Submitted:
14 February 2024
Posted:
14 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Vaccinating children against COVID-19 is an essential public health approach for preventing infection in children and adults. This study aimed to explore parents' attitudes toward and the rate of COVID-19 vaccine hesitancy among children in Oman. Methods: This cross-sectional study used an online, self-administered questionnaire. The 9-item questionnaire was validated earlier and administered between June 2021 and May 2022. Multiple logistic regression was used to determine the factors associated with vaccine hesitancy. The parents received a pre-validated Google questionnaire. Responses from the parents of children younger than 11 years of age were accepted. Results: 384 participants completed the questionnaire, including 207 males (54%). The response rate was 86% (384/447). Of the 384 participants, 69% of the parents hesitated to vaccinate their children aged 1-11-year-old children). In parents of children aged 1–4 years, parental vaccination status was significantly associated with vaccine hesitancy (odds ratio [OR]: 0.116, 95% confidence interval [CI]: 0.044–0.306; p < 0.001). Additionally, vaccine hesitancy was significantly more common in mothers than in fathers (OR: 0.451, 95% CI: 0.240–0.848; p = 0.013).
.
Mothers of children were 77% more likely to be hesitant than fathers (.78, 95% confidence intervals (CI) = 0.50–0.1.23; p = 0.283). Conclusion: Many parents hesitated to vaccinate their children against COVID-19. Consequently, future awareness campaigns and strategies should target new vaccines. The results of our study show that the Arabic version of the 5-point Likert Scale for Vaccination Hesitancy is a valid and reliable tool.
Keywords:
vaccine hesitancy
; children
; COVID-19
; SARS-CoV-2
; Oman
1. Introduction
Since 2019, vaccine hesitancy (VH) has been among the top 10 global health threats [1]. V.H., as defined by the World Health Organization (WHO) Strategic Advisory Group of Experts (SAGE), is the delay in accepting or refusing immunization despite the availability of vaccination services [2]. Vaccination reduces infectious disease incidence, morbidity, and fatality and increases life expectancy [3]. As of 15 November 2022, more than 633 million coronavirus disease 2019 (COVID-19) cases have been confirmed globally, including over 6.5 million deaths [4]. Vaccination against COVID-19 is essential because preventive measures alone are insufficient to inhibit its spread [5]. Globally, COVID-19 affects 1–5% of children <18 years of age [6]. Children with COVID-19 show a wide range of clinical symptoms, from no symptoms to severe infections, such as severe pneumonia and multisystem inflammatory disease (MIS-C) [6,7,8]. Fortunately, only a small percentage of children with COVID-19 require extended hospitalization or intensive care, and fatal outcomes are uncommon [9]. To date, there have been no reports of COVID-19- related mortalities in Omani children [8].
According to recent surveys, 60–80% of adults are willing to receive the COVID-19 vaccine, while 10% remain unwilling, and the rest are uncertain [10,11,12,13,14]. Factors associated with the willingness to be vaccinated against the disease include older age, higher education, higher income, history of chronic disease, and vaccine knowledge [11,13,14]. Regarding parental COVID-19 V.H., the rate of parental acceptance ranged from 59% to 65% [15,16,17,18]. In fact, studies have shown that parental vaccination hesitancy ranges from 4% to 40% worldwide [17,18,19] and from 24% to 61% in Middle Eastern countries [20,21,22,23]. Parents’ acceptance of new vaccination programs is influenced by several variables, particularly during pandemics, and the most frequent reason for caregivers to accept vaccination is to protect their child from infection. Previously, a cross-sectional study assessed parents' willingness to vaccinate their children against COVID-19 and found that 61.4% (95% CI: 53.6–68.7%, I2 = 99.3%) of parents were concerned about vaccine safety issues, and 54% (95% CI: 33–75%) believed that there was lack of evidence regarding the safety of new vaccines [24]. Additionally, several studies have examined what might affect parents' vaccination decisions, including worries about the vaccine side effects, hesitancy and distrust in vaccination, and difficulty getting to healthcare facilities. In Oman, a knowledge gap has been indicated concerning parents' knowledge, behavior, and hesitation regarding vaccinations for children with underlying chronic medical conditions [25,26,27,28,29,30,31,32]. Herein, we aimed to conduct a questionnaire at Sultan Qaboos University Hospital (SQUH) in Oman to examine COVID-19 VH among parents or legal guardians. We also describe the validation of the questionnaire using exploratory and confirmatory factor analyses.
2. Materials and Methods
2.1. Study Design and Settings
This cross-sectional study used electronic data collected through an online, self-administered questionnaire [33]. Data collection was based on social networking sites. Parents were emailed a well-designed, pre-validated Google Questionnaire [33]. Investigators who were native Arabic speakers translated the questionnaire into Arabic. An expert translated the Arabic version of the questionnaire into English to evaluate the preliminary translation. To test the language equivalency, a multilingual expert answered both versions. Under the supervision of the researchers, the participants completed the final Arabic version of the questionnaire, which took approximately eight minutes to complete. A waiver of consent was provided to indicate consent to participate. Participation in the survey was voluntary, and no compensation was provided. Data was collected from participants between 25th October 2021 and 1st May 2022 based on the following inclusion criteria: parents were required to be 18 years of age or older, and all parents with children under the age of 11 were asked to participate in the survey, attend an outpatient pediatric department, and be able to understand the Arabic language. Questionnaires were administered to one parent (father or mother) per family. Parents with children older than 12 years and those who did not consent to participate in the survey were excluded.
2.2. Measures
The parental questionnaire consisted of sociodemographic information and the vaccine hesitancy scale (VHS) for COVID-19 [33]. The sociodemographic portion included information on children (date of birth, gender, medical background) and parents (relationship with the child, date of birth, and educational level). The education levels were divided into five groups: primary school, secondary school, bachelor’s degree, master’s degree, and doctorate degree. Through social networking sites, parents were emailed a well-designed and pre-validated Google questionnaire [33]. A waiver of consent was provided to indicate consent to participate.
2.3. Sample Size
We calculated the sample size assuming that the predicted COVID-19 vaccine coverage would be 50% among children, with an allowable error of 5% and a sample size of 384.
2.4. Vaccine Hesitancy Rate Measurement
The "attitudes toward COVID-19 vaccines" section consists of nine statements with a 5-point Likert scale (3 = Unsure, 1= strongly disagree, 2 = disagree, 4 = agree, 5 = strongly agree), with questions about hesitancy and concerns regarding COVID-19 vaccines [33]. The responses to the positively-worded questions (1, 2, 3, and 9) were as follows: strongly disagree, 1 point; disagree, 2 points; neither agree nor disagree, 3 points; agree, 4 points; and strongly agree, 5 points. The response to the questions (4,5, 6, 7, and 8) were flipped because the questions were negatively-worded with strongly agree, 1 point; agree, 2 points; neither agree nor disagree, 3 points; disagree, 4 points; and strongly disagree, 5 points. The total score for all the 9 items was then summed up to a maximum of 45. Lower scores represented higher vaccine hesitancy and a cut-off value of ≤30 was used to define hesitancy.
2.5. Validation of the Arabic Version of the COVID-19 Questionnaire
Forward and Backward Translation
Two bilingual translators who spoke Arabic as their native language translated the tool into Arabic. The translators were health specialists familiar with the questionnaire's contents. Following the improvements, two multilingual translators reverse-translated the tool into English. Disagreements between the source and the back-translated version were investigated. The bilingual expert panel was revised as many times as necessary on the forward translated tool until a good version was created. This study used standard Arabic since it is the official language of 21 Arab nations in the Gulf countries and is widely taught, understood, and spoken by local Arabs [34].
2.6. Content Validity and Expert Assessment
Content validity refers to the extent to which the questions in a questionnaire indicate the overall theoretical concept the questionnaire should evaluate [34]. The content validity of our study was evaluated at several stages. The content validation form was designed to ensure that the review panel understood the assignment. Second, the review panel in charge of reviewing the questionnaire was chosen based on the reviewers' vaccination knowledge and is designed to examine "content validity" [34]. The content validity of our study was evaluated at several stages. The content validation form was designed to ensure that the review panel understood the assignment. Second, the review panel analysing the questionnaire was selected based on the reviewers' vaccination knowledge. The group included two reviewers: a consultant paediatrician and a biostatistics and pharmacoepidemiology expert.
2.7. Internal Reliability
A pilot sample of 30 participants was used to assess the reliability of the questions (test-retest). The items in this section had a Cronbach's alpha value of 0.91, indicating excellent reliability. The overall Cronbach’s alpha for parents’ hesitancy towards COVID-19 vaccination using V.H was 0.81. The Cronbach’s alpha for each of the domains “confidence “and “risks” were 0.77, 0.82, and 0.80, respectively (table 5). The mean score for all questions that showed positive and significant correlation with the mean score of each subscale indicated that the questionnaire had good convergent validity except for question9[32]. Therefore, scale 9 removed from analysis.
2.8. Statistical Analysis
Descriptive statistics were used to describe the data. Categorical variables are reported as frequencies and percentages. Differences between groups were analyzed using Pearson's Chi-squared test (Fisher's exact test was done for expected cells of <5). The mean and standard deviation were used to present the data for continuous variables, and the analysis was performed using Student's t-tests. The impact of demographic and clinical characteristics (age of the child, mother’s care (yes/no), sickle cell disease (yes/no), history of prior infection (yes/no)) on vaccine hesitancy (yes/no) was analyzed using multiple logistic regression using the simultaneous method. The goodness-of-fit of the multivariable logistic model was examined using the Hosmer and Lemeshow goodness-of-fit statistic [35]. A Confirmatory Factor Analysis (CFA) was used to examine model fit. Cronbach's alpha was used to measure the internal consistency of the questionnaires and was estimated to measure its homogeneity for item-to-total score correlations. Cronbach's alphas were computed for the questionnaire's subscales to measure their internal consistency.
Interpretation of Confirmatory Factor Analysis (CFA) and Exploratory Factor Analysis (EFA):
Principal component analysis (PCA) is a statistical technique that reduces the dimensionality of a dataset. PCA transforms the data into a new coordinate system where the variation in the data can be described with fewer dimensions than the initial data.
Confirmatory factor analysis (CFA) is a statistical method that tests whether measures of construct are consistent with a researcher's understanding of the nature of that construct. The objective of confirmatory factor analysis is to test whether the data fit a hypothesized measurement model.
Exploratory factor analysis (EFA) is a statistical method to identify factors based on data and to maximize the amount of variance explained. Here, the researcher is not required to have any specific hypotheses about how many factors will emerge, and what items or variables these factors will comprise.
The Kaiser-Meyer-Olkin (KMO) test is a measure of the adequacy of a set of variables for factor analysis. It compares the magnitudes of the observed correlation coefficients to the magnitudes of the partial correlation coefficients. The KMO test ranges from 0 to 1, where 0 indicates that the variables are not suitable for factor analysis and 1 indicates that they are perfectly suitable. A common rule of thumb is that a KMO value above 0.6 is acceptable, while a value below 0.5 is unacceptable. In this study, the KMO test values were found to be above 0.6 for all components, and therefore these variables are adequate for factor analysis.
The Bartlett test is a statistical method for testing the equality of variances among different groups of data. The null hypothesis of the Bartlett test is that all groups have the same variance. A p-value of less than 0.05 indicates strong evidence against the null hypothesis and suggests that there is significant heterogeneity of variances among the groups. In the present study, p-value is <0.001 that implies presence of significant variances among the groups.
A scree plot is a graphical representation of the variance explained by each principal component in a principal component analysis. It helps to determine the optimal number of principal components to retain for further analysis. A scree plot shows the eigenvalues of each principal component on the y-axis and the number of principal components on the x-axis. The plot typically shows a sharp decline in the eigenvalues, followed by a levelling off. The point where the slope of the curve changes is called the elbow point, and it indicates the number of principal components that capture most of the variation in the data. Here, in this analysis, the elbow point is around 2.5 which implies that there are approximately three principal components.
The chi-squared test indicates the difference between observed and expected covariance matrices. The smaller the value, better the model fit, and it signifies smaller difference between expected and observed covariance matrices.
The root mean square error of approximation (RMSEA) analyzes the discrepancy between the hypothesized model (with chosen parameter estimates) and the population covariance matrix. The RMSEA ranges from 0 to 1; with smaller values indicating better model fit. A value of .06 or less is indicative of acceptable model fit. Here; RMSEA value was found to be 0.052 which indicates a good model fit
The comparative fit index (CFI) analyses the model fit by examining the discrepancy between the data and the hypothesized model. Generally, a CFI value of 0.95 or higher is considered as an indicator of good fit. In this study, CFI was 0.970, and therefore indicates a good model fit.
In initial EFA, two items (scale 8 and 9) are trying to continuously improve the quality of survey. So, the authors repeated the EFA without including these items. The results of this analysis confirmed the two factors dimension’s structure theoretically defined in the research. The Kaiser-Meyer-Olkin test was 0.800. The seven scales explained a total of 61% of the variance among the items in the study. Bartlett’s test of sphericity proves to be significant, and all commonalities were over the value of 0.600. Three factors identified as part of this EFA aligned with the theoretical preposition in this research. Factor 1 includes scales 1 to 3 referring to trust. Factors 2 gathers scales 4 to 7 which represent safety and efficacy of covid_19 vaccines.
The "extent to which an instrument evaluates a construct of concern and is connected with evidence that measures other constructs in that domain and measures certain real-world criteria" [36] is described as construct validity. Content, criterion-related validity, and structural or factorial validity are used to determine it. Concurrent, convergent, and divergent validity were utilized as criterion-related validity indicators. Convergent validity was determined by examining the sub-scale correlation's inter-item and item-to-mean scores. The two subscales' discriminant (divergent) validity was assessed by computing the factor correlation matrix of the two subscales. The exploratory factor analysis (EFA) was intended to find the number of latent components for the nine items without making assumptions about the factor connections [37]. Before performing EFA, the Kaiser–Meyer–Olkin (KMO) sample adequacy assessment and Bartlett's sphericity test were conducted. KMO values higher than 0.50 and the significance of Bartlett's test of sphericity values (p 0.05) were used to evaluate the factorability of the data. [38].
The confirmatory factor analysis (CFA) that was performed based on participants aimed to measure how well the factor structure identified in the EFA fits the observed data. The overall model fit was evaluated using the comparative fit index (CFI), Tucker-Levis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). CFI and TLI 0.90, RMSEA 0.08, and SRMR 0.11 are considered adequate, while CFI and TLI 0.95, RMSEA 0.05, and SRMR 0.08 are considered good [39,40].
The two-tailed level of significance was set a priori at p < 0.05. Statistical analyses were performed using STATA version 16.1 (STATA Corporation, College Station, TX, USA).
2.9. Ethics
The Medical Research Ethics Committee approved this study (SQU-EC/ 575/2021, MREC #2640, date of approval 7th November 2021). All the parents provided written informed consent and de-identified data were collected and participation was completely voluntary.
3. Results
We approached a total of 447 potential respondents, of whom 63 refused to participate; therefore, we received 384 caregivers’ data for analysis, with a response rate of 86%. There was no missing data. Table 1 shows the characteristics of the respondents and their children. The survey included both fathers (n = 207; 48%) and mothers (n = 177; 46%). More than half of the participants were aged 35 years or older. The mean age of participants (caregivers) was 35 ±8 years, while the mean age of the children was 3 ±0.9 years. Analysis of age distribution among children demonstrated the largest prevalence of children aged <1 year (n = 25; 6.5%), followed by those aged 1–4 years (n = 101; 26%), 5–7 years (n = 116; 30%), and finally 8–11 years (n = 142; 37%). Approximately 285 (74%) of the study participants reported a history of chronic disease among their children. With regard to education, 47% (n = 181) of the participants had completed secondary school, while 41% (n = 151) had a BSc degree.

Table 1.
Respondents’ demographical data and vaccine hesitancy rate(N=384).
| Respondents’ Demographical Data | Data n(%) | Hesitant | P Value |
|---|---|---|---|
|
Children Age, year (Mean ± S.D.) Gender of children’s Male |
2.9 ± 0.94 168(44) |
116(44) |
|
| Female | 216 (56) | 148(56) | 0.912 |
|
Children’s Age group |
|||
|
<1 |
25 (6.5) |
20(80) |
0.227 |
|
1-4 |
101 (26.3) |
74(73) |
|
|
5-7 |
116 (30.2) |
80(69) |
|
|
8-11 |
142 (37) |
90(63) |
|
|
Relationship with child |
|||
|
Father |
207 (54) |
123(66) |
0.283 |
|
Mother |
177 (46) |
141(71) |
|
|
Age of participants, year Age group |
|||
|
18-24 |
24 (6) |
17(71) |
|
|
25-34 |
129 (34) |
94(73) |
0.744 |
|
35-44 |
192 (50) |
126(66) |
|
|
45-54 |
36 (9) |
25(69) |
|
|
≥ 55 |
3 (1) |
2(67) |
|
|
The educational level of the participants |
|||
|
Primary school |
15 (4) |
13(87) |
0.503 |
|
Secondary school |
181 (47) |
121(67) |
|
| BSc degree |
159 (41) |
110(69) |
|
| MSc degree |
25 (7) |
18(72) |
|
|
PhD |
4(1) |
2(50) |
|
Data were number (%).
Regarding the sample of children with chronic conditions, the mean age was 2.6 years, and more than half (56%) were female. The most common chronic medical conditions encountered were sickle cell disease (n = 50; 13% of all cases) and epilepsy (n = 32; 8% of all cases) (Table). Most children (n = 284; 73.90%) had a history of chronic disease, while 100 (26%) were healthy, with no history of chronic disease. Parents of children infected with COVID-19 reported a hesitancy rate of approximately 40% (n = 106). Children with chronic conditions such as depression and systemic lupus erythematosus had parents who showed high VH rates (100%). Furthermore, parents exhibited a high VH rate when their children had been diagnosed with diseases such as diabetes mellitus (n = 8; 89%), sickle cell disease (n = 36; 72%), and bone marrow or solid organ transplantation (n = 21; 70%). There was less vaccine hesitancy reported. VH was 33% and 38% in parents whose children had cardiovascular disease or thalassemia, respectively. Table 1 shows the parents' responses to each item on the vaccine statement regarding hesitancy. In particular, half of the parents (n = 187; 48%) agreed strongly or agreed that a vaccine is an excellent approach to protecting their child from COVID-19. Moreover, almost half of the parents (n = 212; 55%) agreed strongly or agreed that they were concerned that their children would have a serious vaccine side effect. Furthermore, almost three-fourths (n = 284; 74%) agreed or strongly agreed that they trust and rely on information they received regarding COVID-19 vaccination in children.
Source of COVID-19 Information
Interestingly, 56% of parents relied on information regarding COVID-19 and its vaccines mostly from health care professionals, followed by WhatsApp (48%),the Internet (47%), Twitter (20%), and Facebook (16%) (Figure2).
Figure 2 shows the sources of information selected by parents and guardians when deciding whether or not to vaccinate their children against COVID-19. The majority of parents depended on healthcare organizations (n = 219; 57%), WhatsApp (n = 185; 48%), and the Internet (n = 180; 47%) for COVID-19 vaccination information.
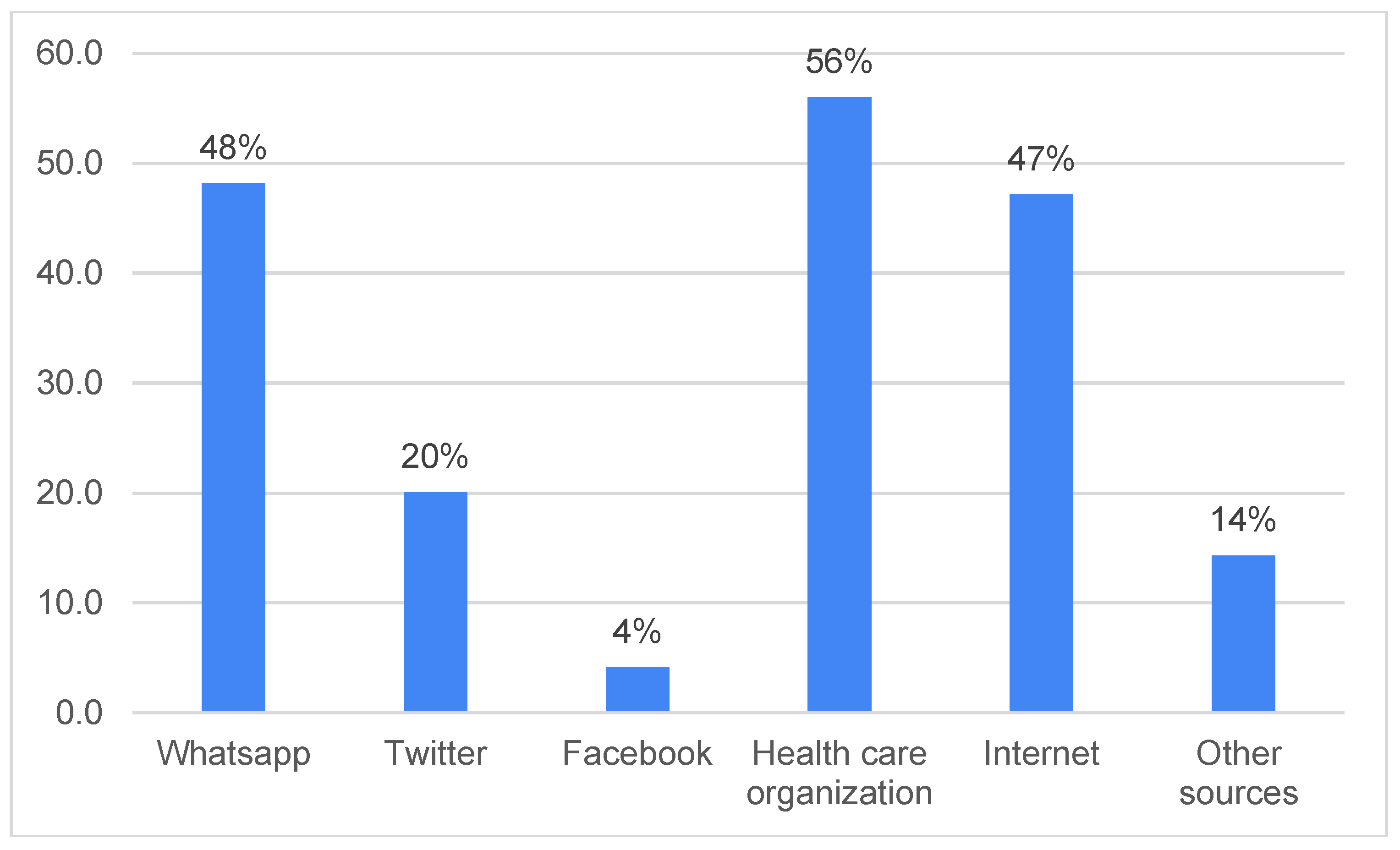
Figure 2.
Parent’s sources of COVID-19 information.
Table 1 shows the incidence of VH and parents' thoughts regarding childhood immunization. The incidence of VH for children's COVID-19 immunization was 69%, and mothers were more hesitant than fathers (71% vs. 66%; Table 1). Table 2 lists pediatric diseases and the prevalence of VH, and shows that there was no statistically significant difference in the VH rate between children with and without chronic diseases (25% vs. 27%; p = 0.733). Table 3 shows that almost one-third of the parents believed that immunizations were essential for their children. In addition, approximately 62% (n = 238) of parents were still determining if they agreed or disagreed with the statement that newer vaccines such as the COVID-19 vaccine had more risks than older vaccines.
Table 2.
Children's diseases and the incidence of vaccine hesitancy.
| Children's Diseases | Hesitant N (%) |
Non Hesitant N(%) |
P-Value |
|---|---|---|---|
| Diabetes Mellitus (DM) |
8(89) | 1(11) | 0.187 |
| cystic fibrosis | 5(56) | 4(44) | 0.387 |
| Sickle cell disease |
36(72) | 14(28) | 0.595 |
| Bone marrow or solid organ transplantation |
21(70) | 9(30) | 0.878 |
| Genetic/metabolic disorders |
11(64) | 6(35) | 0.713 |
| Systemic lupus erythematosus (SLE) |
2(100) | 0(0) | 0.339 |
| Cardiovascular diseases |
2(33) | 4(67) | 0.059 |
| Rheumatoid arthritis |
3(75) | 1(25) | 0.786 |
| Nephrotic syndrome | 3(43) | 4(57) | 0.136 |
| Thyroid disorder |
7(87) | 1(13) | 0.248 |
| Asthma |
14(64) | 8(36) | 0.594 |
| Thalassemia |
6(38) | 10(62) | 0.006 |
| Hemophilia |
1(25) | 3(75) | 0.058 |
| Blood cancer | 20(67) | 10(33) | 0.798 |
| Epilepsy |
26(81) | 6(19) | 0.111 |
| Depression |
2(100) | 0(0) | 0.339 |
| Attention deficit hyperactivity disorder |
6(75) | 2(25) | 0.700 |
| Other chronic diseases | 17(59) | 12(41) | 0.221 |
| Non chronic disease | 74(75). | 25 (25) | 0.135 |
Table 3.
Parental vaccine hesitancy: 9 statements and responses (N=384).
| Questions | Strongly agree | Agree | Strongly disagree | Disagree | Unsure |
|---|---|---|---|---|---|
| 1- Getting the vaccine is an excellent way to protect my child from COVID-19 disease | 55 (14) | 132 (34) | 28 (7) | 48 (13) | 121 (32) |
| 2- Having my child vaccinated is important for the health of others in my community | 94 (24) | 144 (38) | 14 (4) | 42 (11) | 90( 23) |
| 3- The information I receive about the COVID -19 vaccine from my child's healthcare provider is reliable and trustworthy | 74 (19) | 210 (55) | 3 (1) | 15 (4) | 82 (21) |
| 4- New vaccines like COVID -19 vaccines carry more risks than older vaccines | 35 (9) | 71 (19) | 9 (2) | 31 (8) | 238 ( 62) |
| 5- I am concerned about the severe side effects of the COVID -19 vaccine. | 86 (22) | 126 (33) | 10 (3) | 51 (13) | 111 (29) |
| 6- I think the COVID -19 vaccines might cause short-term problems for my child, like fever, pain at the injection site, and fatigue. |
64 (17) | 150 (39) | 7 (2) | 39 (10) | 124 (32) |
| 7- I think the COVID -19 vaccine might cause long-term health problems for my child | 37 (10) | 70 (18) | 14 (4) | 76 (20) | 187 (48) |
| 8- I think my child will not get sick with COVID-19 illness even if they do not get the COVID -19 vaccines | 24 (6) | 78( 20) | 33 (9) | 73( 19) | 176 (46) |
| 9- The COVID -19 illnesses could make my child very sick. | 37 (10) | 71 (19) | 14 (4) | 76 (20) | 186 (47) |
*positive statements(1, 2, 3and 9), negative Statements(4, 5, 6, 7and 8).
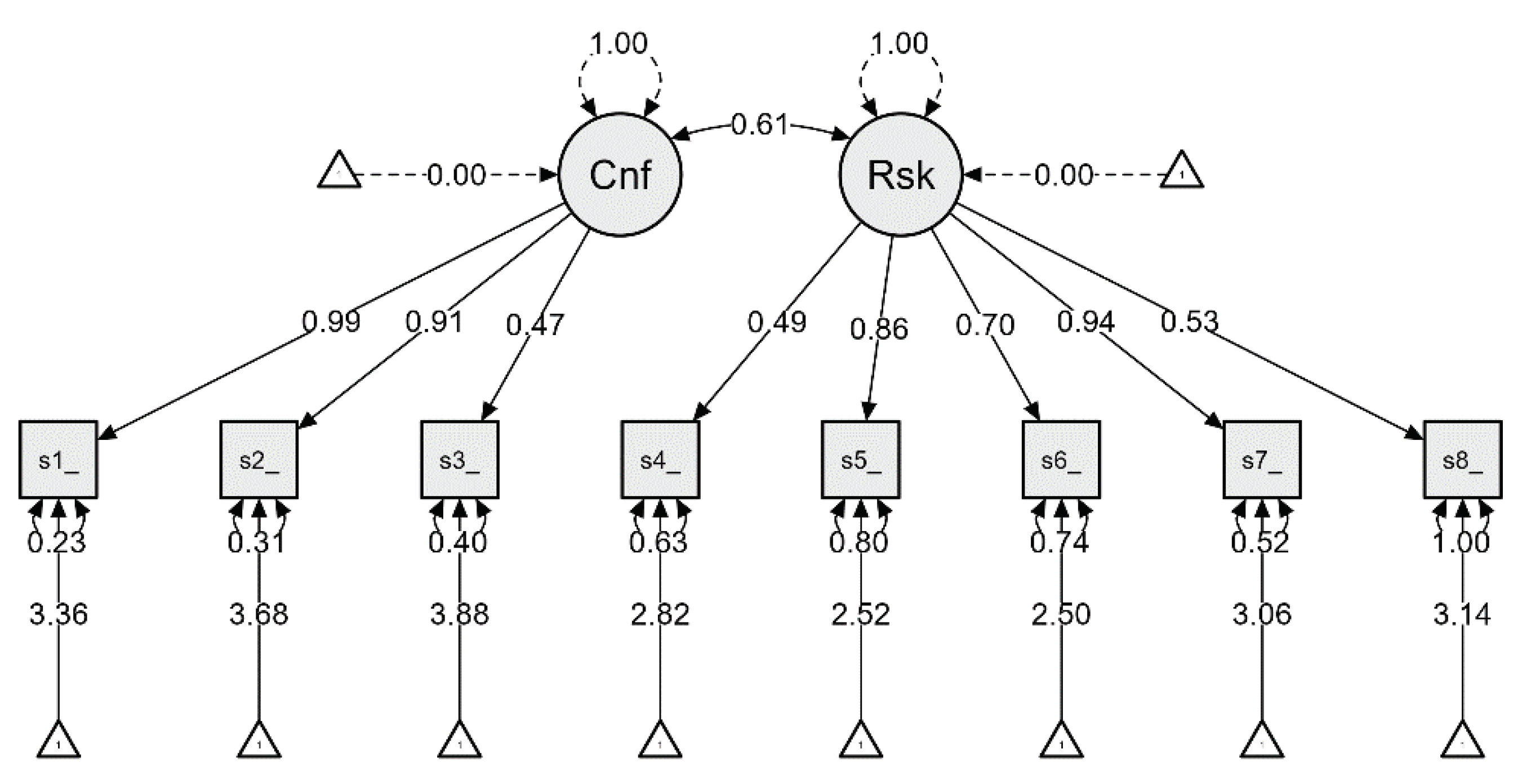
Factorial Validity
Eigenvalues showed that four factors were >1, with a total variance of 61% (figure1). As shown by Table 10, the two-factor model yields good absolute and relative fit indexes. We specifically used the following fit indexes: Chi-square, Normed Fit Index (NFI), Non-Normed Fit Index (NNFI or TLI), table 9 shows Comparative Fit Index (CFI), the Akaike Information Criteria (AIC), and Root Mean Square Error of Approximation (RMSEA). Furthermore, an EFA revealed that the two factors explained 61% of the scale's total variance. The better the model fits the data, the lower the values of the Chi-square and RMSEA indexes, and the higher the values of the NFI, CFI, and TLI indexes. To be more specific, as a general rule, TLI 0.95, CFI 0.95, and RMSEA 0.06 indicate a good fit to the data [41].
An EFA was performed using confirmatory factor analysis, and varimax rotation. The minimum factor loading criteria was set to 0.5. Additionally, the commonality of the scale, which indicates the amount of variance in dimension, was assessed to ensure an acceptable level of explanation. The results show that all commonalities were over 0.500.
Figure 1.
Plots. Model plot. # Factors: Factor1 =~ lambda_1_1*scale1_score + lambda_1_2*scale2_score + lambda_1_3*scale3_score. Factor2 =~ lambda_2_1*scale4_score + lambda_2_2*scale5_score + lambda_2_3*scale6_score + lambda_2_4*scale7_score + lambda_2_5*scale8_score.
Figure 1.
Plots. Model plot. # Factors: Factor1 =~ lambda_1_1*scale1_score + lambda_1_2*scale2_score + lambda_1_3*scale3_score. Factor2 =~ lambda_2_1*scale4_score + lambda_2_2*scale5_score + lambda_2_3*scale6_score + lambda_2_4*scale7_score + lambda_2_5*scale8_score.
An important step involved weighing the overall significance of the correlation matrix through Bartlett's test of sphericity. This provides a measure of the correlation's statistical probability that the correlation matrix has significant correlations among some of its components. The results were significant, as follows: X2 (n = 384) = 993.2 (p 0.001), which indicates its suitability for factor analysis (Table6). Furthermore, the Kaiser-Meyer-Olkin test measure of sampling adequacy (MSA), which indicates the appropriateness of data for factor analysis, was 0.800 (Table5). In this regard, data with an MSA value above 0.800 is considered appropriate for factor analysis. Finally, the factors solution derived from this analysis yielded three factors for the scale, which accounted for 61% of the variations in the data (Table 9).
In this initial EFA, two items (i.e., scales scale 8and 9) are continuously trying to improve the survey's level of quality. Therefore, the authors repeated the EFA without including these items. The results of this analysis confirmed the two factors (dimensions and structure) theoretically defined in the research (see Table6&7). The Kaiser-Meyer-Olkin test result was 0.800, and the seven scales explained a total of 61%(table 9) of the variance among the items in the study. Bartlett's sphericity test proved significant, as all commonalities were over 0.500 (see Table5). In fact, two factors identified as part of this EFA align with the theoretical proposition in this research. Factor 1 includes scales 1–3, referring to Confidence, while factor 2 gathers scales 4–7, representing risks of the COVID-19 vaccine (see tables 7&8).
Table 4 shows the relationship between the underlying factors and VH in children using simple logistic regression. The following variables were found to be non-significant with regard to VH: mothers were more hesitant than fathers (odds ratio (OR) = 0.78, 95% confidence interval (CI) = 0.50–0.1.23; p = 0.283), and parents who received the COVID-19 vaccination and had children aged 1–4 years (OR = .269; 95% CI: .3236–2.9), 5–7 years (OR = .358; 95% CI: .4202-1.6.4), and 8–11 years (OR = .643; 95% CI: .3154–1.4;23 p = 0.118).
Table 4.
Multivariable analysis of demographic and clinical characteristics on parental vaccine hesitancy.
Table 4.
Multivariable analysis of demographic and clinical characteristics on parental vaccine hesitancy.
| Characteristic | Odds Ratio (95% CI) | P Value |
|---|---|---|
| Age group of child (years) | ||
| <1 | 1.000 (reference) | |
| 1–4 | 0.116 (0.044–0.306) | 0.001 |
| 5–7 | 0.685 (0.312–1.504) | 0.346 |
| 8–11 | 0.988 (0.459–2.128) | 0.975 |
| Relationship of respondent to the child | ||
| Father | 1.000 (reference) | |
| Mother | 0.451 (0.240–0.848) | 0.013 |
| Sickle cell disease | 0.629 (0.345–1.149) | 0.132 |
| Has your child ever been infected | 1.453 (0.752–2.808) | 0.266 |
Table 5.
Means, item-to-total correlations, and Cronbach’s alphas after removing specific scale 9 from the Arabic version.
Table 5.
Means, item-to-total correlations, and Cronbach’s alphas after removing specific scale 9 from the Arabic version.
| If Item Dropped | ||||||
|---|---|---|---|---|---|---|
| Item | Cronbach's α | Item-Rest Correlation | Mean | Sd | ||
| Confidence scale1_score |
0.778 |
0.659 |
3.359 |
1.099 |
||
| scale2_score | 0.788 | 0.585 | 3.682 | 1.071 | ||
|
scale3_score Risks |
0.808 | 0.455 | 3.878 | 0.787 | ||
| scale4_score | 0.810 | 0.458 | 2.818 | 0.930 | ||
| scale5_score | 0.792 | 0.580 | 2.516 | 1.245 | ||
| scale6_score | 0.805 | 0.493 | 2.497 | 1.110 | ||
| scale7_score | 0.779 | 0.669 | 3.057 | 1.182 | ||
| scale8_score | 0.814 | 0.411 | 3.138 | 1.133 | ||
| Point estimate | 0.818 | 0.360 | 3.118 | 0.715 | ||
| 95% CI lower bound | 0.789 | 0.318 | 3.047 | 0.688 | ||
| 95% CI upper bound | 0.844 | 0.400 | 3.190 | 0.770 | ||
Table 6.
sampling adequacy & sphericity test.
| 1Kaiser-Meyer-Olkin Test | MSA | |
|---|---|---|
| Overall MSA | 0.800 | |
| scale1_score | 0.755 | |
| scale2_score | 0.726 | |
| scale3_score | 0.882 | |
| scale4_score | 0.863 | |
| scale5_score | 0.832 | |
| scale6_score | 0.805 | |
| scale7_score | 0.841 | |
|
Bartlett's test Χ² |
993 | |
| P | < | 0.001 |
Table 7.
Factor Loadings & Structure Matrix.
| Factor 1 | Factor 2 | Uniqueness | |
|---|---|---|---|
| scale2_score | 0.885 | 0.182 | |
| scale1_score | 0.796 | 0.253 | |
| scale3_score | 0.585 | 0.631 | |
| scale5_score | 0.711 | 0.443 | |
| scale7_score | 0.684 | 0.431 | |
| scale6_score | 0.645 | 0.572 | |
| scale4_score | 0.491 | 0.728 | |
| Factor Loadings (Structure Matrix) | |||
| scale1_score | 0.796 | ||
| scale2_score | 0.885 | ||
| scale3_score | 0.585 | ||
| scale4_score | 0.491 | ||
| scale5_score | 0.711 | ||
| scale6_score | 0.645 | ||
| scale7_score | 0.684 | ||
| Note. Applied rotation method is varimax. | |||
Table 8.
Factor loadings.
| 95% Confidence Interval | ||||||||
|---|---|---|---|---|---|---|---|---|
| Factor | Indicator | Symbol | Estimate | Std. Error | z-value | P | Lower | Upper |
| Confidence | scale1_score | λ11 | 0.987 | 0.048 | 20.578 | < .001 | 0.893 | 1.081 |
| scale2_score | λ12 | 0.915 | 0.048 | 19.206 | < .001 | 0.821 | 1.008 | |
| scale3_score | λ13 | 0.471 | 0.038 | 12.288 | < .001 | 0.396 | 0.547 | |
| Risks | scale4_score | λ21 | 0.487 | 0.049 | 10.005 | < .001 | 0.391 | 0.582 |
| scale5_score | λ22 | 0.865 | 0.061 | 14.065 | < .001 | 0.744 | 0.985 | |
| scale6_score | λ23 | 0.701 | 0.056 | 12.516 | < .001 | 0.591 | 0.811 | |
| scale7_score | λ24 | 0.935 | 0.056 | 16.598 | < .001 | 0.825 | 1.046 | |
| scale8_score | λ25 | 0.531 | 0.060 | 8.828 | < .001 | 0.413 | 0.649 | |
Table 9.
Factor Covariances.
| 95% Confidence Interval | ||||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | z-Value | p | Lower | Upper | |||
| Confidence | ↔ | Risks | 0.611 | 0.043 | 14.356 | < .001 | 0.527 | 0.694 |
Table 10.
Confirmatory Factor Analysis model fit.
| Chi-Square P Value 0.001 | X2/df | CFI | RMSEA | SRMR | TLI |
| Suggested fit model (Ref32) | 2 - 5 | ≥ 0.95 | ≤0.06 | ≤0.05 | ≥0.95 |
| 9-item parental COVID -19 VHS (full sample ) | 2.7 | 0.970 | 0.066 | 0.035 | 0.956 |
Abbreviations: Chi-Square: X2, degree of freedom:df, Comparative Fit Index: CFI, Root Mean Square Error of Approximation: RMSEA, Standardized root mean square residual: SRMR, Tucker-Lewis Index: TLI.
4. Discussion
To date, a significant amount of data has been published on parental COVID-19 VH. [27,42,43,44,45,46,47,48]. Therefore, data on COVID-19 VH are valuable in guiding the planning of future COVID-19 immunization strategies for children..
Vaccination against COVID-19 is currently the most effective method for minimizing the burden of the COVID-19 pandemic. Our survey at SQUH found that most caregivers were hesitant about vaccinating their children against COVID-19 [49].
We found that among the surveyed parents, mostly mothers (77%) were hesitant to vaccinate their children against COVID-19, supporting the idea that women are more reluctant than men regarding vaccination [50,51,52]. Furthermore, men are more likely to be vaccinated since they are at greater risk of severe COVID-19 consequences; therefore, they have a higher perception of risk for themselves and their children. Additionally, women seem to experience more adverse events after vaccination, causing more concern about the possibility that it can affect their children and thereby increasing hesitancy [51,51]. Notably, we also showed that reluctant parents lacked confidence in vaccination since they were worried about their side effects. Most studies show that fear of side effects and safety remains the primary reason for parents to decide to not vaccinate their children [22,52,53].
Few studies have evaluated VH regarding COVID-19 vaccination in the pediatric population, and the results are not consistent. For example, a Chinese study reported a VH of 72.6%[54], while Australian researchers reported a VH of 75.8% [55] and a United Kingdom study reported a VH of 48.2%, with 40.9% of the parents/guardians responding that they were "unsure but leaning towards yes [14]. This variation in rates is not surprising given that the VH phenomenon is considered complicated because it is influenced by various demographic, economic, cultural, and regional factors [56].
One possible explanation for our study's higher overall rate of VH is that younger parents and guardians are aware of the low risk of severe COVID-19 in children. This assumption is consistent with previous studies, which showed that parents or guardians aged >50 years have greater vaccination confidence [36]. Furthermore, the incidence of VH was much higher in children aged younger than 11 years, which affected their parents' perspectives regarding vaccination.
Our study had some limitations. First, this was a single-center study from a tertiary care centre where patients come from all over the country. Additionally, the case mix and severity of the children might not be representative of the country. Moreover, since this was a retrospective cross-sectional study, its design limits its ability to establish a causal-effect relationship. The design could also have led to biases, including social desirability bias, self-selection bias, non-response bias, and residual compounding. Therefore, future research should examine parents' VH in different locations in Oman. In addition, regular childhood immunizations such as the influenza vaccine were not recorded for this age group of children as a control comparison, and the relationship between parents’ and healthcare workers’ VH was also not evaluated. Finally, the strengths of our study include our use of a validated questionnaire to assess VH and obtaining a high response rate [33].
5. Conclusions
In our study, parents' hesitancy toward giving their children COVID-19 vaccinations was higher than that reported in previous studies. Additionally, the female sex and children's age were factors that increased the risk of VH. Parental VH must be urgently addressed to improve the vaccine uptake in guardians of children attending pediatric outpatient departments. Therefore, effective health education and awareness campaigns should focus on this age group to help parents immunize their kids against SARS-CoV-2, which could decrease the spread of the virus in individuals with no symptoms and hopefully strengthen their immune systems.
Author Contributions
Conceptualization, Moataz Mohamed Hassan, Laila Al Yazidi, Nagi Elsidig; Methodology, .; Software, Moataz Mohamed Hassan; Validation, Laila Al Yazidi, Nagi Elsidig, Ibrahim Al-Zakwani; Formal analysis, Ibrahim Al-Zakwani, Moataz Mohamed Hassan; Investigation, Moataz Mohamed Hassan, Laila Al Yazidi, Nagi Elsidig; Resources, Moataz Mohamed Hassan, Laila Al Yazidi, Nagi Elsidig; Data collection, Moataz Mohamed Hassan, Laila Al Yazidi, Nagi Elsidig, Ibrahim Al-Zakwani, Mohamed Al Falahi, Najah Salmi, Yahya Al-Jaffari1, Labiba Al-Amri, Hiam Zeidan; Writing—original draftFunding: None.
Institutional Review Board Statement
All subjects gave informed consent for inclusion before participating in the study. The study was conducted under the Declaration of Helsinki, and the protocol was approved by the Medical Research Ethics Committee, College of Medicine and Health Sciences, Sultan Qaboos University (SQU-EC/ 575/2021, MREC #2640, date of approval 7 November 2021)..
Informed Consent Statement
Informed consent was obtained from all participants.
Data Availability Statement
Data available from the corresponding author on reasonable request.
Acknowledgments
We thank all pediatric doctors and nurses for their cooperation. We also thank the parents who filled out the survey.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Rappuoli, R.; Santoni, A.; Mantovani, A. Vaccines: An achievement of civilization, a human right, our health insurance for the future. J. Exp. Med. 2019, 216, 7–9. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard [Internet]. [cited 2023 Feb 22]. Available online: https://covid19.who.int.
- Yang, Y.; Peng, F.; Wang, R.; Yange, M.; Guan, K.; Jiang, T.; et al. The deadly coronaviruses: The 2003 SARS pandemic and the 2020 novel coronavirus epidemic in China. J. Autoimmun. 2020, 109, 102434. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. Oslo Nor. 1992. 2020, 109, 1088–1095. [Google Scholar]
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; et al. systematic review and meta-analysis of children with coronavirus disease 2019 (COA VID-19). J. Med. Virol. 2021, 93, 1057–1069. [Google Scholar] [CrossRef]
- Al Yazidi, L.S.; Al Hinai, Z.; Al Waili, B.; Al Hashami, H.; Al Reesi, M.; Al Othmani, F.; et al. Epidemiology, characteristics and outcome of children hospitalized with COVID-19 in Oman: A multicenter cohort study. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 104, 655–660. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.I.; et al. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child. Adolesc Health. 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; et al. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. HEPAC Health Econ. Prev. Care 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J. Sydney Health Literacy Lab COVID-19 group. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2021, 21, 318–319. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Al-Marshoudi, S.; Al-Balushi, H.; Al-Wahaibi, A.; Al-Khalili, S.; Al-Maani, A.; Al-Farsi, N.; et al. Knowledge, Attitudes, and Practices (KAP) toward the COVID-19 Vaccine in Oman: A Pre-Campaign Cross-Sectional Study. Vaccines 2021, 9, 602. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Parra Cotanda, C.; Brown, J.C.; Klein, E.J.; et al. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; et al. Would Parents Get Their Children Vaccinated Against SARS-CoV-2? Rate and Predictors of Vaccine Hesitancy According to a Survey over 5000 Families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, S.; Zhao, S.; Wang, J.; Han, Y.; Dong, S.; et al. Vaccine Hesitancy: COVID-19 and Influenza Vaccine Willingness among Parents in Wuxi, China-A Cross-Sectional Study. Vaccines 2021, 9, 342. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Temsah, M.H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; et al. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef] [PubMed]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammed, O.A. Parents’ Hesitancy to Vaccinate Their 5-11-Year-Old Children Against COVID-19 in Saudi Arabia: Predictors From the Health Belief Model. Front. Public Health 2022, 10, 842862. [Google Scholar] [CrossRef] [PubMed]
- Al-Khlaiwi, T.; Meo, S.A.; Almousa, H.A.; Almebki, A.A.; Albawardy, M.K.; Alshurafa, H.H.; et al. National COVID-19 Vaccine Program and Parent’s Perception to Vaccinate Their Children: A Cross-Sectional Study. Vaccines 2022, 10, 168. [Google Scholar] [CrossRef]
- Aldakhil, H.; Albedah, N.; Alturaiki, N.; Alajlan, R.; Abusalih, H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers’ intention to vaccinate their children against COVID-19 in Saudi Arabia. J. Infect. Public Health 2021, 14, 1497–15504. [Google Scholar] [CrossRef]
- Chen, F.; He, Y.; Shi, Y. Parents’ and Guardians’ Willingness to Vaccinate Their Children against COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 179. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlôt, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef]
- Almansour, A.; Hussein, S.M.; Felemban, S.G.; Mahamid, A.W. Acceptance and hesitancy of parents to vaccinate children against coronavirus disease 2019 in Saudi Arabia. PloS One 2022, 17, e0276183. [Google Scholar] [CrossRef]
- Musa, S.; Dergaa, I.; Abdulmalik, M.A.; Ammar, A.; Chamari, K.; Saad, H.B. BNT162b2 COVID-19 Vaccine Hesitancy among Parents of 4023 Young Adolescents (12-15 Years) in Qatar. Vaccines 2021, 9, 981. [Google Scholar] [CrossRef] [PubMed]
- Khatatbeh, M.; Albalas, S.; Khatatbeh, H.; Momani, W.; Melhem, O.; Al Omari, O.; et al. Children’s rates of COVID-19 vaccination as reported by parents, vaccine hesitancy, and determinants of COVID-19 vaccine uptake among children: a multi-country study from the Eastern Mediterranean Region. BMC Public Health 2022, 22, 1375. [Google Scholar] [CrossRef] [PubMed]
- McGregor, S.; Goldman, R.D. Determinants of parental vaccine hesitancy. Can. Fam. Physician Med. Fam. Can. 2021, 67, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Zakhour, R.; Tamim, H.; Faytrouni, F.; Khoury, J.; Makki, M.; Charafeddine, L. Knowledge, attitude and practice of influenza vaccination among Lebanese parents: A cross-sectional survey from a developing country. PloS One 2021, 16, e0258258. [Google Scholar] [CrossRef] [PubMed]
- Alsuwaidi, A.R.; Elbarazi, I.; Al-Hamad, S.; Aldhaheri, R.; Sheek-Hussein, M.; Narchi, H. Vaccine hesitancy and its determinants among Arab parents: a cross-sectional survey in the United Arab Emirates. Hum. Vaccines Immunother. 2020, 16, 3163–3169. [Google Scholar] [CrossRef]
- ElSayed, D.A.; Bou Raad, E.; Bekhit, S.A.; Sallam, M.; Ibrahim, N.M.; Soliman, S.; et al. Validation and Cultural Adaptation of the Parent Attitudes about Childhood Vaccines (PACV) Questionnaire in Arabic Language Widely Spoken in a Region with a High Prevalence of COVID-19 Vaccine Hesitancy. Trop. Med. Infect. Dis. 2022, 7, 234. [Google Scholar] [CrossRef]
- Helmkamp, L.J.; Szilagyi, P.G.; Zimet, G.; Saville, A.W.; Gurfinkel, D.; Albertin, C.; et al. A validated modification of the vaccine hesitancy scale for childhood, influenza and HPV vaccines. Vaccine 2021, 39, 1831–1839. [Google Scholar] [CrossRef]
- Abushariah, M.A.A.M.; Ainon, R.N.; Zainuddin, R.; Alqudah, A.A.M.; Ahmed, M.E.; Khalifa, O.O. Modern standard Arabic speech corpus for implementing and evaluating automatic continuous speech recognition systems. J. Frankl. Inst. 2012, 349, 2215. [Google Scholar] [CrossRef]
- Liu, D.; Shepherd, B.E. Discussion on ‘Assessing the goodness of fit of logistic regression models in large samples: A modification of the Hosmer-Lemeshow test’ by Giovanni Nattino, Michael L. Pennell, and Stanley Lemeshow. Biometrics 2020, 76, 572–574. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- Watkins, M.W. Exploratory factor analysis: A guide to best practice. J. Black Psychol. 2018, 44, 219–246. [Google Scholar] [CrossRef]
- Park, D.I. Development and Validation of a Knowledge, Attitudes and Practices Questionnaire on COVID-19 (KAP COVID-19). Int. J. Environ. Res. Public Health 2021, 18, 7493. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bagateli, L.E.; Saeki, E.Y.; Fadda, M.; Agostoni, C.; Marchisio, P.; Milani, G.P. COVID-19 Vaccine Hesitancy among Parents of Children and Adolescents Living in Brazil. Vaccines 2021, 9, 1115. [Google Scholar] [CrossRef]
- Willis, D.E.; Andersen, J.A.; Bryant-Moore, K.; Selig, J.P.; Long, C.R.; Felix, H.C.; et al. COVID-19 vaccine hesitancy: Race/ethnicity, trust, and fear. Clin. Transl. Sci. 2021, 14, 2200–2207. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; et al. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel. Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef] [PubMed]
- Huynh, G.; Nguyen, H.T.N.; Van Tran, K.; Le An, P.; Tran, T.D. Determinants of COVID-19 vaccine hesitancy among parents in Ho Chi Minh City, Vietnam. Postgrad Med. 2022, 134, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Huang, H.; Shang, J.; Xie, Z.; Jia, R.; Lu, G.; et al. Willingness and influential factors of parents of 3-6-year-old children to vaccinate their children with the COVID-19 vaccine in China. Hum. Vaccines Immunother. 2021, 17, 3969–3974. [Google Scholar] [CrossRef] [PubMed]
- Samannodi, M.; Alwafi, H.; Naser, A.Y.; Alabbasi, R.; Alsahaf, N.; Alosaimy, R.; et al. Assessment of caregiver willingness to vaccinate their children against COVID-19 in Saudi Arabia: a cross-sectional study. Hum. Vaccines Immunother. 2021, 17, 4857–4864. [Google Scholar] [CrossRef] [PubMed]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PloS One. 2021, 16, e0250123. [Google Scholar] [CrossRef] [PubMed]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. Lancet Lond. Engl. 2020, 396, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- Klein, S.L.; Marriott, I.; Fish, E.N. Sex-based differences in immune function and responses to vaccination. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Skeens, M.A.; Hill, K.; Olsavsky, A.; Buff, K.; Stevens, J.; Akard, T.F.; et al. Factors affecting COVID-19 vaccine hesitancy in parents of children with cancer. Pediatr. Blood Cancer 2022, 69, e29707. [Google Scholar] [CrossRef]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; et al. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2021, 21, e110. [Google Scholar] [CrossRef] [PubMed]
- Zakar, R.; Momina, A.U.; Shahzad, S.; Hayee, M.; Shahzad, R.; Zakar, M.Z. COVID-19 Vaccination Hesitancy or Acceptance and Its Associated Factors: Findings from Post-Vaccination Cross-Sectional Survey from Punjab Pakistan. Int. J. Environ. Res. Public Health 2022, 19, 1305. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



