Submitted:
24 February 2024
Posted:
26 February 2024
You are already at the latest version
Abstract
Monkeypox virus belongs to the Orthopoxvirus genus, which belongs to the Poxviridae family. The Monkeypox virus is responsible to cause monkeypox, a developing zoonotic disease that has been identified as the most common orthopoxvirus infection in humans in the post-eradication era of smallpox. The virus can be transmitted by a variety of animals, including monkeys and rodents as well as person-to-person. Monkeypox has a clinical presentation that is quite similar to smallpox but mortality is low, in that the febrile prodrome is followed by a period of skin eruption. Monkeypox cases have extended outside the forests of central Africa, where they were first discovered, to other regions of the globe, where they have been imported. This pattern of transmission is most likely related to a global reduction in orthopoxvirus immunity following the discontinuation of smallpox vaccination in 1980, when smallpox was proclaimed eliminated. As a result, monkeypox might become the very common orthopoxvirus infection that affect humans. The emergence of epidemics outside of Africa emphasizes the disease's global significance. Increased monitoring and identification of monkeypox cases are critical tools for gaining a better knowledge of the disease's ever-changing epidemiology.
Keywords:
Monkeypox virus
; Orthopoxvirus
; Epidemiology
; Zoonotic sources
; Diagnosis
; Treatment
1. Introduction
Viruses are responsible for a substantial number of medically important emerging and reemerging infections as well as a wide spectrum of infectious diseases affection both animal and humans. They represent a far bigger harm to public health globally now than they did a century ago [1]. They are responsible for some of the most frightening and deadly human infections, and their capacity to spread quickly makes them substantial contributors to the morbidity and mortality of worldwide infectious diseases [2] For example, more than 30 million people are believed to have died from AIDS, and more than 30 million are thought to be living with HIV/AIDS. Additionally, it is estimated that more than two million new infections occur each year. Monkeypox is a zoonosis caused by the Monkeypox virus (MPXV), a member of the Orthopoxvirus genus [3]. The MPXV virus is linked to the Variola virus, which causes smallpox. Although the two viruses have many clinical similarities, monkeypox is often milder than smallpox [4]. The MPXV is a double-stranded DNA virus that belongs to the Orthopoxvirus genus. Monkeypox is a zoonotic disease that was originally discovered in the Democratic Republic of the Congo (DRC, previously Zaire) in 1970 as a human pathogen [5]. The monkeypox virus seems to be greater (200-250 nm) under electron microscopy. The brick-shaped Poxviruses has a genome of double stranded linear DNA enclosed in a lipoprotein envelope [6,7]. Apart from relying on host ribosome for translation of mRNA, poxviruses have all of the required replication, transcription, assembly, and egress proteins encoded in their genome [6,8]. Vaccine-induced immunity to the monkeypox virus had previously been obtained; however, elimination of smallpox and consequent failure of vaccine measures enabled the monkeypox to become clinically relevant [9]. Furthermore, because the majority of monkeypox cases arise in rural areas of Africa, possible underreporting might lead to an underestimating of the possible risk of this virus [10]. One feature of the monkeypox virus that has gotten a lot of interest but still hasn't been fully explained the process that helps the virus to survive in nature. That information gap restricts our capacity to effectively forecast how changes in the environment like habitat disruption, climate change, and rainfall etc. may affect prevalence of virus in nature and, by consequence, chances of monkeypox infection in humans. Monkeypox is now restricted in the moist forest areas of Central and West Africa, and rational, prolonged reporting of cases has been mostly confined to the Democratic Republic of the Congo [11].
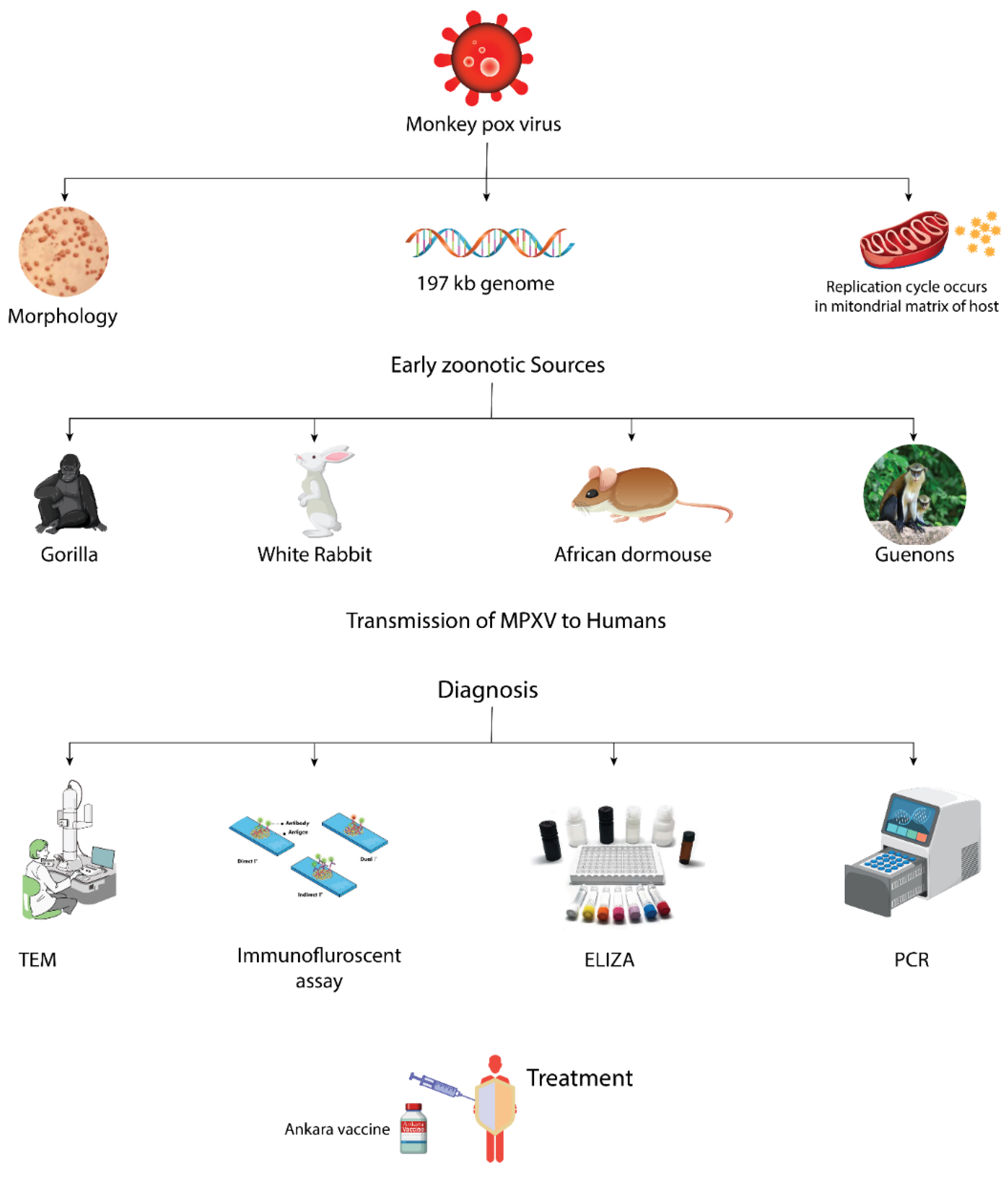
Figure 1.
Graphical Abstract.
Following verified case in the West African clade of monkeypox virus announced on 7 May 2022 in the United Kingdom (UK) and several countries subsequently, global interest has been focused on the monkeypox virus. The growing worldwide monkeypox outbreak was declared a Public Health Emergency of International Concern (PHEIC) on July 23 by WHO. Currently, the WHO European Region is the site to the great majority of reported cases. In order to handle the epidemic with the necessary urgency, WHO/Europe is still committed to working in partnership with communities and countries. The affected person had previously visited Nigeria and returned to the United Kingdom [12]. The most recent cases before this outbreak were reported in 2021. According to the UK Health Security Agency, viral transmission was documented in Europe without epidemiological ties, travel history to Africa, or known exposure to an infected individual [12]. Cases have been detected in different countries like Australia, Canada, USA, Israel, and some European nations, such as the France, United Kingdom, Portugal, Germany, Spain, Italy, Belgium, Sweden, and Netherlands. Over 100 confirmed cases have been reported outside of Africa [13]. The West African clade is responsible for all documented instances outside of Africa. The animal origin, reservoir host for viral circulation, and natural history is yet unknown [14]. Continuous monitoring of the monkeypox virus in endemic areas will aid in our understanding of the virus's zoonotic origin. Monkeypox has moderate clinical symptoms, with a fever, enlargement of lymph node, rash and most people recover within a few weeks. When a suspected or new confirmed case is identified, complete isolation with supportive treatment and quarantine procedures should be in operation. The end of smallpox vaccination in 1980, together with declining immunity among the population and a rise in the number of non-immune people, resulted in an increase in the prevalence of monkeypox [14]. It has been found that the smallpox vaccination can prevent monkeypox [15]. Furthermore, MVA-BN (JYNNEOS in the US, IMVAMUNE in Canada, and IMVANEX in Europe) is the only licensed vaccine for the prevention of monkeypox, and Tecovirimat SIGA (Tpoxx) is a drug approved for the treatment. Despite the fact that they were identified in 1958, these countermeasures are still not extensively used [15]. Despite the fact that monkeypox is still a relatively rare virus, the rising number of cases across Europe and in non-endemic countries is causing concern around the world. Transmission patterns, epidemiological studies, and the ecology of the ailment are all incomplete, and further research is needed. To deal with emerging or reemerging viral threats in a sustainable way, encouraging precautionary measures, awareness campaigns, educating health care workers, and advancing public health preparation with preventative continuous comprehensive monitoring, early detection, rapid risk evaluations, contact tracing, and response activities should be critical. The COVID-19 pandemic emphasizes the need to enhance national healthcare systems as well as develop global laws and regulatory frameworks to react rapidly to possible threats [16]. The World Health Organization and other government agencies are gathering data, identifying information gaps, and prioritizing research issues for monkeypox research in terms of developing a quick-response action plan to combat the outbreaks. Overall, the outbreak must be closely watched, and researchers must continue to investigate treatment alternatives and control methods, as well as encourage the public to follow safety regulations addressed by national and international and national health authorities [17]. In this review, morphology, genome, and replication cycle of monkeypox virus is described. How this virus transmitted from early zoonotic sources into humans, its clinical presentations, epidemiology, diagnosis, as well as treatment strategies.
2. Molecular Biology
2.1. Morphology
Monkeypox virus is one of the biggest and perhaps most versatile virus, among other poxviruses [18]. They comprise brick-like principal characteristics having 220 nm to 450 nm of length and 140 nm to 260 nm of width [19]; hence, MPXV is substantial adequate to be seen with a microscopic examination, and its ultrastructure can be resolved using electron microscopy. To discern structure and function, although, greater resolution given by electron microscopy is required [20]. The lateral bodies, core, outer membrane, and outer lipoprotein envelope are the four primary components of the orthopox virion. The viral double-stranded DNA (dsDNA) and core fibrils are found in the central core, which is surrounding by a closely structured layer of rod-shaped components known as the apical surface. The outer layer, which is made up of multiple exterior glomeruli, encloses the central core, palisade layer, and peripheral bodies (Figure 2.1). The outer lipoprotein envelope is commonly present in spontaneous liberated virions, but the membrane is absent in virions generated via cellular disturbance [21]. At least 80 viral proteins are found in a developed virion [22,23].
2.2. Genome
The monkeypox genome is a single straight dsDNA molecule with a length of 197 kbp, making it one of the biggest viral genomes [20]. Every endpoint of the genome has a series of short repetitive sequences [25] and terminal hairpin loops [26], as well as comparable but reversely positioned terminal copies with a size of roughly 6 kbp [24]. About 190 nonoverlapping open reading frames (>180 bp long) comprising 60 or more amino acid residues make up the genome. Four of them may be found in the inverted terminal repeat [24,27]. MPXV DNA has a low guanine and cytosine content, roughly 31.1 percent [28]. The West African (WA) and Central African (CA) haplotypes of MPXV have been identified as different genetic lineages [29]. The whole genome sequencing of numerous OPVs indicated a high proportion of commonality in the center genes and a large degree of diversity in the regions situated on both ends of the genome. Variable OPV terminal sequences are likely to be related to the pathogenicity of various OPVs [30,31,32], because fixed OPV genes are typically engaged in important viral processes including replication and virion assembly [27]. By interacting with antigen signaling, distribution, and identification, as well as death, several terminal genes contribute to innate immunity [27,33].
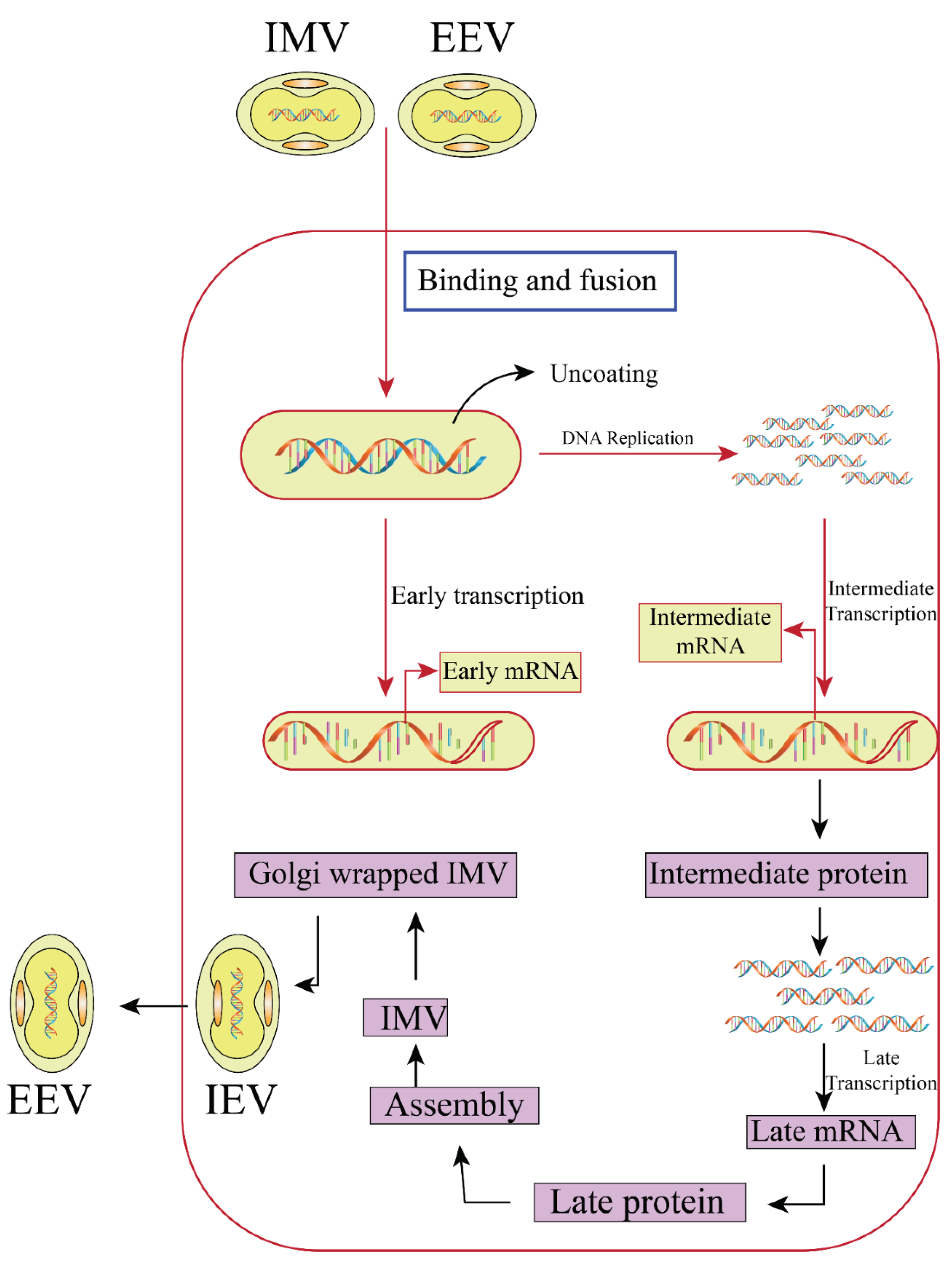
2.3. Replication Cycle
Unlike other DNA viruses, the replication cycle of poxviruses occurs in the mitochondrial matrix of the host cell [34]. Poxviruses penetrate the cell by a series of complex strategy that incorporates adhesion, hemifusion, and core entrance at the cell membrane or after endocytosis [35]. Poxviruses penetrate the cell by various mechanisms depending on whether they are mature virion (MV) with a simple outer membrane or extrinsic enveloped virion (EV) with an outer layer with a distinct amino acid composition. The exterior EV-specific membrane is removed in EV form, revealing the underlying MV membrane, which subsequently unites with the cell. EV is specialized for cell-to-cell dissemination due to its long, mobile projections created by actin polymerization that cling to the cell surface [20,35], despite the fact that MV is more prevalent. During entrance, the adult virion is uncoated for the first time, and once in the cytoplasm, the viruses distribute packed viral proteins and catalytic components that weaken cell defenses and promote expression of earlier genes. Following that, viral DNA-dependent RNA polymerase synthesizes early messenger RNA (mRNA). The second uncoating phase, DNA replication, and the synthesis of intermediate transcriptional regulators are all aided by initial mRNA translation. Intermediate mRNA is then translated and transcribed, resulting in the production of late mRNAs and their transformation into functional and non-structural molecules (Enzymes and early transcription factors). The translated molecules are packaged into adolescent virions, which evolve into internal matured virions, with DNA concatemers generated during the early stages of replication (IMVs). IMVs are infectious only when they are released by cell breakdown because they lacked an outer sheath. IMV particles that do not end up enclosed inside the protein matrix of the cytoplasm acquire a second barrier and become cytoplasmic encapsulated virions (IEVs) [36,37]. They use microtubules to migrate to the inner cell membrane and fuse with it to generate cell-associated virions (CEVs), which cause actin polymerization and the development of filaments that aid CEVs in escaping the cell. Extracellular enveloped virions are the name for CEVs that have escaped the cell (EEVs) (Figure 2) [36].
Figure 2.
Replication cycle of monkeypox virus.
2. Early Insights into Zoonotic Origins of Monkeypox
The emergence and initial connection of MPXV with disease in non-human primates (NHPs) (especially animals of the species Macaca) led to speculation that the virus was an East or South Asian primate pathogen [38]. The discovery of many human illnesses in isolated African settlements, while, raised questions on the virus's Asian origins. Nonetheless, the high number of early human cases involving primates contributed to maintain the view that these animals were primarily responsible for the infection's transmission to humans [38]. Serostudies conducted between 1970 and 1975 among large groups of wild and wild-caught NHPs revealed a lack of anti-Orthopoxvirus antibodies in animals from Asia and parts of Africa where human MPX has not been detected (n = 1614) [38]. Orthopoxvirus seroreactivity was found in a subset of NHPs from West and Central Africa, including reportedly MPXV-specific antibodies from two Cercopitecus aethiops collected in Cote d'Ivoire (n = 207) [39]. Surprisingly, despite extensive viral culture efforts, no isolates were discovered throughout these examinations. In addition, the infection epidemiology in humans failed to show that NHPs were the predominant vehicle of viral transmission to people [40]. People residing in affected regions had frequent contact with these animals, and the high prevalence of illnesses among children who were too little for hunting or prepare monkey meat indicated an alternate source of infection, in addition to or instead of NHPs. A large research study of animals (comprising approximately 43 species) in the Democratic Republic of the Congo in 1979, revealed more serologic evidence of Orthopoxvirus exposure among NHPs, as well as evidence indicating at least one species of terrestrial rodent, most notably squirrels, with the latter displaying presumed MPXV-specific serologic reactivity [40]. This conclusion was in line with data showing 12% of people suspected of being infected by animal contact had recently interacted with squirrels [41]. Additionally, none of the domestic animals examined, including 67 cats and 120 goats and sheep, demonstrated serologic evidence of an infection with the Orthopoxvirus infection [42].
Since 1984, the aim of ecological investigations has shifted, with collections being limited to locations in the DRC with active human cases [43]. The consequence of this shift in focus were twofold: Ecological research began to expand to include components of human behavior like food sources, gender, age related activities and society structure and second, to investigate the relevance of landscape elements (remote forest hunting camps, agricultural plots) in close proximity to village residents as well as further away. This gave rise to the concept that damaged 'agricultural' zones near habitations - regions abundant in squirrels of genus Heliosciurus and Funisciurus, as well as some terrestrial rodents are potential sites where human interaction may lead to viral transmission [42,44]. Indeed, collections were enriched for such species, as well as for NHPs living further away from human habitats, contributing to a significant breakthrough in our knowledge of virus survival and transmission to humans from zoonotic sources, in 1985 MPXV was isolated from a symptomatic, captured squirrel Funiscirurs anerythrus [40]. While the socio-ecological hypothesis for MPXV preservation and transmission was first accepted by scientists, there has been very little new data produced over the years to prove its validity. The virus has been mysterious in its natural source, and the suspected animal source of initial human infections remains a mystery [45,46]. The only other wild animal virus isolation was from a juvenile sooty mangaby (Cercocebus atys) in Cote d'Ivoire in 2012 [47]. The concept that NHPs may have accidental infections comparable to humans, and that they may also be an unintentional infection source for humans, is now widely acknowledged. Apart from that, monkeypox is now thought to be a wildlife zoonosis having a complicated epizootiology and ecology, possibly including a network of sustaining hosts as well as extra vulnerable species capable of spreading the virus to humans [48]. The vulnerability of numerous native rodent species to MPXV infection sparked immediate worry about the prospect of sylvatic transmission, however limited screening operations at the location of animal corpse disposal failed to detect this virus in rodent populations.

Table 1.
Infection of monkeypox virus to a wide range of animals.
| Species Name | Family | Commonly Called | Determination Techniques | Remarks | References |
|---|---|---|---|---|---|
| Graphiurus spp. | Gliridae | African dormouse | Outbreak in pocket pets; Infection investigations in the Lab | After infection, in vivo imaging experiments were carried out. | [49,50] |
| Cynomys ludovicanus | Sciuridae | Black-tailed priarie dog | Outbreak in pocket pets; Infection investigations in the Lab | After infection, in vivo imaging experiments were carried out. | [49,51] |
| Cercopithecus spp. | Ceropithicediae | Guenons | Field examinations | no virus or antigen DNA identified, OPX antibody positive | [52] |
| Gorilla sp. | Hominidae | Gorilla | Outbreak, zoological park | Morbidity reported | [53] |
| Cricetomys spp. | Nesomyidae | Giant pouched rat | Outbreak in pocket pets; Infection investigations in the Lab | After infection, in vivo imaging experiments were carried out. | [49,54] |
| Mus musculus | Muridae | Laboratory mouse, domestic mouse | Infection studies in laboratory | Adult immunological competent mice are often resistant to wild-derived castaneus strains, which have been found to be sensitive in laboratory trials. | [55,56] |
| Myrmecophaga tridactyla | Myrmecophagidae | New World giant anteater | Outbreak, zoological park | Morbidity reported | [53] |
| Petrodromus tetradactylus | Macroscelididae | elephant shrews | Field examinations | no virus or antigen DNA identified, OPX antibody positive | [57,58] |
| Oryctolagus cuniculus | Leporidae | White rabbit | Infection investigations in laboratory | Adult animals are normally not vulnerable; however, outcome varies depending on the inoculation route and the animal's genetic background. | [59] |
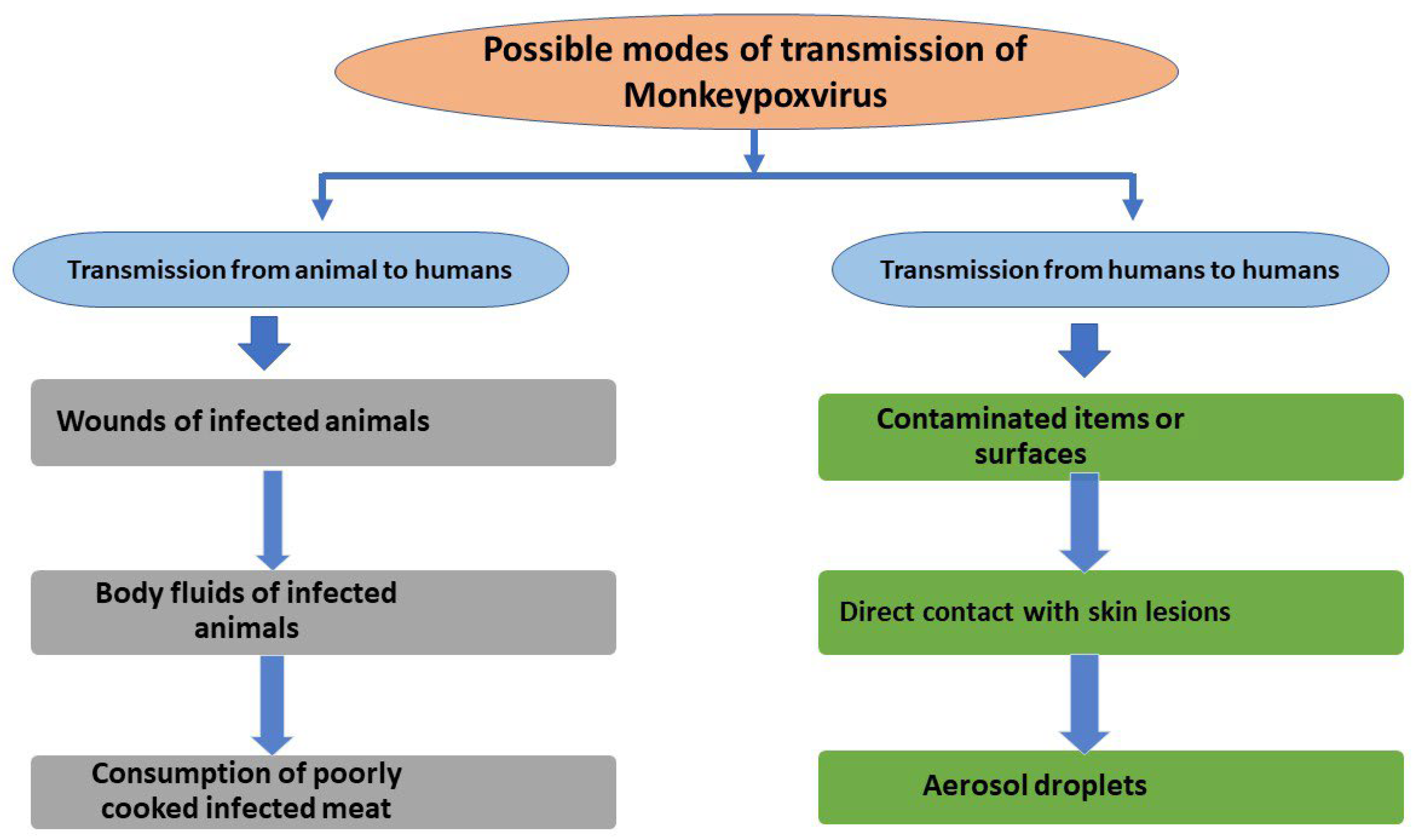
3. Transmission of MPXV to Humans
It is uncertain how MPXV transmits from animals to humans as well as the precise reservoir of monkeypox vertebrate hosts. Aerosol infection has been established in animals [60,61], which might explain the Central African Republic's nosocomial epidemic [62]. Human monkeypox illnesses in humans are thought to be caused through indirect or direct contact with live or dead animals [63,64]. People are forced to hunt tiny mammals (bushmeat) for protein-rich food caused by poverty and ongoing civil turmoil, enhancing their susceptibility to wild mice, which may transmit monkeypox [65]. In August 1970, a 9-year-old girl with smallpox-like vesicular skin lesions in the town of Bukenda in Zaire's Equatorial zone was recognized as the first human case of monkeypox (now Democratic Republic of Congo - DRC) [66]. This patient was discovered during an intensive smallpox monitoring phase that lasted 9 months after WHO confirmed the elimination of smallpox in the DRC. Whether the virus is transmitted from human to human or from animal to human, the pathogenesis of monkeypox start with this transmission. Respiratory droplets are the most prevalent cause of human-to-human transmission. Figure 3 depicts direct contact with contaminated objects/surfaces and direct touch with an infected individual's infections of the skin lesions.
4. The Evolving Epidemiology of Human Monkeypox
Monkeypox in humans was initially detected in Sub-Saharan Africa in 1970 [67], and since then, the World Health Organization (WHO) has received reports of possible cases whenever they have been raised to the health sector.
After smallpox extermination was certified in 1980, a five-year span of rigorous monitoring of human monkeypox in the Democratic Republic of the Congo found and evaluated 338 more illnesses. Throughout West Africa, eight were passively reported and examined [68,69]. Simultaneously, a number of serological investigations in three West African nations found that over 10,000 infants under the age of five who did not have a scar of smallpox vaccination showed no sign of human monkeypox illness, as seen by the disappearance of facial bruising as well as orthopox antibodies. This offered confidence that the infectivity of monkeypox was not growing, although occasional cases continued to be reported [70,71].
According to the Whitehouse research, before 1980 all people born vaccinated against smallpox. In real life, vaccination rates were much above 100%. Because the post-1980 birth cohort presumably constitutes the majority of the DRC's population, we should infer that only a minimum number of residents have immunity induced by smallpox-vaccine against monkeypox [72]. By 1995, investigators had a fundamental grasp of the human monkeypox epidemiology. Human monkeypox was uncommon in people over the age of 15, and more than 70% of cases were linked to interaction with a jungle animal, either one that was found dead or sick and handled by a youngster, or one that were carried by hunter back to the house from the forest. With exception of individuals without a vaccination scar of smallpox, there was very little forward transference to relatives, and they seldom carried illness on to a 3rd generation. Children in West Africa who had not been vaccinated did not experience community-level illness, according to serological investigations of young people there. Nevertheless, in 1996, the cases of monkeypox infections reported in humans in DRC increased dramatically, and from 1997, a total of 88 people had been diagnosed with the disease [73]. Assumptions from 1996 to 2005 recommended that as non-vaccinated cohorts grew older, the age of individuals identified with monkeypox risen; 25% of all illnesses could be followed back to wildlife interaction; and transfer could last up to 9 generations of non-vaccinated interactions, compared to 3 generations in the time prior to 1996 [74]. In the DRC, intensive screening of human monkeypox was resumed in 2006 and 2007. These investigations found that transmission had increased 20-fold since the 1980s, and that vaccinated children had a 5.21-fold reduced chance of disease than those unvaccinated [74,75]. Despite 39 years with no cases recorded, human monkeypox was discovered in Nigeria in 2017. There were 122 verified or suspected cases, comprising 2 healthcare personnel, with infection from recognized zoonotic sources as well as human-to-human transmission both [76]. Since then, isolated instances have been documented in Nigeria. Human’s monkeypox cases have also been discovered as a result of importations. In 2003, an infected rat brought from West Africa triggered an epidemic in the United States. Several patients in Wisconsin started to have symptoms in May, which sparked the outbreak. Authorities found that the persons had contracted the disease from prairie dogs they had purchased as pets. The African rodents, which were sold to various exotic pet merchants across the country and then resold, were thought to have infected the prairie dogs. Prairie dogs marketed as pets were affected, and 47 people were determined to be afflicted [77,78]. Importations have also been found in Nigerian visitors in the U.K, Israel, and Singapore [79]. However, the immigrations did not produce epidemics, they were quickly isolated and hospitalized as they were discovered, and one hospital employee in the United Kingdom fell ill from dirty bed linens [80]. The Congo Basin and West African clades of the monkeypox virus have been discovered using genetic sequencing [81]. These lineages seem to be progressively passed through human to human, with Whitehouse et al. [82] documenting person-to-person transmission for the Congo Basin clade. The Congo Basin lineage is said to be more aggressive, with case fatality rates of up to 11%, although there are still gaps in our understanding of how it spreads [83,84,85]. With an overall case fatality rate of 1–5% [80], the West African monkeypox clade is less virulent. The Whitehouse et al. study [82] includes a large database of case reports, yet there are still unanswered problems concerning human monkeypox. At this time, epidemics tend to be self-contained, although zoonotic and human-to-human transmission seem to be on the rise. According to recent genomic research [86,87], both monkeypox virus lineages appear to be stable at the moment.
Continuous screening and fieldwork research, like the above conducted by Whitehouse et al., is now essential to ensure that if monkeypox communicability rises, it is identified quickly and treated quickly, potentially with vaccination [88]. The Centers for Disease Control and Prevention in the U. S. investigated a new-generation smallpox vaccination that provided substantial protection over monkeypox illness in humans and was safe to use in people with HIV [89]. Smallpox vaccinations of the 2nd generation, which were recently produced, provide excellent protection against monkeypox infection. But, if a shift in transmissibility does occur, is surveillance and research adequately financed to discover it? Is it possible to scale up monkeypox vaccine production if necessary? The concern of whether human monkeypox might fill the epidemiological void, as well as other concerns concerning our capacity to identify and respond if this happened, remained unaddressed. Limited-resource environments, like DRC, require special attention [80,90]. The DRC is now experiencing Ebola outbreaks, as well as epidemics of Lassa fever, Plaque, Yellow fever, chickenpox, measles, cholera, covid-19, and monkeypox [23]. Even though data on chickenpox in the DRC is relatively limited, we know essentially nothing regarding the influence of such infections on monkeypox co-morbidity. New DRC data is in high demand right now. From January 1 to October 18, 2020, over 200 monkeypox fatalities were reported in the DRC, with an estimated case count of 10,000 or more [23].
5. Clinical Presentation of Monkeypox Virus
Since smallpox was eradicated, MPXV is the orthopoxvirus that has caused the attention in humans [91]. The pathophysiology and clinical features of the human MPX (Figure 3), which has an incubation period of 7–17 days, an initial feverish prodromal period of 1–4 days, and a rash period of 14–28 days, generally match those of a distinct, conventional smallpox. The appearance, location, and development of lesions in MPXV and smallpox are comparable [91,92]. A prodrome of fever, headache, muscular pains, backaches, and lymphadenopathy are among the distinctive symptoms. These are subsequently followed by broad, well-circumscribed rashes with a peculiar centrifugal pattern that advance through macular, papular, vesicular, and pustular stages [93,94]. When the lesions turn pustular, a second febrile episode happens, which is frequently accompanied by a worsening of the patient's health [95]. As seen after direct human-to-human transmission, a more severe disease is linked to pronounced sickness, high viremia, and mortality, but not prolonged infection [96]. Smallpox vaccination provides some level of protection, with serious sequelae being seen more frequently in the unprotected group (74%) than the vaccinated group (39.5%) [92].
6. Diagnosis
Skin lesions like dry crusts, blisters, & pustules yield the finest biopsies, which are then preserved in a dry, sterile tube & managed to keep cold. Skin biopsy is a viable option for collecting samples. In the context of distinctions with obvious signs of systemic rash sickness, such as syphilis, scabies, measles, medication-associated allergies, & bacterial skin problems, determining a clear diagnosis can be difficult [97]. Orthopoxviruses, such as chicken pox & smallpox, are typical divergences of monkeypox. TEM (Transmission electron microscopy) & PCR (Polymerase Chain Reaction) were used to identify the monkeypox virus in pustular swabs, and confirmation testing was done using tissue culture, and immunofluorescence assay, & ELISA (Enzyme-Linked Immunosorbent Test) [98,99].
7. Treatment and Management
Monkeypox infection still has no scientifically tested medications. The cure is cooperative symptom control, like most other viral infections. Furthermore, some precautions can be taken to minimize the spreading rate of this disease. Unless all lesion crusts have normally peeled off & a new skin layer has grown, the diseased person should be kept in separation, wearing a protective mask, and keeping lesions clothed as often as possible. Medicines that have shown efficacy towards orthopoxviruses in animal trials & serious vaccinia vaccination problems may be investigated for exploratory use in extreme situations. The monkeypox virus is resistant to the intravenous vaccinia immune globulin, the oral intracellular viral release inhibitor tecovirimat, & the oral DNA polymerase inhibitor brincidofovir [100]. Persons who have been infected with the virus ought to have their temperature & symptoms checked twice a day for 21 days, as this is the recognized top limit of the monkeypox incubation time. Because infectivity coincides with the start of symptoms, close contacts do not need to quarantine while asymptomatic. In certain circumstances, immunization with altered vaccinia, Ankara vaccine (live, non-replicating monkeypox & smallpox vaccine) is advised. Contact between broken skin or mucous membranes and the bodily fluids, respiratory secretions, or scabs of an affected person is regarded as a "serious risk" exposure that necessitates prompt post-exposure immunization. Vaccination after 4 days of infection may avoid the onset of disease, whereas vaccination within fourteen days may lessen the severity of the disease, according to the CDC.
Vaccinia virus has been engineered to be replication-defective. When contrasted to 1st and 2nd-generation smallpox vaccines, the Ankara vaccine is a 2-shot series given 4 weeks apart with a better safety profile. Unlike live vaccinia virus preparations, Ankara doesn't cause a skin reaction or represent a risk of local or widespread dissemination [100]. Furthermore, clinical experiments have demonstrated that recombinant vaccinia Ankara is harmless and increases antibody generation in patients with atopy and impaired immune systems, both of which are recognized contraindications to live vaccinia dosing [101]. Further data acquisition and feasibility research are needed to determine the possible advantages and risks of prophylactic monkeypox immunization in endemic areas. The potential to make informed judgments on how to best manage this neglected tropical disease is hampered by a lack of medical care & diagnostic skills [101,102,103].
8. Preventive Strategies
In endemic locations, preventing the spread of the Monkeypox virus is difficult. It entails restricting all interaction with rodents & primates, as well as reducing direct blood and undercooked meat exposure. Attempts to stop the trade in bushmeat and the intake of wild creatures are economically and culturally challenging because this meat seems to be the only source of protein accessible to the impoverished populations. To raise public understanding and advising on the correct management of probable animal reservoir species like protective clothes, gloves, protective masks, as well as limiting direct contact with diseased persons, significant health education programs are required.
To avoid human-to-human transmission in health care, infectious disease control techniques are essential. Awareness, along with basic facilities & staffing, is required for improved nursing (gloves, safety clothing, face masks) and isolation techniques. Public health professionals should consider smallpox vaccination for health care staff and anyone caring for or being exposed to persons with monkeypox or their specimens. It is predicted that smallpox vaccination provides 85 percent cross-protection against monkeypox infection [104]. After considerable, exposing the body to an infected animal or a diagnosed human case, the CDC (Centers for Disease Control and Prevention) recommends a smallpox vaccine within 2 weeks, preferably within 4 days [105].
During such an outbreak, the transmission of the monkeypox virus can be stopped by isolating diseased creatures and monitoring their interactions for almost 6 weeks from the date of last exposure [105]. Specific directions from domestic and international public health officials should be followed. Domestic and international organizations must raise awareness and take some action (appropriate policies, medical personnel, testing, monitoring, & training). When a case of monkeypox is suspected in a health center in a civilized country (for example, a person with increased body temperature, skin infections, as well as a history of attending an endemic region or interaction with diseased persons), the patient must be positioned in a negative air pressure room or, if such amenities are inaccessible, a personal room. Universal precautions, droplet precautions, & contact precautions should all be followed. Interact with infection control professionals as soon as possible. Increased awareness of the disease and its endemic locations among healthcare staff in affluent nations is also a crucial precaution [105].
9. Discussion
In terms of monitoring and testing capacity, as well as disease symptom management, monkeypox poses problems for public health authorities and healthcare workers. After the Ebola virus disease pandemic, suggestions from the Global Health Security Agenda & the Joint External Evaluations assessments increased surveillance in West Africa. Nevertheless, numerous healthcare personnel in many countries lack experience & information in recognizing, diagnosing, and treating monkeypox, as well as implementing public-health measures to prevent the disease from spreading further. Immediate and protracted economic and physical resource investments are required to build suitable disease surveillance systems. Currently, Monkeypox is not a disease that requires public disclosure under Africa's Integrated Disease Surveillance & Response system. The DRC has made disease monitoring compulsory, which has resulted in a more systematic recording. Despite the frequency of reports, investigations with diagnostic specimens and the adoption of preventive actions like contact monitoring and strict patient quarantine are less thoroughly implemented. Because monkeypox is a virus zoonosis, it is vital to coordinate actions between the animal and human health sectors, involving regular information exchange. Because human monkeypox mimics numerous other fever rash disorders, such as smallpox and varicella, the laboratory verification of infection is essential. In active cases of monkeypox, biopsies of lesions are adequate specimens for virus recognition, as opposed to sputum, serum, and blood specimens collected by healthcare professionals & laboratory technicians for prognosis of several other ailments, and samples must be supported by careful medical information for proper interpretation of clinical findings. The adoption of monkeypox-specific case inquiry questionnaires, as well as teaching health care staff how to use them, can help with proper case investigation and verification [106]. Molecular assays seem to be the most effective method of laboratory diagnosis, but in regions with endemic diseases, local laboratory capability will need to be strengthened. To enable clinical test quality assurance and validation, regional and worldwide reference lab networks must be developed, and suitable preservation & secure transit of samples in places with restricted facilities will necessitate new solutions. Cases of monkeypox are common in wooded rural regions with little access to health facilities. Because of financial and specialized care restrictions, providing clinical supportive treatment and care for consequences like eye & secondary infections, fluid imbalance & respiratory involvement, can be difficult [106,107].
Though infection control strategies and supplies are frequently deficient in rural regions, precautions including contact precautions, proper cleaning, and restricted patient contact can be adopted at treatment centers and patient residences. Infected persons and family members may experience stigma in their neighborhoods because of a lack of awareness about the disease and fears that instances may signify an epidemic like Ebola, and rumors can spread fear; nevertheless, psychosocial care for infected persons and their family members is often overlooked. A global health strategy that targets potentially harmful practices such as hunting and ingestion of bushmeat, as well as interaction with ill people, must include awareness and risk communication for afflicted populations and families. It is critical to involve communities in the development of feasible treatments and to encourage necessary health-seeking behavior. If resources are provided, interactions could be quickly followed to reduce future population exposures and break transmission networks. To increase information on the epidemic course, data on results and long-term consequences must be better reported [107]. To comprehend the effect of monkeypox on man and livestock, as well as the processes of animal to human transmissions, and to enforce appropriate preventative and response strategies, more coordination between human and animal health specialists is required. To avoid disease transmission, countries that share geographically contiguous risk zones must create comprehensive regional strategies and ensure cross-border collaboration.
Monkeypox was recognized as an emerging epidemic requiring quick investigation of existing possible interventions in the World health organization (WHO) Research & Development Blueprint's 2018 list of priority diseases [108]. In this sense, vaccinations and medical therapies established for smallpox could be verified in medical studies against human monkeypox via practical research in areas where the illness is endemic to maximize its possible effects. The growing number of monkeypox cases were reported from African countries that haven't seen the epidemic in years, as well as the numerous factors that influence monkeypox spread, underscore the need to upgrade understanding of the disease and boost planning initiatives. World health organization (WHO), in conjunction with the CDC, has prioritized several areas of action to overcome information and competence shortages in areas with endemic diseases. To increase research of virus transmission routes, including zoonotic & interhuman, related disease monitoring systems for wildlife and humans must be reinforced through community-based incident recording. This involves listing all suspected cases through the Integrated Disease Surveillance and Response system, collecting appropriate disease-specific data to enable lab diagnosis and epidemiological analysis, and following up on positive samples in endemic areas.
Boosting diagnostic laboratories' capacity necessitates expertise in laboratory methods, sample varieties, and secure sample collection, preservation, and transfer. Advances in the diagnostic capability of the monkeypox virus have been demonstrated to boost zoonotic disease detection and mitigation, notably seen during the Ebola virus epidemic response in the DRC's Tshuapa Province [109]. Regional pieces of training aimed at increasing nationwide competence and exchanging country-level achievements have the opportunity to generate a platform for the interchange of best practices and technical assistance. Further efforts to enhance regional-level capabilities will assist global health security. It is critical to include regional training in nationwide response and surveillance strategies to ensure that medical workers and surveillance personnel in endemic disease areas are prepared to diagnose and manage cases. World health organization (WHO) and orthopoxvirus reference institutions like Institute National de Recherche Biomedical (DRC), Institute Pasteur Dakar, & CDC are striving to give assistance and technical support for the necessary public health steps in all of these endeavors. For infection identification and treatment, as with all zoonotic diseases, a full One Healthcare strategy is required, which includes wildlife monitoring & inquiries into the animal reservoirs, which need special resources. Multinational partnerships are critical for exchanging ideas, strengthening regional and national skills, and notifying adjacent countries about monkeypox incidence in humans and animals. Monkeypox has animal reservoirs, unlike smallpox, a human illness with no animal population that was eliminated by vaccination efforts. Tracking the virus's movements beyond its original ecological context will be possible thanks to a new understanding of the animal reservoir and ecological niche. Improved knowledge of monkeypox will aid in the development of novel ways to prevent the virus from spreading further. Furthermore, enhanced diagnostic and response capability for monkeypox will boost regional capacity for responding to other zoonoses and orthopoxvirus outbreaks [110].
10. Conclusions and Future Perspective
Monkeypox is a zoonotic disease transmitted by a virus that is mostly present in West and central Africa. The evolution of the monkeypox virus, the main leading cause of monkeypox, has been discovered. The current COVID-19 pandemic has demonstrated to the globe the need of being properly prepared for future pandemics or outbreaks. As a result, now is the moment to begin implementing organizational institutions to enhance disease monitoring and reporting systems, which are critical in combating infectious disease occurrences throughout the world. The virus persists in animal populations and can occasionally spread to humans. Possible origins of spillover to humans include reservoir hosts, unintentionally contaminated wild hosts, and replication tolerant confined animals. Gaining a greater knowledge of the main origins and mechanisms of MPXV transmission at the animal-human-ecosystem interface will be a vital next step in avoiding the disease's continued appearance and progression. Before, during, and after MPX outbreaks, inter-sectoral research initiatives (ecologic, epidemiologic) will be critical in producing additional knowledge and theories as well as fostering the development of new instruments for evaluating and predicting MPX disease risks. Given the apparent public health relevance of monkeypox in vulnerable countries, on the one hand, and the absence of awareness and resources to combat and manage it on the other, it is evident that monkeypox requires more attention. Some of the most significant actions to enhance the virus's identification, treatment, and dissemination include promoting awareness, enhancing surveillance, and building diagnostic competence. Moreover, research initiatives are required to create information and lead future improvements in monkeypox prevention and management. Clinical studies for modern vaccinia vaccines and antivirals for monkeypox are among them.
References
- Howard, C.R.; Fletcher, N.F. Emerging virus diseases: Can we ever expect the unexpected? Emerg Microbes Infect. 2012;1(12):e46. [CrossRef]
- Kabuga, A.I.; El Zowalaty, M.E. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J. Med Virol. 2019, 91, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Nathanson, N. (2016). The Human Toll of Viral Diseases: Past Plagues and Pending Pandemics. In Viral Pathogenesis (pp. 3-16). Academic Press. [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Brooks, T.; Chand, M.; Flegg, P.; Hardman, A.; Harper, N.; Jarvis, R.; Mawdsley, S.; et al. Human-to-Human Transmission of Monkeypox Virus, United Kingdom, October 2018. Emerg. Infect. Dis. 2020, 26, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Ladnyj ID, Ziegler P, Kima E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull World Health Organ 1972; 46:593–7.
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Kugelman JR, Johnston SC, Mulembakani PM, Kisalu N, Lee MS, Koroleva G, McCarthy SE, Gestole MC, Wolfe ND, Fair JN, Schneider BS, Wright LL, Huggins J, Whitehouse CA, Wemakoy EO, Muyembe-Tamfum JJ, Hensley LE, Palacios GF, Rimoin AW. Genomic variability of monkeypox virus among humans, Democratic Republic of the Congo. Emerg Infect Dis. 2014 Feb;20(2):232-9. [CrossRef]
- Walsh, D. Poxviruses: Slipping and sliding through transcription and translation. PLoS Pathog. 2017 Nov;13(11):e1006634. [CrossRef]
- Nguyen PY, Ajisegiri WS, Costantino V, Chughtai AA, MacIntyre CR. Reemergence of Human Monkeypox and Declining Population Immunity in the Context of Urbanization, Nigeria, 2017-2020. Emerg Infect Dis. 2021 Apr;27(4). [CrossRef]
- Sklenovská N, Van Ranst M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front Public Health. 2018; 6:241. [CrossRef]
- Durski KN, McCollum AM, Nakazawa Y; et al. Emergence of monkeypox – west and Central Africa, 1970–2017. MMWR. 2018; 67:306–310.
- U.K. Health Security Agency. Monkeypox cases confirmed in England -latest updates. 2022. [Online]. Available from: https://www.gov.uk/ government/news/monkeypox-cases-confirmed-in-england-latest-updates. [Accessed on 25 May 2022].
- World Health Organization. Multi-country monkeypox outbreak in non- endemic countries. 2022. [Online]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON385. [Accessed on 25 May 2022]. Back to cited text no. 9.
- Sklenovská N, Van Ranst M. Emergence of monkeypox as the most important orthopoxvirus infection in humans. Front Public Health 2018; 6: 241. [CrossRef]
- World Health Organization. Monkeypox-United Kingdom of Great Britain and Northern Ireland. 2022. [Online]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON381.[Accessed on 25 May 2022].
- Shanmugaraj B, Malla A, Khorattanakulchai N, Phoolcharoen W. SARS- CoV-2 omicron variant: Could it be another threat? J Med Virol 2022; 94(4): 1284-1288. [CrossRef]
- Shanmugaraj, B.; Phoolcharoen, W.; Khorattanakulchai, N. Emergence of monkeypox: Another concern amidst COVID-19 crisis. Asian Pac. J. Trop. Med. 2022, 15, 193–195. [Google Scholar] [CrossRef]
- Ferreira Barreto-Vieira D, Monika Barth O (2015) Negative and positive staining in transmission electron microscopy for virus diagnosis. In: Shah MM (ed) Microbiology in agriculture and human health. InTech, Croatia. [CrossRef]
- Jahrling PB, Huggins JW, Ibrahim MS, Lawler JV, Martin JW (2007) Smallpox and related orthopoxviruses. In: Dembek ZF, Borden I (eds) Medical aspects of biological warfare. Borden Institute, Walter Reed Army Medical Center; Office of the Surgeon General, United States Army; United States Army Medical Dept. Center and School, Washington, DC.
- Moss B, Damon I (2013) Chapter: Poxviridae. In: Knipe DM, Howley PM (eds) Fields virology, 6th edn. Wolters Kluwer Health/Lippincott Williams & Wilkins, Philadelphia.
- Ladnyi ID, Jezek Z, Fenner F, Henderson DA, Arita I (1988) Chapter: Human monkeypox and other poxvirus infections of man. In: Smallpox and its eradication. WHO.
- Resch W, Hixson KK, Moore RJ, Lipton MS, Moss B (2007) Protein composition of the vaccinia virus mature virion. Virology 358(1):233–247. [CrossRef]
- Sklenovská, N. (2020). Monkeypox Virus. In: Malik, Y.S., Singh, R.K., Dhama, K. (eds) Animal-Origin Viral Zoonoses. Livestock Diseases and Management. Springer, Singapore. [CrossRef]
- Shchelkunov SN, Totmenin AV, Safronov PF, Mikheev MV, Gutorov VV, Ryazankina OI, Moss B (2002) Analysis of the monkeypox virus genome. Virology 297(2):172–194. [CrossRef]
- Wittek R, Moss B (1980) Tandem repeats within the inverted terminal repetition of vaccinia virus DNA. Cell 21(1):277–284.
- Baroudy BM, Venkatesan S, Moss B (1982) Incompletely base-paired flip-flop terminal loops link the two DNA strands of the vaccinia virus genome into one uninterrupted polynucleotide chain. Cell 28(2):315–324.
- Seet BT, Johnston JB, Brunetti CR, Barrett JW, Everett H, Cameron C, McFadden G (2003) Poxviruses and immune evasion. Annu Rev Immunol 21:377423. [CrossRef]
- Shchelkunov SN, Totmenin AV, Babkin IV, Safronov PF, Ryazankina OI, Petrov NA, Sandakhchiev LS (2001) Human monkeypox and smallpox viruses: Genomic comparison. FEBS Lett 509(1):66–70. [CrossRef]
- Likos AM, Sammons SA, Olson VA, Frace AM, Li Y, Olsen-Rasmussen M, Damon IK (2005) A tale of two clades: Monkeypox viruses. J Gen Virol 86(Pt 10):2661–2672. [CrossRef]
- Afonso CL, Tulman ER, Lu Z, Zsak L, Sandybaev NT, Kerembekova UZ, Rock DL (2002) The genome of camelpox virus. Virology 295(1):1–9. [CrossRef]
- Chen N, Li G, Liszewski MK, Atkinson JP, Jahrling PB, Feng Z, Buller RM (2005b) Virulence differences between monkeypox virus isolates from West Africa and the Congo basin. Virol J 340(1):46–63. [CrossRef]
- Tulman ER, Delhon G, Afonso CL, Lu Z, Zsak L, Sandybaev NT, Rock DL (2006) Genome of horsepox virus. J Virol 80(18):9244–9258. [CrossRef]
- Barry M, Wasilenko ST, Stewart TL, Taylor JM (2004) Apoptosis regulator genes encoded by poxviruses. Prog Mol Subcell Biol 36:19–37. [CrossRef]
- Buller RM, Palumbo GJ (1991) Poxvirus pathogenesis. Microbiol Rev 55(1):80–122. [CrossRef]
- Moss B (2016) Membrane fusion during poxvirus entry. Semin Cell Dev Biol 60:89–96. [CrossRef]
- Bray M, Buller M (2004) Looking back at smallpox. Clin Infect Dis 38(6):882–889. [CrossRef]
- Roberts KL, Smith GL (2008) Vaccinia virus morphogenesis and dissemination. Trends Microbiol 16(10):472–479. [CrossRef]
- Arita I, Henderson DA. Monkeypox and whitepox viruses in west and Central Africa. Bull World Health Organ. 1976;53:347–353.
- Gispen R, Brand-Saathof BB, Hekker AC. Monkeypox-specific antibodies in human and simian sera from the Ivory Coast and Nigeria. Bull World Health Organ. 1976;53:355–360.
- Khodakevich, L., Ježek, Z., & Kinzanzka, K. (1986). Isolation of monkeypox virus from wild squirrel infected in nature. Isolation of monkeypox virus from wild squirrel infected in nature., (Jan. 11), 98-99. [CrossRef]
- Arita I, Jezek Z, Khodakevich L; et al. Human monkeypox: A newly emerged orthopoxvirus zoonosis in the tropical rain forests of Africa. Am J Trop Med Hyg. 1985;34:781–789. [CrossRef]
- Khodakevich L, Szczeniowski M, Nambu MD; et al. Monkeypox virus in relation to the ecological features surrounding human settlements in Bumba zone, Zaire. Trop Geogr Med. 1987;39:56–63.
- Khodakevich L, Jezek Z, Messinger D. Monkeypox virus: Ecology and public health significance. Bull World Health Organ. 1988;66:747–752.
- Khodakevich L, Szczeniowski M, Manbu MD; et al. The role of squirrels in sustaining monkeypox virus transmission. Trop Geogr Med. 1987;39:115–122.
- Doshi RH, Guagliardo SAJ, Dzabatou-Babeaux A; et al. Strengthening of surveillance during monkeypox outbreak, republic of the Congo, 2017. Emerg Infect Dis. 2018;24:1158–1160. [CrossRef]
- Hutin YJ, Williams RJ, Malfait P; et al. Outbreak of human monkeypox, democratic republic of Congo, 1996 to 1997. Emerg Infect Dis. 2001;7:434–438. [CrossRef]
- Radonic A, Metzger S, Dabrowski PW; et al. Fatal monkeypox in wild-living sooty mangabey, Cote d’Ivoire, 2012. Emerg Infect Dis. 2014;20:1009–1011. [CrossRef]
- Doty JB, Malekani JM, Kalemba LN; et al. Assessing monkeypox virus prevalence in small mammals at the human-animal interface in the democratic republic of the Congo. Viruses. 2017;9:283. [CrossRef]
- Hutson CL, Lee KN, Abel J; et al. Monkeypox zoonotic associations: Insights from laboratory evaluation of animals associated with the multi-state US outbreak. Am J Trop Med Hyg. 2007;76:757–768. [CrossRef]
- Earl PL, Americo JL, Cotter CA; et al. Comparative live bioluminescence imaging of monkeypox virus dissemination in a wild-derived inbred mouse (Mus musculus castaneus) and outbred African dormouse (Graphiurus kelleni). Virology. 2015;475:150–158. [CrossRef]
- Falendysz EA, Londono-Navas AM, Meteyer CU; et al. Evaluation of monkeypox virus infection of black-tailed prairie dogs (Cynomys ludovicianus) using in vivo bioluminescent imaging. J Wildl Dis. 2014;50:524–536.
- Breman JG, Nakano JH, Coffi E; et al. Human poxvirus disease after smallpox eradication. Am J Trop Med Hyg. 1977;26:273–281. [CrossRef]
- Arita I, Henderson DA. Smallpox and monkeypox in non-human primates. Bull World Health Organ. 1968;39:277–283.
- Falendysz EA, Lopera JG, Lorenzsonn F; et al. Further assessment of monkeypox virus infection in gambian pouched rats (cricetomys gambianus) using in vivo bioluminescent imaging. PLoS Negl Trop Dis. 2015;9:e0004130. [CrossRef]
- Americo JL, Moss B, Earl PL. Identification of wild-derived inbred mouse strains highly susceptible to monkeypox virus infection for use as small animal models. J Virol. 2010;84:8172–8180. [CrossRef]
- Earl PL, Americo JL, Moss B. Genetic studies of the susceptibility of classical and wild-derived inbred mouse strains to monkeypox virus. Virology. 2015;481:161–165. [CrossRef]
- Hutin YJ, Williams RJ, Malfait P; et al. Outbreak of human monkeypox, democratic republic of Congo, 1996 to 1997. Emerg Infect Dis. 2001;7:434–438. [CrossRef]
- Doty JB, Malekani JM, Kalemba LN; et al. Assessing monkeypox virus prevalence in small mammals at the human-animal interface in the democratic republic of the Congo. Viruses. 2017;9:283. [CrossRef]
- Marennikova SS, Seluhina EM. Susceptibility of some rodent species to monkeypox virus, and course of the infection. Bull World Health Organ. 1976;53:13–20.
- Prier JE, Sauer RM. A pox disease of monkeys. Ann N Y Acad Sci 1960;85:951-9. [CrossRef]
- Wenner HA, Macasaet D, Kamitsuka PS, Kidd P. MonkeypoxI. Clinical, virologic and immunologic studies. Am J Epidemiol 1968;87:551-66. [CrossRef]
- Nakoune E, Lampaert E, Ndjapou SG et al. A Nosocomial Outbreak of Human Monkeypox in the Central African Republic. Open Forum Infect Dis. 2017;4:ofx168. [CrossRef]
- Durski KN, McCollum AM, Nakazawa Y et al. Emergence of Monkeypox - West and Central Africa, 1970-2017. MMWR Morb Mortal Wkly Rep. 2018;67:306-10. [CrossRef]
- Sklenovská N, Van Ranst M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front Publ Hlth. 2018;6:241. [CrossRef]
- Quiner CA, Moses C, Monroe BP et al. Presumptive risk factors for monkeypox in rural communities in the Democratic Republic of the Congo. PLoS ONE. 2017;12:e0168664. [CrossRef]
- Marennikova SS, Seluhina EM, Malceva NN, Cimiskjan KL, Macevic GR. Isolation and properties of the causal agent of a new variola-like disease (monkeypox) in man. Bull World Hlth Organ 1972;46:599–611.
- World Health Organization. Monkeypox. 2019. https://www.who.int/newsroom/factsheets/detail/monkeypox. Accessed 9 December 2019.
- Rimoin AW, Mulembakani PM, Johnston SC; et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc Natl Acad Sci U S A 2010; 107:16262–7. [CrossRef]
- Centers for Disease Control and Prevention. Human monkeypox— Kasai Oriental, Zaire, 1996–1997. MMWR Morb Mortal Wkly Rep 1997; 4614:304–7.
- Jezek Z, Grab B, Szczeniowski MV, Paluku KM, Mutombo M. Human monkeypox: Secondary attack rates. Bull World Health Organ 1988; 66:465–70.
- Hussain AN, Hussain F, Alam M, Cleri DJ. Smallpox treatment and management. 2019. https://emedicine.medscape.com/article/237229-treatment. Accessed 08 March 2021.
- World Population Review. Median age 2021. http://worldpopulationreview.com/countries/median-age. Accessed 22 January 2020.
- Levine RS, Peterson AT, Yorita KL, Carroll D, Damon IK, Reynolds MG. Ecological niche and geographic distribution of human monkeypox in Africa. PLoS ONE 2007; 2:e176. [CrossRef]
- Hutin YJ, Williams RJ, Malfait P; et al. Outbreak of human monkeypox, Democratic Republic of Congo, 1996 to 1997. Emerg Infect Dis 2001; 7:434–8. [CrossRef]
- Reynolds MG, Doty JB, McCollum AM, Olson VA, Nakazawa Y. Monkeypox re-emergence in Africa: A call to expand the concept and practice of One Health. Expert Rev Anti Infect Ther. 2019; 17:129–39. [CrossRef]
- Yinka-Ogunleye A, Aruna O, Ogoina D; et al. Reemergence of human monkeypox in Nigeria, 2017. Emerg Infect Dis 2018; 24:1149–51. [CrossRef]
- Guarner J, Johnson BJ, Paddock CD; et al.; Veterinary Monkeypox Virus Working Group. Monkeypox transmission and pathogenesis in prairie dogs. Emerg Infect Dis 2004; 10:426–31. [CrossRef]
- Bartlett, J. Monkeypox review. Medscape 2003. https://wwwnc.cdc.gov/eid/article/26/4/19%E2%80%901164_article. Accessed 08 March 2021.
- Simpson, K. , Heymann, D., Brown, C. S., Edmunds, W. J., Elsgaard, J., Fine, P.,... & Wapling, A. (2020). Human monkeypox–After 40 years, an unintended consequence of smallpox eradication. Vaccine, 38(33), 5077-5081. [CrossRef]
- Public Health England. Monkeypox diagnosed in England—First case of onward transmission. 2019. https://www.who.int/csr/don/01-october-2020-monkeypox-drc/en/#:~:text=WHO%20risk%20assessment,group%20of%20viruses%20as%20smallpox.
- Likos AM, Simmons SA; et al. A tale of two clades: Monkeypox viruses. J Gen Virol 2005; 86:1661–2672. [CrossRef]
- Whitehouse, E. R. , Bonwitt, J., Hughes, C. M., Lushima, R. S., Likafi, T., Nguete, B.,... & Reynolds, M. G. (2021). Clinical and epidemiologic findings from enhanced monkeypox surveillance in Tshuapa Province, Democratic Republic of the Congo during 2011–2015.
- World Health Organization. Monkeypox—Democratic Republic of the Congo. 2020. https://www.who.int/csr/don/01-october-2020-monkeypox-drc/en/. Accessed 08 February 2021.
- Lederman ER, Reynolds MG, Karem K, et al. Prevalence of antibodies against orthopoxviruses among residents of Likouala region, Republic of Congo: Evidence for monkeypox virus exposure. Am J Trop Med Hyg 2007; 77:1150–6. [CrossRef]
- Doshi RH, Guagliardo SAJ, Doty JB; et al. Epidemiologic and ecologic investigations of monkeypox, Likouala department, Republic of the Congo, 2017. Emerg Infect Dis 2019; 25:273–81. [CrossRef]
- Davi SD, Kissenkötter J, Faye M; et al. Recombinase polymerase amplification assay for rapid detection of monkeypox virus. Diagn Microbiol Infect Dis 2019; 95:41–5. [CrossRef]
- Li D, Wilkins K, McCollum AM; et al. Evaluation of the GeneXpert for human monkeypox diagnosis. Am J Trop Med Hyg 2017; 96:405–10. [CrossRef]
- World Health Organization. Outbreaks and emergencies bulletin. https://www.afro.who.int/healthtopics/disease-outbreaks/outbreaksand-other-emergencies-updates. Accessed 08 March 2021.
- Petersen BW, Kabamba J, McCollum AM; et al. Vaccinating against monkeypox in the Democratic Republic of the Congo. Antiviral Res 2019; 162:171–7. [CrossRef]
- Reynolds MG, McCollum AM, Nguete B, Shongo Lushima R, Petersen BW. Improving the care and treatment of monkeypox patients in low-resource settings: Applying evidence from contemporary biomedical and smallpox biodefense research. Viruses 2017; 9:380. [CrossRef]
- Damon, I. K. (2011). Status of human monkeypox: Clinical disease, epidemiology and research. Vaccine, 29, D54-D59. [CrossRef]
- McCollum, A. M., & Damon, I. K. (2014). Human monkeypox. Clinical infectious diseases, 58(2), 260-267.
- Yinka-Ogunleye, A., Aruna, O., Ogoina, D., Aworabhi, N., Eteng, W., Badaru, S., ... & Ihekweazu, C. (2018). Reemergence of human monkeypox in Nigeria, 2017. Emerging infectious diseases, 24(6), 1149. [CrossRef] [PubMed]
- Kalthan, E., Tenguere, J., Ndjapou, S. G., Koyazengbe, T. A., Mbomba, J., Marada, R. M.,... & Nakoune, E. R. (2018). Investigation of an outbreak of monkeypox in an area occupied by armed groups, Central African Republic. Medecine et Maladies Infectieuses, 48(4), 263-268. [CrossRef]
- Falcinelli, S. D., Chertow, D. S., & Kindrachuk, J. (2016). Integration of global analyses of host molecular responses with clinical data to evaluate pathogenesis and advance therapies for emerging and re-emerging viral infections. ACS infectious diseases, 2(11), 787-799. [CrossRef]
- Chen, N., Li, G., Liszewski, M. K., Atkinson, J. P., Jahrling, P. B., Feng, Z., ... & Buller, R. M. L. (2005). Virulence differences between monkeypox virus isolates from West Africa and the Congo basin. Virology, 340(1), 46-63. [CrossRef]
- Damon, IK. Status of human monkeypox: Clinical disease, epidemiology, and research. Vaccine. 2011;29:D54-D59. [CrossRef]
- Reynolds MG, Carroll DS, Karem KL. Factors affecting the likelihood of monkeypox’s emergence and spread in the post-smallpox era. Curr Opin Virol. 2012;2(3):335-43. [CrossRef]
- Oladoye, M. J. (2021). Monkeypox: A Neglected Viral Zoonotic Disease. Electronic Journal of Medical and Educational Technologies, 14(2), em2108. [CrossRef]
- McCollum AM, Damon IK. Human monkeypox. Clin Infect Dis. 2014 Jan;58(2):260-7. [PubMed] [Reference list].
- Petersen BW, Kabamba J, McCollum AM, Lushima RS, Wemakoy EO, Muyembe Tamfum JJ, Nguete B, Hughes CM, Monroe BP, Reynolds MG. Vaccinating against monkeypox in the Democratic Republic of the Congo. Antiviral Res. 2019 Feb;162:171-177. [CrossRef]
- Sklenovská N, Van Ranst M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front Public Health. 2018;6:241. [CrossRef]
- Reynolds MG, McCollum AM, Nguete B, Shongo Lushima R, Petersen BW. Improving the Care and Treatment of Monkeypox Patients in Low-Resource Settings: Applying Evidence from Contemporary Biomedical and Smallpox Biodefense Research. Viruses. 2017 Dec 12;9(12). [CrossRef]
- Quiner CA, Moses C, Monroe BP; et al. Presumptive risk factors for monkeypox in rural communities in the Democratic Republic of the Congo. Yang Y, ed. PLoS ONE. 2017; 12(2): e0168664. [CrossRef]
- Petersen, E., Kantele, A., Koopmans, M., Asogun, D., Yinka-Ogunleye, A., Ihekweazu, C., & Zumla, A. (2019). Human monkeypox: Epidemiologic and clinical characteristics, diagnosis, and prevention. Infectious Disease Clinics, 33(4), 1027-1043. [CrossRef]
- Bass J, Tack DM, McCollum AM; et al. Enhancing health care worker ability to detect and care for patients with monkeypox in the Democratic Republic of the Congo. Int Health 2013;5:237–43. [CrossRef]
- Reynolds MG, McCollum AM, Nguete B, Shongo Lushima R, Petersen BW. Improving the care and treatment of monkeypox patients in low-resource settings: Applying evidence from contemporary biomedical and smallpox biodefense research. Viruses 2017;9:E380. [CrossRef]
- World Health Organization. R&D blueprint: List of blueprint priority diseases. Geneva, Switzerland: World Health Organization; 2018.
- Shiferaw ML, Doty JB, Maghlakelidze G; et al. Frameworks for preventing, detecting, and controlling zoonotic diseases. Emerg Infect Dis 2017;23. [CrossRef]
- Durski, K. N., McCollum, A. M., Nakazawa, Y., Petersen, B. W., Reynolds, M. G., Briand, S.,... & Khalakdina, A. (2018). Emergence of monkeypox—West and central Africa, 1970–2017. Morbidity and mortality weekly report, 67(10), 306. [CrossRef]
Figure 3.
different possible modes of monkeypox virus transmission into humans.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



