
Submitted:
25 February 2024
Posted:
26 February 2024
You are already at the latest version
Abstract
Vitamin D3 deficiency is a global phenomenon, which can be coped with supplementation and food fortification. However, vitamin D3 bioaccessibility may depend on factors, such as matrix composition and interactions throughout the gastrointestinal tract. This research focused on the effect of different matrices on vitamin D3 content during digestion, and the effect of pH on its bioaccessibility. The INFOGEST protocol was employed to simulate digestion. Three different types of commercial supplements, two foods naturally rich in vitamin D3, and three fortified foods were investigated. High-Performance Liquid Chromatography was used to determine the vitamin D3 initial content in supplements and foods, as well as after each digestion stage. Results indicated that foods exhibited higher bioaccessibility indices compared to supplements, and a higher percentage retention at the end of the gastric phase. The pH study revealed a positive correlation between increased gastric pH and the corresponding content of vitamin D3. Interestingly, exposing the matrix to low pH during the gastric phase resulted in an increased intestinal content of D3. Vitamin D3 is more bioaccessible from foods than supplements, and its bioaccessibility is susceptible to changes in gastric pH. Fasting conditions (i.e. gastric pH=1) enhances vitamin’s bioaccessibility.
Keywords:
in vitro digestion
; gastric pH
; vitamin D3
; bioaccessibility
; Infogest
1. Introduction
Vitamin D is a biologically active compound found mainly in the forms of ergocalciferol (vitamin D 2), cholecalciferol (vitamin D3) and 25-hydroxycholecalciferol (25(OH)D3) (Scheme 1). Vitamin D3 is a micronutrient, essential for maintaining the overall health and wellness of humans, as it is associated with bone health and immune system boosting [1]. It plays a key role in calcium absorption [2] and has been proposed to act against cancer cell growth [3]. In addition to that, vitamin D3 has been linked with lower risk of developing multiple sclerosis and rheumatoid arthritis, as well as type 1 and type 2 diabetes mellitus [4]. The protective effect of vitamin D3 against SARS-CoV-2 has also been examined and showed that the vitamin can potentially prevent severe illness [5]. Vitamin D3 can be photosynthesized through skin exposure to ultraviolet radiation [6] or ingested through foods and supplements. However, vitamin D3 deficiency is a global concern [7]. Supplementation, as well as consumption of foods rich in vitamin D3 can aid to cope with this phenomenon.
Supplements are available in different forms, such as tablets, capsules or oil-emulsified drops [9]. Vitamin D3 in supplements may be encapsulated in microcapsules, micelles or liposomes to increase its bioavailability [10,11,12]. A meta-analysis of several clinical studies concluded that vitamin D3 bioavailability is better in oil vehicles (capsules or liquid) than in powder tablets (cellulose or lactose) or ethanol [13]. However, another study testing oil and tablets, showed that they were equally efficient in raising serum 25-hydroxyvitamin D, though the authors speculated that these results may be due to the timing of measuring serum concentrations [14].
Foods can either naturally contain vitamin D3, as in fish and eggs, or be fortified with the vitamin, such as milk, orange juice, plant oils, flour, bread and cereals. Different food matrices can result in different bioaccessibility and bioavailability of the vitamin. The structure of the food matrix, the amount and type of dietary lipids (chain length, degree of saturation), as well as the dietary fibres can affect the final bioavailability [8,15]. Foods fortified with vitamin D3 have demonstrated comparable effectiveness to supplements in increasing serum 25(OH)D3 levels [16,17]. It has also been suggested that vitamin D3 absorption is protein-mediated at low concentrations, as those found in dietary sources, while in high pharmacological concentrations the absorption mechanism shifts to passive diffusion [18]. The differences encountered between different foods and supplements indicate that research on various matrices is necessary.
When the vitamin D3-containing matrix is ingested, it undergoes physiological conditions encountered during digestion, including enzyme activity and pH fluctuations. The digestive process is initiated in the mouth with amylase catalysing starch hydrolysis, followed by the stomach, where proteins and lipids are hydrolysed by pepsin and gastric lipase, forming gastric chyme [19]. As gastric chyme moves to the intestine, pancreatin further breaks down the food with assistance from intestinal peristaltic movements. Pepsin and trypsin may play a role in releasing vitamin D3 from its food matrix by disrupting the binding of proteins to vitamin D3. Digestive enzymes in the duodenum, including amylase, lipase, and protease, continue to liberate vitamin D3 from its food matrix [15]. The released vitamin D3 integrates into mixed micelles formed during digestion, consisting of phospholipids, cholesterol, lipid digestion products, and bile salts [8,15,20]. The composition of mixed micelles is influenced by the types of lipids present during digestion [21,22].
The pH variation is another critical factor that might impact the final bioaccessibility of vitamin D3. Lower pH has been shown to lead in decreasing stability of vitamin D3 [23]. Vitamin D3 is isomerized to isotachysterol at acidic pH [24]. Encapsulation of the vitamin has been proposed to protect it from degradation in different pH values [25]. Many encapsulation techniques and materials, such as β-lactoglobulin [26], ovalbumin-pectin nanocomplexes [27], gum arabic, maltodextrin, whey protein concentrate and soy isolate protein [28] has been used to produce systems that are stable in different pH conditions [25]. Food intake alters the basal gastric pH. Different composition of foods result in varying gastric pH values, which may take up to 3 hours to return to basal levels [29]. Consequently, supplements taken after different foods or during fasting may encounter different gastric pH conditions. The timing of supplement intake following food consumption can also lead to variations in the encountered pH values [30].
The aim of this research was to investigate the influence of diverse matrices (including natural foods with vitamin D3 with or without heat treatment, fortified foods, and supplements) on the fate of vitamin D3 at different stages along the gastrointestinal (GI) tract. Using the INFOGEST protocol, these matrices underwent in vitro digestion and vitamin content was determined at different stages of the protocol to evaluate its bioaccessibility. Additionally, the study investigated the effect of gastric pH by testing four different pH values to simulate conditions during fasting and various food consumption. The findings from this research contribute to a deeper understanding on how each digestion stage influences vitamin D3 and the impact of gastric pH variations on its bioaccessibility.
2. Results
Foods naturally containing vitamin D3 (eggs, salmon), fortified foods (milk, cereals, sour cherry juice) and supplements (tablets, capsules containing an oil-based emulsion, oil-based liquid drops) were subjected to in vitro digestion (INFOGEST protocol) [31]. High Performance Liquid Chromatography (HPLC) was used to determine vitamin D3 content and losses in each stage. Eggs and salmon were thermally processed till core temperature reached 70 oC [32] before subjected to digestion. The effect of gastric pH variation was also examined by subjecting vitamin D3 liquid oil-based supplement, to four different gastric pH values.
2.1. Vitamin D3 content of foods and supplements
The detected content of the vitamin for the tablet, capsule and liquid supplement was 20.99±1.17 μg/tablet, 20.24±0.78 μg/capsule and 95.93±0.64 μg/ml, respectively (Figure 1, t=0 min). The liquid supplement had the highest content followed by the tablet and capsule, which had similar content.
Fortified foods had a higher vitamin content than natural foods, as it was expected (Table 1). Between the two natural foods examined, salmon had a higher vitamin D3 content than eggs, as seen in other studies [33]. HPLC analysis of egg and salmon showed a second peak, before vitamin D3’s peak (Figure S3, S4 - Supplementary file), which may correspond to the hydroxylated form 25(OH)D3 [34]. This form is naturally present in these foods [35,36].
2.2. Vitamin D3 bioaccessibility
2.2.1. Vitamin D3 Bioaccessibility from Supplements
Bioaccessibility Index (BI) shows the amount of vitamin D3 remaining after digestion processes, which is available for absorption and was calculated according to equation (2). In Figure 1, the remaining detected content of vitamin D3 is presented. Among the supplements, the liquid one had the highest bioaccessibility followed by the capsule and the tablet (Figure 2).
At the end of the gastric phase, vitamin D3 in the tablet, capsule and liquid supplement was reduced by 55%, 41% and 43%, respectively. Further losses at the end of the intestinal phase were recorded (75% and 20% for the tablet and capsule). On the contrary, in the case of the liquid supplement, there appears to be a 25% increase in vitamin D3 content in the intestinal stage compared to the gastric stage. Greater losses were observed for the tablet at each stage. The reduction in vitamin content during the intestinal phase was more significant for the tablet compared to the gastric content. In contrast, for the capsule, the reduction was more pronounced for the gastric content compared to the initial.
2.2.2. Vitamin D3 Bioaccessibility from Foods
Vitamin detected content in each digestion step of foods, as well as the corresponding bioaccessibility, are presented in Table 1. Sour cherry juice, egg, salmon and cereals had BIs around 1. Milk had the lowest BI (0.40), which is rather low in comparison with the other samples. Foods, except for milk, exhibited higher BIs than supplements, as shown in Figure 2.
Thermal processing of egg and salmon seemed to decrease vitamin D3 content by 43% and 25%, respectively (Table 1).
In the natural food samples vitamin D3 content seemed to increase after gastric step. Vitamin D3’s content in the gastric chyme for the egg and salmon samples was increased by 33% and 48%, respectively, compared to the initial concentration. The intestinal content compared to the gastric content was decreased by 29% for eggs and by 26% for salmon.
The results for the fortified food samples showed 60% and 5% decrease in vitamin content in the gastric phase for milk and cereals, respectively. For the sour cherry juice, there was a slight increase (4%) in the gastric content compared to the initial content. For the milk samples, there was no significant difference between the gastric and intestinal content. Cereals and sour cherry juice showed an increase in the intestinal content (10% and 3%, respectively).
Gastric step seemed to have a greater impact in vitamin D3 for all food samples, either by increasing or decreasing the content.
2.3. Gastric pH effect on vitamin D3 Bioaccessibility
Four different pH values were simulated to investigate the effect of the gastric stage pH on vitamin D3 bioaccessibility. The sample tested was the liquid supplement, as it was the most bioaccessible among the supplements. The gastric and intestinal contents of the vitamin, as well as calculated BIs are presented in Table 2.
There was a profound effect of the gastric digestion step on the vitamin content. Vitamin’s decrease during this stage ranged from 44 to 58%. D3’s gastric content was the highest for pH 7 and the lowest for pH 1 (p < 0.05). Even at pH 7 there was a 44% decrease in vitamin D3 content. This suggests that vitamin D3 stability might be affected not only by pH, but also by the presence of the other components of the gastric fluids.
At every pH level, there was an increase in vitamin D3 content at the end of intestinal digestion phase, except for pH 7. The percentage increases were 78%, 26%, and 10% for pH 1, 3, and 5, respectively. The lower the pH of the gastric phase, the higher the increase in vitamin D3 content in the intestinal phase. On the contrary, when the sample was exposed to gastric pH 7, a notable 23% reduction in vitamin D3 content was observed, from 54 μg/ml after stomach phase to 41 μg/ml after intestinal phase. Exposure to the i.e., lowest pH value of 1 resulted in the highest BI, while pH 7 led to the lowest BI. pH values 3 and 5 had similar BIs.
To determine the possible effect of the carrier’s oxidation (sunflower oil) in vitamin D3 content in each digestion stage, sunflower seed oil oxidation was investigated for two different pH values (Figure 3). Primary oxidation was more profound for pH 3 than pH 7. Primary oxidation products concentration peaked during the gastric phase at 75 min for pH 3 and at 135 min for pH 7. Even though oxidation at pH 7 was significantly delayed during gastric phase, it reached the same peak concentrations of oxidation products at pH 3 (p ≥ 0.05). Secondary oxidation peaked during the intestinal phase of digestion, when primary oxidation products had the lowest concentrations (195min). The concentration of secondary oxidation products was greater for pH 7, however the difference was not statistically significant (p ≥ 0.05).
3. Discussion
Supplements and foods containing vitamin D3, either naturally or fortified, can be used to battle vitamin D3 deficiency [37,38]. When ingested, vitamin D3 is exposed to the GI tract conditions, which can affect the stability of the vitamin and its final bioaccessibility.
Of the three commercial supplements, the oil-based liquid drops had the highest vitamin content. In vitro digestion of supplements showed a higher BI for the oil-based liquid drops, followed by the capsule and the tablet, which is in accordance with previous studies testing vitamin D3 bioavailability [13]. Vitamin D3 is a lipophilic vitamin, which is more stable in oil vehicles [23].
Tablets exhibited higher gastric losses compared to capsules and liquid supplements, with the intestinal stage exerting a more significant impact on the vitamin content of the tablet. Conversely, for capsules, the gastric stage had a more pronounced effect. In the case of the liquid supplement, there was a decrease in content from the initial to the gastric stage, followed by an increase from the gastric to the intestinal stage. This phenomenon may be attributed to the enhanced release of the vitamin from its matrix during this stage, potentially facilitated by the action of pancreatin on the oil matrix (sunflower oil). A similar behavior was noted for carotenoids, as they were undetected in the gastric stage but present in measurable concentrations during the intestinal stage. The authors attributed this outcome partly to the presence of pancreatin in the intestinal stage [39]. Additionally, the antioxidant capacity of α-tocopherol present as an additive in the liquid supplement may have protected vitamin D3 from degradation during in vitro digestion [40]. Differences in the initial concentrations among supplements might also contribute to the different behavior during digestion. Previous research has shown that the BI of omega-3 supplements can be dependent on the initial concentration of the lipophilic components [41].
Heat treatment can adversely affect vitamin D3 content of foods by decreasing it, depending on the method of heating [42,43]. In our study, thermal processing of egg and salmon decreased vitamin D3 content, with egg being more affected than salmon (42% vs 25% decrease, respectively). Vitamin D3, as a lipophilic vitamin, may be better protected in salmon than eggs, as salmon has a greater lipid content. This can result in a greater retention of vitamin D3 in salmon after thermal processing. Vitamin D3 converts to pre-vitamin D3 reversibly when heated, especially in higher temperatures [44]. The reversibility of this conversion may be the explanation of the increase observed in gastric step of both eggs and salmon, after the heat treatment.
Eggs and salmon had lower vitamin D3 content than fortified foods, as it was expected. Salmon had higher content than eggs, as shown in other studies [33]. From the fortified foods, milk had the higher content, followed by the cereals and sour cherry juice. Foods exhibited higher BIs than supplements, apart from milk which had a rather low BI, closer to those of supplements. Previous research has shown that naturally formulated vitamin D3 extracted from agricultural products had higher bioaccessibility than synthetic vitamin D3 [45]. An investigation on vitamin E bioaccessibility revealed that the incorporation of vitamin E-loaded Pickering emulsions into foods led to an increased bioaccessibility of the vitamin, surpassing the bioaccessibility observed when the emulsion was digested alone. This observation was attributed to the natural presence of macronutrients in foods [46]. These findings are in accordance with our results concerning the better bioaccessibility of vitamin D3 from foods.
In natural foods, the gastric phase showed a beneficial impact, leading to an increase in vitamin D3 content, while intestinal phase adversely affected the vitamin’s content. The observed increase during the gastric step may be due to the release of the vitamin from the food matrix, which made it available for detection. The percentage increase in gastric step was higher than percentage decrease in intestinal step, which indicates that the gastric step had a greater effect in vitamin D3 content. The intrinsic antioxidant mechanisms of fish tissue may have acted as a protective agent for vitamin D3. Greater lipid oxidation may cause degradation of the vitamin [47,48]. Enzymatic antioxidants in fish, such as glutathione peroxidase (GPx) can reduce lipid peroxides [49], thus protecting vitamin D3 by decreasing lipid oxidation. Vitamin C and vitamin E, which act as antioxidants, are also present in fish tissue [50]. These vitamins may have also functioned as protective agents against vitamin D3 degradation. Regarding eggs, their digestion causes the release of amino acids and antioxidant peptides, which raise their anti-oxidative capacity, while preserving the bioaccessibility of egg’s naturally occurring antioxidants, zeaxanthin, and lutein [51,52,53]. That phenomenon may have aided in vitamin D3 protection present in eggs during digestion.
Among the fortified foods, milk exhibited a notable reduction in vitamin D3 content from the initial to gastric step. However, the decrease from the gastric to intestinal step was comparatively minimal and lacked statistical significance. This suggests that, like natural foods, the gastric step had a more pronounced impact on milk. Previous studies have shown low bioaccessibility of vitamin D3 from milk [54,55]. Bioaccessibility of vitamin D3 in milk has been found to vary in different types of milk (skim, partially defatted, whole and infant formula milk) [54], indicating the possible role not only of fat content, but also the type of fats present in the matrix. The low bioaccessibility may also be attributed to the interference of calcium with vitamin D3 absorption. Previous research in fortified plant-based milk has shown that calcium forms insoluble calcium soaps that trap the vitamin [56]. Similar results were obtained for water-in-oil-in-water emulsions, where vitamin D3 bioaccessibility was reduced in the presence of calcium [57]. Furthermore, vitamin D3 can bind to milk proteins, such as β-lactoglobulin and β-casein, in both acidic and alkaline conditions with different binding affinities [58]. This may also have resulted in decreased bioaccessibility, as vitamin D3 may not be able to be separated from the milk proteins during saponification and extraction.
Vitamin D3 content in cereals decreased to the gastric stage compared to the initial content, while for the sour cherry juice a slight increase after the gastric stage was observed. After the intestinal stage, there was an increase in content compared to gastric content for both foods. A study on vitamin D3 bioaccessibility from test meals showed that semolina meal had the highest bioaccessibility [59], though not as high as in our study. The cereals used in this study contained whole wheat flour and corn semolina, which are high in antioxidants [60],[61]. A study on in vitro digestion of juice extracts found that the content of some phenolic acids and flavonoids increased either during the gastric stage or the intestinal stage, as well as for some monosaccharides and oligosaccharides, which was attributed to the increased release during digestion [62]. The antioxidant capacity of these compounds during digestion was maintained at elevated levels. Antioxidants have been shown to protect vitamin D3 against degradation [40,63]. The behavior of the vitamin during cereals and juice digestion can be attributed to the increased release of vitamin D3 during digestion as well as the antioxidant capacity of phenolic acids and flavonoids present in cereals and juice, which may have acted as protective agents against vitamin D3 degradation.
Regarding the effect of pH on vitamin D3 liquid supplement, there were two main observations: in the gastric phase, the lower the pH, the higher the decrease in D3. On the other hand, exposure to lower pH at the gastric phase led to higher content of vitamin D3 in the intestinal phase, i.e. higher when the matrix was exposed to pH 1 and lower when exposed to pH 7. A study on vitamin D3 stability in aqueous solution found that lower pH had a negative effect on its stability [23]. Stability and content of vitamin D3 in GI tract may be affected by lipid oxidation, hydrolysis and enzyme action. Metal ions, present in the gastric chyme, can also destabilize vitamin D3, as its degradation may be catalyzed by them [23]. In this case, the matrix of the supplement consists of sunflower seed oil, which is not affected by pepsin present in the gastric phase, as pepsin is a proteolytic enzyme [64]. The decreased content at low pH values can, also, be attributed to the faster primary oxidation of sunflower seed oil in lower pH values, as lipid oxidation can affect vitamin D3 by promoting its degradation [47,48]. Intestinal content is affected more from gastric pH changes. Lower pH leads to greater lipid hydrolysis and release of free fatty acids, which are mixed micelles’ structural components [20]. More free fatty acids can form more mixed micelles available to incorporate vitamin D3 that may lead to better bioaccessibility. A study found that sunflower oil hydrophilicity increases as the pH decreases [65]. Decreased hydrophobicity may affect mixed micelles formation regarding their size, shape and stability, which by extension can affect the vitamin’s bioaccessibility. The increased content of vitamin D3 in intestine could also be attributed to the isomerization processes taking place during different pH values. Vitamin D3 is isomerized to isotachysterol under acidic conditions [44], as well as lumisterol and tachysterol [34]. The isomerization to tachysterol and lumisterol can be reversed and pre-vitamin D3 is formed [66], which is then converted to vitamin D3. The lower pH in gastric stage may have caused the vitamin’s isomerization (Figure S5 - Supplementary file). As the gastric pH increases the isomerization processes can be of smaller magnitude. This phenomenon in combination with the lipid oxidation may explain the decrease in D3 content in gastric phase, as well as the corresponding increase observed in the intestinal stage. However, it is important to exercise caution when interpreting these findings, as vitamin D3 is prone to isomerization and degradation under diverse conditions. This makes its stability in food products potentially uncertain and its analysis challenging. Early studies suggest that factors like substrate/reactant ratio, solvents, and time can have varying impacts on the generation pathway of vitamin D isomers [44].
This research highlighted that Vitamin D3 is more bioaccessible from foods than supplements, and its bioaccessibility is susceptible to changes in gastric pH. Even though exposure to low gastric pH values i.e. pH=1 led to lower detected vitamin D3 content, the corresponding intestinal content was significantly increased. The mechanism(s) behind this phenomenon should be further explored. It is crucial to comprehend the behavior and stability of vitamin D3 during digestion, as its effectiveness when consumed through foods or supplements relies on its bioaccessibility. Understanding how vitamin D3 interacts with other components in the digestive system and under GI conditions is essential for developing supplements and foods that optimize its stability and absorption.
4. Materials and Methods
4.1. Chemicals and Reagents
Bile bovine dried, potassium chloride (KCl), calcium chloride (CaCl2(H2O)2) and magnesium chloride (MgCl2(H2O)6) were purchased from Merck & Co. (New Jersey, NJ, USA). Sodium chloride (NaCl), sodium sulfate (Na2SO4), potassium dihydrogen phosphate (KH2PO4), potassium hydroxide (KOH), hydrochloric acid 37% (HCl), methanol (CH3OH) and ethanol (C2H5OH) were purchased from Chem-Lab NV (Zedelgem, Belgium). Diastase (α-amylase, malt diastase), porcine pepsin, pancreatin, and ammonium carbonate (NH4)2CO3 were purchased from Central Drug House Ltd. (New Delhi, India). Sodium hydroxide (NaOH) was purchased from Lach-Ner Ltd. (Neratovice, Czech Republic). Ascorbic acid (vitamin C, C6H8O6) was purchased from Sigma-Aldrich (Buchs, Switzerland). Hexane (H3C(CH2)4CH3) was purchased from Avantor Performance Materials (Radnor, Pennsylvania, USA). Vitamin D3 standard was purchased from Carl Roth GmbH + Co. KG (Karlsruhe, Germany). All the chemicals and reagents used in this study were of analytical or HPLC grade. The food samples tested were purchased from local vendors, while supplements were purchased from local pharmacies.
4.2 Digestion Procedure
Digestion was simulated in vitro using INFOGEST protocol [31]. Enzyme activity must be determined for each enzyme used. In this study, amylase (mouth), pepsin (stomach) and pancreatin (intestine), as well as bile bovine, were used. The activity for enzymes not given by the manufacturer, was calculated according to the protocol. Simulated digestion fluids were prepared according to the protocol, containing KCl, KH2PO4, NaCl, MgCl2(H2O)6, (NH4)2CO3, HCl, Cacl2(H2O)2. CaCl2(H2O)2 was added immediately before use in each step due to precipitation issues.
The samples used for the digestion experiments were 3 different types of supplements (tablets, capsules containing an oil-based emulsion, oil-based liquid drops), naturally containing vitamin D3 foods (eggs, salmon), and fortified foods (milk, cereals, sour cherry juice).
For each food, 5 g were used in the first step. For the tablet and capsule an amount corresponding to 1200 IU was used, while for the liquid supplement 5000 IU were used (diluted with water to 2 ml final volume). Solid foods were diluted and minced to achieve a paste-like consistency. Thermal processing (70 oC core temperature for 15 s) of eggs and salmon was conducted by heating the samples in a water bath [32]. Gastric pH effect experiments were conducted using the supplement with the highest bioaccessibility, as it was determined from the first round of experiments.
4.2.1. Oral Phase
Firstly, the amount of sample was weighted and simulated salivary fluid (SSF) 1.25x was added. Distilled water was added to reach 1x concentration of SSF. If the sample contained starch, amylase (75 U/ml) was also added. The sample was stirred for 2 min at 37 oC (ONE 14 - SV 1422, memmert, Germany).
4.2.2. Gastric Phase
Simulated gastric fluid (SGF) 1.25x, pepsin (2000 U/ml) and distilled water were added to the mixture at the end of the oral phase. pH adjustment to 3 (protocol value), 1, 4 or 7 (for the pH study) was achieved by adding HCl 1 M (pH 211, HANNA instruments, Woonsocket, RI, USA). The sample was gently shaken for 2 h at 37 oC (ONE 14 - SV 1422, memmert, Germany).
4.2.3. Intestinal Phase
Simulated intestinal fluid (SIF) 1.25x and bile salts (10 mM) were added to the gastric chyme. The mixture was stirred for 30 min at 37 oC until complete bile solubilization. Afterwards, pancreatin (100 U/ml trypsin activity) was added, the pH was adjusted to 7 (NaOH 1 M) (pH 211, HANNA instruments, USA) and distilled water was added. The sample was stirred for 2h at 37 oC (ONE 14 - SV 1422, memmert, Germany).
All samples were stored at -20 oC until further analysis.
4.3. Vitamin D3 Isolation
4.3.1. Samples with Saponification
The isolation method used was based on Yanhai et al. [67], with some modifications. Raw and thermally processed food were diluted in appropriate amount of water. The samples from digestion steps were not diluted. To each sample, 15 g/L solution of vitamin C in ethanol in 1:2 ratio (v/v) and 1.25 g/ml solution of KOH in water in 2:1 ratio (v/v) were added. The sample was heated at 60 oC for 45 min with continuous stirring to achieve lipid saponification. Afterwards, the sample was cooled in room temperature and underwent 2 subsequent extractions with hexane in 1:2 ratio (v/v). For each extraction, hexane was added to the sample and vortexed for 5 min. Then, the mixture was placed in a separating funnel until complete phase separation. Water phase was removed. Hexane phases from the two extraction steps were collected and combined. Na2SO4 was added to remove any residual water. To remove Na2SO4, the sample was filtered through filter paper (retention 10-15 μm). Subsequently, the sample was placed in a rotary evaporator at 40 oC (Laborota 4003, Heidolph, Germany) and evaporated to dryness. Solids were redissolved with 2 ml methanol and filtered through 0.22 μm filter (PTFE).
4.3.2. Samples without Saponification
For the supplements, the isolation of vitamin D3 was conducted as follows. The capsule and tablet were diluted with 5 ml of water. The liquid supplement was used undiluted. Methanol was added to the samples at 1:2 (v/v) ratio, vortexed for 2-3 min and placed in an ultrasonic bath (LBS1 10Lt, FALC instruments, Italy) for 10 min. Then, the mixture was vortexed again for 2-3 min and centrifuged at 2.938 xg (unicen 21, Ortoalresa, Spain) for 15 min to achieve complete phase separation. The organic phase was collected and evaporated to dryness (40 oC, Laborota 4003, Heidolph, Germany). Solids were redissolved in 2 ml methanol and filtered through 0.22 μm filter (PTFE).
Juice and digestion fractions of juice and supplements were extracted twice with hexane. The procedure followed was as described in the previous section (4.3.1).
4.4. High Performance Liquid Chromatography (HPLC)
Vitamin D3 concentration was determined using HPLC with UV detector (KNAUER 1200 system, Germany). The column used for the separation was Eurospher II 100-5 C18A (250 × 4 mm). The mobile phase was HPLC grade methanol and 0.1% formic acid with constant flow rate at 1 ml/min and 25 oC. The injection volume was 20 μL. The UV detector was set to 265 nm wavelength. Vitamin D was eluted at 4.8-4.9 min.
Vitamin D3 concentration in each sample was determined based on the standard curve. The standard curve was constructed using vitamin D3 standard (Figure S1, S2 - Supplementary file). Different concentrations of the standard in the range of 5 to 30 ppm were analysed in the HPLC system to determine the corresponding peak areas. The limit of detection (LOD) was 0.05 ppm, and the limit of quantification (LOQ) was 0.17 ppm (Tables S1, S2 – Supplementary file).
Recovery was determined by spiking raw foods and supplements with a known amount of vitamin D3 standard and analysing the sample. Recovery was calculated according to the following formula:
where is the peak area of the spiked sample, is the peak area of the unspiked sample and is the peak area of vitamin D3 standard, which was used for spiking the sample.
All values in Tables and Figures are corrected based on the recovery of each sample.
4.5. Bioaccessibility Index
Vitamin D3 bioaccessibility index (BI) was calculated using the following formula:
Where and are the amounts of vitamin D3 before and after digestion [68].
4.6. Oxidation Measurement
4.6.1. Peroxide Value
Peroxide value measurement was performed as described by Richards et al. [69], with some modifications. In each sample, 500 ppm BHT was added to stop the oxidation process and vortexed to achieve homogenization. 10 ml of CHCl3-CH3OH (2:1 v/v) were added to 1 gram of the sample. 1.5 ml of NaCl (0.5%) was added and the samples were vortexed and centrifuged at 2.798 xg (unicen 21, Ortoalresa, Spain) for 10 min at ambient temperature. The lower phase of CHCl3 was collected and CHCl3-CH3OH (2:1 v/v) was added until 10 ml final volume was reached. 25 μL of NH4SCN solution (30% w/v) and 25 μL of freshly prepared FeCl2 solution (0.66% w/v) were added and the mixture was vortexed for 2-4 s. A proper amount of the sample was transferred to a Quartz cell and the absorbance was measured in a spectrometer (uniSPEC 2 UV/VIS-Spectrometer, LLG, Germany) at 500 nm. 10 ml of CHCl3-CH3OH (2:1 v/v) was used as blind. The oxidation products were expressed in mmol/kg of lipid phase using a standard curve formed with cumene hydroperoxide solutions [70,71,72].
4.6.2. Thiobarbituric Acid Method (TBARS)
The TBARS method was performed according to Lemon [73], with some modifications. 1.5 grams of the sample were transferred to a test tube containing 5 ml of TCA (7.5% w/v) and vortexed. The mixture was centrifuged for 30 min at 2.798 xg (unicen 21, Ortoalresa, Spain). A 2 ml aliquot was mixed with 2 ml of TBA solution (0.02 M). The mixture was heated in a water bath for 40 min at the constant temperature of 100 oC. Samples were then cooled down to room temperature under running tap water and transferred to a Quartz cell to measure the absorbance (uniSPEC 2 UV/VIS-Spectrometer, LLG, Germany) at 532 nm. TBA:TCA solution (1:1 v/v) was used as blind. The oxidation products were expressed as MDAeq (μmol/l) with the help of the standard curve constructed using TEP solutions.
4.7. Statistical Analysis
Three independent digestion experiments (n=3) were conducted, and the experimental results were expressed as means ± standard deviations. The Minitab 21 Statistical Software (Minitab LLC, State College, PA, USA) was used to statistically process the data by carrying out a one-way ANOVA with Fisher’s test for means comparison. Differences were considered significant at p < 0.05.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Vitamin D3 standard curve; Figure S2: Vitamin D3 standards for standard curve; Figure S3: Raw salmon sample spiked with vitamin D 3; Figure S4: Raw egg sample spiked with vitamin D3; Figure S5: Chromatograph of liquid supplement after gastric digestion at pH 1. (A), (B) and (C) may be isomers of vitamin D3, produced during digestion due to acidic degradation.
Author Contributions
Conceptualization, E.P. and P.V.; methodology, E.P. and P.V; software, E.P. and P.V.; validation, E.P. and P.V.; formal analysis, E.P. and P.V.; investigation, E.P. and P.V.; resources, E.P. and P.V.; data curation, E.P. and P.V.; writing—original draft preparation, E.P.; writing—review and editing, E.P. and P.V.; visualization, E.P. and P.V.; supervision, P.V.; project administration, P.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Ministry of Agriculture, Program for Agricultural Development, ESPA 2014-2020, Submeasure 16.1 and 16.2, grant number Μ16ΣΥΝ-00807
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available upon request to corresponding author: pkvareltzis@cheng.auth.gr.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Combs, G. F.; McClung, J. P. Sources of the Vitamins. In The Vitamins; Elsevier, 2017; pp. 501–530. [Google Scholar]
- Janoušek, J.; Pilařová, V.; Macáková, K.; Nomura, A.; Veiga-Matos, J.; Silva, D. D. da; Remião, F.; Saso, L.; Malá-Ládová, K.; Malý, J.; Nováková, L.; Mladěnka, P. Vitamin D: Sources, Physiological Role, Biokinetics, Deficiency, Therapeutic Use, Toxicity, and Overview of Analytical Methods for Detection of Vitamin D and Its Metabolites. Crit Rev Clin Lab Sci 2022, 59, 517–554. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J. Cellular and Molecular Effects of Vitamin D on Carcinogenesis. Arch Biochem Biophys 2012, 523, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Khazai, N.; Judd, S. E.; Tangpricha, V. Calcium and Vitamin D: Skeletal and Extraskeletal Health. Curr Rheumatol Rep 2008, 10, 110. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Li, X.; Liu, W.; Xiao, Y.; Tang, H.; Wu, Y.; Xiong, Y.; Gao, S. The Role of Vitamin D in the Prevention and Treatment of SARS-CoV-2 Infection: A Meta-Analysis of Randomized Controlled Trials. Clinical Nutrition 2023, 42, 2198–2206. [Google Scholar] [CrossRef] [PubMed]
- Bendik, I.; Friedel, A.; Roos, F. F.; Weber, P.; Eggersdorfer, M. Vitamin D: A Critical and Essential Micronutrient for Human Health. In Frontiers in Physiology; Frontiers Research Foundation; p. 2014.
- Cui, A.; Zhang, T.; Xiao, P.; Fan, Z.; Wang, H.; Zhuang, Y. Global and Regional Prevalence of Vitamin D Deficiency in Population-Based Studies from 2000 to 2022: A Pooled Analysis of 7.9 Million Participants. Front Nutr 2023, 10, 1070808. [Google Scholar] [CrossRef] [PubMed]
- Borel, P.; Caillaud, D.; Cano, N. J. Vitamin D Bioavailability: State of the Art. Crit Rev Food Sci Nutr 2015, 55, 1193–1205. [Google Scholar] [CrossRef] [PubMed]
- Traub, M. L.; Finnell, J. S.; Bhandiwad, A.; Oberg, E.; Suhaila, L.; Bradley, R. Impact of Vitamin D3 Dietary Supplement Matrix on Clinical Response. J Clin Endocrinol Metab 2014, 99, 2720–2728. [Google Scholar] [CrossRef]
- Fox, C. B.; Kim, J.; Le, L. V.; Nemeth, C. L.; Chirra, H. D.; Desai, T. A. Micro/Nanofabricated Platforms for Oral Drug Delivery. Journal of Controlled Release 2015, 431–444. [Google Scholar] [CrossRef]
- Joye, I. J.; Davidov-Pardo, G.; McClements, D. J. Nanotechnology for Increased Micronutrient Bioavailability. Trends Food Sci Technol 2014, 40, 168–182. [Google Scholar] [CrossRef]
- Šimoliūnas, E.; Rinkūnaitė, I.; Bukelskienė, Ž.; Bukelskienė, V. Bioavailability of Different Vitamin D Oral Supplements in Laboratory Animal Model. Medicina (Lithuania) 2019, 55. [Google Scholar] [CrossRef]
- Grossmann, R. E.; Tangpricha, V. Evaluation of Vehicle Substances on Vitamin D Bioavailability: A Systematic Review. Molecular Nutrition and Food Research. 2010, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Helde Frankling, M.; Norlin, A. C.; Hansen, S.; Wahren Borgström, E.; Bergman, P.; Björkhem-Bergman, L. Are Vitamin D3 Tablets and Oil Drops Equally Effective in Raising S-25-Hydroxyvitamin D Concentrations? A Post-Hoc Analysis of an Observational Study on Immunodeficient Patients. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Maurya, V. K.; Aggarwal, M. Factors Influencing the Absorption of Vitamin D in GIT: An Overview. Journal of Food Science and Technology Springer India November 1. 2017, 54, 3753–3765. [Google Scholar] [CrossRef] [PubMed]
- Natri, A.-M.; Salo, P.; Vikstedt, T.; Palssa, A.; Huttunen, M.; Kärkkäinen, M. U. M.; Salovaara, H.; Piironen, V.; Jakobsen, J.; Lamberg-Allardt, C. J. Bread Fortified with Cholecalciferol Increases the Serum 25-Hydroxyvitamin D Concentration in Women as Effectively as a Cholecalciferol Supplement. J Nutr 2006, 136, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Biancuzzo, R. M.; Young, A.; Bibuld, D.; Cai, M. H.; Winter, M. R.; Klein, E. K.; Ameri, A.; Reitz, R.; Salameh, W.; Chen, T. C.; Holick, M. F. Fortification of Orange Juice with Vitamin D2 or Vitamin D 3 Is as Effective as an Oral Supplement in Maintaining Vitamin D Status in Adults. American Journal of Clinical Nutrition 2010, 91, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Reboul, E.; Goncalves, A.; Comera, C.; Bott, R.; Nowicki, M.; Landrier, J. F.; Jourdheuil-Rahmani, D.; Dufour, C.; Collet, X.; Borel, P. Vitamin D Intestinal Absorption Is Not a Simple Passive Diffusion: Evidences for Involvement of Cholesterol Transporters. Mol Nutr Food Res 2011, 55, 691–702. [Google Scholar] [CrossRef]
- Hornbuckle, W. E.; Simpson, K. W.; Tennant, B. C. Gastrointestinal Function. Clinical Biochemistry of Domestic Animals 2008, 413–457. [Google Scholar]
- Reboul, E. Intestinal Absorption of Vitamin D: From the Meal to the Enterocyte. Food and Function. Royal Society of Chemistry 2015, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, B.; Argin, S.; Ozilgen, M.; McClements, D. J. Nanoemulsion Delivery Systems for Oil-Soluble Vitamins: Influence of Carrier Oil Type on Lipid Digestion and Vitamin D3 Bioaccessibility. Food Chem 2015, 187, 499–506. [Google Scholar] [CrossRef]
- Goncalves, A.; Gleize, B.; Roi, S.; Nowicki, M.; Dhaussy, A.; Huertas, A.; Amiot, M. J.; Reboul, E. Fatty Acids Affect Micellar Properties and Modulate Vitamin D Uptake and Basolateral Efflux in Caco-2 Cells. Journal of Nutritional Biochemistry 2013, 24, 1751–1757. [Google Scholar] [CrossRef]
- Temova Rakuša, Ž.; Pišlar, M.; Kristl, A.; Roškar, R. Comprehensive Stability Study of Vitamin D3 in Aqueous Solutions and Liquid Commercial Products. Pharmaceutics 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Yang, X.; Yang, L.; Liu, Z. L.; Zhang, F. Autoxidation of Isotachysterol. Tetrahedron 2004, 60, 2881–2888. [Google Scholar] [CrossRef]
- Esmaeili, M.; Yekta, R.; Abedi, A. S.; Ghanati, K.; Derav, R. Z.; Houshyarrad, A.; Dehkordi, Z. S.; Ajami, M.; Mahmoudzadeh, M. Encapsulating Vitamin D: A Feasible and Promising Approach to Combat Its Deficiency. Pharmaceutical Sciences Tabriz University of Medical Sciences April 1. 2022, 194–207. [Google Scholar] [CrossRef]
- Diarrassouba, F.; Remondetto, G.; Liang, L.; Garrait, G.; Beyssac, E.; Subirade, M. Effects of Gastrointestinal PH Conditions on the Stability of the β-Lactoglobulin/Vitamin D3 Complex and on the Solubility of Vitamin D3. Food Research International 2013, 52, 515–521. [Google Scholar] [CrossRef]
- Xiang, C.; Gao, J.; Ye, H.; Ren, G.; Ma, X.; Xie, H.; Fang, S.; Lei, Q.; Fang, W. Development of Ovalbumin-Pectin Nanocomplexes for Vitamin D3 Encapsulation: Enhanced Storage Stability and Sustained Release in Simulated Gastrointestinal Digestion. Food Hydrocoll 2020, 106, 105926. [Google Scholar] [CrossRef]
- Sharifi, F.; Jahangiri, M. Investigation of the Stability of Vitamin D in Emulsion-Based Delivery Systems. Chemical Industry & Chemical Engineering Quarterly 2017, 24, 157–167. [Google Scholar]
- Sams, L.; Paume, J.; Giallo, J.; Carrière, F. Relevant PH and Lipase for in Vitro Models of Gastric Digestion. Food Funct 2016, 7, 30–45. [Google Scholar] [CrossRef]
- Wang, X.; Ye, A.; Lin, Q.; Han, J.; Singh, H. Gastric Digestion of Milk Protein Ingredients: Study Using an in Vitro Dynamic Model. J Dairy Sci 2018, 101, 6842–6852. [Google Scholar] [CrossRef] [PubMed]
- Brodkorb, A.; Egger, L.; Alminger, M.; Alvito, P.; Assunção, R.; Ballance, S.; Bohn, T.; Bourlieu-Lacanal, C.; Boutrou, R.; Carrière, F.; Clemente, A.; Corredig, M.; Dupont, D.; Dufour, C.; Edwards, C.; Golding, M.; Karakaya, S.; Kirkhus, B.; Le Feunteun, S.; Lesmes, U.; Macierzanka, A.; Mackie, A. R.; Martins, C.; Marze, S.; McClements, D. J.; Ménard, O.; Minekus, M.; Portmann, R.; Santos, C. N.; Souchon, I.; Singh, R. P.; Vegarud, G. E.; Wickham, M. S. J.; Weitschies, W.; Recio, I. INFOGEST Static in Vitro Simulation of Gastrointestinal Food Digestion. Nat Protoc 2019, 14, 991–1014. [Google Scholar] [CrossRef]
- Food Code 2022 | FDA. Available online: https://www.fda.gov/food/fda-food-code/food-code-2022 (accessed 2023-07-25).
- Schmid, A.; Walther, B. Natural Vitamin D Content in Animal Products. Advances in Nutrition 2013, 4, 453–462. [Google Scholar] [CrossRef]
- Temova, Ž.; Roškar, R. Stability-Indicating HPLC–UV Method for Vitamin D3 Determination in Solutions, Nutritional Supplements and Pharmaceuticals. J Chromatogr Sci 2016, 54, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, E.; Cunningham, J.; Sherriff, J.; Lucas, R.; Greenfield, H.; Arcot, J.; Strobel, N.; Black, L. Vitamin D3 and 25-Hydroxyvitamin D3 Content of Retail White Fish and Eggs in Australia. Nutrients 2017, 9, 647. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.; Smith, C.; Bysted, A.; Cashman, K. D. Vitamin D in Wild and Farmed Atlantic Salmon (Salmo Salar)—What Do We Know? Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Flores-Aldana, M.; Rivera-Pasquel, M.; García-Guerra, A.; Pérez-Cortés, J. G.; Bárcena-Echegollén, J. E. Effect of Vitamin D Supplementation on (25(OH)D) Status in Children 12–30 Months of Age: A Randomized Clinical Trial. Nutrients 2023, 15, 2756. [Google Scholar] [CrossRef] [PubMed]
- Villamor, E.; Oliveros, H.; Marín, C.; López-Arana, S.; Agudelo-Cañas, S. Increased Serum Total and Free 25-Hydroxyvitamin D with Daily Intake of Cholecalciferol-Fortified Skim Milk: A Randomized Controlled Trial in Colombian Adolescents. Journal of Nutrition 2023, 153, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Sollano-mendieta, X. C.; Meza-márquez, O. G.; Osorio-revilla, G.; Téllez-medina, D. I. Effect of In Vitro Digestion on the Antioxidant Compounds and Antioxidant Capacity of 12 Plum (Spondias Purpurea L.) Ecotypes. Foods 2021, 10. [Google Scholar] [CrossRef]
- Hemery, Y. M.; Fontan, L.; Moench-Pfanner, R.; Laillou, A.; Berger, J.; Renaud, C.; Avallone, S. Influence of Light Exposure and Oxidative Status on the Stability of Vitamins A and D3 during the Storage of Fortified Soybean Oil. Food Chem 2015, 184, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Floros, S.; Toskas, A.; Pasidi, E.; Vareltzis, P. Bioaccessibility and Oxidative Stability of Omega-3 Fatty Acids in Supplements, Sardines and Enriched Eggs Studied Using a Static In Vitro Gastrointestinal Model. Molecules 2022, Vol. 27, Page 415 2022, 27, 415. [Google Scholar] [CrossRef]
- Jakobsen, J.; Knuthsen, P. Stability of Vitamin D in Foodstuffs during Cooking. Food Chem 2014, 148, 170–175. [Google Scholar] [CrossRef]
- Szlinder-Richert, J.; Malesa-Ciećwierz, M. Effect of Household Cooking Methods on Nutritional Value of Cod and Salmon-Twin Fillet Approach. Carpathian Journal of Food Science and Technology 2018, 10, 142–157. [Google Scholar]
- Mahmoodani, F.; Perera, C. O.; Fedrizzi, B.; Abernethy, G.; Chen, H. Degradation Studies of Cholecalciferol (Vitamin D3) Using HPLC-DAD, UHPLC-MS/MS and Chemical Derivatization. Food Chem 2017, 219, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Lee, H. J.; Shin, C.; Chun, Y. S.; Kim, J.; Jung, H.; Choung, J.; Shim, S. M. Physicochemical Properties and Bioavailability of Naturally Formulated Fat-Soluble Vitamins Extracted from Agricultural Products for Complementary Use for Natural Vitamin Supplements. Food Sci Nutr 2020, 8, 5660–5672. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.; Gonçalves, R. F. S.; Pinheiro, A. C.; Manrique, Y. A.; Barreiro, M. F.; Lopes, J. C. B.; Dias, M. M. In Vitro Digestion and Bioaccessibility Studies of Vitamin E-Loaded Nanohydroxyapatite Pickering Emulsions and Derived Fortified Foods. LWT 2022, 154, 112706. [Google Scholar] [CrossRef]
- Mahmoodani, F.; Perera, C. O.; Abernethy, G.; Fedrizzi, B.; Chen, H. Lipid Oxidation and Vitamin D3 Degradation in Simulated Whole Milk Powder as Influenced by Processing and Storage. Food Chem 2018, 261, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodani, F.; Perera, C. O.; Abernethy, G.; Fedrizzi, B.; Greenwood, D.; Chen, H. Identification of Vitamin D3 Oxidation Products Using High-Resolution and Tandem Mass Spectrometry. J Am Soc Mass Spectrom 2018, 29, 1442–1455. [Google Scholar] [CrossRef] [PubMed]
- Bochkov, V. N.; Oskolkova, O. V.; Birukov, K. G.; Levonen, A. L.; Binder, C. J.; Stöckl, J. Generation and Biological Activities of Oxidized Phospholipids. Antioxid Redox Signal 2010, 12, 1009. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Alavez, M.; Méndez-Rodriguez, L. C.; De Anda Montañez, J. A.; Mejía, C. H.; Galván-Magaña, F.; Zenteno-Savín, T. Vitamins C and E Concentrations in Muscle of Elasmobranch and Teleost Fishes. Comp Biochem Physiol A Mol Integr Physiol 2014, 170, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Sun, J.; Liu, Y.; Zeng, H.; Su, Y.; Yang, Y. ACE Inhibitory Peptides and Antioxidant Peptides Derived from in Vitro Digestion Hydrolysate of Hen Egg White Lysozyme. Food Chem 2012, 135, 1245–1252. [Google Scholar] [CrossRef]
- Young, D.; Nau, F.; Pasco, M.; Mine, Y. Identification of Hen Egg Yolk-Derived Phosvitin Phosphopeptides and Their Effects on Gene Expression Profiling against Oxidative Stress-Induced Caco-2 Cells. J Agric Food Chem 2011, 59, 9207–9218. [Google Scholar] [CrossRef]
- Remanan, M. K.; Wu, J. Antioxidant Activity in Cooked and Simulated Digested Eggs. Food Funct 2014, 5, 1464–1474. [Google Scholar] [CrossRef]
- Lipkie, T. E.; Ferruzzi, M. G.; Weaver, C. M. Low Bioaccessibility of Vitamin D2 from Yeast-Fortified Bread Compared to Crystalline D2 Bread and D3 from Fluid Milks. Food Funct 2016, 7, 4589–4596. [Google Scholar] [CrossRef]
- Hernández-Olivas, E.; Muñoz-Pina, S.; Sánchez-García, J.; Andrés, A.; Heredia, A. Understanding the Role of Food Matrix on the Digestibility of Dairy Products under Elderly Gastrointestinal Conditions. Food Research International 2020, 137, 109454. [Google Scholar] [CrossRef]
- Zhou, H.; Zheng, B.; Zhang, Z.; Zhang, R.; He, L.; McClements, D. J. Fortification of Plant-Based Milk with Calcium May Reduce Vitamin D Bioaccessibility: An in Vitro Digestion Study. J Agric Food Chem 2021, 69, 4223–4233. [Google Scholar] [CrossRef]
- Dima, C.; Dima, S. Bioaccessibility Study of Calcium and Vitamin D3 Co-Microencapsulated in Water-in-Oil-in-Water Double Emulsions. Food Chem 2020, 303, 125416. [Google Scholar] [CrossRef]
- Forrest, S. A.; Yada, R. Y.; Rousseau, D. Interactions of Vitamin D3 with Bovine β-Lactoglobulin A and β-Casein. J Agric Food Chem 2005, 53, 8003–8009. [Google Scholar] [CrossRef]
- Antoine, T.; Icard-Vernière, C.; Scorrano, G.; Salhi, A.; Halimi, C.; Georgé, S.; Carrière, F.; Mouquet-Rivier, C.; Reboul, E. Evaluation of Vitamin D Bioaccessibility and Mineral Solubility from Test Meals Containing Meat and/or Cereals and/or Pulses Using in Vitro Digestion. Food Chem 2021, 347. [Google Scholar] [CrossRef]
- Li, Y.; Ma, D.; Sun, D.; Wang, C.; Zhang, J.; Xie, Y.; Guo, T. Total Phenolic, Flavonoid Content, and Antioxidant Activity of Flour, Noodles, and Steamed Bread Made from Different Colored Wheat Grains by Three Milling Methods. Crop J 2015, 3, 328–334. [Google Scholar] [CrossRef]
- Siyuan, S.; Tong, L.; Liu, R. H. Corn Phytochemicals and Their Health Benefits. Food Science and Human Wellness 2018, 7, 185–195. [Google Scholar] [CrossRef]
- Aguillón-Osma, J.; Luzardo-Ocampo, I.; Cuellar-Nuñez, M. L.; Maldonado-Celis, M. E.; Loango-Chamorro, N.; Campos-Vega, R. Impact of in Vitro Gastrointestinal Digestion on the Bioaccessibility and Antioxidant Capacity of Bioactive Compounds from Passion Fruit (Passiflora Edulis) Leaves and Juice Extracts. J Food Biochem 2019, 43, e12879. [Google Scholar] [CrossRef]
- Goebel, S.; Avallone, S.; Detchewa, P.; Prasajak, P.; Sriwichai, W. Natural and Synthetic Antioxidants Prevent the Degradation of Vitamin D3fortification in Canola Oil during Baking and in Vitro Digestion. Applied Science and Engineering Progress 2021, 14. [Google Scholar] [CrossRef]
- Blanco, A.; Blanco, G. Digestion - Absorption. Med Biochem 2017, 251–273. [Google Scholar]
- Wang, W.; Cui, C.; Wang, Q.; Sun, C.; Jiang, L.; Hou, J. Effect of PH on Physicochemical Properties of Oil Bodies from Different Oil Crops. J Food Sci Technol 2019, 56, 49. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D. Nonclassic Actions of Vitamin D. J Clin Endocrinol Metab 2009, 94, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Yanhai, Z.; Yan, J.; Qun, X.; Rohrer, J. Simultaneous Determination of Vitamins A, E, and D3 in Milk-Based Nutritionals by On-Line Two-Dimensional HPLC.
- Zhu, Y.; Yang, S.; Huang, Y.; Huang, J.; Li, Y. Effect of in Vitro Gastrointestinal Digestion on Phenolic Compounds and Antioxidant Properties of Soluble and Insoluble Dietary Fibers Derived from Hulless Barley. J Food Sci 2021, 86, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Richards, M. P.; Hultin, H. O. Effect of PH on Lipid Oxidation Using Trout Hemolysate as a Catalyst: A Possible Role for Deoxyhemoglobin. J Agric Food Chem 2000, 48, 3141–3147. [Google Scholar] [CrossRef] [PubMed]
- Peroxide Value Method. 2023. Available online: https://www.protocols.io/view/Peroxide-Value-Method-4rm7vz12lx1w/v1 (accessed 2023-08-01).
- Christie, W. W.; Han, X. Isolation of Fatty Acids and Identification by Spectroscopic and Related Techniques. Lipid Analysis 2012, 181–211. [Google Scholar]
- Shantha, N. C.; Decker, E. A. Rapid, Sensitive, Iron-Based Spectrophotometric Methods for Determination of Peroxide Values of Food Lipids. J AOAC Int 1994, 77, 421–424. [Google Scholar] [CrossRef]
- Lemon, D.W. An improved TBA test for rancidity. New Series Circular No. 51, 1975. [Google Scholar]
Scheme 1.
Chemical structures of main dietary forms of vitamin D: (I) ergocalciferol (vitamin D2), (II) cholecalciferol (vitamin D3), (III) 25-hydroxy-cholecalciferol (25(OH)D3) [8].
Scheme 1.
Chemical structures of main dietary forms of vitamin D: (I) ergocalciferol (vitamin D2), (II) cholecalciferol (vitamin D3), (III) 25-hydroxy-cholecalciferol (25(OH)D3) [8].
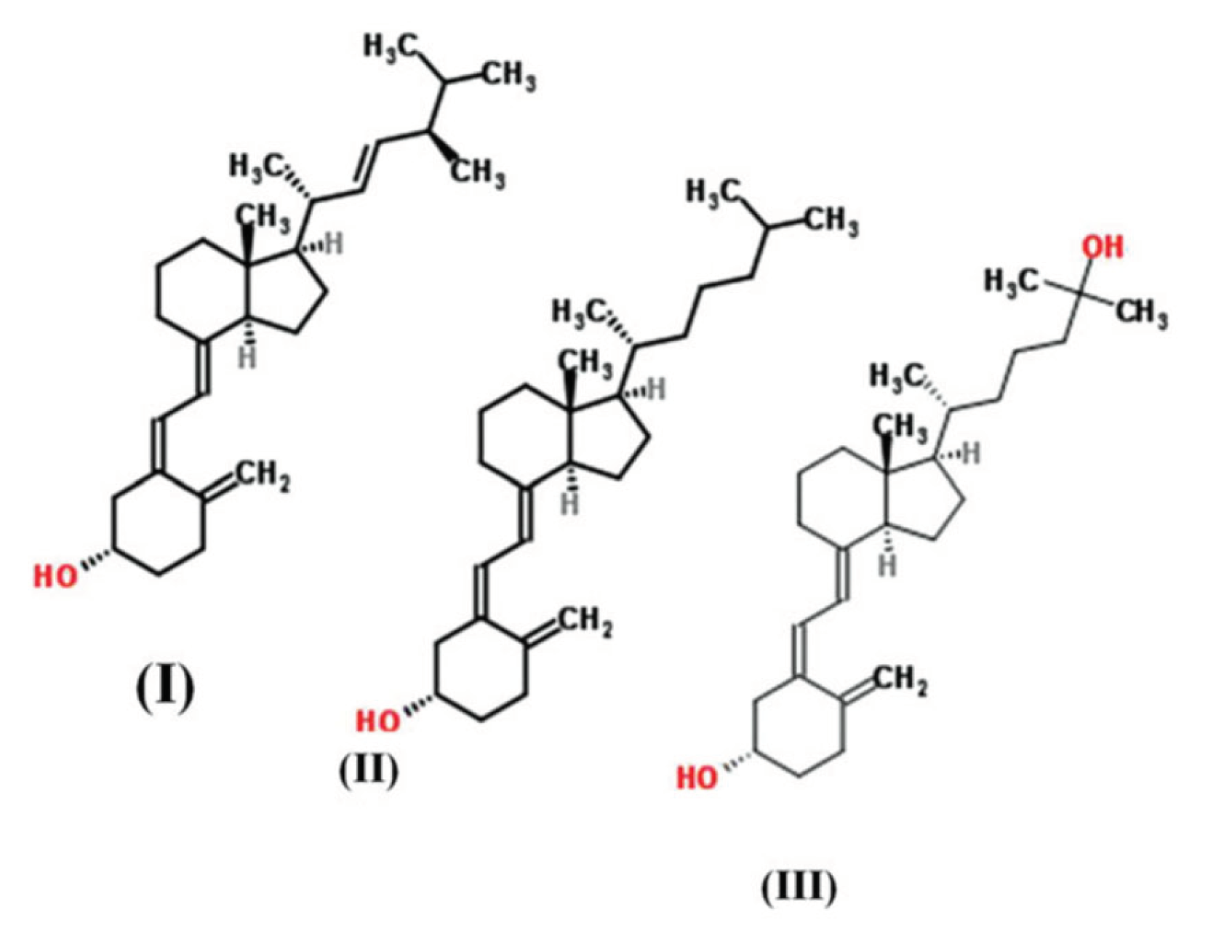
Figure 1.
Vitamin D3 detected content during in vitro digestion of (a) commercial supplements: tablet; capsule; liquid, (b) close-view on tablet and capsule (tablet in μg/tablet, capsule in μg/capsule and liquid in μg/ml). On x-axis 0, 122 and 242 minutes refer respectively to the initial content, content after gastric stage and content after intestinal stage.
Figure 1.
Vitamin D3 detected content during in vitro digestion of (a) commercial supplements: tablet; capsule; liquid, (b) close-view on tablet and capsule (tablet in μg/tablet, capsule in μg/capsule and liquid in μg/ml). On x-axis 0, 122 and 242 minutes refer respectively to the initial content, content after gastric stage and content after intestinal stage.
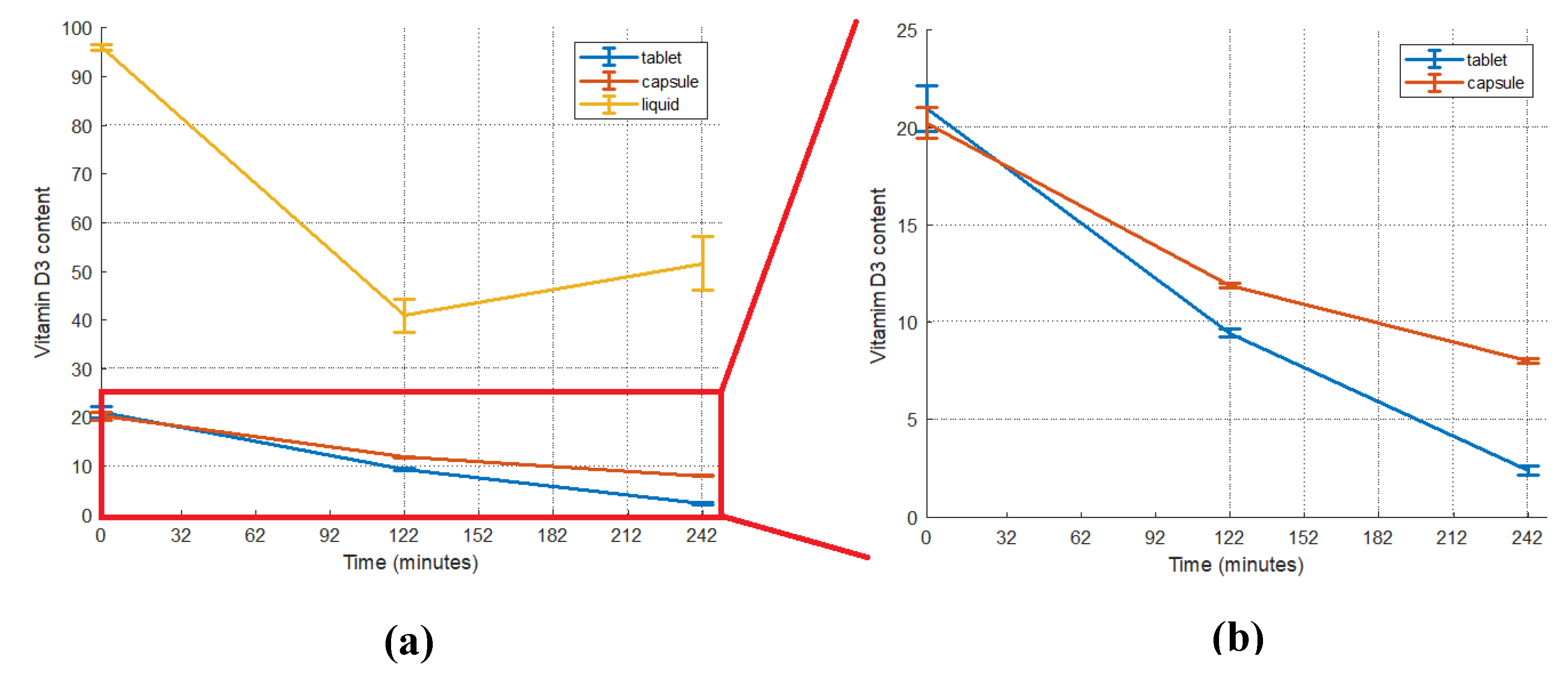
Figure 2.
Bioaccessibility indices for supplements: tablet; capsule; liquid and foods: egg; salmon; milk; cereals; sour cherry juice.
Figure 2.
Bioaccessibility indices for supplements: tablet; capsule; liquid and foods: egg; salmon; milk; cereals; sour cherry juice.
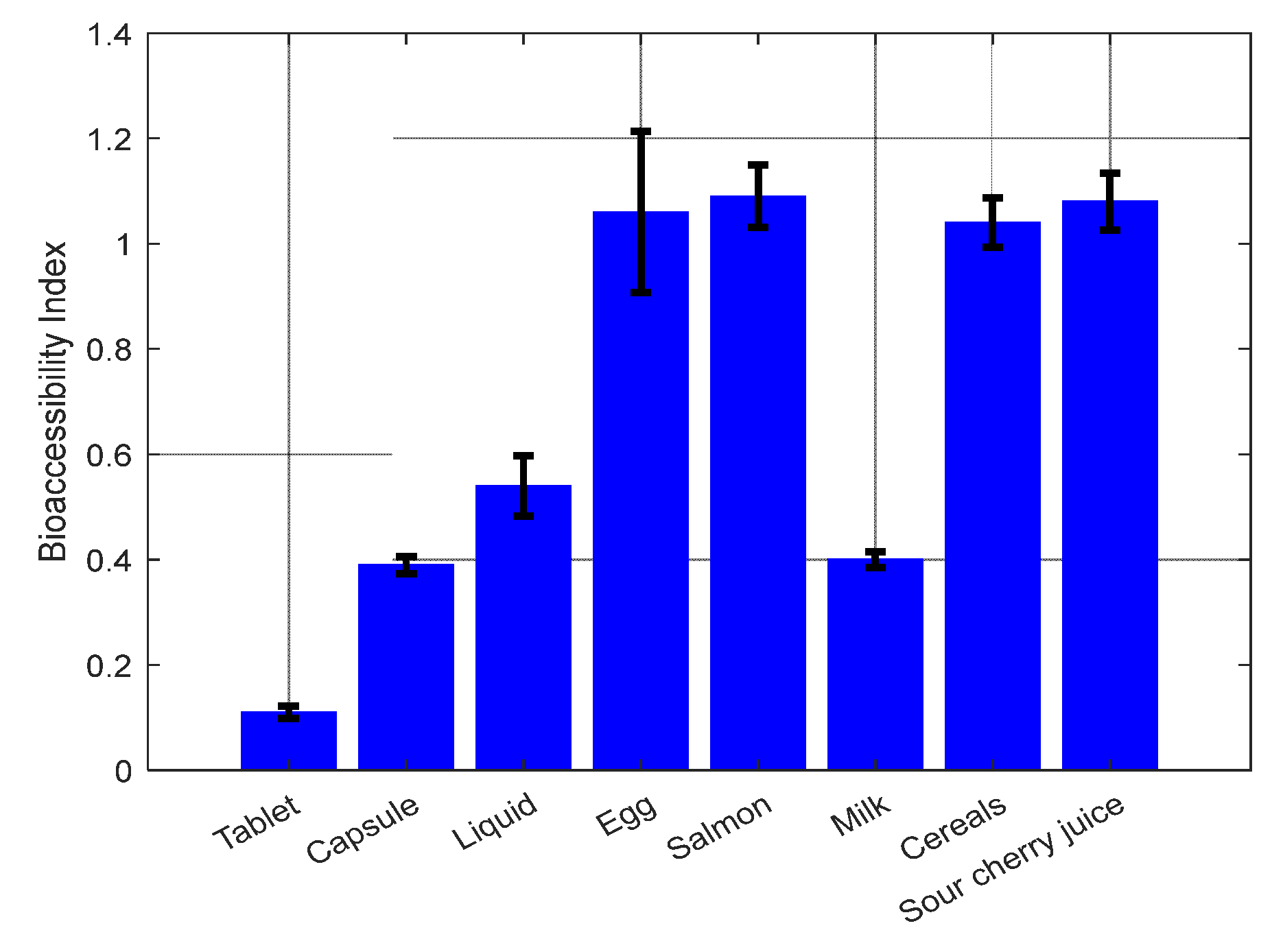
Figure 3.
Effect of gastric pH on (a) primary oxidation and (b) secondary oxidation of sunflower seed oil. On x-axis 0 min refer to the initial concentration, 15 min refer to the concentration after oral phase, 75 and 135 min refer to the concentration after the first and second hour of gastric phase and 195 and 225 min refer to the concentration after the first and second hour of intestinal phase.
Figure 3.
Effect of gastric pH on (a) primary oxidation and (b) secondary oxidation of sunflower seed oil. On x-axis 0 min refer to the initial concentration, 15 min refer to the concentration after oral phase, 75 and 135 min refer to the concentration after the first and second hour of gastric phase and 195 and 225 min refer to the concentration after the first and second hour of intestinal phase.
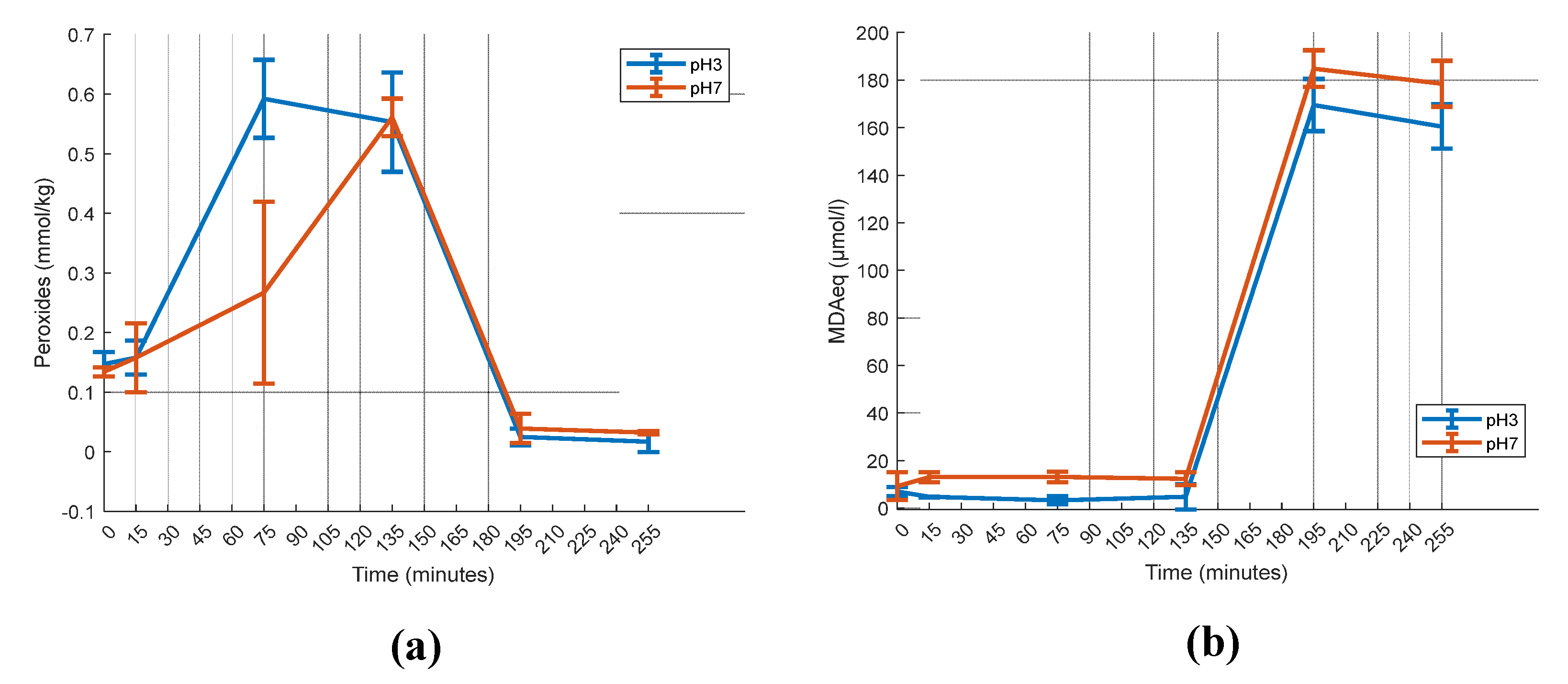

Table 1.
Vitamin D3 detected content and bioaccessibility indices (BI) of foods after INFOGEST protocol.
Table 1.
Vitamin D3 detected content and bioaccessibility indices (BI) of foods after INFOGEST protocol.
| Food Sample | Vitamin D3 detected content (μg/g1) | Bioaccessibility Index (BI) | ||||
|---|---|---|---|---|---|---|
| Initial | Thermally processed | Stomach | Intestine | |||
| Natural | Egg | 0.06±0.004 b | 0.03±0.005 c | 0.08±0.007 a | 0.06±0.008 b | 1.06±0.153 |
| Salmon | 0.50±0.021 c | 0.38±0.020 d | 0.74±0.015 a | 0.55±0.019 b | 1.10±0.060 | |
| Fortified | Milk | 1.53±0.056 a | N/A | 0.62±0.007 b | 0.61±0.004 b | 0.40±0.015 |
| Cereals | 0.89±0.040 a, b | N/A | 0.84±0.005 b | 0.92±0.006 a | 1.04±0.046 | |
| Sour cherry juice | 1.15±0.005 c | N/A | 1.20±0.008 b | 1.24±0.003 a | 1.08±0.054 | |
Table values are means ± standard deviations. Different superscript letters (a, b, c, d) represent statistical differences in the same row (p ≤ 0.05). 1 g in vitamin D3 content refers to the initial food sample.
Table 2.
Vitamin D3 detected content and bioaccessibility indices (BI) in four different gastric pH values after INFOGEST application.
Table 2.
Vitamin D3 detected content and bioaccessibility indices (BI) in four different gastric pH values after INFOGEST application.
| Gastric pH Value | Vitamin D3 Detected Content (μg/ml) | BI | ||
|---|---|---|---|---|
| Initial | Stomach | Intestine | ||
| 1 | 95.93±0.64 a | 39.87±8.97 b, B | 70.86±4.58 c, A | 0.74±0.05 |
| 3 | 40.95±2.69 b, B | 51.71±5.46 c, B | 0.54±0.06 | |
| 5 | 47.14±3.71b, A B | 51.62±2.08 b, B | 0.54±0.02 | |
| 7 | 53.65±6.55 b, A | 41.28±2.89 c, C | 0.43±0.03 | |
Table values are means ± standard deviations. Different superscript lowercase letters (a, b, c, d) represent statistical differences (p ≤ 0.05) in the same row. Different superscript uppercase (A, B, C, D) letters represent statistical differences (p ≤ 0.05) in the same column.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



