
Submitted:
08 February 2024
Posted:
09 February 2024
You are already at the latest version
Abstract
Tick-borne diseases are among the most common vector-borne diseases. These include various infections caused by viruses, bacteria, rickettsiae, spirochetes and protozoa. The aim of our review is to present the relationship between the clinico-epidemiological aspect of some of the emergency tick-borne diseases and their diagnosis, treatment and prevention. We will review three diseases- anaplasmosis, babesiosis and ehrlichiosis. Anaplasmosis and ehrlichiosis are caused by small gram-negative obligate intracellular alphaproteobacteria in the order Rickettsiales, family Anaplasmataceae. The prognosis of disease depends on early diagnosis and proper treatment. The symptoms of anaplasmosis largely overlap with those of ehrlichiosis. Babesiosis is a malaria-like disease that is caused by intraerythrocytic protozoa. Like malaria, the disease proceeds with hemolysis and its severity is determined by the parasitemia. Treatment of babesiosis involves the use of antimalarial agents and antibiotics, most commonly in a combination. Understanding the clinical, epidemiological and laboratory characteristics of tick-borne diseases is crucial for their prevention, diagnosis and treatment.
Keywords:
tick‐borne
; anaplasmosis
; ehrlichiosis
; babesiosis
; diagnosis
; treatment
1. Introduction
As one of the most common vector-borne infections, the tick-borne ones are with great health and economic importance. These include various infections caused by viruses, bacteria, rickettsiae, spirochetes and protozoa. We will review three of these diseases-anaplasmosis, babesiosis and ehrlichiosis. The aim is to present the relationship between clinico-epidemiological aspect of these emergency tick-borne diseases and their diagnosis, treatment and prevention.
The family Anaplasmataceae is classified in the order Rickettiales and currently contains five genera and two candidate genera of obligate intracellular bacteria. Four of the genera contain members that are known to infect humans: Anaplasma, Ehrlichia, Neorickettsia, and “Candidatus Neoehrlichia” [1]. Anaplasma and Ehrlichia are currently ones of emerging tick-borne pathogens. Climate and socioeconomic changes in the distribution and abundance of arthropod vectors and related illnesses have led to increased recognition of a rise in the incidence and recurrence patterns of human diseases caused by these vector-borne pathogens. One of the most significant vector-borne illnesses in the United States is human granulocytic anaplasmosis (HGA). Data elucidates that from 2010 to 2018 there was a roughly 12-fold rise in reported cases in the country [2]. Additionally, there are more and more reports of it in Asia and a few Central and Northern European countries [3,4]. Similarly, a northern expansion of Amblyomma americanum and E. chaffeensis ticks has been linked to an increase in human ehrlichiosis (HME) cases in the United States [5].
Rickettsial diseases are almost indistinguishable in the first few days of the onset, characterized by an unknown febrile condition. Pancytopenia is a characteristic laboratory finding of HME early in the illness and 60 to 70% of patients experience mild to moderate decreased leucocyte ratio, and a great decrease in lymphocyte [6,7,8,9]. Within two weeks of the illness, anemia affects half of the patients [8,9,10]. It’s intriguing to note that most patients experience a large rise in lymphocyte count during convalescence, which is primarily caused by the expansion of activated γδ T cells. This results in both relative and absolute lymphocytosis [11]. One of the pathognomonic signs of HME is significant thrombocytopenia, which is often found in about 70–90% of patients. About 90% of patients have mild or moderate levels of hepatic cytolysis, with bilirubinemia and increased alkaline phosphatase levels. Up to half of adult patients and 70% of pediatric patients have hyponatremia [9,10,12]. HGA rash is uncommon, noted in less than 10% of patients, compared to HME [13,14,15,16]. HGA tends to be a less severe illness than HME.
The antibiotic of choice for the treatment of ehrlichiosis, anaplasmosis, and all other rickettsial infections is doxycycline. Moreover, doxycycline presumptive treatment is advised for patients of all ages, even younger ones under the age of eight. For those who do not respond to doxycycline, other illnesses resistant to it should be put in the differential diagnosis. The suggested course of treatment and dosages is 100 mg every 12 hours for adults, whereas youngsters under 45 kg (100 lbs.) should take 2.2 mg/kg twice daily. The American Academy of Pediatrics Committee on Infectious Diseases and the Centers for Disease Control and Prevention both recommend using doxycycline as a regular treatment for children who may have rickettsial illness. Short courses of doxycycline (approximately 5–10 days) did not cause enamel hypoplasia or discoloration of permanent teeth, according to a recent study. Alternative antibiotics may be considered in cases of severe doxycycline intolerance, allergy, and pregnancy. Although it hasn’t been tested as a substitute treatment in a clinical situation, rifampin seems to be effective against E. chaffeensis in a laboratory setting. Antibiotic prophylaxis after a tick bite is not advised [17,18,19].
HME can be lethal in immunocompetent patients and presents as a multisystem illness akin to toxic or septic shock syndrome [20,21,22]. Manifold research studies have documented a correlation between the administration of sulfonamide antibiotics and severe ehrlichia symptoms [23,24]. Although, it is unclear if this indicates a causal relationship. There have been sporadic cases of laboratory-confirmed reinfections with A. phagocytophilum, despite the possibility of long-term immunity following sporadic infection. As a result, people residing in endemic regions where they may come into contact with infected ticks must take extra precautions to prevent tick bite exposure [25,26]. Avoiding tick bites is one way to prevent tick-borne diseases, and removing ticks right away is still the best course of action. People who reside in endemic areas ought to wear light-colored clothing when they go outside so they can see ticks crawling on them [27]. Adults who are highly susceptible to tick bites should treat exposed areas of skin with chemo-prophylactic repellents, such as DEET (n, n-diethyl-m-toluamide), which blocks tick attachment. After leaving possibly tick-infested regions, people should thoroughly check their body, hair, and clothing for ticks and remove any that are attached right away. Research has indicated that Ehrlichia and Anaplasma require to be attached to the host at least 4–24 hours [27,28,29]. There are no available vaccines or other specific methods of prophylaxis.
Human babesiosis is the third infection that will be reviewed. Human babesiosis is an emergency tick-borne disease (TBD), a malaria-like disease caused by intraerythrocytic parasites of the genus Babesia. It is named after the European parthologist and microbiologist Victor Babes, who first isolated and described the causative agent of the disease [30]. In 1956 a case of human babesiosis was first reported in what was then Yugoslavia, now Croatia. Babesia divergens (B. divergens) was assumed to be the putative causative agent [31]. Nowadays, human babesiosis has beenreported in 19 European countries. Cases of human babesiosis with a proven other member of the genus Babesia- Babesia venatorum (B. venatorum), formerly called EU1, have been described in Italy, Germany, Sweden and Austria. Cases with isolated Babesia microti (B. mictori) have also been described in Germany [32].
2. Anaplasmosis
Anaplasma phagocytophilum has been known to cause disease among domestic and wild animals for decades. In the 20th century, in Scotland, an experiment was done on louping-ill (LI) where sheep living on pastures invaded by ticks acquired a condition represented by an unknown fever [33]. Additionally, the disease was temporarily termed “tick-borne fever” (TBF), and the cause was known to regard to the class Rickettsia. At present time, the name TBF still refers to an infection in domestic ruminants in Europe. Furthermore, its current name originates from the Greek word an, which means ‘without’, and plasma, ‘anything formed or molded’ [34]. The first case of Human granulocytic anaplasmosis (HGA) in the USA dates to 1990, while in Europe (Slovenia) a human being was initially diagnosed seven years later. Those have been patients with a history of tick bite exposure and severe febrile illness [35,36,37].
The condition is usually acquired by a tick bite and the major vector of transmission in Europe is Ixodes ricinus (sheep tick or castor bean tick), in the Eastern US Ixodes scapularis (deer tick or black-legged tick), in the Western US Ixodes pacificus (Western black-legged tick), and Asia Ixodes persulcatus (taiga tick) [38]. They can transmit the bacteria to their offspring (transovarial transmission), although its’ efficacy seems to be insignificant, whereas transstadial transmission is imperative in sustaining A. phagocytophilum within its endemic cycles [39,40,41]. Ticks contract the pathogen when feeding on an infected host. Generally, ruminants are reservoirs of the infection, with a white-footed mouse, Peromyscus leucopus, illustrating the main one and numerous other animals such as horses, dogs, domestic or wild ruminants (some strains), hedgehogs, and wild boars [42,43].
Correspondingly to the activity of nymphal and adult stages of Ixodes scapularis ticks, the disease has seasonal occurrence, with marked peaks in June but continuing through November, in association with outdoor activity [44]. Moreover, it has been observed that the pathogen and its vector’s geographical distribution are increasing in latitude and altitude [45] covering a tremendous amount of territory of continental and Atlantic Europe.
Another important point about Ixodes ticks is that they are frequently coinfected with other organisms. To exemplify that, researchers report that up to 36% of patients with serologic evidence of A. phagocytophilum infection also have positive serology for Borrelia burgdorferi or Babesia microti infection [46,47,48]. Concurrent infections with HGA and Lyme disease, documented by isolation of both agents, are reported [49], and coinfection with tick-borne encephalitis virus has been demonstrated (Powassan and deer tick viral encephalitis) [50]. It is not yet known, whether such concurrent infections will drive increased severity, prolonged duration of illness, or more frequent and severe sequelae [51].
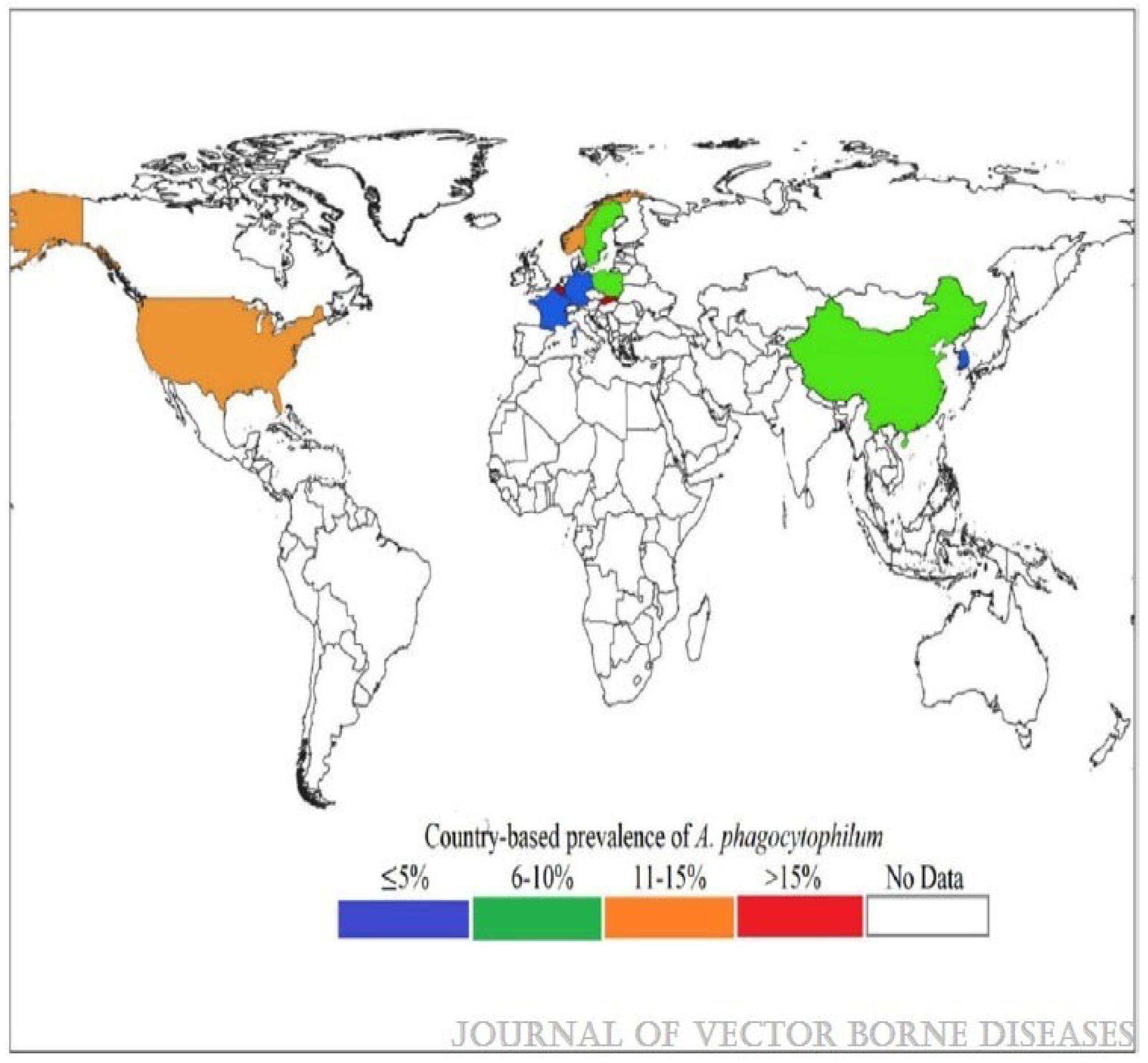
Apart from tick bite transmission, infections among humans have followed blood transfusions [52,53,54]. In addition, nosocomial exposure via direct contact with blood or respiratory secretion from a severely ill patient with HGA was suspected in China [55], but this assertion is still insufficient [56]. At present times, there is a huge amount of data that illustrates the pathogen as a burgeoning health issue due to global warming [57] and anthropogenic influence [58]. For instance, the announced annual report has an upward trend with over a quarter enhancement in the global prevalence of the illness for the 50-year study period, Figure 1 [59].
An epidemiological investigation presented a seroprevalence in Europe which ranges between ~8.3% and 31%. This disparity between the high percentage of seroprevalence and recognized symptomatic cases comes from inadequate diagnosis, or immense percentage of asymptomatic cases [60], or serological cross-reactivity that may give rise to misinterpretation of seroprevalence ratio [61,62].
Anaplasma phagocytophilum belongs to the family Anaplasmataceae, order Rickettsiale, and the class Alphaproteobacteria [63]. It is a small, obligate, gram-negative, intracellular bacterium forming small groups called morulae which are a histopathological hallmark of the disease. Moreover, it prefers to grow within myeloid or granulocytic cells [64]. Anaplasma phagocytophilum is inoculated in the host through a tick bite, following distribution to the bone marrow and spleen, where it can selectively withstand and proliferate within cytoplasmic vacuoles of polymorphonuclear cells. Usually, it modifies the progenitors of myeloid and monocytic cells and can be found in neutrophils in peripheral blood and tissues. Further, Anaplasma’s presence in neutrophils triggers proinflammatory responses leading to deactivation and degranulation of neutrophils and release of cytokines. Interleukin-10, IL12, and IFN-gamma are the main cytokines that contribute to continuous tissue damage. Thus, it protects neutrophils from exerting competent antimicrobial response. Moreover, Anaplasma can also restrict the fusion of lysosomes with the cytoplasmic vacuoles and obstruct signaling pathways in charge of respiratory bursts. The bacterium may also disturb the regulation of phagocyte oxidase, cause procrastination in apoptosis, incompetent binding to and transmigration of activated endothelium, and inhibition of phagocytosis [65].
Ethological diagnosis of human granulocytic anaplasmosis can be confirmed by using several methods. These include serologic, microscopic identification of characteristic morulae in peripheral blood, detection of nucleoid acid by PCR, immunohistochemistry, or culture [65].
Morulae may be found in 25% to 75% of the microscopic samples from patients who have not proceeded with antibiotic therapy. The sensitivity of this diagnostic method is greater during the first week of infection [66] and dramatically decreases within 24–72 hours after initiation of doxycycline [67]. Although, Sungim Choia, Young-Uk Chob, Sung-Han Kima [68], presented a case report of a patient with 5-day-illness history and empirical treatment with doxycycline [69]. The culture of A. phagocytophilum is time-consuming, and thus is not routinely available, whereas PCR is more sensitive, highly specific, and time-saving. As regards serologic diagnosis, the diagnosis is confirmed by the detection of IgM and IgG immunoglobulins [70].
Human granulocytic anaplasmosis has an incubation period of 1 to 2 weeks and is characterized by a febrile condition that ranges from asymptomatic or symptomatic, but self-limiting to fatal [71]. The most common symptoms include fever, chills, sweating, myalgia, arthralgia, gastrointestinal symptoms from the upper tract, and rarely rashes. In contrast, CNS is involved rarely, presenting such as meningoencephalitis, while PNS involvement includes plexopathy, cranial and facial nerve palsies, and demyelinating polyneuropathy which may require long-term recovery [72,73,74,75]. Other rare clinical manifestations involve cerebral infarction in the left basal ganglia [76], seizures, temporary memory impairment, orchitis, glomerulonephritis, myositis with severe rhabdomyolysis, Sweet’s syndrome, and hemophagocytic lymphohistiocytosis (HLH) [77,78,79,80,81,82,83,84]. Importantly, the severity of the disease depends on the patient’s age group, concomitant conditions, and initiation of the treatment. Severe outcomes and hospitalization have been addressed in over a third of the patients. If untreated, manifestations such as respiratory and renal failure, gastrointestinal bleeding, and liver impairment, may occur in about 3% of the cases [85].
Current data elucidates that immunosuppressed such as transplant patients do not appear to experience altered clinical signs of anaplasmosis just as non-transplant ones. What is more, in those cases a good outcome to the antibiotic treatment has been reported [86,87,88].
Paraclinical feathers of the illness include leukopenia, anemia, thrombocytopenia, and hepatic cytolysis. As well as neutropenia with a left shift and mild lymphocytosis can also be seen [89,90,91,92]. Moreover, hyperferritinemia and proinflammatory cytokine release have been marked as risk factors for a severe outcome of Anaplasmosis. For those patients with central nervous system manifestations, CSF analysis shows lymphocytic pleocytosis and steady protein elevation [89,93].
As a rickettsial pathogen, A. phagocytophilum has been recognized as a persistent microorganism in mammalian hosts. However, this may alter following the variants of the bacterium engaged [94].
3. Human Monocytotropic Ehrlichiosis
Ehrlichia is genus in Ehrlichiaceae family, order Rickettsiales, class Alphaproteobacteria. The genus Ehrlichia consists of two species causing illness among humans—Ehrlichia chaffeesis, which causes human monocytic ehrlichiosis (HME), and Ehrlichia ewingii, associated with Ehrlichia ewingii ehrlichiosis. Other species Ehrlichia canis and Ehrlichia ruminantium have generally veterinary significance but may also accidentally infect humans, and from the past few years a newly described pathogen EMLA (Ehrlichia muris-like agent) or E. muris eauclairensis, which has also been associated with human disease [95].
Ehrlichia is a Gram-negative obligate intracellular coccobacillus. As a nonmotile bacteria, Ehrlichia resides and cultivates in cytoplasmic vacuoles, composing aggregates of bacteria called morulae. Under light microscopy morulae resemble intracytoplasmic inclusions that stain dark blue or purple with Romanovsky-type stains and look like a mulberry because it comes from the Latin word ‘morus’ [96]. Ehrlichial morulae have been identified in numerous fluids and tissues such as blood, bone marrow, hepatic sinusoids, splenic cords, lymph nodes, cerebrospinal fluid (CSF) macrophages, and macrophages in the kidney, appendix, and heart.
Ehrlichia are intracellular, gram-negative organisms that have a tick-borne transmission mode. Vectors are ticks from the species Lone Star tick (Amblyomma americanum) the American dog tick (Dermacentor variabilis), as well as Ixodes scapularis (Blacklegged tick). The pathogen can be transmitted trans-stadially but not transovarially. In addition to humans, other hosts include domestic and wild animals such as dogs, cattle, sheep, goats, rodents, and deer. Other possible rare ways of transmission are due to blood transfusion and organ transplant.
The annual incidence ratio of human ehrlichiosis has been determined to be 3 to 5 per 100,000 in endemic territories in the USA [97]. Also, in 2019, the Centers for Disease Control and Prevention stated that about 50% of the cases of ehrlichiosis in the USA were diagnosed in just four states (Missouri, Arkansas, North Carolina, and New York). Moreover, since 2009, more than 115 cases of ehrlichiosis with a causative agent E. muris eauclairensis have been announced in Upper Midwest. In contrast, in Europe, the incidence rate is significantly low since less is known about Ehrlichiosis distribution [98,99,100].
In HME, clinical manifestations appear in between 5 to 14 days post-tick bite. The illness usually presents with a febrile illness characterized by myalgia, headache, nausea, vomiting, diarrhea, anorexia, and rash. Generally, every third patient experiences a rash, which is more common among those infected with E. chaffeensis and is present more frequently in children compared to adults, where it is often found in patients with HIV [101]. The eruption occurs mainly up to 5 days after the febrile condition initiates and can be maculopapular or petechial [102]. Adults with serious disease experience diarrhea, lymphadenomegalia, and confusion, while the pediatrician population experiences edema on the extremities. Moreover, complications occur between 9 to 17% of the cases and include ARDS, DIC syndrome, renal failure, CNS manifestations (CSF lymphocytic pleocytosis and proteinorrahia), and others. Ehrlichia chaffeensis may lead to hemophagocytic lymphohistiocytosis (HLH) [103,104,105,106,107,108,109,110,111,112,113]. Researchers report that relatively one to three in ten infections have been announced in immunocompromised where E. chaffeensis acts as an opportunistic parasite [114,115,116,117].
Etiological diagnosis can be obtained with several methods. For instance, the most widely used is serology because it is a cost-effective and relatively fast method, but it can give false positive\negative results due to cross-reactivity reactions and usually comes negative for most of the tests in the first week of the disease [118]. Another example is visualization of morulae and staining method which is a rapid and seldom used as a confirmatory practice [119,120,121,122,123]. Morulae are typically seen in less than 5% of the leukocytes. Case series documenting individuals for whom morula visualization, as an independent diagnostic sign, had culture or PCR-confirmed HME sensitivity values of roughly one-third [119,121,124].
PCR techniques are increasingly being used as conventional supplements to serologic diagnostic methods to detect DNA from Ehrlichia spp. in whole blood, CSF, and serum. When serologic testing is still negative, an acute-phase whole-blood sample from E. chaffeensis patients can often yield positive results by PCR [119]. A lab procedure that can process clinical specimens utilizing cell culture techniques is necessary for the separation of Ehrlichia species from blood, CSF, and other tissues. Some cultures have shown signs of morulae as early as two days after inoculation, while in others primary isolation has taken a much longer time [120,121,125].
4. Human Babesiosis
Nowadays, human babesiosis has been reported in 19 European countries. Cases of human babesiosis with a proven other member of the genus Babesia- Babesia venatorum (B. venatorum), formerly called EU1, have been described in Italy, Germany, Sweden and Austria. Cases with isolated Babesia microti (B. mictori) have also been described in Germany [32].
Over 100 species of the genus Babesia have been reported, but only a few are pathogenic for humans—B. microti, B. divergens, B. duncani, B. venatorum, and an as yet unnamed strain named MO-1 [126,127]. In North America, the most common causative agent is B. microti, whose vector is I. scapularis, it is widespread in the Midwestern United States [128]. The second most common species in North America is B. duncani, cases of human babesiosis with a proven causative agent of B. duncani have been reported along the Pacific coast of the United States and Canada [128,129]. There are various studies suggesting that vectors of B. duncani are Ixodes species—I. scapularis, I. pacificus also the winter tick, and Dermacentor albipictus [128,130,131]. In Europe, the most common causative agent of human babesiosis is B. divergens, whose vector is I. ricinus. In addition to B. divergens, I. ricinus also carries B. venatorum and B. microti. In South Asia, B. microti is transmitted by Ixodes ovatus Neumann, while cases of Babesia crassa and B. venatorum have been reported from China, probably transmitted by I. persulcatus [132]. People of any age and sex can be affected by human babesiosis. It is most severe in patients over 40 years of age who are immunosuppressed or splenectomized. A different phenomenon of disease transmission has also been described in the USA- in blood transfusions with infected blood.
Babesioses belong to Phylum: Apicomplexa, Class: Sporozoa, Order: Piroplasmida, Family: Babesiidae, Genus: Babesia [133]. Babesiasia are divided according to their size into large Babesiasia (2.5–5)—B. bigemina, Babesia caballi, Babesia canis, etc. and small (1.0–2.5)—B. bovis, Babesia gibsoni, B. microti, Babesia rodhaini, etc. [134]. The biological cycle of babesias occurs in two hosts. Sexual reproduction takes place in crustaceans and asexual phase in vertebrates. Biological stages are as described: in animals—schizogony, erythrocyte cycle: trophozoites—small babesias of 1–2.5 mt and large babesias of 2.5–5 mt (ring-shaped), merozoites, gametes. In the tick: gametogonia (sexual reproduction)—in the stomach of the tick; ookinetes and sporogonia—formation of sporozoites in the salivary glands. Infected ticks, when inoculated with blood, inoculate into the host and after that host sporozoites penetrate erythrocytes. Simple fission (schizogony) follows, producing merozoites. They lyse infected cells and penetrate new erythrocytes. A distinguishing feature is the formation of pairs of parasites or tetrads (4 parasites) resembling a Maltese cross. Some of the trophozoites do not reproduce in the blood but differentiate into male and female gametes [135].
After a tick bite, the babesia get into the capillary blood of the infected person where they target the erythrocytes, unlike Plasmodium ssp. getting into the erythrocytes they start to mature and grow [135]. The early stages of the cycle closely resemble those of Plasmodium ssp. as they look like ring parasites, a budding process follows where they replicate and resemble an “eight”, budding can be repeated where a tetrad known as a “Maltese Cross” is produced. After reaching the merozoite stage, the parasites leave the erythrocyte cells, leading to their hemolysis, and the parasites seek out new cells to infect [136].
Disease can vary in severity depending on various factors—the age of the patient, his immunological status, the type of parasite, etc. The disease is most severe in neonates, in all immunocompromised patients, especially in asplenic patients. It is not known how long it takes for the infection to be transmitted from tick to human; in white-footed mice it has been found to take 36 to 54 hours [137].The incubation period for tick-borne transmission is 1 to 4 weeks, and when the infection results from haemotraesfusion the incubation period is up to 6 weeks [138]. Babesiae possess mechanisms to evade the immune response, which often results in persistence of infection in healthy individuals, which are most often asymptomatic; this is particularly characteristic of B. microti. In case of infection with B. microti in healthy individuals, the disease may proceed asymptomatically; in mild parasitaemia < 4%, the most common symptoms include myalgia, fever, chills, headache, vomiting and diarrhoea. In high parasitaemia (>10%) [139,140], complications such as acute respiratory distress syndrome, renal failure, shock, desiminated intravascular colagulopathy and congestive heart failure may occur. Up to 10% of hospitalized patients end lethally, and if the infection is the result of chemotherapy, this percentage reaches 20% [141]. Infections with proven causative B. divergens can run from mild to severe. Parasitaemia in different cases varies from 0.29 [142] to 20% [143] in mild course of the disease the symptoms are flu-like- athromyalgia, fever, headache, chills, in more severe course haemolytic anaemia, jaundice, renal failure, haemoglobinuria, vomiting and abdominal pain may develop and may end fatally. There have been five reported cases in Europe of infection with proven causative agent B. venatorum, all described in patients over 50 years of age with severe immunosuppression. It can run again from mild to severe. Symptoms reported include- shortness of breath, progressive weakness, intermittent episodes of fever, jaundice, thrombocytopenia, haemoglobinuria, acute renal failure. Parasitaemia ranges from 1.3 to 30% [144]. A study in China found 48 of 2912 seropositive cases, demonstrating that infection with B. venatorum infection is milder in immunocompetent patients compared to B. divergens [145].
In the past, ignorance of the existence of Babesia ssp. and that they can cause disease in humans led to many misdiagnoses. There are still cases in which babesiosis is proven postmortem. Episodes of fever accompanied by haemolytic anaemia and a positive Coombs test, together with elevated procalcitonin levels and a history of tick bite, travel to Babesiosis endemic countries or blood transfusion necessitate thinking in the direction of a diagnosis- Babesiosis [146,147].
The gold standard for proof of babesiosis is detection of the parasite in a blood smear stained by the Giemsa or Romanowsky method. Parasitaemia is small in the initial stages of the disease, necessitating the collection of a series of blood samples, evaluating over 300 fields of view. Differential diagnosis with Malaria is important. It has applications in research because it is a laborious and lengthy process in which animal species are infected with parasites- Babesia divergens, B. microti and B. duncani and the presence of parasitaemia in their blood is monitored for up to two months [146]. The indirect immunofluorescence assay is the most commonly used serological test method. IgG- at borderline titres of 1:32 to 1:160, specificity > 90% and sensitivity > 88% are found. In the course of infection, titres of >1:1028 may be detected, subsequently decreasing to 1:64. A disadvantage of IgG testing is that it cannot differentiate whether the infection is axial, subacute, chronic, or has already passed. IgM- indicate acute infection but can give false positive results, this requires a two stage testing process where individuals with positive IgG Ab are tested for IgM Ab [147,148]. Immunofluorescence assays are inaccurate, nonspecific, variable and often false positive in patients with rheumatologic diseases and those with similar infectious diseases such as malaria and toxoplasmosis [149]. Molecular biology tests: These have the highest sensitivity, are used in patients with low parasitaemia, and it has been shown that reel-time PCR can detect up to 20 genomic copies in 1 microliter of blood. Most commonly, 18sRNA is used for detection of Babesia ssp [150].
Choosing the right therapy and its duration depends on the type of parasite, the immunological status of the patient, the severity of the disease and a number of factors. A combination of antiparasitic and antibiotic medication is usually done. In case of infection with B. microti a standard combination is used- atovaquone/azithromycine [151], a study was conducted which proved that the combination of quinine plus clindamycin has the same effect, but the risk of more frequent and more severe side effects increases [152]. Cases of asplenic patients infected with B. divergaens are regarded as emergencies, as a large proportion of them end lethally [4]. There have been good results from the administration of a combination between clindamycin and quinine for 7 to 10 days [153]. In infection with B. venatorum treatment with clindamycin in combination or not with quinine, followed or not by treatment with atovaquone and azithromycin, gives good results [154].
5. Conclusions
Increasing numbers of human cases of vector-borne diseases are being reported globally, with tick-borne diseases occupying a large proportion of these. This can be attributed to a number of factors: the increased tick population in the Northern Hemisphere due to ecological changes, urbanization and the cosmopolitan lifestyle of modern humans. The diseases we have described were first reported in humans last century, so there is not yet complete clarity about their biology. Knowledge of their epidemiology, mode of infection, clinical characteristics and effective therapy is of essential importance to the health worker. Given the fact that these diseases are a socially significant and emergency condition, a series of events are needed to increase the knowledge of health professionals, develop innovative methods for their detection, determine their susceptibility to drugs intended for their irradiation. Some screening programs, such as testing blood products for the presence of infectious agents and the development of vaccines, have also yielded positive results.
References
- Family Anaplasmataceae (Anaplasmosis, Ehrlichiosis, Neorickettsiosis, and Neoehrlichiosis) - William L. Nicholson, in Principles and Practice of Pediatric Infectious Diseases (Fifth Edition), 2018. [CrossRef]
- Khatat, S.E.H.; Daminet, S.; Duchateau, L.; Elhachimi, L.; Kachani, M.; Sahibi, H. Epidemiological and Clinicopathological Features of Anaplasma phagocytophilum Infection in Dogs: A Systematic Review. Front. Veter.-Sci. 2021, 8, 686644. [Google Scholar] [CrossRef]
- Matei, I.A.; Estrada-Peña, A.; Cutler, S.J.; Vayssier-Taussat, M.; Castro, L.V.; Potkonjak, A.; Zeller, H.; Mihalca, A.D. A review on the eco-epidemiology and clinical management of human granulocytic anaplasmosis and its agent in Europe. Parasites Vectors 2019, 12, 599. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Cui, F.; Wang, L.; Zhang, L.; Zhang, J.; Wang, S.; Yang, S. Investigation of anaplasmosis in Yiyuan County, Shandong Province, China. Asian Pac. J. Trop. Med. 2011, 4, 568–572. [Google Scholar] [CrossRef]
- Gettings, J.R.; Self, S.C.W.; McMahan, C.S.; Brown, D.A.; Nordone, S.K.; Yabsley, M.J. Local and regional temporal trends (2013–2019) of canine Ehrlichia spp. seroprevalence in the USA. Parasites Vectors 2020, 13, 153. [Google Scholar] [CrossRef]
- Paddock CD, Suchard DP, Grumbach KL, et al. Brief report: fatal seronegative ehrlichiosis in a patient with HIV infection. N Engl J Med 1993;329:1164–1167. [PubMed: 8377780]. [CrossRef]
- Olano JP, Hogrefe W, Seaton B, et al. Clinical manifestations, epidemiology, and laboratory diagnosis of human monocytotropic ehrlichiosis in a commercial laboratory setting. Clin Diagn Lab Immunol 2003;10:891 896. [PubMed: 12965923]. [CrossRef]
- Olano JP, Masters E, Hogrefe W, et al. Human monocytotropic ehrlichiosis, Missouri. Emerg Infect Dis 2003;9:1579–1586. [PubMed: 14720399]. [CrossRef]
- Carpenter CF, Gandhi TK, Kong LK, et al. The incidence of ehrlichial and rickettsial infection in patients with unexplained fever and recent history of tick bite in central North Carolina. J Infect Dis 1999;180:900–903. [PubMed: 10438390]. [CrossRef]
- Chapman AS, Bakken JS, Folk SM, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever, ehrlichioses, and anaplasmosis-United States: a practical guide for physicians and other health-care and public health professionals. MMWR Recomm Rep 2006;55 (RR-4):1–27. [CrossRef]
- Caldwell CW, Everett ED, McDonald G, et al. Lymphocytosis of gamma/delta T cells in human ehrlichiosis. Am J Clin Pathol 1995;103:761–766. [PubMed: 7785663]. [CrossRef]
- Paddock CD, Childs JE. Ehrlichia chaffeensis: a Prototypical Emerging Pathogen. Clin Microbiol Rev 2003;16:37–64. [PubMed: 12525424]. [CrossRef]
- Lin M, den Dulk-Ras A, Hooykaas PJ. Anaplasma phagocytophilum AnkA secreted by the type IV secretion system is tyrosine phosphorylated by Abl-1 to facilitate infection. Cell Microbiol 2007;9:2644–2657. [PubMed: 17587335]. [CrossRef]
- Dumler JS, Barat NC, Barat CE, et al. Human granulocytic anaplasmosis and macrophage activation. Clin Infect Dis 2007; 45:199–204. [PubMed: 17578779]. [CrossRef]
- Bakken JS, Dumler JS. Ehrlichiosis and anaplasmosis. Infect Med 2004; 21:433–51.
- Marty AM, Dumler JS, Imes G, et al. Ehrlichiosis mimicking thrombotic thrombocytopenic purpura. Case report and pathological correlation. Human Pathol 1995; 26:920–025. [PubMed: 7635455]. [CrossRef]
- https://www.cdc.gov/ticks/tickbornediseases/ehrlichiosis.
- https://www.cdc.gov/ticks/tickbornediseases/anaplasmosis.
- Ehrlichioses in Humans: Epidemiology, Clinical Presentation, Diagnosis, and Treatment - J. Stephen Dumler, John E. Madigan, Nicola Pusterla, and Johan S. Bakken. [CrossRef]
- Fichtenbaum CJ, Peterson LR, Weil GJ. Ehrlichiosis presents as a life-threatening illness with features of toxic shock syndrome. Am J Med 1993;95:351–357. [PubMed: 8213865]. [CrossRef]
- Walker DH, Dumler JS. Human monocytic and granulocytic ehrlichioses discovery and diagnosis of emerging tick-borne infections and the critical role of the pathologist. Arch Pathol Lab Med 1997;121:785–791. [PubMed: 9278605].
- Sehdev AE, Dumler JS. Hepatic pathology in human monocytic ehrlichiosis. Ehrlichia chaffeensis infection. Am J Clin Pathol 2003;119:859–865. [PubMed: 12817434]. [CrossRef]
- Peters TR, Edwards KM, Standaert SM. Severe ehrlichiosis in an adolescent taking trimethoprim-sulfamethoxazole. Pediatr Infect Dis J 2000;19:170–2. [PubMed: 10694012]. [CrossRef]
- Brantley, RK. Trimethoprim-sulfamethoxazole and fulminant ehrlichiosis [Letter]. Pediatr Infect Dis J 2001;20:231. [PubMed: 11224854]. [CrossRef]
- Dunning Hotopp JC, Lin M, Madupu R, et al. Comparative genomics of emerging human ehrlichiosis agents. PLoS Genet 2006;2:e21. [PubMed: 16482227]. [CrossRef]
- Bakken JS, Dumler JS. Ehrlichiosis and anaplasmosis. Infect Med 2004;21:433–51.
- Katavolos P, Armstrong PM, Dawson JE, Telford SR III. Duration of tick attachment required for transmission of granulocytic ehrlichiosis. J Infect Dis 1998;177:1422–5. [PubMed: 9593039]. [CrossRef]
- des Vignes F, Piesman J, Heffernan R, et al. Effect of tick removal on transmission of Borrelia burgdorferi and Ehrlichia phagocytophila by Ixodes scapularis nymphs. J Infect Dis 2001;183:773– 8. [PubMed: 11181154]. [CrossRef]
- Needham GR. Evaluation of five popular methods of tick removal. Pediatrics 1985;75:997–1002. [PubMed: 4000801]. [CrossRef]
- Babes, V. “Sur l’hemoglobinurie bacterienne du boeuf.” CR Acad. Sci 107 (1888): 692-694.9.
- Skrabalo, Z.; Deanovic, Z. Piroplasmosis in man; report of a case. Doc. Med. Geogr. Trop. 1957, 9, 11–16 9. [Google Scholar]
- Hildebrandt, A.; Zintl, A.; Montero, E.; Hunfeld, K.-P.; Gray, J. Human Babesiosis in Europe. Pathogens 2021, 10, 1165. [Google Scholar] [CrossRef] [PubMed]
- Bakken JS, Dumler JS. Human granulocytic ehrlichiosis. Clin Infect Dis. 2000; 31:554-560. [CrossRef]
- Horowitz HW, Marks SJ, Weintraub M, et al. Brachial plexopathy associated with human granulocytic ehrlichiosis. Neurology. 1996; 46:1026-1029. [CrossRef]
- Chen SM, Dumler JS, Bakken JS, Walker DH. Identification of a granulocytotropic Ehrlichia species as the etiologic agent of human disease. J Clin Microbiol. 1994;32:589–95. [CrossRef]
- Petrovec M, Furlan SL, Zupanc TA, Strle F, Brouqui P, Roux V, Dumler JS. Human disease in Europe is caused by a granulocytic Ehrlichia species. J Clin Microbiol. 1997;35:1556-9. [CrossRef]
- Brouqui PH, Dumler JS, Lienhard R, Brossard M, Raoult D. Human granulocytic ehrlichiosis in Europe. Lancet. 1995;346:782–3. [CrossRef]
- Sumption KJ, Wright D Sumption KJ, Wright DJ, Cutler SJ. Human ehrlichiosis in the UK. Lancet. 1995;346:1487–8. [CrossRef]
- Woldehiwet, Z., Horrocks, B. K., Scaife, H., Ross, G., Munderloh, U. G., Bown, K., et al. (2002). Cultivation of an ovine strain of Ehrlichia phagocytophila in tick cell cultures. J. Comp. Pathol. 127, 142–149. [CrossRef]
- Medlock JM, Hansford KM, Bormane A, Derdakova M, Estrada-Peña A, George JC, et al. Driving forces for changes in the geographical distribution of Ixodes ricinus ticks in Europe. Parasit Vectors. 2013;6:1. [CrossRef]
- Jahfari S, Coipan EC, Fonville M, Van Leeuwen AD, Hengeveld P, Heylen D, et al. Circulation of four Anaplasma phagocytophilum ecotypes in Europe. Parasit Vectors. 2014;7:365. [CrossRef]
- Krücken J, Schreiber C, Maaz D, Kohn M, Demeler J, Beck S, et al. A novel high-resolution melt PCR assay discriminates Anaplasma phagocyt- ophilum and “Candidatus Neoehrlichia mikurensis”. J Clin Microbiol. 2013;51:1958–61.
- James CA, Pearl DL, Lindsay LR, Peregrine AS, Jardine CM. Risk factors associated with the carriage of Ixodes scapularis relative to other tick species in a population of pet dogs from southeastern Ontario, Canada. Ticks Tick Borne Dis. 2019 Feb;10(2):290-298. [PubMed: 30466965]. [CrossRef]
- Dahlgren FS, Heitman KN, Drexler NA, Massung RF, Behravesh CB. Human granulocytic anaplasmosis in the United States from 2008 to 2012: a summary of national surveillance data. Am J Trop Med Hyg. 2015; 93:66–72. [CrossRef]
- Stuen S, Granquist EG, Silaghi C. Anaplasma phagocytophilum—a widespread multi-host pathogen with highly adaptive strategies. Front Cell Infect Microbiol. 2013;3:31. [CrossRef]
- Lee EH, Rikihisa Y. Anti-Ehrlichia chaffeensis antibody complexed with E. chaffeensis induces potent proinflammatory cytokine mRNA expression in human monocytes through sustained reduction of IkappaB-alpha and activation of NF-kappaB. Infect Immun. 1997; 65:2890-2897. [CrossRef]
- Ismail N, Walker DH, Ghose P, et al. Immune mediators of protective and pathogenic immune responses in patients with mild and fatal human monocytotropic ehrlichiosis. BMC Immunol. 2012; 13:26. [CrossRef]
- Ismail N, Crossley EC, Stevenson HL, et al. The relative importance of T-cell subsets in monocytotropic ehrlichiosis: a novel effector mechanism involved in Ehrlichia-induced immunopathology in murine ehrlichiosis. Infect Immun. 2007; 75:4608-4620. [CrossRef]
- Nadelman RB, Horowitz HW, Hsieh TC, et al. Simultaneous- ous human granulocytic ehrlichiosis and Lyme borreliosis. N Engl J Med. 1997;337:27-30. [CrossRef]
- Nilmarie Guzman; Siva Naga S. Yarrarapu; Sary O. Beidas Anaplasma Phagocytophilum.
- Diuk-Wasser MA, Vannier E, Krause PJ. Coinfection by Ixodes tick-borne pathogens: ecological, epidemiological, and clinical consequences. Trends Parasitol. 2016;32: 30–42. [CrossRef]
- Bakken JS, Dumler S. Human granulocytic anaplasmosis. Infect Dis Clin. 2008;22:433–48. [CrossRef]
- Jereb M, Pecaver B, Tomazic J, Muzlovic I, Avsic-Zupanc T, Premru-Srsen T, et al. Severe human granulocytic anaplasmosis transmitted by blood transfusion. Emerg Infect Dis. 2012;18:1354–7. [CrossRef]
- Shields K, Cumming M, Rios J, Wong MT, Zwicker JI, Stramer SL, Alonso CD. Transfusion-associated Anaplasma phagocytophilum infection in a pregnant patient with thalassemia trait: a case report. Transfusion. 2015;55:719–25. [CrossRef]
- Zhang L, Liu Y, Ni D, Li Q, Yu Y, Yu XJ, et al. Nosocomial transmission of human granulocytic anaplasmosis in China. JAMA. 2008;300:2263–70. [CrossRef]
- Krause PJ, Wormser GP. Nosocomial transmission of human granulocytic anaplasmosis? JAMA. 2008;300:2308–9. [CrossRef]
- Bouchard C, Dibernardo A, Koffi J, Wood H, Leighton PA, Lindsay LR. Increased risk of tick-borne diseases with climate and environmental changes. Can Commun Dis Rep 2019;45(4):81–89. [CrossRef]
- Daszak P, Cunningham AA, Hyatt AD. Anthropogenic environmental change and the emergence of infectious diseases in wildlife. Acta Trop 2001;78:103–116. [CrossRef]
- Global status of Anaplasma phagocytophilum infections in human population: A 50-year (1970–2020) meta-analysis - Karshima, Solomon Ngutor1; Ahmed, Musa Isiyaku2; Mohammed, Kaltume Mamman1; Pam, Victoria Adamu Journal of Vector Borne Diseases 60(3):p 265-278, Jul–Sep 2023. [CrossRef]
- Dumler JS, Choi KS, Garcia-Garcia JC, Barat NS, Scorpio DG, Garyu JW, et al. Human granulocytic anaplasmosis and Anaplasma phagocytophilum. Emerg Infect Dis. 2005;11:1828–34. [CrossRef]
- Nordberg M. Tick-borne infections in humans: aspects of immunopathogenesis, diagnosis, and co-infections with Borrelia burgdorferi and Anaplasma phagocytophilum. Ph.D thesis, Linköping University, Sweden; 2012.
- Dumler JS, Barbet AF, Bekker CP, Dasch GA, Palmer GH, Ray SC, et al. Reorganization of genera in the families Rickettsiaceae and Anaplasmataceae in the order Rickettsiales: unification of some species of Ehrlichia with Anaplasma, Cowdria with Ehrlichia and Ehrlichia with Neorickettsia, descriptions of six new species combinations and designation of Ehrlichia equi and HGE agent as subjective synonyms of Ehrlichia phagocytophila. Int J Syst Evol Microbiol 2001;51:2145–2165. [CrossRef]
- Dumler JS, Choi KS, Garcia-Garcia JC, et al. (December 2005). “Human granulocytic anaplasmosis and Anaplasma phagocytophilum”. Emerging Infect. Dis. 11 (12): 1828. PMC 3367650. PMID 16485466. [CrossRef]
- Nilmarie Guzman; Siva Naga S. Yarrarapu; Sary O. Beidas-Anaplasma Phagocytophilum.
- Anaplasma Phagocytophilum-Nilmarie Guzman; Siva Naga S. Yarrarapu; Sary O. Beidas.
- Shah JS, Horowitz R, Harris NS. Human babesiosis and ehrlichiosis–current status. Eur Infect Dis 2012;6:49–56.
- Morulae in neutrophils: A diagnostic clue for human granulocytic anaplasmosis Sungim Choia, Young-Uk Chob, Sung-Han Kima. [CrossRef]
- Davies RS, Madigan JE, Hodzic E, et al. Dexamethasone- induced cytokine changes associated with diminished disease severity in horses infected with Anaplasma phagocytophilum. Clin Vaccine Immunol. 2011;18:1962–1968. [CrossRef]
- Dumler JS, Madigan JE, Pusterla N, et al. Ehrlichioses in humans: epidemiology, clinical presentation, diagnosis, and treatment. Clin Infect Dis. 2007;45(suppl 1):S45–S51. [CrossRef]
- Bakken JS, Dumler JS. Clinical diagnosis and treatment of human granulocytotropic anaplasmosis. Ann N Y Acad Sci 2006;1078:236–247. [CrossRef]
- Guo WP, Huang B, Zhao Q, Xu G, Liu B, Wang YH, Zhou EM. Human-pathogenic Anaplasma spp., and Rickettsia spp. in animals in Xi’an, China. PLoS Negl Trop Dis. 2018 Nov;12(11): e 0006916. [PMC free article: PMC6258427] [PubMed: 30419024]. [CrossRef]
- Kim SW, Kim CM, Kim DM, Yun NR. Manifestation of anaplasmosis as cerebral infarction: a case report. BMC Infect Dis. 2018 Aug 17;18(1):409. [PMC free article: PMC6098650] [PubMed: 30119642]. [CrossRef]
- Goel R, Westblade LF, Kessler DA, Sfeir M, Slavinski S, Backenson B, Gebhardt L, Kane K, Laurence J, Scherr D, Bussel J, Dumler JS, Cushing MM. Death from Transfusion-Transmitted Anaplasmosis, New York, USA, 2017. Emerg Infect Dis. 2018 Aug;24(8):1548-1550. [PMC free article: PMC6056119] [PubMed: 30016241]. [CrossRef]
- Kobayashi KJ, Weil AA, Branda JA. Case 16-2018: A 45-Year-Old Man with Fever, Thrombocytopenia, and Elevated Aminotransferase Levels. N Engl J Med. 2018 May 24;378(21):2023-2029. [PubMed: 29791814]. [CrossRef]
- Manifestation of anaplasmosis as cerebral infarction: a case report - Seok Won Kim, Choon-Mee Kim, Dong-Min Kim and Na Ra Yun. [CrossRef]
- Grant, L.; Mohamedy, I.; Loertscher, L. One man, three tick-borne illnesses. BMJ Case Rep. 2021, 14, e241004. [Google Scholar] [CrossRef] [PubMed]
- Halasz, C.L.G.; Niedt, G.W.; Kurtz, C.P.; Scorpio, D.G.; Bakken, J.S.; Dumler, J.S. A case of sweet syndrome associated with human granulocytic anaplasmosis. Arch. Dermatol. 2005, 141, 887–889. [Google Scholar] [CrossRef] [PubMed]
- Eldaour, Y.; Hariri, R.; Yassin, M. Severe Anaplasmosis presenting as possible CVA: Case report and 3-year Anaplasma infection diagnosis data is based on PCR testing and serology. IDCases 2021, 24, e01073. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A.; Lloji, A.; Doobay, R.; Wang, G.; Knoll, B.; Dhand, A.; Nog, R. Anaplasma phagocytophilum presenting with orchitis in a renal transplant recipient. Transpl. Infect. Dis. 2019, 21, e13129. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Kim, C.M.; Kim, D.M.; Yun, N.R. Manifestation of anaplasmosis as cerebral infarction: A case report. BMC Infect. Dis. 2018, 18, 409. [Google Scholar] [CrossRef] [PubMed]
- Young, N.P.; Klein, C.J. Encephalopathy with seizures having PCR-positive Anaplasma phagocytophilum and Ehrlichia chaffeensis. Eur. J. Neurol. 2007, 14, 2006–2007. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.; Brown, M.; Rabbat, M.; Slim, J. Hemophagocytic Lymphohistiocytosis Associated with Anaplasmosis. J. Glob. Infect. Dis. 2017, 9, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Jameel, M.N.Q.; Ali, S.S.; Mir, S. Human granulocytic anaplasmosis affecting the myocardium. J. Gen. Intern. Med. 2005, 20, 958. [Google Scholar] [CrossRef]
- Dahlgren FS, Mandel EJ, Krebs JW, Massung RF, McQuiston JH. Increasing incidence of Ehrlichia chaffeensis and Anaplasma phagocytophilum in the United States, 2000-2007. Am J Trop Med Hyg 2011;85(1):124–231. [CrossRef]
- Assi MA, Yao JD, Walker RC. Lyme disease followed by human granulocytic anaplasmosis in a kidney transplant recipient. Transpl Infect Dis 2007; 9: 66-72 [PMID: 17313478]. [CrossRef]
- Khatri A, Lloji A, Doobay R, Wang G, Knoll B, Dhand A, Nog R. Anaplasma phagocytophilum presenting with orchitis in a renal transplant recipient. Transpl Infect Dis 2019; 21: e13129 [PMID: 31215144]. [CrossRef]
- Dana A, Antony A, Patel MJ. Vector-borne infections in solid organ transplant recipients. Int J Dermatol 2012; 51: 1-11 [PMID: 22182371]. [CrossRef]
- Aguero-Rosenfeld ME, Horowitz HW, Wormser GP, et al. Human granulocytic ehrlichiosis: a case series from a medical center in New York State. Ann Intern Med. 1996;125:904–908. [CrossRef]
- Bakken JS, Krueth J, Wilson-Nordskog C, et al. Clinical and laboratory characteristics of human granulocytic ehrlichiosis. JAMA. 1996;275:199–205. [CrossRef]
- Schotthoefer AM, Schrodi SJ, Meece JK, et al. Pro-inflammatory immune responses are associated with clinical signs and symptoms of human anaplasmosis. PLoS ONE. 2017;12:e0179655. [CrossRef]
- Lotric-Furlan S, Petrovec M, Avsic-Zupanc T, et al. Epidemiological, clinical and laboratory distinction between human granulocytic ehrlichiosis and the initial phase of tick-borne encephalitis. Wien Klin Wochenschr. 2002;114:636–640.
- Dumler JS, Barat NC, Barat CE, et al. Human granulocytic anaplasmosis and macrophage activation. Clin Infect Dis. 2007;45:199–204. [CrossRef]
- Jiao XY, Fan ZC, Li YZ, et al. Clinical and laboratory features parameters of human granulocytic anaplasmosis (HGA) in patients admitted to hospital in Guangdong Province, China. Trop Doct. 2015;45:209–213. [CrossRef]
- Snorre Stuen, Erik G. Granquist, and Cornelia Silaghi - Anaplasma phagocytophilum - a widespread multi-host pathogen with highly adaptive strategies. [CrossRef]
- CDC. Statistics | Ehrlichiosis |. CDC. Available at https://www.cdc.gov/ehrlichiosis/stats/. March 26, 2020; Accessed: May 25, 2021.
- Rikihisa, Y. 1991. The tribe Ehrlichieae and ehrlichial diseases. Clin. Microbiol Rev. 4:286–308. [CrossRef]
- Tick-borne zoonoses in Europe - Marta Granström. [CrossRef]
- Morais JD, Dawson JE, Green C et al. - First European case of ehrlichiosis. Lancet. 1991; 338: 633-634. [CrossRef]
- Pierard D, Levtchenko E, Dawson JE, Lauwers S - Ehrlichiosis in Belgium. Lancet. 1995; 346: 1233-1234. 1234. [CrossRef]
- Brouqui P, Raoult D, Durand JM - Ehrlichia species as possible causative agents of blood culture-negative. [CrossRef]
- Paddock, C. D., S. M. Folk, G. M. Shore, L. J. Machado, M. M. Huycke, L. N. Slater, A. M. Liddell, R. S. Buller, G. A. Storch, T. P. Monson, D. Rimland, J. W. Sumner, J. Singleton, K. C. Bloch, Y. W. Tang, S. M. Standaert, and J. E. Childs. 2001. Infections with Ehrlichia chaffeensis and Ehrlichia ewingii in persons coinfected with human immunodeficiency virus. Clin. Infect. Dis. 33:1586–1594. [CrossRef]
- https://www.cdc.gov/ehrlichiosis/symptoms/index.html - Ehrlichiosis.
- Nichols Heitman K, Dahlgren FS, Drexler NA, et al. Increasing incidence of ehrlichiosis in the United States: a summary of national surveillance of Ehrlichia chaffeensis and Ehrlichia ewingii infections in the United States, 2008-2012. Am J Trop Med Hyg. 2016;94:52–60. [CrossRef]
- Dunn BE, Monson TP, Dumler JS, et al. Identification of Ehrlichia chaffeensis morulae in cerebrospinal fluid mononuclear cells. J Clin Microbiol. 1992;30:2207–2210. [CrossRef]
- Ismail N, Walker DH, Ghose P, et al. Immune mediators of protective and pathogenic immune responses in patients with mild and fatal human monocytotropic ehrlichiosis. BMC Immunol. 2012;13:26. [CrossRef]
- Dumler JS, Madigan JE, Pusterla N, et al. Ehrlichioses in humans: epidemiology, clinical presentation, diagnosis, and treatment. Clin Infect Dis. 2007;45(suppl 1):S45–S51. [CrossRef]
- Fishbein DB, Dawson JE, Robinson LE. Human ehrlichiosis in the United States, 1985 to 1990. Ann Intern Med. 1994;120:736–743. [CrossRef]
- Schutze GE, Buckingham SC, Marshall GS, et al. Human monocytic ehrlichiosis in children. Pediatr Infect Dis J. 2007;26:475–479. [CrossRef]
- Kumar N, Goyal J, Goel A, et al. Macrophage activation syndrome secondary to human monocytic ehrlichiosis. Indian J Hematol Blood Transfus. 2014;30:145–147. [CrossRef]
- Abbott KC, Vukelja SJ, Smith CE, et al. Hemophagocytic syndrome: a cause of pancytopenia in human ehrlichiosis. Am J Hematol. 1991;38:230–234. [CrossRef]
- Burns S, Saylors R, Mian A. Hemophagocytic lymphohistiocytosis secondary to Ehrlichia chaffeensis infection: a case report. J Pediatr Hematol Oncol. 2010;32:e142–e143. [CrossRef]
- Cheng A, Williams F, Fortenberry J, et al. Use of extracorporeal support in hemophagocytic lymphohistiocytosis secondary to ehrlichiosis. Pediatrics. 2016;138. [CrossRef]
- Hanson D, Walter AW, Powell J. Ehrlichia-induced hemophagocytic lymphohistiocytosis in two children. Pediatr Blood Cancer. 2011;56:661–663. [CrossRef]
- Hamburg BJ, Storch GA, Micek ST, et al. The importance of early treatment with doxycycline in human ehrlichiosis. Medicine (Baltimore). 2008;87:53–60. [CrossRef]
- Paddock CD, Folk SM, Shore GM, et al. Infections with Ehrlichia chaffeensis and Ehrlichia ewingii in persons coinfected with human immunodeficiency virus. Clin Infect Dis. 2001;33:1586–1594. [CrossRef]
- Thomas LD, Hongo I, Bloch KC, et al. Human ehrlichiosis in transplant recipients. Am J Transplant. 2007;7:1641–1647. [CrossRef]
- Paddock, C. D., S. M. Folk, G. M. Shore, L. J. Machado, M. M. Huycke, L. N. Slater, A. M. Liddell, R. S. Buller, G. A. Storch, T. P. Monson, D. Rimland, J. W. Sumner, J. Singleton, K. C. Bloch, Y. W. Tang, S. M. Standaert, and J. E. Childs. 2001. Infections with Ehrlichia chaffeensis and Ehrlichia ewingii in persons coinfected with human immunodeficiency virus. Clin. Infect. Dis. 33:1586–1594. [CrossRef]
- 273/ Walker, D. H. 2000. Diagnosing human ehrlichioses: current status and recommendations. ASM News 66:287–291.
- 61/ Childs, J. E., J. W. Sumner, W. L. Nicholson, R. F. Massung, S. M. Standaert, and C. D. Paddock. 1999. Outcome of diagnostic tests using samples from patients with culture-proven human monocytic ehrlichiosis: implications for surveillance. J. Clin. Microbiol. 37:2997–3000. [CrossRef]
- 73/ Dawson, J. E., B. E. Anderson, D. B. Fishbein, J. L. Sanchez, C. S. Goldsmith, K. H. Wilson, and C. W. Duntley. 1991. Isolation and characterization of an Ehrlichia sp. from a patient diagnosed with human ehrlichiosis. J. Clin. Microbiol. 29:2741–2745. [CrossRef]
- 209/ Paddock, C. D., J. W. Sumner, G. M. Shore, D. C. Bartley, R. C. Elie, J. G. McQuade, C. R. Martin, C. S. Goldsmith, and J. E. Childs. 1997. Isolation and characterization of Ehrlichia chaffeensis strains from patients with fatal ehrlichiosis. J. Clin. Microbiol. 35:2496–2502. [CrossRef]
- 255/ Standaert, S. M., T. Yu, M. A. Scott, J. E. Childs, C. D. Paddock, W. L. Nicholson, J. Singleton, and M. J. Blaser. 2000. Primary isolation of Ehrlichia chaffeensis from patients with febrile illnesses: clinical and molecular characteristics. J. Infect. Dis. 181:1082–1088. [CrossRef]
- 262/ Tan, H. P., J. S. Dumler, W. R. Maley, A. S. Klein, J. F. Burdick, P. F. Fred, P. J. Thuluvath, and J. S. Markowitz. 2001. Human monocytic ehrlichiosis: an emerging pathogen in transplantation. Transplantation 71:1678–1680. [CrossRef]
- 99/ Everett, E. D., K. A. Evans, R. B. Henry, and G. McDonald. 1994. Human ehrlichiosis in adults after tick exposure: diagnosis using polymerase chain reaction. Ann. Intern. Med. 120:730–735. [CrossRef]
- 90/ Dumler, J. S., S. M. Chen, K. Asanovich, E. Trigiani, V. L. Popov, and D. H. Walker. 1995. Isolation and characterization of a new strain of Ehrlichia chaffeensis from a patient with nearly fatal monocytic ehrlichiosis. J. Clin. Microbiol. 33:1704–1711. [CrossRef]
- Gorenflot A, Moubri K, Precigout E, Carcy B, Schetters TP. Human babesiosis. Ann Trop Med Parasitol. 1998. [CrossRef]
- Boeva-Bangyozova, Violina; K.Eneva; Muhtarov, Marin; Dragomirova, Petya. HUMAN BABESIOSIS.JOUR, 2018/02/05.
- Amsden, J. R., Warmack, S., & Gubbins, P. O. (2005). Tick-Borne Bacterial, Rickettsial, Spirochetal, and Protozoal Infectious Diseases in the United States: A Comprehensive Review. Pharmacotherapy, 25(2), 191– 210. [CrossRef]
- Krause PJ, Telford SR, Ryan R, et al. Geographical and temporal distribution of babesial infection in Connecticut. J Clin Microbiol 1991;29:1–4. [CrossRef]
- Rochlin, Ilia, and Alvaro Toledo. “Emerging tick-borne pathogens of public health importance: a mini-review.” Journal of medical microbiology 69.6 (2020): 781. [CrossRef]
- Kumar, A.; O’Bryan, J.; Krause, P.J. The Global Emergence of Human Babesiosis. Pathogens 2021, 10, 1447. [Google Scholar] [CrossRef] [PubMed]
- Jia N, Zheng Y-C, Jiang J-F, Jiang R-R, Jiang B-G et al. Human babesiosis caused by a Babesia crassa Like pathogen: a case series. Clin Infect Dis 2018;67:1110–1119. [CrossRef]
- Homer MJ, Aguilar-Delfin IA, Telford SR, Krause PJ, Persing DH (2000) Babesiosis. Clin Microbiol Rev 13(3):451–469. [CrossRef]
- Laha, Ramgopal, M. Das, and A. Sen. “Morphology, epidemiology, and phylogeny of Babesia: An overview.” Tropical parasitology 5.2 (2015): 94. [CrossRef]
- Madison-Antenucci, Susan, et al. “Emerging tick-borne diseases.” Clinical microbiology reviews 33.2 (2020): 10-1128. [CrossRef]
- Boustani, Maria R., and Jeffrey A. Gelfand. “Babesiosis.” Clinical infectious diseases (1996): 611-614.
- Plesman, Joseph, and Andrew Spielman. “Babesia microti: infectivity of parasites from ticks for hamsters and white-footed mice.” Experimental parasitology 53.2 (1982): 242-248. [CrossRef]
- Herwaldt, Barbara L., et al. “Transfusion-associated babesiosis in the United States: a description of cases.” Annals of internal medicine 155.8 (2011): 509-519. [CrossRef]
- Gray, E. B., and B. L. Herwaldt. “Surveillance for babesiosis—United States, 2014.” Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, GA (2016).
- Kletsova, Ekaterina A., et al. “Babesiosis in Long Island: review of 62 cases focusing on treatment with azithromycin and atovaquone.” Annals of clinical microbiology and antimicrobials 16.1 (2017): 1-7. [CrossRef]
- White DJ, Talarico J, Chang HG, Birkhead GS, Heimberger T, Morse DL. 1998. Human babesiosis in New York State: review of 139 hospitalized cases and analysis of prognostic factors. Arch Intern Med 158:2149–2154. [CrossRef]
- Martinot, M.; Zadeh, M.M.; Hansmann, Y.; Grawey, I.; Christmann, D.; Aguillon, S.; Jouglin, M.; Chauvin, A.; De Briel, D. Babesiosis in immunocompetent patients, Europe. Emerg. Infect. Dis. 2011, 17, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.Y.; MacDonald, C.; Keenan, A.; Xu, K.; Bain, B.J.; Chiodini, P.L. Severe babesiosis due to Babesia divergens acquired in the United Kingdom. Am. J. Hematol. 2021, 96, 889–890. [Google Scholar] [CrossRef] [PubMed]
- Herwaldt, B.L.; Cacció, S.; Gherlinzoni, F.; Aspöck, H.; Slemenda, S.B.; Piccaluga, P.; Martinelli, G.; Edelhofer, R.; Hollenstein, U.; Poletti, G.; et al. Molecular characterization of a non-Babesia divergens organism causing zoonotic babesiosis in Europe. Emerg. Infect. Dis. 2003, 9, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Li, H.; Gao, X.; Bian, A.; Yan, H.; Kong, D.; Liu, X. Human babesiosisi n China: Asystematic review. Parasitol. Res. 2019, 118, 1103–1112. [CrossRef]
- Rollend, L., S.J. Bent, P.J. Krause, S. et al. Quantitative PCR for detection of Babesia microti in Ixodes scapularis ticks and in human blood. Vector Borne Zoonotic Dis., 2013, 13, 784-90. [CrossRef]
- Krause, P.J., S.R. Telford, R. Ryan et al. Diagnosis of babesiosis: evaluation of a serologic test for the detection of Babesia microti antibody. J. Infect. Dis., 1994, 169, 4, 923-6. [CrossRef]
- Krause, P.J.; McKay, K.; Thompson, C.A.; Sikand, V.K.; Lentz, R.; Lepore, T.; Closter, L.; Christianson, D.; Telford, S.R.; Persing, D.; et al. Disease-specific diagnosis of coinfecting tickborne zoonoses: Babesiosis, human granulocytic ehrlichiosis, and Lyme disease. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2002, 34, 1184–1191. [CrossRef]
- Hunfeld, K.P.; Lambert, A.; Kampen, H.; Albert, S.; Epe, C.; Brade, V.; Tenter, A.M. Seroprevalence of Babesia infections in humans exposed to ticks in midwestern Germany. J. Clin. Microbiol. 2002, 40, 2431–2436. [Google Scholar] [CrossRef] [PubMed]
- Wilson, Melisa, et al. “Development of droplet digital PCR for the detection of Babesia microti and Babesia duncani.” Experimental parasitology 149 (2015): 24-31. [CrossRef]
- Saifee NH, Krause PJ, Wu Y. 2016. Apheresis for babesiosis: therapeutic parasite reduction or removal of harmful toxins or both? J Clin Apher 31:454–458. [CrossRef]
- Krause PJ, Lepore T, Sikand VK, Gadbaw J, Jr, Burke G, Telford SR, III, Brassard P, Pearl D, Azlanzadeh J, Christianson D, McGrath D, Spielman A. 2000. Atovaquone and azithromycin for the treatment of babesiosis. N Engl J Med 343:1454–1458. [CrossRef]
- Brasseur, P.; Lecoublet, S.; Kapel, N.; Favennec, L.; Ballet, J.J. Quinine in the treatment of Babesia divergens infections in humans. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 1996, 15, 840–841. [CrossRef]
- Bläckberg, J.; Lazarevic, V.L.; Hunfeld, K.P.; Persson, K.E.M. Low-virulent Babesia venatorum infection masquerading as hemophagocytic syndrome. Ann. Hematol. 2018, 97, 731–733. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Global status of Anaplasma phagocytophilum infections in human population: A 50-year (1970–2020) meta-analysis.
Figure 1.
Global status of Anaplasma phagocytophilum infections in human population: A 50-year (1970–2020) meta-analysis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



