Submitted:
14 February 2024
Posted:
23 February 2024
You are already at the latest version
Abstract
Hashimoto's thyroiditis (HT) is essentially featured by self-tissue destruction by means of the adaptive immune responses that evade immune regulation. Vitamin D carries out an immunomodulatory role that appears to promote immune tolerance. The aim of this study is to elaborate a narrative review about the relationship between vitamin D status and HT and the role of vitamin D supplementation to reduce HT risk by modulating the immune system. There is an extensive literature confirming that vitamin D levels are significantly lower in HT patients compared to healthy people. On the other hand, after the supplementation with cholecalciferol in patients with HT and vitamin D deficiency, thyroid autoantibody titer decreased significantly, However, there are no conclusive results on the effect of vitamin D supplementation on the thyroid function. The confirmation of the beneficial effects of vitamin D in the prevention and treatment of autoimmune thyroid diseases require additional randomized, double-blind, placebo-controlled trials with longer follow-up.
Keywords:
Anti-thyroglobulin antibodies
; Anti-thyroid peroxidase
; Autoimmunity
; Autoimmune thyroiditis
; Hashimoto thyroiditis
; Immune cells
; Vitamin D
; Vitamin D deficiency
; Vitamin D supplementation
1. Introduction
Hashimoto's thyroiditis (HT), also known as chronic autoimmune thyroiditis, is the most prevalent organ-specific autoimmune disorder whose frequency has increased considerably in the last decades. Currently, HT is one of the most common thyroid diseases and its incidence is 0.3–1.5 cases per 1000 people, especially in the female gender. HT is currently the leading cause of primary hypothyroidism, both in adolescents and adults. The main feature of the disease is the presence of thyroid autoantibodies against thyroid peroxidase (TPOAb) or thyroglobulin (TGAb). Antibody titers show a positive correlation with hypothyroidism. This condition is T-cell-mediated autoimmune disorders characterized by thyroid lymphocytic infiltration. Although the exact etiology has not been fully elucidated, pathogenesis of HT is related to an interaction among genetic influences, environmental triggers and epigenetic effects (1, 2).
The classic function of active vitamin D (calcitriol or 1,25-hydroxyvitamin D) is the regulation of calcium and phosphate concentrations, but recent evidence has suggested that vitamin D is also associated with non-skeletal roles (3, 4). Most body cells and organs (muscle, heart, blood vessels, pancreas, brain, mammary gland, colon, prostate, gonads, skin, immune cells, malignant cells etc.) have nuclear vitamin D receptors (VDR) and activating enzymes for calcitriol synthesis that, in these locations, is not regulated by parathyroid hormone. Vitamin D performs most of its biological actions by binding to the VDR and, consequently, modulates the expression/transcription of numerous coding genes responsible for the regulation of cell proliferation, differentiation and apoptosis (genomic pathway). Thus, vitamin D has pleiotropic effects and can even act in a paracrine or autocrine manner in addition to its endocrine function. This fact would explain the additional non-calciotropic effects of vitamin D, as its involvement in autoimmunity, endocrine, infectious, metabolic and neurological diseases, and mood disorders. Obviously, the expression of VDR in immune cells suggests that vitamin D plays a critical role in regulating both innate and adaptive immune systems. That is, vitamin D deficiency could compromise the integrity of the immune system and lead to inappropriate immune responses such as autoimmune diseases (5-8).
While there is current evidence that low vitamin D levels are a risk factor for autoimmune diseases (diabetes, multiple sclerosis, systemic lupus erythematosus, juvenile idiopathic arthritis etc.), it remains uncertain if vitamin D deficiency is a significant factor in the pathogenesis or functional consequences of autoimmune hypothyroidism (1, 9-11).
The aim of this review is to elaborate a comprehensive literature review (narrative review) about (a) recent data on the possible influence of vitamin D deficiency on the pathogenic mechanism of autoimmune hypothyroidism, (b) the relationship between vitamin D status and thyroid function and finally, (c) the evaluation of the effect of vitamin D supplementation on thyroid function This review is based on an electronic search of literature performed by two independent researchers in the PubMed database of the U.S. National Library of Medicine published between January 2011 and December 2023. The following specific keywords (Medical Subject Headings) were used alone or in combination for the search: vitamin D or vitamin D deficiency/insufficiency, Hashimoto thyroiditis, autoimmunity, thyroid autoimmunity, and anti-thyroid antibodies (anti-thyroglobulin antibodies and anti-thyroid peroxidase).
2. Immunomodulatory function of Vitamin D
Active vitamin D launches most of its effects after binding to the vitamin D nuclear receptor (VDR), which subsequently joins the “retinoid X receptor”. This heterodimer acts on the “vitamin D response element” and controls the expression/transcription of numerous coding genes responsible for the regulation of cellular proliferation, differentiation and apoptosis (genomic pathway). The majority of immune cells, including antigen-presenting (macrophages and dendritic cells), T and B cells contain and express the VDR and the vitamin D activating enzyme 1-a-hydroxylase. In this way, vitamin D status has an important role in the activation, proliferation, and phenotype of immune cells, which, in turn, have the capacity to directly activate vitamin D precursor (cells of immune system respond to vitamin D and activate vitamin D in a paracrine or autocrine ways). The wide expression of VDR in immune cells suggests that vitamin D plays a critical role in regulating both innate and adaptive immune systems. This classification (innate and adaptive immune systems) is merely didactic, because both systems operate in an integrated way. The innate immune system activates the adaptive immune system, and the adaptive immune system uses the effector mechanisms of innate immunity to eliminate non-self-progenic antigenic elements.
Figure 1 displays the immunomodulatory effects of active vitamin D on various immune cells lineages.
2.1. Vitamin D and innate immunity
Vitamin D is an important mediator of innate immune responses (figure 1). For example, vitamin D stimulates the differentiation of monocytes into macrophages and, consequently, improves chemotaxis and phagocytic capabilities of innate immune cells. Likewise, vitamin D improves the antimicrobial properties of the immune cells (monocytes, neutrophils and natural killer cells) and barrier epithelia through the modulation gene expression of potent antimicrobial peptides (AMPs), such as cathelicidin and β-defensine, which destroy the cell membranes of bacteria and viruses. On the other hand, vitamin D has important effects on both natural killer cells, monocytes and dendritic cells (DCs). It inhibits the production of inflammatory cytokines such as interleukin IL-1, IL-2, IL-6, IL-8, IL-12 and interferon gamma (IFN-γ) and toll-like receptors (TLR2 y TLR4), resulting in a stage of insufficient immune responsiveness and, in this way, it helps avoid excessive innate responses and consequent tissue damage (systemic inflammation and/or septic shock). Additionally, it impairs DC differentiation and maturation as evidenced by a decreased expression of major histocompatibility complex (MHC) class II molecules, co-stimulatory molecules (CD40, CD80, CD86) and CD1a (type of non-classical antigen-suplading molecule). The ultimate effect of vitamin D with the preservation of the immature phenotype of DCs is a reduction in the number of antigen-presenting cells and activation of naïve T cells, thus contributing to an induction of a tolerogenic state. Thereby, the interaction between immature DCs (tolerogenic phenotype) and T cells causes T cell anergy and apoptosis and fosters the synthesis of tolerogenic cytokines. In fact, inhibition of DC differentiation and maturation is particularly important in the context of autoimmunity and the suppression of self-tolerance.
2.2. Vitamin D and adaptive immunity
Vitamin D also plays a role in the regulation of adaptive immunity (figure 1). Vitamin D modulates the activation and differentiation of naïve CD4+ lymphocytes after the presentation of the antigen by the DCs in the lymph nodes, resulting in a shif from a T-helper 1 (Th1) to a Th2 phenotype. This change implies an inhibition of inflammatory cytokine production (IL-2, IFN-γ and tumor necrosis factor alfa (TNF-α) and an increased production of anti-inflammatory cytokines (IL-4, IL-5 and IL-10). Furthermore, vitamin D affects differentiation to Th17 phenotype, leading to a decrease in the production of inflammatory cytokines such as IL-17 and IL-21 (linked to organ-specific autoimmunity, inflammation, and tissue damage), and facilitates the induction of T regulatory cells (Tregs), causing an increased production of anti-inflammatory cytokines such as transforming growth factor beta (TGF-β) and IL-10. Treg cells are able to suppress the proliferation and production of inflammatory cytokines by CD4+ T cells as well as the proliferation of CD8+ (cytotoxic lymphocytes) and antigen-presenting cells. In this way, vitamin D would modulate cell-mediated immune responses and regulate the inflammatory activity of T cells and, consequently, have a significant role in preventing exaggerated or autoimmune responses.
With regard to B-lymphocyte regulation, vitamin D impact on B cell homeostasis in several ways (through the inhibition of follicular T helper cells). For example, it reduces naïve B cell activation and proliferation, induces apoptosis of activated B cells and suppresses the differentiation of B cells into plasma cells. In addition, vitamin D also inhibits memory B cell generation and reduce the immunoglobulin synthesis (IgG and IgM) in activated B cell. This control on B cell activation and proliferation may be clinically important in autoimmune diseases as B-cells producing autoreactive antibodies play a major role in the pathophysiology of autoimmunity.
In, summary, vitamin D exerts direct and indirect effects on both innate and adaptive immune cells, and these cells widely express the VDR. In fact, vitamin D exerts an immunomodulatory role both in the innate and adaptive immune systems that appears to promote immune tolerance and therefore acts to decrease the likelihood of developing autoimmune disease. (5, 6, 9, 11-16).
3. Hashimoto's thyroiditis
Chronic autoimmune thyroiditis is characterized by self-tissue destruction via the adaptive immune responses which evade immune regulation. Under normal conditions, and once the human body manifests tolerance, the process of autoimmunity does not occur. However, whenever this process of tolerance is altered, autoimmunity occurs, just as it does in HT. It is characterized by a diffuse goiter that reflects intrathyroidal infiltration of B and T lymphocytes with CD4+ type 1 T helper (Th1) subtype predominance, and circulating anti-thyroid peroxidase (TPOAb) and/or anti-thyroglobulin (TGAb) antibodies that causes a differing degree of thyroid hypofunction. Antibody titers are positively correlated with the severity of thyroid inflammation and hypothyroidism. In particular, TPOAb is the most important autoantigen involved in the induction of autoimmune thyroid disease. Thyroid peroxidase has an essential role in the production of thyroid hormones (thyroxine and triiodothyronine) while thyroglobulin produces the storage of thyroid hormones in the thyroid follicles. The diagnosis of HT is based on clinical symptoms, anti-thyroid antibodies and histological features. TPOAb are considered the most important feature of HT and are present in about 95% of patients. Instead, TGAb are present in a lower (60–80%) percentage of cases and therefore are less reliable for diagnosis. It appears that TGAb may constitute the expression of an initial immune response, whereas TPOAb may be the result of a later immune response as if there was an immune escalation. At present, HT is yet an incurable disease with at time unforeseeable consequences and unpredictable evolution, often resulting in lymphocytic destruction of the thyroid parenchyma, which leads to hypothyroidism and the need for thyroid hormone replacement for life (2).
HT has a multifactorial etiology, involving (a) genetic predisposition (the role of genetic factors in HT pathogenesis is suggested both by the high concordance rate for HT in monozygotic twins and by the frequent finding of thyroid autoantibodies or other autoimmune diseases in blood relatives of the HT probands; the results of association studies of VDR polymorphisms -ApaI, BsmI TaqI and Fok1- with autoimmune thyroid diseases are inconclusive), (b) environmental factors (e.g., radiation, smoking habits, stress, infections, iodine and selenium intake and dietary choices) and (c) endogenous factors (e.g., body mass index, adipokines, estrogens, microchimerism and glucocorticoids and potentially the gastrointestinal microbiome). Environmental factors could play an important role, as recent epidemiological changes demonstrate, and development of HT may be due not only to an innate predisposition, but also to environmental factors that have changed rapidly. These factors might finally trigger the development of autoimmunity. Thereby, in individuals with genetic predisposition, the alteration of these immune-endocrine interactions by environmental factors results in the shift of the previous physiological balance in the Th1-Th2 immune response. Consequently, there is a Th1-cell-mediated autoimmune reaction with thyrocyte destruction and hypothyroidism in HT. Furthermore, a shift in the balance between Th17 and Treg cells in thyroid autoimmunity has been recently observed (14, 17-19).
4. Autoimmune mechanism of autoimmune hypothyroidism
The gist of the autoimmune process that occurs in HT is a disruption in self-tolerance to thyroid autoantigens and a subsequent destruction of the thyroid tissue due to the infiltration of CD4+ Th1, macrophages, and plasma cells, which release autoantibodies against thyroid peroxidase (TPOAb) and thyroglobulin (TGAb). Therefore, the diagnosis of HT is generally guided by the detection of elevated titers of these antibodies (16).
First, environmental and genetic factors gives way to the activation of antigen-presenting cells (APCs), predominantly DCs, and these cells present autoantigens to naive CD4+ T cells in lymph nodes, a process that induces the differentiation into Th1, Th2, Th17, or Tregs. Interestingly, these follicular thyroid cells in HT patients have the potential to express major histocompatibility complex class II molecules (MHC-II), which are essential in the process of presenting antigens to CD4+ T cells. In this way, thyroid cells are able to act as APCs by means of the presentation of autoantigens to T cells and the activation of their differentiation. Second, the cytokines released by Th1, including IL-2 and IFN-γ, induce the expression of MHC-II on thyroid cells, and secondarily cause the differentiation of the naive CD4+ T cells into Th1. Finally, Th1 cells, via IL-2 and IFN-γ, induce the activation of CD8+ T cells (cytotoxic T cells). CD8+ T cells induce apoptosis of thyroid cells (Figure 2), which leads to the release of pro-inflammatory cytokines that contribute to the activity and migration of pathological Th17 cells and the suppression of Tregs cells, and consequently amplifies and sustains the immune feedback process. Some authors have suggested that Th1/Th2 cell imbalance and Th1 cell activity enhancement would be the main contributors to the development of HT, but other authors estimate that increased Th17/Treg ratio would play a critical role in the pathogenesis of autoimmune thyroid diseases. This results in positive feedback and the initiation of the autoimmune process and subsequent consolidation. However, in the destruction of the thyroid gland and the mechanism of the autoimmune process, a humoral response also occurs (Figure 2).
The recruitment of Th1 lymphocytes is associated to the stimulation of B lymphocytes, which are placed in the lymph nodes within the tissue of the thyroid gland. Infiltrating B cells release autoantibodies, mainly TPOAb and TGAb, which constitute thyroid self-antigens. Antibodies play a part in the apoptosis of thyroid follicular cells in the procedure of antibody-dependent cell-mediated cytotoxicity (2, 8, 13, 16, 20, 21). In the course of HT, self-reactive CD4+ T lymphocytes recruit B cells and CD8+ T cells into the thyroid. Finally, the progression of the disease leads to the death of thyroid cells and hypothyroidism.
5. Immunomodulatory role of vitamin D in Hashimoto's thyroiditis
As described above, vitamin D exerts an immunomodulatory role both in the innate and adaptive immune systems that appears to promote immune tolerance and, in this case, it could contribute to the inhibition of the immunopathological process in HT. On one hand, active vitamin D induces the differentiation of monocytes into macrophages and boosts their antimicrobial activity via the increase of the transcription of antimicrobial peptide genes, such as beta-defensin and cathelicidin antimicrobial peptide. That is, vitamin D improves chemotaxis and phagocytic capabilities and antimicrobial properties of innate immune cells. On the other hand, vitamin D also plays a role in the regulation of adaptive immunity, as it modulates the activation and differentiation of naïve CD4+ lymphocytes after antigen presentation by DCs in lymph nodes. In other words, Vitamin D carries out an immunomodulatory role both in the innate and adaptive immune systems that appears to promote immune tolerance and, in this case, it could contribute to the inhibition of the immunopathological process in HT.
The potential mechanisms by which vitamin D could contribute to inhibiting the autoimmune process in HT would be varied and complementary, and could be summarized as follows:
(a) Vitamin D inhibits the expression of various proinflammatory cytokine from DCs (IL-12, IL-6 and IL-12) that activate T cells while enhancing the expression of IL-10 (anti-inflammatory or tolerogenic cytokine); this results in a stage of insufficient immune responsiveness and, in this way, it helps avoid excessive innate responses and consequent tissue damage (systemic inflammation and/or septic shock). Additionally, vitamin D impairs DCs differentiation and maturation as evidenced by a decreased expression of MHC-II and co-stimulatory molecules (CD40, CD80, CD86); this preservation of the immature phenotype of DCs results in a reduction in the number of antigen-presenting cells and activation of naïve T cells, thus contributing to an induction of a tolerogenic state. Vitamin D also modulates the activation and differentiation of naïve CD4+ lymphocytes after the presentation of the antigen by the DCs in the lymph nodes, resulting in a shift from a T-helper (Th)1 to a Th2 phenotype which is an inhibition of inflammatory cytokine production (IL-2, IFN-γ and TFN-α) and an increased production of anti-inflammatory cytokines (IL-4, IL-5 and IL-10).
(b) Vitamin D may reduce MHC-II expression in the follicular thyroid cells, thus preventing T-cell activation and proinflammatory cytokine response.
(c) Vitamin D affects differentiation of naïve T cells towards the Th17 phenotype, leading to a decrease in the production of inflammatory cytokines such as IL-17 (linked to organ-specific autoimmunity, inflammation, and tissue damage), and facilitates the induction of T regulatory cells (Tregs) with increased production of anti-inflammatory cytokines such as IL-10 and TGF. Treg cells are able to suppress the proliferation and production of inflammatory cytokines by CD4+ T cells as well as the proliferation of CD8+ (cytotoxic lymphocytes) and APCs. Therefore, vitamin D contributes to the restoration of Th17/Treg ratio (Th17 cells generate mainly proinflammatory activity, and this action accidentally contributes to the development of autoimmune disorders, whereas Tregs helps in the modulation of the immune system and the maintenance of the tolerance to self-antigens, so preventing autoimmunity). In this way, vitamin D would modulate cell-mediated immune responses and regulate the inflammatory activity of T cells and, consequently, have a significant role in preventing exaggerated or autoimmune responses.
(d) Finally, with regard to B-lymphocyte regulation, vitamin D impacts on B cell homeostasis in several ways. For example, reduces naïve B cell activation and proliferation, induces apoptosis of activated B cells as well as suppresses the differentiation of B cells into plasma cells. In addition, vitamin D also inhibits memory B cell generation and reduces the immunoglobulin synthesis (IgG and IgM). This control on B cell activation and proliferation may be clinically important in HT, as B-cells producing autoreactive antibodies play a major role in the pathophysiology of autoimmunity.
Thereby, vitamin D induces a shift from a pro-inflammatory to a more tolerogenic immune status, resulting in a limitation in the development of self-reactive T cells preventing inflammation and autoimmunity (6, 7, 9, 16, 21, 22). Thus, vitamin D appears to play an important immunomodulatory role, and its relationship with autoimmune thyroid disease has been widely studied in recent years.
In addition, a high Th22 cell count has been reported in blood and thyroid of HT patients, being considered as decisive in the Inflammatory effects of IL-22 on thyroid cells (17).
6. Relationship between vitamin D status and Hashimoto's thyroiditis
Many observational studies (case-control or cross-sectional studies) have shown a potential link between hypovitaminosis D and a higher risk of HT onset (22-34). In fact, considering adult population, a low vitamin D status has been reported in patients with autoimmune thyroid diseases or HT, suggesting an association between vitamin D deficiency and thyroid autoimmunity. In fact, several authors reported that the prevalence of vitamin D deficiency in patients with HT was significantly higher compared with healthy individuals, and that serum calcidiol levels were inversely correlated with anti-thyroid antibodies (TGAb and TPOAb), suggesting the involvement of vitamin D in its pathogenesis. In addition, within HT cases, a higher prevalence of vitamin D deficiency and lower calcidiol levels have been detected in patients with hypothyroidism in comparison to patients with euthyroidism or healthy individuals.
On the other hand, few studies have focused on investigating the potential association between low vitamin D levels and HT in children, whose reported results are absolutely similar to those of adults. That is, these authors conclude that, also in children, low serum vitamin D levels are significantly associated with autoimmune thyroid diseases or HT, although they also indicate that it is not an independent risk factor for the progression to overt hypothyroidism (35-39).
However, the results of other observational studies have not found relationship between vitamin D levels and antithyroid antibodies or thyroid function (18, 40-43). Diverse factors could play a part in the discordance between the studies. These include the application of different commercially available kits for serum vitamin D assay or the consensus on a definition of vitamin D deficiency between the studies, as well as potential confounding factors such as BMI, ethnic, seasonal or geographical differences (17).
Nevertheless, recent systematic reviews, meta-analyses, and meta-regression of observational studies (44-48) have confirmed that vitamin D levels were significantly lower in autoimmune hypothyroidism disease or HT patients compared to healthy people. Accordingly, it seems that there is proven evidence supporting a relationship between low vitamin D status and HT.
Further, several authors have reported an inverse correlation between TSH and Vitamin D status in healthy young people as well as in middle-aged and older men (49, 50). Apart from its association with autoimmune thyroid diseases, vitamin D deficiency has been detected in other autoimmune disorders, such as multiple sclerosis, diabetes mellitus, systemic lupus erythematosus, and others (10, 11)
7. Vitamin D supplementation in Hashimoto's thyroiditis
The extensive information suggesting a relationship between low levels of vitamin D and autoimmune thyroid diseases has motivated emerging interest in the investigation of the administration of vitamin D supplements (cholecalciferol) in the prevention/treatment of HT. At present, there is still no specific drug to reduce the antibody titer, but sufficient evidence linking vitamin D deficiency to HT has led to clinical trials that intend to examine the potential beneficial effects of vitamin D supplementation in the prevention and treatment of autoimmune thyroid disorders. Most of the available randomized controlled trials have found that, after supplementation with cholecalciferol in patients diagnosed with HT and vitamin D deficiency, thyroid autoantibodies (TPOAb and TgAb) titers decreased significantly (Table 1), posing that vitamin D treatment may have a beneficial effect on autoimmunity hypothyroidism (in these studies, calcidiol concentration increased reaching above 30 ng/ml). In addition, the reduction in antibody levels was also detected in subjects with normal baseline vitamin D status (51).
However, a recent meta-analysis of randomized controlled trials concludes that most of these studies have not observed a decrease or any trackable change in TSH levels after supplementation with vitamin D, while thyroid hormones remained mostly unaltered after supplementation (10). Although the majority of studies on antithyroid antibodies after vitamin D supplementation showed consistent outcomes, it should be mentioned that other investigations provided contrary results (52-54). Nevertheless, recent systematic reviews and meta-analysis have confirmed that vitamin D supplementation is associated to a reduction of TGAb and TPOAb titers in patients with HT in the short-term. The effect was more intense if patients received cholecalciferol and the duration of treatment was more than 3 months (55-56), However, there are no conclusive results on the effect of vitamin D supplementation on the thyroid function.
The results found in a study with a large number of patients with HT (case-control design) are particularly remarkable. Participants received doses of vitamin D (between 1,000 and 4,000 IU daily) to achieve optimal concentrations (>40 ng/ml). After 12 months of follow-up, a significant reduction in antithyroid antibody titer was observed. Furthermore, it was found that concentration of calcidiol >50 ng/ml was associated with a substantial improvement in thyroid function, including a reduction in TSH levels and symptom severity. That is, vitamin D would offer a safe and economical approach to improve thyroid function and could provide protection against the development of autoimmune thyroiditis. (57).
Exceptionally, clinical trials have been carried out in pediatric age. A recent randomized clinical trial performed exclusively in pediatric patients with HT (average age: 12.6 years) showed that the level of autoantibodies and thyroid volume decreased after vitamin D supplementation. Patients with hypovitaminosis (<30ng/ml) received 50,000 IU pearl every week for 6 weeks, subsequently serum calcidiol level was rechecked and if it reached normal range (>30 ng/ml), the patients continued the intake of cholecalciferol once a month for 6 months. Antithyroid antibody titers (TPOAb and TGAb) decreased significantly, as did the size of both thyroid lobes after intervention. (58) Thus, it is suggested that serum VD level should be routinely checked in these patients and, when observing hypovitaminosis, an appropriate treatment with vitamin D should be carried out.
8. Conclusions
Vitamin D carries out an immunomodulatory role both in the innate and adaptive immune systems that appears to promote immune tolerance and, in this case, it could contribute to the inhibition of the immunopathological process in HT. Although the mechanisms underlying in the interrelationship of vitamin D and HT remain unknown, they are likely related to their anti-inflammatory and immunomodulatory properties. There is an extensive literature analyzing the complex relationship between vitamin D deficiency and autoimmune thyroid disorders; however, data are yet inconclusive. There is a need to solve this ambiguity regarding the causal relationship between vitamin D and thyroid disorders. Since vitamin D supplementation is inexpensive and has minimal side effects, its use may constitute a potential revolution in the treatment of hypothyroidism.
There is still a gap in the knowledge regarding the potential of vitamin D supplementation in the treatment of HT patients, whether vitamin D supplementation will help in decreasing the replacement dose of levothyroxine or whether it will stop the need of levothyroxine replacement if used in early stages of HT.
More studies (preferably randomized, double-blind, placebo-controlled trials with longer follow-up periods) are needed to confirm the beneficial effects of vitamin D in the prevention and treatment of autoimmune thyroid diseases. However, some authors have suggested that, when diagnosing patients with HT, vitamin D replacement may be suggested as an auxiliary treatment, and they even predict that, in the future, vitamin D could become part of the treatment of autoimmune thyroid diseases, especially in those individuals with vitamin D insufficiency.
Compliance with Ethical Standards
Funding
The authors received no financial support for the research, authorship, and/or publication of this article (none declared).
Ethical Approval
Not applicable
Disclosure of potential conflicts of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article (none declared).
Contribution Statement
TDT participated in study design and data analysis, and wrote the first draft of the manuscript. FGV participated in data collection and analysis. All authors participated in manuscript preparation and approved its final version.
Informed consent
Not applicable
Data availability
Not applicable
List of abbreviation
APCs: antigen-presenting cells,
CD8+ T cells: cytotoxic T cells
DCs: dendritic cells
CTL: cytotoxic T lymphocytes
HT: Hashimoto's thyroiditis
IFN-γ: interferon-γ
IL: interleukin
MHC-II: Major histocompatibility complex class II molecules
TG. tiroglobulin
TGAb: anti-thyroglobulin antibodies.
TGF-β: transforming growth factor beta
Th1: CD4+ type 1 T helper
Th2: CD4+ type 2 T helper
Th17: CD4+ type 17 T helper
TNF-α: tumor necrosis factor alfa
TPO: thyroid peroxidasa
TPOAb: anti-thyroid peroxidase antobodies
Treg: CD4+ T regulatory cells
TSH: thyrotrophin
VDR: vitamin D receptors
References
- Bellan M, Andreoli L, Mele C, Sainaghi PP, Rigamonti C, Piantoni S, et al (2020) Pathophysiological Role and Therapeutic Implications of Vitamin D in Autoimmunity: Focus on Chronic Autoimmune Diseases. Nutrients 12: 789.
- Ralli M, Angeletti D, Fiore M, D’Aguanno V, Lambiase A, Artico M, et al (2020) Hashimoto’s Thyroiditis: An Update on Pathogenic Mechanisms, Diagnostic Protocols, Therapeutic Strategies, and Potential Malignant Transformation. Autoimmun. Rev 19: 102649.
- Hossein-Nezhad A, Holick MF (2013) Vitamin D for health: A global perspective. Mayo Clin Proc 88:720–755.
- Palermo NE, Holick MF (2014) Vitamin D, bone health, and other health benefits in pediatric patients. J Pediatr Rehabil Med 7:179–192.
- Prietl B, Treiber G, Pieber TR, Amrein K (2019). Vitamin D and immune function. Nutrients 5:2502–2521.
- Cyprian F, Lefkou E, Varoudi K, Girardi. G (2019) Immunomodulatory Effects of Vitamin D in Pregnancy and Beyond. Front Immunol 10:2739.
- Mele C, Caputo M, Bisceglia A, Sama MT, Zavattaro M, Aimaretti G, et al (2020) Immunomodulatory Effects of Vitamin D in Thyroid Diseases. Nutrients 12:1444.
- Boguslawska J, Godlewska M, Gajda E, Piekielko-Witkowska A (2022) Cellular and molecular basis of thyroid autoimmunity. Eur Thyroid J 11:e210024.
- Altieri B, Muscogiuri G, ¿Barrea L, Mathieu C, Vallone CV, Mascitelli L, et al. (2017) Does vitamin D play a role in autoimmune endocrine disorders? A proof of concept. Rev Endocr Metab Disord 18:335–346.
- Jiang H, Chen X, Qian X, Shao S (2022) Effects of vitamin D treatment on thyroid function and autoimmunity markers in patients with Hashimoto’s thyroiditis-A meta-analysis of randomized controlled trials. J Clin Pharm Ther 47:767–775.
- Gallo D, Baci D, Kustrimovic N, Lanzo N, Patera B, Tanda ML, et al (2023) How Does Vitamin D Affect Immune Cells Crosstalk in Autoimmune Diseases? Int J Mol Sci 24:4689.
- Rosen Y, Daich J, Soliman I, Brathwaite E, Shoenfeld Y (2016) Vitamin D and autoimmunity. Scand J Rheumatol 45:439-447.
- Kim M, Song E, Oh HS, Park S, Kwon H, Jeon MJ, et al (2017) Vitamin D deficiency affects thyroid autoimmunity and dysfunction in iodine-replete area: Korea national health and nutrition examination survey. Endocrine 58:332–339.
- Vieira IH, Rodrigues D, Paiva I (2020) Vitamin D and Autoimmune Thyroid Disease-Cause, Consequence, or a Vicious Cycle? Nutrients 12:2791.
- Zhao R, Zhang W, Ma C, Zhao Y, Xiong R, Wang H, et al (2021) Immunomodulatory Function of Vitamin D and Its Role in Autoimmune Thyroid Disease. Front Immunol 12:574967.
- Lebiedzinski F, Lisowska KA (2023) Impact of Vitamin D on Immunopathology of Hashimoto’s Thyroiditis: From Theory to Practice. Nutrients 15:3174.
- Weetman AP (2021) An update on the pathogenesis of Hashimoto’s thyroiditis. J Endocrinol Invest 44:883-890.
- Babic Leko M, Jureško I, Rozic I, Pleic N, Gunjača I, Zemunik T (2023). Vitamin D and the Thyroid: A Critical Review of the Current Evidence. Int J Mol Sci 24:3586.
- Czarnywojtek A, Florek E, Pietronczyk K, Sawicka-Gutaj N, Ruchała M, Ronen O, et al (2023) The Role of Vitamin D in utoimmune Thyroid Diseases: A Narrative Review. J Clin Med 12:1452.
- Pyzik A, Grywalska E, Matyjaszek-Matuszek B, RoliNski J (2015) Immune disorders in Hashimoto’s thyroiditis: what do we know so far? J Immunol Res 2015:979167.
- Luty J, Ruckemann-Dziurdzinska K, Witkowski JM, Bryl E (2019) Immunological Aspects of Autoimmune Thyroid Disease—Complex Interplay between Cells and Cytokines. Cytokine 116:128–133.
- Koehler VF, Filmann N, Mann WA (2019) Vitamin D Status and Thyroid Autoantibodies in Autoimmune Thyroiditis. Horm Metab Res 51:792–797.
- Kivity S, Agmon-Levin N, Zisappl M, Shapira Y, Nagy EV, Dankó K, et al (2011) Vitamin D and autoimmune thyroid diseases. Cell Mol Immunol 8:243–247.
- Tamer G, Arik S, Tamer I, Coksert D (2011) Relative vitamin D insufficiency in Hashimoto’s thyroiditis. Thyroid 21:891–896.
- Bozkurt NC, Karbek B, Ucan B, Sahin M, Cakal E, Ozbek M, et al (2013) The association between severity of vitamin D deficiency and Hashimoto’s thyroiditis. Endocr Pract 19:479–484.
- Mansournia N, Mansournia MA, Saeedi S, Dehghan J (2014) The association between serum 25OHD levels and hypothyroid Hashimoto’s thyroiditis. J Endocrinol Investig 37: 473–476.
- Unal AD, Tarcin O, Parildar H, Cigerli O, Eroglu H, Demirag NG (2014) Vitamin D deficiency is related to thyroid antibodies in autoimmune thyroiditis. Cent Eur J Immunol 39:493–497.
- Mazokopakis EE, Papadomanolaki MG, Tsekouras KC, Evangelopoulos AD, Kotsiris DA, Tzortzinis AA (2015) Is vitamin D related to pathogenesis and treatment of Hashimoto’s thyroiditis? Hell J Nucl Med 18:222–227.
- Kim D (2016) Low vitamin D status is associated with hypothyroid Hashimoto’s thyroiditis. Hormones 15:385–393.
- Giovinazzo S, Vicchio TM, Certo R, Alibrandi A, Palmieri O, Campenni A, et al (2016) Vitamin D receptor gene polymorphisms/haplotypes and serum 25(OH)D3 levels in Hashimoto’s thyroiditis. Endocrine 55:599–606.
- De Pergola G, Triggiani V, Bartolomeo N, Giagulli VA, Anelli M, Masiello M, et al (2018) Low 25 Hydroxyvitamin D Levels are Independently Associated with Autoimmune Thyroiditis in a Cohort of Apparently Healthy Overweight and Obese Subjects. Endocr. Metab. Immune Disord. Drug Targets 18:646–652.
- Krysiak R, Szkróbka W, Okopien B (2019) The effect of gluten-free diet on thyroid autoimmunity in drug-naïve women with Hashimoto’s thyroiditis: A pilot study. Exp Clin Endocrinol Diabetes 127:417–422.
- Aktaş HS (2020) Vitamin B12 and Vitamin D Levels in Patients with Autoimmune Hypothyroidism and Their Correlation with Anti-Thyroid Peroxidase Antibodies. Med Princ Pract 29:364–370.
- Appunni S, Rubens M, Ramamoorthy V, Saxena A, Tonse R, Veledar E, et al (2021) Association between vitamin D deficiency and hypothyroidism: results from the National Health and Nutrition Examination Survey (NHANES) 2007–2012. BMC Endocrine Disorders 21:224.
- Zaidman V, Maceiras M, Lazzati J, Kutasz E, D’Isa G, Chilleli C, et al (2014) High prevalence of anti-thyroid antibodies associated with a low vitamin D status in a pediatric cohort. Clin Chem Lab Med 52:e119-122.
- Camurdan OM, Döger E, Bideci A, Celik N, Cinaz P (2012) Vitamin D status in children with Hashimoto thyroiditis. J Pediatr Endocrinol Metab 25:467–470.
- Evliyaoglu O, Acar M, Özcabı B, Erginöz E, Bucak F, Ercan O, et al (2015) Vitamin D deficiency and Hashimoto’s thyroiditis in children and adolescents: A critical vitamin D level for this association? J Clin Res Pediatr Endocrinol 7:128–133.
- Metwalley KA, Farghaly HS, Sherief T, Hussein A (2016) Vitamin D status in children and adolescents with autoimmune thyroiditis. J Endocrinol Investig 39:793–797.
- Sönmezgöz E, Ozer S, Yilmaz R, Önder Y, Bütün I, Bilge S (2016) Hypovitaminosis D in children with Hashimoto's thyroiditis. Rev Med Chil 144:611-616.
- D’Aurizio F, Villalta D, Metus P, Doretto P, Tozzoli R (2015) Is vitamin D a player or not in the pathophysiology of autoimmune thyroid diseases? Autoimmun Rev 14:363–369.
- Ke W, Sun T, Zhang Y, He L, Wu Q, Liu J, et al (2017) 25-Hydroxyvitamin D serum level in Hashimoto’s thyroiditis, but not Graves’ disease is relatively deficient. Endocr J 64:581–587.
- Yasmeh J, Farpour F, Rizzo V, Kheradnam S, Sachmechi I (2016) Hashimoto thyroiditis not associated with vitamin D deficiency. Endocr Pract 22:809–813.
- Cvek M, Kalicanin D, Baric A, Vuletic M, Gunjac I, Torlak Lovric V, et al (2021) Vitamin D and Hashimoto’s Thyroiditis: Observations from CROHT Biobank. Nutrients 13:2793.
- Wang J, Lv S, Chen G, Gao C, He J, Zhong H, et al (2015) Meta-analysis of the association between vitamin D and autoimmune thyroid disease. Nutrients 7:2485–2498.
- Štefanic M, Tokic S (2020) Serum 25-hydoxyvitamin D concentrations in relation to Hashimoto’s thyroiditis: A systematic review, meta-analysis and meta-regression of observational studies. Eur J Nutr 59:859–872.
- Taheriniya S, Arab A, Hadi A, Fadel A, Askari G (2021) Vitamin D and thyroid disorders: a systematic review and Meta-analysis of observational studies. BMC Endocrine Disorders 21:171.
- Khozam SA, Sumaili AM, Alflan MA, Shawabketh RAS. (2022) Association Between Vitamin D Deficiency and Autoimmune Thyroid Disorder: A Systematic Review. Cureus 14: e25869.
- Ashok T, Palyam V, Azam AT, Odeynka O, Alhashimi R, Thoota S, et al. (2022) Relationship Between Vitamin D and Thyroid: An Enigma. Cureus 14: e21069.
- Chailurkit LO, Aekplakorn W, Ongphiphadhanakul B (2013) High Vitamin D Status in Younger Individuals Is Associated with Low Circulating Thyrotropin. Thyroid 23:25–30.
- Barchetta I, Baroni M, Leonetti F, De Bernardinis M, Bertoccini L, Fontana M, et al (2015) TSH levels are associated with vitamin D status and seasonality in an adult population of euthyroid adults. Clin Exp Med 15:389–396.
- Krysiak R, Szkrobka W, Okopien B (2017) The Effect of Vitamin D on Thyroid Autoimmunity in Levothyroxine-Treated Women with Hashimoto’s Thyroiditis and Normal Vitamin D Status. Exp. Clin. Endocrinol. Diabetes 125:229–233.
- Vondra K, Stárka L, Hampl R (2015) Vitamin D and thyroid diseases. Physiol Res 64 (Suppl. 2):S95–S100.
- Knutsen KV, Madar AA, Brekke M, Meyer HE, Eggemoen AR, Mdala I, et al (2017) Effect of Vitamin D on Thyroid Autoimmunity: A Randomized, Double-Blind, Controlled Trial Among Ethnic Minorities. J Endocr Soc 1:470–479.
- Vahabi Anaraki P, Aminorroaya A, Amini M, Momeni F, Feizi A, Iraj B, et al (2017) Effect of Vitamin D deficiency treatment on thyroid function and autoimmunity markers in Hashimoto’s thyroiditis: A double-blind randomized placebo-controlled clinical trial. J Res Med Sci 22: 03.
- Wang S, Wu Y, Zuo Z, Zhao Y, Wang K (2018) The effect of vitamin D supplementation on thyroid autoantibody levels in the treatment of autoimmune thyroiditis: a systematic review and a meta-analysis. Endocrine 59:499-505.
- Zhang J, Chen Y, Li H, Li H (2021) Effects of Vitamin D on Thyroid Autoimmunity Markers in Hashimoto’s Thyroiditis: Systematic Review and Meta-Analysis. J Int Med Res 49:1-12.
- Mirhosseini N, Brunel L, Muscogiuri G, Kimball S (2017) Physiological Serum 25-Hydroxyvitamin D Concentrations Are Associated with Improved Thyroid Function—Observations from a Community-Based Program. Endocrine 58:563–573.
- Aghili A, Alijanpour Aghamaleki M, Pornasrollah M, Nooreddini HG, Khafri S, lijanpour S (2020) Effect of Vitamin D Therapy on Hashimoto’s Thyroiditis in Children with Hypovitaminosis D. Int J Pediatr 8:10889–10897.
- Chaudhary S, Dutta D, Kumar M, Saha S, Mondal SA, Kumar A, et al (2016) Vitamin D Supplementation Reduces Thyroid Peroxidase Antibody Levels in Patients with Autoimmune Thyroid Disease: An Open-Labeled Randomized Controlled Trial. Indian J Endocrinol Metab 20:391.
- Simsek Y, Cakır I, Yetmis M, Dizdar OS, Baspinar O, Gokay F (2016) Effects of Vitamin D treatment on thyroid autoimmunity. J Res Med Sci 21:85.
- Nodehi M, Ajami A, Izad M, Asgarian Omran H, Chahardoli R, Amouzegar A, et al (2019) Effects of vitamin D supplements on frequency of CD4+ T-cell subsets in women with Hashimoto's thyroiditis: a double-blind placebo-controlled study. Eur J Clin Nutr 73:1236-1243.
- Chahardoli R, Saboor-Yaraghi AA, Amouzegar A, Khalili D, Vakili AZ, Azizi F (2019) Can Supplementation with Vitamin D Modify Thyroid Autoantibodies (Anti-TPO Ab, Anti-Tg Ab) and Thyroid Profile (T3, T4, ¿TSH) in Hashimoto’s Thyroiditis? A Double Blind, Randomized Clinical Trial. Horm Metab Res 51:296–301.63. Krysiak R, Kowalcze K, Okopień B (2022) The impact of vitamin D on thyroid autoimmunity and hypothalamic-pituitary-thyroid axis activity in myo-inositol-treated and myo-inositol-naïve women with autoimmune thyroiditis: A pilot study. J Clin Pharm Ther 47:1759-1767.
- Bhakat B, Pal J, Das S, Charaborty SK (2023). A Prospective Study to Evaluate the Possible Role of Cholecalciferol Supplementation on Autoimmunity in Hashimoto's Thyroiditis. Assoc Physicians India 71:1.
Figure 1.
Immunomodulatory effects of active vitamin D on various immune cells lineages (adapted from 6).
Figure 1.
Immunomodulatory effects of active vitamin D on various immune cells lineages (adapted from 6).
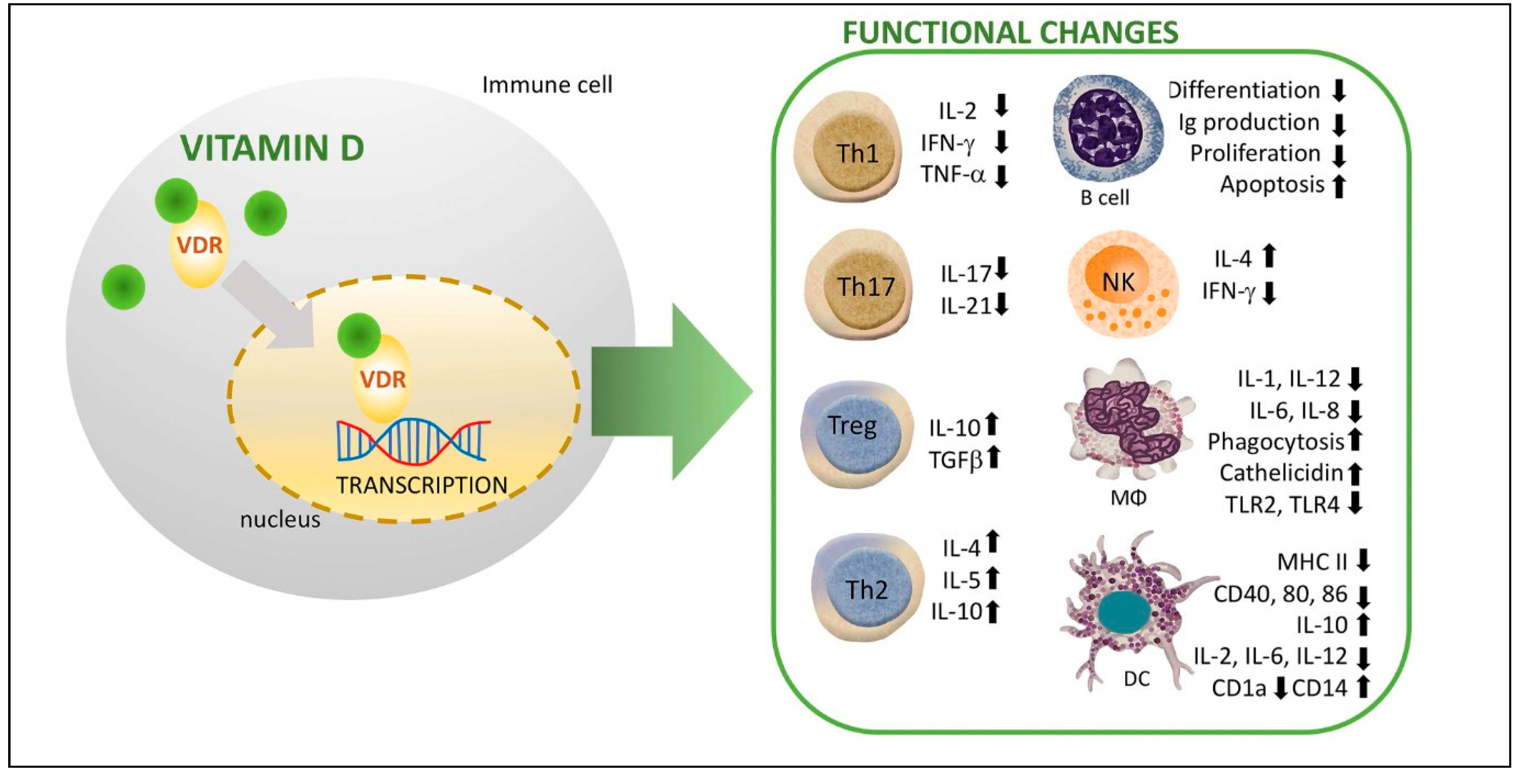
Figure 2.
Autoimmune process: pathogenic necrosis/apoptosis mechanism of thyroid follicular cells (adapted from 2).
Figure 2.
Autoimmune process: pathogenic necrosis/apoptosis mechanism of thyroid follicular cells (adapted from 2).
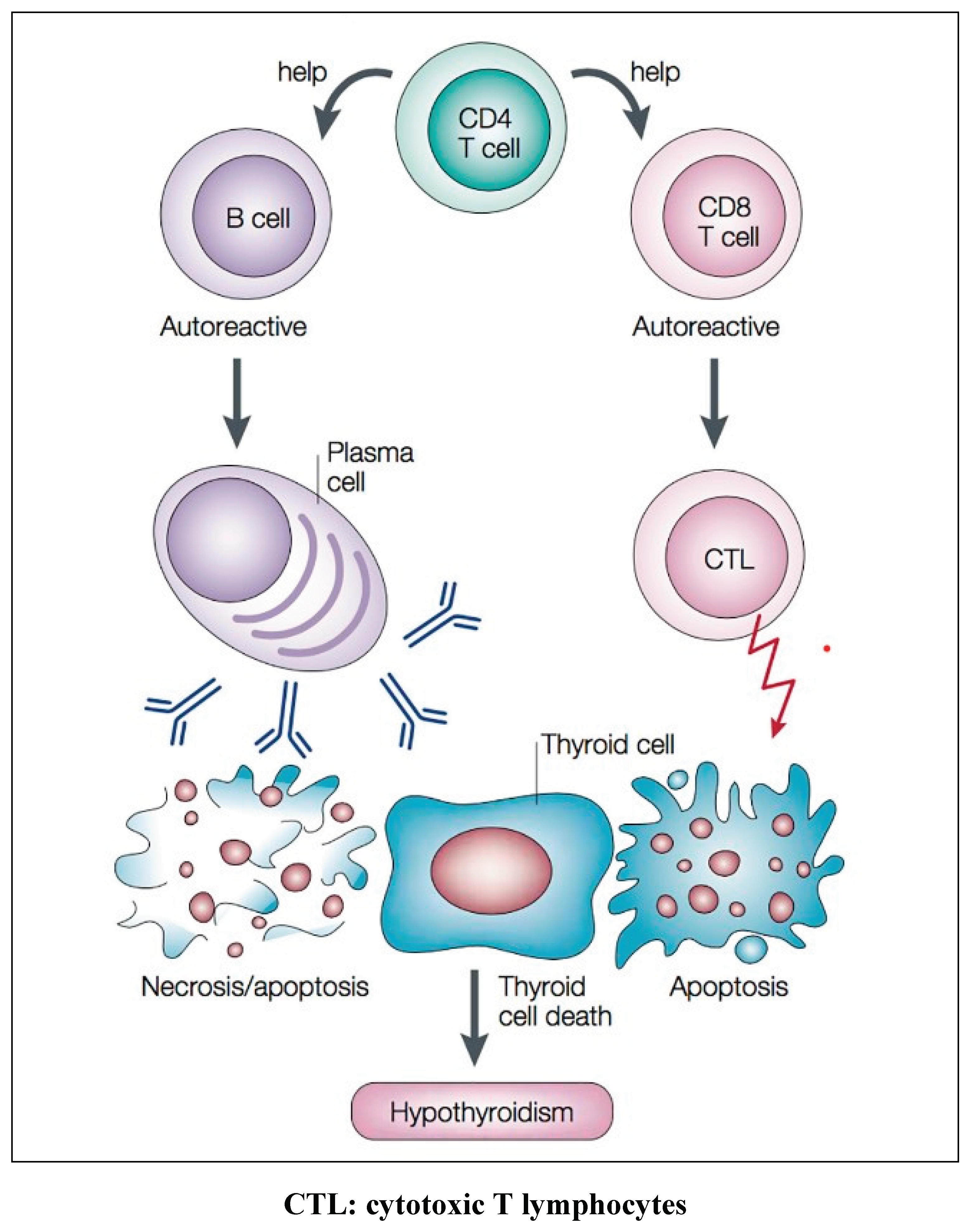

Table 1.
Significant reduction in antithyroid antibody titers after vitamin D (cholecalciferol) supplementation.
Table 1.
Significant reduction in antithyroid antibody titers after vitamin D (cholecalciferol) supplementation.
| Author, Year | Dose of supplementation Duration | Changes in TPOAb | Changes in TGAb |
| Mazokopakis et al, 2015 (28) | 1200-4000 IU/daily for 4 months | Decreased | N.S. |
| Chaudhary et al, 2016 (59) | 60,000 IU weekly, 8 weeks | Decreased | --- |
| Simsek et al, 2016 (60) | 1000 IU/daily for 1 month | Decreased | Decreased |
| Knutsen et al, 2017 (53) | 1000 IU/daily for 4 months | N.S. | --- |
| Krysiak et al, 2017 (51) | 2000 IU daily, 6 months | Decreased | Decreased |
| Mirhosseini et al, 2017 (57) | Doses modified to achieve calciciol concentration >40mg/ml, 12 months | Decreased | Decreased |
| Nodehi et al, 2019 (61) | 50,000 IU weekly, 3 months | ||
| Chahardoli et al, 2019 (62) | 50,000 IU weekly, 3 months | N. S. | Decreased |
| Koehler et al, 2019 (22) | Doses modified to achieve calciciol concentration >40mg/ml, 2 years | Decreased | Decreased |
| Krysiak et al, 2022 (63) | 4000 IU daily for 6 months | Decreased | Decreased |
| Bhakat et al, 2023 (64) | 60,000 IU weekly for 8 weeks | Decreased | Decreased |
N.S.: No significant change.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



