
Submitted:
16 February 2024
Posted:
17 February 2024
You are already at the latest version
Abstract
This retrospective study aimed to compare risk factors for vascular calcification (VC) between pre-hemodialysis (HD) and prevalent HD adult patients while investigating associations with calcification biomarkers. Baseline data from 30 pre-HD and 85 HD patients were analyzed, in-cluding iPTH, vitamin D, FGF-23, fetuin-A, sclerostin and VC scores (Adragao method). Preva-lence of VC was similar in both groups, but HD patients had more frequent VC scores ≥6. Pre-HD patients were older, with higher prevalence of hypertension and less frequent use of calcium phosphate binders. Both groups showed similar patterns of hyperphosphatemia, low vitamin D, and iPTH. Fetuin-A levels were higher in pre-HD, while FGF-23 was elevated in HD patients. Higher VC risk in pre-HD patients was associated with male gender, older age, lower fetuin-A and higher sclerostin, lower ferritin and no vitamin D treatment, while in HD patients with higher sclerostin, FGF23 and urea, and lower iPTH. Conclusion. Progression of CKD from the pre-HD to the HD stage is accompanied by a decreased effect of the inhibitor and an increase in the promoter VC. However, mineral imbalance, hormonal regulation, treatment options, and patient-specific fac-tors should be considered. Further studies are needed to elucidate the underlying pathways.
Keywords:
chronic kidney disease
; vascular calcifications
; FGF-23
; Fetuin-A
; sclerostin
; iPTH
; Adragao score
1. Introduction
Vascular calcification (VC) stands as a hallmark complication of chronic kidney disease (CKD), with its prevalence increasing across CKD stages, culminating in its highest incidence in end-stage kidney disease (ESKD) patients [1]. Evidence suggests that CKD patients having VC from stage 3 to the beginning of dialysis treatment have more rapid progression of calcification during dialysis [2,3].
There is growing evidence that patients with CKD are prone to VC due to disturbed homeostatic mechanisms. Existing literature highlights the interplay of various risk factors, encompassing traditional elements such as age, hypertension, and diabetes (T2D), along with emerging contributors like oxidative stress, mineral metabolism disturbances, and renal bone disease [4]. Additionally, imbalances in circulating biomarkers including parathyroid hormone (iPTH), fibroblast growth factor-23 (FGF-23), and sclerostin that promotes or Fetuin-A that inhibits VC processes have emerged as potential markers of VC susceptibility of CKD patients [3,4,5]. Emerging insights highlight the active role of vascular smooth muscle cells (VSMCs) transitioning into osteoblast-like cells in VC pathogenesis [6]. However, the molecular underpinnings, especially the interplay of calcification promoters and inhibitors, remain inconsistent and remain an evolving area of research [4,7]. While earlier studies focused on establishing the involvement of biomarkers in the pathophysiology of VC in CKD patients, contemporary therapeutic approaches now aim to leverage biomarkers for the prevention and treatment of VC in this population [8,9,10,11,12]. Despite some promising results, they are not yet in use for VC treatment. So far, studies examining the dynamics of VC biomarker changes during the progression from CKD to the dialysis phase are lacking. Understanding how these biomarkers evolve in advanced CKD is crucial for identifying specific targets for interventions aimed at preventing or mitigating VC.
Several factors motivated the examination of VC in our clinical context. The rising number of CKD patients, coupled with the compromised outcomes they face, underscores the significance of identifying modifiable risk factors for VC in CKD stage 5 individuals not yet undergoing dialysis. Furthermore, it is vital to note that VC treatment primarily relies on controlling various risk factors, emphasizing the ongoing need to discover new therapeutic targets to mitigate the adverse consequences of VC. In the available literature, there are no papers that simultaneously analyze the change in biomarkers in patients with advanced CKD and those treated with dialysis. Therefore, this cross-sectional study was undertaken with the aim to compare clinical and biochemical profile between two groups of patients with VC: the pre-hemodialysis (pre-HD) and prevalent HD patients.
2. Materials and Methods
2.1. Patients
This cross-sectional study involved 30 pre-hemodialysis adult patients (pre-HD group) and 85 adults on hemodialysis (HD group) selected from the pool of patients monitored in outpatient departments or treated by chronic HD in three nephrology departments presented in flow chart (Figure 1).
Patients were enrolled if they: 1) had eGFR<15ml/min/1.73m2 and were regularly controlled by a nephrologist in the above-mentioned departments (pre-HD group) or had been on HD for at least 6 months (HD group); 2) agreed to participate in the study, which was approved by the institutional review board; 3) did not have acute cardiovascular complications during the 6 months preceding entry into the study; 4) had no hemodynamically significant lower extremity artery occlusive disease; 5) did not have uncontrolled blood pressure.
The local Ethics Committee evaluated and approved the study protocol (decision No 1690/21, June 9, 2015) and all patients provided written informed consent.
Standard bicarbonate HD sessions lasted 12 hours weekly. Dialysate calcium (dCa) was individualized to meet the specific requirements of each patient by optimizing treatment in order to achieve the target values of serum calcium, phosphate, iPTH and alkaline phosphatase levels recommended by the KDIGO guideline [13]. Calcium based phosphate binders, alphacalcidiol or calcitriol were mostly used in studied patients. Variables of interest taken from the patients’ records were: demographic (age, sex), underlying kidney disease, dialysis duration, systolic and diastolic blood pressures, previous history of cerebrovascular and cardiovascular diseases: coronary artery disease (CAD); congestive heart failure (CHF); peripheral vascular disease (PVD); parathyroidectomy due to secondary hyperparathyroidism and medications (antihypertensives, intestinal phosphate binders, Vitamin D, erythropoetin stimulating agents (ESA), iron treatment).
2.2. Biochemical analyses
The routine biochemical analyses and measurement of VC biomarkers were done using standard techniques in the same laboratory. Routine laboratory analyses were performed before middle week HD in the HD patients or at regular controls in the outpatient department in the pre-HD patients. Also, serum samples for biomarkers were frozen at -80 degrees until analysis which was done altogether at the same time. Laboratory analyses included measurement of serum urea, creatinine, uric acid, total protein, C-reactive protein (CRP), lipid profile, phosphate, calcium corrected for albumin, alkaline phosphatase, hematological parameters, iron status, and iPTH. Mean standard weekly Kt/V and urea reduction ratio (URR) were calculated for the HD group. We also measured serum levels of 25-(OH) Vitamin D, FGF-23, Fetuin-A and sclerostin. An immunoradiometric assay was used to measure iPTH (enzyme-linked immunosorbent assay (ELISA) PTH, CIS bio International) and normal values are 11-62 pg/mL.A commercial chemiluminescent immunoassay (DiaSorin S.p.A., Italy) was used to determine serum 25-(OH) Vitamin D and measuring range is 7.6 - 147.8 ng/mL. Serum levels of sclerostin, FGF23 and Fetuin-A were determined in duplicate by using comercial available ELISA kits (Elabscience, and Cusabio, USA). The detection assay range for sclerostin, FGF-23 and Fetuin-A were 62.4 - 4000 pg/mL, 3.12 - 200 pg/mL and 9.375 - 600 ng/mL, respectively, with reported intra-assay precision of <10%.
2.3. Calcification assessment
Vascular calcification (VC) in the iliac, femoral, radial and digital arteries in plain radiographic films of the pelvis and hands were evaluated by one person. A simple VC score was calculated as described by Adragao et al. [14]. Although there are more sophisticated methods for VC assessment and being aware that determining the Adragao score is a less sensitive measure, for practical reasons we decided to use that method. The presence of linear calcifications in each section is counted as 1 and its absence as 0. The final score is the sum of all the sections, ranging from 0 to 8.
2.4. Brachial blood pressure
Brachial blood pressure (BP) was measured in all patients in the non-fistula arm. Blood pressure was measured three times at 1-minute intervals according to the European Society of Hypertension - Cardiology guidelines [15]. BP was measured during hemodialysis every hour from the beginning of hemodialysis, and the value for statistical processing was expressed as the mean value of systolic and diastolic BP. In the group of pre-HD patients, BP was measured in the outpatients Department and expressed as the mean value of systolic and diastolic BP calculated from measured BP values during the last six months of control. Patients with BP140/90 are classified as having high BP (counted as 1) and when the BP was below these values it was marked with 0.
2.5. Statistical analysis.
Statistical analysis was performed with SPSS 21.0 (SPSS, Inc, Chicago, IL, USA). Continuous variables are presented as means with standard deviation(SD) for normally distributed variables and as median (inter-quartile range, IQR) for non-normally distributed variables. Categorical variables are presented as frequencies. Chi-square tests and Kruskal–Wallis one-way analysis were used to examine differences in various baseline variables between the groups of patients. Multivariable linear regression model including all significant variables in the univariate linear regression models (at a significance level of 0.05) as well as those predictors that are known to affect the dependent variable mentioned in the section Method i.e. demografic data, standard laboratory analyses, FGF-23, iPTH, vitamin D, fetuin-A and sclerostin, and VC score, was used to determine the independent association with VC score as the dependent variable. Two-sided p-values <0.05 were considered significant.
3. Results
3.1. Study population
Baseline characteristics for both studied groups are shown in Table 1. Comparatively, pre-HD patients were older, with a higher prevalence of HTZ, while HD patients were more inclined to receive calcium-based phosphate-lowering treatment. The primary causes of ESKD were comparable between the groups. The median HD vintage prior to inclusion in this study was 69.5 (125.5) months. Subtotal parathyroidectomy had been performed in 11 HD patients before their enrollment.
Continuous normally distributed variables are presented as mean ± SE; continuous skewed variables are presented as median (IQR)M= male, f= female, GN= glomerular disease, APCD= adult polycystic kidney disease, DM2= diabetes mellitus type 2, Tumor= benign and malignant prostate tumor, hepatocellular liver cancer, bronchial carcinoma, urinary bladder cancer ESA- erythropoietin stimulating agents, CVD- cardiovascular diseases (pre-study period: heart failure, previous myocardial infarction, aorto-coronary by-pass surgery, peripheral vascular disease), CVI- cerebrovascular insult.
Among the 115 subjects under study, VC was detected in 46.6% of pre-HD patients and 57.6% of HD patients. Further analysis revealed a marked VC score ≥ 6 in one patient within the pre-HD group and 15 HD patients, representing a statistically significant difference (p=0.030). Additionally, the highest Adragao score of 8 was observed in six HD patients and was not observed within the pre-HD patient group (Table 1).
3.2. Laboratory analyses
Table 2 presents the basal laboratory analyses. In comparison to the pre-HD group, the HD
group exhibited significantly higher serum concentrations of creatinine, potassium, and ferritin,
while serum sodium was significantly lower
Mean serum levels of calcium, phosphate, intact parathormone (iPTH), and vitamin D fell within the normal range for all patients. Individual value revealed that two HD patients had mild hypercalcemia at 2.7 mmol/L. Also, out of normal range phosphatemia (1.0-1.8 mmol/l) was observed in 33.3% of the pre-HD group and 35.3% of HD patients. Furthermore, 50% of pre-HD patients and 56.5% of those in the HD group had iPTH values below 100 pg/ml. Vitamin D concentration below the lower limit of the reference range was found in 64% of pre-HD patients and 53.6% of those in the HD group. In terms of circulating biomarkers, serum levels of FGF-23 were notably lower (p<0.001) in the pre-HD group, while Fetuin-A concentrations were significantly higher (p<0.001) in comparison to HD group.
Table 3 presents a comprehensive comparison of clinical and biochemical characteristics within and between groups, with and without VC.
Among pre-HD patients, those with VC were notably older, and a higher proportion were males. In both HD patient subgroups, there was more frequent use of phosphate binders compared to pre-HD patients. HD patients without VC had the highest mean phosphate values. Moreover, patients without VC in both groups more often exhibited hyperphosphatemia (>1.9 mmol/l) than those without VC, with the difference approaching significance (p=0.057). Furthermore, within the HD group, a significant difference was observed in phosphate distribution; more patients with VC had normal phosphate levels (p=0.02), while more patients without VC had phosphate above reference range (p=0.005). Regardless of the presence or absence of VC, HD patients displayed higher FGF-23 levels and lower fetuin-A concentrations compared to their pre-HD counterparts.
3.3. Predictors of vascular calcification in studied groups
Table 4 provides the predictors of VC across the patient groups. In the univariate linear regression analysis, demographic data (age, gender), history of cardiovascular diseases, serum urea, creatinine, uric acid, leukocyte count, hemoglobin, iron saturation, ferritin, triglyceride, phosphate, calcium, biomarkers, phosphate binders or vitamin D treatment are exhibited associations with VC.The multivariable linear regression analysis in the HD group highlighted higher levels of sclerostin and FGF 23 (both moderate effects), along with elevated urea (strong effect), are associated with increased VC. Meanwhile, higher levels of PTH are associated with a decrease in VC (strong effect). Patient age, gender, serum sclerostin, fetuin-A, ferritin and vitamin D treatment appear to be significant predictors of VC in the pre-HD group. In other words, the higher levels of serum sclerostin and patient age are associated with increased VC, while higher levels of serum fetuin-A are associated with decreased VC, all with moderate effect. Being female is also associated with decreased VC compared to being male. Also, higher levels of serum ferritin had mild protective effect on VC. Receiving vitamin D treatment is associated with reduction in VC, with a weak effect.
4. Discussion
The prevalence of VC among patients with CKD has long been recognized as a complex and concerning phenomenon. The present study sought to compare frequency and potential risk factors and biomarkers associated with VC in both pre-HD and prevalent HD patients. The key findings are as follows: 1) VC is present in substantial of the examined patients in both groups; 2) while the prevalence of VC remained comparable, the severity of VC differed notably, with the HD group displaying a more prominent VC score ≥ 6; 3) examined circulating biomarkers: iPTH, FGF-23, sclerostin and Fetuin-A were association with VC; 4) serum urea, age, gender and treatment with vitamin D appear to be additionally associated with VC.
Our findings are in agreement with previous studies showing a significant prevalence of VC in the pre-HD and HD groups. While the prevalence of VC remained comparable between the groups i.e. 46.6% of pre-HD patients and 57.6% of HD patients, it noteworthy divergence emerged in the severity of VC. The HD group exhibited a more pronounced VC score of ≥ 6. Prior research has shown that rates of VC measured by the Adragao score, remain similar among advanced CKD patients, reaching up to 57% in CKD stages 4-5. However, the prevalence increases to as high as 75% among dialysis patients [14,16,17]. Recent study has shown that dialysis not only contributes to the progression of VC but also triggers its onset [18]. The similar prevalence of VC in both pre-HD and HD groups raises questions about whether there are shared underlying risk factors or if the progression of VC is influenced by different factors in each group.
Association of biomarkers and vascular calcification in pre-HD and HD group of patients.
The investigation of various biomarkers in the present study revealed their dynamic involvement in VC as CKD progressed from pre-HD to HD. This progression is marked by a shift in the balance between inhibitors and promoters of VC, favoring the latter.
One important VC inhibitor, fetuin-A, is known for its ability to mitigate ectopic calcification in CKD and ESKD kidney disease. By impeding calcium phosphate precipitation, fetuin-A serves as a guardian, protecting human vascular smooth muscle cells from damage [19]. The progressive decline in serum fetuin-A levels from CKD stages 2 to 5 reaches its lowest point in dialysis patients. Discrepancies exist in the literature on the role of fetuin-A in VC development. While some studies report a correlation between persistently low serum fetuin-A levels and increased arterial and valvular calcification scores in patients with CKD and ESRD [20], others do not confirm such an association [21]. Although the values were within normal laboratory limits, our findings revealed significantly higher concentrations of fetuin-A in the pre-HD group than in the HD group, which is consistent with prior research. Regardless of the higher concentration, an inverse relationship with VC was observed, indicating that lower levels of fetuin-A correlate with more frequent VC. This reversal challenges the conventional perception of fetuin-A as a straightforward inhibitor and prompts the consideration of other factors or interactions that may modulate its effectiveness in preventing VC during the pre-HD phase.
Another biomarker associated with VC in pre-HD patients is sclerostin levels. Although its concentration exhibited an insignificant increase in the pre-HD group compared with in that HD patients, a notable positive association between VC and sclerostin was identified. This finding suggests that the influence of sclerostin may surpass the impact of higher fetuin-A concentrations in promoting VC at this stage of CKD. The significance of sclerostin in promoting VC appears to be noteworthy, even with a seemingly modest elevation in its concentration.
Sclerostin, a glycoprotein synthesized by osteocytes, primarily operates by inhibiting the canonical Wnt–β-catenin pathway and has the potential to attenuate bone formation and mineralization. While it is well established that sclerostin has extraskeletal functions, particularly in various vascular disorders, the precise mechanism by which it influences the VC process remains controversial. Some authors have reported positive associations, suggesting the promotion of calcification [22], but others have found negative associations, indicating an inhibitory effect [23].
In the HD group, our findings revealed a positive association between VC, sclerostin, and FGF23, whereas iPTH was negatively associated. These results align with the existing literature, highlighting the roles of sclerostin and FGF23 as VC promoters.
FGF-23, primarily produced by osteocytes in the bone, exerts inhibitory effects on 1,25(OH)2D and iPTH production, playing a crucial role in phosphate regulation by suppressing intestinal phosphate absorption and reabsorption in the proximal tubules. In CKD, elevated FGF-23 levels serve as a compensatory response to the reduced ability of the kidneys to excrete phosphate. However, persistently high FGF-23 levels can lead to mineral imbalances and bone abnormalities, contributing to mineral bone disease [24]. Conflicting results on the association between elevated FGF-23 levels and VC in. CKD have been reported [25,26,27,28]. Clinical studies of HD and CKD stages 2-5 patients indicate positive association of higher FGF23 levels and increased VC, as we have found [24,25,26,27]. In contrast, Scialla et al. reported that a much larger cohort of 1501 patients with CKD stages 2– 4 from the CRIC (Chronic Renal Insufficiency Cohort) study did not show such a relationship between FGF23 levels and the prevalence of coronary artery calcification [28].
The third biomarker, iPTH level, was negatively associated with VC in our HD group, indicating that the lower the iPTH level, the higher the risk of developing VC. Based on low iPTH levels, we suspected that 42% of our HD patients had adynamic bone disease [29,30,31,32]. It should not be overlooked that a smaller percentage of HD patients studied here (11%) had iPTH levels higher than 500 pg/ml and were suspected to have secondary hyperparathyroidism, meaning that half of HD patients have some disturbance in the iPH level. It is well known that elevated iPTH levels leading to high-turnover bone disease and low PTH levels, which are risk factors for low bone turnover (adynamic bone disease), can augment VC development and progression [33,34]. When bone turnover is low, as with adynamic bone, the amount of interchangeable calcium and phosphate is decreased, and higher blood concentrations are associated with its intake. Also, bone resorption is more prominent than bone formation, interfering with the buffering function of the skeleton for extra phosphate [35,36]. This phenomenon, known as "calcification paradox", indicates a high risk of ectopic calcifications, including VC in patients with CKD and dialysis during reduced bone mineralization [37]. By contrast, when high bone turnover is present as in secondary hyperparathyroidism, phosphate is released from bone and, again, the reservoir function of the skeleton is destroyed [6].
In dialysis patients with VC, the interplay between iPTH, FGF23, and sclerostin is complex. Each biomarker is independently associated with VC, but their interaction appears to potentiate VC. Secondary hyperparathyroidism in CKD contributes to increased bone turnover by releasing calcium and phosphate, which can contribute to blood VC and indirectly influence FGF23 and sclerostin regulation. Conversely, low iPTH levels, whether induced by drugs, vitamin D, or parathyroidectomy, may result in elevated levels of FGF23 and sclerostin [38,39]. Furthermore, recent analyses have shown that increased sclerostin levels seem to reflect slower bone turnover, which is often associated with lower iPTH levels. In contrast, lower plasma levels of sclerostin are linked to vitamin D deficiency and effective phosphate control in patients undergoing HD [40]. These observations underscore the importance of monitoring and managing the aforementioned biomarkers in clinical practice to prevent complications such as VC and bone abnormalities, prompting further exploration of their complex interactions and potential implications for therapeutic interventions.
Other risk factors for VC in pre-HD and HD group of patients
Besides the imbalances in biomarkers, some demographic and laboratory data were associated with VC in the examined groups. The patients differed in age in favor of the pre-HD group, and older age was a predictor of VC. In the pre-HD group, a higher prevalence of VC was found in men, which is consistent with some studies in patients with CKD [41]. According to previously published data, potential contributors to the observed gender-related differences involve hormonal, lifestyle, genetic, disease duration factors, pericardial/total fat, lipid profile, inflammatory status, variations in matrix Gla protein (MGP), soluble Klotho, vitamin D, sclerostin, iPTH, FGF-23, and osteoprotegerin levels [41]. In addition, serum ferritin level was independently associated with VC in the pre-HD group. This finding is in line with a previous report that ferritin prevents calcification and osteoblastic transformation of muscle cells [42]. Since higher serum ferritin levels have a protective effect on VC, regular monitoring of ferritin levels in pre-HD patients should be considered. Our study also showed that vitamin D therapy had a protective effect against VC in the pre-HD group. More than 60% of the pre-HD patients had vitamin D deficiency/insufficiency, and one-third of them received vitamin D supplementation. Vitamin D supplementation has an adjunctive role in regressing proteinuria, reversing renal osteodystrophy, and restoring calcification inhibitors in patients with CKD [43]. Therefore it is advisable to monitor and restore vitamin D defficiency in CKD patients.
The present analysis did not show an independent association between serum phosphate and VC in either pre-HD or HD patients, which has been cited in numerous studies. To comply with the KDIGO recommendations to control phosphate within a target range to minimize complications such as VC and bone disease [13,44], we prescribed regular HD to our patients, a restrictive phosphate diet, and 94.2% of HD patients took calcium-based phosphate binders, either alone or in combination with vitamin D. Thus, most of the patients studied here had normal phosphate levels, and up to 27% had hyperphosphatemia. Nevertheless, strict control of phosphate and calcium levels is still an obligation of nephrologists to prevent VC and cardiovascular diseases.
Significance and limitations of the study
Our study showed that the progression of CKD from the pre-HD to the HD stage is accompanied by dynamic changes in biomarkers associated with VC, including a decrease in inhibitors and an increase in promoters of VC, which suggests potential avenues for considering interventions, including risk stratification, treatment response assessment, individualized treatment planning, and contributing to research and drug development. It is important to acknowledge several limitations that warrant consideration when interpreting these results. Our study was constrained by its retrospective nature, limitations in data collection, and potential bias. The cross-sectional design of the study restricted our ability to establish temporal relationships between variables and better elucidate the dynamic interactions between risk factors, biomarkers, and the development of VC over time. The relatively modest sample size and patient heterogeneity in both groups limits the generalizability of our findings. While the present study identified associations of VC, it does not establish causation and emphasize the importance of individualizing therapy.
5. Conclusions
Our study showed that biomarkers could be measurable indicators of biological processes underlying VC. The progression of CKD from the pre-HD to the HD stage is accompanied by dynamic changes in VC biomarkers, including a decreasein inhibitor action and an increase in promoter action, which suggests potential avenues for considering interventions. However, mineral imbalances, hormonal regulation, treatment options, and patient-specific factors should be taken into account. The complex interplay of multiple factors may contribute to VC, and further studies are needed to elucidate the underlying pathways.
Author Contributions
Conceptualization, VL, MP, VB, MB.; Methodology, VL, SS, NL; Validation, DS.; Formal Analysis, DS., Lj.Dj; Investigation, VL, MP, VB, MB.; Resources, SS, MP, VB, MB, IM, NP.; Writing – Original Draft Preparation, VL.; Writing – Review & Editing, VL, Lj.Dj.; Visualization, VL.; Supervision, VL.; All authors have read and approved the final article.
Funding
The Society of Nephrology of the Republic of Serbia provided financial support for the laboratory analyses.
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of the Clinical Center of Serbia (decision no. 1690/21, 06/09/2015).
Informed Consent Statement
All patients provided written informed consent.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Acknowledgments
This work was conducted as a part of project No 175089 funded by the Ministry of Science, Education and Technological Development, Belgrade, Republic of Serbia.
Conflicts of Interest
The authors report there are no competing interests to declare.
References
- Budoff, M.-J.; Rader, D.-J.; Reilly, M.-P.; Mohler, E.-R., 3rd.; Lash, J.; Yang, W.; Rosen, L.; Glenn, M.; Teal, V.; Feldman, H.-I.; CRIC Study Investigators. Relationship of estimated GFR and coronary artery calcification in the CRIC (Chronic Renal Insufficiency Cohort) Study. Am J Kidney Dis. 2011; Oct;58(4):519-26. Epub 2011 Jul 23. PMID: 21783289; PMCID: PMC3183168. [CrossRef]
- Kestenbaum, B.R.; Adeney, K.-L.; de Boer, I.-H.; Ix, J.-H.; Shlipak, M.-G.; Siscovick, D.-S. Incidence and progression of coronary calcification in chronic kidney disease: The Multi-Ethnic Study of Atherosclerosis. Kidney Int. 2009; 76(9): 991-8. Epub 2009 Aug 19. PMID: 19692998; PMCID: PMC3039603. [CrossRef]
- Schlieper, G.; Schurgers, L.; Brandenburg, V.; Reutlings-Perger, C.; Floege, J. Vascular calcification in chronic kidney disease: an update. Nephrol Dial Transplant 2016; 31: 31–9. Epub 2015 Apr 26. PMID: 25916871. [CrossRef]
- Gungor, O.; Kocyigit, I.; Yilmaz, M.-I.; Sezer, S. Role of vascular calcification inhibitors in preventing vascular dysfunction and mortality in hemodialysis patients. Semin Dial. 2018; 31(1):72-81. Epub 2017 Jun 13. PMID: 28608927. [CrossRef]
- Wolf M. Update on fibroblast growth factor 23 in chronic kidney disease. Kidney Int 2012; 82: 737–47, doi: 10.1038/ki.2012.176. Epub 2012 May 23. PMID: 22622492; PMCID: PMC3434320. [CrossRef]
- London, G.-M.; Marchais, S.J.; Guérin, A.-P.; Métivier, F. Arteriosclerosis, vascular calcifications and cardiovascular disease in uremia. Curr Opin Nephrol Hypertens. 2005; 14(6):525-31. PMID: 16205470. [CrossRef]
- Kakani, E.; Elyamny, M.; Ayach, T.; El-Husseini, A. Pathogenesis and management of vascular calcification in CKD and dialysis patients. Semin Dial. 2019; 32(6):553-561. Epub 2019 Aug 29. PMID: 31464003. [CrossRef]
- Werida, R. H., Abou-Madawy, S., Abdelsalam, M., & Helmy, M. W. Omega 3 fatty acids effect on the vascular calcification biomarkers fetuin A and osteoprotegerin in hemodialysis patients. Clin Exp Medicine, 2022; 22(2), 301–310. [CrossRef]
- Kestenbaum, B. R., Adeney, K. L., de Boer, I. H., Ix, J. H., Shlipak, M. G., & Siscovick, D. S. Incidence and progression of coronary calcification in chronic kidney disease: the Multi-Ethnic Study of Atherosclerosis. Kidney Int, 2009; 76(9), 991–998. [CrossRef]
- Caluwé, R., Pyfferoen, L., De Boeck, K., & De Vriese, A. S. The effects of vitamin K supplementation and vitamin K antagonists on progression of vascular calcification: ongoing randomized controlled trials. Clinical kidney journal, 2016; 9(2), 273–279. [CrossRef]
- Di Lullo, L., Tripepi, G., Ronco, C., D’Arrigo, G., Barbera, V., Russo, D., Di Iorio, B. R., Uguccioni, M., Paoletti, E., Ravera, M., Fusaro, M., & Bellasi, A. Cardiac valve calcification and use of anticoagulants: Preliminary observation of a potentially modifiable risk factor. Int J Cardiol, 2019; 278, 243–249. [CrossRef]
- Sakaguchi, Y., Hamano, T., Obi, Y., Monden, C., Oka, T., Yamaguchi, S., Matsui, I., Hashimoto, N., Matsumoto, A., Shimada, K., Takabatake, Y., Takahashi, A., Kaimori, J. Y., Moriyama, T., Yamamoto, R., Horio, M., Yamamoto, K., Sugimoto, K., Rakugi, H., & Isaka, Y. A Randomized Trial of Magnesium Oxide and Oral Carbon Adsorbent for Coronary Artery Calcification in Predialysis CKD. Journal of the American Society of Nephrology 2019; 30(6), 1073–1085. [CrossRef]
- Ketteler, M.; Block, G.-A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.-A.; McCann, L.; Moe, S.-M.; Shroff, R.; Tonelli, M.-A.; Toussaint, N.-D.; Vervloet, M.-G.; Leonard, M.-B. Executive summary of the 2017 KDIGO chronic kidney disease-mineral and bone disorder (CKD-MBD) guideline update: what’s changed and why it matters. Kidney Int. 2017; 92:26–36. [CrossRef]
- Adragao, T.; Pires, A.; Lucas, C.; Birne, R.; Magalhaes, L.;Gonçalves, M.; Negrao, A.-P. A simple vascularcalcification score predicts cardiovascular risk in haemodialysis patients. Nephrol Dial Transpl2004; 19:1480–1488. Epub 2004 Mar 19. PMID: 15034154. [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De-Backer, G.; Dominiczak, A.; Galderisi, M.; Grobbee, D.-E.; Jaarsma, T.; Kirchhof, P.; Kjeldsen, S.-E.; Laurent, S.; Manolis, A.-J.; Nilsson, P.-M.; Ruilope, L.-M.; Schmieder, R.E.; Sirnes, P.-A.; Sleight, P.; Viigimaa, M.; Waeber, B.; Zannad, F.; Redon, J.; Dominiczak, A.; Narkiewicz, K.; Nilsson, P.-M.; Burnier, M.; Viigimaa, M.; Ambrosioni, E.; Caufield, M.; Coca, A.; Olsen, M.-H.; Schmieder, R.-E.;Tsioufis, C.; van de Borne, P.; Zamorano, J.-L.; Achenbach, S.; Baumgartner, H.; Bax, J.-J.; Bueno, H.; Dean, V.; Deaton, C.; Erol, C.; Fagard, R.; Ferrari, R.; Hasdai, D.; Hoes, A.-W.; Kirchhof, P.; Knuuti, J.; Kolh, P.; Lancellotti, P.; Linhart, A.;Nihoyannopoulos, P.; Piepoli, M.-F.; Ponikowski, P.; Sirnes, P.-A.;Tamargo, J.-L.; Tendera, M.; Torbicki, A.; Wijns, W.; Windecker, S.;Clement, D.-L.; Coca, A.; Gillebert, T.-C.; Tendera, M.; Rosei, E.-A.; Ambrosioni, E.; Anker, S.-D.; Bauersachs, J.; Hitij, J.-B.; Caulfield, M.; De Buyzere, M.; De Geest, S.;Derumeaux, G.-A.; Erdine, S.; Farsang, C.;Funck-Brentano, C.; Gerc, V.; Germano, G.; Gielen, S.; Haller, H.; Hoes, A.-W.; Jordan, J.; Kahan, T.; Komajda, M.; Lovic, D.; Mahrholdt, H.; Olsen, M.-H.; Ostergren, J.;Parati, G.; Perk, J.;Polonia, J.; Popescu, B.-A.; Reiner, Z.; Rydén, L.; Sirenko, Y.; Stanton, A.; Struijker-Boudier, H.;Tsioufis, C.; van de Borne, P.; Vlachopoulos, C.; Volpe, M.; Wood, D.-A. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013; 34(28):2159-2219. Epub 2013 Jun 14. PMID: 23771844. [CrossRef]
- Gorriz, J.-L.; Molina, P.; Cerveron, M.-J.; Vila, R.; Bover, J.; Nieto, J.; Barril, G.;Martínez-Castelao, A.;Fernández, E.; Escudero, V.; Piñera, C.; Adragao, T.; Navarro-Gonzalez, J.-F.; Molinero, L.-M.; Castro-Alonso, C.; Pallardó, L.-M.; Jamal, S.-A. Vascular calcification in patients with nondialysis CKD over 3 years. Clin J Am SocNephrol 2015;10: 654-666. [CrossRef]
- Damjanovic, T.; Djuric, Z.; Markovic, N.; Dimkovic, S.; Radojicic, Z.; Dimkovic, N. Screening of vascular calcifications in patients with end-stage renal diseases. Gen. Physiol. Biophys 2009; 28 Spec No: 277–283. [PubMed].
- Zhang, H.; Li, G.; Yu, X.; Yang, J.; Jiang, A.; Cheng, H.; Fu, J.; Liang, X.; Liu, J.; Lou, J.; Wang, M.; Xing, C.; Zhang, A.; Zhang, M.; Xiao, X.; Yu, C.; Wang, R.; Wang, L.; Chen, Y.; Guan, T.; Peng, A.; Chen, N.; Hao, C.; Liu, B.; Wang, S.; Shen, D.; Jia, Z.; Liu, Z. China Dialysis Calcification Study Group. Progression of Vascular Calcification and Clinical Outcomes in Patients Receiving Maintenance Dialysis. JAMA Netw Open. 2023;6(5):e2310909. PMID: 37126347; PMCID: PMC10152309. [CrossRef]
- Akbari, M.; Nayeri, H.; Nasri, H. Association of fetuin-A with kidney disease; a review on current concepts and new data. J Nephropharmacol 2019; 8(2): e14.
- Ketteler, M.; Bongartz, P.; Westenfeld, R.; Wildberger, J.-E.; Mahnken, A.-H.; Böhm, R.; Metzger, T.; Wanner, C.; Jahnen-Dechent, W.; Floege, J. Association of low fetuin-A (AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: a cross-sectional study. Lancet 2003; 361:827–33. [CrossRef]
- Ulutas, O.; Taskapan, M.-C.; Dogan, A.;Baysal, T.; Taskapan, H. Vascular calcification is not related to serum fetuin-A and osteopontin levels in hemodialysis patients. Int Urol Nephrol 2018; 50(1):137-142. Epub 2017 Nov 13. PMID: 29134617. [CrossRef]
- Qureshi, A.-R.; Olauson, H.; Witasp, A.; Haarhaus, M.; Brandenburg, V.; Wernerson, A.; Lindholm, B.; Söderberg, M.; Wennberg, L.; Nordfors, L.; Ripsweden, J.; Barany, P.; Stenvinkel, P. Increased circulating sclerostin levels in end-stage renal disease predict biopsy-verified vascular medial calcification and coronary artery calcification. Kidney Int 2015; 88(6):1356-1364. Epub 2015 Sep 2. PMID: 26331407. 1356. [CrossRef]
- Claes, K.-J.; Viaene, L.; Heye, S.; Meijers, B.; d’Haese, P.; Evenepoel, P. Sclerostin: Another vascular calcification inhibitor? J Clin Endocrinol Metab 2013; 98(8):3221-8. Epub 2013 Jun 20. PMID: 23788689. 3221. [CrossRef]
- Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.-H.; Scialla, J.; Wahl, P.; Gutiérrez, O.-M.; Steigerwalt, S.; He, J.; Schwartz, S.; Lo, J.; Ojo, A.; Sondheimer, J.; Hsu, C.-Y.; Lash, J.; Leonard, M.; Kusek, J.-W.; Feldman, H.-I.; Wolf, M. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011; 305(23):2432-2439. [CrossRef]
- Nasrallah, M.-M.; El-Shehaby, A.-R.; Salem, M.-M.; Osman, N.-A.; El Sheikh, E.; Sharaf, E.-l.; Din, U.-A. Fibroblast growth factor-23 (FGF-23) is indepenently correlated to aortic calcification in haemodialysis patients. Nephrol. Dial. Transplant 2010; 25: 2679–2685. Epub 2010 Feb 22. PMID: 20176609. [CrossRef]
- Desjardins, L.; Liabeuf, S.; Renard, C.; Lenglet, A.; Lemke, H.-D.; Choukroun, G.; Drueke, T.-B.; Massy, Z.-A. European Uremic Toxin (EUTox) Work Group. FGF23 is independently associated with vascular calcification but not bone mineral density in patients at various CKD stages. Osteoporos Int 2012; 23: 2017–25. Epub 2011 Nov 23. PMID: 22109743s. 2020;32(10):1931-1940. [CrossRef]
- Baralić, M.; Brković, V.; Stojanov, V.; Stanković, S.; Lalić, N.; Đurić, P.; Đukanović, Lj.; Kašiković, M.; Petrović, M.; Petrović, M.; Stošović, M.; Ležaić, V. al. Dual Roles of the Mineral Metabolism Disorders Biomarkers in Prevalent Hemodilysis Patients: In Renal Bone Disease and in Vascular Calcification. J Med Biochem2019; 38(2):134-144. PMID: 30867641; PMCID: PMC6411002. [CrossRef]
- Scialla, J.-J.; Lau, W.-L.; Reilly, M.-P.; Isakova, T.; Yang, H.-Y.; Crouthamel, M.-H.; Chavkin, N.-W.; Rahman, M.; Wahl, P.; Amaral, A.-P.; Hamano, T.; Master, S.-R.; Nessel, L.; Chai, B.; Xie, D.; Kallem, R.-R.; Chen, J.; Lash, J.-P.; Kusek, J.-W.; Budoff, M.-J.; Giachelli, C.-M.; Wolf, M. Chronic Renal Insufficiency Cohort Study Investigators. Fibroblast growth factor 23 is not associated with and does not induce arterial calcification. Kidney Int 2013;83: 1159–68. Epub 2013 Feb 6. PMID: 23389416; PMCID: PMC3672330. [CrossRef]
- Souberbielle, J. C., Roth, H., & Fouque, D. P. Parathyroid hormone measurement in CKD. Kidney Int 2010; 77(2), 93–100. [CrossRef]
- Cannata-Andia, J.-B.; Rodriguez, G.-M.; Gomez, A.-C. Osteoporosis and adynamic bone in chronic kidney disease. J Nephrol 2013; 26:73-80. PMID: 23023723. [CrossRef]
- Barreto, F. C., Barreto, D. V., Moysés, R. M., Neves, K. R., Canziani, M. E., Draibe, S. A., Jorgetti, V., & Carvalho, A. B. K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease in hemodialysis patients. Kidney Int, 2008; 73(6), 771–777. [CrossRef]
- Ureña, P., & De Vernejoul, M. C. Circulating biochemical markers of bone remodeling in uremic patients. Kidney Int, 1999; 55(6), 2141–2156. [CrossRef]
- Thompson, B., & Towler, D. A. Arterial calcification and bone physiology: role of the bone-vascular axis. Nature reviews. Endocrinology, 2012; 8(9), 529–543. [CrossRef]
- Hernandes, F. R., Canziani, M. E., Barreto, F. C., Santos, R. O., Moreira, V. M., Rochitte, C. E., & Carvalho, A. B. The shift from high to low turnover bone disease after parathyroidectomy is associated with the progression of vascular calcification in hemodialysis patients: A 12-month follow-up study. PloS one, 2017; 12(4), e0174811. [CrossRef]
- London, G. M., Marty, C., Marchais, S. J., Guerin, A. P., Metivier, F., & de Vernejoul, M. C. Arterial calcifications and bone histomorphometry in end-stage renal disease. Journal of the American Society of Nephrology 2004; 15(7), 1943–1951. [CrossRef]
- Adragao, T., Ferreira, A., Frazao, J. M., Papoila, A. L., Pinto, I., Monier-Faugere, M. C., & Malluche, H. H. Higher mineralized bone volume is associated with a lower plain X-Ray vascular calcification score in hemodialysis patients. PloS one, 2017; 12(7), e0179868. [CrossRef]
- Persy, V., D’Haese, P. Vascular calcification and bone disease: the calcification paradox. Trends Mol Med 2009; 15: 405–416.
- Drüeke TB. Hyperparathyroidism in Chronic Kidney Disease. [Updated 2021 Oct 18]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc. 2000. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK278975/.
- Bisson, S. K., Ung, R. V., & Mac-Way, F. Role of the Wnt/β-Catenin Pathway in Renal Osteodystrophy. Int J Endocrinology, 2018; 5893514. [CrossRef]
- Pietrzyk, B.; Wyskida, K.; Ficek, J.; Kolonko, A.; Ficek, R.; Więcek, A.; Olszanecka-Glinianowicz, M.; Chudek, J. Relationship between plasma levels of sclerostin, calcium-phosphate disturbances, established markers of bone turnover, and inflammation in haemodialysis patients. Int Urol Nephrol 2019; 51(3):519-526. Epub 2018 Dec 24. PMID: 30584645; PMCID: PMC6424932. [CrossRef]
- Wu, P.-Y.; Lee, S.-Y.; Chang, K.-V.; Chao, C.-T.; Huang, J.-W. Gender-Related Differences in Chronic Kidney Disease-Associated Vascular Calcification Risk and Potential Risk Mediators: A Scoping Review. Healthcare (Basel) 2021; 9(8):979. PMID: 34442116; PMCID: PMC8394860. [CrossRef]
- Becs, G., Zarjou, A., Agarwal, A., Kovács, K. É., Becs, Á., Nyitrai, M., Balogh, E., Bányai, E., Eaton, J. W., Arosio, P., Poli, M., Jeney, V., Balla, J., & Balla, G. Pharmacological induction of ferritin prevents osteoblastic transformation of smooth muscle cells. J Cell Mol Med, 2016; 20(2), 217–230. [CrossRef]
- Hou, Y. C., Liu, W. C., Zheng, C. M., Zheng, J. Q., Yen, T. H., & Lu, K. C. Role of Vitamin D in Uremic Vascular Calcification. BioMed Res Int 2017, 2803579. [CrossRef]
- NKF-KDOQI Guidelines. Available from: http://www.kidney.org/professionals/KDOQI/guidelineupHDPDVA/index.htm [accessed 21.05.2023].
Figure 1.
Flowchart: patient selection.
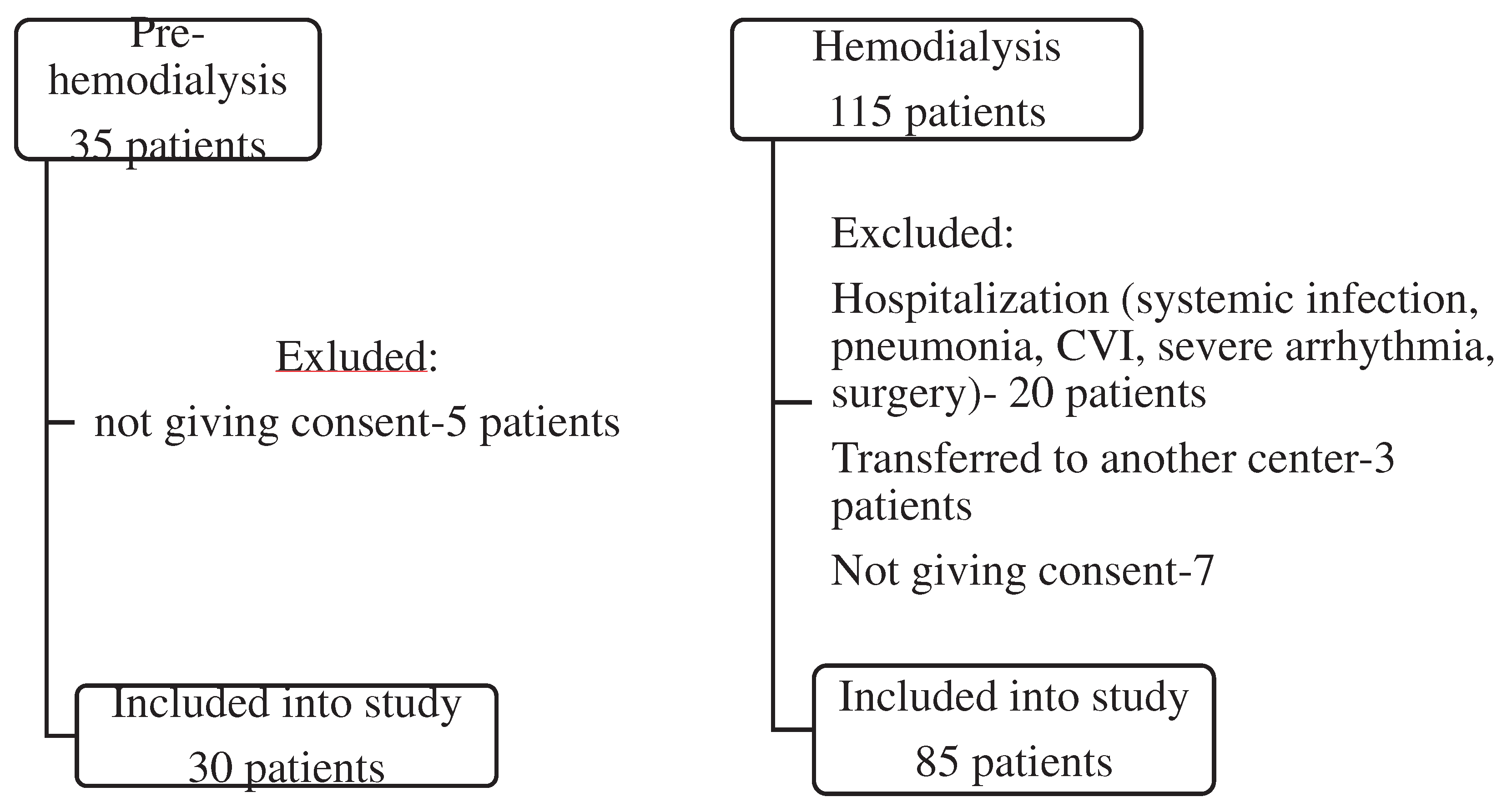

Table 1.
Basal clinical characteristics, presence of co-morbidities, and treatment of the patients in pre- HD and HD groups.
Table 1.
Basal clinical characteristics, presence of co-morbidities, and treatment of the patients in pre- HD and HD groups.
| Pre-HD (No=30) |
HD (No=85) |
p | |
|---|---|---|---|
| Demographics Age, years Sex, m/f |
66.7±2.76 19/11 |
57.72±1.49 40/45 |
0.003 0.141 |
| Underlying kidney disease: (%) GN Nephroangiosclerosis APCD DM2 Nephrolithiasis Others |
3 (10) 6 (20) 2 (6.7) 5 (9.4) 1 (3.3) 13 (43.3) |
15 (17.6) 14 (16.5) 8 (9.4) 8 (9.4) 12 (14.1) 28 (32.9) |
0.394 0.779 1.000 0.442 0.178 0.376 |
| Co-morbidities, yes (%) DM2 Hypertension CVD CVI tumor |
4 (13.3) 27 (90) 14 (46.7) 2 (6.7) 1 (3.3) |
14 (16.4) 65 (76.7) 34 (34.1) 10 (10.6) 8 (8.2) |
0.778 0.029 0.527 0.728 0.442 |
| Treatment, no (%) | |||
| ESA Phosphate binder Alpha D3 Antihypertensive |
7 (23.3) 21 (70) 9 (30) 16 (53.3) |
36 (64.3) 80 (94.1) 25 (29.4) 62 (72.9) |
0.080 0.001 1.000 0.068 |
| VC score, no (%) 0 1-2 ≥ 3 ≥ 6 (8) |
16 (53.3) 4 (13.3) 10 (33.3) 1 (0) |
36 (42.35) 18 (21.2) 31 (37.47) 15 (6) |
0.393 0.384 0.756 0.030 |
Table 2.
Basal laboratory data.
| Pre-HD (N= 30) |
HD (N= 85) |
p-Value | |
|---|---|---|---|
| Cholesterol, mmol/L Triglyceride, mmol/L Hemoglobin, g/L Glycaemia, mmol/L Creatinine, µmol/L Urea, mmol/L Urate, µmol/L Sodium, mmol/L Potassium, mmol/L Calcium, mmol/L Phosphate, mmol/L Feritin, µg/L |
4.83±0.15 1.4 (0.8) 106 (96.7-114.5) 5.2 (4.7-5.55) 552.5 (318-731.2) 23.4 (14.2-32.95) 386.70±24.2 139.87±0.7 4.85±0.1 2.16 (2.05-2.28) 1.53 (1.1-1.8) 84.3(50.75-231.87) |
4.59±1.16 1.65 (1.2-2.8) 108 (101.5-116.5) 4.9 (4.2-6.05) 808 (705.5-915) 21.0 (17.9-26.0) 342.1±10.2 137.86±0.33 5.29±0.08 2.19 (2.1-2.31) 1.65 (1.3-2.03) 355 (131.7-490.1) |
0.891 0.804 0.384 0.663 0.000 0.327 0.100 0.001 0.011 0.541 0.247 0.000 |
| Alkaline phosphatase, IU/L iPTH, pg/ml <100* 25(OH)D ng/ml <29 *(deficiency±insufficiency) |
73.5 (61.5-99.2) 200.9 (34.57) 11 (36.6%) 24.7 (46.22) 19 (64.28) |
87 (60-109) 118 (49.5-238.5) 36 (42.3%) 27.5 (19.2-48.05) 45 (53.6%) |
0.304 0.710 0.879 |
| Fetuin A, ng/ml | 520 (383-600) | 339.5 (244.5-432.6) | 0.000 |
| Sclerostin, pg/ml | 3190 (2550-4520) | 2105 (811-5105) | 0.103 |
| FGF23, pg/ml | 154.5 (71.2-233.6) | 1108 (382-1500) | 0.000 |
All variables are presented as mean ± SD, and median (IQR) * number of patients with percentage in parenthesis.
Table 3.
Differences between patients with and without vascular calcification within each group.
| Pre HD group | HD group | p | |||
|---|---|---|---|---|---|
| 1 VC + |
2 VC neg |
3 VC + |
4 VC neg |
||
| Number | 14 | 16 | 49 | 36 | |
| Age, years | 71.7±2.05 | 62.5±4.68 | 58.66±1,98 | 56.43±2.28 | 1 vs 3, 4 p< 0.001 |
| Sex, m/f | 12/2 | 7/9 | 23/26 | 17/19 | 1 vs 2, 3,4 p < 0.02 |
| ESA, yes /no | 2/12 | 5/11 | 20/29 | 16/20 | 1 vs 4 p= 0.05 |
| Phosphate binder, yes/ no | 9/5 | 12/4 | 47/2 | 33/3 | 1 vs 3,4 p<0.03 2 vs 3 p=0.028 |
| Phosphate, mmol/l | 1.57±0.16 | 1.51±0.11 | 1.54±0.06 | 1.87±0.08 | 4 vs 2, 3 p< 0.018 |
| Phosphate range, mmol/l <1.0 1.0 -1.8 ≥1.9 |
2 8 4* |
2 12 2* |
2 37 a 10 b, * |
0 18 a 18b, * |
a p=0.020 b p= 0.005 * 2+4 vs 1+3, p=0.057 |
| FGF 23, pg/ml | 140.75 (205) | 156 (165.7) | 1006 (1175) | 1500 (830) | 2 vs 3, 4 p< 0.0001 1 vs 3, 4 p< 0.004 |
| Fetuin A, ng/ml | 552.5(295) | 498 (162) | 326 (204) | 377 (193) | 1 vs 3, 4 p =0.001 2 vs 3, 4 p< 0.003 |
Continuous normally distributed variables are presented as mean ± SE; continuous skewed variables are presented as median (IQR) ESA- erythropoietin stimulating agents, FGF 23- fibroblast growth factor 23.
Table 4.
Predictors of vascular calcification in studied groups, selected with multivariable linear regression analysis.
Table 4.
Predictors of vascular calcification in studied groups, selected with multivariable linear regression analysis.
| B | OR | 95% CI for OR | p | |
|---|---|---|---|---|
| Pre-HD group | ||||
| Fetuin-A | -0.0271 | -1.701 | -0.030- -0.024 | 0.001 |
| Sclerostin | 0.0023 | 1.463 | 0.002- 0.003 | 0.001 |
| Gender | -7.465 | -1.607 | -8.128- -6.803 | 0.000 |
| Age | 0.162 | 1.269 | 0.148-0.177 | 0.000 |
| Ferritin | -0.0048 | -0.252 | -0.007- -0.002 | 0.014 |
| Vit D treatment | -0.766 | -0.187 | -1.259- -0.274 | 0.022 |
| (Constant) | 0.236 | 0.263 | ||
| HD Group | ||||
| Sclerostin | 0.0005 | 0.389 | 0.000-0.001 | 0.012 |
| FGF 23 | 0.0015 | 0.315 | 0.000-0.003 | 0.036 |
| Urea | 0.193 | 0.446 | 0.069- 0.318 | 0.004 |
| iPTH | -0.0054 | -0.553 | -0.008- 0.003 | 0.001 |
| (Constant) | 10.908 | 3.295 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



