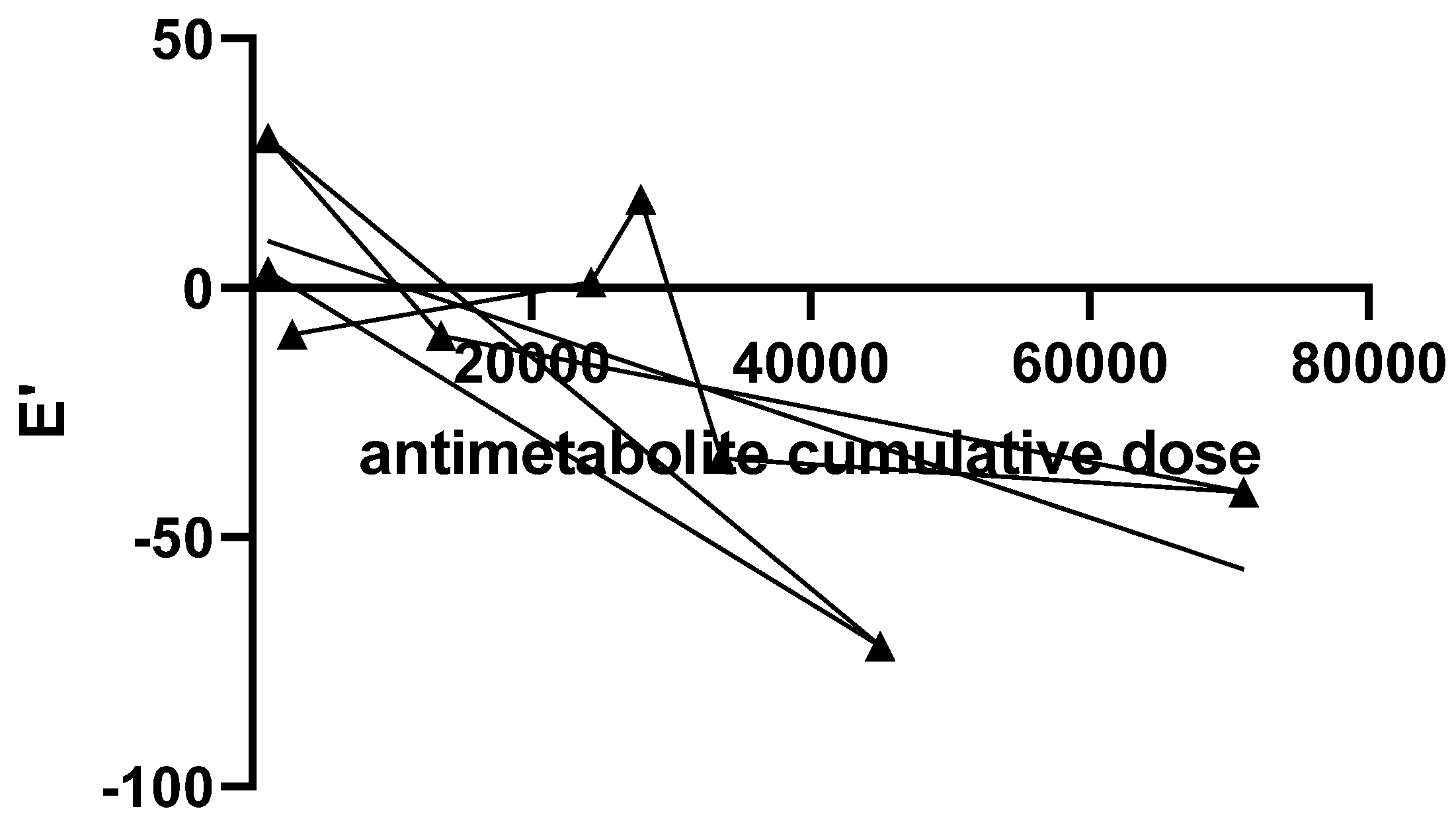
Figure 5.
Linear regression correlation between alkylating agents cumulative dose administered and GLS value percentage variation.
Figure 5.
Linear regression correlation between alkylating agents cumulative dose administered and GLS value percentage variation.
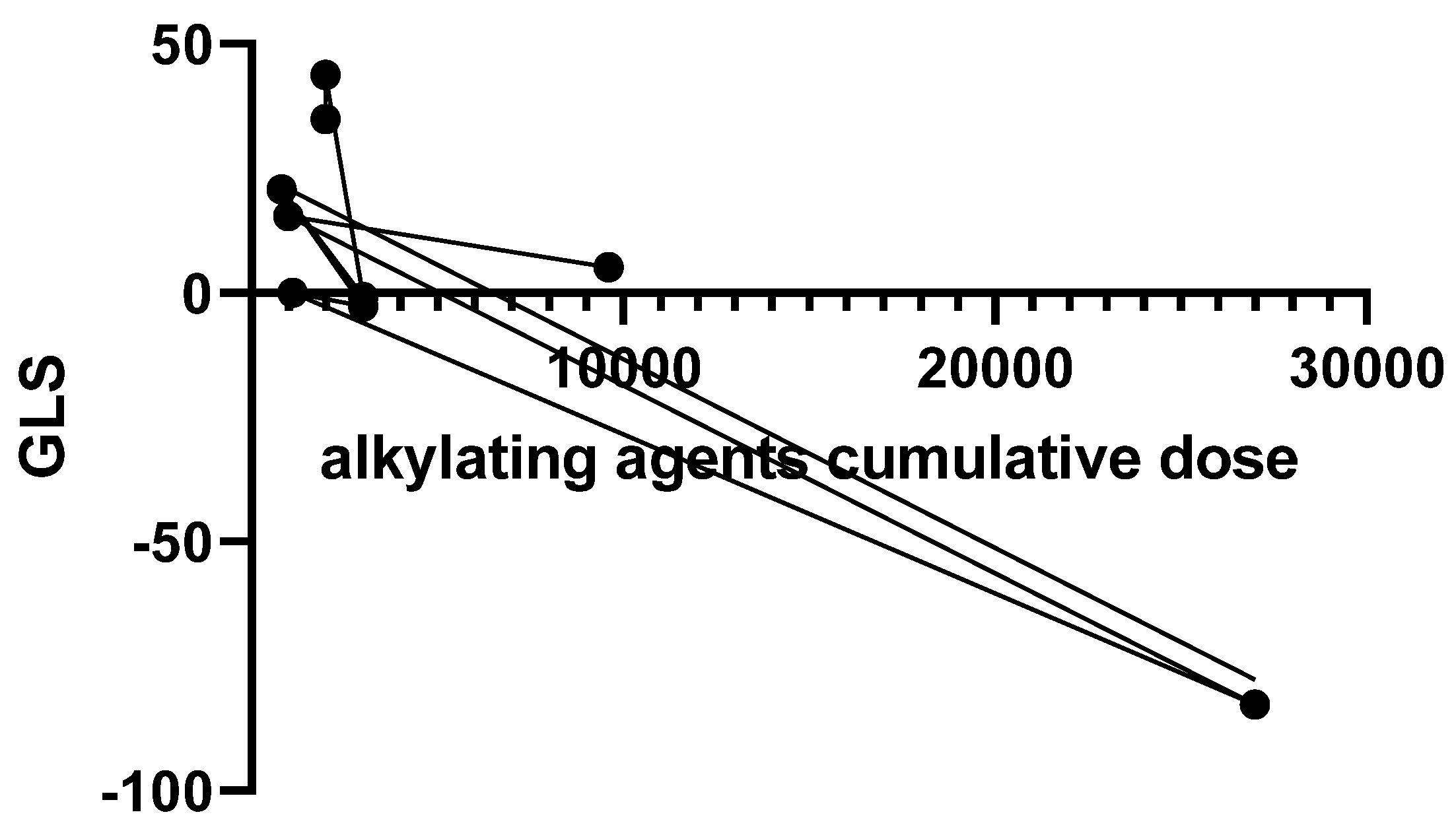
Figure 6.
Analytical statistics, diastolic function, there is no correlation between chemotherapeutic agent classes and E/E’.
Figure 6.
Analytical statistics, diastolic function, there is no correlation between chemotherapeutic agent classes and E/E’.
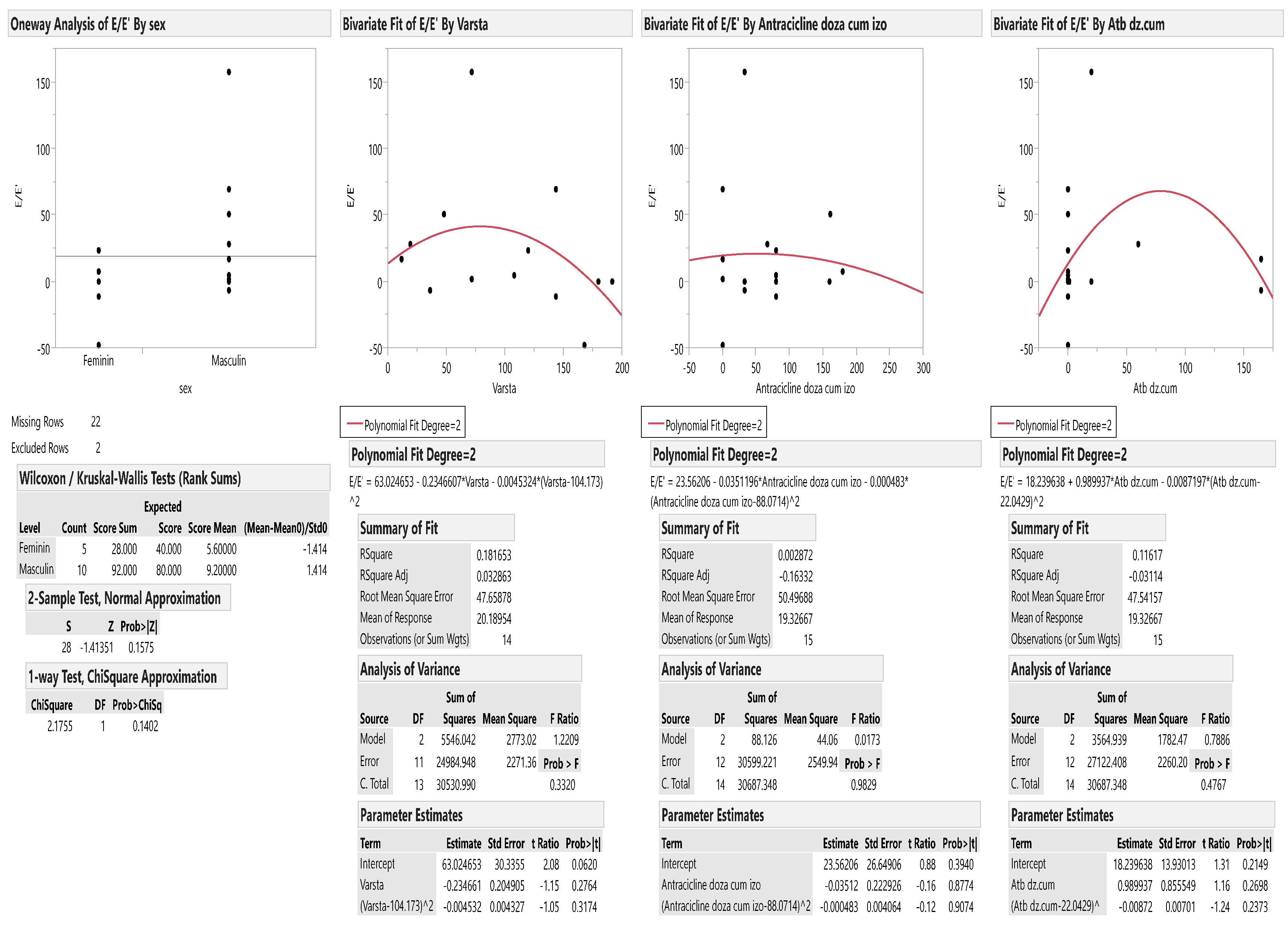
Figure 7.
Analytical statistics, diastolic function, there is no correlation between the restrictive diastolic after the first chemotherapy treatment and the cumulative doses of chemotherapy.
Figure 7.
Analytical statistics, diastolic function, there is no correlation between the restrictive diastolic after the first chemotherapy treatment and the cumulative doses of chemotherapy.
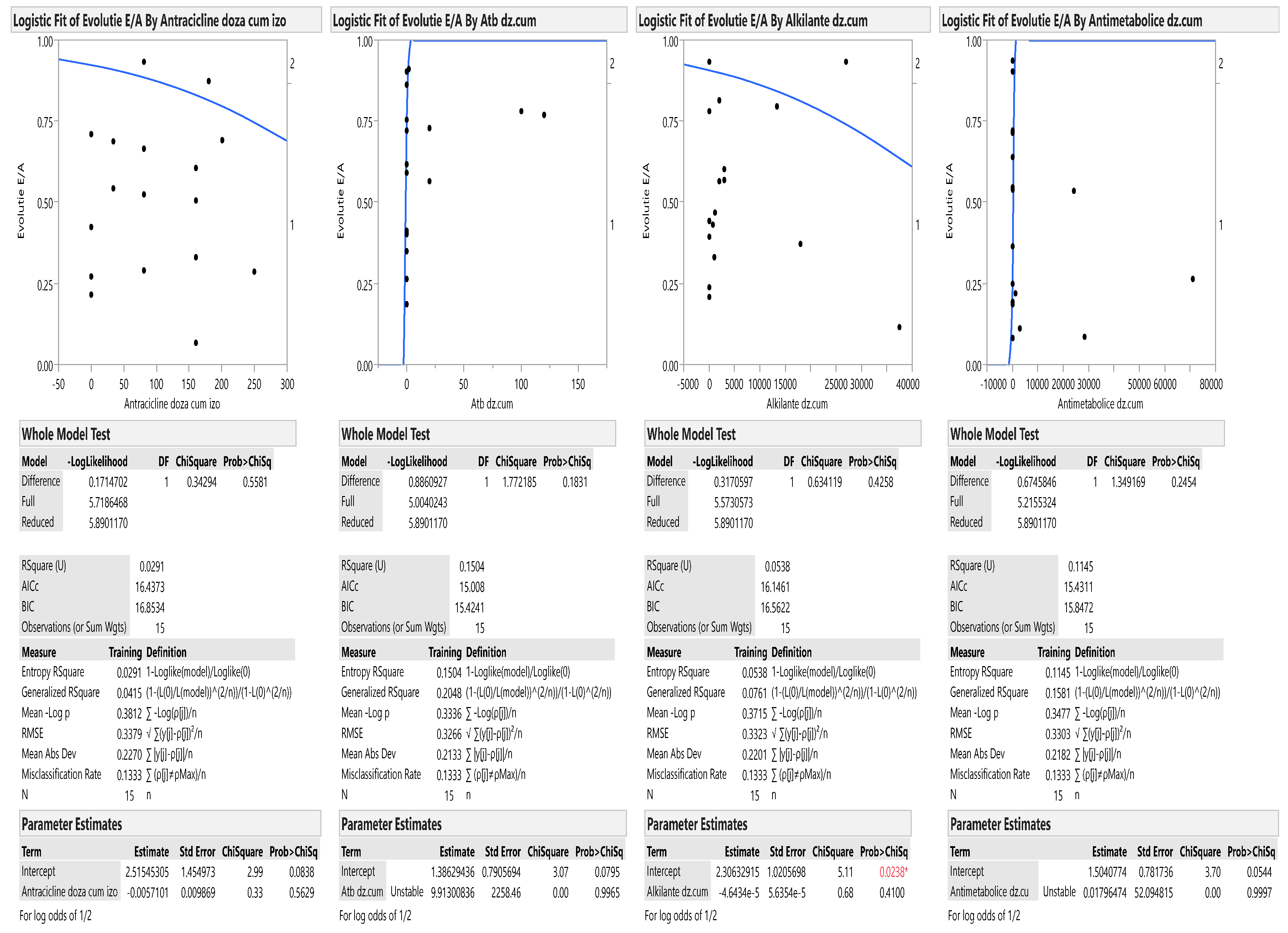

Table 1.
Baseline characteristics.
| Patients included (n = 29) |
|
|---|---|
| Age (years) | 8.63 [1,16] |
| Gender (male) | 18 (62%) |
| Body Surface Area (m2) | 1.04 [0.46,1.81] |
| Saturation of oxygen (%) | 98 [98,100] |
| Systolic blood pressure (mmHg) | 94 [84,110] |
| Diastolic blood pressure (mmHg) | 71 [53,82] |
| Heart rate (bpm) | 94 ± 9.20 |
| Cumulative anthracycline dose (mg/m²) | 120 |
| Follow-up time, years | 1 |
Table 2.
Comparison of cardiac ultrasound and speckle-tracking echocardiography parameters between the initial and second evaluation.
Table 2.
Comparison of cardiac ultrasound and speckle-tracking echocardiography parameters between the initial and second evaluation.
| Parameter | Initial evaluation (mean ± SD) |
Second evaluation (mean ± SD) |
P value |
| EF (Teichholz formula) | 61.56 ± 7.39 | 63.29 ± 7.31 | 0.87 |
| EF (modified Simpson method) |
62.21 ± 4.19 | 59.27 ± 7.14 | 0.03 |
| FS | 32.12 ± 5.90 | 29.99 ± 14.10 | 0.79 |
| GLS | -24.01 ± 5.61 | -22.87 ± 4.28 | 0.43 |
| GCS | -24.43 ± 4.47 | -25.23 ± 5.26 | 0.58 |
| AP2LS | -20.84 ± 11.14 | -21.88 ± 10.01 | 0.57 |
| AP3LS | -24.90 ± 5.59 | -23.37 ± 5.67 | 0.36 |
| AP4LS | -21.72 ± 11.76 | -21.87 ± 3.51 | 0.56 |
| MAPSE | 3.43 ± 4.51 | 2.83 ± 3.59 | 0.70 |
| TAPSE | 2.31 ± 1.47 | 1.95 ± 0.28 | 0.31 |
| S wave | 9.62 ± 2.09 | 8.98 ± 2.69 | 0.32 |
| E’ wave | 11.14 ± 3.47 | 10.80 ± 4.21 | 0.72 |
| A’ wave | 7.59 ± 2.03 | 8.17 ± 3.25 | 0.41 |
| E’/A’ | 1.52 ± 0.49 | 1.47 ± 0.69 | 0.36 |
| E/E’ | 7.29 ± 1.92 | 8.27 ± 3.20 | 0.23 |
| SAXA | -24.59 ± 10.36 | -27.08 ± 8.83 | 0.87 |
| SAXB | -23.41 ± 10.73 | -24.49 ± 5.66 | 0.65 |
| SAXM | -20.52 ± 14.88 | -23.05 ± 4.72 | 0.83 |
| E/A | 1.34 ± 0.17 | 1.47 ± 0.33 | 0.15 |
Legend: AP2LS- apical 2-chamber longitudinal strain; AP3LS- apical 3-chamber longitudinal strain; AP4LS- apical 4-chamber longitudinal strain; EF-ejection fraction, FS- fractional shortening, GCS- global circumferential strain, GLS- global longitudinal strain; SAXA-; SAXB- short-axis at the mitral valve plane; SAXM- short-axis view at the mid-ventricular papillary muscle level.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



