
Submitted:
12 February 2024
Posted:
13 February 2024
You are already at the latest version
Abstract
Traumatic nerve injuries are common lesions that affect several hundred thousand humans, as well as dogs and cats. The assessment of nerve regeneration trough animal models may provide information for translational research and future therapeutic options that can be applied mutually in veterinary and human medicine, in a one health perspective. This review offers a hands-on vision about the non-invasive and conservative approaches on peripheral nerve injury, focusing the role of neurorehabilitation in nerve repair and regeneration. The peripheral nerve injury may lead to hypersensitivity, allodynia and hyperalgesia, with the possibility of joint contractures, decreasing functionality and impairing the quality of life. The question remains regarding how to improve nerve repair with surgical possibilities, but also considering electrical stimulation modalities by modulating sensory feedback, upregulation BDNF, GFNF, TrKB and adenosine monophosphate, maintaining muscle mass and modulating fatigue. This could be improved by the positive synergetic effect of exercises and physical activity with locomotor training, and other physical modalities, such as low-level laser therapy and ultrasounds. In addition, the use of cell-based therapies is an innovative treatment tool in this field. These strategies may help avoiding situations of permanent monoplegic limbs that could lead to amputation.
Keywords:
PNI
; neurorehabilitation
; nerve repair
; electrical stimulation
; exercises
; locomotor training.
1. Introduction
Traumatic nerve injuries are common lesions that affects several hundred thousand humans every year in Europe and the United States of America [1,2]. The usual causes of the most severe cases include motor vehicle and sport accidents [1,3]. A similar reality is seen in veterinary medicine. Thus, in humans, as in dogs and cats, the brachial plexus injury (BPI) represents an example of peripheral nerve injury (PNI) that leads to devastating sensorimotor impairment of the affected limb in different possible degrees [1,4,5].
Clinical signs are the same in humans and in those species, and may include neuropathic pain, inability to bear weight and sensory deficits, which may be seen in, for example, near 57% of the cats that have radial and ulnar nerve injury [6]. Human and veterinary medicine can benefit mutually from research with this one health perspective [7,8].
In this context, assessment of nerve regeneration using animals models, provides information for translational research and future therapeutic option that can be applied in human medicine [7,9].
Regarding Sunderland´s system, based on three different injuries, further described by Seddon (1943) [10] in five categories, classification was according the severity of nerve damage. In the first-degree injury (neuropraxia) there is a slight contusion with focal demyelination and interruption of impulse propagation, but the axons and nerve sheaths remains intact, with possible recovery in 3 months [11,12] and segmental myelinization in about 3 to 6 weeks [11,13]. The second injury (axonotmesis or crush injuries) leads to axon damage and removal of Wallerian sheath with intact Schwann cells and endoneurium. In some cases, there is partially compressed endonerium but perineurium and epineurium are still intact, allowing the regrowth of crushed axons [10]. Lastly, neurotmesis is a complete transection injury that manifests with damaged endoneurium and perineurium, although an intact epineurium with complete anatomical disruption of the nerve [12]. Thus, axonotmesis has a better prognosis for recovery, with necessary time to improve muscle atrophy [14], which leads to worst prognosis and nearly 12-18 months for recovery [15,16].
Therefore, the purpose of this manuscript is to offer a hands-on vision about the non-invasive and conservative approaches for neurorehabilitation on PNI that could be implemented in a veterinary clinical setting. It also focuses on the role of neurorehabilitation in promoting strategies to promote nerve repair and regeneration, avoiding situations of permanent monoplegic affected limbs that could lead to amputation.
2. Diagnostic Assessment of Nerve Repair
The recovery of the nerve function after a lesion can be influenced by many factors, including the degree of nerve injury [14]. Functional recovery also depends on age, the time elapsed between injury and treatment, the distance from the injury site to the target muscle, the distance between the cell body and the site of axonal injury, and on axonal reinnervation itself [17-19].
Degree of nerve injury itself depends on the number and size of fascicles damaged within the nerve. Thus, depending on if it is a partial lesion or a complete one, the nerve is not going to have the same ability for recovery (i.e., neuropraxia, axonotmesis and neurotmesis) [20-24]. Also, the location, if it is a proximal or a distal nerve segment that is affected, and also the distance between the soma and lesion location, can influence the recovery capacity and speed [1,25]. So, there are several factors to be considered: type of injury, type of repair, timing of surgery; fascicles alignment; and patient comorbidities [1,25]. The recovery and functional outcome can be also limited by inflammation, scar tissue and misdirection of regenerating sensory and motor axons, compromising the mechanisms of repair (i.e., remyelination, collateral sprouting, axon regrowth [14,15,26]. All these are critical prognostic factors that may play an important role in regeneration [14,15,27,28].
Peripheral nerve regeneration is a complex process highlighted by Wallerian degeneration, axonal sprouting and remyelination [29]. The response to the injured nerve is influenced by damage degree and secondary degenerative changes, starting with a first degree based on a conduction blockage and mild degeneration. In the second degree, it occurs the calcium mediated process of Wallerian degeneration, distally to the injury site with few histological alterations at the injury site [11]. The third-degree (intra-fascicular injuries), manifests by an evident local reaction, with elastic endoneurium retraction of the severed nerve fiber end. Consecutively, an inflammatory response begins with local hemorrhage and edema, developing a secondary fibrous scar that could lead in neuroma and perineural scar tissue [30].
Regeneration is estimated to a rate of nearly about 1 mm/day [29,31] and different studies on nerve conduction were used [32-37], essentially for the analysis of nerve conduction velocity [32,38] and compound muscle activation potentials (CMAPs) [32,39-41].
Therefore, regenerating and repairing an injured nerve occurs in multiple levels, which include the nerve cell body, the injury site, the segment between the neural cell body and the injury site (proximal stump) and the segment between the injury site and the target organ [14,15].
Electrodiagnostic testing in a clinical setting of a physiotherapy and rehabilitation center is not realistically easy to be applied. However, it is possible to evaluate the nociceptive withdrawal reflex as an outcome measure [32,42,43] and also to document weight [35,44-47] and muscle mass by increase in fiber diameter [37,48-52]. Assessments of functional recovery may be possible by video-based motion analysis that make a precise evaluation of muscle function during locomotion [40,53].
Gait analysis may assess normal and abnormal gait patterns, featuring nerve damage and measuring numeric comparisons [54]. Experimental research advancements in peripheral nerve regeneration, such as computerized video analysis, enable to record footprints, walking patterns and bodyweight distribution, revealing the applicability of several parameters for locomotion evaluation [55]. Also, Schweizer et al. (2020) [56] introduced an alternative approach to assess functional outcomes in sciatic damage and repair after implementation of stem cells based on the swim test [57].
Furthermore, studies have shown monitoring of nerve regeneration by kinetic and kinematic evaluation of locomotion, as well as electrophysiologic and immunohistochemical outcomes [58]. Senger and colleagues (2020) [58] explored motor reinnervation assessment through kinetic, kinematic studies and skilled motor tasks, demonstrating that conditioning electrical stimulation (ES) increased Schwann cell proliferation in chronically injured nerves, enhancing axon regeneration and resulting in sensory and motor functional recovery.
Additionally, systemic (?) biomarkers measurements, such as the levels of neurotrophins and neurotrophic factors could be used as nerve repair parameters [32]. The expression of Brain-derived neurotrophic factor (BDNF) and its signal transduction receptor (TrkB) [32, 42, 59-63], as well as the nerve growth factor (NGF) and Growth associated protein 43 (GAP-43) levels, could be interesting parameters for this type of analysis [43,64].
In the clinical setting, functional recovery may be assessed by video-based motion analysis that precisely evaluates muscle function during locomotion [53,65], demonstrating an increase of BDNF through a neurotrophin dependent mechanism after one week of intensive voluntary exercise [59,63,66].
In a daily basis, peripheral nerve injuries, for example, a BPI, is commonly diagnosed by history, clinical signs and neurological examination [67,68]. Electrodiagnostic assessment may allow a precise identification of the nerve damaged due to the CMAPs that relate to the muscle force of the normal and reinnervated muscle [69], providing functional information and monitoring of the reinnervation process, which is a common practice in human medicine and could be translated for veterinary medicine [70,71], mostly in cats [69]. Although in some complex cases it is still insufficient to give the exact location of the injury. For example, in brachial plexus masses, magnetic resonance imaging could be helpful as a standard complementary exam [72]. In addition, these tests may require a specific timing that has to be considered [70,73], not immediately after injury, but two-six weeks after, when fibrillations in the denervated muscles are present [20,74,75].
3. The Problem of Neuropathic Pain
In human patients, traumatic PNI, such as BPI, is related to a higher incidence of neuropathic pain, when compared to other neuropathies (i.e., diabetic polyneuropathy, stroke, multiple sclerosis, refractory pain) [76-79].
Phantom limb pain is defined as a pain that originates from the region of the former limb that is no longer physically part of the body [80,81]. This phenomenon is interpreted, in human medicine, as a reorganization of the cortical structures related to the areas that suffered the avulsion or amputation [76] and can be present in nearly 54-85% of amputees and 39.3%, in cases of nerve avulsion [76,82,83].
In dogs, the phantom pain has been described to occur in about 60-80% of patients after amputation, within the first 2 years, and up to 10% may be present throughout life [84]. Thus, considering some animal models, to avoid self-mutilation it could be locally applied a substance with discouraging flavor [54,85].
The neuropathic pain can develop after nerve injury due to atypical connections or incorrect interpretation of peripheral axons with the spinal cord through enhanced integration of sensory afferents with the spinal cord circuitry and preservation of the substance P levels [17,86]. To Woolf (1983) [87], there are central mechanisms, after PNI, that may lead to hypersensitivity, allodynia and hyperalgesia in response to mechanical/thermal stimuli [87,88]. The tingling, pulsating and pricking sensations are evoked by toxic activation of large Aβ and Aδ fibers, associated to ectopic impulses in large fast conduction myelinated fibers [89,90]. The burning pain sensation may be due to intraneural stimulation of C nociceptive fibers [91]. Recent studies also suggest a role of the Schwann cells damage [92,93], besides the peripheral glia that could delay structural and functional changes following nerve injury [94].
Sodium channels are considered a main part of this phenomenon and increased number of heterotopic channels (Na+ 1.8, Na+ 1.7 and Na+ 1.3) may decrease the stimulation threshold, resulting in neuropathic pain. Therefore, there are different underlying mechanisms, such as: afferent nerves ectopic activity; peripheral sensitization; central sensitization; inaccurate inhibitory modulation and pathologic activation of microglia [88,95].
This could be one of the explanations why humans with BPI had reported an incidence of 30 to 80 % of neuropathic pain [6,76,97,98] with high presentation of refractory pain [6, 78, 96, 99,100]. In animal models, a study had showed that in BPI, nearly 30 % or more dogs develop mechanical and cold allodynia [6,100,101]. Also, the high variability of sensory cutaneous innervation pattern is consistent with the pattern of weakness that can be observed. If the regeneration rate is near 1 mm per day, both distal nerve and muscles undergo atrophy and are unable to sustain regeneration for functional recovery [17].
Immobilization promotes detrimental effects on the number of fibers of the muscles compared to the contralateral limb [32,48] and can delay recovery, most likely due to a reduction in muscle regeneration rate [32].
The nociceptive pain may be related to joint contractures and is common in BPI, mostly in the carpus due to a faster re-innervation of the flexor muscles and not the extensor muscles, resulting in knuckling posture [102,103]. To avoid this type of injury, when approaching the sciatic nerve, studies have reported the application of kinesiotherapy passive exercises and physical activity stimulation in rat models. Examples of these, were the implementation of a 45o inclined net to avoid long-term muscle inactivation [85,104].
In human medicine, the modality of focal muscle vibration, which is a technique that applies vibratory stimuli to the muscles or its tendons, using a mechanical device [105], may be an innovative non-invasive technique that intends to achieve neuroplasticity through enhancing changes in corticospinal excitability [105,106]. Among other treatments being studied mostly for diabetic neuropathy, are transcranial direct current stimulation (tDCS) and repetitive transcranial magnetic stimulation (rTMS), in association with physiotherapy [105]. In addition, electroacupuncture, a traditional therapy for pain [107], and transcutaneous electrical nerve stimulation (TENS), a neuromodulation modality that has been widely used for symptomatic pain relief by the potential inhibition of activity and excitability of central nociceptive transmission neurons, can also be applied [108].
TENS is commonly used for dogs and cats in a clinical setting, intending to interfere with sensory perception and create an analgesic effect [109]. Also, in human patients is a common therapy for a wide variation of pain conditions [70,110].
The authors use a standard protocol to the relief neuropathic and nociceptive pain., the interferential TENS. This is achieved with two different channels and four rubber and carbon electrodes (7x5 cm) (BTL - 4820 Smart ®, Hertfordshire, GB), placed crossing each other at 90o angle at the pain region or near the affected nerve pathway after the hair is clipped and gel applied. The programmed current is biphasic, symmetric and continuous, performed once or twice a day, 3-5 days a week, and sessions decreased according to pain evaluation. Current parameters are: channel 1 (acute pain) with 80-150 Hz, until a maximum of 2.5 mA, pulse duration until 50 μs and time of treatment 10 min; channel 2 (chronic pain) with 10 Hz, until a maximum of 2 mA, pulse duration between 100-400 μs and time of treatment 10 min (Figure 1).
4. How to Improve PNI repair?
Several non-surgical approaches, such as pharmacological, electrical, laser therapy, and cell-based therapies, have been developed to promote remyelination and improve functional recovery in PNI [14,111-114]. For human patients, the most common treatment implies surgical resolution, and, in cases of a short gap (<1cm), neurorrhaphy is frequently used with end-to-end sutures of the proximal and distal ends [7, 23,115,116].
4.1. Surgical Approach
In regard to the surgical approach, for short gaps (<1cm), the neurorrhaphy technique is used, however it would cause excessive tension for a larger gap [7,23,115,116]. Thus, for medium and larger gaps, the most common technique is nerve grafting nerve reconstruction [7,117,118]. For gaps larger than 3 cm, the autograft is the current gold standard with an immunogenically inert scaffold that stimulates adhesion molecules and neurotrophic factors [7,23].
In human medicine, nerve transfers have been used as a reliable surgical option, preserving muscle and sensory innervation [119,120]. Also, it was described that end-to-end nerve transfers for radial nerve palsies, traumatic ulnar nerve injury and ulnar nerve compressive neuropathy [121,122]. On the other hand, there is a case series describing vein wrapping after nerve repair [123].
Commercially nerve wraps based on collagen are available, such as NeuraWrap Integralife Sciences by bovine-derived type I collagen, already used for nerve repair of a rat sciatic never [124,125]. The AxoGuard nerve wrap (Axogen) by porcine small intestine submucosa was also already used [126,127]. The Hyaluronic acid-carboxy methylcellulose film (HA-CMC) and human amniotic membrane wrap are still in research [128-130].
Other alternative approaches are based on tissue engineering with the use of scaffolds and mesenchymal stem cells and their potential, such as strength, biodegradability, biocompatibility, porosity, cell adhesion, differentiation, proliferation and growth [131].
4.2. Electrostimulation Modality
In the last years, ES has been shown to have potential enhancing regeneration in different types of nerve injuries, including crush lesions [17,132,133], transection [134,135] and long-distance injuries [17,136]. This modality has been helping recovery in the context of one health, due to its therapeutic mechanism to reduce muscle atrophy and promote active muscle reinnervation, increasing the expression of structural protective proteins and neurotrophic factors. Furthermore, it may possibly modulate sensory feedback and reduce neuralgia by inhibiting descending pathways [137].
Previous studies have suggested that the nerve effects of ES could be achieved by upregulating the expression of BDNF [60,138,139], glial cell-like derived neurotrophic factor (GDNF) [137,140], TrKB) [141,142] and adenosine monophosphate (CAMP) [143].
The positive effects of ES in nerve repair were reported in both animals [32,33,40,46,61,135] and humans [32]. This efficient modality could maintain muscle weight, the twitch characteristics, modulating fatigue and mechanosensitivity [32,33,46].
Furthermore, functional electrical stimulation (FES) is an ES technique that uses sequences of short bursts of electrical pulses to stimulate nerves neat the motor plate region or through peripheral afferent nerves, activating peripheral spinal reflex. FES uses a low intensity current sufficient enough to trigger an action potential that induces muscle contraction. Low-frequency FES is used to promote nerve regeneration, however the methods and frequencies applied diverge and need to be standardized, due to increase of nerve damage with high-frequency currents. Additionally, the use of biocompatible gels that provide skin maintenance and current uniform distribution on the electrodes, makes this a better non-invasive stimulation approach with conventional surface electrodes suitable for innervating large muscles close to the skin [137,144].
FES has shown to increase intraneuronal CAMP, improving regenerative ability via increased expression of the neurotrophins and cytoskeletal proteins [17]. Also, this modality may mimic physiological wave of Ca2+ influx that generates a retrograde signal, leading to activation of cell autonomous mechanisms and promoting regeneration. BDNF, NGF and neurotrophins 4/5 may play an essential role in neuronal regeneration and maintenance [17,145-147]. These beneficial effects are associated with up-regulation of BDNF and its TrkB receptors in motoneurons [60,141].
Studies in both humans and animals, have demonstrated that FES promotes preferential re-innervation of motor and sensory neurons, leading to a faster recovery [14,60,148], helping in the remyelination process [14,39], and avoiding nerve injury-induced muscle atrophy [14, 149, 150].
Most studies that are performed in animals’ resort to a low-frequency ES, usually 20 Hz [32,39,53,151,152], or 10 Hz [40,45], although a variable range of values from 20 to 200 Hz [153], or 4 to 75 Hz [33,46], has been documented.
The correct selection of frequency is mandatory, because as mentioned before, higher frequencies can deteriorate and aggravate atrophic muscle events [7,115,154]. Thus, to determine standard parameters, such as duration, it is important to consider extent damage variations of different injuries and possible side effects on the healthy tissues [7,115].
In human medicine, this modality can be also associated with surgical techniques [115,154]. For improving plantar spasticity, it was described a 5 day/week protocol [155] for 3-4 weeks, although longer treatments of 6-12 weeks could be necessary with pulse frequencies of 30-50 Hz and pulse duration until 300 microseconds [155, 156-160]. Treatment time has to consider potential fatigue, but usually ranges from 20-30 min per session [157-159].
Gunter and collaborators (2019) [161] stated that ES didn’t lead to neural damage when continuous stimulation with 20 Hz was applied for 16 h. Also, Agnew and McCreery (1990) [162] had several works demonstrating that ES was safe for application in the treatment of cats with PNI [163]. Furthermore, it was shown that a 20 Hz frequency was considered safe but increasing to 50-100 Hz, even pulsed current and partial fiber recruitment, could lead to neural damage.
Supporting this statement, Waters et al. (1985)[164], applied ES during 12 years in human patients with peroneal nerve lesion, using a frequency of 33 Hz, concluding that there was evidence of long-term safety with frequencies near 30 Hz.
Duty cycle describes the percentage of “on” and “off” stimulation time and it was shown that 50% of efficient stimulation time, with 50 Hz, could stimulate the peroneal nerve of a cat for a period of 16 h, with considerably less damage when compared to 100% stimulation time [162,165].
Thus, multiple animal studies defend the beneficial effects of ES with low frequencies and electrodiagnostic tests revealing highly increase of CMAP scores after ES [166-170].
Actually, long-term stimulators have been surgically implanted in human patients, targeting nerve and securing electrode array [171]. These invasive devices penetrate the nerve to facilitate targeted activation of nerve fascicles [161,171].
Finally, ES may influence the concentration of circulating cytokines [172,173], modulation neuroinflammatory response [174], through the macrophage and microglia action, which could be related to temporary decrease in spasticity up to 40 min after treatments [175].
Additionally, ES could help in the four phases of PNI: oxidative stress stage (0-12h); inflammation stage (12h-3 day); atrophy stage (3-14 days) and atrophic fibrosis stage (14-28 days). The effects of treatment on peripheral neurogenesis vary according to the position of stimulation [176].
The author uses a standard protocol to the PNI that includes: until 50 Hz; duty cycle of 1:5; 10-16 mA; 10 min; and a trapezoid pulsated current (BTL - 4820 Smart ®, Hertfordshire, GB).
Figure 2.
Functional electrical stimulation on the flexor muscle group of the hindlimb applied on a dog (A) and on a cat (B).
Figure 2.
Functional electrical stimulation on the flexor muscle group of the hindlimb applied on a dog (A) and on a cat (B).

4.3. Exercises and Physical Activity
Even if there is not a clear relation between rehabilitation exercises and axon regeneration, there are specific physical exercises that avoid secondary lesions, such as disuse muscle atrophy, contracture, edema, stasis and pain. There is no developed standard treatment to be applied, the used ones differing mostly in intensity duration and time [32].
However, exercises may promote angiogenesis, neurogenesis and neurotrophins expression, increasing nerve vascular integrity, decreasing apoptosis and modulating inflammation. Experimental findings, mostly in rodents, have shown the impact of exercise on synaptogenesis, myelination, neural recovery, growth development and muscle reinnervation. Examples are the resorting to treadmill training [32,36,41,177], high speed exercise running [178,179], swimming [35,180], voluntary locomotor exercises of endurance and resistance [66,181], isometric exercises [182], sensory retraining [183], manual stimulation [184], passive range of motion exercises and joint mobilizations [37,62].
The mechanisms of action related to the influence of physical exercises in nerve repair are different and based on research [32], resulting in the evidences that this could be due to neurotrophin increment, such as BDNF and Glial maturation factor (GMF), resulting in survival and regeneration of damaged axons [61,185].
Thus, effects of these exercises differ according to intensity and volume of training, as well as the type of nerve injury. For example, running in the land treadmill for 10 weeks could lead to a faster nerve repair in rats [33], probably related to reduce level of myelin associated glycoprotein (MAG) on axonal growth inhibitor [9]. The MAG and complex gangliosides are related to long-term axon stability in both central nervous system and peripheral nervous system [186], as a minor component of periaxonal myelin [187], allowing axoncytoarchitecture and regulating axon outgrowth [186], which is particularly important in human patients with peripheral nervous system immune diseases, such as Guillain-Barre Syndrome [188].
Axon regeneration development by treadmill training has been previously demonstrated and was shown in rats [9,34,189] and mouses [9,36,190] with moderated daily training for 2 weeks [9].
The efficacy of exercise seems to start from the 4th regeneration week after nerve injury and not before that [32]. Therefore, overtraining and high workload could interfere with peripheral nerve recovery, mostly in the initial stages with detrimental effects [60], that could imply a physiological stimulus that interferes with anatomical and biochemical recovery [60,152]. However, sensory rehabilitation with intensive protocols could promote sensory perception [32, 183].
Also, immobilization seems to have detrimental consequences on the count of number of neural fibers, delaying repair because of reduction in regeneration rate and not by the influence on nerve regeneration [32].
As expected, GDNF, BDNF and Insulin-Like Growth Factor-1 (IGF-1) protein levels are increased in muscles that are exercised and may improve blood flow, activation of Schwann cells [191], leading to neovascularization, angiogenesis and enhanced metabolism rate [192]. In addition, it seems to have impact in decreasing neuropathic pain and allodynia, but with poor positive effects described in humans [192].
Locomotor training could be one of the best options to help in PNI, starting with moderate exercise that increases in intensity and volume [7]. The BDNF, which is highly related to locomotor training, it is also potentiated in association with electrical activity [60], promoting remyelination. The increase in neurotrophic factors by locomotor training may be limited by the distance between the end axonal tops estimated by 5 mm [6].
Spontaneous peripheral nerve recovery is commonly inadequate and depends on the type of injury and damage extension [1]. A few studies in animals where moderate exercises and rehabilitation methods of motor and sensory functions were used, reveal that such an approach could improve coordination and sensory-motor tasks [41], and the locomotor training could be an example of that in dogs, cats and humans [193] (Figure 3).
4.4. Combination of Electrical Stimulation and Locomotor Training
There is evidence in the current literature that brief low-frequency electrical stimulation effectively promotes axon regeneration, maximizing functional recovery in PNI, namely in facial nerve stimulation with 20 Hz for 30 min/day after a crush injury as well as after transection of the sciatic nerve with silicone tube and collagen gel surgical repair [194].
Thompson and collaborators (2014) [195] showed that moderate treadmill training and brief ES (with 20 Hz, for 1h, in the sciatic nerve pathway) were applied in different groups of mice, for 5 days/week, revealing enhancement of axon repair. The same efficacy was proved in human patients submitted to carpal tunnel release due to medial nerve injury by constriction of the wrist ligaments (94). Thus, these studies could be translated between human and veterinary medicine to improve recovery following injuries [148].
One the other hand, Elzinga et al. (2015) [196] showed that the same type of ES stimulated axon growth and muscle reinnervation after nerve surgery in rats and humans, improving regeneration in delayed nerve repair. In addition, activity-based exercises, such as land treadmill combined with electrical stimulation, after PNI, increases the potential of axon regeneration [60,134,195]. The same was reported with 20 Hz for 1 h in rats, mice [60,196] and human patients [197,198].
Prior investigations, had addressed the role of ES for the complex pathophysiology of neuropathic pain, particularly in the inhibition of synaptic stripping and the excessive excitability of the dorsal roost ganglion, reducing pain and improving neurological function [176]. This modality could be safely used in conjunction with other treatments, such as pharmacological, cell-based therapies and rehabilitation techniques [17,176]. Every day exercise with bipolar ES for 20 min significantly improved nerve regeneration and sensorimotor recovery, assessed by gait analysis, coordination tests and electrophysiological outcomes. Nowadays, there are human medicine clinical trials being conducted based on the effect of conditioning ES as a preoperative treatment prior to nerve decompression and reconstruction [199].
An early moderated and progressive training with electrical stimulation and locomotor training could help reducing neuropathic pain [32,42], preventing neurotrophin-mediated hyperexcitability [32,200] and reducing facilitation of the monosynaptic H-reflex [32,36]. Additionally, this combination could be critical to enhance chances of recovering mobility, avoiding secondary muscle or joint contractures [6].
To Menchetti and colleagues (2020) [6], 25% of cats showed improved neurological condition with the support of physical therapies in time scenario, which is considered fundamental. Thus, FES and treadmill exercise has been shown to have positive synergetic effects on nerve regeneration and muscle reinnervation [14].
The exact mechanism of ES and locomotor training to be implemented is still poorly established, however CAMP and BDNF are reported to play a key role. ES could cause an increased influx of Ca2+ into the neurons followed by an increase in intracellular CAMP levels [14], and could be used as a rehabilitation intervention to stimulate and accelerate the process of nerve regeneration.
4.5. Other Rehabilitation Modalities
Low-level laser therapy (LLLT) is another modality that could be applied in a clinical setting after PNI [14]. This induces upregulation of nitric monoxide that is related to necrosis and apoptosis [201]. The nitric monoxide and other free radicals that result from lipidic peroxidation of the central and peripheral nervous systems, may have an important role in neuropathic pain [202] and might be inhibited by laser therapy.
LLLT could be combined with TENS, which was implemented in radial nerve injury of human patients, translating in significant effects compared with a control group, maintaining this improvement for 1-3 years [137]. Therefore, laser therapy was commonly applied in PNI every day, during 5 consecutive days, followed by application once or twice a week, with positive effects [14].
These studies were based on the possible ability to promote regeneration and functional recovery of injured peripheral nerves, accelerating myelination, increasing axonal diameter, stimulation Schwann cells proliferation and improving motor nerve function [14,203-205]. The mechanisms behind this could be associated to DNA and RNA synthesis with consequent protein synthesis alongside cell proliferation, modifying nerve cell action potentials. The tissue biostimulation effects with possible increase in axonal diameter are important, although many issues arise due to the lack of standardized parameters [7].
As for the author’s suggestion, the use of a 980 nm laser is essential, with a power of 10-19mW/cm2 at the level of the PNI, for 3 to 5 days in a row, followed by 3 times per week, then two times, usually until 8 weeks of treatment (Figure 4).
The combination of laser therapy with ultrasounds is also a possibility, which has mechanical and thermal properties, stimulating blood circulation, release of BDNF, increase cell metabolism and tissue nutrition [7, 154]. Some authors considered ultrasound to be more effective than LLLT in improving strength, pain and sensory deficits. Although, according to Page et al. (2013) [206], there was no evidence of better results in using ultrasounds with the implementation of a splint, when compared to any other surgical procedure.
For the authors, ultrasounds are usually performed with intensity ranging from 1 to 2.5 w/cm2, in a pulsed mode, with a duty cycle of 20% for 10 min. Recommended speed of the movement with the head sound over the skin should be slower but never static and are mostly performed with longitudinal or circular patterns.
On the other hand, the use of LLLT plus splints showed to help in carpal contractures in human medicine [207].
4.6. Cell-Based Therapies and PNI
Cell-based therapies are the most innovative treatment approaches in the PNI field. This can help damaged tissues by targeting differentiation processes that influence cell morphology, metabolic activity, growth factors secretion and signal response [1,29].
Stem cells can help in nerve regeneration by promoting a neuroprotective microenvironment that modulates degeneration and apoptosis, supporting neurogenesis, axonal growth and remyelination [208] (Figure 5). Increased cell metabolism could be also related to increase in neurotrophin 3 (NT-3), neurotrophin 1 (NT-1), neurotrophin 4 (NT-4), ciliary-derived neurotrophic factor (CDNF), BDNF, NGF and GDNF 4 [208-210].
In addition, stem cells, such as mesenchymal stem cells (MSCs) may increase neovascularization and promote secretion of tissue inhibitor of metalloproteinase – 8 (VEGF), angiopoietin 1 and transformation of growth factor B and IL-8 [208,210].
5. Conclusions
Recovery and repair of nerve sensory-motor functions depends on several different factors. However, when regeneration happens it still depends on a rate of around 1 mm/day, leading to muscle atrophy, joint contractures, persistent lameness, weakness that enables weight support and possible neuropathic pain. Thus, non-invasive neurorehabilitation modalities could be prescribed in PNI, considering the synergetic power of FES and locomotor training as one of the best therapeutic approaches to obtain faster recovery of sensory-motor functions. It also plays an essential part in avoiding neurogenic atrophy and secondary muscle or joint contractures, which will support reinnervation.
Essentially, these protocols associated with regenerative medicine, including stem cells transplantation (as MSCs), are innovative therapeutic tools in the field of nerve repair, that may help to revert cellular changes, reducing neural apoptosis and supporting neurogenesis (Figure 6). Further studies with similar protocols for PNI should be conducted based on a one health perspective.
Author Contributions
Conceptualization Â.M.; methodology D.G.; validation Â.M. and A.F.; formal analysis, Â.M. and A.F.; investigation D.G., A.C., C.C., Ó.G., A.A. B.L., A.F., R.A., A.C.O. writing—original draft preparation, D.G., A.C. and R.A.; writing—review and editing Â.M, A.V., A.F., A.S.V. and A.C.M.; supervision Â.M., A.C.M. and A.S.V.; project administration Â.M. All authors have read and agreed to the published version of the manuscript.
Funding
The work was supported through the project UIDB/00211/2020 funded by FCT/MCTES through national funds, through the projects 2022.04501.PTDC (Olfabionerve - Olfactory Mucosa Mesenchymal Stem Cells and Biomaterials Promoting Peripheral Nerve Regeneration), Prémios Santa Casa Neurociências – Prize Melo e Castro for Spinal Cord Injury Research (MC-04/17; MC-18-2021), and through the PhD scholarship from FCT 2021.05265.BD (Bruna Lopes).
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgements
The author Rui D. Alvites acknowledges the Centro de Estudos de Ciência Animal (CECA), Instituto de Ciências, Tecnologias e Agroambiente (ICETA), Porto University (UP), and Fundação para a Ciência e Tecnologia (FCT) for the funding and availability of all technical, structural, and human resources necessary for the development of this work.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lavorato, A.; Raimondo, S.; Boido, M.; Muratori, L.; Durante, G.; Cofano, F.; Vincitorio, F.; Petrone, S.; Titolo, P. Tartara, F., et al. Mesenchymal stem cell treatment perspectives in peripheral nerve regeneration: systematic review. Int J Mol Sci. 2021, 22, 572. [Google Scholar] [CrossRef]
- Tremp, M.; Zu Schwabedissen, M.M.; Kappos, E.A.; Engels, P.E.; Fischmann, A.; Scherberich, A.; Schaefer, D.J.; Kalbermatten, D.F. The Regeneration Potential after Human and Autologous Stem Cell Transplantation in a Rat Sciatic Nerve Injury Model can be Monitored by MRI. Cell Transplant. 2015, 24, 203–211. [Google Scholar] [CrossRef]
- Matthes, S.M.; Reimers, K.; Janssen, I.; Liebsch, C.; Kocsis, J.D.; Vogt, P.M.; Radtke, C. Intravenous Transplantation of Mesenchymal Stromal Cells to Enhance Peripheral Nerve Regeneration. BioMed Res. Int. 2013, 2013, 1–6. [Google Scholar] [CrossRef]
- Yousefi, F.; Arab, F.L.; Nikkhah, K.; Amiri, H.; Mahmoudi, M. Novel approaches using mesenchymal stem cells for curing peripheral nerve injuries. Life Sci. 2019, 221, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Moattari, M.; Kouchesfehani, H.M.; Kaka, G.; Sadraie, S.H.; Naghdi, M. Evaluation of nerve growth factor (NGF) treated mesenchymal stem cells for recovery in neurotmesis model of peripheral nerve injury. J. Cranio-Maxillofac. Surg. 2018, 46, 898–904. [Google Scholar] [CrossRef]
- Menchetti, M.; Gandini, G.; Bravaccini, B.; Dondi, M.; Gagliardo, T.; Bianchi, E. Clinical and electrodiagnostic findings and quality of life of dogs and cats with brachial plexus injury. Vet Sci. 2020, 7, 101. [Google Scholar] [CrossRef] [PubMed]
- Lopes, B.; Sousa, P.; Alvites, R.; Branquinho, M.; Sousa, A.C.; Mendonça, C.; Atayde, L.M.; Luís, A.L.; Varejão, A.S.P.; Maurício, A.C. Peripheral Nerve Injury Treatments and Advances: One Health Perspective. Int. J. Mol. Sci. 2022, 23, 918. [Google Scholar] [CrossRef] [PubMed]
- Ribitsch, I.; Baptista, P.M.; Lange-Consiglio, A.; Melotti, L.; Patruno, M.; Jenner, F.; Schnabl-Feichter, E.; Dutton, L.C.; Connolly, D.J.; van Steenbeek, F.G.; et al. Large Animal Models in Regenerative Medicine and Tissue Engineering: To Do or Not to Do. Front. Bioeng. Biotechnol. 2020, 8, 972. [Google Scholar] [CrossRef]
- Maugeri, G.; D’Agata, V.; Trovato, B.; Roggio, F.; Castorina, A.; Vecchio, M.; Di Rosa, M.; Musumeci, G. The role of exercise on peripheral nerve regeneration: From animal model to clinical application. Heliyon. 2021, 7, e08281. [Google Scholar] [CrossRef]
- Seddon, H.J. Three types of nerve injury. Brain. 1943, 66, 237. [Google Scholar] [CrossRef]
- Khaled, M.M.; Ibrahium, A.M.; Abdelgalil, A.I.; El-Saied, M.A.; El-Bably, S.H. Regenerative strategies in treatment of peripheral nerve injuries in different animal models. Tissue Eng Regen Med. 2023, 20, 839–877. [Google Scholar] [CrossRef]
- Zack-Williams, S.D.; Butler, P.E.; Kalaskar, D.M. Current progress in use of adipose derived stem cells in peripheral nerve regeneration. World J Stem Cells. 2015, 7, 51. [Google Scholar] [CrossRef]
- Al-Magsoosi, H.H.; Al-Bayati, H.S.; Al-Timmemi, H.A. immuno-hematological response to radial nerve injury and human umbilical cord-mesenchymal stem cells (Huc-MSCS) therapy in dogs. IRAQ Biochem Cell Arch. 2020, 20, 6447–6456. [Google Scholar]
- Modrak, M.; Talukder, M.A.; Gurgenashvili, K.; Noble, M.; Elfar, J.C. Peripheral nerve injury and myelination: potential therapeutic strategies. J Neurosci Res. 2020, 98, 780–795. [Google Scholar] [CrossRef]
- Campbell, W.W. Evaluation and management of peripheral nerve injury. Clin Neurophysiol 2008, 119, 1951–1965. [Google Scholar] [CrossRef] [PubMed]
- Missios, S.; Bekelis, K.; Spinner, R.J. Traumatic peripheral nerve injuries in children: epidemiology and socioeconomics. J Neurosurg Pediatr. 2014, 14, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Javeed, S.; Faraji, A.H.; Dy, C.; Ray, W.Z.; MacEwan, M.R. Application of electrical stimulation for peripheral nerve regeneration: Stimulation parameters and future horizons. Interdiscip. Neurosurg.: Adv. Tech. Case Manag. 2021, 24, 101117. [Google Scholar] [CrossRef]
- Hoke, A.; Brushart, T. Introduction to special issue: challenges and opportunities for regeneration in the peripheral nervous system, Exp. Neurol. 2010, 223, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Pestronk, A.; Drachman, D.B.; Griffin, J.W. Effects of aging on nerve sprouting and regeneration. Exp. Neurol. 1980, 70, 65–82. [Google Scholar] [CrossRef] [PubMed]
- Grinsell, D.; Keating, C.P. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. Biomed Res Int. 2014, 698256. [Google Scholar] [CrossRef]
- Smith, J.W. Microsurgery of peripheral nerves. Plast Rec Surg. 1964, 33, 317–329. [Google Scholar] [CrossRef]
- Menorca, R.M.; Fussell, T.S.; Elfar, J. C. Peripheral nerve trauma: mechanisms of injury and recovery. Hand Clin. 2013, 29, 317–330. [Google Scholar] [CrossRef]
- Hussain, G.; Wang, J.; Rasul, A.; Anwar, H.; Qasim, M.; Zafar, S.; Aziz, N.; Razzaq, A.; Hussain, R.; Aguilar, J.; et al. Current status of therapeutic approaches against peripheral nerve injuries: a detailed story from injury to recovery. Intern J Bio Sci. 2020, 16, 116–134. [Google Scholar] [CrossRef] [PubMed]
- Houschyar, K.S.; Momeni, A.; Pyles, M.N.; Cha, J.Y.; Maan, Z.N.; Duscher, D.; Jew, O.S.; Siemers, F.; Schoonhoven, J. The role of current techniques and concepts in peripheral nerve repair. Plastic Surg Intern. 2016, 4175293. [Google Scholar] [CrossRef] [PubMed]
- De Albornoz, P.M.; Delgado, P.J.; Forriol, F.; Maffulli, N. Non-surgical therapies for peripheral nerve injury. Br. Med. Bull. 2011, 100, 73–100. [Google Scholar] [CrossRef]
- Noble J, Munro CA, Prasad VS, Midha R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma. 1998, 45, 116–122. [CrossRef]
- Sunderland, S. The anatomy and physiology of nerve injury. Muscle Nerve. 1990, 13, 771–784. [Google Scholar] [CrossRef]
- Post. R.; de Boer, K.S.; Malessy, M.J. Outcome following nerve repair of high isolated clean sharp injuries of the ulnar nerve. PLoS One 2012, 7, e47928.
- Jiang, L.; Jones, S.; Jia, X. Stem cell transplantation for peripheral nerve regeneration: current options and opportunities. Int J Mol Sci. 2017, 18, 94. [Google Scholar] [CrossRef] [PubMed]
- Burnett, M.G.; Zager, E.L. Pathophysiology of peripheral nerve injury: a brief review. Neurosurg Focus. 2004, 16, E1. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006, 126, 663–676. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Pavone, V.; Testa, G.; Pesce, I.; Scaturro, D.; Musumeci, G.; Mauro, G.; Vecchio, M. The role of physical exercise and rehabilitative implication in the process of nerve repair in peripheral neuropathies: a systematic review. Diagnostics (Basel). 2023, 13, 364. [Google Scholar] [CrossRef]
- Marqueste, T.; Alliez, J.-R.; Alluin, O.; Jammes, Y.; Decherchi, P. Neuromuscular rehabilitation by treadmill running or electrical stimulation after peripheral nerve injury and repair. J. Appl. Physiol. 2004, 96, 1988–1995. [Google Scholar] [CrossRef]
- Asensio-Pinilla, E.; Udina, E.; Jaramillo, J.; Navarro, X. Electrical stimulation combined with exercise increase axonal regeneration after peripheral nerve injury. Exp. Neurol. 2009, 219, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-F.; Yang, T.-Y.; Chen, Y.-H.; Yao, C.-H.; Way, T.-D.; Chen, Y.-S. Effects of swimming exercise on nerve regeneration in a rat sciatic nerve transection model. Biomed. Pharmacother. 2017, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Boeltz, T.; Ireland, M.; Mathis, K.; Nicolini, J.; Poplavski, K.; Rose, S.J.; Wilson, E.; English, A.W. Effects of treadmill training on functional recovery following peripheral nerve injury in rats. J. Neurophysiol. 2013, 109, 2645–2657. [Google Scholar] [CrossRef]
- Kim, H.K.W.; Kerr, R.G.; Turley, C.B.; Evans, P.J.; Jay, V.; Salter, R.B. The Effects of Postoperative Continuous Passive Motion on Peripheral Nerve Repair and Regeneration. J. Hand Surg. 1998, 23, 594–597. [Google Scholar] [CrossRef] [PubMed]
- van Meeteren, N.L.; Brakkee, J.H.; Hamers, F.P.; Helders, P.J.; Gispen, W.H. Exercise training improves functional recovery and motor nerve conduction velocity after sciatic nerve crush lesion in the rat. Arch. Phys. Med. Rehabilitation. 1997, 78, 70–77. [Google Scholar] [CrossRef]
- Huang, J.; Lu, L.; Zhang, J.; Hu, X.; Zhang, Y.; Liang, W.; Wu, S.; Luo, Z. Electrical Stimulation to Conductive Scaffold Promotes Axonal Regeneration and Remyelination in a Rat Model of Large Nerve Defect. PLoS ONE. 2012, 7, e39526. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.-H.; Chen, J.-J.J.; Hsu, Y.-M.; Bau, D.-T.; Yao, C.-H.; Chen, Y.-S. High-Frequency Electrical Stimulation Can Be a Comple- mentary Therapy to Promote Nerve Regeneration in Diabetic Rats. PLoS ONE. 2013, 8, e79078. [Google Scholar] [CrossRef]
- Udina, E.; Puigdemasa, A.; Navarro, X. Passive and active exercise improve regeneration and muscle reinnervation after peripheral nerve injury in the rat. Muscle Nerve. 2011, 43, 500–509. [Google Scholar] [CrossRef]
- Cobianchi, S.; Marinelli, S.; Florenzano, F.; Pavone, F.; Luvisetto, S. Short- but not long-lasting treadmill running reduces allodynia and improves functional recovery after peripheral nerve injury. Neuroscience. 2010, 168, 273–287. [Google Scholar] [CrossRef]
- Cobianchi, S.; de Cruz, J.; Navarro, X. Assessment of sensory thresholds and nociceptive fiber growth after sciatic nerve injury reveals the differential contribution of collateral reinnervation and nerve regeneration to neuropathic pain. Exp. Neurol. 2014, 255, 1–11. [Google Scholar] [CrossRef]
- Herbison, G.J.; Jaweed, M.M.; Ditunno, J.F. Electrical stimulation of sciatic nerve of rats after partial denervation of soleus muscle. Arch. Phys. Med. Rehabilitation. 1986, 67, 79–83. [Google Scholar] [CrossRef]
- Jaweed, M.; Herbison, G.J.; Ditunno, J.F. Direct electrical stimulation of rat soleus during denervation-reinnervation. Exp. Neurol. 1982, 75, 589–599. [Google Scholar] [CrossRef]
- Marqueste, T.; Decherchi, P.; Desplanches, D.; Favier, R.; Grelot, L.; Jammes, Y. Chronic electrostimulation after nerve repair by self-anastomosis: Effects on the size, the mechanical, histochemical and biochemical muscle properties. Acta Neuropathol. 2006, 111, 589–600. [Google Scholar] [CrossRef]
- Michel, R.N.; Gardiner, P.F. Influence of overload on recovery of rat plantaris from partial denervation. J. Appl. Physiol. 1989, 66, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Eisen, A.A.; Carpenter, S.; Karpati, G.; Bellavance, A. The effect of muscle hyper- and hypoactivity upon fibre diameters of intact and regenerating nerves. J. Neurol. Sci. 1973, 20, 457–469. [Google Scholar] [CrossRef] [PubMed]
- Herbison, G.J.; Jaweed, M.; Ditunno, J.F.; Scott, C.M. Effect of overwork during reinnervation of rat muscle. Exp. Neurol. 1973, 41, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Herbison, G.J.; Jaweed, M.M.; Ditunno, J.F. Effect of swimming on reinnervation of rat skeletal muscle. J. Neurol. Neurosurg. Psychiatry. 1974, 37, 1247–1251. [Google Scholar] [CrossRef] [PubMed]
- Sobral, L.L.; Oliviera, L.S.; Takeda, S.Y.M.; Somazz, M.C.; Montebelo, M.I.L.; Teodori, R.M. Immediate versus later exercises for rat sciatic nerve regeneration after axonotmesis: Histomorphometric and functional analyses. Rev. Bras. Fisioter. 2008, 12, 311–316. [Google Scholar] [CrossRef]
- Teodori, R.M.; Betini, J.; de Oliveira, L.S.; Sobral, L.L.; Takeda, S.Y.M.; Montebelo, M.I.D.L. Swimming Exercise in the Acute or Late Phase after Sciatic Nerve Crush Accelerates Nerve Regeneration. Neural Plast. 2011, 783901. [Google Scholar] [CrossRef]
- Skouras, E.; Merkel, D.; Grosheva, M.; Angelova, S.K.; Schiffer, G.; Thelen, U.; Kaidoglou, K.; Sinis, N.; Igelmund, P.; Dunlop, S.A.; et al. Manual stimulation, but not acute electrical stimulation prior to reconstructive surgery, improves functional recovery after facial nerve injury in rats. Restor. Neurol. Neurosci. 2009, 27, 237–251. [Google Scholar] [CrossRef]
- Costa, L.M.; Simões, M.J.; Maurício, A.C.; Varejão, A.S. Methods and protocols in peripheral nerve regeneration experimental research: part IV - Kinematic gait analysis to quantify peripheral nerve regeneration in the rat. Int Rev Neurobiol. 2009, 87, 127–139. [Google Scholar]
- Bozkurt, A.; Deumens, R.; ScheVel, J.; O’Dey, D. M.; Weis, J.; Joosten, E. A.; Fu ̈hrmann, T.; Brook, G. A.; Pallua, N. CatWalk gait analysis in assessment of functional recovery after sciatic nerve injury. J. Neurosci. Methods. 2008, 173, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, R.; Schnider J.T.; Fanzio, P.M.; Tsuji, W.; Kostereva, N.; Solari, M.G. Plock, J.A.; Gorantla, V.S. Effect of systemic adipose-derived stem cell therapy on functional nerve regeneration in a rodent model. PRS Global Open. 2020, 1-10. [CrossRef]
- Targosinksi, S.; Henzi, A.; Engmann, A.K.; Rushing, E.J.; Barth, A.A.; Klein, H.J.; Kim, B.; Giovanoli, P. Schwab, M.E.; Plock, J.A., et al. A swim test for functional assessment of rodent peripheral nerve regeneration. J Neurosci Met. 2022, 379, 109663.
- Senger, J.B.; Rabey, K.N.; Morhart, M.J.; Chan, K.M.; Webber, C.A. Conditioning electrical stimulation accelerates regeneration in nerve transfers. Ann Neurol. 2020, 88, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Molteni, R.; Zheng, J.-Q.; Ying, Z.; Gomez-Pinilla, F.; Twiss, J.L. Voluntary exercise increases axonal regeneration from sensory neurons. Proc. Natl. Acad. Sci. USA. 2004, 101, 8473–8478. [Google Scholar] [CrossRef]
- Al-Majed, A.; Brushart, T.M.; Gordon, T. Electrical stimulation accelerates and increases expression of BDNF and trkB mRNA in regenerating rat femoral motoneurons. Eur. J. Neurosci. 2000, 12, 4381–4390. [Google Scholar] [CrossRef]
- English, A.W.; Schwartz, G.; Meador, W.; Sabatier, M.J.; Mulligan, A. Electrical stimulation promotes peripheral axon regeneration by enhanced neuronal neurotrophin signaling. Dev. Neurobiol. 2007, 67, 158–172. [Google Scholar] [CrossRef]
- Martins, D.F.; Mazzardo-Martins, L.; Gadotti, V.M.; Nascimento, F.P.; Lima, D.A.; Speckhann, B.; Favretto, G.A.; Bobinski, F.; Cargnin-Ferreira, E.; Bressan, E.; et al. Ankle joint mobilization reduces axonotmesis-induced neuropathic pain and glial activation in the spinal cord and enhances nerve regeneration in rats. Pain. 2011, 152, 2653–2661. [Google Scholar] [CrossRef] [PubMed]
- Ying, Z.; Roy, R.R.; Edgerton, V.; Gómez-Pinilla, F. Voluntary exercise increases neurotrophin-3 and its receptor TrkC in the spinal cord. Brain Res. 2003, 987, 93–99. [Google Scholar] [CrossRef]
- Seo, T.B.; Oh, M.-J.; You, B.-G.; Kwon, K.-B.; Chang, I.-A.; Yoon, J.-H.; Lee, C.Y.; Namgung, U. ERK1/2-Mediated Schwann Cell Proliferation in the Regenerating Sciatic Nerve by Treadmill Training. J. Neurotrauma. 2009, 26, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Ahlborn, P.; Schachner, M.; Irintchev, A. One hour electrical stimulation accelerates functional recovery after femoral nerve repair. Exp. Neurol. 2007, 208, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pinilla, F.; Ying, Z.; Roy, R.R.; Molteni, R.; Edgerton, V.R. Voluntary Exercise Induces a BDNF-Mediated Mechanism That Promotes Neuroplasticity. J. Neurophysiol. 2002, 88, 2187–2195. [Google Scholar] [CrossRef] [PubMed]
- Troupel, T.; Caenegem, N.V.; Jeandel, A.; Thibaud, J.; Nicolle, A.; Blot, S. Epidemiological, clinical, and electrophysiological findings in dogs and cats with traumatic brachial plexus injury: a retrospectove study of 226 cases. J Vet Intern Med. 2021, 35, 2837–2845. [Google Scholar] [CrossRef]
- Griffiths, I.R.; Duncan, I.D.; Lawson, D.D. Avulsion of the brachial plexus-2. Clinical aspects. J Small Anim Pract. 1974, 15, 177–183. [Google Scholar] [CrossRef]
- Wood, M.D.; Kemp, S.W.; Weber, C.; Borschel, G.H.; Gordon, T. Outcome measures of peripheral nerve regeneration. Annals of Anatomy. 2011, 193, 321–333. [Google Scholar] [CrossRef]
- Belviso, I.; Palermi, S.; Sacco, A.M.; Romano, V.; Corrado, B.; Zappia, M.; Sirico, F. Brachial plexus injuries in sport medicine: Clinical evaluation, diagnostic approaches, treatment options and rehabilitative interventions. J Funct Morphol Kinesiol. 2020, 5, 22. [Google Scholar] [CrossRef]
- Preston, D.C.; Shapiro, B.E. Needle electromyography. Fundamentals, normal and abnormal patterns. Neurol. Clin. 2002, 20, 361–396. [Google Scholar] [CrossRef]
- Anson, A.; Gil, F.; Laredo, F.G.; Soler, M.; Belda, E.; Ayala, M.D.; Agut, A. Correlative ultrasound anatomy of the feline brachial plexus and major nerves of the thoracic limb. Vet Radiol Ultrasound. 2013, 54, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Benecke, R.; Berthold, A.; Conrad, B. Denervation activity in the EMG of patients with upper motor neuron lesions: Time course, local distribution and pathogenetic aspects. J. Neurol. 1983, 230, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Effron, C.R.; Beasley, R.W. Compression neuropathies in the upper limb and electrophysiological studies. In Grabb and Smith’s Plastic Surgery. Thorne, C.H., Bartlett, S.P., Beasley, R.W., Aston, S.J., Gurtner, G.C., Spear, S.L., eds. Philadelphia, USA: Lippincott Williams & Wilkins; 2006, pp. 86.
- Robinson, L.R. Traumatic injury to peripheral nerves. Muscle Nerve. 2000, 23, 863–87. [Google Scholar] [CrossRef]
- Teixeira, M.J.; da Paz, M.G.D.S.; Bina, M.T.; Santos, S.N.; Raicher, I.; Galhardoni, R.; Fernandes, D.T.; Yeng, L.T.; Baptista, A.F.; de Andrade, D.C. Neuropathic pain after brachial plexus avulsion-central and peripheral mechanisms. BMC Neurol. 2015, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Sadosky, A.; McDermott, A. A review of the epidemiology of painful diabetic peripheral neuropathy, postherpetic neuralgia, and less commonly studied neuropathic pain conditions. Pain Practice. 2008, 8, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Flor, H., Nikolajsen, L., Staehelin, T. Phantom limb pain: a case of maladaptive CNS plasticity? Nature reviews. Neuroscience. 2006, 7, 873–81.
- Flor, H.; Elbert, T.; Knecht, S.; Wienbruch, C.; Pantev, C.; Birbaumer, N.; et al. Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature 1995, 375, 482–4. [Google Scholar] [CrossRef]
- Flor, H.; Nikolajsen, L.; Staehelin Jensen, T. Phantom limb pain: A case of maladaptive CNS plasticity? Nat. Rev. Neurosci. 2006, 7, 873–881. [Google Scholar] [CrossRef]
- Menchetti, M.; Gandini, G.; Gallucci, A.; Della Rocca, G.; Matiasek, L.; Matiasek, K.; Gentilini, F.; Rosati, M. Approaching phantom complex after limb amputation in the canine species. J. Vet. Behav. 2017, 22, 24–28. [Google Scholar] [CrossRef]
- Melzack, R. Phantom limbs. Scientific American. 1992, 90–6. [Google Scholar] [CrossRef]
- Ehde. D.M.; Czerniecki, J.M.; Smith, D.G.; Campbell, K.M.; Edwards, W.T.; Jensen, M.P. et al. Chronic phantom sensations, phantom pain, residual limb pain, and other regional pain after lower limb amputation. Arch Phys Med Rehabil. 2000, 81, 1039–44.
- Probstner, D.; Thuler, L.C.; Ishikawa, N.M.; Alvarenga, R.M. Phantom limb phenomena in cancer amputees. Pain Pract. 2010, 10, 249–256. [Google Scholar] [CrossRef]
- Varejão, A.S.P.; Cabrita, A.M.; Geuna, S.; Melo-Pinto, P.; Filipe, V.M.; Gramsbergen, A.; Meek, M.F. Toe out angle: a functional index for the evaluation of sciatic nerve recovery in the rat model. Exp Neurol. 2003, 183. [Google Scholar] [CrossRef]
- M. Vivo ́, A.; Puigdemasa, L.; Casals, E.; Asensio, E.: Udina, X. Navarro, Immediate electrical stimulation enhances regeneration and reinnervation and modulates spinal plastic changes after sciatic nerve injury and repair. Exp. Neurol. 2008, 211, 180–193.
- Woolf, C.J. Evidence for a central component of post-injury pain hypersensitivity. Nature. 1983, 306, 686–688. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Kuner, R.; Jensen, T.S. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021, 101, 259–301. [Google Scholar] [CrossRef] [PubMed]
- Campero, M.; Serra, J.; Marchettini, P.; Ochoa, J.L. Ectopic impulse generation and autoex-citation in single myelinated afferent fibers in patients with peripheral neuropathy andpositive sensory symptoms. Muscle Nerve. 1998, 21, 1661–1667. [Google Scholar] [CrossRef]
- Nordin, M.; Nyström, B.; Wallin, U.; Hagbarth, K.E. Ectopic sensory discharges and pares-thesiae in patients with disorders of peripheral nerves, dorsal roots and dorsal col-umns. Pain. 1984, 20, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, J.; Torebjörk, E. Sensations evoked by intraneural microstimulation of C noci-ceptor fibres in human skin nerves. JPhysiol. 1989, 415, 583–599. [Google Scholar]
- Gonçalves, N.P.; Vægter, C.B.; Andersen, H.; Østergaard, L.; Calcutt, N.A. , Jensen, T.S.Schwann cell interactions with axons and microvessels in diabetic neuropathy. Nat RevNeurol. 2017, 13, 135–147. [Google Scholar]
- De Logu, F.; Li Puma, S.; Landini, L.; Portelli, F.; Innocenti, A.; de Araujo, D.S.M.; Janal, M.N.; Patacchini, R.; Bunnett, N.W.; Geppetti, P.; Nassini, R. Schwann cells expressing nociceptivechannel TRPA1 orchestrate ethanol-evoked neuropathic pain in mice. J Clin Invest. 2019, 129, 5424–5441. [Google Scholar] [CrossRef]
- Salter, M.W.; Beggs, S. Sublime microglia: expanding roles for the guardians of the CNS. Cell. 2014, 158, 15–24. [Google Scholar] [CrossRef]
- Moore, S.A. Managing neuropathic pain in dogs. Front Vet Sci. 2016, 22, 3–12. [Google Scholar] [CrossRef]
- Carvalho, G.A.; Nikkhah, G.; Matthies, C.; Penkert, G.; Samii, M. Diagnosis of root avulsions in traumatic brachial plexus injuries: Value of computerized tomography myelography and magnetic resonance imaging. J. Neurosurg. 1997, 86, 69–76. [Google Scholar] [CrossRef]
- Smith, B.W.; Daunter, A.K.; Yang, L.J.S.; Wilson, T.J. An Update on the Management of Neonatal Brachial Plexus Palsy—Replacing Old Paradigms: A Review. JAMA Pediatr. 2018, 172, 585. [Google Scholar] [CrossRef]
- Rich, J.A.; Newell, A.; Williams, T. Traumatic brachial plexus injury rehabilitation using neuromuscular electrical muscle stimulation in a polytrauma patient. BMJ Case Rep. 2019, 12, e232107. [Google Scholar] [CrossRef]
- Abdel-Aziz, S.; Ghaleb, A.H. Cervical Spinal Cord Stimulation for the Management of Pain from Brachial Plexus Avulsion. Pain Med. 2014, 15, 712–714. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Liu, P.; Rui, J.; Zhao, X.; Lao, J. The clinical characteristics of neuropathic pain in patients with total brachial plexus avulsion: A 30-case study. Injury 2016, 47, 1719–1724. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yuzhou, L.; Yingjie, Z.; Jie, L.; Xin, Z. A new rat model of neuropathic pain: Complete brachial plexus avulsion. Neurosci. Lett. 2015, 589, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, J.R.; Meek, M.; Robinson, P.H.; Gramsbergen, A. Methods to evaluate functional nerve recovery in adult rats: walking track analysis, video analysis and the withdrawal reflex. J Neurosci Met. 2000, 96, 89–96. [Google Scholar] [CrossRef]
- Meek, M.F.; Van Der Werff, J.F.A.; Nicolai, J.P.A.; Gramsbergen, A. Biodegradable p (DLLA-e-CL) Nerve guides versus autologous nerve grafts: electromyographic amd video analysis. Muscle & Nerve. 2001, 24, 753–759. [Google Scholar]
- Watson, N.C.; Jejurikar, S.; Kalliainen, L.K.; Calderon, M.S.; URbanchek, M.G.; Eguchi, T.; Kuzon, J.R. Range of motion physiotherapy reduces the force deficit in antagonists to denervated rat muscles. J Surg Res. 2001, 99, 156–160. [Google Scholar] [CrossRef]
- Du, Z.; Zhang, J.; Han, X.; Yu, W.; Gu, X. Potential novel therapeutic strategies for neuropathic pain. Front Mol Neurosci. 2023, 16, 1138798. [Google Scholar] [CrossRef]
- Chandrashekhar, R.; Wang, H.; Dionne, C.; James, S.; and Burzycki, J. Wearable focal muscle vibration on pain, balance, mobility, and sensation in individuals with diabetic peripheral neuropathy: a pilot study. Int. J. Environ. Res. Public Health. 2021, 18, 2415. [Google Scholar] [CrossRef]
- Heo, J.; Jo, J.; Lee, J.; Kang, H.; Choi, T.; Lee, M.; Kim, J. Electroacupuncture for the treatment of frozen shoulder. Medicine (Baltimore). 2021, 100, e28179. [Google Scholar] [CrossRef]
- Johnson, M. I.; Paley, C. A.; Jones, G.; Mulvey, M. R.; and Wittkopf, P. G. Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults: a systematic review and meta-analysis of 381 studies (the meta-TENS study). BMJ Open. 2022, 12, e051073. [Google Scholar] [CrossRef]
- Martins, Â.; Gouveia, D.; Cardoso, A.; Viegas, I.; Gamboa, Ó.; Ferreira, A. A comparison between body weight-supported treadmill training and conventional over-ground training in dogs with incomplete spinal cord injury. Front Vet Sci. 2021, 8, 597949. [Google Scholar] [CrossRef]
- Lovaglio, A.; Socolovsky, M.; Di Masi, G.; Bonilla, G. Treatment of neuropathic pain after peripheral nerve and brachial plexus traumatic injury. Neurol. India. 2019, 67, 32. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.; Dailey, T.; Duncan, K.; Abel, N.; Borlongan, C.V. Peripheral Nerve Injury: Stem Cell Therapy and Peripheral Nerve Transfer. Int J Mol Sci. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Blits, B.; Boer, G.J.; Verhaagen, J. Pharmacological, cell, and gene therapy strategies to promote spinal cord regeneration. Cell Transplant. 2002, 11, 593–613. [Google Scholar] [CrossRef] [PubMed]
- Faroni, A.; Mobasseri, S.A.; Kingham, P.J.; Reid, A.J. Peripheral nerve regeneration: experimental strategies and future perspectives. Adv Drug Deliv Rev. 2015, 82–83, 160–167.
- Magnaghi, V.; Procacci, P.; Tata, A.M. Chapter 15: Novel pharmacological approaches to Schwann cells as neuroprotective agents for peripheral nerve regeneration. Int Rev Neurobiol. 2009, 87, 295–315. [Google Scholar]
- Vijayavenkataraman, S. Nerve guide conduits for peripheral nerve injury repair: A review on design, materials and fabrication methods. Acta Biomater. 2020, 106, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Raza, C.; Riaz, H.A.; Anjum, R.; Shakeel, N.U.A. Repair strategies for injured peripheral nerve: Review. Life Sci. 2020, 243, 117308. [Google Scholar] [CrossRef]
- Isvoranu, G.; Manole, E.; Neagu, M. Gait Analysis Using Animal Models of Peripheral Nerve and Spinal Cord Injuries. Biomedicines. 2021, 9, 1050. [Google Scholar] [CrossRef] [PubMed]
- Leite, A.P.S.; Pinto, C.G.; Tiburcio, F.C.; Sartori, A.A.; de Castro Rodrigues, A.; Barraviera, B.; Ferreira, R.S.J.; Filadelpho, A.L.; Matheus, S.M.M. Heterologous fibrin sealant potentiates axonal regeneration after peripheral nerve injury with reduction in the number of suture points. Injury. 2019, 50, 834–847. [Google Scholar] [CrossRef]
- Morris, M.; Brogan, D.M.; Boyer, M.I.; Dy, C.J. Trends in nerve transfer procedures among board-eligible orthopedic hand surgeons. J Hand Surg Global. 2021, 3, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, J.; Mackinnon, S.E.; Watanabe, O.; et al. The effect of duration of muscle denervation on functional recovery in the rat model. Muscle Nerve. 1997, 1997. 20, 858e866. [Google Scholar] [CrossRef]
- Brown, J.M.; Tung, T.H.; Mackinnon, S.E. Median to radial nerve transfer to restore wrist and finger extension: technical nuances. Neurosurgery. 2010, 66(3 Suppl Operative), 75e83. [Google Scholar] [CrossRef]
- Mackinnon, S.E.; Roque, B.; Tung, T.H. Median to radial nerve transfer for treatment of radial nerve palsy: case report. J Neurosurg. 2007, 107, 666e671. [Google Scholar] [CrossRef]
- Dy, C.J.; Aunins, B.; Brogan, D.M. Barriers to epineural scarring: role in treatment of traumatic nerve injury and chronic compressive neuropathy. J Hand Surg Am. 2018, 43, 360–367. [Google Scholar] [CrossRef]
- Kokkalis, Z.T.; Mavrogenis, A.F.; Ballas, E.G.; Papagelopoulos, P.J.; Soucacos, P.N. Collagen nerve wrap for median nerve scarring. Orthopedics. 2015, 38, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Soltani, A.M.; Allan, B.J.; Best, M.J.; Mir, H.S.; Panthaki, Z.J. Revision decompression and collagen nerve wrap for recurrent and persistent compression neuropathies of the upper extremity. Ann Plast Surg. 2014, 72, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, L.; Adam, C.; Legagneux, J.; Bruneval, P.; Masmejean, E. Reduction of neural scarring after peripheral nerve suture: an experimental study about collagen membrane and autologous vein wrapping. Chir Main. 2012, 31, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Papatheodorou, L.K.; Williams, B.G.; Sotereanos, D.G. Preliminary results of recurrent cubital tunnel syndrome treated with neurolysis and porcine extracellular matrix nerve wrap. J Hand Surg Am. 2015, 40, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Magill, C.K.; Tuffaha, S.H.; Yee, A.; et al. The short- and long-term effects of Seprafilm on peripheral nerves: a histological and functional study. J Reconstr Microsurg. 2009, 25, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Ozgenel, G.Y.; Filiz, G. Effects of human amniotic fluid on peripheral nerve scarring and regeneration in rats. J Neurosurg. 2003, 98, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, M.P.; Abdelfattah, H.M.; Welch, I.W.; Vosbikian, M.M.; Kane, P.M.; Rekant, M.S. Recurrent cubital tunnel syndrome treated with revision neurolysis and amniotic membrane nerve wrapping. J Shoulder Elbow Surg. 2016, 25, 2057–2065. [Google Scholar] [CrossRef]
- Liu, T.; Xu, J.; Pan, X.; Ding, Z.; Xie, H.; Wang, X.; Xie, H. Advances of adipose-derived mesenchymal stem cells-based biomaterial scaffolds for oral and maxillofacial tissue engineering. Bioact Mater. 2021, 6, 2467–2478. [Google Scholar] [CrossRef]
- Zorko, B.; Rozman, J.; Seliškar, A. Influence of electrical stimulation on regeneration of the radial nerve in dogs. Acta Vet. Hung. 2000, 48, 99–105. [Google Scholar] [CrossRef]
- Foecking, E.M.; Fargo, K.N.; Coughlin, L.M.; Kim, J.M.; Sam, J.; Jones, K.J. Crush Injury Enhances Functional Recovery of Rat Facial Nerve, 2012, 49, pp. 451–458.
- Brushart, T.M.; Hoffman, P.N.; Royall, R.M.; Murinson, B.B.; Witzel, T. Gordon Electrical stimulation promotes motoneuron regeneration without increasing its speed or conditioning the neuron. J Neurosci. 2002, 22, 6631–6638. [Google Scholar] [CrossRef]
- Geremia, N.M.; Gordon, T.; Brushart, T.M.; Al-Majed, A.A.; Verge, V.M.K. Electrical stimulation promotes sensory neuron regeneration and growth-associated gene expression. Exp Neurol. 2007, 205, 347–359. [Google Scholar] [CrossRef]
- Huang, J.; Lu, L.; Hu, X.; Ye, Z.; Peng, Y.; Yan, X.;Geng, D.; Luo, Z. Electrical stimulation accelerates motor functional recovery in the rat model of 15-mm sciatic nerve gap bridged by scaffolds with longitudinally oriented microchannels, Neurorehabil Neural Repair. 2010, 24, 736–745.
- Ni, L.; Yao, Z.; Zhao, Y.; Zhang, T.; Wang, J; Li, S.; Chen, Z. Electrical stimulation therapy for peripheral nerve injury. Front Neurol. 2023, 14, 1–13.
- Huang, J.; Zhang, Y.; Lu, L.; Hu, X.; Luo, Z. Electrical stimulation accelerates nerve regeneration and functional recovery in delayed peripheral nerve injury in rats. Eur J Neurosci. 2013, 38, 3691–701. [Google Scholar] [CrossRef]
- Song, S.; McConnell, K.W.; Amores, D.; Levinson, A.; Vogel, H.; Quarta, M.; et al. Electrical stimulation of human neural stem cells via conductive polymer nerve guides enhances peripheral nerve recovery. Biomaterials. 2021, 275, 120982. [Google Scholar] [CrossRef]
- Cobianchi, S.; Casals-Diaz, L.; Jaramillo, J.; Navarro, X. Differential effects of activity dependent treatments on axonal regeneration and neuropathic pain after peripheral nerve injury. Exp Neurol. 2013, 240, 157–67. [Google Scholar] [CrossRef]
- Al-Majed, A.A.; Tam, S.L.; Gordon, T. Electrical stimulation accelerates and enhances expression of regeneration-associated genes in regenerating rat femoral motoneurons. Cell Mol Neurobiol. 2004, 24, 379–402. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, K.A.; Irintchev, A.; Al-Majed, A.A.; Simova, O.; Brushart, T.M.; Gordon, T, et al.. BDNF/TrkB signaling regulates HNK-1 carbohydrate expression in regenerating motor nerves and promotes functional recovery after peripheral nerve repair. Exp Neurol. 2006, 198, 500–10.
- Batty, N.J.; Torres-Espín, A.; Vavrek, R.; Raposo, P.; Fouad, K. Single-session cortical electrical stimulation enhances the efficacy of rehabilitative motor training after spinal cord injury in rats. Exp Neurol. 2020, 324, 113136. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.; Gouveia, D.; Cardoso, A.; Gamboa, Ó.; Millis, D.; Ferreira, A. Nervous system modulation through electrical stimulation in companion animals. Acta Vet Scand. 2021, 63, 22. [Google Scholar] [CrossRef]
- Boyd, J.G.; Gordon, T. Neurotrophic factors and their receptors in axonal regeneration and functional recovery after peripheral nerve injury, Mol Neurobiol. 2003, 27, 277–324.
- Lu, B.; Pang, P.T.; Woo, N.H. The yin and yang of neurotrophin action. Nat Rev Neurosci. 2005, 6, 603–614. [Google Scholar] [CrossRef]
- Richner, M.; Ulrichsen, M.; Elmegaard, S.L.; Dieu, R.; Pallesen, L.T.; Vaegter, C.B. Peripheral nerve injury modulates neurotrophin signaling in the peripheral and central nervous system. Mol Neurobiol. 2014, 50, 945–970. [Google Scholar] [CrossRef]
- Gordon, T. Electrical Stimulation to Enhance Axon Regeneration After Peripheral Nerve Injuries in Animal Models and Humans. Neurotherapeutics. 2016, 13, 295–310. [Google Scholar] [CrossRef]
- Dow, D.E.; Dennis, R.G.; Faulkner, J.A. Electrical stimulation attenuates denervation and age-related atrophy in extensor digitorum longus muscles of old rats. J Gerontol A Biol Sci Med Sci. 2005, 60, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Eberstein, A.; Eberstein, S. Electrical stimulation of denervated muscle: is it worthwhile? Med Sci Sports Exerc. 1996, 28, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Brushart, T.M.; Jari, R.; Verge, V.; Rohde, C.; Gordon, T. Electrical stimulation restores the specificity of sensory axon regeneration. Exp. Neurol. 2005, 194, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Tam, S.L.; Archibald, V.; Jassar, B.; Tyreman, N.; Gordon, T. Increased Neuromuscular Activity Reduces Sprouting in Partially Denervated Muscles. J. Neurosci. 2001, 21, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Love, F.M.; Son, Y.-J.; Thompson, W.J. Activity alters muscle reinnervation and terminal sprouting by reducing the number of schwann cell pathways that grow to link synaptic sites. J. Neurobiol. 2003, 54, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Alvites, R.; Rita Caseiro, A.; Santos Pedrosa, S.; Vieira Branquinho, M.; Ronchi, G.; Geuna, S.; Varejão, A.S.P.; Colette Maurício, A.; Spurkland, A. Peripheral nerve injury and axonotmesis: State of the art and recent advances. Cogent. Med. 2018, 5, 1466404. [Google Scholar] [CrossRef]
- Bula-Oyola, E.; Belda-Lois, J.; Porcar-Seder, R.; Page, A. Effectiveness of electrophysical modalities in the sensorimotor rehabilitation of radial, ulnar, and median neuropathies: A meta-analysis. Plos One. 2021, 0248484. [Google Scholar] [CrossRef]
- Colbert, A.P.; Markov, M.S.; Carlson, N.; Gregory, W.L.; Carlson, H.; Elmer, P.J. Static Magnetic Field Therapy for Carpal Tunnel Syndrome: A Feasibility Study. Arch Phys Med Rehabil. 2010, 91, 1098–104. [Google Scholar] [CrossRef]
- Ozkan, F.U.; Saygı, E.K.; Senol, S.; Kapcı, S.; Aydeniz, B.; Aktaş, İ.; et al. New treatment alternatives in the ulnar neuropathy at the elbow: ultrasound and low-level laser therapy. Acta Neurol Belg. 2015, 115, 355–60. [Google Scholar] [CrossRef]
- Bilgin Badur, N.; Unlu Ozkan, F.; Aktas, I. Efficacy of shortwave diathermy in ulnar nerve entrapment at the elbow: a double-blind randomized controlled clinical trial. Clin Rehabil. 2020, 34, 1048–55. [Google Scholar] [CrossRef] [PubMed]
- Oshima, C.; Nakazawa, H.; Izukura, H.; Miyagi, M.; Mizutani, A.; Harada, T.; et al. Low Level Laser Therapy for Radial Nerve Palsy Patients: Our Experience. LASER Ther. 2018, 27, 56–60. [Google Scholar] [CrossRef]
- Kim, J.K.; Jeon, S.H. Minimal clinically important differences in the Carpal Tunnel Questionnaire after carpal tunnel release. J Hand Surg. 2013, 38, 75–9. [Google Scholar] [CrossRef]
- Gunter, C.; Delbeke, J.; Ortiz-Catalan, M. Safety of long-term electrical peripheral nerve stimulation: review of the state of the art. J NeuroEng Rehab. 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Agnew, W.F.; McCreery, D.B. Considerations for safety with chronically implanted nerve electrodes. Epilepsia. 1990, 31, S27–32. [Google Scholar] [CrossRef] [PubMed]
- McCreery, D.B.; Agnew, W.F.; Yuen, T.G.H. Bullara, L.A. Relationship between stimulus amplitude, stimulus frequency and neural damage during electrical stimulation of sciatic nerve of cat. Med Biol Eng Comput. 1995, 33, 426–9. [Google Scholar] [CrossRef]
- Waters, R.L.; McNeal, D.R.; Faloon, W. Clifford B. Functional electrical stimulation of the peroneal nerve for hemiplegia. Long-term clinical follow-up. J Bone Jt Surg. 1985, 67, 792–3. [Google Scholar] [CrossRef]
- Agnew, W.F.; McCreery, D.B.; Yuen, T.G.H.; Bullara, L.A. Histologic and physiologic evaluation of electrically stimulated peripheral nerve: considerations for the selection of parameters. Ann Biomed Eng. 1989, 17, 39–60. [Google Scholar] [CrossRef] [PubMed]
- Hasiba-Pappas, S.; Kamolz, L.; Luze, H.; Nischwitz, S.; Holzer-Geissler, J.; Tuca, A.; Rienmuller, T.; Polz, M.; Ziesel, D.; Winter, R. Does electrical stimulation through nerve conduits improve peripheral nerve regeneration? – A systematic review. J Pers Med. 2023, 13, 414. [Google Scholar] [CrossRef] [PubMed]
- Kubiak, C.A.; Kung, T.A.; Brown, D.L.; Cederna, P.S.; Kemp, S.W.P. State-of-The-Art techniques in treating peripheral nerve injury. Plast. Reconstr. Surg. 2018, 141, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.M.; Curran, M.W.T.; Gordon, T. Neuroscience The use of brief post-surgical low frequency electrical stimulation to enhance nerve regeneration in clinical practice. J. Physiol. 2016, 594, 3553–3559. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Kao, C.H.; Chen, C.C.; Ke, C.J.; Yao, C.H.; Chen, Y.S. Time-course effect of electrical stimulation on nerve regeneration of diabetic rats. PLoS ONE. 2015, 10, e0116711. [Google Scholar] [CrossRef]
- Song, J.; Sun, B.; Liu, S.; Chen, W.; Zhang, Y.; Wang, C.; Mo, X.; Che, J.; Ouyang, Y.; Yuan, W.; et al. Polymerizing pyrrole coated poly (l-lactic acid-co-ε-caprolactone) (PLCL) conductive nanofibrous conduit combined with electric stimulation for long-range peripheral nerve regeneration. Front. Mol. Neurosci. 2016, 9, 117. [Google Scholar] [CrossRef]
- Dorrian, RM.; Berryman, C.F.; Lauto, A.; Leonard, A.V. Electrical stimulation for the treatment of spinal cord injuries: a review of the cellular and molecular mechanisms that drive functional improvements. Front Cell Neurosci. 2023, 17, 1095259. [Google Scholar] [CrossRef]
- Griffin, L.; Decker, M. J.; Hwang, J. Y.; Wang, B.; Kitchen, K.; Ding, Z. , et al. Functional electrical stimulation cycling improves body composition, metabolic and neural factors in persons with spinal cord injury. J. Electromyogr. Kinesiol. 2009, 19, 614–622. [Google Scholar]
- Bakkum, A. J.; Paulson, T. A.; Bishop, N. C.; Goosey-Tolfrey, V. L.; Stolwijk-Swüste, J. M.; van Kuppevelt, D. J. et al. Effects of hybrid cycle and handcycle exercise on cardiovascular disease risk factors in people with spinal cord injury: A randomized controlled trial. J. Rehabil. Med. 2015, 47, 523–530.
- Ayanwuyi, L.; Tokarska, N.; McLean, N. A.; Johnston, J. M.; Verge, V. M. K. Brief electrical nerve stimulation enhances intrinsic repair capacity of the focally demyelinated central nervous system. Neural Regen. Res. 2022, 17, 1042–1050. [Google Scholar] [PubMed]
- Hahm, S.-C.; Yoon, Y. W.; Kim J. High-Frequency transcutaneous electrical nerve stimulation alleviates spasticity after spinal contusion by inhibiting activated microglia in rats. Neurorehabil. Neural Rep. 2014, 29, 370–381.
- Chu, X.; Song, X.; Li, Q.; Li, Y.; He, F.; Gu, X.; Ming, D. Basic mechanisms of peripheral nerve injury and treatment via electrical stimulation. Neural Regen Res. 2022, 17, 2185–2193. [Google Scholar] [PubMed]
- Martins, D.F.; Martins, T.C.; Batisti, A.P.; Leonel, L.D.S.; Bobinski, F.; Belmonte, L.A.O.; Mazzardo-Martins, L.; Cargnin-Ferreira, E.; Santos, A.R.S. Long-Term Regular Eccentric Exercise Decreases Neuropathic Pain-like Behavior and Improves Motor Functional Recovery in an Axonotmesis Mouse Model: The Role of Insulin-like Growth Factor-1. Mol. Neurobiol. 2017, 55, 6155–6168. [Google Scholar] [CrossRef]
- Sobral, L.L.; Oliviera, L.S.; Takeda, S.Y.M.; Somazz, M.C.; Montebelo, M.I.L.; Teodori, R.M. Immediate versus later exercises for rat sciatic nerve regeneration after axonotmesis: Histomorphometric and functional analyses. Rev. Bras. Fisioter 2008, 12, 311–316. [Google Scholar] [CrossRef]
- López-Álvarez, V.M.; Modol, L.; Navarro, X.; Cobianchi, S. Early increasing-intensity treadmill exercise reduces neuropathic pain by preventing nociceptor collateral sprouting and disruption of chloride cotransporters homeostasis after peripheral nerve injury. Pain 2015, 156, 1812–1825. [Google Scholar] [CrossRef]
- de Moraes, A.A.; de Almeida, C.A.S.; Lucas, G.; Thomazini, J.A.; DeMaman, A.S. Effect of swimming training on nerve morphological recovery after compressive injury. Neurol. Res. 2018, 40, 955–962. [Google Scholar] [CrossRef]
- Ilha, J.; Araujo, R.T.; Malysz, T.; Hermel, E.E.S.; Rigon, P.; Xavier, L.L.; Achaval, M. Endurance and Resistance Exercise Training Programs Elicit Specific Effects on Sciatic Nerve Regeneration After Experimental Traumatic Lesion in Rats. Neurorehabilit. Neural Repair 2007, 22, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Pachter, B.R.; Eberstein, A. Passive Exercise and Reinnervation of the Rat Denervated Extensor Digitorum Longus Muscle after Nerve Crush. Am. J. Phys. Med. Rehabilitation 1989, 68, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Florence, S.L.; Boydston, L.A.; Hackett, T.A.; Lachoff, H.T.; Strata, F.; Niblock, M.M. Sensory enrichment after peripheral nerve injury restores cortical, not thalamic, receptive field organization. Eur. J. Neurosci. 2001, 13, 1755–1766. [Google Scholar] [CrossRef]
- Sinis, N.; Guntinas-Lichius, O.; Irintchev, A.; Skouras, E.; Kuerten, S.; Pavlov, S.P.; Schaller, H.E.; Dunlop, S.A.; Angelov, D.N. Manual stimulation of forearm muscles does not improve recovery of motor function after injury to a mixed peripheral nerve. Med. Sci. Sports Exerc. 2006, 38, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- Cobianchi, S.; de Cruz, J.; Navarro, X. Assessment of sensory thresholds and nociceptive fiber growth after sciatic nerve injury reveals the differential contribution of collateral reinnervation and nerve regeneration to neuropathic pain. Exp. Neurol. 2014, 255, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pan, B.; Fromholt, S.E.; Hess, E.J.; Crawford, T.O.; Griffin, J.W.; Sheikh, K.A.; Schnaar, R.L. Myelin-associated glycoprotein and complementary axonal ligands, gangliosides, mediate axon stability in the CNS and PNS: neuropathology and behavioral deficits in single- and double-null mice. Exp Neurol. 2005, 195, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Trapp, B.D.; Andrews, S.B.; Cootauco, C.; Quarles, R. The myelin-associated glycoprotein is enriched in multivesicular bodies and periaxonal membranes of actively myelinating oligodendrocytes. J Cell Biol. 1989, 109, 2417–26. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.P.; Taylor, R.S. Guillain-Barre Syndrome. StatPearls. 2022. [Google Scholar]
- Sabatier, M.J.; Redmon, N.; Schwartz, G.; English, A.W. Treadmill training promotes axon regeneration in injured peripheral nerves. Exp. Neurol. 2008, 211, 489–493. [Google Scholar] [CrossRef] [PubMed]
- English, A.W.; Cucoranu, D.; Mulligan, A.; Sabatier, M. Treadmill training enhances axon regeneration in injured mouse peripheral nerves without increased loss of topographic specificity. J. Comp. Neurol. 2009, 517, 245–255. [Google Scholar] [CrossRef]
- Hunter, G.; Sarvestany, A.A.; Roche, S.; Symes, R.; Gillinwater, T.H. SMN-dependent intrinsic defects in Schwann cells in mouse models of spinal muscular atrophy. Hum Mol Genet. 2014, 23, 2235–50. [Google Scholar] [CrossRef]
- Armada-da-Silva, P.; Pereira, C.; Amado, S.; Veloso, A. Role of physical exercise for improving posttraumatic nerve regeneration. Int Ver Neurobiol. 2013, 109, 125–49. [Google Scholar]
- Martins treino locomotor.
- Willand, M.; Nguyen, M.; Borschel, G.; Gordon, T. Electrical stimulation to promote peripheral nerve regeneration. Neurorehabil neural repair. 2016, 30, 30,490–6. [Google Scholar] [CrossRef]
- Thompson, N.J.; Sengelaub, D.R.; English, A.W. Enhancement of peripheral nerve regeneration due to treadmill training and electrical stimulation is dependent on androgen receptor signaling. Dev Neurobiol. 2014, 74, 531–540. [Google Scholar] [CrossRef]
- Elzinga, K.; Tyreman, N.; Ladak, A.; Savaryn, B.; Olson, J.; Gordon, T. Brief electrical stimulation improves nerve regeneration after delayed repair in Sprague Dawley rats. Exp Neurol. 2015. [Google Scholar] [CrossRef]
- Gordon, T.; Amirjani, N.; Edwards, D.C.; Chan, K.M. Brief post-surgical electrical stimulation accelerates axon regeneration and muscle reinnervation without affecting the functional measures in carpal tunnel syndrome patients. Exp Neurol. 2010, 223, 192–202. [Google Scholar] [CrossRef]
- Wong, J.N.; Olson, J.L.; Morhart, M.J.; Chan, K.M. Electrical stimulation enhances sensory recovery: A randomized control trial. Ann Neurol. 2015. [Google Scholar] [CrossRef]
- Juckett, L.; Saffari, T.M.; Ormseth, B.; Senger, J.; Moore, A. The effect of electrical stimulation on nerve regeneration following peripheral nerve injury. Biomolecules. 2022, 12, 1856. [Google Scholar] [CrossRef]
- López-Álvarez, V.M.; Modol, L.; Navarro, X.; Cobianchi, S. Early increasing-intensity treadmill exercise reduces neuropathic pain by preventing nociceptor collateral sprouting and disruption of chloride cotransporters homeostasis after peripheral nerve injury. Pain 2015, 156, 1812–1825. [Google Scholar] [CrossRef]
- Bal-Price, A.; Brown, G.C. Nitric-oxide-induced necrosis and apoptosis in PC12 cells mediated bu mitochondria. J Neurochem. 2000, 75, 1455–64. [Google Scholar] [CrossRef] [PubMed]
- Khalil, Z.; Khodr, B. A role for free radicals and nitric oxide in delayed recovery in aged rats with chronic constriction nerve injury. Free Rad Biol and Med. 2001, 31, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, R.I.; Marcolino, A.M.; de Jesus Guirro, R.R.; Mazzer, N.; Barbieri, C.H.; de Cássia Registro Fonseca, M. Comparative effects of wavelengths of low-power laser in regeneration of sciatic nerve in rats following crushing lesion. Lasers Med Sci. 2010, 25, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Gigo-Benato, D.; Geuna, S.; de Castro Rodrigues, A.; Tos, P.; Fornaro, M.; Boux, E.; Battiston, B. Giacobini-Robecchi, M.G. Low-power laser biostimulation enhances nerve repair after end-to-side neurorrhaphy: a double-blind randomized study in the rat median nerve model. Lasers Med Sci. 2004, 19, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.C.; Yang, Y.C.; Liu, B.S. Large-area irradiated low-level laser effect in a biodegradable nerve guide conduit on neural regeneration of peripheral nerve injury in rats. Injury. 2011, 42, 803–13. [Google Scholar] [CrossRef]
- Page, M.; OConnor, D.; Pitt, V.; Massy-Westropp, N. Therapeutic ultrasound for carpal tunnel syndrome. Cochrane Database Syst Rev. 2013, 3, CD009601. [Google Scholar] [CrossRef] [PubMed]
- Bekhet, A.; Ragab, B.; Abushouk, A.; Elgebaly, A.; Ali, O. Efficacy of low-level laser therapy in carpal tunnel syndrome management: a systematic review and meta-analysis. Lasers Med Sci. 2017, 32, 32,1439–1448. [Google Scholar] [CrossRef] [PubMed]
- Cofano, F.; Boido, M.; Monticelli, M.; Zenga, F.; Ducati, A.; Vercelli, A.; Garbossa, D. Mesenchymal Stem Cells for Spinal Cord Injury: Current Options, Limitations, and Future of Cell Therapy. Int. J. Mol. Sci. 2019, 20, 2698. [Google Scholar] [CrossRef] [PubMed]
- Rowland, J.W.; Hawryluk, G.W.; Kwon, B.; Fehlings, M.G. Current status of acute spinal cord injury pathophysiology and emerging therapies: Promise on the horizon. Neurosurg. Focus 2008, 25, E2. [Google Scholar] [CrossRef]
- Gazdic, M.; Volarevic, V.; Harrell, C.R.; Fellabaum, C.; Jovicic, N.; Arsenijevic ́, N.; Stojkovic, M. Stem Cells Therapy for Spinal Cord Injury. Int. J. Mol. Sci. 2018, 19, 1039. [Google Scholar] [CrossRef]
- Kumar, P.; Kandoi, S.; Misra, R.; Vijayalakshmi, S.; Rajagopal, K.; Verma, R.S. The mesenchymal stem cell secretome: A new paradigm towards cell-free therapeutic mode in regenerative medicine. Cytokine Growth Factor Rev. 2019, 46, 1–9. [Google Scholar]
Figure 1.
Interferential transcutaneous electrical nerve stimulation applied in the carpus of a dog with neuropathic pain.
Figure 1.
Interferential transcutaneous electrical nerve stimulation applied in the carpus of a dog with neuropathic pain.

Figure 3.
Land treadmill locomotor training with bicycle movements performed in a dog with monoplegia.
Figure 3.
Land treadmill locomotor training with bicycle movements performed in a dog with monoplegia.

Figure 4.
Laser therapy applied in a carpus of a cat with brachial plexus injury.
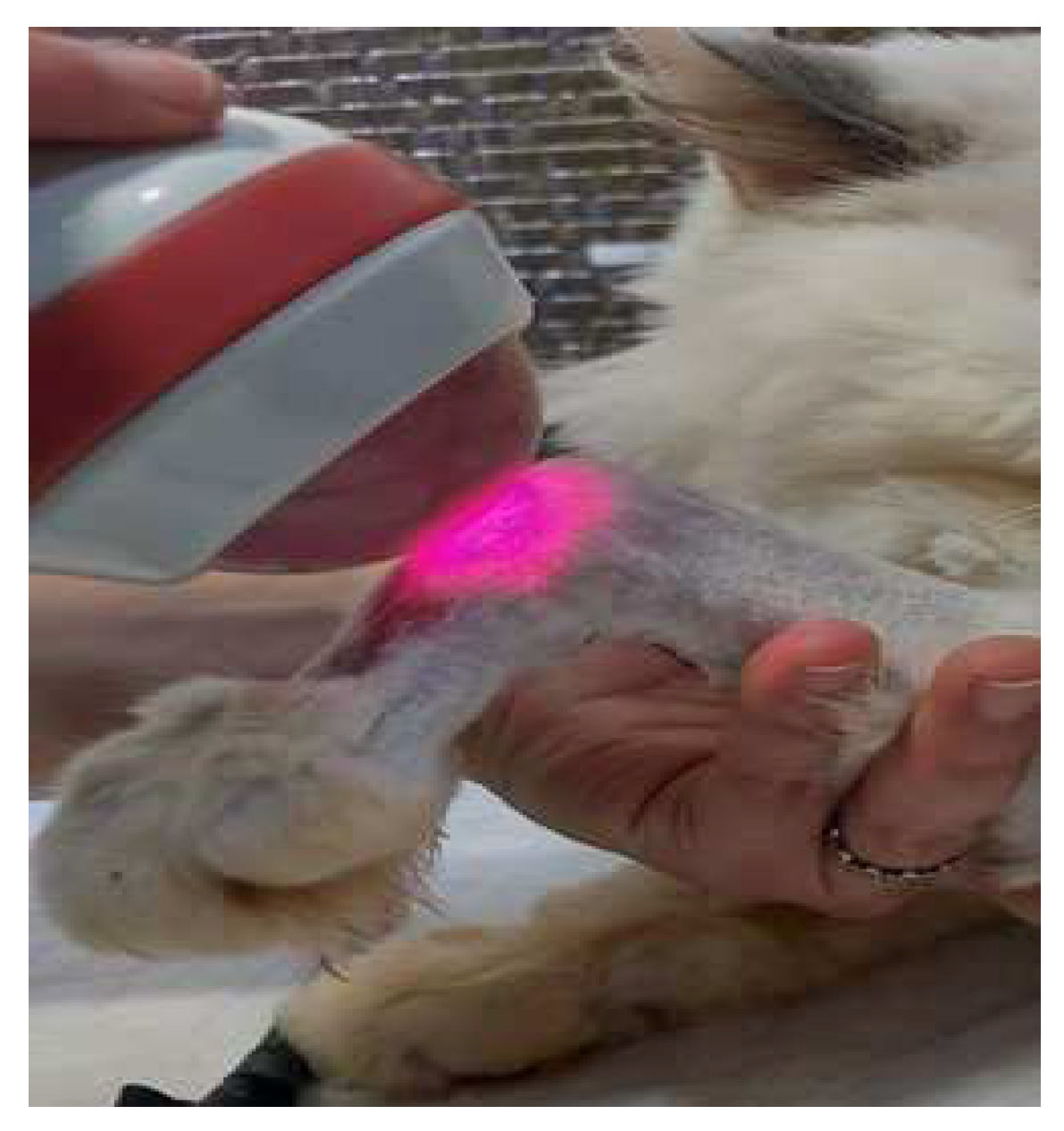
Figure 5.
Mesenchymal stem cell-based therapies and their beneficial effects.
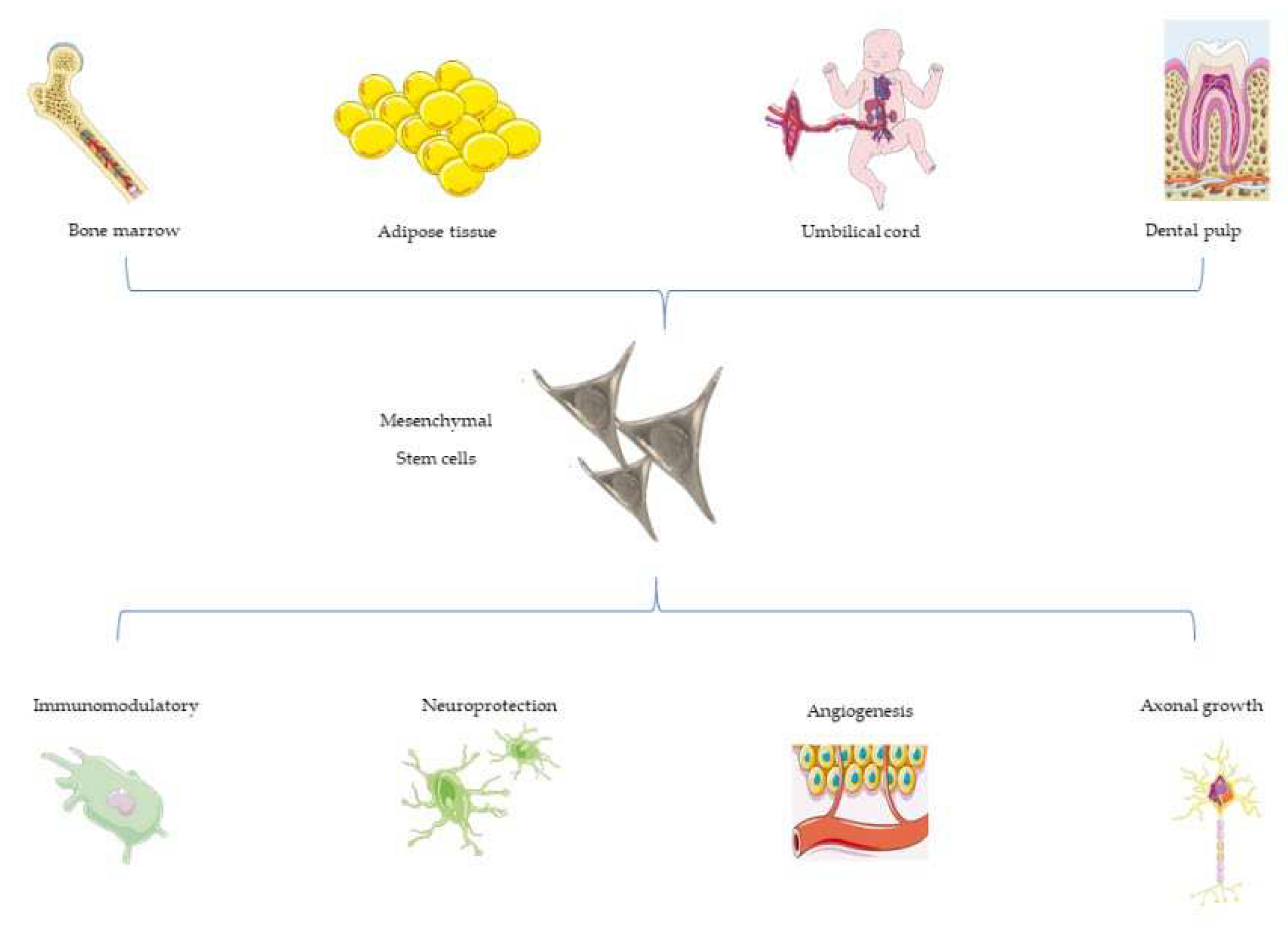
Figure 6.
Multimodal protocol approach to improve peripheral nerve injury repair.
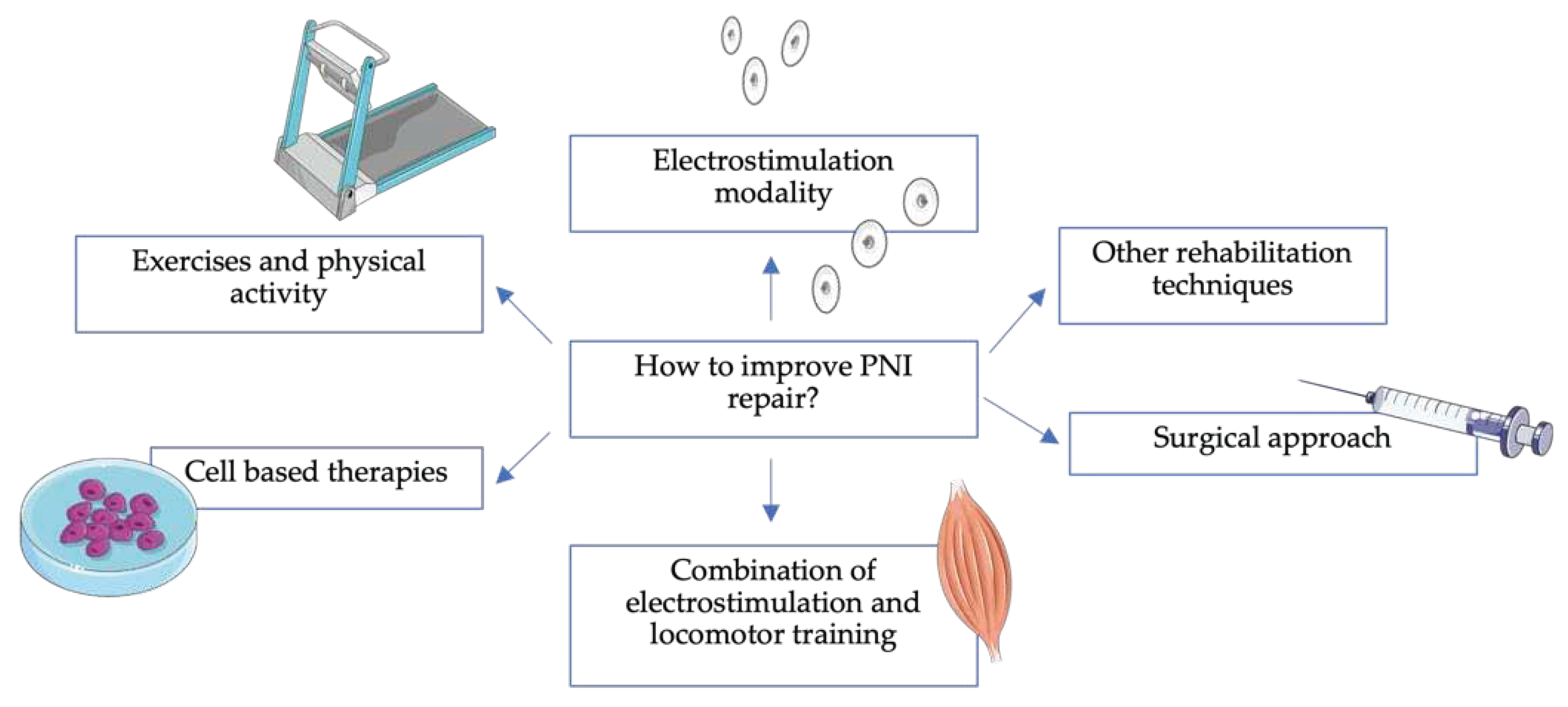
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



