
Submitted:
21 February 2024
Posted:
21 February 2024
You are already at the latest version
Abstract
Ischemic stroke is one of the leading causes of death and permanent disability in the world. Rapid diagnosis and intervention are crucial for reducing its consequences on individuals and societies. Identifying reliable biomarkers for early detection, prognostics and therapy is a criti-cal imperative for improving the stroke patient treatment. Metabolomics has been shown as a promising tool for biomarker discovery since many of the post-ischemic metabolites can found in the plasma or serum of the patient. In this research, we have performed comparative targeted metabolomic analysis of stroke thrombi, patient serums and healthy control serums in order to determine the alteration in the patients’ metabolome. The most statistically altered metabolites characterized in patient compared to control serums were glutamate and serotonin, followed by several lipid metabolites (phospholipids and triacylglycerols) and glucose. In stroke thrombi compared to patient’s serums, the most significantly altered metabolites were classified as li-pids, with choline-containing phospholipids and sphingomyelins having the highest discrimi-natory score. The results of this study could help in understanding the roles of different meta-bolic changes occurring during thrombosis and cerebral ischemia and possibly suggest new metabolic biomarkers of the ischemic stroke.
Keywords:
ischemic stroke
; stroke thrombi
; targeted metabolomics
; metabolic biomarkers
1. Introduction
Stroke remains one of the leading causes of death and permanent disability in the world, with ischemic stroke (IS) representing over 80-85% of all incident strokes [1]. The stroke frequency is expected to grow with the increasing age of the population [2]. Rapid diagnosis and intervention are essential in the reduction of mortality and morbidity [3].
Mechanical thrombectomy (MT) is an endovascular procedure involving recanalization of an intracranial occlusion by removing a thrombus using a retrievable stent or aspiration catheter [4]. Until the development of MT in 2015, intravenous thrombolysis was the only medical therapy shown to improve patient outcomes in acute ischemic stroke [5], but with narrow treatment window and numerous complications ranging from brain haemorrhage, cardiac complications, seizures and deep vein thrombosis in later stages of treatment [6]. The composition and structural organization of the stroke thrombi was not researched until recent years due to unavailability of the thrombus material. The development of MT has enabled the retrieval of stroke thrombi and allowed the possibility of detailed analysis of the thrombi composition [7].
Metabolomics is a key tool for analysing end products of cellular metabolism which serve as dynamic and sensitive indicators of physiological distress, reflecting the interaction between genetic predispositions, environmental factors and disease states [8]. Recently the increased research interest in metabolomics of cerebrovascular diseases and stroke has identified altered serum metabolic profiles in patients having these complex pathologies [9,10,11,12,13,14,15]. Due to the impaired integrity of the blood-brain barrier in the ischemic brain, many of the post-ischemic metabolites are more easily found in the plasma or serum of the patient [16].
Metabolomics research of stroke thrombi in IS was, to our knowledge, performed in two studies so far, done only as non-target metabolomics analysis and without comparison with patient or healthy control serums [17,18]. Therefore, metabolomics data on stroke thrombi is still very limited. In this research, we have performed detailed, targeted metabolomics analysis of stroke thrombi, corresponding patient serums and healthy control serums, with special interest on lipid metabolites due to the well-known influence of lipids in the pathology of atherosclerosis and cerebrovascular diseases. The aim of this study was to differentiate the most significant metabolites that might serve as metabolic biomarkers of the ischemic stroke. The comparative metabolomics analysis of stroke thrombi and serum metabolites could help in defining the metabolic alterations in cerebral ischemia and offer insights into the dynamic relationship between the site of injury and the systemic response in stroke pathophysiology.
2. Materials and Methods
2.1. Study subjects
Patients enrolled in the study were urgently admitted to University Hospital Centre “Zagreb“ Neurology Department and University Hospital Centre “Sestre milosrdnice” Radiology Department in Zagreb, Croatia, receiving mechanical thrombectomy (MT) with or without bridging intravenous thrombolytic therapy (IVT) between. They had been selected based on our University Centre stroke guidelines which are mainly based on European Stroke Organization (ESO) mechanical thrombectomy guidelines published in 2019 [19] and ESO thrombolysis guidelines published in 2021 [20] and ESO thrombolysis recommendation before MT published in 2022 [21].
All included patients (N = 14) were adults (> 18 years), had a focal neurologic deficit defined as at least 4 points on National Institute of Health Stroke Scale (NIHSS) and duration of symptoms up to 24 hours. The non-contrast computed tomography (CT) was used to exclude cerebral haemorrhage or other causative intracranial pathology other than ischaemia. CT angiography confirmed intracranial large vessel occlusion of the anterior or posterior circulation (internal carotid artery [ICA], carotid T, M1, M2 segments of the middle cerebral artery [MCA], A1 segment of the anterior cerebral artery [ACA], P1 segment of the posterior cerebral artery [PCA], basilar artery [BA], vertebral artery [VA]) and an Alberta Stroke Program Early CT Score (ASPECT) between 6 and 10. Patients that arrived later than 6 hours from symptom onset and underwent MT had CT perfusion imaging demonstrating core/penumbra mismatch defined as core volume less than 70 mL, critically hypoperfused volume/core ratio larger than 1, 2 and mismatch volume larger than 10 mL. Patients that received bridging IVT had symptom duration up to 4 - 5 hours or perfusion mismatch on CT perfusion imaging according to the aforementioned criteria. All the patients that received IVT were administered with alteplase (0,9 mg/kg).
Types of strokes were defined as cardioembolism, large-artery atherosclerosis or other causes based on the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification [22]. Mechanical thrombectomy was performed using all three main techniques: stent retriever technique, contact aspiration and combined technique.
Participants in the control group (N = 14) were selected from Department of Neurosurgery, University Hospital Centre “Sestre milosrdnice”, Zagreb, Croatia. The baseline assessments were conducted for all participants, including demographic information, medical history, and relevant clinical measures ensuring comparability with the stroke group as closely as possible.
In the control group, exclusion criteria included history of stroke and any other cerebrovascular events or neurological disorders (other than stroke), severe cardiovascular diseases, confirmed chronic inflammatory conditions, confirmed severe renal or hepatic diseases, uncontrolled hypertension as well as pregnancy and intake of medications that could interfere with the study outcomes.
2.2. Clinical and Biochemical Measurements
For clinical laboratory and targeted metabolomics analysis, venous blood samples were collected after 12 h fasting for control group and immediately before IVT and MT for patient group. 10 mL of venous blood was collected and centrifuged (750 × g for 15 min after 30 min at room temperature) to separate serum from cellular components. The serum aliquots were stored in glass tubes at -80°C until measurements were performed.
Biochemical parameters were measured at the Biochemistry Laboratory of University Hospital Centre “Zagreb” and University Hospital Centre “Sestre milosrdnice” in Zagreb, Croatia. Biochemical analyses of serums samples in clinical setting were involved measurement of blood glucose, lipid profile (total cholesterol [tCH], triglycerides [TG], HDL-cholesterol [HDL-CH], LDL-cholesterol [LDL-CH]) as well as coagulation profile (prothrombin time [PT], activated partial thromboplastin time [aPTT]), international normalized ratio [INR]) by standard laboratory procedures [23,24]. Weight (kg) and height (m) measurements were done in a standardized manner. Body weight (BW) was measured by standard medical balance, accurate to 0.1 kg. Body height (BH) was measured using the stadiometer with a precision of 0.1 cm. Body mass index (BMI) was calculated by standard formula BMI = BW (kg)/BH (m2). Systolic and diastolic blood pressure were measured using sphygmomanometer.
2.3. Preparation of Stroke Thrombi for Targeted Metabolomics Analysis
After MT procedure, each thrombus sample was washed with cold saline solution and stored in glass tubes at -80°C until metabolomics analysis. Collected stroke thrombi were weighted on ice and 3-fold volume of ice-cold isopropanol was used as extraction solvent (Table 1).
The samples were vortexed and sonicated on ice 3 times for 30 seconds at max amplitude. Samples were spin-down between cycles and held on ice for 1 min. After third sonication cycle, samples were vortexed for 30 sec and centrifuged at 10 000 x g for 5 min at 4°C. The supernatants were used for further analysis on AbsoluteIDQ p400 kit (Biocrates Life Science AG, Innsbruck, Austria) with mass spectrometry (Q Exactive Plus hybrid quadrupole - Orbitrap; Thermo Fisher Scientific, Bremen, Germany).
Serums and stroke thrombi samples were transported in dry ice to the Laboratory of Proteomics, Clinic for Internal Diseases, Faculty of Veterinary Medicine in Zagreb, Croatia, where targeted metabolomics analysis was performed.
2.4. Targeted Metabolomics Analysis
Concentration of 408 endogenous metabolites divided into 11 analytical classes, including amino acids (N = 21), biogenic amines (N = 21), monosaharides comprising the sum of hexoses, including glucose (N = 1), phosphatidylcholines (N = 172), lysophosphatidylcholines (N = 24), sphingomyelins (N = 31), ceramides (N = 9), diglycerides (N = 18), triglycerides (N = 42), cholesteryl esters (N = 14) and acylcarnitines (N = 55) were measured in patient serums, control serums and stroke thrombi samples with Biocrates AbsoluteIDQ p400 kit using mass spectrometry (MS) according to the manufacturer’s protocol. Metabolites were quantified using the combination of liquid chromatography-mass spectrometry (LC-MS/MS) and flow-injection analysis-mass spectrometry (FIA-MS/MS). The LC-MS/MS analysis allowed the quantification of amino acids and biogenic amines while the FIA-MS/MS was used to quantify acylcarnitines, glycerophospholipids, glycerides, hexoses, cholesteryl esters, and sphingolipids.
Sample preparation and metabolite extraction were performed according to the manufacturer instructions provided with the kit and described in detail previously [25]. In short, the 10 μL of each sample, calibration standards, blank samples (phosphate-buffered saline; BDH PROLABO, Lutterworth, UK), and three quality control samples (low, QC1; medium, QC2 and high, QC3) were prepared on the specific 96-well plate for protein removal, internal standard normalisation and derivatization. The samples were extracted using 5 mM ammonium acetate (Sigma-Aldrich, St. Louis, MO, USA) in methanol (Honeywell, Charlotte, NC, USA). Finally, extracts were diluted with the LC-MS-grade water prior to LC-MS/MS analysis and with FIA mobile phase (made by mixing 290 mL MeOH and a 10 mL ampule Biocrates FIA mobile phase additive, provided with the kit) prior to FIA-MS/MS analysis.
Mass spectrometry analysis was performed on a Dionex Ultimate 3000 UHPLC system (Thermo Fisher Scientific, Germering, Germany) coupled to a Q Exactive Plus hybrid quadrupole - Orbitrap mass spectrometer using an electrospray ionization source. A Thermo p400 HR UHPLC column provided with the kit was used to separate metabolites from the samples. The column temperature was maintained at 50°C. Mobile phase A contained 0.2 % formic acid in H2O, and B contained 0.2 % formic acid in acetonitrile. The injection volume was 5 μL. The total run time was 5.81 min, and the gradient change of 0 to 95 % of mobile phase B over 4 min. The flow rate was 0.8 mL/min.
For the FIA-MS/MS analysis, metabolites were eluted using the FIA mobile phase at a flow rate of 0.05 mL/min for the first 1.6 min, then the flow rate increased to 0.2 mL/min for 1.2 min and then decreased back to 0.05 mL/min for the end of the sequence.
The mass spectrometer was operated in positive and negative ion modes for both LC-MS/MS and FIA-MS/MS according to the instructions from Biocrates kit.
The MetIDQ software package Version Boron, an integral part of the Absolute IDQ p400 kit, was used for the data processing, quality assessment, and data export. The quantification of the LC-MS metabolites was processed via XCalibur Quan 4.1 software (Thermo Fisher Scientific, Waltham, MA, USA) based on a seven-point calibration curve and isotope labelled internal standards for most analytes, while the FIA-MS/MS analysis used a single-point calibrator with the representative internal standards. All reagents used in this analysis were of LC-MS grade and purchased from Merck (Darmstadt, Germany), Honeywell (Charlotte, NC, USA) and Sigma-Aldrich (St. Louis, MO, USA).
Blank samples were used for the calculation of the limits of detection (LOD). In terms of quantification, if the compounds were quantified with restriction, then the calibration curves had expected coefficients of determination (R2) < 0.99 according to the manufacturer guidelines. When specific standards were not commercially available and verification of the accuracy was not possible by the manufacturer, the measuring was performed “semi-quantitatively”.
2.5. Statistical Analyses
The MedCalc 22.019 (Frank Schoonjans, Mariakerke, Belgium) was used for descriptive statistical analysis and for the comparison of clinical and biochemical data between the study groups using Student’s t-test or Mann-Whitney test, depending on distribution normality.
The MetaboAnalyst v.4.0 software (http://www.metaboanalyst.ca, accessed on 15 November 2023) was used for univariate and multivariate statistical analysis of metabolites. Metabolites with 50% missing values were removed and replace by LoDs (1/5 of the minimum positive value of each variable). The concentrations of each metabolite were normalised by median, log transformed, and Pareto scaled. The overall differences in the metabolomics profile between control and patient serum samples and between patient serums and stroke thrombi were analysed by Student’s t-test, a partial least square–discriminant analysis (PLS-DA), the variable importance on projection (VIP) and hierarchical clustering analysis (HCA). For all statistical analysis a p-value ≤ 0.05 was considered to be statistically significant.
3. Results
3.1. Clinical features of study population
Clinical and laboratory parameters of study participants are shown in Table S1 and Table 2. There were no differences in DBP, SBP and BMI betwwen groups, but ishemic stroke (IS) patients were significantly older than controls (71.43±12.26 vs. 51.29±15.09). Clinical laboratory values of lipid parameters (TG, tCH, LDL-CH and HDL-CH) did not show significant differences between groups whereas glucose showed significant alterations between patient and control groups. The comparison of coagulation factors (PV, aPTV and INR) between IS and control groups revealed that there were no significant differences between groups.
3.2. Metabolomics analysis
3.2.1. Comparison of patient serums versus control serums
In order to determine differences in the serum metabolome, metabolites concentrations in ischemic stroke (IS) patient serums were compared with healthy control serums. The targeted approach (Biocrates analysis) detected 193 metabolites (above the limit of detection, LOD) between two groups (Table S2) which were classified into groups of amino acids (N = 21), biogenic amines (N = 9), hexoses, including glucose (N = 1), acylcarnitines (N = 4), cholesteryl esters (N = 6), diglycerides (N = 9), triglycerides (N = 29), lysophosphatidylcholines (N = 9), phosphatidylcholines (N = 50), ether phosphatidylcholines (N = 27), sphingomyelins (N = 26) and ceramides (N = 2). Using the MetIDQ™ software 159 lipid metabolites were relatively and 34 metabolites were absolutely quantified. The list of 193 metabolites was used for further statistical analysis.
The multivariate, partial least squares discriminant analysis (PLS-DA) was performed to identify the metabolites that were the most discriminant between patient group (N = 14) and control group (N = 14) serums (Figure 1a). This analysis showed a relatively clear intergroup separation of patient group from control group, but showing at the same time overlapping of two analysed groups. The validity of PLS-DA was confirmed by cross-validation and indicated that the best classifier model comprised three components (R2 = 0.90, Q2 = 0.29).
The overall Variable Importance in the Projection (VIP) score plot generated from the PLS-DA model selected and ranked 15 individual metabolites that contributed significantly to the discrimination between patient and control groups (Figure 1b). Higher VIP scores suggest greater importance for discrimination between groups. Some of the important metabolites obtained by this separation include groups of amino acids (glutamate, phenylalanine, ornithine and aspartate), biogenic amines (serotonin and methionine sulfoxide), hexoses, including glucose, diglyceride (DG [41:1]), triglycerides (TG [48:2], TG [48:1], TG [53:3], TG [56:6] and TG [50:3]), lysophosphatidylcholine (LPC [18:2]) and ether phosphatidylcholine (PC-O [42:4]) (Figure 1b). Among them, glutamate, serotonin, triglycerides (TG [48:2] and TG [48:1]), ether phosphatidylcholine (PC-O [42:4]) and phenylalanine mostly contributed to the metabolic differences between two analysed groups (VIP > 2), with glutamate, ether phosphatidylcholine (PC-O [42:4]), and phenylalanine having higher abundance and serotonin and triglycerides (TG [48:2] and TG [48:1]) having lower abundance in patient serums compared to control samples (Figure 1b).
The univariate analysis (Student t-test) resulted in the identification of 37 metabolites with significantly different concentrations between patient and control serums. These include amino acids (phenylalanine, ornithine, glutamate, aspartate, leucine, serine, valine and isoleucine), serotonin, hexoses (including glucose), diglyceride (DG [34:1]), triglycerides (TG [48:1], TG [48:2], TG [50:3], TG [50:4], TG [53:3] and TG [56:6]), lysophosphatidylcholines (LPC [16:0], LPC [18:2] and LPC [20:3]), phosphatidylcholines (PC [32:0], PC [35:1], PC [37:4], PC [39:4] and PC [39:7]), ether phosphatidylcholine (PC-O [42:4]), and sphingomyelins (SM [32:1], SM [34:1], SM [34:2], SM [35:1], SM [36:1], SM [37:1], SM [38:1], SM [38:2], SM [40:2], SM [41:2] and SM [42:2]) (Table S3).
From 37 significantly altered metabolites, all amino acids, sphingomyelins, phosphatidylcholines, ether phosphatidylcholines, two lysophosphatidylcholines (LPC [16:0] and LPC [20:3]), diglyceride as well as hexoses were significantly increased in patient serums compared to control serums. On the other hand, lysophosphatidylcholine (LPC [18:2]), serotonin, and all triglycerides were significantly decreased in the patient serums compared to control serums.
Hierarchical cluster analysis (HCA) was performed using 37 significant metabolites from the Student t-test to obtain visualization of the differentially abundant metabolites and the alteration in serum metabolites between two groups in form of heat map (Figure 2). The results that referred to two main clusters were related to the compared samples and metabolites using Euclidean as a distance measure and ward as a clustering algorithm. Sample group clustering for the targeted metabolomics with overlapping of some patient samples and control samples are shown in Figure 2. Interestingly, the metabolomics pattern of the control group (samples 3, 11, 13, 2, 1, 4, and 12) was closer to the group of patients. On the other hand, the metabolomics pattern of the samples 23, 25, 22, 17, 20, 19, and 16 in patient group was closer to control group.
According to both multivariate and univariate analysis, the concentrations of following metabolites were statistically altered between patient and control serums: glutamate, phenylalanine, ornithine, aspartate, serotonin, hexose, triglycerides (TG [48:1], TG [48:2], TG [50:3], TG [53:3], and TG [56:6]), lysophosphatidylcholines (LPC [18:2]) and ether phosphatidylcholine (PC-O [42:4]) (Figure 3).
3.2.2. Comparison of patient stroke thrombi versus patient serum
Stroke thrombi metabolome from IS patients was compared with the serum metabolome of the same patient. The targeted analysis detected 125 metabolites (above the limit of detection, LOD) between the two groups which were used for further statistical analysis and classified into groups of amino acids (N = 21), biogenic amines (N = 4), hexoses, including glucose (N = 1), acylcarnitines (N = 2), cholesteryl esters (N = 1), diglycerides (N = 4), triglycerides (N = 8), lysophosphatidylcholines (N = 3), phosphatidylcholines (N = 34), ether phosphatidylcholines (N = 22), sphingomyelins (N = 23) and ceramides (N = 2) (Table S4). Among them, 97 metabolites were relatively, 27 metabolites were absolutely quantified, and one metabolite was quantified with restrictions.
In order to identify metabolites that were the most discriminant between stroke thrombi group (N = 14) and patient serums group (N = 14), PLS discriminant analysis was performed. The validity of PLS-DA was confirmed by cross-validation and showed that the best classifier model comprised two components (R2 = 0.89, Q2 = 0.84). This analysis showed a clear intergroup separation of the two groups (Figure 4a). The list of 15 most important metabolites that contributed significantly to the discrimination between two groups determined by overall VIP score included methionine sulfoxide, triglycerides (TG [52:4] and TG [54:3]), phosphatidylcholines (PC [32:0], PC [40:9], PC [38:7] and PC [36:5]), ether phosphatidylcholines (PC-O [34:0], PC-O [32:0], PC-O [34:1], PC-O [36:2]), sphingomyelins (SM [44:1), SM [40:1] and SM [42:1]) and ceramide (Cer [42:2]). Among them, ether phosphatidylcholine (PC-O [34:0]) was the most influential metabolite with the VIP > 2 having higher abundance in stroke thrombi samples than in serum samples (Figure 4b).
Of 125 detected metabolites, 68.8% (N = 86) had significantly different concentrations between stroke thrombi samples and serum samples of the same patient according the univariate analysis (Student t-test). These include amino acids (N = 9), biogenic amines (N = 4), hexoses, including glucose (N = 1), acylcarnitines (N=2), diglycerides (N =1), cholesteryl esters (N = 1), triglycerides (N = 8), lysophosphatidylcholines (N = 3), phosphatidylcholines (N = 23), ether phosphatidylcholines (N = 14), sphingomyelins (N = 8) and ceramides (N = 2). Among them, all sphingolipids, 23 out of 37 all phosphatidylcholines, 7 out of 9 amino acids, 2 out of 4 biogenic amines, cholesteryl ester and diglyceride were significantly higher in stroke thrombi compared to serum samples. On the other hand, all acylcarnitines, triglycerides, lysophosphatidylcholines, and 14 out of 37 all phosphatidylcholines were significantly lower in stroke thrombi compared to serum samples (Table S5).
Hierarchical cluster analysis (HCA) was performed using 86 significant metabolites from the Student t-test (p <0.05) to visually represent the differentially abundant metabolites between two groups in form of heat map (Figure 5).
The results that referred to two main clusters were related to the compared samples and metabolites using Euclidean as a distance measure and ward as a clustering algorithm to perform the cluster analysis. Sample group clustering for the targeted metabolomics with overlapping of one stroke thrombus sample (sample 20) are shown in Figure 5.
According to both VIP scores and Student t-test, the concentration of following metabolites were statistically significant between stroke thrombi and serum samples from the same patients: methionine sulfoxide, triglycerides (TG [52:4] and TG [54:3]), phosphatidylcholines (PC [32:0], PC [36:5], PC [38:7], PC [40:9]), ether phosphatidylcholines (PC-O [32:0], PC-O [34:0], PC-O [34:1] and PC-O [36:2]), sphingomyelins (SM [40:1], SM [42:1] and SM [44:1]) and ceramide (Cer [42:2]) (Figure 6).
4. Discussion
Ischemic stroke (IS) followed by cerebral ischemia causes the cascade of highly complex and interrelated pathophysiological processes such as energy failure and excitotoxicity, oxidative stress, blood-brain barrier dysfunction, microvascular injury, post-ischemic inflammation, and finally, death of neurons, glia, and endothelial cells [26]. Due to the impaired integrity of the blood-brain barrier after cerebral ischemia, many of the post-ischemic metabolites are more easily found in the plasma or serum of the patient [16]. Therefore, metabolomics represents a key tool for analysing end products of cellular metabolism in various pathologies [8]. Metabolomic research of stroke thrombi in ischemic stroke is very limited. To our knowledge, only several studies have been performed as non-target metabolomic analysis and using solely stroke thrombi, being mainly focused on single group of metabolites such as glucose and sorbitol [17] or glycerophospholipids in very small number of stroke thrombi samples [18]. In this study, we have performed comparative targeted metabolomic analysis of 14 stroke thrombi, corresponding patient serums and healthy control serums and identified specific subset of stroke-related metabolites.
According to both multivariate and univariate analysis, the concentrations of some metabolites were statistically significant between patient and control serums, while some were statistically significant between patient serums and stroke thrombi.
Glutamate concentration was significantly increased in patient serums compared to control serums (Figure 2 and Figure 3), with the highest VIP score (VIP > 2.5, Figure 1b), which is in accordance to reported studies. Glutamate is excitatory amino acid and neurotransmitter having important role in mediating neuronal damage during cerebral ischemia [13]. It is considered the main contributor to the ischemic brain tissue excitotoxicity as a result of energy failure [27] and higher concentrations of glutamate in the blood and cerebrospinal fluid have been reported and associated with poor clinical outcome and neurological impairment after stroke [15,28].
Contrary to glutamate, serotonin concentration was significantly decreased in patient serums compared to control serums (Figure 2 and Figure 3), also having high VIP score (VIP > 2, Figure 1b). This is in accordance to some early reports indicating decreased plasma serotonin levels in patients with acute ischemic stroke [29]. On the other hand, some studies reported elevated post-stroke plasma serotonin levels compared to healthy subjects [30] while some reported no significant differences in serotonin levels [31]. The suggested reason could be in the dynamics of the platelet serotonin (PS) content in one- day period after stroke, since the patients with low PS content had more severe status than patients with values greater than normal [31]. Serotonin is well known as excitatory glutamatergic neurotransmitter that modulates neural activity and regulates mood and behaviour, but it also very important regulator of platelet aggregation and cardiovascular function [32]. Abnormal serotoninergic mechanism may lead to a pro-thrombotic state, while downregulation may increase the risk of bleeding [33]. Many studies have shown that selective serotonin reuptake inhibitors (SSRIs) can improve clinical outcome from ischemic stroke [34] possibly due to the effecting neuronal cell survival, synaptic plasticity and neuronal connections [35].
Phenylalanine concentration was also increased in patients vs. controls serums in this study (Figure 2 and Figure 3) with VIP > 2 (Figure 1b), which is also in accordance with related studies, where it is suggested to be a compensatory response to high neurotoxic concentrations of glutamate, due to phenylalanine inhibition of excitatory glutamatergic synaptic transmission [27].
Excessive release of aspartate, another excitatory amino acid significantly elevated in patient serums (Figure 2 and Figure 3), is believed to be as a result of membrane depolarization after cerebral ischemia and related to excitotoxicity and oxidative stress [36].
In microglial cells, ornithine is a key substrate for polyamines biosynthesis, which are involved in regulation of inflammatory reactions and cell renewal processes after cerebral ischemia [37], but the main metabolic fate for ornithine in the brain is most probably conversion to glutamate and GABA via ornithine aminotransferase [38]. Therefore, increased ornithine concentration in patient serums (Figure 2 and Figure 3) suggests both involvement in neuronal damage and cell renewal after cerebral ischemia.
Methionine sulfoxide, a cell oxidative stress product, was significantly elevated in stroke thrombi compared to patients serums (Figure 5 and Figure 6; VIP > 1.5, Figure 4b), as previously reported to be elevated in stroke patients’ plasma and associated with increased risk of ischemic stroke [39,40].
Beside several significantly altered amino acids that are involved in ischemic metabolic serum profile, glucose concentrations have also been significantly increased in patient serums showed by both standard laboratory blood tests (Table 2) and metabolomics serum analysis (Figure 2 and Figure 3; VIP > 1.5, Figure 1b), as previously reported in many studies and considered to be an predictor of poor stroke outcome [41]. Hyperglycaemia was reported to be present in almost 40 % of stroke patients [42] and it is suggested to promote ischemic injury by several proposed mechanisms, including acidosis due to anaerobic metabolism of glucose to lactic acid, superoxide and nitric oxide production, enhanced glucose-sodium exchange, abnormal protein glycosylation and advanced glycation products [43].
The majority of statistically significant metabolites in this study were lipids - phospholipids, sphingolipids and triacylglycerols, representing 7/13 metabolites between patient and control serums (Figure 3) and 14/15 metabolites between stroke thrombi and patient serums (Figure 6). The only lipid metabolite that was significantly elevated in patient serums vs. controls was ether phosphatidylcholine (PC-O [42:4]) (Figure 2 and Figure 3; VIP > 2, Figure 1b), possibly having C22:0 fatty alcohol linked via ether linkage at the position C-1 and eicosatetranoic acid (C20:4) at the position C-2, which categorizes this ether phospholipid as plasmalogen [44]. Ether phospholipids, including plasmalogens, have different biological functions such as modulation of membrane trafficking, cell signalling, oxidative status and storage of polyunsaturated fatty acids (PUFA) and their compositions and their contents are altered in the plasma of patients suffering from different brain disorders [45]. Interestingly, all other ether phospholipids in this study (PC-O [34:0], PC-O [32:0], PC-O [34:1], PC-O [36:2], Figure 5 and Figure 6) were characterized in significantly higher concentrations in stroke thrombi compared to patient serum, with PC-O (34:0) having the highest VIP score (VIP > 2; Figure 4b), pointing out their potential as a stroke biomarker of oxidative stress and brain injury. On the other hand, “classical” phospholipid species such as phosphatidyl choline (PC [32:0], PC [36:5], PC [38:7], PC [40:9]; VIP > 1.5, Figure 4b) were significantly increased in patient serum samples compared to stroke thrombi (Figure 5 and Figure 6), moreover, all having very high abundance of PUFA content. The only exception was PC (32:0) as the only phosphatidyl choline species that was significantly decreased in patient serums compared to stroke thrombi (Figure 5 and Figure 6). Interestingly, the fatty acids composition is identical as in PC-O (32:0), which is also much more expressed in thrombi than in patient serum samples. The only lysophosphatidyl choline species characterized as statistically significant and discriminatory in this study was LPC (18:2), which was lower in patient serum compared to healthy control serums (Figure 3; VIP > 1.5, Figure 1b). Choline-containing phospholipids are acetylcholine precursors and they have been proposed as adjuvant therapy in acute stroke due to their anti-inflammatory effects and choline’s involvement in membrane synthesis, which is suggested as beneficial for reducing cell injury in ischemic brain [46].
Clinical laboratory analysis of all lipid parameters (TG, tCH, LDL-CH and HDL-CH) did not show significant differences between patient and control serums (Table 2), despite their common association with high risk of atherosclerosis and subsequently ischemic stroke [47]. In accordance to this, in our metabolomics study there were no significant differences detected in cholesterol or cholesterol ester species between these two groups. On the other hand, triacylglycerol species (TG [48:1] and [48:2], VIP > 2; TG [50:3], [53:3] and [56:6], VIP > 1.5, Figure 1b) were significantly decreased in patient serums compared to control serums (Figure 2 and Figure 3), while TG (52:4) and TG (54:3) (VIP > 1.5, Figure 4b) were decreased in stroke thrombi compared to patient serums (Figure 5 and Figure 6). This is in accordance with previous studies, characterizing TG as bioenergetic compounds of lipid droplets that are also present in neural cells, which were reported to have low abundance in plasma patients having stroke recurrence after transient ischemic attack, possibly due to low accumulation or formation of cerebral lipid droplets as a product of a defective ischemia-associated stress response [48].
From all sphingolipid metabolites characterized in this study, sphingomyelins (SM [40:1], [42:1] and [44:1]) and ceramide Cer (42:2) were detected as significantly higher in stroke thrombi than in patient serums (Figure 5 and Figure 6; VIP > 1.5, Figure 4b). Taking into consideration only univariate analysis, from 26 detected SM species between patient and control serums, 11 SM species were significantly increased in patient serums (Figure 2). Sphingolipids, beside their well-known role as structural membrane components, have important functions as bioactive, signaling molecules involved in multiple cellular processes and mechanisms related to ischemia-related stress response [49], inflammation [50], and also serving as second messengers during platelet activation in coagulation process [51]. In thrombin-stimulated platelets, active sphingomyelinase enzyme hydrolyses sphingomyelin to phosphocholine and ceramide, which is involved in signal transduction events during platelet activation [52]. Variations in sphingolipid metabolites plasma levels have also been associated with numerus metabolic and vascular diseases [53]. Long-chain ceramides are involved in apoptotic pathways and inflammation related to cerebral ischemia [54] and their elevated serum levels have been reported as predictors of risk and severity of the ischemic stroke [55,56] as well as related to adverse cardiovascular risk and events [57]. Rise in ceramide levels is a result of inflammation and tissue damage as well as a product of a strong increase in acidic and/or neutral sphingomyelinase activity (ASM/NSM), producing ceramide from sphingomyelin, which was reported to occur in focal cerebral ischemia [58]. The ASM / ceramide system is critically involved in ischemic stroke pathogenesis and studies have reported improvement in ischemic brain injury after ASM inhibition and lowering ceramide content [59]. Sphingomyelins, as major constituents of lipid rafts, are involved in signaling cascades and their deficiency has shown to suppress the inflammation induced by cerebral ischemia damage after ischemic stroke in mice [60] while their higher serum content was related to higher risk of myocardial infarction [61]. Besides ceramides, sphingomyelin SM (44:2) was reported as a potential stroke biomarker [62], SM (38:1) and Cer (34:1) were reported as biomarkers of cerebral microvascular disease [63], while SM (32:1) levels were reported to be inversely related to incident ischemic stroke in large multi-cohort metabolomics study [64]. The reason why some particular SM or Cer species are elevated or decreased in different pathologies remains unclear.
4.1. Study Limitations
Our study has several limitations. The research was conducted using a relatively small number of subjects, which may influence the statistical power of the study and affect generalizability of study results due to the heterogeneity of aetiologies, comorbidities, clinical presentations and demographics of ischemic stroke patients. Since the patients’ blood was not collected after overnight fasting, potential nutritional influence on metabolite profile cannot be excluded. Furthermore, other stroke risk factors such as physical activity, smoking and alcohol consummation were not evaluated. Age differences between the analysed groups may also influence the accuracy of the compared metabolic profiles. Therefore, this research could be validated and confirmed in a larger and more diverse study.
5. Conclusions
The comparative targeted metabolomics analysis of stroke thrombi, corresponding patient serums and healthy control serums obtained in this work identified specific subset of stroke-related metabolites. Due to the scarce information on stroke thrombi metabolomics profile present in the literature, these results provide valuable information about the thrombi composition in correlation with the patient ischemic serum metabolites, reflecting the pathophysiological processes occurring as a consequence of cerebral ischemia. These data could help to elucidate the roles of particular metabolites in coagulation and pathogenesis of ischemic stroke and suggest new potential candidates for early diagnostic, prognostic and therapeutic biomarkers of ischemic stroke.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Clinical and laboratory parameters obtained by standard laboratory procedures in the control and patient serums; Table S2: Concentrations (μmol dm−3) of all valid metabolites obtained by targeted metabolomics (AbsoluteIDQ® p400 HR Kit, Biocrates LifeSciences AG, Innsbruck, Austria) in the control and patient serums; Table S3: Significant metabolites with differential abundance between two groups (serum of control; serum of patients) obtained by LC-MS/MS and FIA-MS/MS analysis; Table S4: Concentrations (μmol dm−3) of all valid metabolites obtained by targeted metabolomics (AbsoluteIDQ® p400 HR Kit, Biocrates LifeSciences AG, Innsbruck, Austria) in the serum and stroke thrombi of patients; Table S5: Significant metabolites with differential abundance between serums and thrombi of patient obtained by the LC-MS/MS and FIA-MS/MS analysis.
Author Contributions
Conceptualization, D.F. and I.K.; methodology, D.F, I.K., I.R., D.R.M, J.K., D.O., V.K., M.J.S., R.K. and K.S.; validation, I.K., D.F., I.R. and K.S.; formal analysis, D.F., I.K. and I.R.; investigation, D.F., I.K., I.R, K.S., and R.K.; resources, T.S., K.R., M.J.S., M.R.B., R.K., Z.P and V.M.; data curation, I.R., I.K. and D.F.; writing - original draft preparation, D.F, I.K., I.R. and K.S.; writing - review and editing, D.F, I.K., Z.P, M.R.B. and V.M.; visualization, I.K, D.F. and I.R.; supervision, D.F. and I.K.; project administration, D.F., I.K. and V.M.; funding acquisition, V.M, D.F., I.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Adris Fundation grant “SphingoMark & Thrombectomy” to D.F, grant no. 13127; University of Zagreb Support grant “Sphingolipidomics of stroke thrombi and serum in ischemic stroke” to I.K., grant no. 10106-23-2513; European Commission ERA chair FP7 grant, VetMedZg to V.M., grant no. 621394.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University Hospital Centre “Zagreb“ (protocol code 02/21 AG, 28.10.2019) and University Hospital Centre “Sestre milosrdnice” (protocol code EP-18031/19-12, 23.01.2020) and by the Ethics Committee of the School of Medicine, University of Zagreb (protocol code 380-59-10106-20-111/15 and 23.01.2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data are included in this paper and the Supplementary Materials. The datasets acquired during the current study are available from the corresponding authors upon request.
Acknowledgments
We gratefully acknowledge technical assistance from Anita Pustički Sajković, Adrijana Culak and Goran Kapustić (Department of Medical Chemistry, Biochemistry and Clinical Chemistry, School of Medicine, Zagreb, Croatia).
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, P.B. The Global Burden of Stroke: Persistent and Disabling. Lancet. Neurol. 2019, 18, 417–418. [Google Scholar] [CrossRef] [PubMed]
- Herpich, F.; Rincon, F. Management of Acute Ischemic Stroke. Crit. Care Med. 2020, 48, 1654. [Google Scholar] [CrossRef] [PubMed]
- Raha, O.; Hall, C.; Malik, A.; D’Anna, L.; Lobotesis, K.; Kwan, J.; Banerjee, S. Advances in Mechanical Thrombectomy for Acute Ischaemic Stroke. BMJ Med. 2023, 2, e000407. [Google Scholar] [CrossRef] [PubMed]
- Meretoja, A.; Keshtkaran, M.; Saver, J.L.; Tatlisumak, T.; Parsons, M.W.; Kaste, M.; Davis, S.M.; Donnan, G.A.; Churilov, L. Stroke Thrombolysis: Save a Minute, Save a Day. Stroke 2014, 45, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Han, T.S.; Gulli, G.; Fry, C.H.; Affley, B.; Robin, J.; Fluck, D.; Kakar, P.; Sharma, P. Adverse Consequences of Immediate Thrombolysis-Related Complications: A Multi-Centre Registry-Based Cohort Study of Acute Stroke. J. Thromb. Thrombolysis 2022, 53, 218. [Google Scholar] [CrossRef]
- Jolugbo, P.; Ariëns, R.A.S. Thrombus Composition and Efficacy of Thrombolysis and Thrombectomy in Acute Ischemic Stroke. Stroke 2021, 52, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Jacob, M.; Lopata, A.L.; Dasouki, M.; Abdel Rahman, A.M. Metabolomics toward Personalized Medicine. Mass Spectrom. Rev. 2019, 38, 221–238. [Google Scholar] [CrossRef]
- Lee, Y.; Khan, A.; Hong, S.; Jee, S.H.; Park, Y.H. A Metabolomic Study on High-Risk Stroke Patients Determines Low Levels of Serum Lysine Metabolites: A Retrospective Cohort Study. Mol. Biosyst. 2017, 13, 1109–1120. [Google Scholar] [CrossRef]
- Costamagna, G.; Bonato, S.; Corti, S.; Meneri, M. Advancing Stroke Research on Cerebral Thrombi with Omic Technologies. Int. J. Mol. Sci. 2023, 24. [Google Scholar] [CrossRef]
- Khan, A.; Shin, M.S.; Jee, S.H.; Park, Y.H. Global Metabolomics Analysis of Serum from Humans at Risk of Thrombotic Stroke. Analyst 2020, 145, 1695–1705. [Google Scholar] [CrossRef]
- Sun, D.; Tiedt, S.; Yu, B.; Jian, X.; Gottesman, R.F.; Mosley, T.H.; Boerwinkle, E.; Dichgans, M.; Fornage, M. A Prospective Study of Serum Metabolites and Risk of Ischemic Stroke. Neurology 2019, 92, E1890–E1898. [Google Scholar] [CrossRef]
- Tao, S.; Xiao, X.; Li, X.; Na, F.; Na, G.; Wang, S.; Zhang, P.; Hao, F.; Zhao, P.; Guo, D.; et al. Targeted Metabolomics Reveals Serum Changes of Amino Acids in Mild to Moderate Ischemic Stroke and Stroke Mimics. Front. Neurol. 2023, 14, 1153193. [Google Scholar] [CrossRef]
- Li, W.; Shao, C.; Li, C.; Zhou, H.; Yu, L.; Yang, J.; Wan, H.; He, Y. Metabolomics: A Useful Tool for Ischemic Stroke Research. J. Pharm. Anal. 2023, 13, 968–983. [Google Scholar] [CrossRef]
- Chumachenko, M.S.; Waseem, T. V; Fedorovich, S. V Metabolomics and Metabolites in Ischemic Stroke. 33. [CrossRef]
- Daneman, R. The Blood–Brain Barrier in Health and Disease. Ann. Neurol. 2012, 72, 648–672. [Google Scholar] [CrossRef]
- Suissa, L.; Guigonis, J.M.; Graslin, F.; Doche, E.; Osman, O.; Chau, Y.; Sedat, J.; Lindenthal, S.; Pourcher, T. Metabolome of Cerebral Thrombi Reveals an Association between High Glycemia at Stroke Onset and Good Clinical Outcome. Metab. 2020, Vol. 10, Page 483 2020, 10, 483. [Google Scholar] [CrossRef]
- Martha, S.R.; Levy, S.H.; Federico, E.; Levitt, M.R.; Walker, M. Machine Learning Analysis of the Cerebrovascular Thrombi Lipidome in Acute Ischemic Stroke. J. Neurosci. Nurs. 2023, 55, 10–17. [Google Scholar] [CrossRef]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; de Vries, J.; White, P.; et al. European Stroke Organisation (ESO) – European Society for Minimally Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy inAcute Ischaemic StrokeEndorsed by Stroke Alliance for Europe(SAFE). Eur. Stroke J. 2019, 4, 6. [Google Scholar] [CrossRef]
- Berge, E.; Whiteley, W.; Audebert, H.; Marchis, G.M. De; Fonseca, A.C.; Padiglioni, C.; Ossa, N.P. de la; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) Guidelines on Intravenous for Acute Ischaemic Stroke. Eur. Stroke J. 2021, 6, I. [Google Scholar] [CrossRef]
- Turc, G.; Tsivgoulis, G.; Audebert, H.J.; Boogaarts, H.; Bhogal, P.; De Marchis, G.M.; Fonseca, A.C.; Khatri, P.; Mazighi, M.; Pérez de la Ossa, N.; et al. European Stroke Organisation – European Society for Minimally Invasive Neurological Therapy Expedited Recommendation on Indication for Intravenous Thrombolysis before Mechanical Thrombectomy in Patients with Acute Ischaemic Stroke and Anterior Circulation Large Vessel Occlusion. Eur. Stroke J. 2022, 7, I. [Google Scholar] [CrossRef]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Hrvatska komora medicinskih biokemičara Priručnik o Preporučenim Metodama u Medicinsko-Biokemijskim Laboratorijima; HKMB: Zagreb, 1998; (Croatian chamber of medical biochemists: Manual on Suggested Methods in Medical-Biochemical Laboratories, HKMB, Zagreb, 1998; Publisher HKMB, Zagreb).
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Rubić, I.; Burchmore, R.; Weidt, S.; Regnault, C.; Kuleš, J.; Rafaj, R.B.; Mašek, T.; Horvatić, A.; Crnogaj, M.; Eckersall, P.D.; et al. Multi Platforms Strategies and Metabolomics Approaches for the Investigation of Comprehensive Metabolite Profile in Dogs with Babesia Canis Infection. Int. J. Mol. Sci. 2022, 23, 1575. [Google Scholar] [CrossRef]
- Brouns, R.; De Deyn, P.P. The Complexity of Neurobiological Processes in Acute Ischemic Stroke. Clin. Neurol. Neurosurg. 2009, 111, 483–495. [Google Scholar] [CrossRef]
- Sidorov, E.; Sanghera, D.K.; Vanamala, J.K.P. Biomarker for Ischemic Stroke Using Metabolome: A Clinician Perspective. J. Stroke 2019, 21, 31. [Google Scholar] [CrossRef]
- Aliprandi, A.; Longoni, M.; Stanzani, L.; Tremolizzo, L.; Vaccaro, M.; Begni, B.; Galimberti, G.; Garofolo, R.; Ferrarese, C. Increased Plasma Glutamate in Stroke Patients Might Be Linked to Altered Platelet Release and Uptake. J. Cereb. Blood Flow Metab. 2005, 25, 513–519. [Google Scholar] [CrossRef]
- Ishizaki, F. A Follow-up Study of Platelet-Rich Plasma Serotonin in Clinical Subtypes of Cerebral Infarction. J. Neural Transm. 1987, 69, 123–129. [Google Scholar] [CrossRef]
- Ban, Y.; Watanabe, T.; Miyazaki, A.; Nakano, Y.; Tobe, T.; Idei, T.; Iguchi, T.; Ban, Y.; Katagiri, T. Impact of Increased Plasma Serotonin Levels and Carotid Atherosclerosis on Vascular Dementia. Atherosclerosis 2007, 195, 153–159. [Google Scholar] [CrossRef]
- Golimbet, V.E.; Brusov, O.S.; Faktor, M.I.; Zlobina, G.P.; Lezheiko, T. V.; Lavrushina, O.M.; Petrova, E.A.; Savina, M.A.; Skvortsova, V.I. Effects of the Interaction of Variants of the Serotonin Transporter and Brain-Derived Neurotrophic Factor on Platelet Serotonin Levels in Stroke Patients. Neurosci. Behav. Physiol. 2011, 41, 554–557. [Google Scholar] [CrossRef]
- Berger, M.; Gray, J.A.; Roth, B.L. The Expanded Biology of Serotonin. Annu. Rev. Med. 2009; 60, 355–366. [Google Scholar] [CrossRef]
- de Abajo, F.J. Effects of Selective Serotonin Reuptake Inhibitors on Platelet Function. Drugs Aging 2011, 28, 345–367. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Qureshi, M.M.; Abdalkader, M.; Martins, S.O.; Yamagami, H.; Qiu, Z.; Mansour, O.Y.; Sathya, A.; Czlonkowska, A.; Tsivgoulis, G.; et al. Global Impact of COVID-19 on Stroke Care and IV Thrombolysis. Neurology 2021, 96, E2824–E2838. [Google Scholar] [CrossRef] [PubMed]
- Miedema, I.; Horvath, K.M.; Uyttenboogaart, M.; Koopman, K.; Lahr, M.M.H.; De Keyser, J.; Luijckx, G.J. Effect of Selective Serotonin Re-Uptake Inhibitors (SSRIs) on Functional Outcome in Patients with Acute Ischemic Stroke Treated with TPA. J. Neurol. Sci. 2010, 293, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Yang, H.; Chen, J.; Fang, J.; Chen, C.; Liang, R.; Yang, G.; Wu, H.; Wu, C.; Li, S. Analysis of Serum Metabolites for the Discovery of Amino Acid Biomarkers and the Effect of Galangin on Cerebral Ischemia. Mol. Biosyst. 2013, 9, 2311–2321. [Google Scholar] [CrossRef] [PubMed]
- Cigdem, B.; Bolayir, A.; Celik, V.K.; Kapancik, S.; Kilicgun, H.; Gokce, S.F.; Gulunay, A. The Role of Reduced Polyamine Synthesis in Ischemic Stroke. Neurochem. J. 2020, 14, 243–250. [Google Scholar] [CrossRef]
- Das, A.; Fröhlich, D.; Achanta, L.B.; Rowlands, B.D.; Housley, G.D.; Klugmann, M.; Rae, C.D. L-Aspartate, L-Ornithine and L-Ornithine-L-Aspartate (LOLA) and Their Impact on Brain Energy Metabolism. Neurochem. Res. 2020, 45, 1438–1450. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, R.; Hu, J.; Guasch-Ferre, M.; Li, J.; Sorond, F.; Zhao, Y.; Shutta, K.H.; Salas-Salvado, J.; Hu, F.; Clish, C.B.; et al. Metabolomic Profiles Associated With Incident Ischemic Stroke. Neurology 2022, 98, e483–e492. [Google Scholar] [CrossRef] [PubMed]
- Djite, M.; Chao de la Barca, J.M.; Bocca, C.; Gaye, N.M.; Barry, N.O.; Mbacke, M.N.; Cissé, O.; Kandji, P.M.; Thioune, N.M.; Coly-Gueye, N.F.; et al. A Metabolomic Signature of Ischemic Stroke Showing Acute Oxidative and Energetic Stress. Antioxidants 2024, 13, 60. [Google Scholar] [CrossRef] [PubMed]
- Yong, M.; Kaste, M. Dynamic of Hyperglycemia as a Predictor of Stroke Outcome in the ECASS-II Trial. Stroke 2008, 39, 2749–2755. [Google Scholar] [CrossRef]
- Hafez, S.; Coucha, M.; Bruno, A.; Fagan, S.C.; Ergul, A. Hyperglycemia, Acute Ischemic Stroke, and Thrombolytic Therapy. Transl. Stroke Res. 2014, 5, 442–453. [Google Scholar] [CrossRef]
- Robbins, N.M.; Swanson, R.A. Opposing Effects of Glucose on Stroke and Reperfusion Injury. Stroke 2014, 45, 1881–1886. [Google Scholar] [CrossRef]
- Han, X.; Holtzman, D.M.; McKeel, D.W. Plasmalogen Deficiency in Early Alzheimer’s Disease Subjects and in Animal Models: Molecular Characterization Using Electrospray Ionization Mass Spectrometry. J. Neurochem. 2001, 77, 1168–1180. [Google Scholar] [CrossRef] [PubMed]
- Udagawa, J.; Hino, K. Plasmalogen in the Brain: Effects on Cognitive Functions and Behaviors Attributable to Its Properties. Brain Res. Bull. 2022, 188, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Sagaro, G.G.; Amenta, F. Choline-Containing Phospholipids in Stroke Treatment: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2875. [Google Scholar] [CrossRef]
- Holmes, M. V.; Millwood, I.Y.; Kartsonaki, C.; Hill, M.R.; Bennett, D.A.; Boxall, R.; Guo, Y.; Xu, X.; Bian, Z.; Hu, R.; et al. Lipids, Lipoproteins, and Metabolites and Risk of Myocardial Infarction and Stroke. J. Am. Coll. Cardiol. 2018, 71, 620–632. [Google Scholar] [CrossRef]
- Purroy, F.; Ois, A.; Jove, M.; Arque, G.; Sol, J.; Mauri-Capdevila, G.; Rodriguez-Campello, A.; Pamplona, R.; Portero, M.; Roquer, J. Lipidomic Signature of Stroke Recurrence after Transient Ischemic Attack. Sci. Rep. 2023, 13, 13706. [Google Scholar] [CrossRef]
- Zhang, H.; Hu, Y.Y.; Murong, S.X.; Tong, E.T.; Dhodda, V.K.; Sailor, K.; Dempsey, R.J.; Vemuganti, R.L.R. Sphingolipids in Rat Model of Transient Focal Cerebral Ischemia: Implication for Stroke Injury. J. Neurochem. 2002, 81, 108–111. [Google Scholar] [CrossRef]
- Grösch, S.; Alessenko, A. V.; Albi, E. The Many Facets of Sphingolipids in the Specific Phases of Acute Inflammatory Response. Mediators Inflamm. 2018, 2018. [Google Scholar] [CrossRef]
- Simon, C.G.; Chatterjee, S.; Gear, A.R.L. Sphingomyelinase Activity in Human Platelets. Thromb. Res. 1998, 90, 155–161. [Google Scholar] [CrossRef]
- Romiti, E.; Vasta, V.; Meacci, E.; Farnararo, M.; Linke, T.; Ferlinz, K.; Sandhoff, K.; Bruni, P. Characterization of Sphingomyelinase Activity Released by Thrombin-Stimulated Platelets. Mol. Cell. Biochem. 2000, 205, 75–81. [Google Scholar] [CrossRef]
- Buciuc, M.; Vasile, V.C.; Conte, G.M.; Scharf, E.L. Ceramide Dynamics and Prognostic Value in Acute and Subacute Ischemic Stroke: Preliminary Findings in a Clinical Cohort. J. Neurol. Res. 2020, 10, 209–219. [Google Scholar] [CrossRef]
- Tian, H.P.; Qiu, T.Z.; Zhao, J.; Li, L.X.; Guo, J. Sphingomyelinase-Induced Ceramide Production Stimulate Calcium-Independent JNK and PP2A Activation Following Cerebral Ischemia. Brain Inj. 2009, 23, 1073–1080. [Google Scholar] [CrossRef]
- Gui, Y. kun; Li, Q.; Liu, L.; Zeng, P.; Ren, R.F.; Guo, Z.F.; Wang, G.H.; Song, J.G.; Zhang, P. Plasma Levels of Ceramides Relate to Ischemic Stroke Risk and Clinical Severity. Brain Res. Bull. 2020, 158, 122–127. [Google Scholar] [CrossRef]
- Lee, T.H.; Cheng, C.N.; Lee, C.W.; Kuo, C.H.; Tang, S.C.; Jeng, J.S. Investigating Sphingolipids as Biomarkers for the Outcomes of Acute Ischemic Stroke Patients Receiving Endovascular Treatment. J. Formos. Med. Assoc. 2023, 122, 19–28. [Google Scholar] [CrossRef] [PubMed]
- McGurk, K.A.; Keavney, B.D.; Nicolaou, A. Circulating Ceramides as Biomarkers of Cardiovascular Disease: Evidence from Phenotypic and Genomic Studies. Atherosclerosis 2021, 327, 18–30. [Google Scholar] [CrossRef]
- Yu, Z.F.; Nikolova-Karakashian, M.; Zhou, D.; Cheng, G.; Schuchman, E.H.; Mattson, M.P. Pivotal Role for Acidic Sphingomyelinase in Cerebral Ischemia-Induced Ceramide and Cytokine Production, and Neuronal Apoptosis. J. Mol. Neurosci. 2000, 15, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Mohamud Yusuf, A.; Hagemann, N.; Hermann, D.M. The Acid Sphingomyelinase/ Ceramide System as Target for Ischemic Stroke Therapies. Neurosignals. 2019, 27, 32–43. [Google Scholar] [CrossRef]
- Xue, J.; Yu, Y.; Zhang, X.; Zhang, C.; Zhao, Y.; Liu, B.; Zhang, L.; Wang, L.; Chen, R.; Gao, X.; et al. Sphingomyelin Synthase 2 Inhibition Ameliorates Cerebral Ischemic Reperfusion Injury Through Reducing the Recruitment of Toll-Like Receptor 4 to Lipid Rafts. J. Am. Heart Assoc. 2019, 8. [Google Scholar] [CrossRef]
- Floegel, A.; Kühn, T.; Sookthai, D.; Johnson, T.; Prehn, C.; Rolle-Kampczyk, U.; Otto, W.; Weikert, C.; Illig, T.; von Bergen, M.; et al. Serum Metabolites and Risk of Myocardial Infarction and Ischemic Stroke: A Targeted Metabolomic Approach in Two German Prospective Cohorts. Eur. J. Epidemiol. 2018, 33, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Deng, X.; Zhu, J.; Chen, S.; Jiao, C.; Ruan, Y. The Identification of Novel Stroke-Related Sphingolipid Biomarkers Using UPLC-MS/MS. Clin. Chim. Acta 2024, 552, 117652. [Google Scholar] [CrossRef]
- Azizkhanian, I.; Sheth, S.A.; Iavarone, A.T.; Lee, S.; Kakarla, V.; Hinman, J.D. Plasma Lipid Profiling Identifies Biomarkers of Cerebral Microvascular Disease. Front. Neurol. 2019, 10, 474611. [Google Scholar] [CrossRef]
- Lind, L.; Salihovic, S.; Ganna, A.; Sundström, J.; Broeckling, C.D.; Magnusson, P.K.; Pedersen, N.L.; Siegbahn, A.; Prenni, J.; Fall, T.; et al. A Multi-Cohort Metabolomics Analysis Discloses Sphingomyelin (32:1) Levels to Be Inversely Related to Incident Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) Partial least squares-discriminant analysis (PLS-DA) score plots were performed in patient group (blue circle; N = 14) and control group (red circle; N = 14) serums using targeted metabolomics approach; (b) Variable Importance in Projection (VIP) score plot showing relative abundance of 15 most significant metabolites identified by PLS-DA that differ between patient and control serums. The colored boxes on the right indicate the relative abundance of metabolite; red box indicates high abundance and blue low abundance of a specific metabolite. Glu - glutamate; TG - triglyceride; PC-O - ether phosphatidylcholine; Phe - phenylalanine; H1 - hexoses (including glucose); Orn - ornithine; Asp - aspartate; LPC - lysophosphatidylcholine; Met-SO - methionine sulfoxide; DG - diglyceride.
Figure 1.
(a) Partial least squares-discriminant analysis (PLS-DA) score plots were performed in patient group (blue circle; N = 14) and control group (red circle; N = 14) serums using targeted metabolomics approach; (b) Variable Importance in Projection (VIP) score plot showing relative abundance of 15 most significant metabolites identified by PLS-DA that differ between patient and control serums. The colored boxes on the right indicate the relative abundance of metabolite; red box indicates high abundance and blue low abundance of a specific metabolite. Glu - glutamate; TG - triglyceride; PC-O - ether phosphatidylcholine; Phe - phenylalanine; H1 - hexoses (including glucose); Orn - ornithine; Asp - aspartate; LPC - lysophosphatidylcholine; Met-SO - methionine sulfoxide; DG - diglyceride.
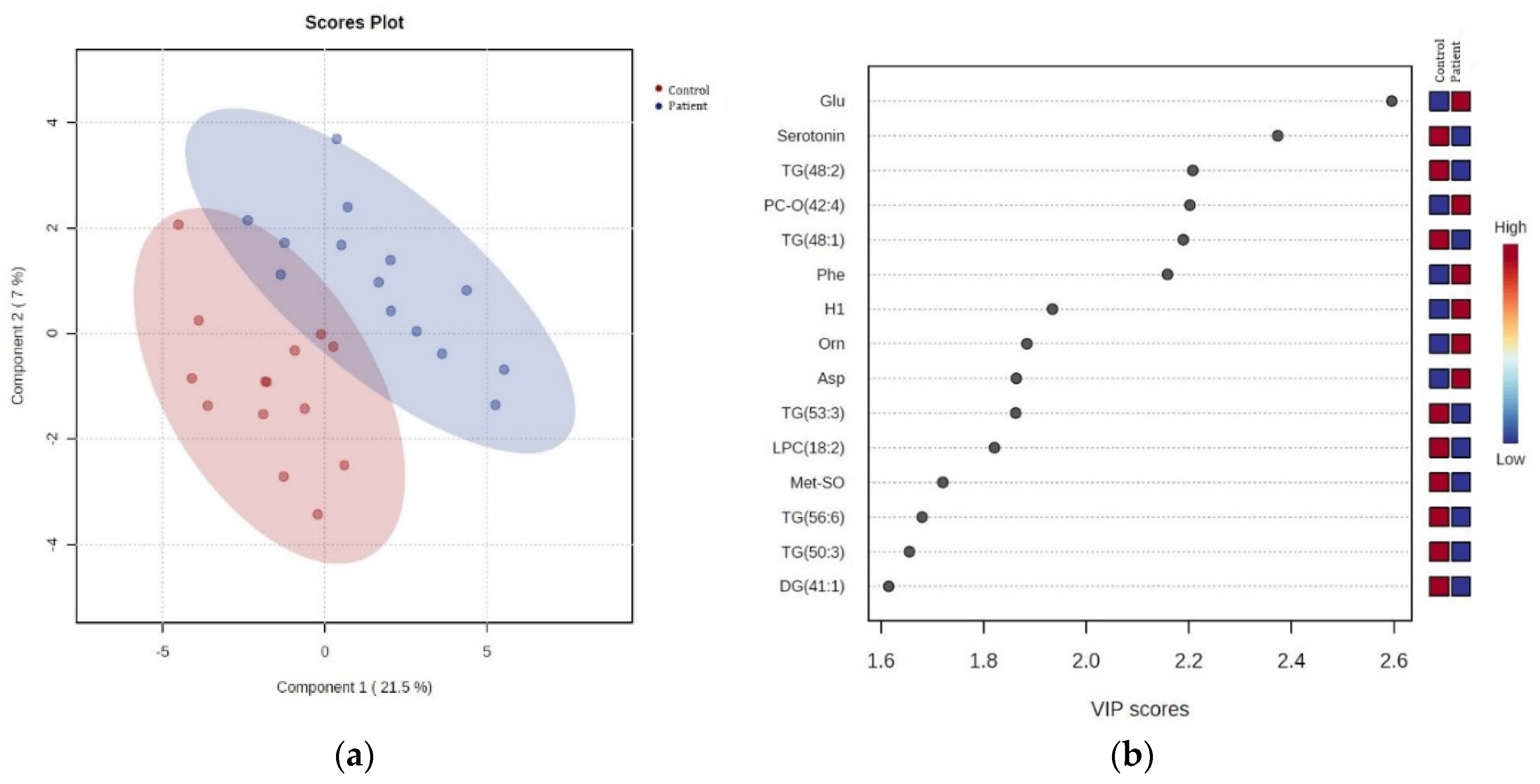
Figure 2.
Hierarchical cluster analysis (HCA) of the significant different metabolites obtained using t-test (p < 0.05) between two groups (patient serums - green panel; control serums - red panel). Each coloured cell on the map corresponds to the intensity value, red colour - max metabolite concentration, green colour - min metabolite concentration. Data was normalization by median, log transformed and Pareto-scaled. TG - triglyceride, PC - phosphatidylcholine; SM - sphingomyelin; Ile - isoleucine, xLeu - leucine; Val - valine; Asp - aspartate; Phe - phenylalanine; Glu - glutamate; Orn - ornithine; Ser - serine, PC-O - ether phosphatidylcholine; LPC - lysophosphatidylcholine; DG - diglyceride; H1 - hexoses (including glucose).
Figure 2.
Hierarchical cluster analysis (HCA) of the significant different metabolites obtained using t-test (p < 0.05) between two groups (patient serums - green panel; control serums - red panel). Each coloured cell on the map corresponds to the intensity value, red colour - max metabolite concentration, green colour - min metabolite concentration. Data was normalization by median, log transformed and Pareto-scaled. TG - triglyceride, PC - phosphatidylcholine; SM - sphingomyelin; Ile - isoleucine, xLeu - leucine; Val - valine; Asp - aspartate; Phe - phenylalanine; Glu - glutamate; Orn - ornithine; Ser - serine, PC-O - ether phosphatidylcholine; LPC - lysophosphatidylcholine; DG - diglyceride; H1 - hexoses (including glucose).
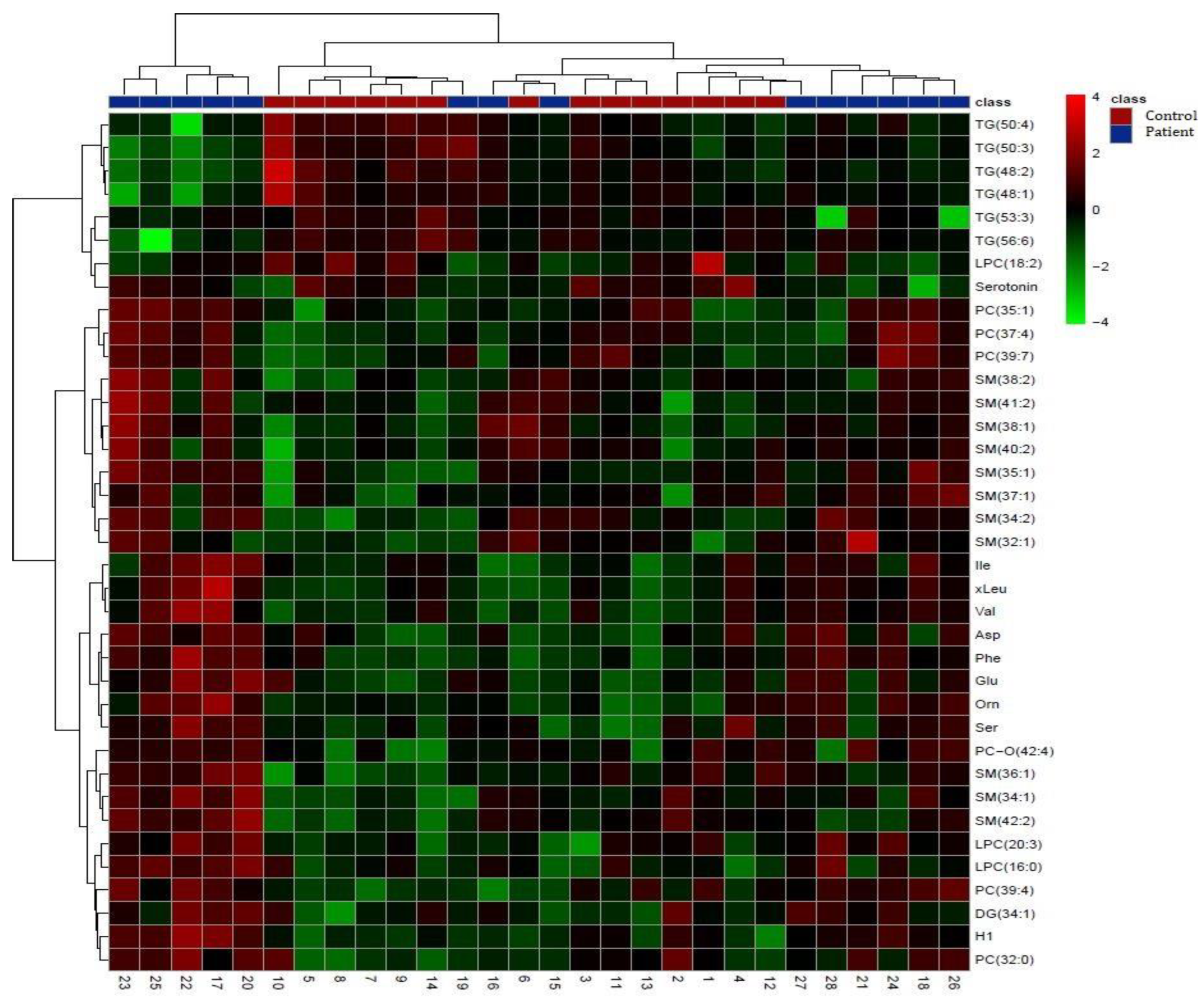
Figure 3.
Concentrations of significantly altered metabolites in patient serums vs. control serums that overlap in univariate (Student t-test) and multivariate (PLS-DA) analyses. Data are presented as box and whiskers plot (mean ± SD). Red - control serums; green - patient serums; TG - triglyceride; PC-O - ether phosphatidylcholine; LPC - lysophosphatidylcholines; H1 - hexoses (including glucose).
Figure 3.
Concentrations of significantly altered metabolites in patient serums vs. control serums that overlap in univariate (Student t-test) and multivariate (PLS-DA) analyses. Data are presented as box and whiskers plot (mean ± SD). Red - control serums; green - patient serums; TG - triglyceride; PC-O - ether phosphatidylcholine; LPC - lysophosphatidylcholines; H1 - hexoses (including glucose).
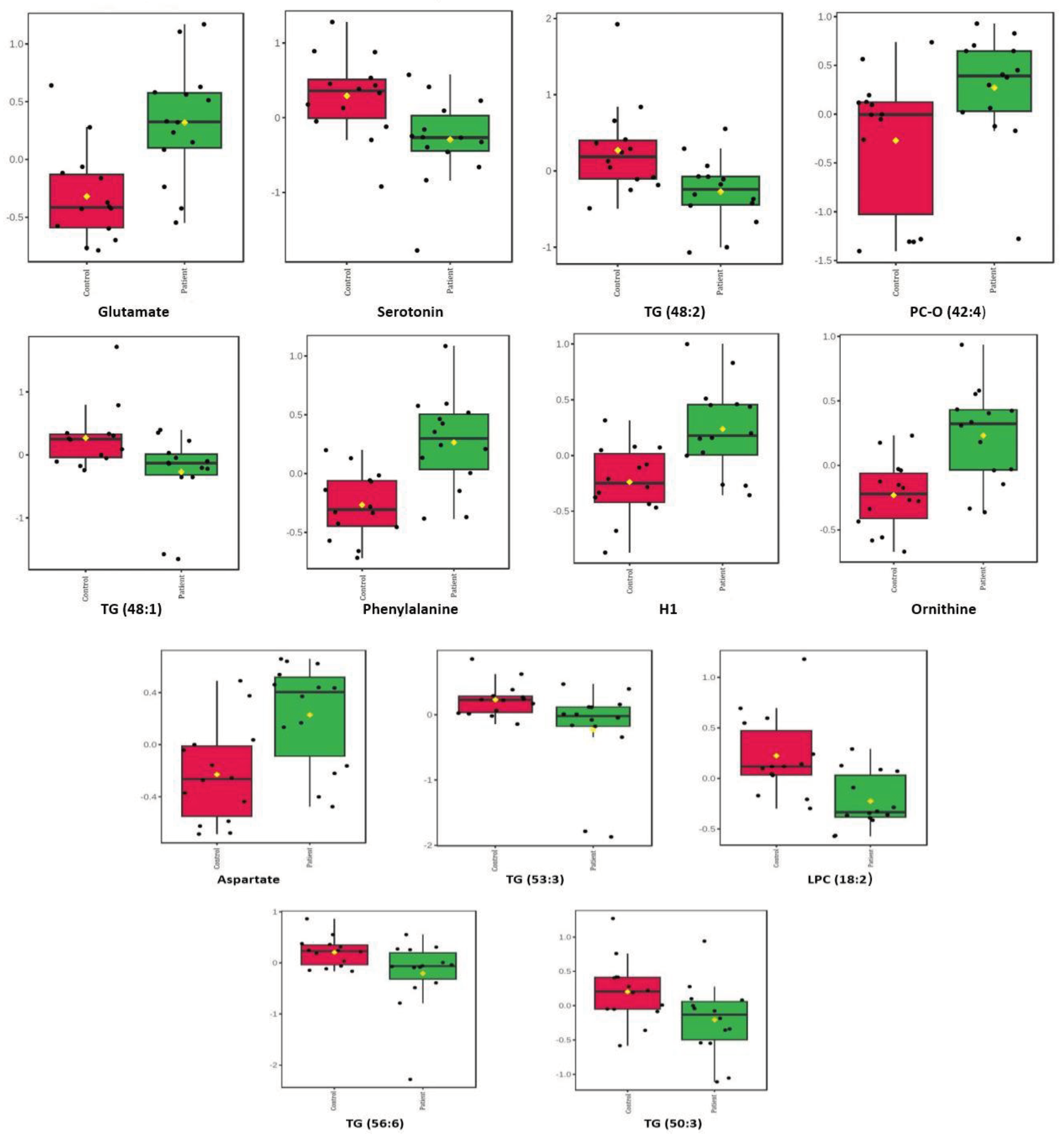
Figure 4.
(a) Partial least squares-discriminant analysis (PLS-DA) score plots were performed in stroke thrombi samples (N = 14; red circle) and serum samples (N =1 4; blue circle) using targeted metabolomics approach; (b) Variable Importance in Projection (VIP) score plot showing relative abundance of 15 most significant metabolites identified by PLS-DA that differ between stroke thrombi and serum samples. The colored boxes on the right indicate the relative abundance of metabolite; red box indicates high abundance and blue low abundance of a specific metabolite. PC-O - ether phosphatidylcholine; Met-SO - methionine sulfoxide; SM - sphingomyelin; PC - phosphatidylcholine; Cer - ceramide; TG - triglyceride.
Figure 4.
(a) Partial least squares-discriminant analysis (PLS-DA) score plots were performed in stroke thrombi samples (N = 14; red circle) and serum samples (N =1 4; blue circle) using targeted metabolomics approach; (b) Variable Importance in Projection (VIP) score plot showing relative abundance of 15 most significant metabolites identified by PLS-DA that differ between stroke thrombi and serum samples. The colored boxes on the right indicate the relative abundance of metabolite; red box indicates high abundance and blue low abundance of a specific metabolite. PC-O - ether phosphatidylcholine; Met-SO - methionine sulfoxide; SM - sphingomyelin; PC - phosphatidylcholine; Cer - ceramide; TG - triglyceride.
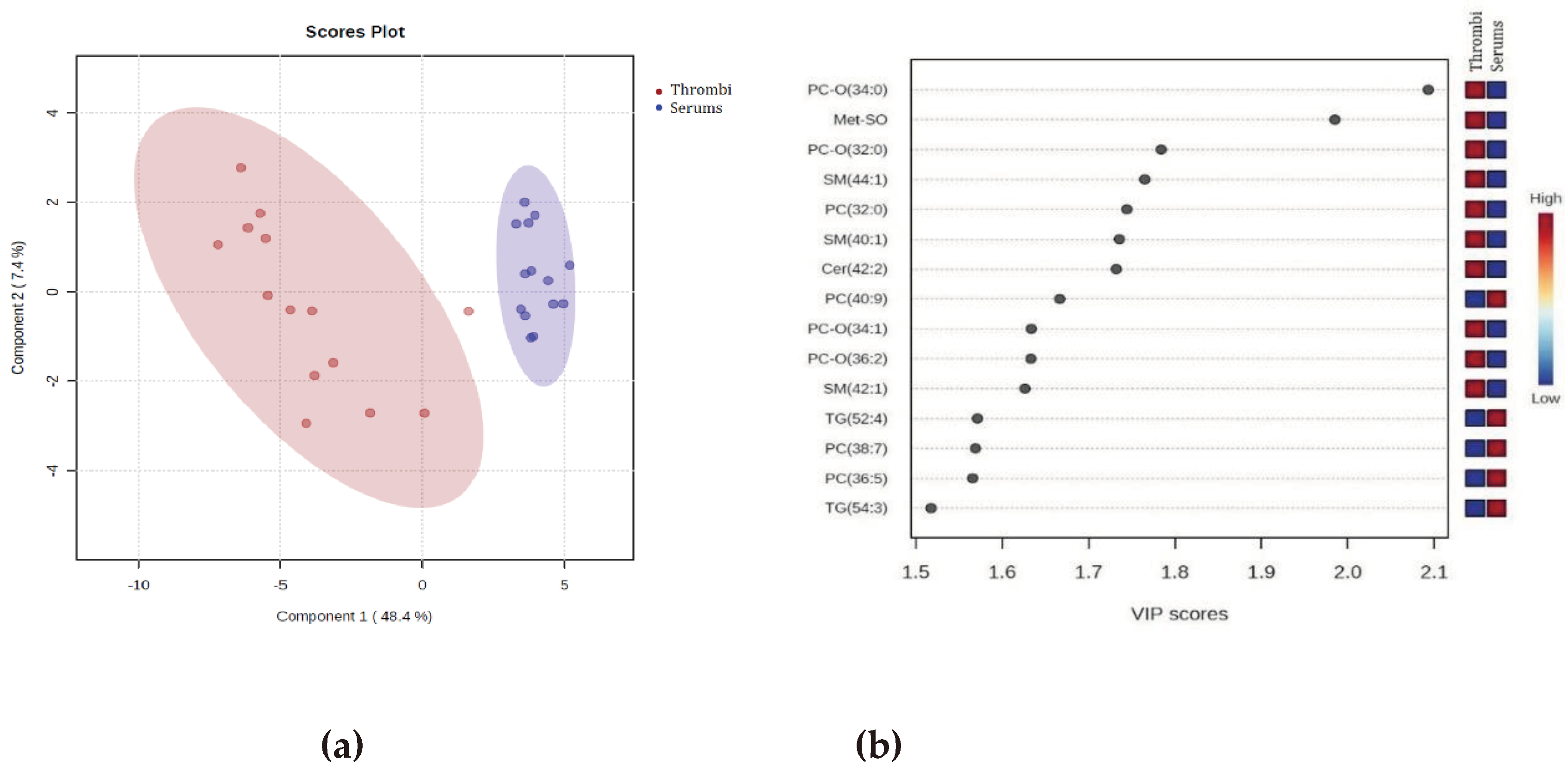
Figure 5.
Hierarchical cluster analysis (HCA) of the significant different metabolites obtained using t-test (p < 0.05) between two groups (stroke thrombi - red panel; patient serum samples - green panel). Each coloured cell on the map corresponds to the intensity value, red colour - max metabolite concentration, green colour - min metabolite concentration. Data was normalization by median, log transformed and Pareto-scaled. TG - triglyceride, PC - phosphatidylcholine; PC-O - ether phosphatidylcholine; Gln - glutamine, Arg - arginine; LPC - lysophosphatidylcholine; SM - sphingomyelin; Cer - ceramide; DG - diglyceride; AC- acylcarnitine; t4-OH-Pro - trans-4-hydroxy-L-proline; Cit - citruline; Ala - alanine; Met - methionine; Phe - phenylalanine; Tyr - tyrosine; Gly - glycine; Val - valine; Met-SO - methionine sulfoxide Met-SO - methionine sulfoxide; H1 - hexoses (including glucose).
Figure 5.
Hierarchical cluster analysis (HCA) of the significant different metabolites obtained using t-test (p < 0.05) between two groups (stroke thrombi - red panel; patient serum samples - green panel). Each coloured cell on the map corresponds to the intensity value, red colour - max metabolite concentration, green colour - min metabolite concentration. Data was normalization by median, log transformed and Pareto-scaled. TG - triglyceride, PC - phosphatidylcholine; PC-O - ether phosphatidylcholine; Gln - glutamine, Arg - arginine; LPC - lysophosphatidylcholine; SM - sphingomyelin; Cer - ceramide; DG - diglyceride; AC- acylcarnitine; t4-OH-Pro - trans-4-hydroxy-L-proline; Cit - citruline; Ala - alanine; Met - methionine; Phe - phenylalanine; Tyr - tyrosine; Gly - glycine; Val - valine; Met-SO - methionine sulfoxide Met-SO - methionine sulfoxide; H1 - hexoses (including glucose).
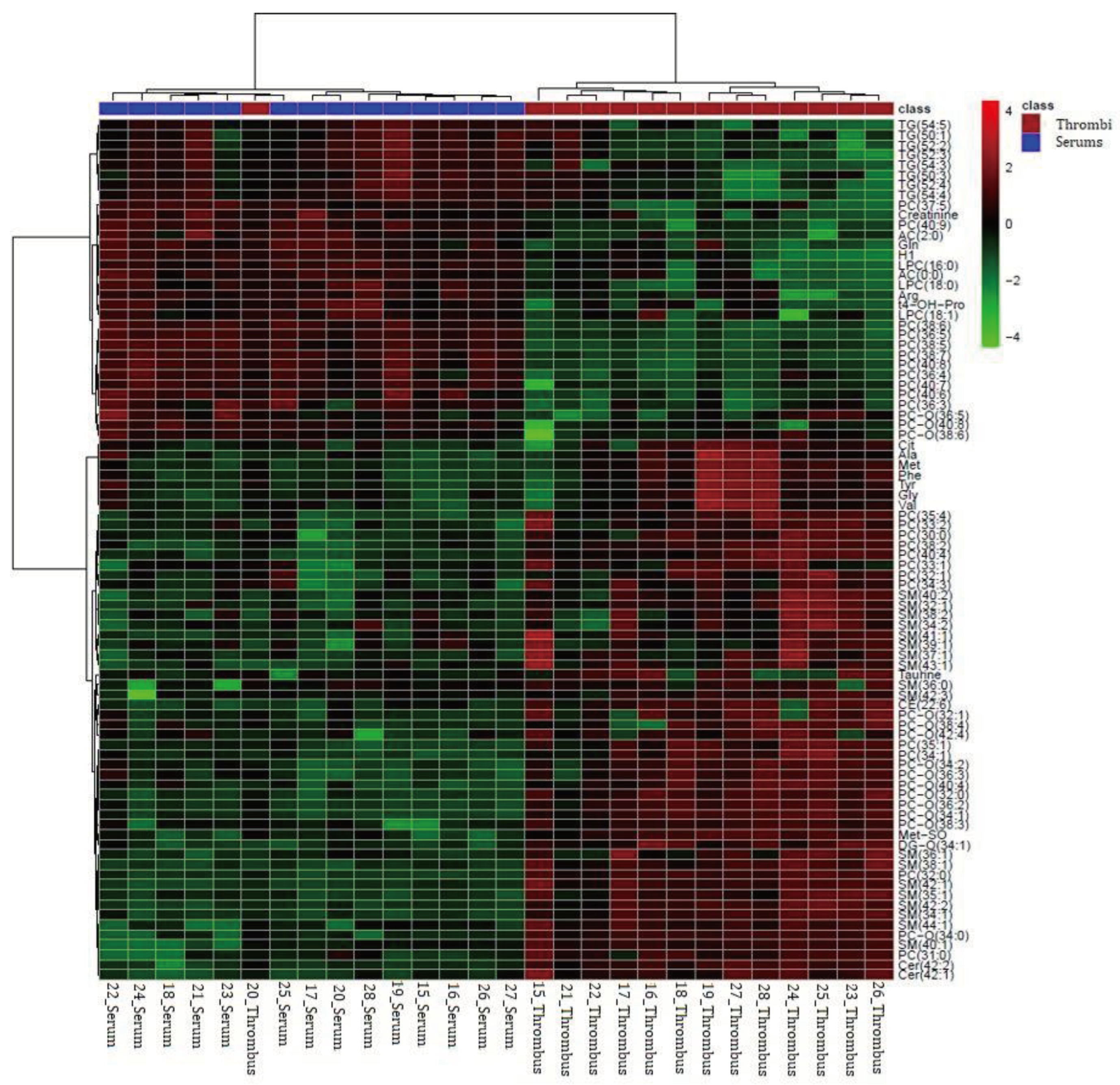
Figure 6.
Concentrations of significantly altered metabolites in stroke thrombi samples vs. patient serum samples that overlap in univariate (t-test) and multivariate (PLS-DA) analyses. Data are presented as box and whiskers plot (mean ± SD). Red - stroke thrombi samples, green - patient serum samples. TG - triglyceride; PC-O - ether phosphatidylcholine; LPC - lysophosphatidylcholines; SM - sphingomyelins; PC - phosphatidylcholine; Cer - ceramide.
Figure 6.
Concentrations of significantly altered metabolites in stroke thrombi samples vs. patient serum samples that overlap in univariate (t-test) and multivariate (PLS-DA) analyses. Data are presented as box and whiskers plot (mean ± SD). Red - stroke thrombi samples, green - patient serum samples. TG - triglyceride; PC-O - ether phosphatidylcholine; LPC - lysophosphatidylcholines; SM - sphingomyelins; PC - phosphatidylcholine; Cer - ceramide.
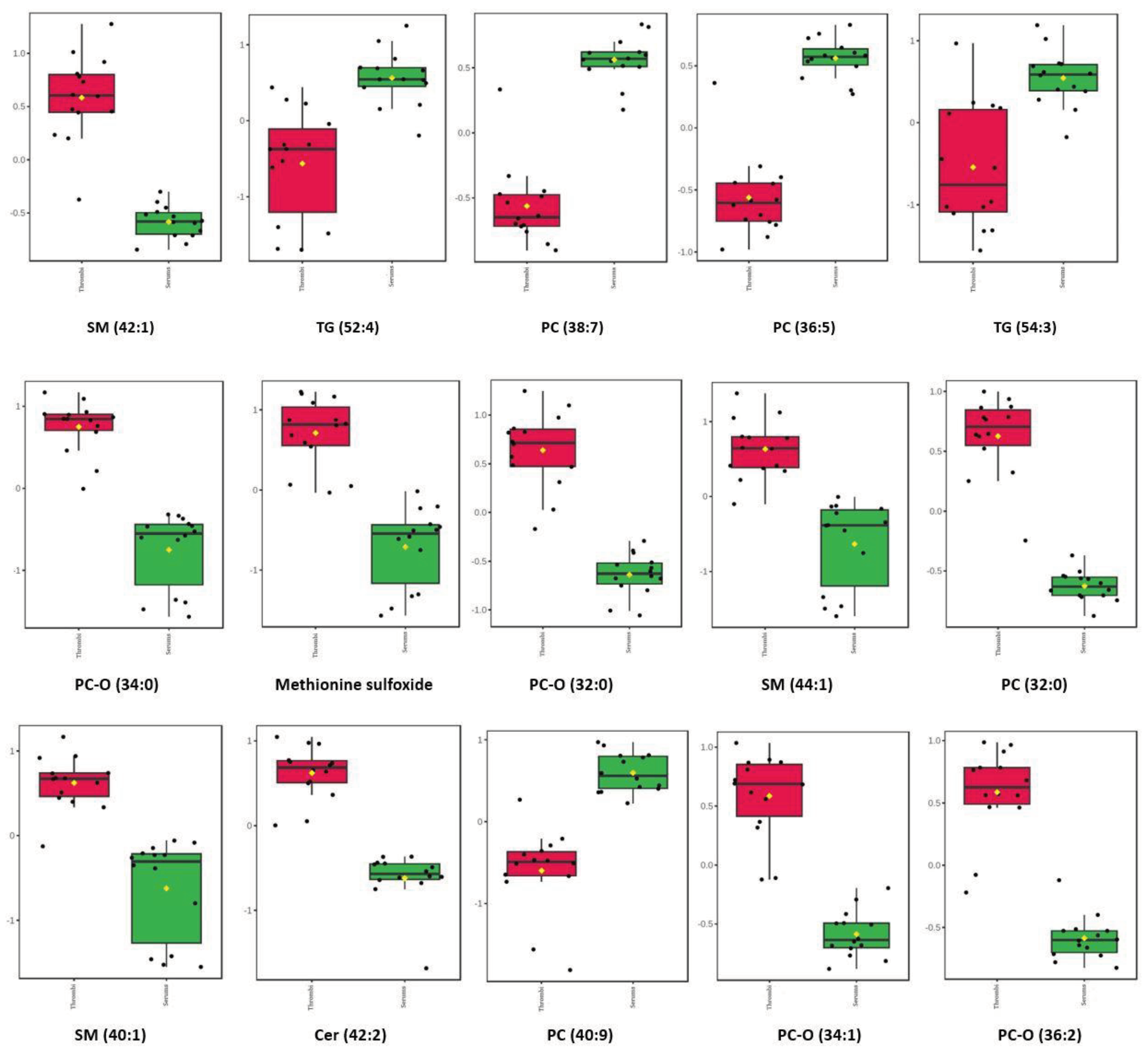

Table 1.
Stroke thrombi mass and isopropanol volume.
| Stroke thrombi samples |
Mass/mg | Volume of isopropanol / μL |
|---|---|---|
| 1. | 27.1 | 81.3 |
| 2. | 27.8 | 83.4 |
| 3. | 30.8 | 92.4 |
| 4. | 71.0 | 213.0 |
| 5. | 56.5 | 169.5 |
| 6. | 20.8 | 62.4 |
| 7. | 32.8 | 98.4 |
| 8. | 29.3 | 87.9 |
| 9. | 37.0 | 111.0 |
| 10. | 20.8 | 62.4 |
| 11. | 52.2 | 156.6 |
| 12. | 13.3 | 39.9 |
| 13. | 20.7 | 62.1 |
| 14. | 30.9 | 92.7 |
Table 2.
Basic and laboratory characteristics of study participants.
| Patient | Control | p-value | |
|---|---|---|---|
| Age | 70.36±12.82 | 52.29±15.09 | 0.002 |
| Sex M/F | 8/6 | 8/6 | |
| BMI (kg/m2) | 26.34±4.07 | 23.79±5.35 | 0.192 |
| DBP (mmHg) | 79.71±9.21 | 83.79±14.46 | 0.382 |
| SBP (mmHg) | 146.43±16.70 | 135.50±14.31 | 0.074 |
| TG (mmol/L) | 1.51±0.47 | 1.49±0.73 | 0.907 |
| tCH (mmol/L) | 5.17±0.67 | 5.11±1.10 | 0.874 |
| LDL-CH (mmol/L) | 3.07±1.16 | 3.09±1.08 | 0.962 |
| HDL-CH (mmol/L) | 1.02±0.19 | 1.22±0.37 | 0.079 |
| Glucose (mmol/L) | 8.12±1.26 | 5.73±0.85 | <0.0001 |
| PV | 0.91±0.17 | 0.98±0.14 | 0.251 |
| aPTT | 24.37±1.79 | 23.79±2.48 | 0.485 |
| INR | 1.07±0.10 | 1.04±0.06 | 0.464 |
M, male; F female; BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure TG, triglycerides, tCH, total cholesterol; HDL-CH, high-density lipoprotein cholesterol; LDL-CH, low-density lipoprotein cholesterol; PT, prothrombin time; aPTT, activated partial thromboplastin time; INR, international normalized ratio. Data are expressed as mean ± standard deviation (SD). Differences between groups were evaluated by Student’s t-test due to normal distribution of all parameters.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



