
Submitted:
20 February 2024
Posted:
21 February 2024
You are already at the latest version
Abstract
Cardiovascular disease (CVD) is the leading cause of death worldwide. Cardiac rehabilitation (CR) has proven to be effective in reducing the rate of recurrence and disease as secondary prevention (evidence-based intervention) in patients who have suffered from myocardial infarction (MI). CR is a multidisciplinary path in which the patient is followed pharmacologically, from a psychological, nutritional, nursing and physiotherapy point of view. Post-MI patients present a reduction in the performance of the diaphragm muscle, the main inspiratory muscle, and this condition can become a risk factor for further relapses or for the onset of heart failure. Despite the solidity of the international guidelines for CR, the latter are lacking in specifically indicating an evaluation and training path regarding the inspiratory muscles in post-MI patients who have not undergone cardiac surgery. The article reviews the information on the adaptation of the diaphragm post-MI and highlights the need for clearer indications for a rehabilitation process that gives importance to the diaphragm.
Keywords:
Myocardial infarction
; diaphragm
; cardiovascular disease
; physiotherapy
; rehabilitation
; cardiac rehabilitation
Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide [1]. The number of patients with CVD has nearly doubled over a 31-year period (1990, 271 million; 2019, 523 million), with the number of deaths increasing from 12.1 million (1990) to 18.6 million (2019) [1]. Ischemic heart disease (IHD) encompasses cardiovascular events such as acute myocardial infarction (MI), chronic stable angina and chronic IHD, heart failure caused by IHD [1]. IHD stands at 49.2% of all deaths in 2019, with a higher disease propensity in men than women, and a higher mortality rate for men [1,2].
IHD (and stroke) are the most important causes of mortality and illness from premature cardiovascular disease (pCVD). In 2019, the percentage of deaths from pCVD for men per 100,000 people was 22.7%, while for women it was 8.9% [2]. Risk factors involve metabolic and behavioral factors (diabetes, obesity), as well as environmental causes (air pollution, non-optimal temperatures) [2]. IHD was considered a fatal event related to more developed countries, while the most recent data show heterogeneity at a global level [3].
In the 80s and 90s there was a reduction in the occurrence of myocardial infarction, while with the most updated data, it seems that this cardiac event has reached a plateau, without further decline [3]. Probably, the use of the Universal Definition of Myocardial Infarction (UDMI) which has expanded and better-defined cardiac damage caused by the absence of oxygen, has considered pathological events not included in the past decades [3]. Currently, the fourth UDMI divides myocardial damage or MI as follows: the infarction is defined by the presence of cardiac troponin (cTn) 99th percentile upper reference limit and can be acute (depending on variations in cTn), or chronic (≤20 % of cTn values) [4,5]. MI can be encountered as a spontaneous or peri-procedural event, with patients having CVD or non-CVD. MI caused by acute coronary stenosis in the presence of plaque/thrombus or type 1; Type 2 MI when the heart's demand for oxygen does not meet an adequate quantity of oxygen transported during stress (motor, emotional), regardless of the presence or absence of plaque/thrombus [4,5]. When a cardiac patient dies with alteration of the electrocardiogram, in the absence of blood tests, it is defined as type 3 MI. Type 4a MI when the event occurs during a percutaneous coronary intervention procedure, type 4b MI when the event ischemic is caused by an in-stent thrombus, and MI type 4c caused by a recurrence of stenosis or restenosis. Finally, type 5 MI includes ischemia after coronary artery bypass grafting surgery, with cTn value values greater than 10 times the 99th percentile upper reference limit and during the first two days after surgery. Furthermore, type 5 MI must be diagnosed with instrumental tests, such as angiography or echocardiography [4,5].
Other authors point out the need to further improve the definitions emerging from the fourth UDMI; the classification of type 2 MI may be inadequately specific from a phenotypic point of view, or too complex to apply for a clinical setting [6,7].
The article reviews (narrative review) the information on the adaptation of the diaphragm post-MI and highlights the need for clearer indications for a rehabilitation process that gives importance to the diaphragm.
Rehabilitation after MI
Cardiac rehabilitation (CR) as secondary prevention (evidence-based intervention) in patients who have undergone MI has proven effective in reducing the rate of relapse and disease [8,9]. CR is a multidisciplinary path in which the patient is followed pharmacologically, from a psychological, nutritional, nursing and physiotherapy point of view [9].
The rehabilitation approach is always individualized and based on the clinician's assessment; the start of CR for patients with MI can occur as early as one week after the acute event [9]. There is no single recommendation for the duration of CR. Generally, looking at recent literature, the average duration is 8 weeks, with a weekly frequency of 2.5 days [10]. The pillar of CR is physical exercise [8,9]. The rapid onset of CR allows for an improvement in left ventricular remodeling (increases the percentage of ejection frequencies), with increases in cardiopulmonary performance [9].
Theoretically, through the pursuit of CR the patient can implement on average the capacity for exercise tolerance from 6.5 to 7.5 metabolic equivalents of task or METs, values measured with cardiopulmonary testing; one MET is 3.5 ml O2/kg/min or at 1 Kcal/kg/h [11]. Each gain of one MET corresponds to a decline in causes of mortality of 8-26% [12]. CR can be divided into phase I (inpatient), phase II (outpatient setting), phase III and IV, where the patient follows a training course regardless of the presence of healthcare personnel [13].
For phase II, the literature recommends following an aerobic workout, using stationary bikes and/or free body exercises, combining resistance training with exercises with machines or resistances to be lifted. Aerobic work should be moderate to intense, for a minimum of thirty minutes and three sessions per week [14]. This allows us to improve cardiac metabolism and cardiac perfusion, with benefits to the endothelial structure and function of the microvascular system; positively changes blood viscosity with antithrombotic effects [14]. Aerobic training could be organized as high-intensity interval (HIIT), for more delicate patients (bedridden, advanced age, reduced ejection frequency); the benefits are like continued training with less delicate patients [15]. Moderate-intense exercise is aerobic work between 60% and 85% of maximum heart rate or corresponding to a Rating of Perceived Exertion (RPE) value of 12-14 [16]. HIIT is cardiac work that reflects a maximum heart rate of 85-95% or an RPE of 15-17, lasting 30 seconds up to 5 minutes; each set of HIIT is followed by 1-3 minutes of moderate aerobic work (60-85%) [16]. Anaerobic activity should be integrated during the week with aerobic training. The clinician should plan two-three weekly sessions for the patient to involve the major muscle groups or according to the person's work or sporting needs. Sets should be between 1-3, with 10-15 repetitions and a lifting intensity that reflects 30-80% of the patient's one-repetition maximum (1RM), and an RPE that corresponds to 11-13 [16]. More specifically, for the upper limb muscles the load should be between 30-70% of 1RM, while for the lower limb muscles the expected load should be 40-80% of 1RM [17].
The progression of aerobic and anaerobic workloads must be progressive and subjective [16]. The parameters to be used to implement intensity should be based on frequency, duration, amount of work and type of exercise [17]. Furthermore, the amount of CR energy expenditure carried out by the patient during the week should be around 1000–2000 kcal [17].
Currently, heterogeneity persists in the different CR centers, despite the current literature [18]. Furthermore, disparities in the use of CR are reported. The possibility of returning to work after an MI and after 8 weeks of rehabilitation mainly involves males (78.9%), compared to women [14]. Patients with a body mass index (BMI) of ≥ 25 kg/m2 appear to demonstrate better cardiovascular improvements; furthermore, patients with a lower capacity to sustain physical exercise demonstrate greater improvements compared to more conditioned people [14]. CR is like a drug, with systemic and local effects, and considering the chronicity of the disease, physical activity should be carried out throughout the patient's life.
Adherence
The literature demonstrates low adherence of patients with MI and CR (35% in the US, 30% in European countries) [9]. It is estimated that in the most economically developed countries, only three people out of 66 ischemic events access CR, while in the least economically developed countries, only 1 person out of 66 patients with MI follow a CR regimen [19]. The reasons for low adherence include factors such as advanced age, low educational and economic status, decline in motor and cognitive functions; difficulty accessing rehabilitation centers (distance or lack of means of transport), female patients, the presence of multiple comorbidities, smoking [20]. Furthermore, a lack of information or encouragement to participate in CR from the clinician can limit access to rehabilitation [19]. CR is not able to express all the preventive potential for low adherence, even though rehabilitation is considered by international guidelines as Level 1A [17,20].
Among the reasons that must be included to understand low adherence, there are the relative and absolute contraindications that the clinician must follow. Absolute contraindications (unstable angina, dyspnea on exertion and at rest, etc.) do not allow the patient to follow CR [21]. CR can be performed on patients with a stable clinical picture, and not all patients who have undergone MI can access rehabilitation immediately or in the long term. Probably, the unfavorable clinical situation can discourage the patient from accessing CR, even if safe clinical stabilization could occur after a long period of time.
To improve
In the most recent recommendations for CR, as in the guidelines of the European Association of Preventive Cardiology, the American College of Cardiology and American Heart Association, no specific indications appear for patients with MI which reflect the different classifications of the fourth UDMI [17,22]. Furthermore, a deficiency to point out in these guidelines, which is the focus of the article, concerns the absence of rehabilitation indications involving the respiratory muscles and, in particular, the diaphragm muscle [9].
Non-conservative cardiology and diaphragm
In clinical practice it is not usual to evaluate the diaphragmatic status in clinical and rehabilitation settings [24]. We know that an invasive approach in the cardiovascular field can cause paresis, temporary or permanent. Paresis or simple diaphragmatic weakness can be found following atrial fibrillation ablation, with a rate of 0.37-1.6%; phrenic nerve injury could be caused by electrical or thermal damage, especially the right nerve [25]. Women have a greater risk of damaging the right phrenic nerve during ablation (anatomical positional reasons of the nerve), the recovery of which for both sexes can vary from three months to over a year [26]. A phrenic injury can occur with the placement of a cardiac implantable electronic device for different reasons, such as phrenic compression due to hematoma formation, contact of the nerve with anesthesia, indirect contact with the nerve (venous wall and a rigid catheter), or the presence of anatomical alterations [27,28]. The detection rate of diaphragmatic injury is very low 0.63% and transient [28].
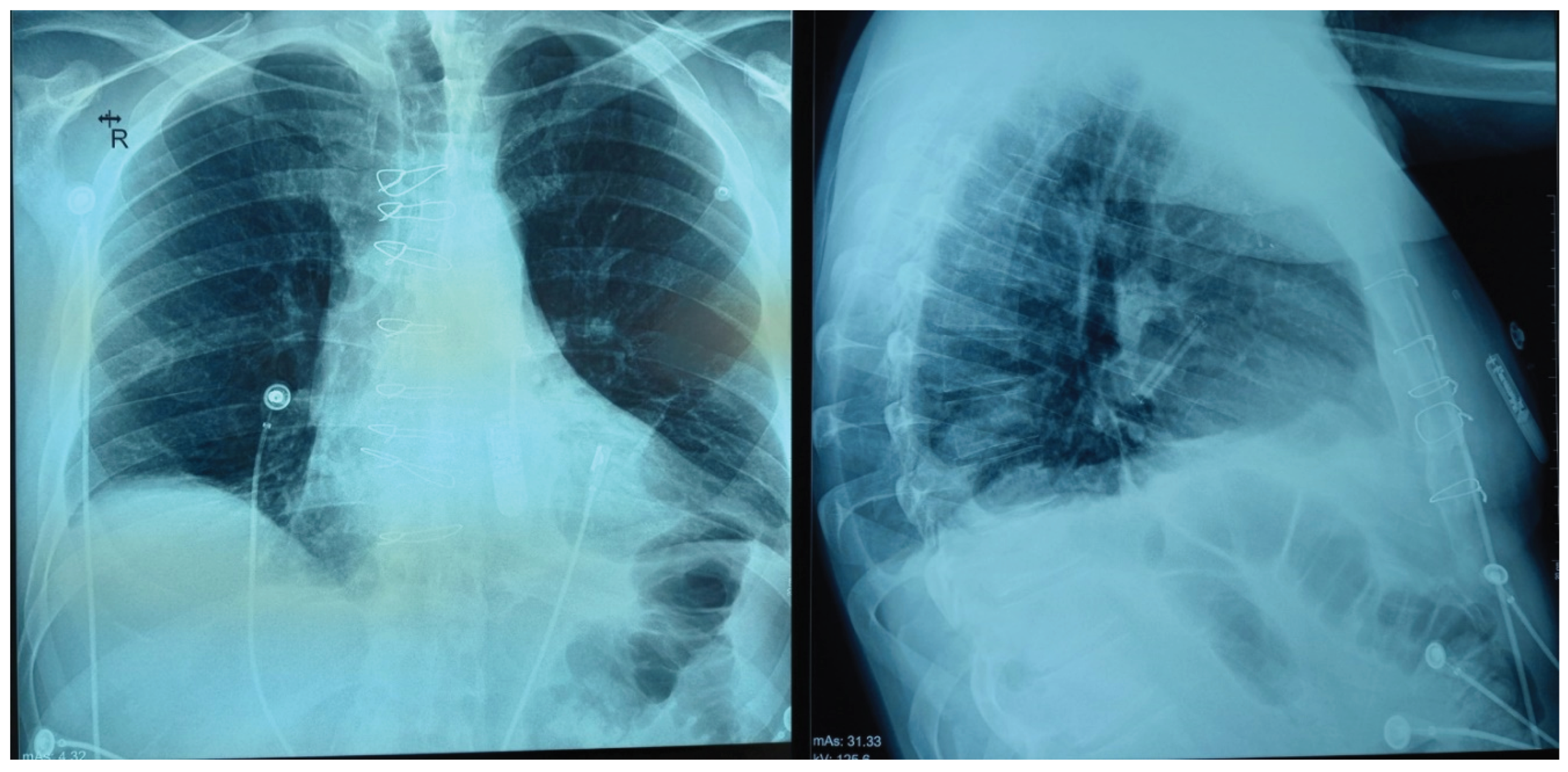
The negative involvement of diaphragmatic function after thoracic cardiac surgery has a higher percentage, with a maximum value of 60% of patients undergoing surgery [29]. This condition is often underestimated by the clinician [29]. Generally, it is the left phrenic nerve that is subject to greater risk of damage, compared to the right phrenic nerve, with recovery between six and twenty-four months after surgery [30,31]. The resulting elevation can be unilateral or bilateral (see Figure 1). An interesting fact that emerged from a study with a follow-up of 131 months with 23 cardiac surgery patients is that 26% worsened after a transient improvement in diaphragmatic function [31].
We have no data on the adaptation of the vagus nerve in the crural portion of the diaphragm after an invasive cardiac approach. Recall that the vagus nerve innervates the diaphragmatic muscular area of the esophageal hiatus [32]. We have no data on the possible direct relationship between left ventricular function and diaphragm function.
MI and diaphragm
Post-MI patients (and stable angina) have reduced muscular strength of the respiratory muscles, that is, a reduced ability to generate the correct thoracic pressures measurable through a forced inspiration against an occluded mouthpiece (maximal inspiratory pressure, MIP) [33]. MIP in addition to the diaphragm muscle, it also involves other muscles involved in inspiration. An average MIP of 80 cmH2O is considered a physiological value, while less than 80 cmH2O (for men) or less than 70 cmH2O (for women), is equivalent to respiratory dysfunction [33].
In post-MI animal model, the diaphragm undergoes atrophy and decline in contractile force and vascular alterations [34]. These adaptations occur within hours of the advent of MI and continue for many months [35]. The reasons are multiple. Proteolytic mechanisms such as the caspase pathway and the ubiquitin proteasome system (ubiquitin-ligase enzymes, muscle RING finger-1 and muscle atrophy F-box), carbonylation by oxidation of contractile proteins and cytoplasmic proteins are activated [34,35]. Within a few hours of MI, again on an animal model, the diaphragm loses 20% of its contractile capacity, which value remains for several months post-MI [35]. Further studies are necessary to know whether the adaptations on the animal model are the same or not on the human model.
This rapid adaptation could explain some symptoms reported by patients, such as dyspnea, fatigue, and exercise intolerance [35]. The ubiquitin proteasome system has a close relationship with the titin protein within the sarcomere, near the central I band, the Z disk and M band; the activation of proteolytic signals alter the organization and function of the sarcomere, making the diaphragm weaker [36]. Carbonylation negatively affects the myosin heavy chain (MHC) and actin, altering contractile expression, proteins within the mitochondrion (aconitase, creatine kinase) and within the cytoplasm (aldolase, enolase, carbonic anhydrase III, glyceraldehyde 3), making the diaphragm less resistant [37]. Oxidation stimulates the activation of nicotinamide adenine dinucleotide phosphate type 4 (NADPH oxidase-4 or NOX-4), which is found in the sarcoplasmic reticulum and mitochondria; NOX-4 impairs mitochondrial function and calcium release within the cytoplasm, contributing, in part, to diaphragmatic dysfunction [38]. It seems that the dysfunction particularly affects the IIb/x fibers or anaerobic fibers [38]. Oxidation is accentuated by the fact that there is an accumulation of iron within the fibers of the diaphragm and a concomitant decrease in the gene that synthesizes transferrin [34].
An explanation for this adaptation could be linked to the increase in inflammatory cytokines (tumor necrosis factor-alpha, interleukin-6, interleukin-1beta, angiotensin II) that flow from the heart into the blood circulation, which inflammatory information can involve the diaphragm, creating a deficient contractile environment [35]. IM creates a systemic inflammatory environment in the short and long term, with proteolysis and diaphragmatic oxidation [35].
In post-MI patients (and in animal models), a non-physiological adaptation of the diaphragm is therefore one of the important causes, in the short and long term, of fatigue, dyspnea, and impaired airway clearance [35,38]. In animal models, MI causes alterations in numerous genes that concern diaphragmatic function, of which 42 genes are increased and 70 genes are decreased [34]. In particular, the genes responsible for stabilizing the synaptic plate and the muscle fiber decreased, but not the growth factors such as brain-derived neurotrophic factors (BDNF). This could mean that there would not be neurodegenerative damage, but an environment that favors neuromuscular remodeling [34]. There is a decrease in the genes that regulate the organization of membrane proteins (sodium/potassium pump) and the release of calcium within the cytoplasm; the result is an alteration of membrane excitability, with relative contractile dysfunction [34].
Some genes that regulate certain extracellular matrix proteins, such as elastin, are decreased after MI, with a possible increase in stiffness and more fibrosis; this leads the muscle fiber to incorrectly manage mechanometabolic/mechanotransductive information [34]. Some proteins that allow the stabilization of the sarcomere, such as myomesin-2, and proteins involved in correct mechanotransduction, such as the myocardial zonula adherens protein or MYZAP, are downregulated. Furthermore, the contractile cell responds in a non-homogeneous manner with additional gene responses to try to maintain structural stability as much as possible during workloads [34]. Again, on an animal model, the genes that determine the metabolic response are in a precarious balance, that is, it seems that the muscle fibers are in a state of "anabolic resistance", with resistance to insulin. The cell does not appear to be in a metabolic context of atrophy but there appears to be difficulty in repairing the fiber in physiological times; a drag on the inflammatory status [34]. We know that after a MI, the sympathetic nervous system systemically increases [39]. The sympathetic nervous system increases its activity on the diaphragm after MI, probably to improve neurocoordination at the synaptic plate level [34,40].
The patient who undergoes post-MI CR has a dysfunctional diaphragm, and in this situation, a reduced respiratory work capacity could be one of the causes favoring the development of heart failure [35].
Diaphragm overload
The post-MI diaphragm appears to undergo work overload and resistance to anabolic signals [34]. Comparing the concept of overload to motor skeletal muscles in a sporting context, we could talk about overtraining syndrome (OTS), that is, the lack of time necessary for the restoration of muscle structure and function after the management of a powerful stressor [41]. There are convergences between OTS and post-MI diaphragmatic dysfunction. In the presence of OTS there is an increase in fibrosis of the extracellular matrix, a dysfunction of the neuromuscular junction, a mitochondrial dysfunction, an increase in oxidation phenomena, ultrastructural disorganization of the myofibrils [41]. The muscle seems to have to manage an inflammatory environment with an elevation of cytokines, which are not necessarily found in the muscle, but at a systemic level; there is a functional alteration of membrane proteins and the sarcoplasmic reticulum [41]. OTS presents chronic muscular structural adaptations, similarly as the post-MI diaphragm. Furthermore, OTS could create autonomic system dysfunction, as present in patients with MI [39,42].
The diaphragm is always under pressure. Let's consider that during a eupneic breath the diaphragm is involved for 70% compared to other respiratory accessory muscles; other skeletal muscles for motor actions are involved in a much smaller percentage, with loading and unloading cycles, such as 1% of the extensor digitorum longus muscle and 14% of the soleus muscle [36]. Furthermore, when we are standing and moving, a third of the diaphragm is removed from respiratory functions, as it is used for posture functions (intra-abdominal pressures) and to improve neuromotor function (parasympathetic stimulation) [43,44]. When the diaphragm is not functionally adequate, it can cause low back pain; this last symptom can be linked to the presence of coronary heart disease, even if the reasons are not fully clarified [45,46].
In conditions of post-MI-related diaphragmatic dysfunction, we can assume that the portion of the diaphragm involved in breathing is further reduced.
We might assume that a rehabilitation training for the diaphragm does not have to be intense and should be organized with adequate rest between sessions. Not taking post-MI diaphragmatic adaptation into account, a CR without adequate evaluation of the diaphragm and with demanding workloads probably risks obtaining unfavorable results for the patient.
The cardiopulmonary test does not evaluate diaphragm function
The international guidelines for RC give strong indications on the fact that, before undertaking a rehabilitation cycle, the patient must undergo a cardiopulmonary exercise test (CPET), measuring peak oxygen consumption (VO2peak), both for people who will follow a procedure in specialized centers and for physical activity carried out at home [17,47]. The test allows you to obtain data under stress; the objective is to identify a suitable CR path for each patient [9]. The values taken from the post-MI patient allow us to obtain data that can be prognostic [48]. Furthermore, the test is repeated at the end or halfway through the rehabilitation process to monitor the results obtained or to increase the training parameters, respectively. Typically, low exercise tolerance as assessed by CPET is predictive of a higher rate of cardiac recurrence, regardless of the type of surgical or conservative approach used to manage MI [48].
VO2peak is the result of cardiac output and peripheral tissue oxygen consumption. VO2peak varies based on different factors such as age, gender, clinical and sporting history, body mass index; the value may depend on the rheological parameters of the blood, the functional capacity of the cardiovascular system and the lungs [48]. Furthermore, it is not so simple to deduce parameters for prescribing the ideal aerobic intensity of a training process; with little value, however, for obtaining data to set up resistance training [17]. If there are no concomitant pathologies, a diaphragm in dysfunction but not paretic, does not affect CPET [49].
A tool that could be combined with CPET to have a greater information framework on diaphragmatic function is the use of electromyography for the diaphragm muscle (EMGdi). EMGdi during the test does not correctly distinguish the influence of other muscles, such as the scalene and external intercostal muscles [50].
To obtain parameters more representative of the post-MI diaphragmatic function
Considering that MI is the acute expression coming from chronic pathological adaptations, we do not know what happens to the diaphragm muscle before the infarction occurs. We have no data on the diaphragm in patients who are at risk of MI, excluding the presence of concomitant pathologies that may already have induced adaptations.
In the presence of risk factors for the onset of MI in a patient, the function of the diaphragm should be verified but, currently, we are not in the clinical habit of evaluating this muscle. A low MIP value is a risk factor for developing MI and one of the causes of mortality in cardiovascular diseases; in patients with chronic heart failure, it is a negative prognostic indicator of survival [24,33]. Over time, a low MIP value negatively impacts lung function [33].
Improving the function of the diaphragm and MIP muscle allows us to increase the survival rate in patients with cardiovascular diseases [33]. A properly functioning diaphragm positively influences cardiac function, decreasing the need for contractile force of the cardiac chambers during inhalation and exhalation: it improves and facilitates venous (and lymphatic) return; helps regulate left ventricular afterload; influences pericardial pressures; positively affects the heart rate rhythm (HRV); it is essential for regulating baroreceptor information [24].
There are many evaluations that can be carried out to try to understand the function of the diaphragm, both functional and imaging. In addition to the instrumentation that evaluates the MIP, there is the sniff test or sniff nasal inspiratory pressures (SNIP) which can be measured with a digital manovacuometer. From this instrumentation it is possible to calculate the values of the pressures generated by the diaphragm (force) at the gastric (sniff Pga), esophageal (sniff Poes) and transdiaphragmatic (sniff Pdi) levels [51]. There is no gold standard reference for comparing SNIP values but a diaphragm that is not in dysfunction could have values of 52-150 cmH2O for sniff Poes, values of 82-204 cmH2O for sniff Pdi and values of 68-62 cmH2O for sniff Pga [51,52].
Tests for electrical or magnetic stimulation of the phrenic nerve for the diaphragm can be used, evaluating the response at rest or under stress, but these approaches are not always easy to find in clinical practice [29,51,53]. Electromyography can be used during instrumental examinations to obtain additional information [51].
Instrumental tests to evaluate the image of the diaphragm, thickness, and movement that the clinician can use include fluoroscopy, magnetic resonance tomography, computed tomography, chest x-ray [53].
A simpler instrument that is more easily found in a rehabilitation context is ultrasound. On ultrasound examination the diaphragm appears as a thin hypo-echoic layer between two hyperechoic lines, which represent the peritoneal fascia and the pleura [29]. With an unforced breath and in the supine position, the right hemidiaphragm lowers by about 2 centimeters and with a thickness of about 22 millimeters on average (about 20 millimeters at the end of the exhalation), and with a total descent and ascent of approximately one and a half seconds for each breath (in total about 3 seconds for a eupnoeic breath) [29]. Typically, an unforced movement of the diaphragm below 1.5-2 centimeters could be considered as a muscle in dysfunction [29]. By averaging the thickness (thickening fraction, TF) between contraction and relaxation (inhalation and exhalation, respectively), it is possible to identify percentages of functionality. An average TF below 20% is most likely an indication of diaphragmatic paresis; a TF of approximately 20-36% could be a sign of a dysfunctional diaphragm [54]. The value of ultrasound measurements represents 93% of the sensitivity and 100% of the specificity in the detection of diaphragmatic problems [55]. Echocardiography could be used as a routine in the rehabilitation process to monitor the progress of thickness and function of the diaphragm muscle.
Spirometry is not of much value in establishing only diaphragmatic dysfunction, but rather frank lesions of the diaphragm. Weakness of the breathing muscles can lead to spirometric results that indicate a restrictive pattern; the FEV1-FVC ratio does not undergo large variations [55]. A value that could be indicative of respiratory muscle suffering is the decrease in forced vital capacity or FVC, but it remains a non-elective test to understand diaphragmatic dysfunction [56].
In the literature we can find some non-instrumental evaluation strategies, such as palpation of the different parts of the diaphragm and the related evaluation scale, and a motor test that the patient can carry out to understand if the diaphragm is correctly inserted in the neuromotor context [57,58,59].
Diaphragm muscle training
We do not have sufficient data to have gold standard indications on diaphragm muscle training in post-MI patients [17]. As we propose, other authors support the usefulness of a clinical assessment of the respiratory muscles before starting CR and adding specific exercises for the diaphragm (inspiratory muscle training, IMT) to the rehabilitation process in post-MI patients; these two strategies should be routine [33].
A study with post-MI patients (seems to be the only one in the literature), following a CR and training for the respiratory muscles (via devices with incremental resistances, based on the MIP percentage, with loads of 30-60%), compared to the group of patients who performed CR without IMT, had broader general performance parameters (METs, MIP, lower limb muscle strength) [60].
Some data show that patients undergoing cardiac surgery, following the addition of specific exercises for the respiratory muscles (not well specified), compared to just carrying out usual rehabilitation training, had improved functional parameters of the diaphragm. Thickness, contraction speed and range of motion increased, with a higher TF value [29]. Not all patients are able to adequately recover diaphragmatic contractile function, and this could negatively impact the success of CR [29]. IMT appears to have many beneficial effects even in patients with chronic heart failure (CHF). A recent study highlighted the actual usefulness of adding IMT (device with inspiratory resistance corresponding to 30% of the baseline subjective MIP) to the usual CR, compared to training alone without IMT: all the parameters measured at the start increased, such as the MIP, resting heart rate and better blood pressure values, heart rate reserve, higher score in health-related quality of life and in the Minnesota Living with Heart Failure Questionnaire [61].
We need to have further and larger studies to understand the real benefits with IMT in post-MI patients. We need to understand how to organize breathing training, such as the number of sessions per week, the number of repetitions and sets, as well as the total training time and breaks between sets, rest time between sessions and the other. We need to understand whether it is better to use an incremental load in inspiration using the percentage of the baseline MIP value, or it is better to use an incremental load based on the heart rate derived from the CPET. What type of training to follow: aerobic; aerobic and anaerobic; HIIT.
As underlined in the text, a reduction in inspiratory capacity is a risk factor for relapse or worsening of the cardiovascular condition. Recent data highlight an increase in pneumonia (2-7%) in post-MI patients, probably related to the presence of diaphragmatic dysfunction [62]. Further research efforts must be made to determine the best responses to achieve maximum patient clinical benefits during CR.
Conclusions
Cardiac rehabilitation (CR) has been shown to be effective in reducing the rate of recurrence and disease as secondary prevention in patients who have undergone MI. CR is a multidisciplinary path in which the patient is followed pharmacologically, from a psychological, nutritional, nursing and physiotherapy point of view. Patients who have suffered from MI (and stable angina) have reduced muscular strength of the respiratory muscles, that is a reduced ability to generate the correct thoracic pressures measurable through a forced inspiration against an occluded mouthpiece (maximal inspiratory pressure (MIP). We know that a reduced diaphragmatic contractile capacity can be a risk factor for recurrent MI and heart failure. International guidelines do not give specific indications on inspiratory/diaphragm muscle training in post-MI patients. Research should make further effort to better frame the respiratory rehabilitation process in this type of patients and give more robust indications on the initial evaluation of the diaphragm before undertaking the rehabilitation process.
Author Contributions
All authors had the same role in drafting the article. All authors have read and agreed to the published version of the manuscript.
Funding
The article has been funded by the Italian Ministry of Health.
Institutional Review Board Statement
Ethics approval is not required for this article.
Informed Consent Statement
Informed Consent Statement is not required for this article.
Data Availability Statement
There is no further data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roth GA, Mensah GA, Johnson CO; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020; 76(25):2982-3021. [CrossRef]
- Lababidi H, Salerno PR, Wass SY, Shafiabadi Hasani N, Bourges-Sevenier B, Al-Kindi S. The Global Burden of premature cardiovascular disease, 1990-2019. Int J Cardiol Cardiovasc Risk Prev. 2023: 19:200212. [CrossRef]
- Nedkoff L, Briffa T, Zemedikun D, Herrington S, Wright FL. Global Trends in Atherosclerotic Cardiovascular Disease. Clin Ther. 2023; 45(11):1087-1091. [CrossRef]
- Thygesen, K. 'Ten Commandments' for the Fourth Universal Definition of Myocardial Infarction 2018. Eur Heart J. 2019; 40(3):226. [CrossRef]
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019; 40(3):237-269. [CrossRef]
- de Lemos JA, Newby LK, Mills NL. A Proposal for Modest Revision of the Definition of Type 1 and Type 2 Myocardial Infarction. Circulation. 2019; 140(22):1773-1775. [CrossRef]
- Lindahl B, Mills NL. A new clinical classification of acute myocardial infarction. Nat Med. 2023 Sep; 29(9):2200-2205. [CrossRef]
- Ögmundsdottir Michelsen H, Sjölin I, Schlyter M, Hagström E, Kiessling A, Henriksson P, Held C, Hag E, Nilsson L, Bäck M, Schiopu A, Zaman MJ, Leosdottir M. Cardiac rehabilitation after acute myocardial infarction in Sweden - evaluation of programme characteristics and adherence to European guidelines: The Perfect Cardiac Rehabilitation (Perfect-CR) study. Eur J Prev Cardiol. 2020; 27(1):18-27. [CrossRef]
- Kim C, Sung J, Lee JH et al. Clinical Practice Guideline for Cardiac Rehabilitation in Korea: Recommendations for Cardiac Rehabilitation and Secondary Prevention after Acute Coronary Syndrome. Korean Circ J. 2019; 49(11):1066-1111. [CrossRef]
- Supervia M, Turk-Adawi K, Lopez-Jimenez F et al. Cardiac Rehabilitation Availability and Density around the Globe. EClinicalMedicine. 2019; 13:31-45. [CrossRef]
- O'Connell ME, Suskin N, Prior PL. Measuring True Change in Individual Patients: Reliable Change Indices of Cardiac Rehabilitation Outcomes, and Implications for Quality Indicators. CJC Open. 2021; 3(9):1139-1148. [CrossRef]
- Szmigielska K, Jegier A. Clinical Outcomes of Cardiac Rehabilitation in Women with Coronary Artery Disease-Differences in Comparison with Men. J Pers Med. 2022; 12(4):600. [CrossRef]
- Thakker R, Khan M, Al-Hemyari B. Cardiac Rehabilitation After Hospitalization for Acute Coronary Syndrome. Curr Cardiol Rep. 2023. [CrossRef]
- Kasperowicz A, Cymerys M, Kasperowicz T. Effectiveness of cardiac rehabilitation in exercise capacity increase in patients with ST-segment elevation myocardial infarction. Int J Environ Res Public Health. 2019;16(21):4085. [CrossRef]
- Qin S, Tian Z, Boidin M, Buckley BJR, Thijssen DHJ, Lip GYH. Irisin is an Effector Molecule in Exercise Rehabilitation Following Myocardial Infarction (Review). Front Physiol. 2022: 13:935772. [CrossRef]
- Squires RW, Kaminsky LA, Porcari JP, Ruff JE, Savage PD, Williams MA. Progression of Exercise Training in Early Outpatient Cardiac Rehabilitation: AN OFFICIAL STATEMENT FROM THE AMERICAN ASSOCIATION OF CARDIOVASCULAR AND PULMONARY REHABILITATION. J Cardiopulm Rehabil Prev. 2018; 38(3):139-146. [CrossRef]
- Ambrosetti M, Abreu A, Corrà U et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2021; 28(5):460-495. [CrossRef]
- Abreu A, Frederix I, Dendale P, Janssen A, Doherty P, Piepoli MF, Völler H, Davos CH; Secondary Prevention and Rehabilitation Section of EAPC Reviewers:. Standardization and quality improvement of secondary prevention through cardiovascular rehabilitation programmes in Europe: The avenue towards EAPC accreditation programme: A position statement of the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology (EAPC). Eur J Prev Cardiol. 2021; 28(5):496-509. [CrossRef]
- Grace SL, Kotseva K, Whooley MA. Cardiac Rehabilitation: Under-Utilized Globally. Curr Cardiol Rep. 2021; 23(9):118. [CrossRef]
- Wang L, Liu J, Fang H, Wang X. Factors associated with participation in cardiac rehabilitation in patients with acute myocardial infarction: A systematic review and meta-analysis. Clin Cardiol. 2023; 46(11): 1450–1457. [CrossRef]
- Verdicchio C, Freene N, Hollings M et al. A Clinical Guide for Assessment and Prescription of Exercise and Physical Activity in Cardiac Rehabilitation. A CSANZ Position Statement. Heart Lung Circ. 2023; S1443-9506(23)04214-2. [CrossRef]
- Virani SS, Newby LK, Arnold SV; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023; 148(9):e9-e119. [CrossRef]
- Van Damme A, McDermott S, McMurtry S, Kung JY, Gyenes G, Norris C. Secondary Prevention and Rehabilitation for Spontaneous Coronary Artery Dissection: A Systematic Review. Can J Cardiol. 2023; 39(11S):S395-S411. [CrossRef]
- Salah HM, Goldberg LR, Molinger J; et al. Diaphragmatic Function in Cardiovascular Disease: JACC Review Topic of the Week. J Am Coll Cardiol. 2022; 80(17):1647-1659. [CrossRef]
- Boussuges A, Chaumet G, Poirette L. Interest of ultrasonographic assessment of diaphragmatic function in cardiac rehabilitation center: a case report. Medicine (Baltimore). 2015; 94(19):e801. [CrossRef]
- Mol D, Renskers L, Balt JC; et al. Persistent phrenic nerve palsy after atrial fibrillation ablation: Follow-up data from The Netherlands Heart Registration. J Cardiovasc Electrophysiol. 2022; 33(3):559-564. [CrossRef]
- Harris K, Maniatis G, Siddiqui F, Maniatis T. Phrenic nerve injury and diaphragmatic paralysis following pacemaker pulse generator replacement. Heart Lung. 2013; 42(1):65-6. [CrossRef]
- López-Gil M, Fontenla A, Juliá J, Parra JJ, Arribas F. Phrenic paralysis during cardiac electronic device implantation: incidence, causes and clinical course. Europace. 2016; 18(10):1561-1564. [CrossRef]
- Maranta F, Cianfanelli L, Rizza V; et al. Diaphragm Dysfunction after Cardiac Surgery: Insights from Ultrasound Imaging during Cardiac Rehabilitation. Ultrasound Med Biol. 2022; 48(7):1179-1189. [CrossRef]
- Aguirre VJ, Sinha P, Zimmet A, Lee GA, Kwa L, Rosenfeldt F. Phrenic nerve injury during cardiac surgery: mechanisms, management and prevention. Heart Lung Circ. 2013; 22(11):895-902. [CrossRef]
- Gayan-Ramirez G, Gosselin N, Troosters T, Bruyninckx F, Gosselink R, Decramer M. Functional recovery of diaphragm paralysis: a long-term follow-up study. Respir Med. 2008; 102(5):690-8. [CrossRef]
- Bordoni B, Marelli F, Morabito B, Sacconi B, Caiazzo P, Castagna R. Low back pain and gastroesophageal reflux in patients with COPD: the disease in the breath. Int J Chron Obstruct Pulmon Dis. 2018; 13:325-334. [CrossRef]
- Smith JR, Taylor BJ. Inspiratory muscle weakness in cardiovascular diseases: Implications for cardiac rehabilitation. Prog Cardiovasc Dis. 2022; 70:49-57. [CrossRef]
- Yegorova S, Yegorov O, Ferreira LF. RNA-sequencing reveals transcriptional signature of pathological remodeling in the diaphragm of rats after myocardial infarction. Gene. 2021: 770:145356. [CrossRef]
- Bowen TS, Mangner N, Werner S; et al. Diaphragm muscle weakness in mice is early-onset post-myocardial infarction and associated with elevated protein oxidation. J Appl Physiol (1985). 2015; 118(1):11-9. [CrossRef]
- van der Pijl RJ, Granzier HL, Ottenheijm CAC. Diaphragm contractile weakness due to reduced mechanical loading: role of titin. Am J Physiol Cell Physiol. 2019; 317(2):C167-C176. [CrossRef]
- Barreiro E, Hussain SN. Protein Carbonylation in Skeletal Muscles: Impact on Function. Antioxid Redox Signal. 2010; 12(3):417-29. [CrossRef]
- Hahn D, Kumar RA, Muscato DR, Ryan TE, Schröder K, Ferreira LF. Nox4 Knockout Does Not Prevent Diaphragm Atrophy, Contractile Dysfunction, or Mitochondrial Maladaptation in the Early Phase Post-Myocardial Infarction in Mice. Cell Physiol Biochem. 2021; 55(4):489-504. [CrossRef]
- Chen HS, van Roon L, Schoones J, Zeppenfeld K, DeRuiter MC, Jongbloed MRM. Cardiac sympathetic hyperinnervation after myocardial infarction: a systematic review and qualitative analysis. Ann Med. 2023; 55(2):2283195. [CrossRef]
- Delbono O, Rodrigues ACZ, Bonilla HJ, Messi ML. The emerging role of the sympathetic nervous system in skeletal muscle motor innervation and sarcopenia. Ageing Res Rev. 2021: 67:101305. [CrossRef]
- Cheng AJ, Jude B, Lanner JT. Intramuscular mechanisms of overtraining. Redox Biol. 2020: 35:101480. [CrossRef]
- Armstrong LE, Bergeron MF, Lee EC, Mershon JE, Armstrong EM. Overtraining Syndrome as a Complex Systems Phenomenon. Front Netw Physiol. 2022: 794392. [CrossRef]
- Bordoni B, Escher A, Compalati E, Mapelli L, Toccafondi A. The Importance of the Diaphragm in Neuromotor Function in the Patient with Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2023; 18:837-848. [CrossRef]
- Bordoni B, Escher AR. The Importance of Diaphragmatic Function in Neuromuscular Expression in Patients With Chronic Heart Failure. Cureus. 2023; 15(2):e34629. [CrossRef]
- Sannasi R, Dakshinamurthy A, Dommerholt J, Desai V, Kumar A, Sugavanam T. Diaphragm and core stabilization exercises in low back pain: A narrative review. J Bodyw Mov Ther. 2023; 36:221-227. [CrossRef]
- Fernandez M, Ordoñana JR, Hartvigsen J; et al. Is Chronic Low Back Pain Associated with the Prevalence of Coronary Heart Disease when Genetic Susceptibility Is Considered? A Co-Twin Control Study of Spanish Twins. PLoS One. 2016; 11(5):e0155194. [CrossRef]
- Nabutovsky I, Breitner D, Heller A; et al. Home-Based Cardiac Rehabilitation Among Patients Unwilling to Participate in Hospital-Based Programs. J Cardiopulm Rehabil Prev. 2024; 44(1):33-39. [CrossRef]
- Du M, Ye X, Li D, Yang C, Dai R. Development of a prediction model for exercise tolerance decline in the exercise assessment of patients with acute myocardial infarction undergoing percutaneous coronary intervention revascularization in the acute phase. J Thorac Dis. 2023; 15(8):4486-4496. [CrossRef]
- Richman PS, Yeung P, Bilfinger TV, Yang J, Stringer WW. Exercise Capacity in Unilateral Diaphragm Paralysis: The Effect of Obesity. Pulm Med. 2019: 2019:1090982. [CrossRef]
- Domnik NJ, Walsted ES, Langer D. Clinical Utility of Measuring Inspiratory Neural Drive During Cardiopulmonary Exercise Testing (CPET). Front Med (Lausanne). 2020: 7:483. [CrossRef]
- Caleffi Pereira M, Cardenas LZ, Ferreira JG; et al. Unilateral diaphragmatic paralysis: inspiratory muscles, breathlessness and exercise capacity. ERJ Open Res. 2021; 7(1):00357-2019. [CrossRef]
- Evans SA, Watson L, Cowley AJ, Johnston ID, Kinnear WJ. Normal range for transdiaphragmatic pressures during sniffs with catheter mounted transducers. Thorax. 1993; 48(7):750-3. [CrossRef]
- Mangner N, Winzer EB, Linke A, Adams V. Locomotor and respiratory muscle abnormalities in HFrEF and HFpEF. Front Cardiovasc Med. 2023:10:1149065. [CrossRef]
- Fayssoil A, Mansencal N, Nguyen LS; et al. Diaphragm Ultrasound in Cardiac Surgery: State of the Art. Medicines (Basel). 2022; 9(1):5. [CrossRef]
- Ricoy J, Rodríguez-Núñez N, Álvarez-Dobaño JM, Toubes ME, Riveiro V, Valdés L. Diaphragmatic dysfunction. Pulmonology. 2019; 25(4):223-235. [CrossRef]
- Fayssoil A, Nguyen LS, Ogna A; et al. Diaphragm sniff ultrasound: Normal values, relationship with sniff nasal pressure and accuracy for predicting respiratory involvement in patients with neuromuscular disorders. PLoS One. 2019; 14(4):e0214288. [CrossRef]
- Bordoni B, Marelli F, Morabito B, Sacconi B. Manual evaluation of the diaphragm muscle. Int J Chron Obstruct Pulmon Dis. 2016; 11:1949-56. [CrossRef]
- Bordoni B, Morabito B. The Diaphragm Muscle Manual Evaluation Scale. Cureus. 2019; 11(4):e4569. [CrossRef]
- Bordoni B, Escher AR. Functional evaluation of the diaphragm with a noninvasive test. J Osteopath Med. 2021; 121(11):835-842. [CrossRef]
- Kurzaj M, Dziubek W, Porębska M, Rożek-Piechura K. Can Inspiratory Muscle Training Improve Exercise Tolerance and Lower Limb Function After Myocardial Infarction? Med Sci Monit. 2019: 25:5159-5169. [CrossRef]
- Ahmad AM, Hassan MH. Effects of Addition of Inspiratory Muscle Training to Exercise-Based Cardiac Rehabilitation on Inspiratory Muscle Strength, Peak Oxygen Consumption, and Selected Hemodynamics in Chronic Heart Failure. Acta Cardiol Sin. 2022; 38(4):485-494. [CrossRef]
- Liu Y, Dai Y, Liu Z; et al. The Safety and Efficacy of Inspiratory Muscle Training for Patients With Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention: Study Protocol for a Randomized Controlled Trial. Front Cardiovasc Med. 2021: 7:598054. [CrossRef]
Figure 1.
The image shows an elevation of both hemidiaphragms, in the presence of median sternotomy and presence of subcutaneous pacemaker. A: frontal plane; B: sagittal plane.
Figure 1.
The image shows an elevation of both hemidiaphragms, in the presence of median sternotomy and presence of subcutaneous pacemaker. A: frontal plane; B: sagittal plane.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



