
Submitted:
22 February 2024
Posted:
22 February 2024
You are already at the latest version
Abstract
Carbapenem antibiotics are the drug of choice for treating multidrug-resistant bacterial infections. Metallo-beta-lactamases (MBLs) are carbapenemase capable of hydrolyzing nearly all therapeutically available beta-lactam antibiotics. Consequently, a need to assess the frequency and phenotypic resistance phenomena of two MBL genes in diarrheal and urinary tract infections (UTIs). Samples were collected through a cross-sectional study, with MBLs genes detected via PCR. Two hundred twenty eight diarrheal bacteria were isolated from 240 samples. The most predominant pathogens were Escherichia coli (32%) and Klebsiella spp. (7%). Phenotypic resistance to amoxicillin-clavulanic acid, aztreonam, cefuroxime, cefixime, cefepime, imipenem, meropenem, gentamicin, netilmicin, and amikacin was 50.4%, 65.6%, 66.8%, 80.5%, 54.4%, 41.6%, 25.7%, 41.2%, 37.2%, and 42.9%, respectively. Total 142 UTI pathogens were obtained from 150 urine samples, with Klebsiella spp. (39%) and Escherichia coli (24%) are the major pathogens. Phenotypic resistance to amoxycillin-clavulanic acid, aztreonam, cefuroxime, cefixime, cefepime, imipenem, meropenem, gentamicin, netilmicin, and amikacin was 93.7%, 75.0%, 91.5%, 93.7%, 88.0%, 72.5%, 13.6%, 44.4%, 71.1%, and 43%, respectively. Twenty four diarrheal isolates carried either blaNDM-1 or blaVIM genes; the overall MBL gene prevalence was 10.5%. Thirty six UTI pathogens carried either blaNDM-1 or blaVIM genes (25.4%). Seven isolates carried both blaNDM-1 and blaVIM genes. MBL genes exhibited a strong association with phenotypic carbapenem and other beta-lactam antibiotic resistance. Resistance to carbapenems requires active surveillance and stewardship.
Keywords:
Bangladesh
; Metallo-beta-lactamase
; bla-NDM-1
; bla-VIM
; antimicrobial resistance
; co-resistance
; diarrhea
; urinary tract infections
; antimicrobial stewardship programs
1. Introduction
Carbapenems are last-line antibiotics prescribed for treating multidrug-resistant (MDR) Gram-negative bacterial infections [1]. As such, their prescribing should be carefully managed, assisted by designating them as ‘Watch’ antibiotics to be used with care and subject to antimicrobial stewardship programs to reduce antimicrobial resistance (AMR) [2,3]. However, there are concerns with rising rates of AMR in Bangladesh, enhanced by sub-optimal healthcare standards and high levels of misuse of antibiotics [4,5,6,7,8,9]. This includes appreciable purchasing of ‘Watch’ antibiotics without a prescription, adding to AMR despite current legislation exacerbated by their ready availability in drug outlets [10,11,12,13,14].
The emergence of carbapenemase-producing organisms (CPO) with the capacity to hydrolyze carbapenem antibiotics has been reported worldwide [15,16,17], and is an increasing concern [18,19]. Primarily Klebsiella pneumoniae was reported as only carbapenemase-producing bacteria; subsequently, different other bacterial species within the order of Enterobacterales were found with the competence of carbapenem-hydrolysis and labeled as Carbapenem-Resistant Enterobacterales (CRE) [20]. However, a notable heterogeneity exists in the mechanisms of CRE [18,21,22]. There are mainly two types of CRE depending on the carbapenemase production capacity: carbapenemase-producing (CP)-CRE and non-CP-CRE [23]. Earlier research identified that CP-CRE is more virulent than non-CP-CRE, and is associated with substantially higher mortality [18,23].
CPO can be transmitted between patients more conveniently with the help of transferable integrons and mobile genetic elements (MGEs) than non-CPO [21,24,25]. Biochemically, carbapenemases are categorized into two major groups: the first is serine-beta-lactamase, which includes serine at their active site and hydrolyzes the amide bond in the beta-lactam ring of antibiotics. The second category comprises metallo-β-lactamases (MBLs), enzymes containing necessary zinc ions in their active sites that enable intended drugs to undergo hydrolytic [18]. Nine types of MBLs have been documented, of which three genes are globally prevalent, i.e. blaIMP, blaNDM, and blaVIM) [26]. The MBL-group antibiotic resistance genes (ARGs) are increasingly considered as emerging hazards and significant threats to global public health [27].
In low and middle-income countries (LMICs), diarrhea is a significant contributor to child mortality [28,29]. Overall, pediatric diarrhea currently accounts for more than 1.7 billion cases annually, resulting in pediatric diarrhea being the second leading cause of mortality in children aged five and below [30]. In 2017, it was estimated that pediatric diarrhea was responsible for over 533,000 deaths globally in children under five years of age, giving an estimated mortality rate of 78.4 (70.1-87.1) per 100,000 children [31]. Moreover, dehydration caused by diarrhea also contributes significantly to approximately 1.5 to 2.5 million deaths annually among young children [30]. Consequently, identification and management need to be taken seriously.
Potential MDR in diarrheal bacteria arises from selective pressure from sustained antimicrobial exposure, especially antibiotics from the ‘Watch’ and ‘Reserve’ groups [14]. As a result, complicating treatment, resulting in numerous antibiotics having limited potency. Consequently, treating causative bacteria is becoming difficult and expensive [32]. Carbapenem-resistant hypervirulent diarrheal pathogens have now been reported in several countries as global emerging health threats [33,34], which need to be taken seriously to reduce future morbidity, mortality, and costs associated with AMR [35,36,37,38].
Urinary tract infections (UTIs) are among the most prevalent and endemic bacterial diseases globally [39,40]. Currently, approximately 40% of women have experienced a UTI at some point in their life [41]. The commonly associated uropathogens are Escherichia coli, Klebsiella pneumonia, K. oxytoca, Citrobacter freundii, Pseudomonas aeruginosa and Serratia marcescens [40]. However, increasing resistance to carbapenems among pathogens that cause common UTI infections has become an emerging problem [42,43,44].
All the diarrheal pathogens and most UTI bacteria belong to the Enterobacterales order of gram-negative bacteria that are increasingly resistant to carbapenem antibiotics in clinical and community settings worldwide [17,45]. The World Health Organization (WHO) has labeled CRE as a global priority pathogen, considering their high transmission ability and hypervirulent emergence capacity [46]. Coordinated healthcare efforts and public health initiatives are imperative to prevent the transmission of CPO. Multiple studies have emphasized the need for continuous surveillance covering the epidemiology, phenotypic susceptibilities, and nucleic acid–based carbapenemase detection analyses, which are crucial to implementing appropriate treatments and controlling the spread of CPOs [47,48,49]. Such activities can be performed under the umbrella of antimicrobial stewardship programs (ASPs) [50,51,52]. There have been concerns regarding available resources and personnel to undertake ASP activities in LMICs [51,53]. However, this is now changing [54,55,56], although there are still concerns with their implementation in Bangladesh [57].
The present study investigated the prevalence of two classical MBL genes, blaVIM and blaNDM-1, and associated phenotypic resistance in pathogens isolated from diarrhea and UTI cases in Dhaka, Bangladesh. The findings can be used to guide future activities among all key stakeholder groups in Bangladesh, given rising concerns in these priority groups, building on the experiences in other countries [58].
2. Materials and Methods
We first documented the study plan and how samples were collected before isolating and detecting bacteria, antimicrobial susceptibility testing, and minimum inhibitory concentrations. Finally, molecular detection of MBL genes and data analysis were done.
2.1. Study plan and sample collections
A longitudinal cross-sectional study was conducted from January 2020 to December 2020 to analyze carbapenem-resistance in diarrheal bacteria. Most of the study subjects were enrolled between April and August 2020, when diarrheal episodes soared in Bangladesh. Stool samples were collected from patients with acute diarrhea from Uttara Adhunik Medical College Hospital in Uttara, Dhaka, Bangladesh. Samples were collected aseptically in sterile containers. The samples were subsequently transferred to the university laboratory, which maintained the cold storage facilities. Samples were then processed and cultured on the same day to obtain the best results.
Urine samples were collected between April 2018 and March from Gonoshasthaya Samaj Vittik Medical College, located in Savar, and Gonoshasthaya Nagar Hospital in Dhaka. Patients were provided with sterile vials, and midstream urine samples were collected aseptically and kept at 4 ͦ C before transporting them to the university laboratory. Urine samples were transported in an insulated ice box to the laboratory.
The study patients also completed a standard questionnaire containing basic demographic data. Exclusion criteria included terminally ill and immunodeficient patients, particularly those with cancer, transplant, tuberculosis, kidney diseases, and HIV/AIDS.
2.2. Isolation and identification of bacteria
Diarrheal stools were diluted in phosphate-buffered saline and inoculated on Eosin-methylene blue-Levine (EMB-Levine) agar (Liofilchem Inc, Italy), Thiosulfate-citrate-bile salts-sucrose Agar (TCBS) (Oxoid Ltd, Basingstoke, UK) and Salmonella-Shigella (SS) Agar (Oxoid Ltd, Basingstoke, UK) simultaneously. EMB agar is selective for gram-negative bacteria, TCBS agar is selective for Vibrio spp., particularly for V. cholerae and V. parahaemolyticus, and SS agar is fairly selective and differential for Salmonella spp. and some Shigella strains. Following inoculation, the agar plates were incubated for 18-24h at 37 ͦ C. The UTI samples were plated onto CLED media (Liofilchem Inc, Italy) and MacConkey agar (Liofilchem Inc, Italy) media. CLED media supports both gram-positive and gram-negative bacteria, while MacConkey agar is a selective media for gram-negative bacteria only. These plates were kept in aerobic condition at 37˚C for 24 h. For a specific type of pure culture, a single colony was taken from the culture plate and subsequently streaked onto Trypticase Soy agar (TSA) media and then incubated overnight at 37 ͦ C. Bacterial isolates were first presumptively identified by various biochemical methods including Kligler Iron Agar (KIA), IMVIC (Indole, Methyl red, Voges-Proskauer and Citrate utilization), catalase and oxidase tests. API 20E (bioMerieux Inc., France) kit was used to identify Enterobacterales and other Gram-negative rods. Bacterial identifications were further confirmed by 16s rDNA sequencing (Macrogen Inc., South Korea).
2.3. Antimicrobial susceptibility test
Antimicrobial susceptibility patterns of the study isolates were obtained using the Kirby-Bauer disk diffusion method. The classical β-lactam antibiotics, Amoxicillin-clavulanic acid (30 μg), Cefuroxime Sodium (30 μg), cefixime (30 μg), Cefepime (30 μg) were evaluated. For carbapenems, imipenem (10 μg) and meropenem (10 μg) were tested. Aztreonam (30 μg) was examined from the monobactam group. As aminoglycoside representative, gentamicin (30 μg), netilmicin (30 μg), and amikacin (30 μg) were examined.
According to the standard guideline provided by the Clinical and Laboratory Standards Institute (CLSI), a point five McFarland turbidity standard was prepared. Subsequently, the suspensions were subsequently plated onto Mueller–Hinton agar (MHA) (Oxoid, Basingstoke, UK) media. Using sterile forceps, antibiotic discs were then properly placed onto the media, and the plates were then put in an incubator (37ºC) for overnight incubation. The sensitive bacteria were inhibited by the diffused antibiotics and developed a zone of clearance around the disc. The zone diameter was subsequently measured for evaluating antibiotic susceptibility patterns. Escherichia coli ATCC25922 was used as the susceptible-control reference strain for disc diffusion testing. The multiple antibiotic resistance (MAR) index was calculated and interpreted using the formula: x/y, where ‘x’ represents the number of antibiotics to which an isolate was resistant, and ‘y’ represents the total number of antibiotics tested [59].
2.4. Determining minimum inhibitory concentrations (MIC)
After determining the antimicrobial susceptibility pattern, the agar dilution method was used to ascertain the minimal concentration of meropenem (MIC) needed to prevent bacterial growth. In this method, different concentrations of meropenem powder were used in MHA medium from 0.5 to 32 μg/ml. For the inoculum preparation, one pure culture colony was inoculated into TSB media and kept at 37 °C for two to three hours. To compare visually, a 0.5 McFarland standard was used (density 108 CFU/ml). Plates were inoculated using a micropipette, and the inoculum was allowed to dry without moving the plates. The plates were inverted and placed into the incubator at 37 °C for 18 to 20 h. A control plate without meropenem was used to test the growth of the bacterial isolates. The Etest for meropenem was done in parallel using strips (Liofilchem Inc, Italy) carrying antibiotic concentration gradient (from 0.016 to 256 μg/mL) to validate the agar microdilution MIC results [60]. Results were interpreted for Enterobacteriaceae as per CLSI guidelines, and the clinical breakpoints for meropenem resistance were considered when the MIC value was ≥ 4 μg/mL [61].
2.5. Molecular detection of metallo-beta-lactamase (blaNDM-1 and blaVIM) genes
Polymerase chain reactions were used to detect two MBL genes, such as blaNDM-1 and blaVIM in all the diarrheal and UTI bacterial isolates. The template bacterial DNA was extracted by the boiling method from bacteria cultured on nutrient agar media [62]. Specific primer sets for the respective MBL genes were obtained previous literature [63] and prepared by a commercial manufacturer (IDT Singapore Pte Ltd, Singapore). For a single PCR reaction, 12 μL 2X PCR pre-mixture (Thermo Fisher Scientific Inc., CA) was mixed with 2.0 μL prepared bacterial DNA, five picomols of each primer (1 μL), and the deionized water to make a final volume of 24 μL. Reactions went through 95°C for 10 min for an initial denaturation followed by 32 cycles of amplification by a thermal cycler (Applied Biosystems 2720 , Singapore), following denaturation 30s at 94 ° C, annealing 30s at 54–56 °C based on two primer sets, extension 1 min at 72°C, and a final extension of 7 min at 72° C. Amplified PCR products were subjected to electrophoresis through 1.2% agarose gel at 100 volts for 30 minutes, then stained with ethidium bromide, and visualized under UV light. A molecular weight standard was run beside to measure the amplified PCR product sizes (GeneRuler, Thermo Fisher Scientific, CA)
2.6. Data analysis
The SPSS statistical software package (version 25) was used to enter and analyze data. Descriptive and inferential statistical methods were utilized to describe diarrheal, the UTI pathogens, various metallo-beta-lactamase genes they carried, and their phenotypic characteristics. Pearson’s Chi-square test tested associations between various categorical data. Statistical significance was measured by computing a two-tailed p-value (≤0.05).
2.7. Ethical clearance
The Ethics and Research Review Committee of the Biological Sciences Faculty, Jahangirnagar University gave its two separate approvals to study diarrheal pathogens [(BBEC/JU M2017 3(3), dated 15th March 2017] and UTI etiology [(BBEC/JU M2017 3(4), dated 15th March 2017]. Ethical permission taken from JU was accepted among the three hospitals from where samples were collected. Every research technique conformed with the Declaration of Helsinki for human subjects' medical research. In the case of adult participants, urine and diarrheal samples were obtained with written consent. Written informed consent from legal guardians was taken for those who were younger than 18 years old. Privacy of the personal information was strictly protected.
3. Results
3.1. Study population
A total of 240 diarrheal samples were obtained from patients with acute diarrhea attending Uttara Adhunik Medical College Hospital. Clinical symptoms of the patients included 3 to 5 times bowl movement with loose stools for the last 2–3 days, with or without fever, vomiting, and abdominal pain. Bacteria were detected in 228 samples. The overall detection rate of bacteria was 95.0% (228/240). The diarrheal episodes were well distributed by gender (134 males [56%] and 106 females [44%]). The age range was from three months to 80 years. The median age was one year. Further subclassification showed that the children within the ten-year age group accounted for over 80% of cases. Table 1 shows the frequency of diarrheal bacteria isolation by the age of the study participants.
A total of 150 urine specimens with UTI infections were collected from two hospitals in Dhaka and cultured on MacConkey agar and Trypticase soy agar plates. Bacteria were detected in 142 samples; the overall detection rate was 94.67% (142/150). Among these, 34 (24%) patients were male and 108 (76%) patients were female. The age range of UTI-positive patients was 4 to 76 years. A 10-year range age classification identified the highest UTI infections in the 21-30 years age-group (35.2%). UTI cases were identified higher among females (76.1%, 108/142) compared to males (23.9%, 34/142). The detailed age distribution of diarrheal and UTI patients is shown in Table 1.
3.2. Bacterial prevalence
Various bacterial species were isolated and identified from collected diarrheal specimens, such as 102 Escherichia coli (44.7%), 20 Klebsiella spp. (8.8%), 19 Escherichia fergusonii (8.3%), 13 Citrobacter freundii (5.7%), 15 Enterobacter spp. (6.6%) including Enterobacter hormaechei, E. cloacae, E. mori, and E. tabaci. Other low frequently identified bacteria were Shigella spp., Acinetobacter nosocomiali, A. radioresist, Aeromonas caviae, Bacillus cereus, Citrobacter europaeus, C. murliniae, C. pasteuri, Enterococcus faecium, E. gilvus, E. hirae, Klebsiella oxytoca, K. variicola, Proteus mirabilis, Pseudomonas parafulva, Serratia marcescens, Staphylococcus warneri, Staphylococcus epidermidis, and Vibrio neocaledonicus. A wide variety of bacteria were isolated from collected urine samples dominated by 56 Klebsiella spp. (39%), 34 Escherichia coli (24%), 17 Enterobacter spp. (12.0%), 14 Proteus spp. (10%), 14 Pseudomonas spp. (10%), 5 Staphylococcus spp. (3%). The other identified UTI pathogens were Acinetobacter pittii, Enterobacter cloacae, E. hormaechei, Proteus mirabilis, and Pseudomonas putida.
3.3. Phenotypic resistance and minimum inhibitory concentration
Among 228 isolates obtained from the diarrheal samples, resistance against beta-lactam and aminoglycoside antibiotics was observed. Among the isolates, 50.4% showed resistance to amoxicillin + clavulanic acid, 65.5% to aztreonam, 66.8% to cefuroxime, 80.5% to cefixime, 54.4% to cefepime, 41.6% to imipenem, 25.7% to meropenem, 41.2% to gentamicin, 37.2% to netilmicin and 42.9% to amikacin. Meropenem showed maximum activity, while cefixime, a third-generation cephalosporin, was the least active.
Among the 142 UTI isolates, 93.7% showed resistance to amoxicillin + clavulanic acid, 75.0% to aztreonam, 91.5% to cefuroxime, 93.7% to cefixime, 88% to cefepime, 72.5% to imipenem, 13.6% to meropenem, 44.4% to gentamicin, 71.5% to netilmicin and 43% to amikacin. For UTI isolates, meropenem also showed the highest potency, while amoxicillin plus clavulanic acid and cefixime were the least active antibiotics. For overall cases, UTI pathogens exhibited very significantly higher resistance (p=0.001) against β-lactam antibiotics and aminoglycoside antibiotics tested except for meropenem (Figure 1A). Significant higher resistance of meropenem by disk-diffusion test in diarrheal pathogens (p=0.001) showed good agreement with the meropenem-MIC assay (Figure 1B). The isolates exhibited varying degrees of meropenem MIC, ranging from ≤0.5 to ≥32 µg/ml. Most isolates were sensitive (MIC, ≤1 µg/ml). Pathogens with MIC values of ≥4 µg/ml were considered resistant. MIC value ≥32 µg/mL of meropenem was found in over 21% of diarrheal pathogens compared to 5% of UTI pathogens (Figure 1B, p=0.001).
3.4. Prevalence of MBL Genes
Among the 228 diarrheal isolates, both blaNDM-1 and blaVIM genes were detected in 12 (5.3%) isolates where the carriage of blaNDM-1 and blaVIM genes were mutually exclusive. Among the 142 UTI isolates the blaNDM-1 gene was detected in 13 (9.2%) isolates, and the blaVIM gene was detected in 23 (16.2%) isolates. Overall, a significantly higher prevalence of the two MBL genes was identified in UTI isolates compared to diarrheal pathogens (p=0.001).
3.5. Association of Phenotypic and Genotypic (blaNDM-1 and blaVIM gene) Resistance
There were 228 diarrheal isolates of which 12 isolates were blaNDM-1 positive and other 12 isolates were blaVIM positive. Of the 12 blaNDM-1 positive isolates, 67% were resistant to amoxicillin + clavulanic acid and Imipenem, 58.2% to aztreonam, 50% to cefuroxime and cefepime, 83% to cefixime, 41.7% to meropenem, gentamicin, and amikacin, 25% to netilmicin. However, of the 216 blaNDM-1 negative isolates, 49.5% to amoxicillin + clavulanic acid, 66% to aztreonam, 68% to cefuroxime, 80% to cefixime, 55% to cefepime, 40% to imipenem, 25% to meropenem, 41% to gentamicin, 38% to netilmicin and 43% to amikacin. We detected a very weak association between the phenotypic resistance of some beta-lactam and aminoglycoside antibiotics and the presence of blaNDM-1 (aztreonam, cefuroxime, cefixime, cefepime, gentamicin, and netilmicin). Resistance percentages between blaNDM-1 positive and blaNDM-1 negative pathogens appeared almost equal against these antibiotics. However, the association is quite strong in the case of amoxicillin + clavulanic acid, imipenem, meropenem, and amikacin (Figure 2A).
Among the 12 blaVIM-positive diarrheal isolates, 50% were resistant to amoxicillin + clavulanic acid and cefepime, 58% to aztreonam, 67% to cefuroxime, cefixime, and gentamicin, 75% to imipenem, 41.7% to meropenem, and 25% to netilmicin, and 33% to amikacin. However, of the 216 blaVIM negative isolates, 50.5% were resistant to amoxicillin + clavulanic acid, 66% to aztreonam and cefuroxime, 81.3% to cefixime, 54.7% to cefepime, 39.7% to imipenem and gentamicin, 24.8% to meropenem, 38% to netilmicin and 43.5% to amikacin. Consequently, the absence or presence of the blaVIM gene in diarrheal isolates has only a limited effect on the resistance to most of the antibiotics used in this study except imipenem (p=0.05), meropenem (p=0.25) and gentamycin (p=0.17), which is shown in Figure 2B.
There were 142 UTI isolates, of which 13 isolates were blaNDM-1 positive, and the other 23 isolates were blaVIM positive. Among the 13 blaNDM-1 positive isolates, all were resistant to amoxicillin + clavulanic acid, cefuroxime, cefixime, cefepime, gentamicin, netilmicin and amikacin, 84.6% to imipenem, 77% to aztreonam and 69% to meropenem. blaNDM-1 negative isolates also showed a similar level of resistance to amoxicillin + +clavulanic acid, aztreonam, cefuroxime, cefixime, cefepime, and imipenem. Amoxicillin + clavulanic acid, cefuroxime, and cefixime seemed almost ineffective for UTI infections regardless of the presence of the blaNDM gene. However, meropenem (p=0.000), gentamicin (p=0.000), netilmicin (0.05), and amikacin (p=0.001) antibiotics appeared to have more effect on isolates without the blaNDM gene (Figure 2C).
Among the 23 blaVIM-positive isolates, all were resistant to amoxicillin + clavulanic acid and cefuroxime. 96% to cefixime and cefepime, 87% to aztreonam, imipenem and netilmicin, 83% to gentamicin, 65% to amikacin and 39% to meropenem. However, blaVIM-negative isolates also showed similar resistance levels to amoxicillin + clavulanic acid, aztreonam, cefuroxime, cefixime, and cefepime but were more susceptible to imipenem (p=0.17), meropenem (p=0.000), gentamicin (p=0.000), netilmicin (p=0.18) and amikacin (p=0.06). UTI isolates were most susceptible to meropenem (p=0.000) (Figure 2D).
The associations of MIC values for meropenem were further analyzed for the two MBL-carrying diarrheal and UTI pathogens. The MIC levels for diarrheal isolates carrying the MBL genes (blaNDM-1 and blaVIM) were almost equal with pathogens without MBL genes (Table 2). However, the UTI isolates with the carriage of blaNDM-1, and blaVIM appeared with significantly higher levels of meropenem MIC (Table 2).
3.6. Co-Resistance Phenotype and Multiple Antibiotic Resistance (MAR) Index
Among all 370 bacterial isolates in our study, 60 carried at least one of the two MBL genes (blaNDM-1, blaVIM). Most of these isolates carried only one type of gene, although some carried both genes. Co-existing MBL genes were found in 7 (13%) bacterial isolates, while the other 53 (87%) isolates carried only one MBL gene. Only blaNDM-1 carrying five isolates showed resistance to all the beta-lactam and aminoglycoside antibiotics tested, while the other 10 showed sensitivity to a wide variety of these antibiotics. MAR index values appeared from 0 (absolute sensitive) to 1 (absolute resistant) based on the ten antibiotics tested by disk diffusion (Table 3).
Only blaVIM-containing isolates also exhibited a similar pattern of resistance and sensitivity. MAR index values for blaVIM-positive pathogens were 0.2-1.0. In contrast, when blaVIM and blaNDM-1 co-exist, only one isolate appeared sensitive to meropenem, and the other five isolates were completely resistant to all the antibiotics tested (Table 3). MAR index values for all the co-carrying of two MBL genes were very high, 0.9 to 1.0 (Figure 3).
4. Discussion
This study identified the prevalence of two MBL genes in diarrheal and UTI samples in Bangladesh. The rate of detection of blaNDM-1 and blaVIM genes was almost equal in the diarrheal and UTI samples, which was approximately ten percent. This rate is similar to the prevalence rate observed previously in India [64]; however, lower than those found in Northeast Iran [65]. These variations in prevalence rates may result from sample size, variations in antibiotic use patterns, and dissemination across different geographic regions. Currently, the prevalence of MBL genes is not very high in Bangladesh compared to other ESBL genes, probably because carbapenem antibiotics are still limited in Bangladesh. However, these genes spread rapidly and pose a great danger to human health in Bangladesh, along with high consumption of antibiotics from the ‘Watch’ list, including those dispensed without a prescription [10,11]. Numerous issues in managing infections by MBL producers remain unresolved due to a lack of clinical experience and contradictory epidemiological data. These need to be addressed going forward as part of the National Action Plan in Bangladesh to reduce AMR and beyond [66].
This study reported the association of MBL genes to phenotypic antibiotic resistance. In the case of diarrheal isolates, almost three-fourths of the blaNDM-1 positive isolates showed resistance to all the beta-lactam antibiotics used; however, there was less resistance to aminoglycosides. Having said this, blaNDM-1 negative isolates also showed a similar resistance rate to aztreonam, cefuroxime, cefixime, cefepime, gentamicin, and netilmicin. However, in the case of amoxicillin + clavulanic acid, imipenem, meropenem, and amikacin, the resistance rate was much lower in blaNDM-1 negative isolates compared to blaNDM-1 positive isolates. Encouragingly, blaNDM-1 negative isolates were still susceptible to meropenem. This needs to remain with their prudent use.
In the case of UTI isolates, all blaNDM-1 positives were fully resistant to amoxicillin + clavulanic acid, cefuroxime, cefixime, cefepime, gentamicin, netilmicin and amikacin and almost fully resistant to imipenem and meropenem. In addition, the blaNDM-1 negative UTI isolates also showed a similar level of resistance to all the beta-lactam antibiotics as blaNDM-1 positives except meropenem. However, they showed a much lower level of resistance to aminoglycosides. Other ESBL or resistance genes or variables that were not examined in this investigation may account for the inconsistent genotype-phenotype correlation. However, this remains to be seen. Sample size could also be a factor in this case. A substantial correlation between MDR and the presence of ESBL genes was also found by Manandhar et al. [67]. A similar association was also seen for blaVIM gene and phenotypic resistance to imipenem, meropenem and the three aminoglycosides. The resistance rate to meropenem was very low, which is also encouraging for the future. However, again there needs to be considerable care with the prescribing and dispensing of this antibiotic to prevent the development of resistance in Bangladesh.
When the blaNDM-1 or blaVIM genes were present, they displayed decreased sensitivity to every antibiotic tested. These findings are similar to other published studies [44,68]. However, the coexistence of these two genes showed increased resistance to beta-lactam and aminoglycoside antibiotics. Bacteria can accumulate a number of genes due to the co-resistance phenomena. The coexistence of multiple genes in the same bacteria results in enhanced resistance to various antimicrobials [44,69], which again needs to be avoided where possible. In this study, when both MBL genes co-exist, they were resistant to all the beta lactam and aminoglycosides tested except to meropenem in only one isolate. Notably, in our study, all six isolates carrying both MBL genes were UTI isolates. Empirical antibiotics are traditionally used to treat uncomplicated UTIs. It is possible that over time, bacteria developed more co-resistance as a result of this frequent use. Consequently, educational and ASP activities are needed among healthcare professionals and patients to enhance the appropriate use of antibiotics in these conditions [55,70,71,72].
In our study, the phenotypic antibiotic resistance pattern of the isolates was determined with seven beta-lactam and three aminoglycoside antibiotics through the disc diffusion method. Bacteria isolated from diarrheal samples showed varying degrees of phenotypic resistance to the various antibiotics studied. These isolates exhibited the highest level of resistance to aztreonam, cefuroxime, cefixime, and cefepime. However, the isolates were more susceptible to amoxicillin + clavulanic acid, two carbapenems, and the three aminoglycosides studied. The diarrheal isolates were most sensitive to meropenem. Similar types of sensitivity of diarrheal isolates to meropenem were found in a study in India [73]. However, much lower resistance to imipenem and meropenem antibiotics was observed among E. coli isolates in a hospital-based study in China [74]. The efficacy of all generations of cephalosporin antibiotics against UTI isolates was extremely low. Due to their widespread use in the treatment of UTI and other illnesses, these antibiotics may have higher levels of resistance [75]. Clinicians have begun to rely more on carbapenems as a result of the decreased potency of cephalosporins. From this study, we observed that meropenem was one of the most effective β-lactam antibiotics available, which needs to be preserved. These isolates also showed good susceptibility to gentamicin and amikacin antibiotics. An earlier study in Bangladesh found that 15% of gram-negative UTI isolates were resistant to imipenem [8]. This was five times less than the results of our investigation, illustrating an upward trend in carbapenem resistance in Bangladeshi UTI bacteria, which is a growing concern that needs to be urgently addressed. Over the previous ten years, other studies have also revealed a rising trend of carbapenem resistance [16]. Imipenem and meropenem antibiotics are some of the few effective antibiotics used to treat various infections. Consequently, the rapid increase in resistance against these antibiotics is a real concern, leading to their designation as ‘Watch’ antibiotics; consequently, they should be subject to ASPs to limit inappropriate prescribing and dispensing [3,14,76].
Our study collected two types of samples (diarrheal and UTI). For diarrheal samples, the average pathogen detection rate of bacteria was very high (95%). Viral carriage, though, was not investigated in this research. Different bacteria were isolated from the collected diarrheal samples, of which Escherichia coli was the predominant bacteria. Similarly, E. coli was the predominant bacteria in clinical samples in Nepal [77], and among diarrheal samples from India [73]. For UTI samples, the overall pathogen detection rate was 94.67%. The major etiologic agent found was Klebsiella spp., which accounted for up to one-third of the total UTI isolates. Escherichia coli was the second most prevalent bacteria found. This observation is quite unusual since, in most previous studies, E. coli was the major pathogen, and Klebsiella spp. was the second dominant pathogen [78,79]. We will be investigating this further.
We are aware of a number of limitations with this study. Risk behavior data from diarrheal and UTI patients was not culled in depth. In addition, we used a cross-sectional research approach without follow-up as we wanted to initially document the extent of resistant pathogens in these common conditions in ambulatory care in Bangladesh to help guide future activities, with ambulatory care accounting for up to 95% of human antibiotic use in LMICs [80]. The sample size was also relatively small, with only two MBL genes and a small number of β-lactam and aminoglycoside antibiotics assessed. However, internal validity was maintained in this study by replicating independent tests as required. Despite these limitations, we believe this study has elucidated significant diarrheal and UTI pathogens, their carriage of metallo-beta-lactamase genes, as well as co-resistance and the genotypic-phenotypic relationship to antibiotic resistance, providing future guidance to all key stakeholder groups in Bangladesh.
5. Conclusions
In conclusion, our study showed that meropenem is the most efficacious antibiotic for diarrheal and UTI pathogens among patients with these conditions in Bangladesh. The study also reported the emergence of MBL genes in Bangladeshi diarrheal and UTI pathogens. The combination of these genes exerted more resistance than they did separately. When only one MBL gene was present, absolute resistance to the carbapenem group of antibiotics was not conferred; however, in conjunction, they were resistant to all tested antibiotics, even to meropenem, except in one case. This emergence of resistance to these critical antibiotics is a concern. Consequently, it is crucial that activities are instigated now to stop the growth and dissemination of these isolates. This includes refining the curricula of all key healthcare professionals, including those managing pharmacies and drug stores in Bangladesh, to ensure adequate knowledge regarding the appropriate management of these common conditions on qualification in Bangladesh and the consequences of inappropriate antibiotic use in both mortality and costs with rising AMR. The recently published AWaRe book giving guidance on the appropriate management of these conditions is a good start.
We have seen in other countries that improved education of pharmacists and drug store personnel, including guidelines, can improve appropriate management, providing direction to key stakeholders in Bangladesh. Alongside this, educating patients to reduce requests for antibiotics to treat diarrhea in children and UTIs where this is not appropriate. The instigation of ASPs can help in this regard, alongside improved surveillance of resistance patterns. These activities are essential if the Government of Bangladesh is to meet the objectives of the NAP. We will be following up on this in future studies.
Author Contributions
Conceptualization: ASS, NI, MJH, SI; methodology: ASS, NI, MAA, MJH, SI; validation: all authors; formal analysis: ASS, NI, MAA, KA, MBH, SN, SI; investigation: ASS, NI, MAA, KA, MBH, SN, SI.; resources: SI, MJH; data curation: ASS, NI, BG, SI; writing—original draft: ASS, NI, BBG, SI.; writing—all authors; visualization ASS, NI, BBG, SI; supervision: SI.; project administration: SI. All authors have read and agreed to the published version of the manuscript.
Funding
This research received research funding from the Bangladesh Medical Research Council (BMRC) to Dr. Salequl Islam and partial research funding from ‘the Integrated Health Science Research and Development Fund 2021’, the government of Bangladesh, awarded to Dr. Shamsun Nahar.
Data Availability Statement
Additional data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Papp-Wallace, K.M.; Endimiani, A.; Taracila, M.A.; Bonomo, R.A. Carbapenems: past, present, and future. Antimicrobial agents and chemotherapy 2011, 55, 4943-4960.
- Sharland, M.; Zanichelli, V.; Ombajo, L.A.; Bazira, J.; Cappello, B.; Chitatanga, R.; Chuki, P.; Gandra, S.; Getahun, H.; Harbarth, S. The WHO essential medicines list AWaRe book: From a list to a quality improvement system. Clinical Microbiology and Infection 2022, 28, 1533-1535. [CrossRef]
- Sharland, M.; Gandra, S.; Huttner, B.; Moja, L.; Pulcini, C.; Zeng, M.; Mendelson, M.; Cappello, B.; Cooke, G.; Magrini, N. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use—the new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. The Lancet Infectious Diseases 2019, 19, 1278-1280. [CrossRef]
- Ahmed, I.; Rabbi, M.B.; Sultana, S. Antibiotic resistance in Bangladesh: A systematic review. International Journal of Infectious Diseases 2019, 80, 54-61. [CrossRef]
- Islam, S.; Urmi, U.L.; Rana, M.; Sultana, F.; Jahan, N.; Hossain, B.; Iqbal, S.; Hossain, M.M.; Mosaddek, A.S.M.; Nahar, S. High abundance of the colistin resistance gene mcr-1 in chicken gut-bacteria in Bangladesh. Scientific Reports 2020, 10, 17292. [CrossRef]
- Hoque, R.; Ahmed, S.M.; Naher, N.; Islam, M.A.; Rousham, E.K.; Islam, B.Z.; Hassan, S. Tackling antimicrobial resistance in Bangladesh: A scoping review of policy and practice in human, animal and environment sectors. PloS one 2020, 15, e0227947. [CrossRef]
- Monira, S.; Shabnam, S.A.; Ali, S.I.; Sadique, A.; Johura, F.-T.; Rahman, K.Z.; Alam, N.H.; Watanabe, H.; Alam, M. Multi-drug resistant pathogenic bacteria in the gut of young children in Bangladesh. Gut pathogens 2017, 9, 1-8. [CrossRef]
- Haque, T.A.; Urmi, U.L.; Islam, A.B.M.M.K.; Ara, B.; Nahar, S.; Mosaddek, A.S.M.; Lugova, H.; Kumar, S.; Jahan, D.; Rahman, N.A.A. Detection of qnr genes and gyrA mutation to quinolone phenotypic resistance of UTI pathogens in Bangladesh and the implications. Journal of Applied Pharmaceutical Science 2022, 12, 185-198. [CrossRef]
- Begum, N.; Shamsuzzaman, S. Emergence of carbapenemase-producing urinary isolates at a tertiary care hospital in Dhaka, Bangladesh. Tzu Chi Medical Journal 2016, 28, 94-98. [CrossRef]
- Islam, M.A.; Akhtar, Z.; Hassan, M.Z.; Chowdhury, S.; Rashid, M.M.; Aleem, M.A.; Ghosh, P.K.; Mah-E-Muneer, S.; Parveen, S.; Ahmmed, M.K. Pattern of antibiotic dispensing at pharmacies according to the WHO Access, Watch, Reserve (AWaRe) classification in Bangladesh. Antibiotics 2022, 11, 247. [CrossRef]
- Orubu, E.; Samad, M.; Rahman, M.; Zaman, M.; Wirtz, V. Mapping the antimicrobial supply chain in Bangladesh: a scoping-review-based ecological assessment approach. Global Health: Science and Practice 2021, 9, 532-547. [CrossRef]
- Nizame, F.A.; Shoaib, D.M.; Rousham, E.K.; Akter, S.; Islam, M.A.; Khan, A.A.; Rahman, M.; Unicomb, L. Barriers and facilitators to adherence to national drug policies on antibiotic prescribing and dispensing in Bangladesh. Journal of Pharmaceutical Policy and Practice 2021, 14, 1-13. [CrossRef]
- Kabir, H.; Hasan, M.K.; Akter, N.; Tassdik, H.; Islam, M.F.; Jannat, H.; Tutul, A.H.; Akter, O.; Ara, R.; Islam, M.D. Antibiotics administration without prescription in Bangladesh. IJID regions 2023, 7, 11-17. [CrossRef]
- Sulis, G.; Sayood, S.; Katukoori, S.; Bollam, N.; George, I.; Yaeger, L.H.; Chavez, M.A.; Tetteh, E.; Yarrabelli, S.; Pulcini, C. Exposure to World Health Organization's AWaRe antibiotics and isolation of multidrug resistant bacteria: a systematic review and meta-analysis. Clinical Microbiology and Infection 2022, 28, 1193-1202.
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-producing organisms: a global scourge. Clinical infectious diseases 2018, 66, 1290-1297. [CrossRef]
- Nordmann, P.; Naas, T.; Poirel, L. Global spread of Carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis 2011, 17, 1791-1798, doi:10.3201/eid1710.110655. [CrossRef]
- van Duin, D.; Doi, Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence 2017, 8, 460-469.
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J Infect Dis 2017, 215, S28-S36, doi:10.1093/infdis/jiw282. [CrossRef]
- Wilson, H.; Török, M.E. Extended-spectrum β-lactamase-producing and carbapenemase-producing Enterobacteriaceae. Microbial genomics 2018, 4. [CrossRef]
- Van Duin, D.; Arias, C.A.; Komarow, L.; Chen, L.; Hanson, B.M.; Weston, G.; Cober, E.; Garner, O.B.; Jacob, J.T.; Satlin, M.J. Molecular and clinical epidemiology of carbapenem-resistant Enterobacterales in the USA (CRACKLE-2): a prospective cohort study. The Lancet Infectious Diseases 2020, 20, 731-741. [CrossRef]
- Goodman, K.; Simner, P.; Tamma, P.; Milstone, A. Infection control implications of heterogeneous resistance mechanisms in carbapenem-resistant Enterobacteriaceae (CRE). Expert review of anti-infective therapy 2016, 14, 95-108. [CrossRef]
- Livingstone, D.; Gill, M.; Wise, R. Mechanisms of resistance to the carbapenems. Journal of Antimicrobial Chemotherapy 1995, 35, 1-5.
- Tamma, P.D.; Goodman, K.E.; Harris, A.D.; Tekle, T.; Roberts, A.; Taiwo, A.; Simner, P.J. Comparing the outcomes of patients with carbapenemase-producing and non-carbapenemase-producing carbapenem-resistant Enterobacteriaceae bacteremia. Clinical Infectious Diseases 2017, 64, 257-264. [CrossRef]
- Codjoe, F.S.; Donkor, E.S. Carbapenem resistance: a review. Medical Sciences 2017, 6, 1. [CrossRef]
- Macesic, N.; Hawkey, J.; Vezina, B.; Wisniewski, J.A.; Cottingham, H.; Blakeway, L.V.; Harshegyi, T.; Pragastis, K.; Badoordeen, G.Z.; Dennison, A. Genomic dissection of endemic carbapenem resistance reveals metallo-beta-lactamase dissemination through clonal, plasmid and integron transfer. Nature Communications 2023, 14, 4764. [CrossRef]
- Wiegand, I.; Hilpert, K.; Hancock, R.E. Agar and broth dilution methods to determine the minimal inhibitory concentration (MIC) of antimicrobial substances. Nat Protoc 2008, 3, 163-175. [CrossRef]
- Walsh, T.R.; Toleman, M.A.; Poirel, L.; Nordmann, P. Metallo-β-lactamases: the quiet before the storm? Clinical microbiology reviews 2005, 18, 306-325.
- Reddy, K.S. Global Burden of Disease Study 2015 provides GPS for global health 2030. The Lancet 2016, 388, 1448-1449. [CrossRef]
- Mokomane, M.; Kasvosve, I.; Melo, E.d.; Pernica, J.M.; Goldfarb, D.M. The global problem of childhood diarrhoeal diseases: emerging strategies in prevention and management. Therapeutic advances in infectious disease 2018, 5, 29-43. [CrossRef]
- WHO. Diarrhoeal disease: WHO. 2017.
- Troeger, C.E.; Khalil, I.A.; Blacker, B.F.; Biehl, M.H.; Albertson, S.B.; Zimsen, S.R.; Rao, P.C.; Abate, D.; Ahmadi, A.; brahim Ahmed, M.L.C. Quantifying risks and interventions that have affected the burden of diarrhoea among children younger than 5 years: an analysis of the Global Burden of Disease Study 2017. The Lancet Infectious Diseases 2020, 20, 37-59. [CrossRef]
- Wang, W.; Zhao, L.; Hu, Y.; Dottorini, T.; Fanning, S.; Xu, J.; Li, F. Epidemiological study on prevalence, serovar diversity, multidrug resistance, and CTX-M-type extended-spectrum β-lactamases of Salmonella spp. from patients with diarrhea, food of animal origin, and pets in several provinces of China. Antimicrobial agents and chemotherapy 2020, 64. [CrossRef]
- Zheng, B.; Xu, H.; Lv, T.; Guo, L.; Xiao, Y.; Huang, C.; Zhang, S.; Chen, Y.; Han, H.; Shen, P. Stool samples of acute diarrhea inpatients as a reservoir of ST11 hypervirulent KPC-2-producing Klebsiella pneumoniae. MSystems 2020, 5, 10.1128/msystems. 00498-00420. [CrossRef]
- Ba, X.; Guo, Y.; Moran, R.A.; Doughty, E.L.; Liu, B.; Yao, L.; Li, J.; He, N.; Shen, S.; Li, Y. Global emergence of a hypervirulent carbapenem-resistant Escherichia coli ST410 clone. Nature Communications 2024, 15, 494. [CrossRef]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet 2022, 399, 629-655. [CrossRef]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. The Lancet infectious diseases 2019, 19, 56-66. [CrossRef]
- Dadgostar, P. Antimicrobial resistance: implications and costs. Infection and drug resistance 2019, 3903-3910. [CrossRef]
- Hofer, U. The cost of antimicrobial resistance. Nature Reviews Microbiology 2019, 17, 3-3. [CrossRef]
- Medina, M.; Castillo-Pino, E. An introduction to the epidemiology and burden of urinary tract infections. Therapeutic advances in urology 2019, 11, 1756287219832172. [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nature reviews microbiology 2015, 13, 269-284. [CrossRef]
- Foxman, B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. The American journal of medicine 2002, 113, 5-13. [CrossRef]
- Eshetie, S.; Unakal, C.; Gelaw, A.; Ayelign, B.; Endris, M.; Moges, F. Multidrug resistant and carbapenemase producing Enterobacteriaceae among patients with urinary tract infection at referral Hospital, Northwest Ethiopia. Antimicrobial resistance and infection control 2015, 4, 1-8. [CrossRef]
- Dasgupta, C.; Rafi, M.A.; Salam, M.A. High prevalence of multidrug resistant uropathogens: A recent audit of antimicrobial susceptibility testing from a tertiary care hospital in Bangladesh. Pakistan journal of medical sciences 2020, 36, 1297.
- Urmi, U.L.; Nahar, S.; Rana, M.; Sultana, F.; Jahan, N.; Hossain, B.; Alam, M.S.; Mosaddek, A.S.M.; McKimm, J.; Rahman, N.A.A. Genotypic to Phenotypic Resistance Discrepancies Identified Involving β-Lactamase Genes, bla KPC, bla IMP, bla NDM-1, and bla VIM in Uropathogenic Klebsiella pneumoniae. Infection and drug resistance 2020, 2863-2875.
- Tompkins, K.; van Duin, D. Treatment for carbapenem-resistant Enterobacterales infections: recent advances and future directions. European Journal of Clinical Microbiology & Infectious Diseases 2021, 40, 2053-2068.
- Clancy, C.J.; Potoski, B.A.; Buehrle, D.; Nguyen, M.H. Estimating the treatment of carbapenem-resistant Enterobacteriaceae infections in the United States using antibiotic prescription data. In Proceedings of the Open forum infectious diseases, 2019; p. ofz344. [CrossRef]
- Hansen, G.T. Continuous evolution: perspective on the epidemiology of carbapenemase resistance among Enterobacterales and other Gram-negative bacteria. Infectious diseases and therapy 2021, 10, 75-92. [CrossRef]
- Löfmark, S.; Sjöström, K.; Mäkitalo, B.; Edquist, P.; Wisell, K.T.; Giske, C.G. Carbapenemase-producing Enterobacteriaceae in Sweden 2007–2013: experiences from seven years of systematic surveillance and mandatory reporting. Drug Resistance Updates 2015, 20, 29-38. [CrossRef]
- Miriagou, V.; Cornaglia, G.; Edelstein, M.; Galani, I.; Giske, C.; Gniadkowski, M.; Malamou-Lada, E.; Martinez-Martinez, L.; Navarro, F.; Nordmann, P. Acquired carbapenemases in Gram-negative bacterial pathogens: detection and surveillance issues. Clinical microbiology and infection 2010, 16, 112-122. [CrossRef]
- WHO. Antimicrobial stewardship programs in health-care facilities in low-and middle-income countries: a WHO practical toolkit. 2019.
- Pierce, J.; Apisarnthanarak, A.; Schellack, N.; Cornistein, W.; Al Maani, A.; Adnan, S.; Stevens, M.P. Global Antimicrobial Stewardship with a Focus on Low-and Middle-Income Countries: A position statement for the international society for infectious diseases. International Journal of Infectious Diseases 2020, 96, 621-629. [CrossRef]
- Nathwani, D.; Varghese, D.; Stephens, J.; Ansari, W.; Martin, S.; Charbonneau, C. Value of hospital antimicrobial stewardship programs [ASPs]: a systematic review. Antimicrobial Resistance & Infection Control 2019, 8, 1-13. [CrossRef]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; Gould, I.; Hara, G.L. Antibiotic stewardship in low-and middle-income countries: the same but different? Clinical microbiology and infection 2017, 23, 812-818.
- Harun, M.G.D.; Anwar, M.M.U.; Sumon, S.A.; Hassan, M.Z.; Mohona, T.M.; Rahman, A.; Abdullah, S.A.H.M.; Islam, M.S.; Kaydos-Daniels, S.C.; Styczynski, A.R. Rationale and guidance for strengthening infection prevention and control measures and antimicrobial stewardship programs in Bangladesh: A study protocol. BMC health services research 2022, 22, 1-11. [CrossRef]
- Akpan, M.R.; Isemin, N.U.; Udoh, A.E.; Ashiru-Oredope, D. Implementation of antimicrobial stewardship programmes in African countries: a systematic literature review. Journal of global antimicrobial resistance 2020, 22, 317-324. [CrossRef]
- Otieno, P.A.; Campbell, S.; Maley, S.; Obinju Arunga, T.; Otieno Okumu, M. A Systematic Review of Pharmacist-Led Antimicrobial Stewardship Programs in Sub-Saharan Africa. International Journal of Clinical Practice 2022, 2022. [CrossRef]
- Sumon, S.; Anwar, M.; Akther, F.; Priyanka, A.; Tamanna, T.; Rahman, A.; Islam, M.; Harun, M.D. Perceptions of antibiotic stewardship programmes and determinants of antibiotic prescribing patterns among physicians in tertiary hospitals in Bangladesh: implications for future policy and practice. Journal of Hospital Infection 2024, 144, 56-65. [CrossRef]
- Haque, M.; Godman, B. Potential strategies to improve antimicrobial utilisation in hospitals in Bangladesh building on experiences across developing countries. Bangladesh Journal of Medical Science 2021, 20, 469-477. [CrossRef]
- M. Kurdi Al-Dulaimi, M.; Abd. Mutalib, S.; Abd. Ghani, M.; Mohd. Zaini, N.A.; Ariffin, A.A. Multiple antibiotic resistance (MAR), plasmid profiles, and DNA polymorphisms among Vibrio vulnificus isolates. Antibiotics 2019, 8, 68.
- Bulik, C.C.; Fauntleroy, K.A.; Jenkins, S.G.; Abuali, M.; LaBombardi, V.J.; Nicolau, D.P.; Kuti, J.L. Comparison of meropenem MICs and susceptibilities for carbapenemase-producing Klebsiella pneumoniae isolates by various testing methods. Journal of clinical microbiology 2010, 48, 2402-2406. [CrossRef]
- Humphries, R.M.; Hindler, J.A.; Epson, E.; Horwich-Scholefield, S.; Miller, L.G.; Mendez, J.; Martinez, J.B.; Sinkowitz, J.; Sinkowtiz, D.; Hershey, C. Carbapenem-resistant Enterobacteriaceae detection practices in California: what are we missing? Clinical Infectious Diseases 2018, 66, 1061-1067.
- Barbosa, C.; Nogueira, S.; Gadanho, M.; Chaves, S. DNA extraction: finding the most suitable method. In Molecular microbial diagnostic methods; Elsevier: 2016; pp. 135-154.
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagnostic microbiology and infectious disease 2011, 70, 119-123. [CrossRef]
- Gupta, V.; Datta, P.; Chander, J. Prevalence of metallo-β lactamase (MBL) producing Pseudomonas spp. and Acinetobacter spp. in a tertiary care hospital in India. Journal of Infection 2006, 52, 311-314.
- Mirbagheri, S.Z.; Meshkat, Z.; Naderinasab, M.; Rostami, S.; Nabavinia, M.S.; Rahmati, M. Study on imipenem resistance and prevalence of blaVIM1 and blaVIM2 metallo-beta lactamases among clinical isolates of Pseudomonas aeruginosa from Mashhad, Northeast of Iran. Iranian Journal of Microbiology 2015, 7, 72.
- Ministry of Health and Family Welfare (MoHFW), G.o.B. National Action Plan: Antimicrobial Resistance Containment in Bangladesh 2017-22.; 2017.
- Mishra, S.; Acharya, J.; Kattel, H.; Koirala, J.; Rijal, B.; Pokhrel, B. Metallo-beta-lactamase producing gram-negative bacterial isolates. 2012.
- Emeraud, C.; Escaut, L.; Boucly, A.; Fortineau, N.; Bonnin, R.A.; Naas, T.; Dortet, L. Aztreonam plus Clavulanate, Tazobactam, or Avibactam for Treatment of Infections Caused by Metallo-beta-Lactamase-Producing Gram-Negative Bacteria. Antimicrob Agents Chemother 2019, 63, doi:10.1128/AAC.00010-19. [CrossRef]
- Canton, R.; Ruiz-Garbajosa, P. Co-resistance: an opportunity for the bacteria and resistance genes. Curr Opin Pharmacol 2011, 11, 477-485, doi:10.1016/j.coph.2011.07.007. [CrossRef]
- Rice, L.B. Antimicrobial stewardship and antimicrobial resistance. Medical Clinics 2018, 102, 805-818. [CrossRef]
- de Carvalho, F.R.T.; Telles, J.P.; Tuon, F.F.B.; Rabello Filho, R.; Caruso, P.; Correa, T.D. Antimicrobial stewardship programs: A review of strategies to avoid polymyxins and carbapenems misuse in low middle-income countries. Antibiotics 2022, 11, 378. [CrossRef]
- Sono, T.M.; Yeika, E.; Cook, A.; Kalungia, A.; Opanga, S.A.; Acolatse, J.E.E.; Sefah, I.A.; Jelić, A.G.; Campbell, S.; Lorenzetti, G. Current rates of purchasing of antibiotics without a prescription across sub-Saharan Africa; rationale and potential programmes to reduce inappropriate dispensing and resistance. Expert review of anti-infective therapy 2023, 21, 1025-1055. [CrossRef]
- Al Jarousha, A.M.K.; El Jarou, M.A.; El Qouqa, I.A. Bacterial enteropathogens and risk factors associated with childhood diarrhea. The Indian Journal of Pediatrics 2011, 78, 165-170. [CrossRef]
- Zhou, Y.; Zhu, X.; Hou, H.; Lu, Y.; Yu, J.; Mao, L.; Mao, L.; Sun, Z. Characteristics of diarrheagenic Escherichia coli among children under 5 years of age with acute diarrhea: a hospital based study. BMC infectious diseases 2018, 18, 1-10. [CrossRef]
- Meyer, E.; Schwab, F.; Schroeren-Boersch, B.; Gastmeier, P. Dramatic increase of third-generation cephalosporin-resistant E. coli in German intensive care units: secular trends in antibiotic drug use and bacterial resistance, 2001 to 2008. Critical care 2010, 14, 1-9. [CrossRef]
- Zanichelli, V.; Sharland, M.; Cappello, B.; Moja, L.; Getahun, H.; Pessoa-Silva, C.; Sati, H.; van Weezenbeek, C.; Balkhy, H.; Simão, M. The WHO AWaRe (Access, Watch, Reserve) antibiotic book and prevention of antimicrobial resistance. 2023. [CrossRef]
- Ansari, M.; Aryal, S.C.; Rai, G.; Rai, K.R.; Pyakurel, S.; Bhandari, B.; Sah, A.K.; Rai, S.K. Prevalence of multidrug-resistance and bla VIM and bla IMP genes among gram-negative clinical isolates in tertiary care hospital, Kathmandu, Nepal. Iranian journal of microbiology 2021, 13, 303.
- Chander, A.; Shrestha, C.D. Prevalence of extended spectrum beta lactamase producing Escherichia coli and Klebsiella pneumoniae urinary isolates in a tertiary care hospital in Kathmandu, Nepal. BMC Research notes 2013, 6, 1-6. [CrossRef]
- Ronald, A. The etiology of urinary tract infection: traditional and emerging pathogens. The American journal of medicine 2002, 113, 14-19. [CrossRef]
- Duffy, E.; Ritchie, S.; Metcalfe, S.; Van Bakel, B.; Thomas, M. Antibacterials dispensed in the community comprise 85%-95% of total human antibacterial consumption. Journal of clinical pharmacy and therapeutics 2018, 43, 59-64. [CrossRef]
Figure 1.
Phenotypic antibiotic resistance in isolates from diarrheal and UTI. A). Antibiotic susceptibility was evaluated largely by standard disk-diffusion methods for both diarrheal and UTI pathogens. P-values were calculated using chi-square statistics of phenotypic antibiotic resistance shown between two different groups of clinical pathogens. B). Differential meropenem MIC of diarrheal and UTI isolates were shown.
Figure 1.
Phenotypic antibiotic resistance in isolates from diarrheal and UTI. A). Antibiotic susceptibility was evaluated largely by standard disk-diffusion methods for both diarrheal and UTI pathogens. P-values were calculated using chi-square statistics of phenotypic antibiotic resistance shown between two different groups of clinical pathogens. B). Differential meropenem MIC of diarrheal and UTI isolates were shown.
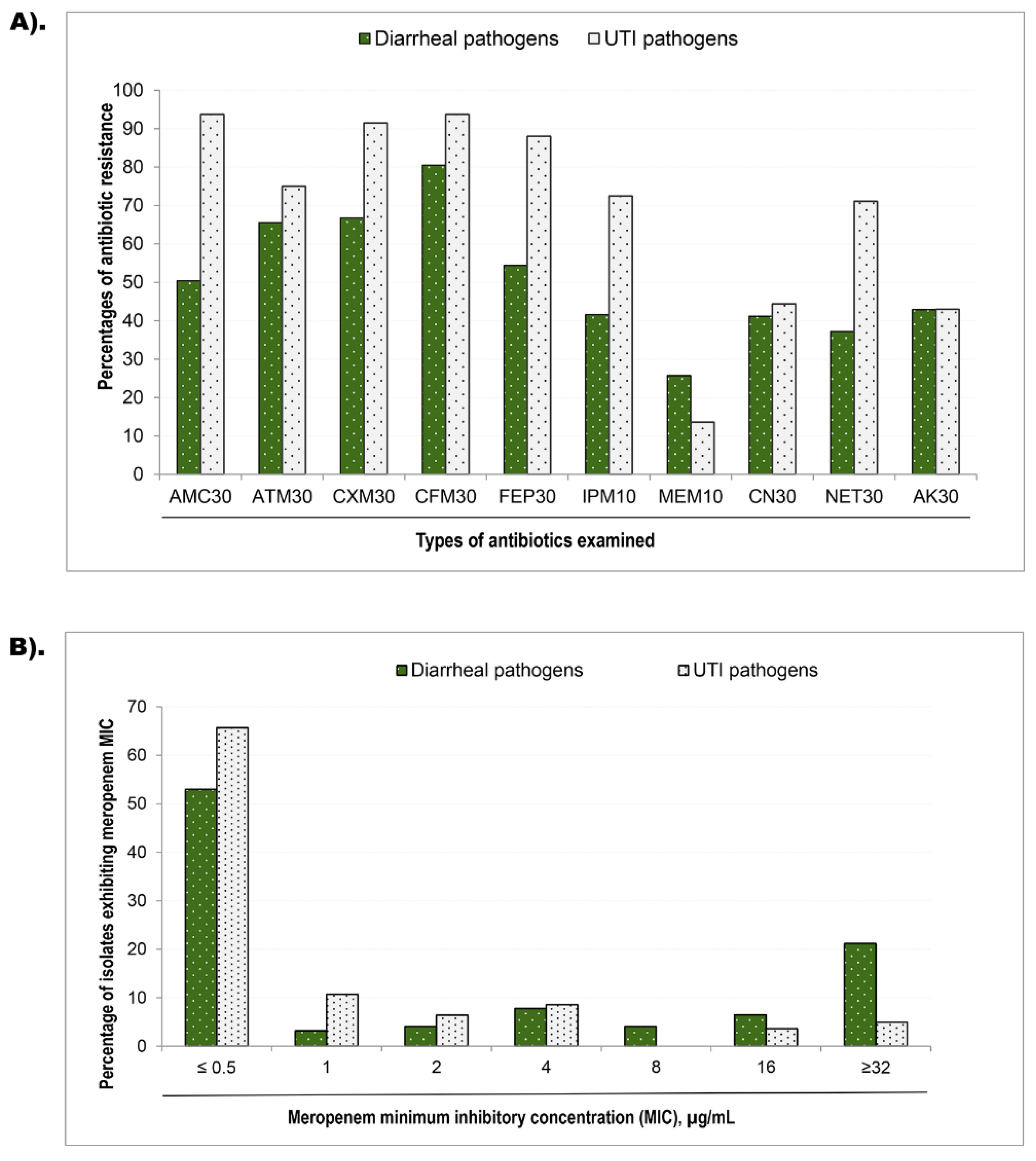
Figure 2.
Impact of two metallo-β-lactamase genes (MBL) to the phenotypic susceptibilities of β-lactam, carbapenem, and aminoglycoside antibiotics. The susceptibilities of the MBL-positive and -negative isolates were assessed against ten antibiotics, namely Amoxycillin-clavulanic acid (AMC 30 µg), Aztreonam (ATM 30 µg), Cefuroxime Sodium (CXM 30 µg), Cefixime (CFM 30 µg), Cefepime (FEP 30 µg), Imipenem (IMP 10 µg), Meropenem (MEM 10 µg), Gentamicin (CN 30 µg), Netilmicin (NET 30 µg), and Amikacin (AK 30 µg) . A). The Y-axis values of black-spotted bars indicate the percentage of blaNDM-1 gene-carrying diarrheal pathogen showing as resistance against respective antibiotics shown on the X-axis. Similarly, the white bars illustrate the percentages of resistance isolates that do not carry the bla-NDM-1 gene. Resistance of B) blaVIM-positive (n=12) and -negative (n=226) diarrheal pathogens, C) blaNDM-1-positive (n=13) and -negative (n=129) UTI pathogens, and D) blaVIM-positive (n=23) and -negative (n=119) UTI isolates are presented separately.
Figure 2.
Impact of two metallo-β-lactamase genes (MBL) to the phenotypic susceptibilities of β-lactam, carbapenem, and aminoglycoside antibiotics. The susceptibilities of the MBL-positive and -negative isolates were assessed against ten antibiotics, namely Amoxycillin-clavulanic acid (AMC 30 µg), Aztreonam (ATM 30 µg), Cefuroxime Sodium (CXM 30 µg), Cefixime (CFM 30 µg), Cefepime (FEP 30 µg), Imipenem (IMP 10 µg), Meropenem (MEM 10 µg), Gentamicin (CN 30 µg), Netilmicin (NET 30 µg), and Amikacin (AK 30 µg) . A). The Y-axis values of black-spotted bars indicate the percentage of blaNDM-1 gene-carrying diarrheal pathogen showing as resistance against respective antibiotics shown on the X-axis. Similarly, the white bars illustrate the percentages of resistance isolates that do not carry the bla-NDM-1 gene. Resistance of B) blaVIM-positive (n=12) and -negative (n=226) diarrheal pathogens, C) blaNDM-1-positive (n=13) and -negative (n=129) UTI pathogens, and D) blaVIM-positive (n=23) and -negative (n=119) UTI isolates are presented separately.
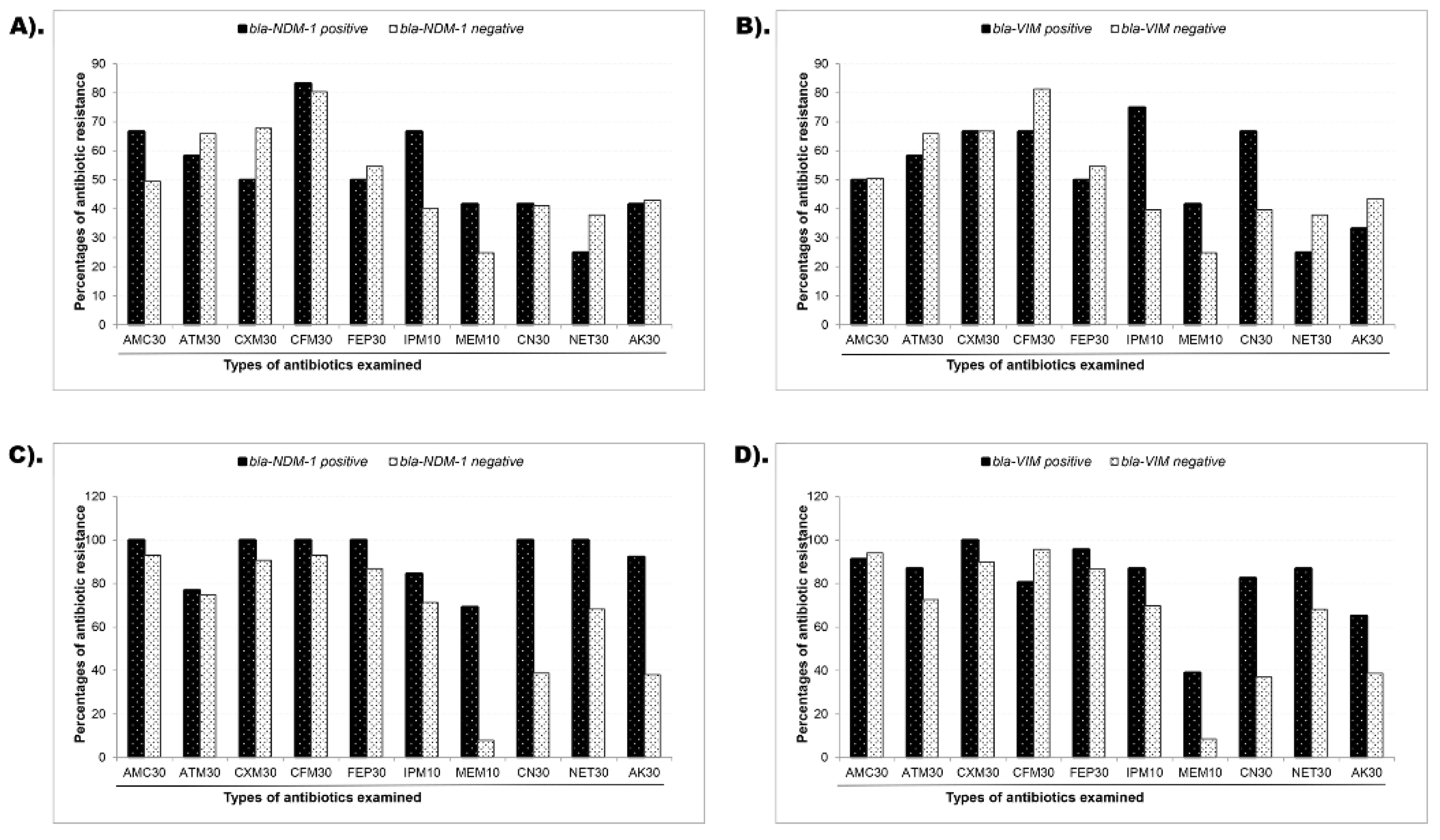
Figure 3.
Multiple antibiotic resistance (MAR) index of single carrying and co-carrying metallo-β-lactamase (MBL) genes. The multiple antibiotic resistance (MAR) index was calculated by dividing the number of antibiotics an isolate was resistant by the total number of antibiotics tested. The dot plot shows the MAR index values of the pathogens that carried a single MBL gene exclusively (either blaNDM-1 or blaVIM) and concurrently (both blaNDM-1 and blaVIM together) in the diarrheal pathogens and uropathogens. The MAR index values were placed on the Y-axis, and the group of MBL-gene carriage was placed on the X-axis. Each dot represents the MAR index value of one bacterial pathogen.
Figure 3.
Multiple antibiotic resistance (MAR) index of single carrying and co-carrying metallo-β-lactamase (MBL) genes. The multiple antibiotic resistance (MAR) index was calculated by dividing the number of antibiotics an isolate was resistant by the total number of antibiotics tested. The dot plot shows the MAR index values of the pathogens that carried a single MBL gene exclusively (either blaNDM-1 or blaVIM) and concurrently (both blaNDM-1 and blaVIM together) in the diarrheal pathogens and uropathogens. The MAR index values were placed on the Y-axis, and the group of MBL-gene carriage was placed on the X-axis. Each dot represents the MAR index value of one bacterial pathogen.
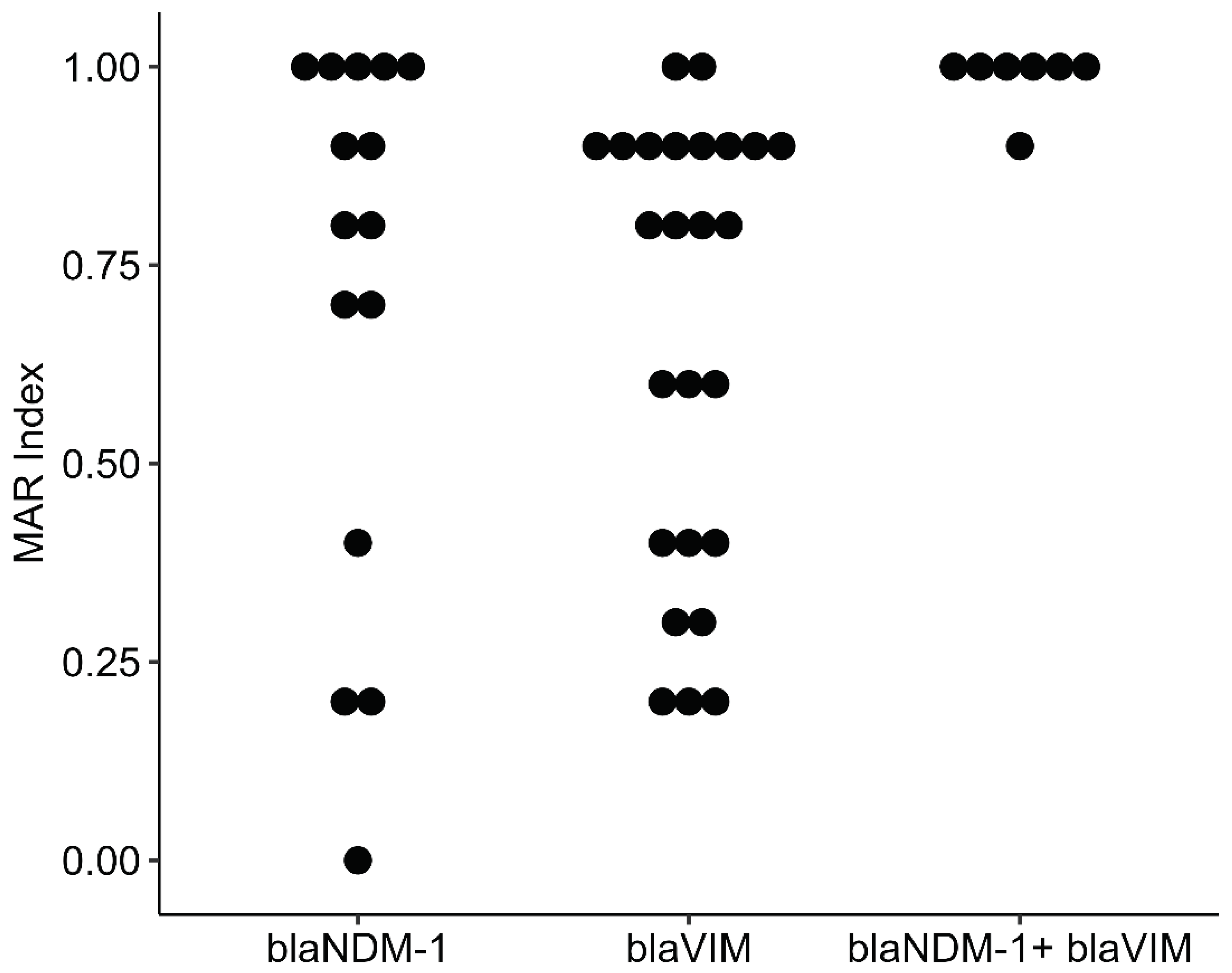

Table 1.
Isolation of diarrheal and urinary tract infection pathogens by age of study participants.
| Age group (Years) | Diarrheal pathogens (n=228) |
Urinary tract infection pathogens (n=142) | |||
|---|---|---|---|---|---|
| Frequency | Percentage | Frequency | Percentage | ||
| 1-10 | 191 a | 83.8 | 5 | 3.5 | |
| 11-20 | 5 | 2.2 | 22 | 15.5 | |
| 21-30 | 8 | 3.5 | 50 b | 35.2 | |
| 31-40 | 10 | 4.4 | 19 b | 13.4 | |
| 41-50 | 0 | 0 | 27 b | 19.0 | |
| 51-60 | 5 | 2.2 | 8 | 5.6 | |
| 61-70 | 0 | 0 | 9 | 6.3 | |
| 71-80 | 9 | 3.9 | 2 | 1.4 | |
| Total | 228 | 100 | 142 | 100 | |
a , One hundred ninety one (83.9%) of 228 diarrheal bacteria were isolated from aged <10 years. b , Over 60% (86/142) of the UTI isolates were grown from 21-50 years age range.
Table 2.
Association of the minimum inhibitory concentration of meropenem with the presence of blaNDM-1 and blaVIM in diarrheal bacteria and uropathognes. .
Table 2.
Association of the minimum inhibitory concentration of meropenem with the presence of blaNDM-1 and blaVIM in diarrheal bacteria and uropathognes. .
| MIC values (µg/mL) | Diarrheal pathogens | Urinary tract infection pathogen | |||||||
|---|---|---|---|---|---|---|---|---|---|
| bla-NDM-1 carriage a | bla-VIM carriage b | bla-NDM-1 carriage c | bla-VIM carriage d | ||||||
| Yes (n=12) ∆ | No (n=216) | Yes (n=12) | No (n=216) | Yes (n=13) | No (n=129) | Yes (n=23) | No (n=119) | ||
| ≤0.5 | 6 (50) | 109 (55) | 7 (58) | 108 (55) | 2 (15) | 90 (71) | 12 (52) | 80 (68) | |
| 1.0 | 1 (8) | 7 (3.5) | 1 (8) | 7 (3.6) | 1 (7.7) | 14 (11) | 1 (4.3) | 14 (12) | |
| 2.0 | 0 (0) | 9 (4.5) | 0 (0) | 9 (4.6) | 0 (0) | 9 (7.1) | 0 (0) | 9 (7.7) | |
| 4.0 | 0 (0) | 17 (8.6) | 1 8) | 16 (8.1) | 6 (46) | 6 (4.7) | 7 (30) | 5 (4.3) | |
| 8.0 | 1 (8) | 14 (7.1) | 0 (0) | 14 (7.1) | 1 (7.7) | 4 (3.1) | 0 (0) | 5 (4.3) | |
| 16 | 1 (8) | 1 (0.5_ | 0 (0) | 2 (1) | 0 (0) | 2 (1.6) | 0 (0) | 2 (1.7) | |
| ≥32 | 3 (25) | 41 (21) | 3 (25) | 41 (21) | 3 (23) | 2 (1.6) | 3 (13) | 2 (1.7) | |
∆, number (percentage); a, Fisher exact test identified no statistical significant differences (p=0.9); b, No statistically significant difference exists (p=0.3); c, UTI isolates carrying blaNDM-1 exhibited statistically significant higher MIC values for meropenem (p<0.001); d, blaVIM-positive UTI isolates were statistically higher resistant to meropenem (p<0.001).
Table 3.
Phenotypes resistance associated with blaNDM-1, blaVIM, and co-occurrence of the both genes.
Table 3.
Phenotypes resistance associated with blaNDM-1, blaVIM, and co-occurrence of the both genes.
| MBL genes a | Isolate ID | Phenotypic susceptibility assessment b | MAR index c | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AMC 30 | CXM 30 | CFM 30 | FEP 30 | IMP 10 | MRP 10 | CN 30 | NET 30 | AK 30 | |||
|
blaNDM-1 |
PBD20 | R | R | R | R | R | R | S | S | R | 0.8 |
| PBD24 | R | S | S | S | S | S | S | S | R | 0.2 | |
| PBD78 | R | S | R | S | S | S | S | S | S | 0.2 | |
| PBD78C1 | R | R | R | R | R | R | S | S | S | 0.7 | |
| PBD78C2 | R | R | R | R | R | R | S | S | S | 0.7 | |
| PBD86 | S | S | S | S | S | S | S | S | S | 0 | |
| PBD86C1 | R | R | R | R | R | R | R | R | R | 1 | |
| PBD86C2 | R | R | R | R | R | R | R | R | R | 1 | |
| PBD103 | S | R | R | S | S | S | R | S | R | 0.4 | |
| UJ8 | R | R | R | R | R | S | R | R | S | 0.8 | |
| UJ18C2 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ29 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ49 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ56C1 | R | R | R | R | S | R | R | R | R | 0.9 | |
| UJ73 | R | R | R | R | R | S | R | R | R | 0.9 | |
|
blaVIM |
PBD5 | R | S | R | R | R | R | S | S | S | 0.6 |
| PBD8 | R | R | R | S | R | S | S | S | S | 0.4 | |
| PBD40 | S | R | R | S | R | S | S | S | S | 0.3 | |
| PBD53C2 | R | R | S | S | R | S | S | S | R | 0.4 | |
| PBD55 | S | S | S | S | S | R | R | S | S | 0.2 | |
| PBD77 | S | S | S | S | S | S | R | R | S | 0.2 | |
| PBD80C2 | S | R | R | R | S | S | R | S | S | 0.4 | |
| PBD81 | R | R | R | S | S | S | S | S | S | 0.3 | |
| PBD87 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ15 | R | R | R | R | R | R | R | R | S | 0.9 | |
| UJ19 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ39 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ57 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ59 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ62 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ75 | R | R | R | R | R | S | R | R | S | 0.8 | |
| UJ76C1 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ77 | R | R | R | R | R | S | R | R | S | 0.8 | |
| UJ78C2 | R | R | R | R | R | S | R | R | S | 0.8 | |
| UJ98 | R | R | R | R | S | R | S | S | S | 0.6 | |
| UJ108C1 | S | R | S | S | R | S | S | S | S | 0.2 | |
| UJ112 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ116 | R | R | R | R | S | S | R | R | R | 0.8 | |
| UJ120 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ123 | R | R | R | R | R | S | S | S | S | 0.6 | |
| blaNDM-1+ blaVIM | UJ48 | R | R | R | R | R | R | R | R | R | 1 |
| UJ79C1 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ79C2 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ87C1 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ87C2 | R | R | R | R | R | S | R | R | R | 0.9 | |
| UJ88 | R | R | R | R | R | R | R | R | R | 1 | |
| UJ90 | R | R | R | R | R | R | R | R | R | 1 | |
a, Metallo-β-Lactamase (MBL) genes; ID, Identity; AMC 30, Amoxicillin 30 µg; CXM 30, Cefuroxime 30 µg; CFM 30, Cefixime 30 µg; FEP 30, Cefepime 30 µg ; IMP 10, Imipenem 10 µg; MRP 10 , Meropenem 30 µg; CN 30, Gentamicin 30 µg ; NET 30 , Netilmicin 30 µg ; Ak 30, Amikacin 30 µg; R, Resistant; S, Sensitive; blaNDM-1 , New Delhi metallo beta lactamase-1; blaVIM , verone integron-encoded metallo-beta-lactamase; b, Phenotypic susceptibility assessment determines the effectiveness of various antibiotics and evaluates how microorganism responds against those antibiotics; c, The multiple antibiotic resistance (MAR) index was calculated and interpreted using the formula: x/y, where ‘x’ represents the number of antibiotics to which an isolate was resistant, and ‘y’ represents the total number of antibiotics tested.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



