Submitted:
05 February 2024
Posted:
06 February 2024
You are already at the latest version
Abstract
Background: Diabetes mellitus (DM) and osteoporosis are two of the most widespread metabolic disease in the world. The aim of this study is to investigate the prevalence of DM among patients affected by osteoporosis and fragility fractures, and to search differences in clinical features. Methods: 713 patients belonging to CTO Bone Unit because of osteoporosis and fragility fractures were divided into two groups, according to the diagnosis of DM. The clinical and bone characteristics of patients were compared. Results: Prevalence of DM was 10.8%. When compared to patients without DM, the median age at the time of first fracture was similar (72 years ± 14 IQR vs 71 years ± 12 IQR); prevalence of combination of vertebral and hip fractures was higher (p=0.039), as well as prevalence of males, although not significantly (p=0.051). Bone mineral density (BMD) at all sites was higher in DM group; Trabecular Bone Score (TBS), instead, was significantly lower (p<0.001). Conclusions: Patients with fragility fractures and DM more frequently show combination of major fractures with higher BMD levels. In these patients, TBS could be a better indicator of bone health than BMD and therefore should be used as a diagnostic tool in clinical practice.
Keywords:
Osteoporosis
; diabetes mellitus
; fragility fractures
; Bone Mineral Density (BMD)
; Trabecular Bone Score (TBS)
; bone fragility
1. Introduction
Osteoporosis is a metabolic disease of bone tissue, very common in general population and even more in elderly [1]. This condition is characterized by decrease in bone mineral density (BMD) and degradation of the tissue microarchitecture, with progressive increase in the risk of fragility fractures [2]. The latter represent a serious health issue since they have heavy consequences from both health and social point of view [3]. Diabetes mellitus (DM) is another widespread metabolic disease [4], whose incidence is expected to grow quickly in the upcoming decades, due to the increase in average life expectancy and the epidemic diffusion of an unhealthy lifestyle [5]. In 2020, in Italy, prevalence of type 2 DM was around 5.9% (3.5 million people). Prevalence tends to grow with age, reaching 21% in the population over 75 years of age [6]. Chronic complications of DM affect most body tissues [7], and bone is no exception. It has been well described the existence of a complex crosstalk between glucose homeostasis and bone metabolism [8,9]. Both type 1 and type 2 DM, in fact, are recognised among the causes of secondary osteoporosis [10], leading to a reduced resistance to mechanical stress and to an increased risk of incurring fragility fractures [11,12,13,14,15]. Chronic hyperglycaemia, oxidative stress, accumulation of advanced glycation end products (AGEs) are some of the most relevant mechanisms that cause abnormalities of the bone’s micro and macro architecture and that lead to the alteration of the physiological bone turnover and trabecular network [16]. Chronic complications of DM, as well as neuropathy, retinopathy, poor balance, and sarcopenia, increase the risk of falls and consequent fractures [17,18]. The risk is greater with longer duration of DM and certain DM therapies [13,19]. DM-related bone fragility is also characterized by the presence of a diagnostic paradox: despite the increased risk of fracture, patients with type 2 DM often show a normal or even increased BMD [20] at all sites evaluated by execution of dual energy X-ray absorptiometry (DXA) scan [20,21], so osteoporosis may be often undiagnosed [22]. Instead, bone microarchitecture is altered in patients with DM; this parameter can be evaluated in the lumbar spine using Trabecular Bone Score Software (TBS), a measure of grey level texture performed on images obtained by DXA [23,24]. A deterioration of TBS represents a risk factor for developing fragility fractures independently of BMD levels [25], and in a recent meta-analysis a negative association between DM and TBS values was found [26]. Many studies have described the existence of relevant differences between BMD and TBS values in patients with and without DM. Do these differences remain clinically significant when we consider a selected population of patients who have already had fragility fractures? The purpose of the present study is to determinate prevalence and clinical characteristics of patients with DM in a population affected by fragility fractures and to evaluate whether BMD and TBS are significantly different between patients with and without DM even when only a population of patients who have already had fragility fractures is considered.
2. Materials and Methods
This is a single-centre retrospective, case-controlled study.
2.1. Case selection
We consulted the medical records of all consecutive patients affected by osteoporosis and fragility fractures attending the Bone Unit of the CTO Hospital of Rome between January 2010 and May 2023. Exclusion criteria were the presence of fractures due to causes not related to osteoporosis.
Patients were divided according to the presence of DM, for comparative analysis. The presence of DM was self-reported by patients during the first visit, confirmed and fully characterized by consulting the electronic medical record of the Diabetes Service. The diagnosis of DM was confirmed by the finding of HbA1c greater than or equal to 6,5% (47 mmol/mol) at least twice, or a fasting blood glucose greater than or equal to 126 mg/dl in two different occasions, or HbA1c greater than or equal to 6,5% (47 mmol/mol) plus fasting blood glucose greater than or equal to 126 mg/dl at the same time, inside the electronic medical record. Informed written consent was obtained for clinical data collection.
2.2. Data Collection
For all patients, data on age, sex, body mass index (BMI – kg/m2), age at time of the first fracture, site of fracture, smoking habit, presence of rheumatoid arthritis (RA) and chronic obstructive pulmonary disease (COPD), long-term cortisone therapy, family history of osteoporosis or fragility fractures, BMD measured in the lumbar spine, femoral neck and total hip, TBS were collected from medical records. Fragility fractures were catalogued as vertebral fractures, hip fractures, combination of vertebral and hip fractures and other non-vertebral or non-hip sites (clavicle, arm, elbow, pelvis, ankle, rib, tibia, foot, shoulder, knee).
For patients with DM, additional data were recorded: type of DM (type 1 or type 2), specific therapy. Information on DM chronic complications were available by the systematic screening of chronic complications recorded in the electronic medical record of the Diabetes Service and were reported as: peripheral neuropathy, retinopathy, nephropathy, coronary heart disease, carotid artery atheromasia and peripheral arterial disease. In addition, illness duration (years), glycated haemoglobin (HbA1c) (% - mmol/mol) at the time of the first visit at the Bone Unit were collected.
2.3. BMD assessment
BMD was assessed by skilled operators in our center by DXA [21] using an Hologic Discovery densitometer. In the lumbar scan, vertebrae that presented artefacts due to arthrosis or vertebral collapse were excluded from the BMD calculation. Daily phantom scans were performed for quality control prior to clinical activity. TBS iNsight Imaging Software was used to elaborate TBS from DXA scan of the spine. TBS >1,350 was considered indicative of normal microarchitecture, TBS between 1,350 and 1,200 indicated partially degraded microarchitecture, TBS < 1,200 was considered degraded microarchitecture [24]. Presence of vertebral fractures was ascertained by morphometric X-ray absorptiometry scan [27], executed with the same densitometer and by the same skilled operators.
2.4. Statistical analysis
Statistical analysis was performed using Jamovi Version 2.3.28 [28]. Continuous variables were described as median and interquartile range (IQR) and the Mann-Whitney U test were applied. Qualitative data were expressed as frequencies and compared by χ2-test. A p < 0.05 was considered significant. A linear multivariate regression was performed to find confounding factors. Odds ratio (OR) was calculated.
3. Results
Clinical records of 713 patients affected by fragility fractures were examined: median age was 81 ± 11 IQR years, with 27 (3.8%) patients being males. The median BMI was 23.7 ± 4.34 IQR kg/m2, median age at the time of the first fracture was 71 ± 12 IQR years. Median BMD at the lumbar spine was 0.771 ± 0.180 IQR g/cm2, median BMD at the femoral neck was 0.573 ± 0.112 IQR g/cm2, median BMD at the total hip was 0.713 ± 0.139 IQR g/cm2, median TBS was 1.240 ± 0.125 IQR. A family history of osteoporosis was reported by 199 (27.9%) patients, smoking habit by 130 (18.2%) and alcohol excess by 7 (1%). 29 (4.1%) patients were affected by RA, 44 (6.2%) patients by COPD and 40 (5.6%) were on long-term cortisone therapy. Regarding the site of fracture, 593 (83.2%) patients presented vertebral fractures, 36 (5%) hip fractures, 32 (4.5%) a combination of vertebral and hip fractures, 59 (8.3%) non-vertebral and non-hip fractures. Descriptive analysis are reported in Table 1.
In this population, 77 (10.8%) patients were affected by DM: 70 (90.9%) were Type 2 DM patients, the median duration of disease was 15 ± 10 IQR years, median HbA1c levels were 50 ± 12 IQR mmol/mol (6.8 ± 1.1 IQR %); 13% was on nutritional therapy, 58% on oral hypoglicemic drugs, 22% on insulin therapy, 7% on a combination of insulin and oral hypoglicemic drugs; regarding DM’s chronic complications, 19.5% had coronary heart disease, 39% carotid artery atheromasia or peripheral arterial disease, 19.5% peripheral neuropathy, 20.8% nephropathy and 10.4% retinopathy. DM patients’ specific characteristics are summarized in Table 2.
Bone and clinical characteristics of DM patients are compared with those of the 636 non-DM patients. The comparative analysis are shown in Table 3.
No significant differences were found in median age (p=0.221) and median age at the time of the first fracture (p=0.674). BMI and prevalence of males were higher in DM group (respectively p<0.001 and p=0.051)(Figure 1).
Similarly, smoking habit was found to be higher in DM patients (p = 0.030). Presence of a family history of osteoporosis and long-term cortisone therapy were significantly higher in subjects without DM (respectively p<0.001 and p=0.024). No significant differences were found in prevalence of alcohol excess, RA and COPD.
When analysing bone characteristics, patients with DM show much more frequently combination of major fractures, such as vertebral and hip fractures (p = 0.039, OR 2.44 (CI 95% [1.02; 5.86]) (Figure 2).
BMD values in DM patients were significantly higher at all the examined sites (lumbar spine p=0.002; femoral neck p=0.007; total hip p=0.031). On the contrary, the median TBS was significantly lower in DM population (p<0.001)(Figure 3).
To explore the influence of confounders on TBS, a linear multivariate regression was conducted: only BMI (p = 0.026) and DM (p<0.001) seem to predict significantly reduced TBS value; presence of COPD shows a less significant negative influence on TBS value (p=0.051); presence of smoking, alcohol excess, RA and long-term cortisone therapy did not show statistically significant results.
4. Discussion
Several studies in literature have highlighted a higher incidence of fragility fractures in patients with DM, compared to the general population [11,12,13,19,22,29], placing this disease among the causes of secondary osteoporosis [10]. Our analysis, carried out in a selected population of patients affected by fragility fractures due to severe osteoporosis belonging to a Bone Unit, revealed a prevalence of DM of only around 10%. Our results appear discordant with previous literature evidence. However we cannot conclude that DM patients are less than expected in a group of patients with fragility fracture because our data are retrospectively collected from a Bone Unit database, where the presence of DM is recorded only according to an anamnestic information.
We did not find statistical differences in median age at the time of the first fracture, so DM does not seem to cause an earlier development of bone fragility. A higher, although not significant, prevalence of males was found in the DM group: this result supports the evidence that men affected by DM may be exposed to a higher risk of developing bone fragility compared to those without DM [11,19]. Much more interesting data come from the bone structure analysis: the present research found that patients with DM have a higher risk to develop combination of vertebral and hip fractures, a condition that can lead to a worse clinical condition and more serious consequences for health.
As already reported in literature, this study found higher BMD levels in patients with DM and fragility fractures: this finding confirms that fractures tend to occur at higher BMD than in subjects without DM [17,20]. It is important to focus attention on this specific characteristic because it may lead to a delay in the diagnosis and treatment of osteoporosis. Due to the limited reliability of BMD in the diagnosis of osteoporosis in the DM population, the need for other diagnostic tools is emerging. Our study confirms that TBS, which evaluates bone microarchitecture, is significantly reduced in patients with DM, even compared to other patients with fragility fractures [23,26]. However, it must be considered that TBS can be influenced by numerous other factors, such as BMI, smoking, alcohol excess, chronic pathologies, and the use of certain drugs [30]. The analysis conducted on the available data highlighted that the presence of DM and BMI have a negative effect on the TBS value; a less significant negative influence was found for COPD; on the contrary, smoking habit, alcohol excess, RA and long-term cortisone therapy do not appear to influence the TBS value in a significant way in the studied population. This result deserves particular attention, in fact, Type 2 DM and high BMI are closely linked elements and affect a large part of the world population. As already highlighted in previous literature, both DM and high BMI have negative effects on bone metabolism, however showing non compromised densitometric values [31]. The use of TBS as a diagnostic tool for DM-related bone fragility could be a valid aid in the clinical setting. The appearance of fragility fractures in people affected by DM represents a particularly serious event. In fact, glycaemic control can worsen because of the stress related to trauma, surgery and medications. Furthermore, healing times in presence of DM are prolonged, along with the hospitalisation and incidence of infectious complications after surgery is higher [32]. Immobility after a fracture, leading to a reduction in physical activity and mood, can cause a poor adherence to specific therapies, with a further increase of insulin resistance. The patient may be exposed to a greater risk of developing other chronic complications of DM, such as major cardiovascular events and pressure ulcers [33], which can also lead to death. Considering these risks, it must be highlighted the fundamental need of making an early diagnosis of osteoporosis and preventing fragility fractures in this specific population.
5. Conclusions
According to our research, although with the described limits, the prevalence of DM in the fragility fracture population does not seems to be particularly high. The development of fragility fractures is not anticipated in patients with DM, but they have a higher risk to show combinations of major fractures, such as vertebral and hip fractures. The instrumental analysis confirms that BMD tends to be higher, while TBS significantly lower in DM individuals compared to non-DM ones, even when only fractured patients are taken into consideration. So, TBS should be considered to improve diagnostic strategies. The importance of an early diagnosis of osteoporosis and the prevention of fractures in patients with DM should be stressed and applied in everyday clinical practice, due to the heavy impact that fragility fractures may have on DM metabolic control and its progression towards chronic complications.
Author Contributions
Conceptualization, L.U. and I.N.; methodology, L.U.; software, S.WS.; validation, R.A., S.F. and Z.Z.; formal analysis, S.Z.; investigation, I.N.; resources, C.P.; data curation, L.G.; writing—original draft preparation, I.N.; writing—review and editing, L.U.; visualization, R.A.; supervision, L.U.; project administration, C.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nuti R, Brandi ML, Checchia G, Di Munno O, Dominguez L, Falaschi P, et al. Guidelines for the management of osteoporosis and fragility fractures. Intern Emerg Med 2019;14:85–102. [CrossRef]
- Johnston CB, Dagar M. Osteoporosis in Older Adults. Medical Clinics of North America 2020;104:873–84. [CrossRef]
- Piscitelli P, Neglia C, Feola M, Rizzo E, Argentiero A, Ascolese M, et al. Updated incidence and costs of hip fractures in elderly Italian population. Aging Clin Exp Res 2020;32:2587–93. [CrossRef]
- Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2022;65:1925–66. [CrossRef]
- Lovic D, Piperidou A, Zografou I, Grassos H, Pittaras A, Manolis A. The Growing Epidemic of Diabetes Mellitus. Curr Vasc Pharmacol 2020;18:104–9. [CrossRef]
- Ministero della Salute, Relazione al Parlamento 2021 sullo stato delle conoscenze e delle nuove acquisizioni in tema di diabete mellito - Legge 16 marzo 1987, n. 115, recante “Disposizioni per la prevenzione e la cura del diabete mellito” https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=3229. n.d.
- Dal Canto E, Ceriello A, Rydén L, Ferrini M, Hansen TB, Schnell O, et al. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol 2019;26:25–32. [CrossRef]
- Napoli N, Chandran M, Pierroz DD, Abrahamsen B, Schwartz A V., Ferrari SL. Mechanisms of diabetes mellitus-induced bone fragility. Nat Rev Endocrinol 2017;13:208–19. [CrossRef]
- Hofbauer LC, Busse B, Eastell R, Ferrari S, Frost M, Müller R, et al. Bone fragility in diabetes: novel concepts and clinical implications. Lancet Diabetes Endocrinol 2022;10:207–20. [CrossRef]
- Napoli N, Incalzi RA, De Gennaro G, Marcocci C, Marfella R, Papalia R, et al. Bone fragility in patients with diabetes mellitus: A consensus statement from the working group of the Italian Diabetes Society (SID), Italian Society of Endocrinology (SIE), Italian Society of Gerontology and Geriatrics (SIGG), Italian Society of Orthopaedics and Traumatology (SIOT). Nutr Metab Cardiovasc Dis 2021;31:1375–90. [CrossRef]
- Janghorbani M, Van Dam RM, Willett WC, Hu FB. Systematic Review of Type 1 and Type 2 Diabetes Mellitus and Risk of Fracture. Am J Epidemiol 2007;166:495–505. [CrossRef]
- Weber DR, Haynes K, Leonard MB, Willi SM, Denburg MR. Type1Diabetes IsAssociatedWith an Increased Risk of Fracture Across theLifeSpan:APopulation- Based Cohort Study Using The Health Improvement Network (THIN). Diabetes Care 2015;38:1913–20. [CrossRef]
- Van Hulten V, Rasmussen N, Driessen JHM, Burden AM, Kvist A, van den Bergh JP. Fracture Patterns in Type 1 and Type 2 Diabetes Mellitus: A Narrative Review of Recent Literature. Curr Osteoporos Rep 2021;19:644–55. [CrossRef]
- Bai J, Gao Q, Wang C, Dai J. Diabetes mellitus and risk of low-energy fracture: a meta-analysis. Aging Clin Exp Res 2020;32:2173–86. [CrossRef]
- Wang H, Ba Y, Xing Q, Du J-L. Diabetes mellitus and the risk of fractures at specific sites: a meta-analysis. BMJ Open 2019;9:e024067. [CrossRef]
- Palermo A, D’Onofrio L, Buzzetti R, Manfrini S, Napoli N. Pathophysiology of Bone Fragility in Patients with Diabetes. Calcif Tissue Int 2017;100:122–32. [CrossRef]
- Eller-Vainicher C, Cairoli E, Grassi G, Grassi F, Catalano A, Merlotti D, et al. Pathophysiology and Management of Type 2 Diabetes Mellitus Bone Fragility. J Diabetes Res 2020;2020:7608964. [CrossRef]
- Hamann C, Kirschner S, Günther KP, Hofbauer LC. Bone, sweet bone - Osteoporotic fractures in diabetes mellitus. Nat Rev Endocrinol 2012;8:297–305. [CrossRef]
- Napoli N, Strotmeyer ES, Ensrud KE, Sellmeyer DE, Bauer DC, Hoffman AR, et al. Fracture risk in diabetic elderly men: The MrOS study. Diabetologia 2014;57:2057–65. [CrossRef]
- Valderrábano RJ, Linares MI. Diabetes mellitus and bone health: epidemiology, etiology and implications for fracture risk stratification. Clin Diabetes Endocrinol 2018;4:9. [CrossRef]
- Krugh M, Langaker MD. Krugh M, Langaker MD. Dual-Energy X-Ray Absorptiometry. 2023 Jun 5. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 30085584. 2023.
- Bonds DE, Larson JC, Schwartz A V, Strotmeyer ES, Robbins J, Rodriguez BL, et al. Risk of fracture in women with type 2 diabetes: the Women’s Health Initiative Observational Study. J Clin Endocrinol Metab 2006;91:3404–10. [CrossRef]
- Dhaliwal R, Cibula D, Ghosh C, Weinstock RS, Moses AM. Bone quality assessment in type 2 diabetes mellitus. Osteoporos Int 2014;25:1969–73. [CrossRef]
- Silva BC, Leslie WD, Resch H, Lamy O, Lesnyak O, Binkley N, et al. Trabecular bone score: A noninvasive analytical method based upon the DXA image. Journal of Bone and Mineral Research 2014;29:518–30. [CrossRef]
- McCloskey E V, Odén A, Harvey NC, Leslie WD, Hans D, Johansson H, et al. A Meta-Analysis of Trabecular Bone Score in Fracture Risk Prediction and Its Relationship to FRAX. J Bone Miner Res 2016;31:940–8. [CrossRef]
- Ho-Pham LT, Nguyen T V. Association between trabecular bone score and type 2 diabetes: a quantitative update of evidence. Osteoporosis International 2019;30:2079–85. [CrossRef]
- Guglielmi G, Diacinti D, van Kuijk C, Aparisi F, Krestan C, Adams JE, et al. Vertebral morphometry: current methods and recent advances. Eur Radiol 2008;18:1484–96. [CrossRef]
- The jamovi project (2022). jamovi. (Version 2.3) [Computer Software]. Retrieved from https://www.jamovi.org. n.d.
- Janghorbani M, Feskanich D, Willett WC, Hu F. Prospective study of diabetes and risk of hip fracture: the Nurses’ Health Study. Diabetes Care 2006;29:1573–8. [CrossRef]
- Leslie WD, Krieg MA, Hans D. Clinical factors associated with trabecular bone score. Journal of Clinical Densitometry 2013;16:374–9. [CrossRef]
- Palermo A, Tuccinardi D, Defeudis G, Watanabe M, D’Onofrio L, Lauria Pantano A, et al. BMI and BMD: The Potential Interplay between Obesity and Bone Fragility. Int J Environ Res Public Health 2016;13. [CrossRef]
- Gortler H, Rusyn J, Godbout C, Chahal J, Schemitsch EH, Nauth A. Diabetes and Healing Outcomes in Lower Extremity Fractures: A Systematic Review. Injury 2018;49:177–83. [CrossRef]
- Norris R, Parker M. Diabetes mellitus and hip fracture: a study of 5966 cases. Injury 2011;42:1313–6. [CrossRef]
Figure 1.
Median BMI and prevalence of males are higher in DM group. # p<0.001, p=0.051.
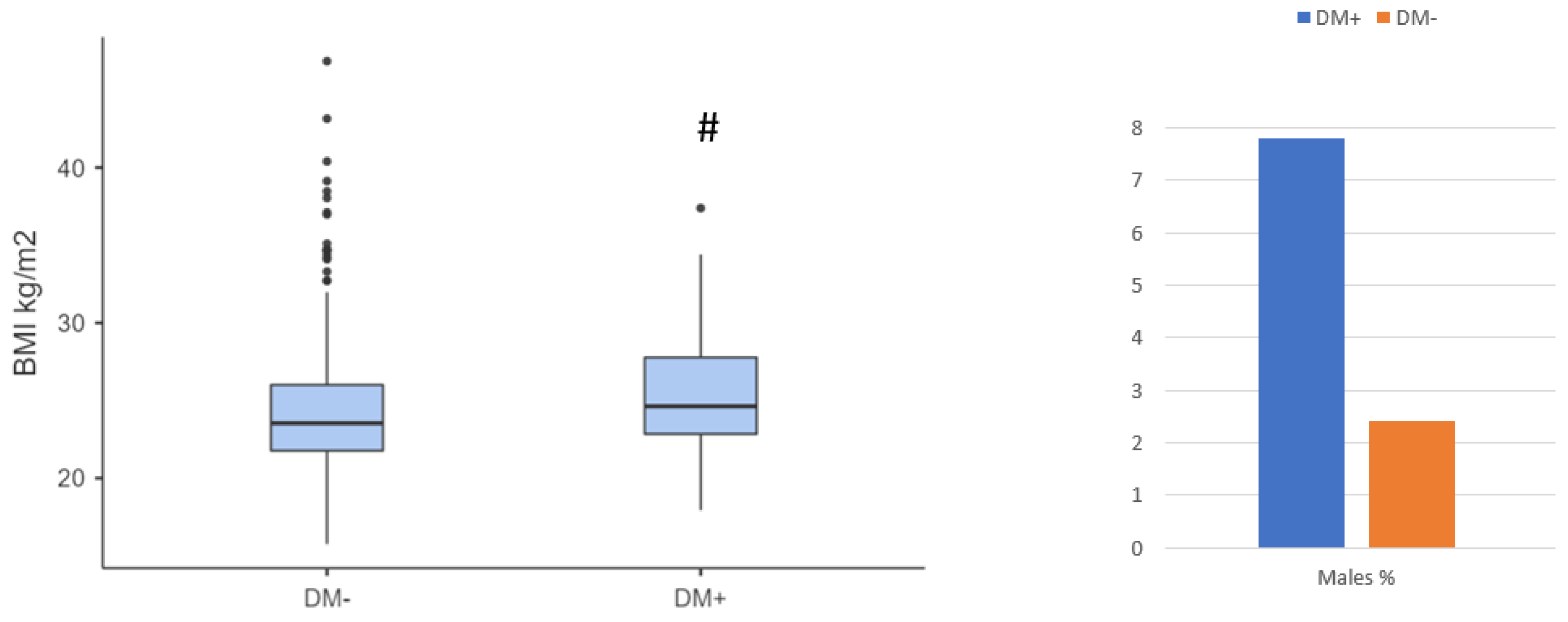
Figure 2.
Prevalence of patients with a combination of vertebral and hip fracture. * p=0.039.
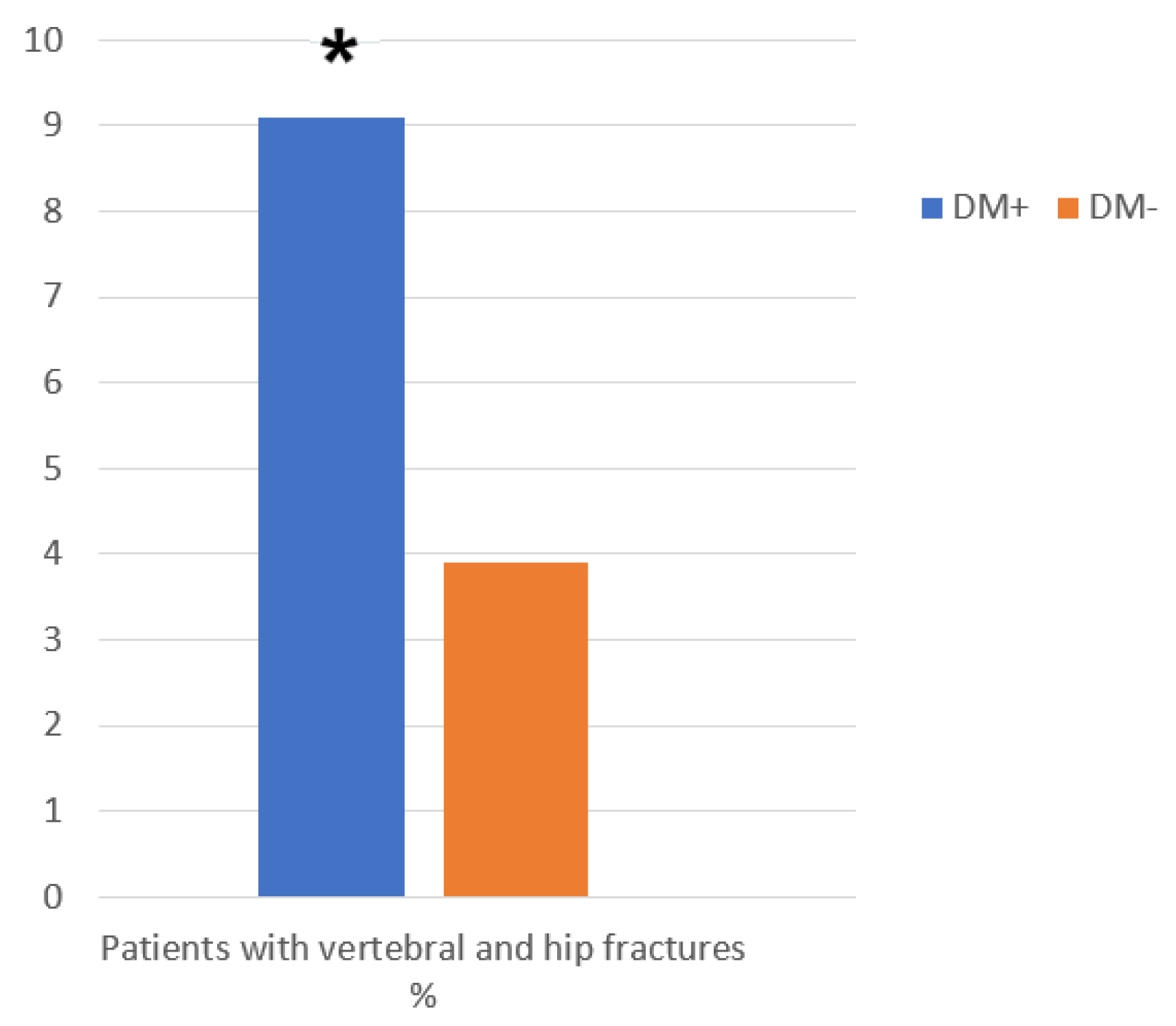
Figure 3.
BMD and TBS values in DM patients and in control group. * (p=0.002); # (p=0.007); £ (p=0.031); $ (p<0.001).
Figure 3.
BMD and TBS values in DM patients and in control group. * (p=0.002); # (p=0.007); £ (p=0.031); $ (p<0.001).
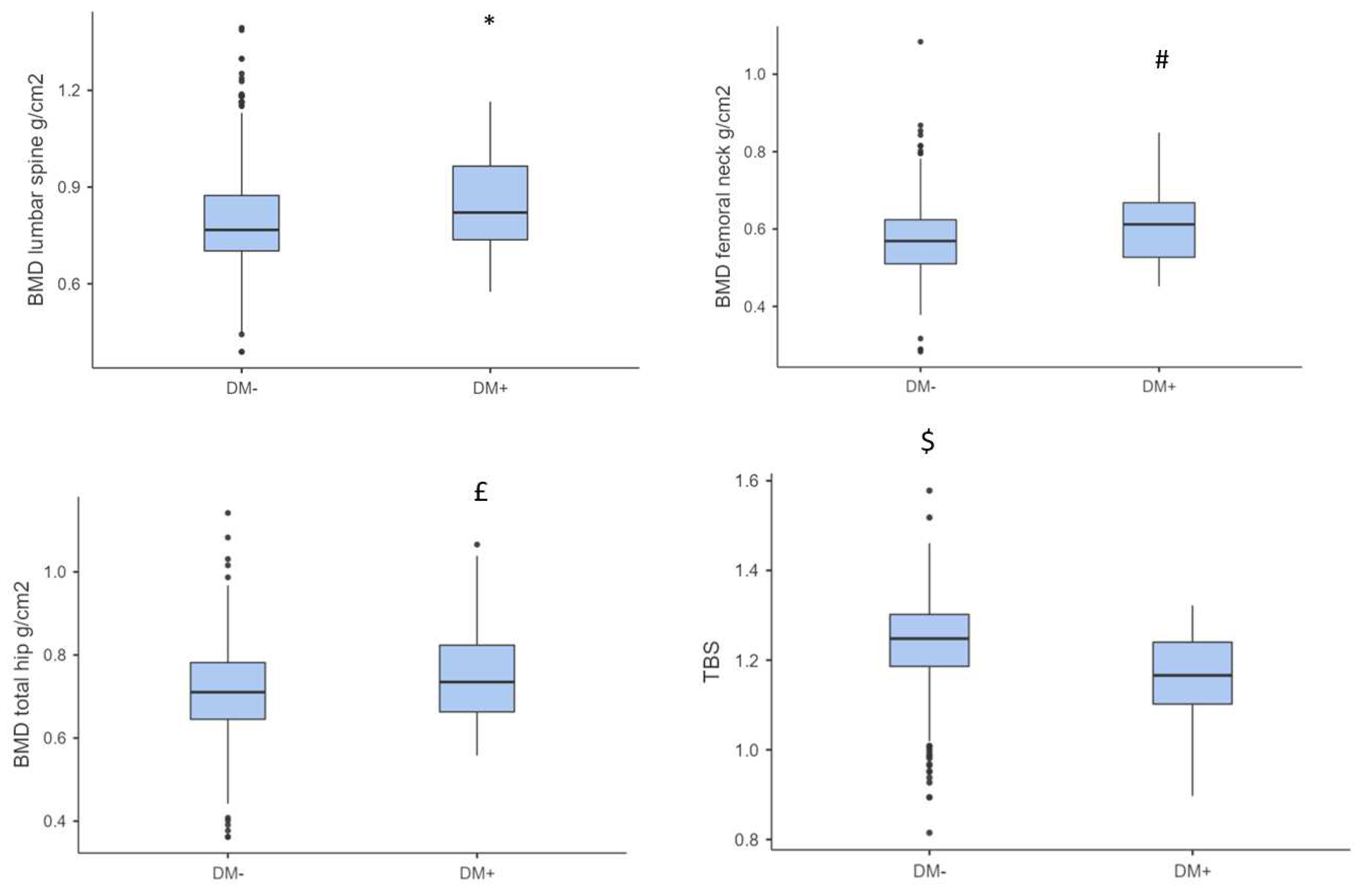

Table 1.
Demographic and clinical features of all patients with fragility fractures.
| Variables | Total |
|---|---|
| Participants n. (%) | 713 |
| Males n. (%) | 27 (3.8) |
| Median Age (years ± IQR) | 81 ± 11 |
| Median BMI (kg/m2 ± IQR) | 23.7 ± 4.34 |
| Median age at the time of first fracture (years ± IQR) | 71 ± 12 |
| Median BMD lumbar spine (g/cm2 ± IQR) | 0.771 ± 0.180 |
| Median BMD femoral neck (g/cm2 ± IQR) | 0.573 ± 0.112 |
|
Median BMD total hip (g/cm2 ± IQR) |
0.713 ± 0.139 |
| Median TBS ± IQR | 1.240 ± 0.125 |
| Family history of Osteoporosis n. (%) | 199 (27.9) |
| Smoking habit n. (%) | 130 (18.2) |
| Alcohol excess n. (%) | 7 (1) |
| RA n. (%) | 29 (4.1) |
| COPD n. (%) | 44 (6.2) |
| Cortisone therapy n. (%) | 40 (5.6) |
| Vertebral fractures n. (%) | 593 (83.2) |
| Hip fractures n. (%) | 36 (5) |
| Both vertebral and hip fractures n. (%) | 32 (4.5) |
| Non-vertebral - non-hip fractures n. (%) | 59 (8.3) |
1 Qualitative data are expressed as absolute numbers (n.) and percentage of the total (%). Continuous variables are expressed as median and IQR. BMI: body mass index, BMD: bone mineral density, TBS: trabecular bone score, RA: rheumatoid arthritis, COPD: chronic obstructive pulmonary disease.
Table 2.
DM patients’ specific characteristics.
| Patients with DM n. | 77 |
|---|---|
| Type 2 DM n. (%) | 70 (90.9) |
| Median Duration of DM ± IQR | 15 ± 10 |
| Median HbA1c mmol/mol ± IQR | 50 ± 12 |
| Median HbA1c % ± IQR | 6.8 ± 1.1 |
| Nutritional therapy n. (%) | 10 (13) |
| Oral hypoglycemic drugs n. (%) | 45 (58) |
| Insulin n. (%) | 17 (22) |
| Insulin + oral hypoglycemic drugs n. (%) | 5 (7) |
| Coronary heart disease n. (%) | 15 (19.5) |
| Carotid artery atheromasia - peripheral arterial disease n. (%) | 30 (39) |
| Peripheral Neuropathy n. (%) | 15 (19.5) |
| Retinopathy n. (%) | 8 (10.4) |
| Nephropathy n. (%) | 16 (20.8) |
1 DM: diabetes mellitus, HbA1c: glycated hemoglobin.
Table 3.
Comparative analysis of patients divided according to presence of DM.
| Variables | DM+ | DM- | p-Value |
|---|---|---|---|
| Participants n. (%) | 77 (10.8) | 636 (89.2) | |
| Males n. (%) | 6 (7.8) | 21 (3.3) | 0.051 |
| Median Age (years ± IQR) | 82 ± 8 | 80 ± 12 | 0.221 |
| Median BMI (kg/m2 ± IQR) | 24.6 ± 4.94 | 23.5 ± 4.24 | <0.001 |
| Median age at the time of first fracture (years ± IQR) | 72 ± 14 | 71 ± 12 | 0.674 |
|
Median BMD lumbar spine (g/cm2 ± IQR) Median TBS ± IQR |
0.821 ± 0.229 | 0.767 ± 0.172 | 0.002 |
| Median BMD femoral neck (g/cm2 ± IQR) | 0.612 ± 0.141 | 0.569 ± 0.114 | 0.007 |
| Median BMD total hip (g/cm2 ± IQR) | 0.735 ± 0.161 | 0.710 ± 0.137 | 0.031 |
| Median TBS ± IQR | 1.170 ± 0.138 | 1.250 ± 0.116 | <0.001 |
| Family history of Osteoporosis n. (%) | 1 (1.3) | 198 (31.1) | <0.001 |
| Smoking habit n. (%) | 21 (27.3) | 109 (17.1) | 0.030 |
| Alcohol excess n. (%) | 0 (0) | 7 (1.1) | 0.355 |
| RA n. (%) | 2 (2.6) | 27 (4.2) | 0.489 |
| COPD n. (%) | 4 (5.2) | 40 (6.3) | 0.706 |
| Cortisone therapy n. (%) | 0 (0) | 40 (6.3) | 0.024 |
| Vertebral fractures n. (%) | 59 (76.6) | 534 (84) | 0.104 |
| Hip fractures n. (%) | 5 (6.5) | 31 (4.9) | 0.540 |
| Both vertebral and hip fractures n. (%) | 7 (9.1) | 25 (3.9) | 0.039 |
| Non-vertebral - non-hip fractures n. (%) | 6 (7.8) | 53 (8.3) | 0.871 |
1 DM+: patients affected by diabetes mellitus, DM-: patients unaffected by diabetes mellitus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



