
Submitted:
26 February 2024
Posted:
27 February 2024
You are already at the latest version
Abstract
Etiological factors involved in myelodysplastic syndrome (MDS) include immunologic, oxidative stress, and inflammatory factors, among others, and these are targets for microRNAs (miRNs). Here, we evaluated whether some miRNs may affect the tumor development comparing untreated and 5-azacitidine (5-AZA) MDS-treated patients. Peripheral blood samples were collected from 20 controls and 24 MDS patients, and selected miRNs related to redox balance and inflammation, including miR-18a, miR-21, miR-34a and miR-146a, were isolated and measured by quantitative real-time polymerase chain reaction (qRTPCR). A differential expression profile of miRNs was detected in untreated MDS patients and 5-AZA group. MiR-18a, miR-21, miR-34a and miR-146a were significantly overexpressed in untreated MDS, compared to controls. However, we did not observe any miRNs profile alteration during the progression of the disease. On the other hand, 5-AZA treatment tends to restore miRNs expression levels. Relating to prognostic risk factors, high risk MDS groups (high IPSS-R, high cytogenetic risk, high molecular risk (HMR) mutations tended to be related with higher expression levels of miR-18a and miR-34a. Higher miRNs expression is correlated with lower glutathione peroxidase activity, while they are related with a higher profile of pro-inflammatory cytokines (IL-2, IL-6, IL-8, TNF-α). Although our study was limited by the low number of MDS patients included, we identified miRNs deregulation involved in the MDS development, that could regulate redox sensors and inflammatory responses. Finally, 5-AZA treatment is related with lower miRNs expression levels in MDS patients.
Keywords:
myelodysplastic syndrome (MDS)
; microRNAs (miRNs)
; oxidative stress
; inflammatory cytokines
; 5-azacitidine (5-AZA)
1. Introduction
Myelodysplastic Syndromes (MDS) are hematological disorders with an elevated rate of mortality in the aged population, in which 1 out of 3 patients progress towards acute myeloid leukemia (AML). The course of the disease is highly variable, and, therefore, a recent classification and several prognostic score systems have been incorporated for the diagnosis in daily clinical practice [2,3]. In this line, therapies differ between risk groups, in which higher-risk patients are treated with hypomethylating agents such us 5-azacitidine (5-AZA) [4].
Factors determining the pathogenesis and progression of MDS have not been fully elucidated. Among them, oxidative stress plays an important role in the tumorigenesis, as it has been observed in a wide variety of solid and hematological tumors [5]. Recently, our group demonstrated the implication of this biological mechanism in the MDS development and progression of the disease [6]. Oxidative stress has been involved also in the aberrant expression of microRNAs (miRNs), which regulate cellular events such as proliferation, apoptosis, metastasis, and adaptation to hypoxia [7,8]. In turn, miRNs regulate the expression of key components of the cellular antioxidant response. According to this, numerous studies have revealed a set of miRNs that are ROS-sensitive, regulating their transcription. Moreover, the dysregulation of both redox signaling and miRNs has been associated with tumor-promoting inflammation [9].
The precise functions and molecular mechanisms of miRNs/redox connection are still not clear, and the possible interplay between redox regulation and cancer processes is currently being studied [10]. Several antioxidant systems, including superoxide dismutase (SOD)/catalase (CAT) system, are targets of miRNs (miR-21 and miR-146a, respectively), interfering with their antioxidant functions [11,12]. Related to MDS, several studies have provided evidence of an altered miRNs expression profiling in cancer pathogenesis with a potential clinical utility in the diagnosis, genetics changes, and defining risk groups [13].
An altered cellular redox status and cytokines expression have been observed in MDS patients [6]. To date, however, no information explains the interplay between oxidative stress parameters, inflammation, and miRNs in the pathogenesis of MDS patients. So, we considered it worthwhile to examine for the first time the potential interplay between miRNs and MDS, and the possible impact of the hypomethylating agent 5-AZA treatment on these responses in MDS patients.
2. Material and Methods
2.1. Study design
2.1.1. Patients and controls
A total of 24 myelodysplastic syndrome (MDS) patients (12 males and 12 females; mean age of 70 years) of the San Cecilio´s University Hospital of Granada, were included in the study. MDS patients were registered on the Spanish MDS Registry (RESMD), and their subtypes were defined according to the World Health Organization (WHO-2016) [3]; as early-stage disease (ES, <5% bone marrow blasts) and advances-stage disease (ASD, >5% bone marrow blasts). The ES subgroup included 2 patients with single lineage dysplasia (MDS-SLD), 7 ones with multilineage dysplasia (MDS-MLD), 1 with SLD and ring sideroblasts (MDS-RS-SLD), 2 with MLD and ring sideroblasts (MDS-RS-MLD), 2 with ring sideroblasts (MDS-RS), and 2 with isolated del(5q) MDS (del5q). The ASD subgroup involved 4 patients with excess blasts-1 (MDS EB-1), and 4 with excess blasts-2 (MDS EB-2). Based on the revised International Prognostic Scoring System (IPSS-R) all patients were divided into lower-risk disease (IPSS-R very low, low, intermediate) and higher-risk disease (IPSS-R high, very high). The cytogenetic risk categories were divided into: Favorable (Very good, −Y, del(11q); Good (normal, del(20q), del(5q) alone or with 1 other anomaly, and del(12p)); Poor (complex with 3 abnormalities, der(3q) or chromosome 7 abnormalities); Very poor (complex with ≥3 abnormalities), and Intermediate (all other single or double abnormalities not listed).
MDS patients were classified according to the established therapy as untreated MDS patients (patients at diagnosis or only with supportive care including erythropoietin, Epo and/or granulocyte macrophage colony-stimulating factor, GM-CSF) or treated MDS patients (patients treated with hypomethylating agents such as 5-AZA from 3 to 7 cycles). Only one MDS patient received chemotherapy treatment and was included within treated patients.
Samples from 20 healthy volunteer donors (control group) were also analyzed. All controls (median age 70 years; range 42-88 years), had normal hemograms and they had no history of neoplastic disease, or previous exposure to chemotherapy drugs, radiation therapy, or immunotherapy.
2.1.2. Blood samples
Peripheral blood samples were collected by peripheral venipuncture from the antecubital vein in MDS patients and controls between 8-10 a.m. Blood samples were centrifuged at 3,000 rpm for 15 min. Plasma and erythrocytes were separated (erythrocytes were washed twice with cold saline) and were aliquoted and stored at -80°C for oxidative stress parameters studies. Aliquots of miRNs plasma assays were collected into RNase/DNase-free tubes and immediately aliquoted and frozen at -80°C until the assays were performed.
2.1.3. RNA solation and quantification of circulating miRNs levels
The total RNA extraction was performed using a miRNeasy Serum/Plasma advanced isolation kit (Qiagen, Toronto, Canada) according to the manufacturer’s instructions. Briefly, 200 μL of plasma samples were used to extract the total RNA, and an equal volume of denaturing solution was added (20 μL). Four miRNs (miR-18a-5p, hsa-miR-21-5p, hsa-miR-34a-5p, and hsa-miR-146a-5p) with a potential role in oxidative stress and inflammation were analyzed.
2.1.4. Quantitative real-time amplification (qRT-PCR)
Real-Time PCR technique was performed in a Stratagene Mx3005P QPCR System (Agilent Technologies, Barcelona, Spain) according to the manufacturer’s protocol, using TaqMan Fast Advanced Master Mix (2x) and TaqMan probes (20x) (assay names: hsa-miR-18a-5p, assay ID: 478551; hsa-miR-21-5p, assay ID: 477975; hsa-miR-34a-5p, assay ID: 478048; hsa-miR-146a-5p, assay ID: 478399; (Thermo Fisher Scientific, Waltham, MA, USA). The total reaction volume was 20 μL per well. The reaction conditions were enzyme activation, 20 seconds at 95 °C, denaturation, 3 seconds at 95 °C (40 cycles), and elongation, 30 seconds at 60 °C. The levels of plasma miRNs expression were normalized to hsa-miR-30b-5p (assay ID: 47995, Thermo Fisher Scientific, Waltham, MA, USA) as a housekeeping gene using the 2−ΔCt and 2−ΔΔCt formulas.
2.2. Statistical Analysis
Relative expressions of miRNs between MDS groups were compared using the nonparametric Mann-Whitney U test or Kruskal-Wallis's tests. Data are expressed as mean ± SEM. Correlations between miRNs and oxidative stress parameters and cytokines were analyzed using the Pearson's correlation coefficient. GraphPad Prism v. 6.0 (GraphPad Software, Inc., La Jolla, CA, USA) was used to analyze data. A p < 0.05 was considered statistically significant.
3. Results
3.1. Differential patterns of miRNs expression in MDS patients
Relative expression of miR-18a-5p, hsa-miR-21-5p, hsa-miR-34a-5p, and hsa-miR-146a-5p was analyzed using hsa-miR-30b-5p as an endogenous control because its expression did not vary in MDS patients and controls [14]. MDS untreated patients had significantly higher levels of miR-18a (p = 0.012), miR-21 (p < 0.001), and miR-34a (p = 0.019) compared to the controls (Figure 1A–C). This increment was significantly higher in the 5-AZA treated group for miR-21 and miR-34a (Figure 1B,C). Although miR-146a expression tends to increase in the MDS untreated patients, no significant differences were observed in the groups (Figure 1D). Moreover, compared to the untreated patients, 5-AZA group tends to decrease the expression of the four studied miRNs. The treatment with 5-AZA, however, did not recover the expression to the levels of the control group (Figure 1).
3.2. miRNs expression and risk factors in MDS patients
To explore if the changes observed in the miRNs profile from untreated MDS patients are conserved during the disease progression, we categorized MDS patients according to the recent WHO classification, as early stage (ES, n = 13; <5% bone marrow blasts) and advanced stage (AS, n = 6; >5% bone marrow blasts). Differences between both stages of the disease in the miRNs expression profile, were not detected (Figure 2).
We next analyzed any relationship between miRNs expression and the clinical characteristics, such as IPSS-R score, cytogenetic risk, and mutational profile. For this evaluation, untreated MDS patients were divided into two groups according different categories: IPSS-R: high risk (n = 9) vs. low risk (n = 10); Cytogenetic risk: favorable (good karyotypes, n = 13) vs. unfavorable (intermediate, poor, and very poor karyotypes, n = 6); Molecular risk: high risk (presence of at least one mutation in any of high molecular risk (HMR) genes (TP53, ETV6, ASXL1, RUNX1, EZH2), n = 11) vs. low risk (absence of mutations in HMR genes, n = 8); and Mutational score (number of total mutations present in the dysplastic clone (≤2 total mutations, n = 13) vs. (>3 total mutations, n = 6??? ES QUE NO DA TOTAL DE 19).
Based on the IPSS-R prognostic stratification, we observed that the expression of miR-18a and miR-34a trend to increase in MDS patients with a high IPSS-R risk compared with those with a low risk of progression (Figure 3A,C). miR-21 and miR-146a expression levels, however, did not differ between both groups (Figure 3B,D).
When we analyzed miRNs expression based on cytogenetic risk, we highlighted the significant increase in miR-21 (p = 0.01) and miR-146a (p = 0.02) levels in the MDS group with high cytogenetic risk compared to favorable cytogenetic risk group (Figure 3F,H). miR-18a and miR-34a levels tend to increase in the high-risk group although this increase is not significant (Figure 3E,G).
Finally, we categorized MDS patients concerning molecular risk (high risk, presence of at least one mutation in any of high molecular risk (HMR) genes) vs. low risk (absence of mutations in HMR genes).
We observed that miR-21 and miR-34a values trend to be higher in the MDS group that present molecular risk factors than the MDS group with no-HMR mutations (Figure 3J,K).
Also, about molecular risk, we evaluated miRNs expression between untreated MDS group based on the mutational score (number of total mutations present in the dysplastic clone, ≤2 (n = 13) vs. >3 (n = 5) total mutations). Similarly, we did not observed differences between patients with a high number of total mutations (>3 total mutations) with respect to those with low mutational score (≤2 total mutations), although miR-34a values trend to be elevated in the MDS group with high risk.
3.3. miRNs profile could be related to redox signaling and inflammation in MDS patients
In our previous work, we analyzed the oxidative stress and inflammatory markers in MDS patients versus the control group [6]. Here we evaluated possible correlations between the miRNs expression profile, the endogenous antioxidant system, and inflammatory markers.
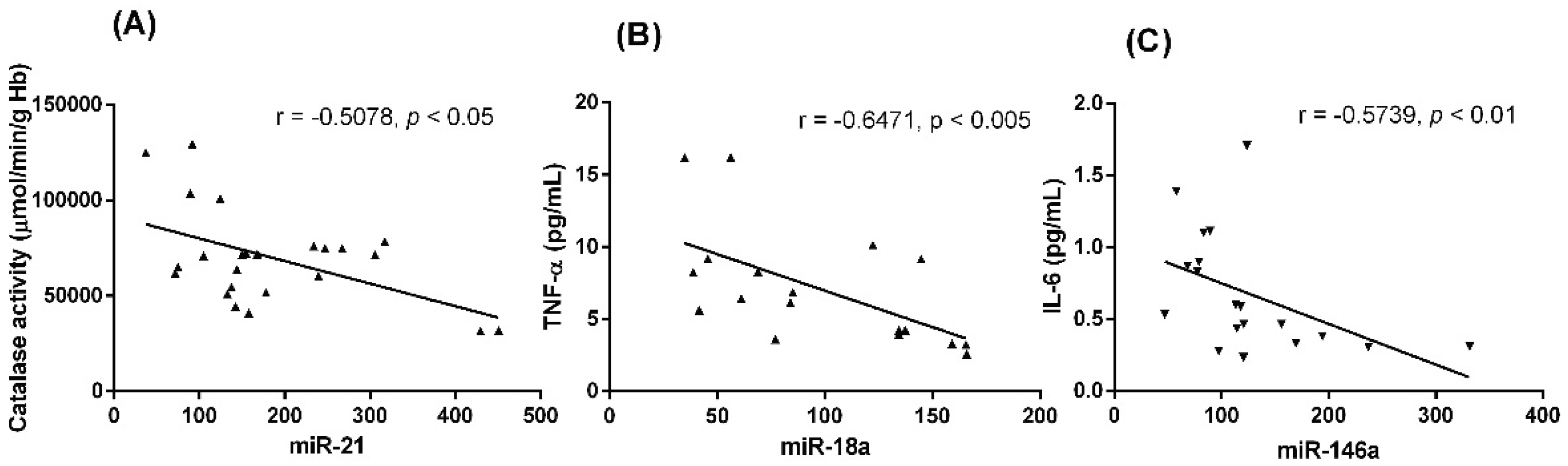
Firstly, we studied the relation between the following antioxidant defense molecules: the glutathione cycle, SOD, CAT, glutathione reductase (GRd), glutathione peroxidase (GPx), and the markers of oxidative damage (lipid peroxidation, LPO, and advanced oxidation protein products, AOPP), with the four miRNs expression here analyzed in MDS patients. From all analyses, only a negative correlation between miR-21 and CAT activity (r = -0.507, p < 0.05) was found (Figure 4A).
Secondly, and taking into an account that in the previous study we analyzed the plasma cytokine levels (IL-1β, IL-2, IL-6, IL-8, IL-10, TNF-α, and INF-ɣ), here we correlated these parameters with miRs relative expressions in MDS patients. The negative correlations between miR-18a and TNF-α (r 0 -0.6471, p <0.005), and between miR-146a and IL-6 levels were detected (r = -0.472, p < 0.05) (Figure 4B,C).
4. Discussion
miRNs are important regulators of the differentiation and maintenance of hematopoietic stem/progenitor cells, and changes in their expression levels could initiate and promote tumor development. A wide variety of alterations in miRNs from MDS patients has been reported [13,14,15,16]. Thus, we addressed here the possible role of some miRNs in the MDS pathogenesis.
We found that plasma miR-18a, miR-21, miR-34a expression significantly increased in MSD patients compared with controls. This is in according with the previous reports showed an increased expression of miR-18a and miR-21 in the bone marrow and peripheral blood from MDS patients [15]. Moreover, plasma mir-146a expression trend to be higher in the group of MDS patients. It is possible that attention should be paid to this miRN, and the difference could be detected in a greater number of patients. These differences may suggest that tissue expression and plasma levels of this miRN may be differently regulated. Based on our results, upregulation of miR-18a, miR-21, and miR-34a could contribute to the ineffective hematopoiesis in MDS. In this sense, miR-34a has been related with an increase in the apoptosis of bone marrow progenitors [17] and with hematopoietic suppression [18].
Nextly, we compared the miRNs profile expression with the risk of the disease progression according to WHO classification, early (<5% bone marrow blasts) and advanced (>5% bone marrow blasts) MDS stages. We observed that the plasma expression levels of miR-18a, miR-21, miR-34a, and miR-146a did not discriminate between both stages of the disease in MDS patients. Other studied miRNs, including miR-422 and miR-617, however, were associated with MDS progression in bone marrow samples [19]. These differences between early MDS subtypes and advanced ones could suggest that altered miRNs expression happens from the initial stages of the disease and it may be an event that contributes to the pathogenesis of MDS.
To deepen the role of miRNs on MDS disease, we then investigate the possible variation of their plasma expression levels according to risk prognostic factors of the disease. According to the IPSS-R, we observed that miR-18a and miR-34a expression tended to increase in high-risk (intermediate-/high/very high) than in low-risk (low and very low) MDS groups, supporting the finding of Choi et al. with miR-21 [20].
Concerning cytogenetic risk, some studies revealed that a karyotype change ((del(5q)/trisomy 8/del(20q)) correlates with a unique profile of miRNs. MDS patients with del(5q) have substantially decreased miRN-146a in the bone marrow cells [16]. We did not study differences between miRNs expression levels and an MDS-specific karyotype due to the low number of patients. Here, dividing MDS patients according to cytogenetic risk, we detected an increasing trend in plasma miR-21 and miR-146a expression levels in high-risk patients compared with low-risk ones.
Analysis of the relationship between the presence of somatic mutations and the levels of circulating miRNs in MDS demonstrated that MDS patient with at least one mutation in HMR genes presented higher expression levels of miR-21 and miR-34a than those without HMR mutations. In general, miRNs expression increases in MDS patients with the presence of risk prognostic factors, a finding that required further studies that support their use as prognostic biomarkers of risk progression towards AML.
We previously identified an improvement of the intracellular oxidative status in MDS patients, with a significant decrease in the GSSG·GSH−1 ratio and glutathione peroxidase (GPx) activity. Moreover, the control of the hydrogen peroxide detoxification was related to the increase in the catalase (CAT) activity, explaining the decrease in the cellular oxidative damage (lipid peroxidation, LPO, and advanced oxidative protein products, AOPP [6]. According to this, we considered it worthwhile to analyze here miRNs plasma levels with a potential role in oxidative stress.
It was reported that miR-21 inhibits SOD3 preventing hydrogen peroxide production [11], a precursor of ROS that is removed by GPx and CAT. Here, we show that the levels of hydrogen peroxide in MDS patients depend, at least in part, of the elevated miR-21 levels that negatively control CAT activity. In this line, miR-21 may prevent a further increase in CAT activity in MDS patients, favoring oxidative stress in them.
Some shreds of evidences have revealed that miRNs regulate the genes associated with the secretion of different cytokines, including TNF-α, IL-1, IL-6, among others [21]. About the deregulation of the inflammatory signaling in MDS, we previously observed an upregulation in the IL-2, IL-6, IL-8, and TNF-α concentration in plasma samples from MDS patients, reflecting an alteration of the inflammatory signaling [6]. In the present study, we emphasize that miR-146a expression correlates negatively with IL-6, which may prevent further increase in IL-6 in MDS patients. In this sense, it was reported that miR-146a acts as an anti-inflammatory microRNA controls IL-6 production in aging and some pathological conditions to restrict inflammatory responses [21,22,23]. miR-146a suppresses the expression of IRAK1 and TRAF6, resulting in inhibition of NF-κB pathway [23,24]. In addition, it is worth highlighting a negative correlation between the expression of miR-18a and TNF-α levels. miR-18a has been shown to be highly expressed in glioma and can affect proliferation, migration, and invasion of human glioblastoma cells [25]. Its expression is related to the regulating of TNF-α production, but more studies are needed to explain this correlation.
Finally, our group has also recently described that 5-AZA treatment increases oxidative stress in MDS patients, with a decrease in the catalase activity related to a marked increase in plasma LPO [6]. Analogously, we investigated whether treatment with 5-AZA modified the expression profiles of the miRNs studied. We observed that 5-AZA group decreased all miRNs expression compared with untreated MDS patients, although the levels of the control group were not recovered. According to this, low miR-21 expression levels in the serum from MDS patients seem to predict a response to hypomethylating agents [26]. Similarly, treatment with an epigenetic therapy (lenalidomide) decrease miR-34a-3p and miR-34a-5p expression levels in peripheral blood monocytes [27].
5. Conclusions
To summarize, miRNs are known to regulate critical cellular processes and, in the present investigation, miR-18a, miR-21, miR-34a and miR-146a have been related to the MDS pathogenesis, being associated with risk MDS groups, and correlated with pro-inflammatory cytokines. In this sense, miRNs could be used as a possible therapeutic tool, in which the inhibition or downregulation of these miRNs might re-establish MDS microenvironment. Finally, 5-AZA treatment could restore miRNs expression levels in the serum from MDS patients.
Author Contributions
Conceptualization, P.M. and D.A.-C.; Methodology, P.M. and I.R.; Formal analysis, P.G. and A.G-L.; Investigation, P.M., E.C. and P.G.; Resources, D.A.-C. and G.E.; Data curation, A.G-L., I.R. and M.S.L.; Writing-original draft preparation, P.M.; Writing-review and editing, P.M., I.R, D.A.-C. and G.E.; Supervision, D.A-C.; Project administration, D.A.-C. and T.H.; Funding acquisition, D.A.-C. and T.H. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partially supported by grant no. CB/10/00238 (CIBERfes, Centro de Investigación Biomédica en Red de Fragilidad y Envejecimiento Saludable, ISCIII), cofunded by the European Regional Development Fund/European Social Fund “Investing in your future”), and from the Consejería de Innovación, Ciencia y Empresa, Junta de Andalucía (CTS-101), Spain. P.M. is sup-ported by a Río Hortega fellowship from the ISCIII, Spain, and the UGC de Laboratorios Clínicos, Hospital Universitario San Cecilio, Granada, Spain.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Granada’s Ethical Committee of Hospital Universitario Clínico San Cecilio (no. 0250-N-20), being approved on 28 May 2020.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author (dacuna@ugr.es) on reasonable request. Materials described in the manuscript will be freely available to any research to use them for noncommercial purposes.
Conflicts of Interest
The authors declare no competing interests.
References
- G. Garcia-Manero, K.S. Chien, G. Montalban-Bravo, Myelodysplastic syndromes: 2021 update on diagnosis, risk stratification and management, Am. J. Hematol. 95 (2020) 1399–1420. [CrossRef]
- D.R. Bond, H.J. Lee, A.K. Enjeti, Unravelling the epigenome of myelodysplastic syndrome: Diagnosis, prognosis, and response to therapy, Cancers (Basel). 12 (2020) 1–25. [CrossRef]
- J.M. Bennett, Changes in the Updated 2016: WHO Classification of the Myelodysplastic Syndromes and Related Myeloid Neoplasms, Clin. Lymphoma, Myeloma Leuk. 16 (2016) 607–609. [CrossRef]
- P. Fenaux, L. Ades, Review of azacitidine trials in Intermediate-2-and High-risk myelodysplastic syndromes, Leuk. Res. 33 (2009) S7–S11. [CrossRef]
- M.D. Jelic, A.D. Mandic, S.M. Maricic, B.U. Srdjenovic, Oxidative stress and its role in cancer, J. Cancer Res. Ther. 17 (2021) 22–28. [CrossRef]
- P. Montes, A. Guerra-Librero, P. García, M.E. Cornejo-Calvo, M.D.S. López, T. de Haro, L. Martínez-Ruiz, G. Escames, D. Acuña-Castroviejo, Effect of 5-Azacitidine Treatment on Redox Status and Inflammatory Condition in MDS Patients, Antioxidants 11 (2022) 1–15. [CrossRef]
- D.P. Bartel, MicroRNAs: Genomics, Biogenesis, Mechanism, and Function, Cell 116 (2004) 281–297. [CrossRef]
- K. Saliminejad, H.R. Khorram Khorshid, S. Soleymani Fard, S.H. Ghaffari, An overview of microRNAs: Biology, functions, therapeutics, and analysis methods, J. Cell. Physiol. (2019). [CrossRef]
- C. Chakraborty, A.R. Sharma, G. Sharma, S.S. Lee, The Interplay among miRNAs, Major Cytokines, and Cancer-Related Inflammation, Mol. Ther. - Nucleic Acids 20 (2020) 606–620. [CrossRef]
- J. Lan, Z. Huang, J. Han, J. Shao, C. Huang, Redox regulation of microRNAs in cancer, Cancer Lett. 418 (2018) 250–259. [CrossRef]
- X. Zhang, W.-L. Ng, P. Wang, L. Tian, E. Werner, H. Wang, P. Doetsch, Y. Wang, MicroRNA-21 Modulates the Levels of Reactive Oxygen Species Levels by Targeting SOD3 and TNFα, Cancer Res 72 (2012) 4707–4713. [CrossRef]
- Q. Wang, W. Chen, L. Bai, W. Chen, M.T. Padilla, A.S. Lin, S. Shi, X. Wang, Y. Lin, Receptor-interacting protein 1 increases chemoresistance by maintaining inhibitor of apoptosis protein levels and reducing reactive oxygen species through a microRNA-146a-mediated catalase pathway, J. Biol. Chem. 289 (2014) 5654–5663. [CrossRef]
- Y.A. Veryaskina, S.E. Titov, I.B. Kovynev, S.S. Fedorova, T.I. Pospelova, I.F. Zhimulev, MicroRNAs in the Myelodysplastic Syndrome, Acta Naturae 13 (2021) 4–15. [CrossRef]
- J.S. Choi, M.H. Nam, S.Y. Yoon, S.H. Kang, MicroRNA-194-5p could serve as a diagnostic and prognostic biomarker in myelodysplastic syndromes, Leuk. Res. 39 (2015) 763–768. [CrossRef]
- A. Pons, B. Nomdedeu, A. Navarro, A. Gaya, B. Gel, T. Diaz, S. Valera, M. Rozman, M. Belkaid, E. Montserrat, M. Monzo, Hematopoiesis-related microRNA expression in myelodysplastic syndromes, Leuk. Lymphoma 50 (2009) 1854–1859. [CrossRef]
- D.T. Starczynowski, F. Kuchenbauer, B. Argiropoulos, S. Sung, R. Morin, A. Muranyi, M. Hirst, D. Hogge, M. Marra, R.A. Wells, R. Buckstein, W. Lam, R.K. Humphries, A. Karsan, Identification of miR-145 and miR-146a as mediators of the 5q-syndrome phenotype, Nat. Med. 16 (2010) 49–58. [CrossRef]
- T.D. Bhagat, L. Zhou, L. Sokol, R. Kessel, G. Caceres, K. Gundabolu, R. Tamari, S. Gordon, I. Mantzaris, T. Jodlowski, Y. Yu, X. Jing, R. Polineni, K. Bhatia, A. Pellagatti, J. Boultwood, S. Kambhampati, U. Steidl, C. Stein, W. Ju, G. Liu, P. Kenny, A. List, M. Bitzer, A. Verma, miR-21 mediates hematopoietic suppression in MDS by activating TGF-β signaling., Blood 121 (2013) 2875–2881. [CrossRef]
- X. Wang, P. Liu, H. Zhu, Y. Xu, C. Ma, X. Dai, L. Huang, Y. Liu, L. Zhang, C. Qin, miR-34a, a microRNA up-regulated in a double transgenic mouse model of Alzheimer’s disease, inhibits bcl2 translation, Brain Res. Bull. 80 (2009) 268–273. [CrossRef]
- M.D. Merkerova, Z. Krejcik, H. Votavova, M. Belickova, A. Vasikova, J. Cermak, Distinctive microRNA expression profiles in CD34 bone marrow cells from patients with myelodysplastic syndrome, Eur. J. Hum. Genet. 19 (2011) 313–319. [CrossRef]
- Y. Choi, E.H. Hur, J.H. Moon, B.K. Goo, D.R. Choi, J.H. Lee, Expression and prognostic significance of microRNAs in Korean patients with myelodysplastic syndrome, Korean J. Intern. Med. 34 (2019) 390–400. [CrossRef]
- F.R. Luly, M. Lévêque, V. Licursi, G. Cimino, C. Martin-Chouly, N. Théret, R. Negri, L. Cavinato, F. Ascenzioni, P. Del Porto, MiR-146a is over-expressed and controls IL-6 production in cystic fibrosis macrophages, Sci. Rep. 9 (2019). [CrossRef]
- K. Das, L.V.M. Rao, The Role of microRNAs in Inflammation, Int. J. Mol. Sci. 23 (2022). [CrossRef]
- G.K. Dipa Bhaumik, Scott, S. Schokrpur, Hiruyeh, C.K. Patil, A. V Orjalo, G.J. Lithgow, J. Campisi, MicroRNAs miR - 146a / b negatively modulate the senescence - associated inflammatory mediators IL - 6 and IL - 8, 1 (2009) 402–411. [CrossRef]
- E. Maffioletti, E. Milanesi, A. Ansari, O. Zanetti, S. Galluzzi, C. Geroldi, M. Gennarelli, L. Bocchio-Chiavetto, miR-146a Plasma Levels Are Not Altered in Alzheimer’s Disease but Correlate With Age and Illness Severity, Front. Aging Neurosci. 11 (2020) 11–14. [CrossRef]
- Y. Jiang, J. Zhou, J. Zhao, D. Hou, H. Zhang, L. Li, D. Zou, J. Hu, Y. Zhang, Z. Jing, MiR-18a-downregulated RORA inhibits the proliferation and tumorigenesis of glioma using the TNF-α-mediated NF-κB signaling pathway, EBioMedicine 52 (2020) 102651. [CrossRef]
- Y. Kim, J.W. Cheong, Y.K. Kim, J.I. Eom, H.K. Jeung, S.J. Kim, D. Hwang, J.S. Kim, H.J. Kim, Y.H. Min, Serum microRNA-21 as a potential biomarker for response to hypomethylating agents in myelodysplastic syndromes, PLoS One 9 (2014). [CrossRef]
- Z. Krejčík, M. Beličková, A. Hruštincová, J. Kléma, Z. Zemanová, K. Michalová, J. Čermák, A. Jonášová, M. Dostálová Merkerová, Aberrant expression of the microRNA cluster in 14q32 is associated with del(5q) myelodysplastic syndrome and lenalidomide treatment, Cancer Genet. 208 (2015) 156–161. [CrossRef]
Figure 1.
Changes in the relative expression of the miRNs transcripts in MDS untreated and MDS 5-AZA-treated patients. The following miRNs levels are represented: (A) miR-18a, (B) miR-21, (C) miR-34a, (D) miR-146a. Data are expressed as means ± SEM of miRNs (miR), using miR-30b as an endogenous control in plasma samples of 24 myelodysplastic syndrome (MDS) patients and controls. * p < 0.05, ** p < 0.01, *** p < 0.001 vs. Control.
Figure 1.
Changes in the relative expression of the miRNs transcripts in MDS untreated and MDS 5-AZA-treated patients. The following miRNs levels are represented: (A) miR-18a, (B) miR-21, (C) miR-34a, (D) miR-146a. Data are expressed as means ± SEM of miRNs (miR), using miR-30b as an endogenous control in plasma samples of 24 myelodysplastic syndrome (MDS) patients and controls. * p < 0.05, ** p < 0.01, *** p < 0.001 vs. Control.
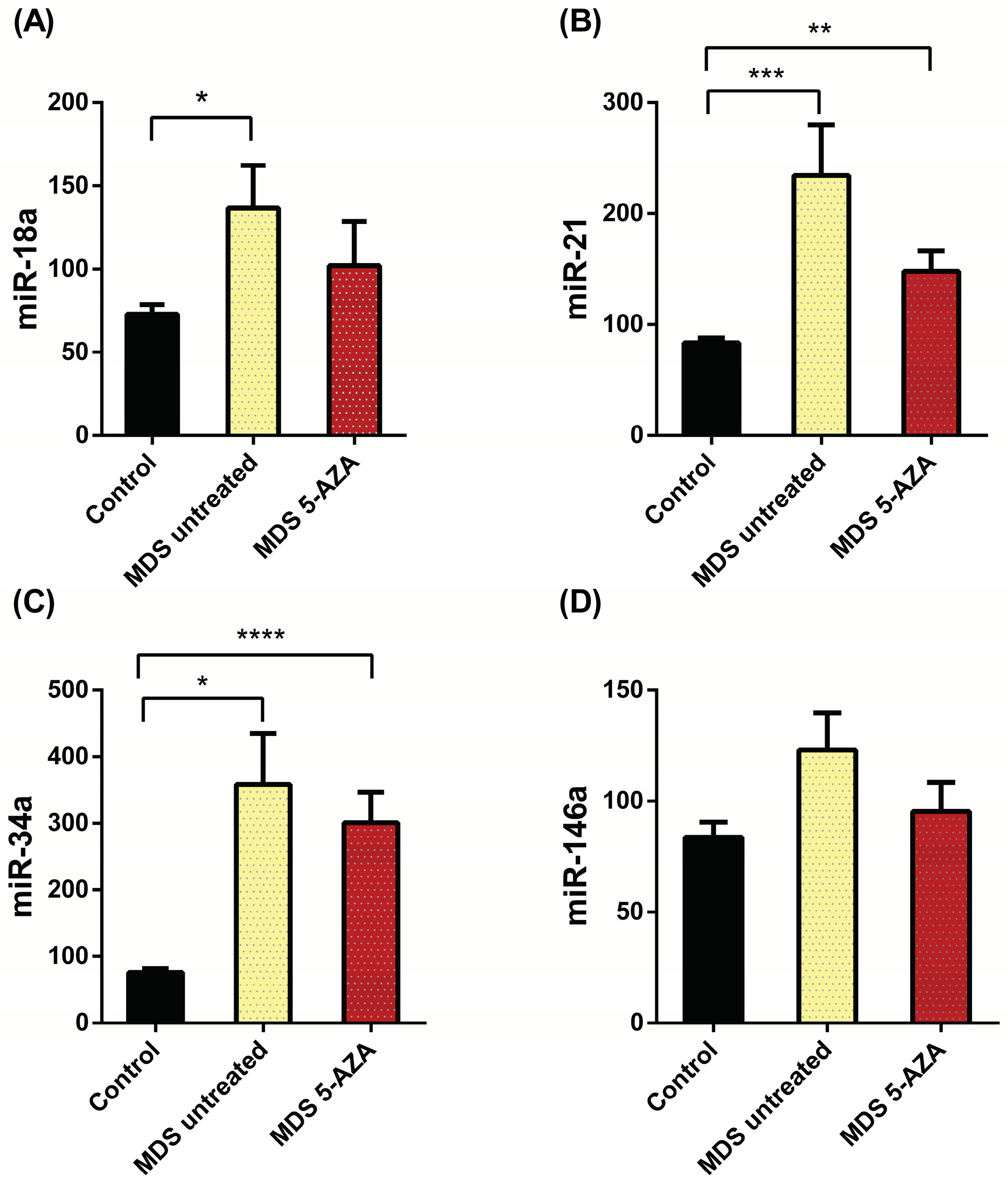
Figure 2.
Changes in the relative expression of the miRNs transcripts in MDS untreated patients during the disease progression. The relative expression of (A) miR-18a, (B) miR-21, (C) miR-34a, and (D) miR-146a is represented. Data are expressed as means ± SEM of miRNs (miR), using miR-30b as an endogenous control in plasma samples of 19 untreated myelodysplastic syndrome (MDS) patients according disease progression: Early Stage (ES) untreated MDS and Advanced Stage (AS) untreated MDS. No significant differences were observed (p > 0.05).
Figure 2.
Changes in the relative expression of the miRNs transcripts in MDS untreated patients during the disease progression. The relative expression of (A) miR-18a, (B) miR-21, (C) miR-34a, and (D) miR-146a is represented. Data are expressed as means ± SEM of miRNs (miR), using miR-30b as an endogenous control in plasma samples of 19 untreated myelodysplastic syndrome (MDS) patients according disease progression: Early Stage (ES) untreated MDS and Advanced Stage (AS) untreated MDS. No significant differences were observed (p > 0.05).
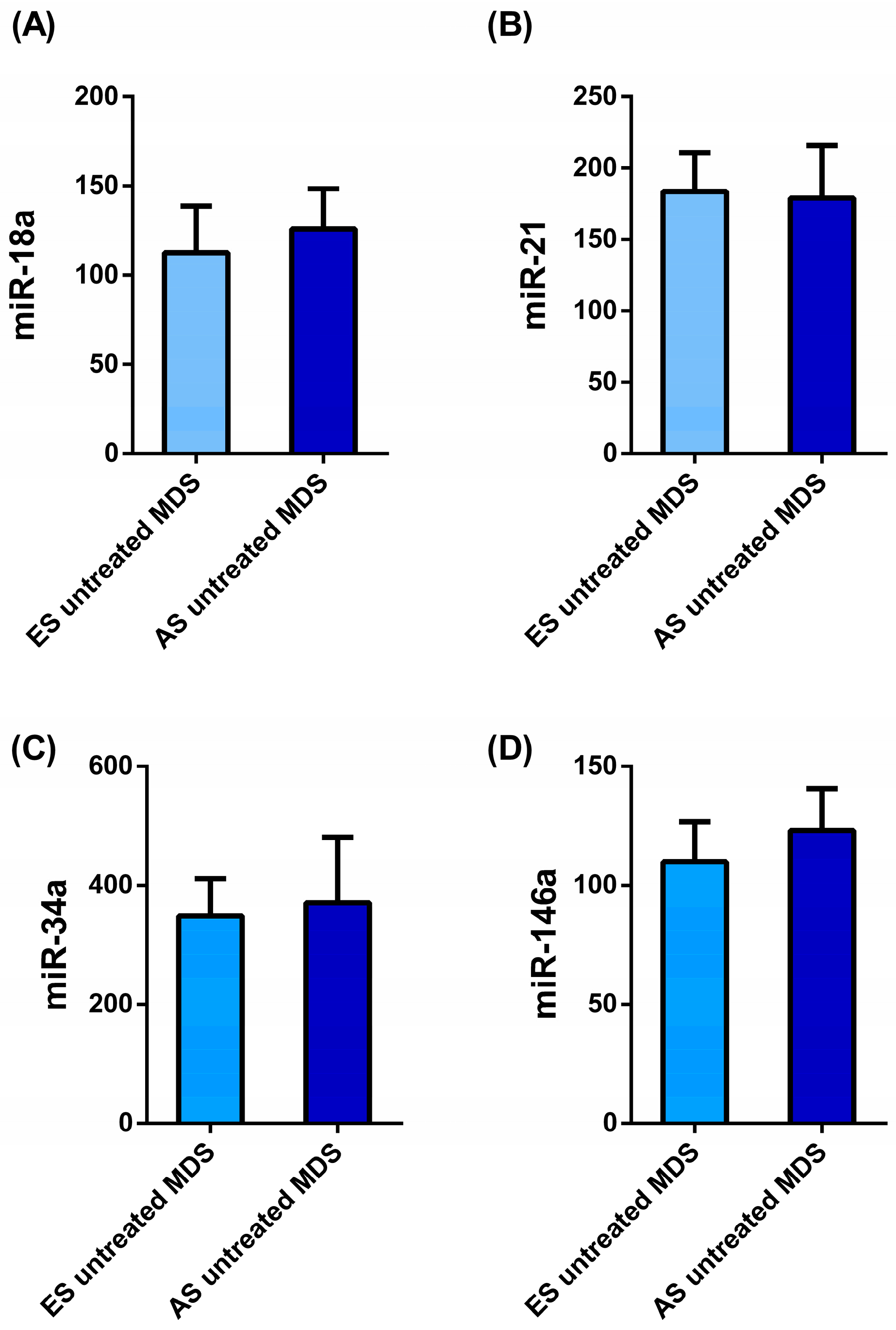
Figure 3.
The relative expression of (A, E, I) miR-18a, (B, F, J) miR-21, (C, G, K) miR-34a, and (D, H, I) miR-146a, using miR-30b as an endogenous control in plasma samples of 24 patients with myelodysplastic syndrome (MDS), classified according to the following risk prognostic factors: IPSS-R score (A, B, C, D), cytogenetic risk (E, F, G, H) and molecular risk (I, J, K, I). The p values were calculated by the non-parametric Mann-Whitney test. Data are presented as mean ± SEM. * p < 0.05 vs. control.
Figure 3.
The relative expression of (A, E, I) miR-18a, (B, F, J) miR-21, (C, G, K) miR-34a, and (D, H, I) miR-146a, using miR-30b as an endogenous control in plasma samples of 24 patients with myelodysplastic syndrome (MDS), classified according to the following risk prognostic factors: IPSS-R score (A, B, C, D), cytogenetic risk (E, F, G, H) and molecular risk (I, J, K, I). The p values were calculated by the non-parametric Mann-Whitney test. Data are presented as mean ± SEM. * p < 0.05 vs. control.
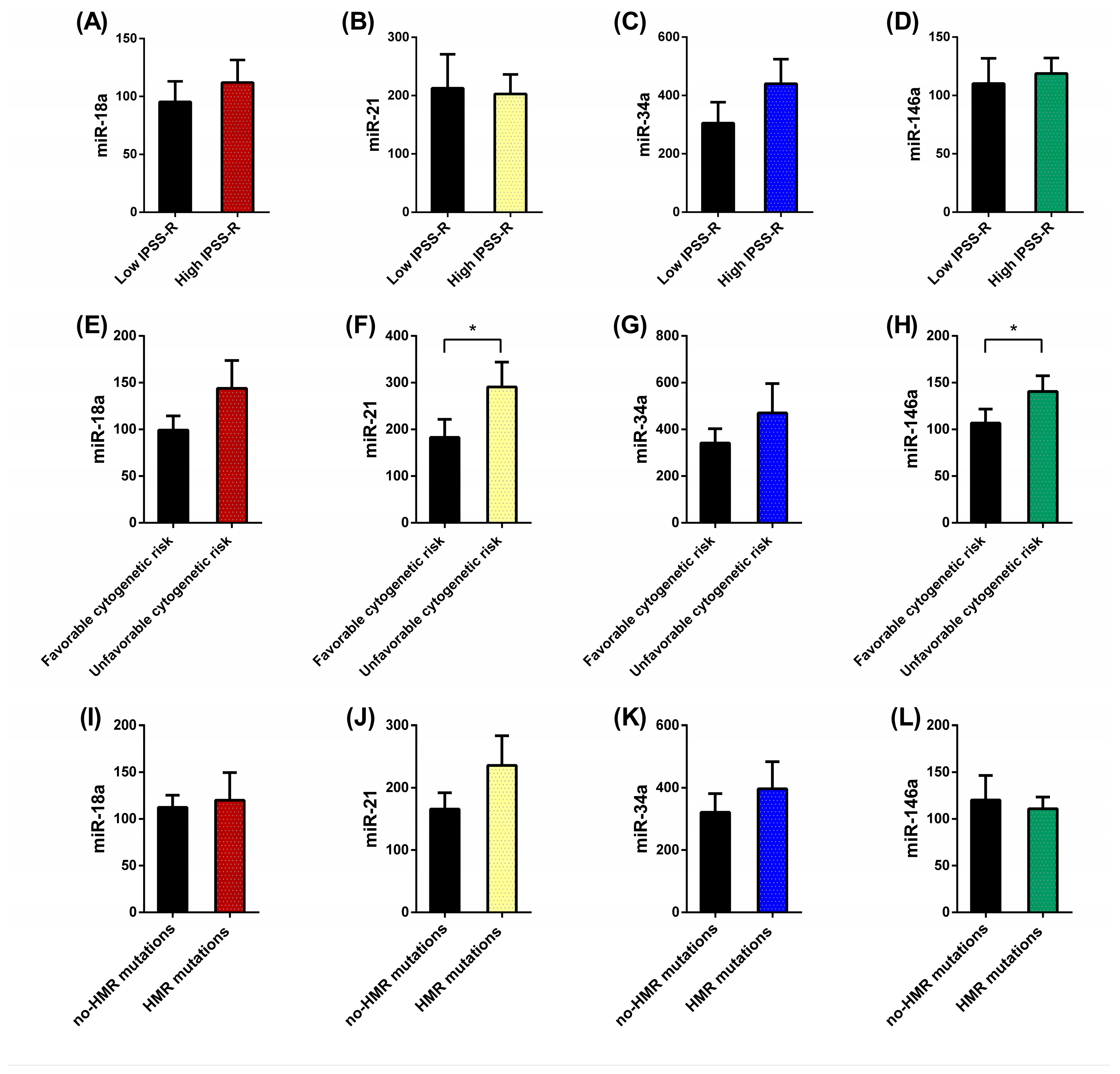
Figure 4.
Correlation analysis between (A) miR-21 and CAT activity, miR-18a and TNF-α (B), and miR-146a and IL-6 (C) in MDS patients. Analysis was done with the Pearson's correlation coefficient.
Figure 4.
Correlation analysis between (A) miR-21 and CAT activity, miR-18a and TNF-α (B), and miR-146a and IL-6 (C) in MDS patients. Analysis was done with the Pearson's correlation coefficient.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



