
Submitted:
06 February 2024
Posted:
07 February 2024
You are already at the latest version
Abstract
Approximately half of head and neck squamous cell carcinoma (HNSCC) cases recur, and most of them recur within the first two years after treatment. Although it has been suggested that the interval to recurrence after radical treatment and prognosis in patients with HNSCC are associated, investigations are insufficient. In this study, patients diagnosed with HNSCC at Kyushu University Hospital were retrospectively analyzed (n = 500). A total of 234 patients experienced recurrence, with 110 and 124 patients experiencing early recurrence (ER) (recurrence within 2–6 months) and late recurrence (LR) (recurrence after 7 months), respectively. There were two independent risk factors for poor prognosis in the multivariate analyses: ER (hazard ratio [HR] = 3.200, 95% confidence interval [CI] = 1.570–6.521, p = 0.001) and no radiotherapy (HR = 0.374, 95% CI = 0.191–0.733, p = 0.004). In patients with recurrent HNSCC, a short interval to recurrence is a risk factor for poor prognosis and survival. This study demonstrated the prognostic value of ER in patients. During the selection of treatment for patients with recurrence, the recurrent area, initial treatment content, and strategy of changing salvage therapy depending on the recurrence status should be considered.
Keywords:
squamous cell carcinoma
; recurrence
; radiotherapy
1. Introduction
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common cancer in the world [1]. For local HNSCCs (LHNSCCs) without distant metastases, radical treatment, including surgical therapy, radiotherapy/chemoradiotherapy, or a combination of both, is preferred depending on the stage [1]. However, given that locally advanced HNSCCs (LAHNSCCs) account for more than 60% of LHNSCCs, approximately half of them recur subsequently [2,3], and most of them recur within the first two years after treatment [4,5].
Interestingly, the interval to recurrence after radical resection has been reported to be associated with clinical outcomes in certain malignant tumors. In gastric [6], liver [7], pancreatic [8], kidney [9], and esophageal [10] cancers, early recurrence (ER) after radical resection has a poorer prognosis than late recurrence (LR). Even in HNSCC, an association between recurrence timing and patient survival has been reported [11,12,13]; however, investigations are insufficient.
In addition, HNSCC shares the concept of platinum resistance with ovarian cancer [14]; recurrence within six months of platinum-based chemotherapy is defined as platinum-resistive cancer, and recurrence after that is defined as platinum-sensitive cancer [15]. Platinum-resistive HNSCC is known to have a poor prognosis [16]. For the initial treatment of LAHNSCC, none of the patients were treated with chemotherapy alone but underwent chemotherapy in combination with radiotherapy or surgery. In other words, in HNSCC based on radiotherapy in combination with platinum preparations as the radical treatment, it is difficult to distinguish whether patients with recurrence within six months are truly resistant to platinum preparations or are actually resistant to radiotherapy.
The primary purpose of our study was to explore the relationship between recurrence time and overall survival (OS) in patients with HNSCC. The second purpose was to analyze platinum and radiotherapy resistance, as well as survival outcomes in HNSCC, and identify the risk factors for poor prognosis in patients with recurrent HNSCC.
2. Materials and Methods
2.1. Patient Cohort
We retrospectively collected and analyzed the data of 643 patients who had HNSCC without distant metastasis at the time of initial treatment and received radical treatment at Kyushu University Hospital between January 1, 2015, and December 31, 2021.
The exclusion criteria were as follows: Recurrence was defined as the appearance of a new lesion six weeks after the disappearance of lesions following radical treatment [17], and patients in whom lesions appeared in less than six weeks (n = 4) were excluded from the analysis as residuals. Patients with heterochronic occurrence of a multiplicity of cancers in the head and neck area (n = 105) were also excluded from the analysis because of the unknown origin of the recurrence. Patients who could not be followed up for more than two years (n = 34) were also excluded from the analysis. Finally, 500 patients were included in this study. The patient observation period was until death or December 31, 2023, and the median follow-up period was 40 months (range: 4–293).
This study was conducted in compliance with the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Review Board of Kyushu University (No. 22301-00). Informed consent was mostly obtained in writing, and some patients were granted the opportunity to refuse participation by opting out on the institution’s website.
2.2. Definitions
ER was defined as disease recurrence within six months of radical treatment, whereas LR was defined as recurrence after more than six months. In addition, platinum-resistive patients, as previously reported [14,15], were defined as patients who showed recurrence within six months of platinum preparation use, and radiation-resistant patients were those in whom lesions disappeared after the completion of radiotherapy but had recurred within six months.
The tumor–node–metastasis classification was based on the Union for International Cancer Control classification (8th edition). OS was defined as the period from initial treatment to death.
2.3. Statistical Analysis
For the statistical significance test, continuous variables were assessed using the Mann–Whitney U test, and categorical variables were assessed using Fisher’s exact test. OS was calculated using the Kaplan–Meier method and was compared using the log-rank test. Clinicopathological factors that might affect OS were identified using univariate and multivariate Cox proportional hazards models. Risk was expressed as hazard ratio (HR) and the 95% confidence interval (CI) was determined using the reference groups. For statistical analysis, the SPSS Statistics software program ver. 22.0 (IBM Japan, Ltd., Tokyo, Japan) was used in all tests, and a p < 0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
The patients’ baseline characteristics are shown in Table 1. Among the 500 patients, 377 (75.4%) were male, and 123 (24.6%) were female. The median patient age was 67 years (range: 20–92). The most common cancer site was the oral cavity (145 patients [29.0%]), followed by the hypopharynx (113 patients [22.6%]). According to the T classification, T1/T2 accounted for 246 patients (49.2%), whereas T3/T4 accounted for 254 patients (50.2%). In addition, according to N classification, N0 was the most common with 252 patients (50.4%).
A total of 302 patients (60.4%) underwent surgery for initial treatment, among whom radiotherapy with or without chemotherapy was administered after surgery in 126 patients who were extracapsular spread positive [18,19] and margin positive [18,19]. These were considered risk factors for poor prognosis, with radiotherapy alone in 28 patients, cisplatin combination (100 mg/m2, triweekly) in 87 patients, and TS-1 combination (100 mg/body/day) in 11 patients. In addition, neoadjuvant chemotherapy (docetaxel 60 mg/m2 on day 1, cisplatin 60 mg/m2 on day 1, 5FU 600 mg/m2 days 1–4) was performed on 19 patients. Radiotherapy or chemoradiotherapy was administered to 198 patients (39.6%) as the initial treatment with radiotherapy or chemoradiotherapy alone, cisplatin combination (100 mg/m2, triweekly), and TS-1 combination (100 mg/body/day) for 17, 147, and 34 patients, respectively. Platinum preparations were used for chemoradiotherapy or neoadjuvant chemotherapy at initial treatment in 253 patients (50.6%).
Among the patients who underwent surgery, the margin status was assessed in 297 patients, out of which 115 (38.7%) were found to be margin positive. Lymph nodes were dissected in 202 patients, 47 (23.3%) of whom had extracapsular spread. In addition, perineural invasion (pn), lymph vessel invasion (ly), and blood vessel invasion (v) were assessed in 288 patients, and 94 (32.6%) tested positive for either of them.
3.2. OS by Recurrence Status
Among the 500 patients who received the initial treatment, 234 (46.8%) experienced recurrence during the observation period. A total of 110 patients had ER (22.0%), and 124 patients had LR (24.8%), with 110 patients (22.0%) showing recurrence at 2–6 months, 59 patients (11.8%) at 7–12 months, 31 patients (6.2%) at 13–24 months, and 34 patients (6.8%) after 25 months (Figure 1).
The characteristics of the patients with ER (recurrence within six months) and LR (recurrence in more than six months) are shown in Table 1. Among patients with LR, the percentage of nasopharyngeal and laryngeal cancers was higher (p = 0.014); there were more patients with T1 (p = 0.003); and fewer patients were positive for either pn, ly, or v (p = 0.002). However, no significant difference was observed in radiotherapy and platinum use histories.
The OS curves of the ER and LR groups are shown (Figure 2). The ER group had a significantly worse prognosis than the LR group (p < 0.001).
3.3. Survival Rate by Resistance to Platinum Preparation and Radiotherapy
Among the 253 patients who used a platinum preparation at the initial treatment, 52 (20.6%, 52/253) had platinum-resistant recurrence, whereas 54 (21.3%, 54/253) had platinum-sensitive recurrence. The platinum-resistive group had a significantly poorer prognosis than the platinum-sensitive group (p = 0.026, Figure 3-a).
Among the 324 patients who received radiotherapy at initial treatment (including after surgery), 75 (23.1%, 75/324) had radiotherapy-resistive recurrence, whereas 80 (24.7%, 80/324) had radiotherapy-sensitive recurrence. The radiation-resistant group had a significantly worse prognosis than the radiation-sensitive group (p = 0.003, Figure 3-b).
3.4. Survival Rate by Pathological Findings of Surgery Patients
Patients who were margin positive (n = 115) had a significantly worse prognosis than patients who were margin negative (n = 182) (p = 0.023, Figure 4-a).
Patients with lymph node extracapsular spread (n = 47) had a significantly worse prognosis than patients without extracapsular spread (n = 67) and with pN0 (n = 88) (p = 0.000, Figure 4-b).
In addition, patients who were positive for perineural invasion (pn), lymph vessel invasion (ly), or blood vessel invasion (v) (n = 94) had a significantly worse prognosis than patients who were negative for these factors (n = 194) (p = 0.000, Figure 4-c).
3.5. Predictors of Outcomes
The results of the univariate and multivariate analyses predicting OS are summarized in Table 2. Multivariate analyses revealed that in LAHNSCC, the independent risk factors for poor prognosis were ER (HR = 3.200, 95% CI = 1.570–6.521, p = 0.001) and no radiotherapy (HR = 0.374, 95% CI = 0.191–0.733, p = 0.004). Platinum resistance, platinum sensitivity, radiation resistance, or radiation sensitivity were not significant prognostic factors.
4. Discussion
In this retrospective study, 46.8% of patients who received surgical therapy or radiotherapy/chemoradiotherapy for curative purposes experienced recurrence, and approximately half of the patients with recurrence experienced it within six months. This result is similar to that of a previous study [20]. In addition, this study demonstrated that recurrence-free interval affects prognosis. This is one of the few studies reporting that interval to recurrence is a prognostic factor for survival in patients with recurrent HNSCC after treatment with various modalities.
Previous studies demonstrating the association between the interval to recurrence and clinical outcomes mainly arose after radical resection to recurrence in other carcinomas [6,7,8,9,10] and HNSCC [12,21]. In all reports, patients with ER had a significantly worse prognosis than those with LR. In addition, few studies have demonstrated an association between the interval to recurrence after radiotherapy for HNSCC and clinical outcomes. According to these studies, a short interval to salvage surgery after radiotherapy for HNSCC is a significant negative prognostic factor [22,23]. To the best of our knowledge, only three reports have investigated the association between recurrence after initial treatment (including all treatment modalities) and prognosis, similar to the present study [11,20,24]. Among them, 2 previous studies defined cases with a recurrence-free interval of less than 12 months as ER, whereas the remaining, which were similar to ours, defined recurrence in less than 6 months as ER. All of them concluded that a longer recurrence-free interval leads to a better prognosis. In the present study, we defined ER as recurrence within six months. This is due to doubts regarding the concept of platinum resistance, which is widely used in head and neck cancer treatment. For the investigation of the association between interval to HNSCC recurrence and prognosis, we also examined whether patients who showed recurrence within six months after platinum use were resistant to only platinum or originally resistant to any treatment modality. The results of the present study suggest that the prognosis is poor for patients with ER regardless of the treatment modality; thus, the poor prognosis of platinum-resistant patients may not have been due to platinum sensitivity only. The above shows that there are doubts on whether the concept of platinum resistance/sensitivity in the head and neck area captures the true nature of tumors.
ER is mainly due to the aggressive biological behavior of the tumors themselves, such as rapid growth rate and treatment resistance [22]. A study of patients who underwent chemoradiotherapy after surgery reported that patients with very ER in whom macroscopic tumors recurred while waiting for radiotherapy accounted for approximately 20% of all patients, and such patients had a poor prognosis [25]. However, an accurate mechanism for poor prognosis in patients with ER has not been demonstrated. Some genomic and proteomic analyses have reported the possibility of identifying poor prognoses, but they are still in the research phase [26]. For this reason, the identification and selection of patients with ER before treatment are still difficult. In addition, even if patients are identified, preventive measures are difficult. This study also demonstrated the difficulties in improving the OS of patients with a poor prognosis. In fact, among the patients undergoing surgery, even though many who were extracapsular spread positive [18,19], margin positive [18,19], and pn/ly/v positive [19], which are considered risk factors for poor prognosis, underwent postoperative radiotherapy or chemoradiotherapy, all positive patients had a poor prognosis. This shows that even if multimodal treatment involving surgery, radiotherapy, and chemotherapy is performed, it is difficult to completely eliminate the poor prognostic environment as a tumor factor. To overcome this difficulty, trials involving preoperative immunotherapy using immune checkpoint inhibitors (ICIs) and their use as maintenance therapy after chemoradiotherapy or surgery as new strategies to improve OS are currently underway, and results are anticipated. In addition, given the results of this study, we propose a treatment strategy based on a different approach for patients with recurrence. Currently, when selecting treatment for patients with recurrence, it is recommended to devise treatment strategies [27] that are based on the recurrence area, initial treatment content, and combined positive score before ICI use [28]. However, we conclude that changing salvage therapy depending on the recurrence status could also be a good strategy. In fact, in small-cell lung cancer, patients are divided into patients with sensitive relapse, in whom initial chemotherapy works and the interval to recurrence is long, and patients with refractory relapse, in whom the interval to recurrence is short and the treatment strategies are different [29,30]. Taking similar measures for HNSCC may improve the prognosis of patients with ER.
The strength of this study is the addition of the perspective of resistance to platinum preparations and radiotherapy at the time of recurrence as factors that may affect OS. Multivariate analyses revealed that ER status, rather than resistance to platinum preparations or radiotherapy, affected OS. However, this study has several limitations. First, this was a retrospective study, and the limitations and selection risks of bias could not be eliminated. Second, the survey results cannot be generalized to different populations. Third, the prognostic factors to be subjected to multivariate analyses were limited by the sample size. For example, factors that may affect the recurrence risk and prognosis of patients with HNSCC, such as resection margin; extracapsular spread; ly, pn, and v; and human papillomavirus status, could not be included because of limitations in the sample size. To include all prognostic predictors in future studies, it is necessary to increase the sample size. This will help in obtaining more accurate estimates of recurrence risk.
5. Conclusions
After treatment with various modalities, approximately half of the patients with recurrent HNSCC experienced recurrence during the observation period. Furthermore, half of the patients showed recurrence within two to six months. Interval to recurrence is a significant independent prognostic risk factor for OS, and this study demonstrated the prognostic values of patients with ER. ER cases should be considered for different treatment strategies (e.g., addition of drugs) rather than LR cases because of the presumed poor prognostic factors of tumor characteristics.
Author Contributions
Mioko Matsuo: Writing—Original Draft, Conceptualization, Methodology, Investigation. Kazuki Hashimoto: Validation. Ryunosuke Kogo: Resources. Masanobu Sato: Data Curation. Tomomi Manako: Data Curation. Takashi Nakagawa: Supervision.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in compliance with the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Review Board of Kyushu University (No. 22301-00).
Informed Consent Statement
Informed consent was mostly obtained in writing, and some patients were granted the opportunity to refuse participation by opting out on the institution’s website.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to privacy reasons but are available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank Editage (www.editage.jp) for the English language editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and Neck Squamous Cell Carcinoma. Nat Rev Dis Primers 2020, 6, 92. [Google Scholar] [CrossRef]
- Chow, L.Q.M. Head and Neck Cancer. N Engl J Med 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Sacco, AG; Cohen, EE. Current Treatment Options for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma. J Clin Oncol 2015, 33, 3305–3313. [Google Scholar] [CrossRef] [PubMed]
- Borsetto, D.; Sethi, M.; Polesel, J.; Tomasoni, M.; Deganello, A.; Nicolai, P.; Bossi, P.; Fabbris, C.; Molteni, G.; Marchioni, D.; Tofanelli, M.; Cragnolini, F.; Tirelli, G.; Ciorba, A.; Pelucchi, S.; Corazzi, V.; Canzi, P.; Benazzo, M.; Lupato, V.; Giacomarra, V.; Cazzador, D.; Bandolin, L.; Menegaldo, A.; Spinato, G.; Obholzer, R.; Fussey, J.; Boscolo-Rizzo, P. The Risk of Recurrence in Surgically Treated Head and Neck Squamous Cell Carcinomas: A Conditional Probability Approach. Acta Oncol 2021, 60, 942–947. [Google Scholar] [CrossRef]
- Lacas, B.; Carmel, A.; Landais, C.; Wong, S.J.; Licitra, L.; Tobias, J.S.; Burtness, B.; Ghi, M.G.; Cohen, E.E.W.; Grau, C.; Wolf, G.; Hitt, R.; Corvò, R.; Budach, V.; Kumar, S.; Laskar, S.G.; Mazeron, J.J.; Zhong, L.P.; Dobrowsky, W.; Ghadjar, P.; Fallai, C.; Zakotnik, B.; Sharma, A.; Bensadoun, R.J.; Ruo Redda, M.G.; Racadot, S.; Fountzilas, G.; Brizel, D.; Rovea, P.; Argiris, A.; Nagy, Z. T.; Lee, J.W.; Fortpied, C.; Harris, J.; Bourhis, J.; Aupérin, A.; Blanchard, P.; Pignon, J. P. ; MACH-NC Collaborative Group, Meta-analysis of Chemotherapy in Head and Neck Cancer (MACH-NC): An Update on 107 Randomized Trials and 19,805 Patients, On Behalf of MACH-NC Group. Radiother Oncol 2021, 156, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.W.; Liu, D.L.; Chen, J.X.; Lin, L.Z.; Zhuang, L.P.; Hou, X.H. Early and Late Recurrences in Lymph Node-Negative Gastric Cancer: A Retrospective Cohort Study. Ann Saudi Med 2021, 41, 336–349. [Google Scholar] [CrossRef]
- Yan, W.T.; Li, C.; Yao, L.Q.; Qiu, H.B.; Wang, M.D.; Xu, X.F.; Zhou, Y.-H.; Wang, H.; Chen, T.H.; Gu, W.M.; Zhong, J.H.; Wu, H.; Pawlik, T. M.; Lau, W. Y.; Shen, F.; Yang, T. Predictors and Long-Term Prognosis of Early and Late Recurrence for Patients Undergoing Hepatic Resection of Hepatocellular Carcinoma: A Large-Scale Multicenter Study. Hepatobiliary Surg Nutr 2023, 12, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.P.; Xu, S.; Gao, Y.X.; Zhao, Z.M.; Zhao, G.D.; Hu, M.G.; Tan, X.L.; Lau, W.Y.; Liu, R. Early and Late Recurrence Patterns of Pancreatic Ductal Adenocarcinoma After Pancreaticoduodenectomy: A Multicenter Study. Int J Surg 2023, 109, 785–793. [Google Scholar] [CrossRef]
- Lee, C.H.; Chung, J.; Kwak, C.; Jeong, C.W.; Il Seo, S.; Kang, M.; Hong, S.H.; Song, C.; Park, J.Y.; Hwang, E.C.; Lee, H.; Ku, J.Y.; Seo, W.I.; Choi, S.H.; Ha, H.K.; Korean Renal Cancer Study Group. Targeted therapy response in early versus late recurrence of renal cell carcinoma after surgical treatment: A propensity score-matched study using the Korean Renal Cancer Study Group database. Int J Urol 2021, 28, 417–423. [Google Scholar] [CrossRef]
- Zhang, Y.; Gao, J.; Zheng, A.; Yang, H.; Li, J.; Wu, S.; Zhao, J.; Meng, P.; Zhou, F. Definition and Risk Factors of Early Recurrence Based on Affecting Prognosis of Esophageal Squamous Cell Carcinoma Patients After Radical Resection. Transl Oncol 2021, 14, 101066. [Google Scholar] [CrossRef]
- Chang, J.H.; Wu, C.C.; Yuan, K.S.P.; Wu, A.T.H.; Wu, S.Y. Locoregionally Recurrent Head and Neck Squamous Cell Carcinoma: Incidence, Survival, Prognostic Factors, and Treatment Outcomes. Oncotarget 2017, 8, 55600–55612. [Google Scholar] [CrossRef] [PubMed]
- Weckx, A.; Riekert, M.; Grandoch, A.; Schick, V.; Zöller, J.E.; Kreppel, M. Time to Recurrence and Patient Survival in Recurrent Oral Squamous Cell Carcinoma. Oral Oncol 2019, 94, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Rettig, E.; Fakhry, C. Understanding the Impact of Survival and Human Papillomavirus Tumor Status on Timing of Recurrence in Oropharyngeal Squamous Cell Carcinoma. Oral Oncol 2016, 52, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Oronsky, B.; Ray, C.M.; Spira, A.I.; Trepel, J.B.; Carter, C.A.; Cottrill, H.M. A Brief Review of the Management of Platinum-Resistant-Platinum-Refractory Ovarian Cancer. Med Oncol 2017, 34, 103. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; Worden, F.; Saba, N.F.; Iglesias Docampo, L.C.; Haddad, R.; Rordorf, T.; Kiyota, N.; Tahara, M.; Monga, M.; Lynch, M.; Geese, W.J.; Kopit, J.; Shaw, J.W.; Gillison, M.L. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N Engl J Med 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Tsukahara, K.; Okamoto, I.; Katsube, Y.; Shimizu, A.; Kondo, T.; Hanyu, K.; Fushimi, C.; Okada, T.; Miura, K. Clinical Outcomes of Platinum-Based Chemotherapy plus Cetuximab for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck: Comparison Between Platinum-Sensitive and Platinum-Resistant Patients. Acta Otolaryngol 2019, 139, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Safi, A.F.; Kauke, M.; Grandoch, A.; Nickenig, H.J.; Zöller, J.E.; Kreppel, M. Analysis of Clinicopathological Risk Factors for Locoregional Recurrence of Oral Squamous Cell Carcinoma – Retrospective Analysis of 517 Patients. J Craniomaxillofac Surg 2017, 45, 1749–1753. [Google Scholar] [CrossRef]
- Cooper, J.S.; Zhang, Q.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; Lustig, R.; Ensley, J.F.; Thorstad, W.; Schultz, C.J.; Yom, S.S.; Ang, K.K. Long-Term Follow-Up of the RTOG 9501/Intergroup Phase III Trial: Postoperative Concurrent Radiation Therapy and Chemotherapy in High-Risk Squamous Cell Carcinoma of the Head and Neck. Int J Radiat Oncol Biol Phys 2012, 84, 1198–1205. [Google Scholar] [CrossRef]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; Cognetti, F.; Bourhis, J.; Kirkpatrick, A.; van Glabbeke, M.; European Organization for Research and Treatment of Cancer Trial 22931. Postoperative Irradiation with or Without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N Engl J Med 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Haring, C.T.; Kana, L.A.; Dermody, S.M; Brummel, C.; McHugh, J.B.; Casper, K.A.; Chinn, S.B.; Malloy, K.M.; Mierzwa, M.; Prince, M.E.P.; Rosko, A.J.; Shah, J.; Stucken, C.L.; Shuman, A.G.; Brenner, J.C.; Spector, M.E.; Worden, F.P.; Swiecicki, P.L. Patterns of recurrence in head and neck squamous cell carcinoma to inform personalized surveillance protocols. Cancer 2023, 129, 2817–2827. [Google Scholar] [CrossRef]
- Liao, C.T.; Chang, J.T.; Wang, H.M.; Ng, S.H.; Hsueh, C.; Lee, L.Y.; Lin, C.H.; Chen, I.H.; Huang, S.F.; Cheng, A.J.; Yen, T.C. Salvage Therapy in Relapsed Squamous Cell Carcinoma of the Oral Cavity: How and When? Cancer 2008, 112, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, Y.; Li, Z.; Liu, S.; Li, H.; Xu, Z. Benefit of Salvage Total Pharyngolaryngoesophagectomy for Recurrent Locally Advanced Head and Neck Cancer After Radiotherapy. Radiat Oncol 2017, 12, 164. [Google Scholar] [CrossRef] [PubMed]
- Heft Neal, M.E.; Brennan, J.; Haring, C.T.; Brenner, J.C.; Worden, F.; Swiecicki, P.; Mierzwa, M.; Casper, K.A.; Malloy, K.M.; Stucken, C.L.; McLean, S.A.; Prince, M.E.; Bradford, C.R.; Wolf, G.T.; Shuman, A.G.; Chinn, S.B.; Chepeha, D.B.; Rosko, A.J.; Spector, M.E. Predictors of Survival in Patients Undergoing Oropharyngeal Surgery for Cancer Recurrence After Radiation Therapy. Eur Arch Otorhinolaryngol 2020, 277, 2085–2093. [Google Scholar] [CrossRef] [PubMed]
- Lupato, V.; Giacomarra, V.; Alfieri, S.; Fanetti, G.; Polesel, J. Prognostic Factors in Salvage Surgery for Recurrent Head and Neck Cancer: A Systematic Review and Meta-analysis. Crit Rev Oncol Hematol 2022, 169, 103550. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Abraham, J.; Ross, E.; Ridge, J.A.; Lango, M.N.; Liu, J.C.; Bauman, J.R.; Avkshtol, V.; Galloway, T. J. Rapid Recurrence in Head and Neck Cancer: Underappreciated Problem with Poor Outcome. Head Neck 2021, 43, 212–222. [Google Scholar] [CrossRef]
- Salehi, A.; Wang, L.; Coates, P. J.; Norberg Spaak, L.; Gu, X.; Sgaramella, N.; Nylander, K. Reiterative Modeling of Combined Transcriptomic and Proteomic Features Refines and Improves the Prediction of Early Recurrence in Squamous Cell Carcinoma of Head and Neck. Comput Biol Med 2022, 149, 105991. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Head and Neck Cancers, version 1.2024. http://www.nccn.org/Home.
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; Fuereder, T.; Hughes, B.G.M.; Mesía, R.; Ngamphaiboon, N.; Rordorf, T.; Wan Ishak, W.Z.; Hong, R.; González Mendoza, R.; Roy, A.; Zhang, Y.; Gumuscu, B.; Cheng, J.D.; Jin, F.; Rischin, D.; Lerzo, G.; Tatangelo, M.; Varela, M.; Zarba, J.J.; Boyer, M.; Gan, H.; Gao, B.; Hughes, B.; Mallesara, G.; Rischin, D.; Taylor, A.; Burian, M.; Fuereder, T.; Greil, R.; Barrios, C.H.; de Castro Junior, D.O.; Castro, G.; Franke, F.A.; Girotto, G.; Lima, I.P.F.; Nicolau, U.R.; Pinto, G.D.J.; Santos, L.; Victorino, A.; Chua, N.; Couture, F.; Gregg, R.; Hansen, A.; Hilton, J.; McCarthy, J.; Soulieres, D.; Ascui, R.; Gonzalez, P.; Villanueva, L.; Torregroza, M.; Zambrano, A.; Holeckova, P.; Kral, Z.; Melichar, B.; Prausova, J.; Vosmik, M.; Andersen, M.; Gyldenkerne, N.; Jurgens, H.; Putnik, K.; Reinikainen, P.; Gruenwald, V.; Laban, S.; Aravantinos, G.; Boukovinas, I.; Georgoulias, V.; Psyrri, A.; Kwong, D.; Al-Farhat, Y.; Csoszi, T.; Erfan, J.; Horvai, G.; Landherr, L.; Remenar, E.; Ruzsa, A.; Szota, J.; Billan, S.; Gluck, I.; Gutfeld, O.; Popovtzer, A.; Benasso, M.; Bui, S.; Ferrari, V.; Licitra, L.; Nole, F.; Fujii, T.; Fujimoto, Y.; Hanai, N.; Hara, H.; Matsumoto, K.; Mitsugi, K.; Monden, N.; Nakayama, M.; Okami, K.; Oridate, N.; Shiga, K.; Shimizu, Y.; Sugasawa, M.; Tahara, M.; Takahashi, M.; Takahashi, S.; Tanaka, K.; Ueda, T.; Yamaguchi, H.; Yamazaki, T.; Yasumatsu, R.; Yokota, T.; Yoshizaki, T.; Kudaba, I.; Stara, Z.; Wan Ishak, W.Z.; Cheah, S.K.; Aguilar Ponce, J.; Gonzalez Mendoza, R.; Hernandez Hernandez, C.; Medina Soto, F.; Buter, J.; Hoeben, A.; Oosting, S.; Suijkerbuijk, K.; Bratland, A.; Brydoey, M.; Alvarez, R.; Mas, L.; Caguioa, P.; Querol, J.; Regala, E.E.; Tamayo, M.B.; Villegas, E.M.; Kawecki, A.; Karpenko, A.; Klochikhin, A.; Smolin, A.; Zarubenkov, O.; Goh, B.C.; Cohen, G.; du Toit, J.; Jordaan, C.; Landers, G.; Ruff, P.; Szpak, W.; Tabane, N.; Brana, I.; Iglesias Docampo, L.; Lavernia, J.; Mesia, R.; Abel, E.; Muratidu, V.; Nielsen, N.; Cristina, V.; Rordorf, T.; Rothschild, S.; Hong, R.; Wang, H.; Yang, M.; Yeh, S.; Yen, C.; Ngamphaiboon, N.; Soparattanapaisarn, N.; Sriuranpong, V.; Aksoy, S.; Cicin, I.; Ekenel, M.; Harputluoglu, H.; Ozyilkan, O.; Harrington, K.; Agarwala, S.; Ali, H.; Alter, R.; Anderson, D.; Bruce, J.; Burtness, B.; Campbell, N.; Conde, M.; Deeken, J.; Edenfield, W.; Feldman, L.; Gaughan, E.; Goueli, B.; Halmos, B.; Hegde, U.; Hunis, B.; Jotte, R.; Karnad, A.; Khan, S.; Laudi, N.; Laux, D.; Martincic, D.; McCune, S.; McGaughey, D.; Misiukiewicz, K.; Mulford, D.; Nadler, E.; Neupane, P.; Nunnink, J.; Ohr, J.; O’Malley, M.; Patson, B.; Paul, D.; Popa, E.; Powell, S.; Redman, R.; Rella, V.; Rocha Lima, C.; Sivapiragasam, A.; Su, Y.; Sukari, A.; Wong, S.; Yilmaz, E.; Yorio, J. Pembrolizumab Alone or with Chemotherapy Versus Cetuximab with Chemotherapy for Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck (KEYNOTE-048): A Randomised, Open-Label, Phase 3 Study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- O’Brien, M.E.; Ciuleanu, T.E.; Tsekov, H.; Shparyk, Y.; Cuceviá, B.; Juhasz, G.; Thatcher, N.; Ross, G.A.; Dane, G.C.; Crofts, T. Phase III Trial Comparing Supportive Care Alone with Supportive Care with Oral Topotecan in Patients with Relapsed Small-Cell Lung Cancer. J Clin Oncol 2006, 24, 5441–5447. [Google Scholar] [CrossRef]
- Horita, N.; Yamamoto, M.; Sato, T.; Tsukahara, T.; Nagakura, H.; Tashiro, K.; Shibata, Y.; Watanabe, H.; Nagai, K.; Nakashima, K.; Ushio, R.; Ikeda, M.; Kobayashi, N.; Shinkai, M.; Kudo, M.; Kaneko, T. Amrubicin for Relapsed Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis of 803 Patients. Sci Rep 2016, 6, 18999. [Google Scholar] [CrossRef]
Figure 1.
Recurrence time and frequency.
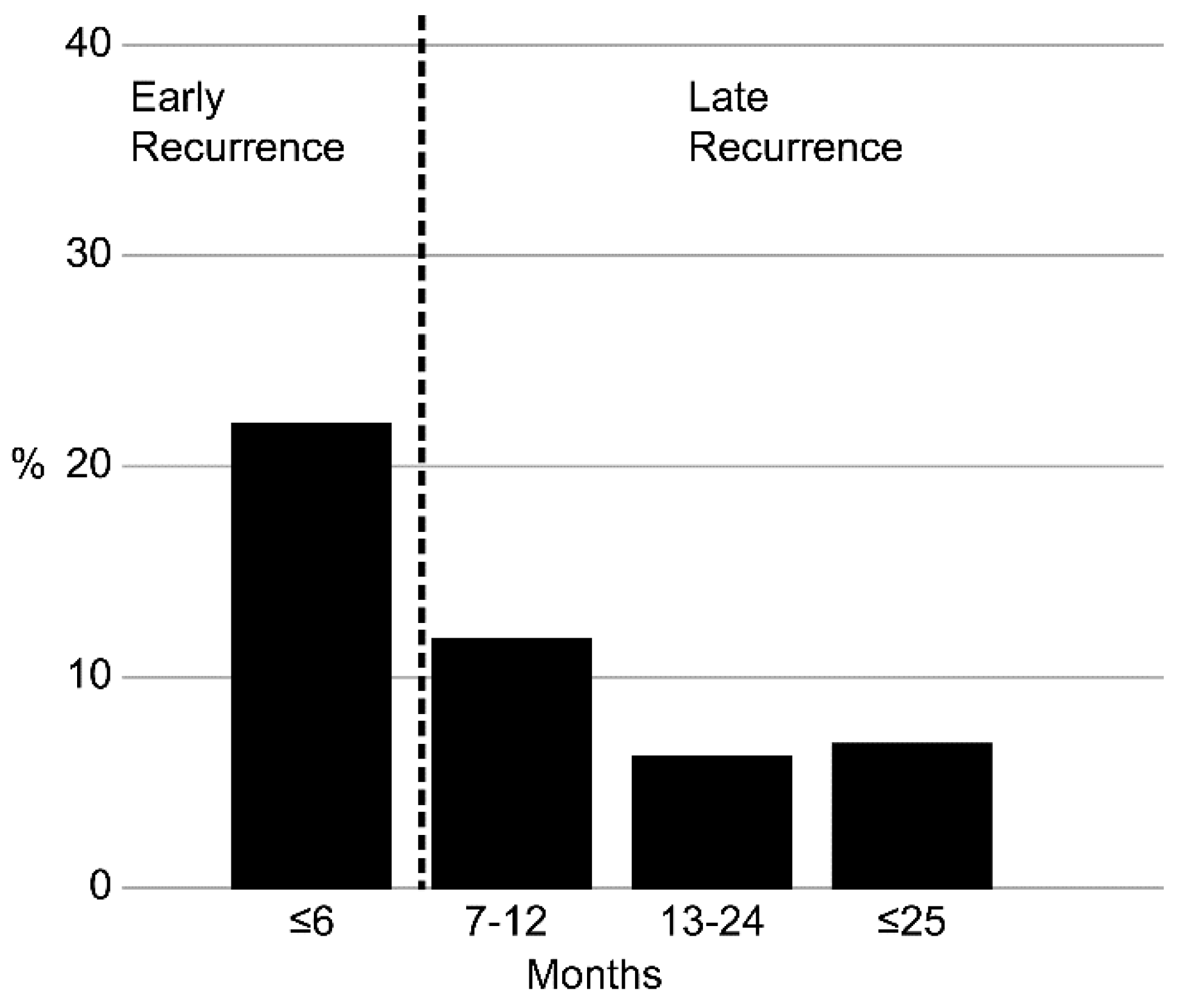
Figure 2.
Survival curves for ER (recurrence in two to six months) and LR (recurrence after seven months).
Figure 2.
Survival curves for ER (recurrence in two to six months) and LR (recurrence after seven months).
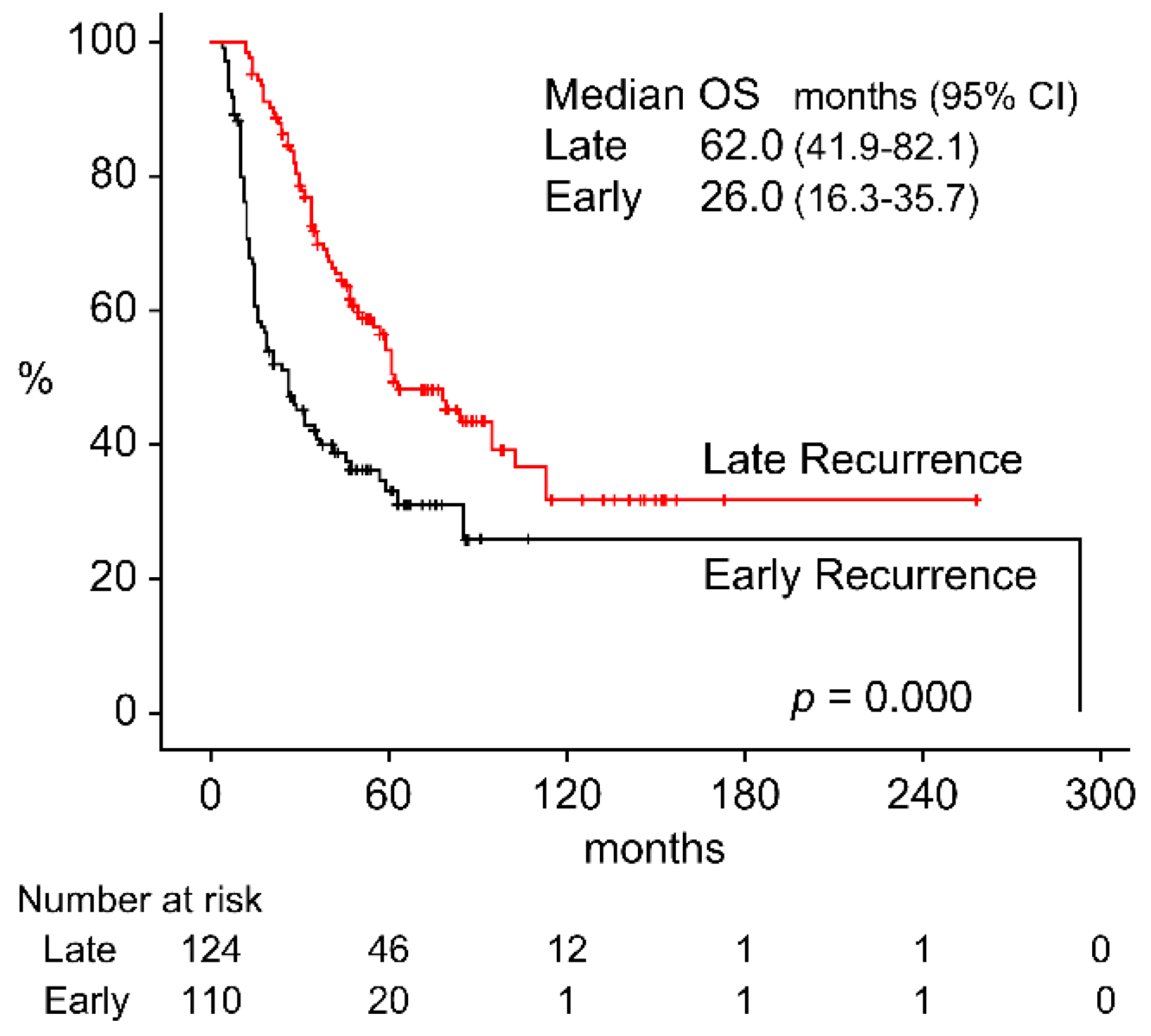
Figure 3.
(a) Survival curves for platinum-resistive recurrence and platinum-sensitive recurrence. (b) Survival curves for radiotherapy-resistive recurrence (recurrence in two to six months) and radiotherapy-sensitive recurrence (recurrence after seven months).
Figure 3.
(a) Survival curves for platinum-resistive recurrence and platinum-sensitive recurrence. (b) Survival curves for radiotherapy-resistive recurrence (recurrence in two to six months) and radiotherapy-sensitive recurrence (recurrence after seven months).
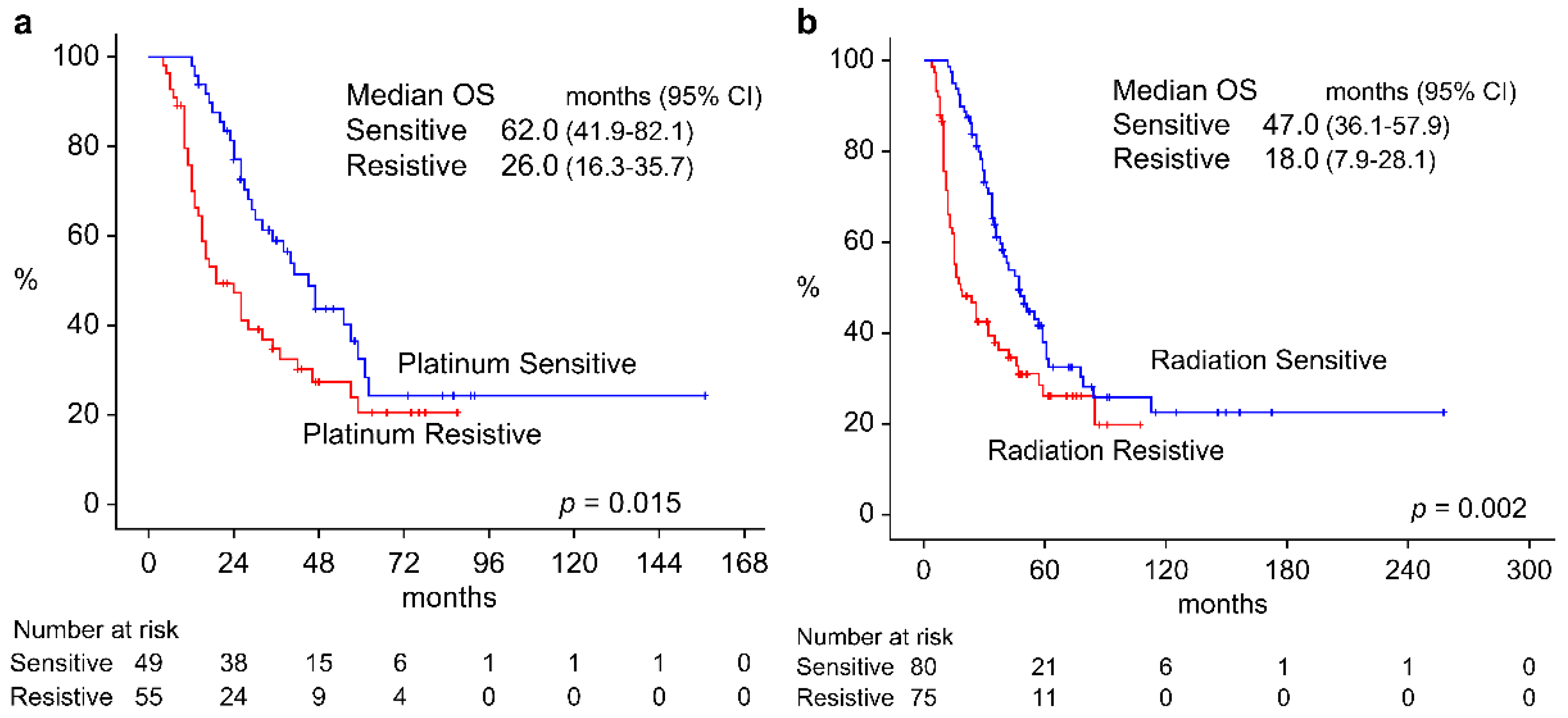
Figure 4.
(a) Survival curves for patients who were margin positive and margin negative. (b) Survival curves for patients with and without extracapsular spread and had pN0. (c) Survival curves for patients who were positive for either pn, ly, or v and patients who were negative for all of pn, ly, and v.
Figure 4.
(a) Survival curves for patients who were margin positive and margin negative. (b) Survival curves for patients with and without extracapsular spread and had pN0. (c) Survival curves for patients who were positive for either pn, ly, or v and patients who were negative for all of pn, ly, and v.
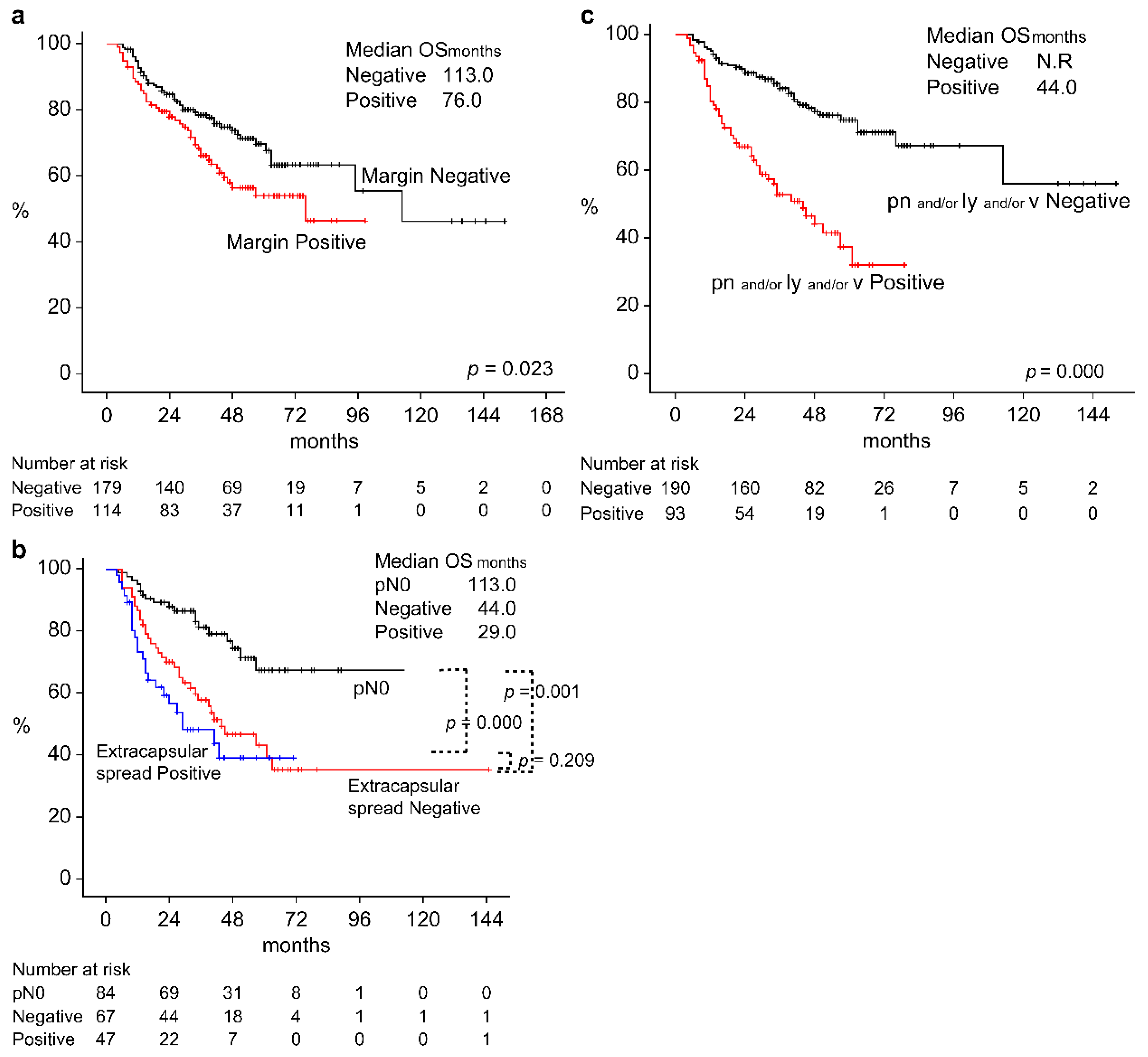

Table 1.
Baseline Characteristics of All Patients (n = 500).
| All (n = 500) |
Recurrence (n = 234) |
p value | |||
| ER (n = 110) |
LR (n = 124) |
||||
| Gender | Male Female |
377 123 |
80 30 |
96 28 |
0.450 (F) |
| Age (years), mean (SD) |
Median |
20–92 (67) |
33–92 (65) |
20–86 (66) |
0.995 (M) |
| Area | Oral cavity Nasopharynx Oropharynx Hypopharynx Larynx Nasal sinus External auditory canal |
145 21 79 113 64 41 37 |
51 2 15 20 7 9 6 |
33 7 16 32 20 12 4 |
0.014 (F) |
| T classification | T1 T2 T3 T4 |
84 162 112 142 |
9 32 20 49 |
23 41 26 34 |
0.003 (M) |
| N classification | N0 N1 N2 N3 |
252 74 155 19 |
44 16 43 7 |
59 12 47 6 |
0.370 (M) |
| P16 | Positive Negative Unmeasured |
48 43 409 |
7 12 91 |
7 10 107 |
0.736 (F) |
| Initial treatment | Surgery alone + chemoradiotherapy (platinum+) + radiotherapy (platinum-) + neoadjuvant chemotherapy (platinum+) Radiotherapy alone chemoradiotherapy (platinum+) chemoradiotherapy (platinum-) |
157 87 39 19 17 147 34 |
30 29 12 5 5 21 8 |
41 17 11 3 4 29 19 |
0.103 (F) |
| Postoperative pathological findings of the surgical therapy group |
Non-surgery group Surgery group Margin Positive Negative Unknown Extracapsular spread Yes No p0 pn, ly, vn Yes No Unknown |
198 302 115 182 5 47 67 88 94 194 10 |
34 76 35 39 2 24 21 15 42 29 4 |
52 72 30 38 3 8 20 13 19 45 4 |
0.103 (F) 0.795 (F) 0.091 (F) 0.002 (F) |
| Multiplicity cancer in other organs | No Yes |
394 106 |
93 17 |
98 26 |
0.313 (F) |
F: Fisher’s exact test; M: Mann–Whitney U test.
Table 2.
Univariate and Multivariate Analyses of Variables for OS in Patients with Recurrence (n = 234).
Table 2.
Univariate and Multivariate Analyses of Variables for OS in Patients with Recurrence (n = 234).
| Variables | OS univariate analysis | OS multivariate analysis | |
| HR (95% CI), p value | HR (95% CI), p value | ||
| Recurrence time | ER: Recurrence in two to six months after treatment (n = 110) LR: Recurrence in more than seven months after treatment (n = 124) |
2.126 (1.509–2.995), p = 0.000 Ref |
3.200(1.570–6.521) p = 0.001 Ref |
| Radiotherapy |
Recurrence in two to six months after radiotherapy (n = 75) Recurrence in more than seven months after treatment (n = 80) Recurrence without treatment (n = 79) |
1.824 (1.237–2.690), p = 0.002 Ref 0.593(0.382–0.923), p = 0.021 |
0.567 (0.232–1.390) p = 0.215 Ref 0.374 (0.191–0.733) p = 0.004 |
| Platinum preparation |
Platinum-resistive recurrence (n = 52) Platinum-sensitive recurrence (n = 54) Recurrence without platinum administration (n = 128) |
1.721 (1.078–2.747), p = 0.023 Ref 0.737(0.488–1.114), p = 0.148 |
0.998(0.501–1.988), p = 0.995 Ref 0.881 (0.535–1.452) p = 0.619 |
| Multiplicity cancer in other organs | No (n = 191) Yes (n = 43) |
Ref 1.387 (0.929, 2.071), p = 0.110 |
- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



