
Submitted:
08 February 2024
Posted:
08 February 2024
You are already at the latest version
Abstract
While some research supports utilizing plain radiography for measuring biomechanical alignment of the spine for prognosis and treatment, there are contrasting viewpoints regarding both the value and utilization of these procedures in conservative care. Evaluation of both conservative and non-conservative approaches to spinal care revealed vast differences in radiographic utilization and interpretation between orthopedic surgeons, primary care physicians, chiropractic physicians, and physical therapists, which may account for the different viewpoints and rationale in the literature. A research summary is provided regarding the various methods of spinal analysis utilized by these professions to help determine if there is any unique diagnostic or prognostic value associated with radiographic utilization that could assist in advancing conservative spinal assessment and treatment. Understanding any unique value provided through biomechanical assessment utilizing plain radiography of the spine established in the literature may help chiropractic physicians determine the appropriate use of radiographic procedures in clinical practice and how to coordinate efforts with other conservative and non-conservative professions to improve spinal healthcare.
Keywords:
Sagittal spinal balance
; coronal spinal balance
; spinal biomechanical assessment
; plain radiography utilization:postural assessment
; spinal assessment
; spinal radiographic parameters:
1. Introduction
Improper spinal balance and alignment has been shown to cause biomechanical dysfunction, which may be an important factor for spinal health and longevity [1,2,3,4,5,6,7]. Altered spinal balance can increase stress to the spine in the form of higher mechanical load and dysfunctional movement patterns, which could contribute to an increased risk of pain, decreased quality of life (QOL) and spinal degeneration [1,3,6,7,8,9,10,11,12].
The global economic impact of musculoskeletal pain is a growing crisis gaining international attention, causing disability in one out of every two individuals affected [13,14]. Neck and low back pain are the most common musculoskeletal conditions and have been the leading causes of years lost to disability in the world over the past several decades [15,16,17,18,19,20]. Interestingly, literature suggests that 85% of all chronic low back pain cases are diagnosed as “non-specific low back pain,” not as a result of injury, but as a result of an unknown cause, typically from spinal biomechanical dysfunction [21]. Given the impact mechanical pain and end stage spinal degeneration has on world health, measurable diagnostic and prevention strategies are essential in conservative care.
While there are many approaches to assess the spine, plain radiography of the spine (PROTS) has long been considered an acceptable diagnostic tool within both conservative and surgical settings [22]. Some literature suggests that in conservative settings, such as primary care physicians, emergency room services and chiropractic care, PROTS should be limited to cases in which red flags are suspected, as PROTS may not have any positive impact on acute care outcomes [23,24,25,26,27]. Other studies suggest that PROTS may have value in conservative spinal care beyond screening for trauma and red flags, in the form of biomechanical assessment [28,29,30,31].
Alterations in spinal biomechanical measurements unique to PROTS have been identified as a risk factor for developing spinal degeneration, and these measurements have demonstrated value in the surgical setting [32,33,34,35,36,37]. Surgical correction of these imbalances has shown to improve long-term outcomes by reducing the risk of adjacent segment disease, decreasing functional disability, and improving QOL of scores [34,38,39,40]. While there is established value in utilizing PROTS in orthopedic surgery, there are varied opinions regarding the utilization and appropriateness of PROTS in clinical practice within the chiropractic profession [28,41,42,43,44,45,46].
This study reviews the literature regarding potential unique value related to biomechanical analysis in PROTS that may be utilized in the conservative management of spinal health. The goal of this review is to a) examine if there is unique value of PROTS in conservative spinal care and b) determine if there is enough evidence to warrant further research regarding radiographic biometric utilization in conservative care settings to better manage mechanical spine pain, prevent spondylosis, and improve spinal health.
2. Data Collection
Methods of spinal assessment were reviewed using literature from PubMed, Index to Chiropractic Literature, and Chiropractic Biophysics (CBPNonprofit.com) with no language or publication year exclusions. The initial searches were completed through July 2023. The authors were interested in the following primary outcomes: (1) quantitative results concerning radiographic evaluation of the spine; (2) method and quality of radiographic measurement; (3) method and quality of non-radiographic measurement. Any published literature involving spinal radiographic measurements and non-radiographic postural assessment in relation to normal parameters, spinal conditions, and treatment outcomes was included in the study. Studies were excluded if they did not contain an accurate description of radiographic evaluation or postural assessment or if they were determined to be redundant or unrelated to spinal assessment.
The search strategy was based on concepts that describe radiographic parameters in relation to normal parameters, asymptomatic patients, symptomatic patients, degenerative changes, and surgical outcomes. For example, studies on normal spinopelvic anatomy were located using terms such as “normal,” “healthy,” or “asymptomatic,” while terms for deformities include “kyphosis”, “cervical lordosis (CL),” “thoracic kyphosis (CK),” “cervical vertical axis (CVA),” “lordosis,” or “scoliosis.” In addition, terms used to describe spinal radiographic parameters included “pelvic incidence (PI),” “pelvic tilt (PT),” “sacral slope (SS),” “T1 Slope (T1S),” “sagittal vertical axis (SVA)” or “parameters” combined with “pre-operative,” “post-operative,” “chiropractic,” and/or “postural correction.” Additional searches were performed based on references in reviewed literature to identify studies potentially eligible for our review. Summary reports of selected studies were divided up evenly between the authors. Disagreements regarding inclusion were resolved by discussion.
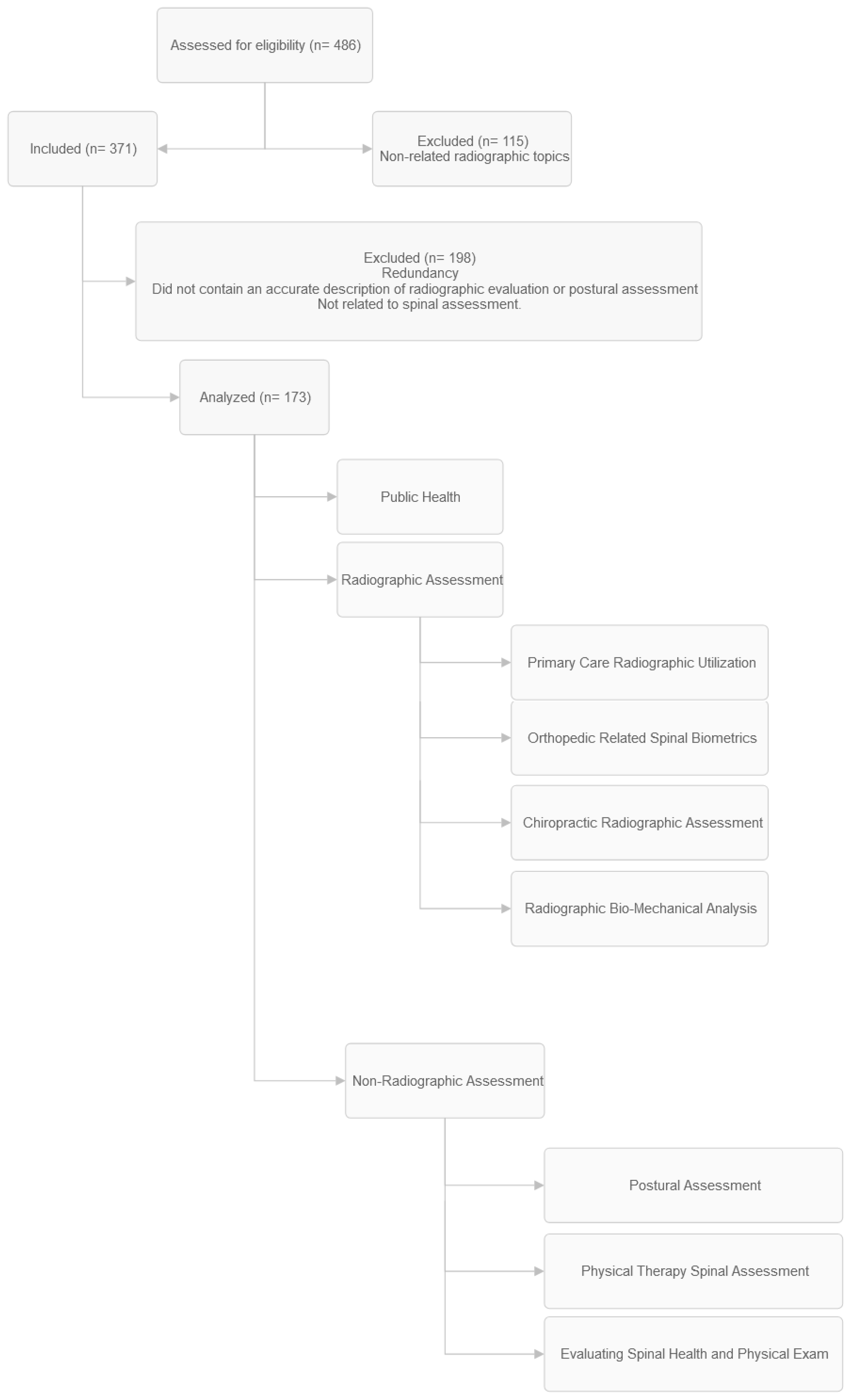
The authors independently sourced articles related to the search criteria. A shared database was created for the authors to collect, import, and review information. Upon discovery of related articles, the authors independently imported the article title, citation, and summary into the database. The full article was then attached as a PDF to the database for review. A total of 486 articles were imported into the database.
The article database was divided equally among the authors for review for inclusion and exclusion. Each article was summarized independently by the respective reviewers in 1-2 paragraph summaries according to the study objectives. These included the following categories: orthopedic/neurology radiology, radiographic method of the spinopelvic parameters assessment, the quantitative characteristics of the spinopelvic parameters (LL, SS, PI, and PT), quantitative characteristics of cervical-thoracic parameters (T1S, TIA, CL, TK, and CVA), primary care, postural assessment, computerized assessment, physical therapy, spine related public health, and physical exam. The information was imported into the database so that all authors would have access to the summaries. Once the summaries were completed and inclusion/exclusion parameters established, the authors collaborated to determine the final inclusion documents. Ultimately, 173 articles were included, and 313 articles were excluded. Included articles ranged from 1990-2023.
Figure 1.
Diagram of data collection.
3. Results
Of the 486 articles that were reviewed, 173 were included. These are divided into 2 main categories: radiographic methods and non-radiographic methods. The non-radiographic category is further divided into postural assessment methods, computerized postural assessment, physical therapy methodology and physical exam. The radiographic methods are further categorized into the following sections: cervical spine assessment, thoracic and pelvic assessment, chiropractic clinical rationale, primary care rationale for radiography, and orthopedic methodology.
3.1. Primary Care Radiographic Utilization
There were 3 publications reviewed related to PROTS in primary care offices [23,24,47]. The literature suggests PROTS for low back pain without indications of suspected serious underlying conditions does not improve outcomes; therefore, primary care physicians should refrain from routine imaging in patients without these red flag indicators. In one study [24] the most common radiographic findings that were reported to patients were the following: discovertebral degeneration (69%), no abnormality (31%), deformity (39%), congenital abnormalities (17%), posterior arch defects (8%), other discovertebral disease (4%), alignment abnormalities (2%), bone formation (1%), sacroiliac disease (1%). There was 1 paper that discussed the use of cervical spine x-rays in an emergency care and triage setting [25].
3.2. Orthopedic Related Spinal Biometrics
Seventeen articles related to radiographic parameters and surgical outcomes published from 2012 to 2022 were included [34,35,36,38,39,40,48,49,50,51,52,53,54,55,56,57,58]. Five articles did not find improved patient outcomes with surgical correction of spinal balance. In the case of single level lumbar fusion, Rhee et al found focal lumbar lordosis and restoration of sagittal balance for single-level lumbar degenerative spondylolisthesis did not yield clinical improvements [57] (see Figure 2; Appendix A). Sielatycki et al. could not correlate a relationship between measured lordosis and outcomes [48]. Kato et al. reviewed 178 pre and post-surgical patients and could not demonstrate any post-surgical association in outcome between those with and without spinal deformity. [49]. Rhee et al stated “Overall, the restoration of focal lumbar lordosis and restoration of sagittal balance for single-level lumbar degenerative spondylolisthesis does not seem to yield clinical improvements but well-powered studies on this specific topic is lacking in the current literature” [57]. Lee et al concluded “Cervical laminoplasty increased the probability of cervical kyphotic alignment. However, cervical sagittal alignment and clinical outcomes were not clearly related.” [52]
A total of 6 articles found correlation between corrected spinal balance and improved patient outcomes. Ochtman et al. concluded “...lower PT (pelvic tilt) was significantly correlated with improved ODI (Oswestry Disability Index) and VAS (visual analog scale) pain in patients with sagittal malalignment caused by lumbar degenerative disorders that were treated with surgical correction of the sagittal balance” [56]. Vialle et al. states “Providing correct sagittal balance by surgical correction of a spinal deformity is of paramount importance. In the short term, it ensures a good position of the fused segment with regard to the gravity plumb line, allowing the best conditions for fusion. In the long term, good sagittal balance facilitates preservation of the adjacent levels” [59]. Radiographic attention to post-surgical lordosis also appears to be related to hip degeneration and may improve long term clinical signs [50]. Ling et al. state that T1 slope, C7 slope and cSVA are the most important radiographic parameters to be analyzed that affect surgical outcome [33]. Aoki et al. suggests post-surgical PI-LL mismatch appears to impact residual symptoms such as low back pain LBP, leg pain and numbness and maintaining spinopelvic balance should be emphasized in spinal surgery [53]. Merrill et al. suggested that in addition to PI-LL mismatch, the PT-TK relationship is an important factor in maintaining sagittal balance. [36] Kim et al. found that “C2-7 sagittal vertical axis and sagittal morphotype of the cervical kyphosis are correlated with HRQoL. Changes in cervical lordosis minus T1 slope correlate to HRQoL improvements.” [34]. One article found patients with 1 or 2 level lumbar total disc replacements with a segmental range of motion (ROM) >5° identified on flexion-extension x-rays had statistically significant better outcomes as seen in Oswestry Disability Questionnaire and Stauffer-Coventry scores [58].
The last article was related to post-surgical spinal biometrics and hip degeneration. It was stated that “PI, SS, and PI-LL were associated with the progression of hip joint narrowing after spinal fusion, especially after fusion of four or more levels.” [50] The articles go on to state “Surgeons need to be aware of the risk of increased hip joint narrowing in patients with a large PI, SS, and PI-LL after fusion surgery.”
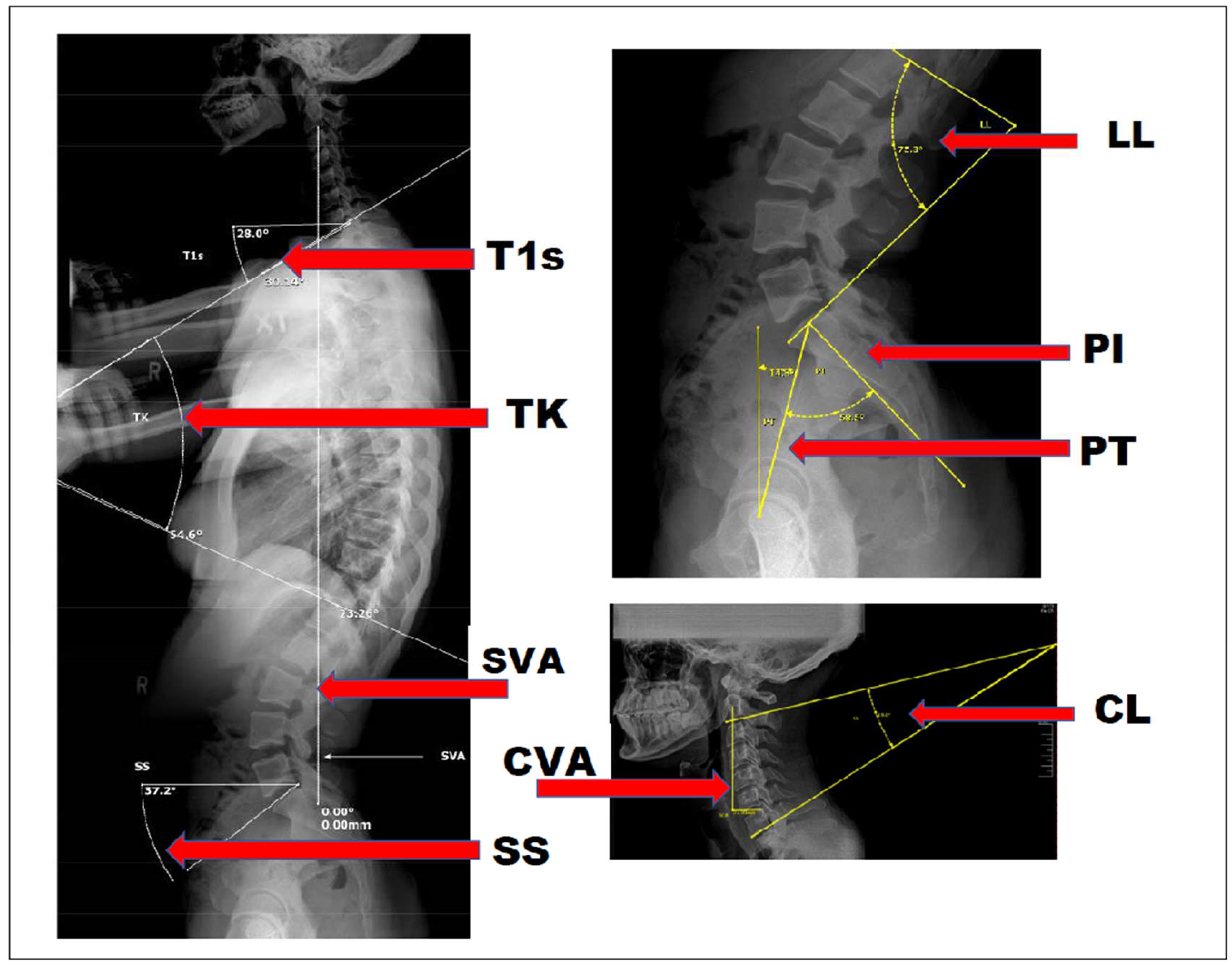
Figure 2.
Radiographic measurements.
3.3. Chiropractic Radiographic Assessment
A total of 19 articles related to chiropractic radiography were reviewed. Of the 19, 4 articles discussed cervical lordosis and/or anterior head translation (AHT) [60,61,62,63]. Saunders et al. stated that head weighting based on cervical radiographs may prove to be a useful therapeutic tool in addressing FHP and the concurrent loss of the normal cervical lordosis [60]. Harrison et al. concluded that cervical traction and spinal manipulation based on cervical radiographs decreased chronic neck pain with improvement of cervical lordosis through segmental and global cervical alignment as well as decreased anterior head weight-bearing [61]. Fortner et al. found that cervical extension traction, extension exercise, and spinal manipulation based on cervical radiographs improved global cervical lordosis, decreased degenerative cervical kyphosis, reduced neck pain and disability, and improved overall health [62]. Wickstrom et al. concluded there was relief of cervical radiculopathy resulting from non-surgical correction of forward head posture and cervical kyphosis based on radiograph interpretation [63]. One article investigated the relationship between the cervical spine and occlusal contacts and found that changes in posture and occlusion can be observed after the NUCCA chiropractic procedure based on radiographic interpretation [64].
Three articles reviewed thoracic hyperkyphosis (THK) [65,66,67], and 2 correlated thoracic hypokyphosis with the physiological relationship to lung functions [68,69]. Oakley et al. concluded thoracic hyperkyphosis may be reduced/corrected by posture-specific, thoracic extension protocols including mirror image extension traction and exercises, as well as spinal manipulation based on PROTS [65]. Miller et al. found that thoracic hyperkyphosis can be reduced through a multimodal rehabilitation program emphasizing mirror image thoracic extension procedures as determined by PROTS [61]. Oakley et al. found successful reduction in thoracic curve by an average of 12° concomitant with the improvement in pain, disability, and quality of life measures, and in some cases, improvement in vital capacity following treatment using the Chiropractic BioPhysics (CBP) technique methods [67]. Betz et al. found nonsurgical correction in thoracic hypokyphosis/straight back syndrome can be achieved by mirror image traction procedures, as well as corrective exercise and manipulation as a part of CBP technique protocols that were consistent with relief of exertional dyspnea and pain [68]. Mitchell et al. concluded that nonsurgical improvement in thoracic kyphosis in a patient with straight back syndrome is possible and that it may positively influence lung capacity, health, and function following a CBP care program [69]. Two articles reviewed the relationship between LBP and lumbar lordosis/flat back syndrome [70,71]. Harrison et al. found lumbar extension traction increased lumbar lordosis, measured by lateral lumbar radiographs, in patients with chronic LBP associated with hypolordosis which is a common factor in LBP [70]. Harris et al. also found that improvement in lumbar lordosis as well as sacral base angle, pelvic tilt and sagittal balance simultaneously reduced pain [71]. Two articles focused on scoliosis specifically with results showing that all patients had a reduction of curvature concomitant with a reduction in pain levels using mirror imaging exercises, traction and spinal manipulative therapy. [72,73] Additionally, 2 focused on the reliability/repeatability of measurements, analysis and radiographic positioning in general and stated that X-ray line drawing is reliable, normal values for the sagittal spinal curvatures exist in the literature, the normal sagittal spinal curvatures are important clinical outcomes of care and patient positioning and postural radiographs are highly reproducible [45,74]. Another 2 suggested PROTS are irrelevant due to not improving outcomes and reasons given for imaging were not supported by evidence [41,43]. Lastly, 1 paper discussed the biomechanical evaluation of posture and alignment, then described the 6 types of subluxation that satisfy Nelson’s criteria that currently underpin the basis for routine radiographic examination for biomechanical data related to the diagnosis and treatment of patients in modern chiropractic practice [75].
3.4. Radiographic Biomechanical Analysis
The review of radiographic biomechanical analysis included 56 studies (see Table 1: Radiographic Biomechanical Analysis Studies). Regarding specific forms of spinal biometrics, there were a number of categories that were identified for the purpose of this section. Several of these categories were highly represented across multiple disciplines; these measurements appeared to be more global in nature and concentrated in the sagittal plane. The number of articles referencing these topics is as follows: sagittal vertical axis: 34, cervical lordosis / T1 slope / cranio-cervical angle: 23, anterior head translation: 28, absolute rotational angle: 26, thoracic kyphosis: 15, sacral base angle / lumbar lordosis / pelvic incidence: 18, cobb method and gore methods: 11 (see Table 1, Sagittal Categories). Lee et al. findings were as follows: “T1 slope was a key factor determining cervical spine sagittal balance. Both spinopelvic balance and TI (thoracic inlet) alignment have a significant influence on cervical spine sagittal balance via T1 slope, but TIA (thoracic inlet angle) had a stronger effect than TK (thoracic kyphosis). An individual with large T1 slope required large CL (cervical lordosis) to preserve physiologic sagittal balance of the cervical spine. [76] Additionally, global and sagittal balance are correlated with quality of life and inferior surgical outcome with the most significant measurements being sagittal C7 plumbline and gravity line effecting ODI [1]. Compared to U.S. norms, the Generational decline in physical component summary (PCS) score was more rapid in symptomatic adult spinal deformity patients with no other reported comorbidities. Specifically, PCS scores for patients with isolated thoracic scoliosis were similar to values reported by individuals with chronic back pain, while patients with lumbar scoliosis combined with severe sagittal malalignment demonstrated worse PCS [77]. Global measurements in the frontal /coronal (AP) plane were markedly less represented in the collated topics. The number of articles referencing these topics are as follows: Frontal Vertical Axis: 7, Idiopathic Scoliosis: 6, Pseudo-scoliosis: 1, and Cobb Angle: 6 (see Table 1: Coronal Plane). However, the interesting nexus of sagittal spine balance and frontal/coronal plane balance was found by Ma et al. Their conclusions were as follows: “A basic goal in the treatment of spinal deformity is to achieve proper alignment. To achieve this purpose, the surgeon must pay attention to global spinal balance. The following main points can be concluded from the data of this investigation. Children with AIS [Adolescent Idiopathic Scoliosis] showed signs of increased pelvic tilt and decreased TK. In AIS, coronal balance is correlated to sagittal balance. We believe coronal balance and sagittal balance are equally important for decision-making when dealing with AIS” [78].
Segmental spinal biometrics was also dominated by measurements in the sagittal plane, although to a less significant degree. These topics included Relative Rotational Angle: 13 and Georges Line: 1 (see Table 1: Sagittal Categories). When conditions were the focus of the article, the conditions were as follows. The number of articles referencing the condition follows the condition: Spondylosis / DJD / DDD / Central Canal Stenosis / Myelopathy: 17, Spinal Related Pain / Radiculopathies: 15, Headaches: 3, Idiopathic Scoliosis: 5, Pseudo scoliosis: 1, Spondylolithesis: 1, Vertigo: 1, and TMJ: 1 (see Table 1: Conditions).
When considering the above delineated conditions, predictive measuration of sagittal alignment appears to dominate the research, although not exclusively. Xing et al. found: “T1S (T1 Slope) was involved in the occurrence and development of cervical disc degeneration, and TIA could be considered as a constant morphological parameter in both the normal population and cervical disc degeneration patients” [79]. Additionally, Sun et al. found that: “The study showed that T1 slope less than 18.5° was an independent risk factor for DCSM, which means that cervical spine sagittal im balance aggravates as the T1 slope becomes smaller, which may increase the incidence of DCSM” [5]. The findings were similar for the lumbar spine as reported by Keorochana, et al.: “Changes in sagittal alignment may lead to kinematic changes in the lumbar spine. This may subsequently influence load bearing and the distribution of disc degeneration at each level. Sagittal alignment, disc degeneration, and segmental mobility likely have a reciprocal influence on one another” [8]. Clinical interventions for the conditions listed were as follows. The number of articles referencing the topic were: Therapeutic Exercises: 13, Spinal Manipulation: 12, Corrective Spinal Traction: 12, and Spinal Surgery: 6 (Table 1: Treatments). Those that showed clinical and or structural improvements included: Lordosis or Kyphosis improvement: 10, symptomatic improvements: 9, telomere length: 1 (see Table 1: Improved Symptoms / Quality of Life).
3.5. Non-Radiographic Spinal Assessment
Twenty articles were reviewed on non-radiographic methods to assess spinal alignment. Measurements included, but were not limited to: forward head posture, tragus wall distance, scoliosis, craniovertebral angle, thoracic kyphosis, natural head position, cervical and lumbar curve, sagittal head tilt, and sagittal shoulder-C7 angle (see Appendix B). Four articles were directly relating to visual assessment from photography or mobile app [80,81,82,83]. Singla et al. found several methods that were reliable to measure various postures [80]. Bryan et al. found visual postural assessment had a high interrater reliability but have low validity utilizing visual assessment for lumbar lordosis using photographs of clothed subjects [81]. Boland et al., utilizing the PostureScreen Mobile® app, found substantial to almost perfect (ICC≥0.81) inter-rater and intra-rater agreement [82]. Stolinski et al. demonstrated good repeatability and reproducibility and checked validity against the Rippstein plurimeter measurements [83].
Seven articles addressed visual assessment of body and spinal posture [84,85,86,87,88,89,90]. The tragus wall distance was found to have high intra-rater reliability, but the measurement of a single patient by multiple raters was not supported [84]. Fedorak et al. concluded that “Intrarater reliability of the visual assessment of cervical and lumbar lordosis was statistically fair, whereas interrater reliability was poor” [85]. Nam et al. found that the assessment of forward head posture was reliably measured between two physical therapists [86]. Yanagawa et al. found that using the Flexicurve for the assessment of thoracic kyphosis showed the reliability being high for kyphosis height, but the reliability for kyphosis length was less (ICC value of .54) [87]. Dunn et al. reported that confirmation x-ray was needed for adult idiopathic scoliosis severity rather than solely relying on screening results [88]. Lundström et al. found that trained observer analysis of natural head position and correct head orientation without x-ray can be reliable and intraobserver reliability is often high [89]. Yip et al. found that the craniovertebral angle in subjects with neck pain was smaller than in normal subjects [90]. Seven articles addressed the validity of various measurement systems for body posture assessment [81,91,92,93,94,95,96].
A literature review from Fortin, et al. found that most of the studies showed good intra- and inter-rater reliability for measurements taken directly on the person or from photographs, but the validity of the measurements was not always demonstrated [91]. Goldberg et al. concluded that the Quantec system can be useful for monitoring patients as an alternative to radiography, but for the ascertainment of Cobb angles the two systems are not measuring the same aspect of the deformity [92]. Fortin et al. found that: “The correlation between 2D and 3D indices was good to excellent for shoulder, pelvis, trunk list, and thoracic scoliosis (0.81 r 0.97; P 0.01) but fair to moderate for thoracic kyphosis, lumbar lordosis, and thoracolumbar or lumbar scoliosis (0.30 r 0.56; P 0.05). The correlation between 2D and radiograph spinal indices was fair to good (0.33 to 0.80) with Cobb angles and 0.76 for trunk list; P 0.05)” [96]. Tools such as the flexi-curve (also known as a flexi-ruler) [87] have been demonstrated to be invalid in the cervical and lumbar region, as they do not accurately represent the total angle of the curve, its shape, or its magnitude [93,94,95]. In the thoracic spine, these methods are reliable and valid [95]. Two articles were focused on devices to measure curvatures of the spine, a surface topography DIERS formetric 4D [97] and the spinal mouse [98]. One article was specific to sitting posture and its effects on musculoskeletal and pulmonary function [99].
3.6. Physical Therapy Spinal Assessment
Eleven articles were assessed identifying methodologies utilized by physical therapists in practice to identify and define spinal health. Two articles focused on how and when physical therapists use diagnostic imaging [100,101]. This indicated that when physical therapists do order diagnostic imaging, it is often used to make decisions about whether or not the condition is in the therapist's scope of practice, whether or not to refer out, and when to co-manage conditions with other healthcare providers [100,101]. Two studies did not use diagnostic imaging. One of these studies investigated the use of an ergonomic training program in conjunction with strengthening and stretching exercises on chronic LBP patients. Posture was analyzed utilizing the Zebris WinSpine Pointer Posture method, which quantifies thoracic kyphosis and lumbar lordosis [102]. One was a mini-review of the literature regarding postural re-education in the treatment of scoliosis [103].
Seven articles did use diagnostic imaging. Four articles investigated the use of treatment protocols based on factors found through radiographic examination, with AHT, SVA, C7P, TK, LL, and SS being of particular importance [104,105,106,107,108]. Of these 4 articles, 3 investigated lower back pain treatment protocols utilizing SVA, C7P, LL, and SS as defined through radiograph to quantify treatment outcomes with ODI to validate results. One study investigated the treatment of lumbosacral radiculopathy, with the addition of AHT corrective exercises analyzing LL, ODI scoring, back and leg pain, Modified Schober Test, and latency and amplitude of H-reflex (a diagnostic criteria for lumbosacral radiculopathy [106]. One of the studies investigated rehabilitation of patients with suspected cervicogenic dizziness, loss of cervical lordosis (CL) and AHT as defined by radiographic examination, and Head Repositioning Accuracy (HRA) deficiencies as defined by the CROM device [104]. Two of the articles investigated treatment of scoliosis, utilizing radiographic examination to define the magnitude of the scoliosis as measured by the Cobb Angle Method [105,109]. Within the reviewed literature above, the radiographic assessment of C7P [108], CVA [105], CL [104], TK [103,105], LL [110], and SS [108] did appear to have clinically significant impacts on patient outcomes.
3.7. Non-Radiographic Spinal Evaluation Utilizing Physical Exam
Three articles discussed physical exams. There was 1 article that looked at effects of passive motion analysis and mobilization on cervical lordosis, ROM, and forward head posture on patients who displayed problems in cervical posture [111]. One study examined patients with cervical radiculopathy using orthopedic and neurological tests such as Valsalva’s maneuver, cervical distraction, Spurling’s or upper limb tension test. These values should be interpreted with caution in the absence of any other clinical information due to the lack of primary studies investigating the accuracy of these tests [112]. The last study that looked at physical exams evaluated 15 articles that met their inclusion criteria for manual assessment of cervical spine dysfunction. It found that there was methodological weakness in their interpretation of reference standards such as radiography, diagnostic nerve block and reported pain from the subject, as well as in the representative study population [113].
4. Conclusions
An estimated 85% of all chronic low back pain cases are diagnosed as “non-specific low back pain,” otherwise known as mechanical low back pain [21]. Altered spinal balance can increase stress to the spine in the form of higher mechanical load and dysfunctional movement patterns, which may contribute to an increased risk of pain and degeneration [8]. Given the impact mechanical spine pain and end stage spinal degeneration has throughout the world, measurable diagnostic, treatment, and prevention strategies may be of benefit in the conservative setting. PROTS has long been considered an acceptable diagnostic tool within both conservative and surgical settings for detecting trauma, red flags, and measuring spinal alignment [22,37]. However, some suggested clinical guidelines for conservative practitioners recommend PROTS be limited to only evaluation for trauma and red flags, without biomechanical assessment or intervention [41,42]. The aim of this study was to review the literature to determine if biomechanical analysis in PROTS may add unique value in the conservative management of spinal health, in addition to screening for trauma and red flags.
This review included 173 articles. Three publications were related to PROTS in primary care offices. Collectively, these publications suggest PROTS for low back pain without indications of suspected serious underlying conditions are not clinically valuable; therefore, primary care physicians should refrain from routine imaging in patients without these red flag indicators. This may partially be due to a) research suggesting radiographs for acute, non-traumatic pain does not change outcomes within the first six weeks [23,24,41]; b) PROTS does not alter the treatment plan in primary care settings [23,47,114]. There are limitations to these studies; despite the importance of spinal balance, radiographic reporting rarely includes any mention of spinal biomechanical abnormalities, with only 2% of reports including comments on alignment abnormalities [24]. Additionally, no specifics were given in regard to the evaluation, treatment strategies, or education level of the physical therapists and chiropractic doctors involved in the patient care in the above studies. Therefore, without comparing manual therapy approaches utilizing PROTS vs not utilizing PROTS, no conclusion can be made on the value of PROTS in the management of acute care patients.
One article discussed the use of cervical spine x-rays in an emergency care and triage setting [25]. Within this study, the Canadian C-Spine Rule was developed as a highly sensitive decision rule for use of C-spine radiography in alert and stable trauma patients in emergency departments (EDs) with 100% sensitivity and 42.5% specificity. The goal of this study was to investigate ways to reduce practice variation and inefficiency in EDs use of C-spine radiography. Considering that the primary focus in EDs is immediate lifesaving or life preserving intervention, this C-spine rule for important C-spine injuries (fracture, ligamentous instability) in the EDs is appropriate. Nevertheless, the C-spine rule neglects postural and biomechanical alterations that may result in mechanical spine pain and/or degenerative changes, and therefore may not be appropriate in conservative care settings that manage mechanical spine problems and long-term spinal health.
Fifty-six studies related to radiographic biometrics were included in this study. The number of studies on sagittal biometric values are as follows (some studies included multiple biometric values): sagittal vertical axis (n=34), cervical lordosis / T1 slope / cranio-cervical angle (n=23), anterior head translation (n=28), absolute rotational angle (n=26), thoracic kyphosis (n=15), sacral base angle / lumbar lordosis / pelvic incidence (n=18), cobb method and gore methods (n=11) (see Table 1). Collectively, it appears sagittal biometrics measured with PROTS may have some predictive value. Sheikh et al. stated “Significant associations were found between satisfaction and disability and global coronal and sagittal (sagittal vertical axis [SVA]) alignment.” [115] They later concluded “The ability to restore global alignment depends on the severity of the preoperative deformity as well as the correction of the main aspect of the deformity. Achieving global coronal and sagittal alignment is an independent predictor of both satisfaction and disability at 2 years post-op.” This suggests that the early correction of SVA prior to surgery may improve post-surgical outcomes, but more research is needed to confirm this.
Specifically for the cervical spine, the T1 slope relates directly to cervical sagittal balance, as an individual with a large T1 slope requires large cervical lordosis to preserve physiologic sagittal balance of the cervical spine [76,116,117]. Altered T1 slope has been shown to be a predisposing factor in degenerative cervical spondylotic myelopathy (DCSM) [118]. According to Sun et al.: “… T1 slope less than 18.5° was an independent risk factor for DCSM [Degenerative Cervical Spondylotic Myelopathy], which means that cervical spine sagittal imbalance aggravates as the T1 slope becomes smaller, which may increase the incidence of DCSM” [5]. The authors also state T1 slope is “the only parameter showing significant correlation with both spinopelvic balance and TI alignment, which means it is an important parameter influencing TI alignment and spinopelvic balance” [5]. Though currently, to the present study’s authors’ knowledge, there are no studies displaying the ability to non-surgically influence T1 slope; the value potentially lies in the encouragement of preventive strategies--such as exercise and postural awareness--to reduce the risk of DCSM in patients with T1 slope less than 18.5°.
Additional evidence has shown sagittal balance involves numerous parameters, including pelvic tilt, thoracic kyphosis, and cervical lordosis with various compensations seen throughout the spine and pelvis when these measurements deviate from normal values [36]. The complex multifactorial mechanisms associated with the development of symptomatic spondylosis (e.g., age, genetics, spinal balance, segmental motion, previous injuries, occupational status, hydration level) create challenges in predicting the rate and effect of development [119]. These articles suggest that biometric values measured in PROTS may have some predictive value for the development of spondylosis, and further studies should be conducted to determine a) whether changing these parameters reduces the rate of symptomatic spondylosis and b) if abnormal biometrics, coupled with other risk factors, offer better predictability of developing symptomatic spondylosis.
Six systematic review articles related to biometrics and post-surgical outcomes published from 2015 to 2022 were included in this review [33,34,37,38,56,57]. Ochtman et al. concluded “...lower PT (pelvic tilt) was significantly correlated with improved ODI (Oswestry Disability Index) and VAS (visual analog scale) pain in patients with sagittal malalignment caused by lumbar degenerative disorders that were treated with surgical correction of the sagittal balance” [56]. However, in the case of single level lumbar fusion, Rhee and colleagues found focal lumbar lordosis and restoration of sagittal balance for single-level lumbar degenerative spondylolisthesis did not seem to yield clinical improvements [57]. As we see in these examples, orthopedic literature is not trying to determine whether or not PROTS is valuable, but rather where the value in PROTS is greatest.
Three of the 6 articles were in relation to cervical sagittal balance and post-surgical outcomes, two of which found that sagittal alignment is associated with quality of life scores while the third concluded that restoration of cervical lordosis may decrease the incidence of adjacent segment disease [33,34,38]. The 6th and final study discussed the overall importance of spinopelvic alignment considerations, stating, “It is essential to accurately assess and measure these sagittal values to understand their potential role in the disease process, and to promote spinopelvic balance at surgery” [120]. Given that assessment of spinopelvic alignment is important in surgical planning and surgical approach to spinal correction, it is reasonable that greater utilization of these factors be incorporated into conservative spinal care.
Additionally, outside of traditional standard views, when reviewing patients with 1 or 2 level lumbar total disc replacements, it was found that a range of motion (ROM) >5° identified on flexion-extension x-rays had statistically significant better outcomes as seen in Oswestry Disability Questionnaire and Stauffer-Coventry scores [58]. As the trend in orthopedic research is to utilize normal values in assessment for surgery, the potential to utilize these measures in non-surgical patients highlights the importance of implementation in conservative spinal care as well. With orthopedics leading the way, more research is needed to investigate PROTS in conservative spinal care for improved segmental motion preservation and long-term patient outcomes.
Twenty articles were reviewed on non-radiographic methods to assess spinal alignment. Measurements included, but were not limited to: forward head posture, tragus wall distance, scoliosis, craniovertebral angle, thoracic kyphosis, natural head position, cervical and lumbar curve, sagittal head tilt, and sagittal shoulder-C7 angle (see Appendix B). There are mixed results regarding the validity of non-radiographic spinal assessment. Fedorak et al. concluded that “Intrarater reliability of the visual assessment of cervical and lumbar lordosis was statistically fair, whereas interrater reliability was poor” [85]. Meanwhile, Lundström et al. suggested that trained observer analysis of natural head position and correct head orientation without x-ray can be reliable and intra-observer reliability is often high [89]. Nam et al. found that there was high inter-rater and intra- rater reliability for visual evaluation of forward head posture and suggests that computer assessment helps to increase the value and reliability [86].
Computerized and instrumented postural assessments have been shown to have value, though some studies suggest these tools lack specificity when compared to radiographic evaluation. Tools such as the flexi-curve (also called flexi ruler) have been demonstrated to be invalid in the cervical and lumbar region, as they do not accurately represent the total angle of the curve, its shape nor magnitude [93,94,95]. Similarly, posture analysis (specifically with a mobile application), while beneficial as an indicator of postural abnormality, is neither accurate for true measurement of internal spinal angles and measurements, nor adequate for spinal correction [82,90]. While useful, non-radiographic postural analysis does not provide accurate, quantitative measures on the cumulative, causative factors that may be contributing to sagittal and global balance, such as PT-TK mismatch, PI-LL mismatch, decreased CL, Cervical Kyphosis, T1s, TIA, SVA, PT, SS, or PIA, which can only be accurately measured via PROTS.
Furthermore, other literature suggests PROTS may be able to identify biomechanical imbalances sooner than visual postural assessments in some cases, as the underlying spinal deformity must progress to a higher level of severity before significant postural changes can be observed. For example, anterior head translation (AHT) and a thoracic hyperkyphosis (THK) can be visualized without radiographs and used as predictors for increased spinal pain and headaches [87,111]. However, even in the absence of AHT, loss of cervical lordosis has been associated with altered cervical kinematics which may contribute to the development of spinal degeneration and reduced HRQOL scores [29,121]. Once cervical kyphosis begins, the deformity tends to perpetuate itself, shifting the head forward and inducing abnormal forces throughout the cervical spine that further progress the deformity [122]. Considering loss of cervical lordosis may increase the progression of cervical spondylosis, early detection and correction of cervical lordosis may reduce risk of future surgical need and improve spinal longevity; however, more research is needed to confirm this correlation.
Eleven articles were assessed identifying methodologies utilized by physical therapists in practice to identify and define spinal health. Historically, the trend in physical therapy for evaluating spinal balance has not included PROTS, as this is not within the scope of practice of physical therapy [100,101]. However, due to limitations in postural assessment, there has been increasing literature in physical therapy that suggests PROTS could be valuable in physical therapy practice [100,101,104,105,106,107,108]. Some literature suggested value in PROTS in the form of treatment protocols, with AHT, SVA, C7P, TK, LL, and SS being of particular importance [104,105,106,107,108]. Within this reviewed literature, the radiographic assessment of C7P [108] CVA [105], CL [104], TK [103,103], LL [110], and SS [108] did appear to have clinically significant impacts on patient outcomes.
Evidence continues to surface that conservative spine care may be able to improve biomechanical imbalances that are identified in postural screening and PROTS [60,64,103,105,106,109,123,124]. For example, correcting abnormal thoracic kyphosis has been achievable, which may negate the negative effects of abnormal sagittal balance of the thoracic spine, such as decreased HRQOL, increased risk of falls, decreased forced expiratory volume in the first second, and complications of osteoporosis [65,66,67,68,69,125]. Oakley et al. published a retrospective case series of 10 patients that “demonstrated an average reduction in hyperkyphosis of 11.3° over an average of 25 treatments, over an average of 9 weeks, with a reduction in pain levels and disability ratings” [65].
Conservative practitioners trained in the correction of spinal imbalances have also shown success in the correction of cervical lordosis and forward head posture, thus improving balance, dizziness, radicular symptoms, headaches, and neck pain in many cases [29,60,61,62,63,104,126,127,128,129,130,131,132,133,134]. Moustafa et al. found the addition of forward head posture correction to a functional restoration program seemed to positively affect disability, 3-dimensional spinal posture parameters, back/leg pain, and S1 nerve root function of patients with chronic discogenic lumbosacral radiculopathy [106]. The changes in forward head posture in lumbar radiculopathy management outcomes in experimental and control groups were demonstrably improved radiographically in the intervention group vs. the non-intervention group [106]. Lumbar radiographic parameters have been shown to be correctable as well in conservative treatment, with decreases in lumbar radiculopathy and mechanical back pain and increases in HRQOL scores [70,71,107,108,110].
Interestingly, the literature suggests that 69% of primary finding in radiographic studies is discovertebral degeneration [24]. This poses a clinical challenge: there is conflicting evidence regarding the relationship of degenerative changes and spine pain, as imaging findings of spine degeneration are present in high proportions of asymptomatic individuals, which increases in prevalence with age [24,135,136,137,138,139]. Conversely, a 2015 systematic literature review and meta-analysis utilizing MRI demonstrated a greater incidence of symptoms in the presence of disc disease and spondylosis in symptomatic versus asymptomatic adults 50 years of age or younger [139]. Meanwhile, a 2022 study found no association between “age-inappropriate” and “age-appropriate” disc degeneration in terms of LBP [138]. However, this study has 2 major limitations that affect the strength of their conclusion: a) the overall prevalence of LBP onset was relatively low, as subjects were drawn from routine health examinations and b) the Disc Degeneration Disease (DDD) score utilized in this study is recorded as the sum of all 5 lumbar levels, which allows for a severely degenerated segment to be rated as mild if combined with 4 mildly degenerated discs, thus reducing the discriminative power of the LBP diagnosis.
Regardless of the presence or absence of pain, disc narrowing increases the risk of stenosis and/or radicular compression, zygapophyseal degeneration, motion segment laxity, decreased ROM, and facetogenic pain [140,141,142,143,144,145,146,147]. Furthermore, disc degeneration leads to nerve innervation in growth beyond the outer third of the annulus fibrosis into the inner two thirds [148]. This phenomenon, which increases with degeneration severity, may make the disc more susceptible to nociceptive stimulation, increasing the risk of experiencing discogenic back pain. It is important to note, however, that imaging is only one component of diagnostic testing and needs to be utilized with other diagnostic tests and physical exam findings in order to determine the proper pain generator and appropriate patient management.
Literature suggests that the utilization of PROTS may have unique value in the management of spine health, in addition to screening for red flags, through the evaluation of spinal parameters. However, there is limited comparative research between postural assessment and radiographic assessment for the correction of spinal imbalance and any beneficial outcomes that may exist. There are limited high quality studies showing improved long-term health outcomes between patients demonstrating spinal correction as measured utilizing plain radiography compared to patients with "non-corrected" spinal imbalances. Additionally, longitudinal health studies also present challenges, as there are many parameters that can affect health long-term. Most conservative research focuses on very few evidence-based techniques that are contributing considerable amounts of research at their own expense.
Although there is research showing that PROTS utilized within the first 6 weeks of conservative care in a primary care physician’s office for acute, non-traumatic spine pain does not improve outcomes, the potential value in PROTS may lie in early detection of spinal imbalance, potentially guiding long-term prevention and management strategies [23,114]. Although newer published research is showing a significant genetic component to disc pathology (29%-75%), the environmental factors which can be controlled (smoking, ergonomics, BMI, strength and mechanics) may be of more importance to those genetically susceptible to disc pathology, including spinal balance [119]. Therefore, the primary care guidelines restricting the use of PROTS to only suspected red flags may not be appropriate for conservative practitioners who base care on spinal biomechanics and alignment, such as the physical therapy and chiropractic professions. Future collaborative research between chiropractic, physical therapy, and orthopedic institutes should focus on how conservative practitioners might be able to better utilize PROTS to adequately assess and non-surgically improve spinal alignment, measure the extent of improvement, short term and long-term outcomes of improvement, and whether early improvement of spinal balance can reduce risk developing mechanical spine pain and spondylosis.
This paper describes important evidence on the usage of radiographic assessment. Like all studies, it does have limitations. Articles were not all obtained using systematic review protocols but relied, in part, on snowball sampling relevant articles. Given the depth of published literature on PROTS and the breadth of the topic, this was not an exhaustive review of all literature available. The authors felt it pertinent to determine if enough evidence was available to support further research on the utilization of PROTS for biomechanics analysis in conservative spinal care for better patient outcomes. There is limited research on patient outcomes when utilizing radiographs for biomechanical analysis compared to non-radiographic assessment. As a result, while there is extensive research on the biomechanical parameters unique to radiographs, it is difficult to determine the value this may provide in conservative care. There are also limited studies on the ability of conservative to demonstrate correction of radiographic parameters. Questions remain surrounding the inter and intra practitioner standardization and repeatability of radiographic assessment. Additionally, there are many lifestyle and environmental factors that affect patient outcome that make it difficult to demonstrate improved outcome as a result of correcting the biomechanical alterations recorded with radiographic procedures. Despite limitations, there appears to be enough evidence that encourages further investigation regarding the utilization and values of radiographic analysis in conservative care.
Plain radiography of the spine (PROTS) may provide a unique value in the assessment of spinal health correlations between radiographic measurements including, but not limited to, T1 slope, thoracic inlet angle, sagittal vertical axis, cervical lordosis, pelvic incidence angle, lumbar lordosis, pelvic tilt- thoracic kyphosis mismatch, pelvic incidence-lumbar lordosis mismatch, cervical vertical axis, and sacral slope are well documented in the literature as potential predictive indicators of future spinal degeneration, functional disability and quality of life scores. While non-radiographic postural observation demonstrates value, various parameters cannot be adequately measured without the utilization of plain radiography. Considering current suggested primary care guidelines do not include biomechanical considerations, the recommendation to limit PROTS to trauma and red flags may not be appropriate for all conservative spinal healthcare professionals. The orthopedic approach of utilizing PROTS for biomechanical assessment may be more appropriate for conservative care practitioners, such as the chiropractic profession, with the goal of measuring, predicting, and improving spinal health.
There is increasing literature available demonstrating the ability of chiropractic care and rehabilitative procedures to improve radiographic parameters. Considering the impact of improper spinal biomechanics on spinal health, future collaboration between orthopedic and conservative practitioners, such as the chiropractic profession, could provide benefit from utilizing radiographic biomechanical analysis in order to non-surgically improve spinal biometrics that are associated with spinal health.
The research associated with the value of PROTS should encourage the chiropractic profession to adopt the orthopedic model of radiographic utilization, which remains focused on measuring and correcting spinal parameters. More research is needed within the conservative care professions regarding the utilization and improvement of spinal biomechanical parameters (as currently emphasized in orthopedic literature) and its effect on treatment and long-term benefit to patient health outcomes.

Table 1.
Radiographic Biomechanical Analysis Studies.
| Article | Citation # | Sagittal Plane Methods: Sagittal Vertical Axis /Cobb Method / Gore Method / Georges Line / Absolute Rotational Angle | Sagittal Cervical / Thoracic Kyphosis: Cervical Lordosis / T1 Slope / C7 Slope Spino-Crainio Angle / Anterior Head Translation / Cervical Lordosis Improvement | Sagittal Lumbar / Pelvic Lordosis: Sacral Base Angle / Pelvic Incidence | Coronal Plane: Fontal Vertical Axis / Idiopathic Scoliosis / Pseudo-Scoliosis | Treatments: Spinal Manipulation / Spinal Traction / Therapeutic Exercise | Conditions: Spinal Pain / Radiculopathy / Spondylolesthesis / DJD / DDD / Central Canal Stenosis / Myelopathy | Spinal Surgery | Improved Symptoms / Quality Of Life |
|---|---|---|---|---|---|---|---|---|---|
| Region | Cervical, Thoracic, Lumbar, Pelvis | Cervical, Thoracic | Lumbar, Pelvis | Cervical, Thoracic, Lumbar, Pelvis | Cervical , Thoracic, Lumbar , Pelvis | Cervical , Thoracic, Lumbar | Cervical, Thoracic, Lumbar | Cervical, Thoracic, Lumbar | |
| Banno T, Togawa D, et al. (2016) | [149] | Yes | Yes | ||||||
| Berger RJ, Sultan AA, et al. (2018) | [32] | Yes | Yes | Yes | Yes | ||||
| Bess S, Line B, et al. (2016) | [77] | Yes | Yes | Yes | |||||
| Chun SW, Lim CY, et al. (2017) | [10] | Yes | Yes | Yes | |||||
| Daffin L, Stuelcken MC, et al. (2019) | [150] | Yes | |||||||
| de Schepper EI, Damen J, et al. (2010) | [151] | Yes | |||||||
| Fedorchuk C, Lightstone DF, et al. (2017) | [126] | Yes | Yes | Yes | Neck Pain, Lower Back Pain, Telomere Length | ||||
| Fedorchuk C, Lightstone DF, et al. (2017) | [152] | Yes | Yes | Yes | Yes | Yes | Lower Back Pain | ||
| Ferrantelli JR, Harrison DE, et al. (2005) | [127] | Yes | Yes | Yes | Neck Pain, Headaches, Lower Back Pain | ||||
| Fortner MO, Oakley PA, et al. (2017) | [125] | Yes | Yes | Yes | Yes | Neck Pain, Headaches | |||
| Fortner MO, Oakley PA, et al. (2018) | [128] | Yes | Yes | Yes | Yes | Dizziness | |||
| Fortner MO, Oakley PA, et al. (2018) | [129] | Yes | Yes | Yes | Yes | Neck Pain, Headaches, Lower Back Pain | |||
| Glassman SD, Bridwell K, et al. (2005) | [11] | Yes | Yes | ||||||
| Harrison DE, Cailliet R, et al. (1999) | [2] | Yes | Yes | Yes | |||||
| Harrison DE, Cailliet R, et al. (1999) | [153] | Yes | |||||||
| Harrison DE, Cailliet R, et al. (1999b) | [154] | Yes | Yes | ||||||
| Harrison DE, Cailliet R, et al. (2002) | [130] | Yes | Yes | ||||||
| Henshaw M, Oakley PA, et al. (2018) | [155] | Yes | Yes | Yes | Lower Back Pain | ||||
| Jaeger JO, Oakley PA, et al. (2018) | [123] | Yes | Yes | TMJ | |||||
| Kang JH, Park RY, et al. (2012) | [156] | Yes | Yes | ||||||
| Keorochana G, Taghavi CE, et al. (2011) | [8] | Yes | Yes | Yes | |||||
| Moustafa IM, Diab AA, et al. (2018) | [131] | Yes | Yes | Yes | Yes | ||||
| Knott PT, Mardjetko SM, et al. (2010) | [157] | Yes | Yes | Yes | |||||
| Labelle H, Roussouly P, et al. (2005) | [158] | Yes | Yes | Yes | |||||
| Lamartina C, Berjano P (2014) | [159] | Yes | Yes | Yes | |||||
| Lee SH, Kim KT, et al. (2012) | [160] | Yes | Yes | ||||||
| Lee SH, Son ES, et al. (2015) | [76] | Yes | Yes | Yes | |||||
| Ling FP, Chevillotte T, et al. (2018) | [33] | Yes | Yes | ||||||
| Liu S, Lafage R, et al. (2015) | [161] | Yes | Yes | Yes | |||||
| Ma Q, Wang L, et al. (2019) | [78] | Yes | Yes | ||||||
| Mac-Thiong JM, Transfeldt EE, et al. (2009) | [1] | Yes | |||||||
| Maruyama T, Kitagawa T, et al. (2003) | [124] | Yes | Yes | Yes | |||||
| Merrill RK, Kim JS, et al. 2017 Sep;7(6):536–42. | [36] | Yes | Yes | Yes | |||||
| Miyakoshi N, Itoi E, et al. (2003) | [3] | Yes | Yes | Yes | |||||
| Mohanty C, Massicotte EM, et al. (2015) | [4] | Yes | Yes | Yes | Yes | ||||
| Morningstar M. (2002) | [132] | Yes | Yes | Yes | Thoracic Spine Pain | ||||
| Morningstar MW, (2003) | [133] | Yes | Yes | Yes | Yes | Yes | Thoracic spine pain | ||
| Moustafa IM, Diab AA, et al. (2016) | [134] | Yes | Yes | Yes | Yes | Cervical Radiculopathy | |||
| Moustafa IM, Diab AAM, et al. (2017) | [104] | Yes | Yes | Yes | Yes | ||||
| Nicholson KJ, Millhouse PW, et al. (2018) | [162] | Yes | yes | Yes | |||||
| Oakley P, Sanchez L, et al. (2021) | [163] | Yes | Yes | Yes | |||||
| Okada E, Matsumoto M, et al. (2011) | [164] | Yes | Yes | Yes | |||||
| Passias PG, Alas H, et al. (2021) | [9] | Yes | Yes | Yes | |||||
| Protopsaltis TS, Lafage R, et al. (2018) | [165] | Yes | Yes | ||||||
| Raastad J, Reiman M, et al. (2015) | [166] | Yes | |||||||
| Sadler SG, Spink MJ, et al. (2017) | [167] | Yes | |||||||
| Silber JS, Lipetz JS, et al. (2004) | [168] | Yes | Yes | ||||||
| Sun J, Zhao HW, et al. (2018) | [5] | Yes | Yes | Yes | |||||
| Troyanovich SJ, Harrison D, et al. (2000) | [169] | Yes | Yes | ||||||
| Watanabe K, Kawakami N, et al. (2007) | [170] | Yes | Yes | Yes | Yes | ||||
| Weng C, Wang J, et al. (2016) | [116] | Yes | Yes | ||||||
| Xing R, Liu W, et al. (2018) | [79] | Yes | Yes | Yes | |||||
| Yang X, Kong Q, et al. (2014) | [12] | Yes | Yes | Yes | |||||
| Young WF, (2000) | [171] | Yes | Yes | ||||||
| Yu M, Silvestre C, et al. (2013) | [172] | Yes | Yes | Yes | Yes | ||||
| Yu M, Zhao WK, et al. (2015) | [173] | Yes | Yes | Yes | |||||
| Total | 56 | 48 | 34 | 17 | 11 | 12 | 26 | 6 | 9 |
Author Contributions
Conceptualization, Arnone; methodology, Arnone; software, McCanse; validation, Arnone, Farmen, and McCanse; formal analysis, all authors; investigation, all authors; resources, McCanse; data curation, McCanse; writing—original draft preparation, all authors; writing—review and editing, Farmen; visualization, Arnone; supervision, Arnone and McCanse; project administration, Arnone and McCanse. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
| Radiographic Mensuration | ||
| Sagittal Vertical Axis (SVA) | The standard measurement of sagittal balance uses the center of the body of C7 as the measuring point for a vertical line that is perpendicular to the ground. The posterior-superior edge of S1 is also used as a second measuring point for a vertical line. The distance between these two lines constitutes the sagittal vertical axis (SVA). | Knott PT, Mardjetko SM, Techy F. The use of the T1 sagittal angle in predicting overall sagittal balance of the spine. Spine J. 2010;10(11):994–8. |
| Cervical 7 Plumbline (C7-P) | The C7 plumb line is a radiographic reference to determine the sagittal vertical axis, the most traditional measurement of sagittal balance of the spine. A vertical line is drawn from the center of the C7 vertebral body in a caudal direction. The line should connect with, or be within 5mm of, the superior-posterior endplate of S1. | Kim D, Davis DD, Menger RP. Spine Sagittal Balance. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534858/# |
| Cervical Lordosis (CL) Cobb Method |
Measured commonly with the Cobb Angle Method which utilizes the superior endplate of C3 and inferior endplate of C7 as references for determining sagittal alignment. A line is drawn along the superior endplate of the superior end vertebra C3 and a second line drawn along the inferior endplate of the inferior end vertebra C7. The acute angle formed by perpendicular lines drawn from the superior and inferior endplates of the two end vertebrae on a lateral radiograph is the angle of sagittal alignment. |
Silber JS, Lipetz JS, Hayes VM, Lonner BS. Measurement variability in the assessment of sagittal alignment of the cervical spine: a comparison of the gore and cobb methods. J Spinal Disord Tech. 2004 Aug;17(4):301–5. |
| Cervical Lordosis (CL) Gore Method |
The Gore Method relies on the posterior vertebral body as the referencing landmark.1 The posterosuperior and posteroinferior vertebral body endpoints are marked, and the line connecting these two points represents the posterior vertebral body line. Lines are drawn paralleling the posterior vertebral body line of the two end vertebrae (C3 and C7), and the acute angle formed by the intersection of these lines is the angle (°) of sagittal alignment. |
Silber JS, Lipetz JS, Hayes VM, Lonner BS. Measurement variability in the assessment of sagittal alignment of the cervical spine: a comparison of the gore and cobb methods. J Spinal Disord Tech. 2004 Aug;17(4):301–5. |
| Cervical Lordosis (CL) Harrison Posterior Tangent Method |
The Harrison Posterior Tangent Method relies on lines being drawn along the posterior vertebral body margins from C2-C7 whereas the posterior tangents were the slopes along the curve. | Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ, Holland B. Cobb method or Harrison posterior tangent method: which to choose for lateral cervical radiographic analysis. Spine (Phila Pa 1976). 2000 Aug 15;25(16):2072-8. doi: 10.1097/00007632-200008150-00011. PMID: 10954638. |
| Thoracic Kyphosis (TK) | Thoracic kyphosis is measured between the upper T1 endplate and the lower T12 endplate. However, many articles measure thoracic kyphosis between T4 and T12 because of the poor quality of normal radiographs due to the superposition of the humeral heads. | J. C. Le Huec, W. Thompson, Y. Mohsinaly, C. Barrey & A. Faundez. Sagittal balance of the spine, European Spine Journal volume 28, pages 1889–1905 (2019) |
| Thoracic Inlet Angle (TIA) | The TIA is formed when the T1 vertical line of the upper endplate (from the center of the T-1 upper endplate) meets with the line formed between the upper end of the manubrium and the center of the T-1 upper endplate. | Sun J, Zhao HW, Wang JJ, Xun L, Fu NX, Huang H. Diagnostic Value of T1 Slope in Degenerative Cervical Spondylotic Myelopathy. Med Sci Monit Int Med J Exp Clin Res. 2018 Feb 7;24:791–6. |
| T1 Slope (T1S) | T1 slope is the angle formed by drawing a line along the superior endplate of T1 and horizontal reference line at the median sagittal cervical vertebra from the CT radiographs. | Sun J, Zhao HW, Wang JJ, Xun L, Fu NX, Huang H. Diagnostic Value of T1 Slope in Degenerative Cervical Spondylotic Myelopathy. Med Sci Monit Int Med J Exp Clin Res. 2018 Feb 7;24:791–6. |
| Pelvic Tilt (PT) | The angle between two of the following radiographic lines: A line from the center of the S1 endplate to the center of the femoral head, and A vertical line is drawn intersecting the center of the femoral head. | Kim D, Davis DD, Menger RP. Spine Sagittal Balance. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534858/# |
| Pelvic Incidence (PI) |
PI is defined as the angle between a line drawn perpendicularly to the surface of the superior endplate of the sacrum and a line connecting the midpoint of the superior endplate of the sacrum to the center of the femoral head. | Kim D, Davis DD, Menger RP. Spine Sagittal Balance. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. |
| Sacral Slope (SS) | The angle between the sacral endplate and a line horizontal to the ground. | Mendoza-Lattes S, Ries Z, Gao Y, Weinstein SL. Natural history of spinopelvic alignment differs from symptomatic deformity of the spine. Spine. 2010 Jul 15;35(16):E792-798. |
| Lumbar Lordosis (LL) | The lumbar lordosis (LL) according to Roussouly is measured between the point of inflection from lumbar lordosis to thoracic kyphosis and the upper S1 endplate. | J. C. Le Huec, W. Thompson, Y. Mohsinaly, C. Barrey & A. Faundez. Sagittal balance of the spine, European Spine Journal volume 28, pages 1889–1905 (2019) |
| Lumbar Lordosis (LL) Harrison Posterior Tangent Method |
Alternatively, Lumbar Lordosis can be measured utilizing the Harrison Posterior Tangent Method from L1-L5, also known as Absolute Rotation Angle (ARA). | Tadeusz J Janik, Donald D. Harrison, Rene Cailliet, Stepah J. Troyanovich, Deed Harrison. Can the Sagittal Lumbar Curvature be Closely Approximated by an Ellipse? Journal of Orthopaedic Research Vol. 16, No. 6 1998, p. 766-770 Thr Journal of Bone and Joint Surgery Inc. |
Appendix B
| Visual Postural Assessment | |||
| Craniovertebral Angle (CVA) | Where a line drawn from the tragus of the ear to the C7 vertebra intersects a horizontal line, the CV angle is formed. | 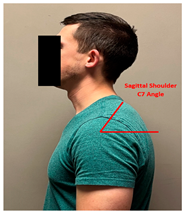 |
Singla D, Veqar Z, Hussain ME. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiropr Med. 2017 Jun;16(2):131-138. doi: 10.1016/j.jcm.2017.01.005. Epub 2017 Mar 18. |
| Sagittal Head Tilt (SHT) | This angle, which is formed between a line from the canthus of the eye and the tragus of the ear and the horizontal, is a measure of the posture of the upper cervical spine. | 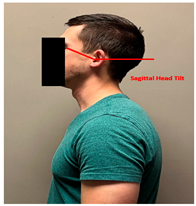 |
Singla D, Veqar Z, Hussain ME. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiropr Med. 2017 Jun;16(2):131-138. doi: 10.1016/j.jcm.2017.01.005. Epub 2017 Mar 18. |
| Sagittal Shoulder-C7 Angle | Where a horizontal line passing through the lateral shoulder meets the line drawn from C7 to the lateral shoulder, the point of intersection forms the sagittal shoulder-C7 angle. | 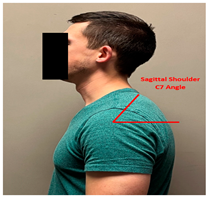 |
Singla D, Veqar Z, Hussain ME. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiropr Med. 2017 Jun;16(2):131-138. doi: 10.1016/j.jcm.2017.01.005. Epub 2017 Mar 18. |
| Tragus Wall Distance (TWD) | Measurement of the tragus to a wall behind the subject utilizing a 30cm combination square. |  |
Shipe NK, Billek-Sawhney B, Canter TA, Meals DJ, Nestler JM, Stumpff JL. The intra- and inter-rater reliability of the tragus wall distance (TWD) measurement in non-pathological participants ages 18-34. Physiother Theory Pract. 2013 May;29(4):328–34. |
| Anterior Head Translation (AHT) | A vertical line originating from the posterior inferior body corner of C7 and measuring the horizontal displacement of the posterior superior corner of C2 relative to this vertical line drawn superiorly from the posterior inferior body C7. |  |
Moustafa IM, Diab AA, Harrison DE. The effect of normalizing the sagittal cervical configuration on dizziness, neck pain, and cervicocephalic kinesthetic sensibility: a 1-year randomized controlled study. Eur J Phys Rehabil Med. 2017 Feb;53(1):57–71. |
| Flexicurve Ruler | A malleable band of metal covered with plastic and approximately 60 cm in length. The ruler can be bent in only one plane and retains the shape to which it is bent. Commonly used to measure thoracic kyphosis. |  |
Yanagawa TL, Maitland ME, Burgess K, Young L, Hanley D. Assessment of Thoracic Kyphosis Using the Flexicurve for Individuals with Osteoporosis. Hong Kong Physiother J. 2000 Aug;18(2):53–7. |
References
- Mac-Thiong, J.-M.; Transfeldt, E.E.; Mehbod, A.A.; Perra, J.H.; Denis, F.; Garvey, T.A.; Lonstein, J.E.; Wu, C.; Dorman, C.W.; Winter, R.B. Can C7 Plumbline and Gravity Line Predict Health Related Quality of Life in Adult Scoliosis? Spine (Phila Pa 1976) 2009, 34, E519–527. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Troyanovich, S.J.; Harrison, S.O. A Review of Biomechanics of the Central Nervous System--Part I: Spinal Canal Deformations Resulting from Changes in Posture. J Manipulative Physiol Ther 1999, 22, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Miyakoshi, N.; Itoi, E.; Kobayashi, M.; Kodama, H. Impact of Postural Deformities and Spinal Mobility on Quality of Life in Postmenopausal Osteoporosis. Osteoporos Int 2003, 14, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, C.; Massicotte, E.M.; Fehlings, M.G.; Shamji, M.F. Association of Preoperative Cervical Spine Alignment with Spinal Cord Magnetic Resonance Imaging Hyperintensity and Myelopathy Severity: Analysis of a Series of 124 Cases. Spine (Phila Pa 1976) 2015, 40, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Zhao, H.-W.; Wang, J.-J.; Xun, L.; Fu, N.-X.; Huang, H. Diagnostic Value of T1 Slope in Degenerative Cervical Spondylotic Myelopathy. Med Sci Monit 2018, 24, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Oren, J.H.; Challier, V.; Lafage, R.; Ferrero, E.; Liu, S.; Vira, S.; Spiegel, M.A.; Harris, B.Y.; Liabaud, B.; et al. Global Sagittal Axis: A Step toward Full-Body Assessment of Sagittal Plane Deformity in the Human Body. J Neurosurg Spine 2016, 25, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Okamoto, M.; Hatsushikano, S.; Shimoda, H.; Ono, M.; Watanabe, K. Normative Values of Spino-Pelvic Sagittal Alignment, Balance, Age, and Health-Related Quality of Life in a Cohort of Healthy Adult Subjects. Eur Spine J 2016, 25, 3675–3686. [Google Scholar] [CrossRef] [PubMed]
- Keorochana, G.; Taghavi, C.E.; Lee, K.-B.; Yoo, J.H.; Liao, J.-C.; Fei, Z.; Wang, J.C. Effect of Sagittal Alignment on Kinematic Changes and Degree of Disc Degeneration in the Lumbar Spine: An Analysis Using Positional MRI. Spine 2011, 36, 893–898. [Google Scholar] [CrossRef]
- Passias, P.G.; Alas, H.; Bess, S.; Line, B.G.; Lafage, V.; Lafage, R.; Ames, C.P.; Burton, D.C.; Brown, A.; Bortz, C.; et al. Patient-Related and Radiographic Predictors of Inferior Health-Related Quality-of-Life Measures in Adult Patients with Nonoperative Spinal Deformity. J Neurosurg Spine 2021, 1–7. [Google Scholar] [CrossRef]
- Chun, S.-W.; Lim, C.-Y.; Kim, K.; Hwang, J.; Chung, S.G. The Relationships between Low Back Pain and Lumbar Lordosis: A Systematic Review and Meta-Analysis. Spine J 2017, 17, 1180–1191. [Google Scholar] [CrossRef]
- Glassman, S.D.; Bridwell, K.; Dimar, J.R.; Horton, W.; Berven, S.; Schwab, F. The Impact of Positive Sagittal Balance in Adult Spinal Deformity. Spine (Phila Pa 1976) 2005, 30, 2024–2029. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Kong, Q.; Song, Y.; Liu, L.; Zeng, J.; Xing, R. The Characteristics of Spinopelvic Sagittal Alignment in Patients with Lumbar Disc Degenerative Diseases. Eur Spine J 2014, 23, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Blyth, F.M.; Briggs, A.M.; Schneider, C.H.; Hoy, D.G.; March, L.M. The Global Burden of Musculoskeletal Pain—Where to From Here? Am J Public Health 2019, 109, 35–40. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sanchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. The Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef] [PubMed]
- Bang, A.A.; Bhojraj, S.Y.; Bang, A.T. Back Pain and Musculoskeletal Pain as Public Health Problems: Rural Communities Await Solution. Journal of Global Health 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-Adjusted Life Years (DALYs) for 291 Diseases and Injuries in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. The Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. The Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.-A.; Safiri, S. Neck Pain: Global Epidemiology, Trends and Risk Factors. BMC Musculoskelet Disord 2022, 23, 26. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.-A.; Hoy, D.; Buchbinder, R.; Mansournia, M.A.; Bettampadi, D.; Ashrafi-Asgarabad, A.; Almasi-Hashiani, A.; Smith, E.; Sepidarkish, M. Global, Regional, and National Burden of Neck Pain in the General Population, 1990-2017: Systematic Analysis of the Global Burden of Disease Study 2017. Bmj 2020, 368. [Google Scholar] [CrossRef]
- Kado, D.M.; Huang, M.-H.; Nguyen, C.B.; Barrett-Connor, E.; Greendale, G.A. Hyperkyphotic Posture and Risk of Injurious Falls in Older Persons: The Rancho Bernardo Study. J Gerontol A Biol Sci Med Sci 2007, 62, 652–657. [Google Scholar] [CrossRef]
- Koch, C.; Hänsel, F. Non-Specific Low Back Pain and Postural Control During Quiet Standing—A Systematic Review. Front. Psychol. 2019, 10, 586. [Google Scholar] [CrossRef] [PubMed]
- Young, K.J. A Tale of Specialization in 2 Professions: Comparing the Development of Radiology in Chiropractic and Medicine. J Chiropr Humanit 2019, 26, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, D.; Fielding, K.; Bentley, E.; Miller, P.; Kerslake, R.; Pringle, M. The Role of Radiography in Primary Care Patients with Low Back Pain of at Least 6 Weeks Duration: A Randomised (Unblinded) Controlled Trial; National Co-ordinating Centre for HTA. Great Britain, 2001. [Google Scholar]
- Kendrick, D. Radiography of the Lumbar Spine in Primary Care Patients with Low Back Pain: Randomised Controlled Trial. BMJ 2001, 322, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.L.; Clement, C.M.; Lesiuk, H.; De Maio, V.J.; Laupacis, A.; Schull, M.; McKnight, R.D.; Verbeek, R. The Canadian C-Spine Rule for Radiography in Alert and Stable Trauma Patients. Jama 2001, 286, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Https://Www.Choosingwisely.Org/Wp-Content/Uploads/2017/08/ACA-Choosing-Wisely-List.Pdf - Google Search. Available online: https://www.google.com/search?q=https%3A%2F%2Fwww.choosingwisely.org%2Fwp-content%2Fuploads%2F2017%2F08%2FACA-Choosing-Wisely-List.pdf&client=firefox-b-1-d&sxsrf=ALiCzsZoV4bF70pEVPbhNnSldW64sMONHQ%3A1668805388253&ei=DPN3Y7fjDrWoptQPsKqX8Ac&ved=0ahUKEwi3mfbC0Lj7AhU1lIkEHTDVBX4Q4dUDCA8&uact=5&oq=https%3A%2F%2Fwww.choosingwisely.org%2Fwp-content%2Fuploads%2F2017%2F08%2FACA-Choosing-Wisely-List.pdf&gs_lcp=Cgxnd3Mtd2l6LXNlcnAQA0oECEEYAUoECEYYAFDVCFiSD2DxE2gBcAB4AIABWogBsQGSAQEymAEAoAEBwAEB&sclient=gws-wiz-serp (accessed on 18 November 2022).
- Jenkins, H.J. Awareness of Radiographic Guidelines for Low Back Pain: A Survey of Australian Chiropractors. Chiropr Man Therap 2016, 24, 39. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.A.; Harrison, D.E. Radiophobia: 7 Reasons Why Radiography Used in Spine and Posture Rehabilitation Should Not Be Feared or Avoided. Dose-Response 2018, 16, 155932581878144. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A.M.; Hegazy, F.A.; Harrison, D.E. Does Rehabilitation of Cervical Lordosis Influence Sagittal Cervical Spine Flexion Extension Kinematics in Cervical Spondylotic Radiculopathy Subjects? J Back Musculoskelet Rehabil 2017, 30, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Jackson, B.L.; Barker, W.F. Reliability of the Pettibon Patient Positioning System for Radiographic Production. J Vertebral Subluxation Res 2000, 4, 3–11. [Google Scholar]
- Lopes, M.A. “What Are the Effects of Diagnostic Imaging on Clinical Outcomes in Patients with Low Back Pain Presenting for Chiropractic Care? A Matched Observational Study.” Jenkins et al., Chiropractic & Manual Therapies 2021;29:46. Chiropr Man Therap 2022, 30, 11. [Google Scholar] [CrossRef]
- Berger, R.J.; Sultan, A.A.; Tanenbaum, J.E.; Cantrell, W.A.; Gurd, D.P.; Kuivila, T.E.; Mroz, T.E.; Steinmetz, M.P.; Goodwin, R.C. Cervical Sagittal Alignment and the Impact of Posterior Spinal Instrumented Fusion in Patients with Lenke Type 1 Adolescent Idiopathic Scoliosis. J Spine Surg 2018, 4, 342–348. [Google Scholar] [CrossRef]
- Ling, F.P.; Chevillotte, T.; Leglise, A.; Thompson, W.; Bouthors, C.; Le Huec, J.-C. Which Parameters Are Relevant in Sagittal Balance Analysis of the Cervical Spine? A Literature Review. Eur Spine J 2018, 27, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-W.; Hyun, S.-J.; Kim, K.-J. Surgical Impact on Global Sagittal Alignment and Health-Related Quality of Life Following Cervical Kyphosis Correction Surgery: Systematic Review. Neurospine 2020, 17, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.; Lafage, V.; Patel, A.; Farcy, J.-P. Sagittal Plane Considerations and the Pelvis in the Adult Patient. Spine 2009, 34, 1828–1833. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.K.; Kim, J.S.; Leven, D.M.; Kim, J.H.; Cho, S.K. Beyond Pelvic Incidence-Lumbar Lordosis Mismatch: The Importance of Assessing the Entire Spine to Achieve Global Sagittal Alignment. Global Spine J 2017, 7, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.A.; Amin, A.; Omeis, I.; Gokaslan, Z.L.; Gottfried, O.N. Implications of Spinopelvic Alignment for the Spine Surgeon. Neurosurgery 2012, 70, 707–721. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Shao, Y.; Liu, H.; Zhang, J.; He, F.; Chen, A.; Yang, H.; Pi, B. Association between Sagittal Balance and Adjacent Segment Degeneration in Anterior Cervical Surgery: A Systematic Review and Meta-Analysis. BMC Musculoskelet Disord 2019, 20, 430. [Google Scholar] [CrossRef] [PubMed]
- Youn, Y.-H.; Cho, K.-J.; Na, Y.; Kim, J.-S. Global Sagittal Alignment and Clinical Outcomes after 1-3 Short-Segment Lumbar Fusion in Degenerative Spinal Diseases. Asian Spine J 2022, 16, 551–559. [Google Scholar] [CrossRef]
- Hori, Y.; Matsumura, A.; Namikawa, T.; Kato, M.; Takahashi, S.; Ohyama, S.; Ozaki, T.; Yabu, A.; Nakamura, H. Does Sagittal Imbalance Impact the Surgical Outcomes of Short-Segment Fusion for Lumbar Spinal Stenosis Associated with Degenerative Lumbar Scoliosis? J Orthop Sci 2019, 24, 224–229. [Google Scholar] [CrossRef]
- Corso, M.; Cancelliere, C.; Mior, S.; Kumar, V.; Smith, A.; Côté, P. The Clinical Utility of Routine Spinal Radiographs by Chiropractors: A Rapid Review of the Literature. Chiropr Man Therap 2020, 28, 33. [Google Scholar] [CrossRef]
- Oakley, P.A.; Betz, J.W.; Harrison, D.E.; Siskin, L.A.; Hirsh, D.W. International Chiropractors Association Rapid Response Research Review Subcommittee Radiophobia Overreaction: College of Chiropractors of British Columbia Revoke Full X-Ray Rights Based on Flawed Study and Radiation Fear-Mongering. Dose Response 2021, 19, 15593258211033142. [Google Scholar] [CrossRef]
- Ammendolia, C.; Bombardier, C.; Hogg-Johnson, S.; Glazier, R. Views on Radiography Use for Patients with Acute Low Back Pain among Chiropractors in an Ontario Community. Journal of manipulative and physiological therapeutics 2002, 25, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.A.; Cuttler, J.M.; Harrison, D.E. X-Ray Imaging Is Essential for Contemporary Chiropractic and Manual Therapy Spinal Rehabilitation: Radiography Increases Benefits and Reduces Risks. Dose-Response 2018, 16, 155932581878143. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.E.; Harrison, D.D.; Troyanovich, S.J. Reliability of Spinal Displacement Analysis of Plain X-Rays: A Review of Commonly Accepted Facts and Fallacies with Implications for Chiropractic Education and Technique. Journal of manipulative and physiological therapeutics 1998, 21, 252–266. [Google Scholar] [PubMed]
- Lopes, M.A.; Coleman, R.R.; Cremata, E.J. Radiography and Clinical Decision-Making in Chiropractic. Dose-Response 2021, 19, 155932582110448. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Fu, R.; Carrino, J.A.; Deyo, R.A. Imaging Strategies for Low-Back Pain: Systematic Review and Meta-Analysis. The Lancet 2009, 373, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Sielatycki, J.A.; Armaghani, S.; Silverberg, A.; McGirt, M.J.; Devin, C.J.; O’Neill, K. Is More Lordosis Associated with Improved Outcomes in Cervical Laminectomy and Fusion When Baseline Alignment Is Lordotic? The Spine Journal 2016, 16, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Nouri, A.; Wu, D.; Nori, S.; Tetreault, L.; Fehlings, M.G. Impact of Cervical Spine Deformity on Preoperative Disease Severity and Postoperative Outcomes Following Fusion Surgery for Degenerative Cervical Myelopathy: Sub-Analysis of AOSpine North America and International Studies. Spine (Phila Pa 1976) 2018, 43, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Shimizu, T.; Goto, K.; Kuroda, Y.; Okuzu, Y.; Otsuki, B.; Fujibayashi, S.; Matsuda, S. The Impact of Spinopelvic Parameters on Hip Degeneration After Spinal Fusion. Spine 2022, 47, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Labelle, H.; Rouissi, J.; Bodin, A. Pre- and Post-Operative Sagittal Balance in Idiopathic Scoliosis: A Comparison over the Ages of Two Cohorts of 132 Adolescents and 52 Adults. Eur Spine J 2013, 22, 203–215. [Google Scholar] [CrossRef]
- Lee, C.K.; Shin, D.A.; Yi, S.; Kim, K.N.; Shin, H.C.; Yoon, D.H.; Ha, Y. Correlation between Cervical Spine Sagittal Alignment and Clinical Outcome after Cervical Laminoplasty for Ossification of the Posterior Longitudinal Ligament. SPI 2016, 24, 100–107. [Google Scholar] [CrossRef]
- Aoki, Y.; Nakajima, A.; Takahashi, H.; Sonobe, M.; Terajima, F.; Saito, M.; Takahashi, K.; Ohtori, S.; Watanabe, A.; Nakajima, T.; et al. Influence of Pelvic Incidence-Lumbar Lordosis Mismatch on Surgical Outcomes of Short-Segment Transforaminal Lumbar Interbody Fusion. BMC Musculoskelet Disord 2015, 16, 213. [Google Scholar] [CrossRef] [PubMed]
- Passias, P.G.; Pierce, K.E.; Passano, B.; Tariq, M.B.; Ahmad, S.; Singh, V.; Owusu-Sarpong, S.; Krol, O.; Imbo, B.; Passfall, L.; et al. What Are the Major Drivers of Outcomes in Cervical Deformity Surgery? J Craniovertebr Junction Spine 2021, 12, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Abelin-Genevois, K. Sagittal Balance of the Spine. Orthopaedics & Traumatology: Surgery & Research 2021, 107, 102769. [Google Scholar] [CrossRef] [PubMed]
- Ochtman, A.E.A.; Kruyt, M.C.; Jacobs, W.C.H.; Kersten, R.F.M.R.; le Huec, J.C.; Öner, F.C.; van Gaalen, S.M. Surgical Restoration of Sagittal Alignment of the Spine: Correlation with Improved Patient-Reported Outcomes: A Systematic Review and Meta-Analysis. JBJS Rev 2020, 8, e1900100. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Visintini, S.; Dunning, C.E.; Oxner, W.M.; Glennie, R.A. Does Restoration of Focal Lumbar Lordosis for Single Level Degenerative Spondylolisthesis Result in Better Patient-Reported Clinical Outcomes? A Systematic Literature Review. J Clin Neurosci 2017, 44, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.C.; Girardi, F.P.; Cammisa, F.P.; Lim, M.R.; Tropiano, P.; Marnay, T. Correlation between Range of Motion and Outcome after Lumbar Total Disc Replacement: 8.6-Year Follow-Up. Spine (Phila Pa 1976) 2005, 30, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Vialle, R.; Levassor, N.; Rillardon, L.; Templier, A.; Skalli, W.; Guigui, P. Radiographic Analysis of the Sagittal Alignment and Balance of the Spine in Asymptomatic Subjects. VO L U M E.
- Saunders, E.S. Improvement of Cervical Lordosis and Reduction of Forward Head Posture with Anterior Head Weighting and Proprioceptive Balancing Protocols.
- Harrison, D.E.; Harrison, D.D.; Betz, J.J.; Janik, T.J.; Holland, B.; Colloca, C.J.; Haas, J.W. Increasing the Cervical Lordosis with Chiropractic Biophysics Seated Combined Extension-Compression and Transverse Load Cervical Traction with Cervical Manipulation: Nonrandomized Clinical Control Trial. J Manipulative Physiol Ther 2003, 26, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Fortner, M.O.; Oakley, P.A.; Harrison, D.E. Non-Surgical Improvement of Cervical Lordosis Is Possible in Advanced Spinal Osteoarthritis: A CBP® Case Report. J Phys Ther Sci 2018, 30, 108–112. [Google Scholar] [CrossRef]
- Wickstrom, B.M.; Oakley, P.A.; Harrison, D.E. Non-Surgical Relief of Cervical Radiculopathy through Reduction of Forward Head Posture and Restoration of Cervical Lordosis: A Case Report. Journal of physical therapy science 2017, 29, 1472–1474. [Google Scholar] [CrossRef]
- Westersund, C.D.; Scholten, J.; Turner, R.J. Relationship between Craniocervical Orientation and Center of Force of Occlusion in Adults. Cranio 2017, 35, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.A.; Jaeger, J.O.; Brown, J.E.; Polatis, T.A.; Clarke, J.G.; Whittler, C.D.; Harrison, D.E. The CBP® Mirror Image® Approach to Reducing Thoracic Hyperkyphosis: A Retrospective Case Series of 10 Patients. J Phys Ther Sci 2018, 30, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.E.; Oakley, P.A.; Levin, S.B.; Harrison, D.E. Reversing Thoracic Hyperkyphosis: A Case Report Featuring Mirror Image® Thoracic Extension Rehabilitation. J Phys Ther Sci 2017, 29, 1264–1267. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.A.; Harrison, D.E. Reducing Thoracic Hyperkyphosis Subluxation Deformity: A Systematic Review of Chiropractic Biophysics® Methods Employed in Its Structural Improvement. Journal of Contemporary Chiropractic 2018, 1, 59–66. [Google Scholar]
- Betz, J.W.; Oakley, P.A.; Harrison, D.E. Relief of Exertional Dyspnea and Spinal Pains by Increasing the Thoracic Kyphosis in Straight Back Syndrome (Thoracic Hypo-Kyphosis) Using CBP® Methods: A Case Report with Long-Term Follow-Up. J Phys Ther Sci 2018, 30, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.R.; Oakley, P.A.; Harrison, D.E. Nonsurgical Correction of Straight Back Syndrome (Thoracic Hypokyphosis), Increased Lung Capacity and Resolution of Exertional Dyspnea by Thoracic Hyperkyphosis Mirror Image® Traction: A CBP® Case Report. J Phys Ther Sci 2017, 29, 2058–2061. [Google Scholar] [CrossRef]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Janik, T.J.; Holland, B. Changes in Sagittal Lumbar Configuration with a New Method of Extension Traction: Nonrandomized Clinical Controlled Trial. Arch Phys Med Rehabil 2002, 83, 1585–1591. [Google Scholar] [CrossRef]
- Harrison, D.E.; Oakley, P.A. Non-Operative Correction of Flat Back Syndrome Using Lumbar Extension Traction: A CBP® Case Series of Two. J Phys Ther Sci 2018, 30, 1131–1137. [Google Scholar] [CrossRef]
- Harrison, D.E.; Oakley, P.A. Scoliosis Deformity Reduction in Adults: A CBP® Mirror Image® Case Series Incorporating the “non-Commutative Property of Finite Rotation Angles under Addition” in Five Patients with Lumbar and Thoraco-Lumbar Scoliosis. J Phys Ther Sci 2017, 29, 2044–2050. [Google Scholar] [CrossRef]
- Haggard, J.S.; Haggard, J.B.; Oakley, P.A.; Harrison, D.E. Reduction of Progressive Thoracolumbar Adolescent Idiopathic Scoliosis by Chiropractic Biophysics® (CBP®) Mirror Image® Methods Following Failed Traditional Chiropractic Treatment: A Case Report. J Phys Ther Sci 2017, 29, 2062–2067. [Google Scholar] [CrossRef]
- Harrison, D.E.; Harrison, D.D.; Colloca, C.J.; Betz, J.; Janik, T.J.; Holland, B. Repeatability over Time of Posture, Radiograph Positioning, and Radiograph Line Drawing: An Analysis of Six Control Groups. J Manipulative Physiol Ther 2003, 26, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.E.; Oakley, P.A. NECESSITY FOR BIOMECHANICAL EVALUATION OF POSTURE, ALIGNMENT AND SUBLUXATION. PART I. THE 6 SUBLUXATION TYPES THAT SATISFY NELSON’S CRITERION FOR VALID SUBLUXATION THEORY. J Contemporary Chiropr 2018, 1, 9–19. [Google Scholar]
- Lee, S.-H.; Son, E.-S.; Seo, E.-M.; Suk, K.-S.; Kim, K.-T. Factors Determining Cervical Spine Sagittal Balance in Asymptomatic Adults: Correlation with Spinopelvic Balance and Thoracic Inlet Alignment. Spine J 2015, 15, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Bess, S.; Line, B.; Fu, K.-M.; McCarthy, I.; Lafage, V.; Schwab, F.; Shaffrey, C.; Ames, C.; Akbarnia, B.; Jo, H.; et al. The Health Impact of Symptomatic Adult Spinal Deformity: Comparison of Deformity Types to United States Population Norms and Chronic Diseases. SPINE 2016, 41, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Wang, L.; Zhao, L.; Wang, Y.; Chen, M.; Wang, S.; Lv, Z.; Luo, Y. Coronal Balance vs. Sagittal Profile in Adolescent Idiopathic Scoliosis, Are They Correlated? Front Pediatr 2019, 7, 523. [Google Scholar] [CrossRef] [PubMed]
- Xing, R.; Liu, W.; Li, X.; Jiang, L.; Yishakea, M.; Dong, J. Characteristics of Cervical Sagittal Parameters in Healthy Cervical Spine Adults and Patients with Cervical Disc Degeneration. BMC Musculoskelet Disord 2018, 19, 37. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.; Veqar, Z.; Hussain, M.E. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiropr Med 2017, 16, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Bryan, J.M.; Mosner, E.; Shippee, R.; Stull, M.A. Investigation of the Validity of Postural Evaluation Skills in Assessing Lumbar Lordosis Using Photographs of Clothed Subjects. J Orthop Sports Phys Ther 1990, 12, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Boland, D.M.; Neufeld, E.V.; Ruddell, J.; Dolezal, B.A.; Cooper, C.B. Inter- and Intra-Rater Agreement of Static Posture Analysis Using a Mobile Application. J Phys Ther Sci 2016, 28, 3398–3402. [Google Scholar] [CrossRef]
- Stolinski, L.; Kozinoga, M.; Czaprowski, D.; Tyrakowski, M.; Cerny, P.; Suzuki, N.; Kotwicki, T. Two-Dimensional Digital Photography for Child Body Posture Evaluation: Standardized Technique, Reliable Parameters and Normative Data for Age 7-10 Years. Scoliosis Spinal Disord 2017, 12, 38. [Google Scholar] [CrossRef]
- Shipe, N.K.; Billek-Sawhney, B.; Canter, T.A.; Meals, D.J.; Nestler, J.M.; Stumpff, J.L. The Intra- and Inter-Rater Reliability of the Tragus Wall Distance (TWD) Measurement in Non-Pathological Participants Ages 18-34. Physiother Theory Pract 2013, 29, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Fedorak, C.; Ashworth, N.; Marshall, J.; Paull, H. Reliability of the Visual Assessment of Cervical and Lumbar Lordosis: How Good Are We? Spine 2003, 28, 1857–1859. [Google Scholar] [CrossRef]
- Nam, S.H.; Son, S.M.; Kwon, J.W.; Lee, N.K. The Intra- and Inter-Rater Reliabilities of the Forward Head Posture Assessment of Normal Healthy Subjects. J Phys Ther Sci 2013, 25, 737–739. [Google Scholar] [CrossRef]
- Yanagawa, T.L.; Maitland, M.E.; Burgess, K.; Young, L.; Hanley, D. Assessment of Thoracic Kyphosis Using the Flexicurve for Individuals with Osteoporosis. Hong Kong Physiotherapy Journal 2000, 18, 53–57. [Google Scholar] [CrossRef]
- Dunn, J.; Henrikson, N.B.; Morrison, C.C.; Nguyen, M.; Blasi, P.R.; Lin, J.S. Screening for Adolescent Idiopathic Scoliosis: A Systematic Evidence Review for the U.S. Preventive Services Task Force; U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews, Ed.; Agency for Healthcare Research and Quality (US): Rockville (MD), 2018. [Google Scholar]
- Lundström, A.; Lundström, F.; Lebret, L.M.; Moorrees, C.F. Natural Head Position and Natural Head Orientation: Basic Considerations in Cephalometric Analysis and Research. Eur J Orthod 1995, 17, 111–120. [Google Scholar] [CrossRef]
- Yip, C.H.T.; Chiu, T.T.W.; Poon, A.T.K. The Relationship between Head Posture and Severity and Disability of Patients with Neck Pain. Man Ther 2008, 13, 148–154. [Google Scholar] [CrossRef]
- Fortin, C.; Feldman, D.E.; Cheriet, F.; Labelle, H. Clinical Methods for Quantifying Body Segment Posture: A Literature Review. Disabil Rehabil 2011, 33, 367–383. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, C.J.; Kaliszer, M.; Moore, D.P.; Fogarty, E.E.; Dowling, F.E. Surface Topography, Cobb Angles, and Cosmetic Change in Scoliosis. Spine (Phila Pa 1976) 2001, 26, E55–63. [Google Scholar] [CrossRef]
- Harrison, D.E.; Haas, J.W.; Cailliet, R.; Harrison, D.D.; Holland, B.; Janik, T.J. Concurrent Validity of Flexicurve Instrument Measurements: Sagittal Skin Contour of the Cervical Spine Compared With Lateral Cervical Radiographic Measurements. Journal of Manipulative and Physiological Therapeutics 2005, 28, 597–603. [Google Scholar] [CrossRef]
- McFarland, C.; Wang-Price, S.; Richard, S. Clinical Measurements of Cervical Lordosis Using Flexirule and Inclinometer Methods in Individuals with and without Cervical Spine Dysfunction: A Reliability and Validity Study. J Back Musculoskelet Rehabil 2015, 28, 295–302. [Google Scholar] [CrossRef]
- Hannink, E.; Dawes, H.; Shannon, T.M.L.; Barker, K.L. Validity of Sagittal Thoracolumbar Curvature Measurement Using a Non-Radiographic Surface Topography Method. Spine Deform 2022, 10, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Fortin, C.; Feldman, D.E.; Cheriet, F.; Labelle, H. Validity of a Quantitative Clinical Measurement Tool of Trunk Posture in Idiopathic Scoliosis. Spine (Phila Pa 1976) 2010, 35, E988–994. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.F.; Knecht, K.; Balaban, G.; Dvorak, J.; Grob, D. A New Skin-Surface Device for Measuring the Curvature and Global and Segmental Ranges of Motion of the Spine: Reliability of Measurements and Comparison with Data Reviewed from the Literature. Eur Spine J 2004, 13, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, B.F.; Starks, Z.; Bhatia, S. Reliability of the DIERS Formetric 4D Spine Shape Parameters in Adults without Postural Deformities. BioMed Research International 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Szczygieł, E.; Zielonka, K.; Mętel, S.; Golec, J. Musculo-Skeletal and Pulmonary Effects of Sitting Position - a Systematic Review. Ann Agric Environ Med 2017, 24, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Keil, A.P.; Baranyi, B.; Mehta, S.; Maurer, A. Ordering of Diagnostic Imaging by Physical Therapists: A 5-Year Retrospective Practice Analysis. Physical Therapy 2019, 99, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Boyles, R.E.; Gorman, I.; Pinto, D.; Ross, M.D. Physical Therapist Practice and the Role of Diagnostic Imaging. journal of orthopaedic & sports physical therapy 2011, 41, 829–837. [Google Scholar]
- Jaromi, M.; Nemeth, A.; Kranicz, J.; Laczko, T.; Betlehem, J. Treatment and Ergonomics Training of Work-Related Lower Back Pain and Body Posture Problems for Nurses. J Clin Nurs 2012, 21, 1776–1784. [Google Scholar] [CrossRef] [PubMed]
- Borysov, M.; Moramarco, M.; Sy, N.; Lee, S.G. Postural Re-Education of Scoliosis - State of the Art (Mini-Review). Curr Pediatr Rev 2016, 12, 12–16. [Google Scholar] [CrossRef]
- Moustafa, I.M.; Diab, A.A.; Harrison, D.E. The Effect of Normalizing the Sagittal Cervical Configuration on Dizziness, Neck Pain, and Cervicocephalic Kinesthetic Sensibility: A 1-Year Randomized Controlled Study. Eur J Phys Rehabil Med 2017, 53, 57–71. [Google Scholar] [CrossRef]
- Diab, A.A. The Role of Forward Head Correction in Management of Adolescent Idiopathic Scoliotic Patients: A Randomized Controlled Trial. Clin Rehabil 2012, 26, 1123–1132. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A. The Effect of Adding Forward Head Posture Corrective Exercises in the Management of Lumbosacral Radiculopathy: A Randomized Controlled Study. J Manipulative Physiol Ther 2015, 38, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A. Extension Traction Treatment for Patients with Discogenic Lumbosacral Radiculopathy: A Randomized Controlled Trial. Clin Rehabil 2013, 27, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Diab, A.A.M.; Moustafa, I.M. The Efficacy of Lumbar Extension Traction for Sagittal Alignment in Mechanical Low Back Pain: A Randomized Trial. J Back Musculoskelet Rehabil 2013, 26, 213–220. [Google Scholar] [CrossRef]
- Morningstar, M.W.; Woggon, D.; Lawrence, G. Scoliosis Treatment Using a Combination of Manipulative and Rehabilitative Therapy: A Retrospective Case Series. BMC Musculoskelet Disord 2004, 5, 32. [Google Scholar] [CrossRef] [PubMed]
- Diab, A.A.; Moustafa, I.M. Lumbar Lordosis Rehabilitation for Pain and Lumbar Segmental Motion in Chronic Mechanical Low Back Pain: A Randomized Trial. J Manipulative Physiol Ther 2012, 35, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Gong, W. The Effects of Cervical Joint Manipulation, Based on Passive Motion Analysis, on Cervical Lordosis, Forward Head Posture, and Cervical ROM in University Students with Abnormal Posture of the Cervical Spine. J Phys Ther Sci 2015, 27, 1609–1611. [Google Scholar] [CrossRef]
- Rubinstein, S.M.; Pool, J.J.M.; van Tulder, M.W.; Riphagen, I.I.; de Vet, H.C.W. A Systematic Review of the Diagnostic Accuracy of Provocative Tests of the Neck for Diagnosing Cervical Radiculopathy. Eur Spine J 2007, 16, 307–319. [Google Scholar] [CrossRef]
- Hollerwöger, D. Methodological Quality and Outcomes of Studies Addressing Manual Cervical Spine Examinations: A Review. Man Ther 2006, 11, 93–98. [Google Scholar] [CrossRef]
- Wáng, Y.X.J.; Wu, A.-M.; Ruiz Santiago, F.; Nogueira-Barbosa, M.H. Informed Appropriate Imaging for Low Back Pain Management: A Narrative Review. J Orthop Translat 2018, 15, 21–34. [Google Scholar] [CrossRef]
- Sheikh Alshabab, B.; Gupta, M.C.; Lafage, R.; Bess, S.; Shaffrey, C.; Kim, H.J.; Ames, C.P.; Burton, D.C.; Smith, J.S.; Eastlack, R.K.; et al. Does Achieving Global Spinal Alignment Lead to Higher Patient Satisfaction and Lower Disability in Adult Spinal Deformity? Spine 2021, 46, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.; Wang, J.; Tuchman, A.; Wang, J.; Fu, C.; Hsieh, P.C.; Buser, Z.; Wang, J.C. Influence of T1 Slope on the Cervical Sagittal Balance in Degenerative Cervical Spine: An Analysis Using Kinematic MRI. Spine (Phila Pa 1976) 2016, 41, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-H.; Ha, J.-K.; Chung, J.-H.; Hwang, C.J.; Lee, C.S.; Cho, J.H. A Retrospective Study to Reveal the Effect of Surgical Correction of Cervical Kyphosis on Thoraco-Lumbo-Pelvic Sagittal Alignment. Eur Spine J 2016, 25, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Jun, H.S.; Kim, J.H.; Ahn, J.H.; Chang, I.B.; Song, J.H.; Kim, T.H.; Park, M.S.; Kim, Y.C.; Kim, S.W.; Oh, J.K. T1 Slope and Degenerative Cervical Spondylolisthesis. Spine (Phila Pa 1976) 2015, 40, E220–226. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, N.; Podgórski, M.; Haładaj, R.; Polguj, M.; Olewnik, Ł. Risk Factors of Intervertebral Disc Pathology-A Point of View Formerly and Today-A Review. J Clin Med 2021, 10, 409. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.A.; Amin, A.; Omeis, I.; Gokaslan, Z.L.; Gottfried, O.N. Implications of Spinopelvic Alignment for the Spine Surgeon. Neurosurgery 2015, 76 Suppl. S1, S42–S56. [Google Scholar] [CrossRef] [PubMed]
- Ao, S.; Liu, Y.; Wang, Y.; Zhang, H.; Leng, H. Cervical Kyphosis in Asymptomatic Populations: Incidence, Risk Factors, and Its Relationship with Health-Related Quality of Life. J Orthop Surg Res 2019, 14, 322. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, L.A. The Biomechanics of Cervical Spondylosis. Adv Orthop 2012, 2012, 493605. [Google Scholar] [CrossRef]
- Jaeger, J.O.; Oakley, P.A.; Moore, R.R.; Ruggeroli, E.P.; Harrison, D.E. Resolution of Temporomandibular Joint Dysfunction (TMJD) by Correcting a Lateral Head Translation Posture Following Previous Failed Traditional Chiropractic Therapy: A CBP® Case Report. Journal of physical therapy science 2018, 30, 103–107. [Google Scholar] [CrossRef]
- Maruyama, T.; Kitagawa, T.; Takeshita, K.; Mochizuki, K.; Nakamura, K. Conservative Treatment for Adolescent Idiopathic Scoliosis: Can It Reduce the Incidence of Surgical Treatment? Pediatr Rehabil 2003, 6, 215–219. [Google Scholar] [CrossRef]
- Fortner, M.O.; Oakley, P.A.; Harrison, D.E. Treating “slouchy” (Hyperkyphosis) Posture with Chiropractic Biophysics®: A Case Report Utilizing a Multimodal Mirror Image® Rehabilitation Program. J Phys Ther Sci 2017, 29, 1475–1480. [Google Scholar] [CrossRef]
- Fedorchuk, C.; Lightstone, D.F.; McCoy, M.; Harrison, D.E. Increased Telomere Length and Improvements in Dysautonomia, Quality of Life, and Neck and Back Pain Following Correction of Sagittal Cervical Alignment Using Chiropractic BioPhysics® Technique: A Case Study. J Mol Genet Med 2017, 11. [Google Scholar] [CrossRef]
- Ferrantelli, J.R.; Harrison, D.E.; Harrison, D.D.; Stewart, D. Conservative Treatment of a Patient with Previously Unresponsive Whiplash-Associated Disorders Using Clinical Biomechanics of Posture Rehabilitation Methods. J Manipulative Physiol Ther 2005, 28, e1–8. [Google Scholar] [CrossRef]
- Fortner, M.O.; Oakley, P.A.; Harrison, D.E. Alleviation of Posttraumatic Dizziness by Restoration of the Cervical Lordosis: A CBP® Case Study with a One Year Follow-Up. Journal of Physical Therapy Science 2018, 30, 730–733. [Google Scholar] [CrossRef]
- Fortner, M.O.; Oakley, P.A.; Harrison, D.E. Alleviation of Chronic Spine Pain and Headaches by Reducing Forward Head Posture and Thoracic Hyperkyphosis: A CBP® Case Report. J Phys Ther Sci 2018, 30, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Janik, T.J.; Holland, B. A New 3-Point Bending Traction Method for Restoring Cervical Lordosis and Cervical Manipulation: A Nonrandomized Clinical Controlled Trial. Arch Phys Med Rehabil 2002, 83, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A.; Hegazy, F.; Harrison, D.E. Does Improvement towards a Normal Cervical Sagittal Configuration Aid in the Management of Cervical Myofascial Pain Syndrome: A 1- Year Randomized Controlled Trial. BMC Musculoskelet Disord 2018, 19, 396. [Google Scholar] [CrossRef]
- Morningstar, M. Cervical Curve Restoration and Forward Head Posture Reduction for the Treatment of Mechanical Thoracic Pain Using the Pettibon Corrective and Rehabilitative Procedures. J Chiropr Med 2002, 1, 113–115. [Google Scholar] [CrossRef]
- Morningstar, M.W. Cervical Hyperlordosis, Forward Head Posture, and Lumbar Kyphosis Correction: A Novel Treatment for Mid-Thoracic Pain. J Chiropr Med 2003, 2, 111–115. [Google Scholar] [CrossRef]
- Moustafa, I.M.; Diab, A.A.; Taha, S.; Harrison, D.E. Addition of a Sagittal Cervical Posture Corrective Orthotic Device to a Multimodal Rehabilitation Program Improves Short- and Long-Term Outcomes in Patients With Discogenic Cervical Radiculopathy. Arch Phys Med Rehabil 2016, 97, 2034–2044. [Google Scholar] [CrossRef]
- Brinjikji, W.; Luetmer, P.H.; Comstock, B.; Bresnahan, B.W.; Chen, L.E.; Deyo, R.A.; Halabi, S.; Turner, J.A.; Avins, A.L.; James, K. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. American journal of neuroradiology 2015, 36, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Vining, R.D.; Potocki, E.; McLean, I.; Seidman, M.; Morgenthal, A.P.; Boysen, J.; Goertz, C. Prevalence of Radiographic Findings in Individuals with Chronic Low Back Pain Screened for a Randomized Controlled Trial: Secondary Analysis and Clinical Implications. J Manipulative Physiol Ther 2014, 37, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Karis, D.S.A.; Vleggeert-Lankamp, C.L.A. Association between Modic Changes, Disc Degeneration, and Neck Pain in the Cervical Spine: A Systematic Review of Literature. Spine J 2020, 20, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Otani, K.; Sekiguchi, M.; Konno, S.-I. Relationship between Lumbar Disc Degeneration on MRI and Low Back Pain: A Cross-Sectional Community Study. Fukushima J Med Sci 2022, 68, 97–107. [Google Scholar] [CrossRef]
- Brinjikji, W.; Diehn, F.E.; Jarvik, J.G.; Carr, C.M.; Kallmes, D.F.; Murad, M.H.; Luetmer, P.H. MRI Findings of Disc Degeneration Are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis. AJNR Am J Neuroradiol 2015, 36, 2394–2399. [Google Scholar] [CrossRef] [PubMed]
- Modic, M.T.; Ross, J.S. Lumbar Degenerative Disk Disease. Radiology 2007, 245, 43–61. [Google Scholar] [CrossRef] [PubMed]
- Eubanks, J.D.; Lee, M.J.; Cassinelli, E.; Ahn, N.U. Prevalence of Lumbar Facet Arthrosis and Its Relationship to Age, Sex, and Race: An Anatomic Study of Cadaveric Specimens. Spine 2007, 32, 2058. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; Tamai, K.; Yamato, M.; An, H.S.; Yoshida, H.; Saotome, K.; Kurihashi, A. The Relationship between Facet Joint Osteoarthritis and Disc Degeneration of the Lumbar Spine: An MRI Study. Eur Spine J 1999, 8, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Pollintine, P.; Hole, B.D.; Dolan, P.; Adams, M.A. Discogenic Origins of Spinal Instability. Spine 2005, 30, 2621. [Google Scholar] [CrossRef]
- Fujiwara, A.; Lim, T.-H.; An, H.S.; Tanaka, N.; Jeon, C.-H.; Andersson, G.B.J.; Haughton, V.M. The Effect of Disc Degeneration and Facet Joint Osteoarthritis on the Segmental Flexibility of the Lumbar Spine. Spine 2000, 25, 3036. [Google Scholar] [CrossRef]
- Mimura, M.; Panjabi, M.M.; Oxland, T.R.; Crisco, J.J.; Yamamoto, I.; Vasavada, A. Disc Degeneration Affects the Multidirectional Flexibility of the Lumbar Spine. Spine (Phila Pa 1976) 1994, 19, 1371–1380. [Google Scholar] [CrossRef]
- Hassett, G.; Hart, D.J.; Manek, N.J.; Doyle, D.V.; Spector, T.D. Risk Factors for Progression of Lumbar Spine Disc Degeneration: The Chingford Study. Arthritis & Rheumatism 2003, 48, 3112–3117. [Google Scholar]
- Machino, M.; Nakashima, H.; Ito, K.; Ando, K.; Ito, S.; Kato, F.; Imagama, S. Cervical Disc Degeneration Is Associated with a Reduction in Mobility: A Cross-Sectional Study of 1211 Asymptomatic Healthy Subjects. J Clin Neurosci 2022, 99, 342–348. [Google Scholar] [CrossRef]
- Groh, A.M.R.; Fournier, D.E.; Battié, M.C.; Séguin, C.A. Innervation of the Human Intervertebral Disc: A Scoping Review. Pain Med 2021, 22, 1281–1304. [Google Scholar] [CrossRef] [PubMed]
- Banno, T.; Togawa, D.; Arima, H.; Hasegawa, T.; Yamato, Y.; Kobayashi, S.; Yasuda, T.; Oe, S.; Hoshino, H.; Matsuyama, Y. The Cohort Study for the Determination of Reference Values for Spinopelvic Parameters (T1 Pelvic Angle and Global Tilt) in Elderly Volunteers. Eur Spine J 2016, 25, 3687–3693. [Google Scholar] [CrossRef]
- Daffin, L.; Stuelcken, M.C.; Sayers, M.G.L. The Effect of Cervical Spine Subtypes on Center of Pressure Parameters in a Large Asymptomatic Young Adult Population. Gait Posture 2019, 67, 112–116. [Google Scholar] [CrossRef] [PubMed]
- de Schepper, E.I.T.; Damen, J.; van Meurs, J.B.J.; Ginai, A.Z.; Popham, M.; Hofman, A.; Koes, B.W.; Bierma-Zeinstra, S.M. The Association between Lumbar Disc Degeneration and Low Back Pain: The Influence of Age, Gender, and Individual Radiographic Features. Spine (Phila Pa 1976) 2010, 35, 531–536. [Google Scholar] [CrossRef]
- Fedorchuk, C.; Lightstone, D.F.; McRae, C.; Kaczor, D. Correction of Grade 2 Spondylolisthesis Following a Non-Surgical Structural Spinal Rehabilitation Protocol Using Lumbar Traction: A Case Study and Selective Review of Literature. J Radiol Case Rep 2017, 11, 13–26. [Google Scholar] [CrossRef]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Troyanovich, S.J.; Harrison, S.O. A Review of Biomechanics of the Central Nervous System--Part II: Spinal Cord Strains from Postural Loads. J Manipulative Physiol Ther 1999, 22, 322–332. [Google Scholar] [CrossRef]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Troyanovich, S.J.; Harrison, S.O. A Review of Biomechanics of the Central Nervous System--Part III: Spinal Cord Stresses from Postural Loads and Their Neurologic Effects. J Manipulative Physiol Ther 1999, 22, 399–410. [Google Scholar] [CrossRef]
- Henshaw, M.; Oakley, P.A.; Harrison, D.E. Correction of Pseudoscoliosis (Lateral Thoracic Translation Posture) for the Treatment of Low Back Pain: A CBP® Case Report. J Phys Ther Sci 2018, 30, 1202–1205. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-H.; Park, R.-Y.; Lee, S.-J.; Kim, J.-Y.; Yoon, S.-R.; Jung, K.-I. The Effect of the Forward Head Posture on Postural Balance in Long Time Computer Based Worker. Ann Rehabil Med 2012, 36, 98–104. [Google Scholar] [CrossRef]
- Knott, P.T.; Mardjetko, S.M.; Techy, F. The Use of the T1 Sagittal Angle in Predicting Overall Sagittal Balance of the Spine. The Spine Journal 2010, 10, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Labelle, H.; Roussouly, P.; Berthonnaud, E.; Dimnet, J.; O’Brien, M. The Importance of Spino-Pelvic Balance in L5-S1 Developmental Spondylolisthesis: A Review of Pertinent Radiologic Measurements. Spine (Phila Pa 1976) 2005, 30, S27–34. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, C.; Berjano, P. Classification of Sagittal Imbalance Based on Spinal Alignment and Compensatory Mechanisms. Eur Spine J 2014, 23, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Kim, K.-T.; Seo, E.-M.; Suk, K.-S.; Kwack, Y.-H.; Son, E.-S. The Influence of Thoracic Inlet Alignment on the Craniocervical Sagittal Balance in Asymptomatic Adults. J Spinal Disord Tech 2012, 25, E41–47. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Lafage, R.; Smith, J.S.; Protopsaltis, T.S.; Lafage, V.C.; Challier, V.; Shaffrey, C.I.; Radcliff, K.; Arnold, P.M.; Chapman, J.R.; et al. Impact of Dynamic Alignment, Motion, and Center of Rotation on Myelopathy Grade and Regional Disability in Cervical Spondylotic Myelopathy. J Neurosurg Spine 2015, 23, 690–700. [Google Scholar] [CrossRef]
- Nicholson, K.J.; Millhouse, P.W.; Pflug, E.; Woods, B.; Schroeder, G.D.; Anderson, D.G.; Hilibrand, A.S.; Kepler, C.K.; Kurd, M.F.; Rihn, J.A.; et al. Cervical Sagittal Range of Motion as a Predictor of Symptom Severity in Cervical Spondylotic Myelopathy. Spine (Phila Pa 1976) 2018, 43, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.; Sanchez, L.; Harrison, D. MEDICAL RADIOLOGISTS MAY NOT CONSIDER THE CERVICAL LORDOSIS IN RADIOLOGY REPORTS: A COMPARISON OF SUBJECTIVE QUALITATIVE ASSESSMENT VERSUS OBJECTIVE QUANTITATIVE MENSURATION IN 100 CONSECUTIVE PATIENTS AT ONE MEDICAL IMAGING CENTER. J Contemporary Chiropr 2021, 4, 17–25. [Google Scholar]
- Okada, E.; Matsumoto, M.; Fujiwara, H.; Toyama, Y. Disc Degeneration of Cervical Spine on MRI in Patients with Lumbar Disc Herniation: Comparison Study with Asymptomatic Volunteers. European Spine Journal 2011, 20, 585–591. [Google Scholar] [CrossRef]
- Protopsaltis, T.S.; Lafage, R.; Smith, J.S.; Passias, P.G.; Shaffrey, C.I.; Kim, H.J.; Mundis, G.M.; Ames, C.P.; Burton, D.C.; Bess, S.; et al. The Lumbar Pelvic Angle, the Lumbar Component of the T1 Pelvic Angle, Correlates With HRQOL, PI-LL Mismatch, and It Predicts Global Alignment. Spine (Phila Pa 1976) 2018, 43, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Raastad, J.; Reiman, M.; Coeytaux, R.; Ledbetter, L.; Goode, A.P. The Association between Lumbar Spine Radiographic Features and Low Back Pain: A Systematic Review and Meta-Analysis. Semin Arthritis Rheum 2015, 44, 571–585. [Google Scholar] [CrossRef]
- Sadler, S.G.; Spink, M.J.; Ho, A.; De Jonge, X.J.; Chuter, V.H. Restriction in Lateral Bending Range of Motion, Lumbar Lordosis, and Hamstring Flexibility Predicts the Development of Low Back Pain: A Systematic Review of Prospective Cohort Studies. BMC Musculoskelet Disord 2017, 18, 179. [Google Scholar] [CrossRef] [PubMed]
- Silber, J.S.; Lipetz, J.S.; Hayes, V.M.; Lonner, B.S. Measurement Variability in the Assessment of Sagittal Alignment of the Cervical Spine: A Comparison of the Gore and Cobb Methods. J Spinal Disord Tech 2004, 17, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Troyanovich, S.J.; Harrison, D.; Harrison, D.D.; Harrison, S.O.; Janik, T.; Holland, B. Chiropractic Biophysics Digitized Radiographic Mensuration Analysis of the Anteroposterior Cervicothoracic View: A Reliability Study. J Manipulative Physiol Ther 2000, 23, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Kawakami, N.; Nishiwaki, Y.; Goto, M.; Tsuji, T.; Obara, T.; Imagama, S.; Matsumoto, M. Traction versus Supine Side-Bending Radiographs in Determining Flexibility: What Factors Influence These Techniques? Spine 2007, 32, 2604–2609. [Google Scholar] [CrossRef] [PubMed]
- Young, W.F. Cervical Spondylotic Myelopathy: A Common Cause of Spinal Cord Dysfunction in Older Persons. Am Fam Physician 2000, 62, 1064–1070. [Google Scholar] [PubMed]
- Yu, M.; Silvestre, C.; Mouton, T.; Rachkidi, R.; Zeng, L.; Roussouly, P. Analysis of the Cervical Spine Sagittal Alignment in Young Idiopathic Scoliosis: A Morphological Classification of 120 Cases. Eur Spine J 2013, 22, 2372–2381. [Google Scholar] [CrossRef]
- Yu, M.; Zhao, W.-K.; Li, M.; Wang, S.-B.; Sun, Y.; Jiang, L.; Wei, F.; Liu, X.-G.; Zeng, L.; Liu, Z.-J. Analysis of Cervical and Global Spine Alignment under Roussouly Sagittal Classification in Chinese Cervical Spondylotic Patients and Asymptomatic Subjects. Eur Spine J 2015, 24, 1265–1273. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



