
Submitted:
14 February 2024
Posted:
15 February 2024
You are already at the latest version
Abstract
Background and objective: Obesity is a growing global epidemic. The composition of the intestinal microbiota can be influenced by several factors. Studies highlight the role of intestinal bacteria in the pathophysiology of obesity. So, the objective of this study was to investigate whether the use of probiotics, together with healthy lifestyle habits, contributes to weight reduction in obese indi-viduals by analyzing the intestinal microbiota profile. Methods: A prospective study was carried out with 45 adults with obesity. Participants underwent guidance on healthy lifestyle habits, re-ceived a probiotic component containing different microbiological strains and were followed for 60 days. Clinical parameters, body composition, biochemical analysis and intestinal microbiota assessment were performed before and after treatment. After 60 days, it was observed that the bacterial strains present in the probiotic were present in the patients' intestinal microbiota. Par-ticipants also showed improvements in physical activity, sleep quality, anxiety management, as well as changes in some eating habits, such as a reduction in the consumption of processed foods and a significant increase in water intake. Results: A reduction in BMI, fasting glucose, insulin, HOMA-IR, LDL cholesterol and triglycerides was observed, in addition to an increase in HDL cholesterol, improvement in bowel movement frequency and stool consistency. Analysis of the intestinal microbiota revealed an increase in microbial diversity and a better balance between the bacterial phyla Firmicutes and Bacteroidetes. Conclusions: The changes related to improving the composition of the intestinal microbiota, dietary habits, increased physical activity, reduced anxiety, and better sleep quality have significantly contributed to weight loss and improvements in physiological parameters in obese individuals.
Keywords:
intestinal microbiota
; probiotics
; obesity
; lifestyle habits
; weight loss
1. Introduction
Obesity is a growing global epidemic [1], associated with a wide range of chronic diseases, such as type 2 diabetes, high blood pressure, dyslipidemia, hepatic steatosis, obstructive sleep apnea, mood disorders and musculoskeletal disorders, in addition to certain types of cancer [2]. These comorbidities represent a significant public health challenge, with negative consequences on the quality of life and life expectancy of affected individuals [1].
According to the WHO, in 2016, 39% of the global adult population was overweight [3,4] and 13% were considered obese [4]. Between 1980 and 2023, the prevalence of obesity in the world population has tripled [1]. In Brazil, the prevalence of obesity in the adult population increased from 11.8% in 2006 to 22.4% in 2021, according to the Vigitel survey (Surveillance of chronic diseases by telephone survey) carried out by the Ministry of Health [5].
Obesity is characterized by an energy imbalance resulting from several factors, such as dysregulated appetite and dysfunction in food reward signaling [1,6]. These changes trigger multiple biological, histological, immunological and metabolic changes in adipose, liver, muscle, brain and intestinal tissues [4,7]. It has been observed that the gut microbiome, which consists of trillions of microorganisms, plays an important role in host physiology and is closely linked to obesity [3]. The intestinal microbiome interacts in a complex way with the body, and an imbalance in this microbial community can contribute to the development and progression of obesity [7].
Through advanced omics technologies, such as metagenomics, metatranscriptomics, metaproteomics and metabolomics, we can analyze in detail this interaction between the microbiome and the host [3,4]. Studies have revealed that healthy individuals have greater bacterial diversity compared to those with high adiposity, insulin resistance and dyslipidemia, common characteristics in obese patients [7,8]. Furthermore, patients with obesity exhibit a reduced count of bacterial species, indicating a relatively impoverished intestinal microbiota [4,9]. This reduction is associated with a lower proportion of microorganisms from the Bacteroidetes phylum and higher levels of the Firmicutes phylum [4].
However, the composition of the intestinal microbiota can be influenced by several factors [10]. Healthy eating habits [11,12,13,14], encouraging moderate physical activity [14], careful sleep routine [13] and anxiety management [15] were associated with beneficial changes in the intestinal microbiota, contributing to weight reduction [16].
Studies highlight the role of intestinal bacteria in the pathophysiology of obesity, mainly through involvement in low-grade inflammation associated with intestinal dysbiosis [4]. This occurs when the homeostasis of intestinal bacteria is disturbed leading to changes in the composition, function and distribution of microorganisms in the intestine, resulting in a state that predisposes the emergence of intestinal pathogenic conditions [12].
Overall, this imbalance increases Firmicutes species such as Agathobacter rectalis, Blautia coccoides, Limosilactobacillus reuteri, Hathewaya histolytica, and Staphylococcus aureus [3,4]. On the other hand, there are reports of significant reduction in the relative abundance of several members of the phylum Bacteroidetes, such as (Prevotella and Alistipes) in addition to Faecalibacterium prausnitzii, Lactiplantibacillu plantarum, Lacticaseibacillus paracasei, Lacticaseibacillus rhamnosus and phylum Verrucomicrobia (Akkermansia muciniphila) [17,18].
In addition to positive lifestyle habit adjustments, there is a growing body of evidence that probiotics improve, maintain, or restore gut microbiota, thus opening the door to innovative maneuvers targeting microbiota architecture and diversity [3]. Research shows that several probiotics, used alone or in symbiotic combinations, can exert anti-obesity effects through species- and strain-specific mechanisms, such as modulation of the intestinal microbiota, greater satiety, and reduced insulin resistance [4,19,20,21].
Probiotics act through three main mechanisms of action in the treatment of obesity: antagonistic effects on the growth of pathogenic microorganisms and competitive adhesion to the intestinal mucosa and epithelium (antimicrobial activity), increased production of the intestinal mucus layer and reduced intestinal permeability (barrier function) and modulation of the gastrointestinal immune system (immunomodulation) [22].
The probiotic bacteria strains Bifidobacterium longum, Lacticaseibacillus casei, Levilactobacillus brevis, Lacticaseibacillus rhamnosus, Lactobacillus delbrueckii, Lactobacillus helveticus, Lactococcus lactis and Streptococcus thermophilus may play a role in aiding weight loss in obese individuals through diverse mechanisms of action [3,4,9,12,18,19,20,22]. These strains can modulate the metabolism of fats, optimizing their breakdown, reducing absorption in the intestine, preventing them from being stored in adipose tissue, promoting their use as an energy source [17,23]. Another notable action is the ability to regulate the inflammatory response in the intestine, reducing low-grade inflammation associated with obesity, which can have a positive impact on metabolism and body weight regulation [24]. Furthermore, Probiotic strains can affect satiety and appetite signals by modulating the production of hunger-related hormones, such as ghrelin, promoting a greater feeling of fullness. Thus, these mechanisms can help reduce the desire for high-calorie and unhealthy foods [25].
Although there is data indicating that probiotics may play a role in the treatment of obesity, it is important to highlight the need for more solid and comprehensive research to conclusively evaluate their effectiveness, especially their action in addition to healthy lifestyle habits. Therefore, the objective of this study was to investigate whether treatment with probiotics, together with the adoption of healthy lifestyle habits, is effective in reducing weight in obese individuals.
2. Materials and Methods
Study Design
A prospective before-and-after study was carried out with patients treated at a primary health care clinic in Uberlândia in the State of Minas Gerais, Brazil, from October 2022 to April 2023. Initially, 107 patients were invited to participate. Of these, 45 obese patients (BMI ≥30kg/m2) aged 18 years or older were included. However, 62 patients were excluded due to the following criteria: use of probiotics in the last 90 days, continuous use of medications in the last 15 days, antibiotics in the last 15 days, presence of clinical evidence of intestinal diseases, serious diseases such as heart disease, nephropathy, chronic liver disease, immunodeficiencies, chronic neuropathy or hospitalization in the last two months.
Forty-five patients were recruited at their first clinic visit (T0). Patients received guidance on the importance of physical activity, sleep hygiene recommendations and anxiety management. Patients were not encouraged to change their eating pattern, however, guidance was given to have a healthy diet, especially to avoid industrialized, processed and ultra-processed products, increase water intake and fiber consumption and avoid ingesting soft drinks. following the criteria of the Food Guide for the Brazilian population. In addition to these instructions, patients used a probiotic component, a capsule containing a combination of the following bacterial strains: Bifidobacterium longum, Lacticaseibacillus casei, Levilactobacillus brevis, Lacticaseibacillus rhamnosus, Lactobacillus delbrueckii, Lactobacillus helveticus, Lactococcus lactis, and Streptococcus thermophilus (1 capsule, 108 CFU/capsule/day) for a duration of 60 days. The probiotics were manufactured by Nutramedic – AGA and AGA comercial EIRELI, Brazil. Patients were monitored by regular phone calls regarding the practice of healthy lifestyle habits, in addition to receiving weekly guidance and encouragement via a multiplatform instant messaging service application for smartphones. All were reevaluated after 60 days (T1). Patients were monitored by regular phone calls regarding the practice of healthy lifestyle habits, in addition to receiving weekly guidance and encouragement via a multiplatform instant messaging service application for smartphones. All were reevaluated after 60 days (T1).
Anthropometric and Body Composition Variables and Biochemical Parameters
Body mass index (BMI) was calculated using body weight and height measured with bare feet and minimal clothing according to the World Health Organization definition and classification [26]. Body composition parameters (mass and percentage of body fat and lean mass) were acquired using the Inbody 120 bioimpedance scale (South Korea).
A biochemical assessment through a 12-hour fasting blood test was performed at T0 and T1, including: fasting blood glucose, HbA1C, insulin, HOMA-IR index, HDL cholesterol, LDL cholesterol and triglycerides. These analyzes were carried out in a certified medical laboratory (Sabin, Uberlândia – Minas Gerais, Brazil).
Stool Shape and Consistency
The form of stools was analyzed using the Bristol Stool Scale [27].
Life Habits
All patients benefited from an interview including dietary pattern survey using the ELSA Brazil questionnaire, [28] (to assess dietary patterns, particularly in terms of fiber intake, water, processed foods and soda consumption), anxiety questionnaire (Hamilton) [29], sleep questionnaire (Pittsburgh Sleep Quality Index - PSQI) [30] and international physical activity questionnaire (IPAQ) [31]. These questionnaires were administered at T0 and T1.
Intestinal Microbiota Analysis
Metagenomic Analysis by DNA Sequencing
DNA from stool samples was isolated as described by HEISEN (2016) [32]. For comprehensive metagenomic analysis, shotgun DNA sequencing of the stools was utilized to assess the taxonomy of the intestinal microbiota. The quality and quantity of DNA samples were checked using Nanodrop Photometer 2000 (Thermo Scientific), and the DNA was sequenced on an Illumina HiSeq 2500 Sequencer. Samples (50 ng as quantified by Qbit) were processed with the Illumina Nextera DNA-Sample-Preparation Kit according to the manufacturer’s protocol. Sequencing was done with 2x100 nucleotides (paired-end sequencing) in 8 lanes with 300 GB of raw data. On average, sequencing reached 2.1 GB/sample. The samples were sequenced with a sequencing depth of 10.9 million reads per paired-end sequencing file (s = 6.3 million).
Bioinformatics Analysis of Sequencing Data
Raw sequences obtained from metagenomic samples of 45 patients underwent a quality check using FastQC software (https://www.bioinformatics.babraham.ac.uk/projects/fastqc/). Quality check comprising by base sequence quality, by sequence quality scores, by base sequence content, by sequence GC content, by N base content, sequence length distribution, sequence duplication levels, kmer content and overrepresented sequences. All samples presented satisfactory values for each parameter tested. Then, the sequences were processed using PRINSEQ to remove low-quality reads, cut poly-Ns and A/T tails. Each sample was subjected to a BLASTX analysis using an in-house developed tool (MALThttp://ab.inf.uni-tuebingen.de/software/malt/) against the NCBI-NR database with a maximum allowed e-value of 1.0. BLASTX files were imported into MEGAN5 (http://ab.inf.uni-tuebingen.de/software/megan5/). MEGAN5 clusters reads into taxonomic and functional categories based on BLASTX hits. The minimum bit score used for analysis was 50 and a minimum support of 50 reads for each taxonomic category was used for the LCA algorithm. Ultimately, the reads were assigned to a taxonomic and functional category. On average, about 50% of the readings in each sample were assigned to some category, 79% of them to the genus level and about 61% to the species level. The samples were normalized with respect to each other. Functional annotation of the reads was based on the KEGG library (Kyoto Encyclopedia for Genes and Genomes, http://www.genome.jp/kegg/).
Statistical Analysis
A paired sample of n=45 was calculated with study power of 81.35% (0.8135), effect size of 0.38 and α=0.05. The calculation was carried out using G-power Software 3.1.9.7.
Descriptive and inferential statistical analysis was performed. The descriptive analysis was carried out using absolute and relative frequencies for qualitative variables. Quantitative variables were analyzed using their means and standard deviation.
For inferential analysis, the following procedures were employed: for quantitative variables (discrete and continuous), normality tests were initially conducted using the KS and SW tests. Subsequently, a paired Student’s t-test was performed. For qualitative variables, McNemar’s test was used for nominal variables, and the Wilcoxon test was applied for ordinal variables. The strength of association between qualitative variables was assessed by calculating the odds ratio, accompanied by the respective 95% confidence interval (CI 95%). A significance value of p<0.05 was used to determine statistically significant differences. The analyses were carried out using IBM SPSS software, version 25.0.
3. Results
Of the 45 patients included in the study, 30 (66.7%) were female. Compared to the general population, the participants included in the study had a higher socioeconomic level. The age range of the group varied between 26 and 52 years. The results obtained revealed that all bacterial strains contained in the probiotic used in the treatment were detected in the intestinal microbiota of all patients included in the study (Figure 1).
Table 1 presents the characteristics of the study population in relation to lifestyle habits at time points T0 and T1. After a 60-day period, the percentage of participants classified as highly active increased from 17.8% to 75.6% (OR=14.29; p<0.001), while there was a significant reduction in the percentage of participants classified as sedentary, decreasing from 44.4% to 6.7% (OR=0.09; p<0.001). An increase in patients without anxiety was observed after treatment (OR=55.00; p<0.001), as well as a significant reduction in patients with severe anxiety (OR=0.04; p<0.001). Additionally, participants reported a significant improvement in sleep quality, with the mean PSQI score decreasing (OR=14.39; p < 0.001), indicating an overall improvement in sleep quality. Regarding the consumption of fiber-rich foods, there was no significant change (p=0.15), with over 85% of patients consuming them both before and after treatment, as the majority already had this dietary habit. As for water intake, there was a significant increase in the daily amount of water consumed by participants after treatment (OR=10.72; p<0.001). In terms of soda consumption, there was an increase in the number of patients who stopped consuming this type of beverage (OR=5.50; p<0.001). Regarding the consumption of processed foods, there was a significant reduction in the frequency of consumption of these foods after treatment (OR=41.00; p<0.001) (Table 1). It is worth noting that there was no change in the dietary pattern of the patients.
After the 60-day period, a significant improvement was observed in several physiological parameters (Table 2). An average reduction of 6.04 kg in body weight (p < 0.001) and 6.29 kg in fat mass (p < 0.001) was observed. The average BMI reduced by 1.1 kg/m² (p = 0.003). Fasting glucose and glycated hemoglobin levels showed an average reduction of 8.33 mg/dL and 0.15% (p < 0.001). Insulin levels (µUI/mL) reduced by an average of 5.5 (p<0.001). The HOMA-IR index showed an average reduction of 0.99 (p=0.002). Furthermore, an improvement in the lipid profile was observed with a significant mean increase in HDL cholesterol of 8.4 mg/dL (p < 0.001), a mean reduction in LDL cholesterol of 25.69 mg/dL (p < 0.001) and the triglyceride levels also decreased by 67.45 mg/dL (p < 0.001). Regarding the frequency of evacuation of participants, there was an increase of 44.4% in the number of participants who began to evacuate daily (OR=9.14; p<0.001). Regarding stool consistency, assessed by the Bristol Scale, there was a 55.3% increase in the percentage of patients with stools classified as type 3 and type 4, compared to the other types (OR=10.81; p < 0.001) (Table 2).
The results of this study revealed significant changes in the composition of the intestinal microbiota in patients with obesity after 60 days of treatment. Figure 2 shows the rates for the phyla in relation to the period before and after treatment. There was no significant variation in the balance between phyla. A statistically significant increase in the diversity of phyla was observed (p<0.001). The phyla Proteobacteria (p<0.001) and Euryarchaeota (p<0.001) showed an average reduction. There was no significant difference in the presence of the firmicutes phylum in the pre- and post-treatment periods. The other phyla showed a significant increase in their presence in the intestinal microbiota (p<0.001): Fusobacteria, Tenericutes, Euryarchaeota, Verrucomicrobia, Actinobacteria and Bacteroidetes.
Regarding bacterial species, several showed statistically significant differences (p<0.001) when comparing before and after the 60-day treatment period. In the Firmicutes phylum, there was a reduction in Ruminococcus spp., Oribacterium sinus, Lachnospira spp, Limosilactobacillus spp, and Dorea longicatena. There was also a significant increase in Roseburia hominis, Lactobacillus spp, and Eubacterium spp (Figure 3). In the Bacteroidetes phylum (Figure 4), in addition to a substantial increase in diversity, there was a significant increase in various species such as Barnesiella intestinihominis, Alistipes putredini, species of Prevotella, and a reduction in Bacteroides dorei and Alistipes obesi. As for other detected phyla, a reduction in their presence in the intestinal microbiota was observed for species such as Methanobrevibacter smithii (Euryarchaeota phylum), Escherichia coli, Acinetobacter baumannii, Klebsiella pneumoniae, Staphyococcus aureus, Proteus mirabilis, Desulfovibrio piger, Bilophila wadsworthia, Parasutterella excrementihominis, and Citrobacter freundii (Proteobacteria phylum) (Figure 5).
It is noteworthy that, among the 45 patients included in this study, only 5 of them opted exclusively for the use of probiotics, refusing to adhere to the proposal to modify their lifestyle habits, even after continuous stimulation. In these patients, no significant weight loss was observed (with an average loss of only 1 kilogram over 60 days) and their clinical parameters did not show notable improvements (data not shown).
4. Discussion
This is the first study conducted involving the combined use of a multispecies probiotic and lifestyle changes, with an analysis of the intestinal microbiota, aiming to improve both the intestinal microbiota and various clinical and health parameters, with an emphasis on weight loss. The research involved 45 patients with obesity over a 60-day period and yielded promising results. Previous studies have indicated that the introduction of probiotics can positively influence bacterial composition, resulting in beneficial effects on the health of patients with obesity [15,33,34]. One possible explanation for these effects is related to the increase in short-chain fatty acid (SCFA)-producing bacteria, as well as the reduction in lipopolysaccharide (LPS) producers [7,35,36]. These changes in the gut microbiota have been associated with a reduction in tissue and organ inflammation induced by LPS. Additionally, probiotics may play a role in reducing opportunistic pathogens and their harmful metabolites, such as trimethylamine, LPS, and indole [22]. In the study by Narmaki et al. [37], it was observed that probiotics can reduce fat accumulation, lower inflammation levels, and improve insulin sensitivity. These metabolic benefits have been associated with increased neuropeptides and gastrointestinal peptides, as well as an increase in the abundance of various beneficial bacteria [17,38]. However, other studies did not show improvement in weight loss when using probiotics alone [12,39,40]. Therefore, this study aims to investigate the combined effect of probiotics with healthy lifestyle habits.
There was a significant increase in the which plays a fundamental role in maintaining intestinal health [43]. These fatty acids have anti-inflammatory effects and can strengthen the integrity of the intestinal barrier, reducing permeability and inflammation [14]. Physical exercise can influence the production of hormones and neurotransmitters that can indirectly affect the intestinal microbiota [44]. In addition to modulating the production of substances such as GABA (gamma-aminobutyric acid) and serotonin, which can influence the composition and function of the microbiota, being of great importance in the homeostasis of the microbiome-gut-brain axis [45]. Physical exercise can influence the production of hormones and neurotransmitters that can indirectly affect the intestinal microbiota [44]. In addition to modulating the production of substances such as GABA (gamma-aminobutyric acid) and serotonin, which can influence the composition and function of the microbiota, being of great importance in the homeostasis of the microbiome-gut-brain axis [45]. Physical exercise can influence the production of hormones and neurotransmitters that can indirectly affect the intestinal microbiota [44]. In addition to modulating the production of substances such as GABA (gamma-aminobutyric acid) and serotonin, which can influence the composition and function of the microbiota, being of great importance in the homeostasis of the microbiome-gut-brain axis [45].
In the present study, the analysis of the degree of anxiety using the Hamilton Anxiety Scale [28] revealed significant improvements and important correlations with the improvement of the intestinal microbiota in obese patients. In this investigation, a significant reduction in anxiety was observed with the positive impact of treatment with probiotics and changes in lifestyle habits, such as practicing meditation, yoga, deep breathing, in reducing anxiety levels. These results are consistent with previous studies that have shown a correlation between gut health and mental health, highlighting the importance of the gut microbiota in regulating mood and emotional well-being [46,47,48].
The relationship between anxiety and intestinal microbiota has been the subject of increasing interest in scientific literature. Cai and colleagues demonstrated a bidirectional communication between the brain and the intestine, known as the gut-brain axis, which involves the complex interaction between the central nervous system, the immune system and the intestinal microbiota [49]. Changes in the gut microbiota have been linked to neuropsychiatric disorders, including anxiety. A balanced gut microbiota is essential for the adequate production of beneficial neurotransmitters, such as GABA and serotonin, which play a crucial role in regulating mood and emotional well-being [15]. The intestinal microbiota is also responsible for the synthesis of vitamins essential for mood, such as vitamin B12 and folate [13]. Therefore, an imbalance in the intestinal microbiota can lead to changes in the production of these neurotransmitters and vitamins, negatively impacting mood and emotional health [23]. The use of probiotics has been suggested as a therapeutic strategy to create a balanced intestinal environment for the production of these essential substances in mental health [50].
Improvement in sleep quality is also a relevant aspect of this study. The reduction in the average Pittsburgh Sleep Quality Index score [29] indicates an overall improvement in participants’ sleep quality. Adequate sleep quality is essential for health and well-being, and sleep disorders are associated with a variety of health problems, including cardiovascular disease, obesity, and cognitive impairment [51,52]. The significant improvement in sleep quality observed in the study may be related to the influence of the intestinal microbiota on the production and regulation of hormones and neurotransmitters involved in sleep, such as melatonin, GABA and 5-HTP (5-hydroxytryptophan), as well as has been demonstrated in other research [53,54,55]. Some intestinal microorganisms are capable of synthesizing melatonin from tryptophan, an essential amino acid present in the diet. Therefore, a healthy and diverse gut microbiome can contribute to adequate melatonin production, promoting quality sleep [56,57,58].
When it comes to nutrition, a significant increase in daily water intake was observed after treatment. Adequate hydration is essential for the proper functioning of the body, including gastrointestinal health and the composition of the intestinal microbiota [16,59,60,61]. Additionally, in this research, a significant reduction in the frequency of consumption of industrialized products after treatment was observed. This change is positive, since processed foods are generally rich in saturated fats, sugars and additives, and their excessive consumption is associated with a greater risk of intestinal dysbiosis which is associated with obesity, cardiovascular disease and other chronic conditions [10,62]. Interestingly, in this study, individuals who consumed processed or ultra-processed foods had an increased level of Proteobacteria [63,64,65,66]. Furthermore, regular intake of processed foods is associated with an increase in intestinal permeability, resulting in a condition known as “leaky gut” [23,67,68].
The results obtained in this series demonstrated significant improvements in relation to body mass index (BMI), glycemic control and lipid profile. The reduction in BMI may be directly related to changes in habits and the improvement of the intestinal microbiota provided by probiotics [9,69]. Furthermore, improvements in glycemic control were observed, with reductions in fasting glucose, glycated hemoglobin, insulin and HOMA-IR index levels suggesting an improvement in insulin sensitivity and glycemic control. These results are consistent with previous studies linking metabolic health and gut microbiota composition [70,71,72]. The improvement in the lipid profile was also an important finding. The increase in HDL cholesterol and the reduction in LDL cholesterol and triglycerides indicate a positive effect on the prevention and treatment of participants’ cardiovascular health. These changes are of great relevance, since dyslipidemia is a significant risk factor for cardiovascular diseases [1,73]. There was a significant improvement in participants’ bowel movement frequency after treatment.
The treatment also had a positive effect on participants’ bowel movement frequency and stool consistency. Studies have shown that probiotics can promote the balance of the intestinal microbiota, improving intestinal regularity and stool consistency [3,74,75]. Furthermore, a healthy diet and increased water intake are important factors in maintaining intestinal health. This reinforces the importance of integrative approaches that combine the use of probiotics with lifestyle changes to improve intestinal function and the quality of bowel movements [4,8,76].
Regarding the composition of the intestinal microbiota, the results revealed significant changes with an increase in microbial diversity after treatment. The reduction in the phylum Firmicutes and the increase in the phylum Bacteroidetes stand out, indicating an improvement in the balance between these key bacterial phyla. The reduction of the Firmicutes phylum is particularly relevant, as this group of bacteria is associated with nutrient metabolism and energy extraction from food [11,77]. These changes are consistent with previous studies linking obesity and other metabolic disorders to the imbalance between Firmicutes and Bacteroidetes in the gut microbiota [78,79]. The Firmicutes/Bacteroidetes relationship has often been considered as a possible hallmark of obesity, there is still controversy on this issue due to the relative abundance of the Firmicutes and Bacteroidetes phyla being highly variable among individuals within the same population [80]. This is likely due to many lifestyle factors, including diet, physical activity, food additives and contaminants, antibiotic consumption, physical activity, among others that influence the composition of the microbiota in the gastrointestinal tract [2,81,82].
On the other hand, the increase in the Bacteroidetes phylum is associated with a healthier and more diverse microbiota [83]. These bacteria play important roles in the degradation of plant fibers, the production of SCFAs, and the regulation of inflammation in the intestine [84,85,86]. The increase in the Bacteroidetes phylum may contribute to greater SCFA production, which in turn plays a crucial role in maintaining intestinal health by promoting the integrity of the intestinal barrier, regulating the immune response and providing energy to intestinal cells [18,87,88].
When analyzing changes in bacterial species, an increase in several beneficial species was observed, such as Akkermansia muciniphila, Prevotella copri, Ruminococcus bromii, Limosilactobacillus reuteri, Bifidobacterium adolescentis and Bifidobacterium bifidum. These species are associated with health benefits including regulating metabolism, controlling weight, improving the immune system, and reducing inflammation [19,33]. On the other hand, there was a reduction in potentially harmful species, such as Escherichia coli, Bacteroides dorei, Lachnospira pectinoschiza, Lactobacillus acidophilus and Staphylococcus aureus. These changes in bacterial species indicate an improvement in the composition of the intestinal microbiota towards a healthier and more balanced profile [21,37,89,90] (Figure 6; and Supplementary data (Table).
The first part of the figure (BEFORE) is showing the pathogenic bacterias’ resistance mechanisms, as toxins which cause damage and inflammation of the mucosa. The second part (IN TREATMENT) relates the benefits of the probiotics, such as bacteriocins, substances that are able to stop the increase of pathogenic bacteria; is important to notice the inflammation’s reduction. The last part (AFTER) is showing the mucosa and microbiome after treatment, the flora is in homeostasis and, as consequence, there is no inflammation on the mucosa.
On the other hand, the analysis of these results clearly shows that the exclusive administration of probiotics, without the concomitant modification of lifestyle habits, results in a considerably divergent response. Patients who opted for this approach experienced an average weight loss of just 1 kilogram over 60 days, without observing significant improvements in their clinical parameters and improvement in the composition of the intestinal microbiota. These findings highlight the importance of the synergy between the use of probiotics and the adoption of healthy lifestyle habits as a more effective strategy to achieve substantial results in relation to weight loss and the general well-being of patients. Therefore, it reinforces the idea that the combination of probiotics with positive lifestyle changes is essential for achieving significant clinical benefits.
The study has several strengths, including its study design (before-and-after study), a broad panel of measured parameters (anthropometric, biochemical, and lifestyle factors), and microbial analysis of feces demonstrating the influence of probiotic bacteria on the composition of the intestinal microbiota. Additionally, the detailed data collection through in-person meetings, the absence of participant dropouts, and no reported treatment-related side effects are other strong points of the research.
The main limitation of the study is the relatively small number of individuals analyzed. The main reason for this was the use of very strict inclusion and exclusion criteria. However, the criteria applied made it possible to select a homogeneous group of subjects, not affected by diseases or conditions that could have significantly influenced the results of the study. Another limitation was the fact that the control group was not used, resulting in the risk of overestimating the effectiveness of the treatment, and may provide useful insights for future study designs.
5. Conclusions
The results of this study indicate that treatment with probiotics and lifestyle modifications for 60 days promoted significant improvements in several clinical and health parameters. These changes are related to improving the composition of the intestinal microbiota, eating habits, increased physical activity, reduced anxiety and better sleep quality. These findings reinforce the importance of an integrated approach to health care, considering not only the intestinal microbiota, but also other aspects of lifestyle. It is recommended that future studies deepen these analyses, including a more detailed assessment of bacterial species and their relationship with different clinical and health parameters, as well as long-term follow-up to assess the sustainability of these improvements.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary table: Frequency of occurrence of phyla, genera, and species of microorganisms before and after treatment and their role in metabolism.
Author Contributions
Conceptualization, G.P.F. and D.V.D.B.R.; methodology, R.P.M. and G.S.L.; software, R.P.M.; formal analysis, G.P.F.; investigation, G.P.F and and A.R.X and D.V.D.B.R.; resources, D.V.D.B.R.; data curation, G.S.L.; writing—original draft preparation, G.P.F and L.J.P.; writing—review and editing, A.C.C.N and D.V.D.B.R; visualization, G.G.P and L.J.P.; supervision, G.G.P.; project administration, D.V.D.B.R.; funding acquisition, D.V.D.B.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by FAPEMIG, APQ-00965-18.
Institutional Review Board Statement
The study proposal was forwarded and approved by the Ethics and Research Committee of the Federal University of Uberlândia - CAAE n 49391221.8.0000.5152, Opinion number: 5.003.231. All subjects provided their consent to participate in the study and signed the Informed Consent Form. The clinical investigation was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (DVDBR), upon reasonable request. The data that support the findings will be available in [https://repositorio.ufu.br/handle/123456789/39223] at [DOI: 10.14393/ufu.di.2023.521] following an embargo from the date of publication to allow for commercialization of research findings. All data regarding the metagenomic and proteomic analyses conducted by a private company are not available due to patient data protection measures.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mohajan, D.; Mohajan, H.K. Obesity and Its Related Diseases: A New Escalating Alarming in Global Health. Paradigm Academic Press: J Innov Med Res. 2023; 2:3. [CrossRef]
- Kodaira, K.; Abe, F.C.; Galvão, T.F.; Silva, M.T. Time-trend in excess weight in Brazilian adults: A systematic review and meta-analysis. PLoS ONE. 2021; 16: e0257755. [CrossRef]
- Abevanoli, L.; Scarpellini, E.; Colica, C.; Boccuto, L.; Salehi, B.; Sharifi–Rad J.; Aiello, V.; Romano, B.; De Lorenzo, A.; Izzo, A.A.; Capasso, R. Gut Microbiota and Obesity: A Role for Probiotics. Nutrients. 2019; 11:2690. [CrossRef]
- Breton, J.; Galmiche, M.; Dechelotte, P. Dysbiotic Gut Bacteria in Obesity: An Overview of the Metabolic Mechanisms and Therapeutic Perspectives of Next-Generation Probiotics. Microorganisms. 2022; 10:452. [CrossRef]
- Brasil, Ministério da Saúde, Vigitel Brasil 2006-2021 : vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico : estimativas sobre frequência e distribuição sociodemográfica do estado nutricional e consumo alimentar nas capitais dos 26 estados brasileiros e no Distrito Federal entre 2006 e 2021 : estado nutricional e consumo alimentar [recurso eletrônico] / Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. – Brasília: Ministério da Saúde, 2022.
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism. 2019; 92:6–10. [CrossRef]
- Sivamaruthi, B.S.; Kesika, P.; Suganthy, N.; Chaiyasut, C. A Review on Role of Microbiome in Obesity and Antiobesity Properties of Probiotic Supplements. BioMed Res Int. 2019. [CrossRef]
- Masood, A.; Alsheddi, L.; Alfayadh, L.; Bukhari, B.; Elawad, R.; Alfadda, A.A. Dietary and Lifestyle Factors Serve as Predictors of Successful Weight Loss Maintenance Postbariatric Surgery. J Obes. 2019; 7295978. [CrossRef]
- Borgeraas, H.; Johnson, L.K.; Skattebu, J.; Hertel, J.K.; Hjelmesaeth, J. Effects of probiotics on body weight, body mass index, fat mass and fat percentage in subjects with overweight or obesity: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2018; 19:219–232. [CrossRef]
- Duranti, S.; Ferrario, C.; Sinderen, D.V.; Ventura, M.; Turroni, F. Obesity and microbiota: an example of an intricate relationship. Nutr Genes. 2017; 12:18. [CrossRef]
- Vijay, A.; Valdes, A.M. Role of the gut microbiome in chronic diseases: a narrative review. Eur J Clin Nutr. 2022; 76:489-501. [CrossRef]
- Brusaferro, A.; Cozzali, R.; Orabona, C.; Biscarini A, Farinelli E, Cavalli E et al. Is It Time to Use Probiotics to Prevent or Treat Obesity? Nutrients. 2018; 10(11):1613. [CrossRef]
- Parkar, S.G.; Kalsbeek, A.; Cheeseman, J.F. Potential Role for the Gut Microbiota in Modulating Host Circadian Rhythms and Metabolic Health. Microorganisms. 2019; 7:41. [CrossRef]
- Aya, V.; Flórez, A.; Perez, L.; Ramírez, J.D. Association between physical activity and changes in intestinal microbiota composition: A systematic review. PLoS ONE. 2021; 16:e0247039. [CrossRef]
- Hadi, A.; Sepandi, M.; Marx, W.; Moradi, S.; Parastouei, K. Clinical and psychological responses to synbiotic supplementation in obese or overweight adults: A randomized clinical trial. Complement Ther Med. 2019; 47:102216. [CrossRef]
- Fan, Y.; Pedersen, O. Gut microbiota in human metabolic health and disease. Nat Rev Microbiol. 2021; 19:55-71. [CrossRef]
- Sankararaman, S.; Noriega, K.; Velayuthan, S.; Sferra, T.; Martindale, R. Gut Microbiome and Its Impact on Obesity and Obesity-Related Disorders. Curr Gastroenterol. 2023; 25:31–44. [CrossRef]
- Kobyliak, N.; Falalyeyeva, T.; Boyko, N.; Tsyryuk, O.; Beregova, T.; Ostapchenko, L. Probiotics and nutraceuticals as a new frontier in obesity prevention and management. Diabetes Res Clin Pract. 2018; 141:190–199. [CrossRef]
- Vallianou, N.; Stratigou, T.; Christodoulatos, G.S.; Tsigalou, C.; Dalamaga, M. Probiotics, Prebiotics, Synbiotics, Postbiotics, and Obesity: Current Evidence, Controversies, and Perspectives. Curr Obes. 2020; 9:179–192. [CrossRef]
- Wang, Z.; Xin, S.; Ding, L.; Ding, W.; Hou, Y.; Liu, C.Q.; Zhang, X.D. The Potential Role of Probiotics in Controlling Overweight/Obesity and Associated Metabolic Parameters in Adults: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2019. [CrossRef]
- Bui, T.P.N.; Vos, W.M. Next-generation therapeutic bacteria for treating obesity, diabetes, and other endocrine diseases. Best Pract Res Clin Endocrinol Metab. 2021; 35:101504. [CrossRef]
- Park, S.; Bae, J.H. Probiotics for weight loss: a systematic review and meta-analysis. Nutr Res. 2015; 35:566-75. [CrossRef]
- Chattopadhyay, A.; Mythili, S. The journey of gut microbiome – An introduction and its influence on metabolic disorders. Front Biol. 2018; 13:327–341. [CrossRef]
- Boulangé, C.L.; Neves, A.L.; Chilloux, J.; Nicholson, J.K.; Dumas, M.E. Impact of the gut microbiota on inflammation, obesity, and metabolic disease. Genome Medicine. 2016; 8:42. [CrossRef]
- Wiciński, M.; Gębalski, J.; Gołębiewski, J.; Malinowski, B. Probiotics for the Treatment of Overweight and Obesity in Humans—A Review of Clinical Trials. Microorganisms. 2020; 8:1148. [CrossRef]
- A healthy lifestyle–WHO recommendations [Internet]. [cited 14 September 2022]. Available sur.https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations. 14 September.
- Martinez, A.P.; Azevedo, G.R. The Bristol Stool Form Scale: its translation to Portuguese, cultural adaptation and validation. Rev Latino Am Enfermagem. 2012; 20:583–9. [CrossRef]
- Molina, M.D.C.B.; Benseñor, I.M.; Cardoso, L.D.O.; Velasquez-Melendez, G.; Drehmer, M.; Pereira, T.S.S,. Faria C.P.; Melere, C.; Manato, L.; Gomes, A.L.C.; Fonseca, M.J.M.; Sichieri, R. Reproducibility and relative validity of the Food Frequency Questionnaire used in the ELSA-Brasil. Cad de Saude Publica. 2013; 379-389. [CrossRef]
- Thompson, E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med. 2015; 65:601. [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med Rev. 2016; 25:52-73. [CrossRef]
- Matsudo, S.; Araújo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; Braggion, G. International physical activity questionnaire (IPAQ): validity and reproducibility study in Brazil. Rev. Bras. Activation. Phys. Health. 2012; 6:5-18.
- Heinsen, F.A.; Fangmann, D.; Müller, N.; Schulte, D.M.; Rühlemann, M.C.; Türk, K.; Settgast, U.; Lieb, W.; Baines, J.F.; Schreiber, S.; Franke, A.; Laudes, M. Beneficial Effects of a Dietary Weight Loss Intervention on Human Gut Microbiome Diversity and Metabolism Are Not Sustained During Weight Maintenance. Obes Facts. 2016;9:379-391. [CrossRef]
- Szulińska, M.; Łoniewski, I.; van Hemert, S.; Sobieska, M.; Bogdański, P. Dose-Dependent Effects of Multispecies Probiotic Supplementation on the Lipopolysaccharide (LPS) Level and Cardiometabolic Profile in Obese Postmenopausal Women: A 12-Week Randomized Clinical Trial. Nutrients. 2018;10:773. [CrossRef]
- Song, E.J.; Han, K.; Lim, T.J.; Lim, S.; Chung, M.J.; Nam, M.H.; Kim, H.; Nam, Y.D. Effect of probiotics on obesity-related markers per enterotype: a double-blind, placebo-controlled, randomized clinical trial. EPMA J. 2020; 11:31–51. [CrossRef]
- Rouxinol-Dias, A.L.; Pinto, A.R.; Janeiro, C.; Rodrigues, D.; Moreira, M.; Dias, J.; Pereira, P. Probiotics for the control of obesity – Its effect on weight change. Porto Biom J. 2016. [CrossRef]
- Aoun, A.; Darwish, F.; Hamod, N. The Influence of the Gut Microbiome on Obesity in Adults and the Role of Probiotics, Prebiotics, and Synbiotics for Weight Loss. Prev Nutr Food Sci. 2020, 25:113-123. [CrossRef]
- Narmaki, E.; Borazjani, M.; Ataie-Jafari, A.; Hariri, N.; Doost, A.H.; Qorbani, M.; Saidpour, A . The combined effects of probiotics and restricted calorie diet on the anthropometric indices, eating behavior, and hormone levels of obese women with food addiction: a randomized clinical trial. Nutr Neurosci. 2022; 25:963-975. [CrossRef]
- Ataey, A.; Jafarvand, E.; Adham, D.; Moradi-Asl, E. The Relationship Between Obesity, Overweight, and the Human Development Index in World Health Organization Eastern Mediterranean Region Countries. J Prev Med Public Health. 2020; 53:98-105. [CrossRef]
- Mazloom. K.; Siddiqi, I.; Covasa, M. Probiotics: How Effective Are They in the Fight against Obesity? Nutrients. 2019; 11:258. [CrossRef]
- Kobyliak, N.; Conte, C.; Cammarota, G.; Haley, A.P.; Styriak, I.; Gaspar, L.; Fusek, J.; Rodrigo, L.; Kruzliak, P. Probiotics in prevention and treatment of obesity: a critical view. Nutr Metab. 2016; 13:14. [CrossRef]
- Quiroga, R.; Nistal, E.; Estébanez, B.; Damn, D.; Juárez-Fernández, M.; Martínez-Flórez, S.; García-Mediavilla, M.V.; Paz, J.A.; González-Gallego, J.; Sánchez-Campos, S.; Cuevas, M.J. Exercise training modulates the gut microbiota profile and impairs inflammatory signaling pathways in obese children. Exp Mol Med. 2020; 52: 1048–1061. [CrossRef]
- Sohail, M.U.; Yassine, H.M.; Sohail, A.; Thani, A.A.A. Impact of Physical Exercise on Gut Microbiome, Inflammation, and the Pathobiology of Metabolic Disorders. Rev Diabet Stud. 2019; 15:35-48. [CrossRef]
- Kern, T.; Blond, M.B.; Hansen, T.H.; Rosenkilde, M.; Quist, J.S.; Gram, A.S.; Ekstrøm CT, Hansen T, Stallknecht B. Structured exercise alters the gut microbiota in humans with overweight and obesity—A randomized controlled trial. Int J Obes. 2020; 44:125–135. [CrossRef]
- Wang, K.; Mehta, R.S.; Ma, W.; Nguyen, L.H.; Wang, D.D.; Ghazi, A.R.; Yan, Y.; Al-Shaar, L.; Wang, Y.; Hang, D.; Fu, B.C.; Ogino, S.; Rimm, E.B.; Hu, F.B.; Carmody, R.N.; Garrett, W.S.; Sun, Q.; Chan, A.T.; Huttenhower, C.; Song, M. The gut microbiome modifies the associations of short- and long-term physical activity with body weight changes. Microbiome. 2023; 11:121. [CrossRef]
- Hughes, R.L.; Pindus, D.M.; Khan, N.A.; Burd, N.A.; Holscher, H.D. Associations between Accelerometer-Measured Physical Activity and Fecal Microbiota in Adults with Overweight and Obesity. Med Sci Sports Exercise. 2023; 55:680-689. [CrossRef]
- Kang, S.S.; Jeraldo, P.R.; Kurti, A.; Miller, M.E.B.; Cook, M.D.; Whitlock, K.; Goldenfeld, N.; Woods, J.A.; White, B.A.; Chia, N.; Fryer, J.D. Diet and exercise orthogonally alter the gut microbiome and reveal independent associations with anxiety and cognition. Mol Neurodegener. 2014; 9:36. [CrossRef]
- Acharya, K.D.; Graham, M.; Raman, H.; Parakoyi, A.E.R.; Corcoran, A.; Belete, M.; Ramaswamy, B.; Koul, S.; Sachar, I.; Derendorf, K.; Wilmer, J.B.; Gottipati, S.; Tetel, M.J. Estradiol-mediated protection against high-fat diet induced anxiety and obesity is associated with changes in the gut microbiota in female mice. Sci Rep. 2023; 13: 4776. [CrossRef]
- Quicho, M.N.B. Microbiota-Derived Metabolites and Their Effects on Anxiety-Related Behavior. Los Angeles: University of California; 2023.
- Cai, Y.; Liu, P.; Zhou, X.; Yuan, J.; Chen, Q. Probiotics therapy show significant improvement in obesity and neurobehavioral disorders symptoms. Front Cell Infect Microbiol. 2023; 13:1178399. [CrossRef]
- Kaunang, T.M.D.; Setiawan, A.A.; Mayulu, N.; Leonita, I.; Wijaya, A.; Yusuf, V.M.; Mahira, M.F.N.A.; Yudisthira, D.; Gunawan, W.B.; Taslim, N.A.; Purnomo, A.F.; Sabrina, N.; Amalia, N.; Permatasari, H.K.; Nurkolis, F. Are probiotics beneficial for obese patients with major depressive disorder? Opinion for future implications and strategies. Front. Nutr. 2023; 10:1205434. [CrossRef]
- Ko, C.Y.; Liu, Q.Q.; Su, H.Z.; Zhang, H.P.; Fan, J.M.; Yang, J.H.; Hu, A.K.; Liu, Y.Q.; Chou, D.; Zeng, Y.M. Gut microbiota in obstructive sleep apnea–hypopnea syndrome: disease-related dysbiosis and metabolic comorbidities. Clin Sci. 2019; 133:905–917. [CrossRef]
- Kuvat, N.; Tanriverdi, H.; Armutcu, F. The relationship between obstructive sleep apnea syndrome and obesity: A new perspective on the pathogenesis in terms of organ crosstalk. Clin Respir J. 2020; 14:595–604. [CrossRef]
- Wang, Y.; Wouw, M.V.D.; Drogos, L.; Mehrabani, E.V.; Reimer, R.A.; Madsen, L.T.; Giesbrecht, G.F. Sleep and the gut microbiota in preschool-aged children. Sleep. 2022; 45:zsac020. [CrossRef]
- Valentini, F.; Evangelisti, M.; Arpinelli, M.; Nardo, G.D.; Borro, M.; Simmaco, M.; Villa, M.P. Gut microbiota composition in children with obstructive sleep apnoea syndrome: a pilot study. Sleep Med. 2020; 76:140-147. [CrossRef]
- Benedict, C.; Vogel, H.; Jonas, W.; Woting, A.; Blaut, M.; Schürmann, A.; Cedernaes, J. Gut microbiota and glucometabolic alterations in response to recurrent partial sleep deprivation in normal-weight young individuals. Molecular Metabolism. 2016; 5:1175-1186. [CrossRef]
- Anderson, J.R.; Carroll, I.; Azcarate-Peril, M.A.; Rochette, A.D.; Heinberg, L.J.; Peat, C.; Steffen, K.; Manderino, L.M.; Mitchell, J.; Gunstad, J. A preliminary examination of gut microbiota, sleep, and cognitive flexibility in healthy older adults. Sleep Med. 2017; 38:104-107. [CrossRef]
- Sen, P.; Molinero-Perez, A.; O’Riordan, K.J.; McCafferty, C.P.; O’Halloran, K.D.; Cryan, J.F. Microbiota and sleep: awakening the gut feeling. Trends Mol Med. 2021; 27:935-945. [CrossRef]
- Smith, R.P.; Easson, C.; Lyle, S.M.; Kapoor, R.; Donnelly, C.P.; Davidson, E.J.; Parikh, E.; Lopez, J.V.; Tartar, J.L. Gut microbiome diversity is associated with sleep physiology in humans. PLoS ONE. 2019;14:e0222394. [CrossRef]
- Aziz, T.; Hussain, N.; Hameed, Z.; Lin, L. Elucidating the role of diet in maintaining gut health to reduce the risk of obesity, cardiovascular and other age-related inflammatory diseases: recent challenges and future recommendations. Gut Microbes. 2024; 16:2297864. [CrossRef]
- Morales, J.S.; Valenzuela, P.L.; Castillo-García, A.; Butragueño, J.; Jiménez-Pavón, D.; Carrera-Bastos, P.; Lucia, A. The Exposome and Immune Health in Times of the COVID-19 Pandemic. Nutrients. 2022; 14: 24. [CrossRef]
- Rinninella, E.; Tohumcu, E.; Raoul, P.; Fiorani, M.; Cintoni, M.; Mele, M.C.; Cammarota, G.; Gasbarrini, A.; Ianiro, G. The role of diet in shaping human gut microbiota. Best Pract Res Clin Gastroenterol. 2023; 63:101828. [CrossRef]
- Li, J.; Riaz Rajoka, M.S.; Shao, D.; Jiang, C.; Jin, M.; Huang, Q.; Yang, H.; Shi, J. Strategies to increase the efficacy of using gut microbiota for the modulation of obesity. Obes Rev. 2017;18:1260-1271. [CrossRef]
- Gumma, E.Z. Human gut microbiota/microbiome in health and diseases: a review. Antonie van Leeuwenhoek. 2020; 113:2019–2040. [CrossRef]
- Adak, A.; Khan, M.R. An insight into gut microbiota and its functionalities. Cell Mol Life Sci. 2019; 76:473-493. [CrossRef]
- Hur, K.Y.; Lee, M.S. Gut Microbiota and Metabolic Disorders. Diabetes Metab J. 2015; 39:198-203. [CrossRef]
- Leo, E.E.M.; Peñafiel, A.M.; Escalante, V.M.H.; Araujo, Z.M.C. Ultra-processed diet, systemic oxidative stress, and breach of immunological tolerance. Nutrition. 2021; 92:111419. [CrossRef]
- Dahiya, D.K.; Renuka, Puniya, M.; Shandilya, U.K.; Dhewa, T.; Kumar, N.; Kumar, S.; Puniya, A.K.; Shukla, P. Gut Microbiota Modulation and Its Relationship with Obesity Using Prebiotic Fibers and Probiotics: A Review. Front Microbiol. 2017; 8:563. [CrossRef]
- Armet, A.M.; Deehan, E.C.; O’Sullivan, A.F.; Mota, J.F.; Field, C.J.; Prado, C.M.; Lucey, A.J.; Walter, J. Rethinking healthy eating in light of the gut microbiome. Cell Host Microbe. 2022; 30:764-785. [CrossRef]
- Yan, S.; Tian, Z.; Li, M.; Li, B.; Cui, W. Effects of probiotic supplementation on the regulation of blood lipid levels in overweight or obese subjects: a meta-analysis. Food Funct. 2019; 10:1747. [CrossRef]
- Shirvani-Rad, S.; Tabatabaei-Malazy, O.; Mohseni, S.; Hasani-Ranjbar, S.; Soroush, A.R.; Hoseini-Tavassol, Z.; Ejtahed, H.S.; Larijani, B. Probiotics as a Complementary Therapy for Management of Obesity: A Systematic Review. Evid Based Complement Alternat Med. 2021; 22:2021:6688450. [CrossRef]
- Rowland, I.; Gibson, G.; Heinken, A.; Scott, K.; Swann, J.; Thiele, I.; Tuohy, K. Gut microbiota functions: metabolism of nutrients and other food components. Eur J Nutr. 2018; 57:1-24. [CrossRef]
- Asemi, Z.; Zare, Z.; Shakeri, H.; Sabihi, S.S.; Esmaillzadeh, A. Effect of multispecies probiotic supplements on metabolic profiles, hs-CRP, and oxidative stress in patients with type 2 diabetes. Ann Nutr Metab. 2013; 63:1-9. [CrossRef]
- Perna, S.; Ilyas, Z.; Giacosa, A.; Gasparri, C.; Peroni, G.; Faliva, M.A.; Rigon, C.; Naso, M.; Riva, A.; Petrangolini, G.; Redha, A.A.; Rondanelli, M. Is Probiotic Supplementation Useful for the Management of Body Weight and Other Anthropometric Measures in Adults Affected by Overweight and Obesity with Metabolic Related Diseases? A Systematic Review and Meta-Analysis. Nutrients. 2021; 13:666. [CrossRef]
- Fontané, L.; Benaiges, D.; Goday, A.; Llauradó, G.; Pedro-Boteta, J. Influence of microbiota and probiotics on obesity. Clin Investig Arterioscler. 2018; 30:271-279. [CrossRef]
- Rehman, A.; Tyree, S.M.; Fehlbaum, S.; DunnGalvin, G.; Panagos, C.G.; Guy, B.; Patel, S.; Dinan, T.G.; Duttaroy, A.K.; Duss, R.; Steinert, R.E. A water-soluble tomato extract rich in secondary plant metabolites lowers trimethylamine-n-oxide and modulates gut microbiota: a randomized, double-blind, placebo-controlled cross-over study in overweight and obese adults. J Nut. 2023; 153:96–105. [CrossRef]
- Vallianou, N.G.; Kounatidis, D.; Tsilingiris, D.; Panagopoulos, F.; Christodoulatos, G.S.; Evangelopoulos, A.; Karampela, I.; Dalamaga, M. The Role of Next-Generation Probiotics in Obesity and Obesity-Associated Disorders: Current Knowledge and Future Perspectives. Int J Mol Sci. 2023; 24:6755. [CrossRef]
- Cerdó, T.; García-Santos, J.A.; Bermúdez, M.G.; Campoy C. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Nutrients. 2019;11:635. [CrossRef]
- Aguilera, X.E.L.; Manzano, A.; Pirela, D.; Bermúdez, V. Probiotics and Gut Microbiota in Obesity: Myths and Realities of a New Health Revolution. J Pers Med. 2022; 12:1282. [CrossRef]
- Magne, F.; Gotteland, M.; Gauthier, L.; Zazueta, A.; Pesoa, S.; Navarrete, P.; Balamurugan, R. The Firmicutes/Bacteroidetes Ratio: A Relevant Marker of Gut Dysbiosis in Obese Patients? Nutrients. 2020;12:1474. [CrossRef]
- Włodarczyk, M.; S’lizewska, K. Obesity as the 21st Century’s major disease: The role of probiotics and prebiotics in prevention and treatment. Food Bioscience. 2021. [CrossRef]
- Fitch, A.K.; Bays, H.E. Obesity definition, diagnosis, bias, standard operating procedures (SOPs), and telehealth: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022. Obesity Pillars. 2022; 1:100004. [CrossRef]
- Ben Othman, R.; Ben Amor, N.; Mahjoub, F.; Berriche, O.; El Ghali, C.; Gamoudi, A.; Jamoussi, H. A clinical trial about effects of prebiotic and probiotic supplementation on weight loss, psychological profile and metabolic parameters in obese subjects. Endocrinol Diabetes Metab. 2023; 6:e402. [CrossRef]
- Stojanov, S.; Berlec, A.; Štrukelj, B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease. Microorganisms. 2020; 8:1715. [CrossRef]
- Arora, T.; Singh, S.; Sharma, R.K. Probiotics: Interaction with gut microbiome and antiobesity potential. Nutrition. 2013; 29:591-6. [CrossRef]
- Perumpail, B.J.; Li, A.A.; John, N.; Sallam, S.; Shah, N.D.; Kwong, W.; Cholankeril, G.; Kim, D.; Ahmed, A. The Therapeutic Implications of the Gut Microbiome and Probiotics in Patients with NAFLD. Diseases. 2019;7:27. [CrossRef]
- Kim, S.K.; Guevarra, R.B.; Kim, Y.T.; Kwon, J.; Kim, H.; Cho, J.H.; Kim, H.B.; Lee, J.H. Role of Probiotics in Human Gut Microbiome-Associated Diseases. J Microbiol Biotechnol. 2019; 29:1335-1340. [CrossRef]
- Cox, A.J.; West, N.P.; Cripps, A.W. Obesity, inflammation, and the gut microbiota. Lancet Diabetes Endocrinol. 2015; 3:207-15. [CrossRef]
- Barengolts, E. Gut microbiota, prebiotics, probiotics, and synbiotics in management of obesity and prediabetes: review of randomized controlled trials. Endocr Pract. 2016; 22:1224-1234. [CrossRef]
- Maioli, T.U.; Borras-Nogues, E.; Torres, L.; Barbosa, S.C.; Martins, V.D.; Langella, P.; Azevedo, V.A.; Chatel, J.M. Possible Benefits of Faecalibacterium prausnitzii for Obesity-Associated Gut Disorders. Front Pharmacol. 2021; 12:740636. [CrossRef]
- Mithieux, G. Gut Microbiota and Host Metabolism: What Relationship. Neuroendocrinology. 2018; 106:352-356. [CrossRef]
Figure 1.
Analysis of the presence of bacterial species of probiotic before and after treatment of the patients included in the study. *p<0.05 = significant difference by Wilcoxon Test.
Figure 1.
Analysis of the presence of bacterial species of probiotic before and after treatment of the patients included in the study. *p<0.05 = significant difference by Wilcoxon Test.
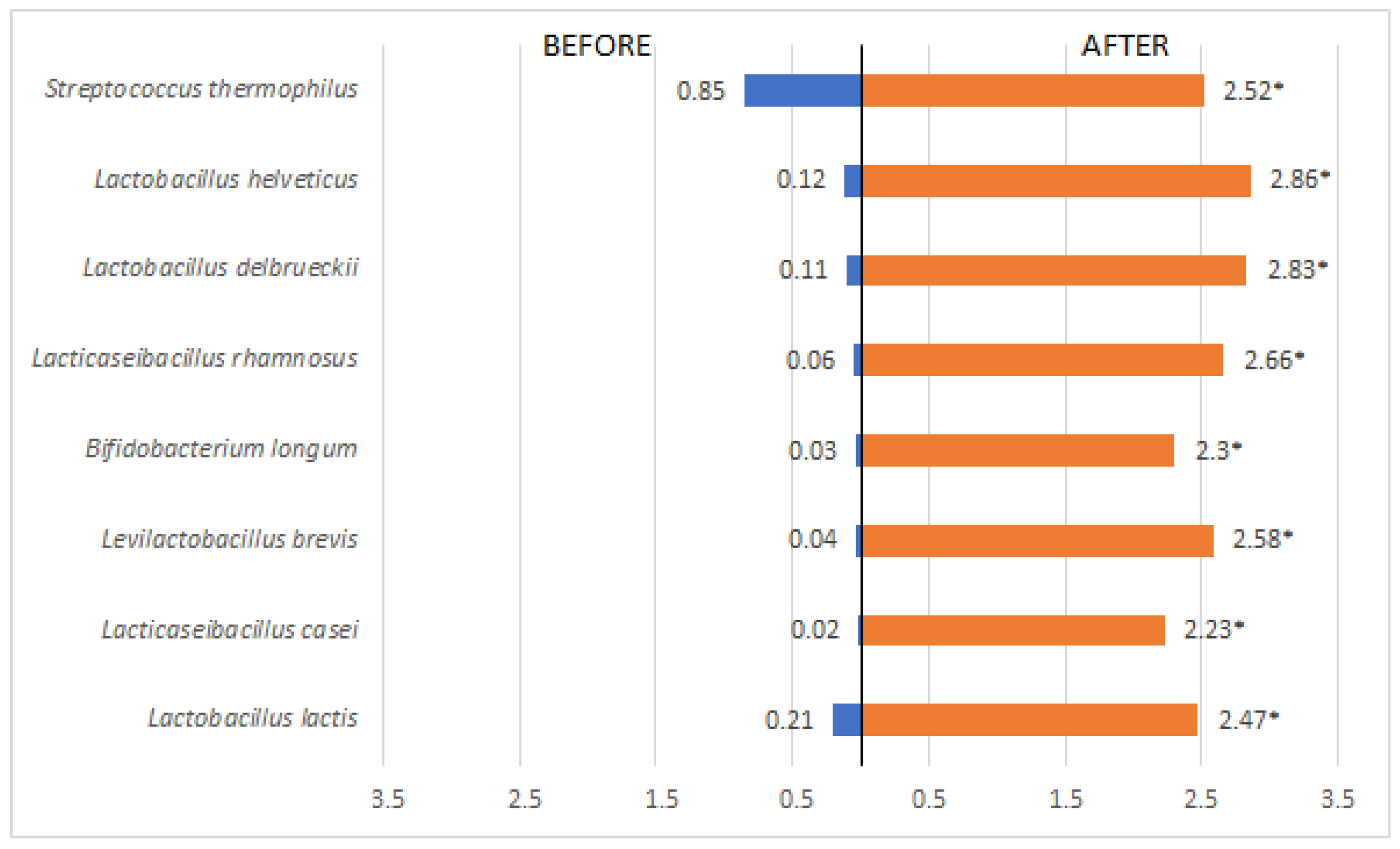
Figure 2.
Analysis of phylum-related rates before and after treatment. *p<0.05 = statistically significant difference by Wilcoxon Test.
Figure 2.
Analysis of phylum-related rates before and after treatment. *p<0.05 = statistically significant difference by Wilcoxon Test.
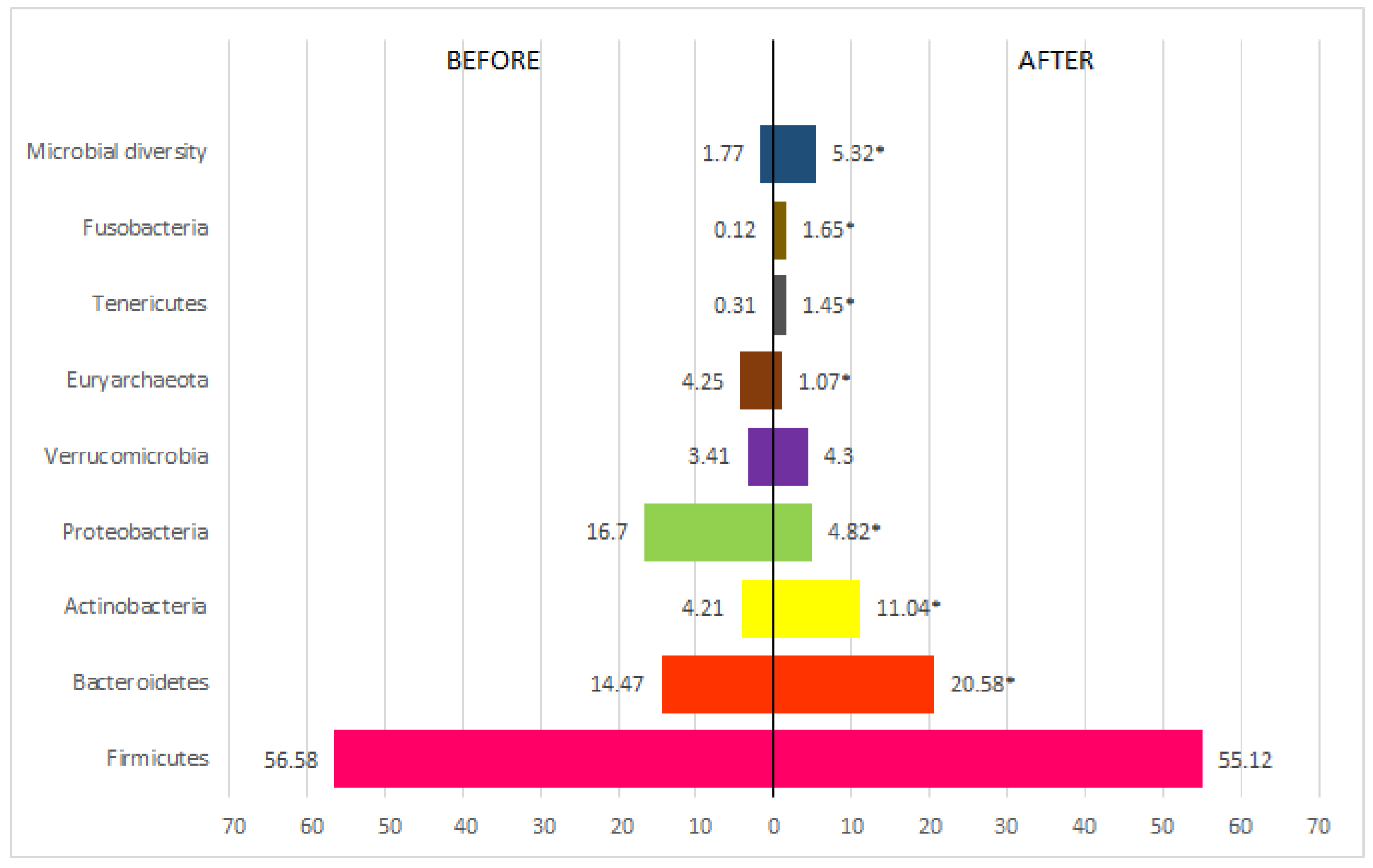
Figure 3.
Bacterial species present in the phylum Firmicutes detected before and after treatment. *p<0.05 = statistically significant difference by the Wilcoxon Test.
Figure 3.
Bacterial species present in the phylum Firmicutes detected before and after treatment. *p<0.05 = statistically significant difference by the Wilcoxon Test.
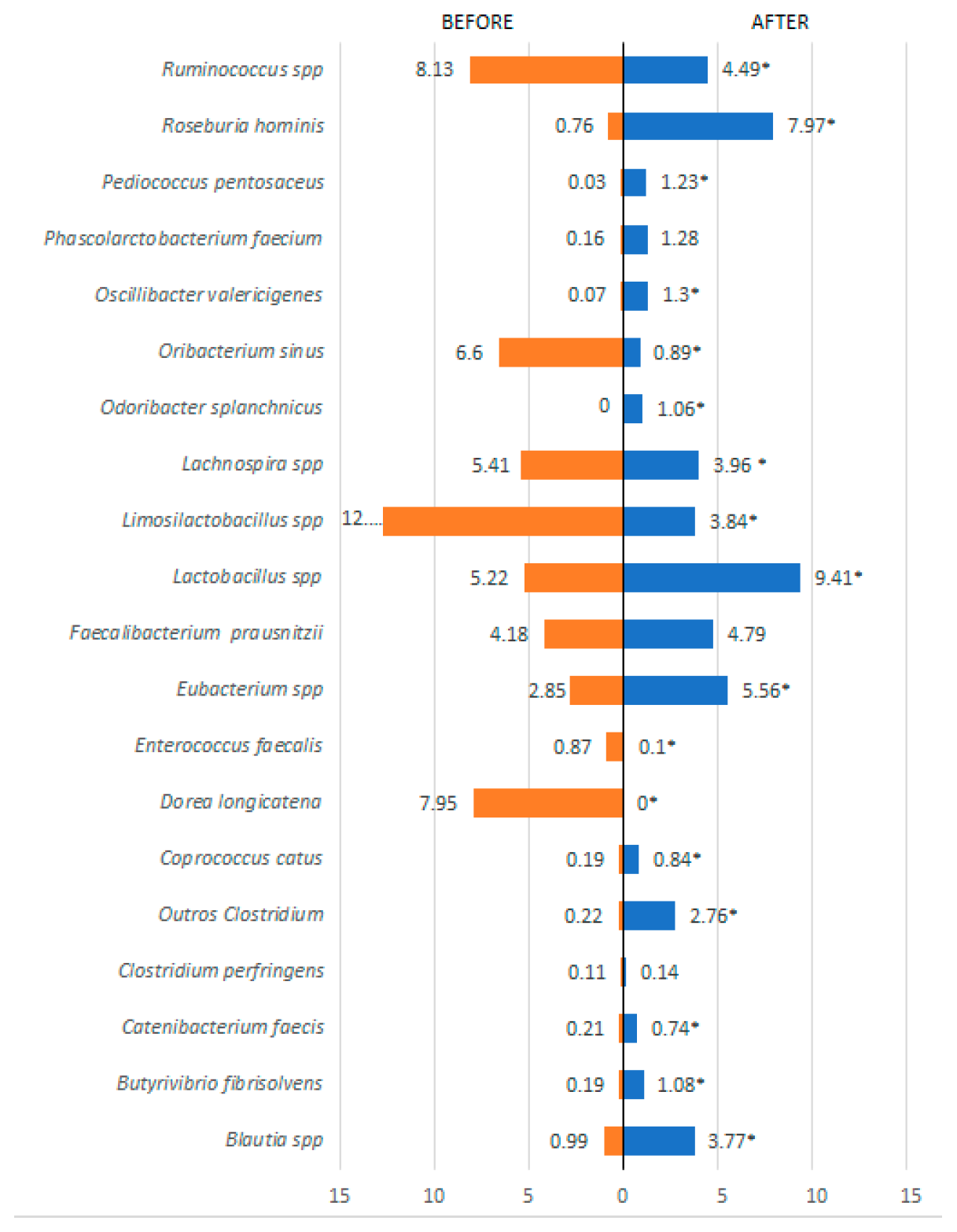
Figure 4.
Bacterial species present in the phylum Bacteroidetes detected before and after treatment. *p≤ 0.05 = statistically significant difference by the Wilcoxon test.
Figure 4.
Bacterial species present in the phylum Bacteroidetes detected before and after treatment. *p≤ 0.05 = statistically significant difference by the Wilcoxon test.
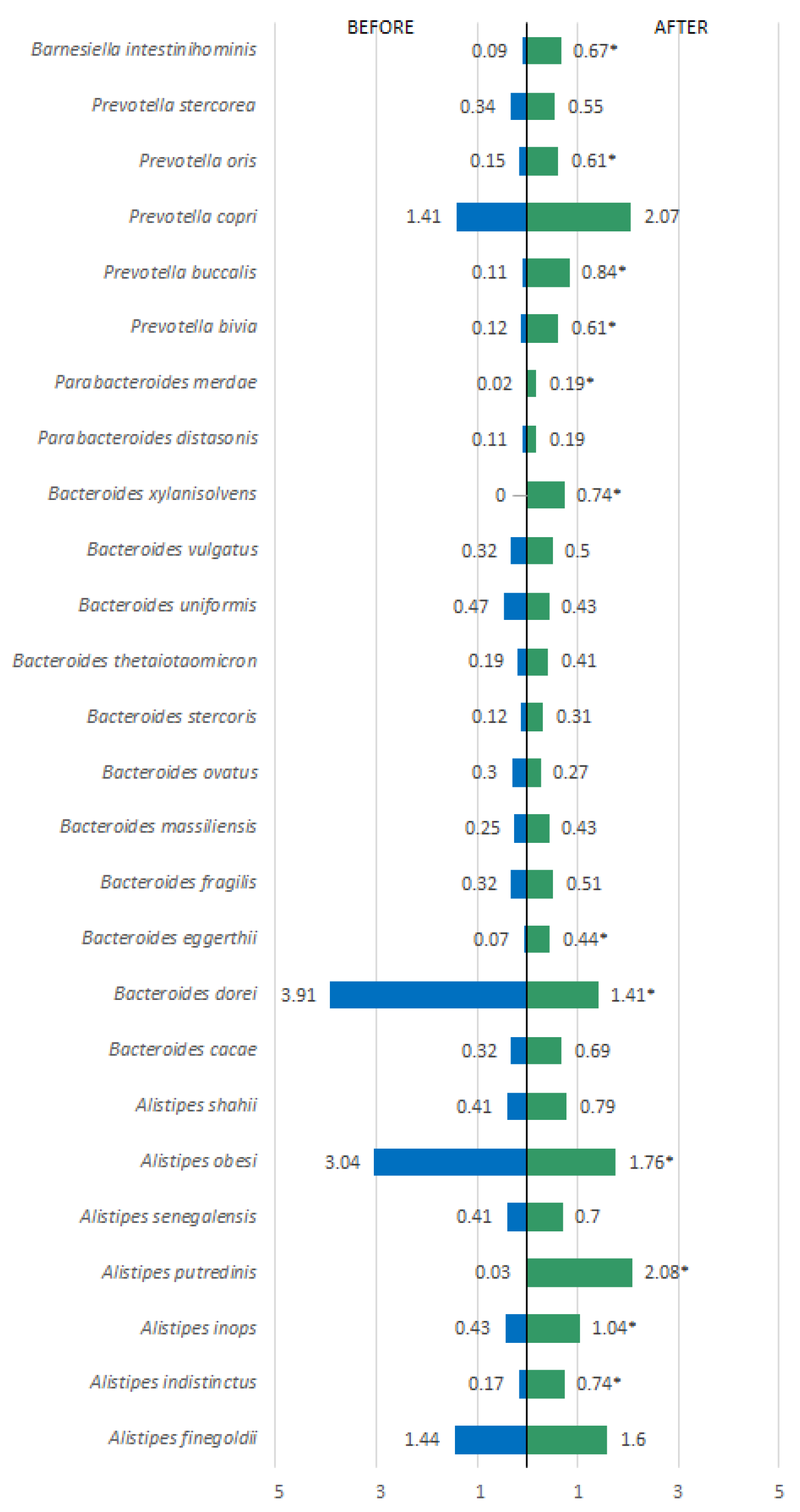
Figure 5.
Bacterial species present in the phyla Verrucomicrobia, Actinobacteria, Proteobacteria, Euryarchaeota, Tenericutes, and Fusobacteria detected before and after treatment. *p<0.05 = statistically significant difference by the Wilcoxon test.
Figure 5.
Bacterial species present in the phyla Verrucomicrobia, Actinobacteria, Proteobacteria, Euryarchaeota, Tenericutes, and Fusobacteria detected before and after treatment. *p<0.05 = statistically significant difference by the Wilcoxon test.
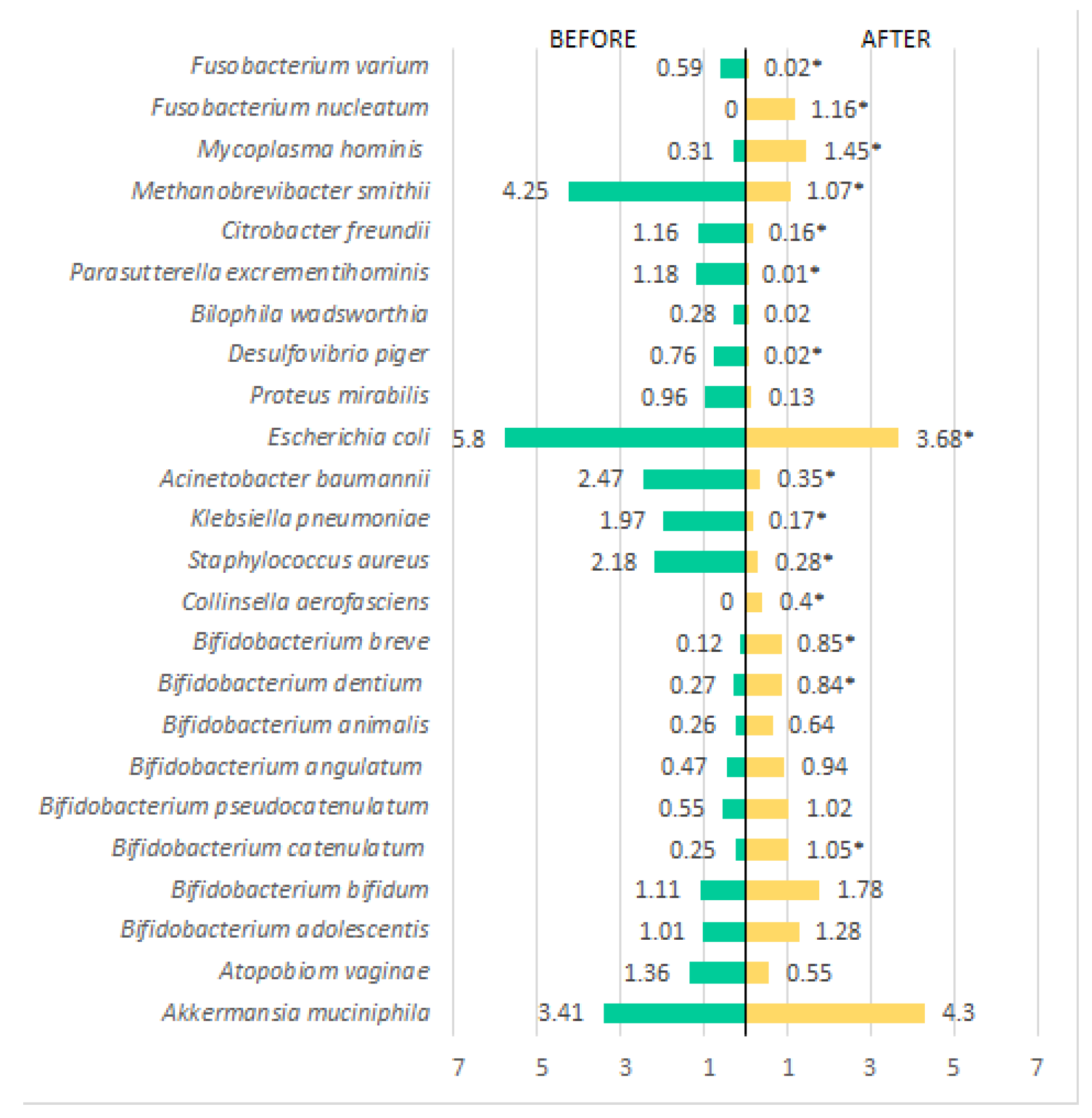
Figure 6.
Schematic Representation of the Evolution of Intestinal Microbiota During Combined Probiotics and Healthy Lifestyle Treatment. A representation of a treatment with probiotics.
Figure 6.
Schematic Representation of the Evolution of Intestinal Microbiota During Combined Probiotics and Healthy Lifestyle Treatment. A representation of a treatment with probiotics.
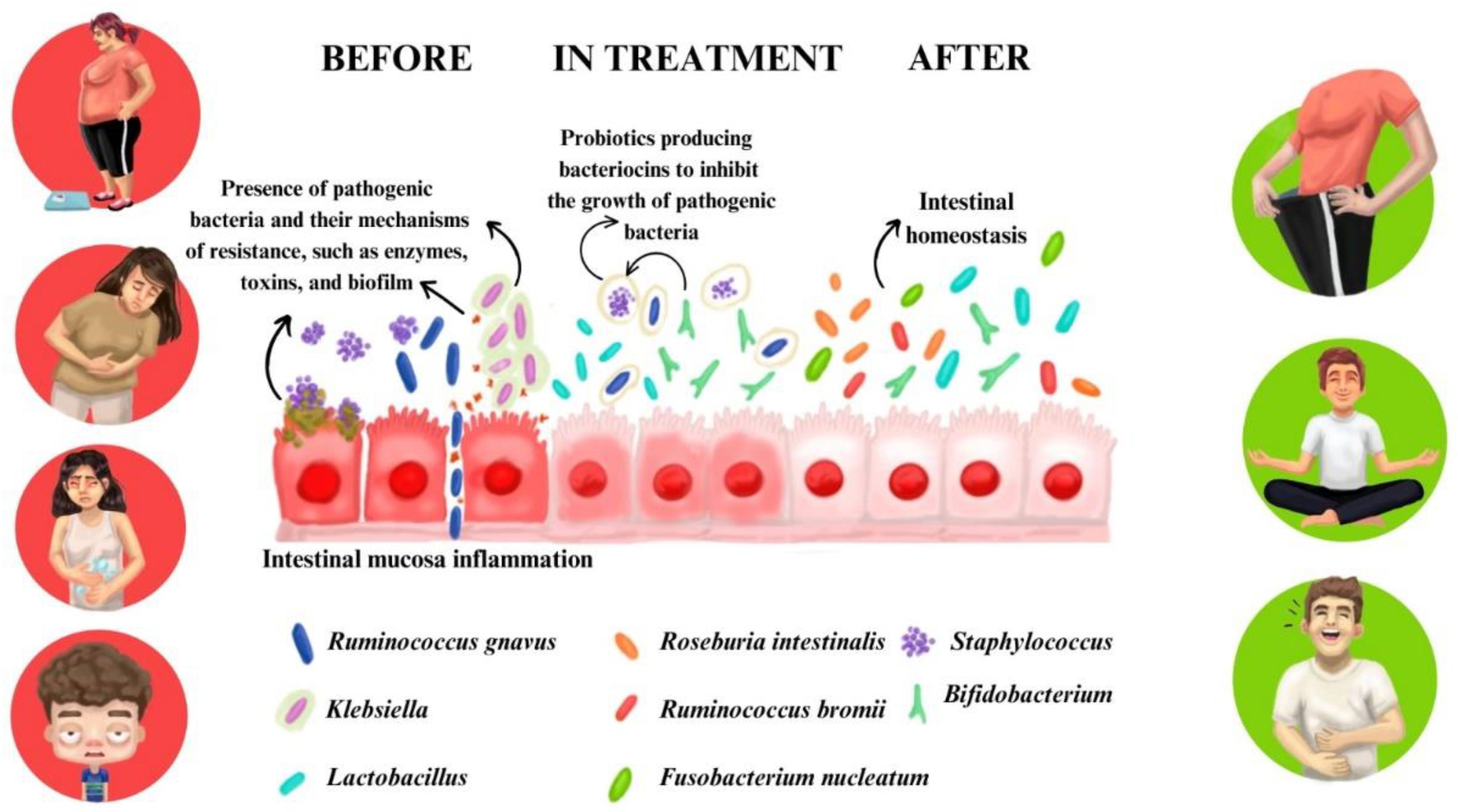

Table 1.
Analysis of variables related to lifestyle habits.
| Variables | Pacients (n=45) | OR (IC)* | Value p** | |
| Before (t0) N(%)1 |
After (t1) N(%) |
|||
| Anxiety - Hamilton | ||||
| No anxiety | 1 (2.2) | 25 (55.6) | 55.00(7.59-307.78) | <0.001 |
| Temporary anxiety | 6 (13.3) | 16 (35.6) | 3.58 (1.14-12.45) | |
| Moderate anxiety | 14(31.1) | 2 (4.4) | 0.10 (0.01-0.51) | |
| Severe anxiety | 24(53.3) | 2 (4.4) | 0.04 (0.00-0.19) | |
| IPAQ | ||||
| Very active | 8 (17.8) | 34 (75.6) | 14.29(4.65-45.58) | <0.001 |
| Active | 9 (20.0) | 8 (17.8) | 0.86 (0.30-2.49) | |
| Irregularly active | 8 (17.8) | 0 (0) | NC2 | |
| Sedentary | 20 (44.4) | 3 (6.7) | 0.09 (0.01-0.35) | |
| Sleep – Pittsburgh | ||||
| Good sleep quality | 14 (31.1) | 39 (86.7) | 14.39 (4.51-49.80) | <0.001 |
| Poor sleep quality | 31 (68.9) | 6 (13.3) | 0.07 (0.02-0.22) | |
| Fiber consumption | ||||
| Yes | 39 (86.7) | 43 (95.6) | 3.30(0.63-17.36) | 0.125 |
| No | 6 (13.3) | 2 (4.4) | 0.30(0.06-1.54) | |
| Water intake (cups/day) | ||||
| 1 | 2 (4.4) | 6 (13.3) | 3.30(0.63-17.36) | <0.001 |
| 2-5 | 31 (68.9) | 5 (11.1) | 0.06(0.02-0.17) | |
| 6-9 | 8 (17.8) | 11 (24.4) | 1.50(0.54-4.16) | |
| ≥ 10 | 4 (8.9) | 23 (51.1) | 10.72(3.29-34.92) | |
| Soda consumption | ||||
| Consumes | 30 (66.7) | 12 (26.7) | 0.18 (0.07-0.45) | <0.001 |
| Does not consume | 15 (33.3) | 33 (73.3) | 5.50(2.23-13.61) | |
| Consumption of processed foods | ||||
| Yes | 41 (91.1) | 9 (20.0) | 0.02(0.01-0.09) | <0.001 |
| No | 4 (8.9) | 36 (80.0) | 41.00(11.63-144.55) | |
t0 = before treatment; t1 = 60 days after treatment; 1 N(%) = number of patients (percentage); 2 NC = not calculated; *OR and CI were calculated by comparing post-treatment period to pre-treatment period; IPAQ: International Physical Activity Questionnaire. ** p<0.05 = statistically significant difference by McNemar test (nominal variables) and Wilcoxon test (ordinal variables).
Table 2.
Analysis of physiological parameters of patients before and after treatment.
| Variables | Patients (n=45) | OR (IC)* | Value p** |
|
| Antes (t0) | Após (t1) | |||
| Weight (kg) (1 | 96.67 ± 14.89 | 90.93 ± 15.01 | - | <0.001 |
| Body fat mass (Kg)( | 39.48 ± 9.58 | 33.19 ± 8.36 | - | <0.001 |
| Lean body mass (kg)( | 28.59 ± 6.17 | 29.21 ±6.42 | - | 0.158 |
| BMI | 34.63 ±4.97 | 33.53 ± 5.35 | - | 0.035 |
| Glucose (mmol/L) | 95.93 ± 9.86 | 87.60 ± 6.49 | - | <0.001 |
| HBa1c (%) | 5.59 ± 0.45 | 5.44 ± 0.36 | - | 0.01 |
| Insulin (µUI/I) | 14.33 ± 7.44 | 8.83 ± 5.14 | - | <0.001 |
| HOMA-IR | 3.36 ± 1.84 | 2.37± 2.65 | - | 0.002 |
| HDL (mmol/L)( | 47.62 ± 12.35 | 56.02 ± 13.70 | - | <0.001 |
| LDL (mmol/L) | 136.36 ± 44.07 | 110.69 ± 39.76 | - | <0.001 |
| Triglycerides (mmol/L) | 171.09 ± 97.66 | 103.64 ± 46.01 | - | <0.001 |
| BMI Classification - N(%)2 | ||||
| Overweight | 0 (0) | 13 (28.9) | NC3 | 0.09 |
| Obesity Grade I | 34 (75.60) | 18 (40) | 0.22(0.09-0.53) | |
| Obesity Grade II | 6 (13.30) | 9 (20) | 1.62(0.53-5.02) | |
| Obesity Grade III | 5 (11.1) | 5 (11.1) | 1.00(0.27-3.72) | |
| Bowel Movement Frequency N(%) | ||||
| Daily | 21 (46.7%) | 40 (89.9%) | 9.14(3.05-27.44) | <0.001 |
| Every Other Day | 10 (22.2%) | 0 (0) | NC | |
| 2 Times/Week | 5 (11.1%) | 3 (6.7%) | 0.54(0.13-2.55) | |
| Every 5 Days or More | 9 (20%) | 1 (2.2%) | 0.09(0.01-0.75) | |
| Bristol Stool Scale - N(%) | ||||
| 3 and 4 | 10 (22.2%) | 34 (75.6) | 10.81(4.07-28.76) | <0.001 |
| Others | 35 (77.8) | 11 (24.4) | 0.09(0.03-0.27) | |
t0 = before treatment; t1 = 60 days after treatment; HBa1c = Glycated hemoglobin. BMI =Body Mass Index; HOMA-IR = Homeostasis model assessment for insulin resistance; LDL= Low-density lipoprotein; HDL= High-density lipoprotein. 1 (±dp)=(Mean ± standard deviation); 2N(%)= Number of patients (percentage); 3NC=not calculated; * OR (Odds Ratio) and CI (Confidence Interval) were calculated by comparing the post-treatment period to the pre-treatment period. ** p<0.05 = statistically significant difference by McNemar test (nominal variables) and Wilcoxon test (ordinal variables) and t-Student test (quantitative variables).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



