
Submitted:
22 February 2024
Posted:
23 February 2024
You are already at the latest version
Abstract
Cognitive impairment affects 34-65% of People with Multiple Sclerosis (PwMS), significantly impacting their quality of life. Clinicians routinely address cognitive deficits with in-clinic neuro-behavioural interventions, but accessibility issues exist. Telerehabilitation is a promising solution that utilises digital tools for home-based cognitive remediation. This narrative review assessed the feasibility and efficacy of cognitive telerehabilitation in PwMS, identifying 13 relevant studies. Regarding the feasibility of cognitive telerehabilitation, evidence shows adherence rates are generally good, although, surprisingly, not all studies reported a measure of compliance with the cognitive training explored. Considering the efficacy of different rehabilitative techniques on cognitive performance of PwMS, findings are generally inconsistent, with only one study reporting consistently positive results. A range of methodological limitations are reported as potential factors contributing to the variability of results. Overcoming some of these issues will be key. Upcoming research is necessary to determine optimal intervention approaches, long-term effects of rehabilitation, and how to best integrate the use of telerehabilitation into routine clinical practice. By exploiting digital tools in the best way and addressing methodological concerns, home-based rehabilitation holds the potential for improving cognitive functions and enhancing the quality of life in PwMS.
Keywords:
telerehabilitation
; cognitive remediation
; multiple sclerosis
; feasibility
; efficacy
1. Introduction
Multiple Sclerosis (MS) is an inflammatory demyelinating disease of the Central Nervous System (CNS) [1]. It is caused by an autoimmune condition which largely leads to the loss of myelin in the white matter of the brain, spinal cord and optic nerves, with the resulting pathological features being diffuse and focal areas of inflammation, demyelination, gliosis, and neuronal injury [2]. MS is the most common non-traumatic cause of neurological disability in younger adults [3] and estimates suggest 2.8 million people world-wide are living with the disease [4]. Given the widespread nature of the lesions within the CNS [5], MS symptoms can be quite heterogeneous, with patients showing impairment in motor activity, sensory functions, visual functions, cognition, and behaviour. MS disease modifying therapy aims at slowing down the progression of the disease and treating the symptoms, while rehabilitation is primarily targeted towards some degree of recovery of motor and cognitive functions [3].
Around 40%-65% of individuals with MS suffer from Cognitive Impairment (CI) [6,7], with deficits manifesting during the disease, even in patients with probable MS, early MS and clinically isolated syndrome [8,9]. The cognitive functions mostly affected are attention, information processing speed, verbal memory, visuospatial skills, and executive functions [10,11]. CI impacts social, work, and day-to-day living [12], and it is related to lower quality of life [13,14]. Indeed, People with MS (PwMS) report lower chances for employment, a greater need for personal assistance, lower likelihood to engage in social activities [7], more difficulties in parenting [15] and greater impairment in some instrumental skills, such as driving [16,17]. Interestingly, the effects of pharmacological interventions are limited in treating cognitive symptoms in MS [18]. Consequently, there has been a growing focus on neuro-behavioural approaches as a means of managing cognitive dysfunction in individuals with MS [19]. The purpose of cognitive remediation techniques is mostly to strengthen residual capacities and promote the learning of new strategies, eventually leading to improved cognitive performance [3].
Behaviourally based cognitive remediation provides many advantages (i.e., non-invasive, no side effects typical of medications), however, the traditional approach requires the patient to travel to the clinic for repeated one-to-one sessions with the clinician for a set period of time, which may last several weeks. This may be a costly approach and not entirely feasible for some patients with MS [20,21]. Chiu and colleagues examined the specific barriers to accessing healthcare services in PwMS and found geographical location and transportation to be a frequent issue [22]. In summary, reported concerns in MS patients included: (a) living in remote and/or rural regions [23]; (b) suffering from fatigue, which may increase the burden of travel [23,24]; (c) inefficiency of existent transit services [24,25,26,27,28]; (d) needing to depend on family members or friends for assistance, thus, having to also rely on others' availability when scheduling appointments; (e) having to make appointments during working hours [23,24]. Home-based options for cognitive rehabilitation may offer a fundamental tool to overcome some of these issues, while potentially reducing health care costs by limiting in-person visits [29].
Naturally, telerehabilitation has received much attention in the context of the Covid-19 pandemic, for which many health care services were limited to emergency care to reduce risk of contagion and due to lockdowns in many countries [30]. This rendered even more evident the need for support services which could allow continuity of health care even when external circumstances may impede in-person medical assistance. Moreover, since the management of symptoms and impairment in MS often requires a comprehensive set of continuous treatments to promote patients’ well-being during the lifespan [22], it may be valuable to have the possibility to extend medical care to home-based services during the disease course, particularly in the context of prolonged treatment and monitoring of outpatients.
Owing to the continuous technological advancement, new forms of technology-based programmes have simultaneously gained interest as potential tools for rehabilitation in PwMS. Examples of such techniques are robotic training, computerised serious games, virtual reality systems and video games. Technology-based rehabilitation provides many advantages, such as: (a) tasks can be built to closely resemble activities of daily living, (b) frequent repetitive training can be easily implemented, (c) multisensory feedback can be available, (d) training difficulty can be adapted to patient's ongoing performance, (e) training can provide an engaging and motivating environment [31,32]. Moreover, many technology-based tools allow for home-based asynchronous rehabilitation, meaning patients can complete the training at home at any time [33]. This may be particularly advantageous in PwMS who struggle to schedule their appointments due to work and other commitments.
Given the growing interest in tele rehabilitative techniques based on the newest technologies, it remains to be established whether there is solid evidence regarding their efficacy in alleviating cognitive deficits in MS, and whether they can be a feasible option in these patients. Regarding the efficacy of cognitive rehabilitation in MS, different evidence-based reviews exist, including both evidence from studies investigating in-clinic rehabilitation and telerehabilitation [34,35,36,37,38]. Conflicting findings are not uncommon and limited evidence seems to be available regarding the efficacy of different rehabilitative techniques in MS. Nonetheless, promising results have also emerged in favour of cognitive remediation in these patients, suggesting more rigorous studies should be implemented to overcome methodological issues of previous research [35,36,37]. The aim of the current narrative review is to present and critically evaluate recent research findings uniquely about home-based digital cognitive rehabilitation in MS, in order to explore its feasibility and efficacy.
2. Materials and Methods
A literature search was conducted using the online database PubMed to gather relevant articles and information for this narrative review. Keywords utilised were "home-based rehabilitation" or “remote rehabilitation” or "telerehabilitation" and "cognition" or "cognitive rehabilitation" or "cognitive remediation" or "cognitive training" and "Multiple Sclerosis". Titles and abstracts of the resulting articles were inspected to narrow down the search for relevant studies. Only articles which strictly investigated the use of home-based digital rehabilitation for cognition were considered, thus, narrative or systematic reviews were not of interest, nor were studies looking at rehabilitation at home paired with "in-person" sessions or telerehabilitation paired with at-home neurostimulation. Studies had to be written in English and they had to be fairly recent. A time-window between January 2005 and September 2023 was set on PubMed.
3. Results
3.1. An overview of the studies on digital telerehabilitation
Thirteen studies investigating the use of computer-based software or programmes, applications, or video games for cognitive rehabilitation at home (digital telerehabilitation) were found and selected to be included in the current narrative review. The studies collected and reported below were published between the year 2007 and the year 2021. Table 1 provides an overview of the studies.
Table 1 presents an overview of the included studies on digital telerehabilitation. Each entry includes the first author's surname and year of publication, groups' size differentiating between intervention and control group, and the specific disease form represented. The study objectives, targeted cognitive domains, outcome measures, and the presence of follow-up assessments are also detailed. Entries are organised from the earliest to the most recent study for easy reference.
Most studies involved predominantly patients with RRMS (12), while some were also able to include patients with SPMS (7), and only a small number involved patients with PPMS (3). This is not surprising considering that RRMS is the most common form of the disease [51]. The majority of the research papers looked at the efficacy of home-based cognitive rehabilitation programmes in alleviating cognitive deficits (10), while a few had the goal to establish the feasibility of telerehabilitation (2). Only one study investigated two different training schedules, still looking at the efficacy of each type of training on cognition.
Two studies focused exclusively on the rehabilitation of working memory [40,46]. Vogt and colleagues used the computerised working memory training programme BrainStim [52], comparing two different training schedules (high intensity vs. low intensity) with no training. The programme involved three modules aimed at the remediation of spatial orientation, visual memory for objects and memory for numbers, and it was adaptive to the ongoing performance of participants [40]. Pedullà and colleagues, in a randomised controlled trial, opted for working memory training with the COGNI-track app, comparing adaptive vs. non-adaptive training. Patients in the adaptive training group performed exercises with increasing-decreasing levels of difficulty based on their performance, while patients in the non-adaptive training group performed exercises at a constant low-level of difficulty. Exercises included a visuospatial working memory task, an “operation” N-back task and a “dual” N-back task [46].
A double-blind, randomised controlled multicentre study focused on the rehabilitation of attention using the computerised Attention Processing Training (APT) programme, targeting different components of attention. To this purpose, Amato and colleagues recruited PwMS who showed impairment on at least two out of seven attention tests. Interestingly, the training exercises were organised in a hierarchical manner to train different components of attention. To provide an example of such training, participants were asked to identify target numbers or letters in the presence of distractor images and noises. An active control group undergoing sham computer training (reading and comprehension, description of pictures, etc.) was included for comparison [6].
The study by Shatil and colleagues opted for personalised cognitive training, which was based on the difficulties emerged from the neuropsychological examination conducted with the computer programme CogniFit Personal Coach (N-CPC). Essentially, the tasks used for cognitive training were determined by individual performance on the N-CPC, so that each person would have a specific individualised training regime. Participants were then allocated to intervention or control groups in a non-randomised fashion. Training was conducted with the same computerised training programme CogniFit Personal Coach used for the neuropsychological evaluation. The control group received no intervention [41].
Lastly, nine studies investigated multi-domain cognitive rehabilitation [39,42,43,44,45,47,48,49,50]. Hildebrandt and colleagues, in a single-blinded study, implemented a home-based software for rehabilitation. Specifically, they utilised a Compact Disk with memory and working memory tasks. The control group received no intervention. Patients in the training group had to memorise a list of words (within a semantic category) to be recalled after they had been distracted with a series of calculations. The software was adaptive and provided acoustic and visual feedback [39]. Charvet and colleagues conducted a double-blind randomised controlled pilot study in which they used the adaptive training web platform Lumosity (Lumos Labs, Inc. Lumosity. Lumos Labs, 2015) to train the most common areas of cognition affected in MS, including information processing speed and working memory. The control group was asked to complete sham activities through a commercially available programme called Hoyle puzzles and board games [32]. De Giglio and colleagues, in a single-blinded pilot study, tried to rehabilitate MS individuals with the videogame Dr Kawashima's Brain Training (DKBT, Nintendo, Kyoto, Japan) and a video game console, particularly aiming at the training of executive functions, working memory and processing speed. The training was made up of different games with specific goals. For example, the game calculation would have participants solve mathematical problems as fast as possible. The control group was a wait list group [43]. Hancock and colleagues implemented a double-blind, randomised control trial to collect pilot data on computerised cognitive training with the programmes Posit Science InSight and Brain Twister visual n-back. Training focused on processing speed and working memory with tasks that resembled games. The control group also received the same training but with constant low level of difficulty, while for the intervention group the training was continuously changing to be more and more challenging [44]. Campbell and colleagues, in an open label randomised controlled trial, looked at the efficacy of training through the computer software RehaCom. Training was adaptive and included modules aimed at the remediation of working memory, visuospatial memory and divided attention. Participants in the control group had to watch a series of natural history documentaries on DVDs [45]. Messinis and colleagues in a multicentre randomised controlled trial also used the computer-based software RehaCom. The training was adaptive and focused on attention, memory and executive functions. The control group took part in aspecific computer-based sham activities, such as reading and comprehension, shopping games, etc. [48]. Charvet and colleagues, in a double-blind randomised control trial, looked at the adaptive computer-based training programme Brain HQ developed by posit Science Corporation. The training targeted processing speed and information processing, attention, working memory and executive functions. Training was multimodal involving the use of both visual and auditory domains. The active control group used the software Hoyle Puzzle and Board Games (2008 version) to conduct a series of sham activities [47]. Vilou and colleagues, in a randomised controlled exploratory study, also used the Brain HQ website developed by Posit Science to train episodic memory, attention and processing speed. Every two weeks exercises were reviewed by an experimenter to adjust the level of difficulty of each task based on performance. There was no intervention described for the control condition [49]. Finally, Blair and colleagues, in a single-blinded pilot study, implemented the Cogmed Working Memory Training (CWMT) to mostly train working memory (both visuospatial working memory and verbal working memory) and attention. Training was adaptive. Each participant was assigned to a trained coach who would revise participants’ progress weekly. The control group was a waitlist group who underwent no intervention but received the usual clinical treatments [50].
3.2. Training frequency and intensity of digital telerehabilitation.
Overall, studies are somewhat consistent regarding the duration of a single session, with most opting for a training session of 30-45 minutes (11), while only two studies implemented one-hour-long sessions. Regarding the number of sessions per week, they ranged from 2 to 6. Looking at the total number of weeks of training, there was some variability, going from a minimum of 4 weeks to a maximum of 12 weeks of training. Finally, regarding the total hours of intervention, there was even more variability, with the lowest number being 8 hours of training in total, and the highest number being 60 hours of training (see Figure 1 for details).
Figure 1 Illustrates the training intensity across the 13 studies. All charts use horizontal bars to represent the different studies, and the length of each bar corresponds to the value of the variable for that study. The studies are ordered alphabetically for ease of reference.
3.3. Feasibility of digital telerehabilitation
Not all studies reported the feasibility of their target intervention, however, those that did, found decent compliance, with some variability. Shatil and colleagues explored unprompted compliance and found 57.6% of participants completed at least half of the prescribed sessions [40]. Charvet and colleagues defined compliance as the adherence to over 50% of target sessions and found 80% overall compliance [32]. De Giglio and colleagues defined compliance as the ratio between number of days in which participants performed the intervention and total planned days, and they found 96% compliance rates [43]. Hancock and colleagues found that 93.75% of patients completed at least 80% of prescribed sessions [44]. Campbell and colleagues measured adherence as the completion of at least 75% of target training sessions, and they found 88.90% of participants satisfying the goal adherence rate [45]. Pedullà and colleagues calculated adherence as the percentage of completed training sessions out of the total percentage of expected training sessions (100%) and found 87% overall adherence [46]. Charvet and colleagues measured compliance in two manners: achievement of at least 50% of target hours of programme use or having at least completed 50% of target weeks of intervention where there was at least 50% of compliance in a week. They then reported that 58,11% of PwMS in the intervention group completed at least 50% of target sessions [47]. Finally, Vilou and colleagues reported that about half of their participants (52.1%) were compliant with the study protocol, although they did not specify the metric used to evaluate compliance [49]. Five studies failed to report a measure of adherence in their result section [6,39,40,48,50]. In their discussion, Amato and colleagues reported that participants achieved high rates of compliance based on self-reports [6]. Vogt and colleagues also reported in the discussion section that almost 100% of participants finished all prescribed training sessions [40]. Finally, Messinis and colleagues reported, once more in the discussion, that high compliance rates may be inferred by the fact that no dropouts were registered in either the intervention or control groups [48].
3.4. Efficacy of digital telerehabilitation
Findings regarding the efficacy of telerehabilitation on ameliorating cognitive symptoms in MS are variable and dependent on the study in question. Overall, the results seem to suggest there is inconclusive evidence regarding the efficacy of home-based cognitive rehabilitation on neuropsychological measures, motor measures and Patient Reported Outcome Measures (PROMs). Only one recent study reported solely positive findings following an 8-week intervention with the software RehaCom in people with SPMS [48]. In this study, participants improved after training on all outcome measures compared to the control group. Replication will be key to make more definite conclusions. All the other studies (12) reported both positive and negative results (see Table 2 for details).
Table 2 shows the efficacy of digital training for each study. The table shows positive results on neuropsychological (NPS) measures in terms of improved performance after the training intervention compared to baseline. Improvements in performance from pre to post intervention on measures other than NPS, such as motor tests or PROMs are also shown. Whether improvements were also seen in the control group is specified in brackets. Negative results on NPS measures and other measures are also reported. The table also shows eventual lasting performance improvements at follow-up assessment. Effect sizes for positive results on NPS measures are also displayed. Entries are organised from the earliest to the most recent study for easy reference.
4. Discussion
The purpose of this narrative review was to explore the feasibility and efficacy of digital cognitive telerehabilitation in PwMS. Thirteen studies were presented, offering an understanding on the subject of interest. Regarding the feasibility of cognitive telerehabilitation, researchers commonly indicate adequate rates of adherence to at-home rehabilitation protocols [32,41,43,44,45,46,47,49]. However, it is worth noting that adherence metrics may vary, with most studies primarily providing the proportion of participants who adhered to a certain percentage of scheduled training [41,44,45,47,49], lacking more detailed insights into the specific duration (minutes/hours) of completed training in comparison to the intended training duration. Only one study reported the number of days in which participants performed the intervention [43] and only one study reported the percentage of completed training vs. the percentage of total training [46]. Five studies failed to report a measure of adherence in their result section [6,39,40,48,50]. Telerehabilitation interventions may depend heavily on individuals' adherence to the prescribed treatment, thus, for instance, only displaying the dropout rate of participants [48] may not be sufficient. Given that many factors can influence compliance, such as degree of satisfaction with the tele-protocol [53], vacation, technological issues, health issues, occupational issues, etc. [32], researchers should monitor session attendance, completion of assigned tasks and actual use of the provided digital tools. Improvements could also be made in reporting the number of participants who successfully complete the training, and further research is warranted to determine the threshold of completed training that signifies satisfactory compliance with the study procedures. Some existent software (e.g., RehaCom) are able to provide accurate measures of treatment adherence offering the actual minutes of completed training vs. total minutes of programmed training for each session. Such tools should be exploited to gain more accurate insights into the feasibility of home-based interventions. Moreover, assessing reasons for non-adherence or dropouts, if possible, may also provide valuable information regarding the practicality and acceptability of telerehabilitation in real-world settings. Surely, it is crucial to report objective measures of adherence to minimise reliance solely on self-reports provided by patients and caregivers, as these have been reported to overestimate adherence in the context of pharmacological treatment [54] and at-home exercise therapy [55].
Regarding the efficacy of the different rehabilitative techniques in improving cognitive performance in MS, there is more inconsistency in the findings. Variable results may be attributed, to some extent, to a wide range of methodological shortcomings across different studies. For example, many studies lacked double-blinding or failed to report whether the study was double-blind, single-blind or open label [39,40,41,43,45,46,49,50]. Lack of double-blinding remains an issue as it may lead to increased cognitive bias and unreliability of findings [56]. Lack of double-blinding is often a direct consequence of inadequate control groups. This is actually the case for various studies which did not involve active sham conditions and/or adopted wait-list control groups [39,40,41,43,49,50]. This is a concern, as lack of blinding may lead to an effect for the treatment group which is not a true effect per se but arises from different group expectations [57]. Lack of controlled randomisation, which is the gold standard in science [58] is also an issue, as a few studies failed to implement controlled randomisation [39,40,41]. Moreover, most studies lacked a follow up assessment, rendering impossible to know whether any eventual benefits of training were maintained over time [32,39,40,41,43,44,47,48,49]. On the positive note, a few studies tried to control for practice effects using alternate forms of neuropsychological testing, when possible [6,32,43,44], and adopting counterbalancing when administering the neuropsychological assessment [44]. It should be noted, however, that some studies have demonstrated how alternate test version may not always be strictly equivalent [59,60]. Therefore, guidelines for the use of alternate test version should be established, in order to further reduce heterogeneity across studies. Interestingly, one study tried to control for practice effects by subtracting the difference of mean scores at the neuropsychological tests in the control group (no active sham condition) with the difference of mean scores in the intervention group [49]. Furthermore, a few studies [32,39,46,47], also reported an intent-to-treat analysis which may be useful to help preserve randomisation, realistic evaluation of an intervention, and minimise the risk of biases due to non-compliance and dropouts [61]. Two studies also provided a Reliable Change Index (RCI) analysis [44,49], which is optimal as RCI is a statistical measure that helps determine whether there was a significant change in score at the individual score level on a particular assessment test. This is useful to determine whether the observed effect is actually a real change or whether it is due to random variability or measurement error [62].
As an additional limitation, studies on cognitive telerehabilitation in MS tend to have relatively small samples, which may reduce statistical power, robustness, and generalisability of the results [63]. Furthermore, there is the issue of heterogeneity among PwMS, as they may exhibit distinct cognitive profiles depending on the location of lesions within the CNS [10]. Consequently, grouping patients together based on diagnostic labels, could potentially overlook the variations in cognitive symptomatology. This challenge in MS research urges researchers to devise ideal strategies to effectively account for disease heterogeneity. Undoubtedly, controlling for baseline characteristics and cognitive profiles of participants is of utmost importance. A common approach is to ensure that the intervention and control groups have similar baseline characteristics through stratified controlled randomisation. If any discrepancies arise between the two groups, appropriate adjustment analysis should be employed to account for these differences [64]. Of greater significance, future studies should strive to overcome recruitment challenges by aiming to increase sample sizes. Multicentre studies will be key in this respect. This expansion would enable grouping analysis, which can aid in identifying disease subtypes based on baseline characteristics [65]. Indeed, a multicentric study on the effectiveness of cognitive rehabilitation and exercise in the clinic (N = 284) was recently published [66]. Similar efforts should be encouraged in the framework of telerehabilitation, and indeed one could argue that telerehabilitation may afford a higher degree of standardisation across centres, thus facilitating multicentric and decentralised trials. Ultimately, such identification may facilitate predictions regarding which group of patients may be more likely to respond positively to a certain treatment. Similar work has been done to explore whether medications are more effective in some MS patients compared to others [67]. Moreover, cluster analysis can provide support in this context, as it provides a data-driven approach to classify patients into homogeneous groups based on specific characteristics, allowing distinct patterns to be identified. This approach facilitates individualised adaptation of cognitive rehabilitation interventions to meet individual needs. While cluster analysis has already been successfully applied in some neurological disorders within the context of cognitive rehabilitation [68,69], there is still room for significant advancement in the field of MS and in the application of digital technologies. The possibility to extend this methodology to the cognitive field may help shed more light into the effectiveness of cognitive rehabilitation. In this regard, a multicentre cross-sectional study applied latent profile analysis to cognitive tests to identify cognitive phenotypes (N = 1212). Cognitive phenotypes can represent a more meaningful measure of the cognitive status of PwMS and can help tailor cognitive rehabilitation strategies [70]. Another approach, instead, may be personalised rehabilitative intervention based on individual deficits emerged by the neuropsychological assessment. By identifying and targeting specific deficits that a person has, rehabilitation efforts can be tailored to their unique needs, hypothetically maximising the potential for improvement. One of the studies included in this review looked at personalised treatment regimens with the use of an app and found some improvements with moderate to large effects [41]. More research will be needed to also explore the possibility of customised treatment.
The variability in findings within the field of tele-rehabilitative methods could also be partly attributed to the heterogeneity of these techniques as well as the heterogeneity of inclusion criteria employed in studies. For instance, some studies recruited participants based on self-reported cognitive deficits [32,40,44] rather than objectively measured cognitive impairment using neuropsychological tests, or individuals with intact cognitive performance [43]. While this approach may be driven by the primary focus on assessing the feasibility of a specific protocol, it becomes crucial, particularly when presenting the efficacy of a telerehabilitation intervention, to recognise that individuals with cognitive impairment could potentially respond distinctively compared to those with intact cognitive abilities. Interestingly, when Hancock and colleagues specifically examined subjects with cognitive impairment on the Symbol-Digit Modalities Test (SDMT), excluding cognitively intact individuals, the treatment effect became statistically non-significant [44]. This may suggest that cognitively impaired individuals may respond less to cognitive training compared to those who are cognitively intact, possibly due to lower brain reserve and/or cognitive reserve. In this regard, however, there are conflicting results. The study performed by Whitlock and colleagues on a sample of 39 older adults aged 60–77 suggests that older adults with lower cognitive functioning may stand to benefit more from cognitive training [71]. Nevertheless, not screening for cognitive impairment may also pose an ethical concern as it may result in 'treating' cognitively intact participants who might still benefit from cognitive boosting interventions but with limited clinical impact. Emphasising the prioritisation of enhancing clinical relevance in research is crucial, considering the importance of generalising and translating findings to real-world situations. Indeed, it is crucial to examine whether study results have a substantial impact that holds significance for patients in their daily lives. While self-report questionnaires can serve as an initial measurement of perceived improvements in functioning, exploring methods to objectively assess meaningful functional changes is an intriguing avenue to explore.
Selection of the appropriate outcome measures can also be challenging. A measure should be sensitive to the cognitive domain of interest and relevant for the intervention being evaluated. For instance, Campbell and colleagues used the subtests from the Brief International Cognitive Assessment for MS (BICAMS) to measure cognitive improvement after rehabilitation with RehaCom software modules targeting working memory, visuospatial memory and divided attention [45]. BICAMS subtests are the SDMT (information processing speed and sustained attention), the California Verbal Learning Test-II (CVLT-II; verbal learning and memory) and the Brief Visuospatial Memory Test Revised (BVMT-R; visuospatial learning and memory) [72]. Although working memory refers to a set of cognitive systems that are considered essential for retaining and manipulating information while engaging in complex tasks such as reasoning, comprehension, and learning [73], thus it is likely involved in various neuropsychological tests, it is usually measured with tests that require the active maintenance and manipulation of information [74]. As a result, perhaps, it would have been interesting to also include measures more sensitive than BICAMS to a possible improvement in working memory following rehabilitation. Similarly, for instance, it would have also been interesting to include a verbal memory module as cognitive training. Indeed, no significant improvement in BICAMS test CVLT-II was reported after cognitive training. Since no verbal memory training was involved in the intervention, this finding is perhaps not surprising. Interestingly, the authors showed that there was a functional imaging difference between control and intervention groups, with the intervention group showing more activation in prefrontal cortex and right temporoparietal regions in response to working memory tasks (in functional Magnetic Resonance Imaging - fMRI), which, however, was not reflected in the scores obtained by the BICAMS tests. Again, this is suggestive that BICAMS neuropsychological subtests may not be sensitive enough to working memory changes [45]. This particular case serves as an illustrative example highlighting the challenge of selecting relevant outcome measures. When evaluating the cognitive gains resulting from an intervention, it becomes crucial to employ sensitive measures of change. Without such appropriate measures, the interpretation of cognitive improvements can be challenging. Some researchers, for instance, also reported a composite score of cognition derived from an average of the different neuropsychological tests used [32,47]. Combining multiple measures into a composite score can provide a more comprehensive assessment of cognitive function and it may increase the statistical power to detect treatment effects when interventions are designed to target multiple cognitive domains. Conversely, this approach could lead to loss of statistical power when assessing the efficacy of domain-specific interventions. Therefore, it remains important to carefully select outcome measures and apply appropriate statistical analyses to create and interpret composite scores.
A further challenge when designing telerehabilitation experiments lies in the decision of treatment intensity and duration. Only one study included in the review compared different training schedules, with no significant differences in pre-post intervention scores at neuropsychological testing, concluding that the effects of training were independent of training intensity. The only difference found was in the CORSI block backwards, for which there was an improvement only in the distributed training group [40]. When qualitatively inspecting the apparent relationship between training results and the overall duration of training, it remains unclear what the optimal intensity and duration of training are [45]. Moreover, in some research scenarios, it is possible that the duration of the intervention may have been too short to allow significant results to emerge in the cognitive measures under investigation. Certainly, further investigations are required to provide clearer insights into the ideal schedule of training for optimal efficacy.
In conclusion, it is imperative to address the methodological concerns discussed above to uphold the validity, reliability, and generalizability of research findings related to cognitive telerehabilitation in MS. Most notably, it is essential to a) pursue standardisation of intervention protocols in cognitive telerehabilitation to minimise study variability and facilitate comparison of results; b) favour the adoption of double-blind randomised controlled trials to achieve a high degree of reliability in assessments, and encourage the use of objective and correct cognitive screening measures; c) broaden and stratify the study sample by promoting multicentre studies to ensure greater representativeness of the study population; and (d) implement long-term follow-up to adequately evaluate the effectiveness of the intervention over time. The adoption of these proposed guidelines will be able to contribute significantly to the improvement of quality of scientific research in the context of cognitive telerehabilitation. Furthermore, ongoing and relentless technological research will enable the development of ever more cutting-edge digital solutions for cognitive telerehabilitation in MS, ensuring highly personalised and more accessible advanced treatment options to effectively manage cognitive challenges and improve quality of life.
5. Conclusions
The current literature review presented recent findings on the feasibility and efficacy of cognitive telerehabilitation using digital platforms in MS. While the feasibility of telerehabilitation for cognition in MS has shown some positive results, and there seems to be promising evidence regarding its efficacy, several methodological limitations and heterogeneity in study designs have been identified as potential reasons for inconclusive findings. Future research should focus on addressing these challenges, including larger sample sizes, standardised outcome measures, and consideration of disease heterogeneity. Additionally, efforts should be made to optimise the intensity and duration of telerehabilitation interventions. By addressing these factors, we can enhance the validity, reliability, and generalisability of research findings, ultimately paving the way for more effective and accessible cognitive rehabilitation for individuals living with MS.
Author Contributions
Conceptualization, A.B. and L.L.; methodology, A.B.; investigation, A.B.; data curation, A.B.; writing—original draft preparation, A.B.; writing—review and editing, A.B., E.M., M.D., M.T., G.G., G.C. and L.L.; visualization, A.B.; supervision, L.L. and G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
G. Comi has received consulting and speaking fees from Novartis, Sanofi Genzyme, Genzyme Corporation, Merck KGgA, Merck Serono SpA, Celgene Group, Bristol-Myers Squibb, Janssen, F. Hoffman-La Roche, and Almirall SpA. L. Leocani received research support from Novartis, Almirall, Biogen, and Merck and consultancy or speaker fees from Novartis, Almirall, Biogen, Merck, Janssen-Cilag, Bristol-Myers Squibb, and Roche. All other authors have no conflicts of interest to declare.
References
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J 2017, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Stadelmann, C.; Wegner, C.; Brück, W. Inflammation, Demyelination, and Degeneration — Recent Insights from MS Pathology. Biochimica et Biophysica Acta (BBA) - Molecular Basis of Disease 2011, 1812, 275–282. [Google Scholar] [CrossRef]
- Maggio, M.G.; Russo, M.; Cuzzola, M.F.; Destro, M.; La Rosa, G.; Molonia, F.; Bramanti, P.; Lombardo, G.; De Luca, R.; Calabrò, R.S. Virtual Reality in Multiple Sclerosis Rehabilitation: A Review on Cognitive and Motor Outcomes. Journal of Clinical Neuroscience 2019, 65, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising Prevalence of Multiple Sclerosis Worldwide: Insights from the Atlas of MS, Third Edition. Mult Scler 2020, 26, 1816–1821. [Google Scholar] [CrossRef]
- Lucchinetti, C.; Brück, W.; Parisi, J.; Scheithauer, B.; Rodriguez, M.; Lassmann, H. Heterogeneity of Multiple Sclerosis Lesions: Implications for the Pathogenesis of Demyelination. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society 2000, 47, 707–717. [Google Scholar] [CrossRef]
- Amato, M.; Goretti, B.; Viterbo, R.; Portaccio, E.; Niccolai, C.; Hakiki, B.; Iaffaldano, P.; Trojano, M. Computer-Assisted Rehabilitation of Attention in Patients with Multiple Sclerosis: Results of a Randomized, Double-Blind Trial. Mult Scler 2014, 20, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.M.; Leo, G.J.; Ellington, L.; Nauertz, T.; Bernardin, L.; Unverzagt, F. Cognitive Dysfunction in Multiple Sclerosis.: II. Impact on Employment and Social Functioning. Neurology 1991, 41, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Achiron, A.; Barak, Y. Cognitive Impairment in Probable Multiple Sclerosis. Journal of Neurology, Neurosurgery & Psychiatry 2003, 74, 443–446. [Google Scholar] [CrossRef]
- Zipoli, V.; Goretti, B.; Hakiki, B.; Siracusa, G.; Sorbi, S.; Portaccio, E.; Amato, M.P. Cognitive Impairment Predicts Conversion to Multiple Sclerosis in Clinically Isolated Syndromes. Mult Scler 2010, 16, 62–67. [Google Scholar] [CrossRef]
- Chiaravalloti, N.D.; DeLuca, J. Cognitive Impairment in Multiple Sclerosis. The Lancet Neurology 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Langdon, D.W. Cognition in Multiple Sclerosis. Current Opinion in Neurology 2011, 24, 244. [Google Scholar] [CrossRef]
- Amato, M.P.; Zipoli, V.; Portaccio, E. Cognitive Changes in Multiple Sclerosis. Expert Review of Neurotherapeutics 2008, 8, 1585–1596. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Benito-León, J.; González, J.-M.M.; Rivera-Navarro, J. Quality of Life and Its Assessment in Multiple Sclerosis: Integrating Physical and Psychological Components of Wellbeing. The Lancet Neurology 2005, 4, 556–566. [Google Scholar] [CrossRef]
- Ozakbas, S.; Cagiran, I.; Ormeci, B.; Idiman, E. Correlations between Multiple Sclerosis Functional Composite, Expanded Disability Status Scale and Health-Related Quality of Life during and after Treatment of Relapses in Patients with Multiple Sclerosis. Journal of the Neurological Sciences 2004, 218, 3–7. [Google Scholar] [CrossRef]
- Shevil, E.; Finlayson, M. Perceptions of Persons with Multiple Sclerosis on Cognitive Changes and Their Impact on Daily Life. Disability and Rehabilitation 2006, 28, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, M.T.; Garay, E.; DeLuca, J. The Influence of Cognitive Impairment on Driving Performance in Multiple Sclerosis. Neurology 2001, 56, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, M.T.; Garay, E.; Millis, S.R.; DeLuca, J. Motor Vehicle Crashes and Violations among Drivers with Multiple Sclerosis. Archives of Physical Medicine and Rehabilitation 2002, 83, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Langdon, D.; Montalban, X.; Benedict, R.H.B.; DeLuca, J.; Krupp, L.B.; Thompson, A.J.; Comi, G. Treatment of Cognitive Impairment in Multiple Sclerosis: Position Paper. J Neurol 2013, 260, 1452–1468. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; DeLuca, J. Will Behavioral Treatments for Cognitive Impairment in Multiple Sclerosis Become Standards-of-Care? International Journal of Psychophysiology 2020, 154, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; Moore, N.B.; Nikelshpur, O.M.; DeLuca, J. An RCT to Treat Learning Impairment in Multiple Sclerosis: The MEMREHAB Trial. Neurology 2013, 81, 2066–2072. [Google Scholar] [CrossRef]
- Filippi, M.; Riccitelli, G.; Mattioli, F.; Capra, R.; Stampatori, C.; Pagani, E.; Valsasina, P.; Copetti, M.; Falini, A.; Comi, G.; et al. Multiple Sclerosis: Effects of Cognitive Rehabilitation on Structural and Functional MR Imaging Measures—An Explorative Study. Radiology 2012, 262, 932–940. [Google Scholar] [CrossRef]
- Chiu, C.; Bishop, M.; Pionke, J.J.; Strauser, D.; Santens, R.L. Barriers to the Accessibility and Continuity of Health-Care Services in People with Multiple Sclerosis: A Literature Review. International Journal of MS Care 2017, 19, 313–321. [Google Scholar] [CrossRef]
- Buchanan, R.J.; Stuifbergen, A.; Chakravorty, B.J.; Wang, S.; Zhu, L.; Kim, M. Urban/Rural Differences in Access and Barriers to Health Carefor People with Multiple Sclerosis. Journal of Health and Human Services Administration 2006, 29, 360–375. [Google Scholar]
- Scheer, J.; Kroll, T.; Neri, M.T.; Beatty, P. Access Barriers for Persons with Disabilities: The Consumer’s Perspective. Journal of Disability Policy Studies 2003, 13, 221–230. [Google Scholar] [CrossRef]
- Minden, S.L.; Frankel, D.; Hadden, L.; Hoaglin, D.C. Access to Health Care for People with Multiple Sclerosis. Mult Scler 2007, 13, 547–558. [Google Scholar] [CrossRef]
- McDoom, M.M.; Koppelman, E.; Drainoni, M.-L. Barriers to Accessible Health Care for Medicaid Eligible People with Disabilities: A Comparative Analysis. Journal of Disability Policy Studies 2014, 25, 154–163. [Google Scholar] [CrossRef]
- Kroll, T.; Jones, G.C.; Kehn, M.; Neri, M.T. Barriers and Strategies Affecting the Utilisation of Primary Preventive Services for People with Physical Disabilities: A Qualitative Inquiry. Health & social care in the community 2006, 14, 284–293. [Google Scholar] [CrossRef]
- Morrison, E.H.; George, V.; Mosqueda, L. Primary Care for Adults with Physical Disabilities: Perceptions from Consumer and Provider Focus Groups. Family medicine 2008, 40, 645–651. [Google Scholar] [PubMed]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabilitation and Assistive Technologies 2017, 4, e7511. [Google Scholar] [CrossRef]
- Grippo, A.; Assenza, G.; Scarpino, M.; Broglia, L.; Cilea, R.; Galimberti, C.A.; Lanzo, G.; Michelucci, R.; Tassi, L.; Vergari, M.; et al. Electroencephalography during SARS-CoV-2 Outbreak: Practical Recommendations from the Task Force of the Italian Society of Neurophysiology (SINC), the Italian League Against Epilepsy (LICE), and the Italian Association of Neurophysiology Technologists (AITN). Neurol Sci 2020, 41, 2345–2351. [Google Scholar] [CrossRef]
- Karakas, H.; Seebacher, B.; Kahraman, T. Technology-Based Rehabilitation in People with Multiple Sclerosis: A Narrative Review. JOURNAL OF MULTIPLE SCLEROSIS RESEARCH 2021, 1, 54–68. [Google Scholar] [CrossRef]
- Charvet, L.; Shaw, M.; Haider, L.; Melville, P.; Krupp, L. Remotely-Delivered Cognitive Remediation in Multiple Sclerosis (MS): Protocol and Results from a Pilot Study. Multiple Sclerosis Journal - Experimental, Translational and Clinical 2015, 1, 2055217315609629. [Google Scholar] [CrossRef] [PubMed]
- Cacciante, L.; Pietà, C. della; Rutkowski, S.; Cieślik, B.; Szczepańska-Gieracha, J.; Agostini, M.; Kiper, P. Cognitive Telerehabilitation in Neurological Patients: Systematic Review and Meta-Analysis. Neurol Sci 2022, 43, 847–862. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, A.R.; Chiaravalloti, N.; Goverover, Y.; DeLuca, J. Evidenced-Based Cognitive Rehabilitation for Persons With Multiple Sclerosis: A Review of the Literature. Archives of Physical Medicine and Rehabilitation 2008, 89, 761–769. [Google Scholar] [CrossRef]
- Mitolo, M.; Venneri, A.; Wilkinson, I.D.; Sharrack, B. Cognitive Rehabilitation in Multiple Sclerosis: A Systematic Review. Journal of the Neurological Sciences 2015, 354, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Goverover, Y.; Chiaravalloti, N.D.; O’Brien, A.R.; DeLuca, J. Evidenced-Based Cognitive Rehabilitation for Persons With Multiple Sclerosis: An Updated Review of the Literature From 2007 to 2016. Archives of Physical Medicine and Rehabilitation 2018, 99, 390–407. [Google Scholar] [CrossRef] [PubMed]
- Brochet, B. Cognitive Rehabilitation in Multiple Sclerosis in the Period from 2013 and 2021: A Narrative Review. Brain Sciences 2022, 12, 55. [Google Scholar] [CrossRef]
- Nair, R. das; Martin, K.-J.; Lincoln, N.B. Memory Rehabilitation for People with Multiple Sclerosis. Cochrane Database of Systematic Reviews 2016. [Google Scholar] [CrossRef]
- Hildebrandt, H.; Lanz, M.; Hahn, H.K.; Hoffmann, E.; Schwarze, B.; Schwendemann, G.; Kraus, J.A. Cognitive Training in MS: Effects and Relation to Brain Atrophy. Restorative Neurology and Neuroscience 2007, 25, 33–43. [Google Scholar]
- Vogt, A.; Kappos, L.; Calabrese, P.; Stöcklin, M.; Gschwind, L.; Opwis, K.; Penner, I.-K. Working Memory Training in Patients with Multiple Sclerosis – Comparison of Two Different Training Schedules. Restorative Neurology and Neuroscience 2009, 27, 225–235. [Google Scholar] [CrossRef]
- Shatil, E.; Metzer, A.; Horvitz, O.; Miller, A. Home-Based Personalized Cognitive Training in MS Patients: A Study of Adherence and Cognitive Performance. NeuroRehabilitation 2010, 26, 143–153. [Google Scholar] [CrossRef]
- Charvet, L.; Shaw, M.; Haider, L.; Melville, P.; Krupp, L. Remotely-Delivered Cognitive Remediation in Multiple Sclerosis (MS): Protocol and Results from a Pilot Study. Multiple Sclerosis Journal - Experimental, Translational and Clinical 2015, 1, 2055217315609629. [Google Scholar] [CrossRef] [PubMed]
- De Giglio, L.; De Luca, F.; Prosperini, L.; Borriello, G.; Bianchi, V.; Pantano, P.; Pozzilli, C. A Low-Cost Cognitive Rehabilitation With a Commercial Video Game Improves Sustained Attention and Executive Functions in Multiple Sclerosis: A Pilot Study. Neurorehabil Neural Repair 2015, 29, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Hancock, L.M.; Bruce, J.M.; Bruce, A.S.; Lynch, S.G. Processing Speed and Working Memory Training in Multiple Sclerosis: A Double-Blind Randomized Controlled Pilot Study. Journal of Clinical and Experimental Neuropsychology 2015, 37, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.; Langdon, D.; Cercignani, M.; Rashid, W. A Randomised Controlled Trial of Efficacy of Cognitive Rehabilitation in Multiple Sclerosis: A Cognitive, Behavioural, and MRI Study. Neural plasticity 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Pedullà, L.; Brichetto, G.; Tacchino, A.; Vassallo, C.; Zaratin, P.; Battaglia, M.A.; Bonzano, L.; Bove, M. Adaptive vs. Non-Adaptive Cognitive Training by Means of a Personalized App: A Randomized Trial in People with Multiple Sclerosis. Journal of NeuroEngineering and Rehabilitation 2016, 13, 88. [Google Scholar] [CrossRef]
- Charvet, L.E.; Yang, J.; Shaw, M.T.; Sherman, K.; Haider, L.; Xu, J.; Krupp, L.B. Cognitive Function in Multiple Sclerosis Improves with Telerehabilitation: Results from a Randomized Controlled Trial. PLOS ONE 2017, 12, e0177177. [Google Scholar] [CrossRef]
- Messinis, L.; Kosmidis, M.H.; Nasios, G.; Konitsiotis, S.; Ntoskou, A.; Bakirtzis, C.; Grigoriadis, N.; Patrikelis, P.; Panagiotopoulos, E.; Gourzis, P.; et al. Do Secondary Progressive Multiple Sclerosis Patients Benefit from Computer- Based Cognitive Neurorehabilitation? A Randomized Sham Controlled Trial. Multiple Sclerosis and Related Disorders 2020, 39, 101932. [Google Scholar] [CrossRef]
- Vilou, I.; Bakirtzis, C.; Artemiadis, A.; Ioannidis, P.; Papadimitriou, M.; Konstantinopoulou, E.; Aretouli, E.; Messinis, L.; Nasios, G.; Dardiotis, E.; et al. Computerized Cognitive Rehabilitation for Treatment of Cognitive Impairment in Multiple Sclerosis: An Explorative Study. Journal of integrative neuroscience 2020, 19, 341–347. [Google Scholar] [CrossRef]
- Blair, M.; Goveas, D.; Safi, A.; Marshall, C.; Rosehart, H.; Orenczuk, S.; Morrow, S.A. Does Cognitive Training Improve Attention/Working Memory in Persons with MS? A Pilot Study Using the Cogmed Working Memory Training Program. Multiple Sclerosis and Related Disorders 2021, 49, 102770. [Google Scholar] [CrossRef]
- Wallin, M.T.; Culpepper, W.J.; Campbell, J.D.; Nelson, L.M.; Langer-Gould, A.; Marrie, R.A.; Cutter, G.R.; Kaye, W.E.; Wagner, L.; Tremlett, H. The Prevalence of MS in the United States: A Population-Based Estimate Using Health Claims Data. Neurology 2019, 92, e1029–e1040. [Google Scholar] [CrossRef] [PubMed]
- Penner, I.; Kobel, M.; Opwis, K. BrainStim–A Recently Developed Tool to Train Different Aspects of Working Memory. In Proceedings of the Proceedings of the INS/GNP Conference; 2006; pp. 17–18. [Google Scholar]
- Shaw, M.T.; Best, P.; Frontario, A.; Charvet, L.E. Telerehabilitation Benefits Patients with Multiple Sclerosis in an Urban Setting. Journal of telemedicine and telecare 2021, 27, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Stirratt, M.J.; Dunbar-Jacob, J.; Crane, H.M.; Simoni, J.M.; Czajkowski, S.; Hilliard, M.E.; Aikens, J.E.; Hunter, C.M.; Velligan, D.I.; Huntley, K. Self-Report Measures of Medication Adherence Behavior: Recommendations on Optimal Use. Translational behavioral medicine 2015, 5, 470–482. [Google Scholar] [CrossRef]
- Nicolson, P.J.; Hinman, R.S.; Wrigley, T.V.; Stratford, P.W.; Bennell, K.L. Self-Reported Home Exercise Adherence: A Validity and Reliability Study Using Concealed Accelerometers. journal of orthopaedic & sports physical therapy 2018, 48, 943–950. [Google Scholar] [CrossRef]
- Furberg, C.D.; Soliman, E.Z. Double-Blindness Protects Scientific Validity. Journal of Thrombosis and Haemostasis 2008, 6, 230–231. [Google Scholar] [CrossRef] [PubMed]
- Boot, W.R.; Simons, D.J.; Stothart, C.; Stutts, C. The Pervasive Problem with Placebos in Psychology: Why Active Control Groups Are Not Sufficient to Rule out Placebo Effects. Perspectives on psychological science 2013, 8, 445–454. [Google Scholar] [CrossRef]
- Hariton, E.; Locascio, J.J. Randomised Controlled Trials—the Gold Standard for Effectiveness Research. BJOG 2018, 125, 1716. [Google Scholar] [CrossRef]
- Cai, Y.; Yang, T.; Yu, X.; Han, X.; Chen, G.; Shi, C. The Alternate-Form Reliability Study of Six Variants of the Brief Visual-Spatial Memory Test-Revised and the Hopkins Verbal Learning Test-Revised. Frontiers in Public Health 2023, 11, 1096397. [Google Scholar] [CrossRef]
- Siciliano, M.; Chiorri, C.; Passaniti, C.; Sant’Elia, V.; Trojano, L.; Santangelo, G. Comparison of Alternate and Original Forms of the Montreal Cognitive Assessment (MoCA): An Italian Normative Study. Neurological Sciences 2019, 40, 691–702. [Google Scholar] [CrossRef]
- McCoy, C.E. Understanding the Intention-to-Treat Principle in Randomized Controlled Trials. West J Emerg Med 2017, 18, 1075–1078. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.S.; Truax, P. Clinical Significance: A Statistical Approach to Defining Meaningful Change in Psychotherapy Research. J Consult Clin Psychol 1991, 59, 12–19. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic press, 2013; ISBN 1-4832-7648-1. [Google Scholar] [CrossRef]
- Lin, Y.; Zhu, M.; Su, Z. The Pursuit of Balance: An Overview of Covariate-Adaptive Randomization Techniques in Clinical Trials. Contemporary Clinical Trials 2015, 45, 21–25. [Google Scholar] [CrossRef]
- van Rooden, S.M.; Heiser, W.J.; Kok, J.N.; Verbaan, D.; van Hilten, J.J.; Marinus, J. The Identification of Parkinson’s Disease Subtypes Using Cluster Analysis: A Systematic Review. Movement Disorders 2010, 25, 969–978. [Google Scholar] [CrossRef]
- Feinstein, A.; Amato, M.P.; Brichetto, G.; Chataway, J.; Chiaravalloti, N.D.; Cutter, G.; Dalgas, U.; DeLuca, J.; Farrell, R.; Feys, P. Cognitive Rehabilitation and Aerobic Exercise for Cognitive Impairment in People with Progressive Multiple Sclerosis (CogEx): A Randomised, Blinded, Sham-Controlled Trial. The Lancet Neurology 2023, 22, 912–924. [Google Scholar] [CrossRef]
- Falet, J.-P.R.; Durso-Finley, J.; Nichyporuk, B.; Schroeter, J.; Bovis, F.; Sormani, M.-P.; Precup, D.; Arbel, T.; Arnold, D.L. Estimating Individual Treatment Effect on Disability Progression in Multiple Sclerosis Using Deep Learning. Nature communications 2022, 13, 5645. [Google Scholar] [CrossRef]
- García-Rudolph, A.; García-Molina, A.; Opisso, E.; Tormos, J.M.; Madai, V.I.; Frey, D.; Bernabeu, M. Neuropsychological Assessments of Patients With Acquired Brain Injury: A Cluster Analysis Approach to Address Heterogeneity in Web-Based Cognitive Rehabilitation. Front. Neurol. 2021, 12, 701946. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Rudolph, A.; Garcia-Molina, A.; Opisso, E.; Tormos Muñoz, J. Personalized Web-Based Cognitive Rehabilitation Treatments for Patients with Traumatic Brain Injury: Cluster Analysis. JMIR Medical Informatics 2020, 8, e16077. [Google Scholar] [CrossRef] [PubMed]
- De Meo, E.; Portaccio, E.; Giorgio, A.; Ruano, L.; Goretti, B.; Niccolai, C.; Patti, F.; Chisari, C.G.; Gallo, P.; Grossi, P. Identifying the Distinct Cognitive Phenotypes in Multiple Sclerosis. JAMA neurology 2021, 78, 414–425. [Google Scholar] [CrossRef]
- Whitlock, L.A.; McLaughlin, A.C.; Allaire, J.C. Individual Differences in Response to Cognitive Training: Using a Multi-Modal, Attentionally Demanding Game-Based Intervention for Older Adults. Computers in human behavior 2012, 28, 1091–1096. [Google Scholar] [CrossRef]
- Benedict, R.H.; Amato, M.P.; Boringa, J.; Brochet, B.; Foley, F.; Fredrikson, S.; Hamalainen, P.; Hartung, H.; Krupp, L.; Penner, I. Brief International Cognitive Assessment for MS (BICAMS): International Standards for Validation. BMC neurology 2012, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A. Working Memory. Current biology 2010, 20, R136–R140. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A. Working Memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Intensity of digital telerehabilitation.
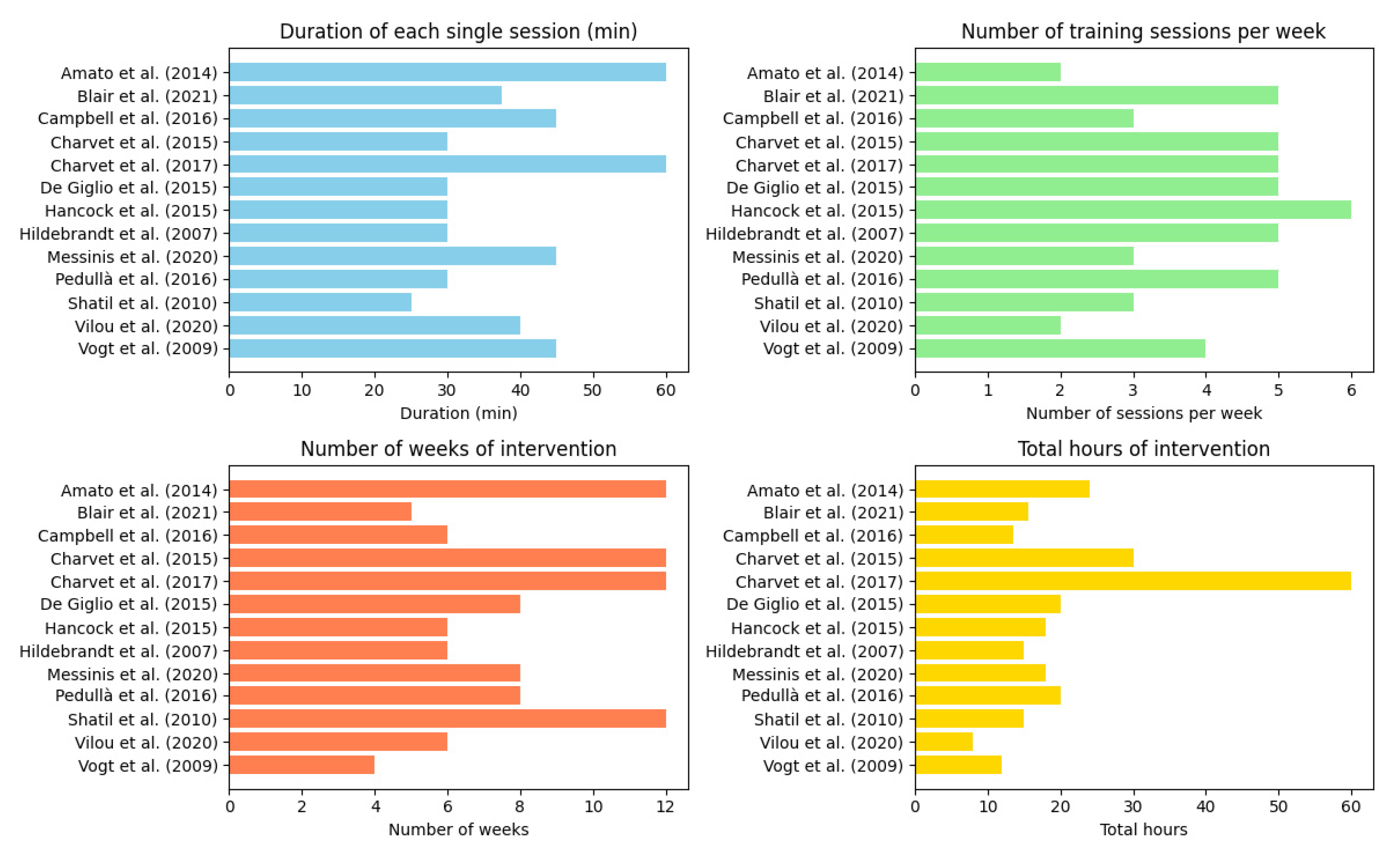

Table 1.
Included studies on digital telerehabilitation.
| Study | Groups (N) | Disease Type | Study Aim | Cognitive Domains Targeted | Outcome Measures | Follow-up Assessment |
|---|---|---|---|---|---|---|
|
Hildebrandt et al. (2007) [39] |
IG (17) CG (25) |
RRMS (42) | Explore efficacy of remote cognitive training | Memory, working memory | Disability, motor, cognition, mood, fatigue, quality of life |
No |
|
Vogt et al. (2009) [40] |
IG intensive training (15) IG distributed training (15) CG (15) |
RRMS (36) SPMS (8) Chronic-progressive MS (1) |
Evaluate two different remote training schedules |
Working memory | Cognition, fatigue, mood, quality of life |
No |
|
Shatil et al. (2010) [41] |
IG (59) CG (48) |
RRMS (107) | Explore unprompted adherence to personalised remote cognitive training | Dependent on individual performance on neuropsychological examination | Cognition, mood, disability, fatigue | No |
|
Amato et al. (2014) [6] |
IG (55) CG (33) |
RRMS (88) | Explore efficacy of remote cognitive training | Attention | Cognition, depression, fatigue, everyday activities | 6 months |
|
Charvet et al. (2015) [42] |
IG (11) CG (9) |
RRMS (20) | Explore feasibility of remote cognitive training | Processing speed, memory | Cognition, motor | No |
|
De Giglio et al. (2015) [43] |
IG (18) CG (17) |
RRMS (35) | Explore efficacy of remote cognitive training | Attention, processing speed, working memory | Cognition, fatigue, quality of life | No |
|
Hancock et al. (2015) [44] |
IG (15) CG (15) |
RRMS (21) SPMS (5) PPMS (4) |
Explore efficacy of remote cognitive training | Processing speed, working memory | Cognition, mood, fatigue, quality of life | No |
|
Campbell et al. (2016) [45] |
IG (19) CG (19) |
RRMS (27) SPMS (11) |
Explore efficacy of remote cognitive training |
Working memory, visuospatial memory, divided attention | Cognition, quality of life, mood, patient reported chronic illness management, self-efficacy, self-reported cognition, fatigue | 4.5 months |
|
Pedullà et al. (2016) [46] |
IG (14) CG (14) |
RRMS (17) SPMS (11) |
Explore efficacy of remote cognitive training | Working memory | Cognition | 6 months |
|
Charvet et al. (2017) [47] |
IG (74) CG (61) |
RRMS (89) SPMS (35) PPMS (7) |
Explore efficacy of remote cognitive training |
Processing speed, attention, working memory, executive functions | Cognition | No |
|
Messinis et al. (2020) [48] |
IG (19) CG (17) |
SPMS (36) | Explore efficacy of remote cognitive training |
Attention, divided attention, verbal memory, visuospatial memory, executive functions | Cognition, fatigue, mood, quality of life | No |
|
Vilou et al. (2020) [49] |
IG (23) CG (24) |
RRMS (47) | Explore efficacy of remote cognitive training | Episodic memory, attention, processing speed | Cognition | No |
|
Blair et al. (2021) [50] |
IG (15) CG (15) |
RRMS (17) SPMS (12) PPMS (1) |
Explore efficacy of remote cognitive training |
Attention, working memory | Cognition, self-reported cognitive function, mood, pain, quality of life | 6 months |
* Abbreviations: CG, Control Group; IG, Intervention Group; PPMS, Primary Progressive Multiple Sclerosis; RRMS, Relapsing Remitting Multiple Sclerosis; SPMS, Secondary Progressive Multiple Sclerosis..
Table 2.
Efficacy of digital telerehabilitation.
| Study |
Positive results on NPS measures |
Positive results on other measures | Negative results on NPS measures | Negative results on other measures | Positive results maintained at follow-up | Effect sizes for (immediate) positive results |
|---|---|---|---|---|---|---|
|
Hildebrandt et al. (2007) [39] |
CVLT-II (learning trials & long delay free recall); PASAT |
NHPT | CVLT-II (short delay free recall, cued recall & long delay cued recall); Object alternation RTs & errors; Alertness with & without cueing | EDSS; Timed walked test; SF-12 bodily & mental scores; BDI; FSS | No follow up assessment performed | Not reported |
|
Vogt et al. (2009) [40] |
Corsi blocks backward (only in the distributed training group); Digit span backward; 2-back task omissions; PASAT; FST |
FSMC; MFIS |
Corsi blocks forward; Digit span forward; SDMT |
CES-D; FAMS | No follow up assessment performed | Corsi block backward: ηp2 = 0.08; Digit span backward: ηp2 = 0.11; 2-back task omissions: ηp2 = 0.06; PASAT: ηp2 = 0.10; FST: ηp2 = 0.14 (distributed training group). Digit span backward: ηp2 = 0.11; 2-back task omissions: ηp2 = 0.06; PASAT: ηp2 = 0.10; FST: ηp2 = 0.11 (high intensity training group) |
|
Shatil et al. (2010) [41] |
General memory; Visual working memory; Verbal auditory working memory (N-CPC) | Auditory (non-linguistic) working memory; Awareness divided attention Avoiding distractions; Hand – eye coordination; Inhibition Naming; Planning response time; Shifting attention Spatial perception; Time estimation; Visual perception; Visual scanning (N-CPC) |
Zung depression scale; EDSS; FSS | No follow up assessment performed | General memory: ηp2 = 0.207; Visual working memory: ηp2 = 0.196; Verbal auditory working memory: ηp2 = 0.191. | |
|
Amato et al. (2014) [6] |
PASAT; SDMT (improvement also in the control group) |
ESS (improvement also in the control group); MADRS (improvement also in the control group); VAS (improvement also in the control group) | Visual search; TMT A & B; SRT; SPART; WLG | FSS | PASAT; SDMT (improvement sustained also in the control group) | Not reported |
|
Charvet et al. (2015) [32] |
General composite cognitive score |
Ecog | WAIS-IV letter number sequence; Corsi block; PASAT; SRT; BVMT-R |
No follow up assessment performed | General composite cognitive score: d = 1.11 | |
| De Giglio et al. (2015)[43] | Stroop test; SDMT | MSQoL-54 mental health composite, rolelimitations-emotional, emotional well-being, cognitive function, health distress | PASAT 3 | MFIS; MSQoL-54 physical health composite, physical function, role limitations- physical, pain, energy, health perceptions, social function, sexual function, overall QoL, sexual function | No follow up assessment performed | Stoop test: F2 = 0.210; SDMT: F2 = 0.177 |
|
Hancock et al. (2015) [44] |
PASAT | SDMT; Stroop test; LNS; Digit backward; Raven's APM; BVMT-R; COWAT; CPT-II; AVLT | BDI; STAI; MFIS; MSQOL-54 | No follow up assessment performed | PASAT: d= 0.90 |
|
|
Campbell et al. (2016) [45] |
SDMT | CVLT-II; BVMT-R | EQ-5D; FAMS; PAM-13; USE-MS; HADS; MSNQ; FSS | not significant | Not reported | |
|
Pedullà et al. (2016) [46] |
SRT consistent long-term retrieval & delayed recall; SDMT; PASAT; WLG | SRT long term storage; SPART; WCST | PASAT; SDMT | Not reported | ||
|
Charvet et al. (2017) [47] |
General composite cognitive score |
SRT; BVMT-R; PASAT; TMT; WAIS-IV letter number sequence; WAIS-IV digit span backward; DKEFS | No follow up assessment performed | General composite cognitive score: d = 0.38 |
||
|
Messinis et al. (2020) [48] |
SDMT, GVLT, BVMT-R | MFIS; BDI-FS; EQ-5D | No follow up assessment performed | SDMT: g = 2.980; GVLT: g = 2.898; BVMT-R: g = 1.699 | ||
|
Vilou et al. (2020) [49] |
GVLT; BVMT-R; TMT-A; Stroop test | SDMT; TMT-B | No follow up assessment performed | GVLT: d = 0.6; BVMT-R: d = 0.38; TMT-A: d = 0.15; Stroop test: d = 0.32 | ||
|
Blair et al. (2021) [50] |
DKEFS colour-word interference test; WAIS-III digit span backward | HADS-D | SDMT; PASAT; CVLT-II; BVMT-R; VSVT; WAIS-III spatial span forward and backward, WAIS-III arithmetic; WAIS-III digit span forward; WAIS-III letter-number sequence | BDI-FS; FSS, MSNQ, HADS-A; SF-36; DEX; CFQ; Brief COPE; PDQ; NPRS | HADS-D |
DKEFS colour-word interference test: d = 0.27; WAIS-III digit span backward: d = 0.69 |
*Abbreviations: APM, Advanced Progressive Matrices; AVLT, Auditory Verbal Learning Test BDI, Beck's Depression Inventory; BDI-FS, Beck's Depression Inventory- fast screening; BVMT-R, Brief Visuospatial Memory Test-Revised; CES-D, Centre for Epidemiologic Studies Depression Scale; CFQ, Cognitive Failures Questionnaire; COWAT, Controlled Oral Word Associations Test; CPT, Conners’ Continuous Performance Test; CVLT, California Verbal Learning Test; DEX, Dysexecutive Questionnaire; DKEFS, Delis-Kaplan Executive Function System; Ecog, Everyday cognition scale; EDSS, Expanded Disability Status Scale; EQ-5D, EuroQOL five-dimension questionnaire; ESS, Environmental Status Scale; FAMS, Functional Assessment of Multiple Sclerosis; FSS, Fatigue Severity Scale; FSMC, Fatigue Scale for Motor and Cognitive Functions; FST, Face Symbol Test; GVLT, Greek Verbal Learning Test; HADS-A, Hospital Anxiety Scale; HADS-D, Hospital Depression Scale; LNS, Letter–Number Sequencing; MADRS, Montgomery and Asberg Depression Rating Scale; MFIS, Modified Fatigue Impact Scale; MSNQ, Multiple Sclerosis Neuropsychological Questionnaire; MSQoL-54, 54-item Multiple Sclerosis Quality of Life Questionnaire; NCP-C, Neuropsychological Examination – CogniFit Personal Coach; NHPT, Nine Hole Peg Test; NPRS, Numeric Pain Rating Scale; PAM-13, Patient Activation Measure; PASAT, Paced Auditory Serial Addition Test; PDQ, Perceived Deficits Questionnaire; QoL, Quality of Life; RTs, Reaction Times; SDMT, Symbol Digit Modalities Test; SF-12, short form of the SF 36 health questionnaire; SF-36, Short Form Health Survey; SPART, 10/36 Spatial Recall Test; SRT, Selective Reminding Test; STAI, State–Trait Anxiety Inventory; TMT, Trail Making Test; USE-MS, Unidimensional Self-Efficacy scale for Multiple Sclerosis; VAS, visual analog scale; VSVT, Victoria Symptom Validity Test; WAIS, Wechsler Adult Intelligence Scale; WCST, Wisconsin Card Sorting Test; WLG, Word List Generation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



