
Submitted:
08 February 2024
Posted:
09 February 2024
You are already at the latest version
Abstract
People are increasingly encouraged to reduce animal food consumption and shift towards plant-based diets, however the implications for children’s health are unclear. In this narrative review of research in high-income settings, we summarize evidence on the increasing consump-tion of plant-based diets in children, and update an earlier systematic review regarding their associations with children’s health outcomes. The evidence indicates that vegan but not vege-tarian diets can restrict growth relative to omnivorous children, and increase the risk of being stunted and underweight although the percentage affected is relatively small. Bone mineral content is reduced in vegetarian and especially vegan children, compared to omnivores. Both vegetarian and vegan children who do not use vitamin B12 supplements manifest with B12 defi-ciency, however supplementation rectifies this problem. Both vegetarians and vegans have lower concentrations of 25 (OH)D if unsupplemented, and lower body iron stores, but usually have normal iron metabolism markers. Both groups are at risk of iodine deficiency and this might affect thyroid health. Children consuming a vegan diet have more favorable lipid profile than omniv-orous children, however the results for vegetarian diet are inconsistent and vary by outcome. Based on the same scientific evidence, national and international dietary recommendations are heterogeneous, with some countries supporting plant-based diets among infants, children and adolescents, and others discouraging them. We offer a research roadmap, highlighting what is needed to provide adequate evidence to harmonize dietary recommendations for plant-based diets in children. A number of measures should urgently be introduced at international and na-tional levels to improve the safety of their use in children.
Keywords:
Keywords: vegetarian
; vegan
; children
; secular trend
; bone health
; growth
; nutrient deficiencies
; clinical practice
1. Introduction
Around the world, populations are being encouraged to switch to plant-based diets in order to reduce the environmental burden linked to animal-food agriculture [1,2]. It has been estimated that the adverse environmental impact of a high-meat diet is four times greater than that of a vegan diet when it comes to greenhouse gas emissions and land use, almost three times higher for impacting biodiversity, and two times higher for water use [3]. However it is not just meat production that elevates greenhouse emissions; dairy foods rank second [4], with dairy cattle being responsible for 20% of food-related gas emitted, following beef cattle with a value of 41% [5].The call to reduce animal-based foods in human diets, originating from within academia [2], has translated recently into numerous national and international dietary guidelines around the world [1,6,7,8].
Consistent with such encouragement, numerous sources of data indicate that more people in high income countries are adopting plant-based diets, including vegan and vegetarian diets. Although formal estimates are available for only a few countries through diet and lifestyle surveys [9,10], an increase in the popularity of plant-based diet keywords in google searches [11] and market trend research also indicate a rapid rate of growth in plant-based dietary patterns in numerous high-income countries [10,12]. Beyond environmental concerns, the main reasons for these trends are concerns over animal welfare and human health [13].
Because plant-based diets restrict the intake of specific food groups, they may have particular implications for children’s health. Vegan and vegetarian diets eliminate several food groups, which changes the profile of micro- and macro-nutrient intake and may increase the risk of inadequate nutrient intakes and nutrient deficiencies, including those of protein, calcium, vitamin D, iodine, zinc, iron and Omega-3 essential fatty acids [14]. Plant-based diets are also lower in energy density, which could increase the risk of energy malnutrition. These dietary characteristics can potentially affect the growth and development of children. However, data remain very sparse. The majority of research comes from adult studies, and many of the published studies in children are now several decades old and included only vegetarian subjects [15]. Importantly, the last decade has seen a new wave of studies of plant-based diets in children that provide more detailed health outcome data, including biomarkers in vegan children [16,17].
Of particular concern, the contemporary increase in plant-based alternatives to animal products is driven by ultra-processed foods, with markedly different and usually inferior nutritional profile compared to traditional animal- or plant-food alternatives [18]. In order to increase palatability, visual appeal and shelf-life, they also contain numerous food additives [1]. In their appearance and names, these products mimic meat, dairy and fish which may appear to indicate nutritional equivalence. However, data on their nutritional composition is scant and little is known about their health impacts [1]. Preliminary data indicate lower height in children substituting cow’s milk with plant-based milk [19], no difference in postprandial inflammatory response between plant-substitute versus real meat [20], and a link between chronic food-additive consumption and dysbiosis [21]. Recent data in adults suggest increased cardiovascular and cancer risks and total mortality linked to following ultra-processed-type plant-based diets [22].
While plant-based diets are becoming more popular, guidelines of pediatric and dietetics institutions around the world as to the safety of vegetarian and vegan diets in children guide are heterogenous and conflicting [1,23,24,25,26,27]. Additionally, most countries lack clear nutritional guidelines for vegetarian and vegan children. A recent Italian study found that nearly 9% of Italian infants were weaned to either a vegetarian or vegan diet, yet almost half (45.2%) of the parents were unable to obtain appropriate dietary advice from their pediatrician due to doctors’ lack of expertise in the subject [28].
All of these issues could affect the safety of plant-based diets among children. The aim of this narrative review is fourfold: (a) to review the available data on secular trends in the consumption of plant-based diets among children in high-income countries; (b) to conduct a systematic review of current data on health outcomes of children on vegetarian and vegan diets; (c) to review the heterogeneity of current dietary advice on plant-based diets for children, and (d) to propose a roadmap of the research questions that urgently need to be addressed, to in order to provide guidelines on how to safely implement these diets in children.
2. Secular trends in plant-based diets in children
Although national survey data remain rare, numerous sources indicate an increased rate of consumption of plant-based diets in high-income countries. In the last 10 years, the number of vegans in Germany increased 15-fold (from 0.1 million in 2012 to 1.58 million people in 2022) [29]. In the 2010 UK National Diet and Nutrition Survey (NDNS), 2% of both adults and children reported being vegetarian, with <1% following a vegan diet [30]. In the most recent 2019 NDNS Rolling Programme, the proportion who self-identified as vegetarian or vegan had risen to 4.5%, a 50% increase overall [31]. According to the Euromonitor Health and Nutrition Survey 2020, the percentage of vegans in Western Europe, US and Australia varied from 1.8 to 4.5%, and of vegetarians from 2.5 to 6.5%, while the proportion reporting that they restrict intake of animal products varied from 28 to 48% [13]. In these settings, therefore, up to half the population reported at least some degree of reducing their dietary intake of animal foods.
These self-reported diet patterns are consistent with data on food sales. In the US, the market for plant-based alternatives to animal products grew three times faster than overall food sales in 2021 [18]. In Australia, between 2014 and 2016 the number of vegan food products rose by 92% [32]. The market value of plant-based food sales and unit sales grew in 13 European countries by 21% in just three years, between 2020 and 2022 [33].
It is to be expected that children will follow adults in these trends. According to the 2021 BBC Good Food Nation survey in the UK [34], 8% of British children declared themselves as vegan, 13% vegetarian, and 21% would like to adopt vegetarianism. Another UK poll indicated that 70% of children wanted to see more vegetarian and vegan meals on their school menu [35]. While data remain scarce, therefore, there is evidence of increasing consumption of vegan and plant-based diets in children in high-income populations.
3. Associations of plant-based diets with child health outcomes
To summarize the literature on this topic, we first describe the previous systematic review by Schuermann et al. [15], and then update it. Schuermann et al. systematically reviewed data on vegetarian and vegan compared to omnivore children from articles published between the 1980s and 2013 [15]. Case-reports and studies from non-industrialized countries were excluded. In their analysis, 24 publications from 16 studies met the inclusion criteria. The studies had heterogeneous methodology, were mostly cross-sectional, usually had small sample sizes, used various definitions of vegetarianism (one study included pescovegetarians (fish-eaters) as vegetarians [36]), often lacked control groups, and tended to include participants from higher social classes. Study samples of vegetarian or vegan children usually included fewer than 100 individuals. The majority of research in that period was conducted on vegetarian children, and in Central Europe (n = 11 studies), with a large proportion of studies from Poland (n = 7) [37,38,39,40,41,42,43,44] but also the UK (n = 4) [45,46,47]. Eight studies were undertaken in the USA [48,49,50,51,52,53,54,55] and most of the US studies were conducted among the Seventh-day Adventist (SDA) population. The majority of studies were published before 2000. Five publications were issued in the 1980s (4 US, 1 UK), ten in the 1990s (1 German, 2 British, 2 Slovak, 1 Belgian and 4 US), and the remaining 9 after 2000 (7 Poland, 1 UK, 1 US).
The age range of the children spanned 0 to 18 years; two studies (43,52) included only infants and/or toddlers. Only two studies focused on vegan diets [45,50]. Overall, children following meat-free (vegetarian, vegan, and, from one study only- pescovegetarian) diets were either similar, or somewhat below, the national or omnivore (OM) reference group in terms of height, weight, body mass index (BMI), fat mass, lean mass and skinfold measures. Vegetarian children demonstrated altered metabolism of bone markers, suggesting impaired bone turnover rate. There were no data on the bone health of vegan children from that research period. Vegetarian children had lower total and LDL cholesterol levels (2 studies). In comparison to the omnivore group or physiological reference data, studies from this period suggested either normal micronutrient status or increased risk of iron and vitamin D3 deficiency in vegetarian children. There were no studies on blood micronutrient status in vegans. Schuermann et al. concluded that the existing data at that time did not allow firm conclusions to be drawn on the health benefits or risks of vegetarian or vegan diets in children and adolescents in industrialized countries[15].
To update the systematic review, we searched the database MEDLINE (via PudMed) for articles in English, German or Polish from the period: 2013- 2023. Only studies assessing health outcomes were selected, those reporting dietary intakes only were excluded. For search terms, the following search string was used: (vegetarian OR vegetarian* OR vegan OR vegan*) AND (infant OR infant* OR infancy OR child OR child* OR toddler OR toddler* OR children OR children * OR adolescent OR adolescent* OR adolescence OR pregnant OR pregnancy OR breastfeeding OR breastfed). Case studies and studies from non-industrialized countries were not included, as the study participants, apart from following plant-based diets, might also have been exposed to inadequate food intake. The Prisma flow diagram for our search results is presented in Figure 1.
One independent reviewer (RQ) used the revised Downs and Black Quality Index score system, known to be a reliable and valid tool for assessing bias in observational and randomized studies to assess the quality of individual publications [57]. The quality assessment tool provided an overall score based on four assessed domains; reporting, external validity, internal validity bias and internal validity confounding. Each domain had an overall total score out of 10, 3, 7 and 6 respectively. Item 27 relating to the statistical power was given a score of 1when a power analysis had been conducted. Thus, the highest possible score for the checklist was 28. Each paper was assigned a grade of “excellent” (24–28 points), “good” (19–23 points), “fair” (14–18 points) or “poor” (<14 points).
Fourteen publications from 13 studies met the same inclusion criteria as those used previously. The majority of the studies were cross-sectional (11), but 2 were longitudinal.
Most studies assessed vegetarians only, however 6 assessed vegans [16,58,59,60,61,62,63]. The sample size ranged from 6 (vegan) [59] to 248 (vegetarian) children [64]. The average sample size of vegan or vegetarian groups was 81 children, being 79 for vegans only, and 83 for vegetarians only. In one small study the vegetarians were described as those who also eat fish (n=10) [59]. The age range of the studies spanned 0 to 18 years. Only 3 studies [16,58,65] assessed socio-economic class (SES) of the family, and the majority of participants were from higher SES. Six studies assessed physical activity, 5 by questionnaires. Only one study, from Poland, [16] matched vegetarian and vegan children with omnivore controls by age, sex, maternal education and rural/urban location. This was also the only study to obtain objective data on measured physical activity, a potential confounder of associations of child diet group with health outcomes such as body fat content and cardiovascular risk.
The majority of studies were conducted in central Europe (Poland 7, Germany 2, Czech Republic 1), or other European countries (Finland 1, Italy 1); there was one study from Canada. Unlike in the previous period (before 2017) in which some studies were conducted among Seven Day Adventists [66] or collective communities [50], none of the newer studies were conducted specifically among a religious or other belief group. Most of them assessed dietary intake as well as health outcomes.
These new studies contribute new knowledge on biomarkers in vegetarian and especially vegan children, and provide the first data on bone health in vegan children, more comprehensive bone data in vegetarians, and the first data on iodine status and its effect on thyroid function in vegetarian and vegan children. Equally importantly, they provide data on contemporary vegan children. A summary of the design and findings of each study is presented in Table 1.
3.1. Body composition and anthropometry
All studies measured at least basic anthropometry. Regarding the comparison of vegetarian children with omnivores, most studies did not observe differences in height (HT) and weight (WT), BMI or body composition. However, some studies showed tendencies to lower values among children on vegetarian and especially on vegan diets. More vegetarian (2.4%) than omnivore toddlers (0%) were classified as stunted or wasted in the German VeChi DietStudy [58]. In a longitudinal Canadian study [64], vegetarian children had higher odds of being underweight (BMI z-score <−2), odds ratio 1.87 (95% CI 1.19, 2.96). In a Polish study [67], vegetarian children tended to have lower mean BMI z-scores (−0.18 ± 0.90 vs. 0.19 ± 0.80, p=0.06) compared to OM controls. Most studies did not show differences in body composition between vegetarian and omnivore children, however a Polish study showed lower gluteofemoral adiposity in vegetarian children using skinfold measurements (thigh girth z -score Δ –0.37, 95 CI% –0.69, –0.05), despite similar total fat and lean mass by deuterium dilution [16].
On the other hand, most studies assessing vegans reported lower values in WT, HT, BMD and body composition in comparison to the omnivore control group. In the VeChi DietStudy [58] more vegetarian (3.6%) than omnivore (0%) toddlers were classified as stunted or wasted. An Italian study [60] showed lower weight expressed in grams and in percentiles at birth and 6 and 12 months, along with shorter body length expressed in growth percentiles at 12 months, and lower BMI at 6 months of vegan compared to OM infants. In a German study [65], although no statistical difference in average HT, WT or mean BMI z-score was observed between vegan and omnivore children, there was a
tendency for vegan children to have lower values (BMI z-score: −0.6 ± 0.9 vs. −0.3 ± 1.0, p=0.15; height: 152 ± 19 vs. 156 ± 20 cm, p=0.49). Despite similar average ages between the three diet groups, vegan children were 4 cm shorter than omnivores. The difference did not achieve statistical significance, however that is due to the analysis incorporating a very wide age range included (6-18 years), resulting in very high standard deviations for height of 19-20 cm.
In a Polish study, vegan school-aged children were on average 3.2 cm shorter than omnivore children matched for sex, age and socio-economic status [16]. This study also showed lower fat indices of vegan children in all body regions measured by skinfolds (suprailiac skinfold z-scoreΔ –0.57, 95% CI –0.97, –0.18; triceps skinfold z-scoreΔ –0.47, 95% CI –0.86, –0.09), hip girth z – scoreΔ –0.58, 95% CI –0.94, –0.21); and lower fat mass index z-score in relation to omnivore (–0.72, 95% CI –1.12, –0.32) but similar lean mass measured by deuterium dilution. In a Czech study [63], significantly more vegan were in the <=3 percentile BMI category (7 out of 79) than in the other two groups (OM: 1 out of 52, vegetarian: 0 out of 69, p=0.03); however there was no overall difference in BMI, HT or WT percentile between groups. In another publication by the same authors [62], vegan children had lower BMI percentiles than omnivore children (vegan: 35.0, IQR 18.2, 63.5; OM: 40.0, IQR 19.5, 55.0, p=0.006)[62].
Overall, it seems that anthropometric markers in vegetarians are comparable to or slightly lower than the reference group, whereas vegan children tend to have lower values of WT, HT and fat mass than omnivore children. They also have higher risk of being stunted and wasted, however the percentage affected is relatively small.
3.2. Bone health
Four studies since 2013 provide the first data on the bone health of vegetarian (n=3) and vegan (n=1) children. These studies, assessing bone mineral content and bone metabolic markers, were all conducted in Poland. In vegetarians there were either no differences in total-body-less-head (TBLH) bone mineral content (BMC) ( 729g ± 226 vs. 768 g ± 237, p= 0.341and bone mineral density (BMD) (0.784 g/cm2± 0.068 vs. 0.799 g/cm2 ± 0.080 p= 0.700) in comparison to the OM reference group [16], or a tendency to lower values of the mean spine BMC ( 57.5g ± 18.7 vs. 63.0 ± 18.1, p= 0.09) and lumbar spine (L1-L4) BMD (0.617 g/cm2± 0.083 vs. 0.645 ± 0.083, p= 0.060) and of mean spine BMD z-score (-0.58 ± 0.72 vs. - 0.19 ± 0.64,) and mean lumbar spine BMD z-score (−0.73 g/cm2 ± 0.91 vs. −0.51 ± 0.75, p= 0.11) in vegetarian compared to OM children in analyses unadjusted for bone or body size [75]. Vegetarians had significantly higher levels of the blood biochemical markers BALP ( 130.7 U/L ± 39.9 vs. 108.4 ± 37.1, p=0.002) and CTX-I (1.976 ± 0.538 vs. 1.749 ± 0.526, p= 0.027), which were interpreted as a higher rate of bone turnover in vegetarian compared to OM children [69]. In another study from the same group, bone and body size unadjusted TBLH-BMD z-score (but not absolute values of TBLH BMD) were lower in vegetarians in comparison to omnivores (-0.583 ± 0.718 vs. -0.194 ± 0.642, p= 0.009). Similar trend was observed for L2-L4 spine BMD (0.621 ± 0.089 vs. 0.649 ± 0.096, p= 0.046) and BMD L2-L4 z-score (- 0.877 ± 0.858 vs. -0.496 ± 0.791, p= 0.019). Vegetarian children had also higher PTH (40.8 pg/Ml, 95%CI 29.5, 57.2, vs. 32.1, 95% CI 23.1, 42.5, p=0.015). In another study from Poland, there was no difference in TBLH BMC, L2–L4 BMC or bone mineral apparent density (BMAD) z-score between 5 – 10 year old vegetarian children in comparison to age, sex and SES status matched omnivores[16]. Unlike in the previous Polish studies investigating bone health of vegetarian children, this study adjusted BMC values for body size and bone area. BMAD adjusts BMC for calculated bone volume rather than bone area,
The only study to evaluate vegan diets [16] showed lower TBLH (Δ-3.7%; 95% CI –7.0, –0.4) and lumbar spine (L2-L4) (Δ-5.6%; 95%CI (–10.6, –0.5) BMC in Polish vegan compared to OM children aged 5-10 years, in analyses adjusted for bone size in order to take into account the lower body size of the vegans. This was confirmed by another approach that corrected for bone size, whereby BMAD z score and percentile were significantly lower for vegans only.
Overall, the available data show a trend to lower BMC and BMD values in vegetarian children, however significant differences were observed in bone and body size unadjusted analyses only. Vegan children have lower values of BMC, the difference attenuates, but persists after adjusting for bone and body size. Vegetarian children have altered bone metabolism markers. There are no data on bone marker metabolism in vegan children.
3.3. Nutritional biomarkers
Seven publications (from 6 studies), assessed nutritional biomarkers, and 5 of these addressed vegan as well as vegetarian children.
Overall, vegetarian children had lower levels of ferritin in some studies (median levels in ng/mL 21.0, IQR 15.0-29.0 vs.27.0 IQR, 21.6, 48.7, p=0.003) [68]; 29, IQR 20-39 vs. 38, IQR 26-52, p= 0.0312) [65], but not in all studies [16,64]. There was no significant difference in haemoglobin (Hb) concentrations [16,65] and a Polish study [68] showed no difference in transferrin levels between vegetarian and omnivore children; while other hematologic parameters and serum iron were within the reference range in the vegetarian children. Vegans, on the other hand, had lower indices of ferritin in 2 studies [16,65]
(Δ in relation to OM –25 %, 95%CI –44.0 - –5.0); median (ng/mL) in vegans 29, IQR 22- 42 vs. 38 in OM, IQR 26 - 52), lower levels of Hb (Δ in g/dL –0.37, 95%CI –0.69, –0.05), erythrocytes (Δ in M/μL –0.23, 95%CI –0.33, –0.12) in one study [16], but similar Hb concentrations to the OM group in another study that had assessed iron metabolism [65].
Vegetarians had lower levels of vitamin B12 and holotranscobalamin (holoTC) and higher levels of other biomarkers suggesting insufficiency of vitamin B12 (methyl malonic acid (MMA), homocysteine (Hs)) than the OM group if the children did not supplement vitamin B12 (serum vit. B12 difference in pmol/L –90.9, 95%CI –156.7, –25.1) [16,63,65]. These differences disappeared in supplemented vegetarian children [16,63]. Similar trends were reported for vegan children, however the data indicate that vitamin B12 deficiency in unsupplemented vegans tends to be more pronounced (serum vit. B12 difference in pmol/L –217.6, 95%CI –305.7, –129.5) [16]. Moreover, a Czech study [63] reported vitamin B12 hypervitaminosis in over-supplementing vegans and vegetarians, the significance of which is unknown.
Across different studies, the rates of vit B12 supplementation were as follows: 39% and 88% in German vegetarians and vegans respectively aged 6-18 years [65]; 35 % and 95% respectively among German vegetarian and vegan toddlers aged 1-3 years [76]; 70% in both vegetarian and vegan children aged 5-10 years in Poland [16]; 68% and 85% of vegetarian and vegan Czech children respectively aged 0-18 years; and 72% in a subgroup of both vegetarian and vegan Czech infants respectively [63]. Based on this data, substabtial proportions of children of vegan and vegetarian children across European populations are not receiving vitamin B12 supplements, which can result in serious hematological, metabolic and neurological complications [77,78,79]. The available evidence regarding the rates of supplementation of vitamin B12 in vegetarian and vegan children is summarized in Figure 2.
Other nutritional biomarkers measured were fat-soluble vitamins A, D and DHA, which were markedly lower among vegan children in a small study of vegan and vegetarian Finnish preschoolers [59]. A study that measured serum vitamin B2, 25- hydroxy vitamin D (25 (OH) D) and folate among German children aged 6-18 years found that only folate differed between the groups, being highest in vegan children [61]. All dietary groups in this study had a high prevalence (>30%) of 25(OH)D and vitamin B2 concentrations below reference values, however the percentage for vitamin B2 tended to be higher in vegan and/or vegetarian than in OM children (vegetarian: 50%, vegan: 54%, omnivore: 37%).
In a Polish study of school-aged children, 25 (OH) D was lower in both unsupplemented vegetarian (Δ in nmol/L –7.1, 95%CI –13.8, –0.3) and vegan (Δ in nmol/L –13.3, 95%CI –20.3, –6.2) children compared to OM controls, with the difference most pronounced in vegans [16]
A Czech study was the first to measure iodine in spot urine (UIC) in vegan and vegetarian infants and children [62]. The UIC values were highest in the OM control group, followed by vegetarian, with the lowest levels among the vegan children. Forty-two percent of vegans, 35% of vegetarians and 20% of omnivore children (p = 0.06) met the criteria for iodine deficiency (i.e., UIC < 100 µg/l). This may have health consequences, as the same study found effects on thyroid function. Higher levels of fT4 were found in vegans than in the OM (p < 0.001), and higher presence of anti-thyroglobulin antibodies (AhTGc) in vegetarian (18.2%) and vegan (35.0%) than in the OM group (2.1%) (p < 0.001) was detected. It was hypothesized that this was due lower iodine intake among vegetarian and vegan children.
Serum amino acid levels (valine, lysine, leucine, isoleucine) were lower in Polish vegetarian children compared to OM controls [73], while branched-chained amino acids (valine, leucine, and isoleucine) were lower in preschool Finish vegan than in omnivores in a study of Hovinen et al. 2023 [59]. However, the health implications of these differences remain unclear.
Overall, both vegetarian and especially vegan children develop signs of vitamin B12 deficiency if their diet is not supplemented with that nutrient. The average percentage of studied vegetarian and vegan children whose diet is not supplemented with vit. B12 is ca. 30%. Both vegetarian and vegan children have lower levels of iron stores (ferritin), however other iron metabolism markers are usually similar to or slightly lower than the reference group. Both vegetarian and especially vegan children are at risk of vitamin D deficiency if they do not supplement, and of inadequate iodine intake. The suboptimal iodine status of vegetarian and vegan children might affect thyroid function. Vegans might have lower levels of other, especially fat-soluble nutrients, however more studies are needed to confirm the preliminary findings.
3.4. Cardiometabolic risk factors
In adults, plant-based diets have been associated with lower NCD risk [80], however whether such benefits are evident in childhood has only recently been addressed.
Polish 5-10 year old vegetarian children had significantly higher ratios of anti-inflammatory to pro-inflammatory adipokines compared with omnivore children [81]. Another study from Poland, assessing 5-10 year old vegetarian and SES matched omnivore children found lower total cholesterol (TC) (Δ in mg/dL –11.5, 95%CI –22.4, –0.6) and HDL-cholesterol (HDL-C) (Δ in mg/dL –6.5, 95%CI –11.1, –1.8) in vegetarians; however also higher serum fasting VLDL-cholesterol (Δin % 14.0, 95%CI 1.0, -28.0), triglycerides (dΔin % 19.0, 95%CI 5.0, 33.0) and glucose levels (Δ in mg/dL 3.1, 95%CI 0.9, 5.4), suggesting less favourable cardiometabolic risk profile in comparison to the meat-eating reference group. There were no differences in fasting insulin levels, high sensitivity C-reactive protein (hs-CRP) or ultrasonography assessed carotid intima-media thickness (cIMT) between vegetarian and omnivore children[16]. German 6-18 year old vegetarians did not differ from the OM reference group in any of the lipid fractions measured: TC, non-HDL-C, HDL-C, LDL-cholesterol (LDL-C) or triglycerides (TG) [61]. No association of serum lipids (non-HDL-C, TC, LDL-C HDL-C, and TG) with vegetarian diet was found in a longitudinal study of Canadian vegetarians [64]. Most recently Polish vegetarian (2-10 years) had significantly lower median values of total oxidant capacity and oxidative stress index along with CRP, and higher total antioxidant capacity [81].
More pronounced differences in cardiometabolic risk factors are reported in vegans. All fractions of blood lipid levels were significantly lower in vegan than omnivore Finish preschoolers [59]. Six to 18 year old German vegans had the lowest non-HDL-C concentration (median in mg/dL 78, IQR 63, 94 vs. 96, IQR 73, 113 in OM, p=0.0010) and LDL-C (median in mg/dL 68, IQR 57, 84 vs. 90, IQR 70, 106 in OM, p=0.0010) in comparison to omnivores, however their HDL-C levels didn’t differ from other groups [65].
Polish 5-10 year old vegans had significantly lower TC (Δ in mg/dL –35.6, 95%CI –48.3, –22.9), LDL-C (Δ–24.0, 95%CI –35.2, –12.9), and HDL-C (Δ–12.2, 95%CI –17.3, –7.1) fractions along with hs-CRP (Δ in % –81, 95%CI –123.0, –39.0) in comparison to the matched omnivore group [16]. The prevalence of low HDL-C levels was highest, and high LDL-C levels lowest, among vegans in this study. There was, however, no difference in fasting serum glucose, insulin levels or cIMT in comparison to omnivores.
Overall, evidence shows that children consuming a vegan diet have more favorable lipid profile than OM children, however the results for vegetarian diet were inconsistent and varied by outcome.
3.4.1. Assessment of bias
The assessments of bias for the articles identified in the review are tabulated in Table S1. Ten studies were rated as fair, and four as poor, with none being rated good or excellent. Very few studies provided data on vegan or vegetarian children that were representative of these populations. There is currently, therefore, a relatively weak evidence base regarding the effects of vegetarian and vegan diets on children’s health. Despite these limitations in the quality of evidence, the existing data does show relative consistency in the associations of both types of diet with health outcomes, as illustrated in Figure 3.
3.4.2. Conflicting position statements of medical and nutritional institutions around the world
While plant-based diets are increasingly consumed by children, and have implications for their health, as reviewed above, there is a notable lack of universal agreement as to the safety of vegetarian, and especially vegan, diets for children around the world. This was recently highlighted in particular for vegan children[82], here we summarize the scenario for both vegan and vegetarian diets.
Positive position statements come from the nutrition and dietetic institutions of the USA, the UK, Italy. The US American Academy of Nutrition and Dietetics (formerly known as American Dietetic Association) has been advocating the safety of well-balanced vegetarian and vegan diets for all life stages, including infancy, childhood and adolescence, for the last 30 years, in their position statements beginning in 1993 [83], followed by updates in 2009 [84] and 2016 [85]. Similarly, the British Dietetic Association (BDA) considers that a well-planned vegan diet can support healthy living in people of all ages [23]. The Italian Society of Nutrition states that a vegetarian diet (which is defined in the position paper as either lacto-ovo vegetarian or vegan diet), providing that it includes a variety of foods and vitamin B12 supplements, provides adequate nutrition for people of all ages [86].
The majority of the other pediatric and nutrition institution from around the world express a more or less cautionary approach, ranging from recommendation to exercise caution, or to avoid veganism in the early stages of life, to statements declaring an outright lack of support for this type of nutrition for children, with emphasis on the high risk of impairments of growth and development.
A joint statement of Health Canada, the Canadian Paediatric Society, Dietitians of Canada, and the Breastfeeding Committee for Canada from 2014 emphasizes the need for professional advice for vegetarian infants, and informs that with careful planning vegetarian diets can meet all the nutritional requirements of a growing child, provided the diet contains milk and eggs. It stresses a higher risk of vegan diets and the need for professional advice for vegan infants [87]. Earlier in 2010, the Canadian Paediatric Society warned of significant medical consequences of inappropriately planned diets in children and the lack of data as to the development, growth patterns and nutrition intakes of children on plant-based diets [88].
The Nutrition Committee of the Argentine Society of Pediatrics emphasizes that parents need to be aware of the risks associated with more restrictive diets, including vegetarian diets in childhood, stresses the need for professional nutritional guidance, and concludes that without careful planning those diets cannot be safely applied in childhood [89].
The Committee on Nutrition and Breastfeeding of the Spanish Pediatric Association emphasizes the need to carefully plan of vegetarian and vegan diets, however it does not recommend veganism, but rather an omnivore diet, or at least an ovo-lacto-vegetarian diet for infants and young children. [90]
The 2016 position statement of the German Nutrition Society (the DGA, Deutsche Gesellschaft fuer Ernaehrung) reads “(…) veganism is not recommended by DGE for (…) infants, children and adolescents.” [91] In the 2020 update to that statement, the DGE upheld their position and does not recommend veganism for children and adolescents, however it added that careful choice of foods, supplements, especially vitamin B12 can lead to adequate provision of nutrients, although this statement does not define any life stage.[92]
The French pediatric hepatology, gastroenterology and nutrition group (GFHGNP) states that a vegan diet does not provide all micronutrients and exposes children to inevitable nutritional deficiencies, which can have serious consequences for health, especially when introduced an early stage [93]. Therefore, GFHGNP does not recommend veganism in infants, children and adolescents.
The Belgian Royal Academy of Medicine does not recommend veganism in small children and describes it as potentially destabilizing growth [94].
The Committee of Human Nutrition Science of the Polish Academy of Sciences states in their 2019 position statement that veganism and other forms of vegetarianism excluding meat should not be applied in infants and young children, as they may adversely affect their development [27]. On a slightly different tone, the position statement of the Polish Society of Pediatric Gastroenterology, Hepatology and Nutrition from 2021 stresses that vegetarian, and especially vegan infants and young children require supplementation and regular consultations with nutrition specialist, and parents of vegan children should be aware that lack of supplementation can have serious consequences for the child’s health or even life [95].
According to the recently published opinion of the Norwegian Nutrition Council (NNC), vegetarian and vegan diets may be suitable at all life stages, including children, if they are well planned and accompanied by supplementation of vitamins and minerals[96]. To back its statement, the NNC cites the most recent US Academy of Nutrition and Dietetics position paper[24].
Finally, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition and the German Nutrition Society reflects the tone of the majority of European position statements, stating that in small children a vegan diet can meet nutrient requirements but that ‘the risks of failing to follow advice are severe’, and stressing the need for regular medical and expert dietetic supervision of vegan children[97].
In summary, the majority of the European statements express concerns about the risks and need for constant medical and dietetic supervision. However, as Kiely pointed out, over 40% of EU countries have general-practitioner led care with a median of 4-month pediatric training and inadequate nutrition education in medical schools. Hence, concerns that without specialist pediatrician and dietetic follow-up, growth and development delays due to an unbalanced vegan or vegetarian diet might not be detected in time, are valid [98].
The apparent contradictions between US and European statements was highlighted by Pawlak [99], who stressed the difference in the clarity of advice provided with regard to supplementation, dietary strategies for vegans, need for medical/dietetic supervision required and responsibilities of parents, and suggested that the efficacy of these statements should be tested in trials.
Despite the universally available evidence, therefore, different organizations are generating contrasting recommendations, with the differences especially marked for vegan diets but also evident for vegetarian diets. It remains unclear if these different approaches are based wholly on children’s health criteria, or whether they are also influenced by other factors such as planetary or animal welfare concerns.
4. Roadmap for future research
While the last decade has seen a new wave of research on the health impacts of plant-based diets in children, a number of outstanding questions remain, and would benefit from further research. These relate in particular to whether health benefits and risks vary by stage of development, the consequences of consuming new plant-based ultra-processed foods, and whether health effects seen in children will have longer-term impacts on adult health. We summarize a number of questions for both research and urgent practice regulation in Table 2.
Firstly, health professionals, especially doctors that provide regular medical care for children, depending on the countries’ medical models (general practitioners or/and pediatricians), should receive basic training enabling them to provide families of those children with fundamental nutritional and supplementation advice. This would prevent at least the most severe consequences of inadequate application of those diets in children. Secondly, dietary and supplementation guidelines tailored to different stages of children’s development but also catering for regional food and cultural habits, should be introduced in each country (as illustrated in Figure 2). This would facilitate both doctors and dieticians to give more detailed dietary counselling in the context of time-constraints of medical consultation and/or lack of advanced nutritional training. Additionally, it would allow caring and educational institutions (creches, schools) to provide appropriately balanced meals for vegetarians and vegans.
And lastly, there is a need of clear regulation of ultra processed meat and dairy alternatives as to their suitability for children and transparency as to their nutritional equivalence (or lack of it) to their animal -based counterparts.
5. Conclusions
Children are increasingly consuming plant-based diets, and the available evidence indicates that this can have implications for their growth and body composition, bone health, nutritional biochemistry and cardio-metabolic risk. The findings of cardiometabolic benefits have major implications for efforts to reduce non-communicable disease risk through the life-course, however children consuming plant-based diets, in particular vegan children, may also be at risk of nutritional deficiencies with long-term effects. Since peak bone mass is attained in early adulthood, low levels of bone density in childhood merit particular attention. A third of those children might be at risk of vitamin B12 deficiency which can result in developmental impairment. The heterogeneity of advice by different national and international organizations indicates that a process of harmonization is warranted, which requires expansion of the evidence base. We highlight a number of areas where further research should be prioritized. Additionally, we identify a number of practice recommendation that should be urgently introduced at national and international levels, to facilitate/improve safety of application of vegan and vegetarian diets in children.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, J.W., M.D. and M.F.; formal analysis, M.D.; writing—original draft preparation, M.D. and J.W.; writing—review and editing, M.D., J.W. and M.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Plant-Based Diets and Their Impact on Health, Sustainability and the Environment A Review of the Evidence WHO European Office for the Prevention and Control of Noncommunicable Diseases; 2021.
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on Healthy Diets from Sustainable Food Systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, P.; Clark, M.; Cobiac, L.; Papier, K.; Knuppel, A.; Lynch, J.; Harrington, R.; Key, T.; Springmann, M. Vegans, Vegetarians, Fish-Eaters and Meat-Eaters in the UK Show Discrepant Environmental Impacts. Nat. Food 2023 47 2023, 4, 565–574. [Google Scholar] [CrossRef] [PubMed]
- FAO The Global Dairy Sector: Facts.; 2013.
- Gerber, P.J.; Steinfeld, H.; Henderson, B.; Mottet, A.; Opio, C.; Dijkman, J.; Falcucci, A.; Tempio, G. Tackling Climate Change through Livestock – A Global Assessment of Emissions and Mitigation Opportunities; 2013.
- Kesse-Guyot, E.; Chaltiel, D.; Wang, J.; Pointereau, P.; Langevin, B.; Allès, B.; Rebouillat, P.; Lairon, D.; Vidal, R.; Mariotti, F.; et al. Sustainability Analysis of French Dietary Guidelines Using Multiple Criteria. Nat. Sustain. 2020 35 2020, 3, 377–385. [Google Scholar] [CrossRef]
- Dietitians Australia National Nutrition Strategy Joint Position Statement. Available online: https://dietitiansaustralia.org.au/advocacy-and-policy/joint-position-statements/national-nutrition-strategy-joint-position-statement (accessed on 24 September 2023).
- European Comission Food-Based Dietary Guidelines in Europe - Table 10 | Knowledge for Policy. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/food-based-dietary-guidelines-europe-table-19_en (accessed on 24 September 2023).
- Business Insider Poland Światowy Dzień Wegetarianizmu - Wegetarianizm w Polsce. Available online: https://businessinsider.com.pl/rozwoj-osobisty/zdrowie/swiatowy-dzien-wegetarianizmu-wegetarianizm-w-polsce/r27z9fq (accessed on 24 September 2023).
- Lantern Papers The Green Revolution, Entendiendo El Auge Del Movimiento Veggie; 2020.
- Cornell University Veganism and Plant-Based Diets On the Rise . Available online: https://blogs.cornell.edu/info2040/2019/11/21/veganism-and-plant-based-diets-on-the-rise/ (accessed on 24 September 2023).
- Vegconomist.com 2023.
- Mascaraque, M. Going Plant-Based: The Rise of Vegan and Vegetarian Food; 2020.
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Schürmann, S.; Kersting, M.; Alexy, U. Vegetarian Diets in Children: A Systematic Review. Eur. J. Nutr. 2017, 56, 1797–1817. [Google Scholar] [CrossRef]
- Desmond, M.A.; Sobiecki, J.G.; Jaworski, M.; Płudowski, P.; Antoniewicz, J.; Shirley, M.K.; Eaton, S.; Ksiązyk, J.; Cortina-Borja, M.; De Stavola, B.; et al. Growth, Body Composition, and Cardiovascular and Nutritional Risk of 5- to 10-y-Old Children Consuming Vegetarian, Vegan, or Omnivore Diets. Am. J. Clin. Nutr. 2021, 113, 1565–1577. [Google Scholar] [CrossRef]
- Weder, S.; Hoffmann, M.; Becker, K.; Alexy, U.; Keller, M. Energy, Macronutrient Intake, and Anthropometrics of Vegetarian, Vegan, and Omnivorous Children (1–3 Years) in Germany (VeChi Diet Study). Nutrients 2019, 11, 832. [Google Scholar] [CrossRef]
- GFI (Good Food Instititute) 2021 U.S. Retail Market Insights. Plant Based Foods.; 2021.
- Morency, M.E.; Birken, C.S.; Lebovic, G.; Chen, Y.; L’Abbé, M.; Lee, G.J.; Maguire, J.L. Association between Noncow Milk Beverage Consumption and Childhood Height. Am. J. Clin. Nutr. 2017, 106, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Crimarco, A.; Landry, M.J.; Carter, M.M.; Gardner, C.D. Assessing the Effects of Alternative Plant-Based Meats v. Animal Meats on Biomarkers of Inflammation: A Secondary Analysis of the SWAP-MEAT Randomized Crossover Trial. J. Nutr. Sci. 2022, 11, 1–5. [Google Scholar] [CrossRef]
- Abiega-Franyutti, P.; Freyre-Fonseca, V. Chronic Consumption of Food-Additives Lead to Changes via Microbiota Gut-Brain Axis. Toxicology 2021, 464, 153001. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.S.; Tresserra-Rimbau, A.; Karavasiloglou, N.; Jennings, A.; Cantwell, M.; Hill, C.; Perez-Cornago, A.; Bondonno, N.P.; Murphy, N.; Rohrmann, S.; et al. Association of Healthful Plant-Based Diet Adherence With Risk of Mortality and Major Chronic Diseases Among Adults in the UK. JAMA Netw. Open 2023, 6, e234714–e234714. [Google Scholar] [CrossRef] [PubMed]
- BDA British Dietetic Association Confirms Well-Planned Vegan Diets Can Support Healthy Living in People of All Ages. Available online: https://www.bda.uk.com/news/view?id=179 (accessed on 2 July 2019).
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- de Medécine de Belgique, A.R. Le {Veganisme} Proscrit Pour Les Enfants, Femmes Enceintes et Allaitantest 2019.
- Die Deutsche Gesellschaft für Ernährung Vegane Ernährung: Nährstoffversorgung Und Gesundheitsrisiken Im Säuglings- Und Kindesalter.
- Wądołowska, L. et al. Stanowisko Komitetu Nauki o Żywieniu Człowieka PAN w Sprawie Wartości Odżywczej i Bezpieczeństwa Stosowania Diet Wegetariańskich E; Olsztyn, 2019.
- Baldassarre, M.E.; Panza, R.; Farella, I.; Posa, D.; Capozza, M.; Di Mauro, A.; Laforgia, N. Vegetarian and Vegan Weaning of the Infant: How Common and How Evidence-Based? A Population-Based Survey and Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Startseite AWA - AWA – Allensbacher Markt- Und Werbeträgeranalyse. Available online: https://www.ifd-allensbach.de/awa/startseite.html (accessed on 23 September 2023).
- Department of Health and the Food Standars Agency National Diet and Nutrition Survey Headline Results from Years 1 and 2 (Combined) of the Rolling Programme (2008/2009 – 2009/10); 2010.
- Stewart, C.; Piernas, C.; Cook, B.; Jebb, S.A. Trends in UK Meat Consumption: Analysis of Data from Years 1–11 (2008–09 to 2018–19) of the National Diet and Nutrition Survey Rolling Programme. Lancet Planet. Heal. 2021, 5, e699–e708. [Google Scholar] [CrossRef] [PubMed]
- Mintel Vegan Food Launches in Australia Grew by 92% between 2014 and 2016. Available online: https://www.mintel.com/press-centre/vegan-food-launches-in-australia-grew-by-92-between-2014-and-2016/ (accessed on 24 September 2023).
- GFI (Good Food Instititute) UK Plant- Based Foods Retail Market Insights 2020-2022; 2022.
- BBC Good Food Nation: Survey Looks at Children’s Eating Habits - BBC Newsround. Available online: https://www.bbc.co.uk/newsround/58653757 (accessed on 23 September 2023).
- Chiorando, M. 70% of British Children Want More Vegan and Veggie School Meals, Says Poll. Plant Based News 2020.
- Nathan, I.; Hackett, A.F.; Kirby, S. A Longitudinal Study of the Growth of Matched Pairs of Vegetarian and Omnivorous Children, Aged 7-11 Years, in the North-West of England. Eur. J. Clin. Nutr. 1997, 51, 20–25. [Google Scholar] [CrossRef]
- Krajcovicová-Kudlácková, M.; Simoncic, R.; Béderová, A.; Grancicová, E.; Magálová, T. Influence of Vegetarian and Mixed Nutrition on Selected Haematological and Biochemical Parameters in Children. Nahrung 1997, 41, 311–314. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Klemarczyk, W.; Gajewska, J.; Chełchowska, M.; Rowicka, G.; Ołtarzewski, M.; Laskowska-Klita, T. Serum Concentration of Adipocytokines in Prepubertal Vegetarian and Omnivorous Children. Med. Wieku Rozwoj. 2011, 15, 326–334. [Google Scholar]
- Hebbelinck, M.; Clarys, P.; De Malsche, A. Growth, Development, and Physical Fitness of Flemish Vegetarian Children, Adolescents, and Young Adults. Am. J. Clin. Nutr. 1999, 70, 579s–585s. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Laskowska-Klita, T.; Klemarczyk, W. Low Levels of Osteocalcin and Leptin in Serum of Vegetarian Prepubertal Children. Med. Wieku Rozwoj. 2003, 7, 587–591. [Google Scholar] [PubMed]
- Ambroszkiewicz, J.; Klemarczyk, W.; Chełchowska, M.; Gajewska, J.; Laskowska-Klita, T. Serum Homocysteine, Folate, Vitamin B12 and Total Antioxidant Status in Vegetarian Children. Adv. Med. Sci. 2006, 51, 265–268. [Google Scholar]
- Ambroszkiewicz, J.; Klemarczyk, W.; Gajewska, J.; Chełchowska, M.; Laskowska-Klita, T. Serum Concentration of Biochemical Bone Turnover Markers in Vegetarian Children. Adv. Med. Sci. 2007, 52, 279–282. [Google Scholar] [PubMed]
- Gorczyca, D.; Paściak, M.; Szponar, B.; Gamian, A.; Jankowski, A. An Impact of the Diet on Serum Fatty Acid and Lipid Profiles in Polish Vegetarian Children and Children with Allergy. Eur. J. Clin. Nutr. 2011, 65, 191–195. [Google Scholar] [CrossRef]
- Gorczyca, D.; Prescha, A.; Szeremeta, K.; Jankowski, A. Iron Status and Dietary Iron Intake of Vegetarian Children from Poland. Ann. Nutr. Metab. 2013, 62, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.A. Growth and Development of British Vegan Children. Am. J. Clin. Nutr. 1988, 48, 822–825. [Google Scholar] [CrossRef] [PubMed]
- Nathan, I.; Hackett, A.; Kirby, S. The Dietary Intake of a Group of Vegetarian Children Aged 7-11 Years Compared with Matched Omnivores. Br. J. Nutr. 1996, 75, 533–544. [Google Scholar] [CrossRef]
- Taylor, A.; Redworth, E.W.; Morgan, J.B. Influence of Diet on Iron, Copper, and Zinc Status in Children Under 24 Months of Age. Biol. Trace Elem. Res. 2004, 97, 197–214. [Google Scholar] [CrossRef]
- Harris, R.D.; Phillips, R.L.; Williams, P.M.; Kuzma, J.W.; Fraser, G.E. The Child-Adolescent Blood Pressure Study: I. Distribution of Blood Pressure Levels in Seventh-Day-Adventist (SDA) and Non-SDA Children. Am. J. Public Health 1981, 71, 1342–1349. [Google Scholar] [CrossRef]
- Kissinger, D.G.; Sanchez, A. The Association of Dietary Factors with the Age of Menarche. Nutr. Res. 1987, 7, 471–479. [Google Scholar] [CrossRef]
- O’Connell, J.M.; Dibley, M.J.; Sierra, J.; Wallace, B.; Marks, J.S.; Yip, R. Growth of Vegetarian Children: The Farm Study. Pediatrics 1989, 84, 475–481. [Google Scholar] [CrossRef]
- Lombard, K.A.; Olson, A.L.; Nelson, S.E.; Rebouche, C.J. Carnitine Status of Lactoovovegetarians and Strict Vegetarian Adults and Children. Am. J. Clin. Nutr. 1989, 50, 301–306. [Google Scholar] [CrossRef]
- Sabaté, J.; Lindsted, K.D.; Harris, R.D.; Sanchez, A. Attained Height of Lacto-Ovo Vegetarian Children and Adolescents. Eur. J. Clin. Nutr. 1991, 45, 51–58. [Google Scholar]
- Sabaté, J.; Llorca, M.C.; Sánchez, A. Lower Height of Lacto-Ovovegetarian Girls at Preadolescence: An Indicator of Physical Maturation Delay? J. Am. Diet. Assoc. 1992, 92, 1263–1264. [Google Scholar] [CrossRef]
- Persky, V.W.; Chatterton, R.T.; Van Horn, L.V.; Grant, M.D.; Langenberg, P.; Marvin, J. Hormone Levels in Vegetarian and Nonvegetarian Teenage Girls: Potential Implications for Breast Cancer Risk. Cancer Res. 1992, 52, 578–583. [Google Scholar]
- Matthews, V.; Wien, M.; Sabaté, J. The Risk of Child and Adolescent Overweight Is Related to Types of Food Consumed. Nutr. J. 2011, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Sievers, E.; Dörner, K.; Hamm, E.; Hanisch, C.; Schaub, J. Vergleichende Untersuchungen Zur Eisenversorgung Lakto-Ovo-Vegetabil Ernährter Säuglinge. Ärztezeitschr Naturheilverf 1991, 32, 106–112. [Google Scholar]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Weder, S.; Hoffmann, M.; Becker, K.; Alexy, U.; Keller, M. Energy, Macronutrient Intake, and Anthropometrics of Vegetarian, Vegan, and Omnivorous Children (1–3 Years) in Germany (VeChi Diet Study). Nutrients 2019, 11, 832. [Google Scholar] [CrossRef]
- Hovinen, T.; Korkalo, L.; Freese, R.; Skaffari, E.; Isohanni, P.; Niemi, M.; Nevalainen, J.; Gylling, H.; Zamboni, N.; Erkkola, M.; et al. Vegan Diet in Young Children Remodels Metabolism and Challenges the Statuses of Essential Nutrients. EMBO Mol. Med. 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Sandullo, F.; Vecchio, M.; Di Ruscio, F.; Franceschini, G.; Peronti, B.; Blasi, V.; Nonni, G.; Bietolini, S. Length-Weight Growth Analysis up to 12 Months of Age in Three Groups According to the Dietary Pattern Followed from Pregnant Mothers and Children during the First Year of Life. Minerva Pediatr. 2021. [Google Scholar] [CrossRef]
- Alexy, U.; Fischer, M.; Weder, S.; Längler, A.; Michalsen, A.; Sputtek, A.; Keller, M. Nutrient Intake and Status of German Children and Adolescents Consuming Vegetarian, Vegan or Omnivore Diets: Results of the Vechi Youth Study. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Světnička, M.; Heniková, M.; Selinger, E.; Ouřadová, A.; Potočková, J.; Kuhn, T.; Gojda, J.; El-Lababidi, E. Prevalence of Iodine Deficiency among Vegan Compared to Vegetarian and Omnivore Children in the Czech Republic: Cross-Sectional Study. Eur. J. Clin. Nutr. 2023. [Google Scholar] [CrossRef] [PubMed]
- Světnička, M.; Sigal, A.; Selinger, E.; Heniková, M.; El-lababidi, E.; Gojda, J. Cross-Sectional Study of the Prevalence of Cobalamin Deficiency and Vitamin B12 Supplementation Habits among Vegetarian and Vegan Children in the Czech Republic. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Elliott, L.J.; Keown-Stoneman, C.D.G.; Birken, C.S.; Jenkins, D.J.A.; Borkhoff, C.M.; Maguire, J.L. Vegetarian Diet, Growth, and Nutrition in Early Childhood: A Longitudinal Cohort Study. Pediatrics 2022, 149, 2021052598. [Google Scholar] [CrossRef] [PubMed]
- Alexy, U.; Fischer, M.; Weder, S.; Längler, A.; Michalsen, A.; Sputtek, A.; Keller, M. Nutrient Intake and Status of German Children and Adolescents Consuming Vegetarian, Vegan or Omnivore Diets: Results of the VeChi Youth Study. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Sabaté, J.; Lindsted, K.; Harris, R.; Johnston, P. Anthropometric Parameters of Schoolchildren With Different Life-Styles. Arch. Pediatr. Adolesc. Med. 1990, 144, 1159. [Google Scholar] [CrossRef]
- Rowicka, G.; Klemarczyk, W.; Ambroszkiewicz, J.; Strucińska, M.; Kawiak-Jawor, E.; Weker, H.; Chełchowska, M. Assessment of Oxidant and Antioxidant Status in Prepubertal Children Following Vegetarian and Omnivorous Diets. Antioxidants 2023, 12. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Klemarczyk, W.; Mazur, J.; Gajewska, J.; Rowicka, G.; Strucińska, M.; Chełchowska, M. Serum Hepcidin and Soluble Transferrin Receptor in the Assessment of Iron Metabolism in Children on a Vegetarian Diet. Biol. Trace Elem. Res. 2017, 180, 182–190. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Szamotulska, K.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. The Assessment of Bone Regulatory Pathways, Bone Turnover, and Bone Mineral Density in Vegetarian and Omnivorous Children. Nutrients 2018, 10, 183. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. Anti-Inflammatory and Pro-Inflammatory Adipokine Profiles in Children on Vegetarian and Omnivorous Diets. Nutrients 2018, 10, 1241. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Szamotulska, K.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. Bone Status and Adipokine Levels in Children on Vegetarian and Omnivorous Diets. Clin. Nutr. 2019, 38, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Kroke, A.; Manz, F.; Kersting, M.; Remer, T.; Sichert-Hellert, W.; Alexy, U.; Lentze, M.J. The DONALD Study. History, Current Status and Future Perspectives. Eur. J. Nutr. 2004, 43, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Ambroszkiewicz, J.; Gajewska, J.; Mazur, J.; Kuśmierska, K.; Klemarczyk, W.; Rowicka, G.; Strucińska, M.; Chełchowska, M. Dietary Intake and Circulating Amino Acid Concentrations in Relation with Bone Metabolism Markers in Children Following Vegetarian and Omnivorous Diets. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Ambroszkiewicz, J.; Chełchowska, M.; Szamotulska, K.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. The Assessment of Bone Regulatory Pathways, Bone Turnover, and Bone Mineral Density in Vegetarian and Omnivorous Children. Nutrients 2018, 10, 183. [Google Scholar] [CrossRef] [PubMed]
- Ambroszkiewicz, J.; Chełchowska, M.; Szamotulska, K.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. The Assessment of Bone Regulatory Pathways, Bone Turnover, and Bone Mineral Density in Vegetarian and Omnivorous Children. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Weder, S.; Keller, M.; Fischer, M.; Becker, K.; Alexy, U. Intake of Micronutrients and Fatty Acids of Vegetarian, Vegan, and Omnivorous Children (1-3 Years) in Germany (VeChi Diet Study). Eur. J. Nutr. 2022, 61, 1507–1520. [Google Scholar] [CrossRef] [PubMed]
- Higginbottom, M.C.; Sweetman, L.; Nyhan, W.L. A Syndrome of Methylmalonic Aciduria, Homocystinuria, Megaloblastic Anemia and Neurologic Abnormalities in a Vitamin B 12 -Deficient Breast-Fed Infant of a Strict Vegetarian. N. Engl. J. Med. 1978, 299, 317–323. [Google Scholar] [CrossRef]
- Smolka, V.; Bekárek, E.; Hlídková, J.; Bucil, D.; Mayerová, Z.; Skopková, T.; Adam, E.; Hrubá, V.; Kozich, L.; Buriánková, J.; Saligová, M.; Buncová, J.Z. Metabolic Complications and Neurologic Manifestations of Vitamin B12 Deficiency in Children of Vegetarian Mothers. Cas Lek Ces. 2001, 140, 732–735. [Google Scholar]
- Mariani, A.; Chalies, S.; Jeziorski, E.; Ludwig, C.; Lalande, M.; Rodière, M. [Consequences of Exclusive Breast-Feeding in Vegan Mother Newborn--Case Report]. Arch. Pediatr. 2009, 16, 1461–1463. [Google Scholar] [CrossRef]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, Vegan Diets and Multiple Health Outcomes: A Systematic Review with Meta-Analysis of Observational Studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. Anti-Inflammatory and Pro-Inflammatory Adipokine Profiles in Children on Vegetarian and Omnivorous Diets. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Jakše, B.; Fras, Z.; Fidler Mis, N. Vegan Diets for Children: A Narrative Review of Position Papers Published by Relevant Associations. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Havala, S.; Dwyer, J. Position of the American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 1993, 93, 1317–1319. [Google Scholar] [CrossRef] [PubMed]
- WJ, C.; AR, M. Position of the American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 2009, 109, 1266–1282. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef]
- Agnoli, C.; Baroni, L.; Bertini, I.; Ciappellano, S.; Fabbri, A.; Papa, M.; Pellegrini, N.; Sbarbati, R.; Scarino, M.L.; Siani, V.; et al. Position Paper on Vegetarian Diets from the Working Group of the Italian Society of Human Nutrition. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1037–1052. [Google Scholar] [CrossRef] [PubMed]
- Health Canada, Canadian Paediatric Society, Dietitians of Canada, and B.C. for C. Nutrition for Healthy Term Infants: Recommendations from Six to 24 Months. Can. J. Diet. Pract. Res. 2014, 75, 107–107. [CrossRef]
- Amit, M.; Society, C.P.; Committee, C.P. Vegetarian Diets in Children and Adolescents. Paediatr. Child Health 2010, 15, 303–314. [Google Scholar] [CrossRef]
- Alberti, M.J.; Desantadina, M.V. [Vegetarian Diets in Childhood]. Arch. Argent. Pediatr. 2020, 118, S130–S141. [Google Scholar] [CrossRef]
- Redecilla Ferreiro, S.; Moráis López, A.; Moreno Villares, J.M.; Leis Trabazo, R.; José Díaz, J.; Sáenz de Pipaón, M.; Blesa, L.; Campoy, C.; Ángel Sanjosé, M.; Gil Campos, M.; et al. [Position Paper on Vegetarian Diets in Infants and Children. Committee on Nutrition and Breastfeeding of the Spanish Paediatric Association]. An. Pediatr. 2020, 92, 306.e1-306.e6. [CrossRef]
- Richter, M.; Boeing, H.; Grünewald-Funk, D.H.H.; Kroke, A.; Leschik-Bonnet, A.; Oberritter, H.; Strohm, D.W.B.; (DGE), für die D.G. für E. e. V. Vegane Ernährung,Position Der Deutschen Gesellschaft Für Ernährung e. V. (DGE). Ernaehrungs Umschau Int. 2016, M220–M230. [Google Scholar]
- Richter, M., Kroke, A., Grünewald-Funk, D., Heseker, H., Virmani, K., W.B. fü. die D.G. für E. e. V. (DGE) Ergänzung Der Position Der Deutschen Gesellschaft Für Ernährung e. V. Zur Veganen Ernährung Hinsichtlich Bevölkerungsgruppen Mit Besonderem Anspruch an Die Nährstoffversorgung. Ernaehrungs Umschau Int. 2020.
- Lemale, J.; Mas, E.; Jung, C.; Bellaiche, M.; Tounian, P. Vegan Diet in Children and Adolescents. Recommendations from the French-Speaking Pediatric Hepatology, Gastroenterology and Nutrition Group (GFHGNP). Arch. Pediatr. 2019, 26, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Belgique, A.R. de M. de Le Veganisme Proscrit Pour Les Enfants, Femmes enceintes et Allaitantest 2019.
- Szajewska, H., Socha, P. and H.A. Principles of Feeding Healthy Infants. Statement of the Polish Society of Gastroenterology, Hepatology and Nutrition for Children (in Polish). Stand Med/Pediatria 2021, 805–822.
- Hay, G.; Fadnes, L.; Meltzer, H.M.; Arnesen, E.K.; Henriksen, C. Follow-up of Pregnant Women, Breastfeeding Mothers and Infants on a Vegetarian or Vegan Diet. Tidsskr. den Nor. laegeforening Tidsskr. Prakt. Med. ny raekke 2022, 142. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Kiely, M.E. Risks and Benefits of Vegan and Vegetarian Diets in Children. Proc. Nutr. Soc. 2021, 80, 159–164. [Google Scholar] [CrossRef]
- Pawlak, R.; Bell, K. Iron {Status} of {Vegetarian} {Children}: {A} {Review} of {Literature}. Ann. Nutr. Metab. 2017, 70, 88–99. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram for the systematic review of studies assessing health outcomes of vegetarian and vegan children from 2013.
Figure 1.
PRISMA 2020 flow diagram for the systematic review of studies assessing health outcomes of vegetarian and vegan children from 2013.
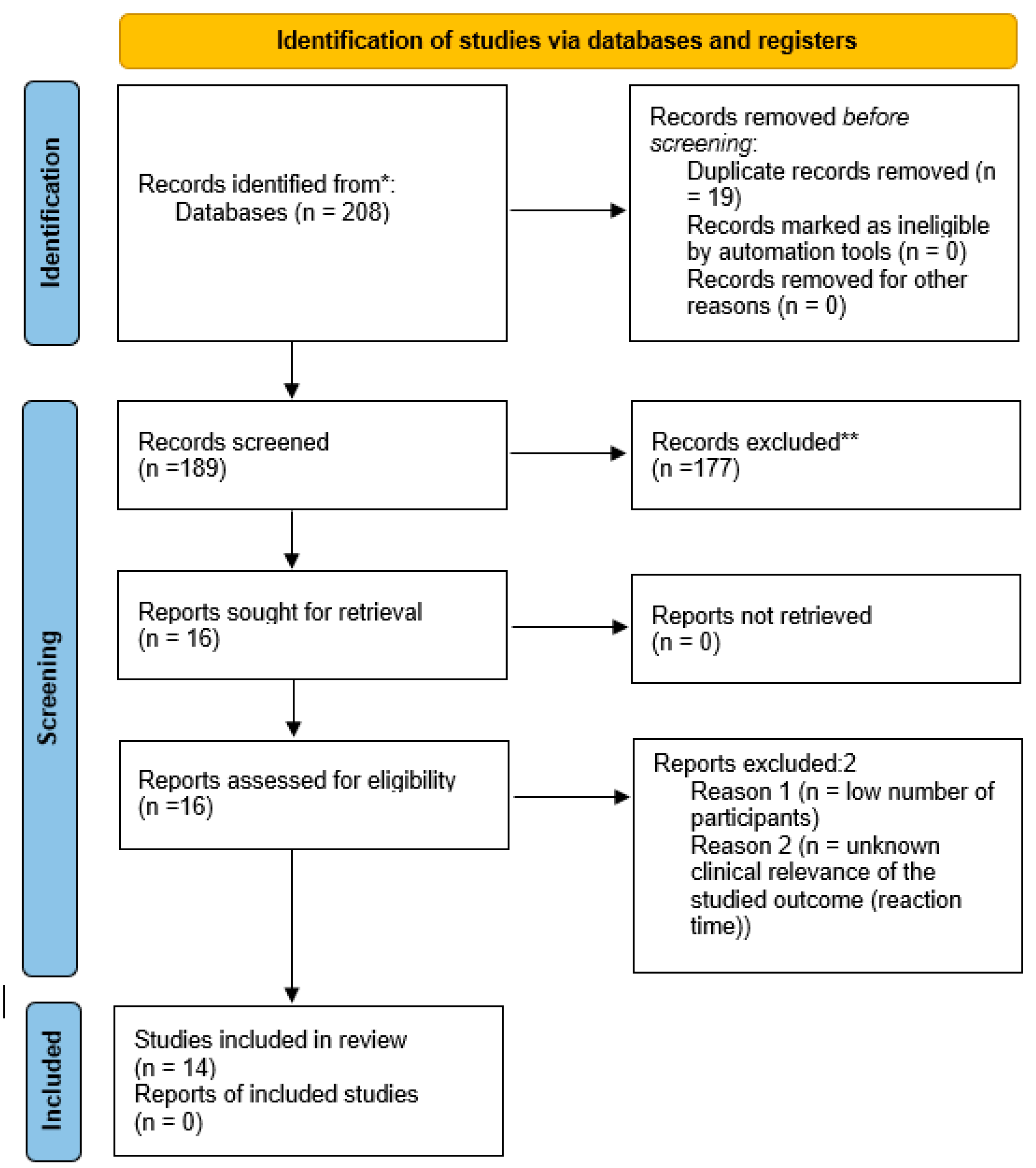
Figure 2.
Vitamin B12 supplementation rates (%) among vegetarian and vegan children by country.
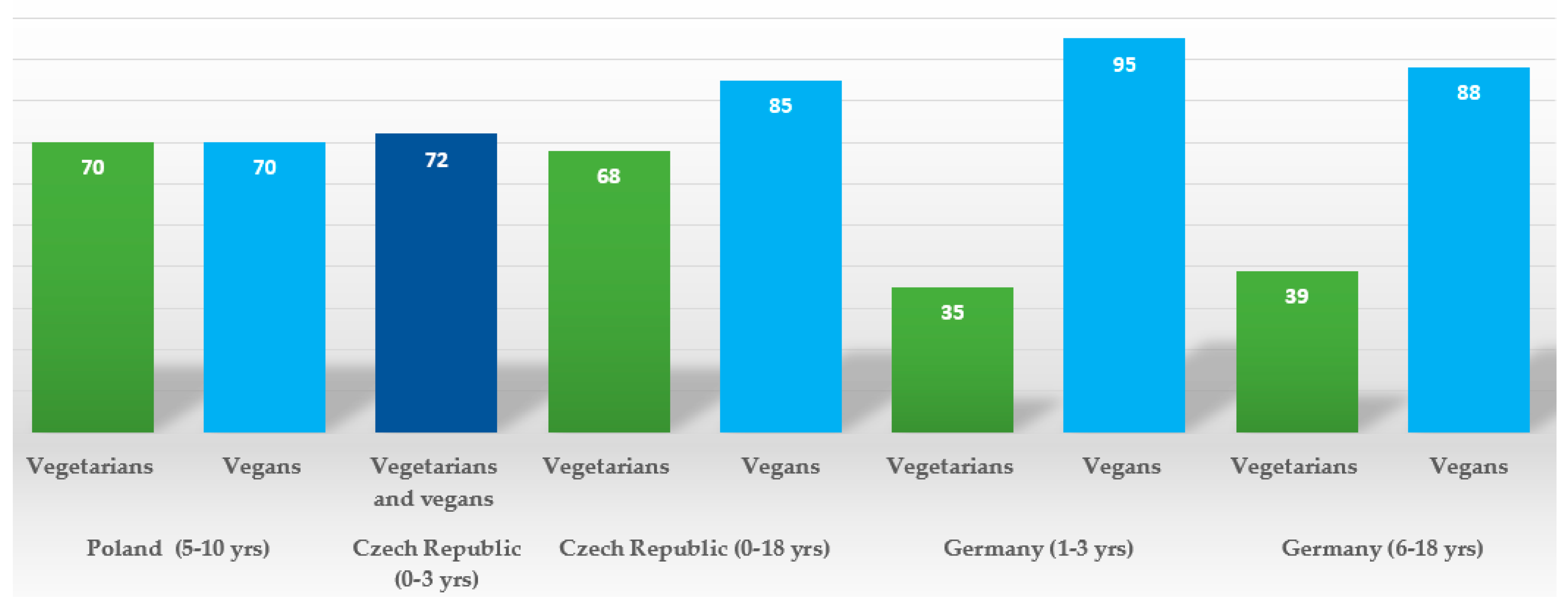
Figure 3.
Summary of impacts of vegetarian and vegan diets on a range of children’s health outcomes, based on the evidence listed in Table 1.
Figure 3.
Summary of impacts of vegetarian and vegan diets on a range of children’s health outcomes, based on the evidence listed in Table 1.
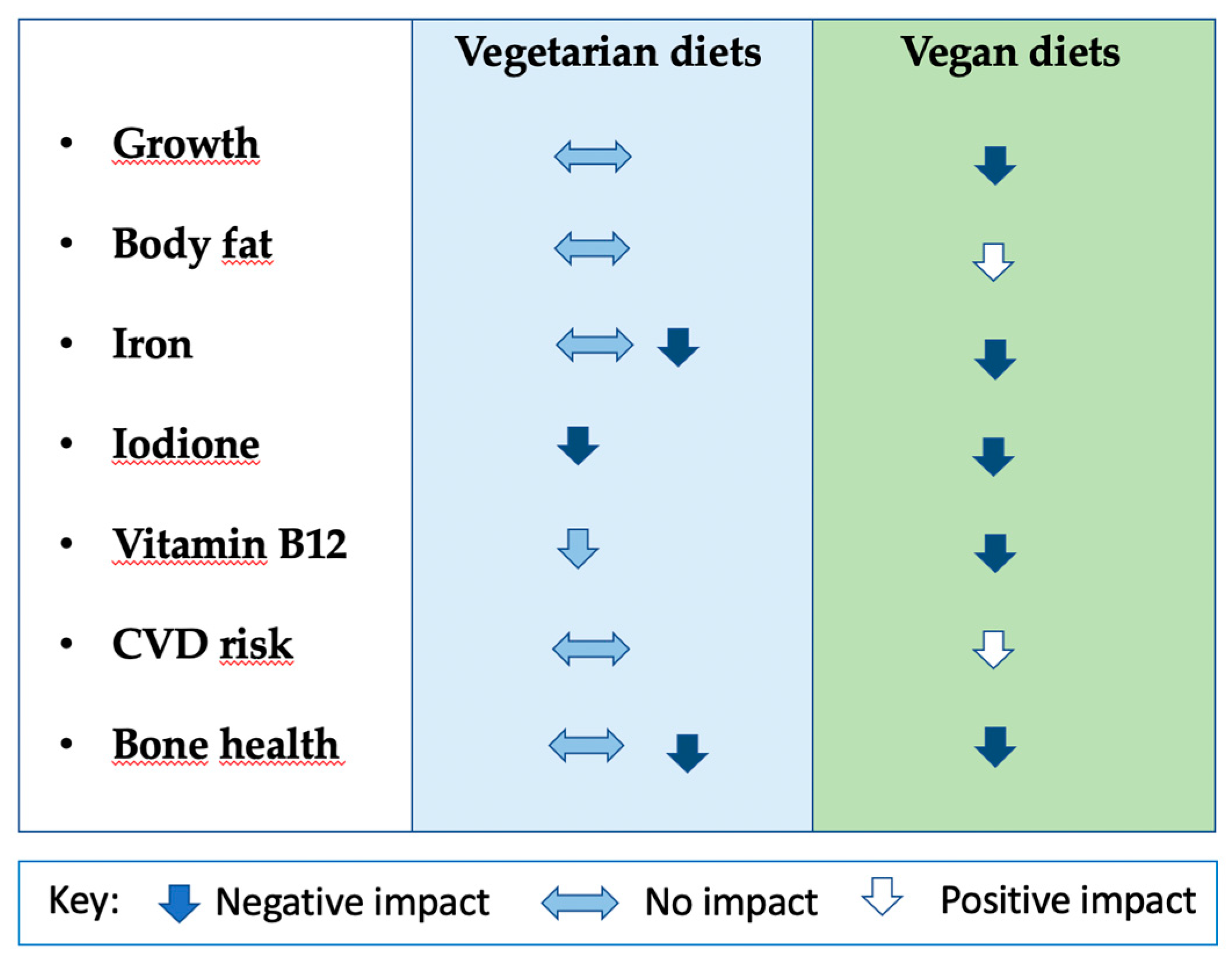

Table 1.
Summary of the health of vegetarian and vegan children data published between 2013 and 2023.
Table 1.
Summary of the health of vegetarian and vegan children data published between 2013 and 2023.
| Authors, year, place | Study characteristics | Participants | Dietary data collection | Health outcomes measured | Results |
|---|---|---|---|---|---|
| Ambroszkiewicz et al. 2017. The Institute of Mother and Child (IMC) in Warsaw, Poland [68]. | Cross-sectional; data collection 2015-2016; from a group of patients seeking dietary counselling at the IMC. | 43 vegetarian (VG) prepubertal children (age range 4.5–9.0 years), 46 omnivore (OM) children. No data on socio-economic status (SES) or physical activity (PA). | 3-day food diary, data on average daily energy, protein, fat, carbohydrates, dietary iron and vitamin intakes collected. | Serum haemoglobin (Hb), red blood cells, and mean corpuscular volume, iron, ferritin, and transferrin, C-reactive protein (CRP), hepcidin (bioactive heptidin-25 molecule) and soluble transferrin receptor concentration (sTfR); weight (WT), height (HT) | Lower ferritin and median hepcidin concentrations in VG; sTfR concentrations significantly higher in VG compared to OM. No difference in serum transferrin between groups; other hematologic parameters and serum iron were within the reference range in both groups. No differences in WT, HT, BMI between VG and OM. |
| Ambroszkiewicz et al 2018. The IMC, Warsaw, Poland [69]. | Cross-sectional; data collection 2014-2017; from a group of patients seeking dietary counselling at the IMC. | 70 children (age range 5–10 years) on a VG diet from birth, 60 OM children. No data on SES. PA study inclusion criteria – more than 2h of activity per week. No information on how this data was collected. | 3-day food diary, data on average daily energy, protein, fat, carbohydrates, and dietary minerals and vitamin intakes collected. | Bone mineral content (BMC), and bone mineral density (BMD) in the total body (tBMD) and at the lumbar spine (BMD L1–L4), lean and fat mass by dual-energy X-ray absorptiometry (DXA); height, weight; bone alkaline phosphatase (BALP), C-terminal telopeptide of type I collagen (CTX-I), osteoprotegerin, nuclear factor κB ligand, sclerostin, and Dickkopf-related protein 1; 25-hydroxyvitamin D (25-OH D) and parathormone (PTH); HT and WT. | No significant differences in body composition, HT, BMI z-scores or BMC and BMD, 25-OH D between VG and OM children, however a trend for spine BMC and BMD of VG to be lower; VG significantly higher level of BALP and CTX-I (interpreted as a higher rate of bone turnover markers) and higher median levels of PTH) than OM. |
| Ambroszkiewicz et al. 2018. The IMC, Warsaw, Poland [70]. | Cross-sectional; data collection 2017-2018; from a group of patients seeking dietary counselling at the IMC. | 62 children (age range 5–10 years) on a VG diet from birth, 55 OM children. No data on SES. PA assessed by questionnaire. | 3-day food diary, data on average daily energy, protein, fat, carbohydrates, and dietary fibre intake collected. | Serum concentrations of adipokines: leptin, soluble leptin receptor (sOB-R), adiponectin, resistin, visfatin, vaspin, and omentin; fat mass, lean mass, and fat free mass by DXA; fat mass index and lean mass index were calculated; HT and WT. | No difference in WT, HT, BMI, and body composition between groups. VG had lower leptin/sOB-R ratio and lower serum concentrations of resistin, compared with OM; average levels of other adipokines did not differ between both groups; VG had significantly higher ratios of anti-inflammatory to pro-inflammatory adipokines: adiponectin/leptin and omentin/leptin compared with OM. |
| Ambroszkiewicz et al. 2019. The IMC, Warsaw, Poland [71]. | Cross-sectional; data collection 2014-2016; from a group of patients seeking dietary counselling at the IMC. | 53 children (age range 5–10 years) on a VG diet, 53 OM children. No data on SES. PA assessed by questionnaire. | 3-day food diary, data on average daily energy, protein, fat, carbohydrates, and dietary minerals and vitamin intakes collected. Complete dietary data was available for 25 pairs of VG & OM. | WT, HT; body composition and BMD by DXA. 25-OH D and PTH, serum carboxy-terminal propeptide of type I collagen (CICP), total osteocalcin and its forms carboxylated and undercarboxylated, CTX-I, leptin and adiponectin levels. | No difference in HT, WT, BMI z-scores or body composition between VG and OM, except for percentage fat mass, lower in VG. Mean total BMD z-score and lumbar spine BMD z-score were lower in VG compared with OM; however absolute values of bone mineral density did not differ; serum leptin level was 2-fold lower in VGs, reflecting lower body fat; VG had higher PTH and CTX; similar levels of adiponectin, osteocalcin, CICP, and 25 (OH) D; BMD z-scores did not correlate with bone metabolism markers and nutritional variables, but were positively associated with anthropometric parameters. |
| Weder et al. 2019. The VeChi DietStudy, Germany [58]. | Cross-sectional; data collection 2016-2018, collecting data from VG, VN, and OM children throughout Germany. OM children partially recruited from the DONALD [72] study (as insufficient OM participants were recruited via the VeChi Study). | 430 children: 127 VG,139 vegan (VN), 164 OM, aged 1-3 years. SES and urbanicity data collected. PA assessed by questionnaire. | 3-day weighed dietary records; breast milk intakes were estimated with the methodology from the DONALD study [72]. Energy, macronutrients, and fibre intakes were calculated. | Data from parents or a paediatrician proxy-assessed WT and HT during the last medical check-up. | Anthropometrics did not significantly differ between diet groups and indicated on average normal growth in all groups. However, more VN (3.6%) and VG (2.4%) than OM children (0%) were classified as stunted or wasted. |
| Hovinen et al. 2021. Municipal day-care centres, Helsinki, Finland [59]. | Cross-sectional; data collection 2017, from 20 municipal day-care centres offering vegan meals in Helsinki. | 6 VN (vegan from birth); 10 VG, 24 OM; median age 3.5 years (1-7 years). Vegetarian children defined as those on a lactovegetarian diet or on a pescetarian diet (eating fish). No data on PA or SES. | The children were consuming nutritionist-planned diets in day-care centres, designed to meet nutritional recommendations. | WT, HT, mid-upper arm circumference (MUAC); numerous biomarkers. Serum amino acids, vitamin A, 25 (OH)D, DHA, and other micronutrients; total cholesterol, HDL -C and LDL -C, endogenous hepatic cholesterol biosynthesis markers, bile acid biosynthesis markers. | HT and BMIs of all children compared to the current Finnish growth references; there was no difference between diet groups in z-scores of HT, BMI, or MUAC. All fractions of blood lipid levels were significantly lower in VN than OM. Biomarkers for amino acids, fat-soluble vitamins A, D and DHA were markedly lower in VN. Bile acid biosynthesis pathway differed most significantly between VN and OM, VN had a bile acid pathway similar to a profile of fasted children. |
| Ferrara et al. 2021. Italy [60]. | Longitudinal study of infants born to mothers on VN, VG and OMN study, follow up in the first year of life; data collection 2017-2018. Participants recruited via the Campus Bio-Medico University Hospital, Romand vegetarian societies. | 63 participants: 21 infants from vegan pregnancies; 21 infants from vegetarian pregnancies; 21 infants from omnivorous pregnancies. | Food frequency questionnaire to classify mothers to appropriate dietary pattern. | Weight at birth, 6 months and 12 months (in grams and in growth percentiles); birth length in cm, body length expressed in growth percentiles at 12 months; BMI at 6 months. |
Vegan infants had lower birthweight, weight at 6 months and 12 months, both when expressed in grams and when expressed in growth percentiles than OMN infants. VN infants had lower body length expressed in growth percentiles at 12 months and lower BMI at 6 months than OMN. N significant differences between OMN and VG. |
| Alexy et al. 2021. The VeChi Youth Study, Germany [65]. | Cross-sectional; data collection 2016-2018, collecting data from VG, VN, and OM children throughout Germany. | 401 children: 149 VG; 115 VN; 137 OM; 6-18 years old, mean age: 12.7 ± 3.9 years; average time on a diet ca. 5.0 (± 3.9) years for vegetarians, and 4.2 (± 3,4) years for vegans. SES and urbanicity data collected. PA assessed by questionnaire. | 3-day weighed dietary records; energy, macronutrients, and selected micronutrients were calculated along with supplement use. | HT, WT; blood parameters: Hb, vitamin B2, and folate; ferritin, 25 (OH)D, holotranscobalamin (holoTC), methylmalonic acid (MMA), triglycerides TG) and total, LDL and HDL cholesterol. | No difference in average HT, WT, BMI z scores, however tendency for the lower values in VN; no significant difference in median Hb, vitamin B2, 25 (OH)D, HDL-C and TG concentrations between diet groups. VN had higher folate concentrations than VG; VN and VG had lower ferritin concentration than OM; VG but not VN had lower concentrations of holoTC and higher concentrations of MMA than OM, reflecting high (88%) vit. B12 supplementation prevalence in VN, but not in VG (39%). VN had the lowest non-HDL-C and LDL-C concentrations in comparison to VG and OM. A high prevalence (>30%) of 25 (OH)D and vitamin B2 concentrations below reference values were found irrespective of the diet group, however that percentage tended to be higher in VN and/or VG than in OM. |
| Desmond et al. The Children’s Memorial Health Institute, Warsaw, Poland [16]. |
Cross-sectional, data collection 2014-2016; recruited advertisements in social media, and websites focused on veganism (VG and VG; and health food stores (OM). OM matched to either VN or VG on age, sex and 2 indices of socio-economic status. | 187 children: 63 VG, 52 VN, 72 OM; age 5-10 years. Average time on a diet ca. 5.3 years for vegetarians, and 5.9 years for vegans. SES and urbanicity data collected. PA data collected by accelerometery. | 4 -day food diary, animal product consumption screener; energy, macro- and most micronutrient intakes along with supplemental practices were ascertained. | Body composition (BC): HT, WT, mid-thigh, waist, and hip girths; and biceps, triceps, subscapular, and suprailiac skinfolds; additionally BC by deuterium dilution and DXA. Cardiovascular risk factors: serum total cholesterol (TC), HDL cholesterol (HDL-C), LDL cholesterol (LDL-C), VLDL cholesterol (VLDL- C), and triglycerides (TG), high-sensitivity C-reactive protein (hs-CRP), fasting glucose, IGF-1, IGFBP-3. Carotid intima-media thickness (cIMT) by ultrasonography. Micronutrient status by complete blood count, including mean corpuscular volume (MCV), serum ferritin, vitamin B12, homocysteine (hcys), 25 (OH)D; bone health was assessed by DXA (bone mineral content in total body and spine (L1-L4) adjusted by body size) and calculating bone apparent mineral density (BMAD). | VG had lower gluteofemoral adiposity but similar total fat and lean mass. VN had lower fat indices in all regions, lower fat mass index z-score, but similar lean mass. VG and VN had lower total and L1-L4 BMC, the difference remained only in VN after accounting for body size. VN were on average 3.15 cm shorter than OM. VG had lower TC, HDL-C, and serum B12 and 25(OH)D without supplementation; higher glucose, VLDL, and TG. Vegans were shorter and had lower TC, LDL-C and HDL-C, hs-CRP, iron status, and serum B12 and 25(OH)D without supplementation, but higher hcys and MCV. Vitamin B12 deficiency, iron-deficiency anaemia, low ferritin, and low HDL were more prevalent in vegans, who also had the lowest prevalence of high LDL. Supplementation resolved low B-12 and 25(OH)D concentrations in both groups. |
| Světnička et al. 2022. The Czech Vegan Children Study (CAROTS), Czech Republic [63]. | Cross-sectional, data collection 2019-2021; recruited via GPs and other specialists, advertisements in social media, and websites focused on veganism. | 200 children: 79 VG, 69 VN and 52 OM; age ranging from 0 to 18 years. No data on PA or SES collected. | 3-day weighed dietary records; energy and macro- and micronutrient intakes along with supplemental practices were ascertained; breast milk intakes were estimated from mothers’ registrations and general recommendations for breast milk intake. | WT, HT; blood concentration of holoTC, cyanocobalamin (B12), folate, hcys, MCV, and Hb. | No difference in BMI percentile, HT and WT percentile between groups; VN tended to have lower medians of BMI and weight percentile; significantly more VN were in the <=3 percentile BMI category than in the other two groups; no significant differences in levels of holoTC, folate, hcys, or MCV; 1 VG and 2 VN children identified as B12 deficient; however, 83% of vegan children and 70% vegetarians supplemented vit. B12. In a subgroup of n=12 VG and n=36 VN, age 0-3 years, breastfed at the moment of examination born to VN/VG mothers, concentrations of holoTC, B12, were lower and hcys higher in VN infants not supplementing vit. B12. 35 VG (44%), 28 VN (40%), and 9 OM children had vitamin B12 hypervitaminosis, related to a high prevalence of over-supplementation in the group. Significant difference in B12, holoTC, and hcys levels of supplemented vs. non-supplemented VG/VN children was detected. |
| Světnička et al. 2023. The Czech Republic [62]. | Cross -sectional, data collection 2019-2021; recruited via GPs and other specialists, advertisements in social media, and websites focused on veganism. | 222 children: 91 VG, 75 were VN and 52 OM; age 0 to 18 years. No data on PA or SES collected. | 3-day weighed dietary records to evaluate iodine intake; the use of iodine supplements and their dosages and frequencies were assessed by questionnaire; breast milk intakes were estimated from mothers’ registrations and general recommendations for breast milk intake. | WT, HT. Serum TSH, fT4, fT3, thyroglobulin, and levels of anti-thyroid peroxidase antibody (ATPOc) and anti-thyroglobulin antibodies (AhTGc) concentration of iodine in spot urine (UIC). | No difference in WT percentile, HT percentile between the groups, but lower BMI z-score in VN and a higher number n = 7 (i.e. 9%) of VN children below the 3rd percentile. No differences in TSH levels, fT3, thyroglobulin or ATPOc between the VG, VN, and OM groups; higher levels of fT4 in VN compared to the OM. The presence of AhTGc was more common in the VG (18.2%)/VN (35.0%) than in the OM group (2.1%). The UIC was found to be highest in the OM group vs. VG and VN. 31 VN, 31 VG and 10 OM children met the criteria for iodine deficiency (i.e., UIC < 100 µg/l). 16.3% vegetarians and 21.8% of vegans took iodine supplements. VN and VG children may be more at higher risk of iodine deficiency, this theory is also supported by higher prevalence of AhTGc positivity. |
| Elliott et al. 2023. The TARGet Kids! cohort study. Canada [64]. |
A longitudinal cohort study. data was collected repeatedly between 2008 and 2019 during scheduled health supervision visits in primary care practices. | 8,907 children, including 248 VG children at baseline; aged 6 months to 8 years. 69% (6175 of 8907) of children had 2 or more measures. Growth data were available on 8794 children. No data on PA or SES collected. | Dietary group assessed by parental self- declaration of the child being on vegetarian or vegan diet. Both were classified as vegetarian (VG). | HT, WT, serum ferritin, 25 (OH)D, and serum lipids (non-HDL-C, TC, LDL-C, HDL-C, and TG). | No association between vegetarian diet and BMI z-score, height-for-age z-score, serum ferritin, 25 (OH)D, or serum lipids. VG had higher odds of underweight (BMI z-score <−2); no association of diet with overweight or obesity. |
| Rowicka et al. 2023 The IMC, Warsaw, Poland [67]. |
Cross- sectional; data collection 2020-2021; from a group of patients seeking dietary counselling at the IMC. | 32 VG children (age range 2–10 years) on a vegetarian diet from birth; 40 OM children. No data on SES collected. | 3-day food diary, average daily energy intake, the percentage of energy from protein, fat, and carbohydrates, and vitamin intakes. | HT, WT. Serum CRP, calprotectin, total oxidant capacity (TOC), total antioxidant capacity (TAC), reduced (GSH), and oxidized (GSSG) glutathione; the oxidative stress index (OSI) and the GSH/GSSG ratio were calculated. | No difference in BMI and BMI z-scores between dietary groups; however, VG tended to have lower values. VG had significantly lower median values of TOC, GSH and GSSG as well as CRP, and higher TAC compared with OM. The OSI was significantly lower in VG. |
| Ambroszkiewicz et al. 2023. The IMC, Warsaw, Poland [73]. | Cross-sectional; data collection 2020-2021; from a group of patients seeking dietary counselling at the IMC. | 51 VG, (among the VG group there were 9.6% vegan children) age range 4–9 years); most of them on a vegetarian diet from birth; 25 OM children. No data on SES collected, PA assessed by questionnaire. | 3-day food diary; average daily dietary energy, protein, fiber, calcium, phosphorus, magnesium, vitamin D, and amino acid intakes were assessed in 61 (80%) of the studied children. | WT, HT; serum amino acids, 25-OH- D, PTH, bone metabolism markers (osteocalcin, CTX-I, osteoprotegerin, IGF-I), albumin, and prealbumin. | No difference in BMI between VG and OM; serum concentrations of 4 amino acids (valine, lysine, leucine, isoleucine) were 10–15% lower in VG than OM; serum differences in amino acid levels were less marked than dietary intake differences. VG had lower (but still normal) serum albumin levels; they also had higher levels of CTX-I (bone resorption marker) than OM. There was no significant difference in other bone metabolism markers or PTH levels between groups. |
Abbreviations: 25-OH D - 25 hydroxy vitamin D, AhTGc -anti-thyroglobulin antibodies, ATPOc - anti-thyroid peroxidase antibody, BC- body composition, BMAD - bone apparent mineral density, BMC - bone mineral content, BMD - bone mineral density, CRP - c-reactive protein, DXA - dual-energy X-ray absorptiometry, Hb – haemoglobin, Hcys – homocysteine, holoTC – holotranscobalamin, HT- height, MMA - methylmalonic acid, MUAC - mid-upper arm circumference, OM – omnivore, OSI - the oxidative stress index, PA - physical activity (PA), PTH – parathormone, SES - socio – economic status, , sOB-R - soluble leptin receptor, sTfR - soluble transferrin receptor concentration, TAC - total antioxidant capacity, TOC -total oxidant capacity, UIC - concentration of iodine in spot urine, VG – vegetarian, VN – vegan, WT – weight.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



