
Submitted:
26 February 2024
Posted:
27 February 2024
You are already at the latest version
Abstract
The implementation of sentinel lymph node (SLN) biopsy is changing the scenario in the surgical treatment of early-stage cervical cancer and the oncologic safety of replacing bilateral pelvic lymphadenectomy with SLN biopsy is currently under investigation. One of the undisputed values of SLN biopsy is its diagnostic accuracy in detecting low-volume metastases (LVM) via pathologic ultrastaging. In early-stage cervical cancer, the reported incidence of LVM ranges from 4 to 20%. The prognostic impact and the role of adjuvant treatment in patients with LVM is still unclear. Some non-prespecified analyses in prospective studies showed no impact on the oncologic outcomes compared to node-negative disease. However, the heterogeneity of the studies, the differences in the disease stage and the use of adjuvant treatment, and the concomitant pelvic lymphadenectomy (PLND) make any conclusion on this topic hard. Current guidelines suggest considering micrometastasis (MIC) as a node-positive disease, while isolated tumor cells (ITC) as a node-negative disease, with a low level of evidence. This review aims to highlight the unanswered questions about the definition, identification, prognostic and therapeutic role of LVM and underline the present and future challenges we are facing. We hope this review will guide further research, giving robust evidence on LVM and their impact on clinical practice.
Keywords:
cervical cancer
; low-volume metastases
; micrometastases
; isolated tumor cells
; ultrastaging
; sentinel lymph node
1. Introduction
Radical hysterectomy (RH) with sentinel lymph node (SLN) biopsy and bilateral pelvic lymph node dissection (PLND) represents the standard treatment for women with early-stage cervical cancer and no child-bearing desire[1]. Pelvic lymph node involvement is the major prognostic factor in patients with early-stage cervical cancer [2], and an adequate assessment of pelvic lymph node status is mandatory to guide the most appropriate treatment choice. In the last two decades, SLN biopsy has been progressively implemented in routine clinical practice for early-stage cervical cancer treatment. As for other malignancies (i.e., breast cancer and melanoma), the SLN represents the first node draining the lymphatic vessels from the primary cancer. In cervical cancer, its status reflects the status of all other pelvic (and para-aortic) lymph nodes. Two prospective French multicenter clinical trials (SENTICOL 1 [3] and SENTICOL 2 [4]) demonstrated the feasibility, diagnostic accuracy, and safety of SLN biopsy in early-stage cervical cancer. Two further prospective clinical trials (SENTIX [5] and SENTICOL 3 [6]) are currently ongoing. They will probably give the final answer as to whether SLN biopsy alone will replace bilateral PLND in the surgical treatment of early-stage cervical cancer. Low-volume metastases (LVM) are a peculiar pathologic finding of SLN biopsy. Lymph node involvement is categorized as macrometastases (MAC), micrometastasis (MIC), and isolated tumor cells (ITC) depending on the size of the nodal metastasis. Metastases larger than 2 mm in size are classified as MAC; metastases between 0.2 mm and 2 mm in size and/or comprising more than 200 tumor cells are classified as MIC; ITC indicates tumor deposits comprising less than 200 cells and/or less than 0,2 mm in size [7]. MIC and ITC are both included in the LVM definition. The literature still debates the clinical and prognostic impact of LVM. This critical review points out the open questions of the available literature on this topic. We hope to stimulate further research to give robust evidence about the oncological implications of LVM..
2. Sentinel Lymph Node Assessment: How Low-Volume Metastases are Detected
SLN biopsy has two significant diagnostic advantages compared to bilateral PLND. First, SLN mapping can lead to identification of metastatic lymph nodes in atypical lymphatic drainage pathways. In the SENTIX trial, 4% of patients had their SLN detected in the common iliac and pre-sacral areas, which are seldom included in PLND [8]. Second, SLN biopsy is more accurate than PLND in assessing pelvic nodal involvement. SLNs are indeed submitted to an extensive pathological analysis called “ultrastaging”. It consists of cutting serial sections of each SLN paraffin block, on which additional hematoxylin and eosin (H&E) stains and immunohistochemistry (IHC) are performed (Figure 1). Ultrastaging is done if the SLN is negative for metastases at the first routine H&E section. This extensive pathological staging increases the detection of nodal metastases due to the multiple levels of examination of the SLNs [9]. Mainly, it increases the probability of detecting LVM, such as MIC and ITC, that are usually missed when conventional H&E analysis is performed. In a retrospective series by Cibula et al. [10], traditional pathologic evaluation of SLN would have failed to identify 11% of patients with nodal involvement due to LVM recognizable only with ultrastaging.
3. Are Low-Volume Metastases Clinically Meaningful? Controversies of Current Evidence
Among the literature data on the clinical impact of LVM on recurrence and survival in early-stage cervical cancer, the results of the two prospective trials SENTICOL 1 and SENTICOL 2 conflict with most of the retrospective series available (Table 1).
SENTICOL 1 was a French prospective longitudinal study that evaluated the feasibility and diagnostic accuracy of SLN biopsy in the treatment of patients with FIGO IA1 with lymphovascular space invasion (LVSI) to IB1 cervical carcinoma [3]. All patients received SLN biopsy and subsequent PLND, irrespective of the results of intraoperative frozen section analysis of SLN. Conversely, SENTICOL 2 was a prospective multicenter randomized trial assessing the morbidity and oncologic safety of SLN biopsy alone compared to SLN followed by PLND in patients with 2009 FIGO IA1 with LVSI, IA2, IB1, and IIA1 cervical carcinoma [4]. In 2020, Guani et al. performed a conjunct analysis of the results of both trials focusing on the impact of LVM on disease-free survival (DFS) [11]. Among the 321 SENTICOL 1 and 2 patients, 24 (7.5%) had LVM. In particular, MIC were found in 11 patients (3.4%) and ITC in 13 patients (4.1%). No statistically significant difference in 3 years-DFS was found between patients with LVM and node-negative patients (92.7% vs 93.6%, respectively). Two retrospective series align with these results [12,13]. Stany et al. [12] performed a retrospective review of 129 patients treated for early-stage cervical cancer. The ultrastaging of pelvic nodes identified 26 patients with pelvic LVM previously considered node-negative at routine H&E examination. No difference in risk of recurrence or death was found in patients with LVM compared with node-negative patients. Similarly, in their multicenter retrospective case-control study, Buda et al. [13] evaluated the impact of LVM on DFS in 573 women with FIGO 2018 IA2-IB2 cervical cancer. In all the centers, the same ultrastaging protocol was adopted in the pathologic processing of SLN [14]. Among the 573 patients included in the study, 85 (15%) had positive nodes, and 21 (3,6%) were found with MIC or ITC only in the SLN. No difference in risk of relapse and DFS was found in the LVM population (OR 0.65; 95% CI 0.36 – 1,20) compared to the node-negative group.
These findings contrast with the results of a large retrospective study by Cibula et al. and other retrospective series [15,16,17,18,19] . In 2012, Cibula et al. [15] collected the largest retrospective series addressing the prognostic significance of LVM in early-stage cervical cancer. Six hundred forty-five patients with FIGO 2009 IA2-IIB cervical carcinoma were included in the analysis from eight tertiary centers. All patients received SLN biopsy followed by systematic bilateral PLND, irrespective of the uterine procedure performed. MIC and ITC were found in 7.1% and 3.9% of patients, respectively. The presence of MIC was a significant independent factor for reduced overall survival (OS) (HR 4.60, 95% CI 1.34 - 15.77). Conversely, ITC did not increase the risk of recurrence, nor were associated with decreased OS. Similar results were found in the single-institution series reported by Kocian et al. [16]. Among the 226 patients with early-stage cervical carcinoma, 14 (6,2%), 16 (7,1%), and 8 (3,5%) patients were found with MAC, MIC, and ITC in the SLN, respectively. Of note, 2 patients with MIC and 1 with ITC in the SLN also had MIC and ITC in the non-sentinel pelvic lymph nodes, respectively. After a median follow-up of 65 months, DFS reached 93%, 89%, 69%, and 87% in the node-negative, MAC, MIC, and ITC groups, respectively.
A recently published meta-analysis by Guani et al. aimed to comprehensively evaluate the available data on the clinical impact of LVM in early-stage cervical cancer [20]. A total of 2191 patients from 7 studies were retrieved. The survival analyses compared the LVM (MIC + ITC) population to the node-negative one. Comprehensively, a negative impact on DFS and OS was found for LVM, with HRs of 2.60 (95% CI: 1.55 – 4.34) and 5.65 (95% CI: 2.81 – 11.39), respectively.
Despite the undoubted robustness of Guani et al.’s metanalysis findings, some questions remain unresolved. First, the definition of LVM is arbitrary and adapted from breast cancer staging [7]. Second, no specific analysis was performed for ITC due to the exiguity of the ITC population and the limited number of events. Therefore, no conclusions could be drawn on their clinical significance. Third, the studies included in the metanalysis are limited by a great heterogeneity concerning the study design, the sample size, the stage of disease included in the study, the use of adjuvant treatment, the concomitant PLND and surgical approach. For example, in the Cibula et al. series [15], even patients with 2009 FIGO stage IB2, IIA1-2, and IIB cervical cancer were included. These tumors are now almost universally considered “locally advanced” and treated with exclusive curative radio-chemotherapy. Tumor size, upper vaginal, and parametrial involvement are well-known risk factors for disease relapse and nodal involvement. Including patients with independent poor prognostic factors could have hidden the real impact of LVM on recurrence and survival. Fourth, the lack of a shared ultrastaging technique and protocol may impact the detection of LVM and, therefore, could have influenced the results. An internationally validated protocol for SLN ultrastaging has not been proposed yet, and ultrastaging techniques vary among different institutions. Given the importance of ultrastaging in the detection of LVM, the lack of a standardized protocol raises the question of whether literature data on the prognostic impact of LVM are comparable. Last, little information is available on the recurrence time and site in case of primary treatment failure. In their meta-analysis, Guani et al. [20] estimated that most recurrences in patients with MIC occurred within 3 years after primary treatment. However, they could not retrieve any information about the recurrence site or draw any conclusions on the impact of LVM on disease diffusion and recurrence patterns.
3.1. Macrometastases, Micrometastases, Isolated Tumor Cells. A matter of Size?
Lymph node involvement is categorized as MAC, MIC, and ITC depending on the size of the nodal metastasis according to the American Joint Committee on Cancer (AJCC) recommendations on breast cancer staging [7]. It has been recently implemented in the TNM 8, where MAC and MIC are reported as pN1 and ITC as pN0. Subsequently, these categories have been widely applied to other tumor sites and gynecological cancers (i.e., endometrial and vulvar). Still, the clinical impact of these different types of metastases has not yet been validated specifically for cervical cancer.
Recently, Dostalek et al. [21] addressed this issue and performed a subgroup analysis of the SCCAN project, a multicenter retrospective observational cohort study evaluating the recurrence patterns in patients with cervical cancer. In their series of 172 patients with nodal involvement (79 MAC, 54 MIC and 39 ITC), the authors tried to select the minimum cut-off of nodal metastasis size associated with a better prognosis compared to the entire cohort of node-positive patients. Particularly, they rearranged the cohort with LVM by dividing patients into subgroups according to the size of metastases at intervals of 0,1 mm, ranging from 0,1 to 1 mm. They found that patients with more than 0.4 mm nodal metastases had a significantly shorter DFS than node-negative patients (HR 2.3; 95% CI 1.2-4.6). Additionally, they could not find a metastasis size cut-off that was able to identify a subgroup of patients with a significantly better prognosis than the node-positive cohort. Therefore, the authors concluded that stratifying patients into MIC and MAC according to the size of nodal metastases is artificial and has no prognostic impact. They suggested that patients with positive nodes should be managed uniformly until further evidence regarding the prognostic impact of “very low” volume metastases is available.
Comprehensively, MIC seems to be associated with a poorer prognosis compared to ITC. As previously described, in Guani et al. meta-analysis [20], the authors performed a survival analysis in two different settings, separately comparing the LVM (MIC + ITC) and the MIC populations to the node-negative cohort. A higher risk of recurrence and death was found in the MIC population compared to the combined LVM group. Particularly, HRs for recurrence were 2.60 (95% CI: 1.55 – 4.34) and 4.10 (95% CI: 2.71 – 6.20) in the LVM and MIC population, respectively, whereas HRs for death reached 5.65 (95% CI: 2.81 – 11.39) and 6.94 (95% CI: 2.56 – 18.81) in the corresponding subgroups. Although a specific analysis for ITC was not performed due to the limited number of cases and events, the lower hazards in the combined LVM population suggest that patients with ITC had a better prognosis than the MIC population.
3.2. Impact of Adjuvant Therapy and Complementary PLND
Pelvic lymph node involvement is considered a high-risk factor for treatment failure, like parametrial invasion and positive surgical margins. These factors represent an indication for adjuvant radio-chemotherapy [1]. Involvement of pelvic (and para-aortic) lymph nodes has historically been detected by standard routine pathologic examination with H&E staining, and only in the last two decades, the issue of LVM has emerged. A consensus on the indication for adjuvant treatment in the case of LVM is currently lacking. The 2018 FIGO staging [22] includes MIC in the node-positive group, while it is suggested that the presence of ITC is recorded without changing the stage. Discordance in treatment indications and patient selection emerge in prospective and retrospective studies addressing the clinical impact of LVM [11,16,19]. Despite this, clinical practice has changed over the years, mainly due to the findings of early retrospective reports that elucidated the possible detrimental effect of LVM on survival [15,16,17,18,19].
Notably, pelvic lymph node involvement, either macro- or micro-metastatic, is usually associated with local tumor risk factors, such as LVSI, deep stromal invasion and tumor size. The combination of these tumor risk factors has historically represented an indication for adjuvant radiotherapy according to Sedlis’ criteria (intermediate risk group) [23]. Therefore, in many studies evaluating the impact of LVM on oncologic outcomes in patients with early-stage cervical cancer, a non-negligible amount of patients received adjuvant treatment irrespective of LVM nodal status. Similar to historical studies evaluating the extent of parametrial radicality in surgical treatment of early-stage cervical cancer [24], the use of adjuvant therapy may have interfered with the real impact of LVM on prognosis. For example, in SENTICOL 1 [3], patients with LVM received adjuvant treatment if other concomitant risk factors were present. Of the 13 patients with MIC or ITC, 4 (31%) received an adjuvant treatment. Particularly, one received adjuvant radio-chemotherapy because of parametrial involvement, and the other three received adjuvant radiotherapy in the presence of LVSI. Similarly, in the retrospective series by Stany et al. [12], no difference in risk of recurrence or death was found in patients with LVM compared with node-negative patients, but the post-operative radiation rate was significantly higher in the LVM group (38,5% vs 18,4%). On the one hand, this substantiates the association of the presence of LVM with other significant prognostic factors that are likely an indication for adjuvant treatment. On the other hand, the use of adjuvant radiotherapy could have masked the detrimental effect of LVM on survival outcomes.
Contrarily, in the already mentioned series of Cibula et al. [15], the presence of LVM was associated with decreased OS, even if a high proportion of patients with MIC and ITC received adjuvant treatment. Overall, 33% of patients received adjuvant radiotherapy or radio-chemotherapy, whereas in the LVM population, 82.6% of patients with MIC and 52% with ITC received adjuvant therapy. Precise indication for adjuvant treatment was not specified in the study, and the adjuvant treatment was administered according to internal guidelines of the single institutions participating in the study. However, extrapolation of the data reported in the paper suggests that in a non-negligible proportion of cases, an indication for adjuvant treatment could have been set based on local risk factors. For instance, parametrial involvement was found in 7.1% of patients and represents per se an indication for adjuvant radio-chemotherapy irrespective of nodal status. Additionally, MIC were found in 12.7% of patients with FIGO IIA-IIB and 12.1% of patients with FIGO IB2 tumors. Considering that 36.2% and 43.6% of patients with IB2 and IIA-B tumors had LVSI in their series, it is easy to imagine that the majority of these patients would have received adjuvant treatment irrespective of nodal status. Although the presence of MIC was an independent prognostic factor for OS in the multivariate analysis, patients with locally advanced cervical cancer have independent poor prognostic factors. Therefore, the prognostic significance of LVM is challenging to assess in such a heterogeneous cohort of patients. From another perspective, the knowledge of nodal status in those patients requiring adjuvant treatment according to local tumor risk factors would have been superfluous since the treatment strategy would not have changed according to nodal status. This is in line with the role of LVM observed in endometrial cancer by Ghoniem et al. [25], who reported a higher risk of recurrence in patients with LVM in the SLN and uterine “high-risk” criteria and an almost negligible risk of relapse in patients with low-risk early-stage endometrial cancer with ITC in the SLN.
Currently, only one series excluding patients who received adjuvant treatment is available. Colturato et al. [17] performed a retrospective ultrastaging pathologic analysis of pelvic nodes retrieved from patients with stage IB1-IIA cervical cancer who received exclusive surgical treatment (radical hysterectomy with bilateral PLND). Patients with LVM in the pelvic nodes had an 11.73 times higher risk of recurrence compared to node-negative patients. However, the study’s retrospective nature, the limited sample size, the posterior performance of ultrastaging, and the lack of information about the mean number of positive lymph nodes per patient make the results of this study unlikely to be generalizable. Similarly, Fregnani et al. [18] retrospectively evaluated nodal status by IHC pathologic analysis of pelvic lymph nodes in 289 patients with FIGO IB-IIA cervical carcinoma. In their series, only 36.4% of patients with LVM received adjuvant treatment leading to a significantly worse prognosis of LVM patients compared to patients without LN metastases (HR 3,2; 95% CI: 1,1-9,6). Again, ultrastaging was performed posteriorly, information about the mean number of positive lymph nodes per patient and the site of recurrence is lacking, and patients with high-risk features were included in the analysis. For instance, 11% of patients had a tumor greater than 4 cm in size, 2,5% had parametrial involvement and 4% had positive surgical margins, which are per se associated with a higher risk of tumor recurrence.
Despite the limitations, the findings of these retrospective series have led to routine administration of adjuvant therapy in patients with LVM, especially if MIC are detected. The change over time in clinicians’ attitude to treat LVM is highlighted in the two French prospective trials SENTICOL 1 and SENTICOL 2 [3,4,11]. In contrast with SENTICOL 2 [4], where patients with both MIC and ITC were treated with adjuvant radio-chemotherapy, SENTICOL 1 [3] was designed when SLN biopsy had not been routinely implemented in routine clinical practice and the issue of LVM had not emerged yet. Patients with LVM received adjuvant treatment if other concomitant risk factors were present, whereas an isolated finding of MIC and ITC did not represent an indication for further treatment. Consequently, in SENTICOL 2, a higher rate of adjuvant treatment was recorded compared to SENTICOL 1. Despite this, no statistical difference in DFS was found between patients with LVM receiving adjuvant radio-chemotherapy compared to those who did not (1/13 (7,7%) vs 1/11 (9%), p = NA) [11]. Of note, the population included in both studies represents those patients with a true primary surgical indication, since only those with tumor size less than 4 cm were included in both studies. However, some other aspects must be considered. First, the small sample size and the low number of events recorded in both trials make these studies underpowered to detect any survival impact of LVM. Second, in SENTICOL 1, all patients received concurrent SLN biopsy and systematic PLND. This surgical approach could have mitigated the lower use of adjuvant radio-chemotherapy in SENTICOL 1 patients. In fact, in the combined SENTICOL 1 and 2 study by Guani et al. [11], the authors performed a DFS analysis stratifying patients according to the type of nodal staging they received, SLN biopsy alone versus SLN biopsy followed by PLND. The authors found a favorable DFS trend for patients with LVM treated with concomitant SLN biopsy and PLND compared to those receiving SLN biopsy alone. One out of 6 patients receiving SLN biopsy alone experienced recurrence, whereas 1 of 17 patients receiving SLN biopsy plus PLND recurred. Although of no statistical significance, this trend seems to confirm the findings of Zaal et al. [26], who performed a multicenter retrospective analysis to evaluate the impact of PLND following SLN biopsy in 645 patients with FIGO IA-IIB cervical cancer. PLND was found to give no survival advantage in patients with negative or macrometastatic SLN. In contrast, an overall survival benefit was described if a systematic PLND with the removal of more than 16 nodes was performed in patients with LVM in the SLN.
3.3. The Site of Recurrence: Is It Negligible?
The results of the LACC trial by Ramirez et al. [27] have elucidated a negative impact on DFS and OS of minimally invasive surgery compared to laparotomy and have led to a drastic change worldwide in the surgical approach for cervical cancer treatment. Most of the data available on the oncologic impact of LVM refer to the pre-LACC era, when surgeons’ preference and skills guided the surgical approach. Although information about the surgical approach is not retrievable in most of the studies, a non-negligible number of patients received minimally invasive surgery, which could have impacted the incidence and pattern of recurrences. For example, among the 321 patients in the combined SENTICOL 1 and 2 population, 217 underwent a laparoscopic procedure, whereas only 21 received open surgery [11]. Similarly, 46% of patients included in Buda et al. series [13] underwent laparoscopic radical hysterectomy. Furthermore, information on recurrence sites is almost always lacking in most of the studies previously reported. In the only patient with MIC in the SLN who developed recurrence in the SENTICOL 1 trial, recurrent disease was recorded as pelvic with no further distinction between central parametrial and pelvic side wall recurrence. Similarly, among the patients with LVM who recurred in the series by Kocian et al. [16], no precise definition of the site of recurrence is specified. Two patients developed distant metastatic disease, one developed a recurrence in the pelvis, and 3 patients developed both distant and local recurrent disease. No distinction between distant parenchymal and/or para-aortic nodal involvement nor between parametrial and/or pelvic wall recurrence was specified. It is our opinion that knowledge about the site of recurrence of patients with LVM is of great importance since the true impact of LVM on prognosis and their weight among other risk factors would be elucidated, even after adjuvant treatment administration. For instance, in the small prospective series by Nica et al. [28], the only patient treated with a radical hysterectomy who had LVM in the SLN and experienced central pelvic recurrence, presented a high-risk disease, with parametrial node involvement, and positive vaginal margins. We think that this patient would have recurred irrespective of SLN micro-metastatic involvement. Again, the coexistence of multiple high-risk factors makes it impossible to assess the true impact of LVM on prognosis.
4. Present and Future Challenges
The available literature results present some limitations about the definition of LVM, the role of ITC when considered separately from MIC, and the heterogeneity among the studies available. Therefore, some questions still need to be answered.
One of the first challenges would be understanding the actual prevalence of LVM in specific populations of patients based on the local risk factors, like stage and LVSI. This will help understand the real impact of the problem, especially in patients who will not be candidates for adjuvant treatment (e.g., low-risk and intermediate-risk populations).
In current 2023 ESGO-ESTRO-ESP guidelines [1], adjuvant radio-chemotherapy is indicated in case of metastatic involvement of pelvic lymph nodes (either MAC or MIC) with a IV-A level of evidence, whereas it may be considered in case of ITC in the SLN with a IV-C level of evidence. These statements rely mainly on the results of retrospective studies with great heterogeneity in patients’ selection and adjuvant treatment indication. Particularly, a non-negligible amount of patients included in the studies evaluating the impact of LVM received adjuvant treatment according to local risk factors, irrespective of the presence of LVM in the pelvic nodes, and this may have interfered with estimating the real impact of LVM on prognosis. Adjuvant treatment in the management of early-stage cervical cancer is indicated in case of high-risk criteria, namely parametrial infiltration, positive margins, and lymph node involvement, whereas its use in the case of Sedlis’ intermediate risk factors [23] is a matter of debate and not universally accepted. If the results of the CERVANTES Trial [29] will not support the use of adjuvant treatment in case of intermediate risk factors, it is our opinion that evaluation of patients with nodal LVM and no further local risk factors requiring adjuvant treatment will be the best chance for assessing the true impact of LVM on prognosis.
To our knowledge, the prognostic impact of LVM, either MIC or ITC, confined to the SLN only (without further pelvic lymph node involvement), has not yet been investigated. Two ongoing trials, SENTIX [5] and SENTICOL 3 [6], will probably confirm the reliability of SLN biopsy alone for nodal staging in early-stage cervical cancer. They will likely align with the results of the metanalysis recently published by Parpinel et al. [30], showing similar survival outcomes after SLN biopsy alone and PLND. If SLN biopsy without concurrent PNLD will become the standard surgical assessment of nodal status, the scientific community has to first evaluate the prognostic impact of LVM in the SLN without further nodal involvement. In many of the retrospective series cited above, the mean number of positive lymph nodes is not mentioned and, in some cases, SLN assessment was not even performed. In Kocian et al. series [16], a comprehensive description of nodal status was reported combining the results of SLN ultrastaging and standard H&E analysis of non-sentinel pelvic lymph nodes. Specifically, 1 patient with ITC and 2 patients with MIC in their SLN had ITC and MIC in non-sentinel pelvic nodes, respectively, whereas 7 patients with ITC and 14 patients with MIC in the SLN had no further involvement of pelvic lymph nodes. However, no specific analysis was performed for patients with LVM confined to the SLN only. Recently, Pache et al. [31] published an ancillary analysis of SENTICOL 1-2 trials to exploit the risk factors associated with non-SLN metastases in patients with positive SLN. All non-SLNs were analyzed via ultrastaging to avoid missing LVM. Among 52 patients with at least one positive SLN, metastatic involvement of non-SLN was identified in 7 patients (13,5%). Elder age and LVSI were independently associated with non-SLN involvement. Interestingly, among the 7 patients with non-SLN metastatic involvement, 4 patients had MAC in their SLN, one patient had ITC in the SLN and LVM (MIC + ITC) in non-SLN, and two patients had MIC in their SLN and MAC in non-SLN. Unfortunately, no survival analysis was carried out, and the prognostic impact of multiple LVM involvement of both SLN and non-SLN remains unclear. We believe that isolated LVM in the SLN only may have a better impact on prognosis than multiple nodal involvement. Further investigations should be carried out on this topic; we believe the risk of further nodal involvement other than SLN should be accurately assessed, especially if ITC are found. According to the data we presented, MIC are associated with a significantly higher risk of recurrence and death compared to node-negative patients and seem to require adjuvant treatment. In contrast, no conclusive data is available on ITC. Probably, isolated MIC in the SLN would need further treatment equally to MAC or multiple MIC patients; on the contrary, we think that adjuvant treatment in the case of ITC may be an over-treatment, especially if it will be demonstrated that ITC in the SLN are unlikely associated with further nodal involvement.
Another critical challenge will be to standardize the ultrastaging protocols of the SLN worldwide. Different protocols may lead to varying prevalences of LVM in the same patient population. Additionally, the size and definition of MAC, MIC, and ITC are based on the AJCC recommendations on breast cancer and applied to cervical cancer as well as other gynecological cancers (i.e., endometrial and vulvar). However, the validation for each gynecological cancer would be beneficial. This is an urgent need for all gynecological cancers in which SLN is now routine clinical practice (cervical, endometrial and vulvar cancer).
5. Conclusions
SLN biopsy represents one of the most valuable achievements in the era of precision oncology. As for other malignancies, SLN biopsy has led to a higher diagnostic performance of nodal status assessment compared to standard bilateral PLND in the treatment of early-stage cervical cancer. Implementing SLN in routine clinical practice has raised the question of whether LVM are clinically relevant in treating cervical cancer. As for endometrial cancer, the risk of relapse and the need for adjuvant treatment depend on multiple risk factors, many of which are interlaced with each other and can difficulty be extrapolated. This makes the prognostic impact of LVM challenging to evaluate and currently available studies present many limitations. Particularly, literature is debating on the impact of LVM on prognosis and whether adjuvant radio-chemotherapy is indicated in this group of patients. Comprehensively, based on the results of the recently published meta-analysis by Guani et al. [20], we believe that the prognosis of patients with micrometastatic pelvic lymph node involvement seems similar to those with MAC. In contrast, no conclusive data are available on the clinical significance of ITC.
We believe that excluding confounders and an accurate selection of inclusion criteria to avoid the need for adjuvant treatment based on “local” risk factors would probably lead to a better understanding of the prevalence and prognostic impact of LVM in early-stage cervical cancer. Additionally, we believe that designing a prospective study to assess the LVM impact accurately would be challenging since cervical cancer is declining worldwide and early-stage cervical cancer has an excellent prognosis. The results of two prospective trials, SENTIX and SENTICOL 3, are awaited. We hope that accurate integration with available retrospective series will help elucidate the prognostic role of both MIC and ITC and guide the choice of the most appropriate adjuvant treatment.
Author Contributions
Conceptualization: T.B., T.G., F.L.; writing—original draft preparation: T.B. and T.G.; writing—review and editing, T.B., T.G., G.D.M., G.T., S.N., R.F., and F.L.; supervision, F.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cibula D, Raspollini MR, Planchamp F, et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer - Update 2023. Int J Gynecol Cancer. 2023, 33, 649–666. [Google Scholar] [CrossRef] [PubMed]
- Stehman FB, Bundy BN, DiSaia PJ, et al. Carcinoma of the cervix treated with radiation therapy. A multi-variate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer. 1991, 67, 2776–2785. [Google Scholar] [CrossRef]
- Lécuru F, Mathevet P, Querleu D, et al. Bilateral negative sentinel nodes accurately predict absence of lymph node metastasis in early cervical cancer: results of the SENTICOL study. J Clin Oncol. 2011, 29, 1686–1691. [Google Scholar] [CrossRef] [PubMed]
- Mathevet P, Lécuru F, Uzan C, et al. Sentinel lymph node biopsy and morbidity outcomes in early cervical cancer: Results of a multicentre randomised trial (SENTICOL-2). Eur J Cancer 2021, 148, 307–315. [CrossRef] [PubMed]
- Cibula D, Dusek J, Jarkovsky J, et al. A prospective multicenter trial on sentinel lymph node biopsy in patients with early-stage cervical cancer (SENTIX). Int J Gynecol Cancer. 2019, 29, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Lecuru FR, McCormack M, Hillemanns P, et al. SENTICOL III: an international validation study of sentinel node biopsy in early cervical cancer. A GINECO, ENGOT, GCIG and multicenter study. Int J Gynecol Cancer. 2019, 29, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Zhu H, Doğan BE. American Joint Committee on Cancer’s Staging System for Breast Cancer, Eighth Edition: Summary for Clinicians. Eur J Breast Health. 2021, 17, 234–238. [Google Scholar] [CrossRef]
- Cibula D, Kocian R, Plaikner A, et al. Sentinel lymph node mapping and intraoperative assessment in a prospective, international, multicentre, observational trial of patients with cervical cancer: The SENTIX trial. Eur J Cancer 2020, 137, 69–80. [CrossRef]
- Dundr P, Cibula D, Němejcová K, et al. Pathologic Protocols for Sentinel Lymph Nodes Ultrastaging in Cervical Cancer. Arch Pathol Lab Med. Published. 2019.
- Cibula D, Abu-Rustum NR, Dusek L, et al. Bilateral ultrastaging of sentinel lymph node in cervical cancer: Lowering the false-negative rate and improving the detection of micrometastasis. Gynecol Oncol. 2012, 127, 462–466. [Google Scholar] [CrossRef]
- Guani B, Balaya V, Magaud L, et al. The Clinical Impact of Low-Volume Lymph Nodal Metastases in Early-Stage Cervical Cancer: The Senticol 1 and Senticol 2 Trials. Cancers. 2020, 12, 1061. [Google Scholar] [CrossRef] [PubMed]
- Stany MP, Stone PJ, Felix JC, et al. Lymph Node Micrometastases in Early-Stage Cervical Cancer are Not Predictive of Survival. Int J Gynecol Pathol. 2015, 34, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Buda A, Casarin J, Mueller M, et al. The impact of low-volume metastasis on disease-free survival of women with early-stage cervical cancer. J Cancer Res Clin Oncol. 2021, 147, 1599–1606. [Google Scholar] [CrossRef] [PubMed]
- Grassi T, Dell’Orto F, Jaconi M, et al. Two ultrastaging protocols for the detection of lymph node metastases in early-stage cervical and endometrial cancers. Int J Gynecol Cancer. 2020, 30, 1404–1410. [Google Scholar] [CrossRef] [PubMed]
- Cibula D, Abu-Rustum NR, Dusek L, et al. Prognostic significance of low volume sentinel lymph node disease in early-stage cervical cancer. Gynecol Oncol. 2012, 124, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Kocian R, Slama J, Fischerova D, et al. Micrometastases in Sentinel Lymph Nodes Represent a Significant Negative Prognostic Factor in Early-Stage Cervical Cancer: A Single-Institutional Retrospective Cohort Study. Cancers. 2020, 12, 1438. [Google Scholar] [CrossRef] [PubMed]
- Colturato LF, Signorini Filho RC, Fernandes RC, et al. Lymph node micrometastases in initial stage cervical cancer and tumoral recurrence. Int J Gynaecol Obstet. 2016, 133, 69–75. [Google Scholar] [CrossRef]
- Fregnani JH, Latorre MR, Novik PR, et al. Assessment of pelvic lymph node micrometastatic disease in stages IB and IIA of carcinoma of the uterine cervix. Int J Gynecol Cancer. 2006, 16, 1188–1194. [Google Scholar] [CrossRef]
- Marchiolé P, Buénerd A, Benchaib M, et al. Clinical significance of lympho vascular space involvement and lymph node micrometastases in early-stage cervical cancer: a retrospective case-control surgico-pathological study. Gynecol Oncol. 2005, 97, 727–732. [Google Scholar] [CrossRef]
- Guani B, Mahiou K, Crestani A, et al. Clinical impact of low-volume lymph node metastases in early-stage cervical cancer: A comprehensive meta-analysis. Gynecol Oncol. 2022, 164, 446–454. [Google Scholar] [CrossRef]
- Dostálek L, Benešová K, Klát J, et al. Stratification of lymph node metastases as macrometastases, micrometastases, or isolated tumor cells has no clinical implication in patients with cervical cancer: Subgroup analysis of the SCCAN project. Gynecol Oncol 2023, 168, 151–156. [CrossRef] [PubMed]
- Bhatla N, Berek JS, Cuello Fredes M, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Sedlis A, Bundy BN, Rotman MZ, et al. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group Study. Gynecol Oncol. 1999, 73, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Bianchi T, Grassi T, Bazzurini L, et al. Radical Hysterectomy in Early-Stage Cervical Cancer: Abandoning the One-Fits-All Concept. J Pers Med. 2023, 13, 1292. [Google Scholar] [CrossRef] [PubMed]
- Ghoniem K, Larish AM, Dinoi G, et al. Oncologic outcomes of endometrial cancer in patients with low-volume metastasis in the sentinel lymph nodes: An international multi-institutional study. Gynecol Oncol. 2021, 162, 590–598. [Google Scholar] [CrossRef] [PubMed]
- A Zaal A, Zweemer RP, Zikán M, et al. Pelvic lymphadenectomy improves survival in patients with cervical cancer with low-volume disease in the sentinel node: a retrospective multicenter cohort study. Int J Gynecol Cancer. 2014, 24, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Ramirez PT, Frumovitz M, Pareja R, et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N Engl J Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Nica A, Gien LT, Ferguson SE, et al. Does small volume metastatic lymph node disease affect long-term prognosis in early cervical cancer? Int J Gynecol Cancer. 2020, 30, 285–290. [Google Scholar] [CrossRef]
- Cibula D, Borčinová M, Kocian R, et al. CERVANTES: an international randomized trial of radical surgery followed by adjuvant (chemo) radiation versus no further treatment in patients with early-stage, intermediate-risk cervical cancer (CEEGOG-CX-05; ENGOT-CX16). Int J Gynecol Cancer 2022.
- Parpinel G, Laas-Faron E, Balaya V, et al. Survival after sentinel lymph node biopsy for early cervical cancers: a systematic review and meta-analysis. Int J Gynecol Cancer. 2023, 33, 1853–1860. [Google Scholar] [CrossRef]
- Pache B, Tantari M, Guani B, et al. Predictors of Non-Sentinel Lymph Node Metastasis in Patients with Positive Sentinel Lymph Node in Early-Stage Cervical Cancer: A SENTICOL GROUP Study. Cancers. 2023, 15, 4737. [Google Scholar] [CrossRef]
Figure 1.
Pathologic Ultrastaging of the SLN.
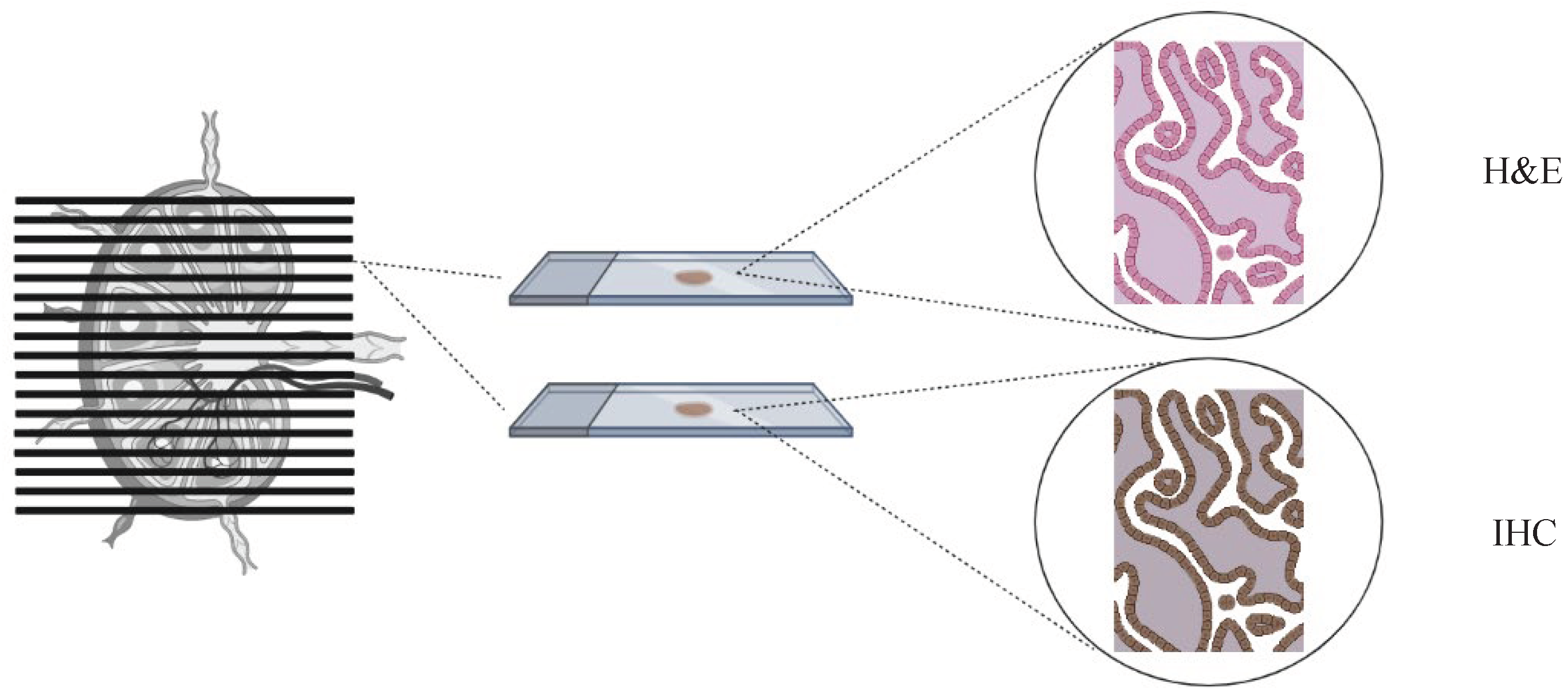

Table 1.
Available literature: study design, population and outcomes explored.
| Author | Date | Study design | Population | FIGO Stage | Prevalence of isolated LVM | Surgical LNtreatment | AdjuvantTreatment | Negative impact of LVM on oncologic outcome* | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LVM | ITC only | MIC only | Node negative | LVM | Endpoint | LVM | MIC | ITC | ||||||
| Marchiolè et al. | 2005 | Retrospective | 52 | IA2-IIB (FIGO 1988) | 12/52 (23%) | 6/52 (11,5%) | 6/52 (11,5%) | PLND | NA | NA | RR | Yes | Yes | Yes |
| Fregnani et al. | 2006 | Retrospective | 289 | IB-IIA (FIGO 1988) | 11/289 (3,8%) | NA | NA | PLND | NA | 4/11 (36%) | DFS | Yes | NA | NA |
| Cibula et al. | 2012 | Retrospective | 645 | IA1-IIB (FIGO 2009) | 71/645 (11%) | 25/645 (4%) | 46/645 (7%) | SLN + PLND | 48/456 (10,5%) | 51/71 (72%) | RFS OS |
NA NA |
Yes Yes |
No No |
| Stany et al. | 2015 | Retrospective | 129 | IA2-IB2 (FIGO 1988) | 26/129 (20%) | NA | NA | PLND | 19/103 (18,5%) | 10/26 (38%) | RFS, OS | No No |
NA | NA |
| Colturato et al. | 2016 | Retrospective | 83 | IB1-IIA (FIGO 2009) | 6/83 (7%) | NA | NA | PLND | 0/77 (0%) | 0/6 (0%) | RR | Yes | NA | NA |
| Guani et al. | 2019 | Prospective | 139 | IA1-IB1 (FIGO 2009) | 13/139 (9%) | 6/139 (4%) | 7/139 (5%) | SLN + PLND | NA | 4/13 (30%) | DFS | No | No | No |
| Nica et al. | 2019 | Prospective | 19 | IA1-IB3 (FIGO 2018) | NA | 9/19 (47%) | 10/19 (53%) | SLN or SLN+PLND |
NA | 14/19 (74%) | RFS | No | No | No |
| Kocian et al. | 2020 | Retrospective | 226 | IA1-IIB (FIGO 2009) | 24/226 (11%) | 8/226 (4%) | 16/226 (7%) | SLN or SLN+PLND |
NA | 17/24 (71%) | DFS OS |
NA NA |
Yes Yes |
No No |
| Buda et al. | 2020 | Retrospective | 573 | IA1-IB2 (FIGO 2018) | 21/573 (3,6%) | 4/573 (0,6%) | 17/573 (3%) | SLN or SLN+PLND |
NA | NA | DFS | No | No | No |
| Guani et al. | 2020 | Prospective | 321 | IA1-IB1 (FIGO 2009) | 24/321 (7%) | 24/321 (4%) | 11/321 (3%) | SLN or SLN+PLND |
NA | 13/24 (54%) | DFS | No | No | No |
| Dostalek et al. | 2023 | Retrospective | 967 | IA1-IIB (FIGO 2018) | 93/967 (10%) | 39/967 (4%) | 54/967 (6%) | SLN or SLN+PLND |
151/795 (19%) | 71/93 (76%) | DFS | NA | Yes | Yes |
RR: Risk of Recurrence, DFS: Disease Free Survival, RFS: Recurrence Free Survival, OS: Overall Survival.
* compared to negative nodal status
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



