
Submitted:
20 February 2024
Posted:
22 February 2024
You are already at the latest version
Abstract
Academic stress affects students' psychological and physiological well-being. Dental undergraduate programs are known for their demanding curriculum, leading to significant stress symptoms. Objective was to determine if salivary cortisol levels were higher in students exposed to academic stress, assess the relationship between stress severity/temperament and cortisol values, and explore relaxation technique effects. Salivary cortisol was measured at two time points for all participants: before exams and during a relaxation period after summer break. A third measurement was conducted for students with high pre-test cortisol levels who received instructions on progressive muscle relaxation(PMR) before subsequent exams. Additionally, participants completed two questionnaires: Perceived Stress Scale(PSS) and Fisher's Temperament Questionnaire. The group analysis based on the PSS indicated that 39 participants reported high stress. Women demonstrated significantly higher stress than men(p=0.042054). A significant difference in stress levels was observed between Director and Builder temperament types(p=0.029276). Cortisol levels showed a significant decrease from the first measurement to the second measurement, and the third measurement after implementing PMR. The grade in the "Dermatovenereology" course correlated with stress level according to the PSS(k=0.578467). Pre-test cortisol levels correlated with the frequency of using PMR guidelines during winter test periods(k=0.416138). Stress negatively affects the immune system and poses health risks. Implementing stress reduction techniques in dental/medical education could benefit students and the healthcare system.
Keywords:
Academic stress
; Cortisol
; PSS
; Temperament
; PMR
1. Introduction
Academic stress (AS) is a significant, everyday stress that impacts students’ psychological and physiological health. Exams, in particular, are considered one of the most pronounced sources of stress among students [1,2,3]. Although the results of studies differ, a significant association between AS and aspects of the immune system has been observed, including a decreased immune response. The heterogeneous results of the various studies probably reflect the insufficient study of the impact of AS itself on students, without looking at other associated factors (high professional competitiveness, lack of time for relaxation and communication with friends and family, etc.) [2,3,4]. Medical and dental faculties are stressful environments for most students; undergraduate programs are often associated with significant symptoms of stress because they are among the longest and most demanding programs [5,6,7]. The most significant causes of AS in these students are exams and clinical exercises [5]. Medical and dental students more often notice, manifest, and report increased anxiety, depression, obsessive-compulsive behaviors (absent the disorder), increased interpersonal sensitivity, among other symptoms [5,6,7]. After enduring long-term academic stress, doctors and dentists may then experience professional stress caused by various factors, such as interactions with patients and other staff, fear of physical violence when working with certain patients, and malpractice lawsuits and other financial concerns [7]. Cortisol plays a key role in the body’s response to stress [8]. In routine diagnostics, cortisol is most commonly measured in the plasma, which requires a blood sample, an invasive method potentially causing additional stress and discomfort [9]. Cortisol can also be measured in the saliva by collecting samples in a sterile container, or by using absorbent materials (so-called Salivette systems), without causing undue stress. This easy and non-invasive method of collecting samples is being increasingly used to measure cortisol [10,11]. Numerous studies have confirmed that the analysis of salivary cortisol, as a stress biomarker, is a reliable alternative to analyzing cortisol in the blood and urine [12,13]. Salivary cortisol is a biologically active form of free cortisol. It has a concentration ten times lower than total serum cortisol and correlates well with plasma cortisol (adult correlation is about 0.75) - this correlation remains high throughout the circadian cycle [14]. Cortisol secretion is affected by the circadian rhythm, with the lowest fluctuations expected in the late afternoon and the highest concentrations of cortisol expected in the morning between 7 and 10 a.m. (The specific time a person wakes has no major influence on the morning cortisol response, and within 30 minutes after waking, the free cortisol level rises from 50% to 75%.) [15]. Salivary cortisol values are affected by a number of factors, including during the body’s response to stress: age and gender, endogenous and exogenous sex hormone values (e.g., menstrual cycle, oral contraceptive use, hormone replacement therapy, pregnancy, breastfeeding), certain medications (psychopharmaceuticals, corticosteroids), smoking, energy-rich diets, coffee and alcohol consumption, and exercise [16]. In addition, it is assumed that salivary cortisol, during stress, is influenced (at least partially) by stable factors such as character traits, although the results from previous studies are not uniform [13,17,18,19]. Numerous studies have suggested that there are benefits to using cortisol as a salivary biomarker and as an indicator of AS [20,21]. Significantly higher cortisol values were measured in students just before and during exam periods, while significantly reduced values were found after exam periods [22,23,24]. However, the existing literature also shows some conflicting results in the relationship between academic stress and salivary cortisol levels [25]. Therefore, we wanted to examine salivary cortisol levels in dental medicine students exposed to AS in relation to perceived stress levels (measured by stress questionnaires). We also looked at the possible correlation between salivary cortisol values and perceived stress severity in the context of personal temperament, also determined by questionnaires. Finally, we looked at relaxation methods as a way to reduce students’ stress during exams.
2. Materials and Methods
This prospective and interventional study was conducted with students of dental medicine during exams and classes and was conducted at the Sestre Milosrdnice University Hospital Centre (SMUHC), at the Department of Dermatovenereology and the Department of Clinical Chemistry, Zagreb, Croatia. The research was conducted in accordance with the basic principles of the Helsinki Declaration (as revised by the World Medical Association Declaration of Helsinki 2013) and was approved by the Ethics Committees of SMUHC and the School of Dental Medicine, Zagreb, Croatia (class: 003-06/21-03/016 and 05-PA-30-XXIX-9/2021). We followed dentistry students, all in the same year of study, and measured their pretest salivary cortisol values immediately before exams, and compared those values with the values measured after a longer, relaxed non-exam period. We compared these levels by sex and temperament characteristics. We examined indicators of perceived stress using the Perceived Stress Scale (PSS) and compared PSS levels of perceived stress (low, medium or high) with pretest salivary cortisol levels. In addition, we investigated the correlation between temperament characteristics (determined by the Fisher Temperament Inventory, or FTI) and stress level (determined by PSS values and pre-test salivary cortisol values). Afterward, we applied the guidelines of progressive muscle relaxation (PMR) to students with the most pronounced stress values (measured at the first exposure to pre-test academic stress) to examine whether / how much the use of PMR affected salivary cortisol values during subsequent academic stress. This study included prospective monitoring of cortisol values during individual time points (Figure 1). Salivary cortisol levels were measured at 2 time points for all students: 1. just before the exam; and 2. after the relaxation period (summer vacation). When cortisol was initially measured (at the first time point), subjects were also given questionnaires about perceived stress (PSS) and temperament (FTI). Additionally, only those students with high pretest cortisol (at the first pretest measurement, 10 respondents) were measured a third time, wherein after the second measurement they received instructions on how to practice PMR. All participants confirmed using PMR before the last exam (third time point), at which time cortisol values were again measured.
2.1. Respondents
This study included 40 subjects, students of the School of Dental Medicine, University of Zagreb, aged 20-25 years (to prove statistical significance α=0.05 statistical power 80%, two-tailed t-test for matched pairs, had to include at least 34 subjects). The inclusion criteria for the study were that participants had to be in their 4th-year of study, be aged 18 or more, sign an informed consent prior to any study procedure. Exclusion criteria were recent use of systemic corticosteroids or immunosuppressive agents (one month prior to study enrollment); having a previously diagnosed psychiatric disorder; chronic smoking and alcohol consumption; pregnancy; having a systemic immune, endocrine or malignant disease (Figure 1).
2.2. Methods
2.2.1. Saliva Collection Method and Salivary Cortisol Analysis
The first salivary cortisol measurement was taken before subjects took the exam (oral dermatovenereology test, held at SMUHC). For all students, salivary cortisol was determined by taking samples of saliva in the morning (9-11 a.m.) to prevent values from being affected by the daily oscillation of cortisol levels. Before taking the sample, subjects rinsed their mouth to clean the oral cavity, then waited 5 minutes. The procedure involved placing absorbent material (cotton pieces) in the mouth, the so-called Salivette system (Sarstedt, Nümbrecht, Germany), on the parotid gland outlet for 5 minutes. Samples were then centrifuged, and the supernatant was stored in a refrigerator (FRYKA-Kältetechnik GmbH, Esslingen, Germany) at -80°C until analyzed. Samples were analyzed by the ELISA (enzyme-linked immunosorbent assay) test by EUROIMMUN (Medizinische Labordiagnostika AG, Lübeck, Germany), at the Department of Clinical Chemistry of SMUHC. The use of this method for measuring cortisol in saliva was confirmed by the manufacturer with the following specifications: limit of detection, 0.15 ng/mL; variation within the test, 3.7%; and variation between tests, 7.4% [26]. To carry out salivary cortisol analysis, murine anti human antibodies were used, and the specific incubation/reaction of antibodies and cortisol was carried out at room temperature (from +18°C to +25°C). The reference average cortisol concentrations were measured by the above mentioned manufacturer’s test, and their values were compared with the ELISA reference average for cortisol [13].
2.2.2. Measuring Stress Using the Perceived Stress Scale (PSS) and Determining Temperament Using the Fisher Temperament Inventory (FTI)
After the exam, an email was sent to each participant with their demographic data (name, gender, year of birth), two questionnaires, the PSS [27] and FTI [28], as well as a question about their exam results/grade. Originally conceived in 1983, the PSS is a scale that is a common instrument for assessing mental stress. It provides insight into how different situations affect respondents’ feelings and perception of stress. It consists of 10 questions answered on the Likert scale (0=never, 4=very often) that provide answers about the feelings and thoughts of respondents during the last month [27]. Individual PSS scores can range from 0 to 40, with higher scores reflecting higher perceived stress (scores: 0-13 = low stress, 14-26 = moderate stress, 27-40 = high stress). The FTI [28] examines four dimensions of human temperament related to the functioning of particular hormonal and neurotransmitter systems. The four dimensions of temperament are curious/energetic (Explorer), careful/according to social standards (Builder), analytical/decisive (Director) and prosocial/empathetic (Negotiator). According to questionnaire’s author, Helen Elizabeth Fisher, each individual is a unique "mixture" of all four dimensions and it is possible for individuals to express only some dimensions of temperament more often. There are four possible answers for each question (strongly disagree, disagree, agree and strongly agree). The result for each scale is formed by summing the points achieved on the individual plots of the scale, with the answer "strongly disagree" on all questions being scored with zero points; the answer "disagree" scored with one point; the answer "agree" with two points; and the answer "strongly agree" with three points. Results on each scale range from 0 to 42 points, where higher results indicate a more pronounced dimension of temperament. Results indicate a primary temperament type, the scale achieving the highest number.
2.2.3. Evaluation of Questionnaires, Follow-Up Procedure and Other Cortisol Measurement
The questionnaires were used as assessment tools for stress (PSS) and as an instrument for assessing the primary type of temperament of each subject individually (FTI), therefore describing parameters which could affect their quality of life. Based on PSS results, students were divided into three groups: low, medium, and high levels of perceived stress. Students were also divided into the four types of temperament (Explorer, Builder, Director, Negotiator) as indicated by FTI results. A second saliva sample was then taken from all subjects (to assess cortisol), this time in a relaxed period without exams (at the very beginning of a new semester and class). Additionally, each participant’s exam grade was recorded, where the best grade was excellent, five, on a range of 1-5.
2.2.4. Third Cortisol Measurement Following Progressive Muscle Relaxation (PMR) - and Its Use in Subjects with a Third Cortisol Measurement
After the second set of saliva samples were collected (taken after the relaxed period - during the period without exams), each student received a document with instructions on PMR and were asked to carefully study them and try to apply them before the next exam period [29,30]. PMR is a relaxation technique developed in the 1920s by Edmund Jacobson that helps relieve the negative effects of stress and control anxiety [31]. It consists of a series of stretching and relaxing exercises for different muscle groups for the whole body, thus achieving a relaxed state of body and mind. In a continuous sequence of exercises, the various muscle groups contract and relax [32]. It has been shown to be successful in healthy, stress-exposed individuals and in people with mental and physical health problems [33]. Relaxation regulates the heartbeat, slows breathing, lowers blood pressure, reduces muscle tension and promotes a psychological experience of whole body relaxation. Exercises are intended for anyone, both healthy individuals and those with mental health issues—anyone exposed to different types of tension or stress. Those study participants (10 respondents) with the highest recorded academic stress (cortisol values) were asked to give a third saliva sample just before their next exam (of a similar type) in order to assess the impact of the application of PMR on academic stress. To gain insight into the effect of PMR, all subjects were forwarded a new questionnaire containing 4 questions about PMR (answers given on the Likert scale [1=never; 5=very often]) and about how useful its application was personally. Participants evaluated the PMR guidelines, their application during examination deadlines, how much they helped to cope with academic stress, and how they influenced academic achievement (in the form of better grades).
2.2.5. Statistical Analysis
The research results are presented in the form of box-plots with median values and interquartile range. Measurements of parameters (salivary cortisol, PSS) were compared separately for each group by gender and Fisher’s temperament types. Comparisons were evaluated by the Mann-Whitney U test with continuity correction for comparison between genders, Kruskal-Wallis ANOVA by ranks test with post-hoc Dunn’s multiple p comparison test for comparison between Fisher’s temperament types, the Wilcoxon rank test and Friedman’s ANOVA with Kendall’s W (coefficient of concordance) for repeated measurements of salivary cortisol levels, since the changes of measured parameters did not follow the normal distribution, which was confirmed by the normality test - Shapiro-Wilk and Kolmogorov tests for each parameter. Also, indicators of asymmetry and curvature indicated an abnormal distribution. The Spearman rank test was used for analysis of correlations between parameters. Results were considered statistically significant at 0.05. Analysis was carried out using the Statistica software package (TIBICO Statistica Version 14.0.0.15.).
3. Results
3.1. Analysis of the Perceived Stress Scale (PSS) Results in Relation to Other Parameters/Variables
PSS levels, as measured immediately after the first exam, showed high perceived stress in almost all students (39/40), with medium stress in one student. There were no subjects with low stress. Since the majority of examinees (97.5% of respondents) had high stress, the respondents were not consequently separated by PSS score. According to descriptive statistics and a comparison of stress level (per PSS) between men and women (Figure 2), significantly higher stress levels were observed in women than in men (Mann-Whitney U test, U=99.5, Z adjusted = -2.021, 2*1 sided exact p =0.042). According to temperament type (per FTI), there was a significant difference in the stress level (per PSS) between Director and Builder, where Builder had significantly higher stress than Director (p=0.029) (Figure 3).
3.2. Results Obtained by Salivary Cortisol Analysis
According to descriptive statistics and a comparison of students’ pre-test cortisol levels by sex, there was no significant difference between genders (Figure 4). However, there was a significant difference between the first (pre-exam) and second (non-exam period) cortisol measurements (ng/mL) for both males (Wilcoxon matched pairs test, N=12, T=0.00, Z =3.059, p=0.002) and females (Wilcoxon matched pairs test, N=28, T=0.00, Z =4.623, p<0.001). When comparing cortisol and temperament types (by Fisher’s division), no significant difference in pre-exam cortisol levels was observed. The comparison is presented in Figure 5. A comparison of the values for the three different cortisol measurements (pre-exam; post-exam at the end of summer vacation; and just before the exam after progressive muscle relaxation [25% of students with the highest cortisol level at the first measurement]) are presented with a graphic representation in Figure 6.
3.3. Exam Scores and Correlations
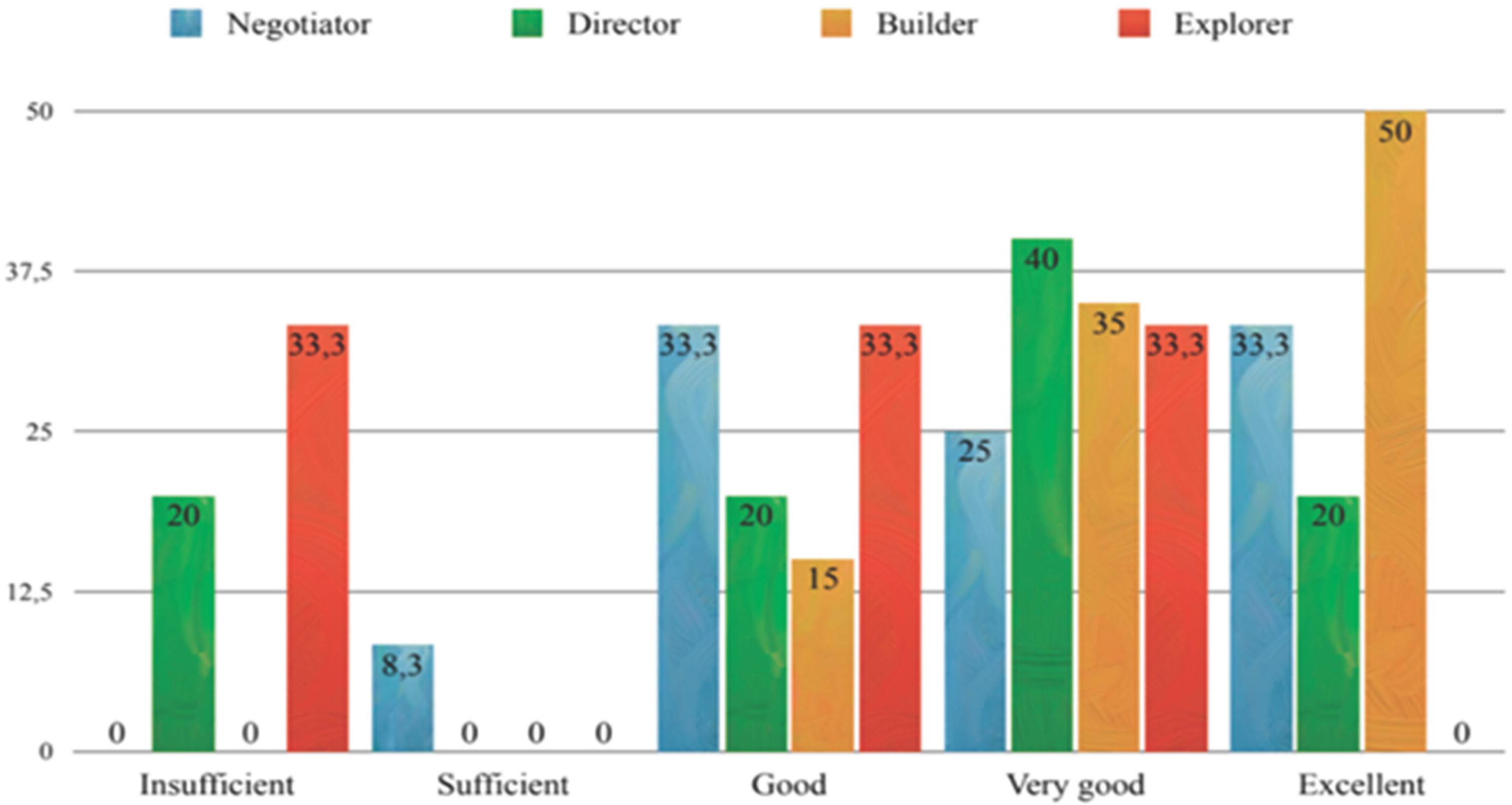
The distributions of test scores (first exam, „Dermatovenereology“) by sex and by temperament type (Fisher’s) are shown in Figure 7 and Figure 8. A correlation between exam scores and stress levels (per PSS) were found, i.e., higher exam scores (better results) were associated with higher stress (Spearman’s ρ = 0.578467, p<0.05). When looking at the impact of PMR on the students’ stress levels, a positive influence was seen. Thus, a positive correlation was observed between pre-exam cortisol levels and the more frequent application of PMR guidelines (Spearman’s ρ =0.416138, p<0.05), with a positive evaluation of these guidelines by students themselves (Spearman’s ρ = 0.363745, p<0.05), and the cortisol level measured after non-exam period (Spearman’s ρ =0.59228, p<0.05).
4. Discussion
Earlier studies have analyzed the effect of acute stress during students’ oral exams (pre-exam stress, specifically) to study the stress paradigm, and they observed increased cortisol levels in anticipation of stressful situations [8,34,35]. In addition to oral exams [7,36,37,38,39,40,41,42,43], a significant source of stress for dental students are clinical exercises, competition with colleagues for grades and the fear of failing an exam or the academic year [36,44,45]. Our research additionally supports/indicates the influence of certain other stress-related factors, such as gender, as significantly higher stress (PSS) was observed in women than men, which corresponds to many studies that have shown that the study of dental medicine is more stressful for women/students than for their male colleagues [37,44,45]. Although in earlier psychoneuroendocrine (PNE) studies women showed a lower response to stress [46,47], according to recent studies, women subjectively perceived experiencing greater stress and had a less favorable cognitive assessment (trouble remembering and learning new things, difficulty with everyday life decisions), likely related to their higher risk of developing mood disorders and anxiety [48,49,50]. Accordingly, recent research shows that women usually report more stress than men [51,52,53]. Although our study indicates significantly higher stress (PSS) in women than men, cortisol values did not significantly differ between the sexes. A few studies, though, observed higher cortisol levels in men than women, where cortisol was measured just before taking a written and oral exam [46,54,55]. A potential explanation is the fact that our respondents were only exposed to an oral and not a written exam. Also, when comparing groups by levels of perceived stress (PSS), low, medium, and high, there was no difference in participants’ pre-exam salivary cortisol levels, though it should be noted that high perceived stress was noted in the majority of our subjects/students (97.5%).
The comparison of our students’ pre-exam cortisol levels with their cortisol values during the non-exam period showed significantly higher pre-exam cortisol values. Our students’ strong cortisol increase in anticipation of the exam corresponds to several previous studies [11,35,56,57], which showed higher cortisol values before exams than during the period immediately after summer vacation. Most previous research results correspond to our results, showing decreased cortisol concentrations in a non-exam period compared to a pre-exam period [35,57,58]. Several studies, however, did not reveal changes in cortisol concentrations when comparing the two periods [59,60], and some studies even indicated an additional increase in cortisol concentration after the exam [23,61]. Although some studies have shown that cognitive assessments affect the cortisol response to stressors [62,63], our results did not prove a correlation between pre-exam stress and PSS, which is in line with previous research, which shows a weak and divergent connection between perceived stress and measured stress [64,65,66]. Another potentially important factor for a person’s experience and perception of stress can also be personality traits. By comparing students’ pre-exam cortisol levels by temperament type (according to Fisher’s division), no significant association was found, but some observations were noted: Explorer and Director temperaments have lower average pre-exam cortisol values than Builder and Negotiator temperaments. According to previous research results, the Explorer temperament (which was the least represented among the surveyed students) is linked to the neurotransmitters dopamine and noradrenaline, with certain behavioral patterns (Fisher et al.,2015). Explorers are characterized by creativity, curiosity, impulsiveness, and tendency toward risky activities and seeking excitement and novelty [28]. Thus, Fisher’s temperaments, like the curious and impulsive Explorer and the extroverted and determined Director, offer a clear picture of why these individuals’ cortisol levels would not increase very much in the pre-exam period. However, despite the promising results of some studies showing an association between personality factors and cortisol response, other studies like ours have failed to establish a consistent link [17,18,19].
In addition, we found a significant difference in stress levels between people of different characteristics. A significantly higher level of stress (the PSS) was seen in Builders. According to Fisher and colleagues, the Director’s character is linked to testosterone (based on earlier research findings on the role of testosterone in cognitive processes and socio-emotional engagement), where individuals with this pronounced Director temperament are characterized by dominance and attention to detail [67]. Based on these findings, compared to women, men should be more analytical/decisive, which has been confirmed by previous studies [28,68]. On the other hand, the presumed biological basis of the Builder temperament is the neurotransmitter serotonin [67]. So, the traits attributed to people with a pronounced Builder dimension (based on previous research) include a connection to serotonin, pronounced numerical and pictorial creativity, pronounced sociability and self-control, as well as self-transcendence [28]. Also according to earlier studies, lower neuroendocrine stress is associated with high self-esteem, high extroversion, low anxiety and low neuroticism [69,70]. The above can explain the lower PSS level in our extroverted and decisive subjects (students) with the Director temperament. Thus, we partially accept the assumption that PSS levels differ between the primary types of temperaments defined by Fisher’s inventory. Our results show an interesting connection (positive correlation) between students’ stress levels (PSS) and exam grades—the greater the student’s perceived stress, the higher the exam grade. Notably, students consider the "Dermatovenereology" exam used for this study one of the more demanding exams. This connection between grades and PSS level may indicate that these students take very seriously their studies and responsibilities for the courses they attend. Concerning temperament traits in relation to exam grades, Builders received the most fives (excellent), while Directors had the most fours (very good). This shows that the Builder traits (numerical and pictorial creativity, pronounced sociability and self-control) in comparison to Director traits (attention to details and lower level of verbal fluency) result in better Builder success in oral exams. By gender, female students more often had the best grade (excellent, five), while men more often had a grade of very good (four). Numerous articles on stress during university studies have established that studying dental medicine is more stressful for female students than for their male colleagues [37,44,45]; our results also confirmed this, showing higher stress (PSS) in female students than male students. Our results related to PMR show that this technique was effective at reducing pre-exam stress. The participants who applied the PMR technique, and who had their cortisol measured a third time before an exam similar to the first, showed a drop in cortisol levels. This group included only 25% of participants who had had the highest pre-exam (first exam) cortisol levels, and their drop in cortisol at subsequent measurements indicates that PMR provided a beneficial effect for these students. The three measurement time points were 1. just before the first exam; 2. during the non-exam period after summer break; and 3. just before the second exam, after applying PMR, and a significant drop in participants’ cortisol levels was observed over those time points. In fact, the lowest cortisol level was observed at the 3rd measurement point, indicating that applying the relaxation technique caused a significant reduction in pre-exam stress. These results confirm what other studies have found concerning stress in students before and after PMR [71,72,73,74]. Pv and Lobo [71] applied the PMR technique in 30 first-year nursing students (random sample) and found a significant reduction in stress. Also, Arabaci et al. [72] and Dehkordi et al. [73] proved that introducing PMR for students during their first clinical experiences helps to relieve stress and contributes to their professional development. Some studies have even recommended that PMR should accompany all formal nursing education in order to encourage greater satisfaction and a positive outlook on their study [74]. So, since a correlation between the pre-examination cortisol level and the frequency/using the PMR guidelines has been proven (k=0.416138), it suggests that students with high pre-exam cortisol and high stress had a greater willingness to apply the guidelines. This shows that the students are aware of the stressful situation they are in and are willing to use relaxation methods to ease their stress, and at the same time work on themselves and their health. Therefore, we support implementation of such useful methods being implemented in the curricula and practices of all biomedical studies, including medicine and dentistry, as these undergraduates often experience significant symptoms of stress due to the lengthy duration and demands of their studies [5,6,7].
Understanding the impact of AS on the organism and the complex relationship of stress-induced interactions between psychological and neuroimmunological factors can help identify students who are prone to AS. If they can be identified early on in their studies, they can be introduced to healthy coping methods before the possible onset of PNE changes that contribute to the development of stress-associated conditions (e.g., cardiovascular, autoimmune and other diseases) [75,76,77,78]. According to the literature data so far, this population is susceptible to stress even after graduation, and therefore it is important to educate them on how to reduce the impact of stress on the body [21]. Since stress affects immune changes and is an important risk factor for many pathological conditions, reducing stress would not only benefit dental and medical students and professionals, but also the entire communities they serve by creating a healthier, more stable healthcare system. Ours is the first study that looked at AS from the aspect of psychoneuroendocrinology, so it is necessary to continue research in this direction and find ways to make life easier for students during their university years and beyond. Despite certain limitations (a relatively small number of participants, unicentric nature), this research serves as a foundation for future multicentric studies with a larger number of participants.
5. Conclusions
This prospective and interventional research has shown that students exhibited a difference in salivary cortisol levels right before exams and after a period without exams. They also exhibited a difference in perceived stress levels (PSS) between the sexes (although there was no difference in pre-exam salivary cortisol levels by gender). In addition, a difference in students’ perceived stress levels (PSS) was also observed when comparing them by Fisher’s primary temperament types (also without a difference in their pre-exam salivary cortisol levels). Finally, our results indicate that using the PMR relaxation technique reduces cortisol values in students exposed to academic stress.
Author Contributions
Conceptualization, B.Š. and L.L.-M.; methodology, B.Š., D.C. and L.L.-M.; software, B.Š., L.Š. and L.L-M.; validation, B.Š., L.Š. and L.L-M.; formal analysis, B.Š., L.Š., M.V. and L.L-M.; investigation, B.Š., M.H. and L.L-M.; resources, L.L.-M.; data curation, B.Š., L.Š. and M.H.; writing—original draft preparation, B.Š., L.Š. and L.L-M.; writing—review and editing, B.Š., L.Š., M.V., M.H., D.C. and L.L-M.; visualization, L.Š.; supervision, L.L-M.; project administration, B.Š., M.V., D.C. and L.L.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committees of SMUHC and the School of Dental Medicine, Zagreb, Croatia (class: 003-06/21-03/016 and 05-PA-30-XXIX-9/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Knowles, S. R.; Nelson, E. A.; Palombo, E. A. Investigating the Role of Perceived Stress on Bacterial Flora Activity and Salivary Cortisol Secretion: A Possible Mechanism Underlying Susceptibility to Illness. Biol. Psychol. 2008, 77, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Jemmott, J. B., III; Magloire, K. Academic Stress, Social Support, and Secretory Immunoglobulin A. J. Pers. Soc. Psychol. 1988, 55, 803–810. [Google Scholar] [CrossRef]
- Mocny-Pachońska, K.; Doniec, R.; Trzcionka, A.; Pachoński, M.; Piaseczna, N.; Sieciński, S.; Osadcha, O.; Łanowy, P.; Tanasiewicz, M. Evaluating the Stress-Response of Dental Students to the Dental School Environment. PeerJ 2020, 8, e8981. [Google Scholar] [CrossRef]
- Sangiorgio, J. P. M.; Seixas, G. F.; Ramos, S. de Paula; Dezan-Garbelini, C. C. Salivary Levels of SIgA and Perceived Stress Among Dental Students. J. Health Biol. Sci. 2018, 6, 9–16. [Google Scholar] [CrossRef]
- Manolova, M. S.; Stefanova, V. P.; Manchorova-Veleva, N. A.; Panayotov, I. V.; Levallois, B. , et al. A Five-Year Comparative Study of Perceived Stress Among Dental Students at Two European Faculties. Folia Med. (Plovdiv) 2019, 61, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Ouda, S.; Sumer, A.; Safi, M.-A.; Nadhreen, A.; Al-Johani, K. Salivary Stress Biomarkers- Are They Predictors of Academic Assessment Exams Stress? J. Clin. Exp. Pathol. 2016, 15, 276–279. [Google Scholar]
- Pani, S. C.; Al Askar, A. M.; Al Mohrij, S. I.; Al Ohali, T. A. Evaluation of Stress in Final-Year Saudi Dental Students Using Salivary Cortisol as a Biomarker. J. Dent. Educ. 2011, 75, 377–384. [Google Scholar] [CrossRef]
- Dhama, K.; Latheef, S. K.; Dadar, M.; Samad, H. A.; Munjal, A.; Khandia, R. , et al. Biomarkers in Stress Related Diseases/Disorders: Diagnostic, Prognostic, and Therapeutic Values. Front Mol Biosci. 2019, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- Kojima, R.; Matsuda, A.; Nomura, I.; Matsubara, O.; Nonoyama, S.; Ohya, Y. , et al. Salivary Cortisol Response to Stress in Young Children with Atopic Dermatitis. Pediatr. Dermatol. 2013, 30, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Singh, S.; Vir, D.; Pershad, D. Automation of Stress Recognition Using Subjective or Objective Measures. Psychol. Stud. 2016, 61, 348–364. [Google Scholar] [CrossRef]
- AlSarhan, M. A.; AlJasser, R. N.; AlOraini, S.; Habib, S. R.; Alayoub, R. A.; Almutib, L. T.; Aldokhi, H. D.; AlKhalaf, H. H. Evaluation and Comparison of Cortisol Levels in Saliva and Hair Among Dental Students. Appl. Sci. 2023, 13, 678. [Google Scholar] [CrossRef]
- Hellhammer, D. H.; Wust, S.; Kudielka, M. B. Salivary Cortisol as a Biomarker in Stress Research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Meštrović-Štefekov, J.; Lugović-Mihić, L.; Hanžek, M.; Bešlić, I.; Japundžić, I.; Karlović, D. Salivary Cortisol Values and Personality Features of Atopic Dermatitis Patients: A Prospective Study. Dermatitis. [CrossRef]
- Inder, W. J.; Dimeski, G.; Russel, A. Measurement of Salivary Cortisol in 2012-Laboratory Techniques and Clinical Investigations. Clin. Endocrinol. 2012, 77, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, J. C.; Wolf, O. T.; Hellhammer, D. H.; Buske-Kirschbaum, A.; von Auer, K.; Jobst, S. , et al. Free Cortisol Levels After Awakening: A Reliable Biological Marker for the Assessment of Adrenocortical Activity. Life Sci. 1997, 61, 2539–2549. [Google Scholar] [CrossRef]
- Kudielka, B. M.; Hellhammer, D. H.; Wurs, S. Why Do We Respond So Differently? Reviewing Determinants of Human Salivary Cortisol Responses to Challenge. Psychoneuroendocrinology 2009, 34, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Grossi, G.; Ahs, A.; Lundberg, U. Psychological Correlates of Salivary Cortisol Secretion Among Unemployed Men and Women. Integr Physiol Behav Sci 1998, 33, 249–263. [Google Scholar] [CrossRef]
- Schommer, N. C.; Kudielka, B. M.; Hellhammer, D. H.; Kirschbaum, C. No Evidence for a Close Relationship Between Personality Traits and Circadian Cortisol Rhythm or a Single Cortisol Stress Response. Psychol. Rep. 1999, 84, 840–842. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Mason, J.; Charney, D.; Yehuda, R.; Riney, S.; Southwick, S. Relationships Between Hormonal Profile and Novelty Seeking in Combat-Related Posttraumatic Stress Disorder. Biol. Psychiatry 1997, 41, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Navazesh, M.; Kumar, S. K. Measuring Salivary Flow: Challenges and Opportunities. J. Am. Dent. Assoc. 2008, 139, 35S–40S. [Google Scholar] [CrossRef]
- Špiljak, B.; Vilibić, M.; Glavina, A.; Crnković, M.; Šešerko, A.; Lugović-Mihić, L. A Review of Psychological Stress Among Students and Its Assessment Using Salivary Biomarkers. Behav. Sci. (Basel) 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Suh, M. Salivary Cortisol Profile Under Different Stressful Situations in Female College Students: Moderating Role of Anxiety and Sleep. J. Neurosci. Nurs. 2018, 50, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Schoofs, D.; Hartmann, R.; Wolf, O. T. Neuroendocrine Stress Responses to an Oral Academic Examination: No Strong Influence of Sex, Repeated Participation and Personality Traits. Stress 2008, 11, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Ringeisen, T.; Lichtenfeld, S.; Becker, S.; Minkley, N. Stress Experience and Performance During an Oral Exam: The Role of Self-Efficacy, Threat Appraisals, Anxiety, and Cortisol. Anxiety Stress Coping 2019, 32, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Pancheri, P.; Biondi, M. In: Leonard, B. E.; Miller, K., Eds. Stress, The Immune System and Psychiatry. Wiley: New York, 1994; pp. 86–111. [Google Scholar]
- Cortisol Saliva Test Instruction. (written on the attached paper prepared for ELISA for salivary cortisol measurement, supplied by the manufacturer).
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H. E.; Island, H. D.; Rich, J.; Marchalik, D.; Brown, L. L. Four Broad Temperament Dimensions: Description, Convergent Validation Correlations, and Comparison with the Big Five. Front Psychol. 2015, 6, 1098. [Google Scholar] [CrossRef] [PubMed]
- Bottaccioli, A. G.; Bottaccioli, F.; Carosella, A.; Cofini, V.; Muzi, P.; Bologna, M. Psychoneuroendocrinoimmunology-Based Meditation (PNEIMED) Training Reduces Salivary Cortisol Under Basal and Stressful Conditions in Healthy University Students: Results of a Randomized Controlled Study. Explore (NY) 2020, 16, 189–198. [Google Scholar] [CrossRef]
- Koschel, T. L.; Young, J. C.; Navalta, J. W. Examining the Impact of a University-Driven Exercise Programming Event on End-of-Semester Stress in Students. Int J Exerc Sci. 2017, 10, 754–763. [Google Scholar] [PubMed]
- Mackereth, P. A.; Tomlinson, L. Progressive Muscle Relaxation: A Remarkable Tool for Therapists and Patients, Integrative Hypnotherapy. In Cawthorn, A.; Mackereth, P. A., Eds. Integrative Hypnotherapy. Churchill Livingstone: Edinburgh, Scotland, 2010; pp. 82–96. [Google Scholar]
- Zargarzadeh, M.; Shirazi, M. The Effect of Progressive Muscle Relaxation Method on Test Anxiety in Nursing Students. Iranian Journal of Nursing and Midwifery Research. 2014, 19, 607–611. [Google Scholar] [PubMed]
- Toussaint, L.; Nguyen, Q. A.; Roettger, C.; Dixon, K.; Offenbächer, M.; Kohls, N. , et al. Effectiveness of Progressive Muscle Relaxation, Deep Breathing, and Guided Imagery in Promoting Psychological and Physiological States of Relaxation. Evid Based Complement Alternat Med. 2021, 2021, 5924040. [Google Scholar] [CrossRef] [PubMed]
- Lowe, G.; Urquhart, J.; Greenman, J. Academic Stress and Secretory Immunoglobulin A. Psychol Rep. 2000, 87, 721–722. [Google Scholar] [CrossRef]
- Lacey, K.; Zaharia, M. D.; Griffiths, J.; Ravindran, A. V.; Merali, Z.; Anisman, H. A Prospective Study of Neuroendocrine and Immune Alterations Associated with the Stress of an Oral Academic Examination Among Graduate Students. Psychoneuroendocrinology 2000, 25, 339–356. [Google Scholar] [CrossRef] [PubMed]
- Heath, J. R.; MacFarlane, T. V.; Umar, M. S. Perceived Sources of Stress in Dental Students. Dent Update. 1999, 26, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A. E.; Lushington, K. Sources of Stress for Australian Dental Students. J. Dent. Educ. 1999, 63, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P. P. N. S.; de Souza Ferreira, F.; Pazos, J. M. Stress Among Dental Students Transitioning from Remote Learning to Clinical Training During Coronavirus Disease 2019 Pandemic: A Qualitative Study. J. Dent. Educ. 2022, 86, 1498–1504. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Dagli, R. J.; Mathur, A.; Jain, M.; Prabu, D.; Kulkarni, S. Perceived Sources of Stress Amongst Indian Dental Students. Eur J Dent Educ. 2009, 13, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Morse, Z.; Dravo, U. Stress Levels of Dental Students at the Fiji School of Medicine. Eur J Dent Educ. 2007, 11, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Muirhead, V.; Locker, D. Canadian Dental Students’ Perceptions of Stress. J. Can. Dent. Assoc. 2007, 73, 323. [Google Scholar] [PubMed]
- Polychronopoulou, A.; Divaris, K. A Longitudinal Study of Greek Dental Students’ Perceived Sources of Stress. J. Dent. Educ. 2010, 74, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Rosli, T. I.; Abdul Rahman, R.; Abdul Rahman, S. R.; Ramli, R. A Survey of Perceived Stress Among Undergraduate Dental Students in Universiti Kebangsaan Malaysia. Singapore Dent J. 2005, 27, 17–22. [Google Scholar]
- Pohlmann, K.; Jonas, I.; Ruf, S.; Harzer, W. Stress, Burnout and Health in the Clinical Period of Dental Education. Eur. J. Dent. Educ. 2005, 9, 78–84. [Google Scholar] [CrossRef]
- Westerman, G. H.; Grandy, T. G.; Ocanto, R. A.; Erskine, C. G. Perceived Sources of Stress in the Dental School Environment. J. Dent. Educ. 1993, 57, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Frankenhaeuser, M.; von Wright, M. R.; Collins, A.; von Wright, J.; Sedvall, G.; Swahn, C. G. Sex Differences in Psychoneuroendocrine Reactions to Examination Stress. Psychosom. Med. 1978, 40, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Kudielka, B. M.; Gaab, J.; Schommer, N. C.; Hellhammer, D. H. Impact of Gender, Menstrual Cycle Phase, and Oral Contraceptives on the Activity of the Hypothalamus-Pituitary-Adrenal Axis. Psychosom. Med. 1999, 61, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Carter-Snell, C.; Hegadoren, K. Stress Disorders and Gender: Implications for Theory and Research. CJNR (Canadian Journal of Nursing Research) 2003, 35, 34–55. [Google Scholar]
- Gater, R.; Tansella, M.; Korten, A.; Tiemens, B. G.; Mavreas, V. G.; Olatawura, M. O. Sex Differences in the Prevalence and Detection of Depressive and Anxiety Disorders in General Health Care Settings: Report from the World Health Organization Collaborative Study on Psychological Problems in General Health Care. Arch Gen Psychiatry. 1998, 55, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Yang, A.; Zhao, Q.; Chen, Z.; Ren, X.; Dai, Q. A Hypothesis of Gender Differences in Self-Reporting Symptom of Depression: Implications to Solve Under-Diagnosis and Under-Treatment of Depression in Males. Front Psychiatry. 2021, 12, 589687. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M. M.; Tyrka, A. R.; Anderson, G. M.; Price, L. H.; Carpenter, L. L. Sex Differences in Emotional and Physiological Responses to the Trier Social Stress Test. J. Behav. Ther. Exp. Psychiatry. 2008, 39, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M. M.; Forsyth, J. P.; Karekla, M. Sex Differences in Response to a Panicogenic Challenge Procedure: An Experimental Evaluation of Panic Vulnerability in a Non-Clinical Sample. Behav. Res. Ther. 2006, 44, 1421–1430. [Google Scholar] [CrossRef] [PubMed]
- Graves, B. S.; Hall, M. E.; Dias-Karch, C.; Haischer, M. H.; Apter, C. Gender Differences in Perceived Stress and Coping Among College Students. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Khaksari, M.; Mahmoodi, M.; Rezvani, M. E.; Sajjadi, M. A.; Karam, G. A.; Hajizadeh, S. Differences Between Male and Female Students in Cardiovascular and Endocrine Responses to Examination Stress. J. Ayub Med. Coll. Abbottabad. 2005, 17, 15–19. [Google Scholar] [PubMed]
- Singh, R.; Goyal, M.; Tiwari, S.; Ghildiyal, A.; Nattu, S. M.; Das, S. Effect of Examination Stress on Mood, Performance and Cortisol Levels in Medical Students. Indian J. Physiol. Pharmacol. 2012, 56, 48–55. [Google Scholar] [PubMed]
- Martinek, L.; Oberascher-Holzinger, K.; Weishuhn, S.; Klimesch, W.; Kerschbaum, H. H. Anticipated Academic Examinations Induce Distinct Cortisol Responses in Adolescent Pupils. Neuro Endocrinol. Lett. 2003, 24, 449–453. [Google Scholar] [PubMed]
- Batabyal, A.; Bhattacharya, A.; Thaker, M.; Mukherjee, S. A Longitudinal Study of Perceived Stress and Cortisol Responses in an Undergraduate Student Population from India. PLoS One. 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Verschoor, E.; Markus, C. R. Affective and Neuroendocrine Stress Reactivity to an Academic Examination: Influence of the 5-HTTLPR Genotype and Trait Neuroticism. Biological Psychology. 2011, 87, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Glaser, R.; Pearl, D. K.; Kiecolt-Glaser, J. K.; Malarkey, W. B. Plasma Cortisol Levels and Reactivation of Latent Epstein-Barr Virus in Response to Examination Stress. Psychoneuroendocrinology. 1994, 19, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Vedhara, K.; Hyde, J.; Gilchrist, I. D.; Tytherleigh, M.; Plummer, S. Acute Stress, Memory, Attention and Cortisol. Psychoneuroendocrinology. 2000, 25, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Preuss, D.; Schoofs, D.; Schlotz, W.; Wolf, O. T. The Stressed Student: Influence of Written Examinations and Oral Presentations on Salivary Cortisol Concentrations in University Students. Stress. 2010, 13, 221–229. [Google Scholar] [CrossRef]
- Hammerfald, K.; Eberle, C.; Grau, M.; Kinsperger, A.; Zimmermann, A.; Ehlert, U. , et al. Persistent Effects of Cognitive-Behavioral Stress Management on Cortisol Responses to Acute Stress in Healthy Subjects--A Randomized Controlled Trial. Psychoneuroendocrinology 2006, 31, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Denson, T. F.; Spanovic, M.; Miller, N. Cognitive Appraisals and Emotions Predict Cortisol and Immune Responses: A Meta-Analysis of Acute Laboratory Social Stressors and Emotion Inductions. Psychol. Bull. 2009, 135, 823–853. [Google Scholar] [CrossRef] [PubMed]
- Lackschewitz, H.; Hüther, G.; Kröner-Herwig, B. Physiological and Psychological Stress Responses in Adults with Attention-Deficit/Hyperactivity Disorder (ADHD). Psychoneuroendocrinology 2008, 33, 612–624. [Google Scholar] [CrossRef] [PubMed]
- Oldehinkel, A. J.; Ormel, J.; Bosch, N. M.; Bouma, E. M.; Van Roon, A. M.; Rosmalen, J. G.; Riese, H. Stressed Out? Associations Between Perceived and Physiological Stress Responses in Adolescents: The TRAILS Study. Psychophysiology 2011, 48, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Schlotz, W.; Kumsta, R.; Layes, I.; Entringer, S.; Jones, A.; Wüst, S. Covariance Between Psychological and Endocrine Responses to Pharmacological Challenge and Psychosocial Stress: A Question of Timing. Psychosom. Med. 2008, 70, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H. E.; Rich, J.; Island, H. D.; Marchalick, D.; Silver, L. Do We Have Chemistry? Four Primary Temperament Dimensions on Mate Choice. [Conference presentation]. APA 2010, San Diego, United States.
- Lucić, A.; Šimić, N. Testing the Fisher’s Temperament Model on a Croatian Sample. In: A. Tokić (Ed.), 21st Psychology Days in Zadar – Book of Selected Proceedings, pp. 97–108. Zadar: University in Zadar.
- Pruessner, J. C.; Gaab, J.; Hellhammer, D. H.; Lintz, D.; Schommer, N.; Kirschbaum, C. Increasing Correlations Between Personality Traits and Cortisol Stress Responses Obtained by Data Aggregation. Psychoneuroendocrinology 1997, 22, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Oswald, L. M.; Zandi, P.; Nestadt, G.; Potash, J. B.; Kalaydjian, A. E.; Wand, G. S. Relationship Between Cortisol Responses to Stress and Personality. Neuropsychopharmacology 2006, 31, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Pv, J.; Lobo, S. M. Effectiveness of Relaxation Technique in Reducing Stress Among Nursing Students. International Journal of Nursing and Health Research 2020, 2, 54–56. [Google Scholar]
- Arabaci, L. B.; Korhan, E. A.; Tokem, Y.; Torun, R. Pre-clinical and Postclinical Anxiety and Stress Levels of First-Year Nursing Students and Factors Affecting Them. Ankara, Turkey: Hacettepe University Nursing Faculty Journal; 2015:1-16.
- Dehkordi, A. H.; Masoudi, R.; Tali, S. S.; Frouzandeh, N.; Naderipour, A.; Pourmirzakalhori, R. , et al. The Effect of Progressive Muscle Relaxation on Anxiety and Stress in Nursing Students at the Beginning of the Internship Program. Journal of Shahrekord University of Medical Sciences 2009, 11, 71–77. [Google Scholar]
- Manansingh, S.; Tatum, S. L.; Morote, E. S. Effects of Relaxation Techniques on Nursing Students’ Academic Stress and Test Anxiety. J. Nurs. Educ. 2019, 58, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Blagec, T.; Glavina, A.; Špiljak, B.; Bešlić, I.; Bulat, V.; Lugović-Mihić, L. Cheilitis: A Cross-Sectional Study-Multiple Factors Involved in the Aetiology and Clinical Features. Oral Dis. 3360. [Google Scholar]
- Lugović-Mihić, L.; Špiljak, B.; Blagec, T.; Delaš Aždajić, M.; Franceschi, N.; Gašić, A.; Parać, E. Factors Participating in the Occurrence of Inflammation of the Lips (Cheilitis) and Perioral Skin. Cosmetics 2023, 10, 9. [Google Scholar] [CrossRef]
- Parać, E.; Špiljak, B.; Lugović-Mihić, L.; Bukvić Mokos, Z. Acne-like Eruptions: Disease Features and Differential Diagnosis. Cosmetics 2023, 10, 89. [Google Scholar] [CrossRef]
- Japundžić, I.; Bembić, M.; Špiljak, B.; Parać, E.; Macan, J.; Lugović-Mihić, L. Work-Related Hand Eczema in Healthcare Workers: Etiopathogenic Factors, Clinical Features, and Skin Care. Cosmetics 2023, 10, 134. [Google Scholar] [CrossRef]
Figure 1.
Hodogram (a simplified roadmap) of the prospective and interventional research.
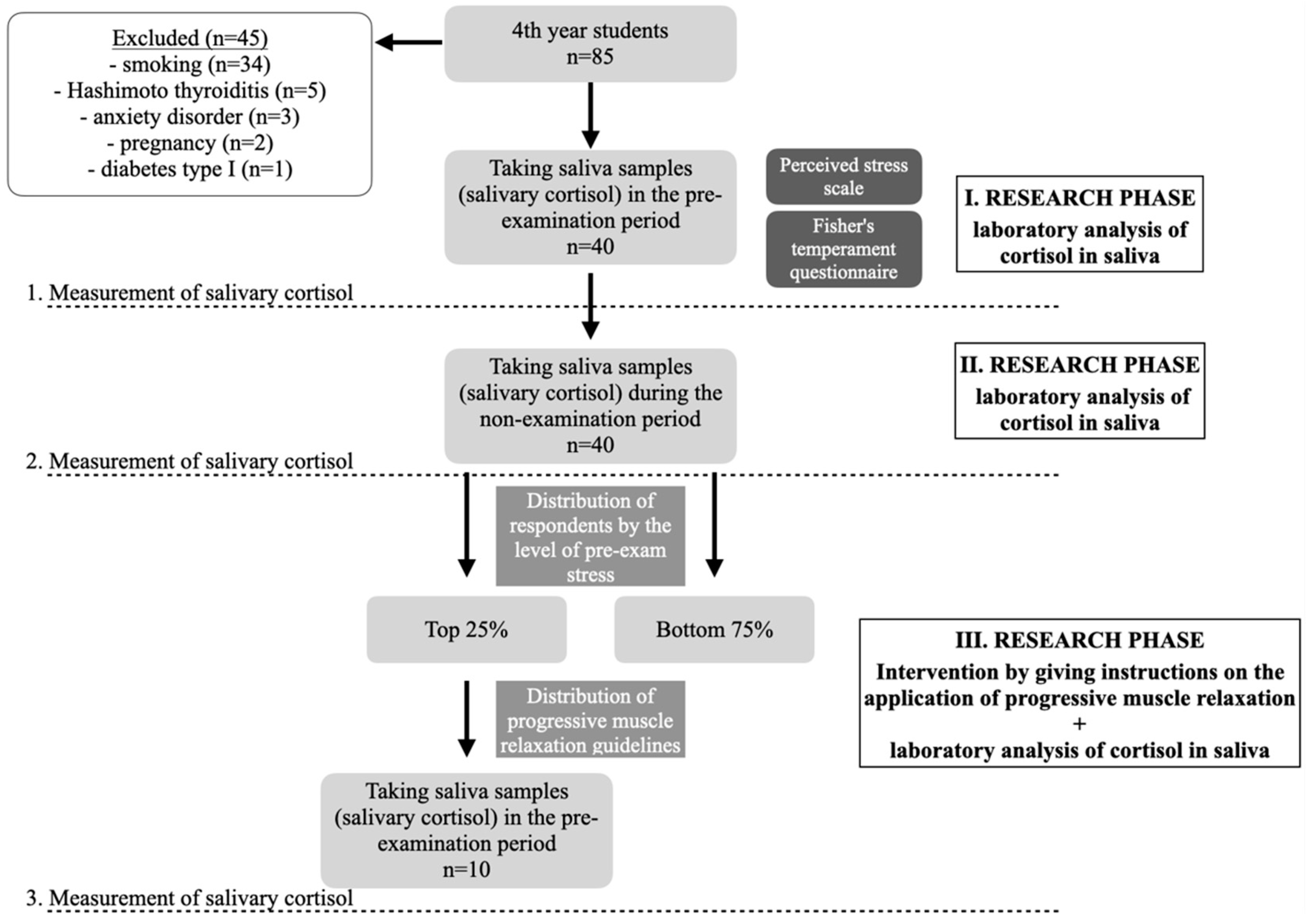
Figure 2.
Comparison of stress levels (PSS) between genders; *indicates statistically significant dana [Mann-Whitney U test, U=99.5, Z adjusted = -2.021, 2*1 sided exact p =0.042].
Figure 2.
Comparison of stress levels (PSS) between genders; *indicates statistically significant dana [Mann-Whitney U test, U=99.5, Z adjusted = -2.021, 2*1 sided exact p =0.042].
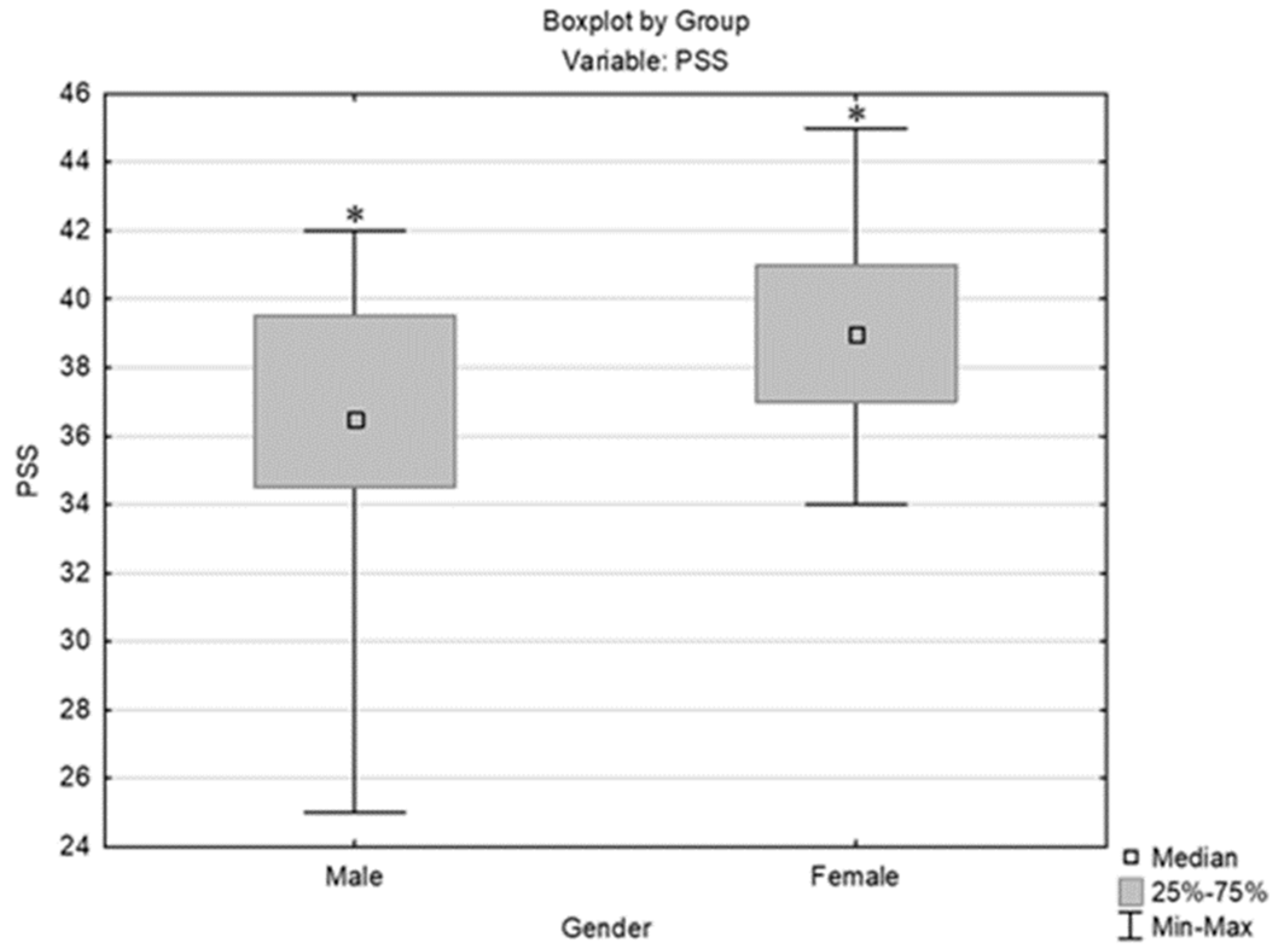
Figure 3.
Comparison of stress level (PSS) by temperament (FTI); *indicates statistically significant data [Kruskal-Wallis test: H (3, N= 40) =8.933, p =0.0302; post hoc Dunn’s test p=0.029].
Figure 3.
Comparison of stress level (PSS) by temperament (FTI); *indicates statistically significant data [Kruskal-Wallis test: H (3, N= 40) =8.933, p =0.0302; post hoc Dunn’s test p=0.029].
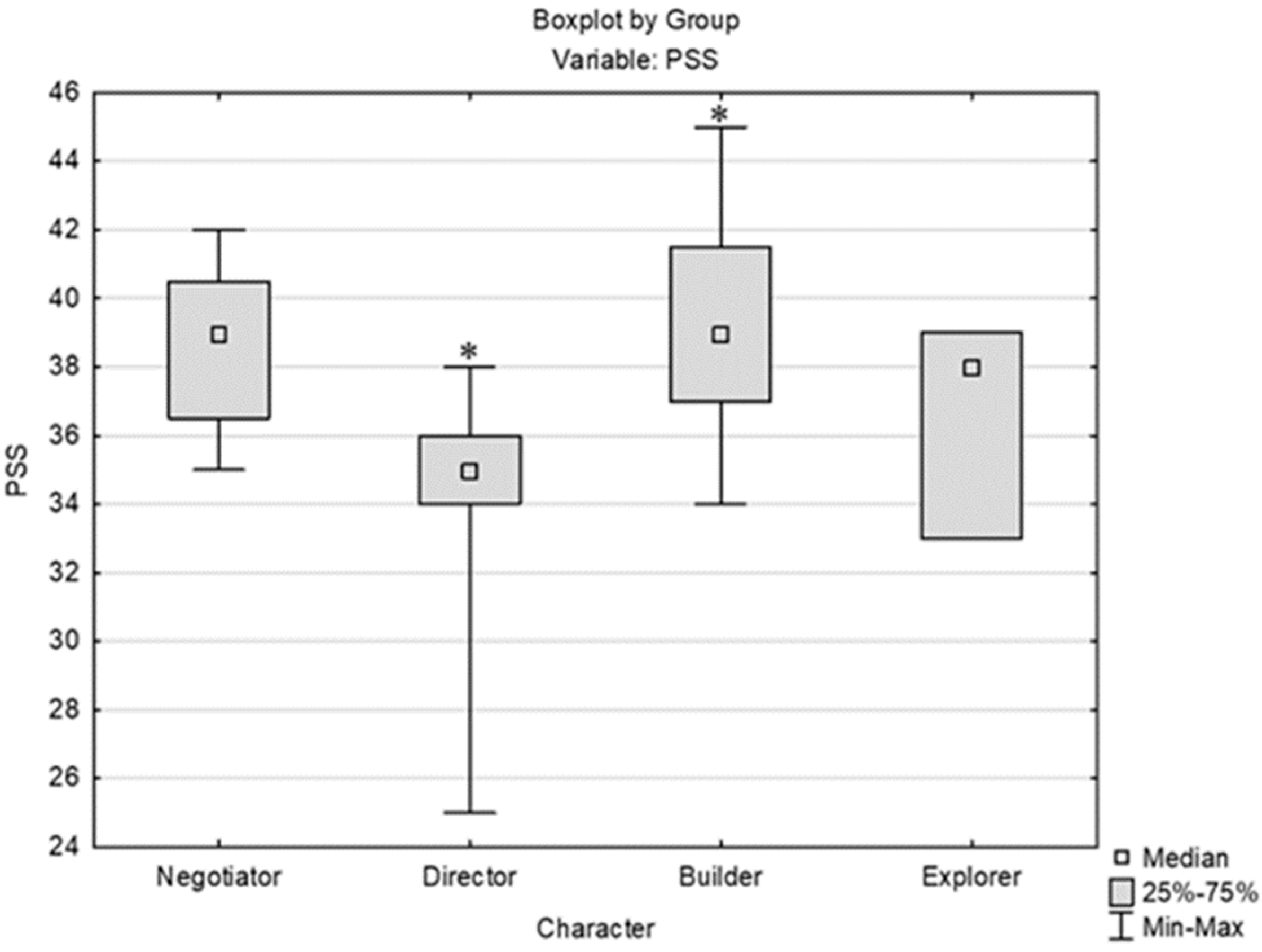
Figure 4.
Comparison of pre-test cortisol levels (ng/mL) between genders [Mann-Whitney U test, U=139.5, Z adjusted = -0.827, 2*1 sided exact p =0.405].
Figure 4.
Comparison of pre-test cortisol levels (ng/mL) between genders [Mann-Whitney U test, U=139.5, Z adjusted = -0.827, 2*1 sided exact p =0.405].
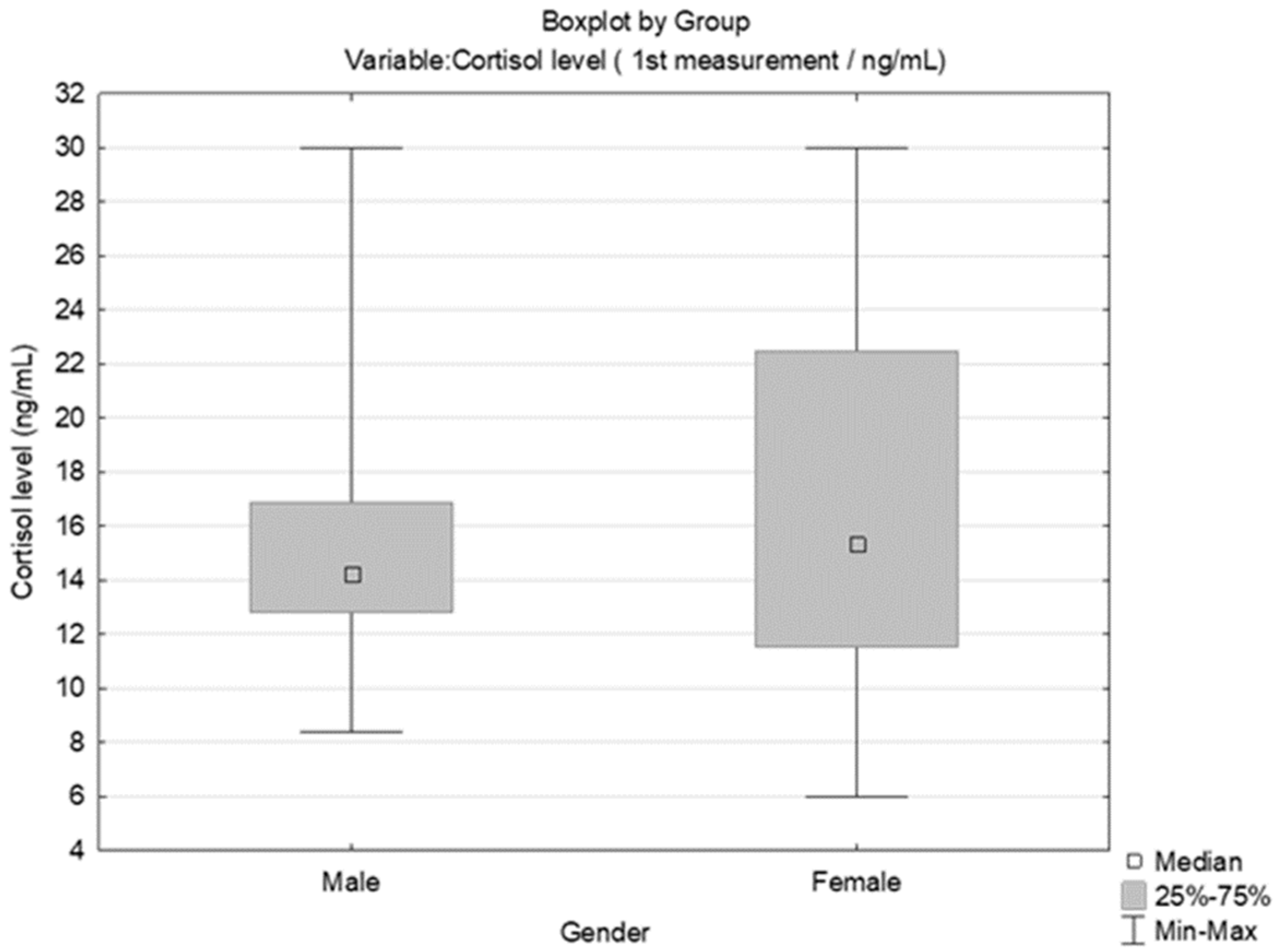
Figure 5.
Comparison of pre-exam cortisol levels (ng/mL) by the Fisher scale of temperament types [Kruskal-Wallis test: H (3, N= 40) =2.335, p =0.5058].
Figure 5.
Comparison of pre-exam cortisol levels (ng/mL) by the Fisher scale of temperament types [Kruskal-Wallis test: H (3, N= 40) =2.335, p =0.5058].
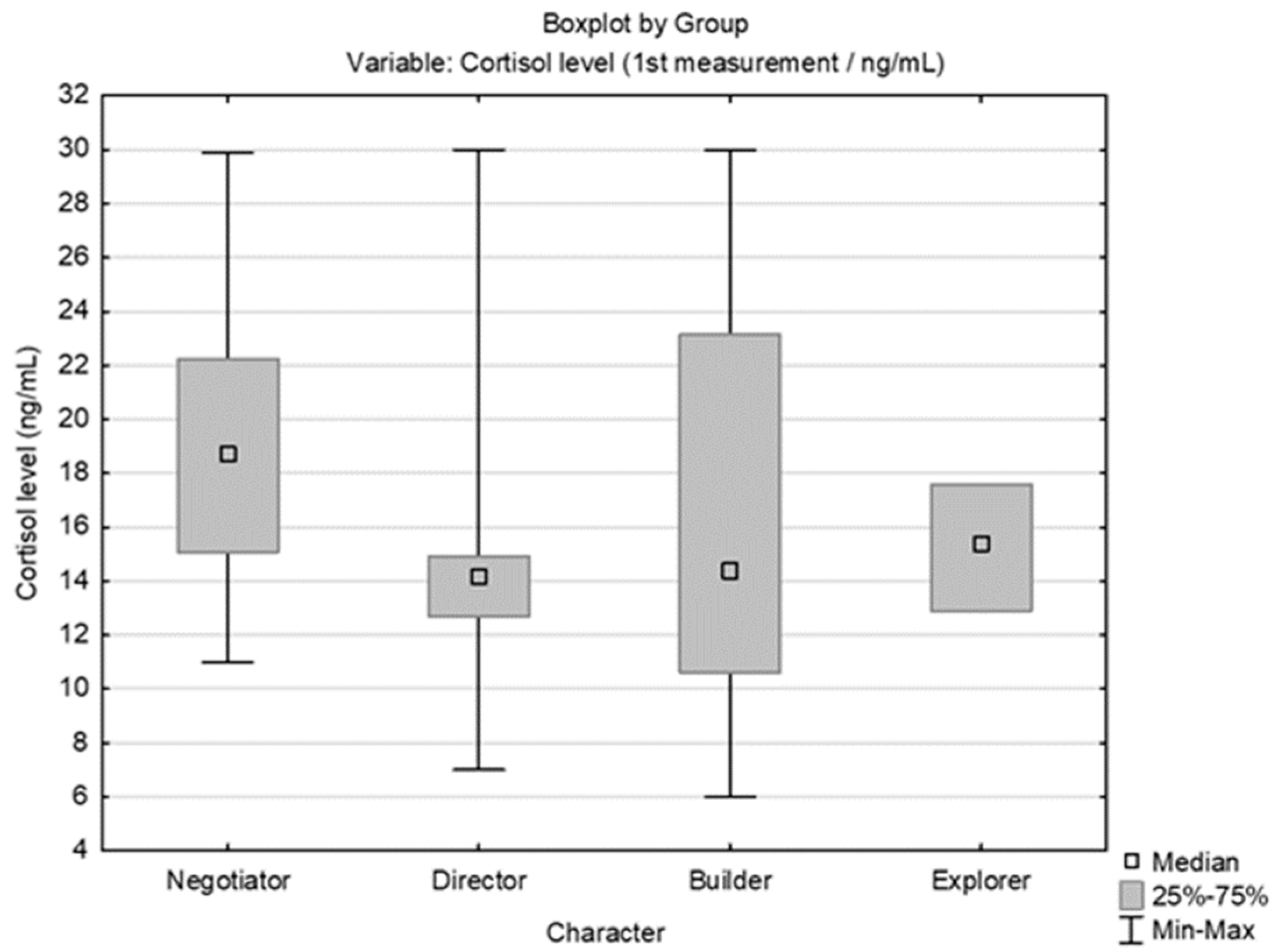
Figure 6.
Comparison of the three cortisol measurements (pre-exam; non-exam period after summer vacation; and after PMI (25% of students who had the highest cortisol level at first measurement) *indicates statistically heterogenous data, p<0,05 (Wilcoxon match paired test) [Friedman ANOVA and Kendall Coeff. of Concordance; ANOVA Chi Sqr. (N = 10, df = 2) = 20.00 p = 0.00005; Coeff. of Concordance = 1, Aver. rank r = 1].
Figure 6.
Comparison of the three cortisol measurements (pre-exam; non-exam period after summer vacation; and after PMI (25% of students who had the highest cortisol level at first measurement) *indicates statistically heterogenous data, p<0,05 (Wilcoxon match paired test) [Friedman ANOVA and Kendall Coeff. of Concordance; ANOVA Chi Sqr. (N = 10, df = 2) = 20.00 p = 0.00005; Coeff. of Concordance = 1, Aver. rank r = 1].
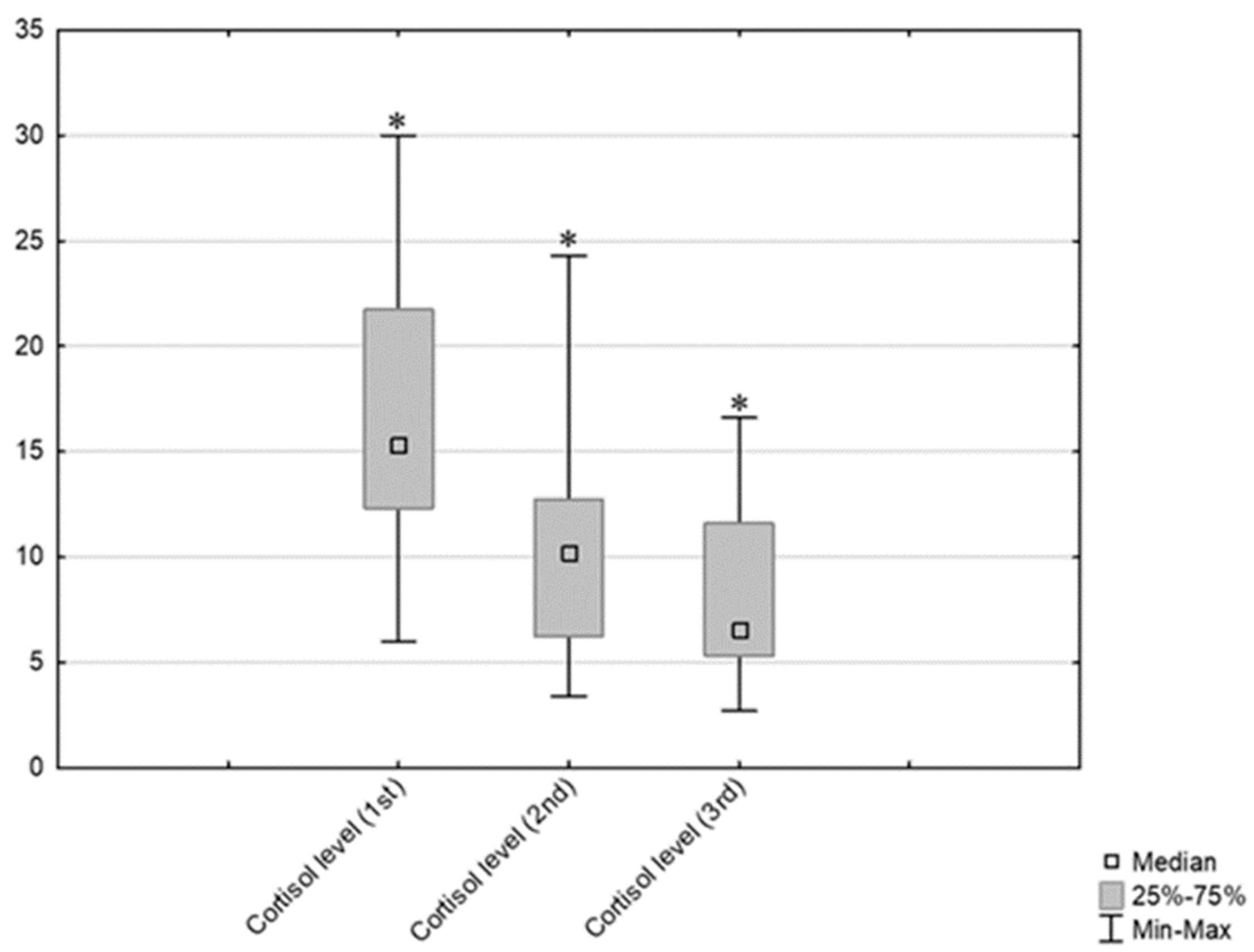
Figure 7.
Distribution of grades (oral exam) according to gender.
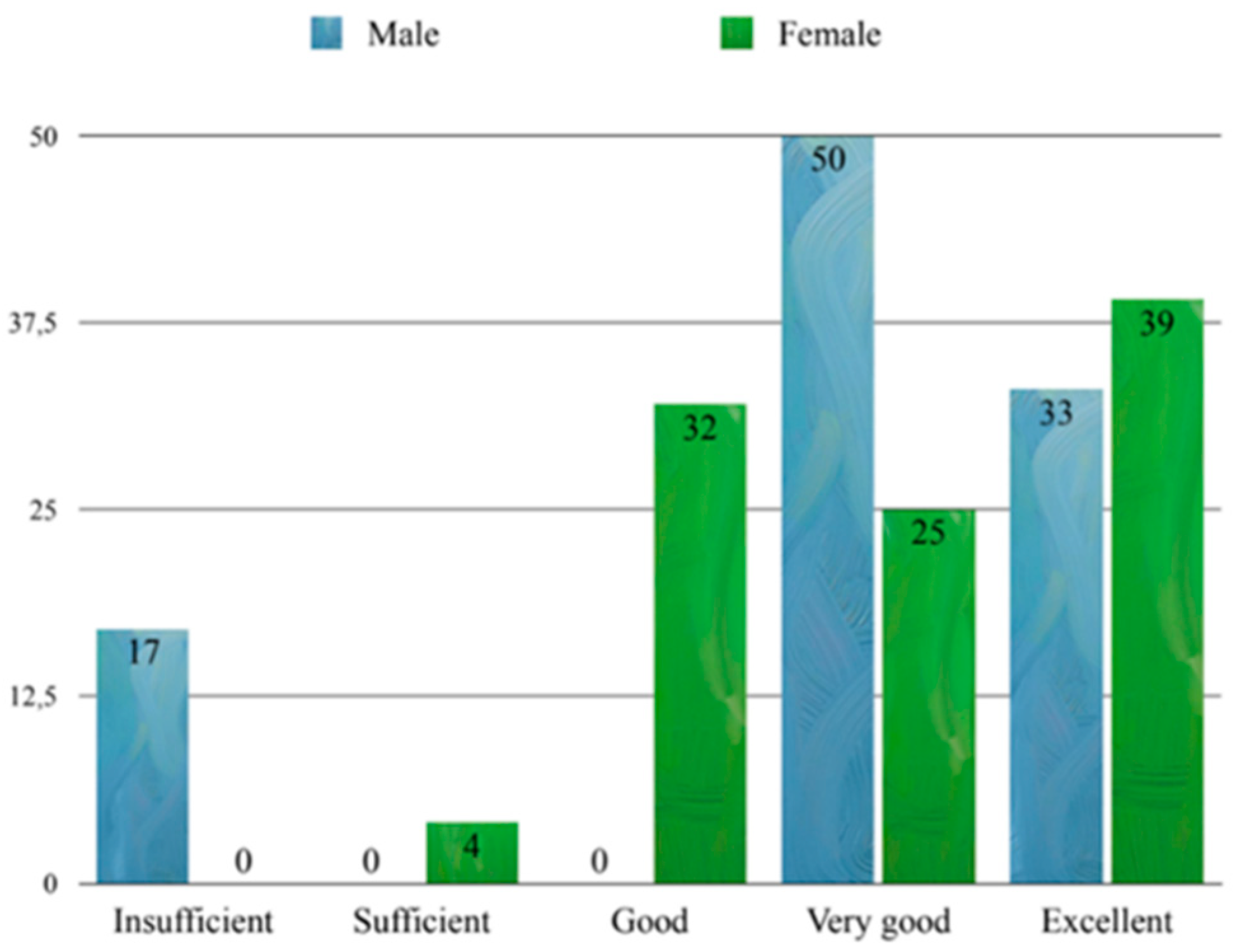
Figure 8.
Distribution of grades (oral exam) by Fisher’s primary types of temperament.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



