
Submitted:
19 February 2024
Posted:
20 February 2024
You are already at the latest version
Abstract
Despite available global efforts and funding, Tuberculosis (TB) continues to affect a considerable number of patients worldwide. Policy makers and stakeholders set clear goals to reduce TB incidence and mortality, but the emergence of multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB) complicate the reach of these goals. Drug-resistance TB needs to be diagnosed rapidly and accurately to effectively treat patients, prevent the transmission of MDR-TB, minimise mortality, reduce treatment costs and avoid unnecessary hospitalisations. In this narrative review, we provide a comprehensive overview of laboratory methods for detecting drug resistance in MTB, focusing on phenotypic, molecular and other drug susceptibility testing (DST) techniques. We found a large variety of methods used, with the BACTEC MGIT 960 being the most common phenotypic DST and the Xpert MTB/RIF being the most common molecular DST. We emphasise the importance of integrating phenotypic and molecular DST to address issues like resistance to new drugs, heteroresistance, mixed infections and low-level resistance mutations. Notably, most of the analysed studies adhered to the outdated definition of XDR-TB and did not consider the pre-XDR definition, thus posing challenges in aligning diagnostic methods with the current landscape of TB resistance.
Keywords:
Mycobacterium tuberculosis
; multidrug-resistant
; extensively drug-resistant
; diagnostic methods
; point-of-care
; phenotypic methods
; molecular methods
; drug resistance detection
; rapid test
1. Introduction
Mycobacterium tuberculosis (MTB) is responsible for tuberculosis (TB) disease in humans. MTB bacilli are transmitted from person to person through close contact by inhalation of infectious aerosols, establishing an infection that may remain latent, yet still maintains a 5-10% probability of progressing to active disease. The lungs are the preferred site of MTB bacilli infection, where they can multiply and cause pulmonary TB in both immunocompetent and immunocompromised hosts. However, in immunocompromised patients, MTB bacilli can disseminate to other body sites, causing extrapulmonary TB [1,2].
In 2022, the World Health Organization (WHO) estimated 7.5 million new TB cases and 1.3 million deaths. Compared to the previous years, this represents a significant global increase in diagnosed and treated TB cases, following two years of disruptions due to the COVID-19 pandemic. Indeed, COVID-19 disruptions are believed to have resulted in an additional half a million TB-related deaths during 2020-2022, compared to what would have been expected if pre-pandemic trends had continued [2]. The WHO’s End TB strategy aims for a 90% reduction in TB incidence and a 95% decrease in TB deaths by 2035 [3]. However, this aim is complicated by drug-resistant TB; in 2022, the WHO estimated 410,000 cases of TB resistant to at least Rifampicin (RIF), the most effective drug in TB treatment [2].
The main mechanism of acquisition of drug resistance in TB involves point-mutation in resistance-associated genes, predominantly single-nucleotide polymorphisms (SNP)s, but insertions and deletions are also possible. However, phenotypic resistance may result from a complex network of mutations in different genes, including compensatory mutations that mitigate the fitness cost of the resistance [4]. The WHO classifies drug-resistant TB into various types: RIF-resistant TB (RR-TB), multi-drug-resistant TB (MDR-TB, resistant to RIF and isoniazid (INH), two of the first-line drugs, FLDs), pre-extensively drug-resistant TB (pre-XDR, MDR-TB additionally resistant to any fluoroquinolone, FQ), and extensively drug-resistant TB (XDR-TB, MDR-TB additionally resistant to any FQ and at least one of the priority A drugs Linezolid (LZD) and Bedaquiline, BDQ) [2,5]. The category of pre-XDR and the new XDR-TB definition were introduced by the WHO in 2021; both definitions have significant clinical relevance [6,7]. With these changes in definitions, diagnostic laboratories must adapt accordingly; surveys among TB reference laboratories in the European region indicate that while laboratories are well-equipped to test resistance to “established” drugs such as FQs, LZD, or second-line injectable drugs (SLIDs) like amikacin (AMK) or kanamycin (KAN), they are less prepared for “novel” drugs such as BDQ, crucial for treating MDR-TB [8,9].
Historically, the laboratory diagnosis of TB resistance relied on phenotypic methods using MTB cultures grown in the presence of antibiotics (referred to hereafter as phenotypic drug-susceptibility testing, pDST). However, modern diagnostics methods have shifted towards molecular techniques that detect mutations in resistance-associated genes (referred to hereafter as molecular DST) [10,11]. Early and accurate diagnosis of drug-resistant TB is crucial for appropriately treating patients, preventing further MDR-TB transmission, reducing mortality and minimising treatment costs and unnecessary hospitalization. Inadequate treatment can select resistant TB subpopulations, leading to MDR-TB, XDR-TB, or novel resistant isolates, thus limiting the available treatment options [12,13,14].
With this narrative review, we aim to provide an overview of recent advancements in diagnostic methods for detecting drug resistance in MTB. One question also motivated us to write this review: how have the new pre-XDR and XDR-TB definitions impacted the current state of MTB drug-resistance diagnostics? We will also discuss the challenges of implementing such methods in routine diagnostics across different settings, such as low- versus high-resource settings. This review is intended to help clinical microbiologists understand the range of available resistance detection methods together with their limitations and highlight the advantages and challenges of implementing specific methods in routine diagnostics.
2. Materials and Methods
The methodology to conduct this narrative review was inspired (with some obvious changes) by a similar article about drug-resistance diagnostics in Staphylococcus aureus published by one of the authors [15] and it was conducted according to the guidelines published by Ferrari [16].
A list of relevant keywords about the topic of this narrative review was developed. The databases PubMed and Web of Science (WoS) were chosen. This was the search string used in the PubMed database (30th April 2023): Tuberculosis, Multidrug-Resistant/diagnosis[Mesh] OR Extensively Drug-Resistant Tuberculosis/diagnosis[Mesh] OR (resistance detection [Title/Abstract] OR antimicrobial susceptibility testing [Title/Abstract] OR microbial sensitivity tests/methods[Mesh] OR microbial sensitivity tests/standards[Mesh] OR point-of-care testing[MeSH] OR point-of-care systems[MeSH] OR phenotypic drug resistance testing OR genotypic drug resistance testing OR resistance prediction [Title/Abstract] OR rapid detection [Title/Abstract] OR rapid diagnosis [Title/Abstract] OR molecular diagnosis [Title/Abstract] OR nucleic acid amplification test[Title/Abstract] OR (sensitivity and specificity[MeSH] AND drug resistance[MeSH])) AND Tuberculosis[Title/Abstract]. This was the search string used in the WoS database (advanced search, 30th April 2023): TS = (“resistance * detection *” OR “* microbial * susceptibility test *” OR “* microbial * sensitivity Test *” OR “point of care“ OR phenotypic drug resistance test * OR genotypic drug resistance test * OR “resistance prediction *” OR “rapid detection *” OR “rapid diagnosis” OR “molecular diagnosis” OR “nucleic* acid* amplification test*” OR (multidrug* resistant AND detection) OR (multidrug* resistant AND diagnosis) OR (extensively drug* resistant AND detection) OR (extensively drug* resistant AND diagnosis) OR (sensitivity specificity AND “drug * resistance *”)) AND TS = (“mycobacterium tuberculosis”).
The inclusion criteria were: 1) studies published in English; 2) studies published between 1st January 2020 and 30th April 2023; 3) all types of articles, including journal articles, reviews, book chapters, editorials, etc. In Figure 1, an overview of the search strategy and the study selection is shown. After applying the search string and the inclusion criteria, we imported 2342 studies into Zotero and we excluded 694 duplicates. This led to 1648 studies which were screened for relevance based on their titles and abstracts.
A total of 679 studies were excluded due to not focusing on drug resistance detection; for example, they focused on MTB identification only. Another 406 studies were excluded because, although drug resistance was detected in these studies, the main focus was not the performance or the feature of a diagnostic method but the molecular epidemiology or the distribution of drug resistance genes. A total of 86 studies were selected for this narrative and 32 further studies were included through a manual search among the references of the selected studies.
3. Results
The results of this review are divided by phenotypic, molecular and other methods. Standard methods will be only briefly covered, with a focus on the latest literature highlighting discrepancies, mistakes, or inaccuracies in these methods. In Table 1, we present a general overview of the major diagnostic methods covered in this review. In the text, we provide specific results of the studies.
3.1. Phenotypic drug susceptibility testing (pDST)
In pDSTs, bacteria are classified as resistant when they can grow in the presence of a drug, indicating that the drug is ineffective. Various types of pDST are available, some of which can determine the exact minimum inhibitory concentration (MIC) - the lowest drug concentration that inhibits 99% (90% in the case of Pyrazinamide, PZA) of visible bacterial growth - while others do not [63,64]. pDSTs require a positive MTB culture, which can take 2-3 weeks. Moreover, the tests need to be conducted in a complex and expensive infrastructure such as a biosafety level 3 laboratory. An additional 2-3 weeks are needed to obtain drug-susceptibility results. Thus, from sample collection to pDST results, a total of 4-6 weeks are needed [65,66]. The gold standards for pDST are the agar proportion method on solid medium (such as Löwenstein–Jensen (LJ) or 7H11 Middlebrook) or the Mycobacterium Growth Indicator Tube (MGIT) liquid medium, which is more common and faster.
3.1.1. Mycobacteria Growth Indicator Tube (MGIT) 960 system (Becton Dickinson)
With the MGIT, the MTB isolate grows on only one drug concentration, the critical concentration (CC) and the isolates are categorized as susceptible or resistant [67,68]. In Taiwan, Wu and co-authors analysed the BDQ resistance through the agar proportion method, MGIT and sequencing of the atpE, Rv0678, and pepQ genes in RR- or MDR-TB isolates. Isolates were divided into two groups: those with a MIC < 0.25 μg/ml (n=28) and those with a MIC ≥ 0.25 μg/ml (n=37). Using the agar proportion method, 18 isolates had a BDQ MIC = 0.25μg/ml; among those, 7/18 were resistant while 11/18 were susceptible according to the MGIT (breakpoint set as 1 μg/ml). Therefore, the authors recommend that a MIC = 0.25 μg/ml should be categorized as intermediate-susceptible, to resolve possible discordances by using different pDST methods. A total of 22 isolates were BDQ-resistant according to the MGIT and 17 of them harboured mutations in the Rv0678 gene [17]. A study by Rahman et al. in Bangladesh assessed resistance to FLDs in 825 sputum samples, revealing MGIT’s high sensitivity for detecting RIF and INH resistance (97.6% and 90.0%, respectively) but lower sensitivity for Streptomycin (SM) and Ethambutol (EMB) (61.3% and 44.9%) compared to the proportion method on LJ medium. The authors highlighted the high cross-country variability in the performance of MGIT regarding SM and EMB detection [18].
3.1.2. SensititreTM Mycobacterium tuberculosis MYCOTBI AST plate (ThermoFisher Scientific Inc).
With the Sensititre is possible to determine the MIC to 12 anti-TB drugs lyophilized on a 96-well plate, through the microdilutions method [69]. In Russia, Ushtanit and colleagues analysed the MICs to Ethionamide (ETH, a SLD) in 349 clinical isolates using the MGIT and the Sensititre MYCOTB with a CC of 5 mg/L. The authors observed a poor correlation between the results of the two pDST methods but did not provide any explanation. The authors proposed to lower the CC to 2.5 mg/L since the majority of ETH-susceptible isolates had a MIC < 2.5 mg/L [19].
3.1.3. Colorimetric assays
The Crystal Violet Decolorization Assay can detect RIF and INH resistance and was developed by Reghunath and co-authors in India. The assay is based on the principle that drug-resistant isolates can decolorize crystal violet dye, while drug-susceptible isolates cannot. Despite the limited number of analysed resistant isolates (14 MDR and 5 INH-monoresistant), the assay demonstrated 100% sensitivity and > 94.0% specificity for both RIF and INH resistance detection. The assay is easy to perform since it requires only antibiotics, dye and Middlebrook broth media. The TAT was nine days and the estimated cost was approximately six euro per sample [20].
Akbal and co-authors evaluated five colorimetric methods for PZA resistance detection in 15 susceptible and 15 resistance isolates and compared the results with the MGIT system. The authors found a good correlation (>90%) with all methods, and that the fastest TAT was eight days. Larger multicenter studies are needed to explore the feasibility of these colorimetric methods, especially in low-resource high-MDR-TB incidence settings [21].
3.1.4. Thin-layer agar (TLA)
Another cheap and rapid diagnostic test that could be useful in low-resource settings or field conditions is the direct thin-layer agar (TLA) DST. Ardizzoni et al. assessed its efficacy in Eswatini using both smear-positive and negative samples, benchmarking against a composite reference of Xpert MTB/RIF and pDST. In the TLA assay, clinical samples are decontaminated and then directly inoculated in 4-quadrant polystyrene agar plates with and without antibiotics. With a TAT of 18.4 days from sample collection to RR result, the TLA showcased superior performance for RR detection with a sensitivity of 93.0% and specificity of 99.4%, surpassing Xpert MTB/RIF’s 62.5% sensitivity and 99.3% specificity. TLA’s advantage was attributed to its detection of the I491F mutation in the rpoB gene (outside of the rifampicin resistance determining region, RRDR), which is common in southern Africa but not included in the Xpert MTB/RIF test [22].
In Ethiopia, Shibabaw and co-authors developed a colorimetric TLA-based assay, the MDR/XDR-TB Colour Test (TB-CX) for RIF-, INH- and ciprofloxacin (CIP)-resistance detection directly from sputum samples. Compared to pDST, the TB-CX method showed a sensitivity of 59.0%, 96.0%, and 95.0% for INH, RIF and MDR-TB detection and a specificity of 96.0%, 94.0%, and 98.0%, respectively. The low sensitivity observed for INH was explained by the suboptimal storage conditions of the TB-CX (four months versus the recommended 66 days) or by the different INH concentrations used between pDST and the TB-CX [23].
3.1.5. Other phenotypic methods
A rapid direct microscopy-based slide DST assay was evaluated in Uganda for the detection of RR on 122 smear-positive sputum samples from re-treatment TB patients. Compared with traditional pDST, the sensitivity and specificity of the assay were 96.0% and 97.8% in the 26 RR-detected isolates [24]. Lee and colleagues developed a rapid pDST method that detects viable MTB isolates by their capacity to hydrolyse fluorescein diacetate. This process releases free fluorescein, which can then be identified through flow cytometry. The authors tested the viability of 39 clinical isolates with anti-TB drugs such as RIF, INH and EMB. All resistant isolates according to traditional pDST (INH-resistant n=12, RIF-resistant n=4 and EMB-resistant n=5) were resistant also according to the flow cytometry. The test is promising since it can deliver susceptibility results in 24 hours after a positive MTB culture is incubated with the respective drug, but more resistant isolates need to be tested [25].
3.2. Molecular drug susceptibility tests
Molecular DSTs for detecting drug-resistance in MTB are mostly based on the detection of mutations in resistance-associated genes. Molecular DSTs are simpler and faster than pDST, with the added advantage of being applicable directly to clinical samples without the need for a prior culture. However, their scope is limited to detecting only known mutations, which means new, unknown, or rare mutations conferring drug resistance may go undetected. Also, molecular DST cannot determine the MICs [70]. The gold standards for the molecular detection of drug resistance in MTB are the commercial WHO-endorsed PCR-based Xpert MTB/RIF and Xpert MTB/RIF Ultra (for detection of TB and RIF resistance) [71], the line probe assays (LPA) based GenoType MTBDRplus (Hain LifeScience) and Nipro NTM + MDRTB detection kit (Nipro Corp.), (for testing RIF and INH resistance) and the GenoType MTBDRsl (Hain LifeScience) (for testing FQs and aminoglycosides) [72].
3.2.1. Xpert MTB/RIF, Xpert MTB/RIF Ultra and Xpert MTB/XDR
The Xpert MTB/RIF (Cepheid, Sunnyvale, CA, United States) allows identifying MTB and its resistance to RIF directly on clinical samples in ca. 90 minutes. This system is based on automated nested real-time PCR in a cartridge and it targets mutations in the rpoB gene [71]. The Xpert MTB/RIF Ultra has improved sensitivity for RIF resistance detection by incorporating additional targets and reducing the limit of detection compared to Xpert MTB/RIF [73,74]. The Xpert MTB/XDR system was approved for testing INH, FQ, AMK, KAN and ETH from sputum samples after a positive result from one of the two previous Xpert assays [75].
In their meta-analysis, Liu and co-authors found that Xpert MTB/RIF used on bronchoalveolar lavage (BAL) samples had a sensitivity of 87.0% and a specificity of 92.0%. Although more invasive, BAL samples are a valid alternative to sputum samples, especially in patients with sputum smear-negative samples or in patients who cannot produce enough quantity of sputum [26]. In their prospective observational study, Ngabonziza and colleagues analyzed the false positive RIF- resistant results when using Xpert MTB/RIF in Rwanda. Of the 154 patients initially diagnosed with RIF resistance using the Xpert MTB/RIF, only 35% had their RIF resistance confirmed upon repeat testing. Patients with a low bacterial load on sputum (94/154) had a higher probability of having a discordant result compared to patients with a high bacterial load. The Xpert MTB/RIF assay was found to have a low positive predictive value (53%) for RIF resistance in samples with a low bacterial load, implying that almost half of the RIF resistance results could be false positives. The authors gave two major explanations for that poor performance: 1) the known specificity limitations of the Xpert MTB/RIF in settings with a low RIF-resistance prevalence and 2) the high number of patients with paucibacillary disease due to the expanded testing indications encouraging early-stage disease testing. The authors recommended that when using the Xpert MTB/RIF, if initial testing indicates RIF resistance in a sample with a low bacterial load, additional sputum samples should be collected to repeat Xpert testing before starting MDR-TB treatment [36].
Xia et al. analysed 57 borderline RIF-resistance isolated cultures in China and found that Xpert MTB RIF showed a superior capacity to detect borderline RIF resistance (48/57, 84.2%) when compared to LJ-based DST (25/57, 43.9%) and microdilution plates (Thermo Fisher, Scientific Inc., USA) (33/57, 57.9%). The authors showed that borderline RIF-resistance detection with pDST can be achieved by reducing the MIC value to 0.5μg/mL or by extending the incubation time to six weeks in LJ-based DST [27]. In Uganda, Ssengooba and co-authors investigated the discordances between the initial and the repeated XpertMTB/RIF testing. The Global Laboratory Initiative recommends repeating the RIF resistance testing in patients with a low pretest probability, for example, new TB cases in a low RR/MDR-TB prevalence setting without previous contact with a resistant TB patient. To determine whether RR was truly detected, the authors used pDST, Genotype MTBDRplus and XpertMTB/RIF Ultra. The authors found that 15/96 (15.6%) isolates had a discordant RR result between the initial and repeated XpertMTB/RIF testing and that 10/96 (10.4%) isolates were false-positive RR isolates. A low bacillary load on the initial sputum was four times more likely to produce discordant RR results upon repeating the XpertMTB/RIF test [28].
In China, Wang and colleagues evaluated the accuracy of the Xpert MTB/RIF test in 251 TB patients who were re-tested due to a low initial bacterial load. The authors found that for samples initially identified by the Xpert MTB/RIF test as RIF-resistant (n=65), the results were not reliable, as only 25 remained RIF-resistant, 10 became RIF-susceptible, and 30 were negative for MTB. Culture and MGIT results further corroborated this, with 36 of the initially RIF-resistant isolates turning out to be culture-negative. The study emphasized that the Xpert MTB/RIF test may yield a significant number of false-resistant results when dealing with paucibacillary samples [29].
In China, Wu and colleagues showed that the implementation of Xpert increased of 9% the DST coverage and by 1% the RIF resistance detection. Also, the Xpert MTB/RIF reduced the median time from the first visit to a TB hospital to RR-TB detection from 62 to 9 days [30]. In Korea, Jeon and colleagues retrospectively analysed the diagnostics of 621 MDR-TB/RR-TB patients and found that the median time to start the treatment was 0 days using Xpert MTB/ RIF, in comparison with 22 days using MTBDRplus and 72 days using pDST. The median treatment delay was 2 days for Xpert, in comparison with 5 days using MTBDRplus and 13 days using pDST [31].
Georghiou and colleagues validated the Xpert MTB/XDR assay and highlighted three major findings. First, the limit of detection of the Xpert MTB/XDR was similar or better compared to the Xpert MTB/RIF (6323 vs. 15241 genomes/ml). Second, the Xpert MTB/XDR detected all mutations conferring resistance to INH, ETH, FQ and the injectable SLD (AMK, KAN and Capreomycin, CAP) in 29 MTB isolates. Third, the Xpert MTB/XDR assay was able to detect heteroresistance (HR, see section 3.2.7) when the populations contained at least 10% INH resistance, 25% FQ resistance, 50% ETH, AMK and KAN resistance and 60% CAP resistance isolates [32]. Cao and co-authors developed a 10-color reflex Xpert MTB/XDR assay (CE-IVD only) to detect resistance to INH, FQ, ETH and SLIDs directly from MTB-positive sputum samples. To detect resistance-associated mutations, the assay analyses mutation-specific melting temperatures using sloppy molecular beacon probes. The assay correctly detected all mutations (except one gyrB mutation) in a sample of 16 resistant isolates. In 214 clinical and 100 sputum isolates, the assay had a sensitivity ranging from 94.1% to 100% in all drugs (except for ETH, where the sensitivity was 88.5%) when compared to sequencing. When compared to pDST, the assay reported slightly less sensitivity, ranging from 70.0% (CAP) to 98.3% (INH). The modified Xpert MTB/XDR assay can be useful as a follow-up test for MTB-positive samples and to assist in diagnosing the primary types of resistance in MDR-TB isolates [33]. Truden and colleagues analyzed 80 MTB isolates in the Balkan area with Xpert MTB/XDR and compared the results with pDST and sequencing. The results showed high specificity for all drugs (100%) except INH (66,7%), due to a mutation in the promoter region of the oxyR-ahpC –57c.t gene, which is of uncertain significance according to the WHO mutation catalog [76]. The sensitivity was 91,9% for INH, 100% for SLID and FQ and 51.9% for ETH resistance, due to widespread mutations across the ethA gene. Therefore, the authors concluded that the Xpert MTB/XDR, while it can confirm the presence of ETH resistance, is not reliable for excluding it [34].
The GeneXpert Omni system is a portable point of care (POC) molecular diagnostic system. The Omni system can be used in field settings or remote areas because it is portable, battery-powered and has cloud-based connectivity which allows for data transfer. Georghiou and colleagues evaluated the performance of the Xpert MTB/RIF Ultra cartridges when run on the Omni device compared to the traditional Xpert. The authors also evaluated the Omni system under field stress conditions such as high temperature and humidity. Already characterized clinical MTB-positive and negative samples were analyzed. In 145/156 (92.9%) cases, the RIF resistance was correctly detected by both assays. The presence of HR isolates might be responsible for the few discrepant cases. The diagnostic performance of Omni system was not affected by stressful field conditions [35].
3.2.2. GenoType MTBDRplus and GenoType MTBDRsl
The GenoType MTBDRplus (Bruker, Germany) allows the identification of MTB complex and its resistance to RIF and INH directly from both pulmonary clinical samples or isolated cultures. The system is based on LPA, PCR amplification and reverse hybridisation of amplified genes with a TAT of ca. five hours [77].
The GenoType MTBDRsl (Hain Lifescience, Germany) can detect resistance to SLDs as FQ (e.g., ofloxacin, OFL and moxifloxacin, MOX) and SLIDs (KAN, AMK and CAP). Van Rie and co-authors used the Genotype MTBDRplus (on smear-positive sputum samples or smear-negative isolated MTB culture) and Xpert MTB/RIF (on sputum samples) and analysed the discrepant results in South Africa. They identified 43 discordant results among the 297 (14.5%) paired samples. In 42/43 of these discordant results, the MTBDRplus identified RIF susceptibility while the Xpert identified RIF resistance. To explain those discordances, the authors suggested the following: the detection of a resistance mutation by the Xpert MTB/RIF which was not included in the MTBDRplus assay; HR, which was possible to detect by Xpert in sputum samples but not possible to detect in cultured samples by MTBDRplus due to the loss of minor resistant population; false positive molecular assay detecting RIF resistance but the MIC was <1 µg/ml; human/administrative errors [38].
Shi and co-authors compared the treatment management and outcome in MDR-TB patients in two groups, before (n=114) and after (n=128) the implementation of molecular resistance detection with Genotype MTBDRplus/MTBDRsl in two Chinese hospitals. The time to diagnose an MDR-TB was significantly more rapid using the Genotype assays compared to the traditional pDST (16 vs. 62 days), as well as a more rapid median culture conversion time (12 vs. 24 months) and a higher rate of treatment success (68% vs. 47%). Lastly, the Genotype assays allowed for a reduction in the duration of ineffective treatment (59 vs. 11 days) [37].
In a study conducted in South-Africa, Mahomed and co-authors compared the RIF- and INH-resistance results of the Genotype MTBDRplus with the MGIT in 8273 isolates. The Genotype MTBDRplus reported a sensitivity and specificity of 95% and 75% for RIF and 93% and 95% for INH. In 14.6% and 7.2% of the cases, a discordant result for RIF and INH resistance was detected. The authors highlighted that if clinicians had started treatment based solely on the MTBDRplus results, 25% of TB-patients would have erroneously received treatment for MDR-TB, while 5% of the TB-patients, who had MDR-TB infection, would have erroneously treated with drugs ineffective against MDR-TB isolates [39].
In Bangladesh, Rahman and colleagues evaluated the performance of GenoType MTBDRsl directly on 218 smear-positive sputum samples (from MDR-TB patients) in detecting OFL, KAN and EMB resistance. Compared with pDST, the Genotype MTBDRsl reported a sensitivity and specificity of 81.8% and 98.8% for OFL, 65.1% and 86.7% for EMB and 100% for KAN. The study was conducted using the older definition of XDR and before the introduction of the pre-XDR definition. If the new pre-XDR definition had been applied, the relatively low reported sensitivity for OFL could have overlooked numerous clinically relevant pre-XDR isolates, which would have been inaccurately identified as MDR. The low sensitivity observed for EMB resistance was attributed to the limited knowledge about EMB resistance mutations and the absence of relevant targets in the MTBDRsl assay. Furthermore, the MTBDRsl assay was evaluated solely on smear-positive sputum samples, suggesting that performance might deteriorate further when applied to smear-negative (paucibacillary) samples [40].
In India, Rufai and colleagues tested the MTBDRsl on 113 MDR-TB isolates and found that the accuracy of the assay in detecting FQ resistance was 100%, compared to the MGIT. The sensitivity for the XDR detection was 85.7% (6/7). In considering a national implementation of this assay, the authors discussed the need to reduce the costs, which were estimated to range from 17.3 to 20.2 USD per test [41]. In another study in India, Jain and co-authors applied the Genotype MTBDRplus and MTBDRsl on extrapulmonary samples and compared the results with Xpert MTB/RIF. Although the authors did not perform any pDST, the two methods reached a good agreement (98.2%) in 94 RIF-susceptible and 15 RIF-resistance isolates [42]. Pinhata and colleagues analysed 385 MDR-TB (according to the MGIT results) isolates in Brazil and found that the MTBDRsl could detect 99.7% of MDR, 87.8% of the pre-XDR and 73.9% of the XDR-TB isolates. The found a sensitivity of 86.4%, 100%, 85.2% and 76.4% for FQ, AMK/KAN, CAP and EMB [43].
In another study conducted in India, the GenoType MTBDRsl assay revealed good performance in detecting resistance to FQ and SLIDs directly from smear-positive sputum samples after confirmation of RR status by Xpert MTB/RIF. Compared with pDST in 225 RR isolates, the sensitivity and specificity of the GenoType MTBDRsl for FQ resistance detection were 100% and 92.3%, whereas for the SLIDs sensitivity and specificity were both 100% [46].
In South Africa, Pillay and co-authors highlighted the high amount of non-actionable results (i.e., indeterminate or invalid results) of the Genotype MTBDRplus and MTBDRsl in smear-negative samples. They found non-actionable results in 92 out of 476 isolates (19.3%) when using MTBDRsl and in 171 out of 427 isolates (40.0%) when using MTBDRsl. Non-actionable results might cause diagnostic and treatment delays and missed resistance [44]. For a systematic review and meta-analysis on the performance of several types of LPAs, we recommend the work of Lin and co-authors [45].
3.2.3. BD MAX MDR-TB from Becton Dickinson
The BD MAX™ MDR-TB test is an automated system that extracts DNA and performs real-time PCR and can detect MTB and its resistance to RIF and INH from respiratory samples. In a prospective multicentre (South Africa, Uganda, India, and Peru) study, Shah and co-authors found that the BD MAX showed a sensitivity for RIF resistance detection of 90.0% and a specificity of 95.0% when compared to pDST. For INH, the sensitivity was 81.5% and the specificity was 100%. Although the authors found only a small sample of resistance isolates, the BD MAX seems promising since it is automated and can process 24 specimens in one round with a TAT of four hours from testing start to results [47].
3.2.4. Sequencing
While other drug-resistance diagnostic tests identify mutations in a few resistance-associated genes, whole-genome sequencing (WGS) analyse all genes and compensatory mutations. Another advantage is that sequencing data could be analysed retrospectively once newly identified resistance genes or mutations are discovered [78,79]. However, there are also disadvantages of using WGS: the need for a positive MTB culture (usually a flagged positive MGIT culture), complex bioinformatic expertise to interpret the results, high costs (approximately 100 Eur per sample [80]) and complex laboratory manual work [78,79]. To shorten the TAT, sequencing can be performed directly on sputum samples. However, this approach may yield lower sensitivity compared to sequencing from positive cultures, due to the presence of other microorganisms or contaminants in the sputum and/or due to low bacterial load [70].
Several platforms exist to perform WGS, such as Illumina, Ion Torrent, PacBio SMRT RSII or Oxford Nanopore MinION [81]. And several tools exist to predict drug resistance profiles from raw WGS data (e.g., fastq files), simplifying the bioinformatic workflow, such as KvarQ [82], TBProfiler [83], CASTB [84], Mykrobe Predictor [85], PhyResSE [86], Resistance Sniffer [63] or Treesist-TB [87]. Lists of resistance-associated mutations are developed and serve as a global standard for interpreting molecular information for drug resistance prediction [88]. In Table 2, we summarise the studies where sequencing methods have been compared with pDST to predict drug resistance.
At the Belgian National Reference Centre for Mycobacteria, WGS is prospectively applied to all MTB complex isolates. Genomic DNA is extracted and purified from the MGIT tubes, without the need for a sub-culture. Soetaert and colleagues found that the TAT for the WGS ranged between eight and 15 days (from the time of culture arrival to the complete reporting of the resistance results). In contrast, pDST required a TAT of eight weeks. The authors observed two major impediments to the routine implementation of WGS: first, insurance systems do not reimburse for the use of WGS and second, the physicians lack confidence or experience in the WGS results [95].
Solari used WGS to analyse discrepant results between pDST and the GenoType MTBDRplus for RIF resistance (n=16) and INH resistance (n=21). Thanks to the WGS, the authors identified missense mutations (missed from the GenoType MTBDRplus) that could justify the resistance to RIF and INH [101].
In England and Wales, Mugwagwa and colleagues found several benefits of replacing routine pDST with WGS: reduced TAT for obtaining drug-resistance results, reduced time that patients spend on inappropriate treatment, reduced treatment duration, reduced number of patients in treatment and reduced diagnostics costs of £780,089 in year 1. Their model predicted that in 10 years, the WGS can have a net cost saving of £7.2M (£3.3M–£11.1M). The authors also showed that the Xpert MTB/RIF or the Xpert MTB/RIF Ultra showed several benefits such as earlier initiation of appropriate treatment (which reduces transmission and number of new infections), reduced unnecessary treatment and hospitalization for TB-negative patients, reduced time to treatment (13 days less for smear-negative TB and 27 days less for MDR-TB) and reduced unnecessary patient isolation. The author concluded that WGS is cheaper than pDST and that greater health advantages could be achieved by combining the major advantages of the WGS (high-throughput) and the Xpert technology (rapidity) [14].
In another study in England, Park and co-authors found that in 12 TB cases, the median TAT from sample collection to WGS results was 35 days (including 16 days to obtain a culture) which was 53.5 days earlier compared to the pDST. WGS also allowed for a more rapid de-escalation of therapy. By using Xpert, in 9/12 TB cases the results were available within 24 hours from the time of sample collection. Treatment for those patients was adjusted based on the subsequent WGS results; for example, INH was stopped in six cases. The authors conclude that although more rapid than DST, WGS still required more than a month to provide results, highlighting logistics problems in sample transportation or slow communication of the results to clinicians [102].
In seven high TB-burden countries, Zurcher and co-authors analysed the mortality in TB patients depending on the concordance or discordance between drug-resistance results predicted by WGS or drug resistance results determined locally (through Xpert MTB/RIF, LPA or pDST). A total of 130 of the 582 analysed isolates (22%) had discordant drug-resistant results. Drug-resistance result agreement between WGS and locally-done DST was 80% for pan-susceptible, 66% for MDR and 33% for pre-XDR and XDR. Local laboratories accurately detected resistance to RIF and INH, but rarely tested for resistance to other drugs. The mortality varied from 6% in correctly treated pan-susceptible patients to 32% in resistant TB patients receiving inadequate treatment due to discordant results. The authors highlighted that routine WGS could enhance TB treatment and decrease mortality [13].
Vogel et al. conducted a proof-of-concept project over 93 weeks to explore the feasibility of routine WGS implementation in the Kyrgyz Republic. They estimated a weekly workload of 55 TB-WGS. Initial implementation costs amounted to just over 230,000 USD. The first WGS sequence cost was 277 USD, projected to decrease to approximately 150 USD with improved training. Five trainings for the staff have cost approximately 48,250 USD. The authors highlighted the following challenges during the implementation: higher-than-expected sequencing costs, capacity building requiring more time than anticipated, infrastructure requirements and the need for careful planning and ongoing expert support [103].
Smith and colleagues compared in real-time the drug-resistance results of the Oxford Nanopore MinION sequencing with those from the Illumina MiSeq sequencing and pDST. MiSeq and MinIon had similar TAT (approximately three days), however, the MinION is more flexible because it might be terminated at any moment when a sufficient throughput for analysis has been reached. The Minion had a lower cost, 57 USD per sample compared to 130 USD with the MiSeq. Features that make the MinION a valuable tool in clinical settings are improved logistics, economic advantages, portability and flexibility [98]. In Australia, Lam and colleagues prospectively analysed the benefits of the routine implementation of WGS compared to pDST and GeneXpert MTB/RIF. Over 3 years, they found 29 MDR-TB from 1107 MTB isolates. By detecting mutations outside of the traditional resistance-determining areas, routine WGS increased drug resistance detection by 20% in contrast to the Xpert MTB/RIF [104].
Green and co-authors used WGS coupled with machine learning (ML) models to predict antibiotic resistance. They developed two deep convolutional neural networks to predict resistance to 13 antibiotics. By comparing the genetic resistance prediction with pDST results publicly available for 23,049 MTB isolates, they found that the ML reached >90% sensitivity and specificity for FLD and SLDs. In addition, the models also identified 18 genomic sites not previously associated with resistance. The use of ML in WGS analysis holds promise in identifying novel loci, genes, and mutations associated with drug resistance [105].
We advise the readers to go to the respective reference for: a review highlighting recent research on the potential of WGS to expedite personalized care, the latest advancements in direct WGS on sputum samples and targeted sequencing [106]; a review analysing ML approaches in predicting resistance [107]; an overview of the WGS workflow on MTB isolates [108].
3.2.5. In-house developed molecular methods
Zhou and colleagues developed a rapid method based on PCR and hybridization assay on a 96-well ELISA microplate to detect RIF (rpoB gene) and INH (katG, and inhA genes) resistance mutations. They tested this PCR-ELISA method in 32 MDR- and 22 pan-susceptible TB isolates and compared the results with pDST and sequencing. The sensitivity of the PCR-ELISA for detecting RIF and INH resistance was 93.7% and 87.5%, while the specificity was 100% for both drugs [48].
In Myanmar, Chang and co-authors developed the QuantaMatrix Multiplexed Assay Platform (QMAP), an assay based on reverse hybridization. In the assay, a gene probe is attached to magnetic micro-particles. Each probe can hybridise with a PCR product present in a sample, which then emits fluorescence. The QMAP assay permitted to identify resistances to RIF, INH, EMB, FQ and SLIDs in six hours from a positive MTB culture. In 190 MTB isolates the QMAP results were 87.9% concordant with pDST. The lowest concordance rate was observed for EMB, where pDST identified 108 resistant isolates while the QMAP only 67. The authors explain this low concordance with the lack of appropriate probes for EMB-resistance-associated genes, unknown mutations responsible for drug resistance, HR or low-level resistance. A total of 23 isolates had a discordant result between QMAP and pDST. The sequencing of the resistance genes in these 23 isolates showed full concordance with QMAP results, demonstrating that the QMAP represents a faster and easier alternative to WGS in the identification of MDR- and XDR-TB [49].
In China, Leung and colleagues developed an in-house target amplicon sequencing assay (TB-NGS) for direct use on respiratory samples, with a TAT of six hours. The system detects 17 mutations conferring resistance to eight anti-TB drugs. The TB-NGS was performed on all the resistant isolates identified through LPAs – 12 resistant to at least one drug, four MDR-TB and six pre-XDR-TB. In 59/62 isolates, the TB-NGS showed a concordant result with pDST. The three cases that showed discordance were identified as pan-susceptible by pDST but were recognized by TB-NGS as minor variant cases with a mutation frequency below 35%. These minor variants, with a frequency < 35%, were differentiated from dominant resistance mutations typically seen at frequencies > 60%. While minor variants do not pose challenges to initial resistance determination, it would be important to further study them for potential progression to full resistance [50].
3.2.6. Other molecular methods
Cho and colleagues evaluated the performance of TBMDR® and XDRA®, assays based on Real-Time PCR for the detection of RIF/INH and FQ/SLID resistance from isolated cultures with a TAT of three hours. The authors analysed 234 clinical samples and compared the results with MGIT and sequencing. The TBMDR reported a sensitivity and a specificity of 95.7% for RIF resistance and a sensitivity of 81.2% and a specificity of 95.8% for INH resistance detection. The XDRA reported a sensitivity of 84.1% and a specificity of 99.1% for FQ resistance and a sensitivity of 67.4% and a specificity of 100% for SLID resistance detection. A concordance rate >95% was observed when comparing the two assays with direct gene sequencing. Although the authors tested these two assays on isolated cultures, both assays can be performed also on sputum samples [51].
In China, Sun and colleagues evaluated the performance of the CapitalBio DNA microarray in detecting RIF and INH resistance in 825 TB patients. Compared to the MGIT, the assay reported a sensitivity and a specificity of 84.0% and 94.0% for RIF-resistance detection and 73.0% and 97.0% for INH-resistance detection. However, it was not possible to determine which mutations in the rpoB, inhA and katG genes were targeted by the microarray system, making it difficult to compare it with other DST methods [52].
In a study, four methods – Abbott RealTime MTB and MTB RIF/INH (Abbott), Hain Lifescience FluoroType MTBDR (Hain), BD Max MDRTB (BD) and Roche cobas MTB and MTB-RIF/INH (Roche) – were compared with Xpert MTB/RIF and GenoType MTBDRplus for RIF and INH resistance detection. Although the authors did not use real-life clinical samples (but a collection of well-characterized resistant isolates), and although they used a score rather than the classical comparison with pDST, all four methods reported performance similar to Xpert and GenoType MTBDRplus with a TAT ranging from three to seven hours from an isolated culture. A particular advantage of these essays is that, apart from the BD Max MDRTB, they can process a large number of samples (n=94) in a single run [109]. For a systematic review and meta-analysis of the performance of the Abbott RIF/INH, the FluoroType MTBDR and the BD Max MDR-TB please refer to Kohli and colleagues [110].
In Thailand, Thant and colleagues evaluated the RIF-RDp assay for RIF-resistance detection. The assay combined the locked nucleic acid (LNA) probes with high-resolution melting (HRM) curve analysis. Briefly, in HRM analysis, the differences in real-time PCR melting curves are analysed to detect resistance-associated mutations. Since the HRM analysis cannot detect all SNPs, LNA probes were used; LNA probes are modified nucleic acids with higher thermal stability and specificity which improve the SNPs detection. Compared to pDST, the assay showed a sensitivity and specificity of 94.6% (52/55) and 98.2% (54/55) for rpoB-based RIF-resistance detection in isolated MTB culture. The TAT was 2.5 h and with an estimated cost per test of 7.18 USD, compared for example to 13.54 USD for Gene Xpert in Thailand. The authors tested the assay in isolated cultures, but validations in clinical samples are needed [53].
Ou and colleagues evaluated the Luminex MagPlex microsphere-based multi-analyte profiling platform (Luminex Corp. Austin, TX, USA) to detect resistance to RIF, INH and EMB. The platform is based on a multiplex PCR amplification of ten resistance-associated mutations. Then, labeled microspheres hybridise with the amplicons and are detected through streptavidin reaction. They analysed 353 MTB isolates from China. Compared to pDST, sensitivity and specificity for RIF-resistance detection were 94.9% and 98.9%, for INH 89.1% and 100%, for EMB 82.1% and 99.7% [54].
The Truenat MTB-RIF Dx is a diagnostic test for the rapid detection of MTB and RIF-resistance directly in sputum samples in approximately 90 min. The system is based on a microchip-based real-time PCR technology. Penn-Nicholson and colleagues evaluated the performance of the Truenat MTB-RIF Dx against the Xpert MTB/RIF, Xpert MTB/RIF Ultra and pDST. In 552 samples with pDST results, the Truenat MTB-RIF Dx assay reported a sensitivity of 84% and a specificity of 95% for RIF-resistance detection. In 252 samples with valid Truenat MTB-RIF Dx and Xpert MTB/RIF results, the sensitivity of Truenat MTB-RIF Dx and Xpert MTB/RIF tests were 83% and 88% while the specificity was 97% for both assays [55].
Liu and colleagues used the CRISPR/Cas technology and developed a Cas12a RR detection system combined with recombinase polymerase amplification, to detect SM resistance in 49 MTB isolated cultures. Compared to sequencing, the assay reached 100% sensitivity and specificity with a TAT of 60 min [111].
3.2.7. Mixed infections, heteroresistance (HR) and low-level drug resistance mutations
Three additional factors complicate the interpretation of phenotypic and molecular DST results: 1) the polyclonal (or mixed) TB infections, when the patient harbours at least two different MTB strains with different drug-resistance patterns [112]; 2) the HR, where drug-susceptible and drug-resistant isolates co-exist in the same host [113]. The HR might originate from a polyclonal infection or when a bacterial subpopulation (or single clone) develops resistance under antibiotic treatment, particularly with subtherapeutic drug levels. HR can be an intermediate step towards full resistance development [114]. For a systematic review of HR in MTB isolates we advise consulting [115]; 3) low-level drug-resistant mutations, when mutations cause a MIC that is below the breakpoint and therefore the isolate is classified as susceptible. But, low-level drug-resistance mutations might be responsible for poor clinical outcomes or can be an intermediate step towards full resistance development [116,117].
Shea and co-authors prospectively tested 1779 MTB isolates for RIF resistance in the US. The authors identified 53 isolates with mutations associated with RIF resistance; in 49/53 isolates the RIF mutation was within the RRDR (a highly conserved region of 81 bp of the rpoB gene, encoding for the RNA polymerase β-subunit [118]), while 4/53 harboured mutations outside the RRDR. Of note, mutations outside of the RRDR are missed by goldstandard molecular DST tests [119]. Of those 53 mutations, 43 had a MIC > 1 µg/ml, while the other ten (seven within RRDR and three outside of the RRDR) had a MIC between 0.25 and 1 µg/ml and were categorized as low-level RIF resistance (while the MIC for the RIF susceptible isolates was lower, between 0.12 and 0.5 µg/ml). The authors suggested that diagnostics algorithms should be developed to detect those low-level RIF-resistance mutations, possible for both pDST (e.g., measuring the MICs below the breakpoint of 1 µg/ml) and molecular DST (e.g., extending the range of detected rpoB mutations) [120].
In a study in Thailand, the authors investigated HR in nine drugs by calculating the frequencies of the variants occurring in less than 100% of reads through WGS and comparing those results with pDST. They found a direct relationship between the frequency of resistance-conferring alleles and MIC values especially for RIF, KAN and AMK. For example, an isolate with 64% reads indicating the mutation Ser441Leu was susceptible to RIF (lower MIC), whereas another isolate with 96% reads indicating the same mutation was resistant to RIF (higher MIC). Although few resistant isolates were analysed, the study highlighted the potential use of WGS to detect HR [121].
In another study, Narang and co-authors developed a SuperSelective Primer-Based Real-Time PCR Assay, to detect rare resistance-associated mutations within a wild-type population. SuperSelective primers are designed with a non-specific 5′ anchor sequence and a short 3′ foot sequence, specific for the target mutations. The assay allows for selective and exponential amplification of resistance mutations. In 23 clinical MTB isolates (including 11 MDR and 6 INH-monoresistant isolates) the assay detected HR populations with a detection limit of 0.01%. The assay is ultrasensitive, but not all isolates were compared with WGS and or with pDST [122]. Tamilzhalagan and co-authors retrospectively performed WGS on MTB isolates from India to detect mutations that might have been undetected by the MGIT. The MGIT classified 131 isolates as RIF-resistant while WGS detected RIF-resistance mutations in 146 isolates. Therefore, the WGS helped identify 15 further isolates with a low-level RIF resistance compared to the MGIT DST [123].
Werngren and co-authors studied the HR in PZA using the MGIT 10% proportion method [124], the Wayne’s test (an enzymatic test detecting a functioning Pyrazinamidase – an enzyme, encoded by the pncA gene, that converts the prodrug PZA into Pyrazinoic acid, which is bactericidal for MTB isolates) and WGS. They experimentally mixed susceptible and resistant bacterial populations. The MGIT detected HR in 13/15 mixed populations and the WGS was able to identify all HR populations except in one case (containing 5% resistance and 95% susceptible population). But, when the authors used less strict filters, e.g., a variant detected in only one read, HR was detected. However, applying less strict filters in WGS might cause more background noise and less specificity because sequencing artifacts or other contaminant bacteria could be reported as “true variants”. The Wayne’s test did not detect any HR [125]; these poor results are in contrast with a systematic review and meta-analysis, where Nasiri found that the sensitivity and specificity of the Wayne test were 86.6% and 96.0% [126].
Whitfield and colleagues also investigated HR to PZA in RR-TB patients in South Africa by comparing the MGIT with several molecular DST methods. The authors reported a discordant phenotype/genotype result in 14/358 isolates (3.9%). Of those 14, HR isolates were detected in three isolates. Those isolates were phenotypically susceptible but contained a resistance mutation at low frequency (2.0%, 6.7% and 3.0%). To identify as much HR as possible, the authors set a very low threshold (1%) of minor variant calling; this limit might be appropriate for deep targeted sequencing (i.e., sequencing specific DNA regions at a higher depth), but not for WGS, where such a low threshold can produce false positives [127]. Wang and co-authors investigated the MICs of isolates with low-level RIF-resistance mutations with the MGIT and microplate alamarBlue assay. They found that a high proportion of isolates with low-level RIF resistance mutations could be missed by using the WHO-recommended CC of 0.5 µg/ml. All but one RIF-resistance isolates were detected by reducing the CC breakpoints to 0.125 µg/ml, and therefore the authors suggest lowering the RIF CC breakpoint to 0.125 µg/ml [128].
3.3. Other diagnostics methods
3.3.1. Biosensor
Hu and colleagues developed a fluorescence nanomaterial-based biosensor to detect RIF and INH (rpoB and katG genes) resistance. When the target genes hybridise with the probes, fluorescence is emitted and the two resistance genes can be detected. The fluorescence biosensor correctly detected five MDR, three RIF-resistance, five INH-resistance and seven pan-susceptible clinical isolates in approximately 95 min [56].
3.3.2. Lab-on-chip
Colman and co-authors evaluated the performance of the Integrated System (Akonni Biosystems, MD) in detecting resistance to RIF and INH from sputum samples. This automated assay is based on DNA extraction and a Lab-on-a-Film disposable to perform the PCR. In 25 sputum samples collected from patients at risk of MDR-TB, the assays revealed a sensitivity and a specificity of 100% and 66.7% for RIF resistance detection and 100% agreement for INH resistance detection compared to pDST. The low specificity to RIF was due to two samples with low-level resistance mutations [58]. Ou and colleagues evaluated the VereMTBTM Detection Kit, a Lab-on-Chip assay based on PCR and microarray. Compared with the MGIT, the assay reported sensitivity and a specificity of 85.7% and 93.9% for RIF and 75.0% and 95.7% for INH-resistance detection in 124 sputum samples. The TAT was three hours. The system can detect in one-step MTB, MDR-TB and also non-tuberculous mycobacteria [57].
3.3.3. Matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS)
The MassARRAY is a MALDI-TOF MS system that detects resistance-mutations for SM, RIF, INH, EMB and FQ. In China, Yang and colleagues evaluated the performance of the MassARRAY in 94 respiratory samples as well as in 128 MTB isolated cultures. Compared to Sanger sequencing, the assay reached 100% accuracy. Compared with the MGIT, the assay’s accuracy ranged from 90.6% for EMB to 98.4% for SM. The assay was also able to detect HR if the resistant sub-population ranged from 5–25%. The assay can process 384 samples in a single run with a TAT of 24 hours [59].
In another study in China the MassARRAY was evaluated for the detection of resistance to RIF, INH, EMB, SM, FQ and SLID in respiratory samples from patients with relapsed TB. Compared to the MGIT, the MassARRAY had a sensitivity of 96.4% and a specificity of 100% for INH, a sensitivity of 93.9% and a specificity of 93.7% for RIF and a sensitivity of 88.9% and a specificity of 100% for EMB. Worst performances were obtained in the sensitivity to other drugs, while the specificity was good (>94.4%). The lower sensitivity was attributed to the incomplete list of resistance genes and the direct application of the assay on clinical samples, rather than on isolated cultures [60]. Wu and colleagues used a nucleotide MALDI-TOF-MS assay, Conlight TB&DR® Detection (Shanghai Conlight Medical Laboratory Co., Ltd.), to detect resistance to eight anti-TB drugs. The method consists of a PCR in the region of gene mutation, a primer extension step using a terminator nucleotides and analysis of the products on MALDI-TOF-MS assay. For the 168 isolates analysed, the average agreement with pDST across all eight drugs was 91.3% [61].
3.3.4. Surface-enhanced Raman spectroscopy (SERS)
SERS is a technique that amplifies the Raman scattering signals of molecules/target genes which are immobilized on nanostructured metallic surfaces, such as silver. This allows for the detection of very low concentrations of molecules. The target genes can be differentiated based on their unique vibrational spectra produced in the SERS process. In a study in China, Wang and co-authors used the SERS to differentiate between pan-susceptible (n=47) and resistant MTB isolates (n=76). ML algorithms permitted the analysis of different spectra and determined the drug resistance status with 99.59% accuracy when compared to pDST [62].
4. Discussion
In this study, we provided an overview of the laboratory methods used to detect drug resistance in MTB. Key parameters for choosing a drug-resistance test for MTB include rapid result turnaround, simplicity of the procedure, cost per test, eventual equipment costs and the sensitivity and specificity of the method. As we expected, the most widely used pDST method was the BACTEC MGIT 960. Although not the most economical or fastest, it has some advantages, for example it can provide the drug susceptibility for a full panel of drugs. Moreover, it complements WGS by supporting the interpretation of results and identification of new mutations associated with drug resistance. A major disadvantage of the MIGT, especially in low-resource settings, is the initial and ongoing costs associated with the installation, maintenance, and upgrade of this automated system. Lastly, as with all culture-based methods, there is a contamination risk during sample handling, potentially leading to inaccurate results [67,68].
The most commonly used molecular tests were Hain MTBDRplus, MTBDRsl and the GenXpert systems. Regarding the GenXpert, its performance is less optimal when the assay is performed in paucibacillary samples and low RIF-resistance settings, see for example [28,29,36], where the authors reported false-positive results. In those conditions, it is recommended to repeat the Xpert testing in case of a first positive result. Other in-house molecular methods are also available, and they might be useful especially at the local level or in low-resource settings since they are relatively inexpensive, see for example [52,53]. However, standardization and cross-laboratory reproducibility are difficult to obtain with these methods. Among the molecular tests, WGS should be by far the best choice, since it provides a fast, reliable and complete antibiogram, giving also additional information, such as molecular typing to identify circulating clones and potential clusters. From a practical standpoint, regional centers for WGS would enable peripheral hospitals or laboratories to send strains or extracted DNA for analysis. Moreover, we found relatively few studies, see for example [80,86,99], where the authors applied sequencing technologies directly to clinical samples. Although this approach is promising, challenges remain for its routine implementation. A valid competitor of WGS is MALDI-TOF, as seen in [59,60,61], which can provide the same information with similar limitations concerning instrument costs and the need for skilled personnel to interpret the results. While numerous molecular DST methods have been developed, an integrated approach that combines phenotypic and molecular DST is still necessary. This approach is particularly crucial for managing mixed infections, HR isolates and isolates with low-level drug resistance mutations, for example [121,127].
Here are the four most common challenges/limitations that we found by reviewing the literature. First, the large majority of the analyzed studies considered the old definition of XDR and did not consider the pre-XDR definition, with few exceptions [13,43,50]; thus, it is impossible to translate the findings in the context of the new pre- and XDR definitions. Also, we found few studies that also analysed isolates resistant to LZD or BDQ, for example [17,97], both in terms of resistance mutations (via WGS) or pDST. Maybe retroactively it should be possible to re-analyse the studies in light of the new pre- and XDR definitions, since for example FQs were often tested. However, the feasibility of this re-analysis remains to be seen. There is a need to implement and standardize the DST on LZD and BDQ, possibly by improving both the phenotypic DST (for example via the MGIT) and the resistance-mutations detection at the molecular level [6,129]. Not surprisingly, BDQ resistance is emerging in several countries, raising concerns that DST and/or regimens are not sufficiently robust to avoid accrual of resistance [130].
Second, the majority of studies we analysed focused on the classical diagnostic performance, such as sensitivity and specificity, of a particular method. But, few studies, for example [30,31,37], also evaluated the clinical utility, such as reduced TAT or treatment duration, mortality reduction, improved treatment or cost-effectiveness of implementing a certain method. Those parameters are crucial to implement and evaluate a diagnostic test. Third, most of the analysed studies were retrospective; very few studies (e.g., [47,95]) conducted a real-time prospective analysis to observe how a certain diagnostic test influences clinical decisions. We found rarely (an exception is [37]) a comparison between patients receiving treatment based on standard pDST versus patients receiving treatment based on the results of a specific molecular DST method. Fourth, as we expected, many emerging POC-based methods are still at the proof of concepts stage (e.g., [53,58]) and were tested on a few clinical isolates. Although rapid and easy to use, their applicability at a scale for routine diagnostics is uncertain. Among those, portable POC tests directly on sputum are particularly promising, for example the automated Truenat MTB-RIF Dx assay [55].
Two further considerations regarding our review: 1) we were very inclusive with the search strategy and we employed broad terms, so we screened a large volume of studies and our literature review was both broad and deep. We could advise authors who want to do similar reviews to carefully consider a balance between breadth and specificity in search terms; 2) although narrative reviews are inherently more subjective than systematic reviews – for example in the study selection and in the extent to which we reported and discussed every study – in our review we offered a more general and context-rich analysis, we wanted to stimulate discussion and to offer a broader rather than a narrow overview of the current literature, its limitations and open challenges.
Microbial drug resistance threatens to be the pandemic of the century, with TB being not immune to this emergence. Among the tools we have to fight drug-resistant TB, the progress of diagnostic methods certainly plays a central role. The choice of the laboratory method to investigate TB-related resistance is a major concern, especially in low-resource settings where TB is most often present. In these contexts, it is not so much the difference between phenotypic or molecular methods that drives the choice, but other criteria such as expertise, facilities, laboratory safety, financial commitment and speed of diagnosis. All these characteristics should be considered when analyzing the various methods in making the most appropriate choice.
Author Contributions
Conceptualization, A.S., and A.M.; methodology, A.S., A.L., F.G. and A.M.; validation, A.S., and A.M.; formal analysis, A.S., A.L., F.G. and A.M; investigation, A.S., A.L., F.G. and A.M; writing—original draft preparation, A.S.; writing—review and editing, A.S., A.L., F.G. and A.M.; visualization, A.S., F.G. and A.M.; supervision, A.S., and A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
We would like to acknowledge the use of OpenAI’s language model, GPT-4, in the preparation of this manuscript. Specifically, GPT-4 was used to improve the English language usage, clarity of text, polishing the manuscript and overall manuscript editing. Please note that GPT-4 was not used to generate original content or influence the interpretations and conclusions of this manuscript. All research, data analysis and content creation were conducted by the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Murray, P.R.; Rosenthal, K.; Pfaller, M.A. Medical Microbiology; Ninth.; ELSEVIER, 2020.
- World Health Organization Global Tuberculosis Report 2023.
- Uplekar, M.; Weil, D.; Lonnroth, K.; Jaramillo, E.; Lienhardt, C.; Dias, H.M.; Falzon, D.; Floyd, K.; Gargioni, G.; Getahun, H.; et al. WHO’s New End TB Strategy. The Lancet 2015, 385, 1799–1801. [Google Scholar] [CrossRef] [PubMed]
- Gygli, S.M.; Borrell, S.; Trauner, A.; Gagneux, S. Antimicrobial Resistance in Mycobacterium Tuberculosis: Mechanistic and Evolutionary Perspectives. FEMS Microbiology Reviews 2017, 41, 354–373. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO Consolidated Guidelines; World Health Organization: Geneva, 2022; ISBN 978-92-4-004685-6.
- Alagna, R.; Cabibbe, A.M.; Miotto, P.; Saluzzo, F.; Köser, C.U.; Niemann, S.; Gagneux, S.; Rodrigues, C.; Rancoita, P.V.M.; Cirillo, D.M. Is the New WHO Definition of Extensively Drug-Resistant Tuberculosis Easy to Apply in Practice? The European respiratory journal 2021, 58. [Google Scholar] [CrossRef] [PubMed]
- Viney, K.; Linh, N.N.; Gegia, M.; Zignol, M.; Glaziou, P.; Ismail, N.; Kasaeva, T.; Mirzayev, F. New Definitions of Pre-Extensively and Extensively Drug-Resistant Tuberculosis: Update from the World Health Organization. Eur Respir J 2021, 57, 2100361. [Google Scholar] [CrossRef] [PubMed]
- Maurer, F.P.; Shubladze, N.; Kalmambetova, G.; Felker, I.; Kuchukhidze, G.; Koeser, C.U.; Cirillo, D.M.; Drobniewski, F.; Yedilbayev, A.; Ehsani, S.; et al. Diagnostic Capacities for Multidrug-Resistant Tuberculosis in the World Health Organization European Region Action Is Needed by All Member States. JOURNAL OF MOLECULAR DIAGNOSTICS 2022, 24, 1189–1194. [Google Scholar] [CrossRef]
- Farooq, H.Z.; Cirillo, D.M.; Hillemann, D.; Wyllie, D.; van der Werf, M.J.; Ködmön, C.; Nikolayevskyy, V. Limited Capability for Testing Mycobacterium Tuberculosis for Susceptibility to New Drugs. Emerging infectious diseases 2021, 27, 985–987. [Google Scholar] [CrossRef]
- Lee, A.; Xie, Y.L.; Barry, C.E.; Chen, R.Y. Current and Future Treatments for Tuberculosis. BMJ (Clinical research ed.) 2020, 368, m216. [Google Scholar] [CrossRef]
- Nguyen, L. Antibiotic Resistance Mechanisms in M. Tuberculosis: An Update. Arch Toxicol 2016, 90, 1585–1604. [Google Scholar] [CrossRef]
- Walker, T.M.; Merker, M.; Kohl, T.A.; Crook, D.W.; Niemann, S.; Peto, T.E.A. Whole Genome Sequencing for M/XDR Tuberculosis Surveillance and for Resistance Testing. Clinical Microbiology and Infection 2017, 23, 161–166. [Google Scholar] [CrossRef]
- Zurcher, K.; Reichmuth, M.L.; Ballif, M.; Loiseau, C.; Borrell, S.; Reinhard, M.; Skrivankova, V.; Homke, R.; Sander, P.; Avihingsanon Anchalee and Abimiku, A.G.; et al. Mortality from Drug-Resistant Tuberculosis in High-Burden Countries Comparing Routine Drug Susceptibility Testing with Whole-Genome Sequencing: A Multicentre Cohort Study. LANCET MICROBE 2021, 2, E320–E330. [Google Scholar] [CrossRef]
- Mugwagwa, T.; Abubakar, I.; White, P.J. Using Molecular Testing and Whole-Genome Sequencing for Tuberculosis Diagnosis in a Low-Burden Setting: A Cost-Effectiveness Analysis Using Transmission-Dynamic Modelling. Thorax 2021, 76, 281–291. [Google Scholar] [CrossRef]
- Sanchini, A. Recent Developments in Phenotypic and Molecular Diagnostic Methods for Antimicrobial Resistance Detection in Staphylococcus Aureus: A Narrative Review. Diagnostics 2022, 12, 208. [Google Scholar] [CrossRef]
- Ferrari, R. Writing Narrative Style Literature Reviews. Medical Writing 2015, 24, 230–235. [Google Scholar] [CrossRef]
- Wu, S.-H.; Chan, H.-H.; Hsiao, H.-C.; Jou, R. Primary Bedaquiline Resistance Among Cases of Drug-Resistant Tuberculosis in Taiwan. Frontiers in microbiology 2021, 12, 754249. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.M.M.; Ather, Md.F.; Nasrin, R.; Hoque, M.A.; Khatun, R.; Rahman, T.; Uddin, M.K.M.; Ahmed, S.; Banu, S. Performance of WHO-Endorsed Rapid Tests for Detection of Susceptibility to First-Line Drugs in Patients with Pulmonary Tuberculosis in Bangladesh. DIAGNOSTICS 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Ushtanit, A.; Kulagina, E.; Mikhailova, Y.; Makarova, M.; Safonova, S.; Zimenkov, D. Molecular Determinants of Ethionamide Resistance in Clinical Isolates of Mycobacterium Tuberculosis. ANTIBIOTICS-BASEL 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Reghunath, A.; Shenoy, V.P.; Kushal, S.; Pandey, A.K. “Crystal Violet Decolorization Assay: A Simplified Colorimetric Test for the Rapid Detection of Multidrug-Resistant Mycobacterium Tuberculosis Isolates”. Microbes Infect 2023, 105108. [Google Scholar] [CrossRef] [PubMed]
- Akbal, A.U.; Durupinar, B.; Coban, A.Y. Colorimetric Methods for Rapid Determination of Pyrazinamide Resistance. International journal of mycobacteriology 2020, 9, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Ardizzoni, E.; Ariza, E.; Mulengwa, D.; Mpala, Q.; de La Tour, R.; Maphalala, G.; Varaine, F.; Kerschberger, B.; Graulus, P.; Page, A.L.; et al. Thin-Layer-Agar-Based Direct Phenotypic Drug Susceptibility Testing on Sputum in Eswatini Rapidly Detects Mycobacterium Tuberculosis Growth and Rifampicin Resistance Otherwise Missed by WHO-Endorsed Diagnostic Tests. Antimicrobial agents and chemotherapy 2021, 65. [Google Scholar] [CrossRef] [PubMed]
- Shibabaw, A.; Gelaw, B.; Kelley, H.V.; Tesfaye, E.; Balada-Llasat, J.M.; Evans, C.A.; Torrelles, J.B.; Wang, S.-H.; Tessema, B. MDR/XDR-TB Colour Test for Drug Susceptibility Testing of Mycobacterium Tuberculosis, Northwest Ethiopia. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases 2020, 90, 213–218. [Google Scholar] [CrossRef]
- Achan, B.; Asiimwe, B.B.; Joloba, M.L.; Gumusboga, M.; Ssengooba, W.; Bwanga, F. The Simple Direct Slide Method Is Comparable to Indirect Lowenstein Jensen Proportion Culture for Detecting Rifampicin Resistant Tuberculosis. Journal of medical microbiology 2021, 70. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-K.; Baek, S.-H.; Hong, M.-S.; Lee, J.-S.; Cho, E.-J.; Lee, J.-I.; Cho, S.-N.; Eum, S.-Y. A Rapid Assessing Method of Drug Susceptibility Using Flow Cytometry for Mycobacterium Tuberculosis Isolates Resistant to Isoniazid, Rifampin, and Ethambutol. TUBERCULOSIS AND RESPIRATORY DISEASES 2022, 85, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-C.; Gao, Y.-L.; Li, D.-F.; Zhao, X.-Y.; Pan, Y.-Q.; Zhu, C.-T. Value of Xpert MTB/RIF Using Bronchoalveolar Lavage Fluid for the Diagnosis of Pulmonary Tuberculosis: A Systematic Review and Meta-Analysis. Journal of clinical microbiology 2021, 59. [Google Scholar] [CrossRef] [PubMed]
- Xia, H.; Song, Y.; Zheng, Y.; Wang, S.; Zhao, B.; He, W.; Liu, D.; Ou, X.; Zhou, Y.; Zhao, Y. Detection of Mycobacterium Tuberculosis Rifampicin Resistance Conferred by Borderline rpoB Mutations: Xpert MTB/RIF Is Superior to Phenotypic Drug Susceptibility Testing. Infection and drug resistance 2022, 15, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Ssengooba, W.; de Dieu Iragena, J.; Komakech, K.; Okello, I.; Nalunjogi, J.; Katagira, W.; Kimuli, I.; Adakun, S.; Joloba, M.L.; Torrea, G.; et al. Discordance of the Repeat GeneXpert MTB/RIF Test for Rifampicin Resistance Detection Among Patients Initiating MDR-TB Treatment in Uganda. Open forum infectious diseases 2021, 8, ofab173. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, X.; Huo, F.; Qin, L.; Liu, R.; Shang, Y.; Yao, C.; Ma, L.; Pang, Y. Analysis of Xpert MTB/RIF Results in Retested Patients with Very Low Initial Bacterial Loads: A Retrospective Study in China. J Infect Public Health 2023, 16, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Rueda, Z.V.; Li, T.; Zhang, Z.; Jiang, Y.; Sha, W.; Yu, F.; Chen, J.; Pan Qichao and Shen, X.; Yuan, Z.; et al. Effect of the Xpert MTB/RIF on the Detection of Pulmonary Tuberculosis Cases and Rifampicin Resistance in Shanghai, China. BMC infectious diseases 2020, 20, 153. [Google Scholar] [CrossRef]
- Jeon, D.; Kang, H.; Kwon, Y.S.; Yim, J.J.; Shim, T.S. Impact of Molecular Drug Susceptibility Testing on the Time to Multidrug-Resistant Tuberculosis Treatment Initiation. Journal of Korean medical science 2020, 35, e284. [Google Scholar] [CrossRef]
- Georghiou, S.B.; Penn-Nicholson, A.; de Vos, M.; Macé, A.; Syrmis, M.W.; Jacob, K.; Mape, A.; Parmar, H.; Cao, Y.; Coulter, C.; et al. Analytical Performance of the Xpert MTB/XDR® Assay for Tuberculosis and Expanded Resistance Detection. Diagnostic microbiology and infectious disease 2021, 101, 115397. [Google Scholar] [CrossRef]
- Cao, Y.; Parmar, H.; Gaur, R.L.; Lieu, D.; Raghunath, S.; Via, N.; Battaglia, S.; Cirillo, D.M.; Denkinger, C.; Georghiou, S.; et al. Xpert MTB/XDR: A 10-Color Reflex Assay Suitable for Point-of-Are Settings To Detect Isoniazid, Fluoroquinolone, and Second-Line-Injectable-Drug Resistance Directly from Mycobacterium Tuberculosis-Positive Sputum. JOURNAL OF CLINICAL MICROBIOLOGY 2021, 59. [Google Scholar] [CrossRef]
- Truden, S.; Sodja, E.; Žolnir-Dovč, M. Drug-Resistant Tuberculosis on the Balkan Peninsula: Determination of Drug Resistance Mechanisms with Xpert MTB/XDR and Whole-Genome Sequencing Analysis. Microbiol Spectr 2023, 11, e0276122. [Google Scholar] [CrossRef]
- Georghiou, S.B.; Alagna, R.; Cirillo, D.M.; Carmona, S.; Ruhwald, M.; Schumacher, S.G. Equivalence of the GeneXpert System and GeneXpert Omni System for Tuberculosis and Rifampicin Resistance Detection. PLoS ONE 2021, 16, e0261442. [Google Scholar] [CrossRef] [PubMed]
- Ngabonziza, J.C.S.; Decroo, T.; Migambi, P.; Habimana, Y.M.; Van Deun, A.; Meehan, C.J.; Torrea, G.; Massou, F.; de Rijk, W.B.; Ushizimpumu, B.; et al. Prevalence and Drivers of False-Positive Rifampicin-Resistant Xpert MTB/RIF Results: A Prospective Observational Study in Rwanda. The Lancet. Microbe 2020, 1, e74–e83. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Davies Forsman, L.; Hu, Y.; Zheng, X.; Gao, Y.; Li, X.; Jiang, W.; Bruchfeld, J.; Diwan, V.K.; Hoffner, S.; et al. Improved Treatment Outcome of Multidrug-Resistant Tuberculosis with the Use of a Rapid Molecular Test to Detect Drug Resistance in China. International Journal of Infectious Diseases 2020, 96, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Van Rie, A.; Whitfield, M.G.; De Vos, E.; Scott, L.; Da Silva, P.; Hayes, C.; Heupink, T.H.; Sirgel, F.A.; Stevens, W.; Warren, R.M. Discordances between Molecular Assays for Rifampicin Resistance in Mycobacterium Tuberculosis: Frequency, Mechanisms and Clinical Impact. The Journal of antimicrobial chemotherapy 2020, 75, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Mahomed, S.; Mlisana, K.; Cele, L.; Naidoo, K. Discordant Line Probe Genotypic Testing vs Culture-Based Drug Susceptibility Phenotypic Testing in TB Endemic KwaZulu-Natal: Impact on Bedside Clinical Decision Making. Journal of clinical tuberculosis and other mycobacterial diseases 2020, 20, 100176. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.M.M.; Nasrin, R.; Rahman, A.; Ahmed, S.; Khatun, R.; Uddin, M.K.M.; Rahman, Md.M.; Banu, S. Performance of GenoType MTBDRsl Assay for Detection of Second-Line Drugs and Ethambutol Resistance Directly from Sputum Specimens of MDR-TB Patients in Bangladesh. PLOS ONE 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Rufai, S.B.; Umay, K.; Singh, P.K.; Singh, S. Performance of Genotype MTBDRsl V2.0 over the Genotype MTBDRsl V1 for Detection of Second Line Drug Resistance: An Indian Perspective. PloS one 2020, 15, e0229419. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Singh, U.; Kumar, V.; Ratnam, R.; Jain, A. Agreement between CBNAAT, Liquid Culture and Line Probe Assay for Detection of Mycobacterium Tuberculosis and Anti-Tubercular Drug Resistance in Extrapulmonary Samples. INDIAN JOURNAL OF MEDICAL MICROBIOLOGY 2022, 40, 365–369. [Google Scholar] [CrossRef]
- Pinhata, J.M.W.; Brandao, A.P.; Gallo, J.F.; Oliveira, R.S. de; Ferrazoli, L. GenoType MTBDRsl for Detection of Second-Line Drugs and Ethambutol Resistance in Multidrug-Resistant Mycobacterium Tuberculosis Isolates at a High-Throughput Laboratory. Diagn Microbiol Infect Dis 2023, 105, 115856. [Google Scholar] [CrossRef]
- Pillay, S.; de Vos, M.; Derendinger, B.; Streicher, E.M.; Dolby, T.; Scott, L.A.; Steinhobel, A.D.; Warren, R.M.; Theron, G. Non-Actionable Results, Accuracy, and Effect of First- and Second-Line Line Probe Assays for Diagnosing Drug-Resistant Tuberculosis, Including on Smear-Negative Specimens, in a High-Volume Laboratory. Clin Infect Dis 2023, 76, e920–e929. [Google Scholar] [CrossRef]
- Lin, M.; Chen, Y.-W.; Li, Y.-R.; Long, L.-J.; Qi, L.-Y.; Cui, T.-T.; Wu, S.-Y.; Lin, J.-Y.; Wu, T.; Yang, Y.-C.; et al. Systematic Evaluation of Line Probe Assays for the Diagnosis of Tuberculosis and Drug-Resistant Tuberculosis. Clin Chim Acta 2022, 533, 183–218. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Kumari, R.; Gupta, S.; Tripathi, R.; Srivastava, A.; Shakya, V.; Gupta, A.; Anupurba, S. Direct Detection of Resistance to Fluoroquinolones/SLIDs in Sputum Specimen by GenoType MTBDRsl v.2.0 Assay A Study from Eastern Uttar Pradesh, India. Annals of clinical microbiology and antimicrobials 2021, 20, 56. [Google Scholar] [CrossRef]
- Shah, M.; Paradis, S.; Betz, J.; Beylis, N.; Bharadwaj, R.; Caceres, T.; Gotuzzo, E.; Joloba, M.; Mave, V.; Nakiyingi, L.; et al. Multicenter Study of the Accuracy of the BD MAX Multidrug-Resistant Tuberculosis Assay for Detection of Mycobacterium Tuberculosis Complex and Mutations Associated With Resistance to Rifampin and Isoniazid. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2020, 71, 1161–1167. [Google Scholar] [CrossRef]
- Zhou, Y.-C.; He, S.-M.; Wen, Z.-L.; Zhao, J.-W.; Song, Y.-Z.; Zhang, Y.; Zhang, S.-L. A Rapid and Accurate Detection Approach for Multidrug-Resistant Tuberculosis Based on PCR-ELISA Microplate Hybridization Assay. Laboratory medicine 2020, 51, 606–613. [Google Scholar] [CrossRef]
- Chang, Y.; Kim, S.; Kim, Y.; Ei, P.W.; Hwang, D.; Lee, J.; Chang, C.L.; Lee, H. Evaluation of the QuantaMatrix Multiplexed Assay Platform for Molecular Diagnosis of Multidrug- and Extensively Drug-Resistant Tuberculosis Using Clinical Strains Isolated in Myanmar. ANNALS OF LABORATORY MEDICINE 2020, 40, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.S.-S.; Tam, K.K.-G.; Ng, T.T.-L.; Lao, H.-Y.; Shek, R.C.-M.; Ma, O.C.K.; Yu, S.-H.; Chen, J.-X.; Han, Q.; Siu, G.K.-H.; et al. Clinical Utility of Target Amplicon Sequencing Test for Rapid Diagnosis of Drug-Resistant Mycobacterium Tuberculosis from Respiratory Specimens. FRONTIERS IN MICROBIOLOGY 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.; Lee, S.J.; Lim, J.; Kim, D.S.; Kim, N.; Park, H.O.; Lee, J.-I.; Son, E.; Cho, S.N.; Aung, W.W.; et al. Evaluation of TBMDR® and XDRA® for the Detection of Multidrug Resistant and Pre-Extensively Drug Resistant Tuberculosis. Journal of clinical tuberculosis and other mycobacterial diseases 2022, 27, 100303. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Sun, Y. Diagnostic Performance of DNA Microarray for Detecting Rifampicin and Isoniazid Resistance in Mycobacterium Tuberculosis. JOURNAL OF THORACIC DISEASE 2021, 13, 4448–4454. [Google Scholar] [CrossRef]
- Thant, Y.M.; Saikaew, S.; Tharinjaroen, C.S.; Phunpae, P.; Pongsararuk, R.; Preechasuth, K.; Butr-Indr, B.; Intorasoot, S.; Tragoolpua, K.; Chaiprasert, A.; et al. Combined Locked Nucleic Acid Probes and High-Resolution Melting Curve Analysis for Detection of Rifampicin-Resistant Tuberculosis in Northern Thailand. DIAGNOSTICS 2022, 12. [Google Scholar] [CrossRef]
- Ou, X.; Zhang, Z.; Zhao, B.; Song, Z.; Wang, S.; He, W.; Pei, S.; Liu, D.; Xing, R.; Xia, H.; et al. Evaluation Study of xMAP TIER Assay on a Microsphere-Based Platform for Detecting First-Line Anti-Tuberculosis Drug Resistance. INTERNATIONAL JOURNAL OF ENVIRONMENTAL RESEARCH AND PUBLIC HEALTH 2022, 19. [Google Scholar] [CrossRef]
- Penn-Nicholson, A.; Gomathi, S.N.; Ugarte-Gil, C.; Meaza, A.; Lavu, E.; Patel, P.; Choudhury, B.; Rodrigues, C.; Chadha, S.; Kazi, M.; et al. A Prospective Multicentre Diagnostic Accuracy Study for the Truenat Tuberculosis Assays. The European respiratory journal 2021, 58. [Google Scholar] [CrossRef] [PubMed]
- Hu, O.; Li, Z.; He, Q.; Tong, Y.; Tan, Y.; Chen, Z. Fluorescence Biosensor for One-Step Simultaneous Detection of Mycobacterium Tuberculosis Multidrug-Resistant Genes Using nanoCoTPyP and Double Quantum Dots. Analytical chemistry 2022, 94, 7918–7927. [Google Scholar] [CrossRef] [PubMed]
- Ou, X.; Li, Q.; Su, D.; Xia, H.; Wang, S.; Zhao, B.; Zhao, Y. A Pilot Study: VereMTB Detection Kit for Rapid Detection of Multidrug-Resistant Mycobcterium Tuberculosis in Clinical Sputum Samples. PloS one 2020, 15, e0228312. [Google Scholar] [CrossRef] [PubMed]
- Colman, R.E.; Hagan, C.; Chiles, P.; Seifert, M.; Catanzaro, D.G.; Kukhtin, A.V.; Norville, R.; Hauns, L.; Bueno, A.; Holmberg, R.C.; et al. Detecting Rifampin and Isoniazid Resistance in Mycobacterium Tuberculosis Direct from Patient Sputum Using an Automated Integrated System. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases 2022, 27, 100304. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Li, A.; Dang, L.; Kang, T.; Ren, F.; Ma, J.; Zhou, Y.; Yang, Y.; Lei, J.; Zhang, T. A Rapid, Accurate, and Low-Cost Method for Detecting Mycobacterium Tuberculosis and Its Drug-Resistant Genes in Pulmonary Tuberculosis: Applications of MassARRAY DNA Mass Spectrometry. FRONTIERS IN MICROBIOLOGY 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; He, G.; Ning, H.; Wu, L.; Wu, Z.; Ye, X.; Qiu, C.; Jiang, X. Application of Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS) in the Detection of Drug Resistance of Mycobacterium Tuberculosis in Re-Treated Patients. Tuberculosis (Edinb) 2022, 135, 102209. [Google Scholar] [CrossRef]
- Wu, X.; Tan, G.; Yang, J.; Guo, Y.; Huang, C.; Sha, W.; Yu, F. Prediction of Mycobacterium Tuberculosis Drug Resistance by Nucleotide MALDI-TOF-MS. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases 2022, 121, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, X.-D.; Tang, J.-W.; Ma, Z.-W.; Usman, M.; Liu, Q.-H.; Wu, C.-Y.; Li, F.; Zhu, Z.-B.; Gu, B. Machine Learning Analysis of SERS Fingerprinting for the Rapid Determination of Mycobacterium Tuberculosis Infection and Drug Resistance. Comput Struct Biotechnol J 2022, 20, 5364–5377. [Google Scholar] [CrossRef]
- Muzondiwa, D.; Mutshembele, A.; Pierneef, R.E.; Reva, O.N. Resistance Sniffer: An Online Tool for Prediction of Drug Resistance Patterns of Mycobacterium Tuberculosis Isolates Using next Generation Sequencing Data. International journal of medical microbiology : IJMM 2020, 310, 151399. [Google Scholar] [CrossRef]
- Hasan, M.; Munshi, S.K.; Banu Momi, Mst. S.; Rahman, F.; Noor, R. Evaluation of the Effectiveness of BACTEC MGIT 960 for the Detection of Mycobacteria in Bangladesh. International Journal of Mycobacteriology 2013, 2, 214–219. [Google Scholar] [CrossRef]
- Richter, E.; Rüsch-Gerdes, S.; Hillemann, D. Drug-Susceptibility Testing in TB: Current Status and Future Prospects. Expert Review of Respiratory Medicine 2009, 3, 497–510. [Google Scholar] [CrossRef]
- Hong, J.M.; Lee, H.; Menon, N.V.; Lim, C.T.; Lee, L.P.; Ong, C.W.M. Point-of-Care Diagnostic Tests for Tuberculosis Disease. Sci. Transl. Med. 2022, 14, eabj4124. [Google Scholar] [CrossRef]
- Schön, T.; Werngren, J.; Machado, D.; Borroni, E.; Wijkander, M.; Lina, G.; Mouton, J.; Matuschek, E.; Kahlmeter, G.; Giske, C.; et al. Multicentre Testing of the EUCAST Broth Microdilution Reference Method for MIC Determination on Mycobacterium Tuberculosis. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases 2021, 27, 288.e1-288.e4. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Handbook on Tuberculosis Laboratory Diagnostic Methods in the European Union: Updated 2018.; Publications Office: LU, 2018. [Google Scholar]
- Lee, J.; Armstrong, D.T.; Ssengooba, W.; Park, J.; Yu, Y.; Mumbowa, F.; Namaganda, C.; Mboowa, G.; Nakayita, G.; Armakovitch, S.; et al. Sensititre MYCOTB MIC Plate for Testing Mycobacterium Tuberculosis Susceptibility to First- and Second-Line Drugs. Antimicrob Agents Chemother 2014, 58, 11–18. [Google Scholar] [CrossRef]
- Migliori, G.B.; Tiberi, S.; Zumla, A.; Petersen, E.; Chakaya, J.M.; Wejse, C.; Muñoz Torrico, M.; Duarte, R.; Alffenaar, J.W.; Schaaf, H.S.; et al. MDR/XDR-TB Management of Patients and Contacts: Challenges Facing the New Decade. The 2020 Clinical Update by the Global Tuberculosis Network. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases 2020, 92S, S15–S25. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Use of Xpert MTB/RIF and Xpert MTB/RIF Ultra on GeneXpert 10-Colour Instruments 2021.
- World Health Organization The Use of Molecular Line Probe Assays for the Detection of Resistance to Second-Line Anti-Tuberculosis Drugs: Policy Guidance; World Health Organization: Geneva, 2016; ISBN 978-92-4-151613-6.
- Zifodya, J.S.; Kreniske, J.S.; Schiller, I.; Kohli, M.; Dendukuri, N.; Schumacher, S.G.; Ochodo, E.A.; Haraka, F.; Zwerling, A.A.; Pai, M.; et al. Xpert Ultra versus Xpert MTB/RIF for Pulmonary Tuberculosis and Rifampicin Resistance in Adults with Presumptive Pulmonary Tuberculosis. The Cochrane database of systematic reviews 2021, 2, CD009593. [Google Scholar] [CrossRef] [PubMed]
- Donovan, J.; Thu, D.D.A.; Phu, N.H.; Dung, V.T.M.; Quang, T.P.; Nghia, H.D.T.; Oanh, P.K.N.; Nhu, T.B.; Chau, N.V.V.; Ha, V.T.N.; et al. Xpert MTB/RIF Ultra versus Xpert MTB/RIF for the Diagnosis of Tuberculous Meningitis: A Prospective, Randomised, Diagnostic Accuracy Study. The Lancet Infectious Diseases 2020, 20, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Mvelase, N.R.; Mlisana, K.P. Xpert MTB/XDR for Rapid Detection of Drug-Resistant Tuberculosis beyond Rifampicin. The Lancet. Infectious diseases 2022, 22, 156–157. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Catalogue of Mutations in Mycobacterium Tuberculosis Complex and Their Association with Drug Resistance 2021.
- Bai, Y.; Wang, Y.; Shao, C.; Hao, Y.; Jin, Y. GenoType MTBDRplus Assay for Rapid Detection of Multidrug Resistance in Mycobacterium Tuberculosis: A Meta-Analysis. PLoS ONE 2016, 11, e0150321. [Google Scholar] [CrossRef]
- Ransom, E.M.; Potter, R.F.; Dantas, G.; Burnham, C.-A.D. Genomic Prediction of Antimicrobial Resistance: Ready or Not, Here It Comes! Clinical chemistry 2020, 66, 1278–1289. [Google Scholar] [CrossRef]
- The CRyPTIC Consortium and the 100,000 Genomes Project Prediction of Susceptibility to First-Line Tuberculosis Drugs by DNA Sequencing. N Engl J Med 2018, 379, 1403–1415. [CrossRef]
- Cabibbe, A.M.; Spitaleri, A.; Battaglia, S.; Colman, R.E.; Suresh, A.; Uplekar, S.; Rodwell, T.C.; Cirillo, D.M. Application of Targeted Next-Generation Sequencing Assay on a Portable Sequencing Platform for Culture-Free Detection of Drug-Resistant Tuberculosis from Clinical Samples. Journal of clinical microbiology 2020, 58. [Google Scholar] [CrossRef]
- Phelan, J.; O’Sullivan, D.M.; Machado, D.; Ramos, J.; Whale, A.S.; O’Grady, J.; Dheda, K.; Campino, S.; McNerney, R.; Viveiros, M.; et al. The Variability and Reproducibility of Whole Genome Sequencing Technology for Detecting Resistance to Anti-Tuberculous Drugs. Genome Med 2016, 8, 132. [Google Scholar] [CrossRef] [PubMed]
- Steiner, A.; Stucki, D.; Coscolla, M.; Borrell, S.; Gagneux, S. KvarQ: Targeted and Direct Variant Calling from Fastq Reads of Bacterial Genomes. BMC Genomics 2014, 15, 881. [Google Scholar] [CrossRef]
- Coll, F.; McNerney, R.; Preston, M.D.; Guerra-Assunção, J.A.; Warry, A.; Hill-Cawthorne, G.; Mallard, K.; Nair, M.; Miranda, A.; Alves, A.; et al. Rapid Determination of Anti-Tuberculosis Drug Resistance from Whole-Genome Sequences. Genome Med 2015, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- Iwai, H.; Kato-Miyazawa, M.; Kirikae, T.; Miyoshi-Akiyama, T. CASTB (the Comprehensive Analysis Server for the Mycobacterium Tuberculosis Complex): A Publicly Accessible Web Server for Epidemiological Analyses, Drug-Resistance Prediction and Phylogenetic Comparison of Clinical Isolates. Tuberculosis (Edinb) 2015, 95, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P.; Gordon, N.C.; Walker, T.M.; Dunn, L.; Heys, S.; Huang, B.; Earle, S.; Pankhurst, L.J.; Anson, L.; de Cesare, M.; et al. Rapid Antibiotic-Resistance Predictions from Genome Sequence Data for Staphylococcus Aureus and Mycobacterium Tuberculosis. Nat Commun 2015, 6, 10063. [Google Scholar] [CrossRef] [PubMed]
- Feuerriegel, S.; Kohl, T.A.; Utpatel, C.; Andres, S.S.; Maurer, F.P.; Heyckendorf, J.; Jouet, A.; Badalato, N.; Foray, L.; Fouad Kamara, R.; et al. Rapid Genomic First- and Second-Line Drug Resistance Prediction from Clinical Mycobacterium Tuberculosis Specimens Using Deeplex-MycTB. The European respiratory journal 2021, 57. [Google Scholar] [CrossRef] [PubMed]
- Deelder, W.; Napier, G.; Campino, S.; Palla Luigi and Phelan, J.; Clark, T.G.; Palla, L.; Phelan, J.; Clark, T.G.; Palla Luigi and Phelan, J.; Clark, T.G. A Modified Decision Tree Approach to Improve the Prediction and Mutation Discovery for Drug Resistance in Mycobacterium Tuberculosis. BMC genomics 2022, 23, 46. [Google Scholar] [CrossRef]
- Walker, T.M.; Miotto, P.; Köser, C.U.; Fowler, P.W.; Knaggs, J.; Iqbal, Z.; Hunt, M.; Chindelevitch, L.; Farhat, M.; Cirillo, D.M.; et al. The 2021 WHO Catalogue of Mycobacterium Tuberculosis Complex Mutations Associated with Drug Resistance: A Genotypic Analysis. The Lancet. Microbe 2022, 3, e265–e273. [Google Scholar] [CrossRef]
- Liu, D.; Huang, F.; Zhang, G.; He, W.; Ou, X.; He, P.; Zhao, B.; Zhu, B.; Liu, F.; Li, Z.; et al. Whole-Genome Sequencing for Surveillance of Tuberculosis Drug Resistance and Determination of Resistance Level in China. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases 2022, 28, 731.e9-731.e15. [Google Scholar] [CrossRef]
- Mbelele, P.M.; Utpatel, C.; Sauli, E.; Mpolya, E.A.; Mutayoba, B.K.; Barilar, I.; Dreyer, V.; Merker, M.; Sariko, M.L.; Swema, B.M.; et al. Whole Genome Sequencing-Based Drug Resistance Predictions of Multidrug-Resistant Mycobacterium Tuberculosis Isolates from Tanzania. JAC-antimicrobial resistance 2022, 4, dlac042. [Google Scholar] [CrossRef]
- Wang, L.; Yang, J.; Chen, L.; Wang, W.; Yu, F.; Xiong, H. Whole-Genome Sequencing of Mycobacterium Tuberculosis for Prediction of Drug Resistance. Epidemiology and infection 2022, 150, e22. [Google Scholar] [CrossRef]
- Che, Y.; Lin, Y.; Yang, T.; Chen, T.; Sang, G.; Chen, Q.; He, T. Evaluation of Whole-Genome Sequence to Predict Drug Resistance of Nine Anti-Tuberculosis Drugs and Characterize Resistance Genes in Clinical Rifampicin-Resistant Mycobacterium Tuberculosis Isolates from Ningbo, China. FRONTIERS IN PUBLIC HEALTH 2022, 10. [Google Scholar] [CrossRef]
- Mesfin, E.A.; Merker, M.; Beyene, D.; Tesfaye, A.; Shuaib, Y.A.; Addise, D.; Tessema, B.; Niemann, S. Prediction of Drug Resistance by Sanger Sequencing of Mycobacterium Tuberculosis Complex Strains Isolated from Multidrug Resistant Tuberculosis Suspect Patients in Ethiopia. PLoS One 2022, 17, e0271508. [Google Scholar] [CrossRef]
- Tania, T.; Sudarmono, P.; Kusumawati, R.L.; Rukmana, A.; Pratama, W.A.; Regmi, S.M.; Kaewprasert, O.; Chaiprasert, A.; Chongsuvivatwong, V.; Faksri, K. Whole-Genome Sequencing Analysis of Multidrug-Resistant Mycobacterium Tuberculosis from Java, Indonesia. Journal of medical microbiology 2020, 69, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Soetaert, K.; Ceyssens, P.-J.; Boarbi, S.; Bogaerts, B.; Delcourt, T.; Vanneste, K.; De Keersmaecker, S.C.J.; Roosens, N.H.C.; Vodolazkaia, A.; Mukovnikova, M.; et al. Retrospective Evaluation of Routine Whole Genome Sequencing of Mycobacterium Tuberculosis at the Belgian National Reference Center, 2019. Acta Clin Belg 2022, 77, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Enkirch, T.; Werngren, J.; Groenheit, R.; Alm Erik and Advani, R.; Karlberg, M.L.; Mansjo, M. Systematic Review of Whole-Genome Sequencing Data To Predict Phenotypic Drug Resistance and Susceptibility in Swedish Mycobacterium Tuberculosis Isolates, 2016 to 2018. ANTIMICROBIAL AGENTS AND CHEMOTHERAPY 2020, 64. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-H.; Xiao, Y.-X.; Hsiao, H.-C.; Jou, R. Development and Assessment of a Novel Whole-Gene-Based Targeted Next-Generation Sequencing Assay for Detecting the Susceptibility of Mycobacterium Tuberculosis to 14 Drugs. Microbiol Spectr 2022, 10, e0260522. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.; Halse, T.A.; Shea, J.; Modestil, H.; Fowler, R.C.; Musser, K.A.; Escuyer, V.; Lapierre, P. Assessing Nanopore Sequencing for Clinical Diagnostics: A Comparison of Next-Generation Sequencing (NGS) Methods for Mycobacterium Tuberculosis. Journal of clinical microbiology 2020, 59. [Google Scholar] [CrossRef] [PubMed]
- Soundararajan, L.; Kambli, P.; Priyadarshini, S.; Let, B.; Murugan, S.; Iravatham, C.; Tornheim, J.A.; Rodrigues, C.; Gupta, R.; Ramprasad, V.L. Whole Genome Enrichment Approach for Rapid Detection of Mycobacterium Tuberculosis and Drug Resistance-Associated Mutations from Direct Sputum Sequencing. Tuberculosis (Edinburgh, Scotland) 2020, 121, 101915. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Su, R.; Zheng, D.; Zhu, Y.; Ma, X.; Wang, S.; Li, H.; Sun, D. Pyrazinamide Resistance and Mutation Patterns Among Multidrug-Resistant Mycobacterium Tuberculosis from Henan Province. INFECTION AND DRUG RESISTANCE 2020, 13, 2929–2941. [Google Scholar] [CrossRef] [PubMed]
- Solari, L.; Santos-Lazaro, D.; Puyen, Z.M. Mutations in Mycobacterium Tuberculosis Isolates with Discordant Results for Drug-Susceptibility Testing in Peru. International journal of microbiology 2020, 2020, 8253546. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Lalvani, A.; Satta, G.; Kon, O.M. Evaluating the Clinical Impact of Routine Whole Genome Sequencing in Tuberculosis Treatment Decisions and the Issue of Isoniazid Mono-Resistance. BMC infectious diseases 2022, 22, 349. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.; Utpatel, C.; Corbett, C.; Kohl, T.A.; Iskakova, A.; Ahmedov, S.; Antonenka, U.; Dreyer, V.; Ibrahimova, A.; Kamarli, C.; et al. Implementation of Whole Genome Sequencing for Tuberculosis Diagnostics in a Low-Middle Income, High MDR-TB Burden Country. Scientific reports 2021, 11, 15333. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.; Martinez, E.; Crighton, T.; Furlong, C.; Donnan, E.; Marais, B.J.; Sintchenko, V. Value of Routine Whole Genome Sequencing for Mycobacterium Tuberculosis Drug Resistance Detection. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases 2021, 113 Suppl, S48–S54. [CrossRef]
- Green, A.G.; Yoon, C.H.; Chen, M.L.; Ektefaie, Y.; Fina, M.; Freschi, L.; Groschel, M., I.; Kohane, I.; Beam, A.; Farhat, M. A Convolutional Neural Network Highlights Mutations Relevant to Antimicrobial Resistance in Mycobacterium Tuberculosis. NATURE COMMUNICATIONS 2022, 13. [Google Scholar] [CrossRef]
- Dookie, N.; Khan, A.; Padayatchi, N.; Naidoo, K. Application of Next Generation Sequencing for Diagnosis and Clinical Management of Drug-Resistant Tuberculosis: Updates on Recent Developments in the Field. FRONTIERS IN MICROBIOLOGY 2022, 13. [Google Scholar] [CrossRef]
- Sharma, A.; Machado, E.; Lima, K.V.B.; Suffys, P.N.; Conceição, E.C.; Conceicao, E.C. Tuberculosis Drug Resistance Profiling Based on Machine Learning: A Literature Review. The Brazilian journal of infectious diseases : an official publication of the Brazilian Society of Infectious Diseases 2022, 26, 102332. [Google Scholar] [CrossRef]
- Dohal, M.; Dvorakova, V.; Sperkova, M.; Pinkova, M.; Spitaleri, A.; Norman, A.; Cabibbe, A.M.; Rasmussen, E.M.; Porvaznik, I.; Skerenova, M.; et al. Whole Genome Sequencing of Multidrug-Resistant Mycobacterium Tuberculosis Isolates Collected in the Czech Republic, 2005-2020. SCIENTIFIC REPORTS 2022, 12. [Google Scholar] [CrossRef]
- de Vos, M.; Scott, L.; David, A.; Trollip Andre and Hoffmann, H.; Georghiou, S.; Carmona, S.; Ruhwald, M.; Stevens, W.; Denkinger, C.M.; Schumacher, S.G. Comparative Analytical Evaluation of Four Centralized Platforms for the Detection of Mycobacterium Tuberculosis Complex and Resistance to Rifampicin and Isoniazid. JOURNAL OF CLINICAL MICROBIOLOGY 2021, 59. [Google Scholar] [CrossRef]
- Kohli, M.; MacLean, E.; Pai, M.; Schumacher, S.G.; Denkinger, C.M. Diagnostic Accuracy of Centralised Assays for TB Detection and Detection of Resistance to Rifampicin and Isoniazid: A Systematic Review and Meta-Analysis. The European respiratory journal 2021, 57. [Google Scholar] [CrossRef]
- Liu, P.; Wang, X.; Liang, J.; Dong, Q.; Zhang, J.; Liu, D.; Wang, S.; Bi, J.; Liu, W.; Wang, Z.; et al. A Recombinase Polymerase Amplification-Coupled Cas12a Mutant-Based Module for Efficient Detection of Streptomycin-Resistant Mutations in Mycobacterium Tuberculosis. FRONTIERS IN MICROBIOLOGY 2022, 12. [Google Scholar] [CrossRef]
- Moreno-Molina, M.; Shubladze, N.; Khurtsilava, I.; Avaliani, Z.; Bablishvili, N.; Torres-Puente, M.; Villamayor, L.; Gabrielian, A.; Rosenthal, A.; Vilaplana, C.; et al. Genomic Analyses of Mycobacterium Tuberculosis from Human Lung Resections Reveal a High Frequency of Polyclonal Infections. Nat Commun 2021, 12, 2716. [Google Scholar] [CrossRef]
- Folkvardsen, D.B.; Thomsen, V.Ø.; Rigouts, L.; Rasmussen, E.M.; Bang, D.; Bernaerts, G.; Werngren, J.; Toro, J.C.; Hoffner, S.; Hillemann, D.; et al. Rifampin Heteroresistance in Mycobacterium Tuberculosis Cultures as Detected by Phenotypic and Genotypic Drug Susceptibility Test Methods. J Clin Microbiol 2013, 51, 4220–4222. [Google Scholar] [CrossRef] [PubMed]
- Andersson, D.I.; Nicoloff, H.; Hjort, K. Mechanisms and Clinical Relevance of Bacterial Heteroresistance. Nat Rev Microbiol 2019, 17, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Ye, M.; Yuan, W.; Molaeipour, L.; Azizian, K.; Ahmadi, A.; Kouhsari, E. Antibiotic Heteroresistance in Mycobacterium Tuberculosis Isolates: A Systematic Review and Meta-Analysis. ANNALS OF CLINICAL MICROBIOLOGY AND ANTIMICROBIALS 2021, 20. [Google Scholar] [CrossRef] [PubMed]
- Van Deun, A.; Barrera, L.; Bastian, I.; Fattorini, L.; Hoffmann, H.; Kam, K.M.; Rigouts, L.; Rüsch-Gerdes, S.; Wright, A. Mycobacterium Tuberculosis Strains with Highly Discordant Rifampin Susceptibility Test Results. J Clin Microbiol 2009, 47, 3501–3506. [Google Scholar] [CrossRef] [PubMed]
- Van Deun, A.; Aung, K.J.M.; Bola, V.; Lebeke, R.; Hossain, M.A.; de Rijk, W.B.; Rigouts, L.; Gumusboga, A.; Torrea, G.; de Jong, B.C. Rifampin Drug Resistance Tests for Tuberculosis: Challenging the Gold Standard. J Clin Microbiol 2013, 51, 2633–2640. [Google Scholar] [CrossRef]
- Siu, G.K.H.; Zhang, Y.; Lau, T.C.K.; Lau, R.W.T.; Ho, P.-L.; Yew, W.-W.; Tsui, S.K.W.; Cheng, V.C.C.; Yuen, K.-Y.; Yam, W.-C. Mutations Outside the Rifampicin Resistance-Determining Region Associated with Rifampicin Resistance in Mycobacterium Tuberculosis. Journal of Antimicrobial Chemotherapy 2011, 66, 730–733. [Google Scholar] [CrossRef]
- Chakravorty, S.; Simmons, A.M.; Rowneki, M.; Parmar, H.; Cao, Y.; Ryan, J.; Banada, P.P.; Deshpande, S.; Shenai, S.; Gall, A.; et al. The New Xpert MTB/RIF Ultra: Improving Detection of Mycobacterium Tuberculosis and Resistance to Rifampin in an Assay Suitable for Point-of-Care Testing. mBio 2017, 8, e00812–17. [Google Scholar] [CrossRef]
- Shea, J.; Halse, T.A.; Kohlerschmidt, D.; Lapierre, P.; Modestil, H.A.; Kearns, C.H.; Dworkin, F.F.; Rakeman, J.L.; Escuyer, V.; Musser, K.A. Low-Level Rifampin Resistance and rpoB Mutations in Mycobacterium Tuberculosis: An Analysis of Whole-Genome Sequencing and Drug Susceptibility Test Data in New York. Journal of clinical microbiology 2021, 59. [Google Scholar] [CrossRef] [PubMed]
- Nonghanphithak, D.; Kaewprasert, O.; Chaiyachat, P.; Reechaipichitkul, W.; Chaiprasert, A.; Faksri, K. Whole-Genome Sequence Analysis and Comparisons between Drug-Resistance Mutations and Minimum Inhibitory Concentrations of Mycobacterium Tuberculosis Isolates Causing M/XDR-TB. PloS one 2020, 15, e0244829. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.; Marras, S.A.E.; Kurepina, N.; Chauhan, V.; Shashkina, E.; Kreiswirth, B.; Varma-Basil, M.; Vinnard, C.; Subbian, S. Ultrasensitive Detection of Multidrug-Resistant Mycobacterium Tuberculosis Using SuperSelective Primer-Based Real-Time PCR Assays. INTERNATIONAL JOURNAL OF MOLECULAR SCIENCES 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Tamilzhalagan, S.; Shanmugam, S.; Selvaraj, A.; Suba, S.; Suganthi, C.; Moonan, P.K.; Surie, D.; Sathyanarayanan, M.K.; Gomathi, N.S.; Jayabal, L.; et al. Whole-Genome Sequencing to Identify Missed Rifampicin and Isoniazid Resistance Among Tuberculosis Isolates-Chennai, India, 2013-2016. Frontiers in microbiology 2021, 12, 720436. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, S.H.; Rüsch-Gerdes, S. MGIT Procedure Manual 2006.
- Werngren, J.; Mansjo, M.; Glader, M.; Hoffner Sven and Forsman, L.D. Detection of Pyrazinamide Heteroresistance in Mycobacterium Tuberculosis. ANTIMICROBIAL AGENTS AND CHEMOTHERAPY 2021, 65. [Google Scholar] [CrossRef] [PubMed]
- Nasiri, M.J.; Fardsanei, F.; Arshadi, M.; Deihim, B.; Khalili, F.; Dadashi, M.; Goudarzi, M.; Mirsaeidi, M. Performance of Wayne Assay for Detection of Pyrazinamide Resistance in Mycobacterium Tuberculosis: A Meta-Analysis Study. NEW MICROBES AND NEW INFECTIONS 2021, 42. [Google Scholar] [CrossRef]
- Whitfield, M.G.; Engelthaler, D.M.; Allender, C.; Folkerts, M.; Heupink, T.H.; Limberis, J.; Warren, R.M.; Van Rie, A.; Metcalfe, J.Z. Comparative Performance of Genomic Methods for the Detection of Pyrazinamide Resistance and Heteroresistance in Mycobacterium Tuberculosis. Journal of clinical microbiology 2022, 60, e0190721. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Liu, R.; Yao, C.; Huo, F.; Shang, Y.; Zhang, X.; Wang, Y.; Xue, Z.; Ma, L.; Pang, Y. Reevaluating Rifampicin Breakpoint Concentrations for Mycobacterium Tuberculosis Isolates with Disputed rpoB Mutations and Discordant Susceptibility Phenotypes. MICROBIOLOGY SPECTRUM 2022, 10. [Google Scholar] [CrossRef]
- Veziris, N.; Bonnet, I.; Morel, F.; Guglielmetti, L.; Maitre, T.; Fournier Le Ray, L.; Sougakoff, W.; Robert, J.; Aubry, A. Impact of the Revised Definition of Extensively Drug-Resistant Tuberculosis. The European respiratory journal 2021, 58. [Google Scholar] [CrossRef]
- Tiberi, S.; Utjesanovic, N.; Galvin, J.; Centis, R.; D’Ambrosio, L.; van den Boom, M.; Zumla, A.; Migliori, G.B. Drug Resistant TB - Latest Developments in Epidemiology, Diagnostics and Management. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases 2022. [CrossRef]
Figure 1.
Flowchart of the search strategy, exclusion and selection of studies in this narrative review. WoS: Web of Science; MTB: Mycobacterium tuberculosis.
Figure 1.
Flowchart of the search strategy, exclusion and selection of studies in this narrative review. WoS: Web of Science; MTB: Mycobacterium tuberculosis.
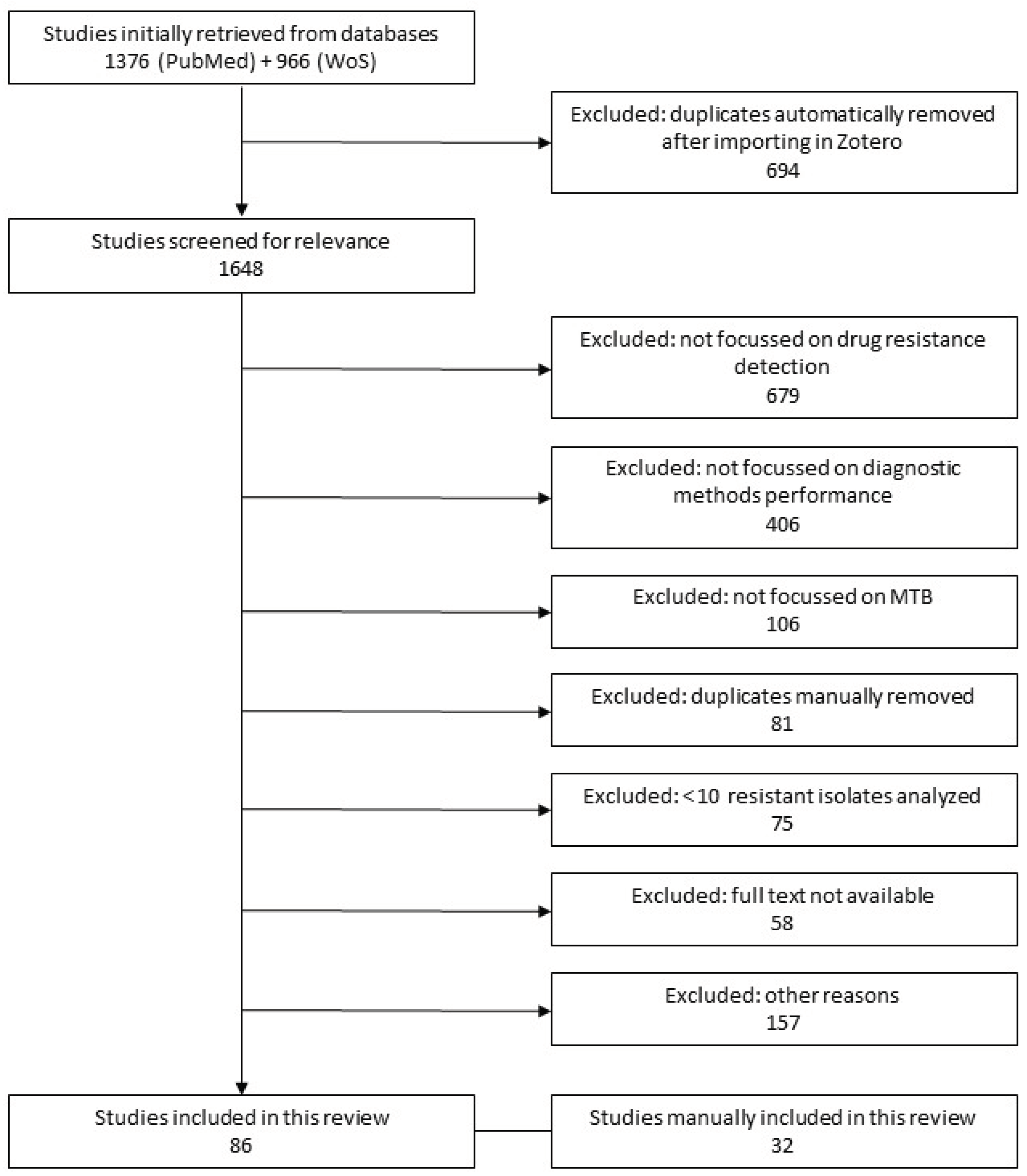

Table 1.
Overview of the diagnostic methods to detect drug resistance in Mycobacterium tuberculosis investigated in this review.
Table 1.
Overview of the diagnostic methods to detect drug resistance in Mycobacterium tuberculosis investigated in this review.
| Method |
Direct/ Indirect1 |
TAT2 | Features | Review section | Ref. | |
| Pros | Cons | |||||
| Phenotypic methods | ||||||
| Mycobacteria Growth Indicator Tube (MGIT) | Direct for ID, indirect for DST | 14-28 days | MTB ID and DST3 Multiple drug testing Customisable4 |
Not rapid Not easy to use5 MIC determination Semiautomated |
3.1.1 | [17,18] |
|
Sensititre MYCOTB |
Indirect | 7-21 days | Multiple drug testing MIC determination |
MTB ID and DST Not customizable Not rapid Not easy to use Semiautomated |
3.1.2 | [19] |
|
Colorimetric assays |
Indirect | 8-9 days | Multiple drug testing Customisable Easy to use Costs Little equipment required |
MTB ID and DST MIC determination Manual Low accuracy/sensitivity Needs standardization Subjective interpretation Limited throughput |
3.1.3 | [20,21] |
| Thin-layer agar (TLA) | Direct | 18 days | Multiple drug testing Customisable Rapid Easy to use Costs Little equipment required |
MTB ID and DST MIC determination Manual Need standardization Low accuracy/sensitivity Subjective interpretation Limited throughput |
3.1.4 | [22,23] |
| Direct microscopy- based slide DST (SDST) | Direct | 14 days | Multiple drug testing Customisable Rapid Easy to use Costs Little equipment required |
MTB ID and DST MIC determination Manual Need standardization Low accuracy/sensitivity Subjective interpretation Limited throughput |
3.1.5 | [24] |
| In-house flow cytometry | Indirect | 1 day | Multiple drug testing Customisable Rapid |
MTB ID and DST MIC determination Semiautomated Need standardization Extensive equipment required |
3.1.5 | [25] |
| Molecular methods | ||||||
|
GeneXpert technology |
Direct | <2 hours | MTB ID and DST Multiple drug testing Easy to use Automated Interpretation standardized |
Not customisable |
3.2.1 | [26,27,28,29,30,31,32,33,34,35,36] |
| GenoType MTBDRplus and MTBDRsl | Direct/ indirect |
1-3 days | MTB ID and DST Multiple drug testing Easy to use |
Not customisable Semiautomated Low accuracy on direct samples |
3.2.2 | [37,38,39,40,41,42,43,44,45,46] |
| BD MAX MDRTB | Direct | 4 hours | MTB ID and DST Multiple drug testing Easy to use Automated Interpretation standardized Medium throughput |
Not customisable |
3.2.3 | [47] |
|
Sequencing technology |
Direct/ indirect |
MTB ID and DST Multiple drug testing High throughput Data can be reanalysed Detect all genes |
Semiautomated Not easy to use |
3.2.4 and Table 2 |
3.2.4 and Table 2 |
|
| In-house PCR-ELISA Microplate Hybridization | Indirect | 4-5 hours | Multiple drug testing Customisable Easy to use Costs Little equipment required |
MTB ID and DST Manual |
3.2.5 | [48] |
|
In-house QuantaMatrix Multiplexed |
Indirect | 6 hours | FLD and SLD testing |
MTB ID and DST Not easy to use Semiautomated |
3.2.5 | [49] |
|
In-house target amplicon sequencing (TBNGS) |
Direct | 6 days | High throughput Rapid Multiple drug testing |
MTB ID and DST Not easy to use Not customisable Semiautomated |
3.2.5 | [50] |
| TB MDR and XDRA | Direct/ indirect |
3 hours | MTB ID and DST Multiple drug testing Easy to use Automated |
Not customisable |
3.2.6 | [51] |
|
DNA Microarray |
Indirect | 6 hours | MTB ID and DST Costs Multiple drug testing High throughput |
Not customisable Not easy to use Semi-automated |
3.2.6 | [52] |
| RIF-RDp, LNA probes and HRM analysis | Direct/ indirect |
2.2 hours | Costs |
MTB ID and DST Test only for RIF Semiautomated Not easy to use |
3.2.6 | [53] |
| MagPlex microspherebased multianalyte profiling | Indirect | 5 hours | Multiple drug testing Customisable |
MTB ID and DST Semiautomated Not easy to use Extensive equipment required |
3.2.6 | [54] |
| Truenat MTB-RIF Dx | Direct | <2 hours | MTB ID and DST Easy to use Portability Rapid Automated Can work at > 40°C and > 80% humidity, field work |
Not customisable Test only for RIF |
3.2.6 | [55] |
| Other methods | ||||||
| Biosensor | Indirect | <2 hours | Easy to use Multiple drug testing Costs Rapid Automated Low sample volume required |
MTB ID and DST Not customisable |
3.3.1 | [56] |
| Lab on chip | Direct | 3 hours | MTB ID and DST Easy to use Rapid Automated Portability/Compact size Low sample volume required |
3.3.2 | [57,58] | |
| MALDI-TOF mass spectrometry | Direct/ indirect |
1 day | MTB ID and DST Multiple drug testing Easy to use High throughput Customisable |
Need standardisation for resistance detection Semiautomated |
3.3.3 | [59,60,61] |
| SERS | Indirect | Not provided | Multiple drug testing Label-free Minimal sample preparation |
Difficult spectra interpretation | 3.3.4 | [62] |
1 Direct on clinical samples or indirect on an isolated culture (cultures must be incubated in a biosafety level 3 laboratory). 2 Not considering the time to obtain a culture. 3 Means whether the method can perform simultaneously MTB ID and DST. 4 Means the ability to update or modify the method to include new drugs or new resistance-associated mutations to be tested. 5 Means whether the method requires specialized personnel and/or extensive training. DST: drug susceptibility test; FLD: first-line drugs; HRM: high-resolution melting; ID: identification; LNA: locked nucleic acid; MALDI-TOF: Matrix-assisted laser desorption ionization time-of-flight; MIC: minimum inhibitory concentration; MTB: Mycobacterium tuberculosis; RIF: Rifampicin; SERS: surface-enhanced Raman spectroscopy; SLD: second-line drugs; TAT: turnaround time.
Table 2.
Overview of the studies included in this narrative review which compared sequencing with pDST.
Table 2.
Overview of the studies included in this narrative review which compared sequencing with pDST.
|
Sequencing technology |
Direct/ Indirect 1 |
Origin, no. and type of isolates | Major Diagnostic performance 2 | Additional comments 3 | Reference | ||
|
WGS Illumina HiSeq |
Indirect | China 4880 MTB |
Sensitivity RIF 96.7%, INH 94.2%, EMB 92.9% PZA 50.5% |
Specificity INH 98.9% RIF 98.8% EMB 98.1% PZA 99.2% |
Several EMB resistance mutations fell within the sub-epidemiological cutoff range and therefore were missed by pDST methods. Expected low sensitivity for PZA detection as MGIT test often yields false-positive results for PZA resistance |
[89] | |
|
WGS Illumina NextSeq 500 |
Indirect | Tanzania 42 RR/MDR-TB |
Overall agreement RIF 95% INH 81% EMB 57% SM 81% |
pDST detected resistances to FQ (6 cases), Clofazimine (1 case), and Cycloserine (1 case) not identified by WGS. Discrepancies arose from unclear MIC breakpoints, limited knowledge of resistance mutations for these drugs and an unsuitable 5% cutoff for resistance variants in WGS. |
[90] | ||
|
WGS Illumina HiSeq |
Indirect | China Russia 215 MTB |
Sensitivity RIF 79.7%, INH 86.3%, EMB 76.5%, SM 88.4%, OFL 83.3%, AMK 70.0% CAP 70.0% |
The best mutation combination to predict MDR-TB was rpoB S450L + rpoB H445A/P + katG S315T + inhA I21T + inhA S94A | [91] | ||
|
WGS Illumina HiSeq |
Indirect | China 59 RR-TB |
Sensitivity RIF 100% INH 95.9% EMB 100% SM 97.3% LEV 100% AMK 75.0% CAP 80.0% |
Specificity RIF - INH 90.0% EMB 64.1% SM 100% LEV 97.2% AMK 100% CAP 96.3% |
The low specificity for EMB could be due to the unreliability of pDST for EMB resistance | [92] | |
|
Sanger |
Indirect | Ethiopia 209 MTB |
Overall agreement RIF 95.2% INH 93.8% EMB 99.0% PZA 94.7% SM 78.9% |
pDST plus Sanger sequencing of selected genes is a reliable approach in Ethiopia | [93] | ||
|
WGS Illumina HiSeq |
Indirect | Indonesia 30 MTB | Overall agreement RIF 93.3% INH 76.6% EMB 63.3% SM 83.3% OFL 76.7% |
WGS detected 15 EMB-resistant isolates compared to 5 by pDST, with the discrepancy attributed to a high breakpoint (5 µg/ml) for EMB testing. WGS found five OFL-resistant isolates, while MGIT found 12. Discrepancy attributed to the CC of 2 µg/ml or a limited FQ-mutation database |
[94] | ||
|
WGS Illumina MiSeq |
Indirect | Belgium 306 MTB |
Sensitivity RIF 100 % INH 90.5 % EMB 100 % PZA 61.1 % |
Specificity >98.0% in all four FLDs. | pDST identified 14 PZA-resistant isolates not detected by WGS, possibly due to undetected resistance mutations in the pncA gene promoter. | [95] | |
|
WGS Ion Torrent |
Indirect | Sweden 1248 MTB |
Sensitivity RIF 100% INH 93.5% EMB 90.0% PZA 92.2% OFL 100% MOX 100% KAN 100% CAP 100% ETH 57.1% |
Specificity RIF 99.5% INH 100% EMB 98.8% PZA 100% OFL 100% MOX 92.5% KAN 100% CAP 100% ETH 89.6% |
An in-house mutation catalogue was used for molecular DST | [96] | |
|
Targeted NGS Ion Torrent |
Indirect | Taiwan 35 MTB |
Sensitivity RIF 100% INH 100% EMB 92.9% PZA 100% SM 100% MOX 100% LEV 92.9% |
Specificity RIF 100% INH 100% EMB 93.8% PZA 100% SM 100% MOX 100% LEV 100% |
One of the few studies where isolates resistant to BDQ (n=2) and LZD (n=2) were analysed | [97] | |
|
Oxford Nanopore MinION |
Indirect/ Direct |
US 431 DNA extracts |
Sensitivity: RIF 100% INH 91% EMB 80% PZA 76% SM 78% AMI 50% KAN 100% FQ 40% ETH 42% |
Specificity: RIF 98% INH 100% EMB 100% PZA 97% SM 93% AMI 100% KAN 98% FQ 100% ETH 97% |
DNA was extracted from early-positive (2-4 days) MGIT cultures. The approach could be considered between direct and indirect. Low sensitivities might be caused by the small number of resistant isolates |
[98] | |
| DNA-enrichment-based WGS Illumina | Direct | India 52 sputum samples |
Sensitivity: RIF 100% INH 100% KAN 100% AMK 100% FQ 100% ETH 93.3% |
Specificity RIF 92.3% INH 100% KAN 100% AMK 100% FQ 95.0% ETH 93.3% |
The authors did not test smear-negative samples. The authors did not compare WGS results for EMB, PZA, LZD or BDQ |
[99] | |
|
Targeted NGS Oxford Nanopore MinION |
Direct | Italy 104 DNA extracts |
100% concordance for RIF, INH, PZA, EMB, SM and CAP resistance between MinION and Illumina MiSeq with minimum coverage variant thresholds of 40X | DNA was extracted from smear-positive sputum sediments previously sequenced with Illumina MiniSeq. The TAT was 3 days |
[80] | ||
|
Targeted sequencing Deeplex-MycTB |
Direct | Germany 50 clinical samples | Overall agreement: RIF 97.4% INH 94.9% EMB 97.4% PZA 97.4% ETH/PTH 75.0% |
In 11 samples the sequencing failed (seven of which were smear negatives) | [86] | ||
| Sanger | Indirect | China 152 MDR-TB |
Sensitivity and specificity for PZA resistance detection were 89.5% and 89.4% considering only pncA | Considering the genes pncA, rpsA, and panD, the sensitivity increased to 92.4% while the specificity remained the same | [100] | ||
1 Dierct on clinical samples or indirect on an isolated culture. 2 As compared to a reference method, often a pDST. 3 These could be study limitations, general observations or conclusions, other key findings, discrepancies explanations or additional remarks. AMK: Amikacin; BDQ: Bedaquiline; CAP: Capreomycin; CC: Critical Concentration; DST: Drug Susceptibility Test; EMB: Ethambutol; ETH: Ethionamide; FLD: First-line drugs; FQ: Fluoroquinolones; INH: Isoniazid; KAN: Kanamycin; LEV: Levofloxacin; MDR-TB: Multidrug-resistant tuberculosis; MOX: Moxifloxacin; OFL: Ofloxacin; PTH: Prothionamide; PZA: Pyrazinamide; RIF: Rifampicin; RR-TB: Rifampicin-resistant tuberculosis; SLD: Second-line drugs; SM: Streptomycin; WGS: Whole genome sequencing.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



